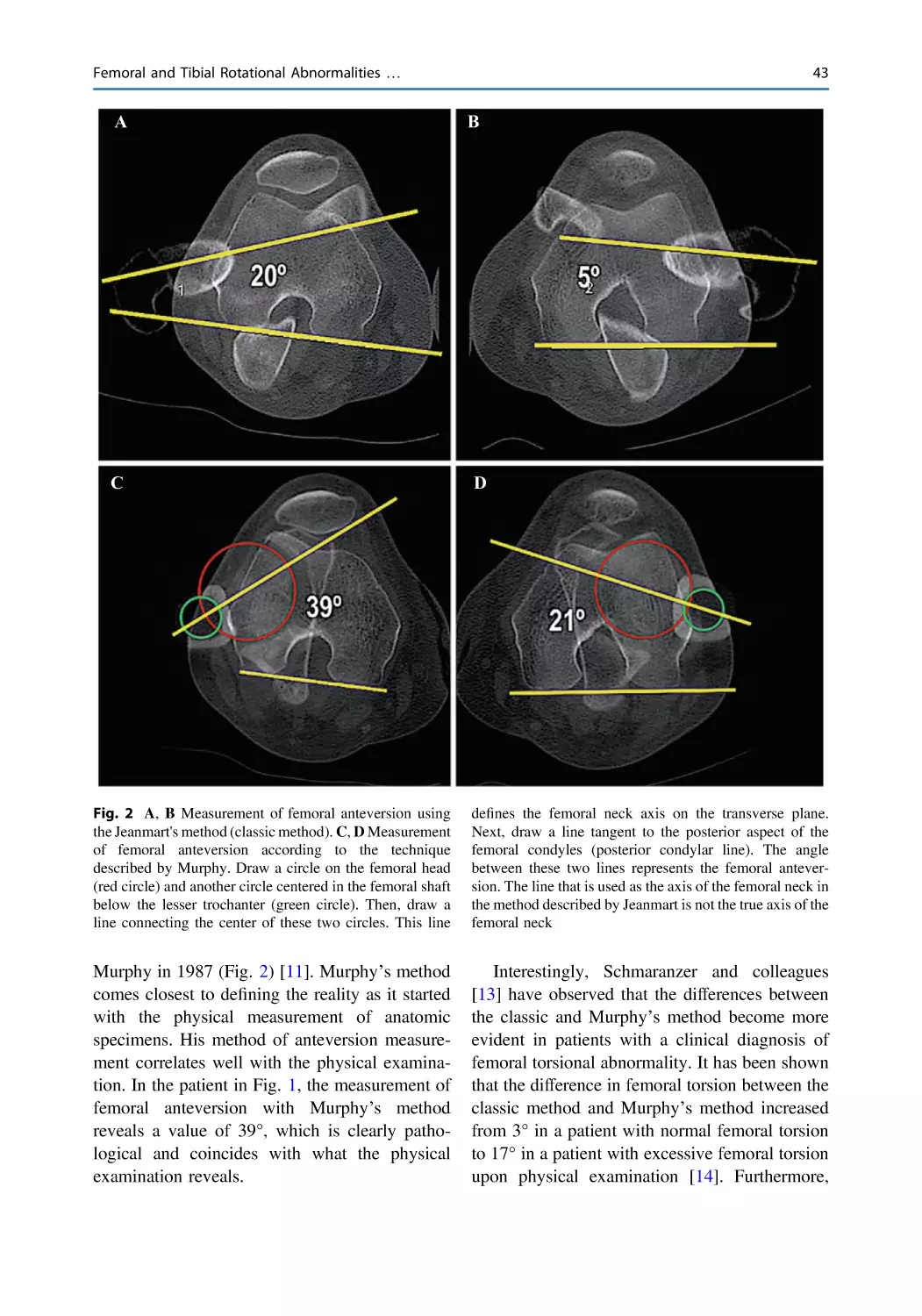
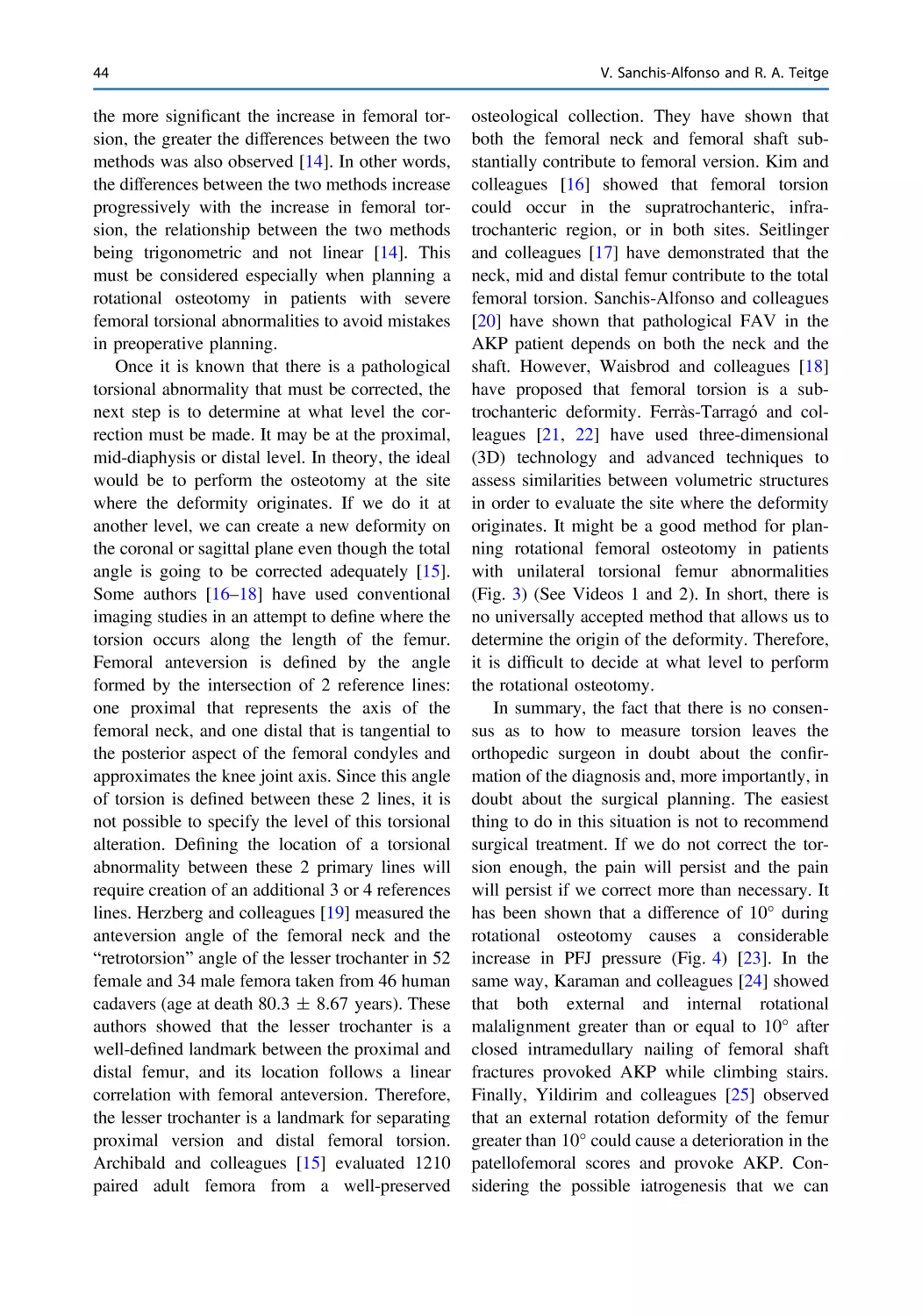
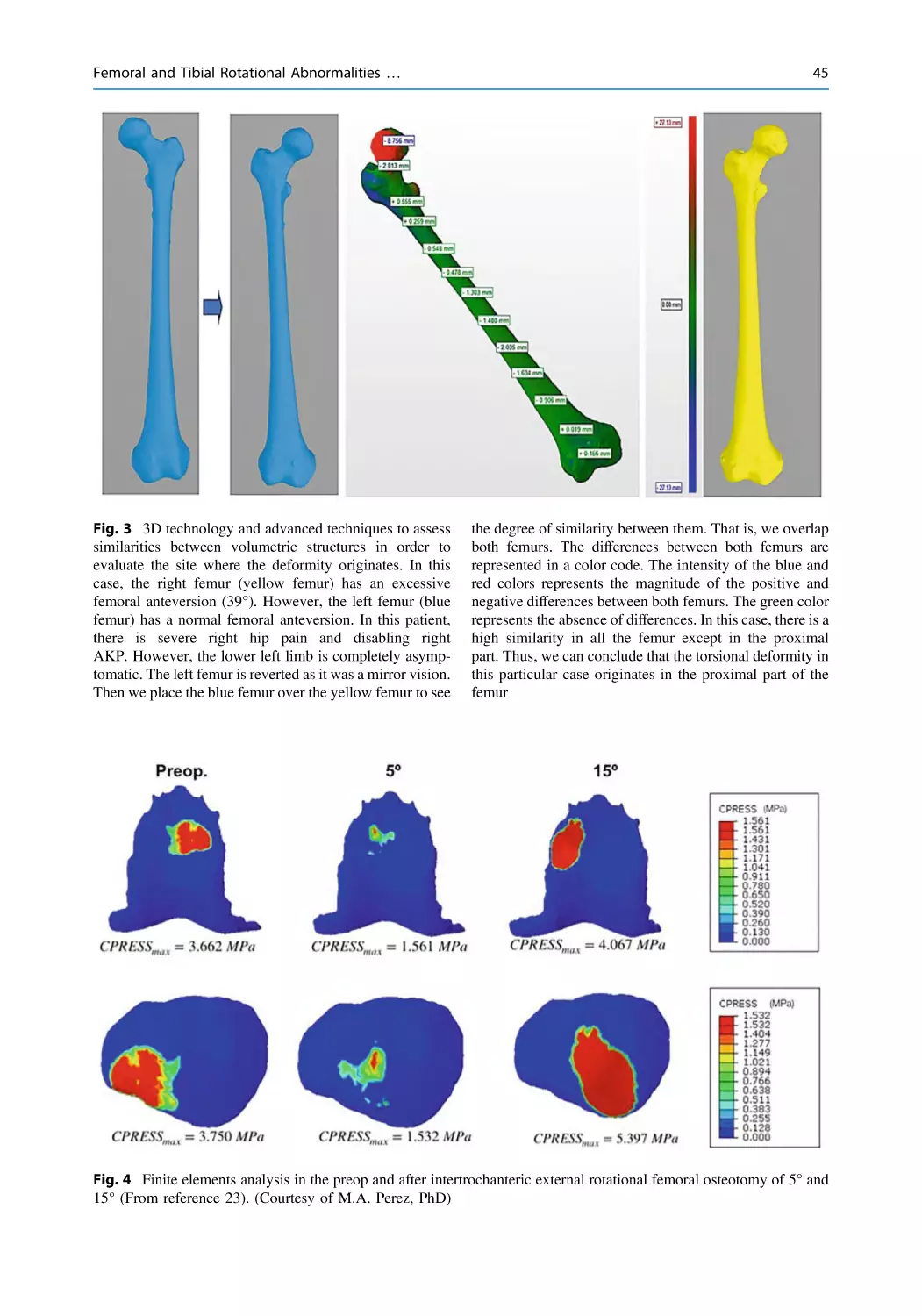
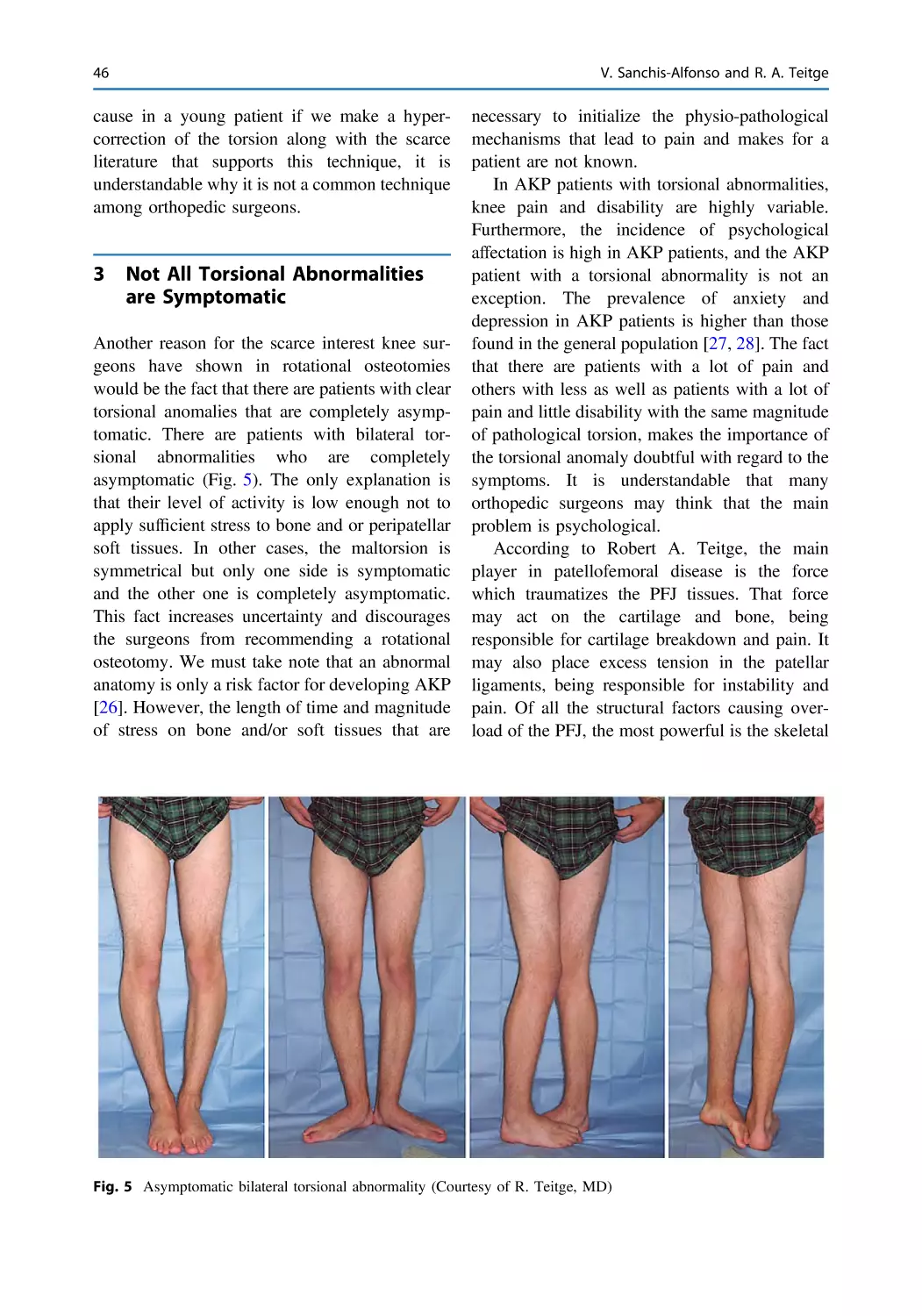
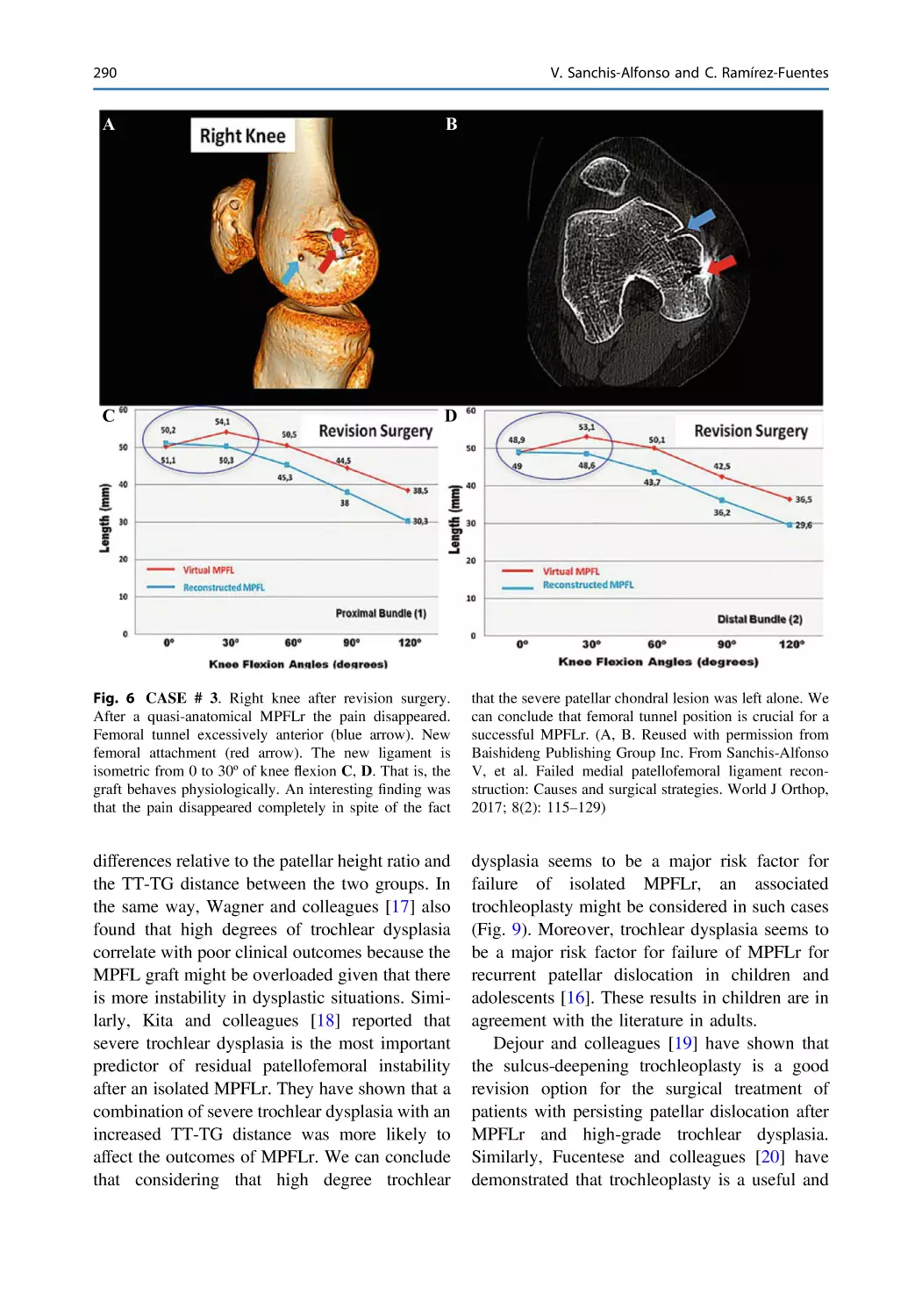
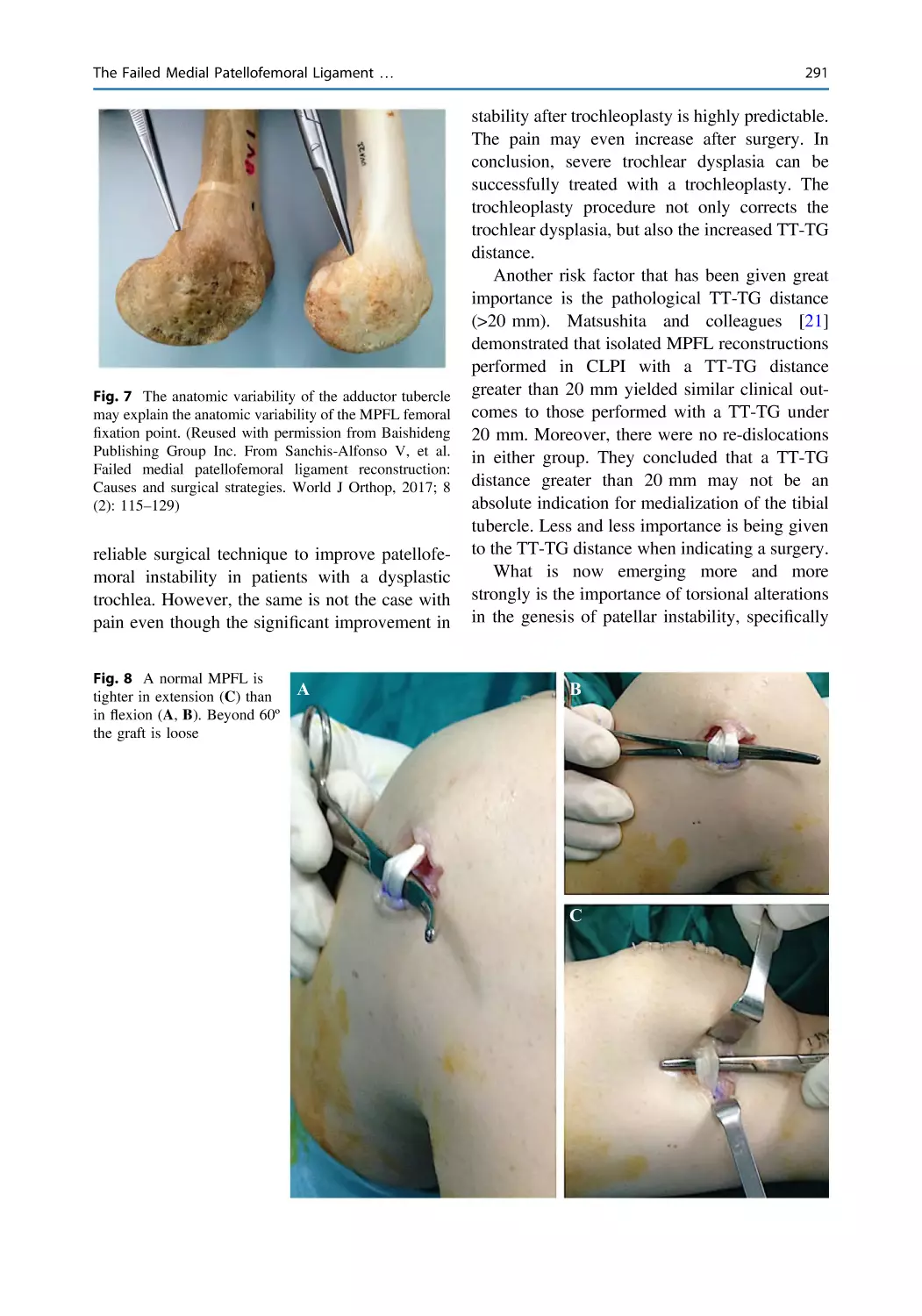
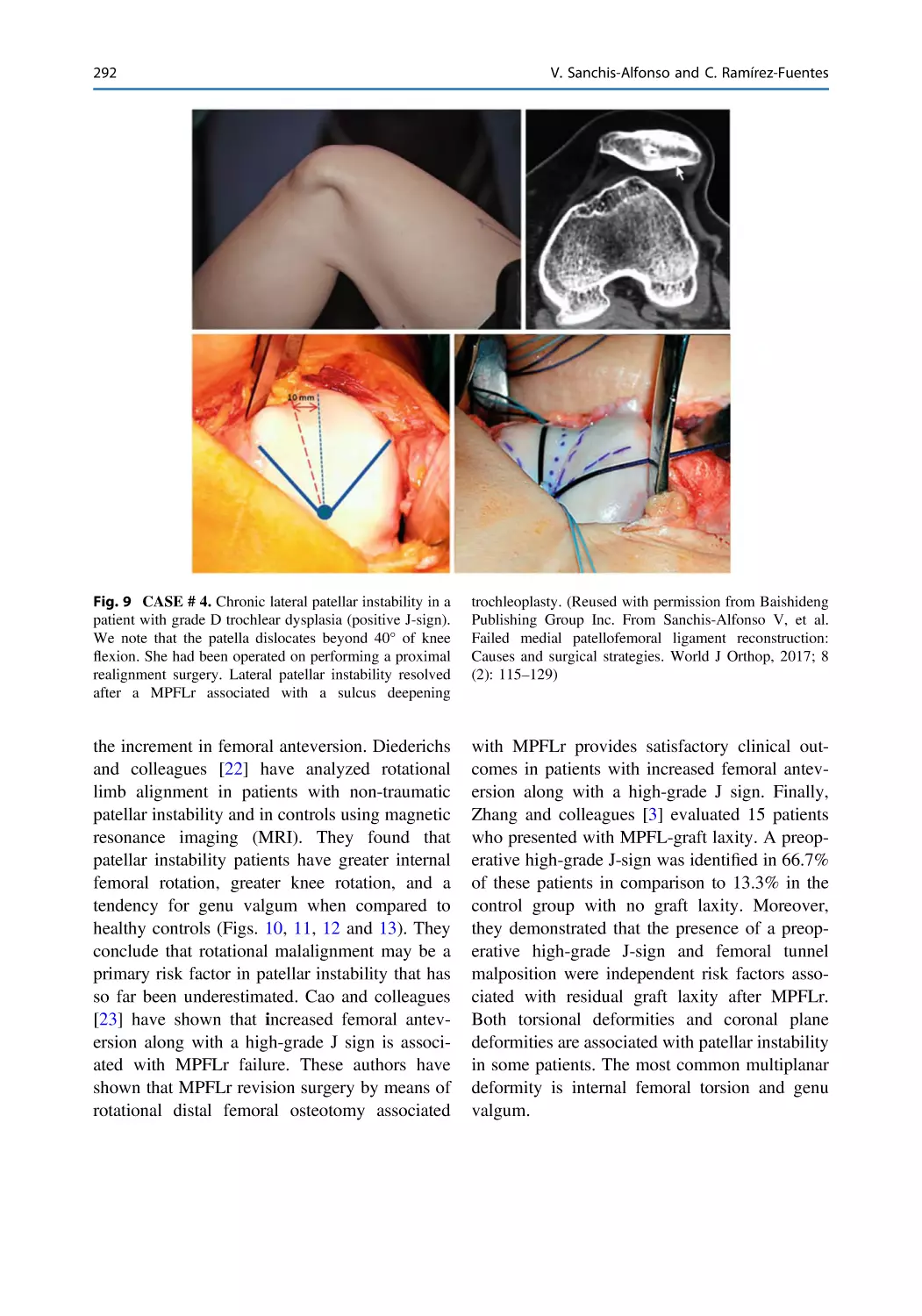
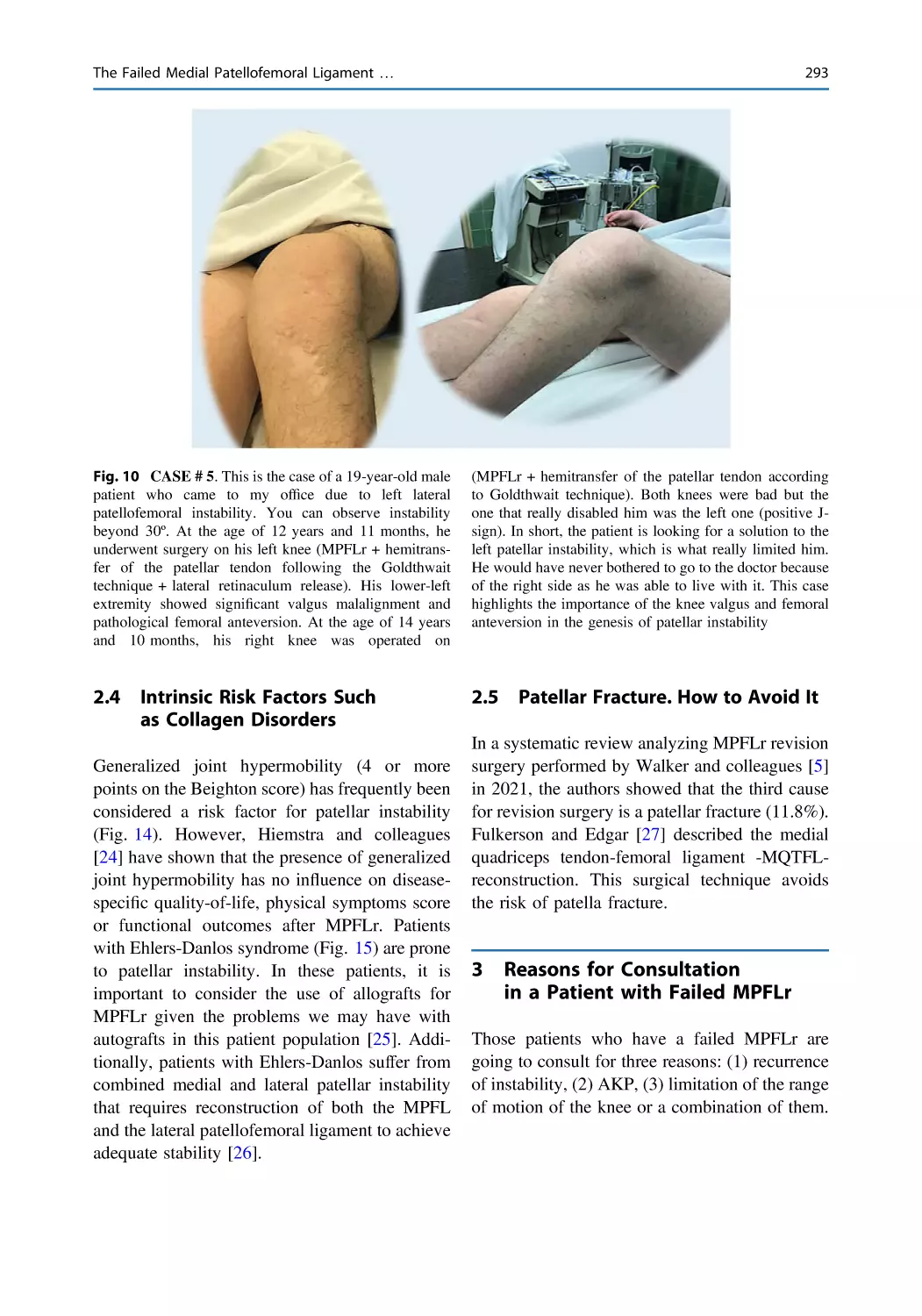
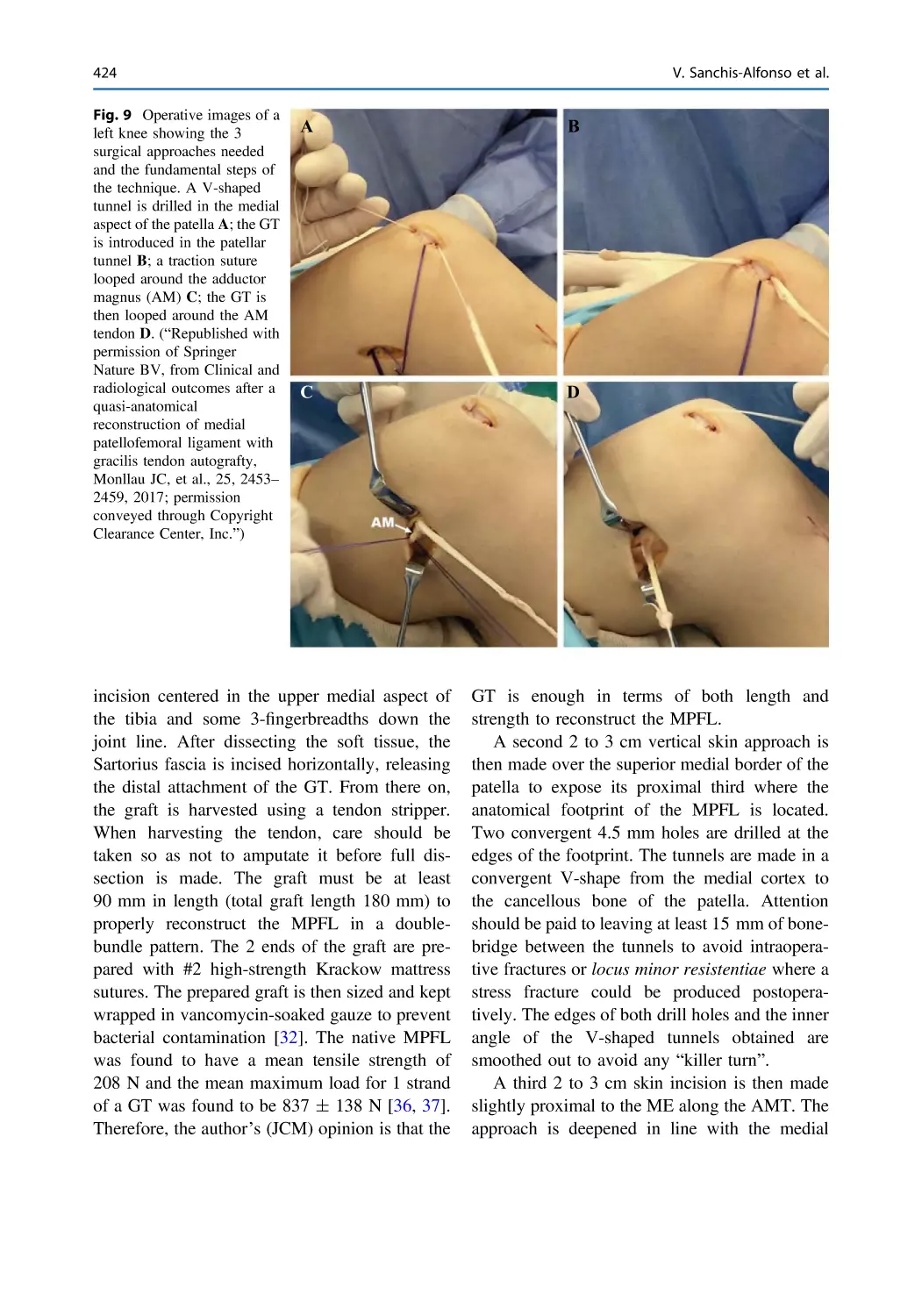
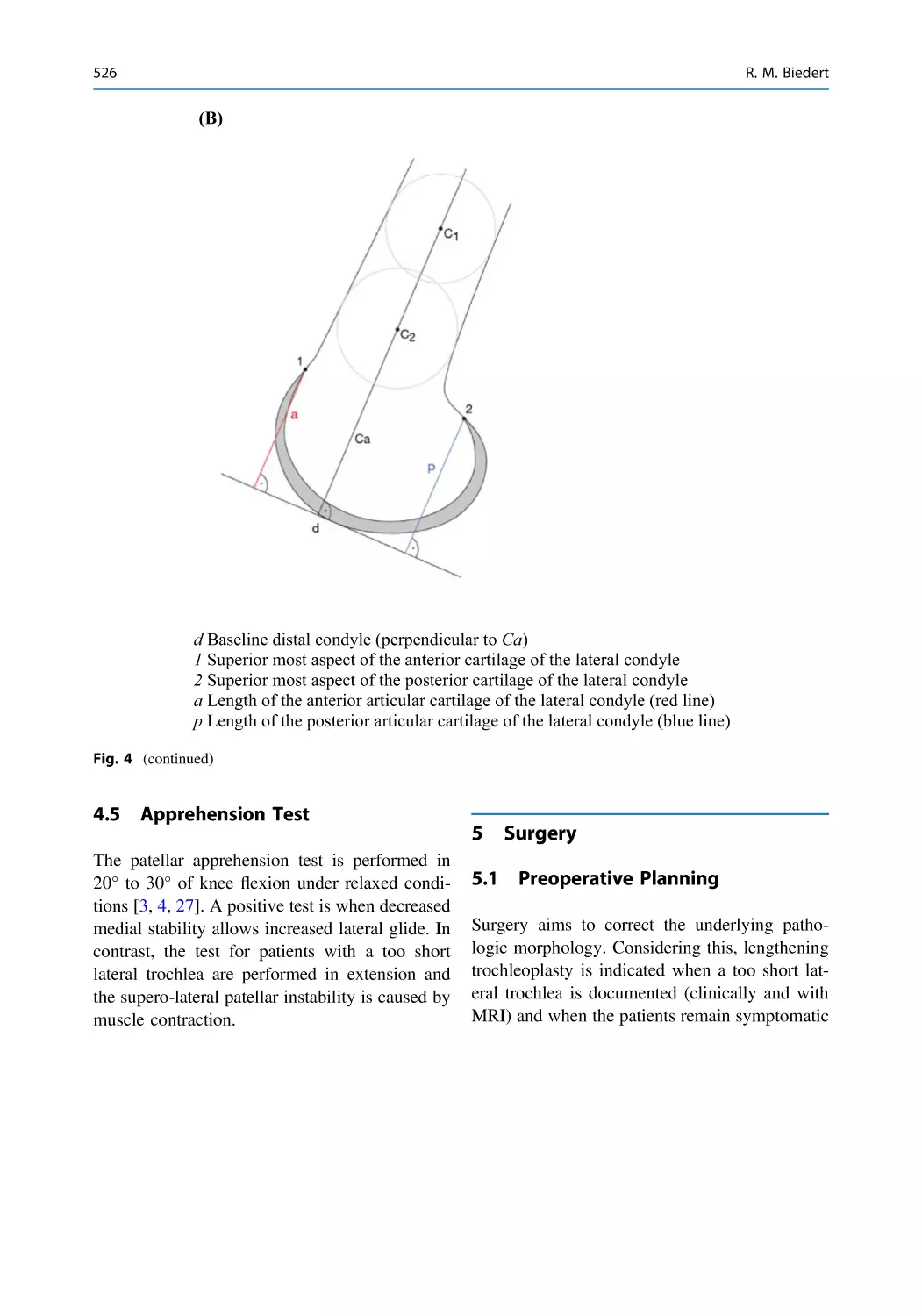
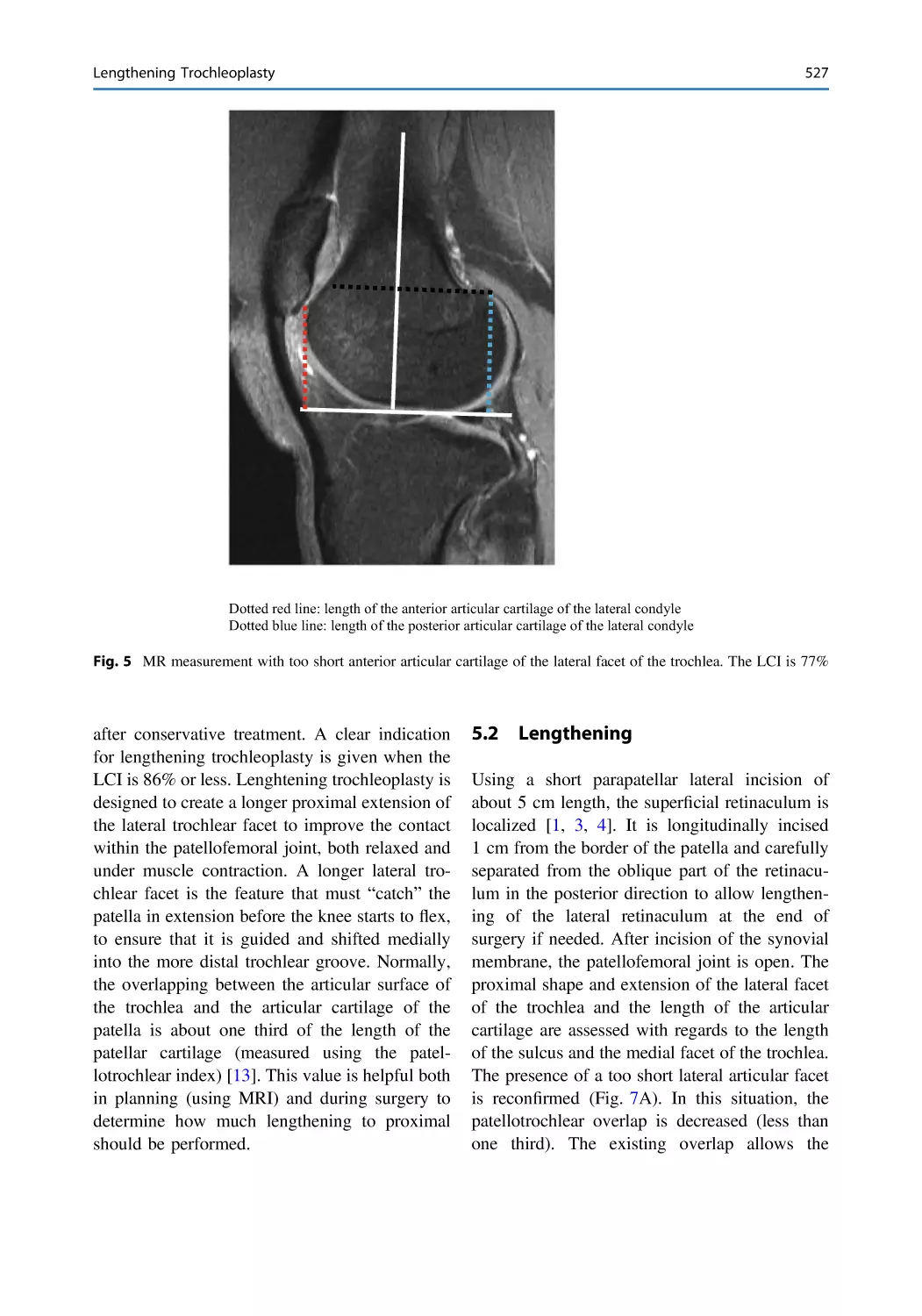
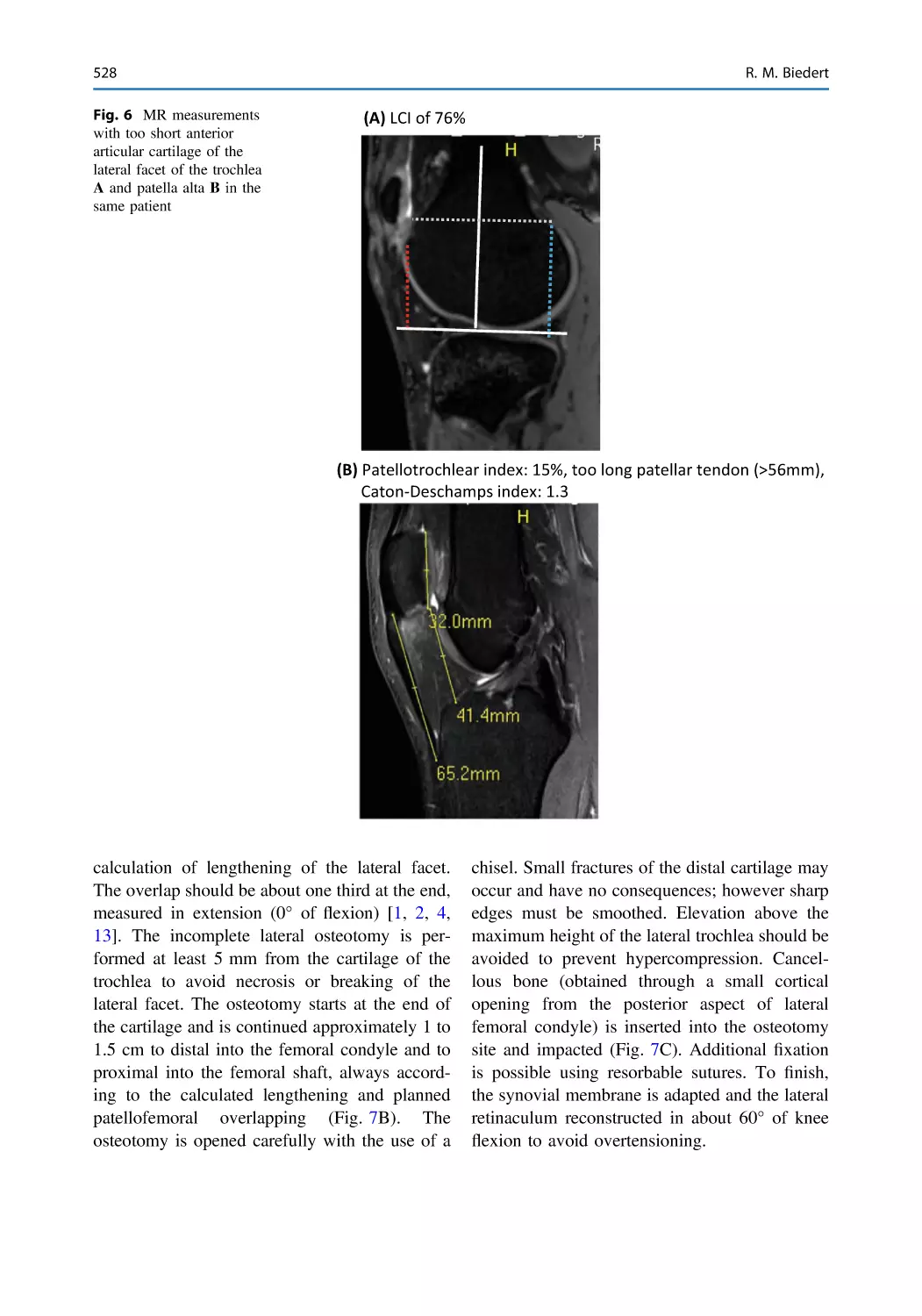
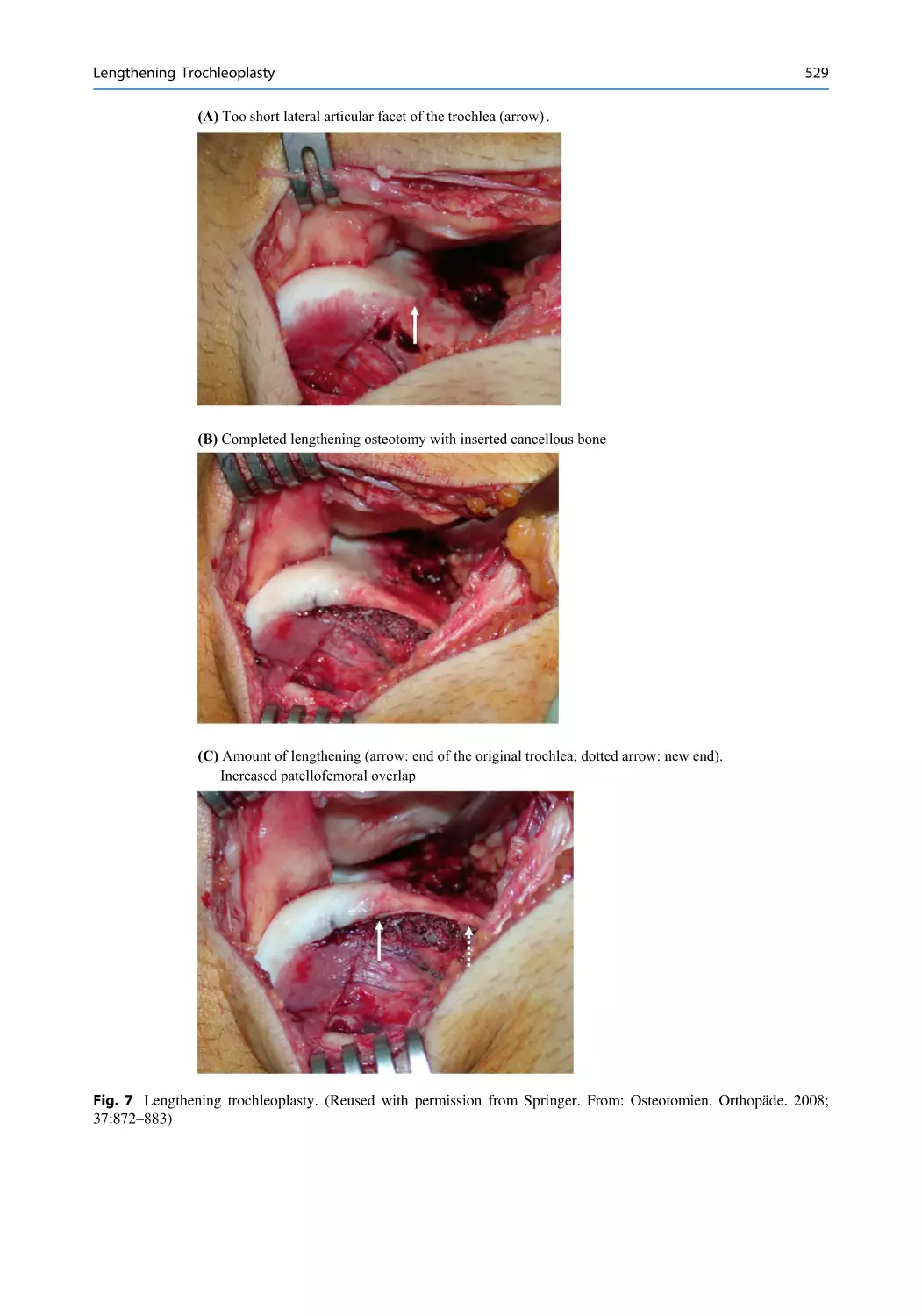
/





















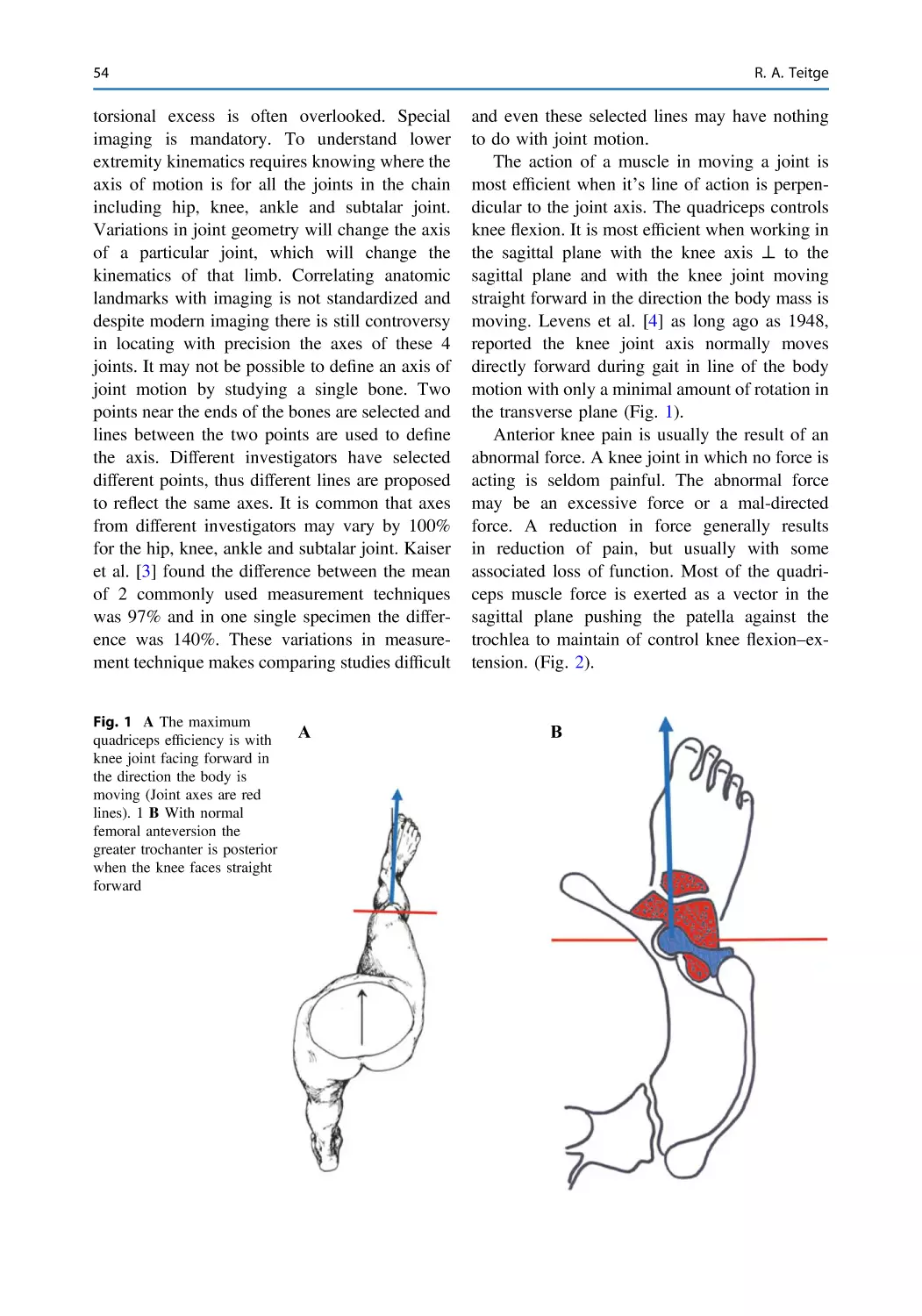










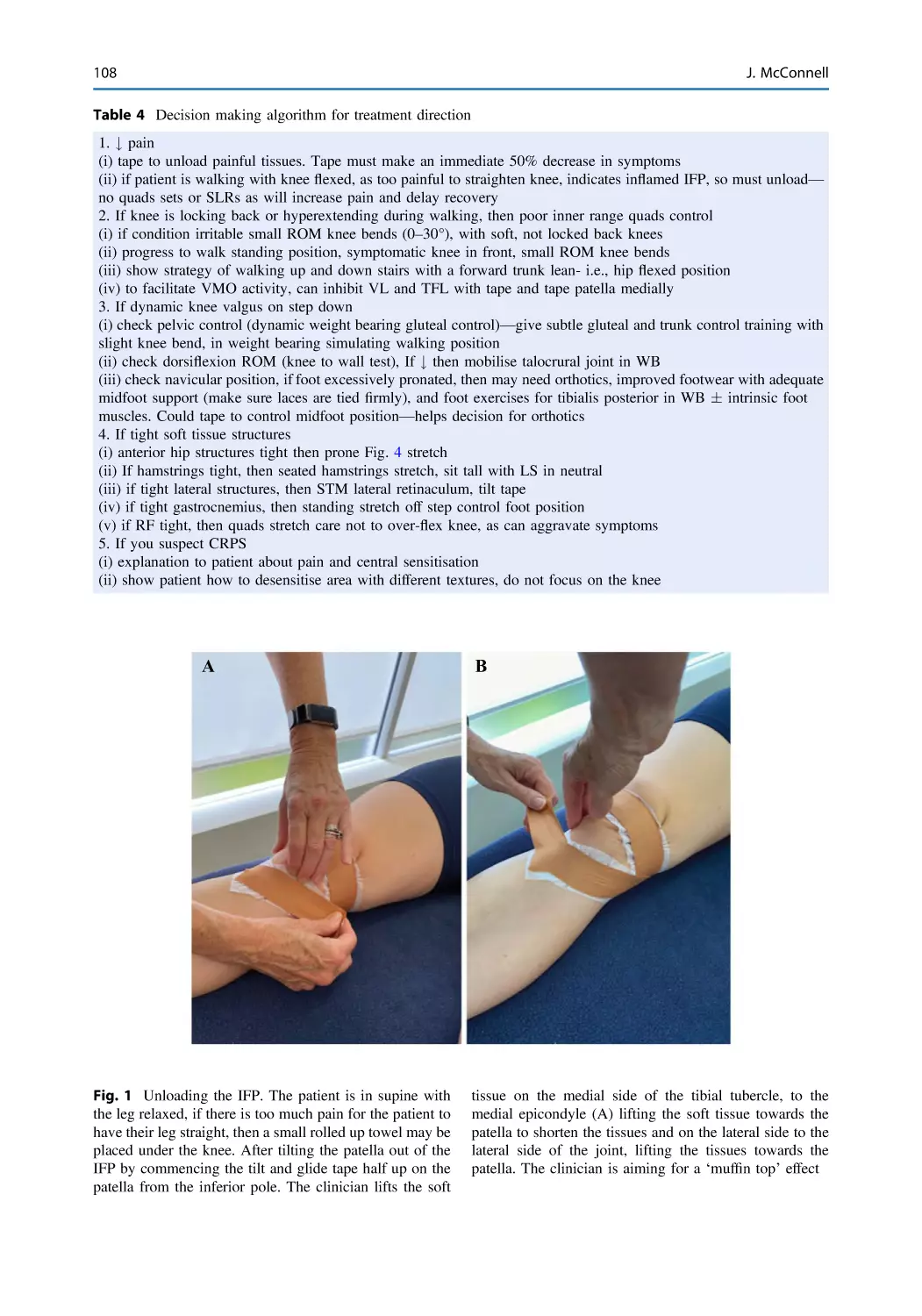


















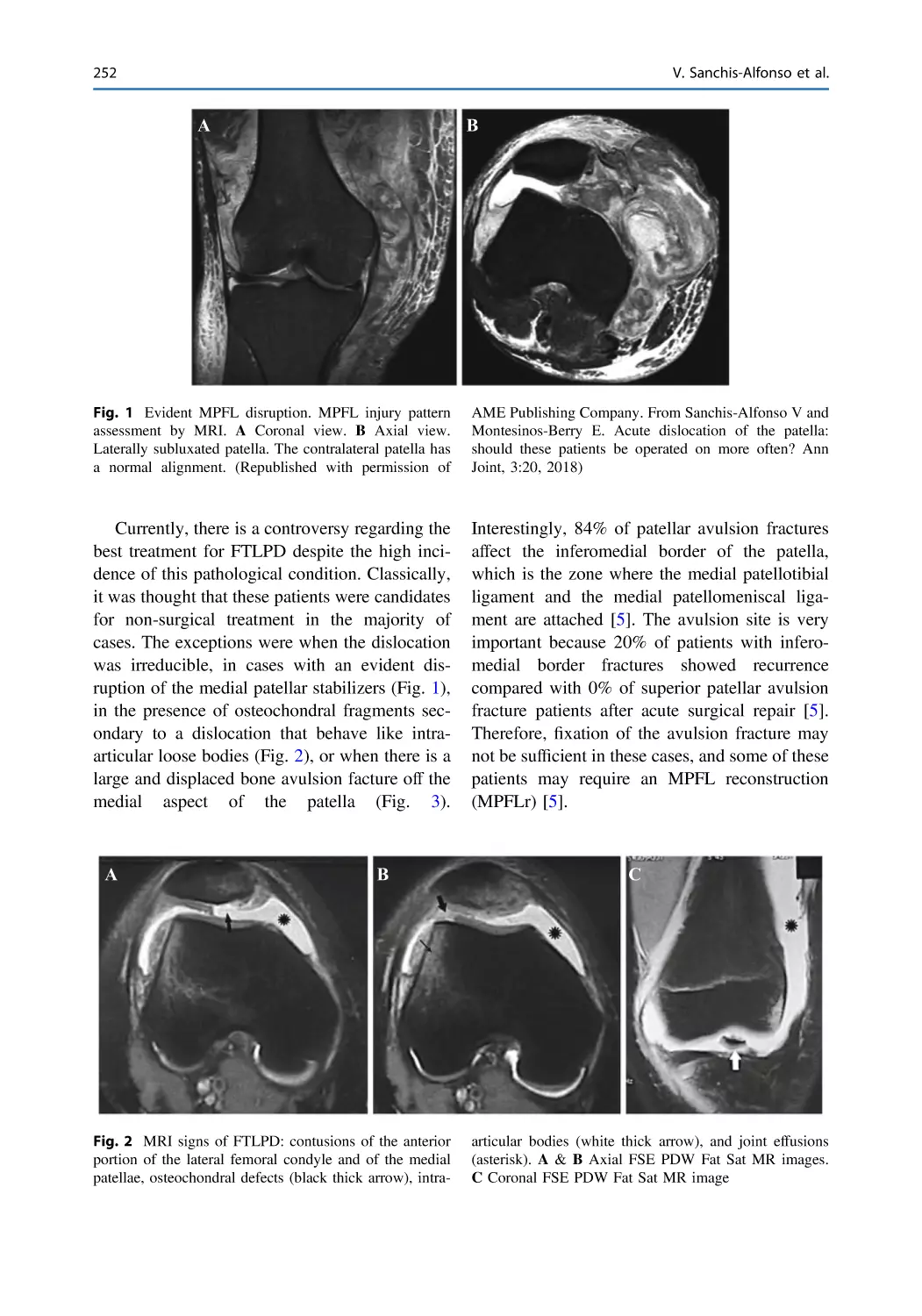





































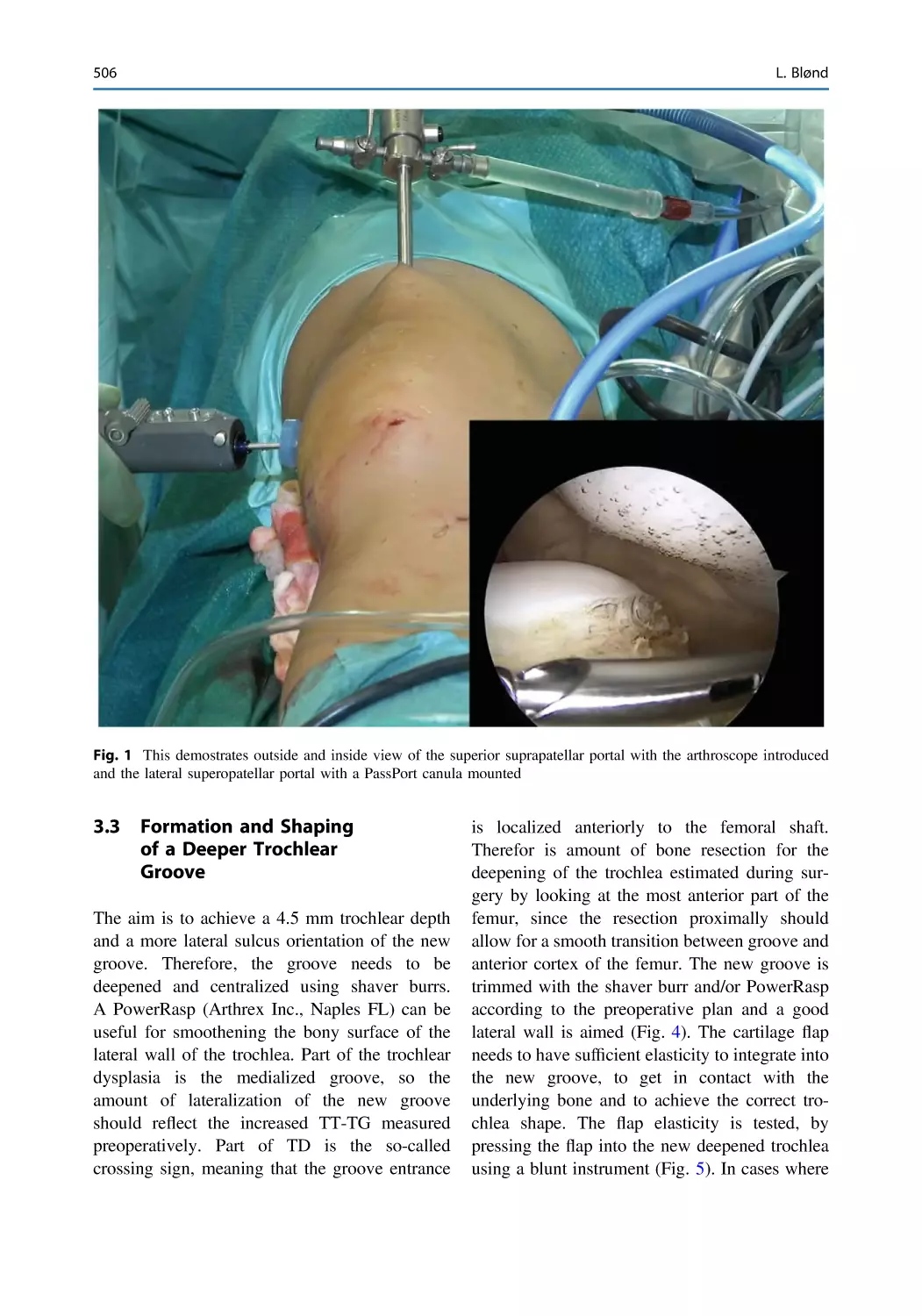






















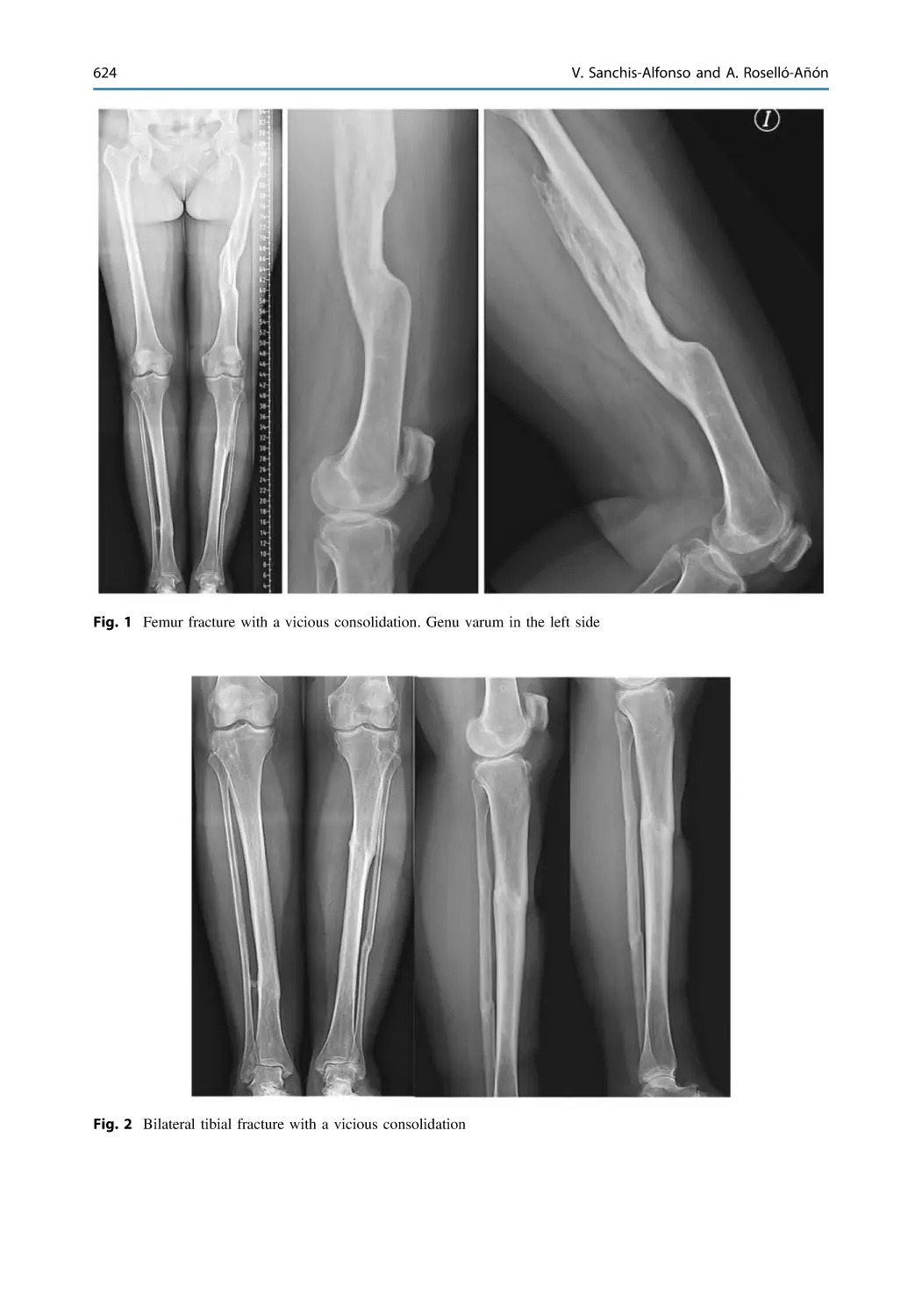




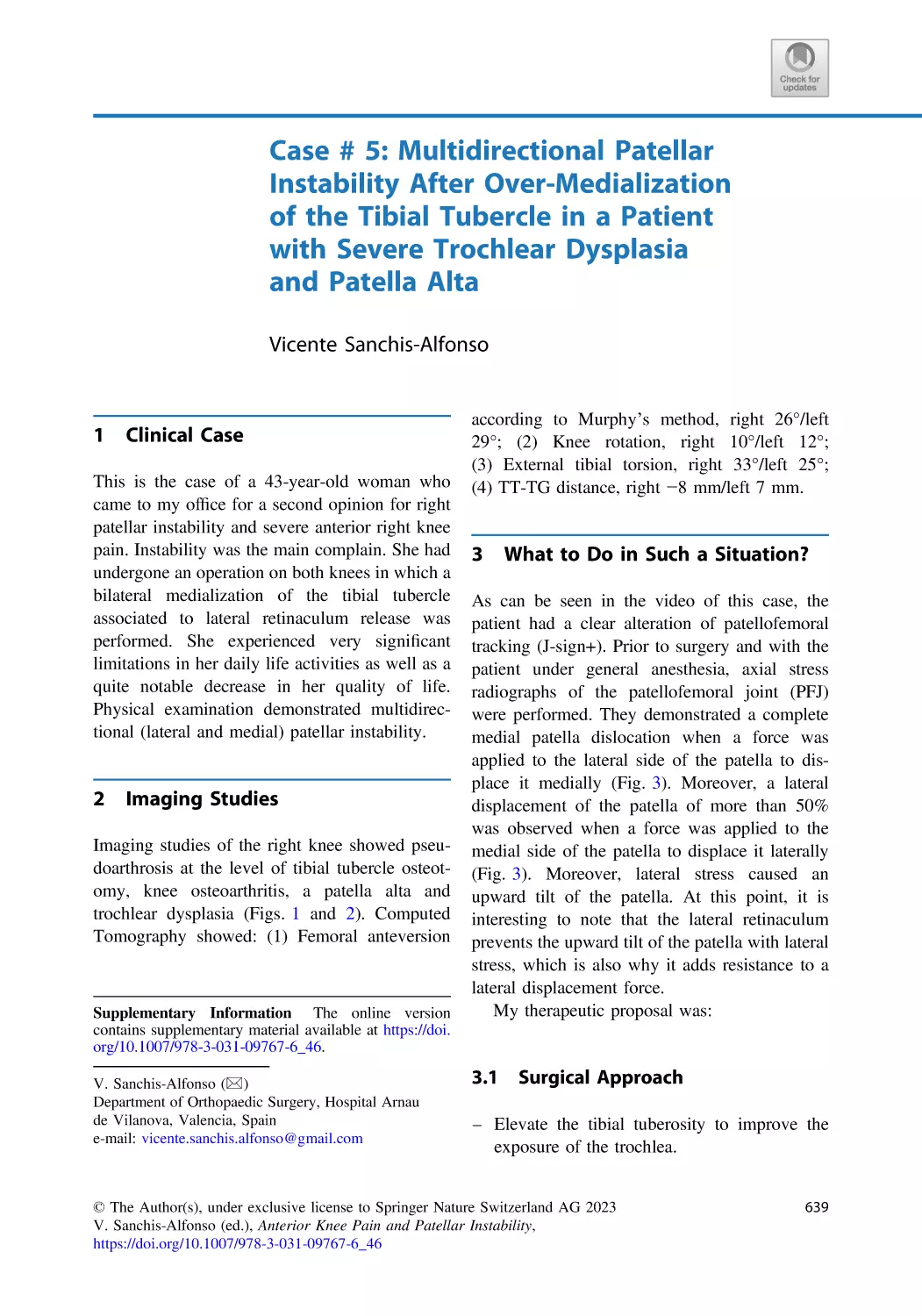






























Author: Sanchis-Alfonso V.
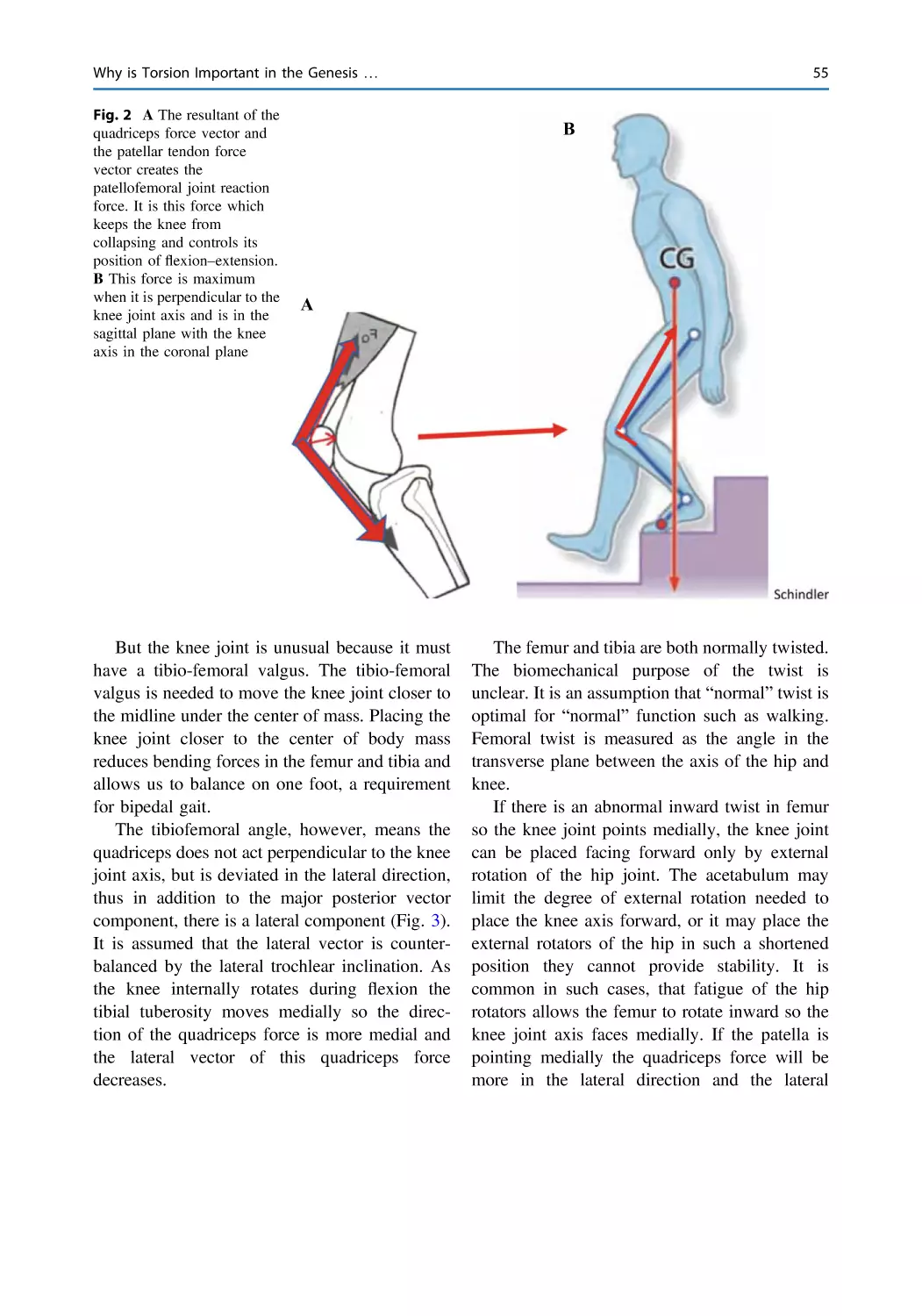
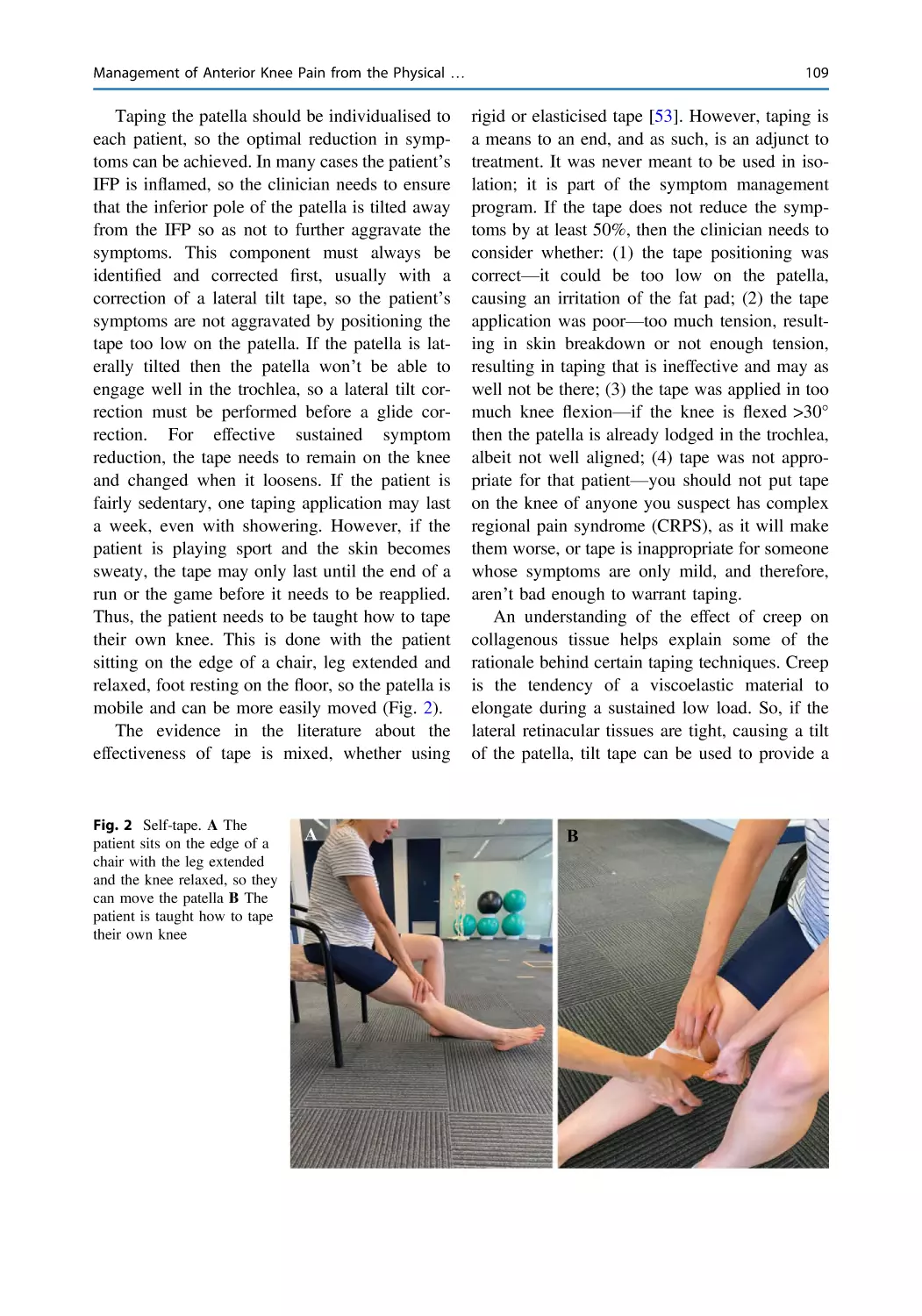
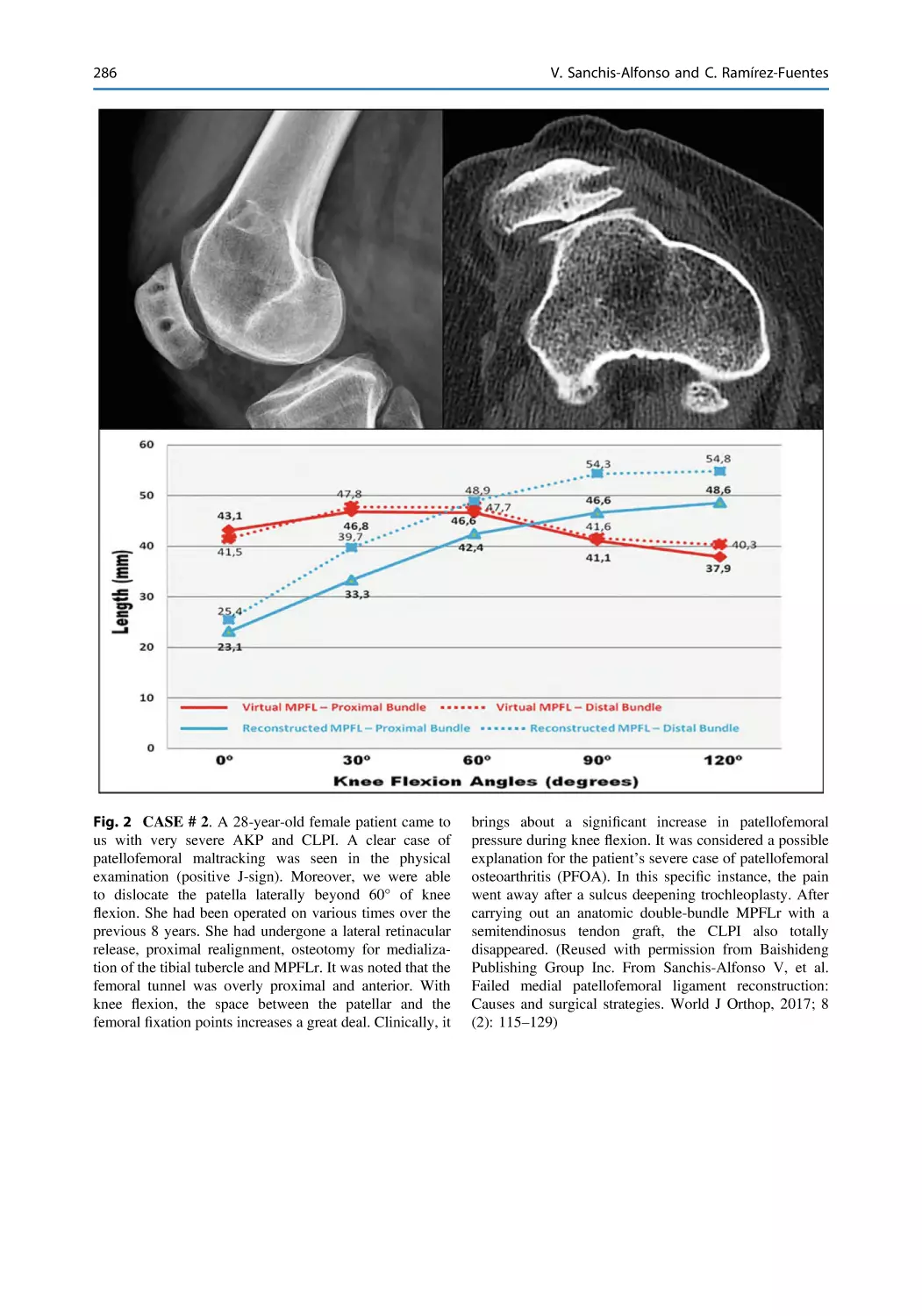
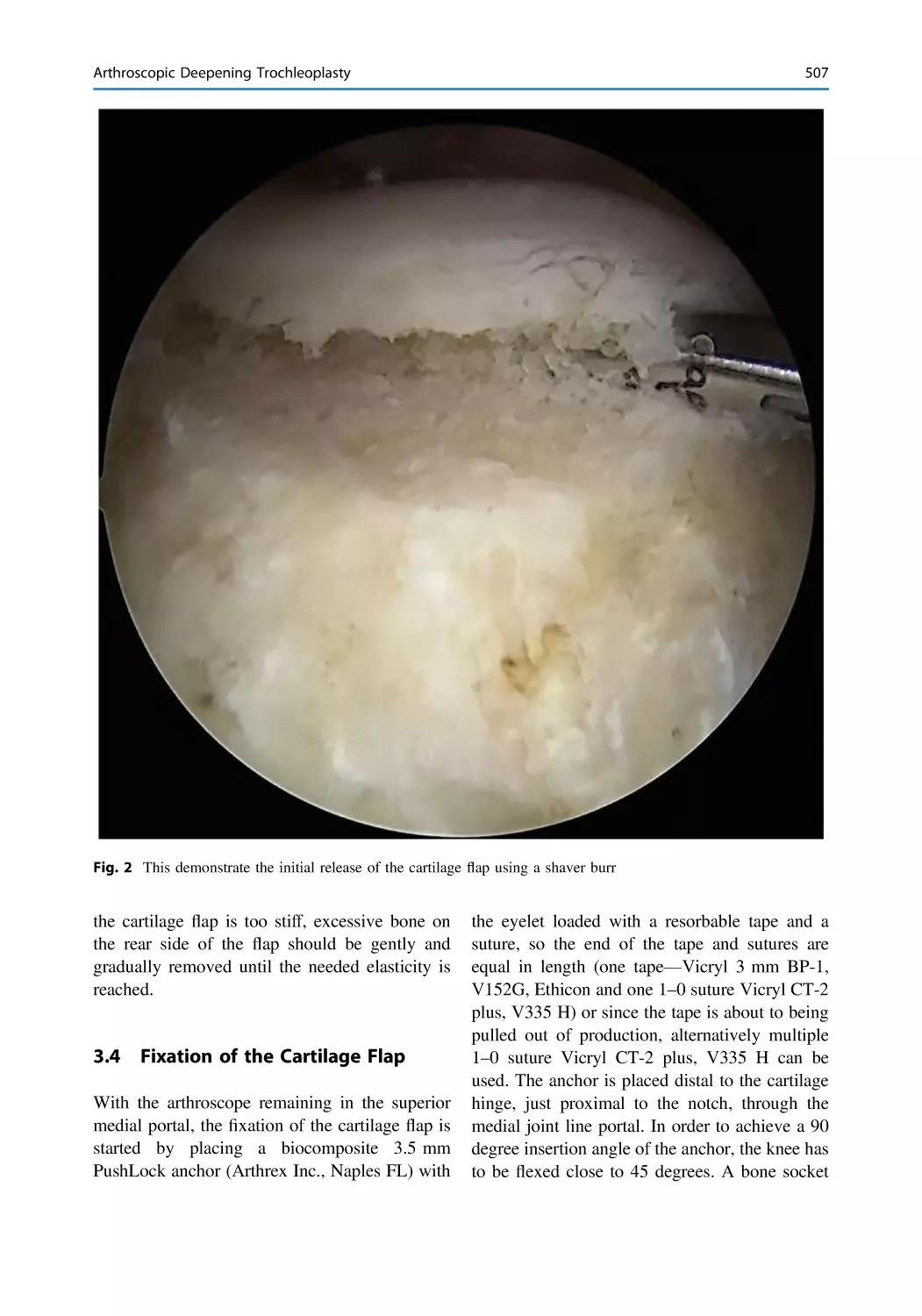
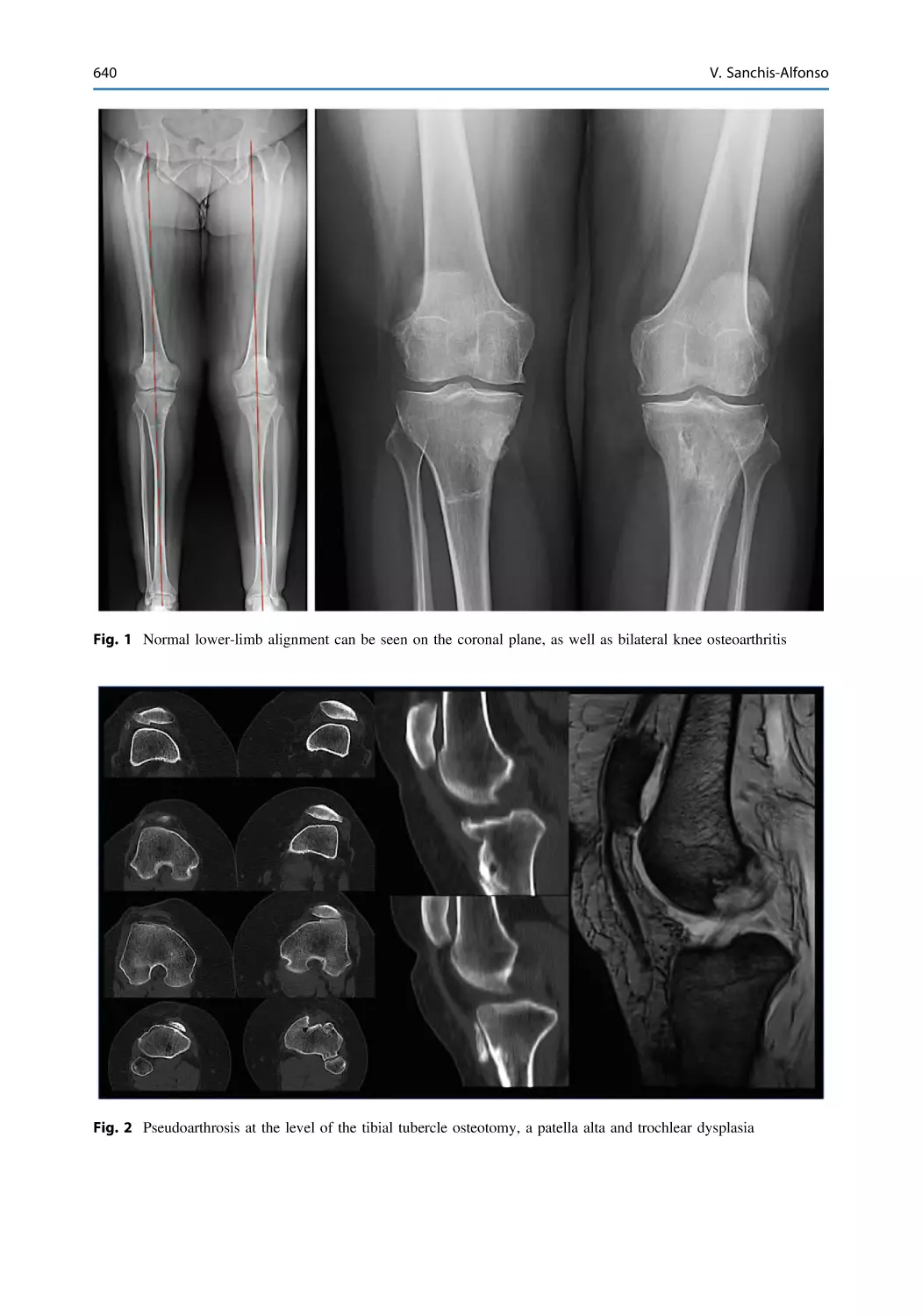
Tags: medicine physiology practical medicine human physiology
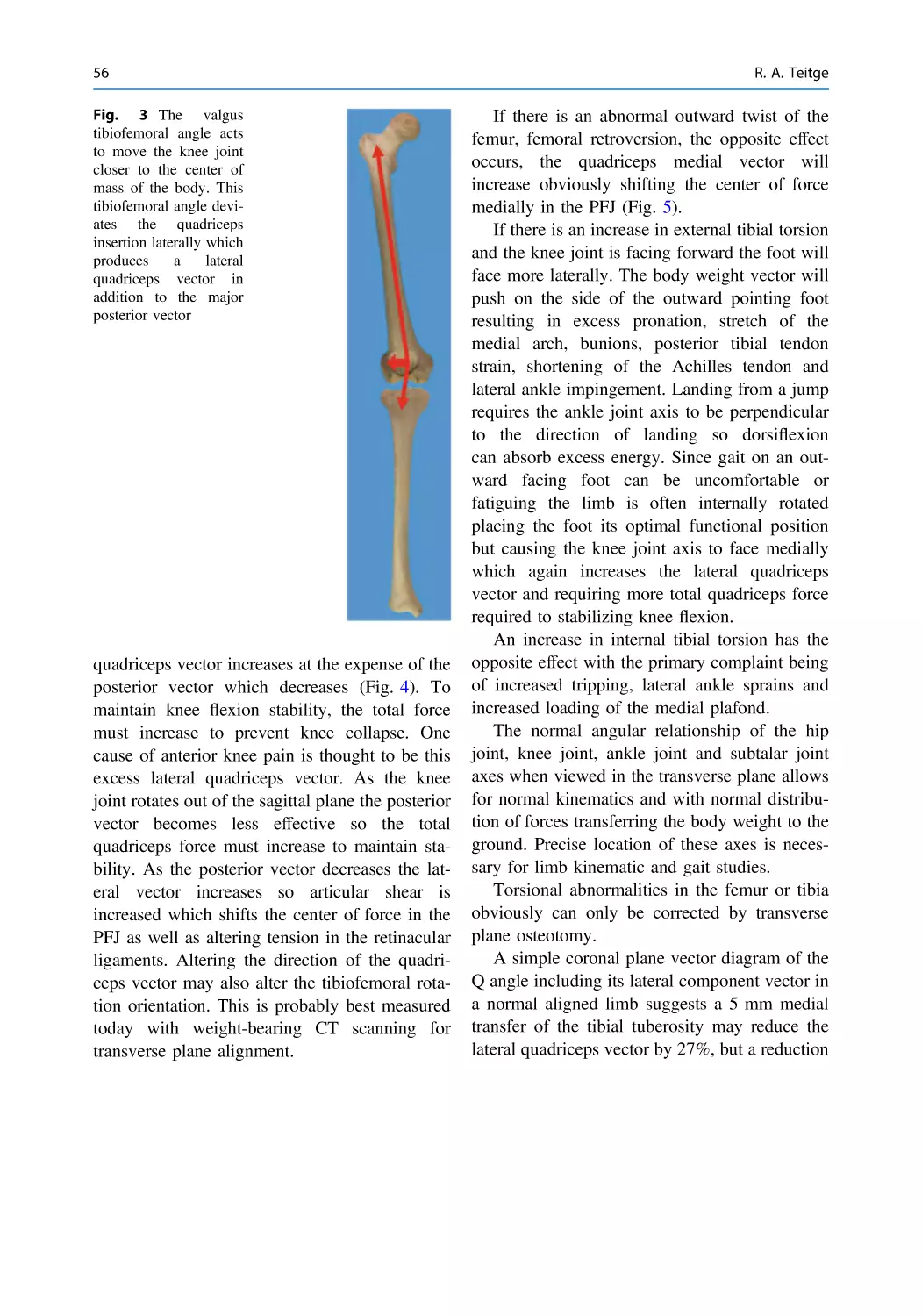
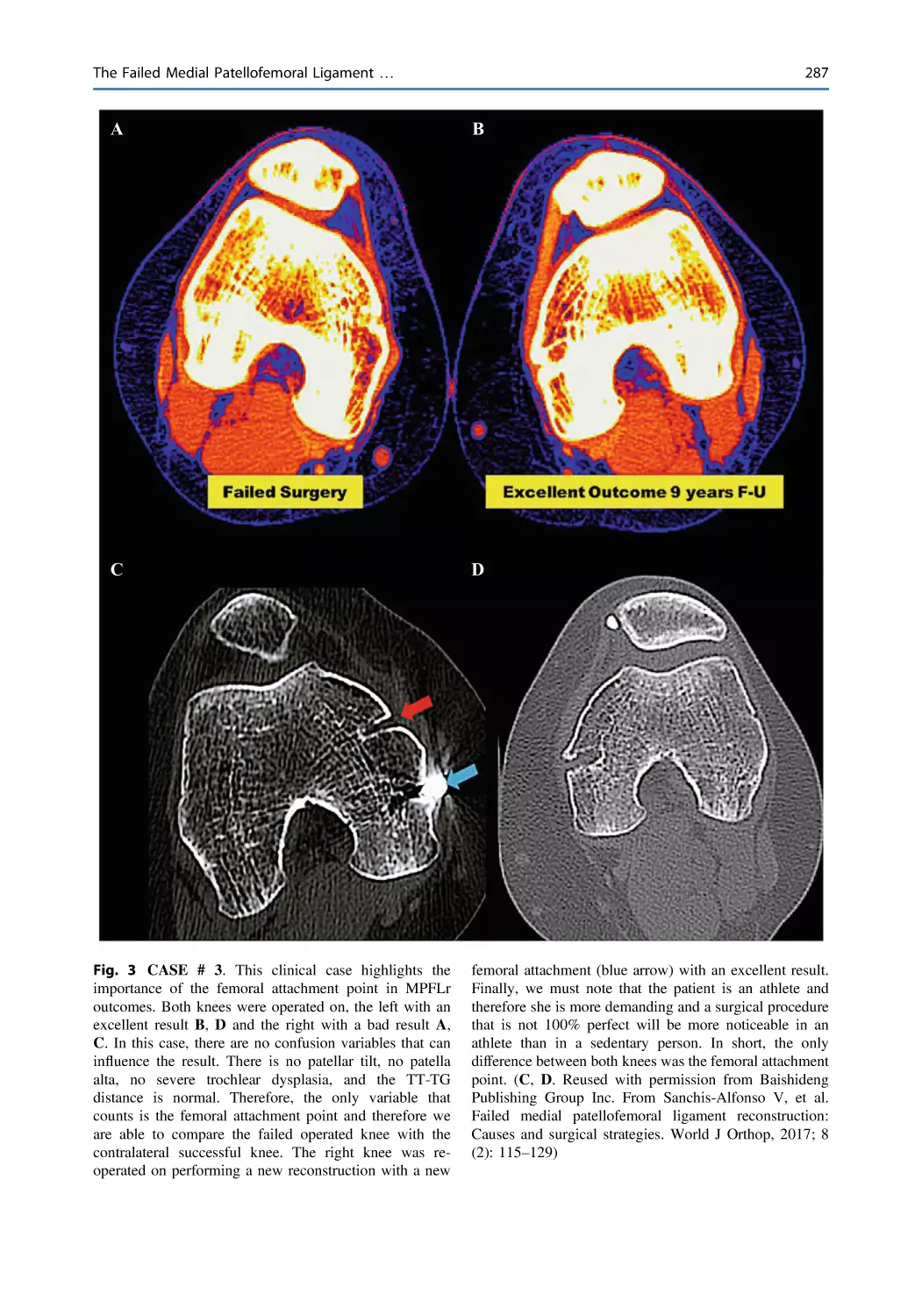
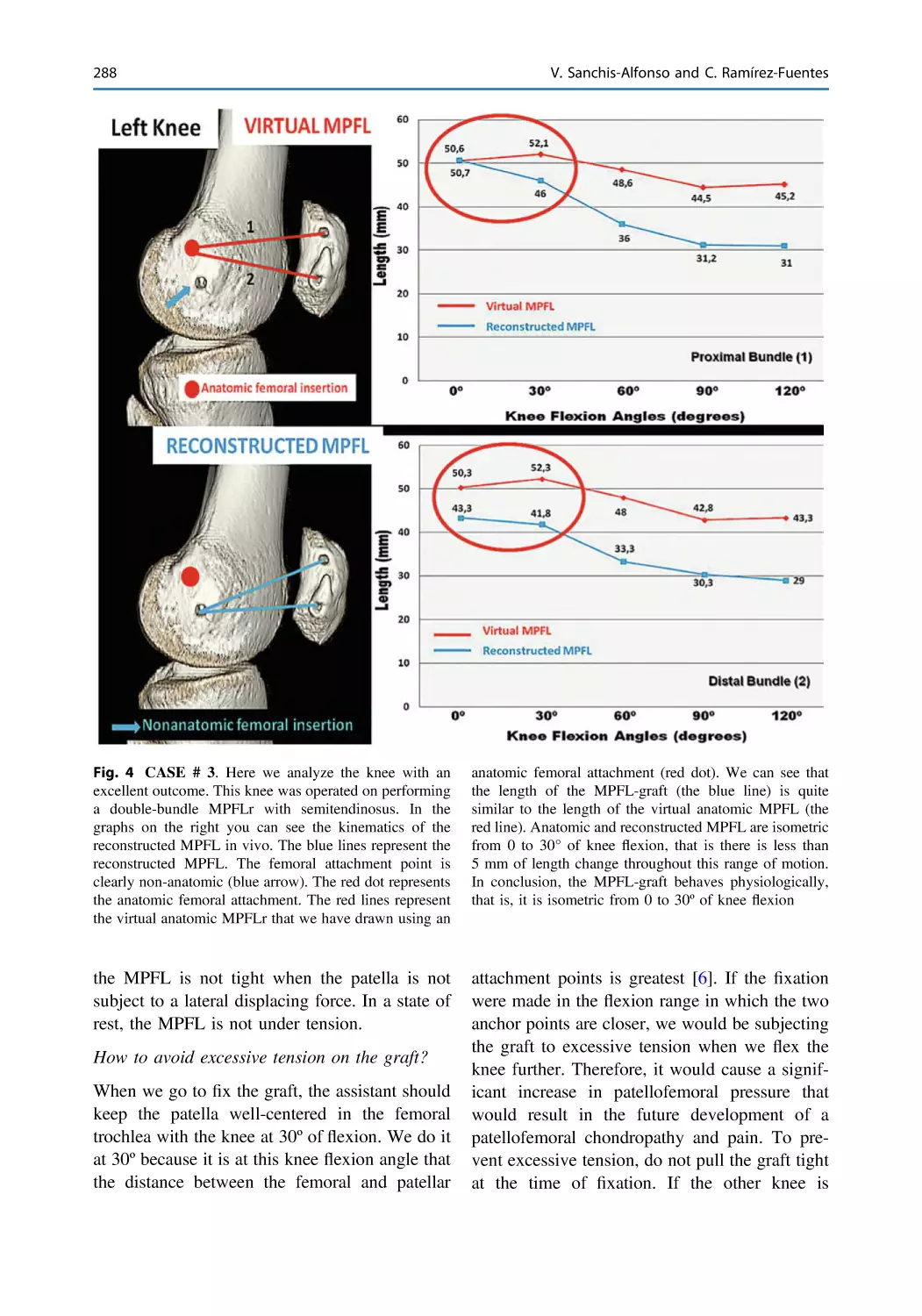
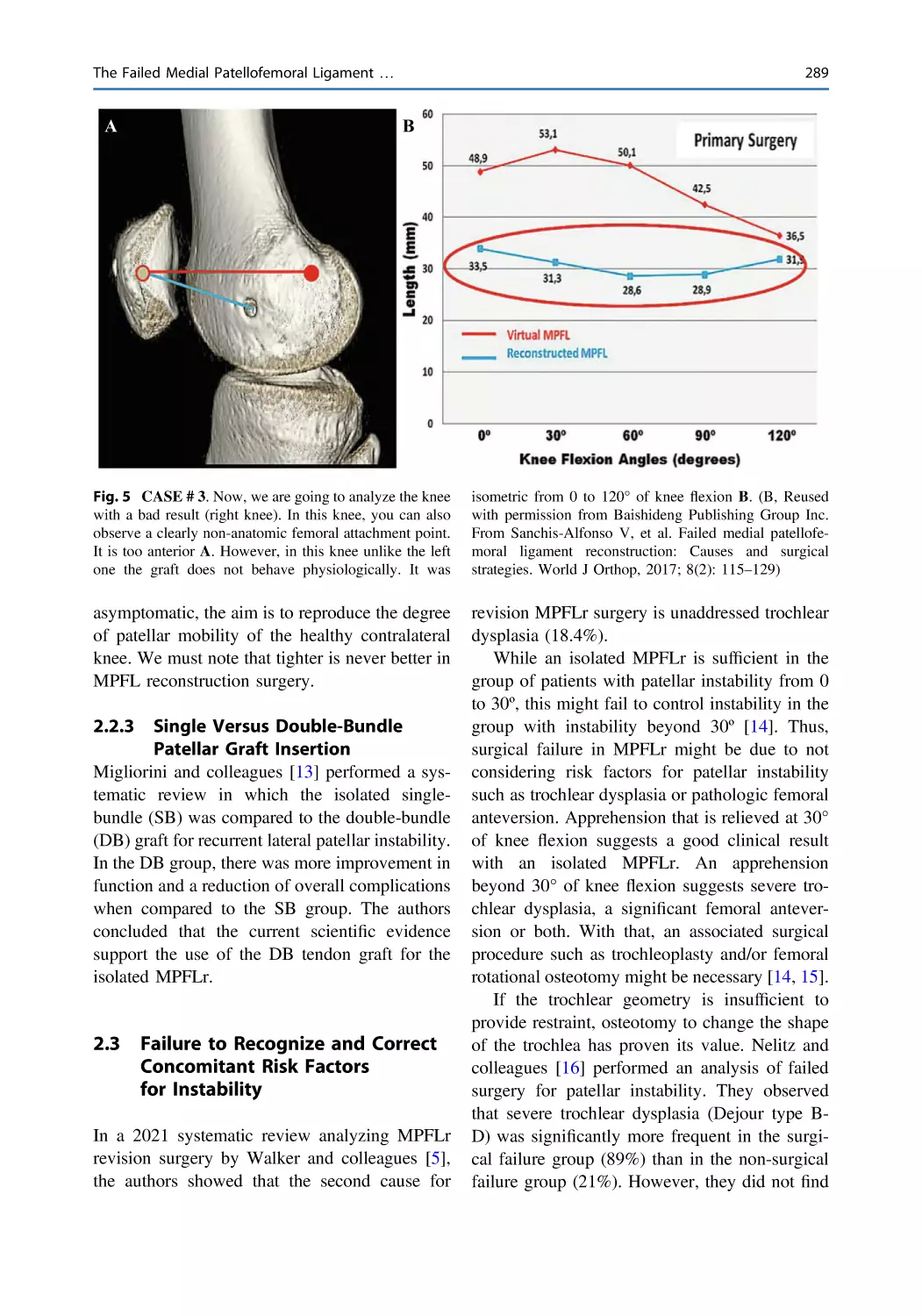
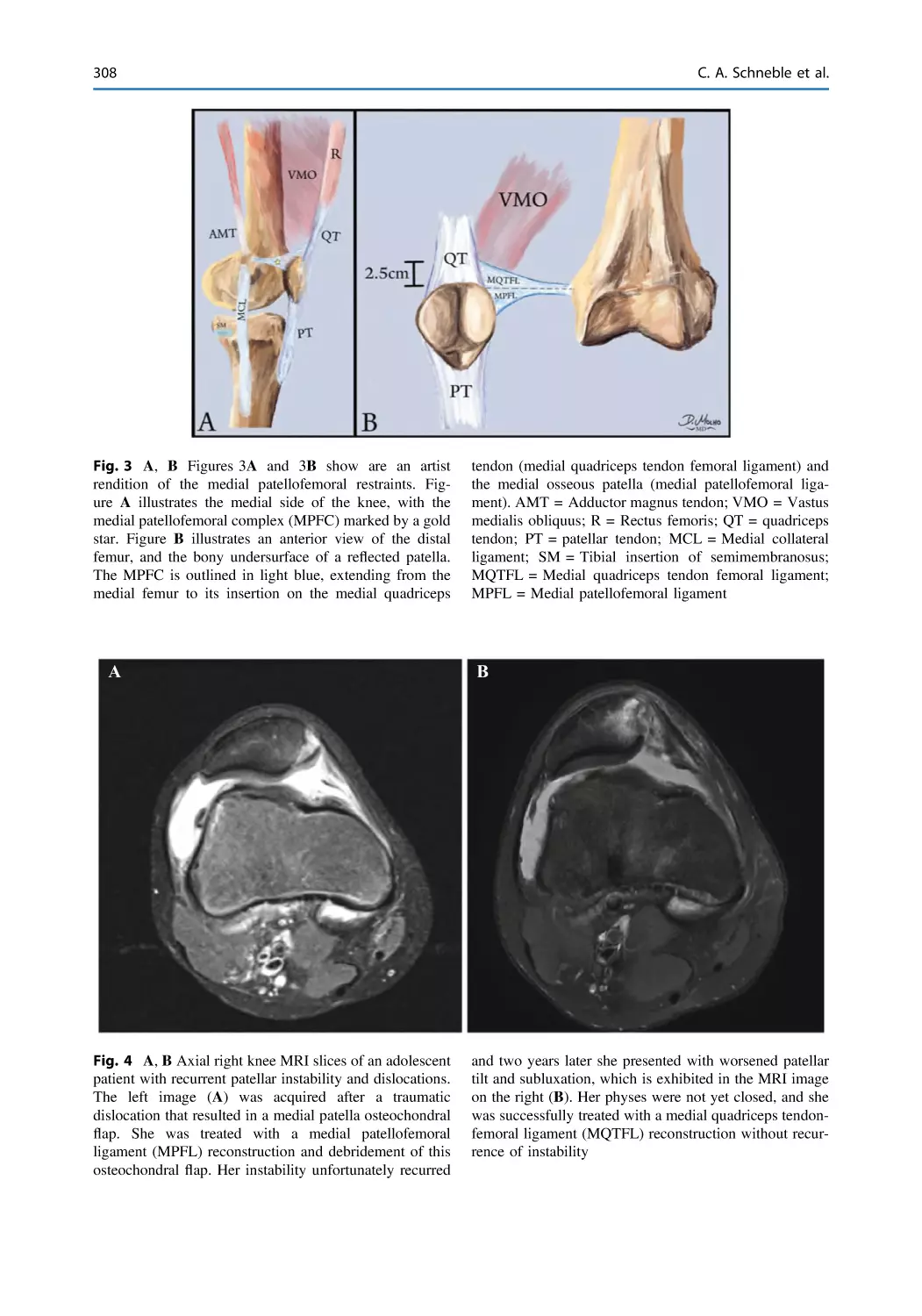
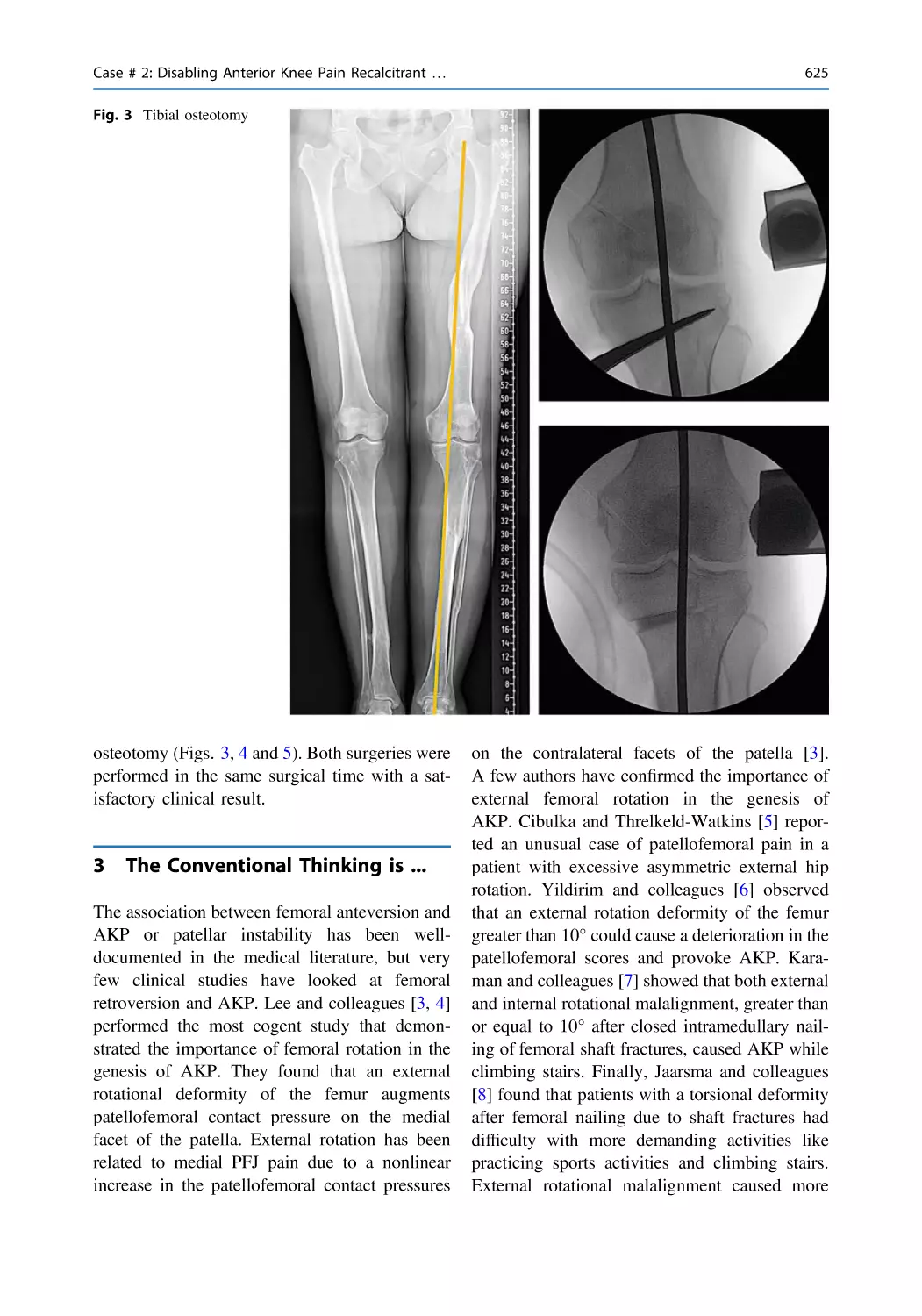
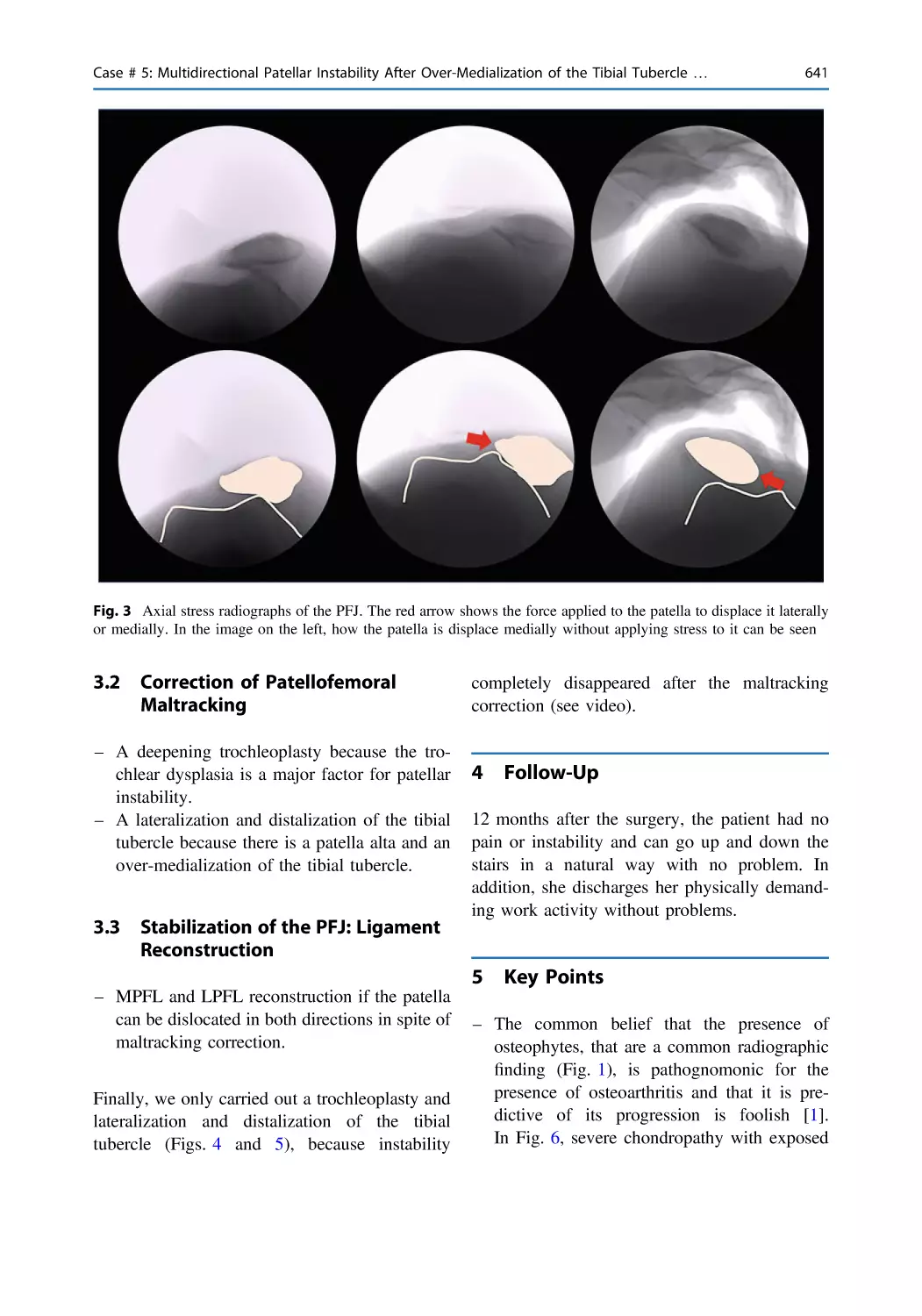
ISBN: 978-3-031-09766-9
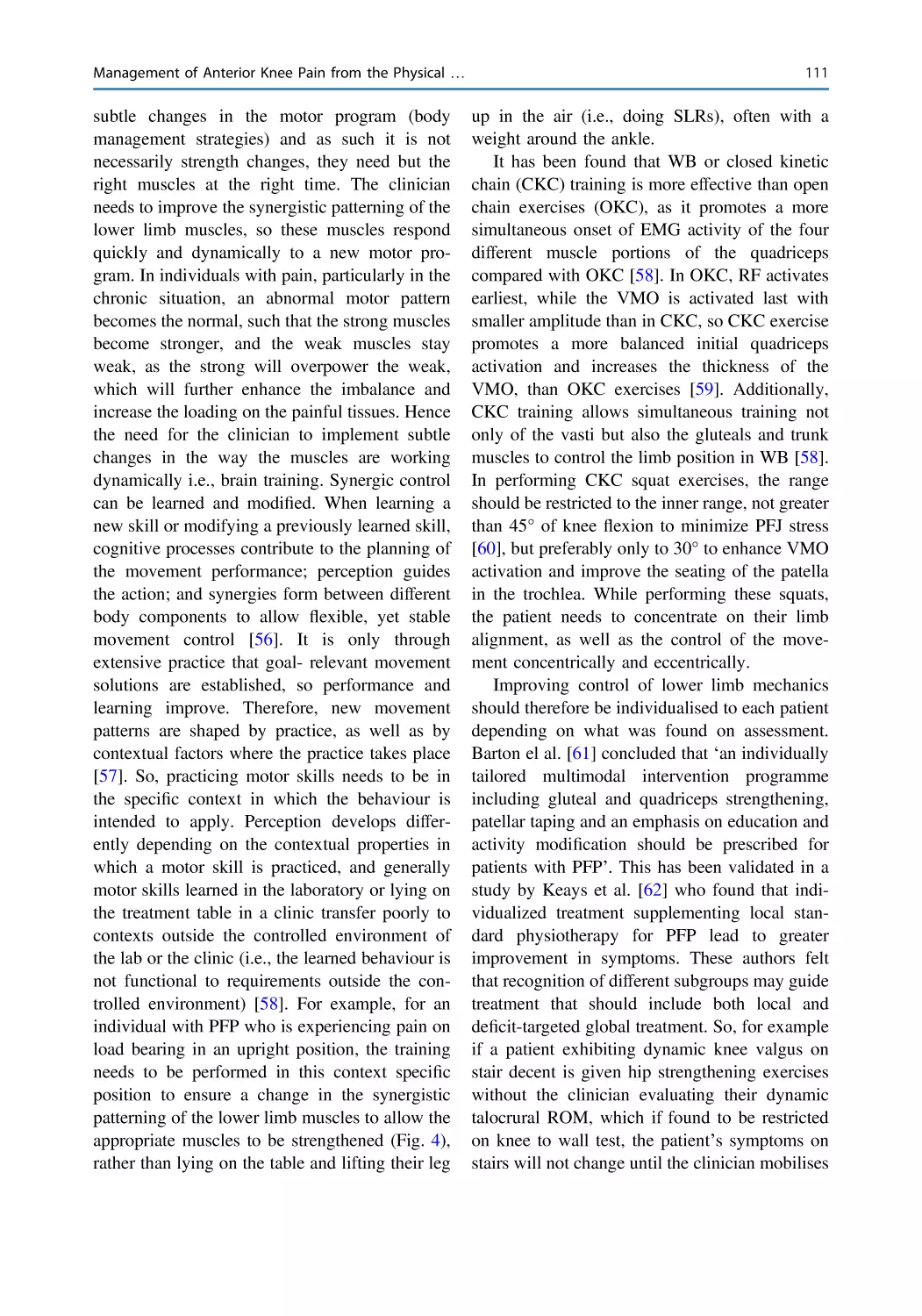
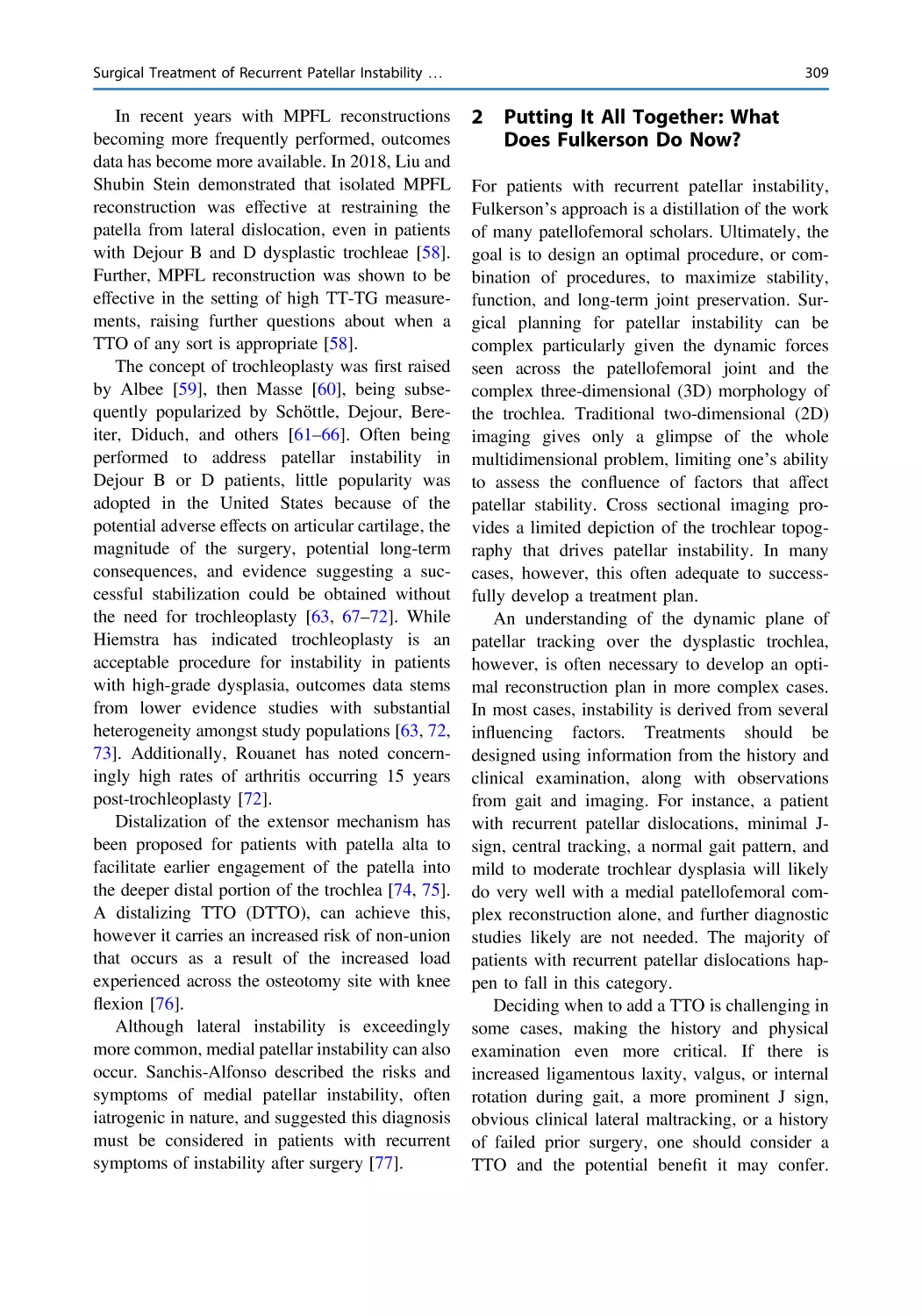
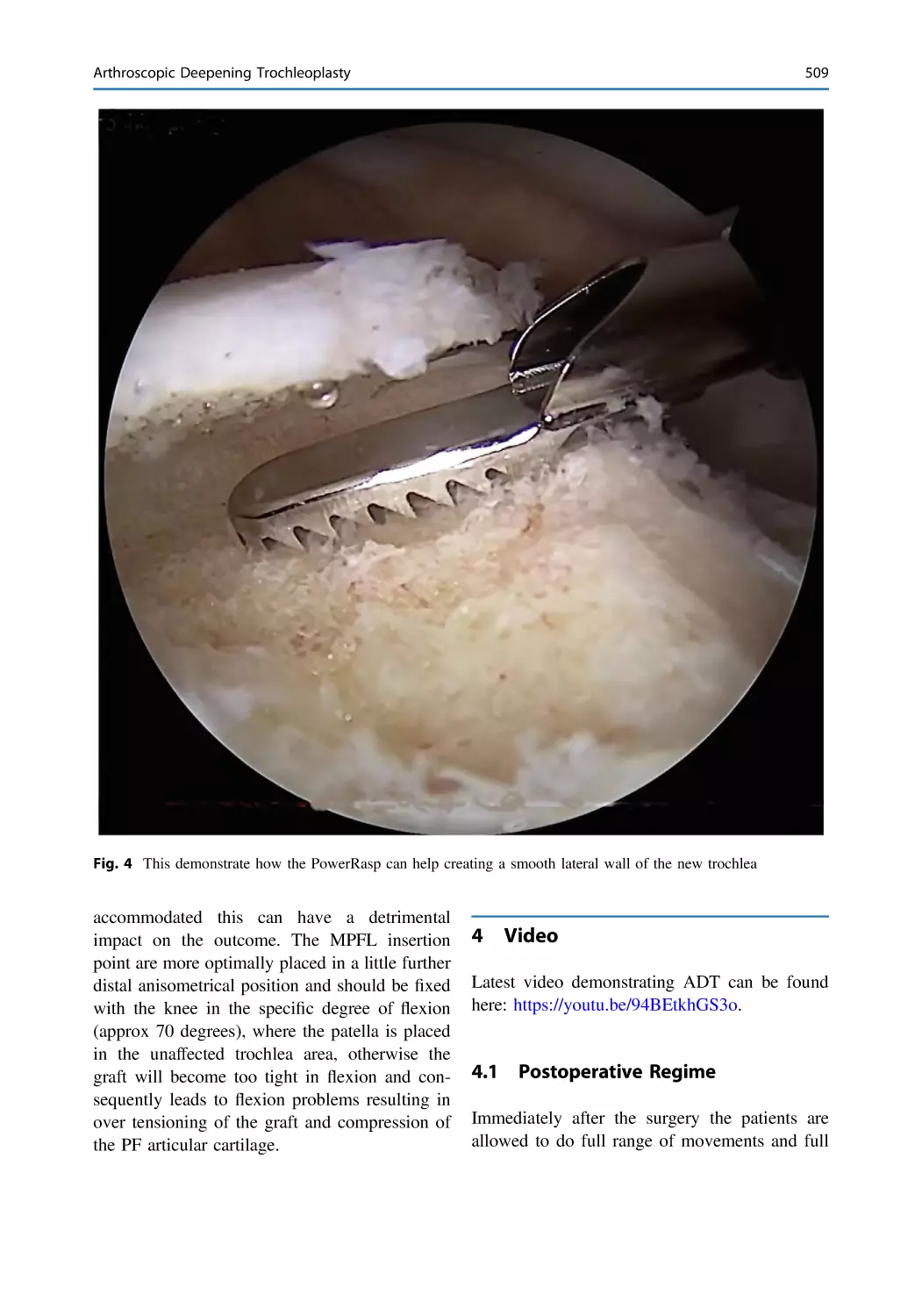
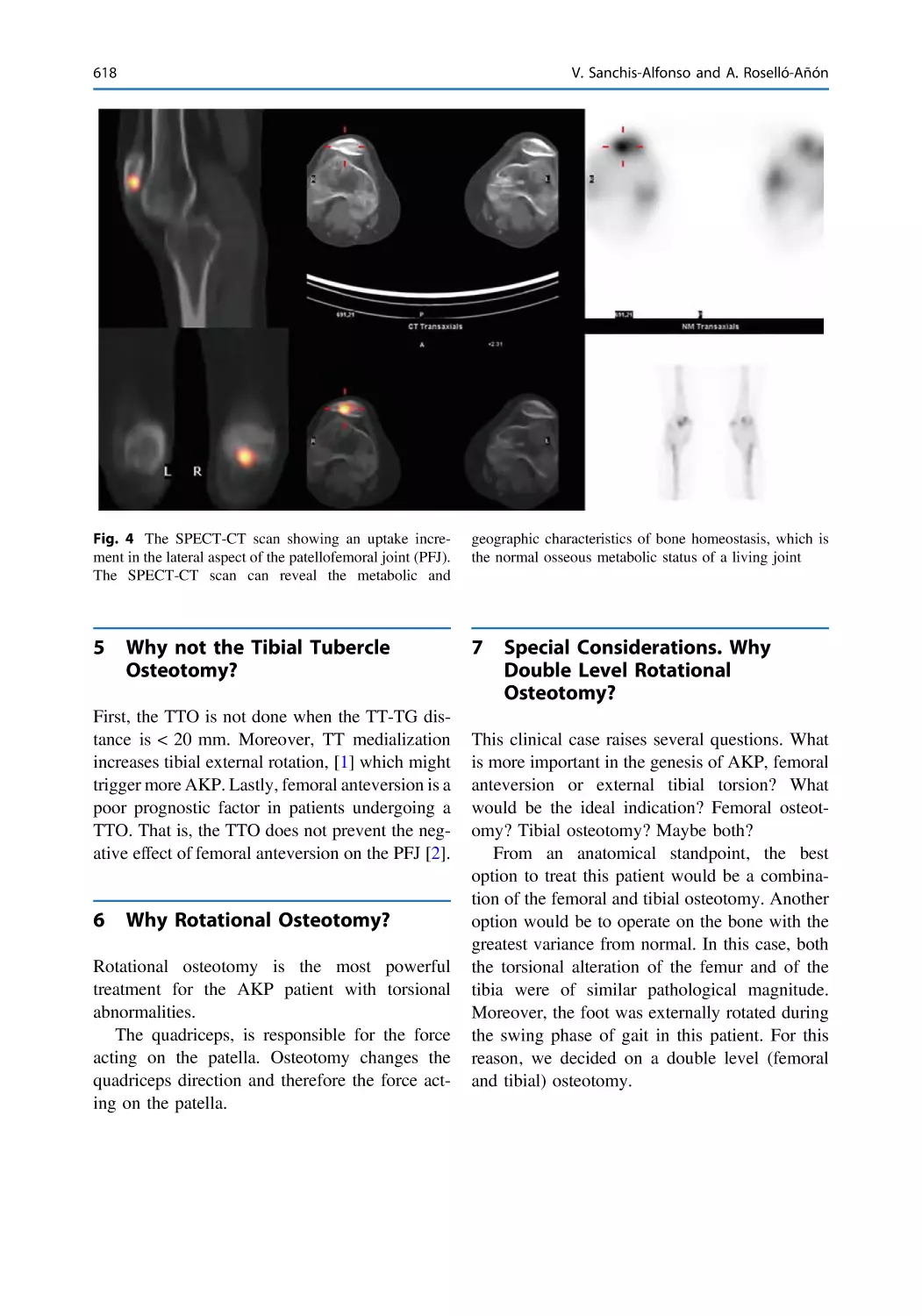
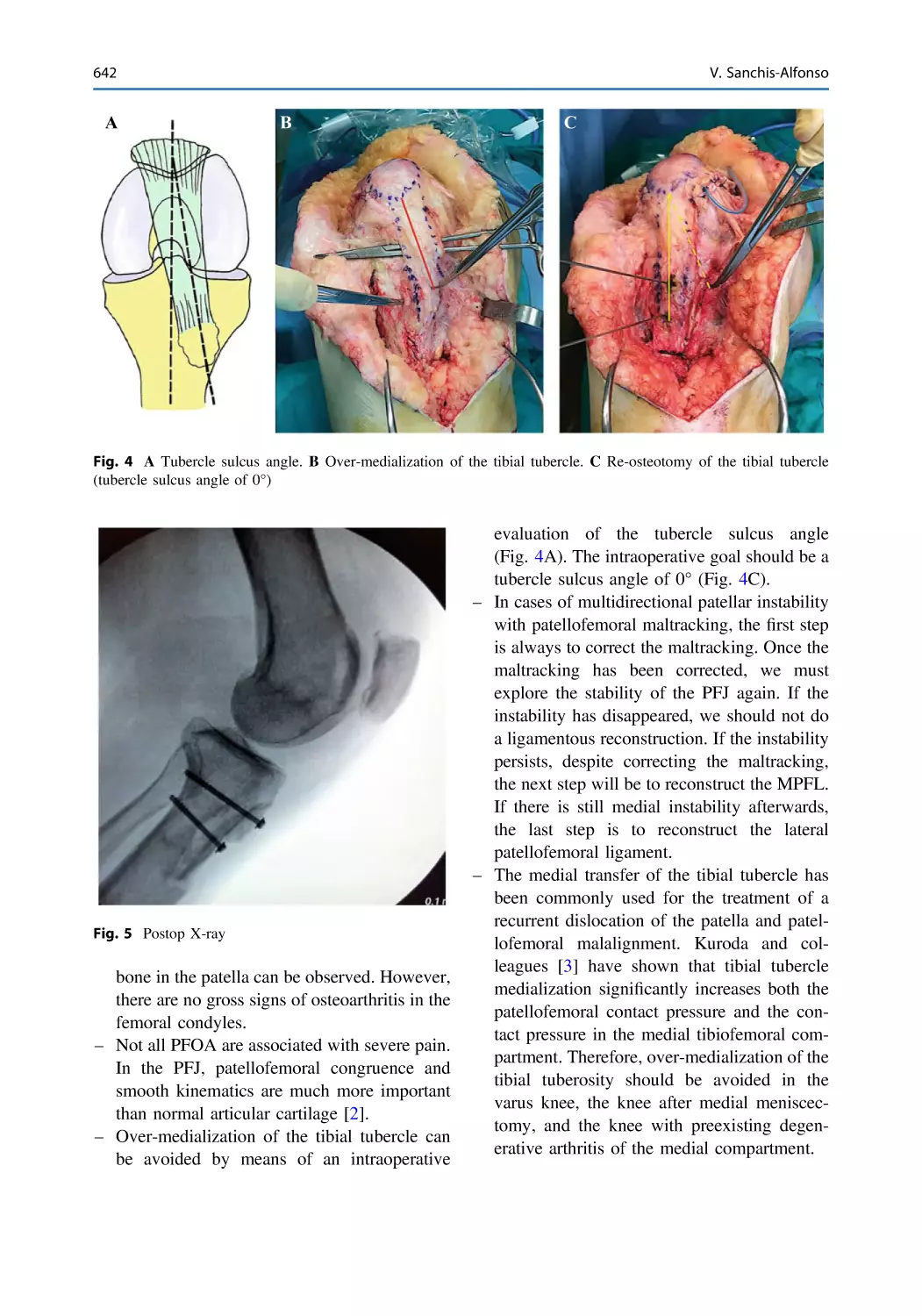
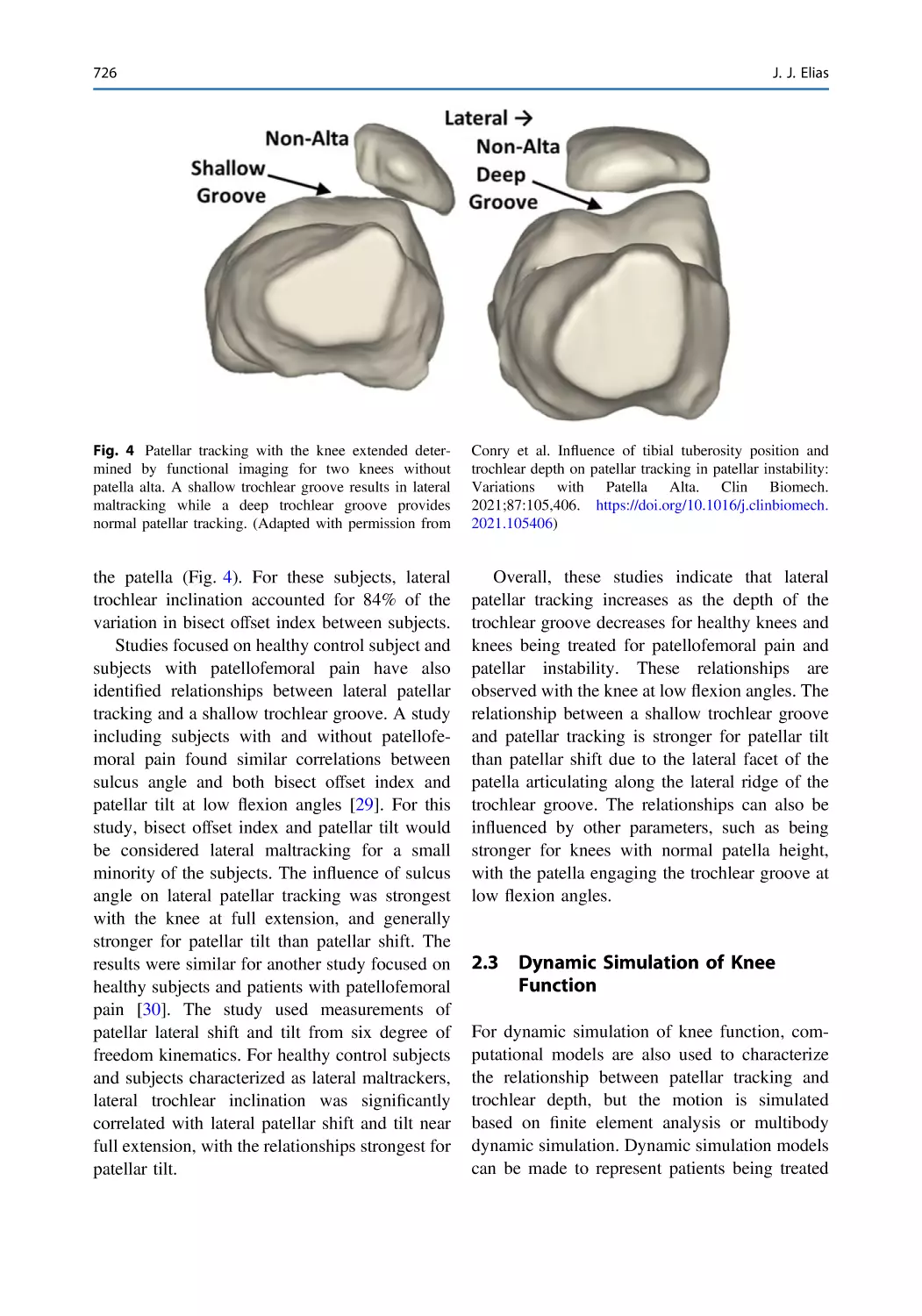
Year: 2023




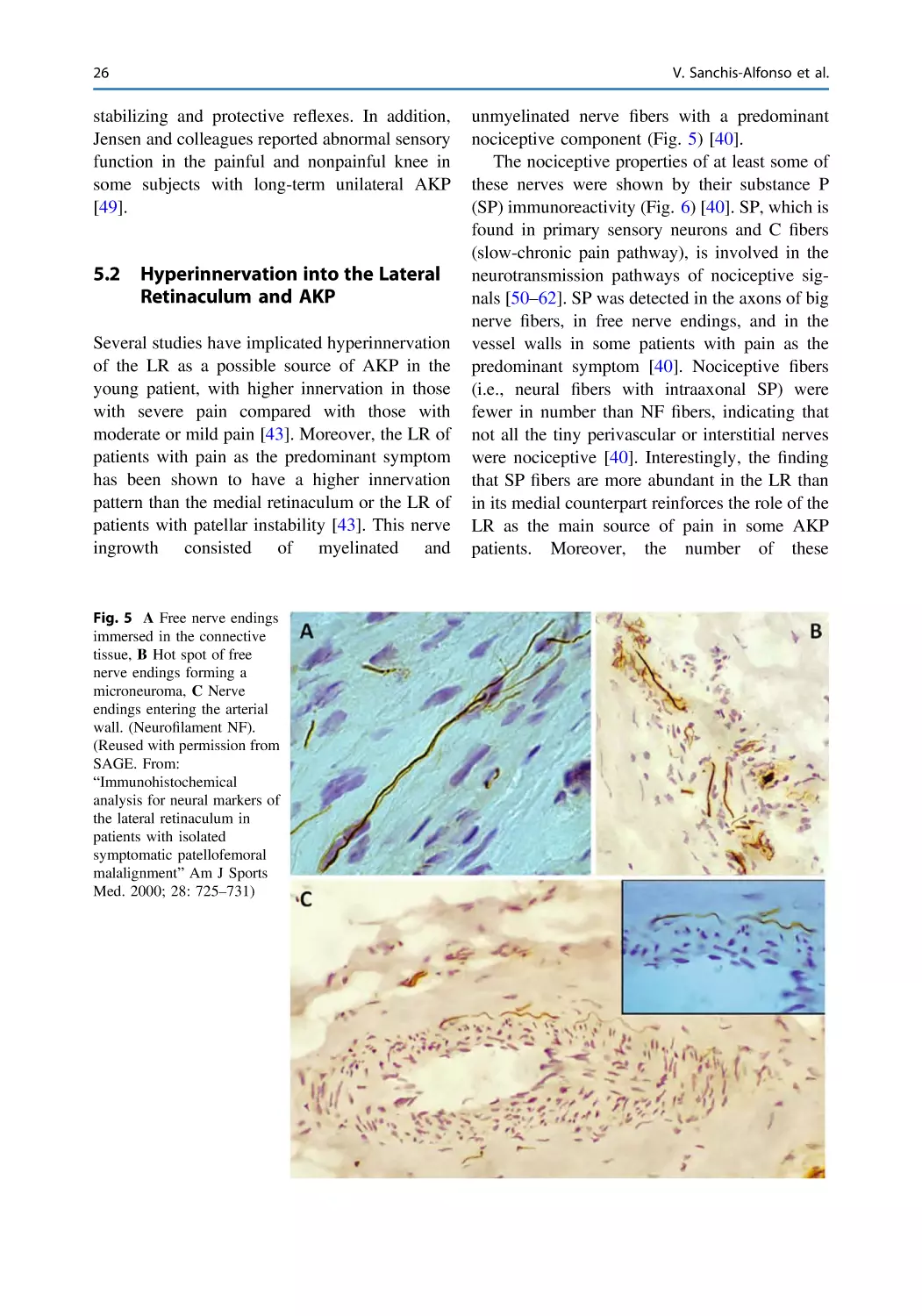
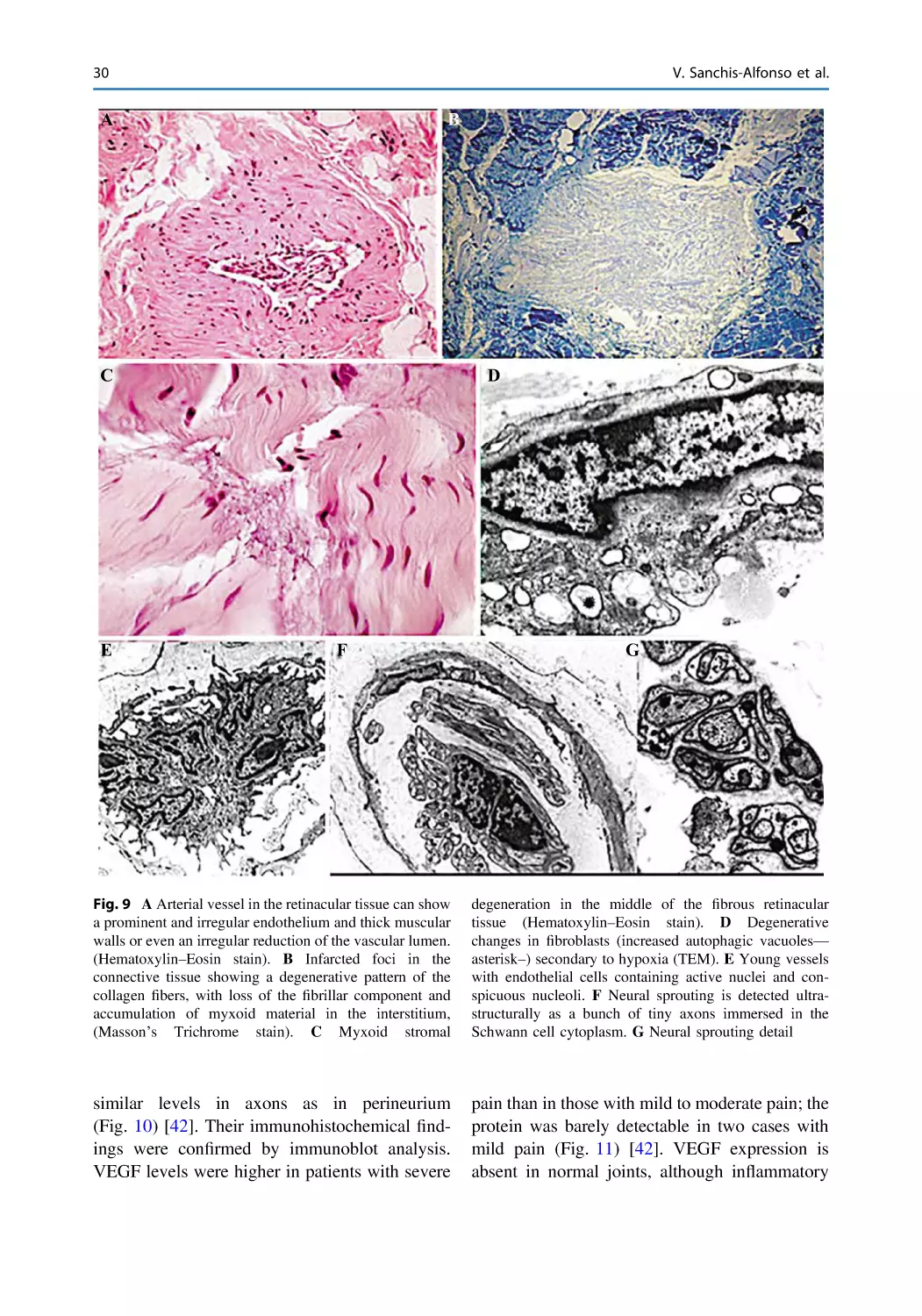
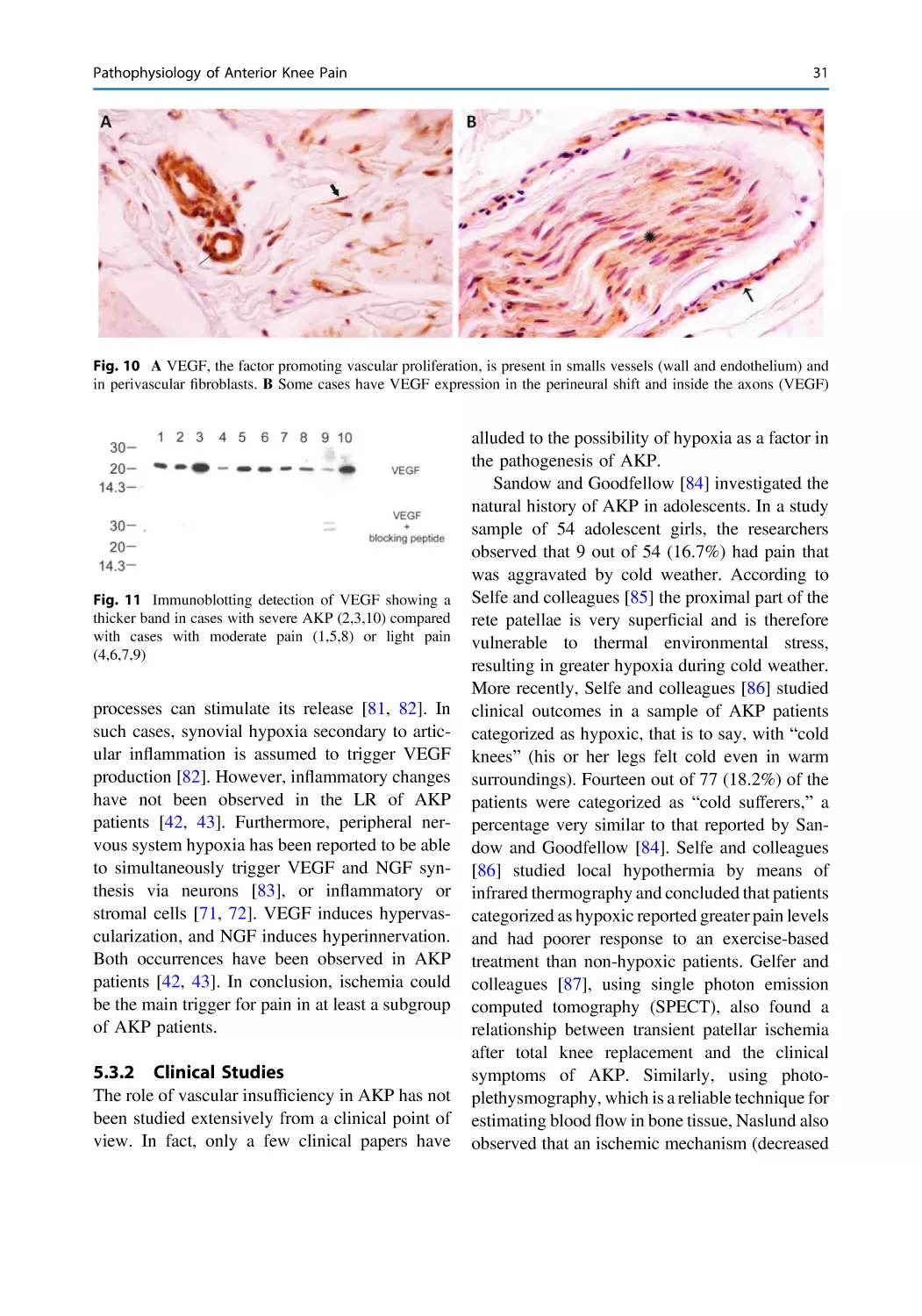
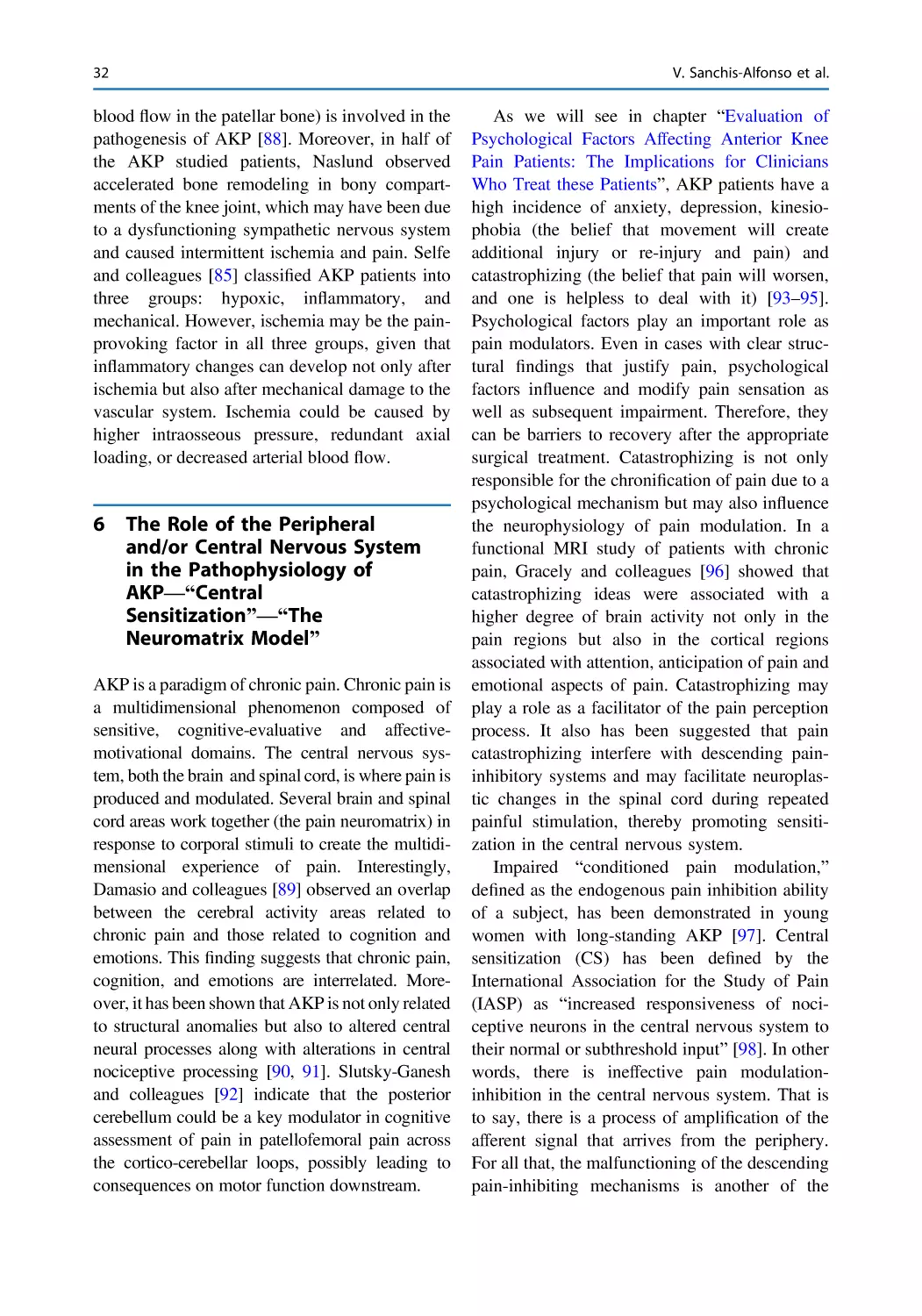
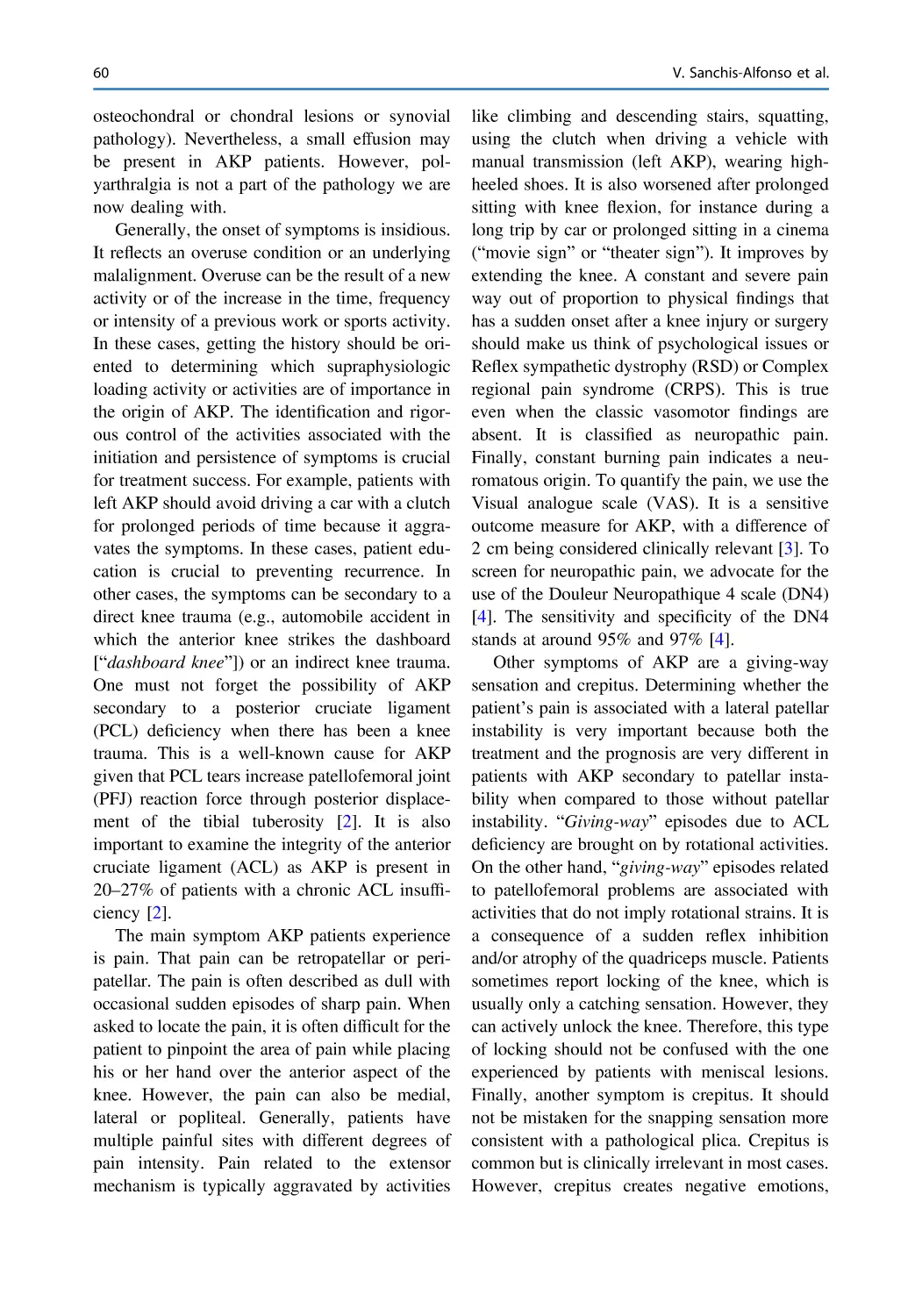
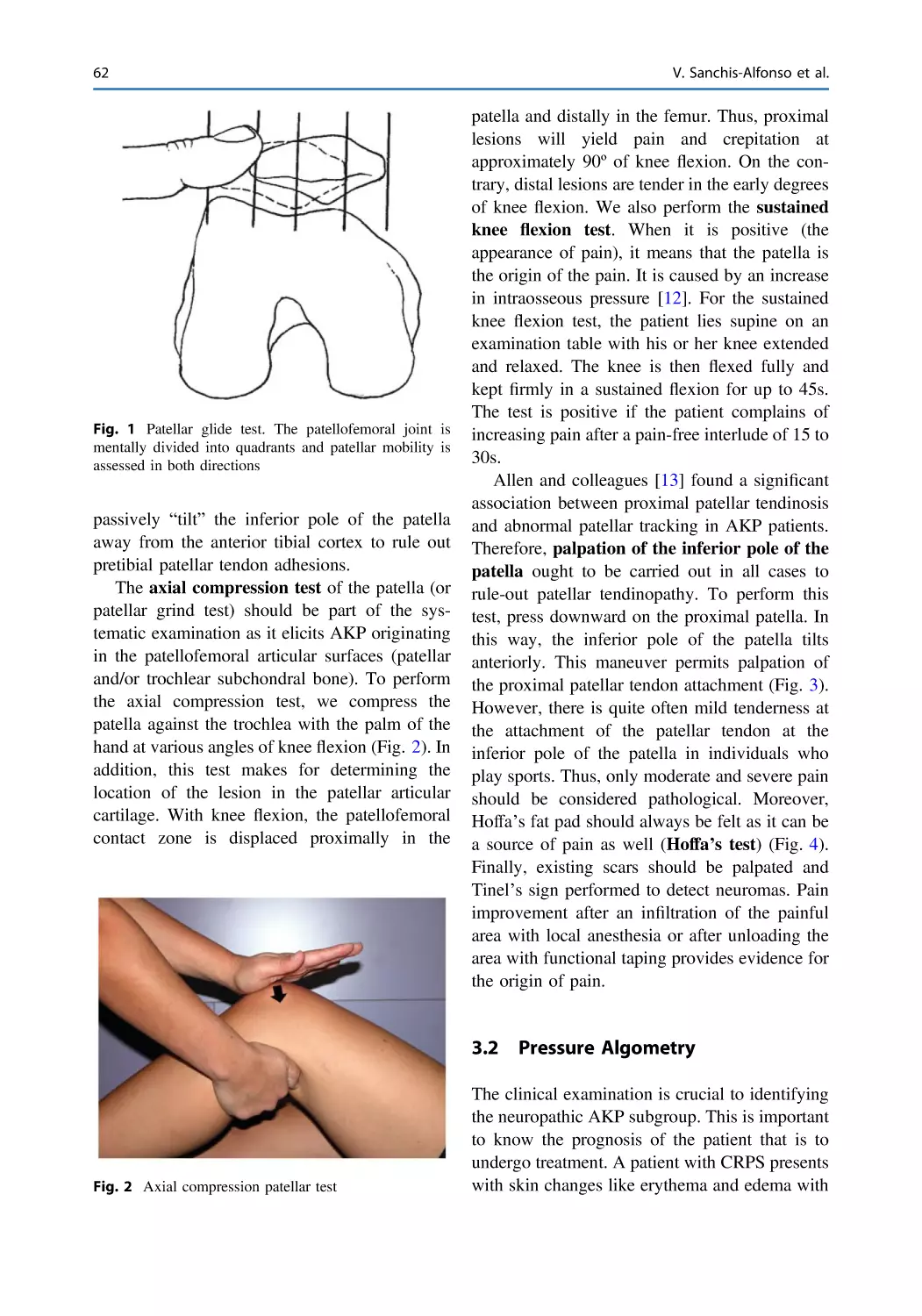
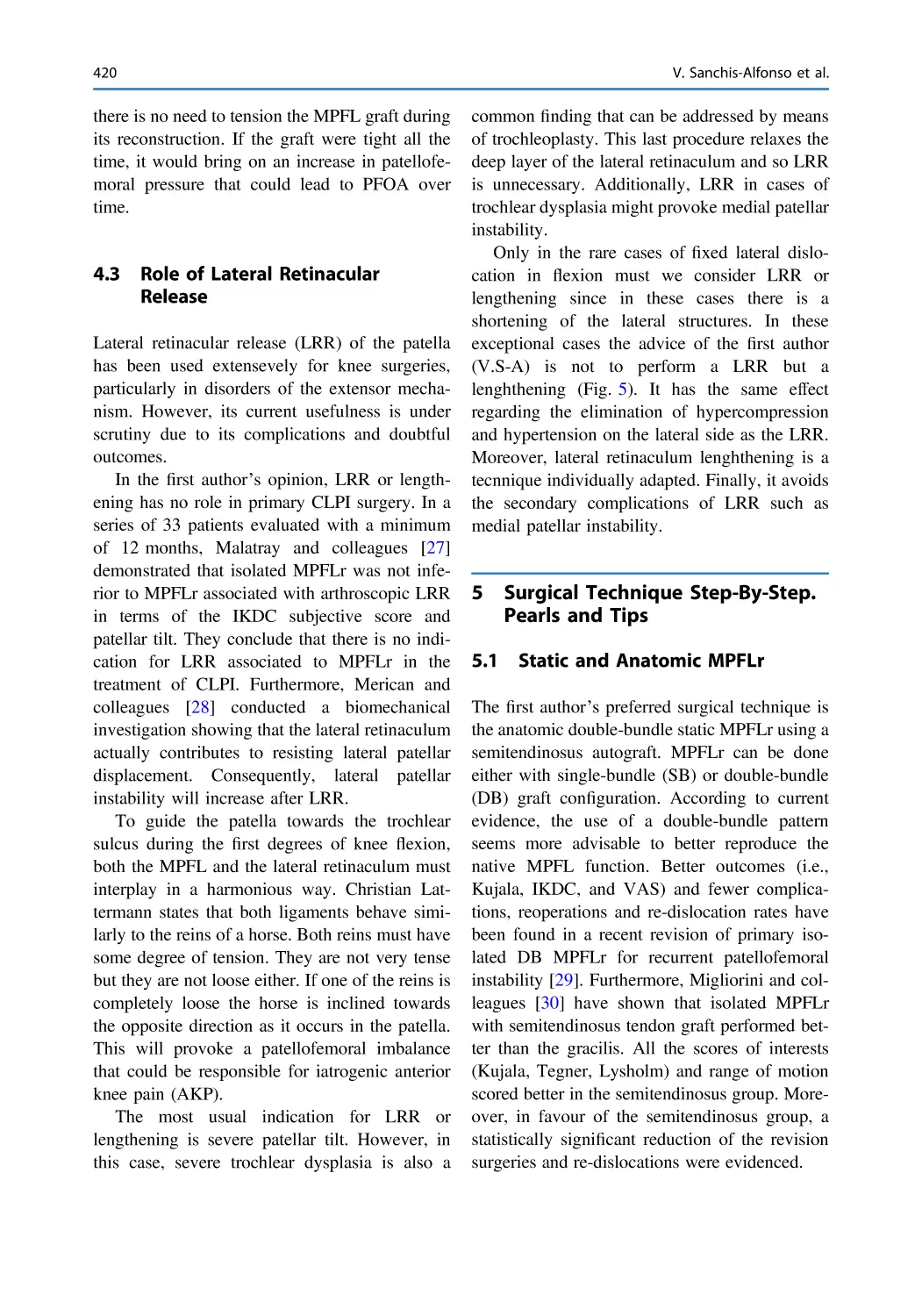
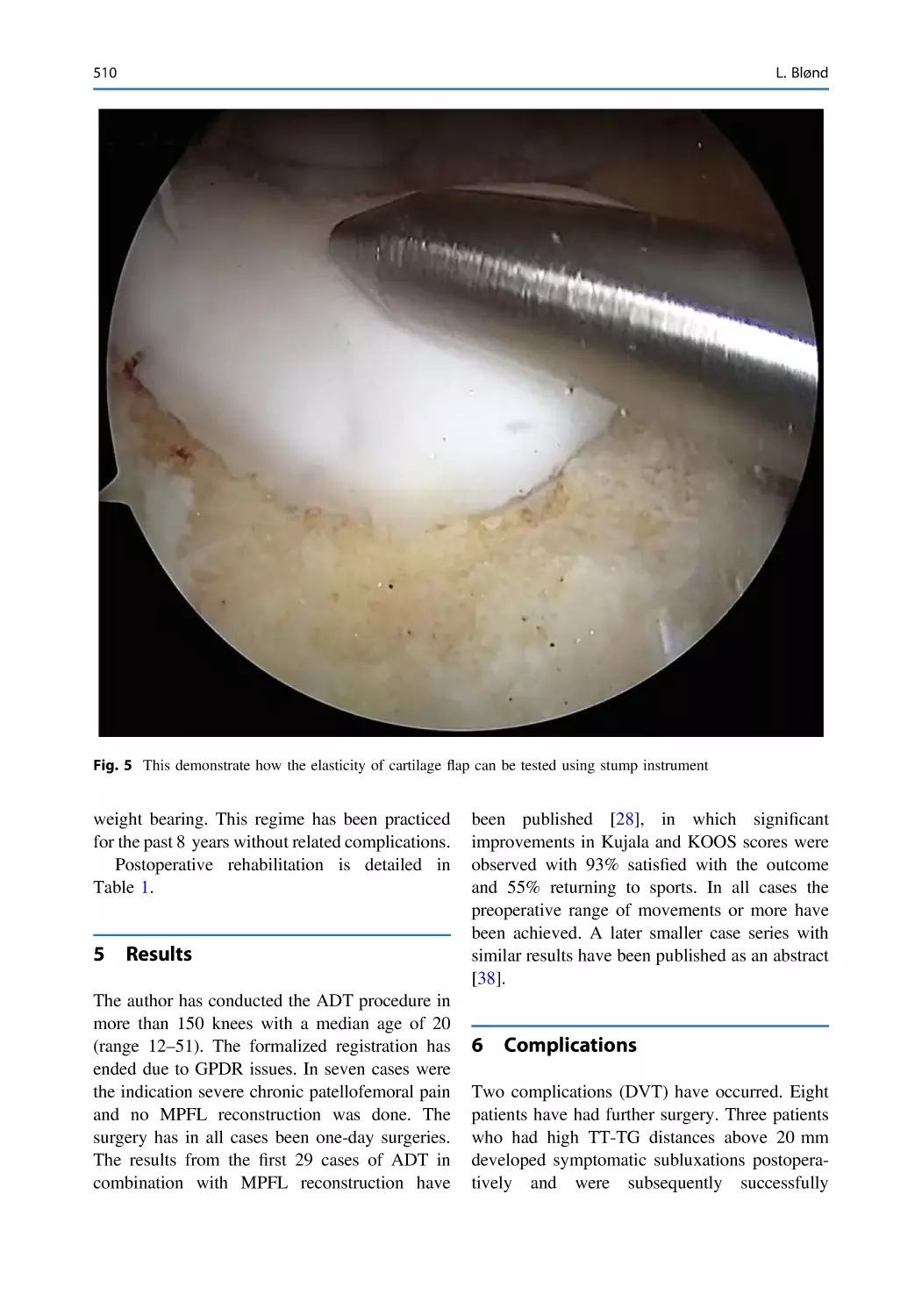
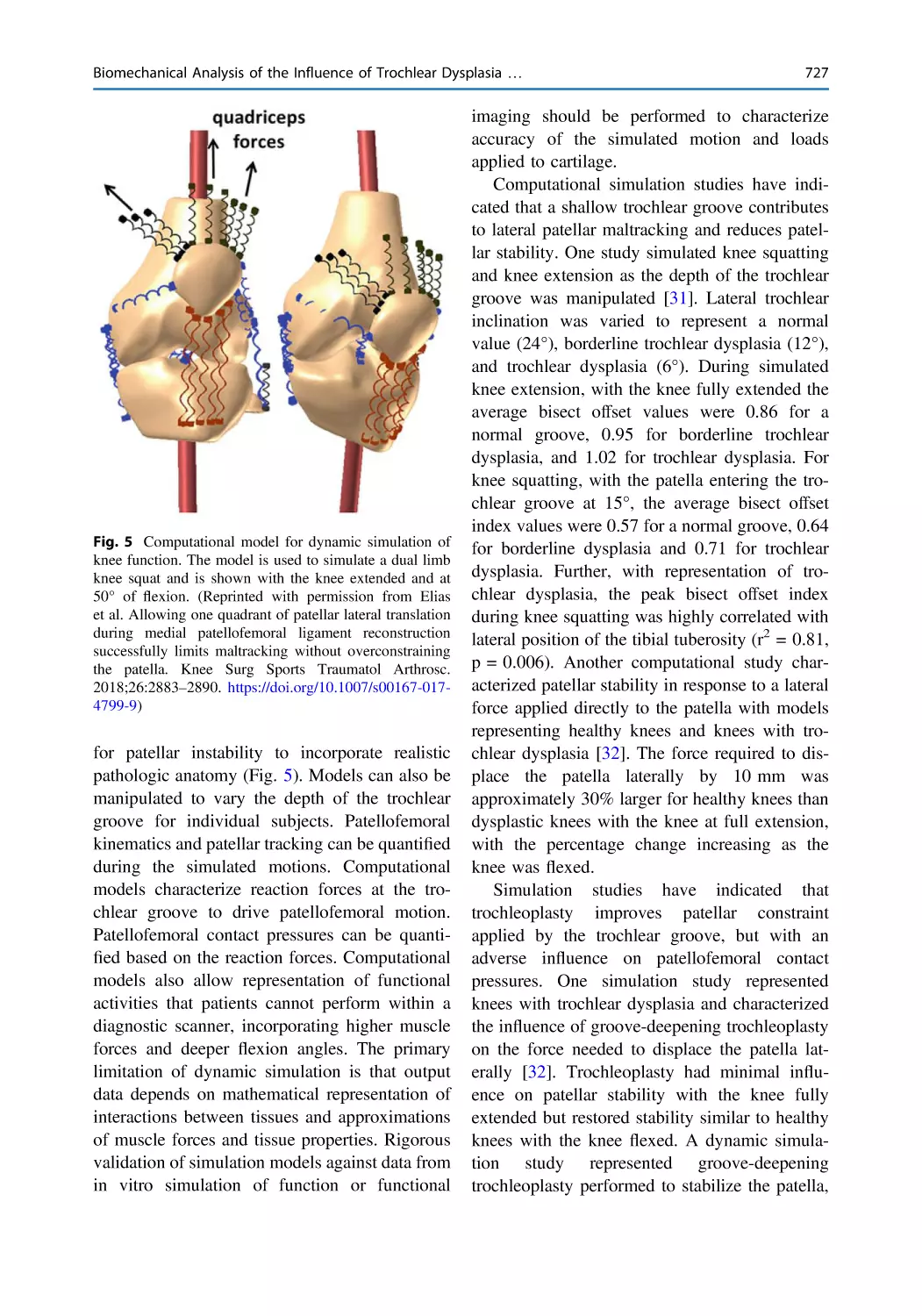
Text
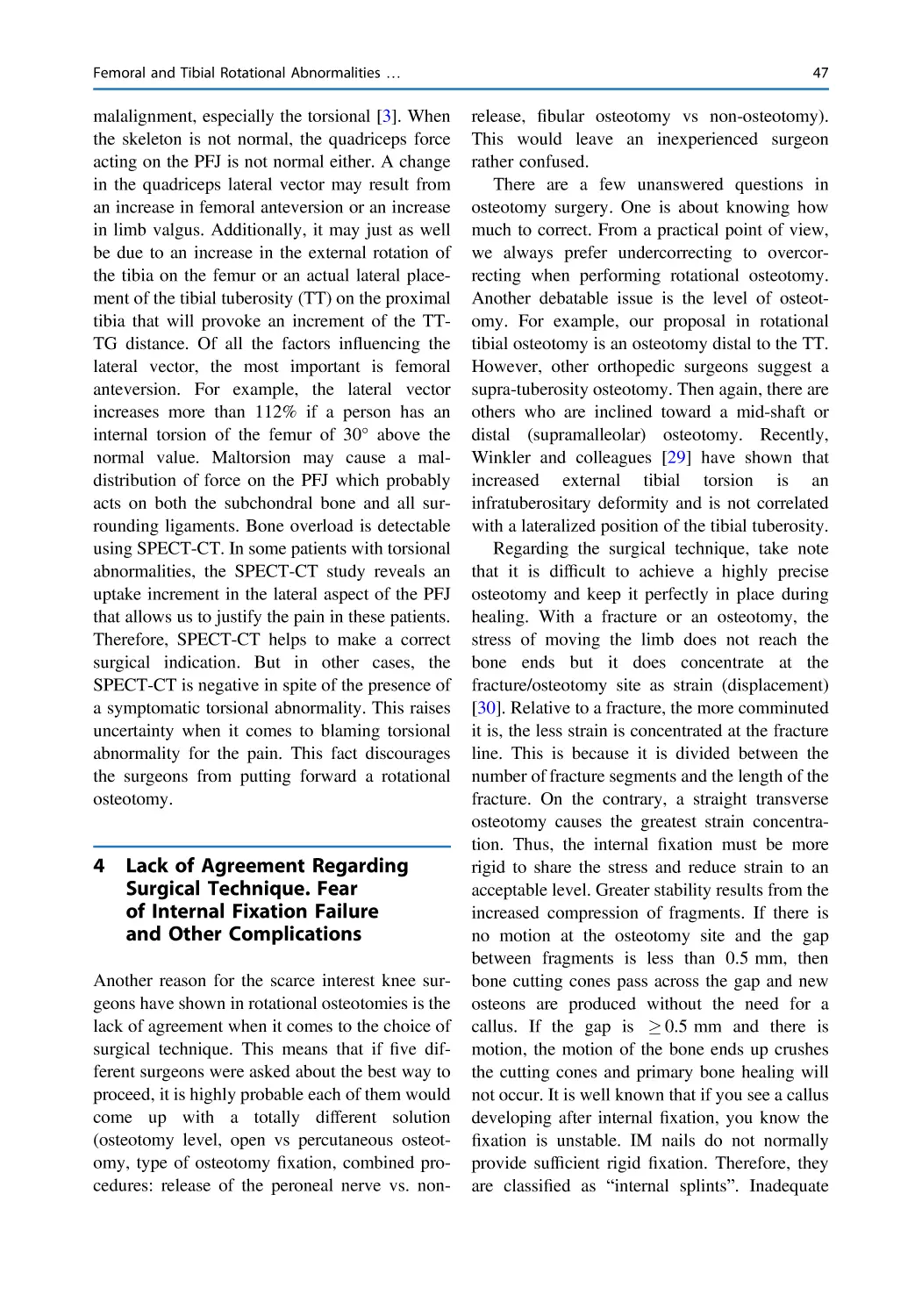
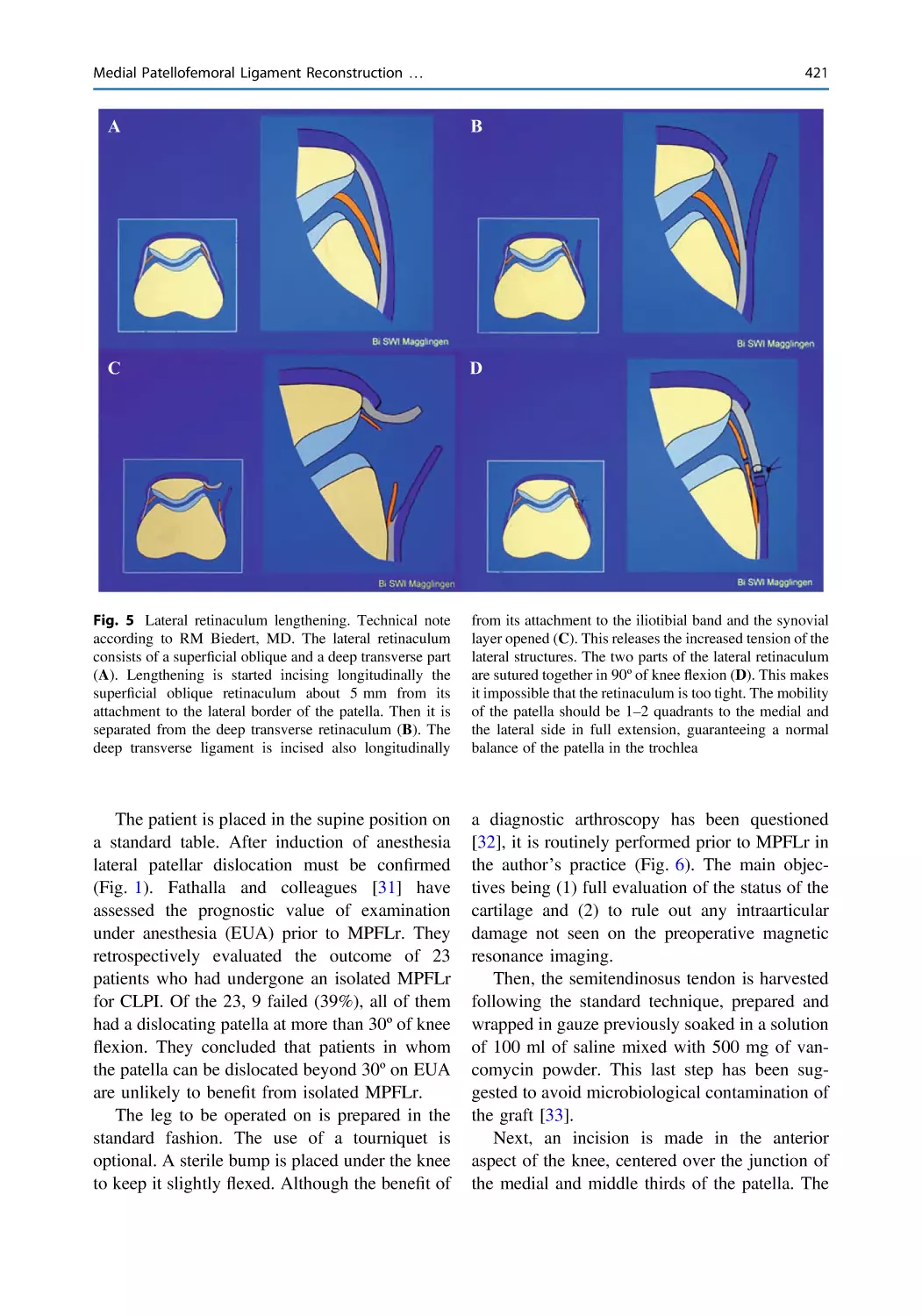
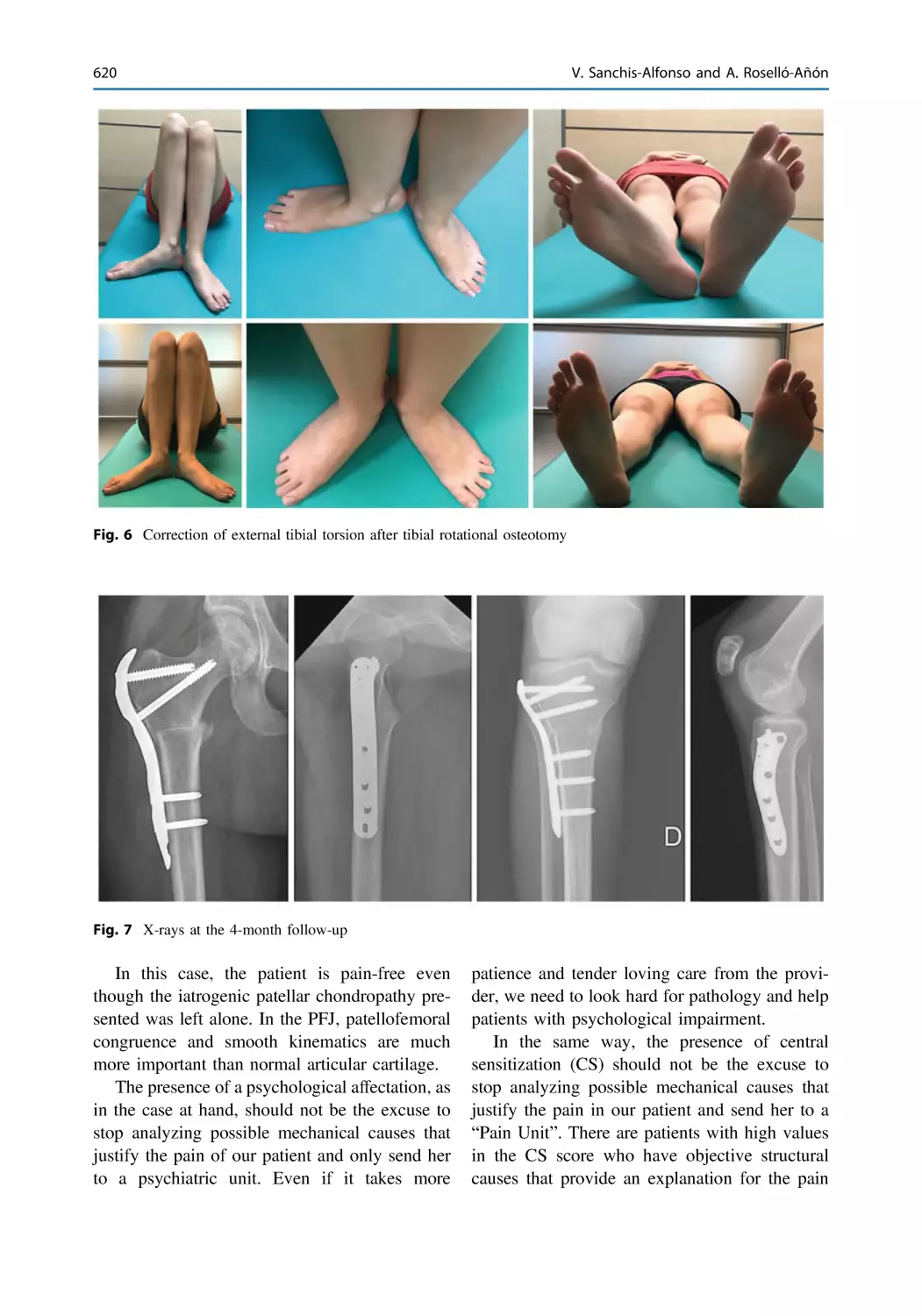
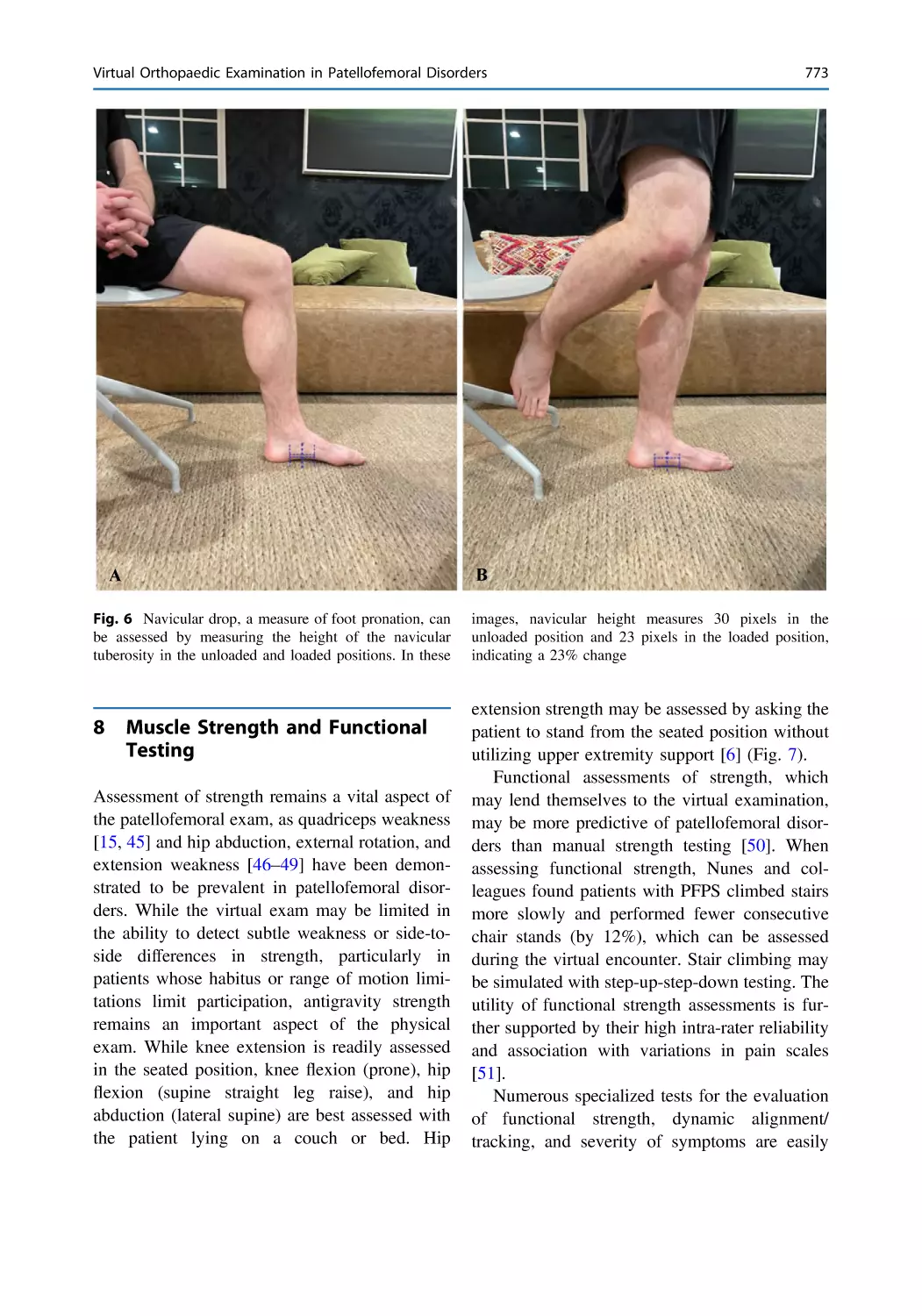
Anterior Knee Pain and Patellar
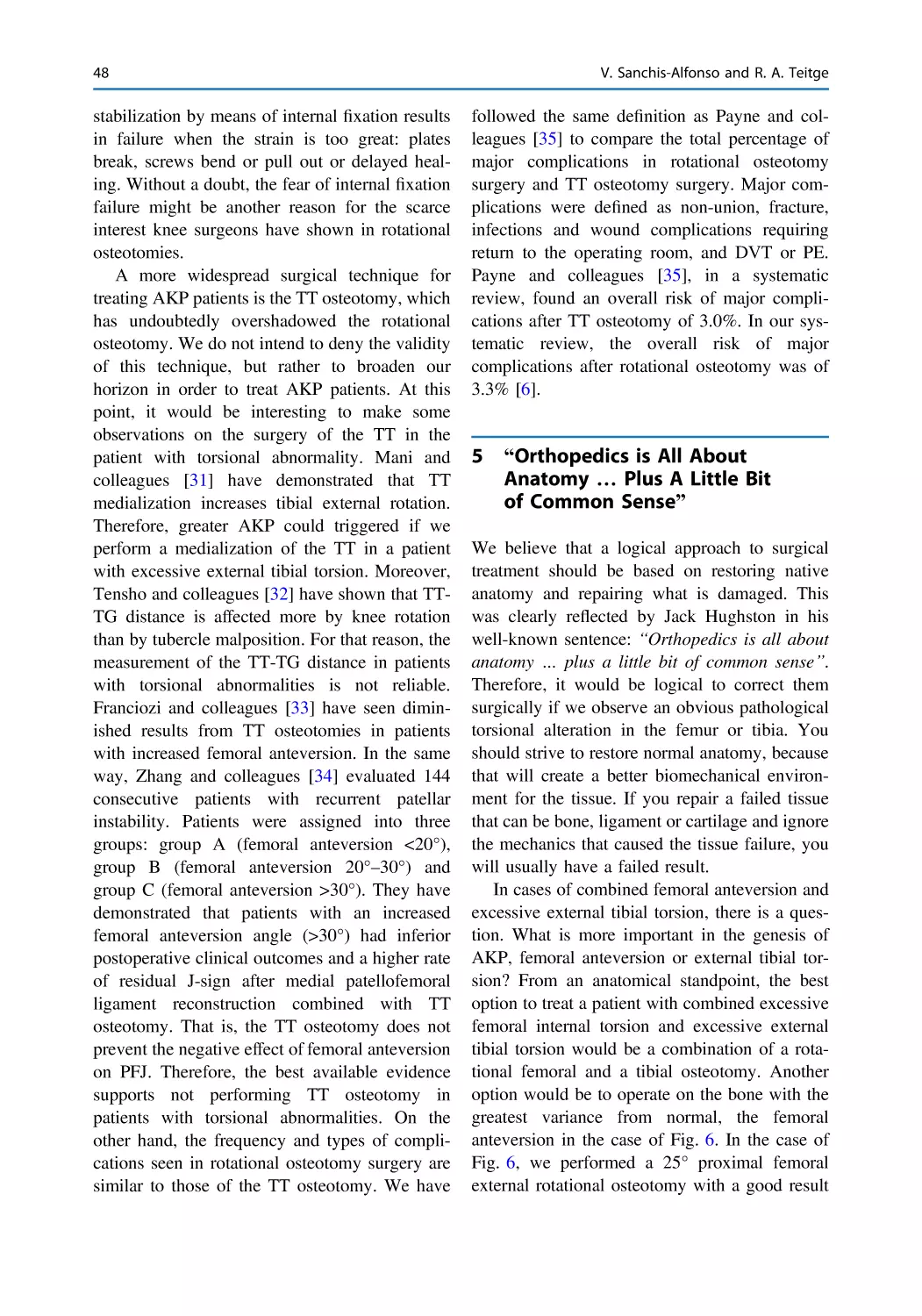
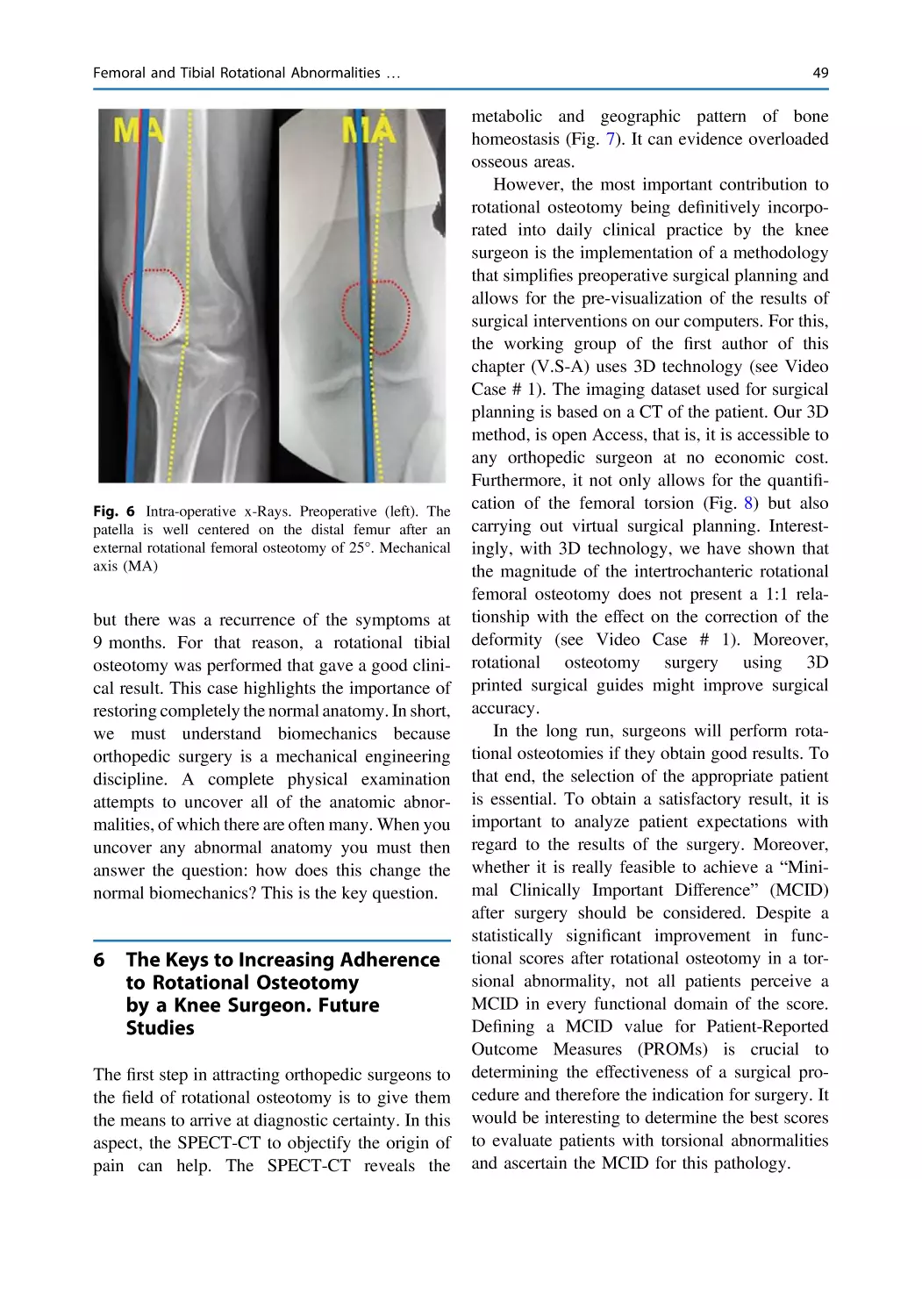
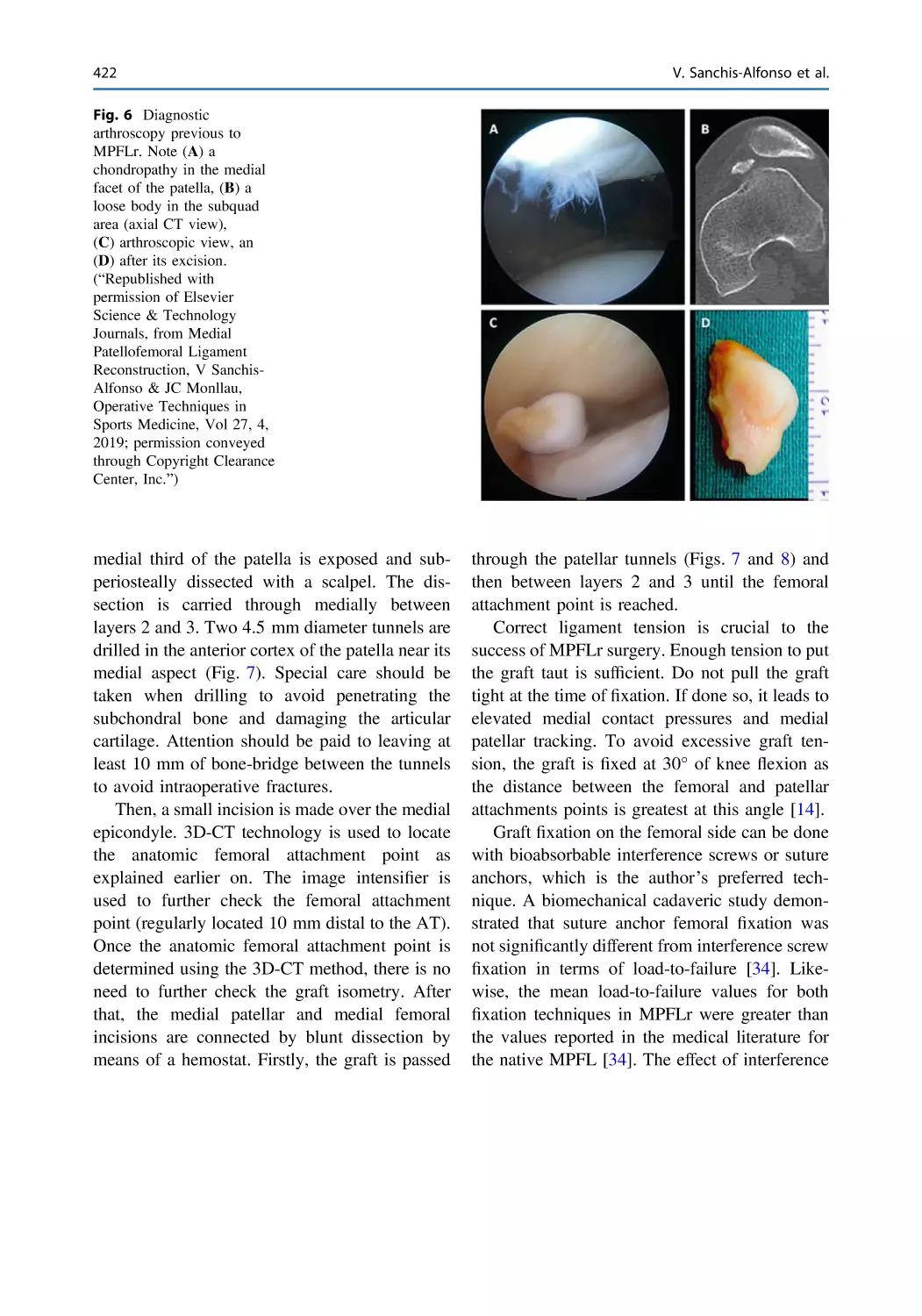
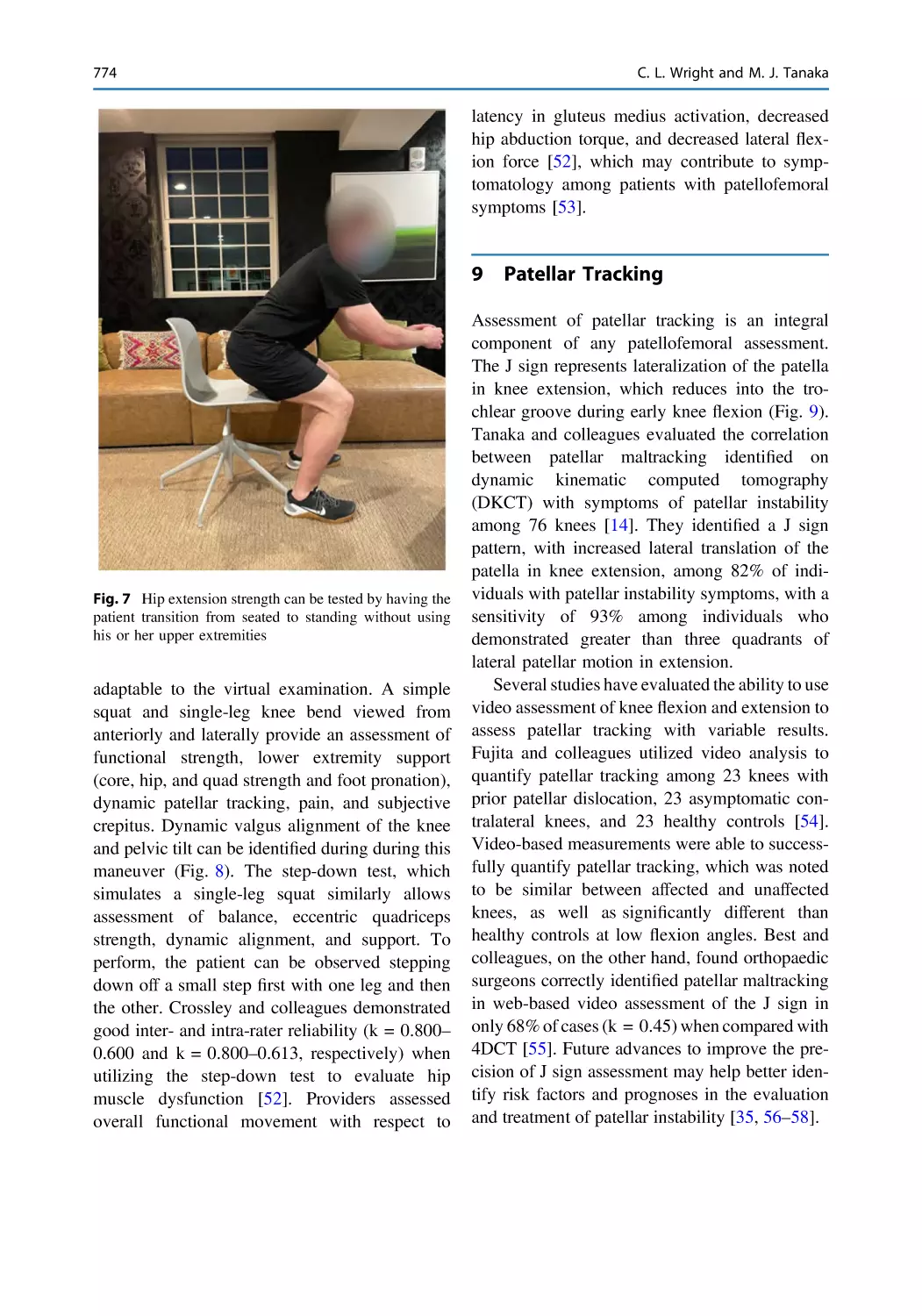
Instability
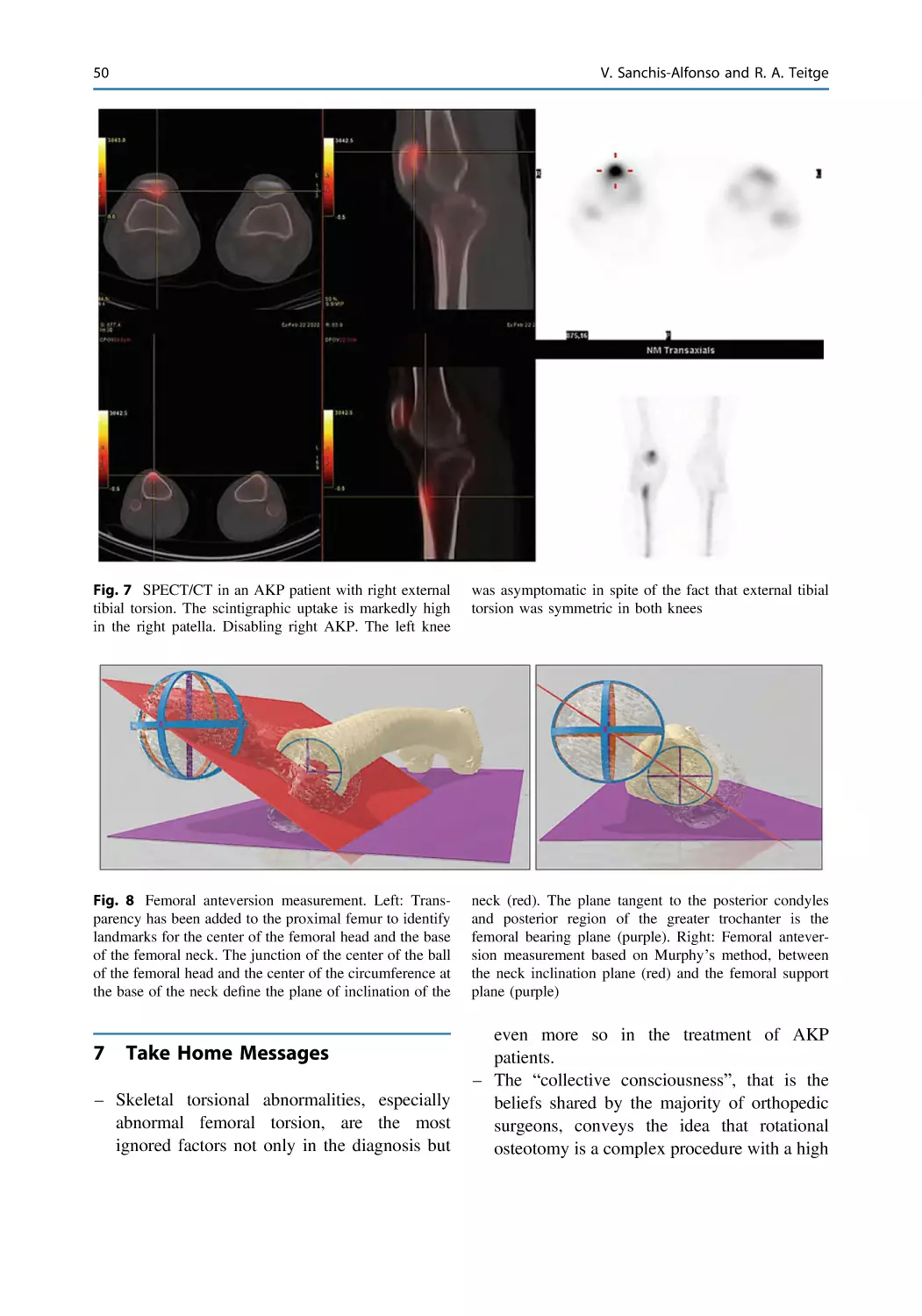
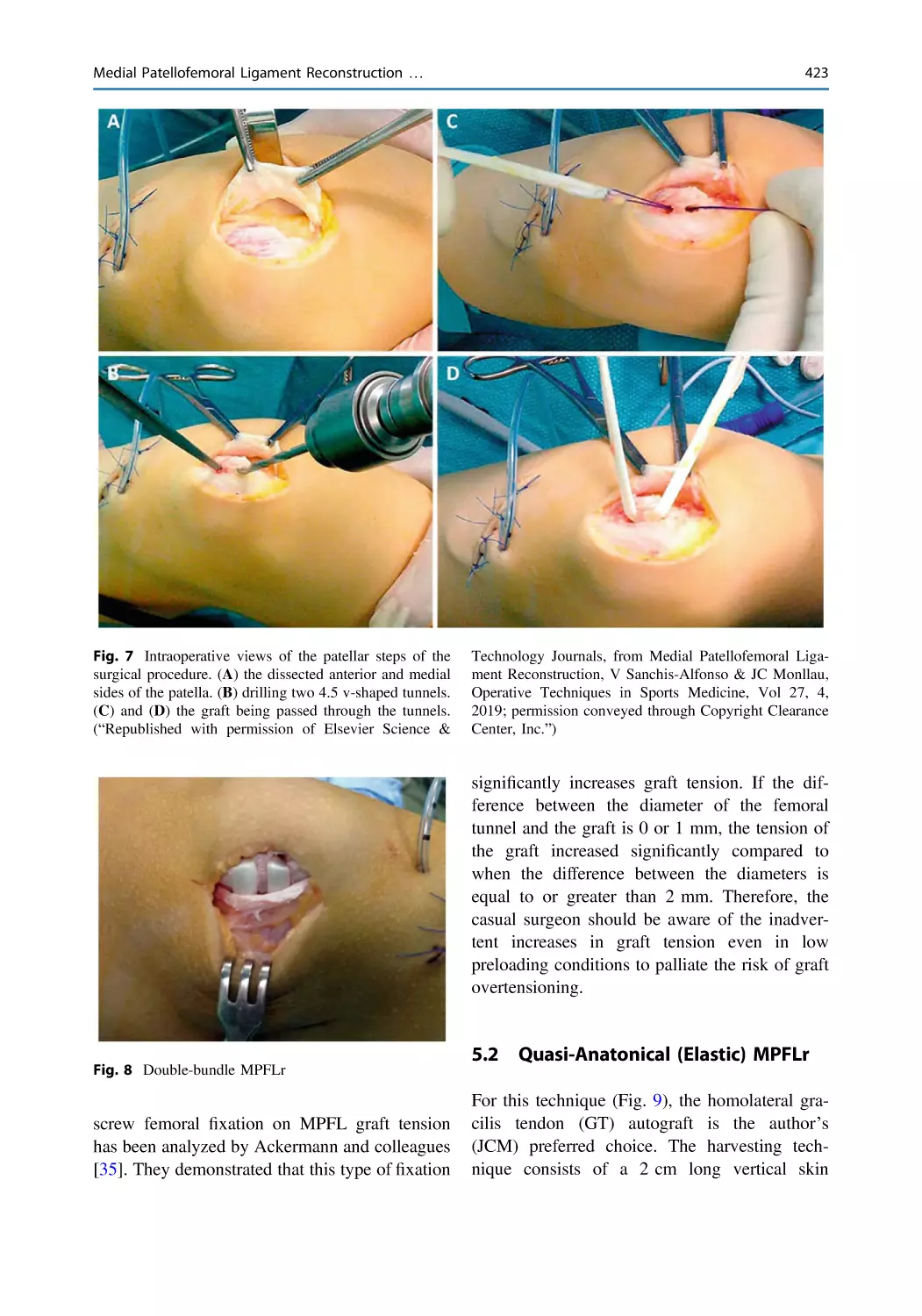
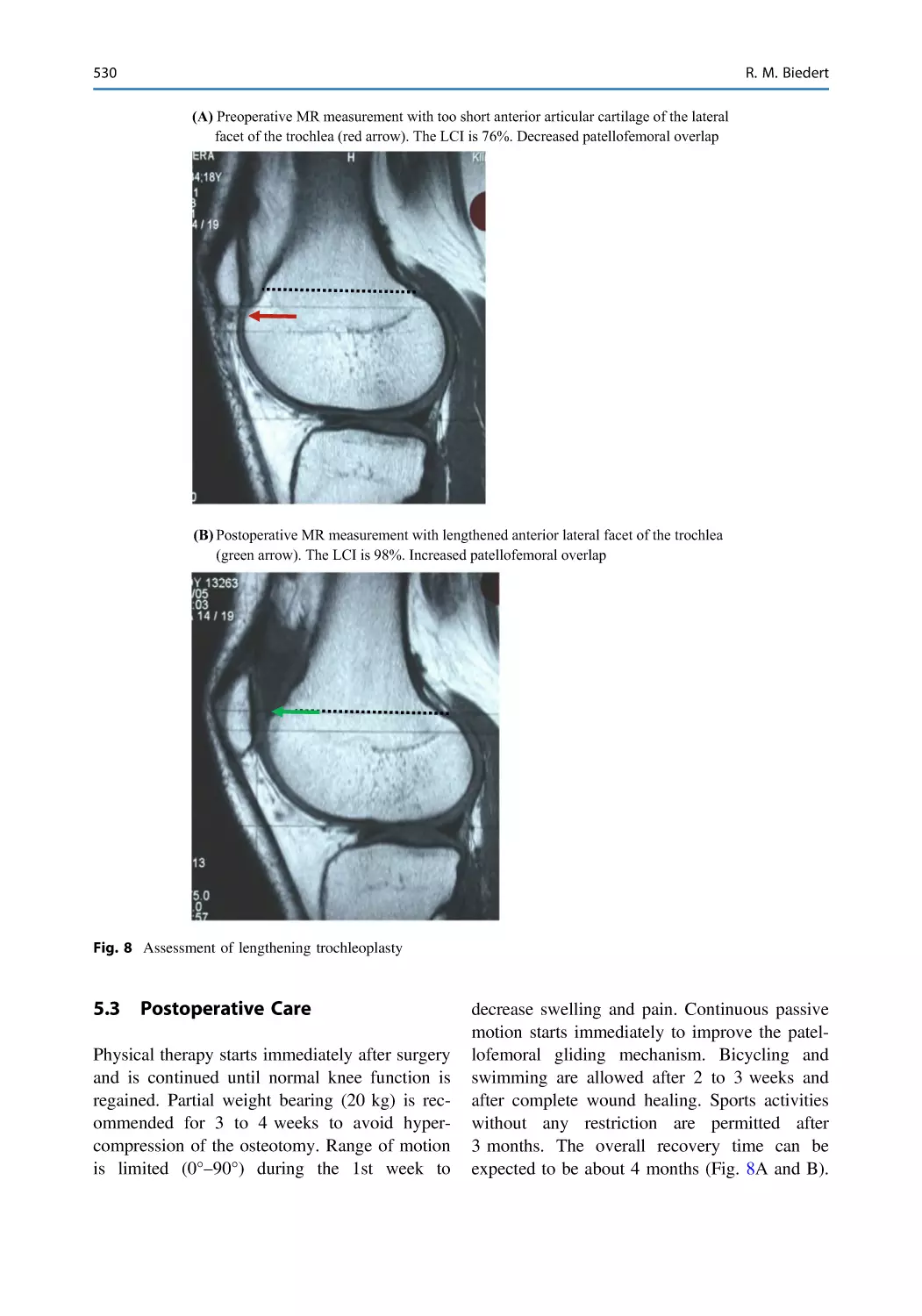
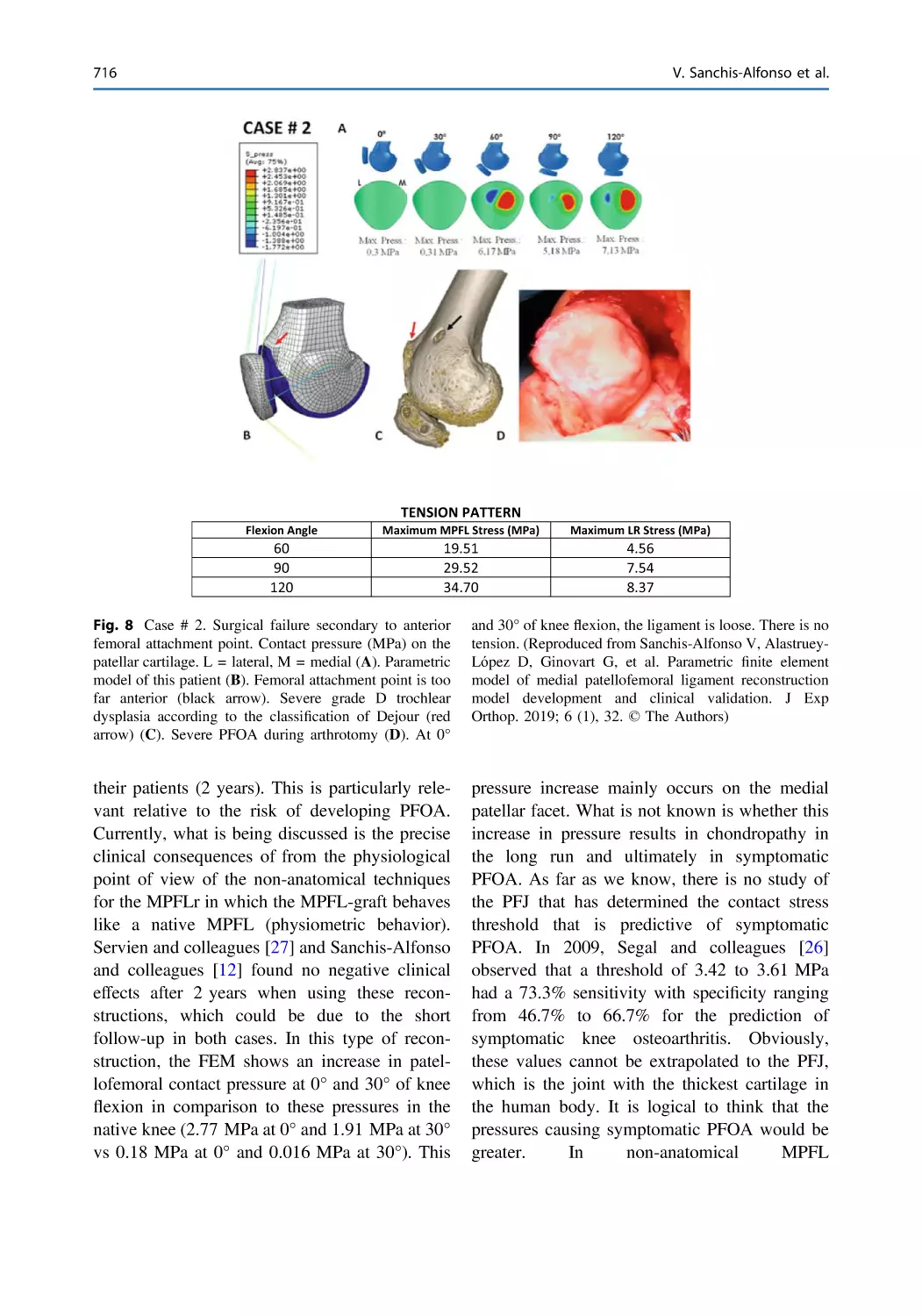
Vicente Sanchis-Alfonso
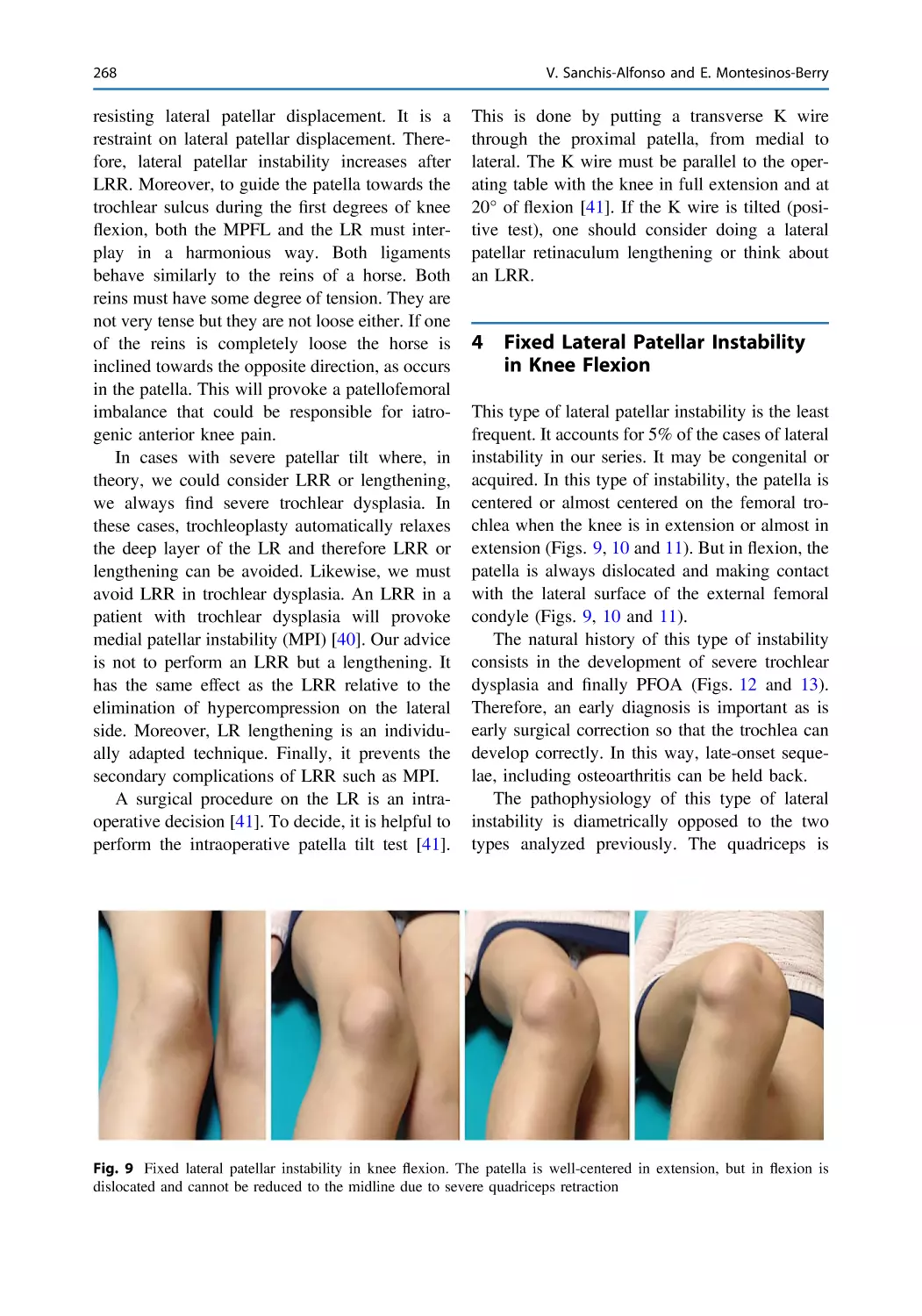
Editor
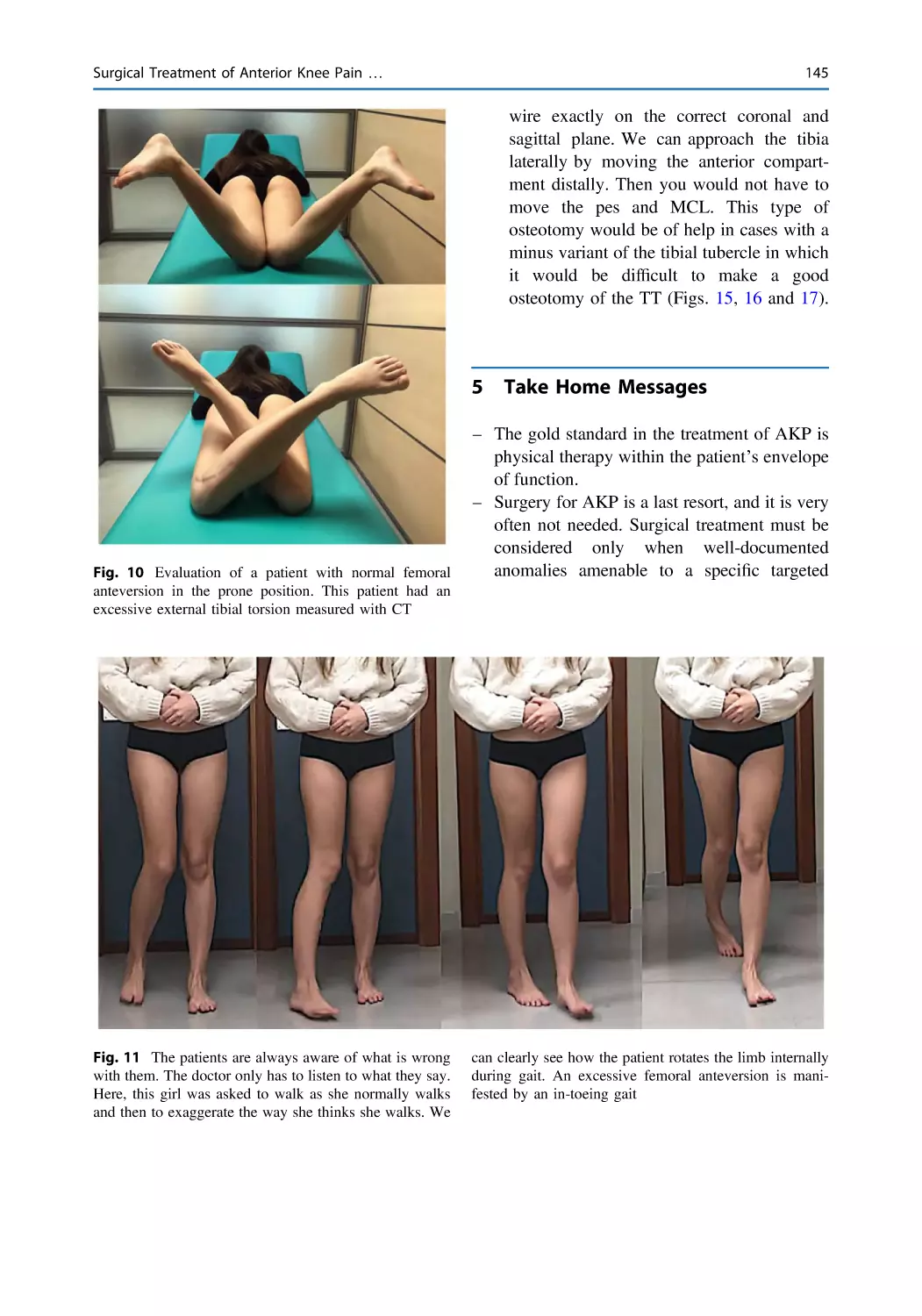
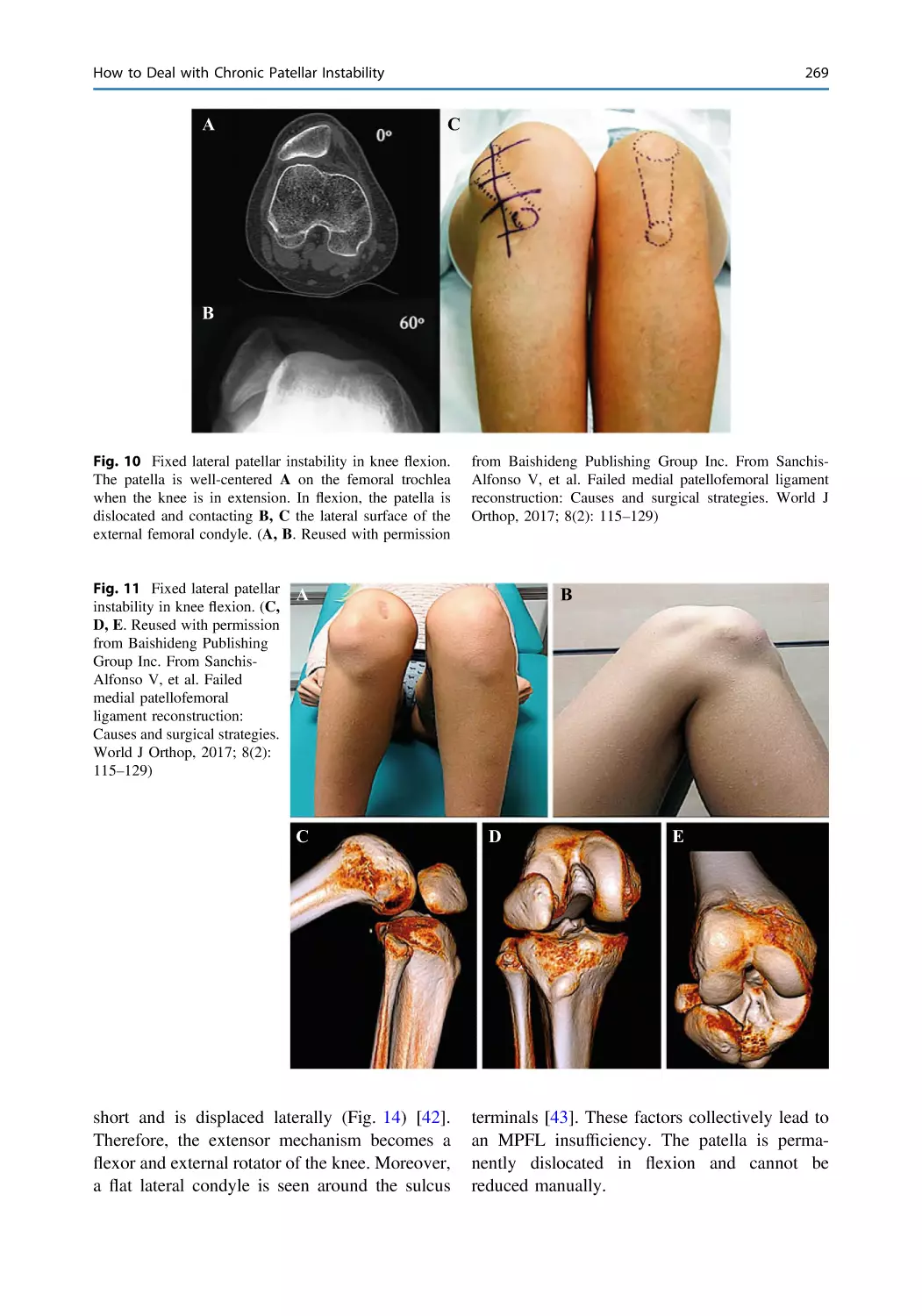
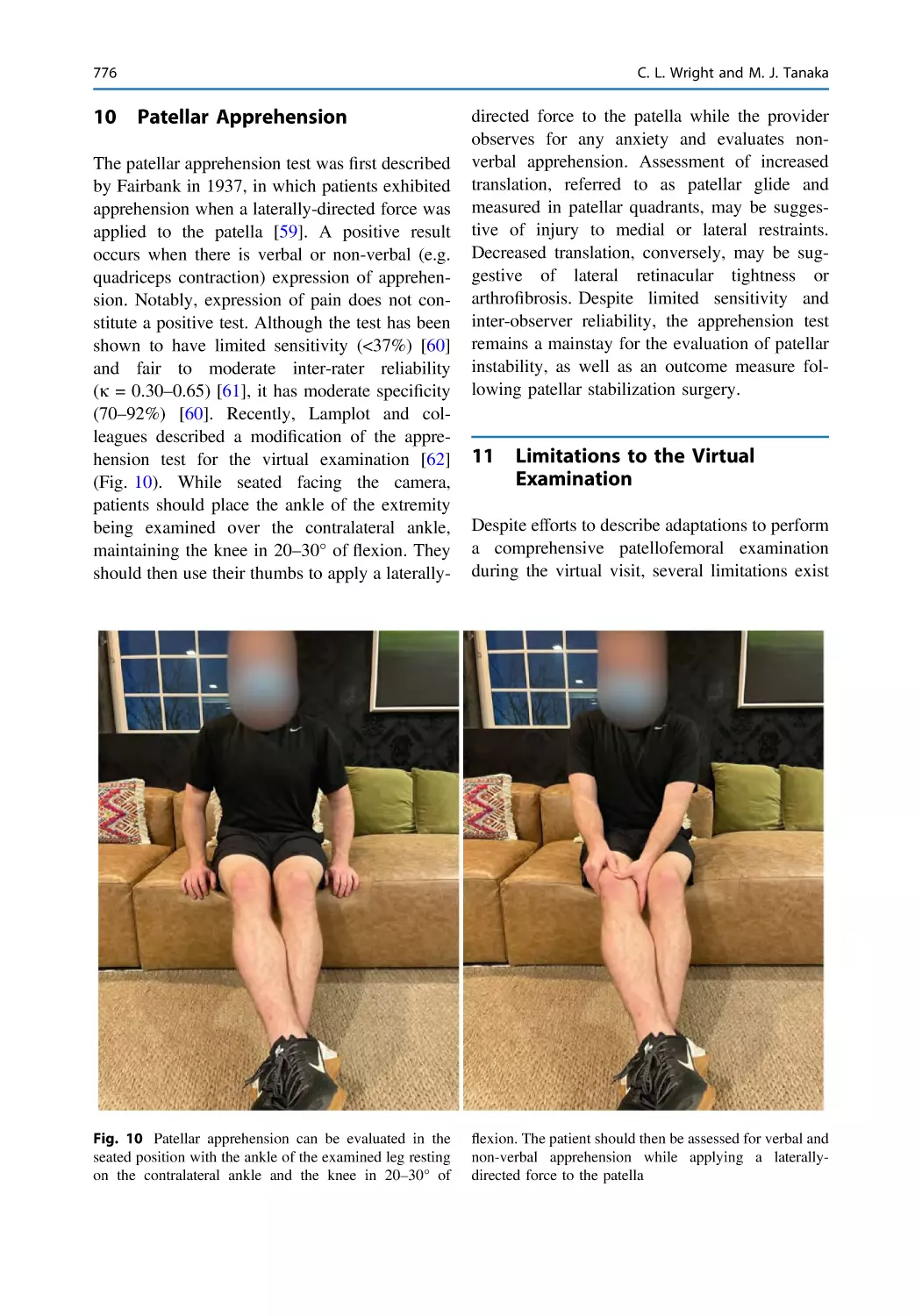
Anterior Knee Pain
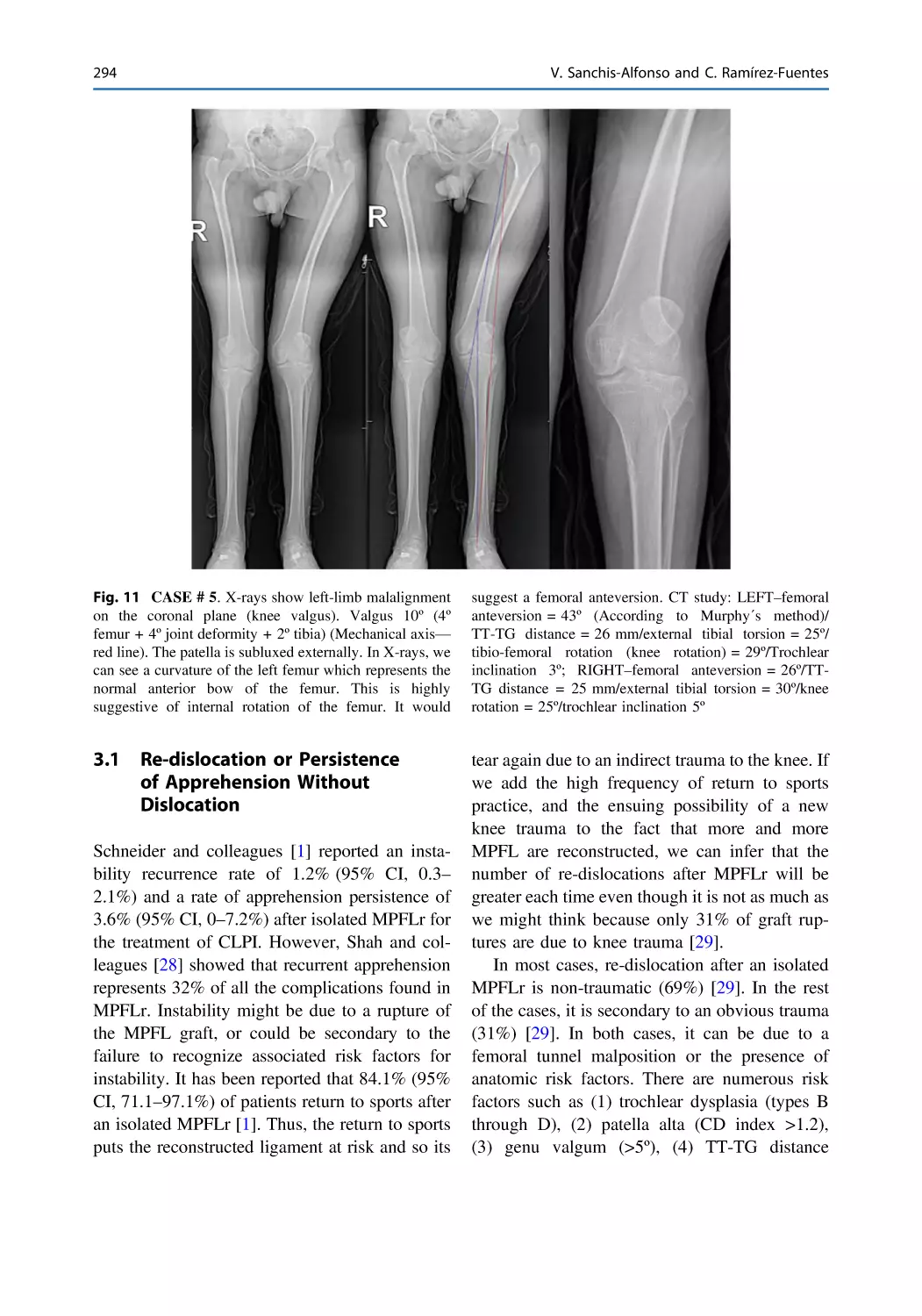
and Patellar Instability
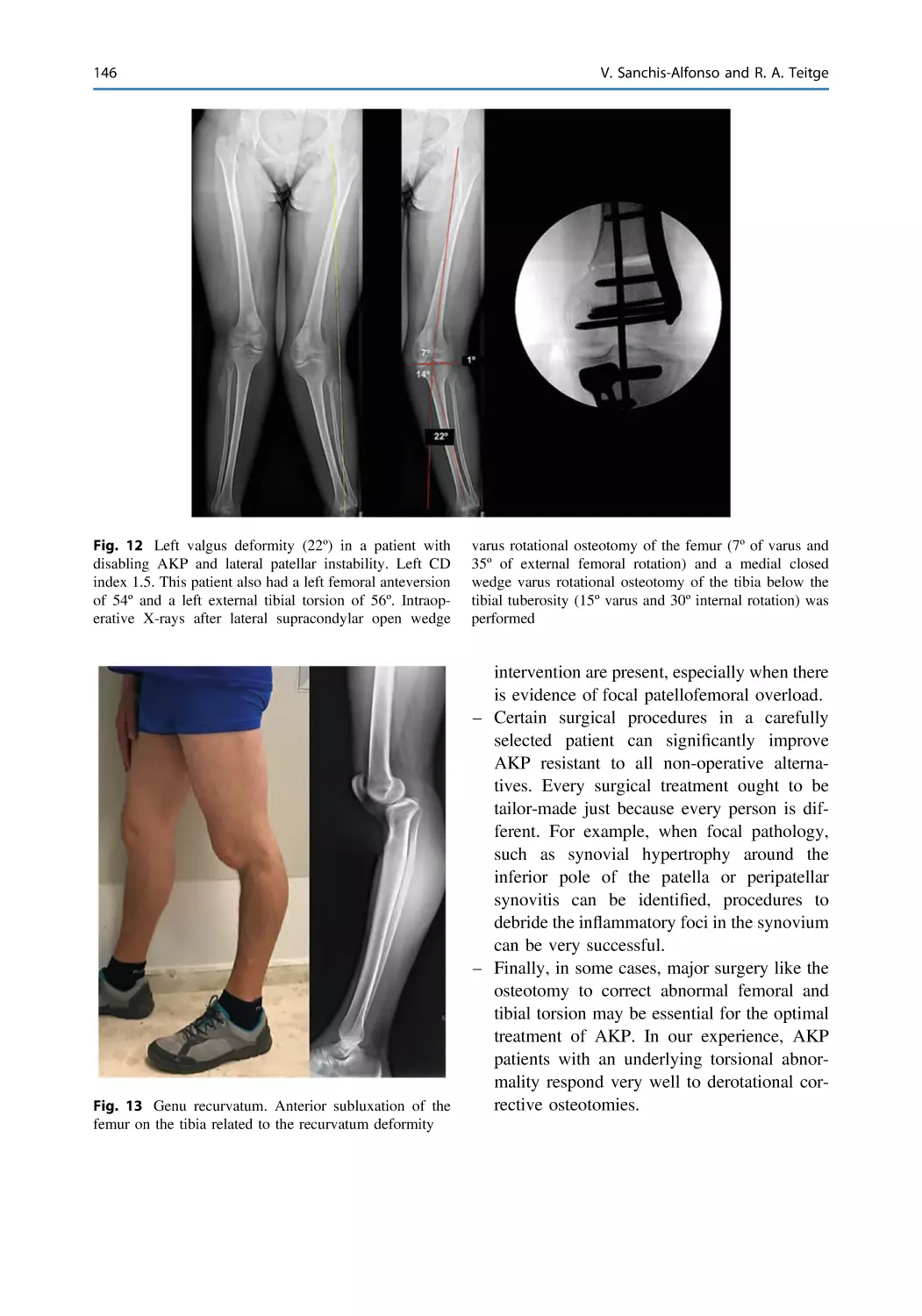
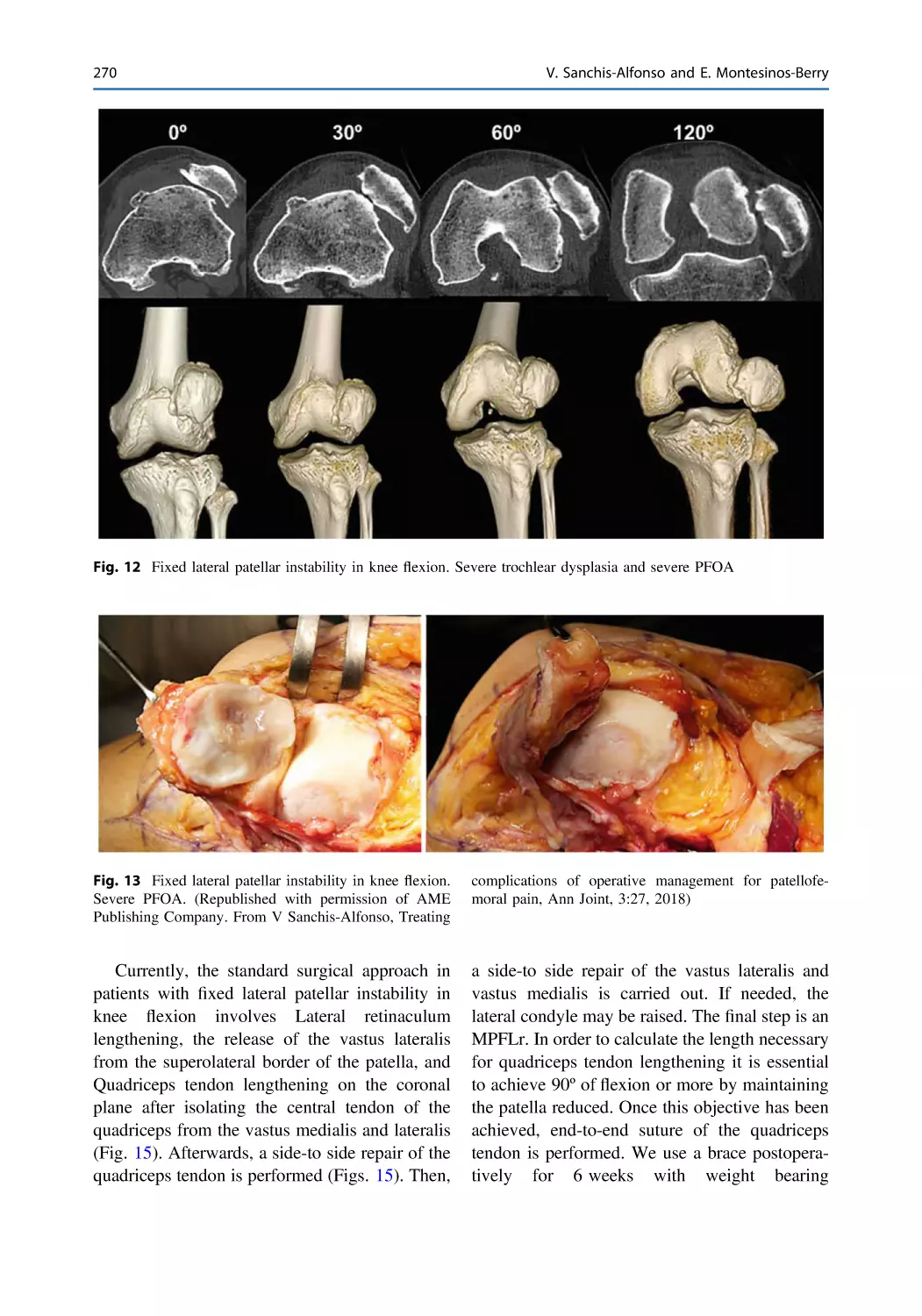
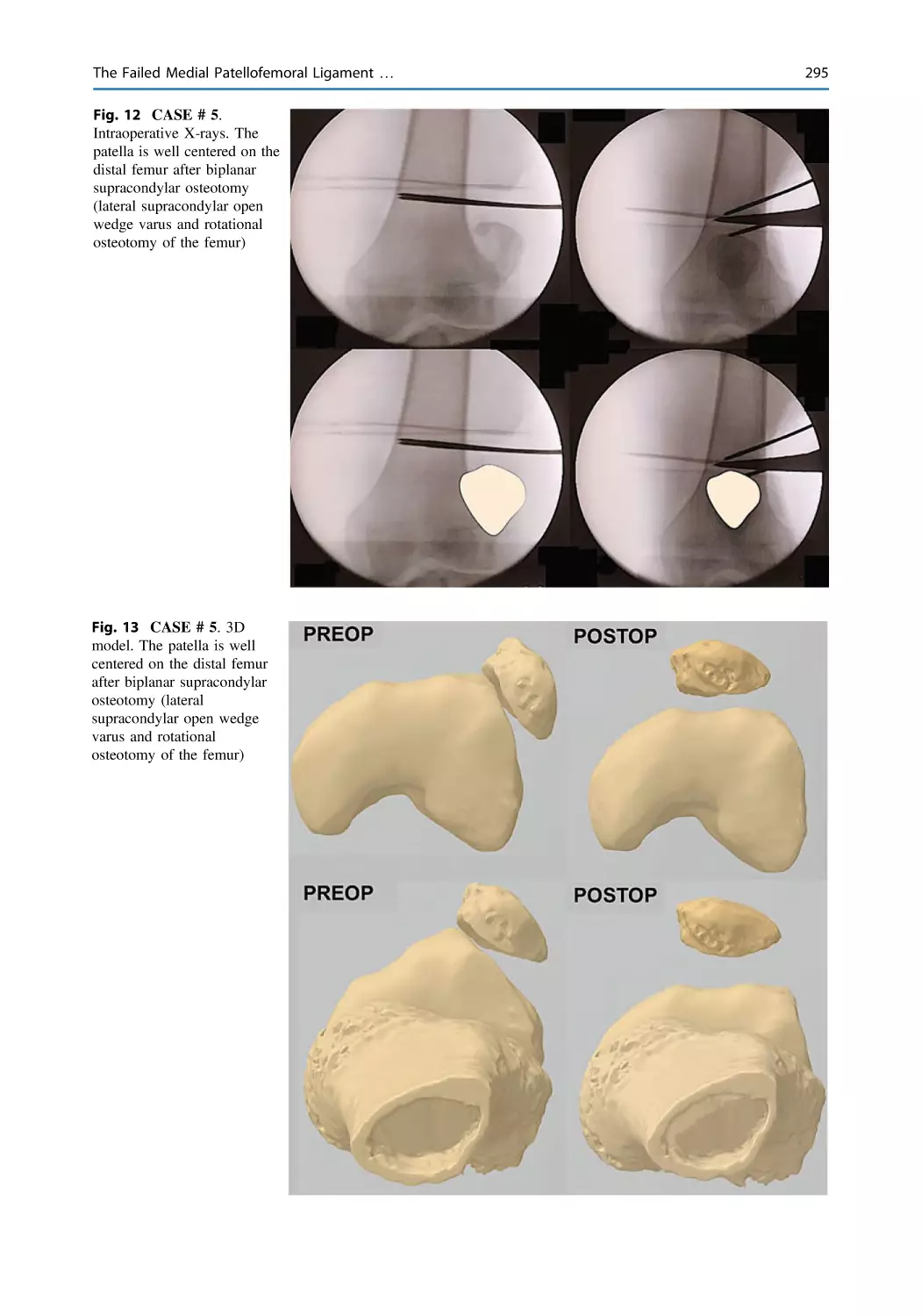
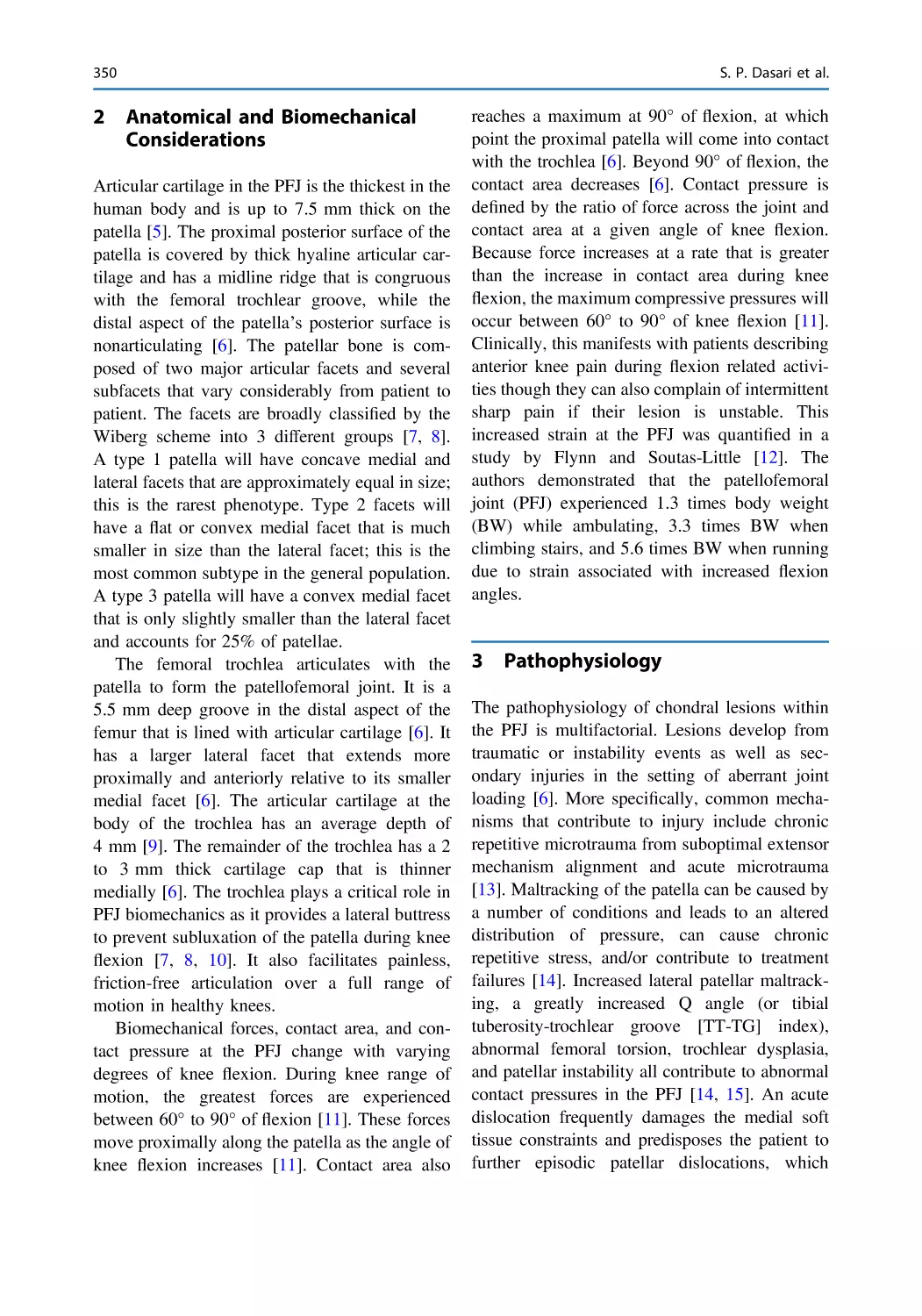
Third Edition
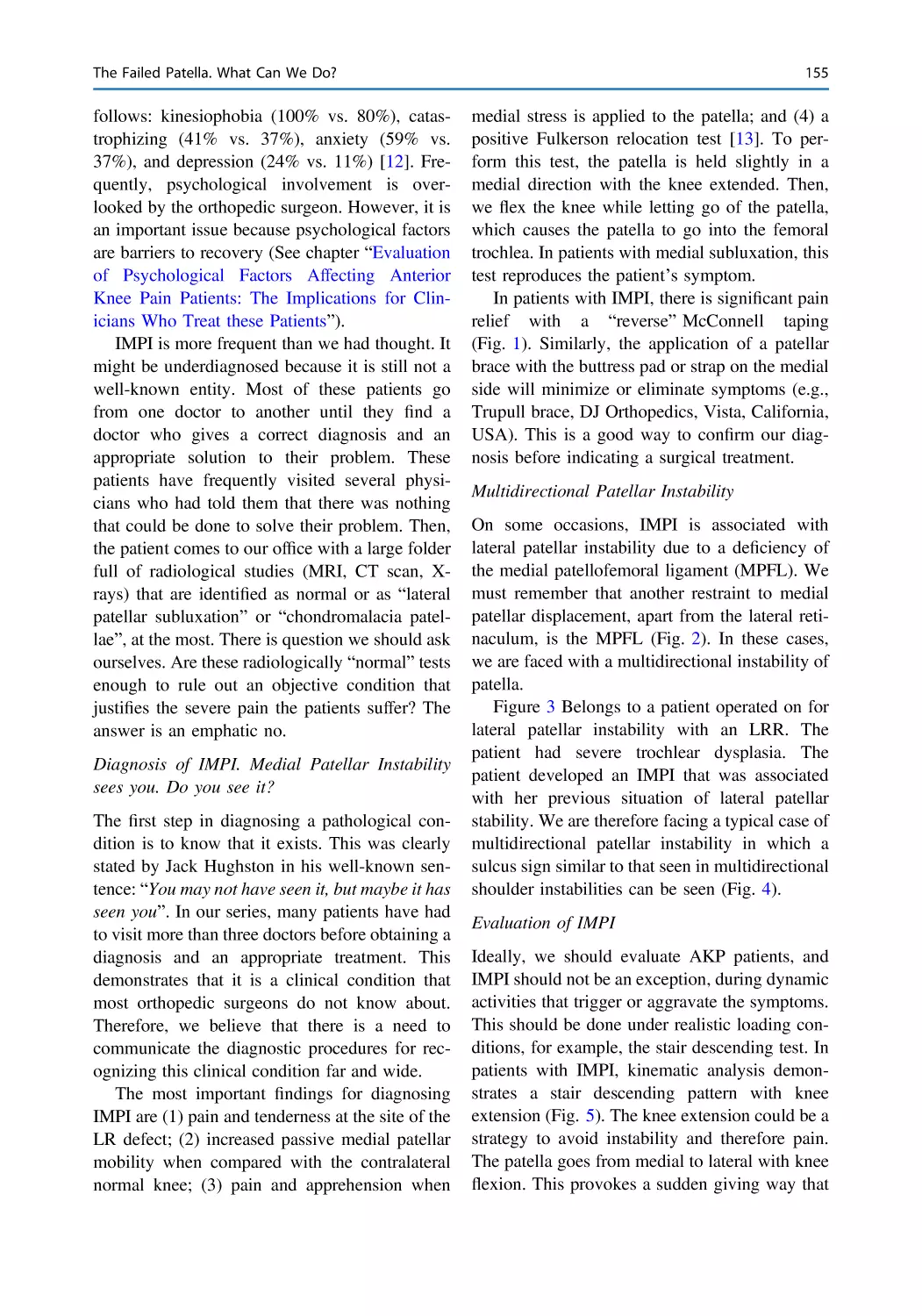
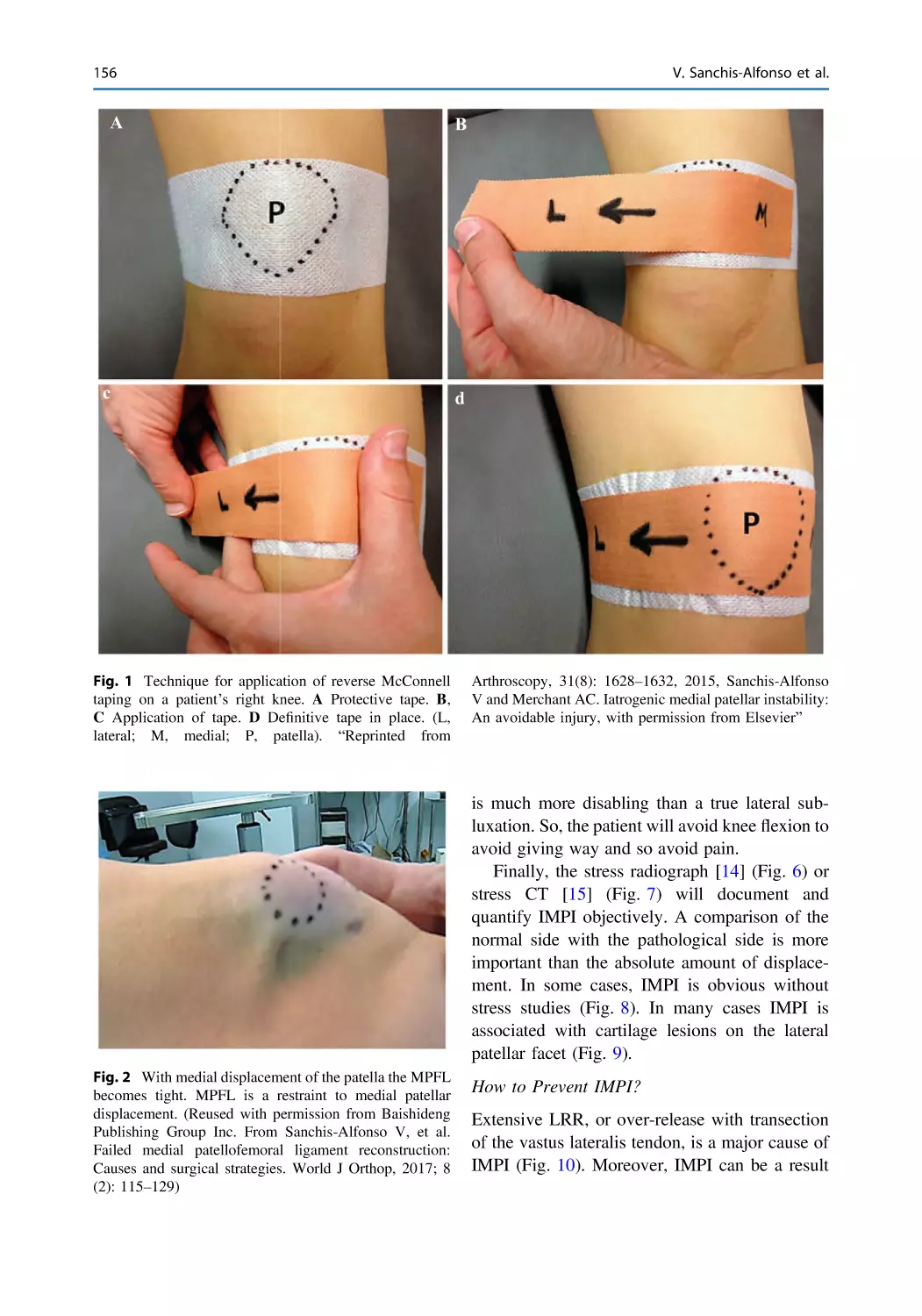
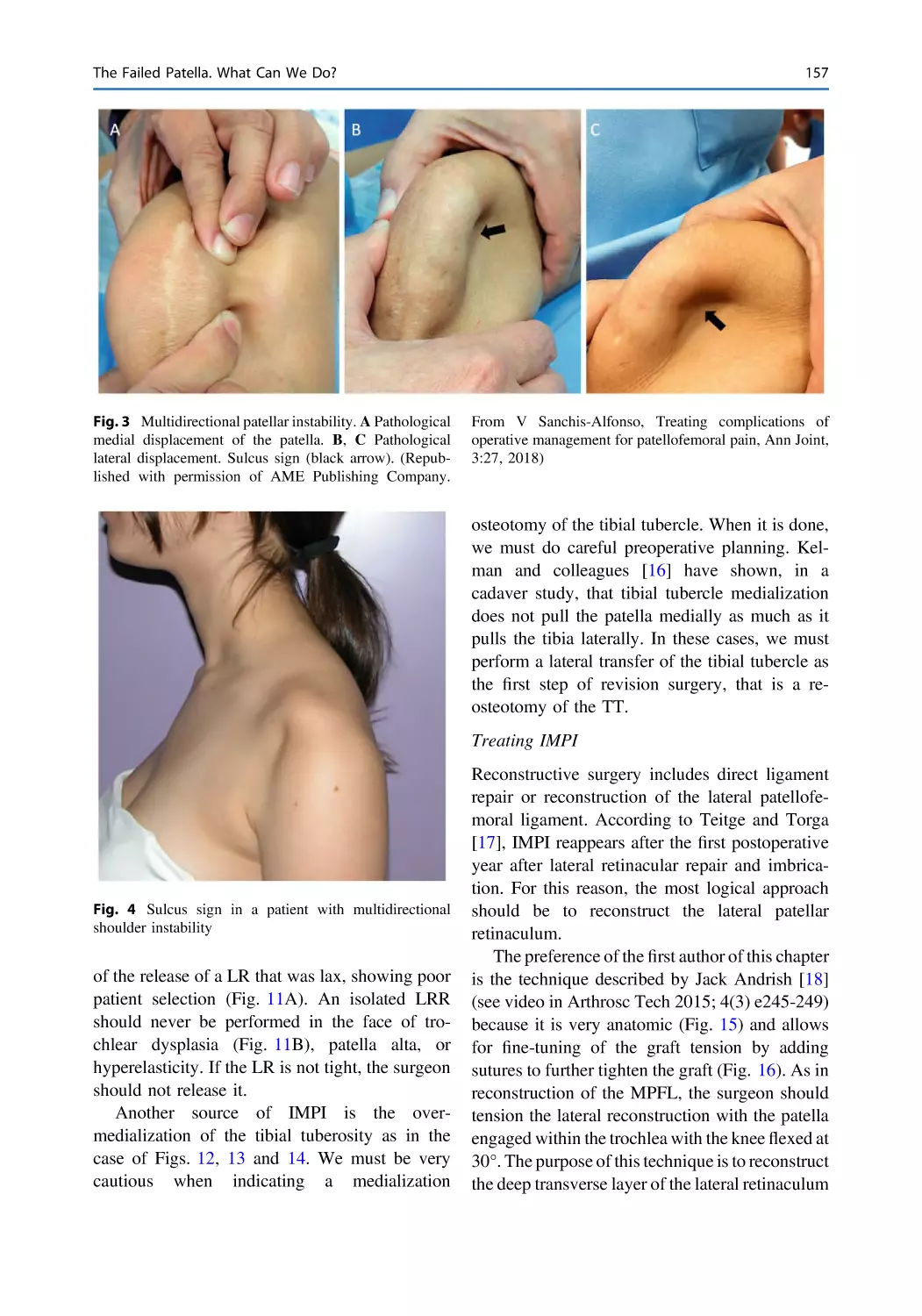
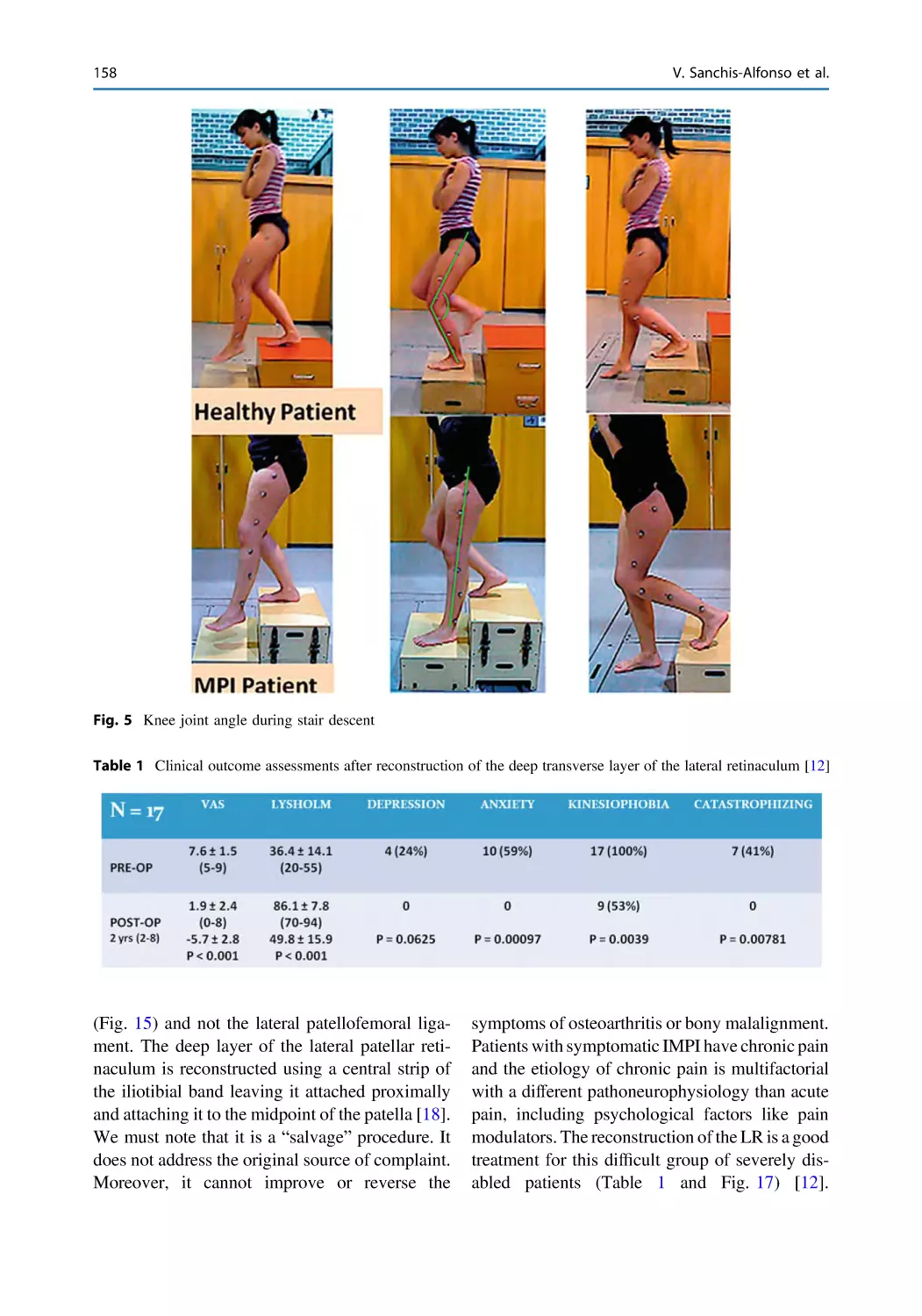
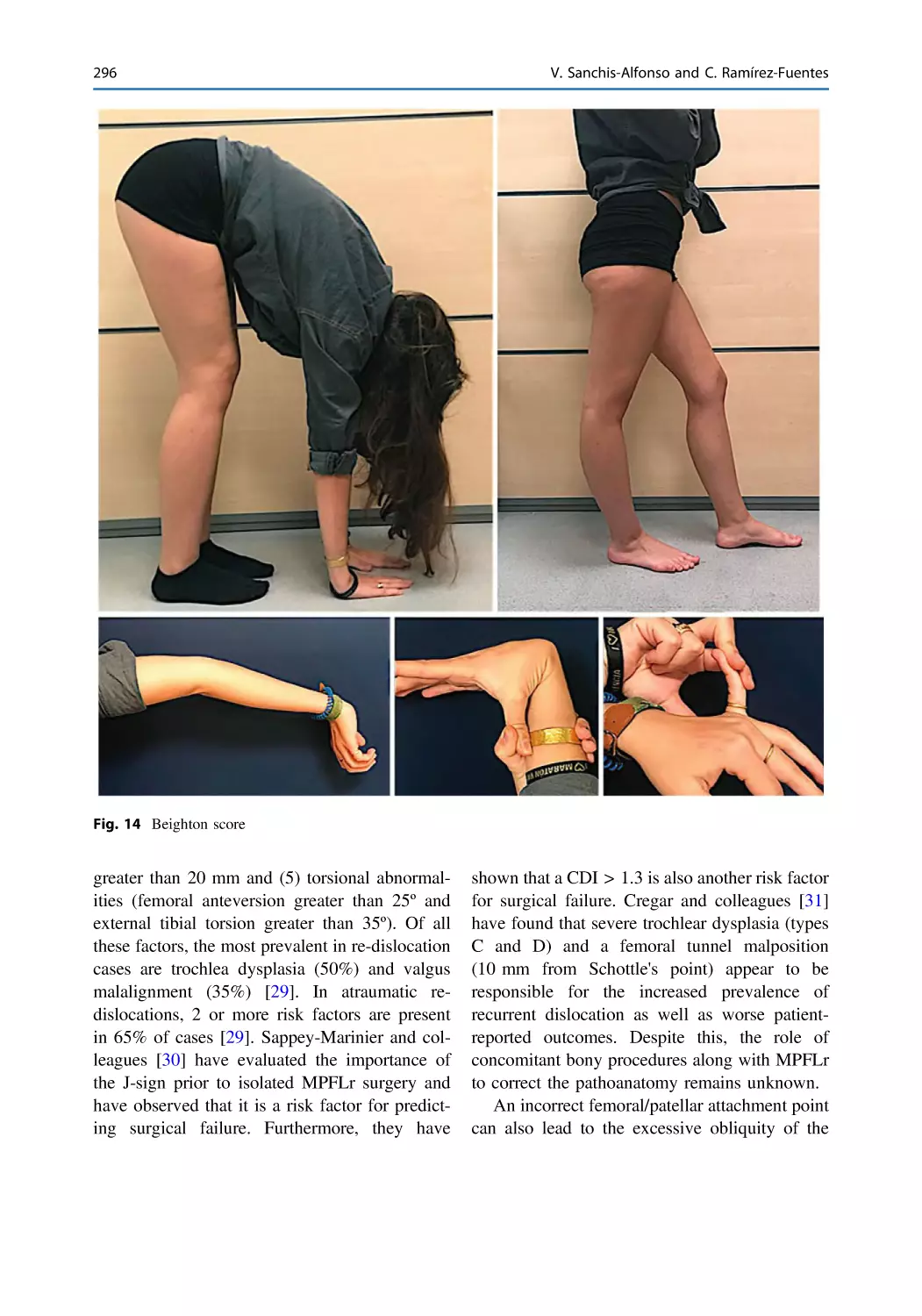
123
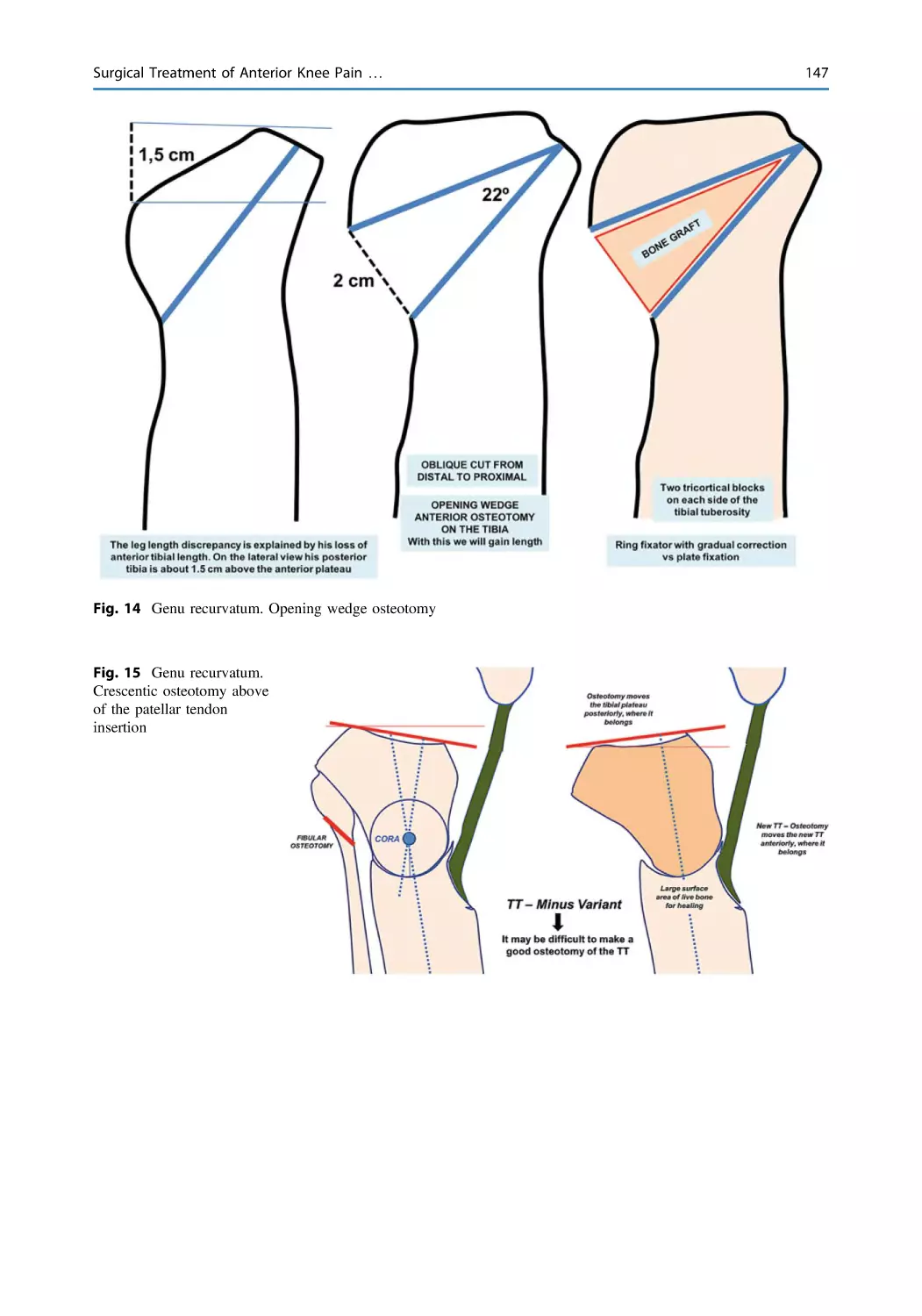
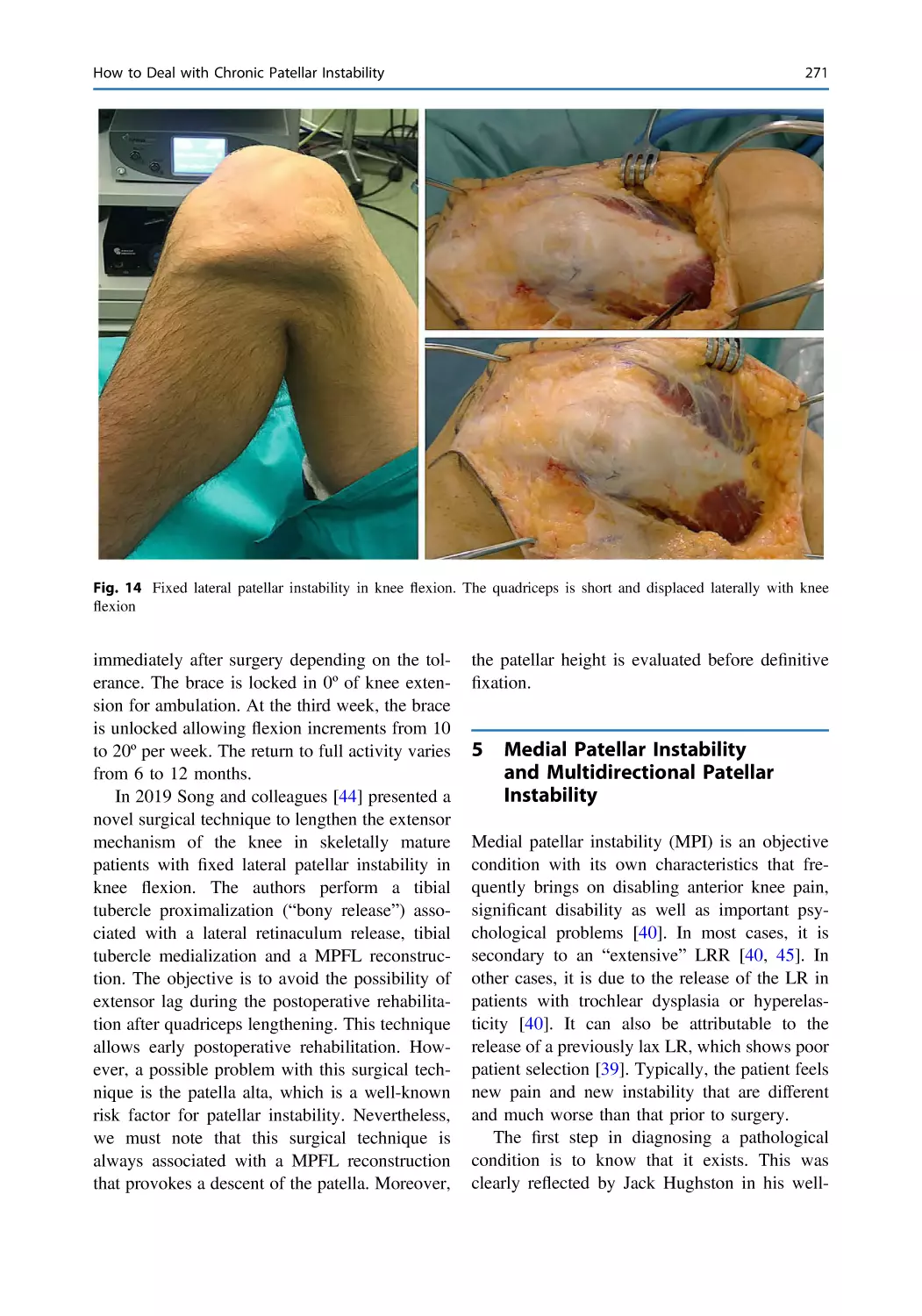
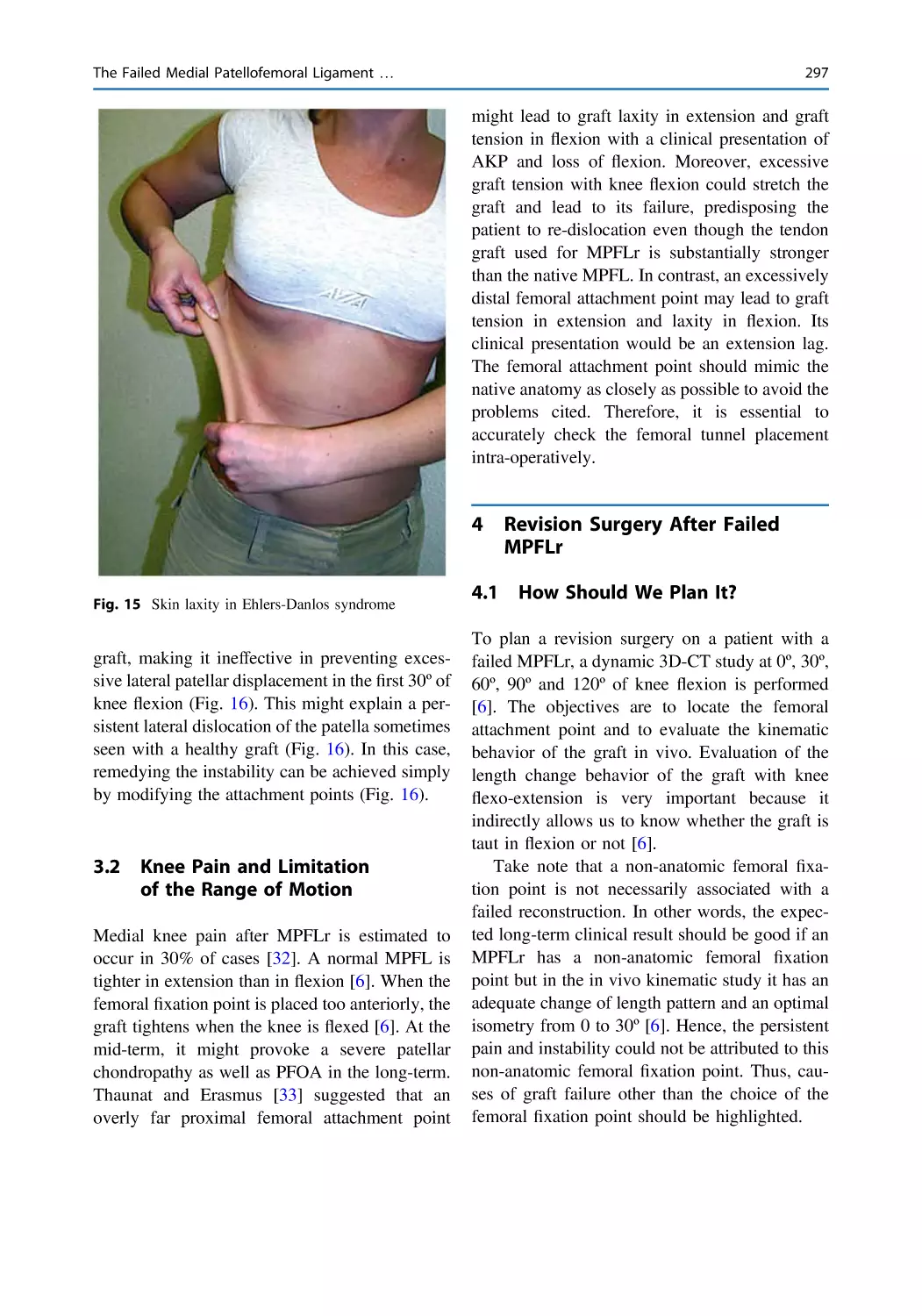
Editor
Vicente Sanchis-Alfonso
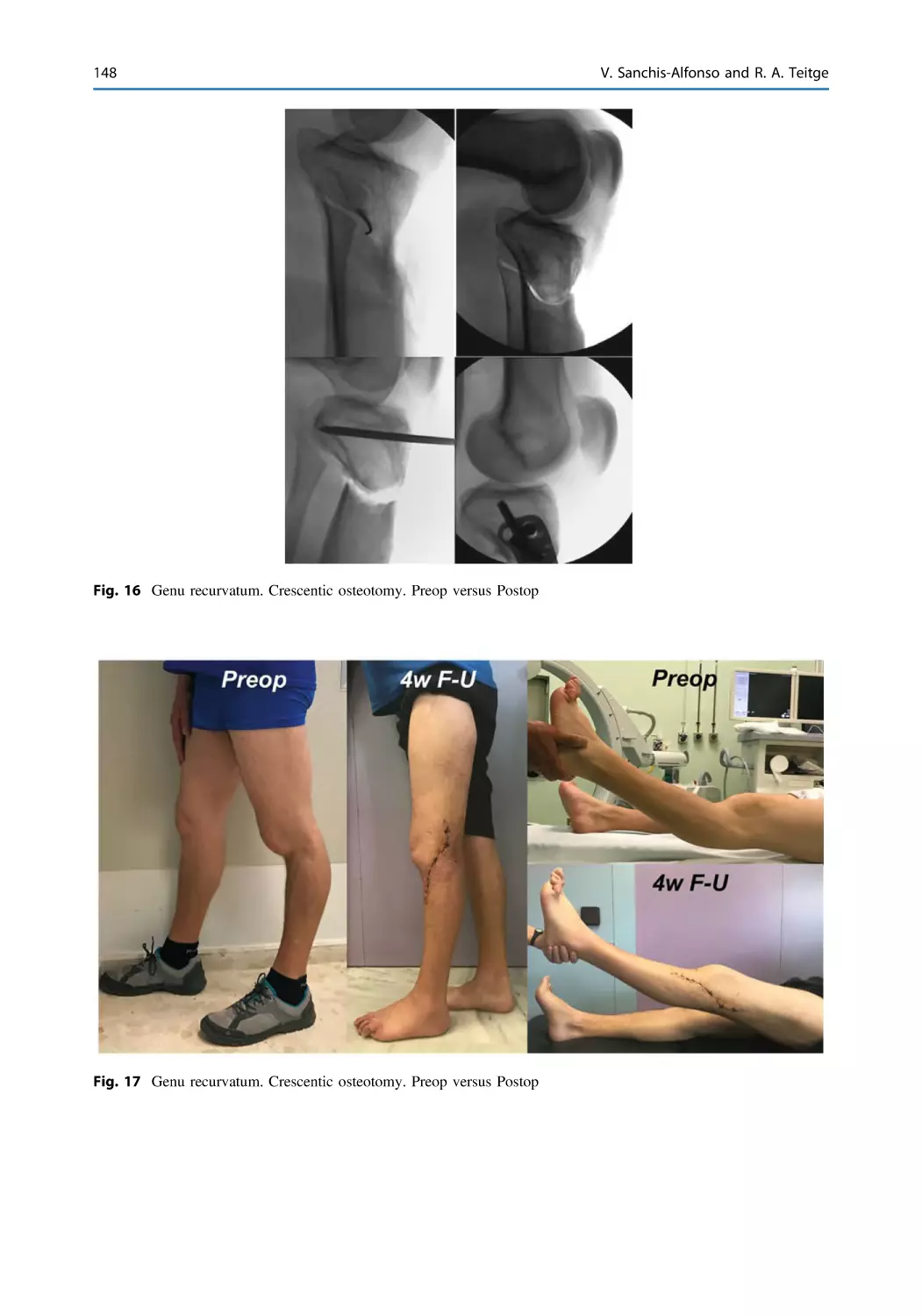
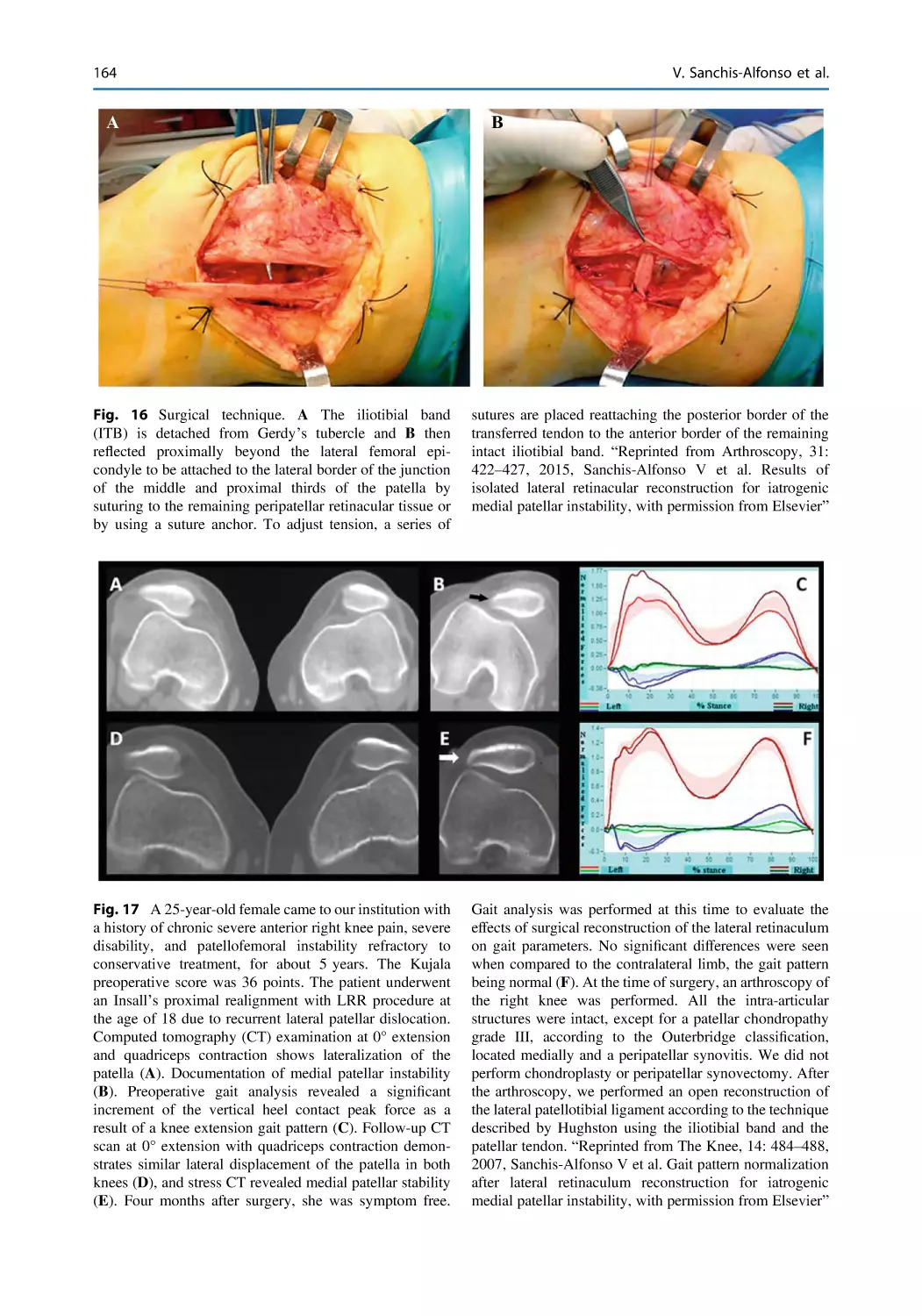
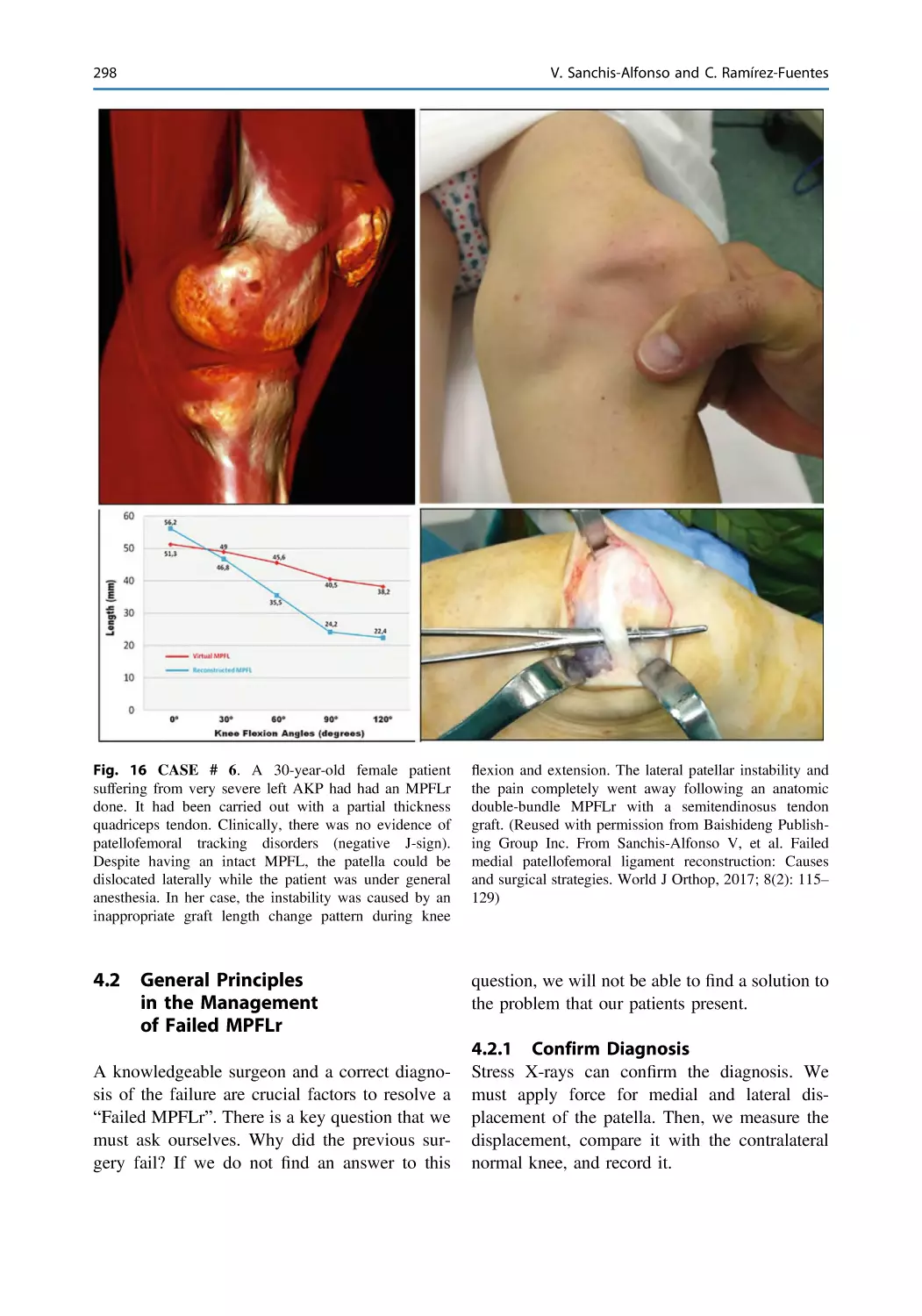
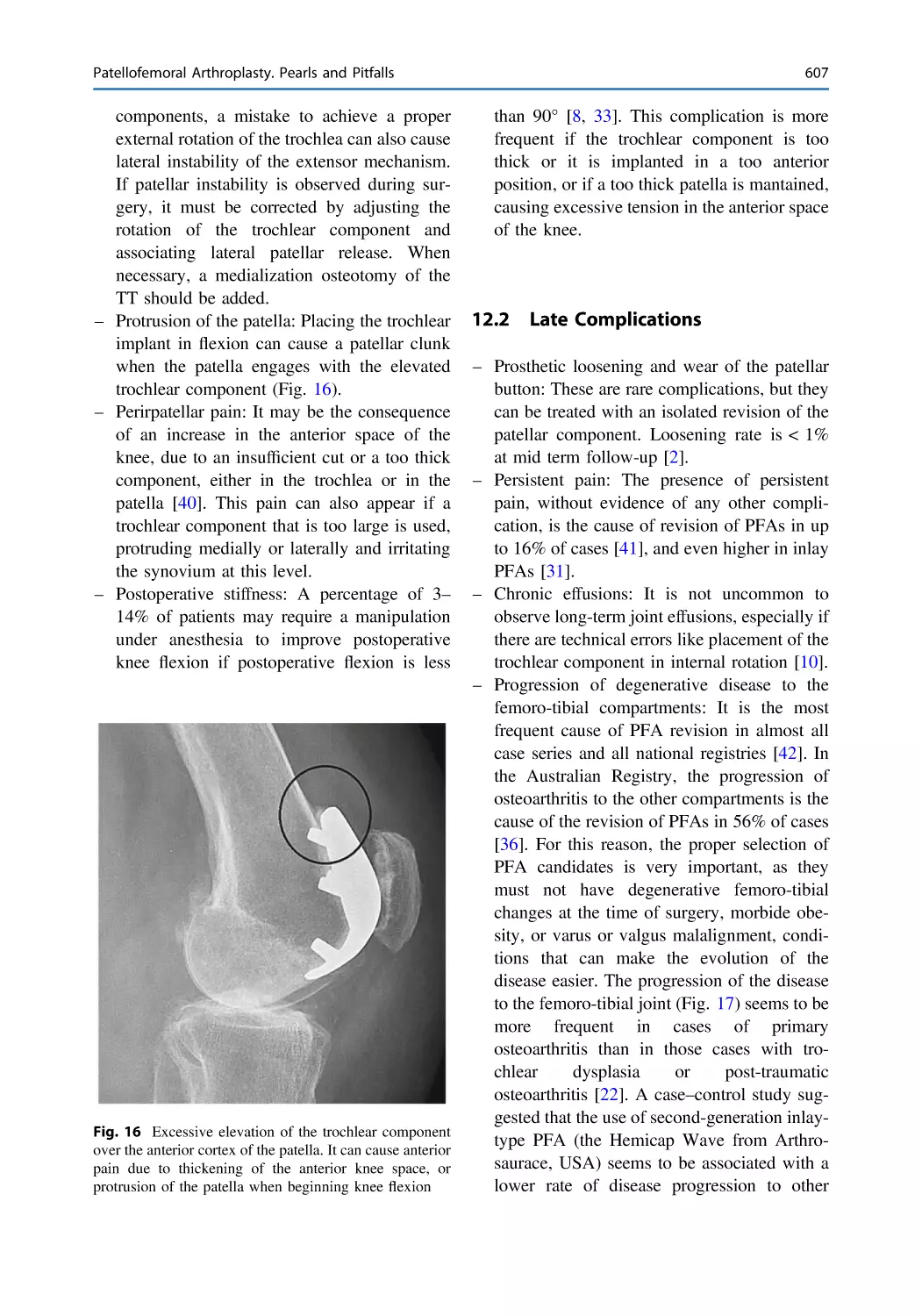
Department of Orthopedic Surgery
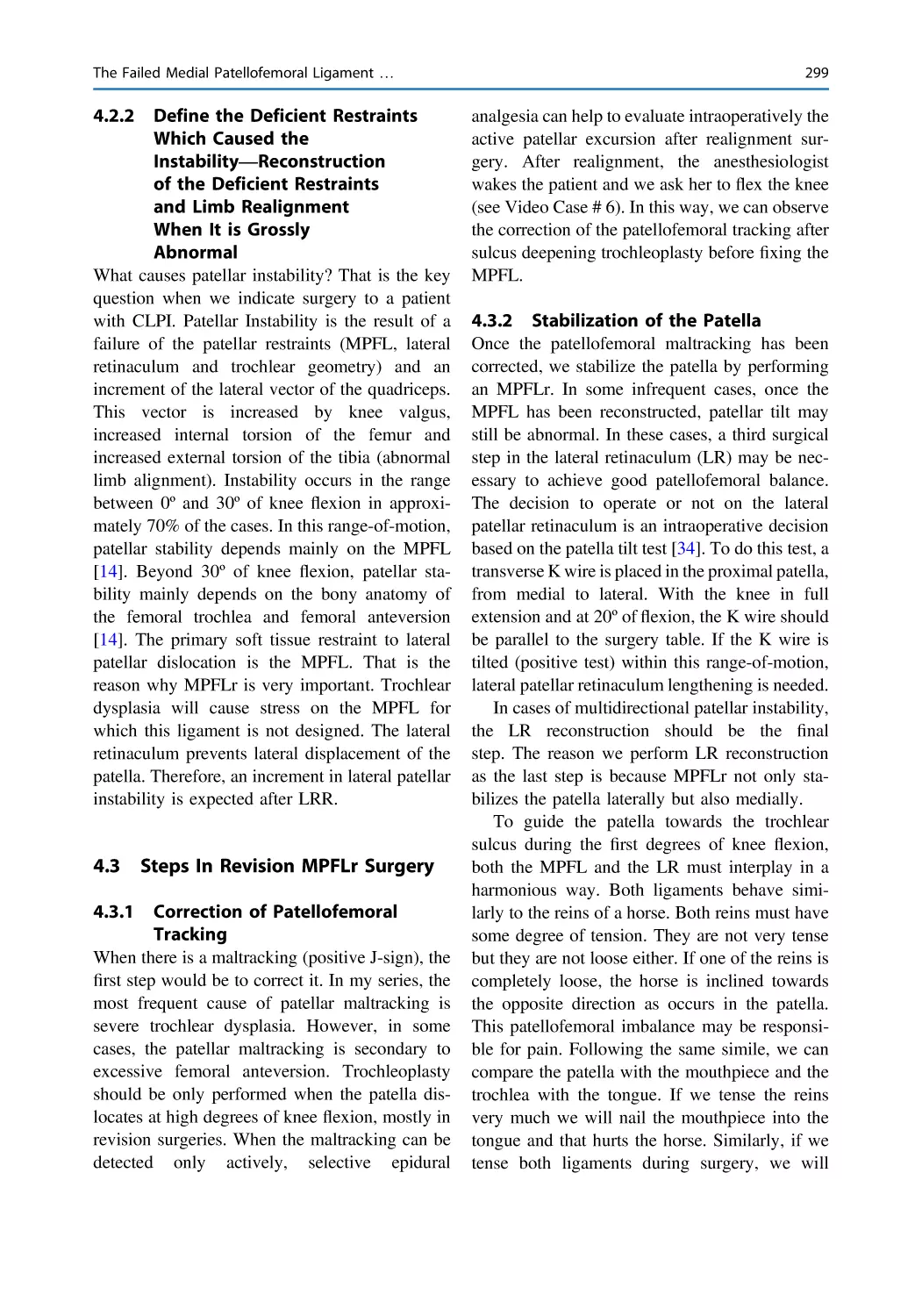
Hospital Arnau de Vilanova
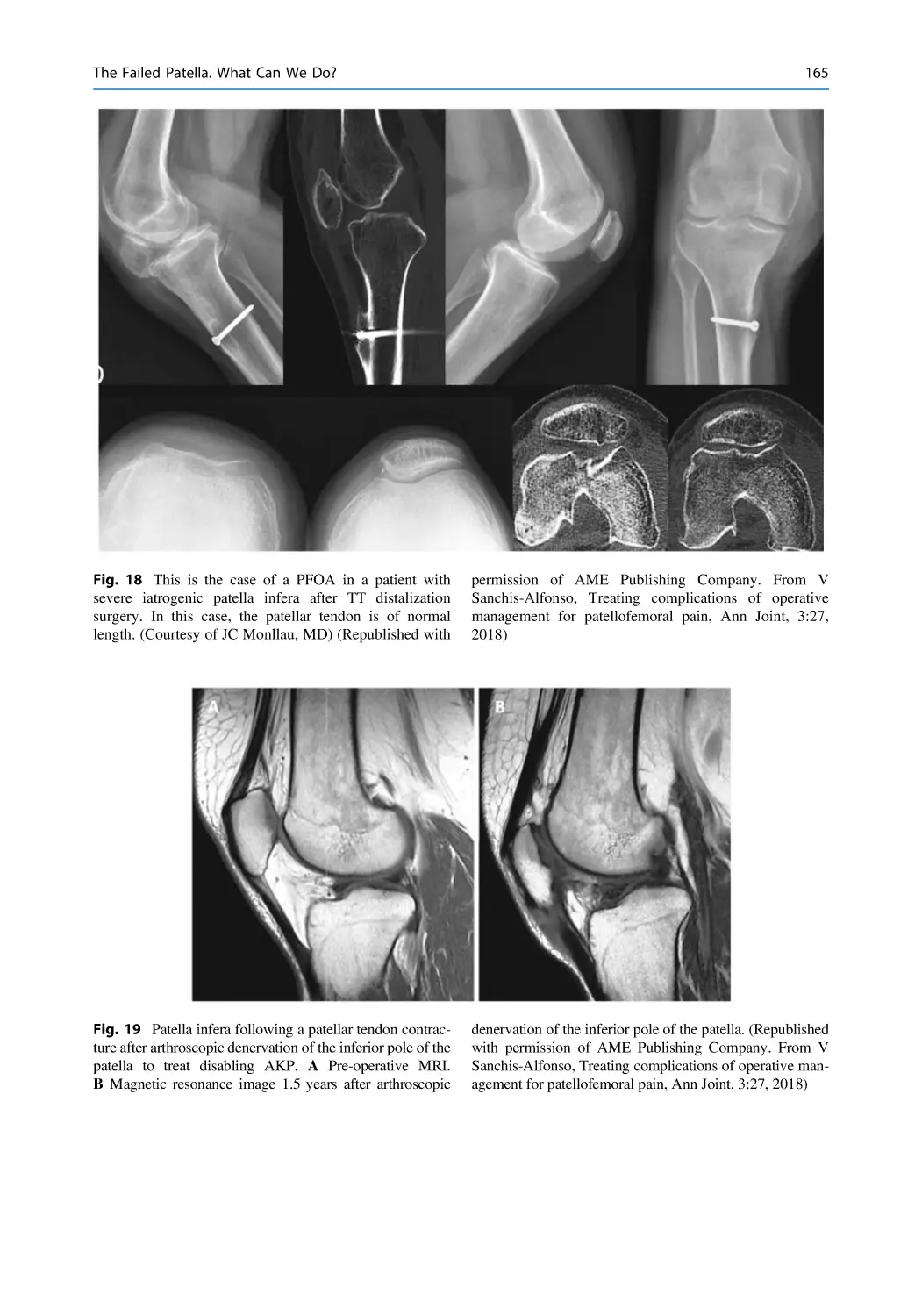
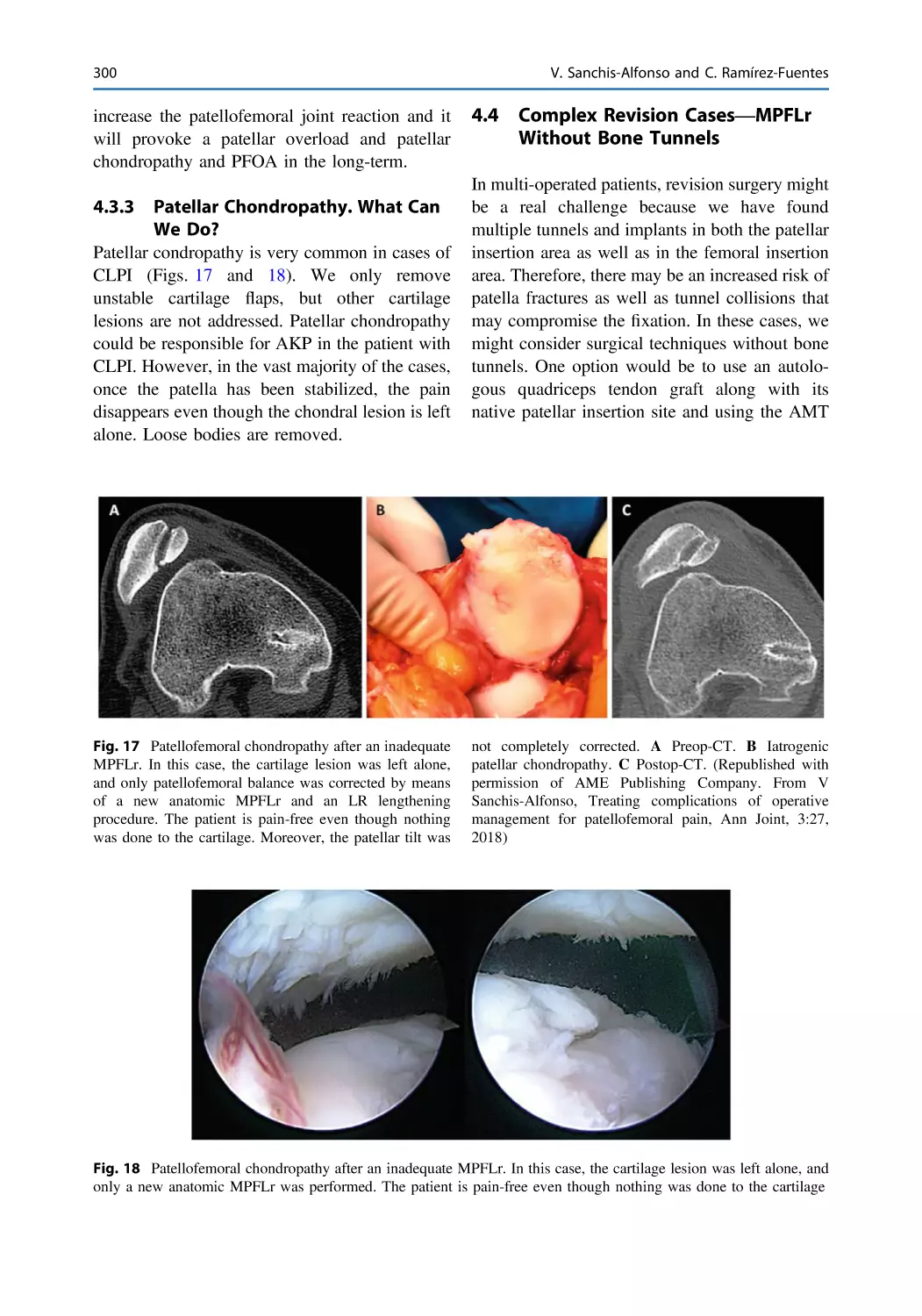
Valencia, Spain
ISBN 978-3-031-09766-9
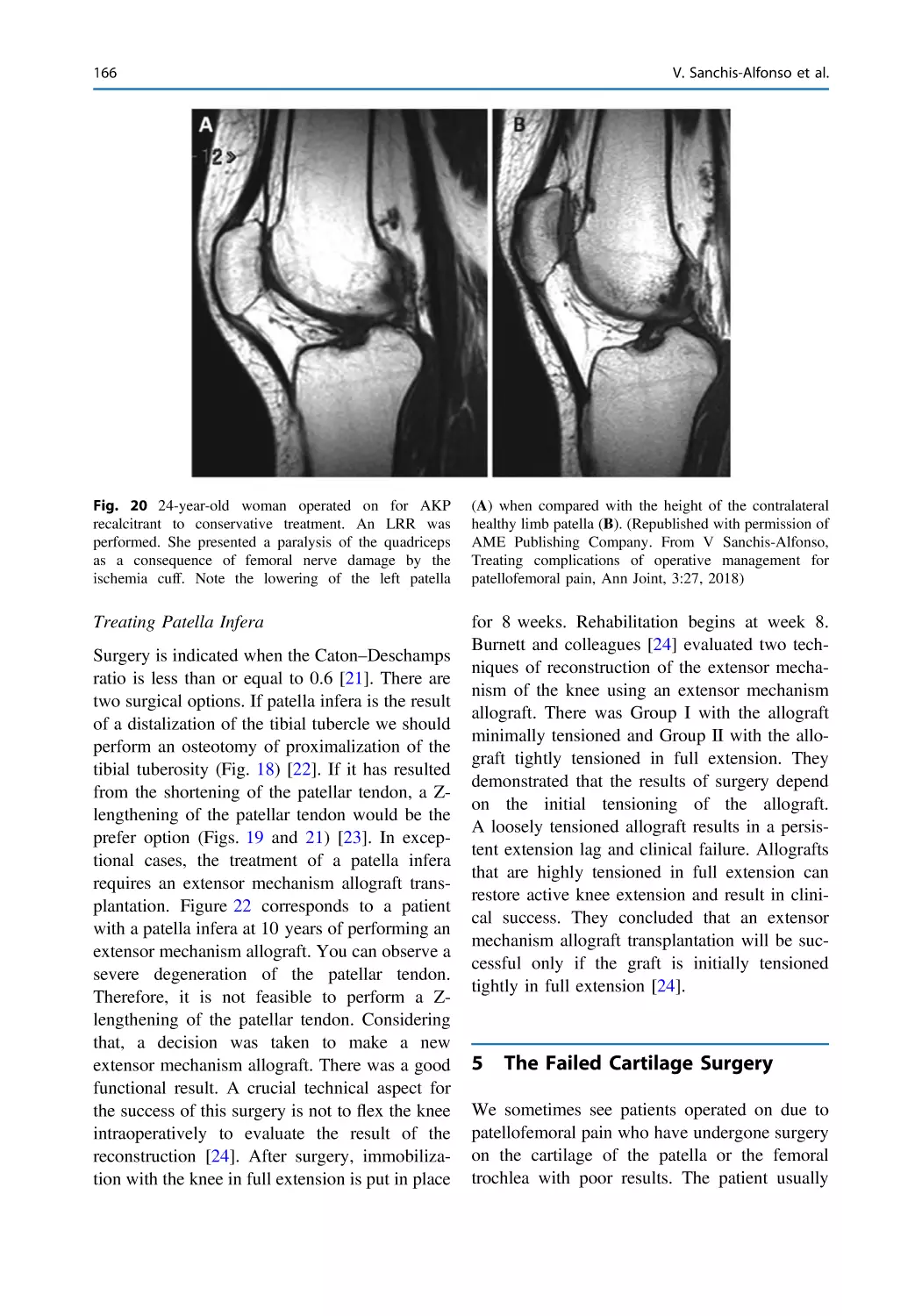
ISBN 978-3-031-09767-6
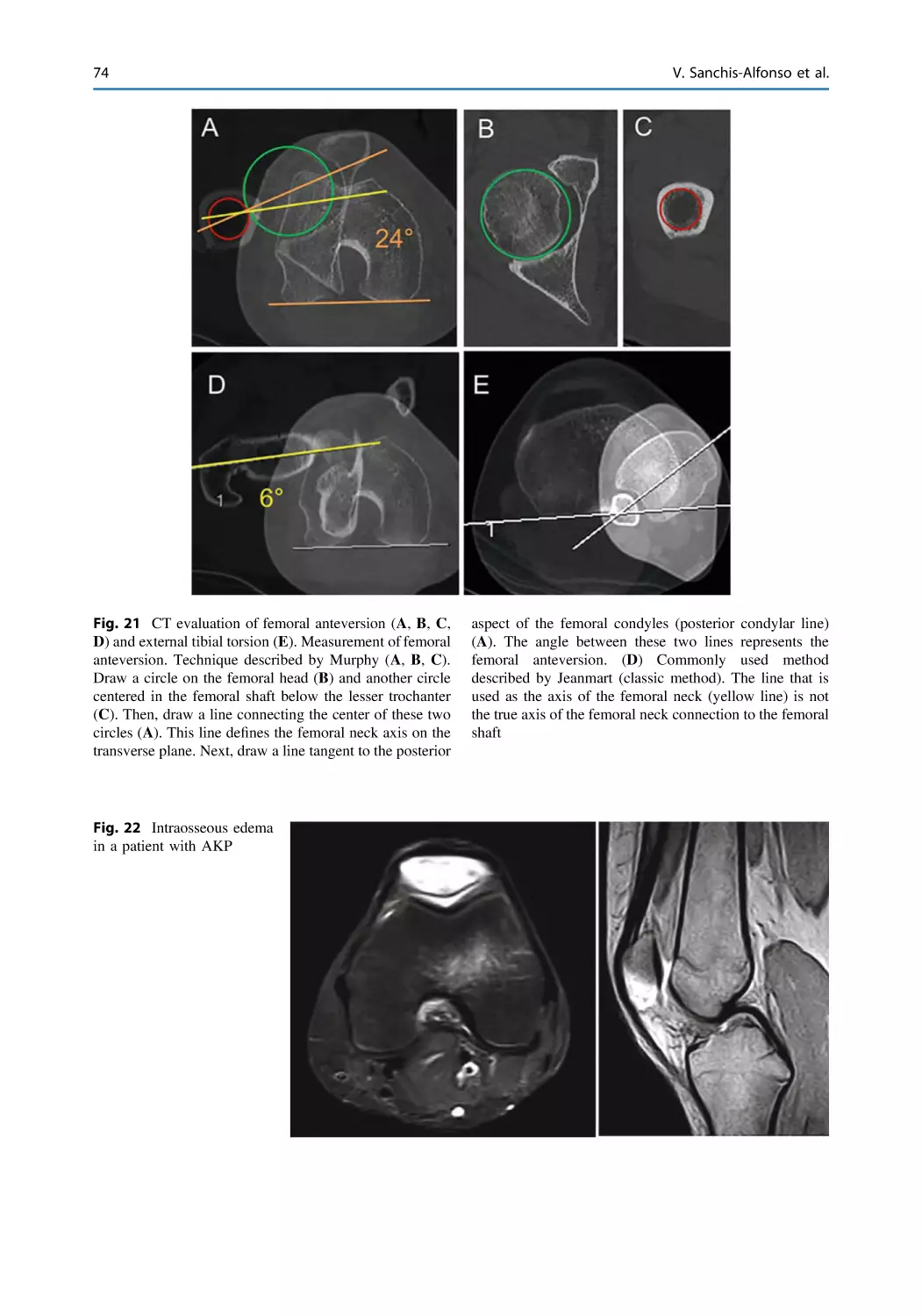
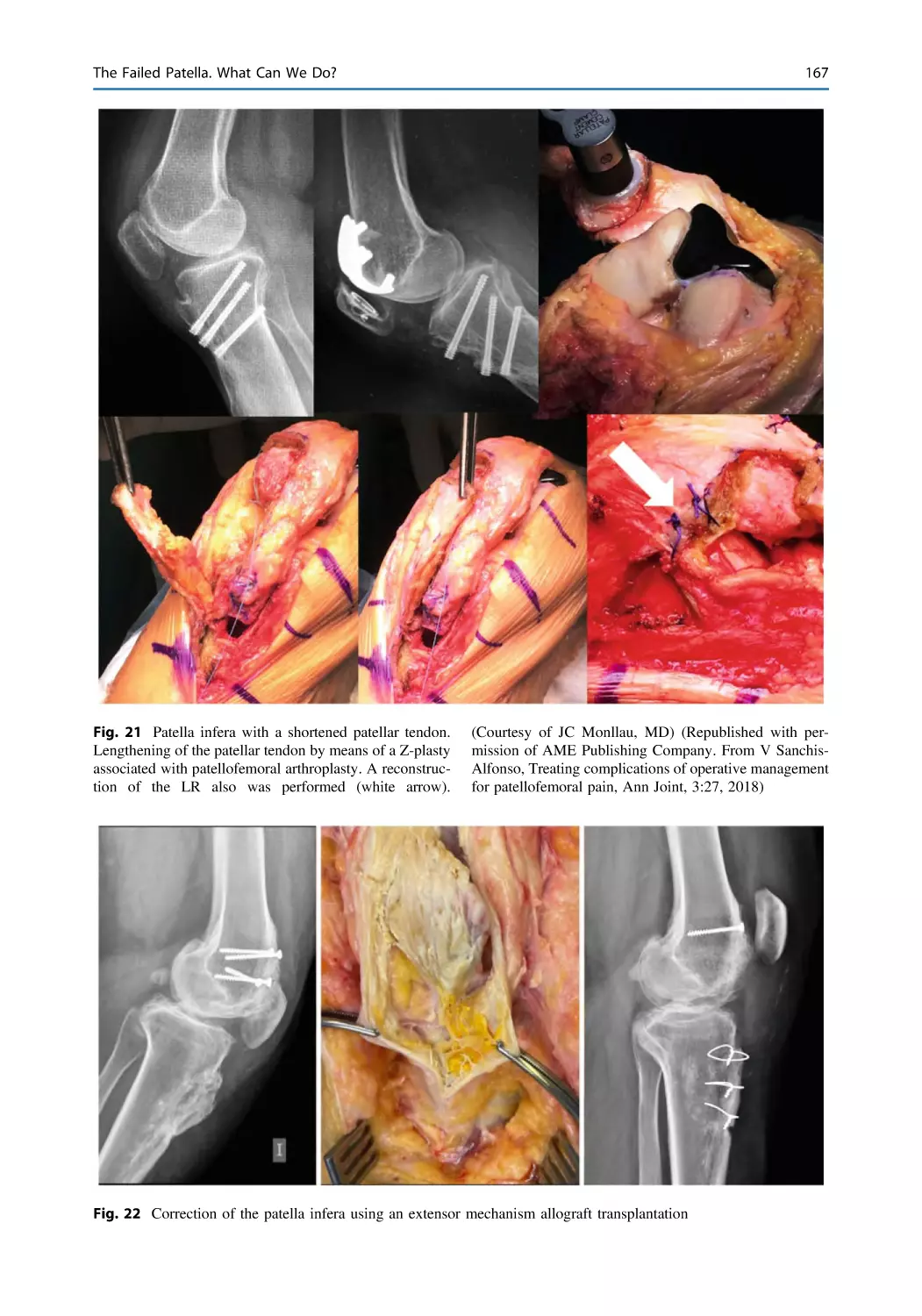
https://doi.org/10.1007/978-3-031-09767-6
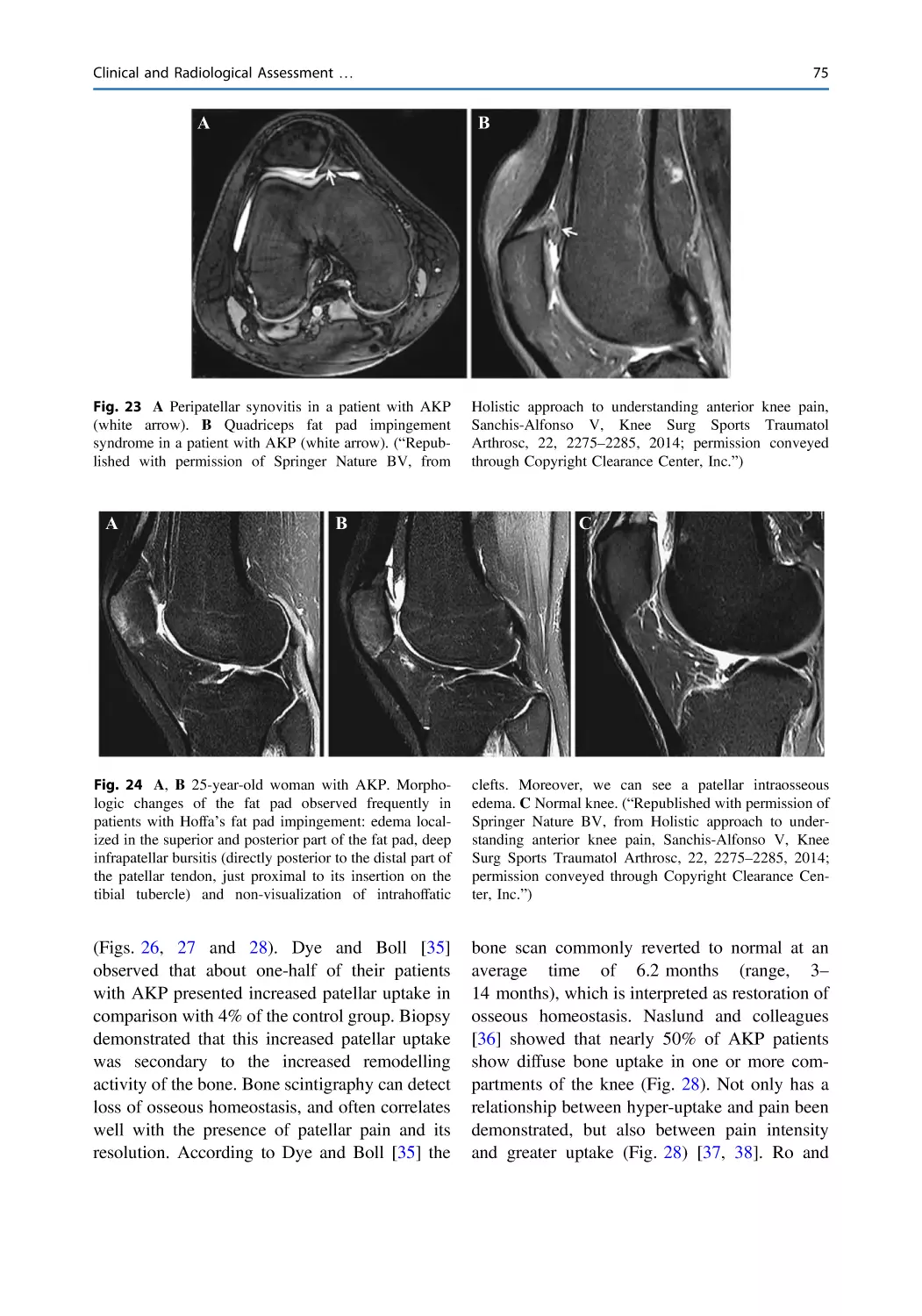
(eBook)
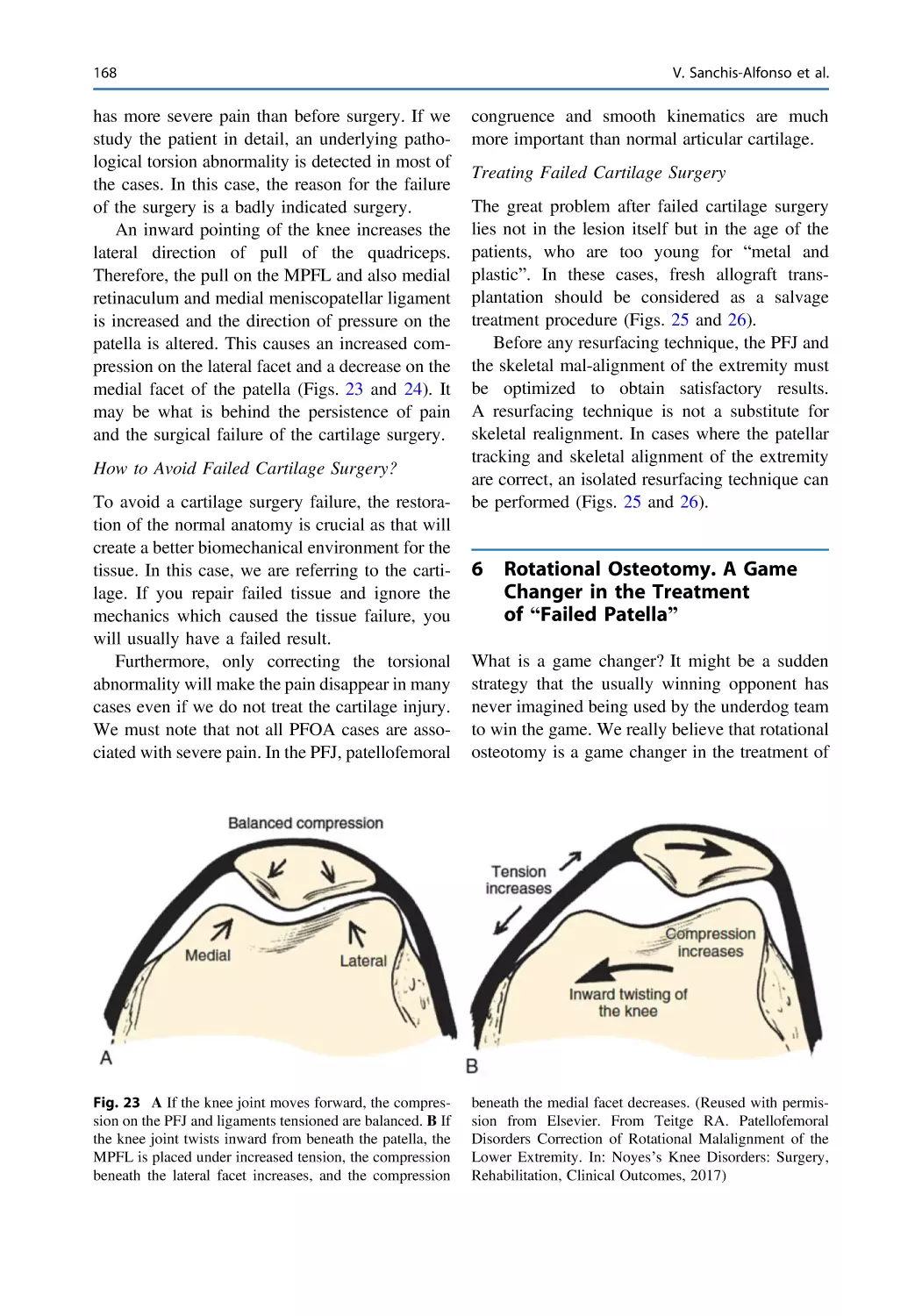
1st edition: © Springer-Verlag London Limited 2006
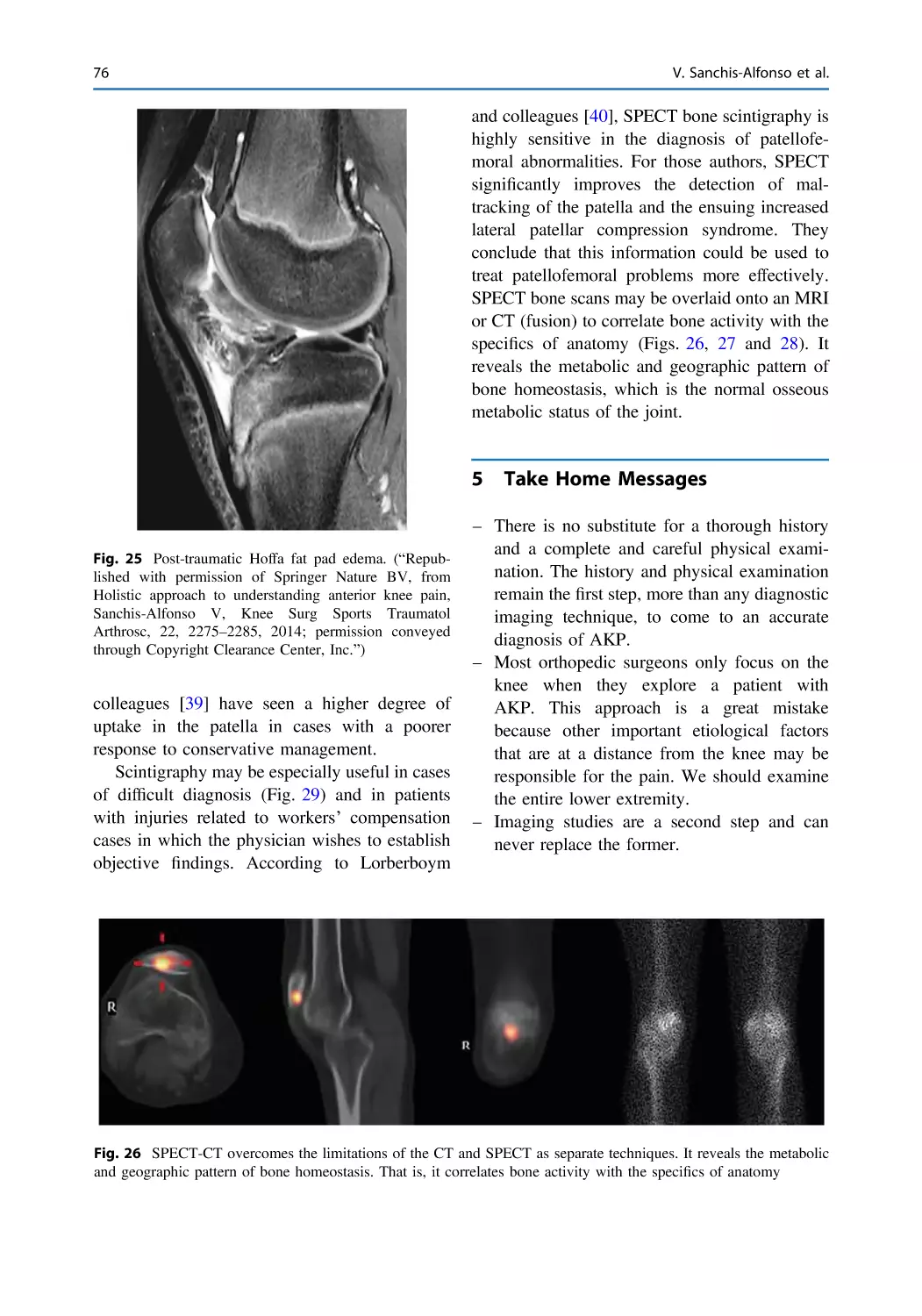
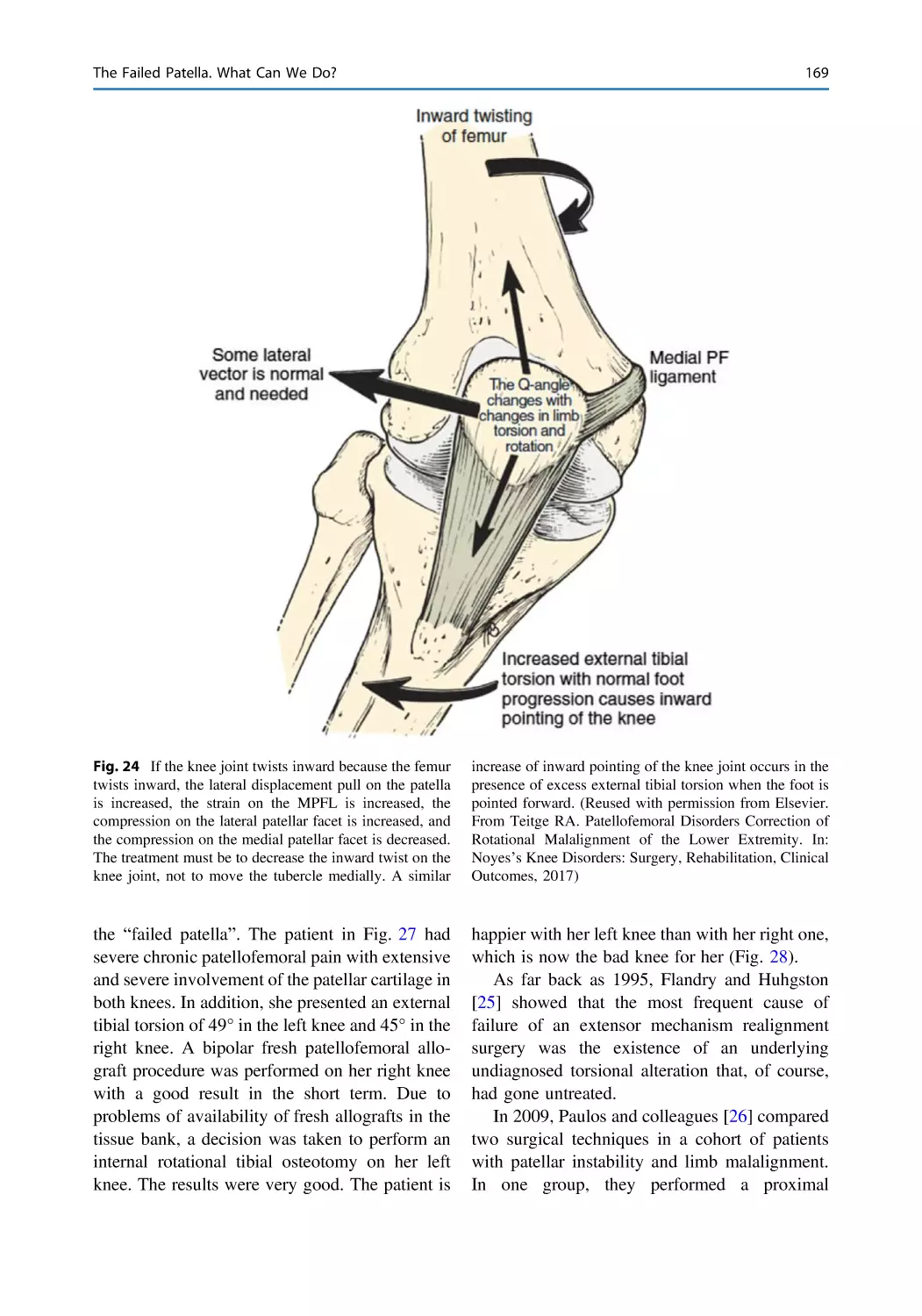
2nd edition: © Springer-Verlag London Limited 2011
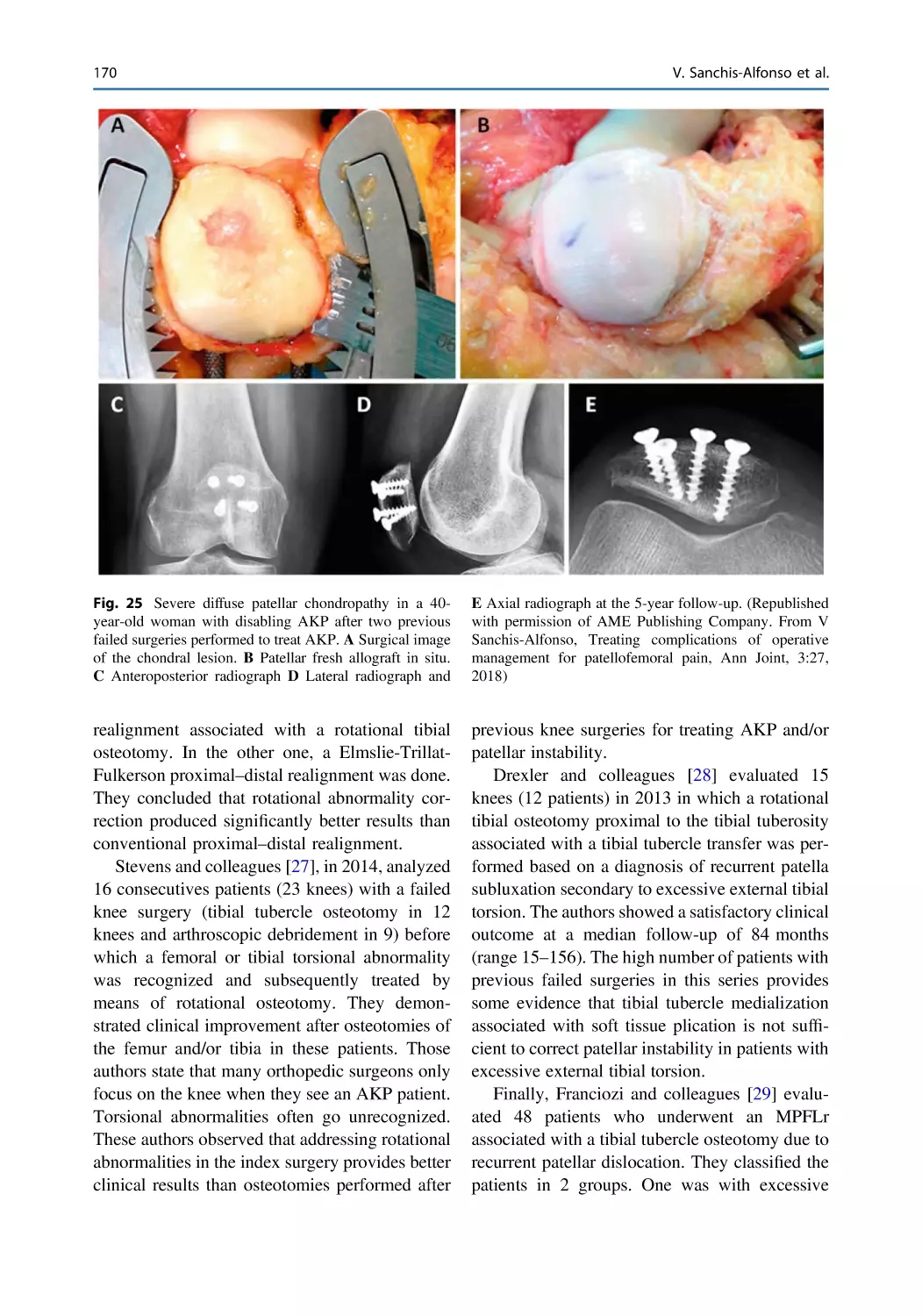
3rd edition: © The Editor(s) (if applicable) and The Author(s), under exclusive license to
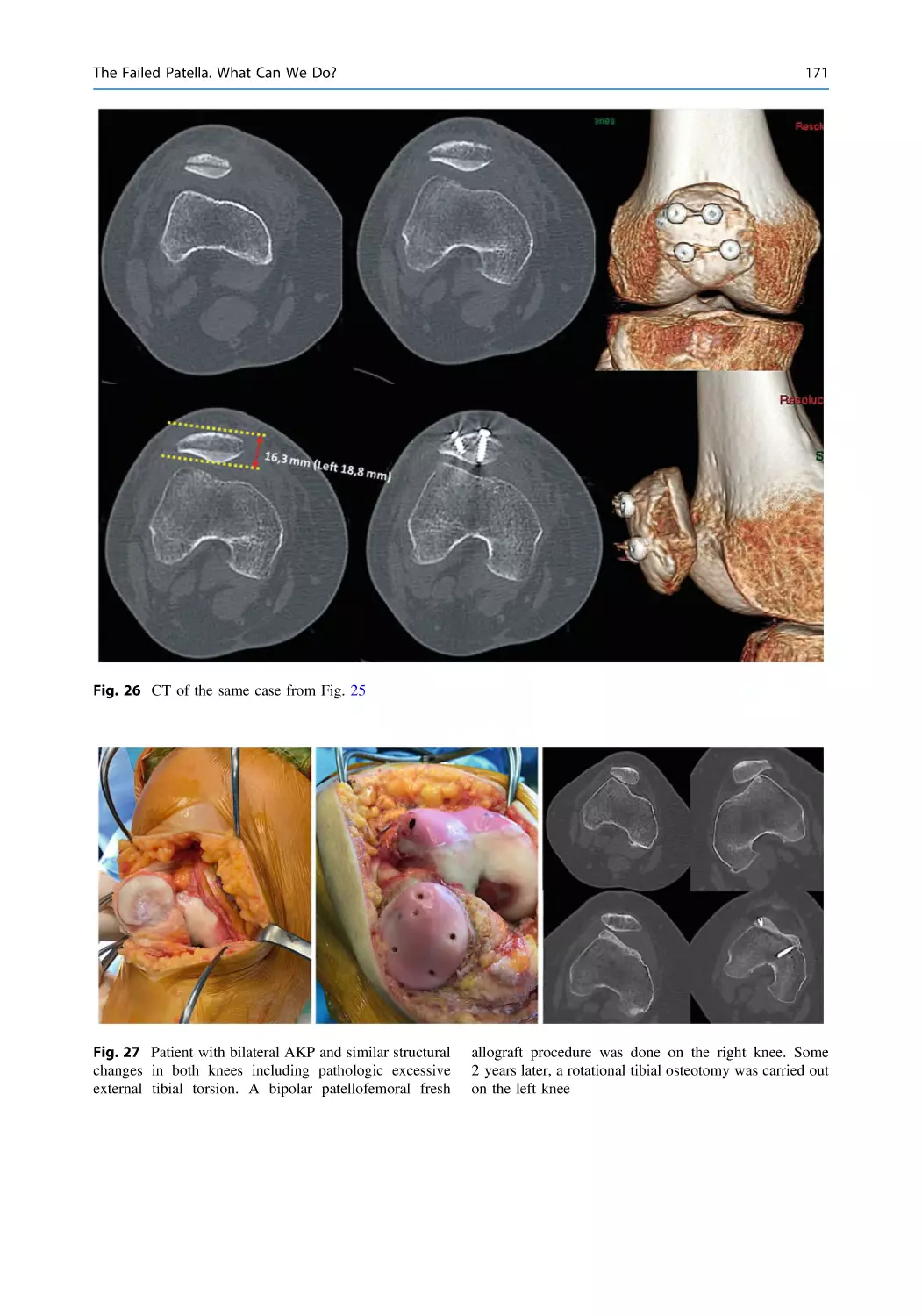
Springer Nature Switzerland AG 2023
This work is subject to copyright. All rights are solely and exclusively licensed by the Publisher,
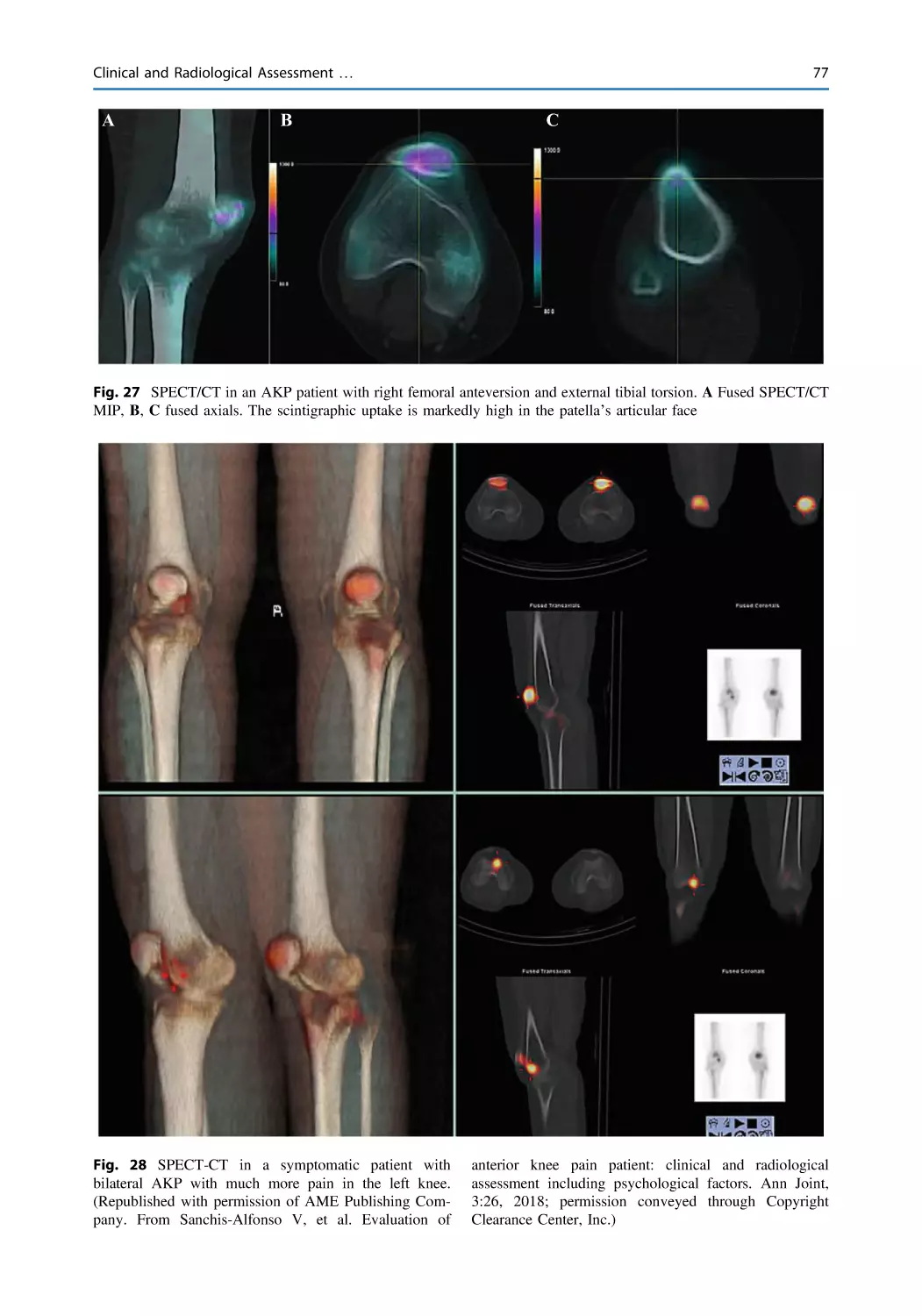
whether the whole or part of the material is concerned, specifically the rights of reprinting, reuse
of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way,
and transmission or information storage and retrieval, electronic adaptation, computer software,
or by similar or dissimilar methodology now known or hereafter developed.
The use of general descriptive names, registered names, trademarks, service marks, etc. in this
publication does not imply, even in the absence of a specific statement, that such names are
exempt from the relevant protective laws and regulations and therefore free for general use.
The publisher, the authors, and the editors are safe to assume that the advice and information in
this book are believed to be true and accurate at the date of publication. Neither the publisher nor
the authors or the editors give a warranty, expressed or implied, with respect to the material
contained herein or for any errors or omissions that may have been made. The publisher remains
neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This Springer imprint is published by the registered company Springer Nature Switzerland AG
The registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland
To my mother, my maternal aunt and my little sister
with all my love
In memoriam (†)
It is very difficult to accept that my little sister is no longer by
my side and that I will never see her again, at least in this life.
My mother used to say that one only dies when we no longer
think of them. If that is true, I can say that my sister is more
alive than ever for me. I think about her all the hours of the day.
I have very vivid and intense memories, and anecdotes of our
times together during the 11 years that her disease lasted. Some
memories are painful, but others make me smile without realizing it. She was a great sister, an amazing person, brave and
determined. She was even generous when dying as she gave us
time to prepare ourselves and say goodbye. The time that she
gave us has made her loss more bearable. I cannot even imagine
how I would be right now if she had died suddenly being
healthy. Mari Carmen, I carry you deeply within me and time
will never erase you from my memory. You will be forever in
my heart; having you close has been the greatest gift I have ever
been bestowed.
Foreword to the Third Edition
It has been a great pleasure to witness the development of this book over
these past few years. This book is much improved over previous editions as
Vicente has incorporated many new ideas and concepts. Moreover, as in
previous editions, he has been able to gather a group of extremely talented
experts to help him write this book. This edition will establish him as the
unchallenged leader in understanding the workings of the Patellofemoral
Joint, why it fails, how it fails, and what we now think are the best
approaches to treatment.
I call him a leader. But what constitutes a leader? For Warren Bennis, an
American academic who focused his entire life on the study of leadership, it
is clear. Returning from World War II to enter university eventually with a
Ph.D. from the Massachusetts Institute of Technology, he studied leadership
in all its facets. He wrote 30 books and left behind a legacy of an almost
17-meter-long shelf of published and working papers in the archives of the
University of Southern California. Once when asked in an interview to say
what it takes to be a great leader, he replied “That’s easy! A great leader has a
vision for accomplishment and a particular passion for a profession and for
persisting in pursuit of his vision in spite of failures. Integrity is imperative
and a leader never lies…about anything. Equally necessary he is curious and
daring. A true leader wonders about everything, wants to learn as much as he
can, experiments and takes risks” (The New York Times, Warren G. Bennis
Obituary, August 1, 2014). Leaders possessing these attributes are indeed
uncommon. Communicating with Vicente, it is clear he possesses vision,
passion, integrity, curiosity, and daring. A vision to understand the Patellofemoral Joint and the passion to follow that dream and deliver perfection for
his patients. Integrity and curiosity, he listens intensely to his patients,
examines them carefully. Moreover, he questions his poor results. Although
he may be quiet, he is daring and courageous to enter uncharted areas performing seemingly foolish complex surgeries. However, only after intense
vii
viii
Foreword to the Third Edition
and deep study has he rejected standard approaches and revealed that the
indications are not so foolish as our conventional treatments. With these
attributes, he is indeed a leader, and this brilliant book should lead us all
forward.
Robert A. Teitge, M.D.
Professor Emeritus of Orthopedic Surgery
Wayne State University
Detroit, Michigan, USA
Foreword to the Second Edition
I am particularly pleased to write the introduction to this fine compendium of
ideas, as Dr. Sanchis Alfonso has been a leader in the understanding of
patellofemoral pain origins. This topic has fascinated me my entire career in
orthopedic surgery, and has been a focus of most of my research and
teaching. In 1985, I published our findings of nerve injury in the peripatellar
retinaculum of patients with patellar imbalance and anterior knee pain,
helping to establish the link between pain and patellofemoral malalignment.
Dr. Sanchis Alfonso has not only added substance and scientific evidence to
the link between musculoskeletal stress and neural changes causing pain, he
has now brought together many good thinkers and scientists to present
interesting and sometimes divergent points of view in this current volume.
The great philosopher Hegel stated “it is through the tension of opposites that
we come to a higher truth”.
Through computer simulated knee mechanical function noted in this book,
Elias and Cosgarea demonstrate how articular loads can be tracked accurately
and that even small aberrations of mechanical function can cause considerable alterations of stress transmitted through articular surfaces. Similarly,
retinacular restraints around the patellofemoral joint will experience profound
changes of loading when alignment is off, overuse is extreme, surgical
balancing is not precise, and at extremes of laxity or tightness. Such is the
nature of patellar and peripatellar stress and the relative anoxia caused by
abnormal loading of peripatellar structure leading to cytokine elaboration and
resulting pain. Thank you Dr. Sanchis Alfonso.
I believe this book is a wonderful compendium of current patellofemoral
thought, not designed as a cookbook with easy answers, because there are
many complex problems around the anterior knee and few easy answers.
Rather, Dr. Sanchis-Alfonso’s text contains many independent thinkers and
scientists with a variety of approaches and concepts, some validated, some
not, but all important in our search of the patellofemoral “holy grail”.
I encourage the reader to think, along with the authors of this textbook,
synthesizing ideas and considering carefully how each concept presented
here applies to the individual patient, always emphasizing non-operative and
simple measures whenever possible, but recognizing the importance of
appropriate surgery when necessary for the relief of pain and suffering in the
challenging patients with recalcitrant patellofemoral pain and instability.
ix
x
Foreword to the Second Edition
In closing, I want to summarize my 32 years of experience with patellofemoral patients by saying that I believe a critical underlying concept for
treating many patients with patellofemoral dysfunction is to recognize that
the structural imbalance we see in patients with patellofemoral malalignment
is at the root of much patellofemoral pain and instability. Therefore, our
challenge is to restore balance and reduce excessive patellofemoral stress in
these patients, using non-operative measures including rest when possible,
but designing necessary surgery to absolutely minimize both articular and
periarticular damages while restoring patellofemoral balance as precisely as
possible.
John P. Fulkerson, M.D.
Clinical Professor of Orthopaedic Surgery
University of Connecticut School of Medicine
Farmington, Connecticut, USA
Foreword to the First Edition
Anterior knee pain is one of the really big problems in my specialty, sports
orthopedic surgery, but also in all other types of orthopedic surgery. Many
years ago Sakkari Orava in Finland showed that among some 1311 Finnish
runners, anterior knee pain was the second most common complaint. In
young school girls around 15 years of age, anterior knee pain is a common
complaint. In ballet classes of the same age as much as 60–70% of the
students complain of anterior knee pain. It is therefore an excellent idea of
Dr. Sanchis-Alfonso to publish a book about anterior knee pain and patellofemoral instability in the active young.
He has been able to gather a group of extremely talented experts to help
him write this book. I am particularly happy that he has devoted so much
space to the non-operative treatment of anterior knee pain. During my active
years as a knee surgeon, one of my worst problems was young girls referred
to me for surgery of anterior knee pain. Girls that already had had 8–12
surgeries for their knee problem–surgeries that had rendered them more and
more incapacitated after each operation. They now came to me for another
operation. In all these cases, I referred them to our pain clinic for careful
analysis, pain treatment followed by physical therapy. All recovered but had
been the victims of lots of unnecessary knee surgery before they came to me.
I am also happy that Suzanne Werner in her chapter refers to our study on
the personality of these anterior knee pain patients. She found that the
patients differ from a normal control group of the same age. I think this is
very important to keep in mind when you treat young patients with anterior
knee pain.
In my mind physical therapy should always be the first choice of treatment. Not until this treatment has completely failed and a pain clinic recommends surgery, do I think surgery should be considered.
In patellofemoral instability the situation is different. When young patients
suffer from frank dislocations of the patella, surgery should be considered.
From my many years of treating this type of patients, I recommend that the
patients undergo an arthroscopy before any attempts to treat the instability
begins. The reason is that I have seen so many cases with normal X-rays that
have 10–15 loose bodies in their knees. If these pieces consist of just cartilage, they cannot be seen on X-ray. When a dislocated patella jumps back, it
often hits the lateral femoral condyle with considerable force. Small cartilage
pieces are blasted away as well from femur as from the patella. If they are
overlooked they will eventually lead to blockings of the knee in the future.
xi
xii
Foreword to the First Edition
The role of the medial patellofemoral ligament can also not be overstressed. When I was taught to operate on these cases, this ligament was not
even known.
I also feel that when patellar instability is going to be operated on, it is
extremely important that the surgeon carefully controls in what direction the
instability takes place. All instability is not in lateral direction. Some patellae
have medial instability. If someone performs a routine lateral release in a case
of medial instability, he will end up having to repair the lateral retinaculum in
order to treat the medial dislocation that eventually occurs. Hughston and
also Teitge have warned against this in the past.
It is a pleasure for me to recommend this excellent textbook by
Dr. Vicente Sanchis-Alfonso.
Ejnar Eriksson, M.D., Ph.D.
Professor Emeritus of Sports Medicine
Karolinska Institute
Stockholm, Sweden
Preface
Take good care of your patients and they will take
good care of you
—Freddie Fu
Medicine is meant to help people! It is OK to make
some money but it´s not the key
—Peter Lauterbur
Santiago Ramón y Cajal, Spanish Nobel Laureate in Medicine, in his book,
“The Tonics of the Will”, he said: “What a great tonic it would be for the
young researcher that his mentor, instead of astonishing him and discouraging him with the sublimity of great completed projects, would explain the
genesis of each scientific creation along with the mistakes and doubts that
preceded them”. This is why I think it is interesting for you to know how the
book you are holding in your hands came to be. This book is not only the
fruit of my effort and perseverance and, clearly, the generosity of all my
colleagues but also of chance. Many years ago, my good friend Donald
Fithian from San Diego told me that to stand out in something I had to focus
on a topic not well known and that many did not like. In those years,
patellofemoral disorders fulfilled both. Paraphrasing a great American poet
Robert Frost in his poem “The Road Not Taken”, I took the least traveled
road 24 years ago, that is, I focused on the patella. As in this poem, it made
all the difference. Without a doubt, I do not regret having chosen this road.
The patella has led to very satisfactory experiences with my patients and
other colleagues. In 2003, I wrote a book in Spanish with the “Editorial
Médica Panamericana”, one of the most prestigious publishing houses in the
Spanish language. It was entitled “Dolor Anterior de Rodilla e Inestabilidad
Rotuliana en el Paciente Joven” (Anterior Knee Pain and Patellar Instability
in the Young Patient). Frankly, I never thought it would be very successful.
That attitude was not due to its quality, of which I was convinced, but due to
its subject matter. This book was the germ for the one I am now referring to.
In 2004, I had the fortune of meeting Prof. Ejnar Eriksson, from the
Karolinska Institute of Stockholm, at an international meeting in Sardinia,
Italy. My good friend, Roland Biedert from Switzerland, had invited me to
participate in a panel session about patellofemoral pain. During the coffee
break, Prof. Eriksson approached me and encouraged me to translate this
book into English. I was quite delighted by his suggestion. So, as soon as I
returned to Spain, I prepared a project and presented it to Springer. I was
lucky that this renowned publishing house accepted the challenge of
xiii
xiv
publishing, in English, an extension of the Spanish edition. It was quite
successful both with regard to sales and the book critics. They even said it
was a model for what a book for specialists should be. That first English
edition was published in December 2005. However, getting there is only half
the battle, as it must be kept up to date. Therefore, in 2011, a second edition
of the book was published in English. I donated my author’s royalties to the
research foundation of the Hospital Clínico Universitario in Valencia, Spain.
It was specifically given for the line of research in breast cancer, which made
my sister very happy. Sadly, she recently died from breast cancer. For this
reason, I proposed doing this third and last edition to Springer, as a tribute to
my sister. This book is, in fact, the third edition in English. Notwithstanding,
we are really before a fourth edition of this book since the first edition was
the one that was published in Spanish.
This monograph reflects my deep interest in the pathology of the knee,
particularly that of the extensor mechanism, and emphasizes the great
importance I give to the concept of subspecialization. This is the only way to
confront the deterioration and the mediocrity of our specialty, Orthopedic
Surgery, and to give our patients better care. In line with the concept of
subspecialization, this book clearly required the participation of various
authors. They are of different nationalities as well as from different schools of
thought. Moreover, the participation of diverse specialists, from a multidisciplinary perspective, affords us a wider vision of this pathology.
With this book, we draw upon the most common pathology of the knee
even though it is the most neglected, the least known, the most problematic
and controversial topic (The Black Hole of Orthopedics). Our knowledge of
its etiopathogenesis is limited. Therefore, its treatment is one of the most
complex among the different pathologies of the knee. On the other hand, we
also face the problem of frequent and serious diagnostic errors that may lead
to unnecessary operations.
This book is organized into four parts. Unlike other publications, it gives
great importance to etiopathogenesis. Albeit in an eminently clinical and
practical manner, the latest theories are presented regarding the pathogenesis
of anterior knee pain and patellar instability (Part I “Etiopathogenic Bases,
Prevention and Therapeutic Implications”). In agreement with John Hunter, I
think that to know the effects of an illness is to know very little. To know the
cause of the effects is what is important. In Part II (“Surgical
techniques-Why, When and How I Do It”), the surgical techniques that are in
use today for the patellofemoral joint are described in detail. They are
described by the surgeons who have designed the technique and who are
recognized by their colleagues as “masters” in their specialty. The third part
of this monograph is given over to the discussion of complex clinical cases.
I believe we learn far more from our own mistakes (“To Err is Human”,
Marcus Tullius Cicero), and those of other specialists than from our own
success (“Learn from the mistakes of others-you can never live long enough
to make them all yourself”, John Luther). The diagnoses reached and how the
cases were resolved are explained in detail (“Good results come from
experience, experience from bad results”, Prof. Erwin Morscher). Finally, in
Preface
Preface
xv
Part IV, new frontiers in anterior knee pain, patellar instability, and patellofemoral osteoarthritis evaluation and treatment are analyzed.
The first objective I have laid out in this book is to highlight the soaring
incidence of this pathology and its impact on young people, athletes,
workers, and the economy. The second goal is to improve prevention and
diagnosis to reduce the economic and social costs of this condition. The final
objective is to improve health care for these patients.
“Anterior Knee Pain and Patellar Instability” is addressed to orthopedic
surgeons (both general and those specialized in knee surgery), specialists in
sports medicine, rehabilitation specialist MDs, and physiotherapists.
Thus, we feel that this monograph will fill an important gap in the literature about the pathology of the extensor mechanism of the knee with this
approach. However, we do not intend to substitute any books on patellofemoral pathology but rather to complement them (“All in all, you’re just
another brick in the wall”, Pink Floyd, The Wall). Although the information
contained herein will evidently require future revision, it serves as an
authoritative reference on one of the most problematic entities in the
pathology of the knee at this time. We hope this book will be a reference in
the future from our youngest to our oldest colleagues. We trust that the reader
will find this book useful and, consequently, be indirectly valuable for
patients.
Valencia, Spain
April 2022
Vicente Sanchis-Alfonso, M.D., Ph.D.
Acknowledgments
At times our own light goes out and is rekindled by a
spark from another person. Each of us has cause to
think with deep gratitude of those who have lighted
the flame within us
—Albert Schweitzer (Nobel Peace Prize)
I wish to express my sincere gratitude to my good friends and colleagues Don
Fithian, John Fulkerson, and Bob Teitge. My journey in knee surgery began
in 1992 in San Diego, California, USA. When I got to San Diego, pure
serendipity put Donald Fithian in my path. Quoting William Shakespeare,
destiny is the one that shuffles the cards, but we are the ones who play them.
But someone has to give us a chance to play. Donald gave me this opportunity. He shuffled the cards. He introduced me in the International Patellofemoral Study Group. I was his guest at the meeting in Lyon, France, in
1998. I will be forever grateful for his invaluable help and friendship. The
next year, in 1999, I was selected to become a member of this organization
and where else but in St. Helena, in Napa County. California again.
Belonging to this group has motivated me to study every day and to stay
updated, in order to keep up with the rest of my colleagues. I have had a deep
respect and admiration for John Fulkerson ever since I read the second
edition of his book ``Disorders of the Patellofemoral Joint'' when I was a
resident in Orthopedic Surgery. For me this book was a real page-turner, a
kind of Harry Potter for today´s teenagers. Reading this book was a breakthrough. John Fulkerson made the patellofemoral joint my professional
passion. Despite being the most important and recognized surgeon in this
field, he turned out to be the most modest and closest to me. He gave me a lot
of support and guidance. Bob Teitge got me into thinking outside of the box.
He gave me the gift of his friendship and all the necessary tools for my
complete professional development. With his incredible generosity, he
shared all his knowledge without expecting anything in return. He also
showed me techniques I had not heard of before that made it possible for me
to help many patients who were considered lost-causes by others. Bob, thank
you for always being there, for helping me improve day by day and for
teaching me to row against the tide.
I am extremely lucky to be surrounded by incredible people who support
me unconditionally. They have provided me with the means and thus the
opportunities to fully develop in my professional life. I would like to
acknowledge Julio Domenech-Fernandez, Erik Montesinos-Berry, Cristina
Ramírez-Fuentes, and Maria Jose Sanguesa-Nebot for their friendship and
invaluable help. Thank you, Julio, you are the best boss that one can have.
Thank you for your understanding. You are truly a motivating and inspiring
xvii
xviii
person. Thank you, Maria Jose, for being the way you are, marvelous, keep it
up. I also want to commend my colleague at the Knee Unit of my hospital,
Alejandro Roselló-Añón. Undoubtedly, he has a bright future ahead of him.
All of you are, in part, responsible for this book.
My gratitude also goes out to my friends Jack Andrish, Roland Biedert,
Antonio Darder-Prats, David Dejour, Scott F. Dye, João Espregueira-Mendes,
Jack Farr, Christian Fink, Ronald Grelsamer, Laura López-Company, Luis
Martí-Bonmatí, Al Merchant, Joan Carles Monllau, James Selfe and to all the
members of the International Patellofemoral Study Group for their constant
encouragement and inspiration.
Furthermore, I have had the privilege and honor to count on the participation of outstanding specialists who have lent prestige to this monograph.
I thank all of them for their time, effort, dedication, kindness, as well as for
the excellent quality of their contributing chapters. They all have demonstrated generosity in sharing their great clinical experience in a clear and
concise way. I am in debt to you all. Personally, and on behalf of those
patients who will undoubtedly benefit from this work, thank you.
My sincere gratitude to Eric L. Goode and Justyna Mazurek for their
inestimable collaboration.
Last but not least, I am extremely grateful to both Springer London and to
the production team for the confidence shown in this project and for completing this project with excellence from the time the cover is opened until
the final chapter is presented.
Spring 1993, photograph at the Albufera Natural Park (Valencia, Spain). Donald Fithian (right),
his wife M.E. (left), and the editor of this book, Vicente Sanchis-Alfonso (in the middle)
Acknowledgments
Acknowledgments
xix
Mount Sinai Medical Center, New York City, NY, USA, 2009. Vicente Sanchis-Alfonso
(right), Ronald Grelsamer (left), and John Fulkerson (in the middle)
Vicente Sanchis-Alfonso, M.D., Ph.D.
Contents
Etiopathogenic Bases, Prevention and Therapeutic Implications
Patellofemoral Pain: An Overview . . . . . . . . . . . . . . . . . . . . . . . . . .
Vicente Sanchis-Alfonso and Ronald P. Grelsamer
3
Pathophysiology of Anterior Knee Pain . . . . . . . . . . . . . . . . . . . . . .
Vicente Sanchis-Alfonso, Esther Roselló-Sastre, Scott F. Dye,
and Robert A. Teitge
19
Femoral and Tibial Rotational Abnormalities Are the Most
Ignored Factors in the Diagnosis and Treatment of Anterior
Knee Pain Patients. A Critical Analysis Review . . . . . . . . . . . . . . .
Vicente Sanchis-Alfonso and Robert A. Teitge
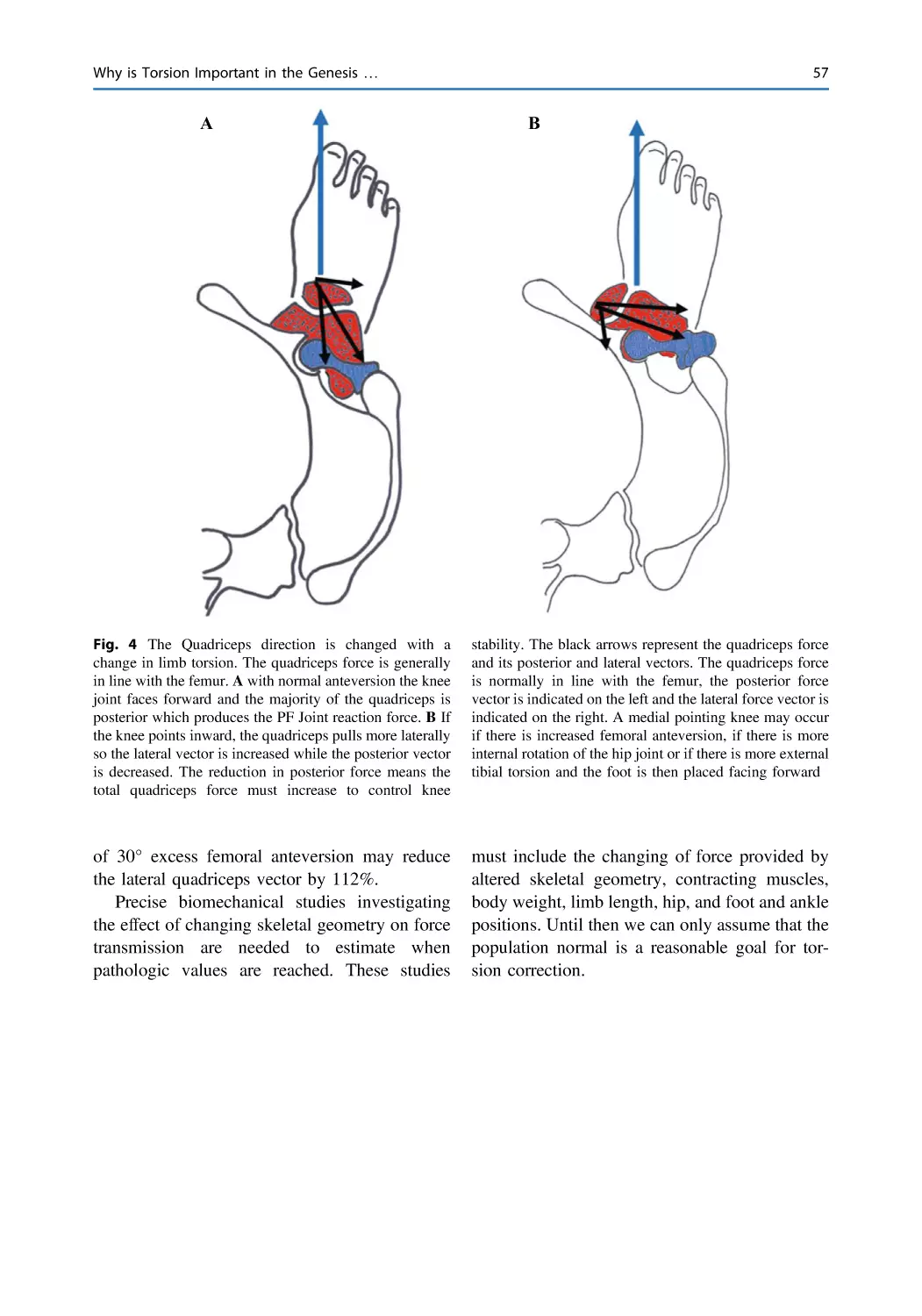
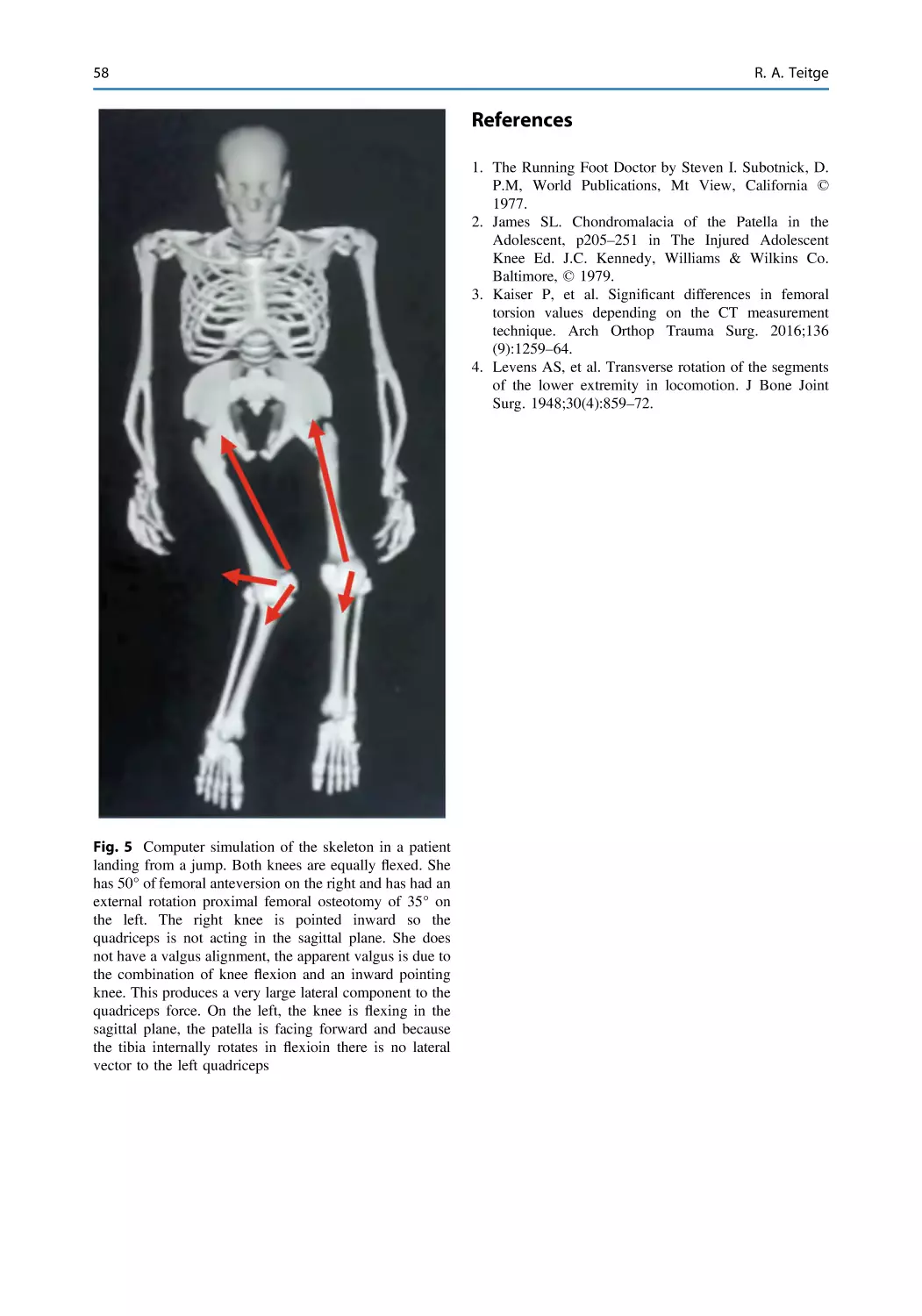
Why is Torsion Important in the Genesis of Anterior Knee
Pain? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Robert A. Teitge
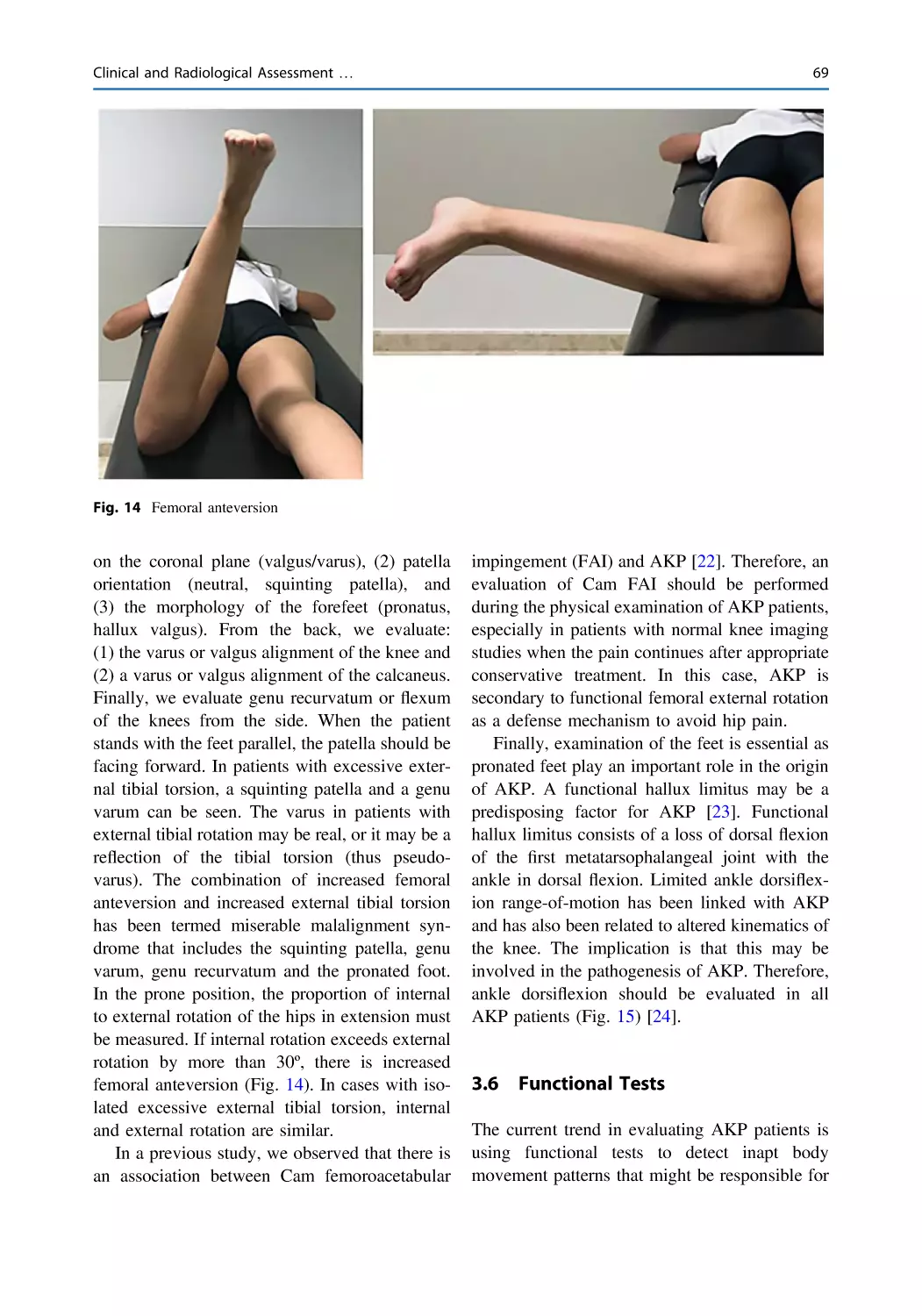
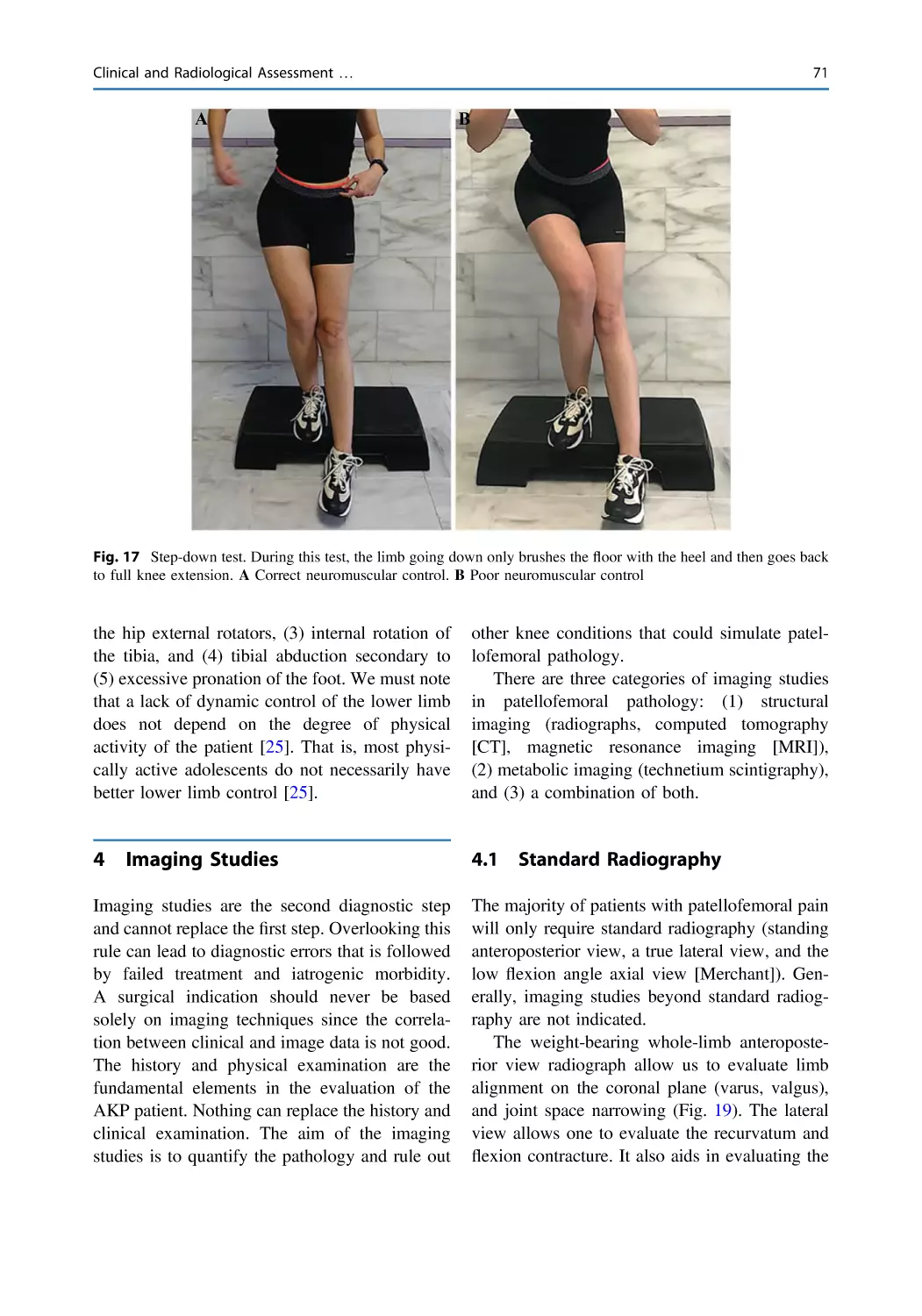
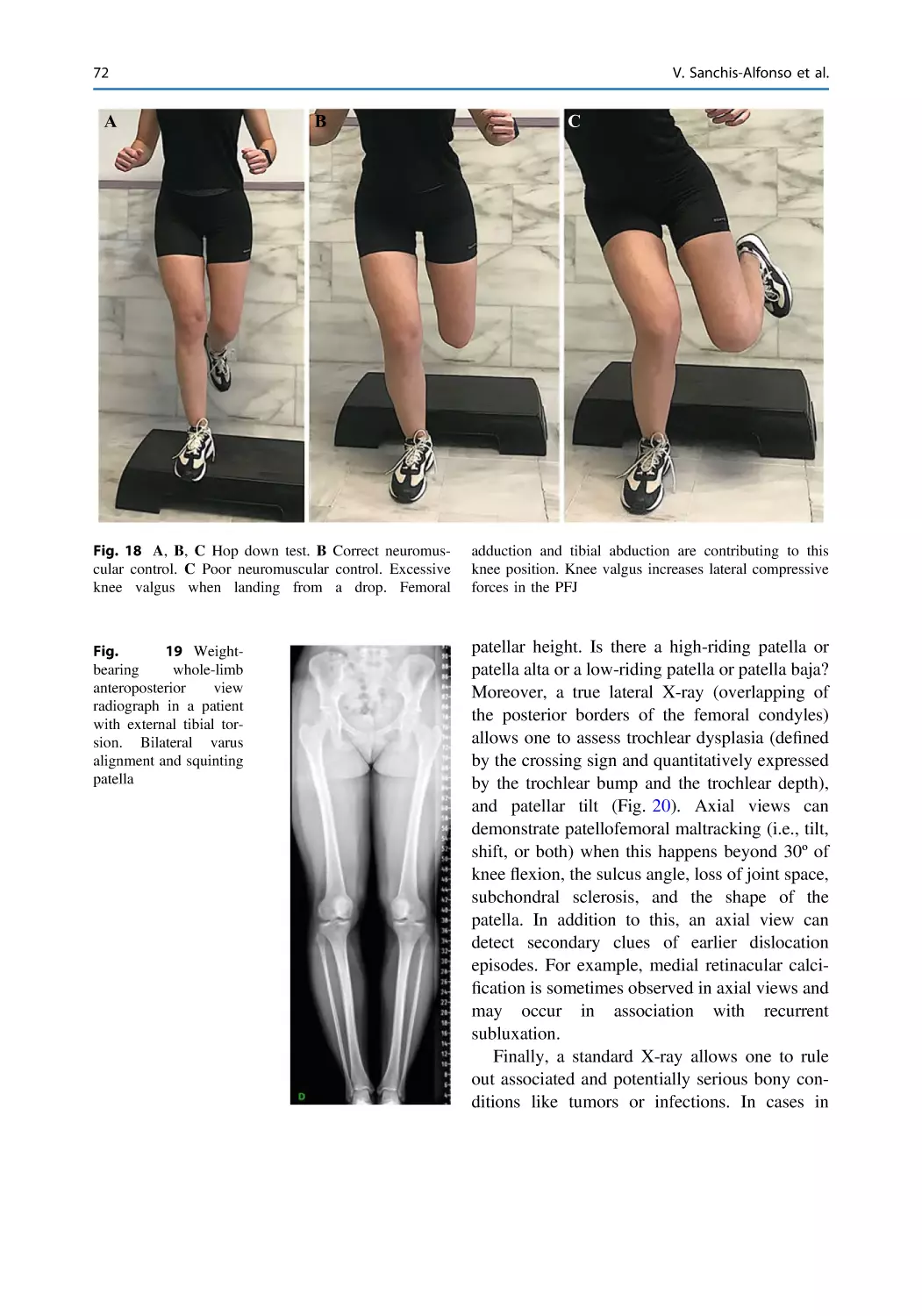
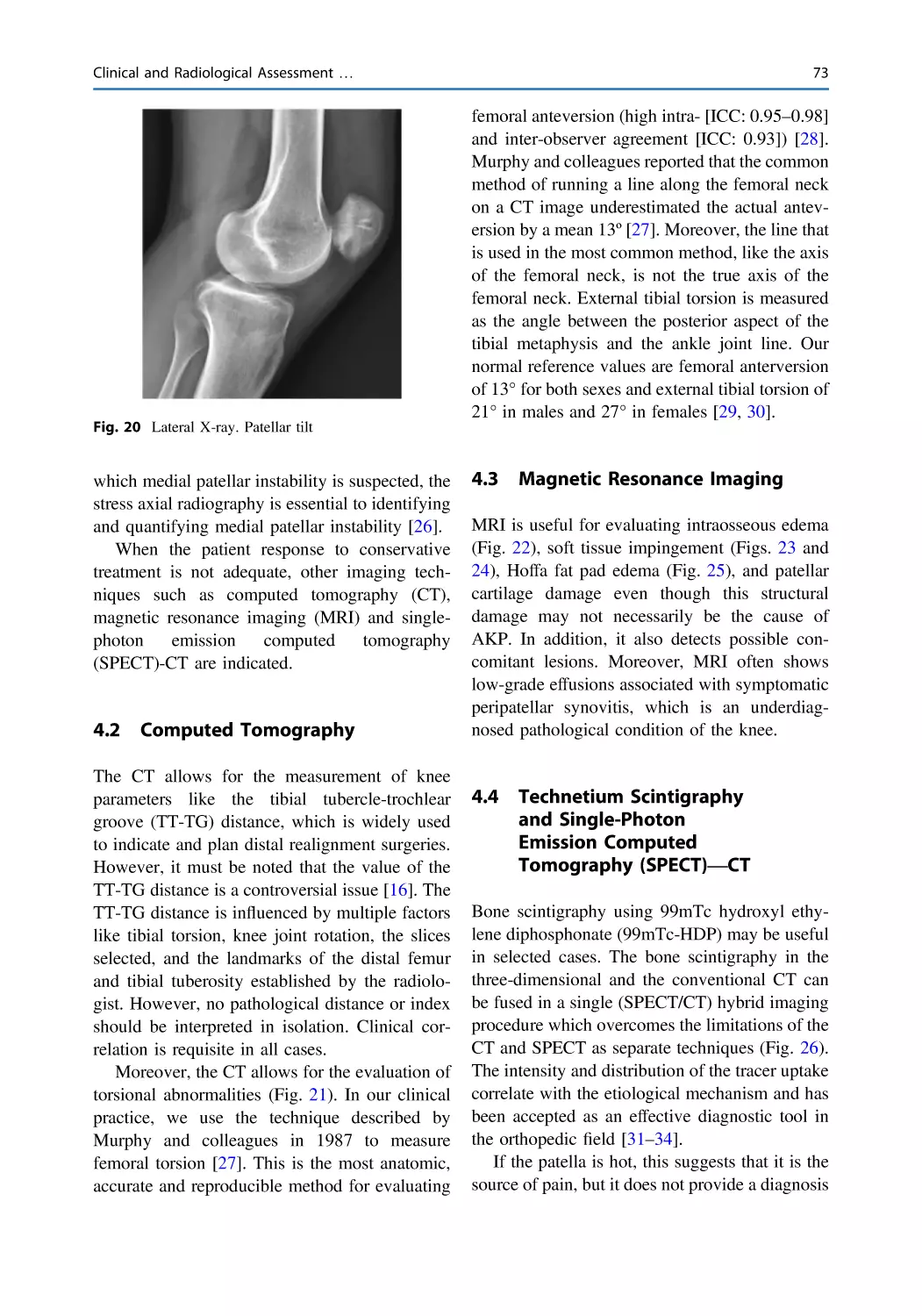
Clinical and Radiological Assessment of the Anterior Knee
Pain Patient . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Vicente Sanchis-Alfonso, Cristina Ramírez-Fuentes,
Laura López-Company, and Pablo Sopena-Novales
41
53
59
Evaluation of Psychological Factors Affecting Anterior Knee
Pain Patients: The Implications for Clinicians Who Treat
These Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Vicente Sanchis-Alfonso, Julio Doménech-Fernández,
Benjamin E. Smith, and James Selfe
81
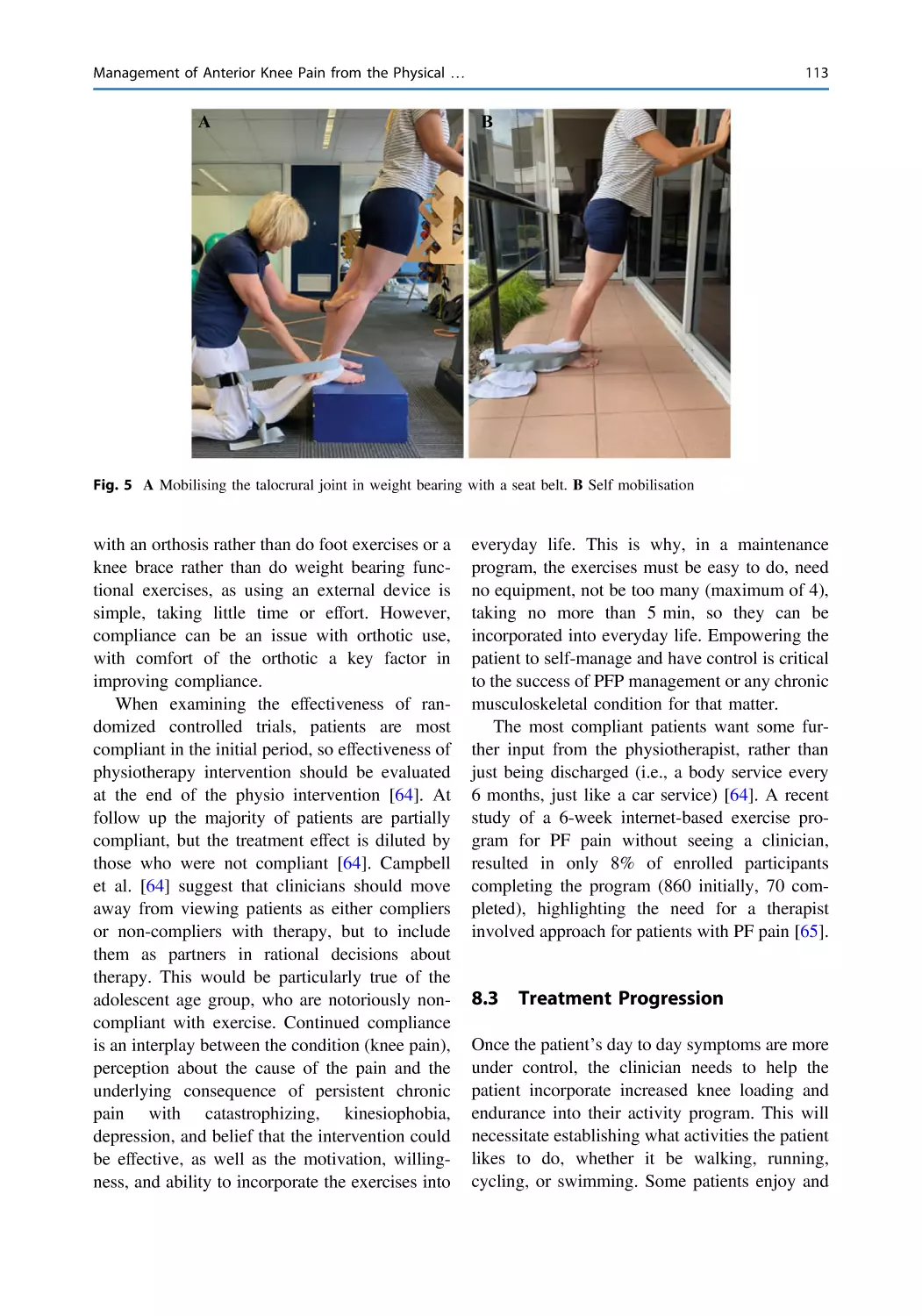
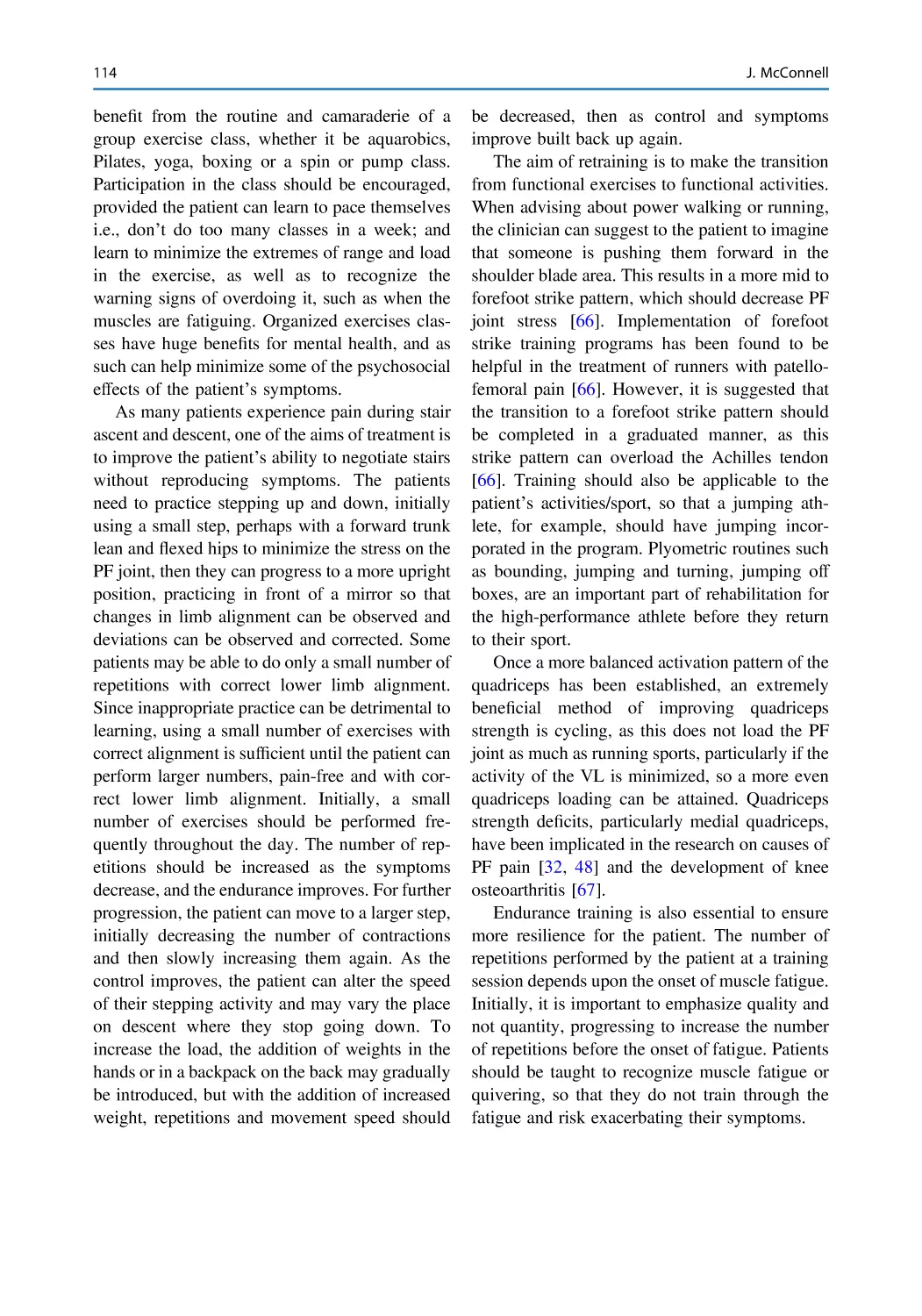
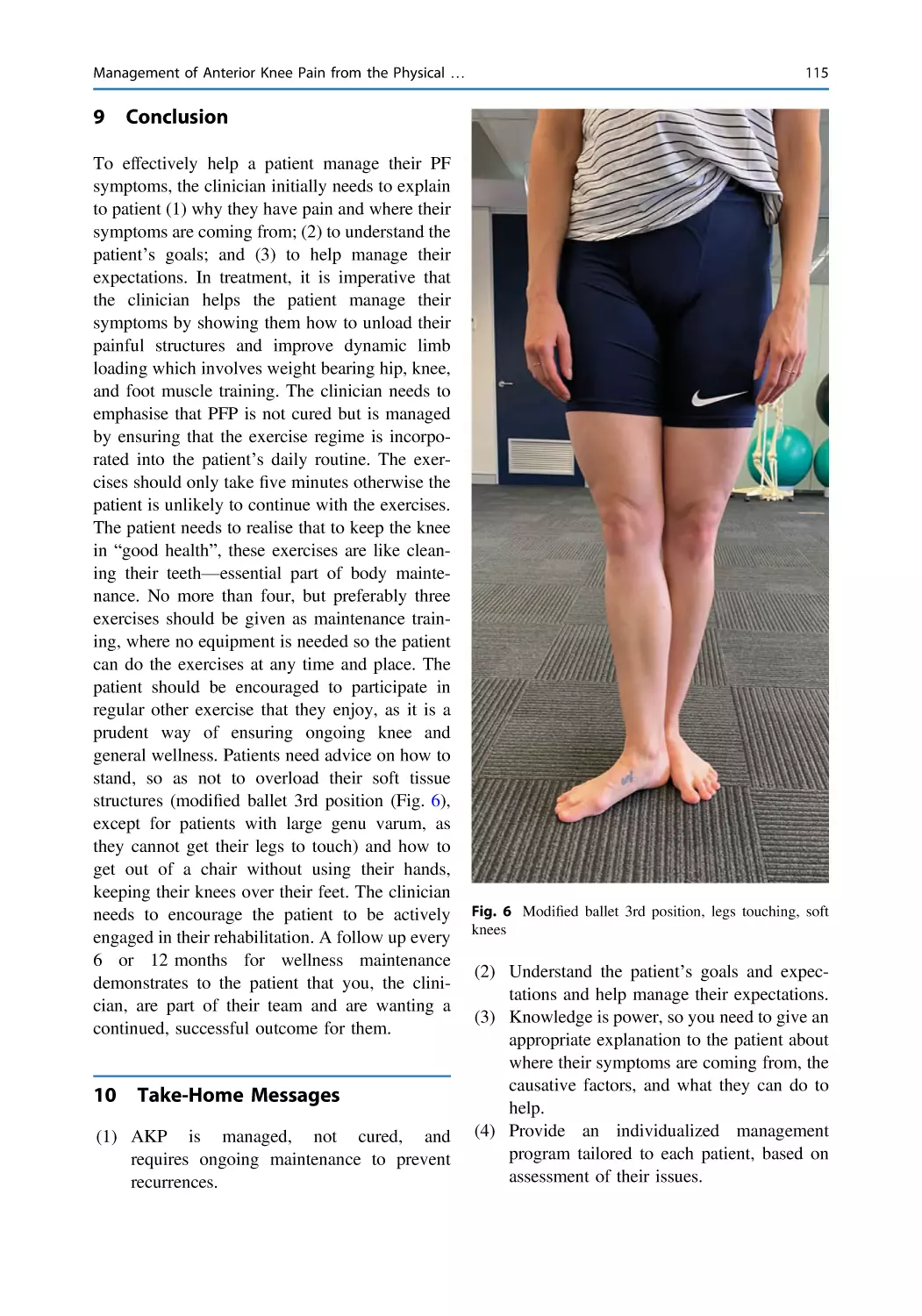
Management of Anterior Knee Pain from the Physical
Therapist’s Perspective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Jenny McConnell
99
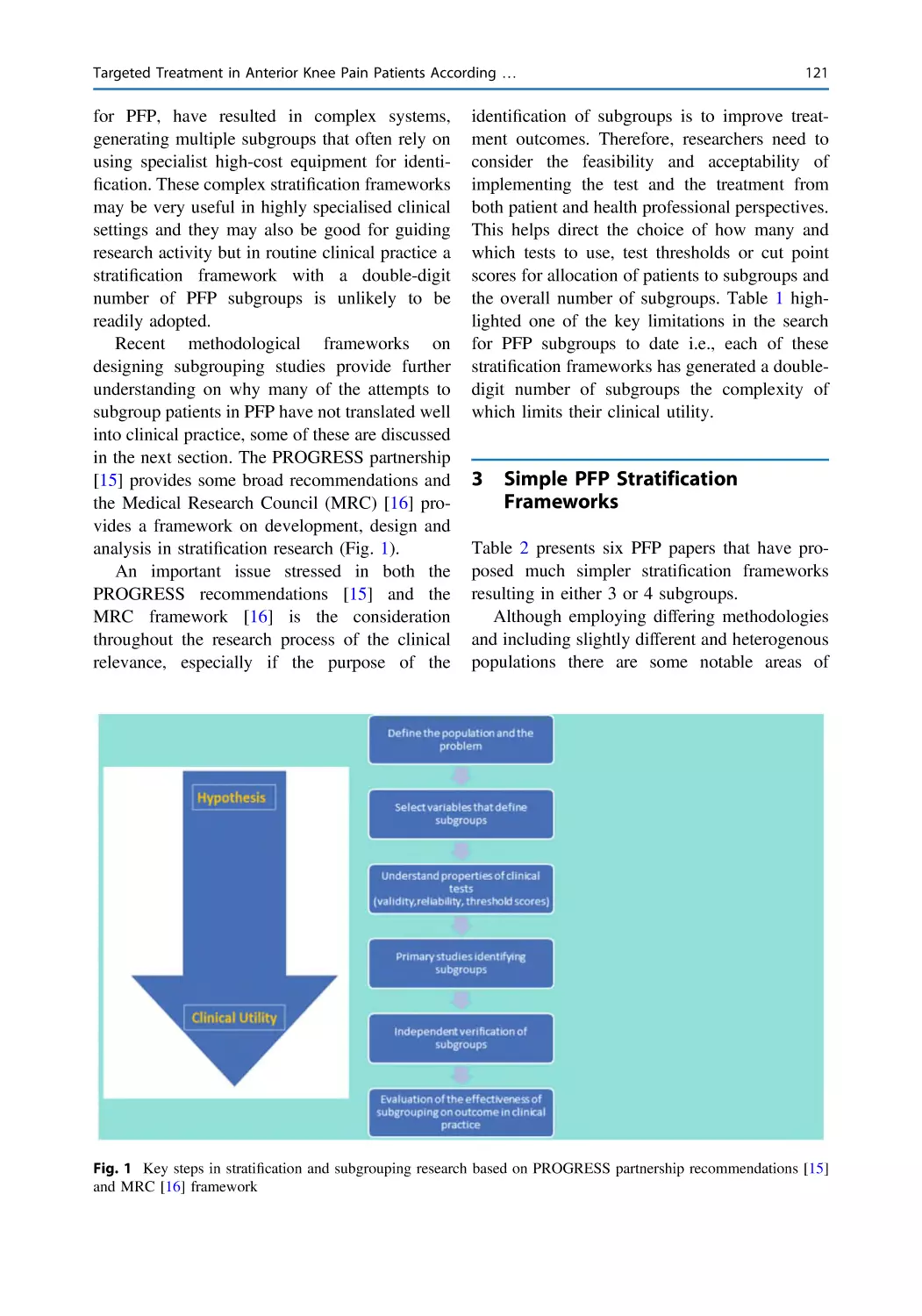
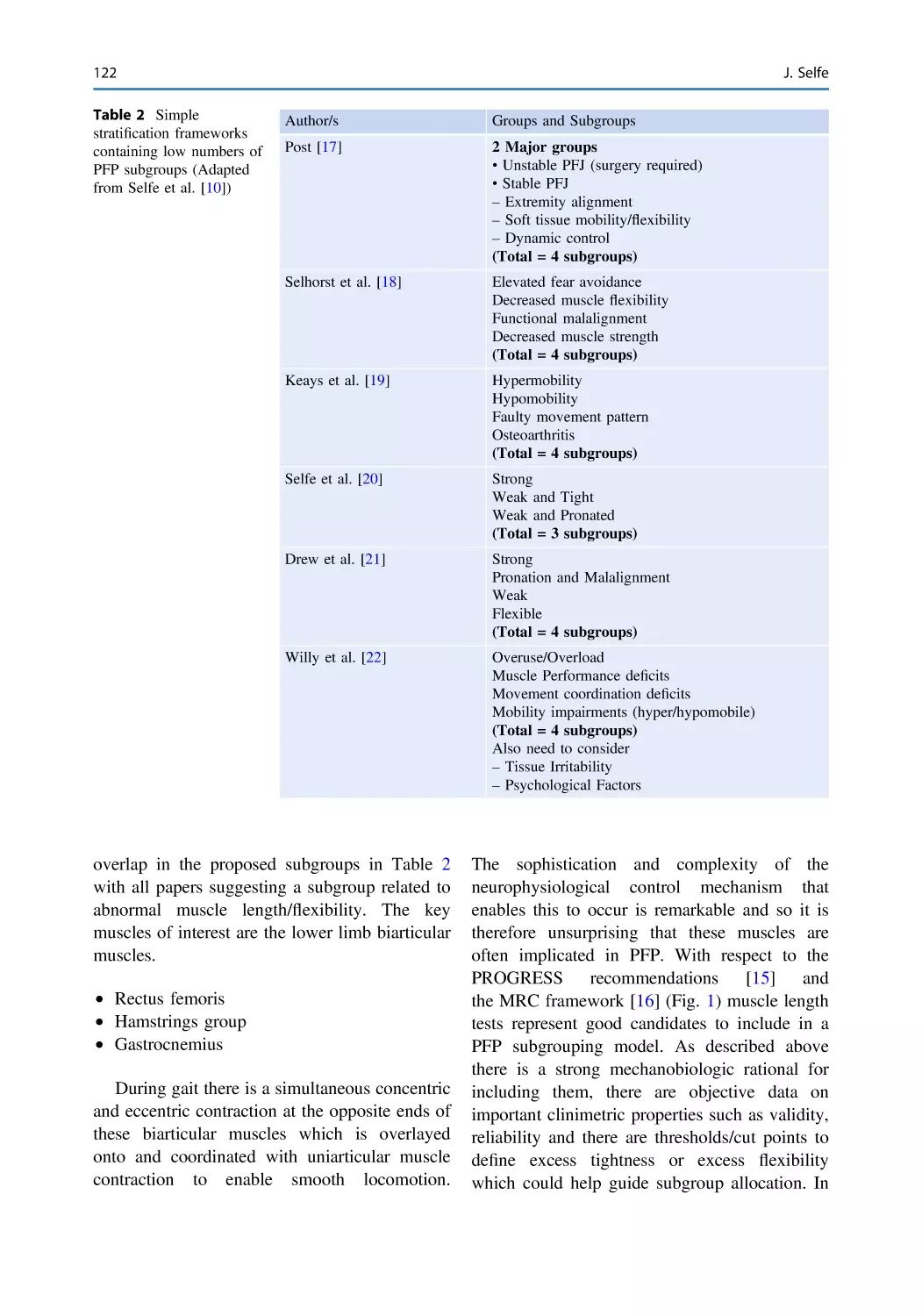
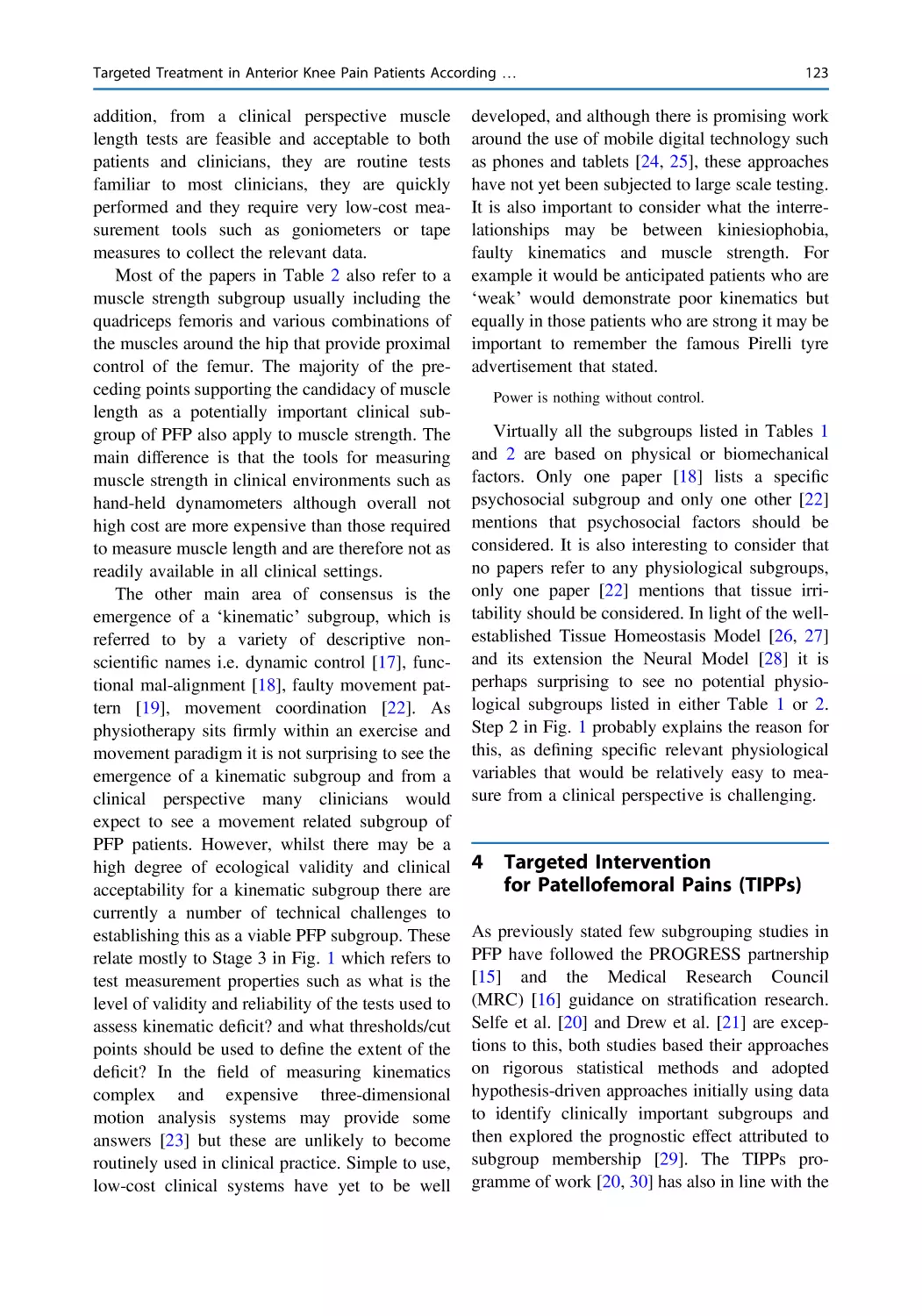
Targeted Treatment in Anterior Knee Pain Patients According
to Subgroups Versus Multimodal Treatment . . . . . . . . . . . . . . . . . 119
James Selfe
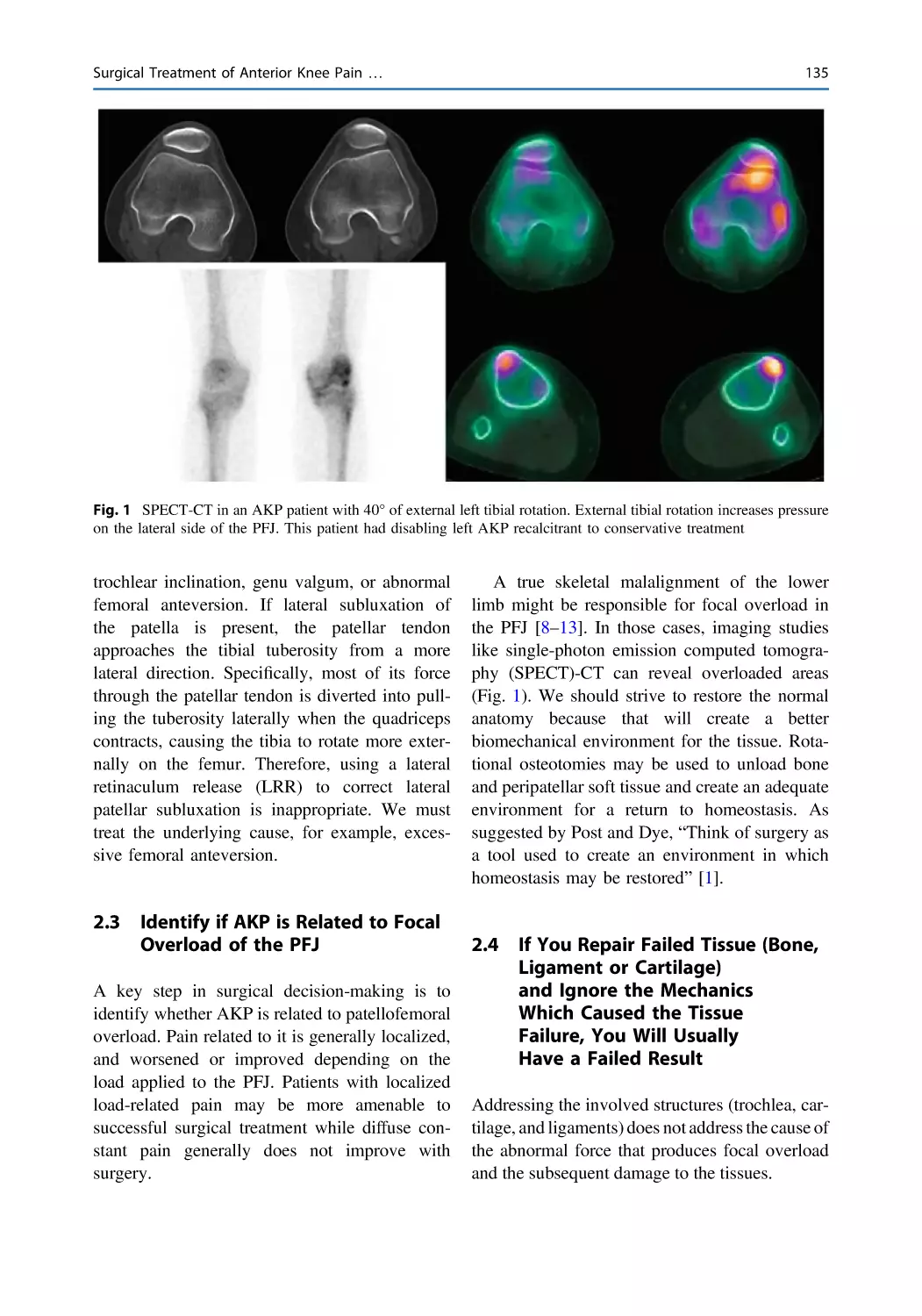
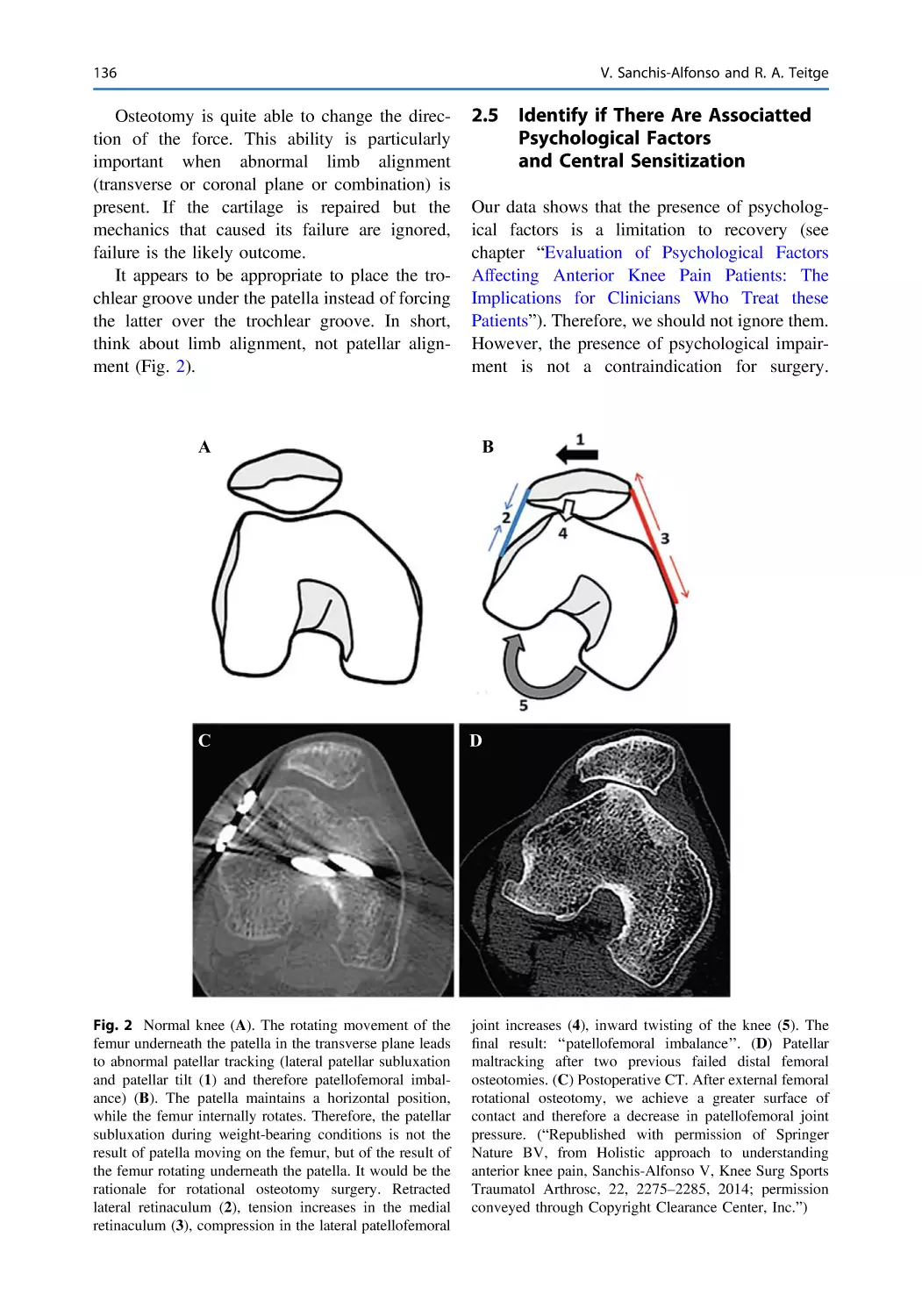
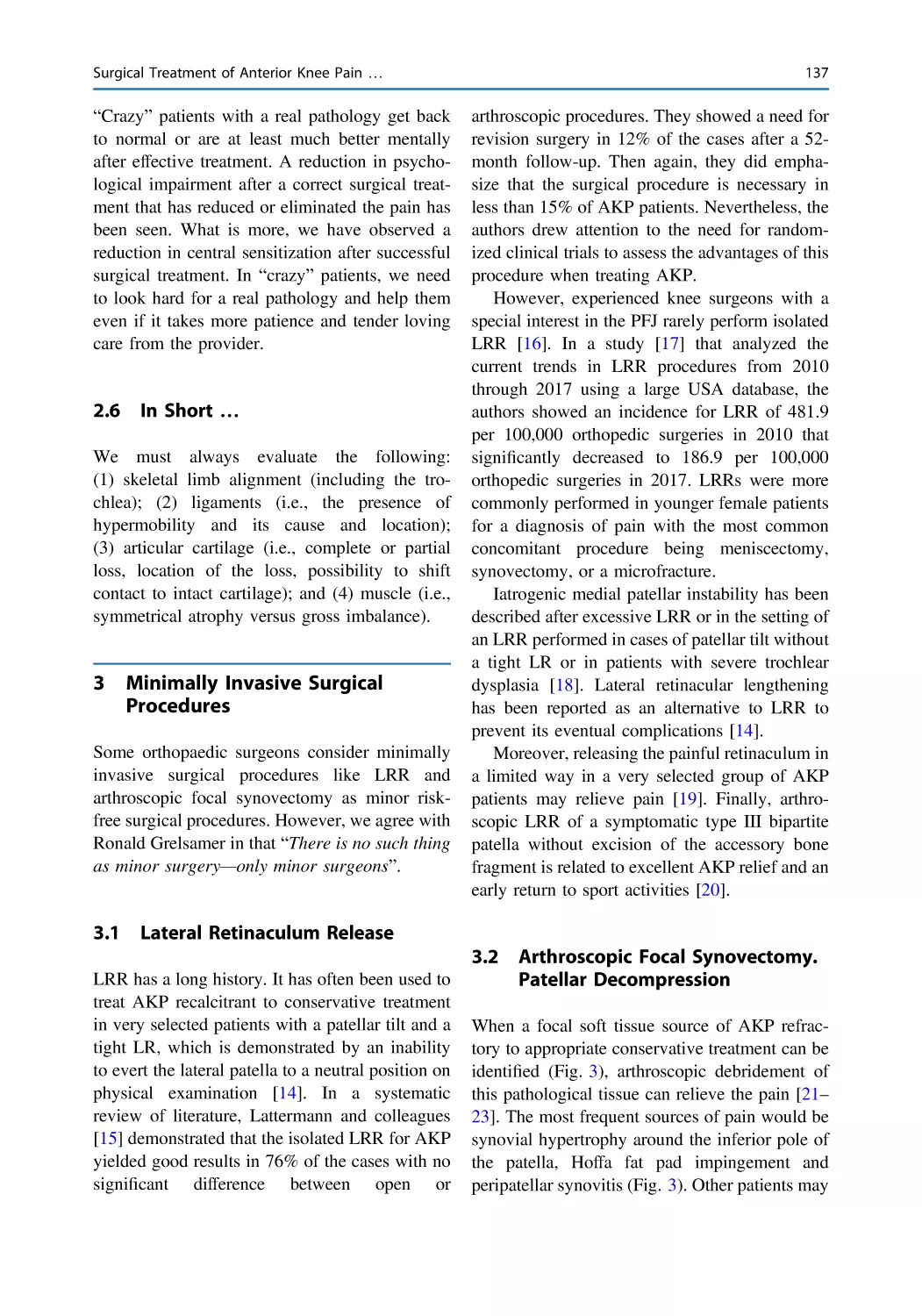
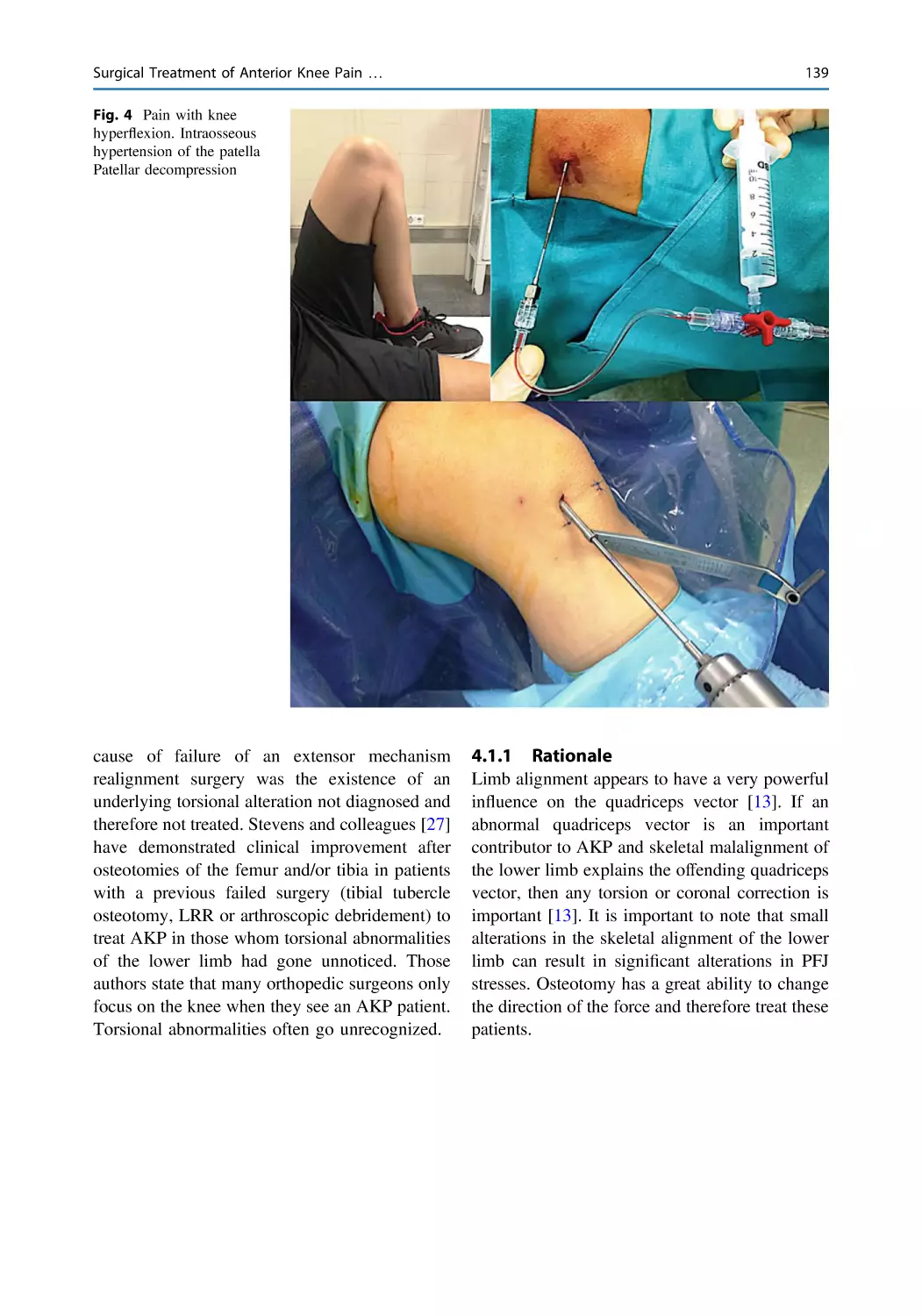
Surgical Treatment of Anterior Knee Pain. When is Surgery
Needed? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
Vicente Sanchis-Alfonso and Robert A. Teitge
xxi
xxii
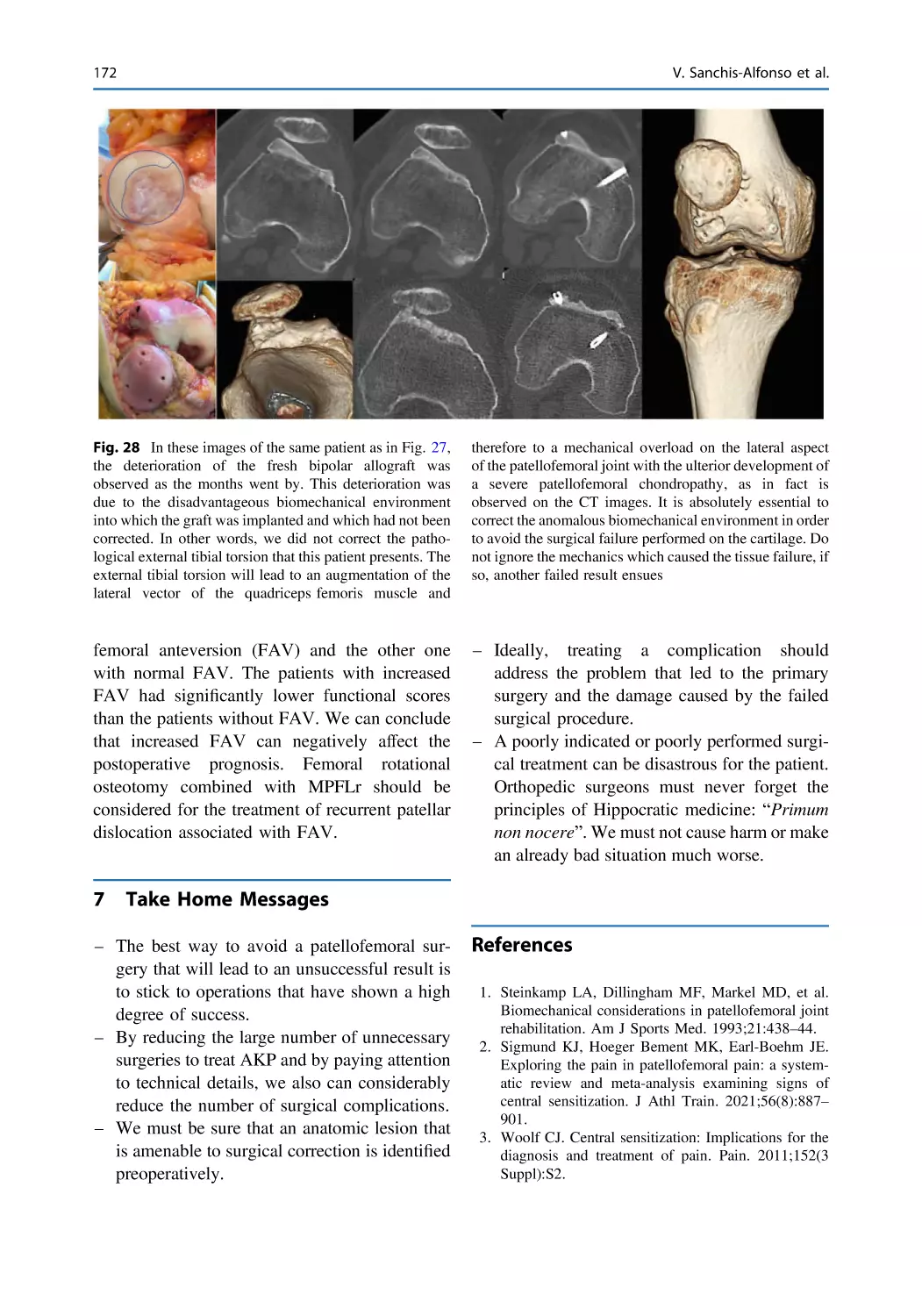
The Failed Patella. What Can We Do? . . . . . . . . . . . . . . . . . . . . . . 151
Vicente Sanchis-Alfonso, Julio Domenech-Fernandez,
and Robert A. Teitge
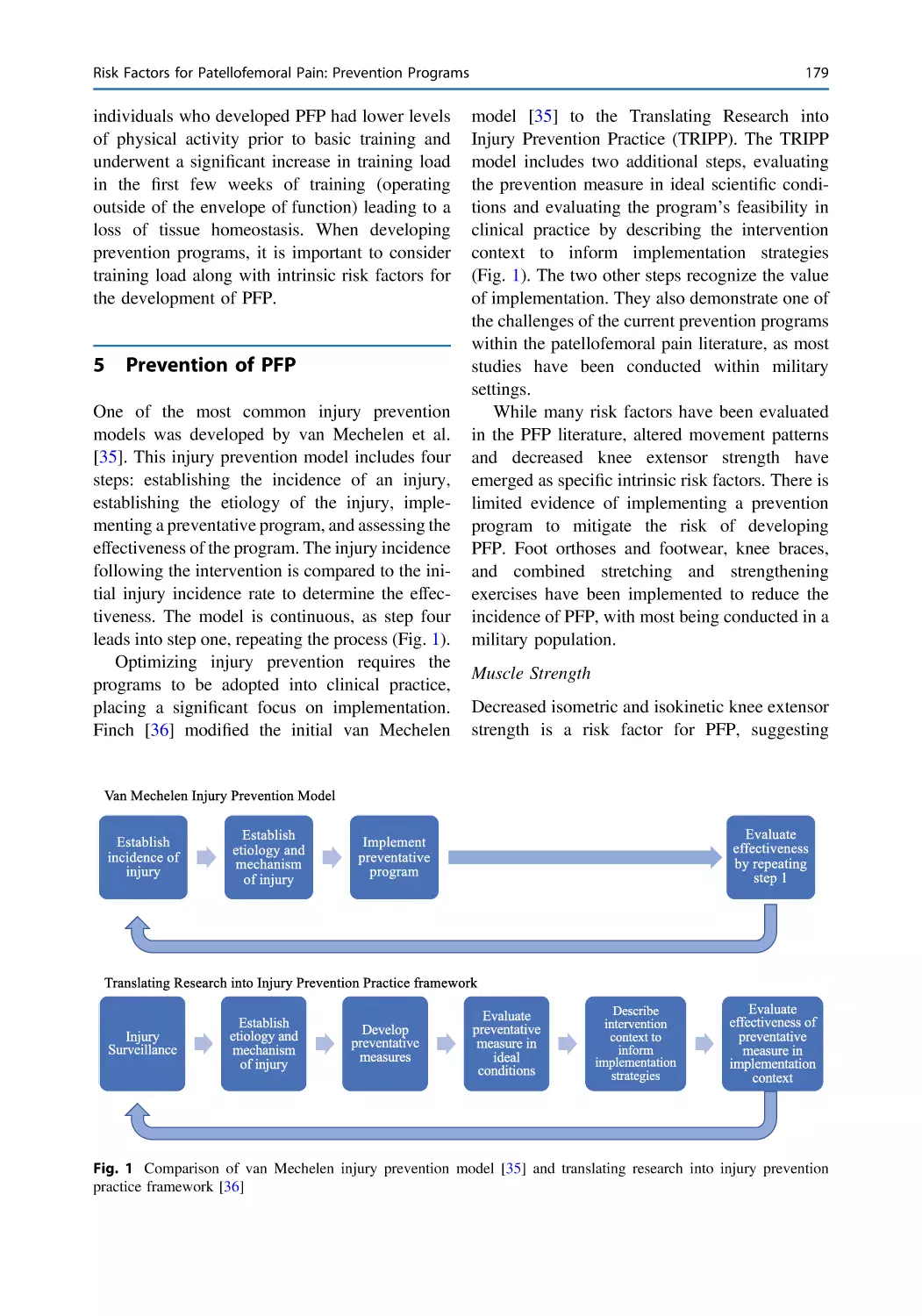
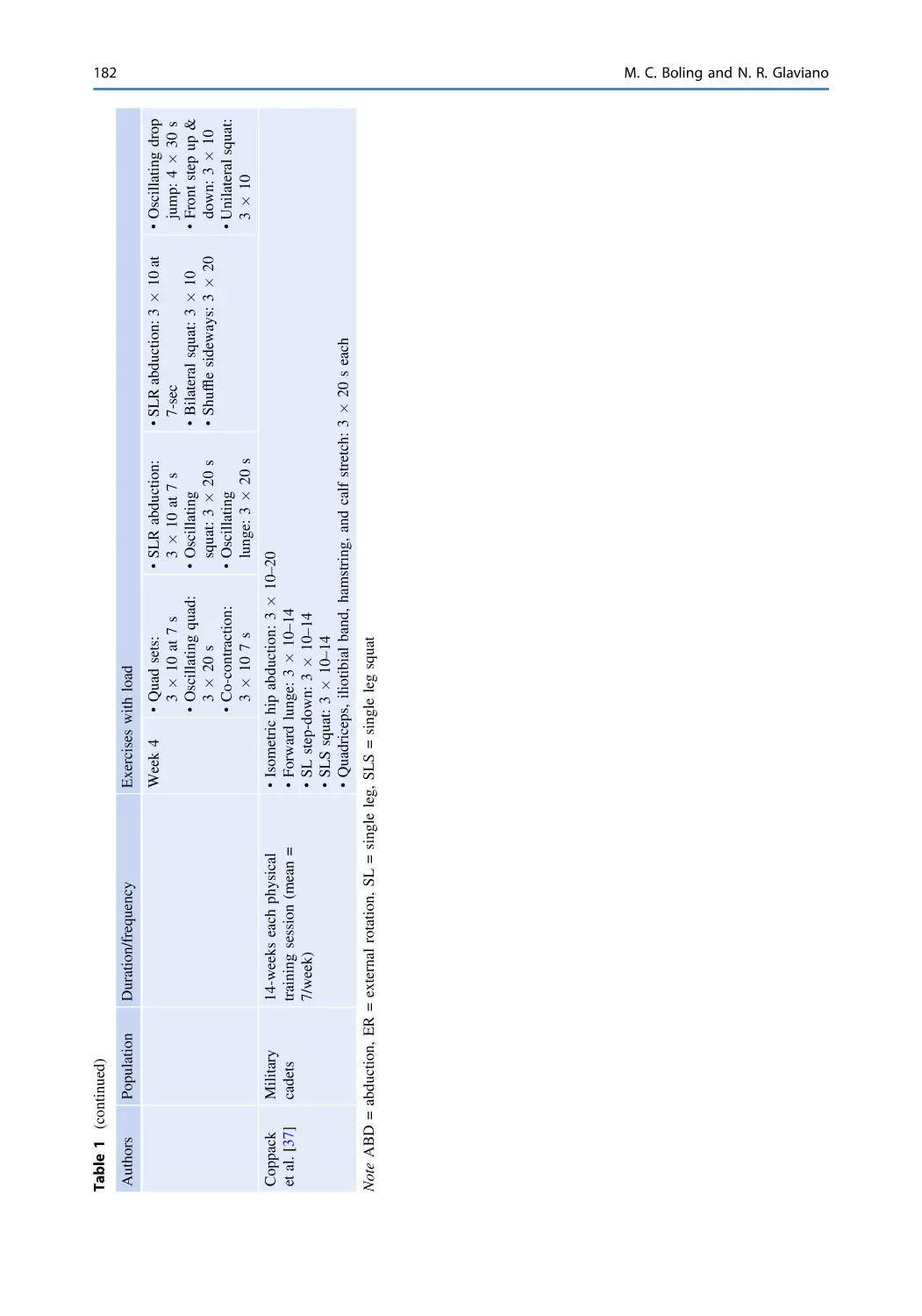
Risk Factors for Patellofemoral Pain: Prevention Programs . . . . . 175
Michelle C. Boling and Neal R. Glaviano
Anterior Knee Pain After Arthroscopic Meniscectomy: Risk
Factors, Prevention and Treatment . . . . . . . . . . . . . . . . . . . . . . . . . 187
Jorge Amestoy, Daniel Pérez-Prieto, and Joan Carles Monllau
Anterior Knee Pain Prevalence After Anterior Cruciate
Ligament Reconstruction: Risk Factors and Prevention. . . . . . . . . 197
Antonio Darder-Sanchez, Antonio Darder-Prats,
and Vicente Sanchis-Alfonso
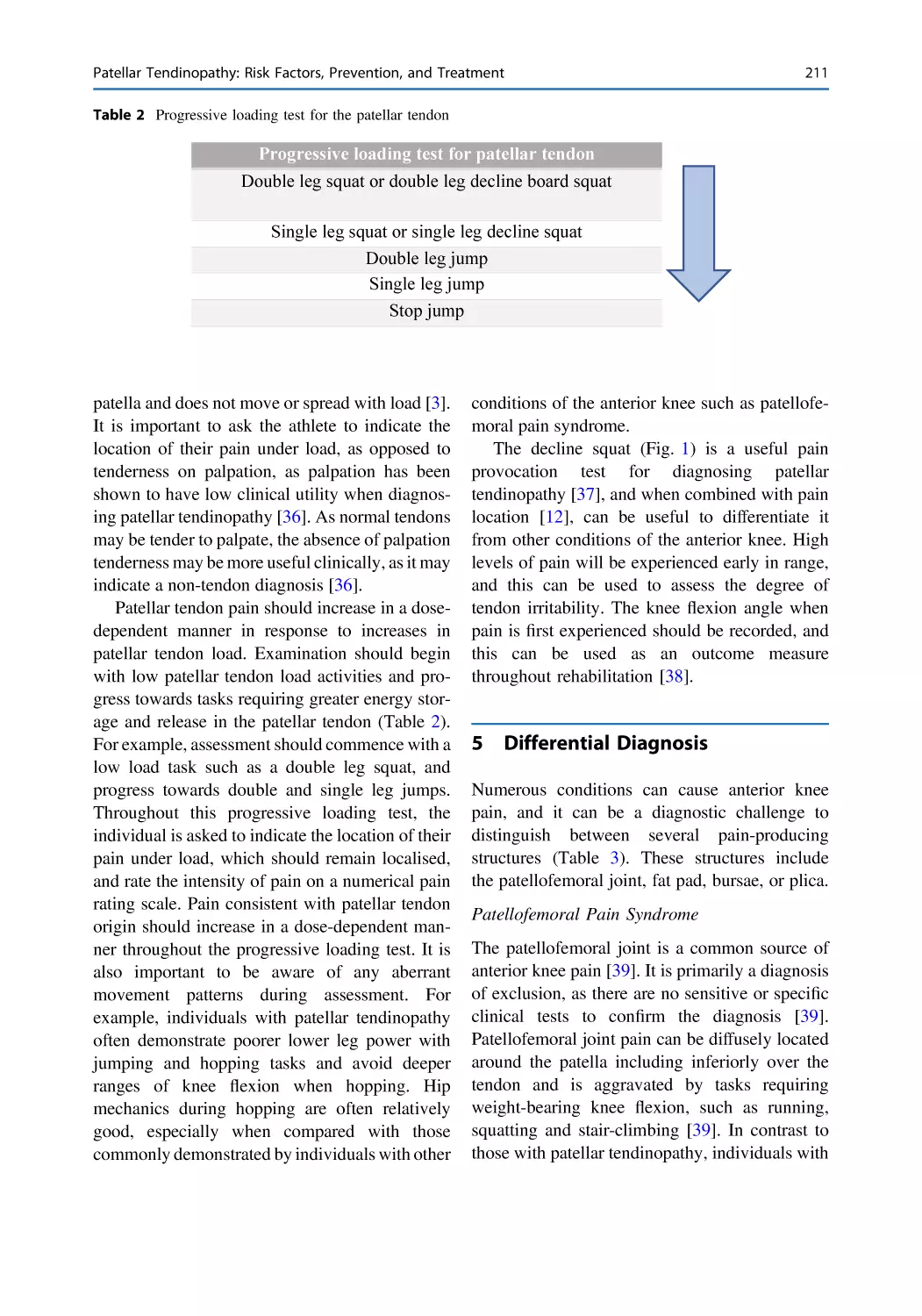
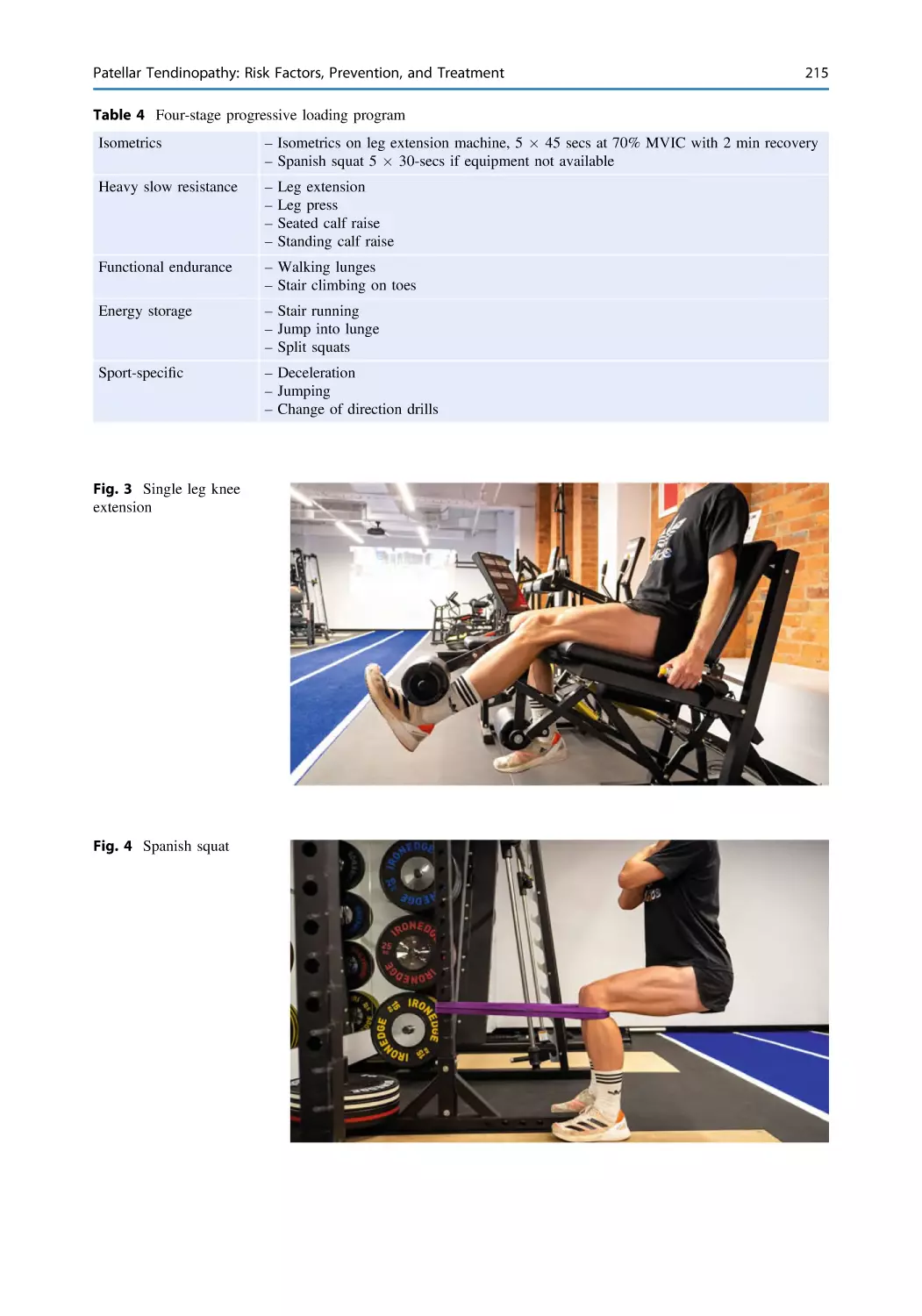
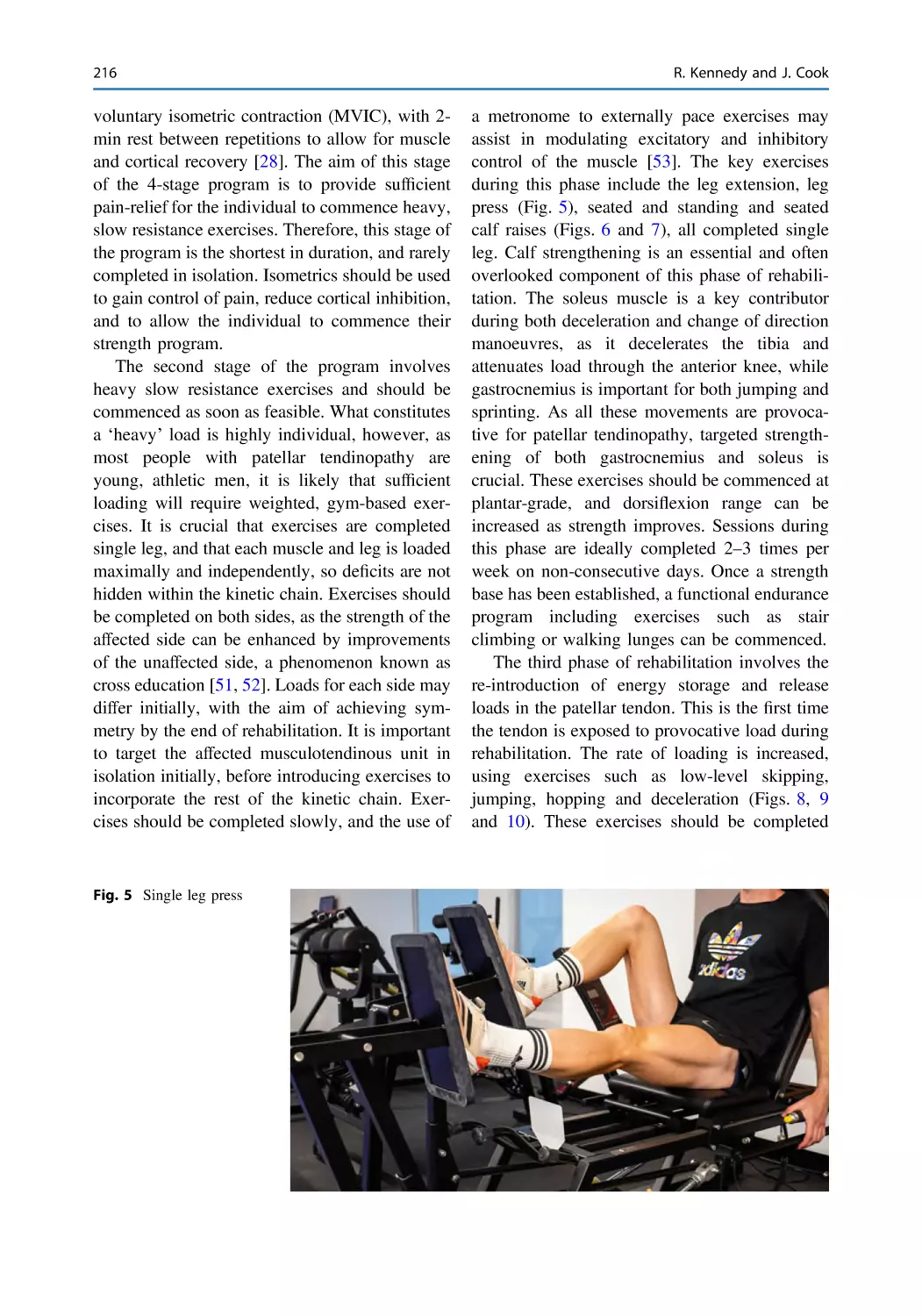
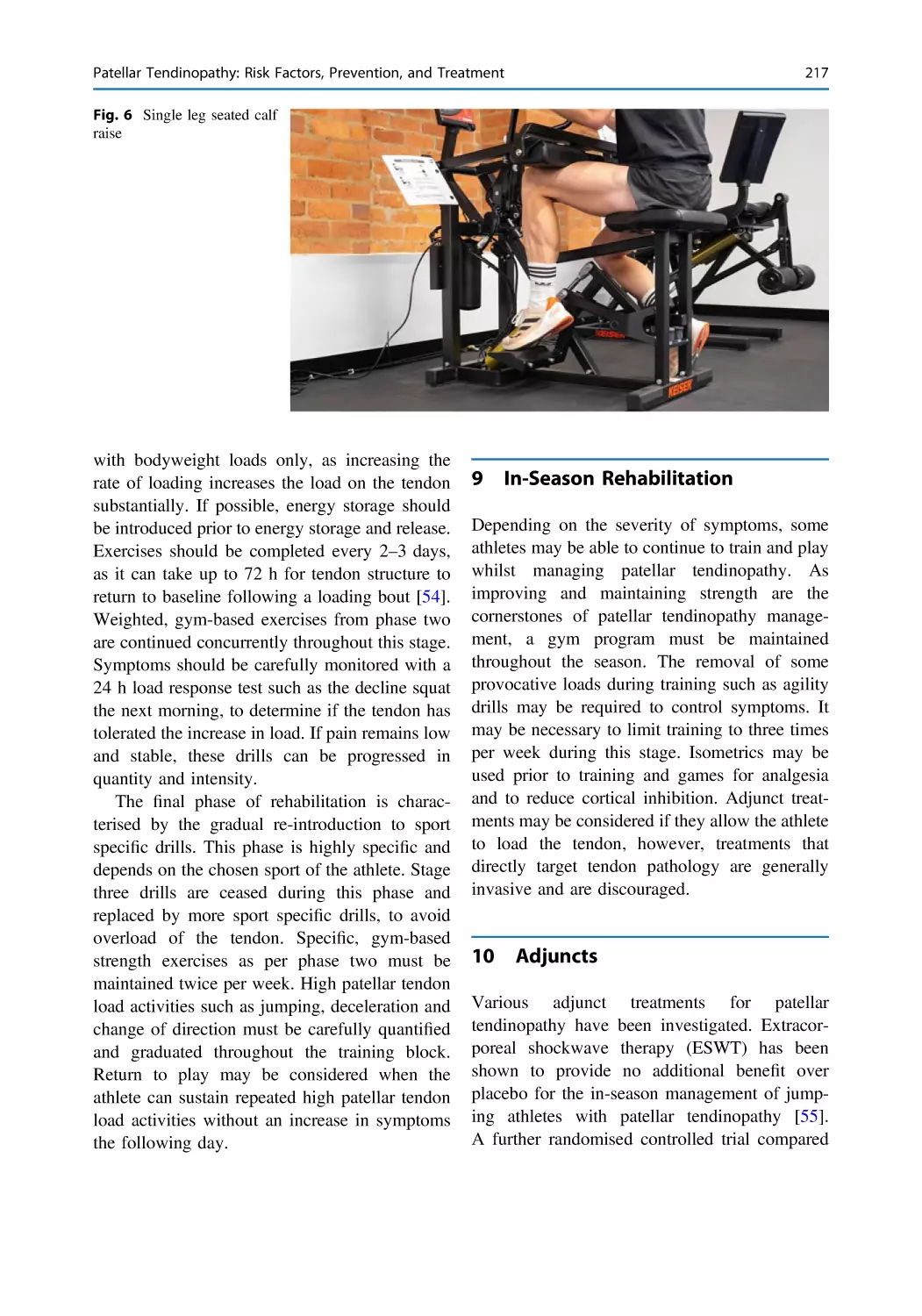
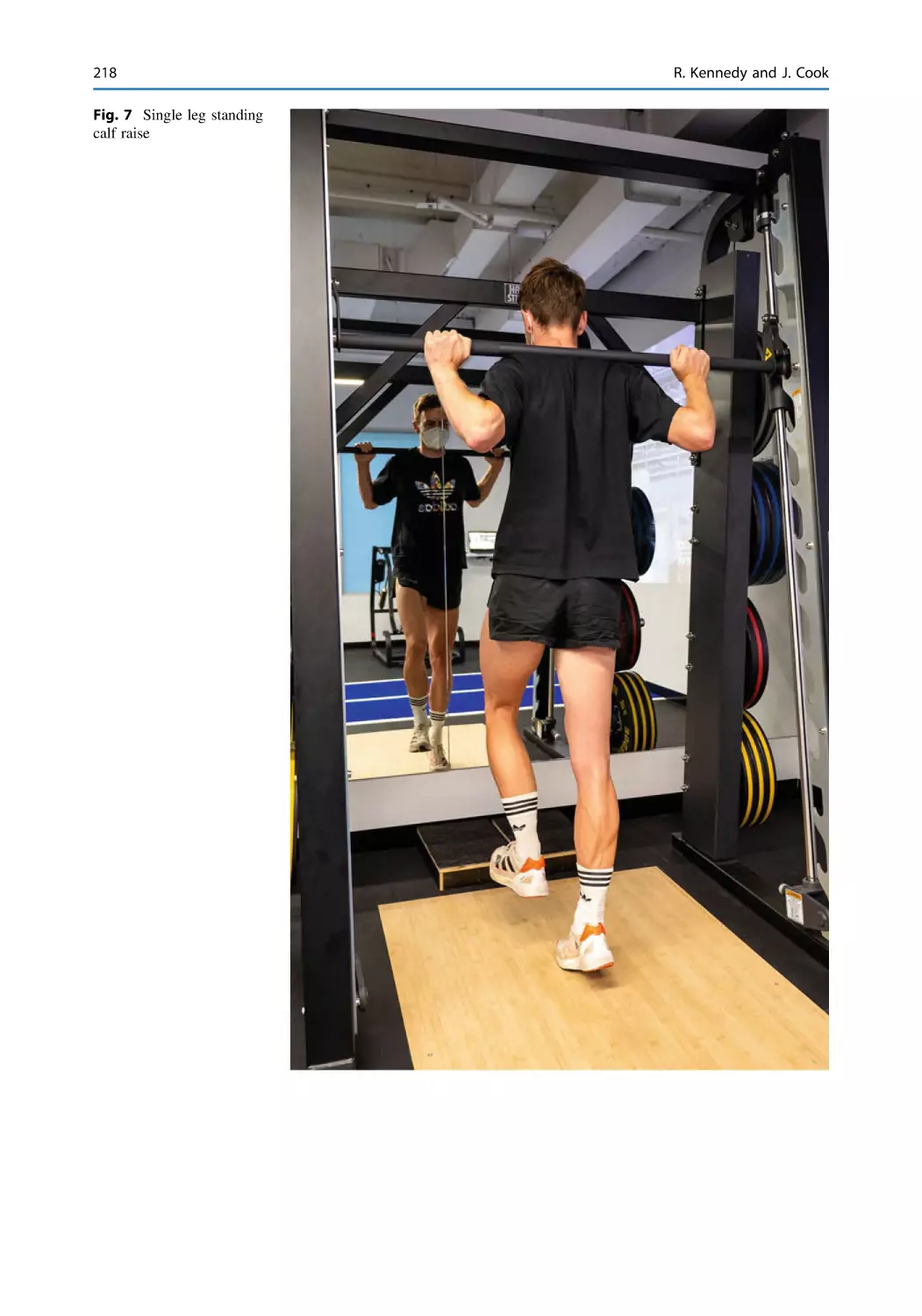
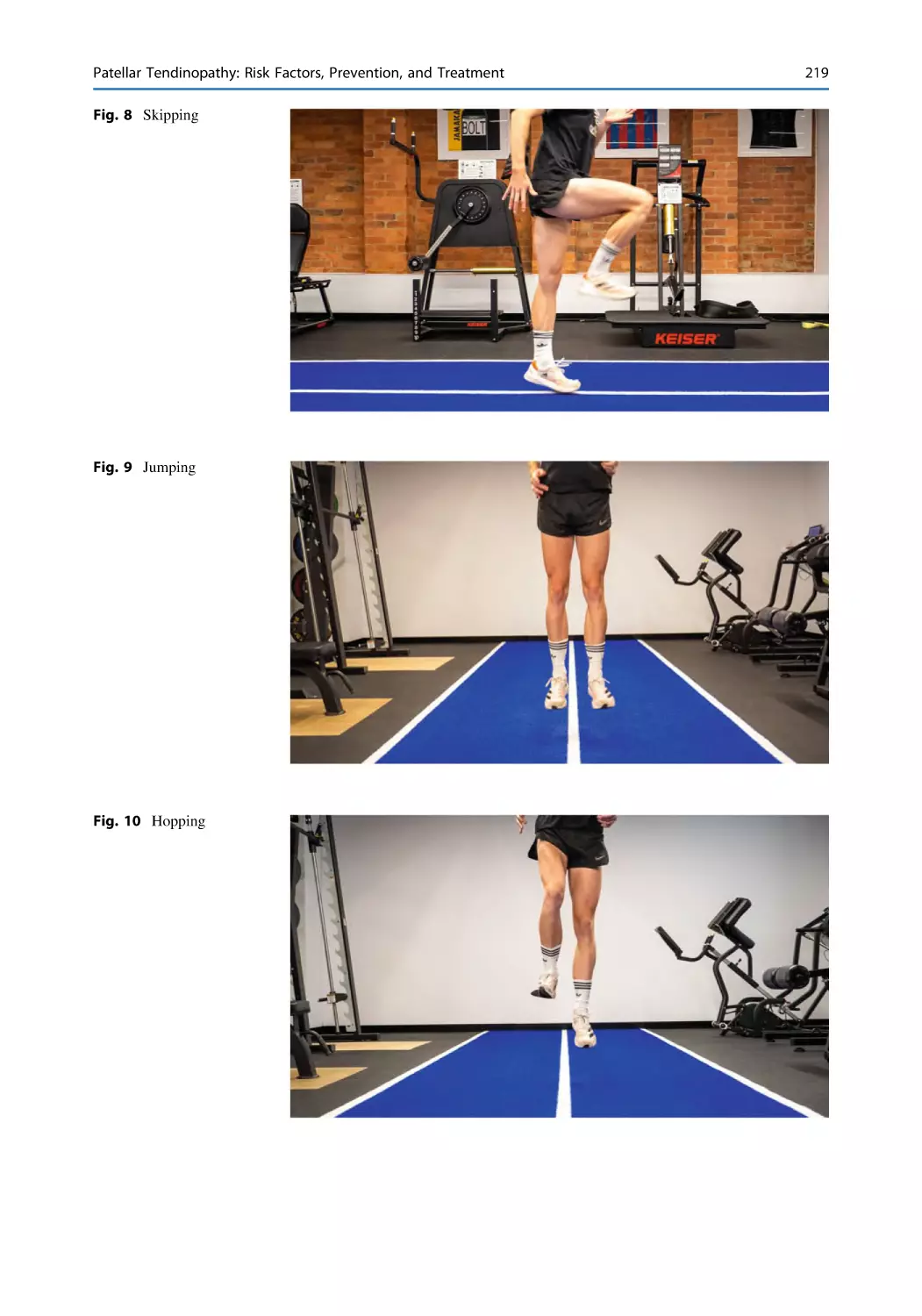
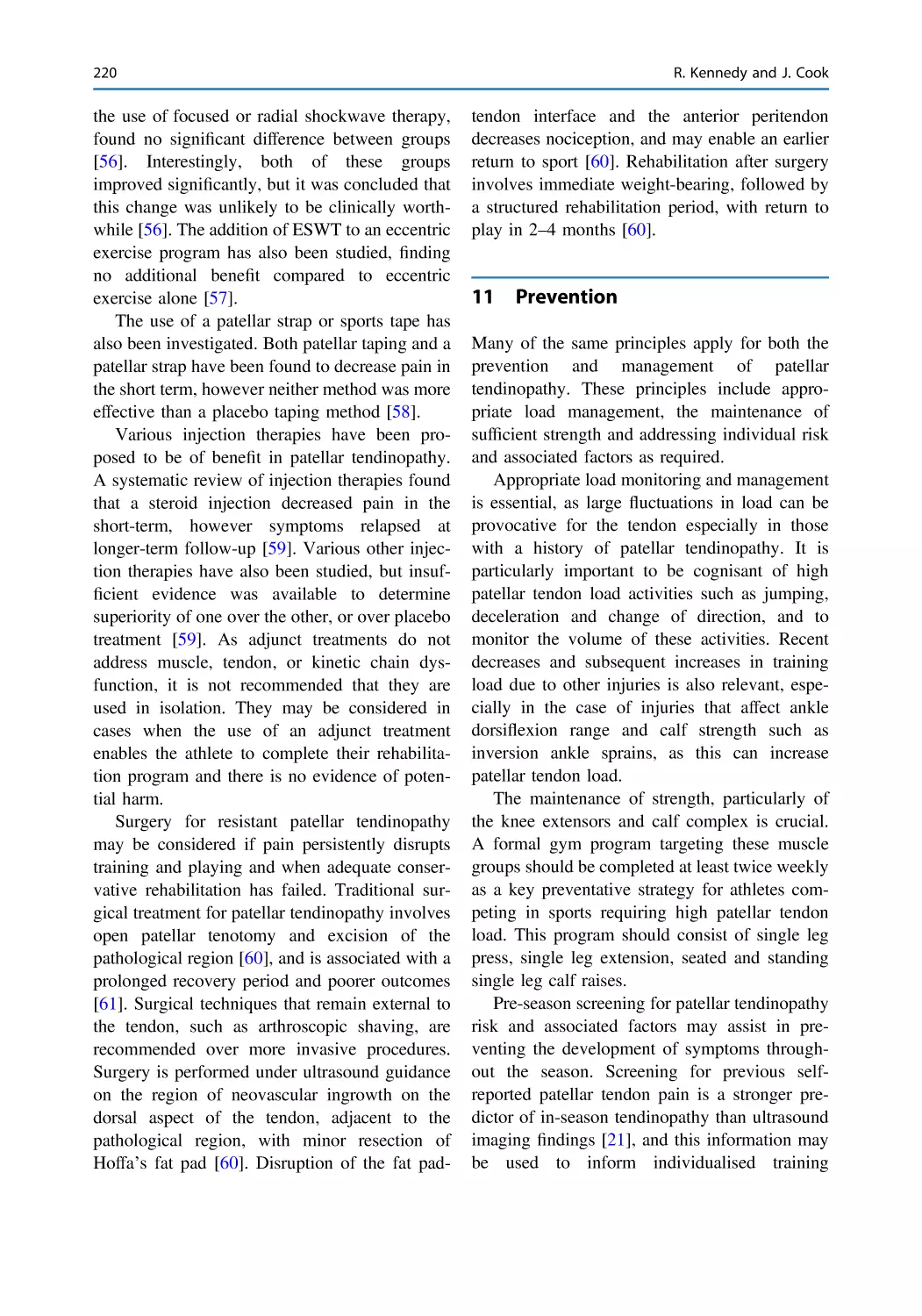
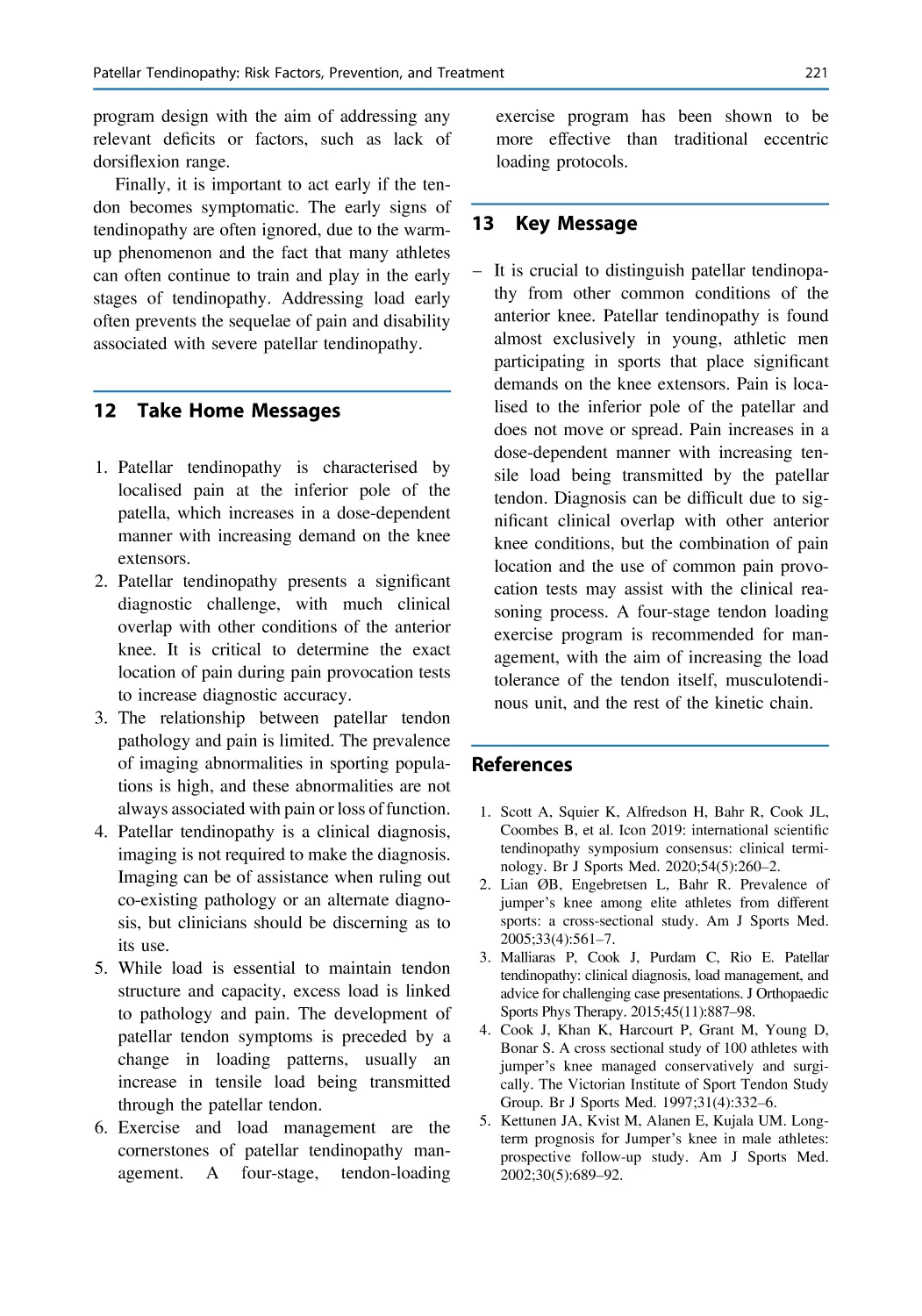
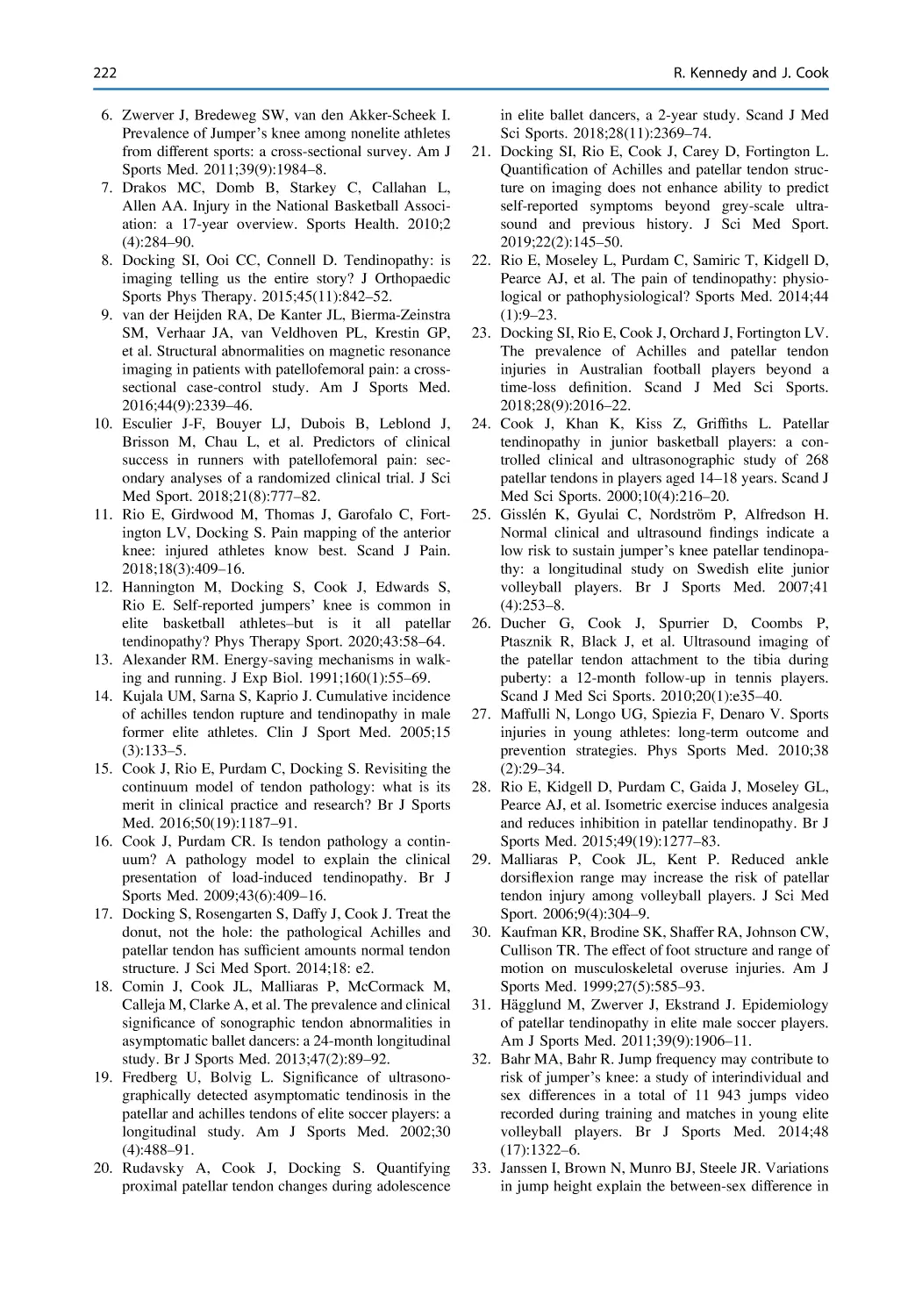
Patellar Tendinopathy: Risk Factors, Prevention,
and Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207
Rochelle Kennedy and Jill Cook
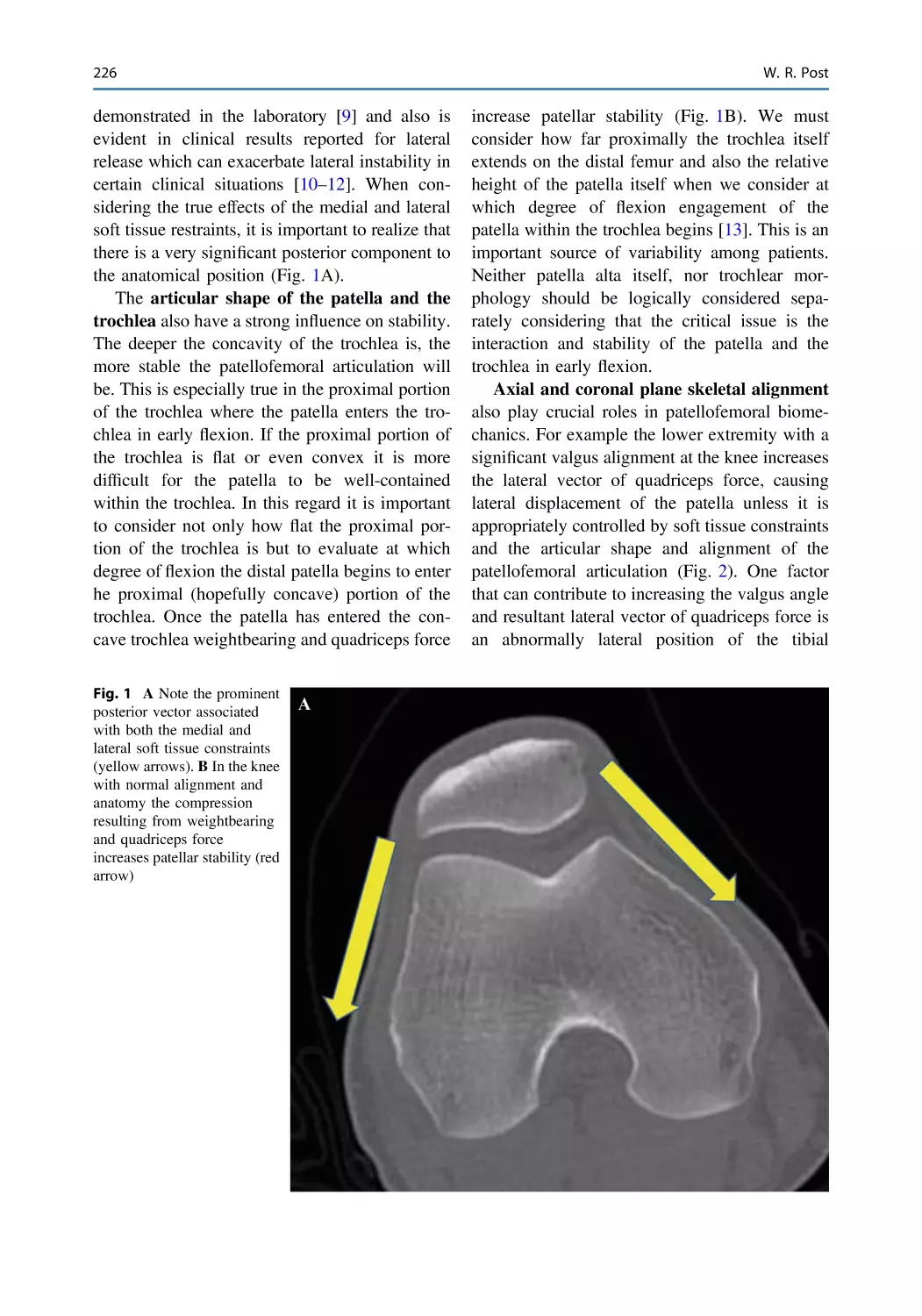
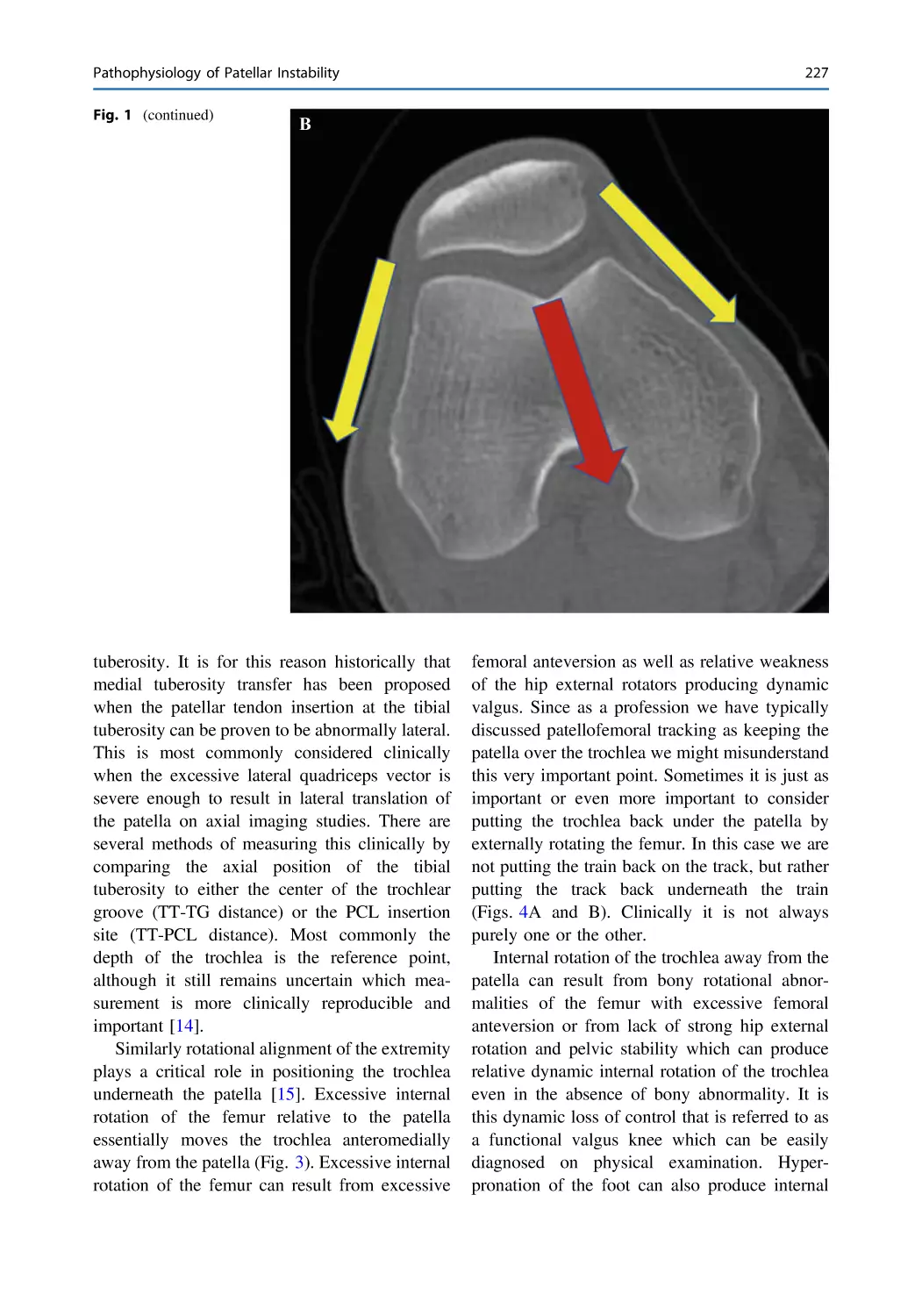
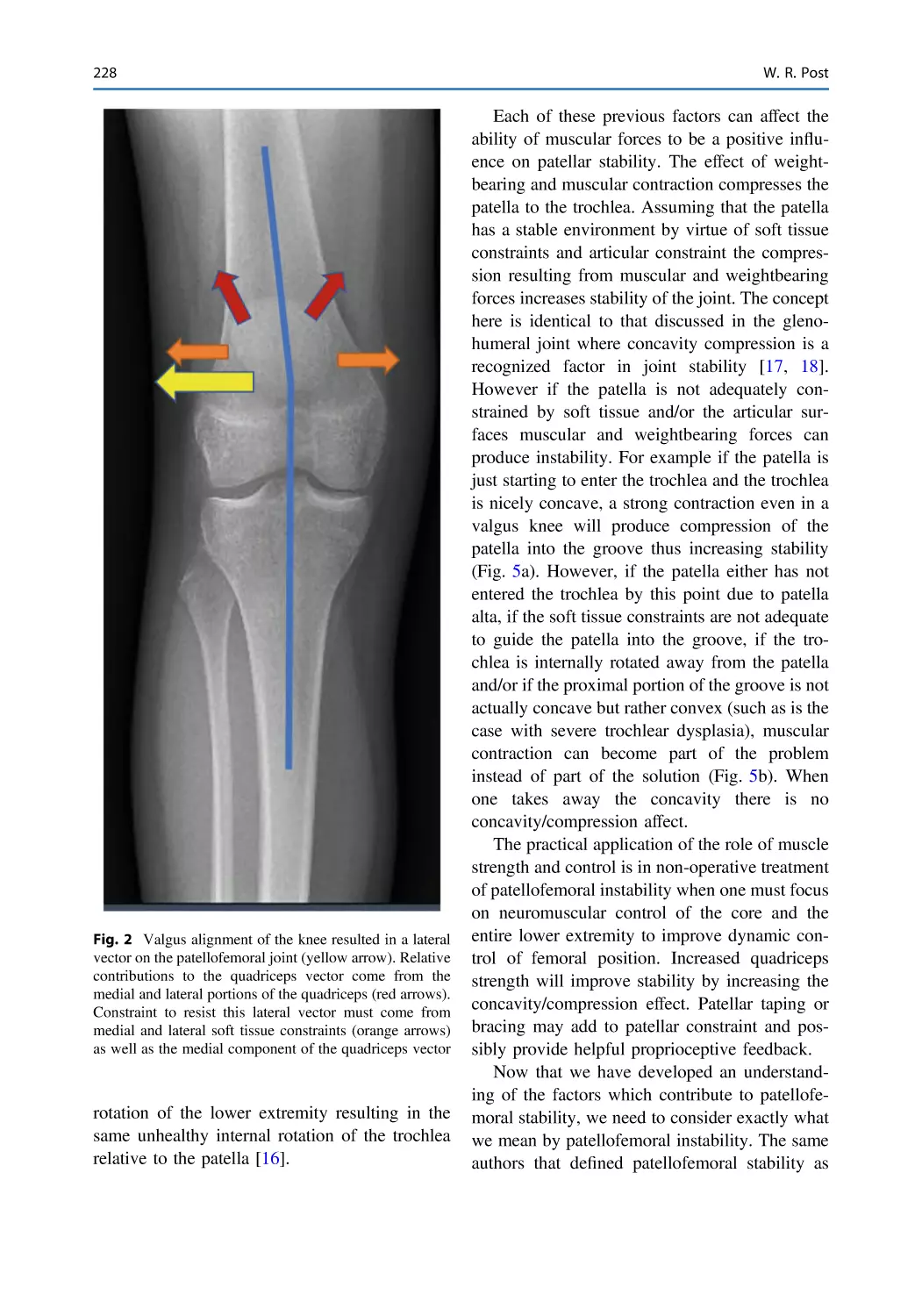
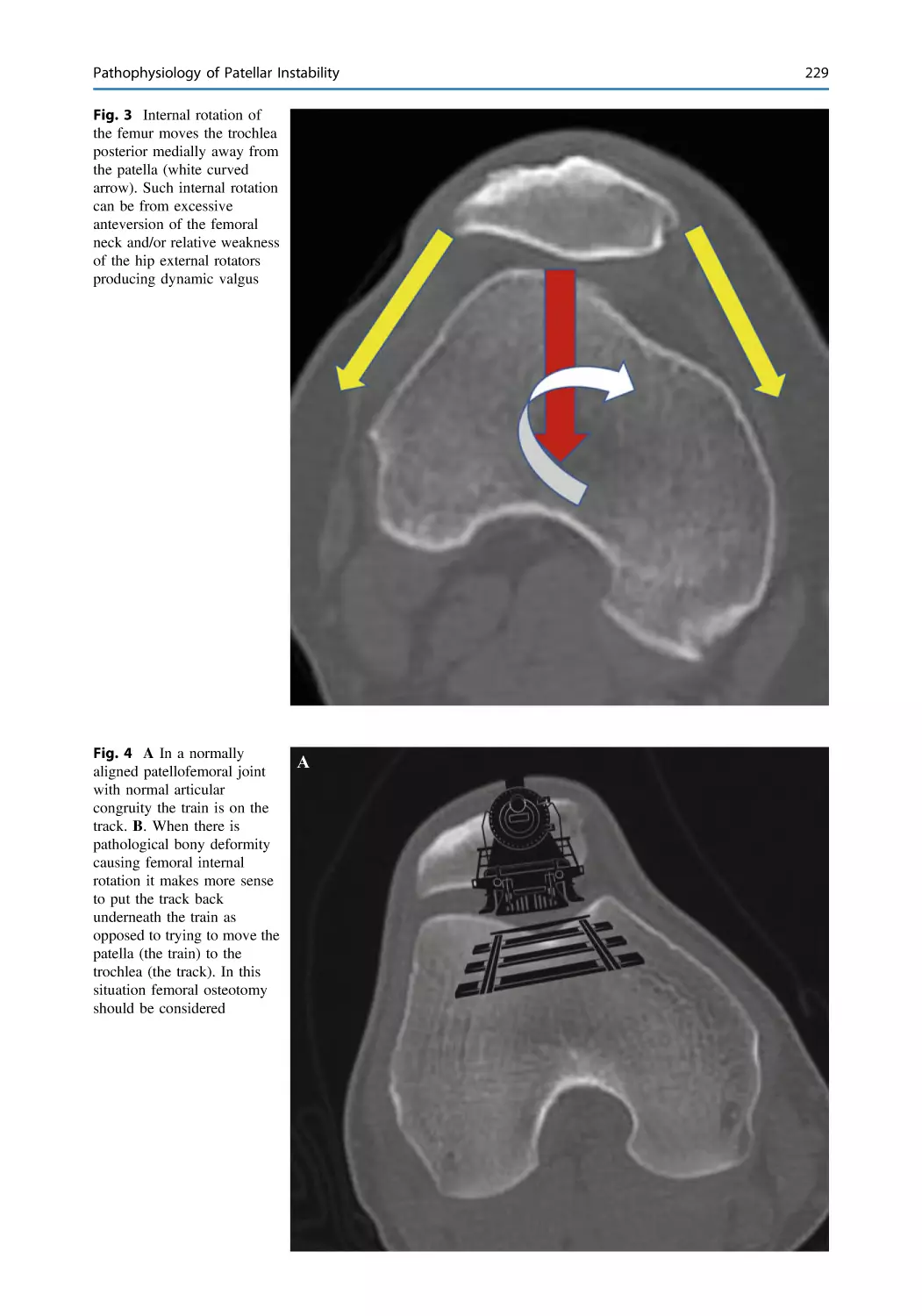
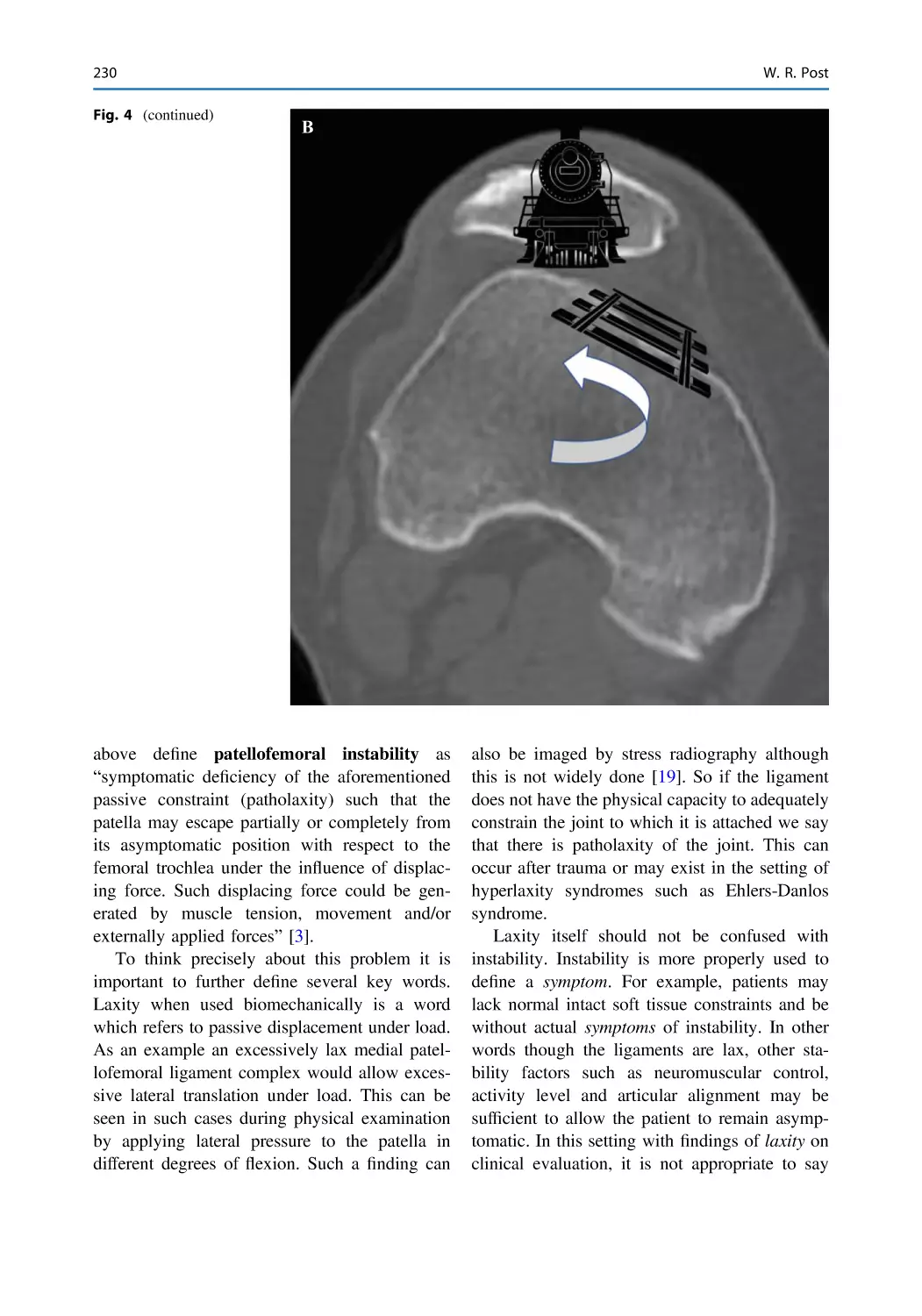
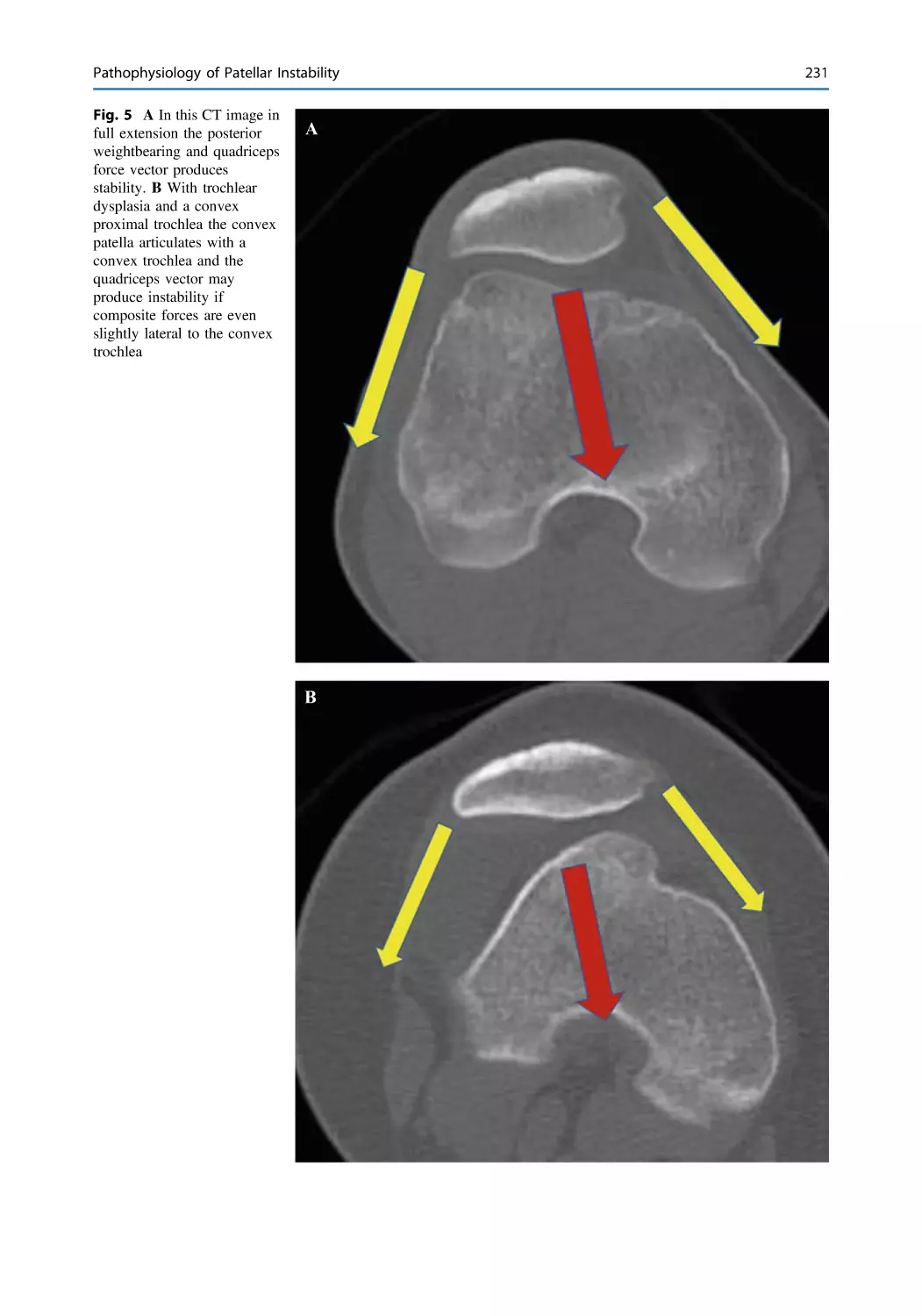
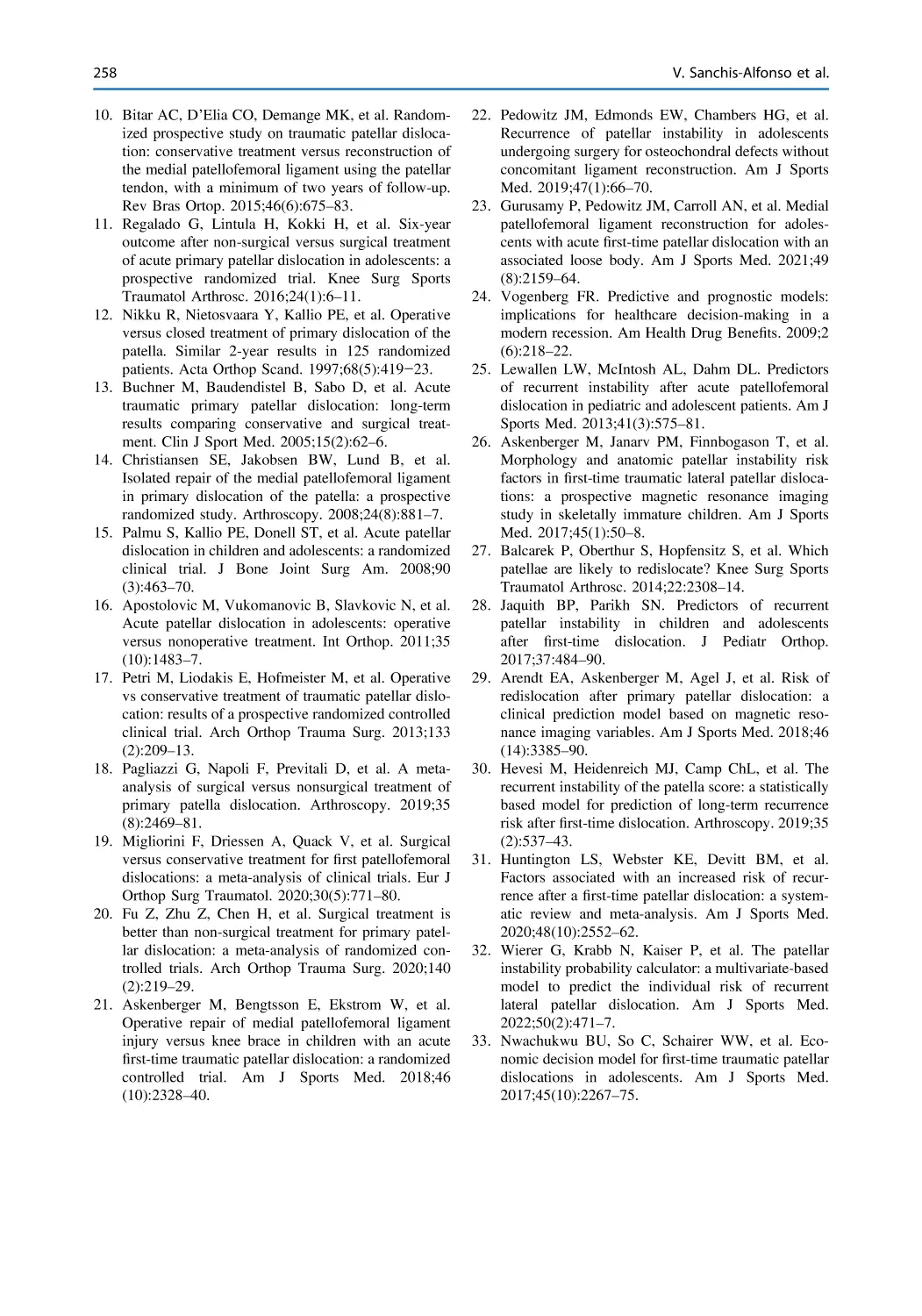
Pathophysiology of Patellar Instability . . . . . . . . . . . . . . . . . . . . . . 225
William R. Post
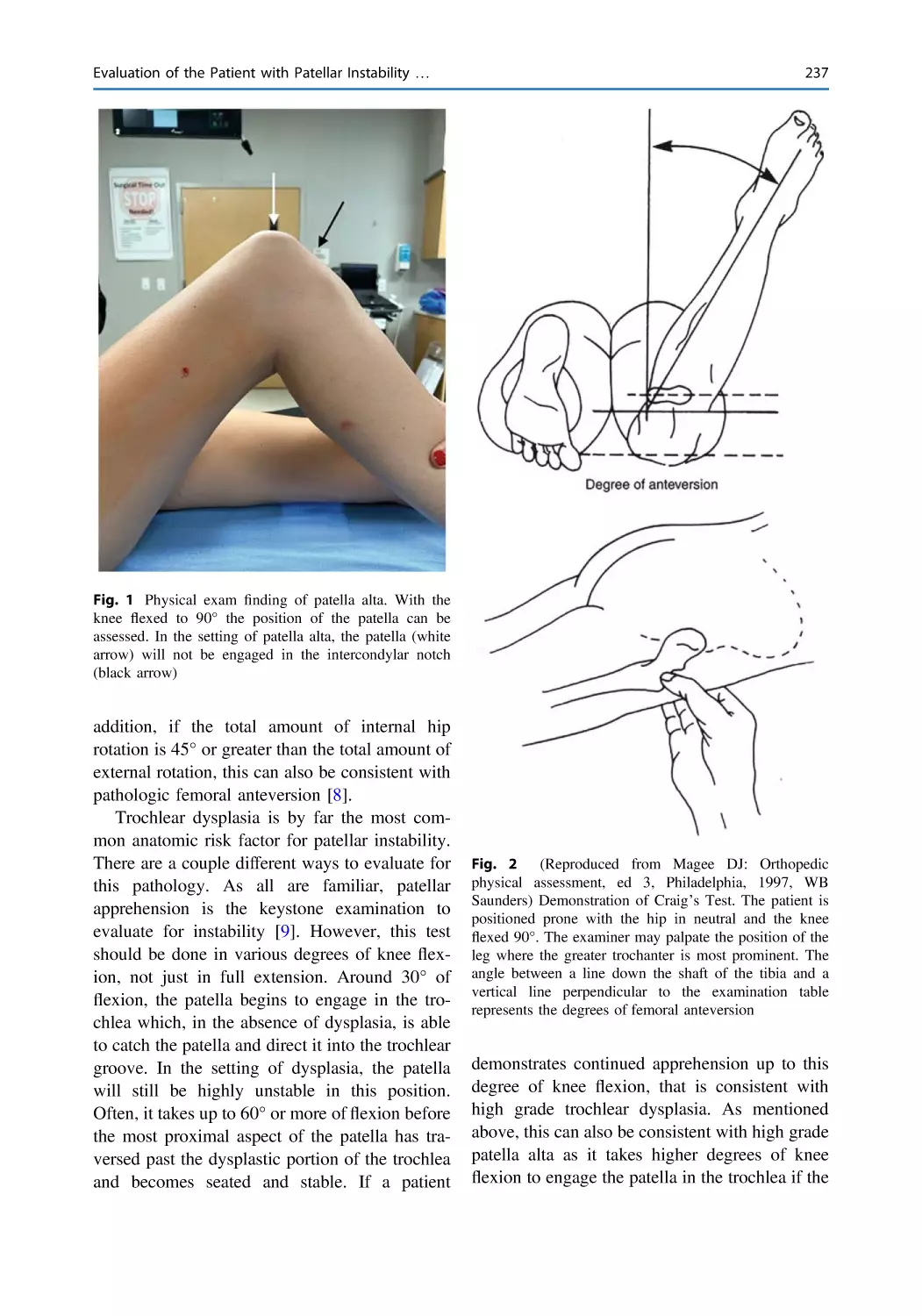
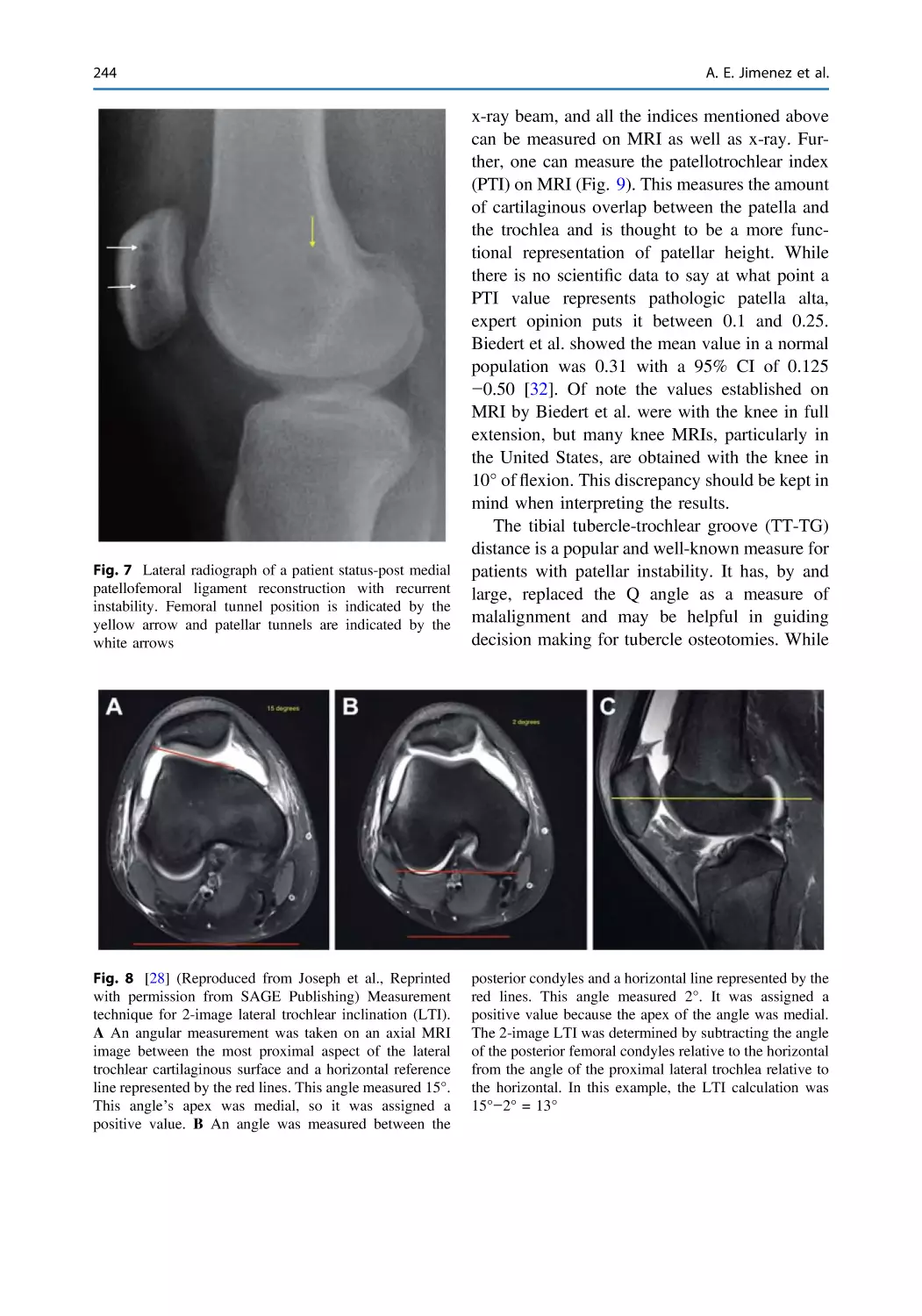
Evaluation of the Patient with Patellar Instability:
Clinical and Radiological Assessment . . . . . . . . . . . . . . . . . . . . . . . 235
Andrew E. Jimenez, Lee Pace, and Donald C. Fithian
Evolving Management of Acute Dislocations of the Patella . . . . . . 251
Vicente Sanchis-Alfonso, Erik Montesinos-Berry,
and Marc Tompkins
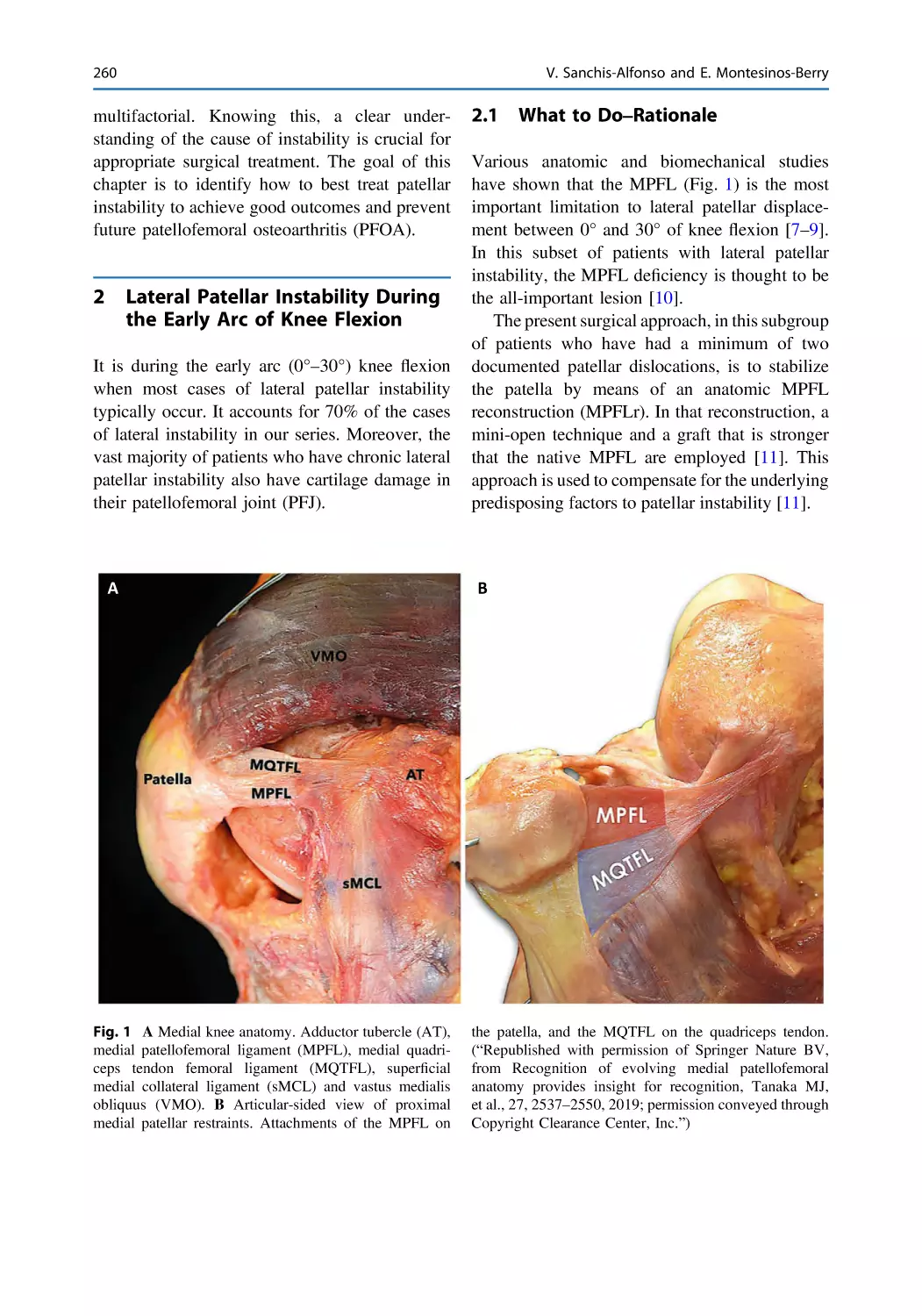
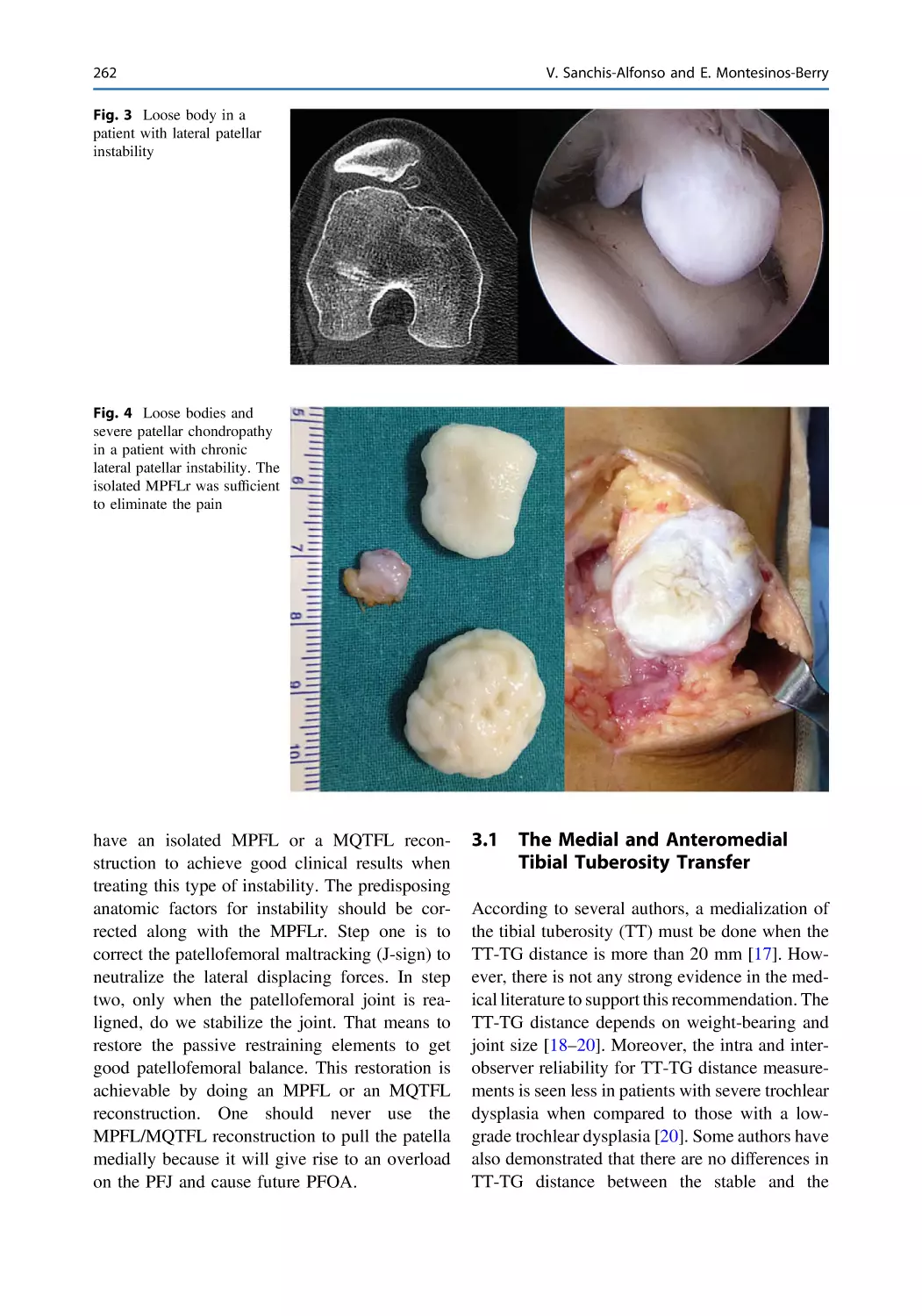
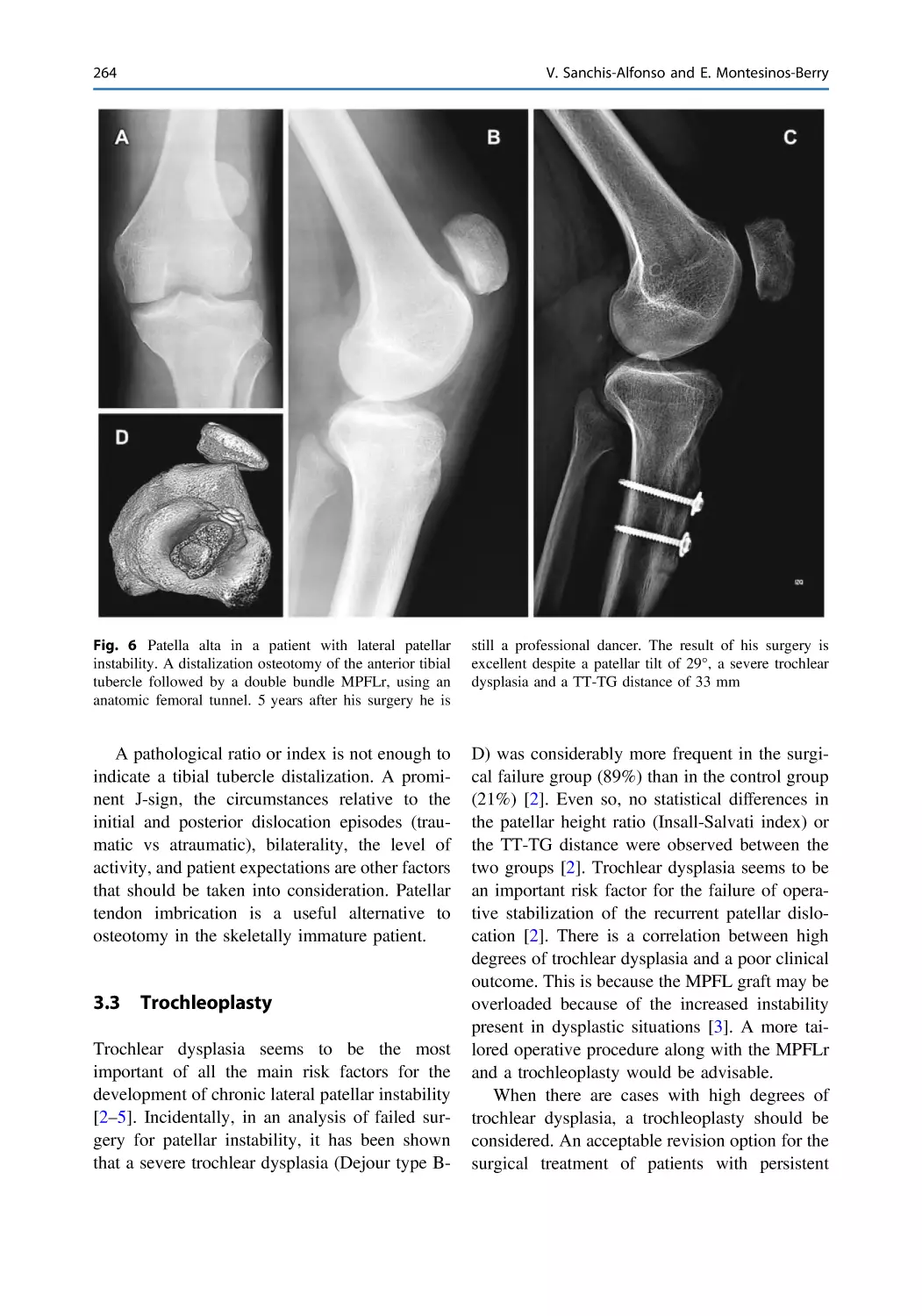
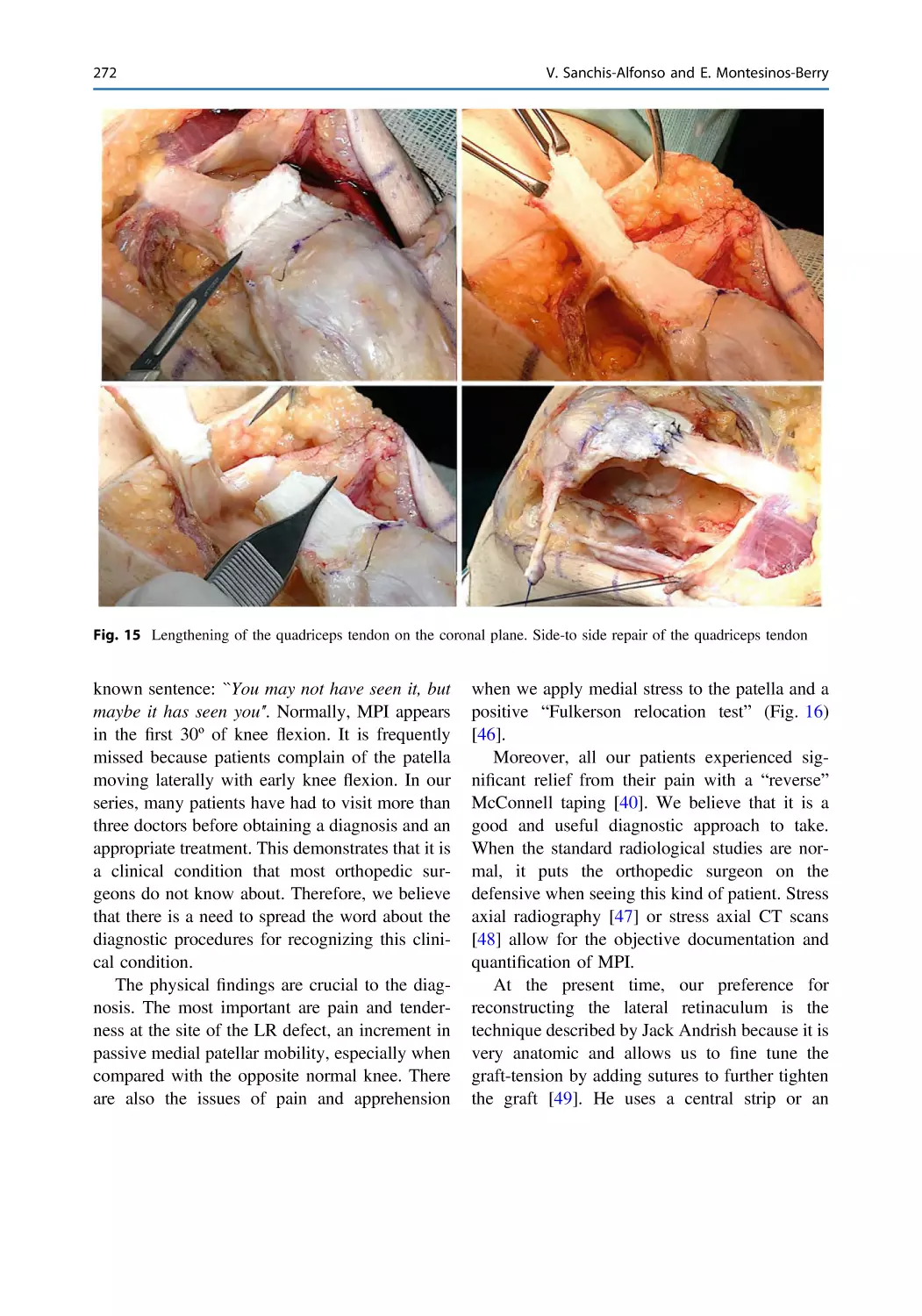
How to Deal with Chronic Patellar Instability . . . . . . . . . . . . . . . . 259
Vicente Sanchis-Alfonso and Erik Montesinos-Berry
Limitations of Patellofemoral Surgery in Children . . . . . . . . . . . . . 277
Mahad Hassan and Marc Tompkins
The Failed Medial Patellofemoral Ligament Reconstruction.
What Can We Do? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283
Vicente Sanchis-Alfonso and Cristina Ramírez-Fuentes
Surgical Treatment of Recurrent Patellar Instability: History
and Current Concepts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305
Christopher A. Schneble, David A. Molho, and John P. Fulkerson
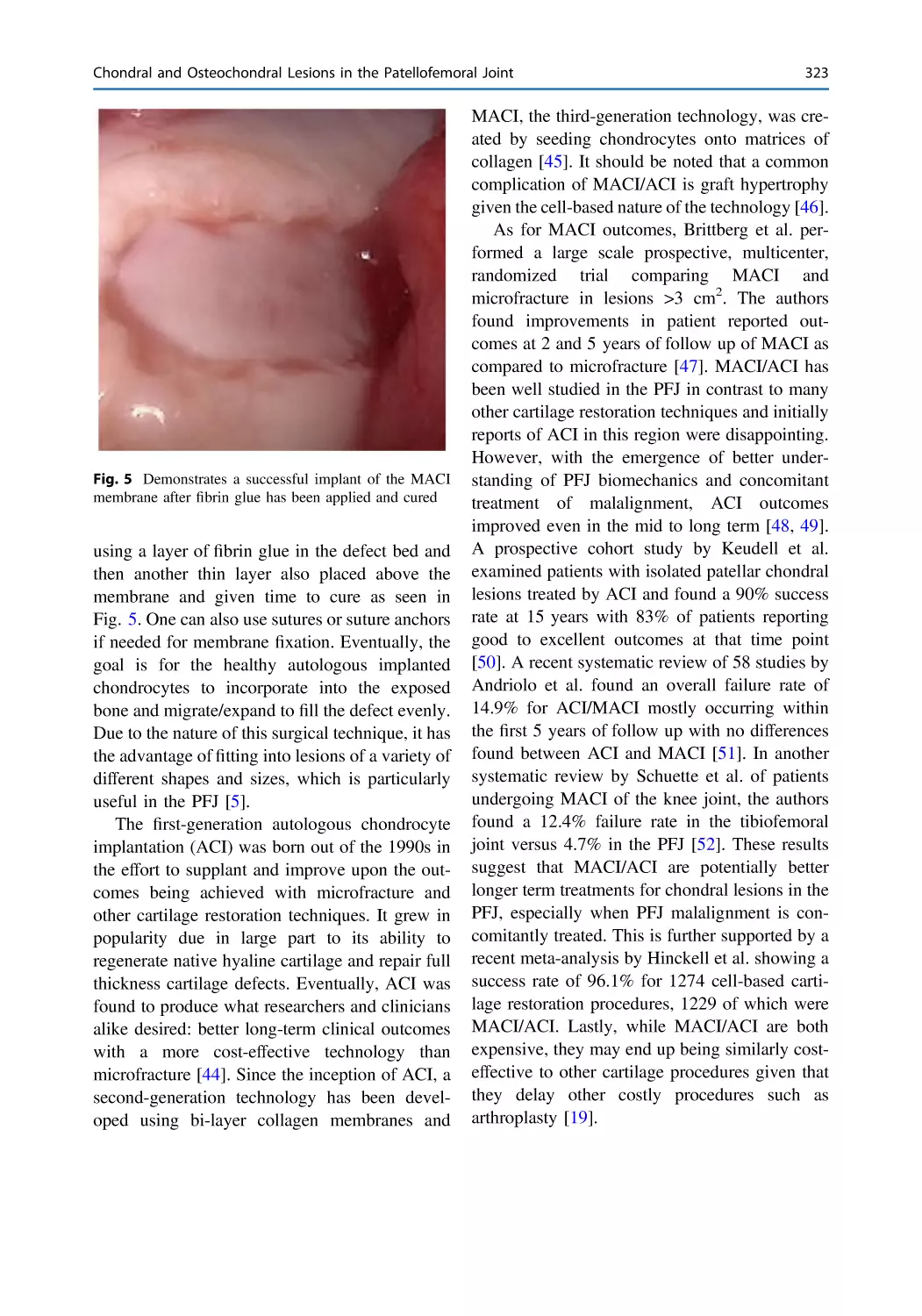
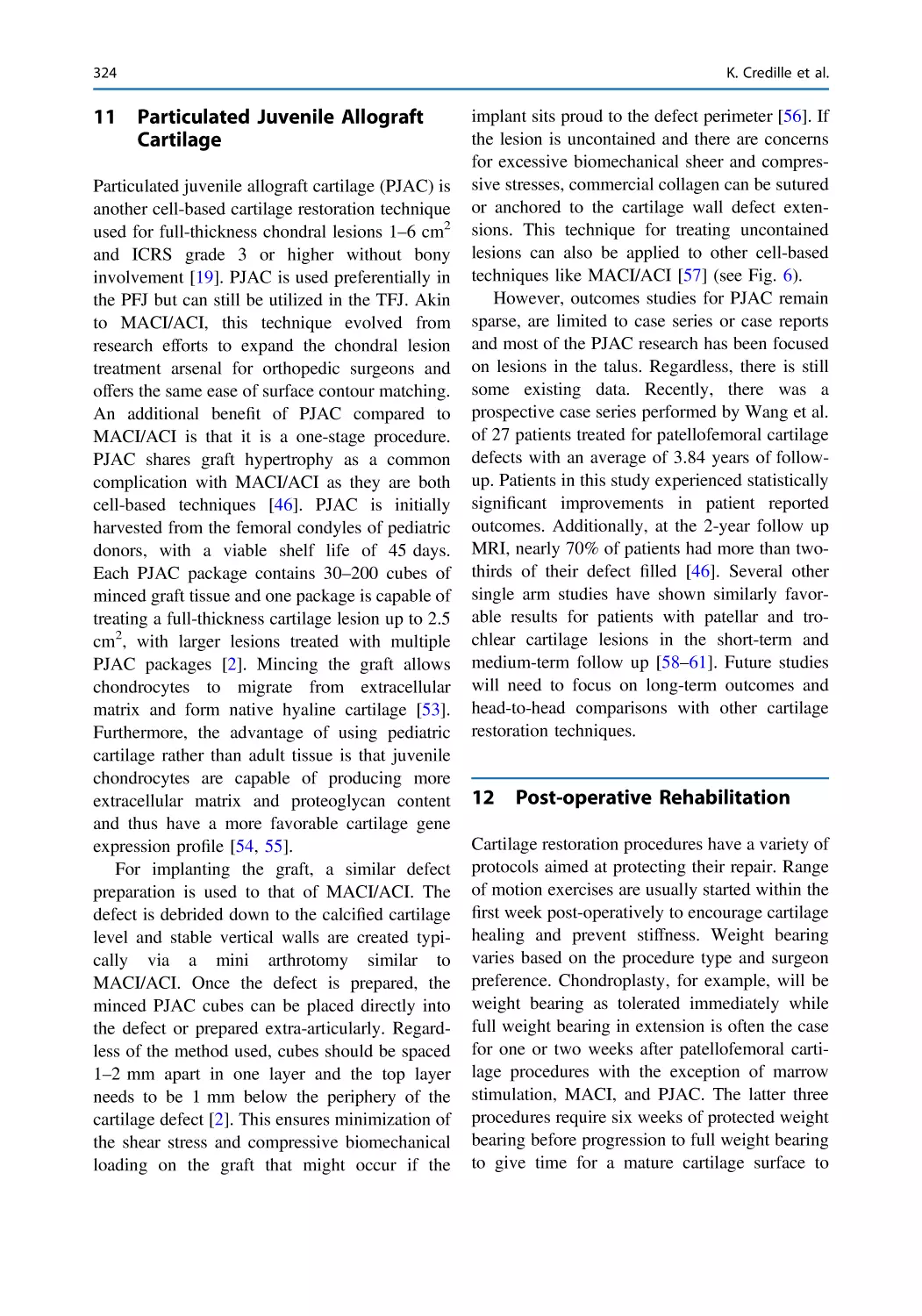
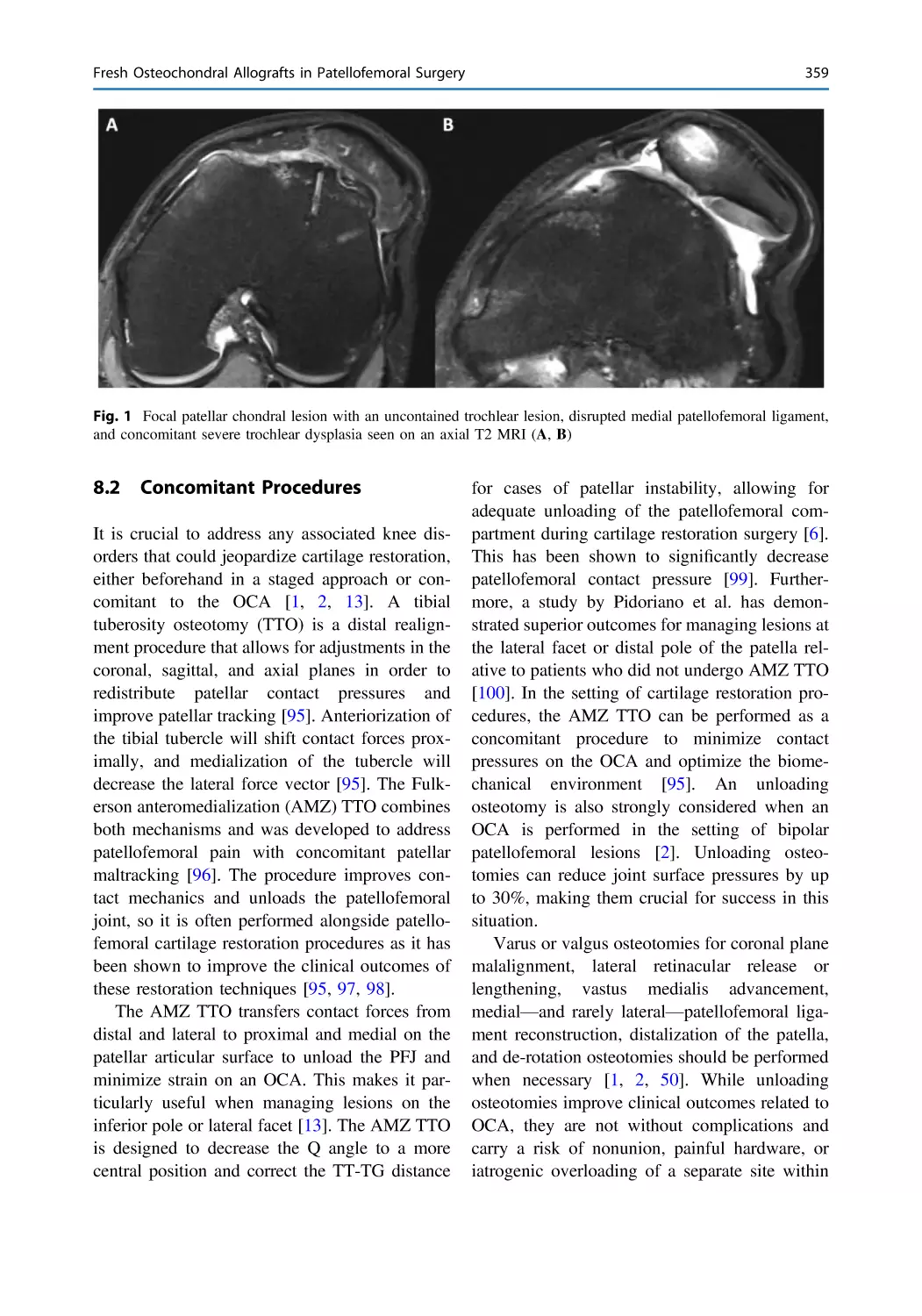
Chondral and Osteochondral Lesions in the Patellofemoral
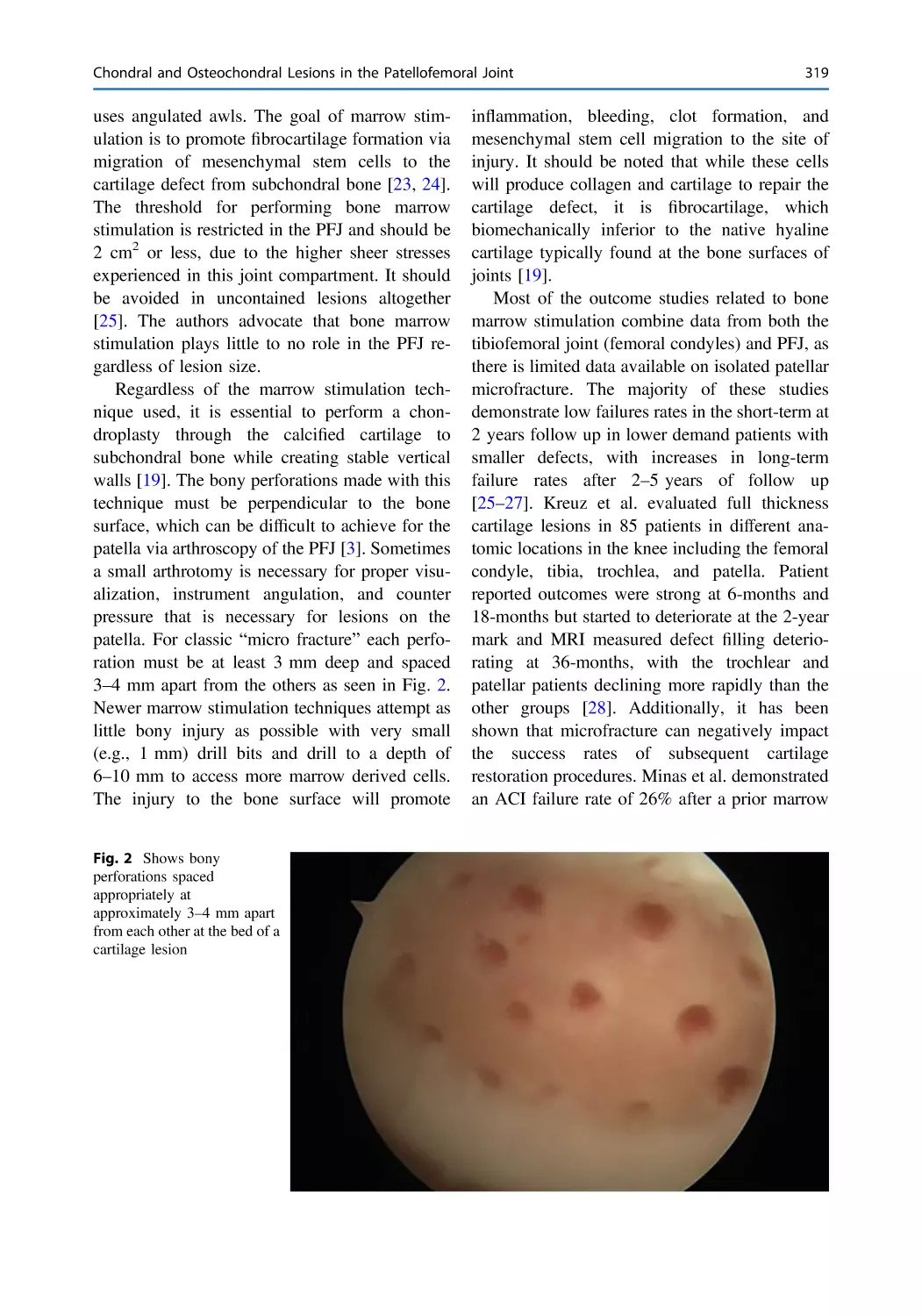
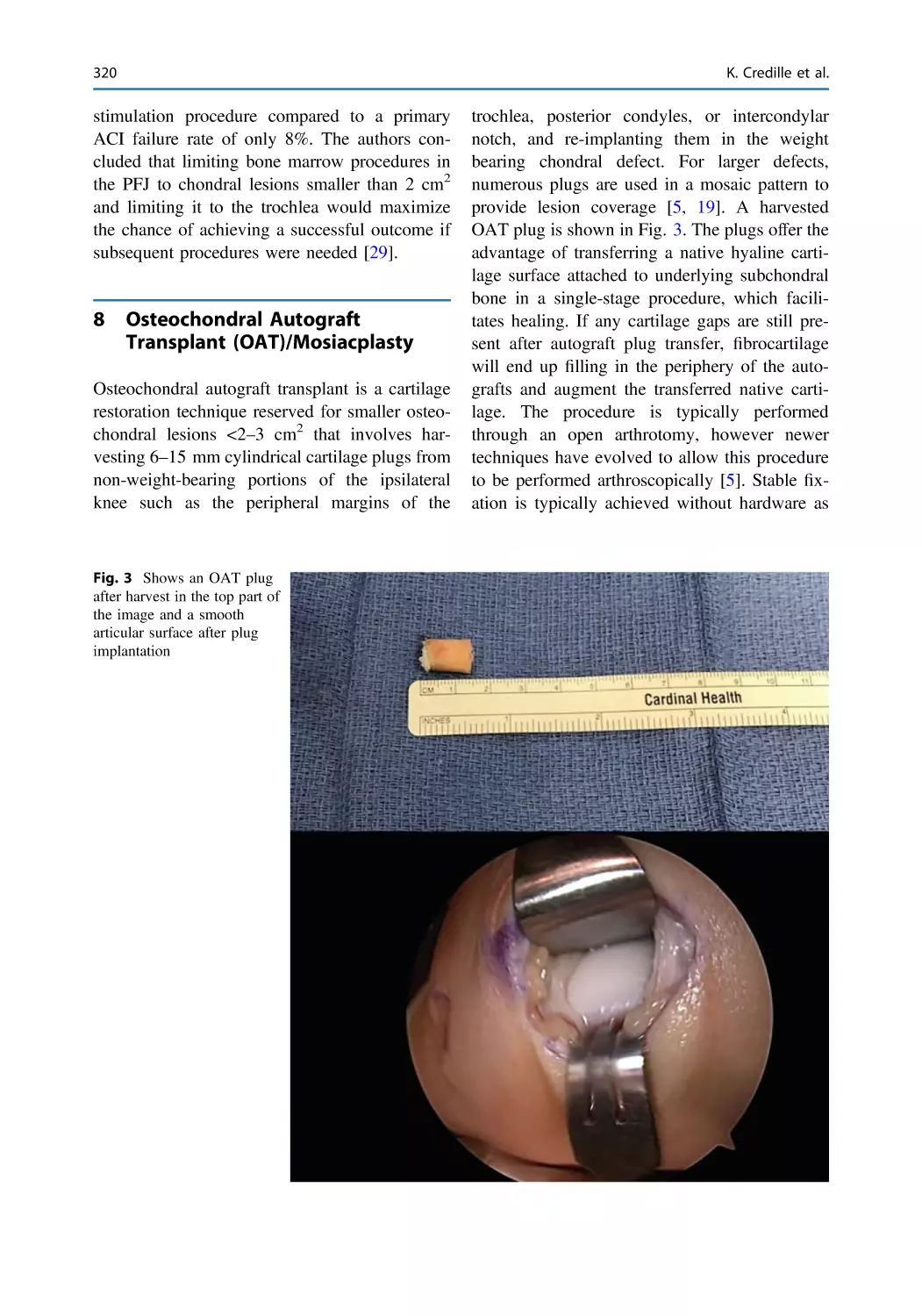
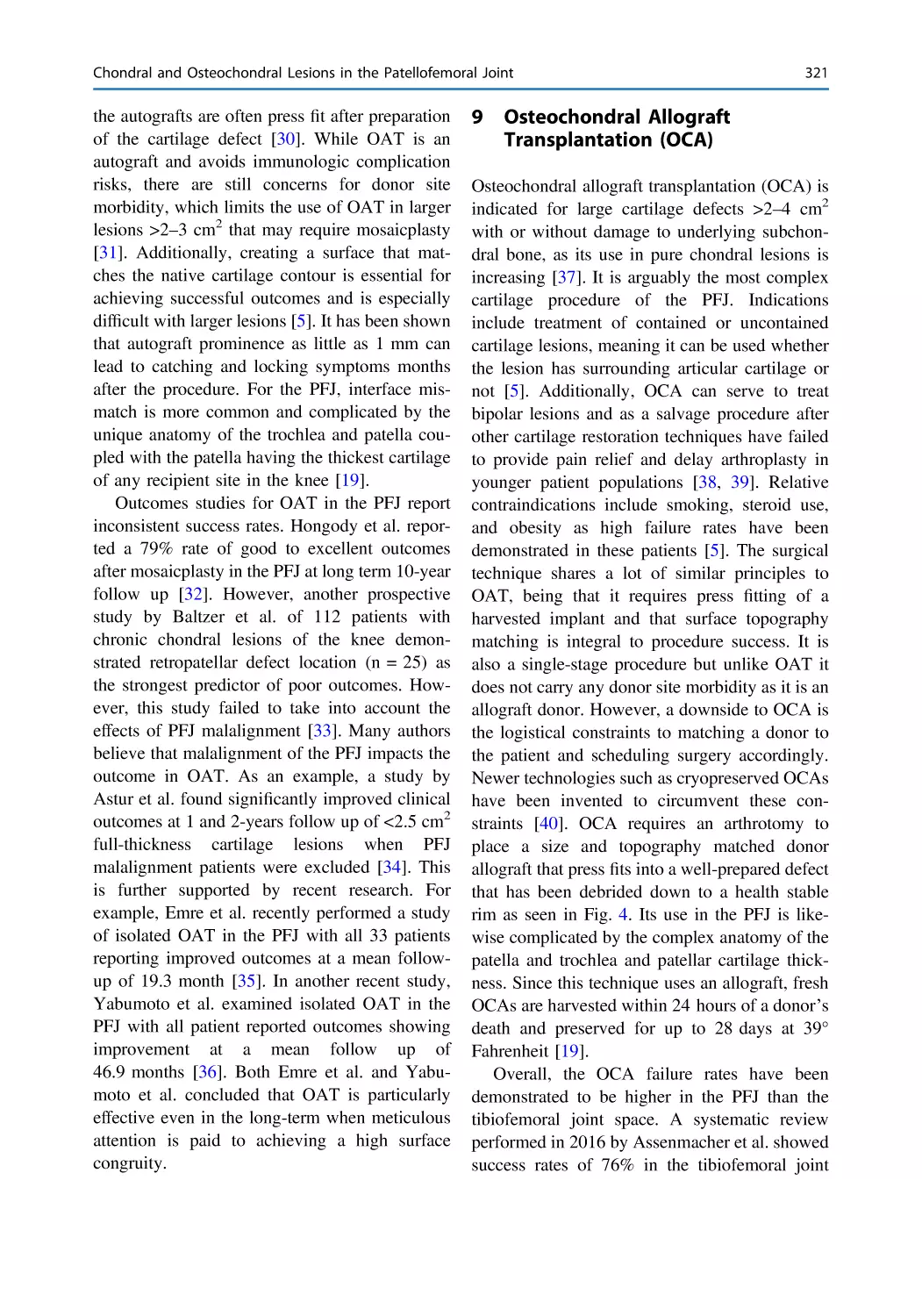
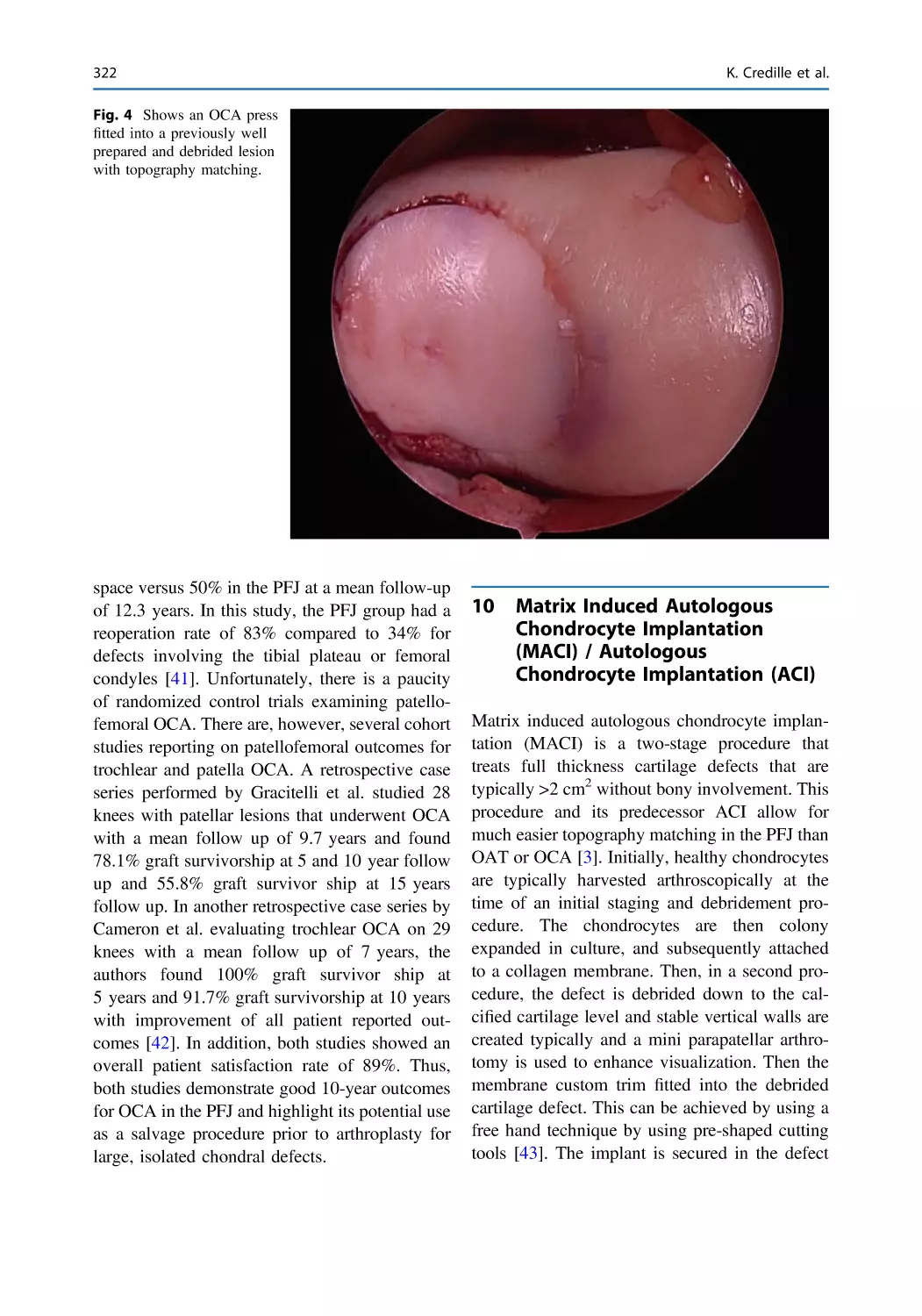
Joint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 315
Kevin Credille, Dhanur Damodar, Zachary Wang,
Andrew Gudeman, and Adam Yanke
Patellofemoral Arthritis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
Christopher S. Frey, Augustine W. Kang, Kenneth Lin,
Doug W. Bartels, Jack Farr, and Seth L. Sherman
Contents
Contents
xxiii
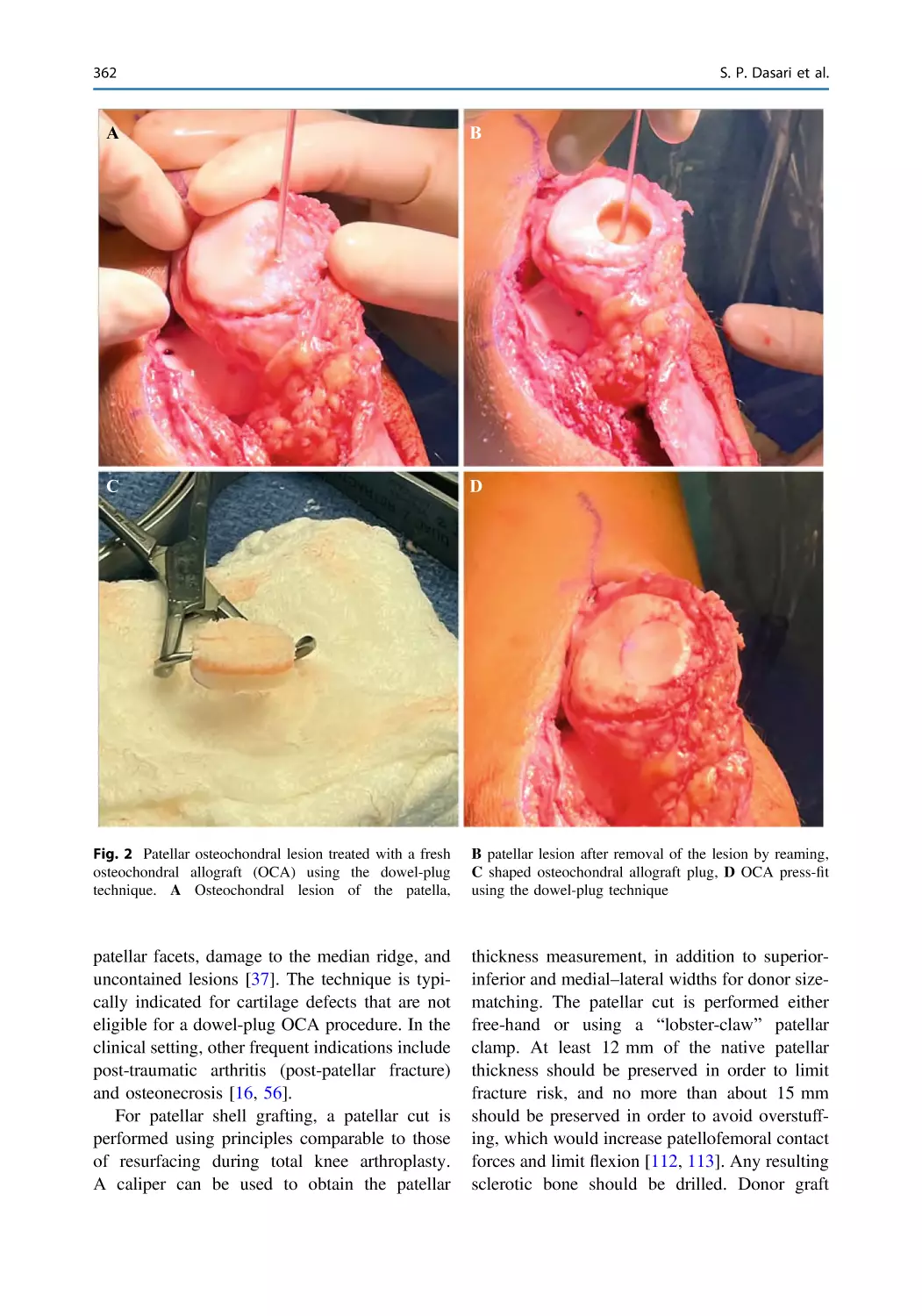
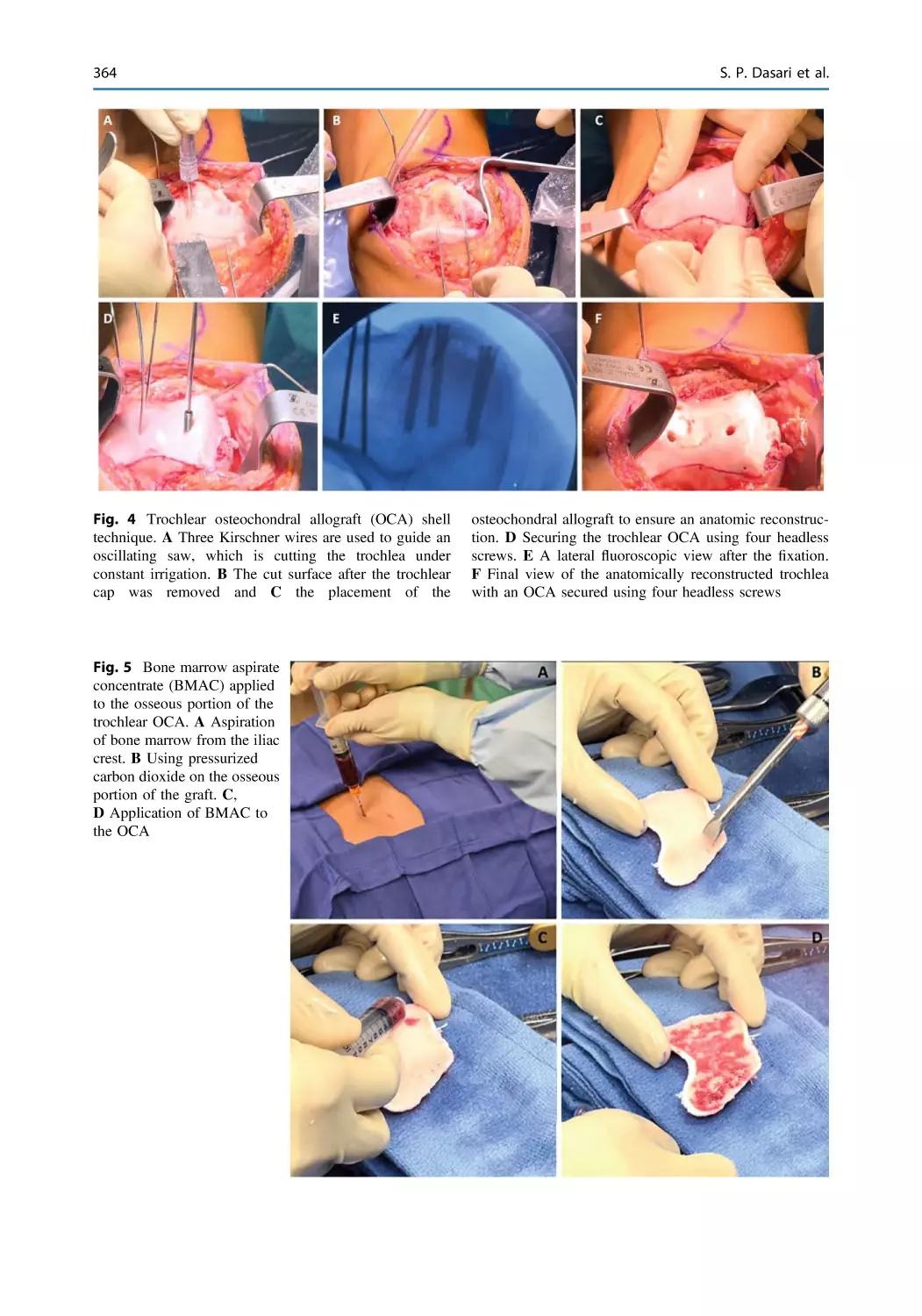
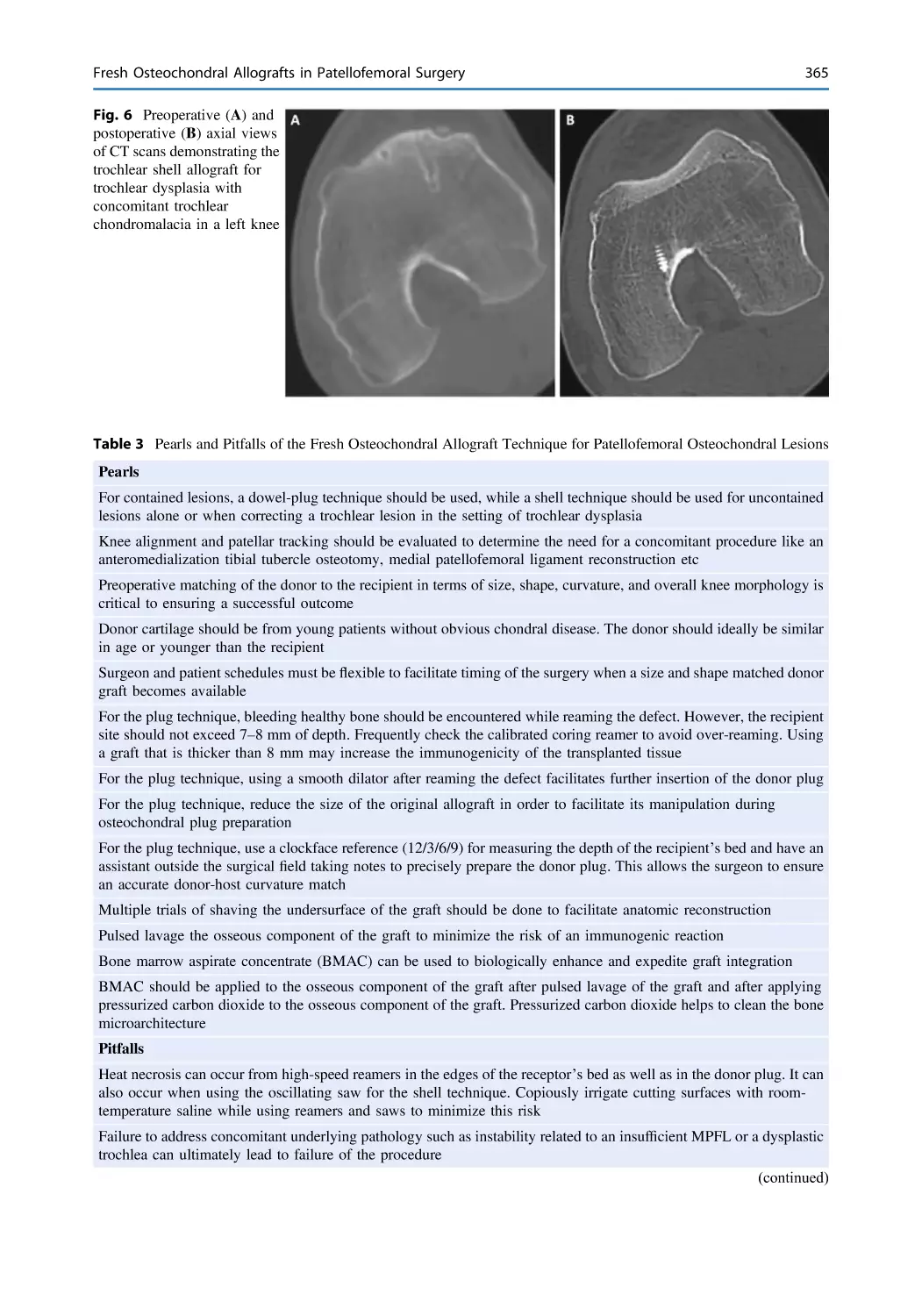
Fresh Osteochondral Allografts in Patellofemoral Surgery . . . . . . 349
Suhas P. Dasari, Enzo S. Mameri, Bhargavi Maheshwer,
Safa Gursoy, Jorge Chahla, and William Bugbee
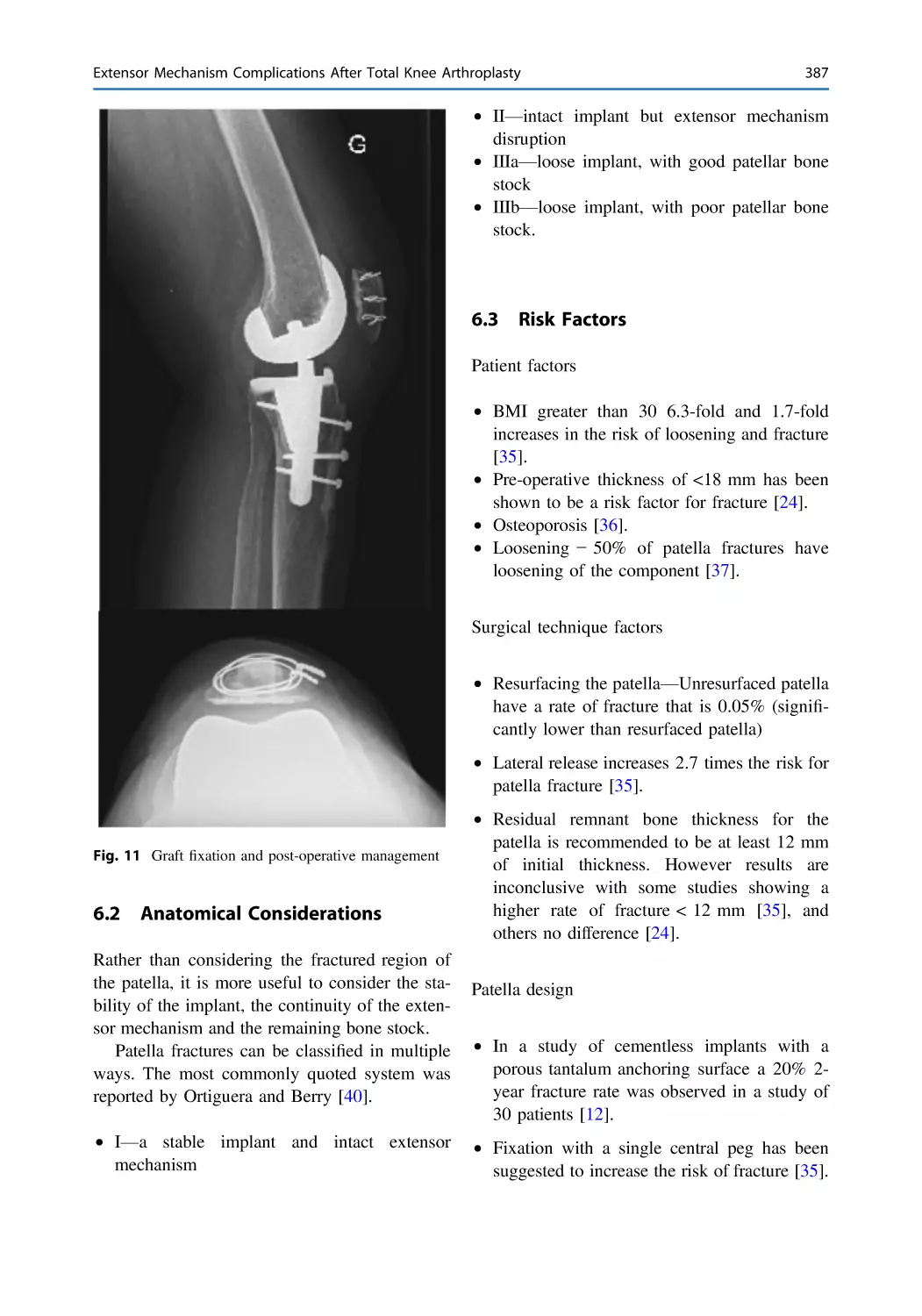
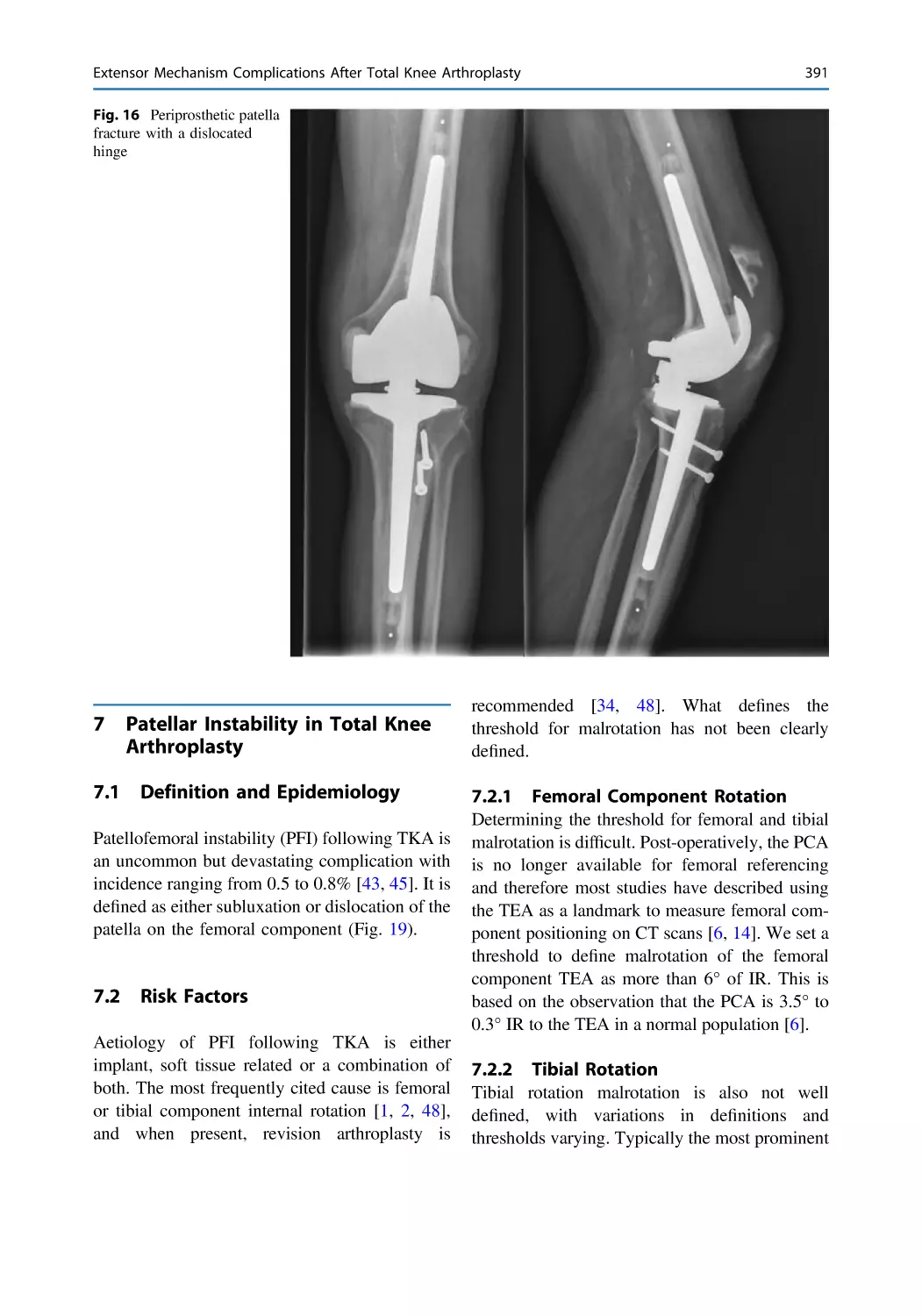
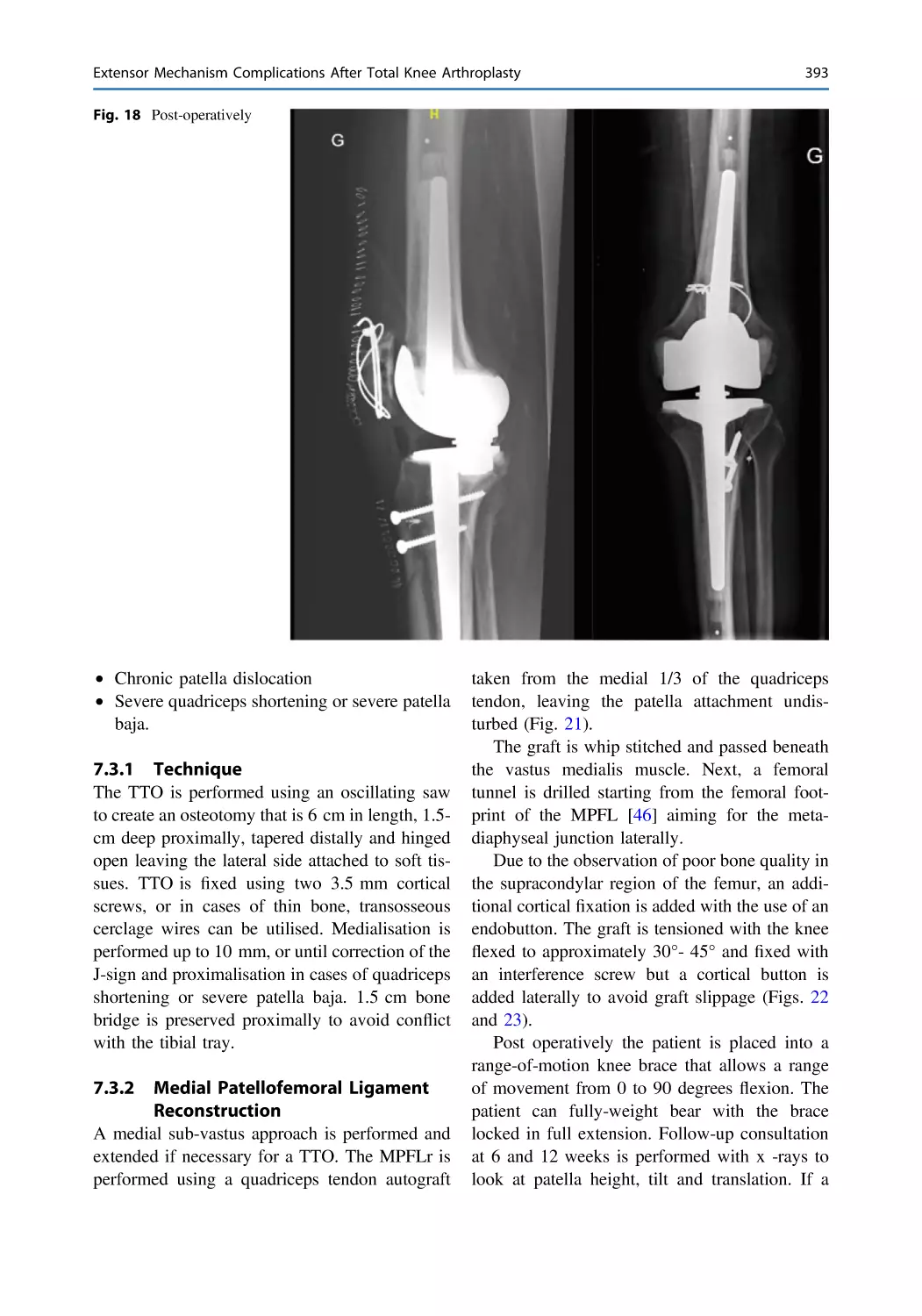
Extensor Mechanism Complications After Total Knee
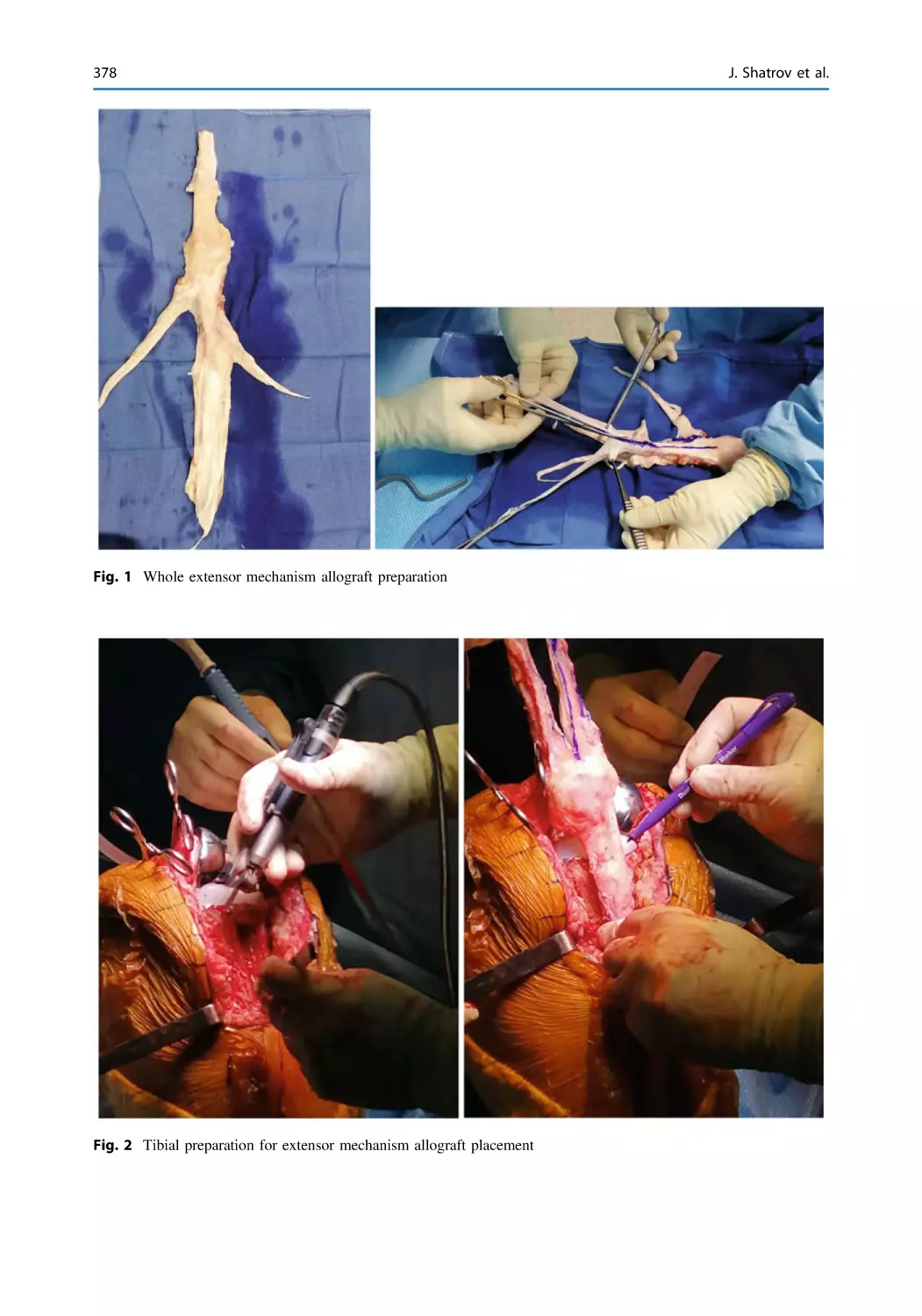
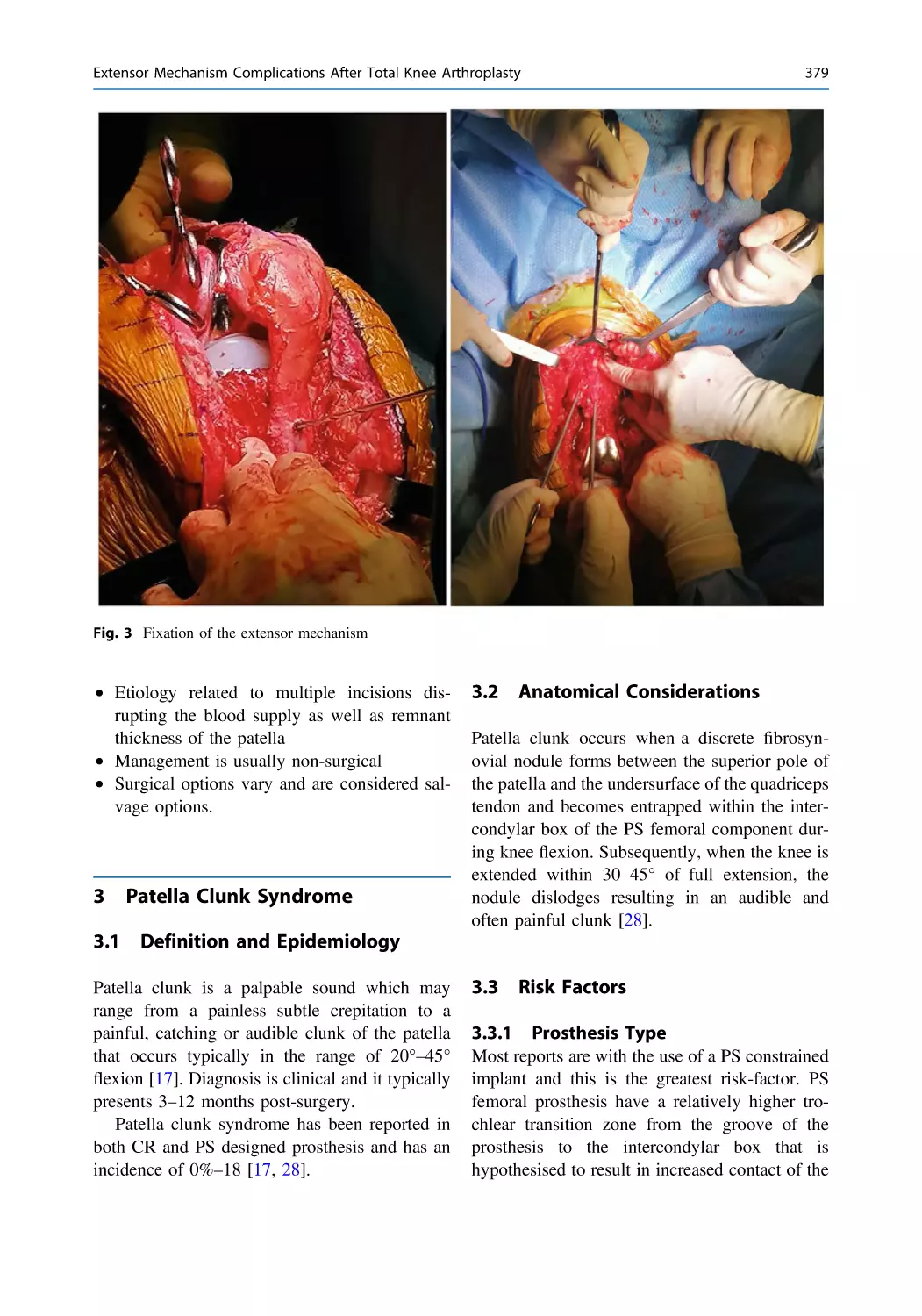
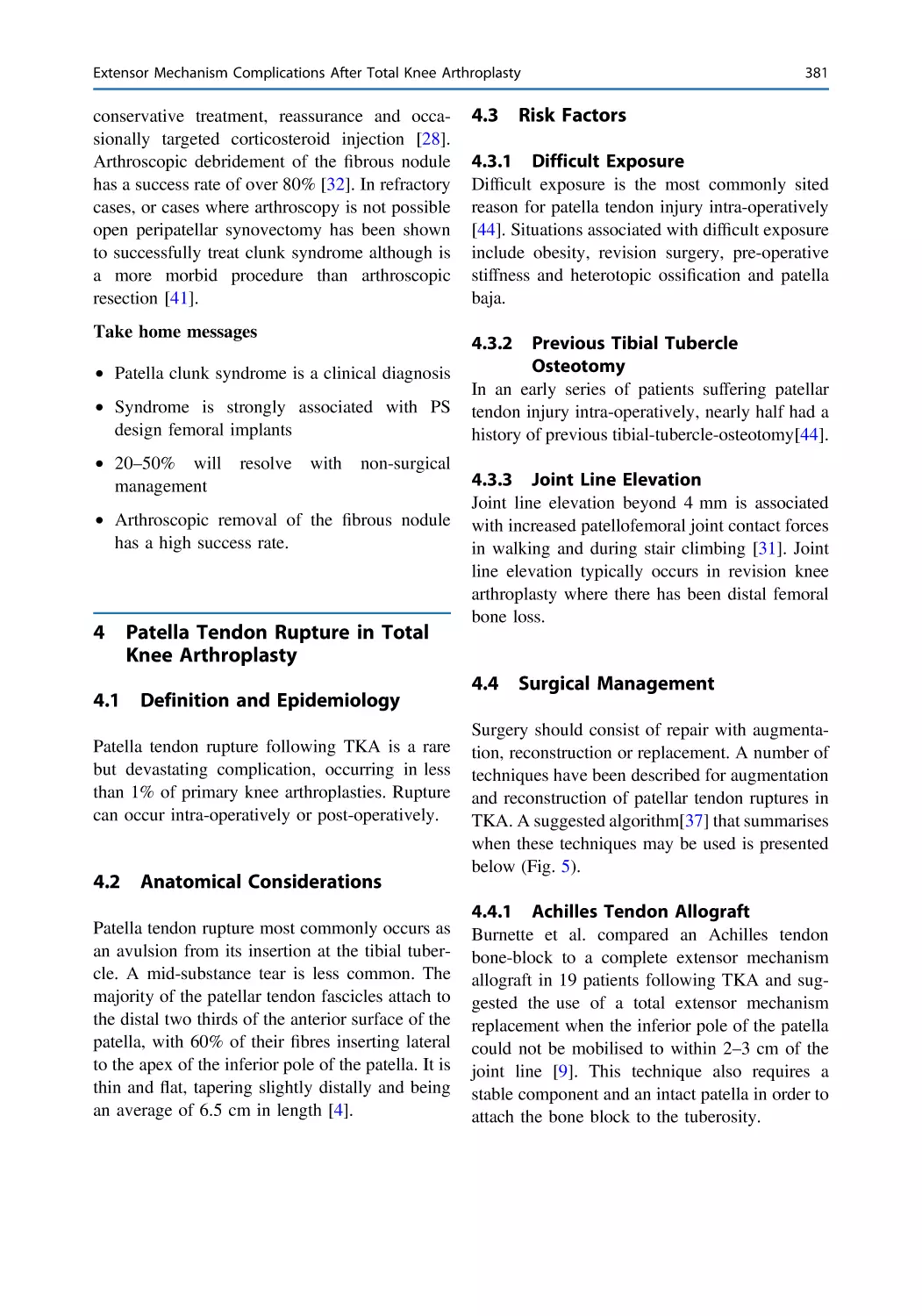
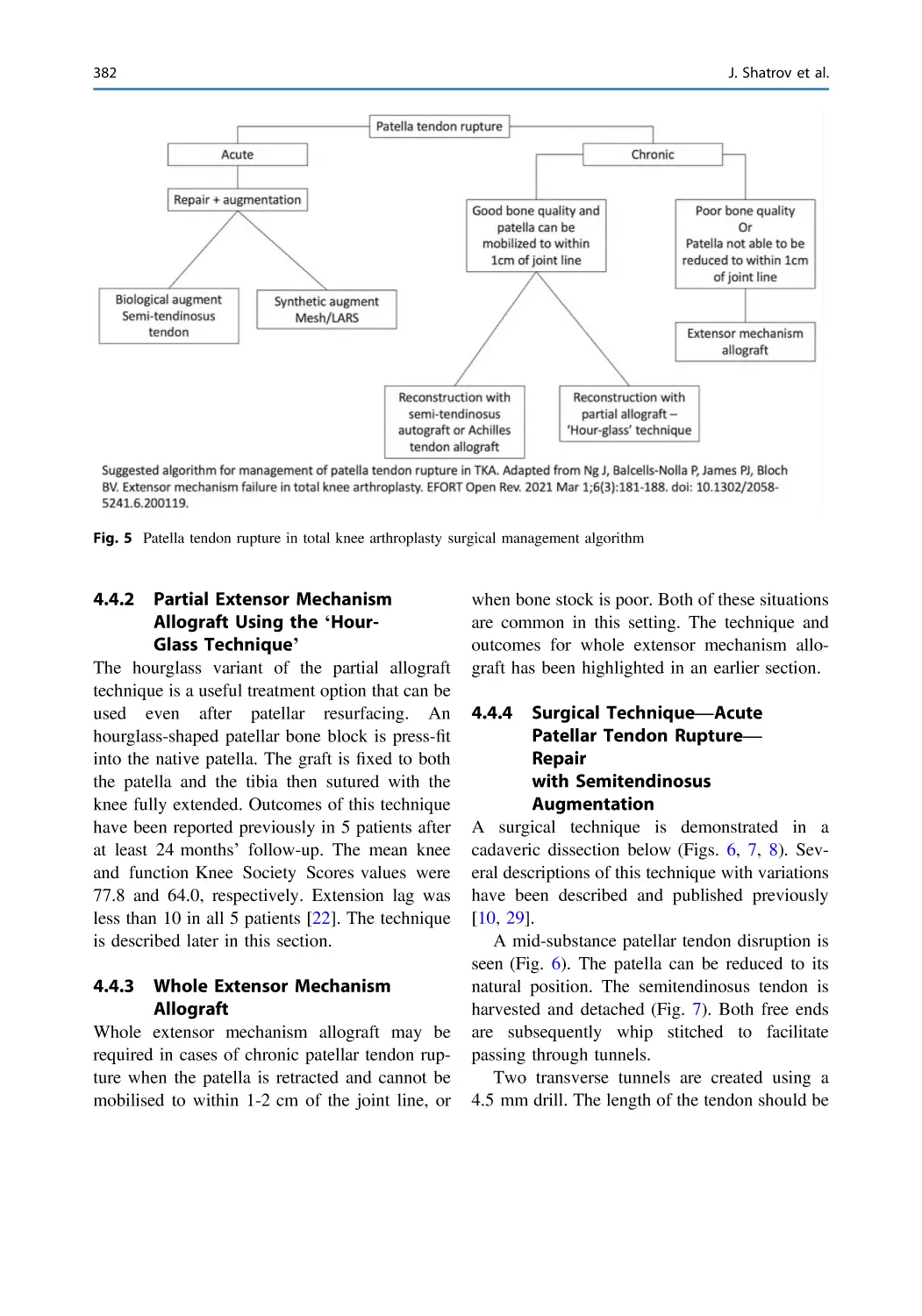
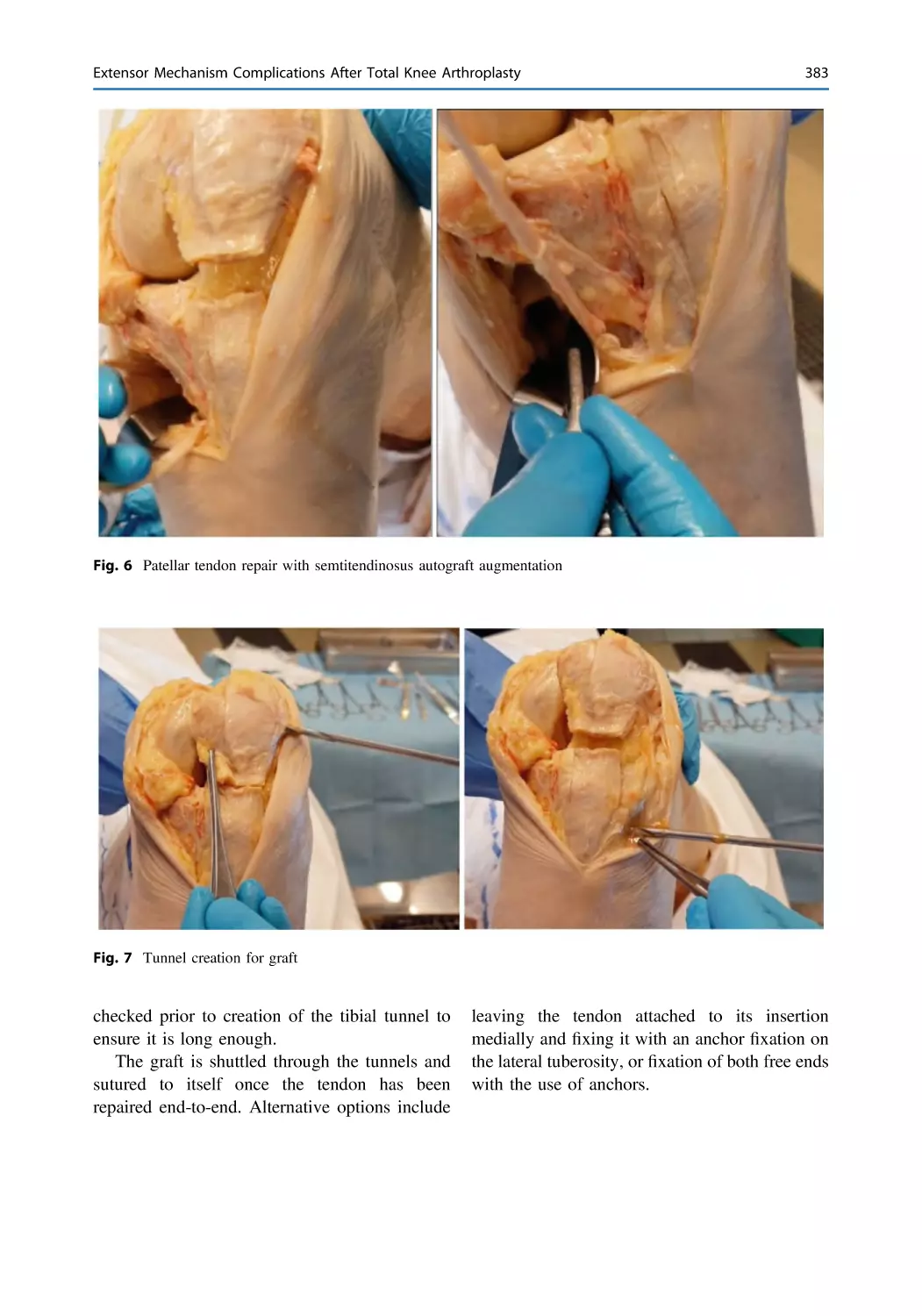
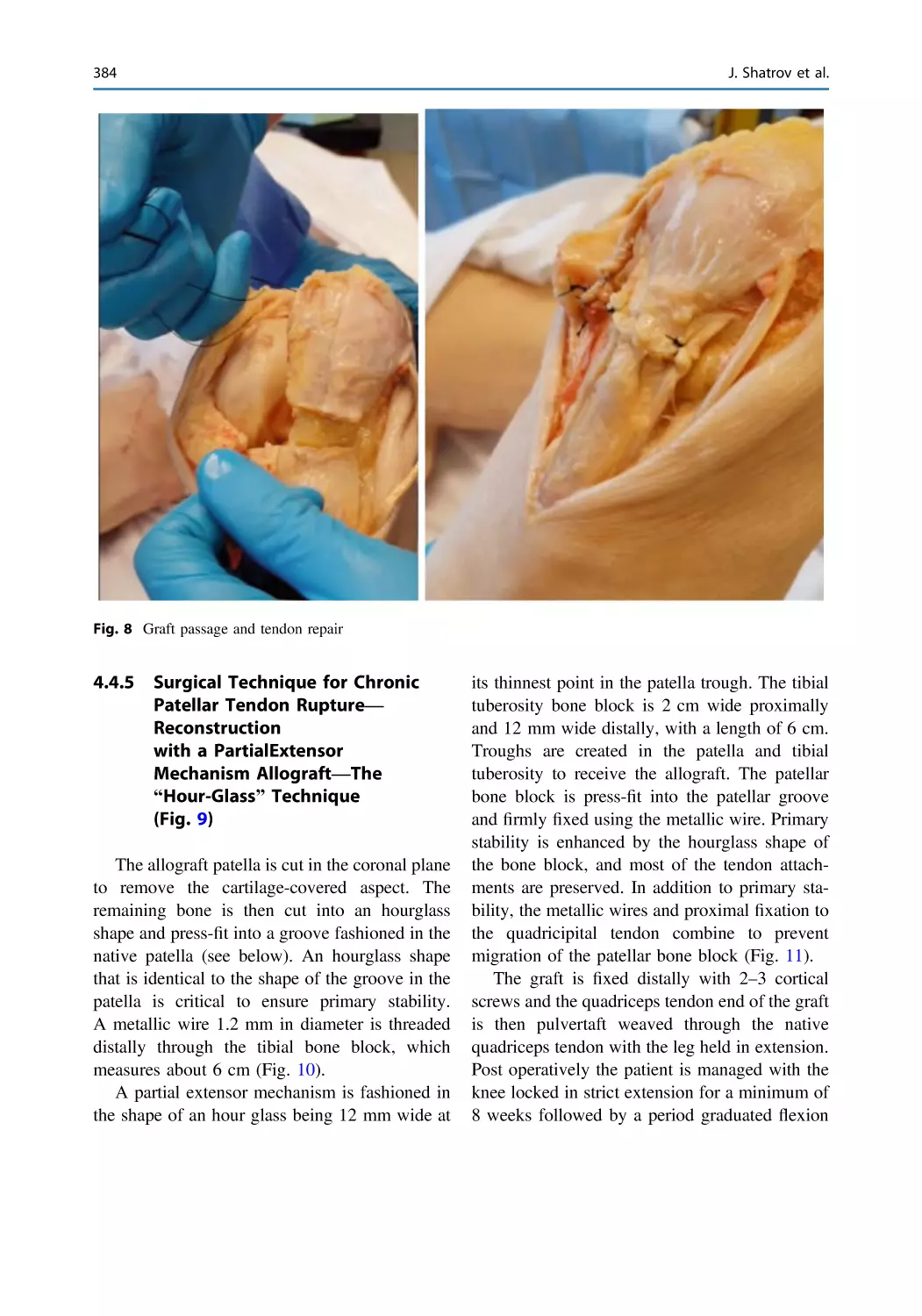
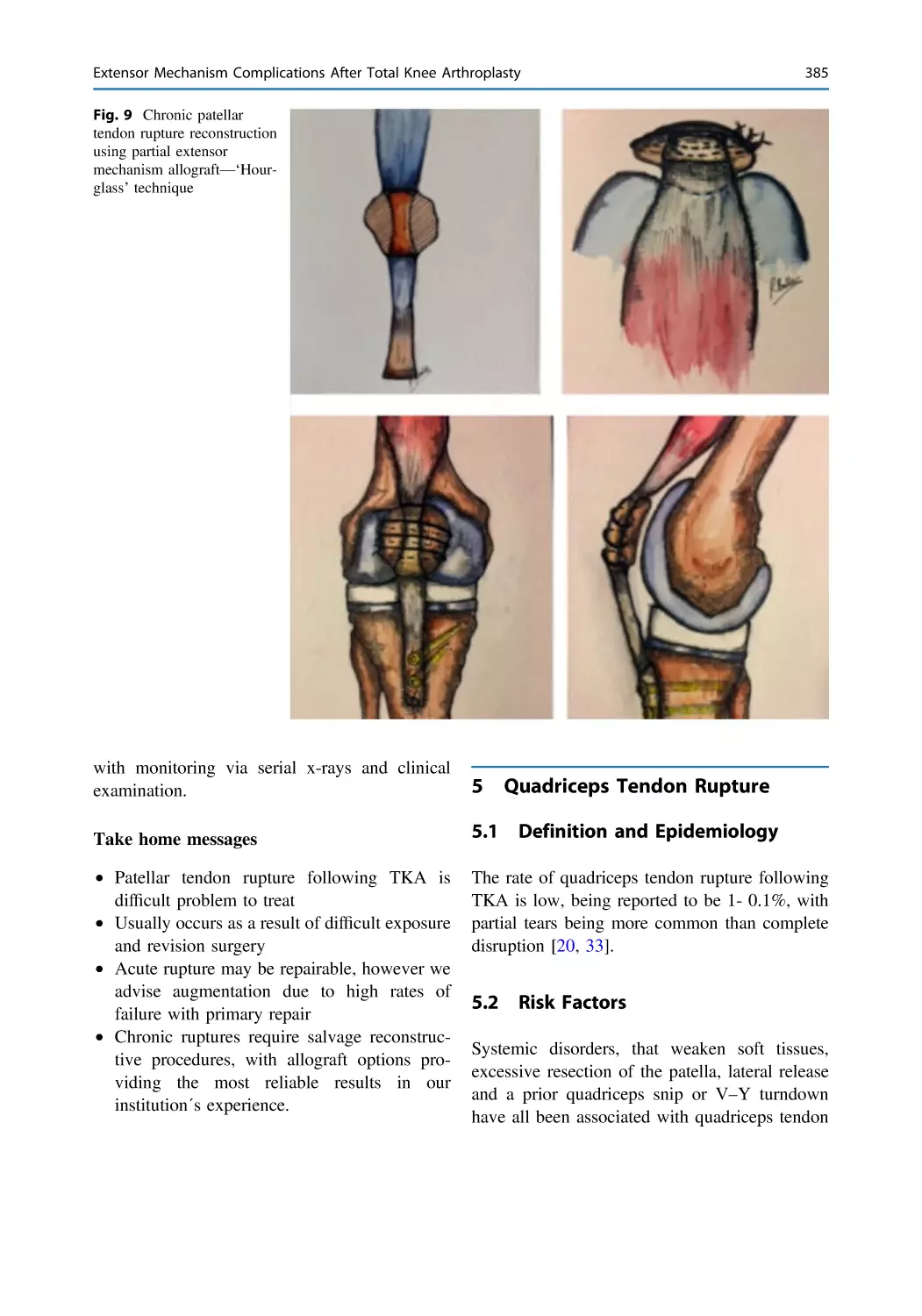
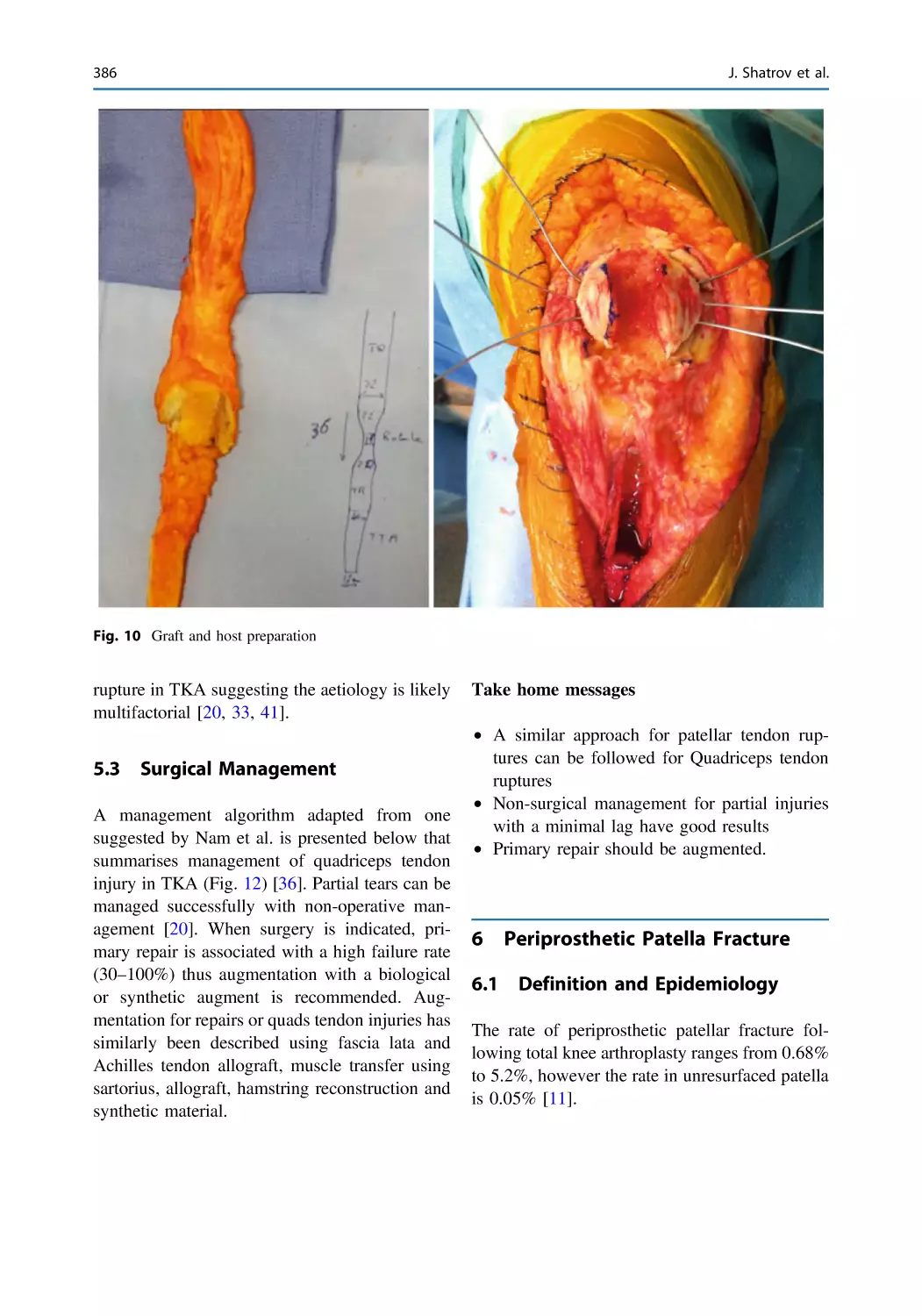
Arthroplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 375
Jobe Shatrov, Cécile Batailler, Gaspard Fournier, Elvire Servien,
and Sebastien Lustig
Surgical Techniques: Why, When and How I Do It
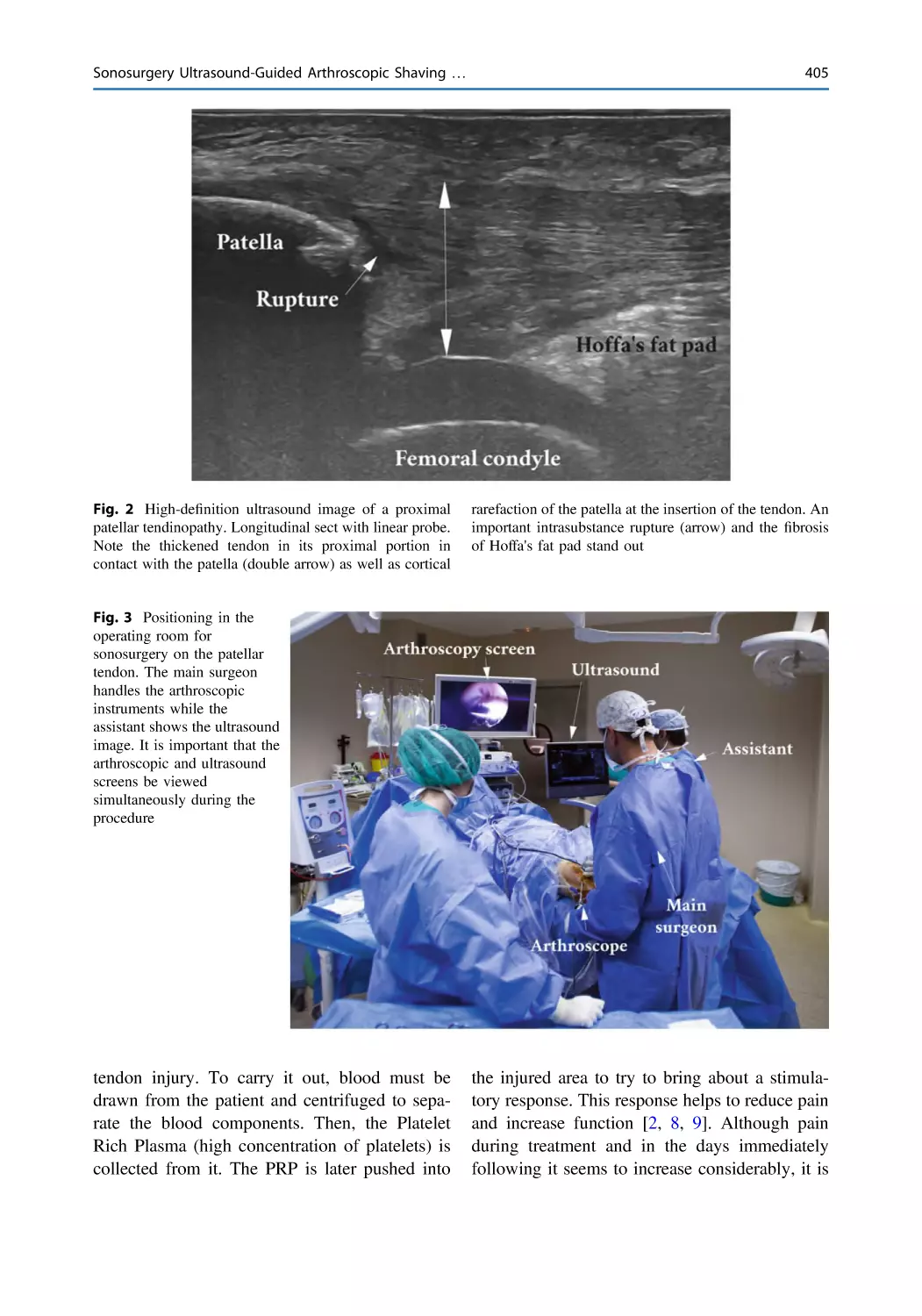
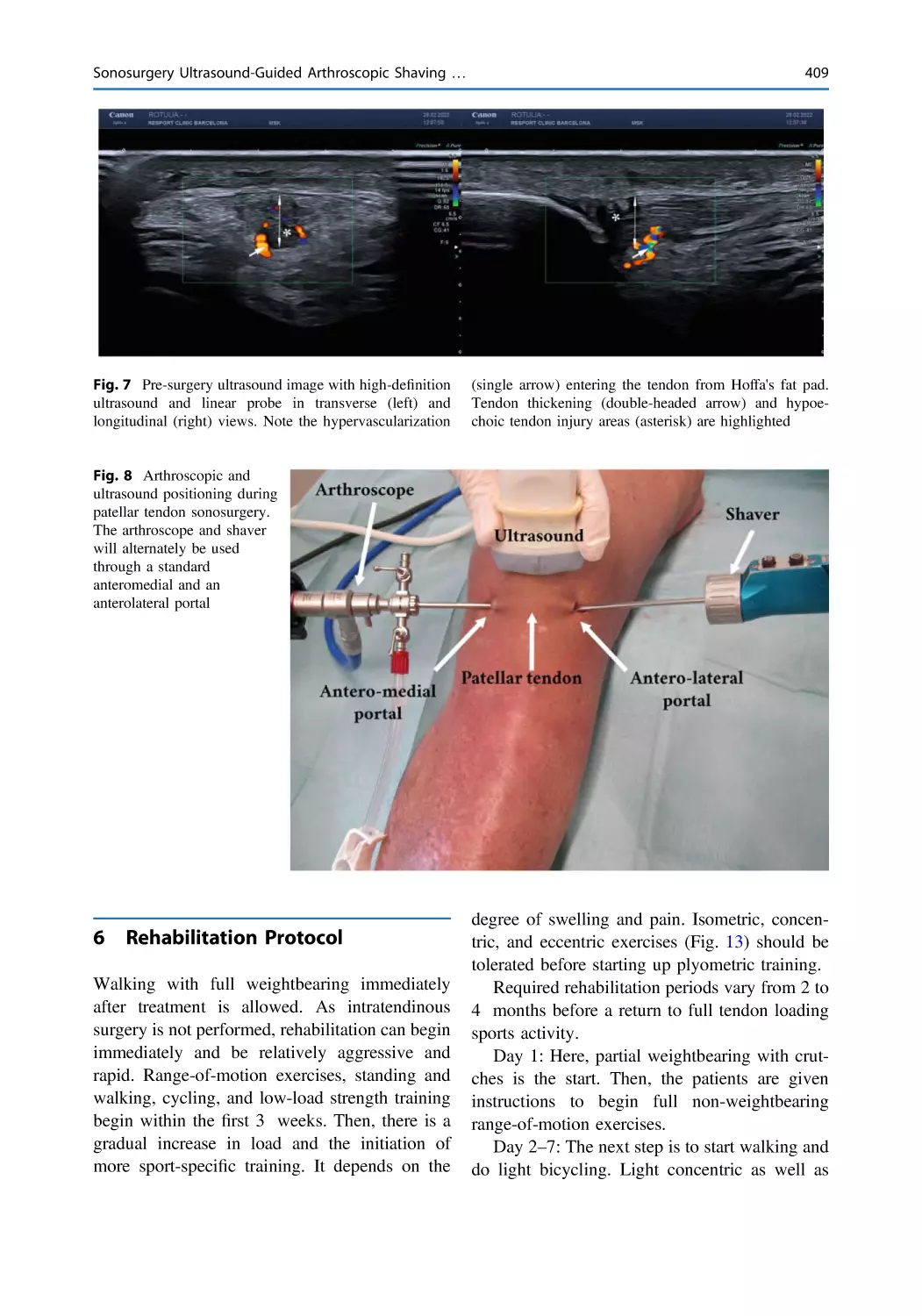
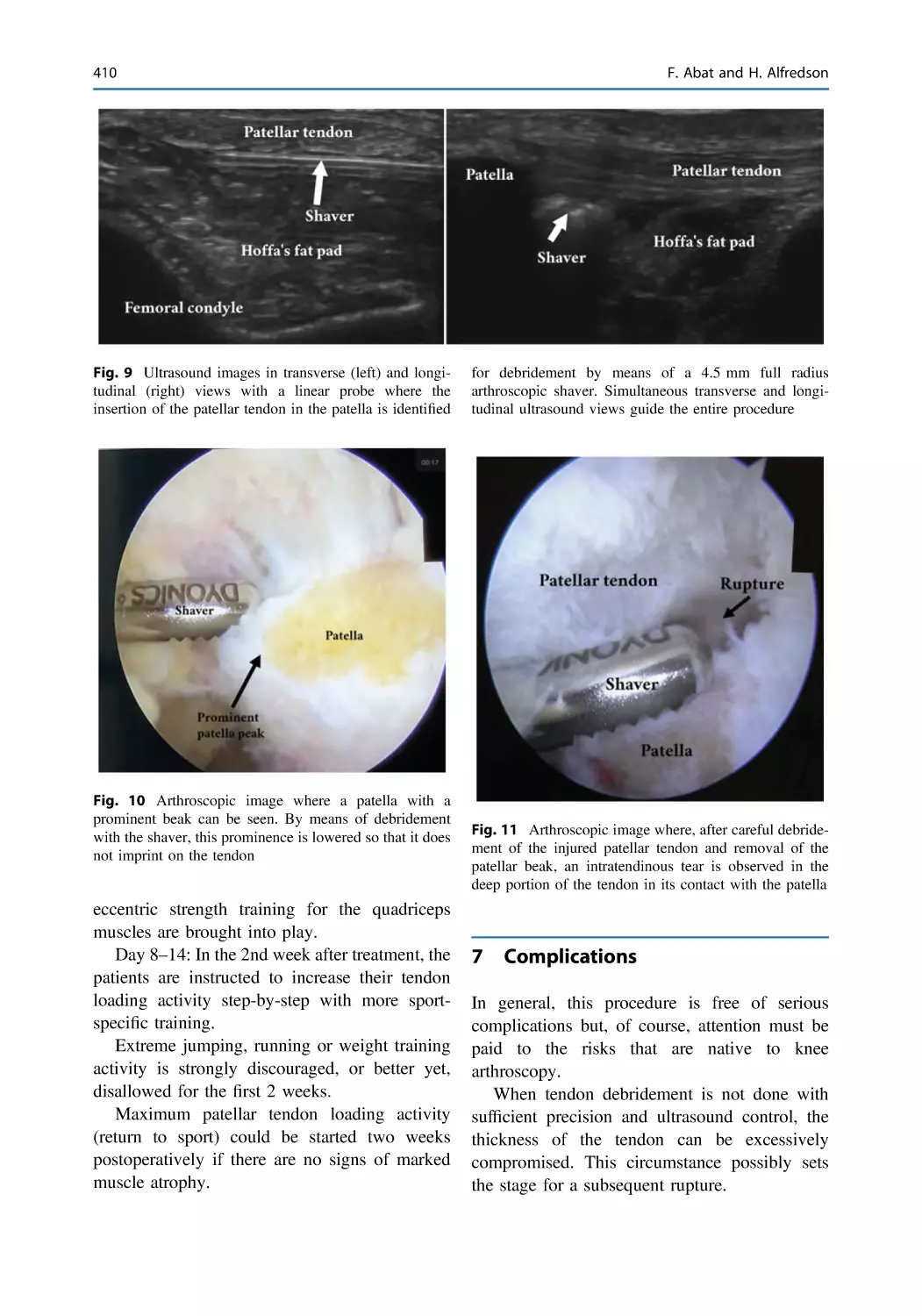
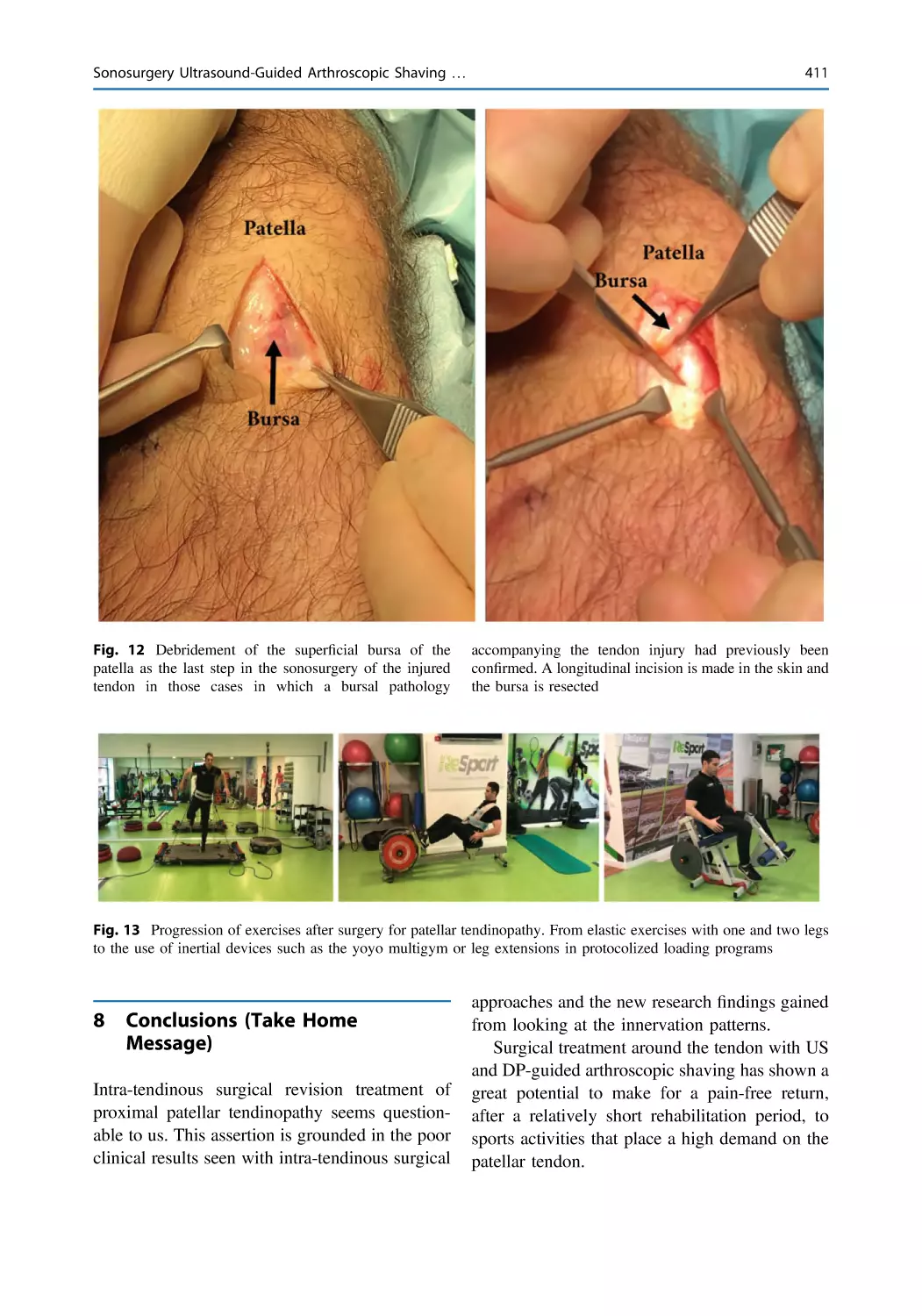
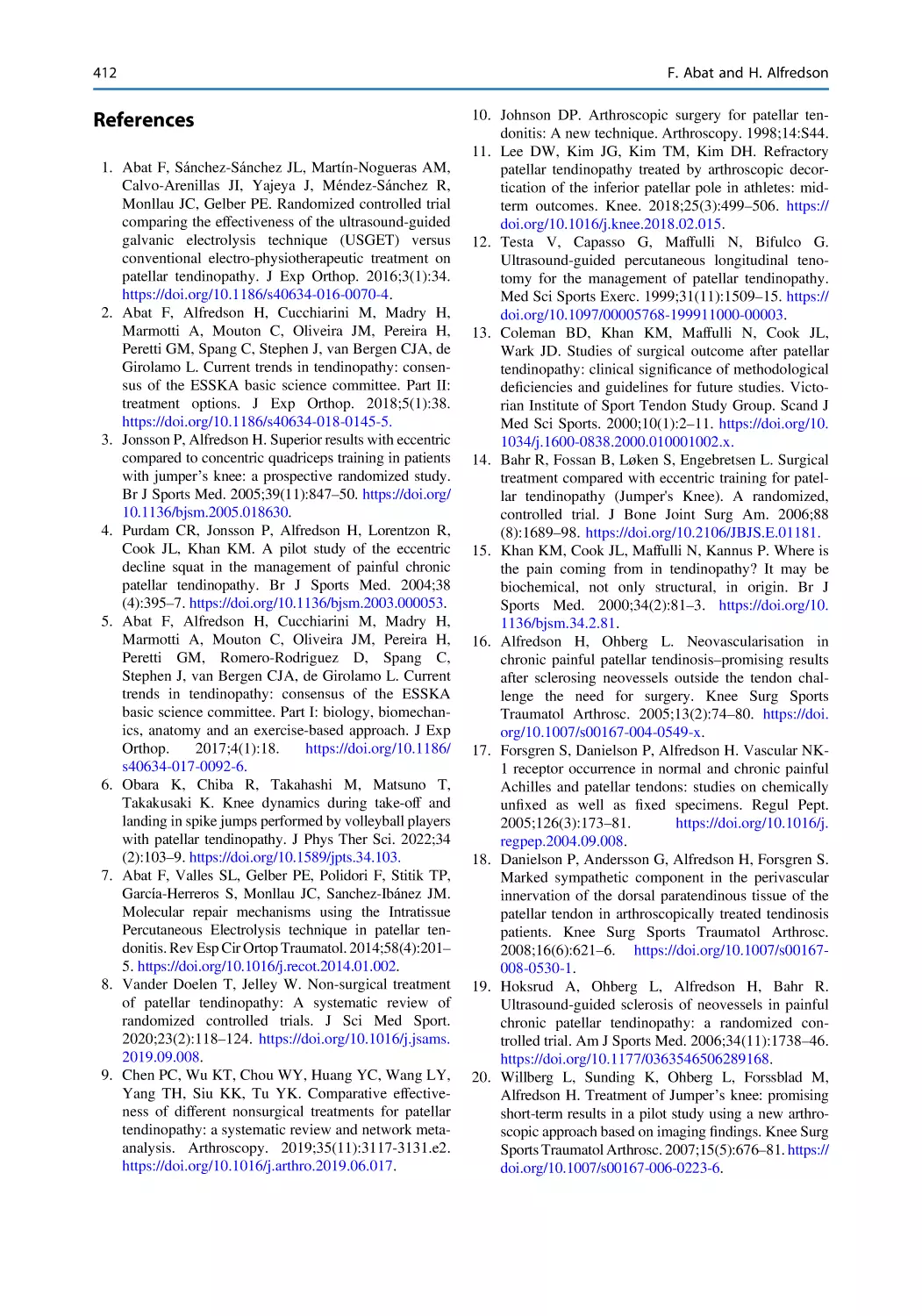
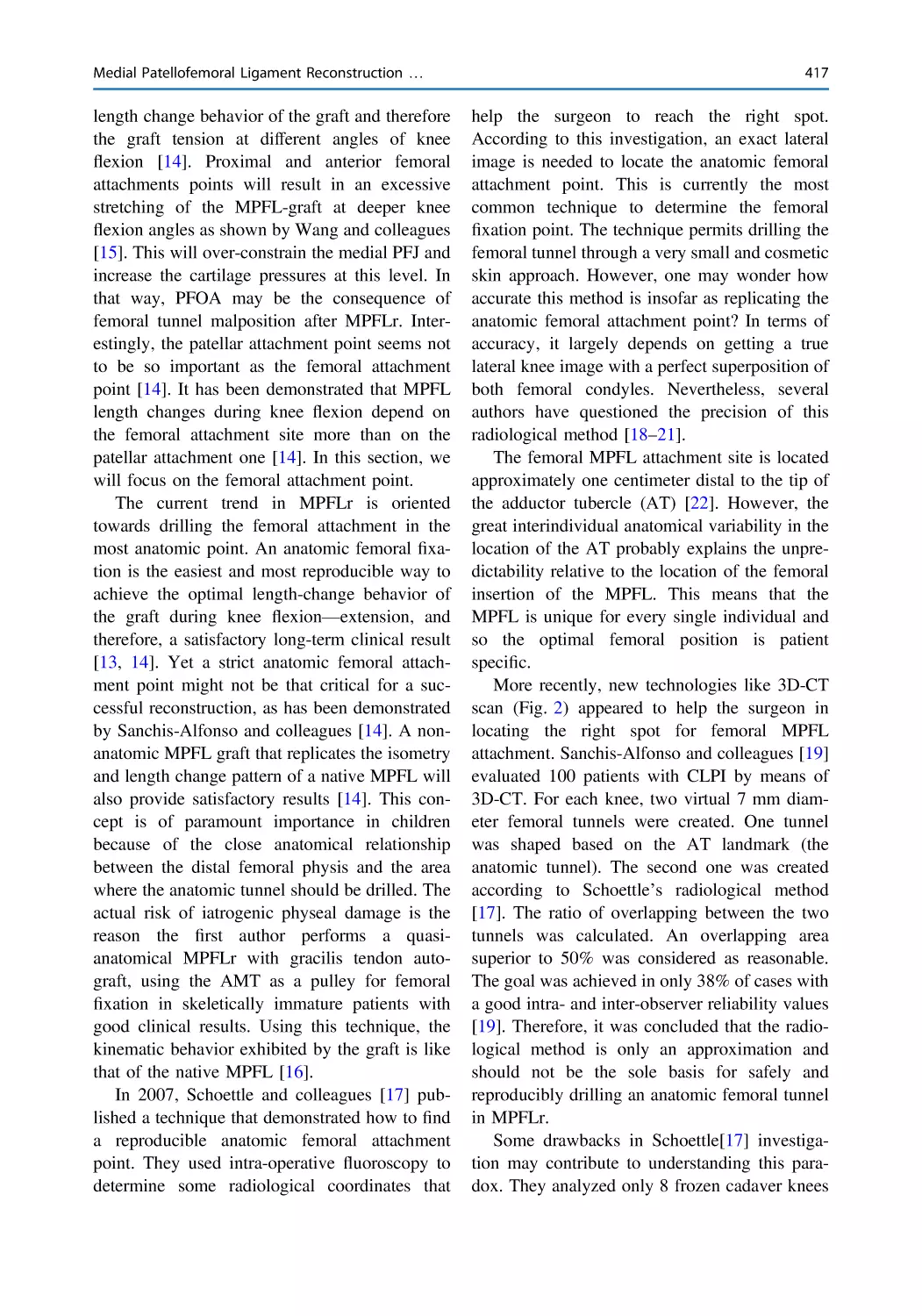
Sonosurgery Ultrasound-Guided Arthroscopic Shaving
for the Treatment of Patellar Tendinopathy When
Conservative Treatment Fails . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 403
Ferran Abat and Håkan Alfredson
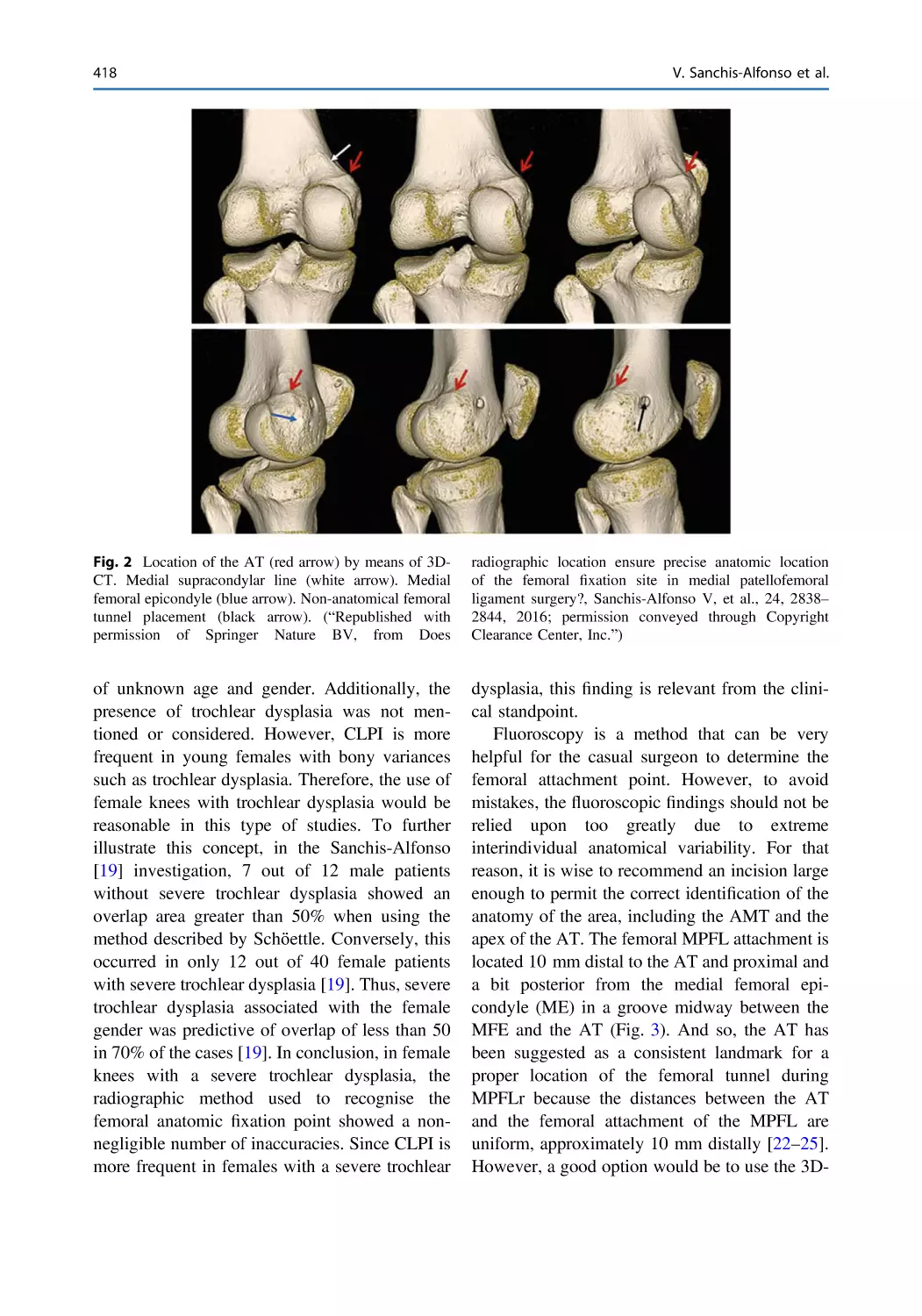
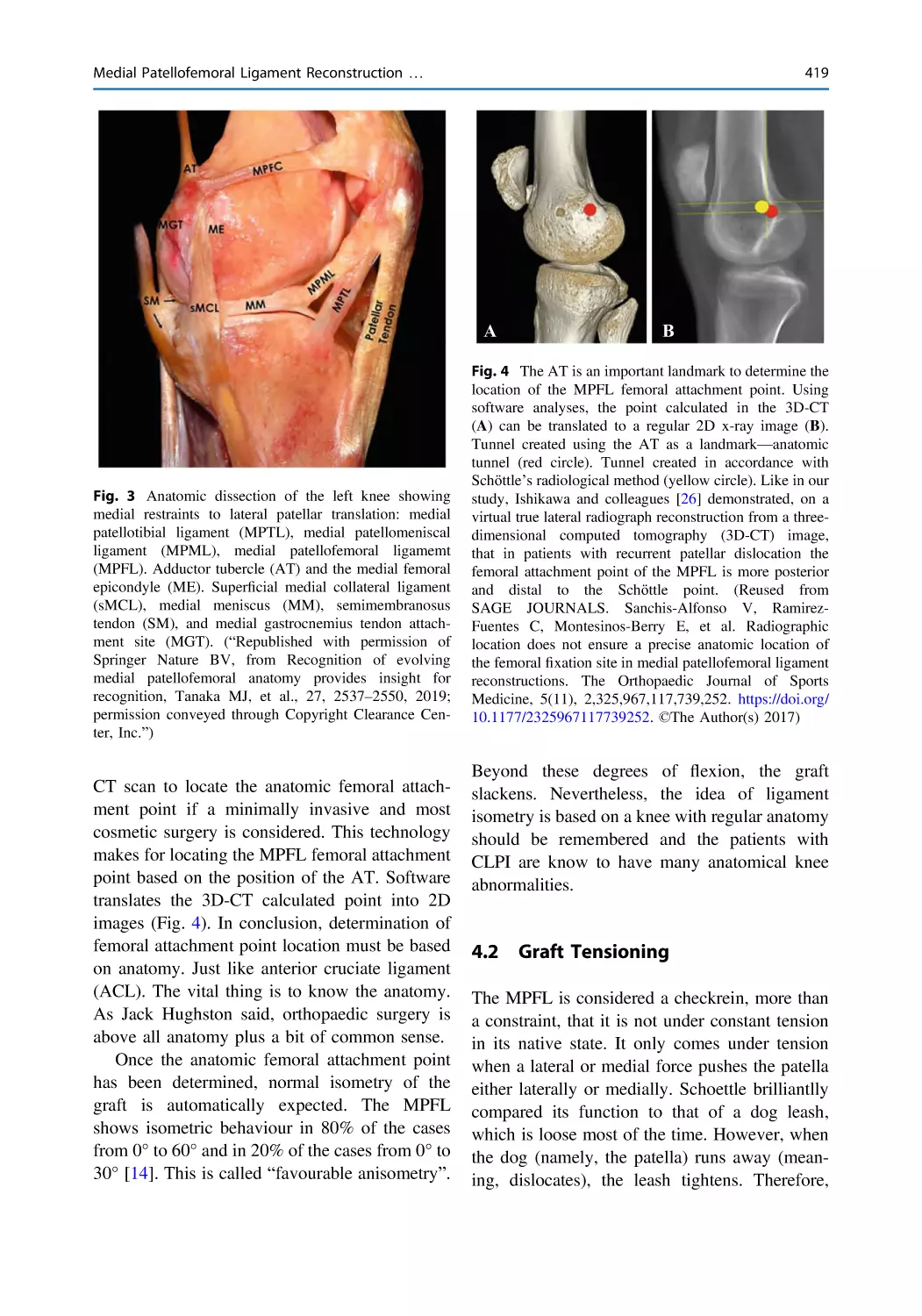
Medial Patellofemoral Ligament Reconstruction: Anatomical
Versus Quasi-anatomical Femoral Fixation . . . . . . . . . . . . . . . . . . . 415
Vicente Sanchis-Alfonso, Maximiliano Ibañez,
Cristina Ramirez-Fuentes, and Joan Carles Monllau
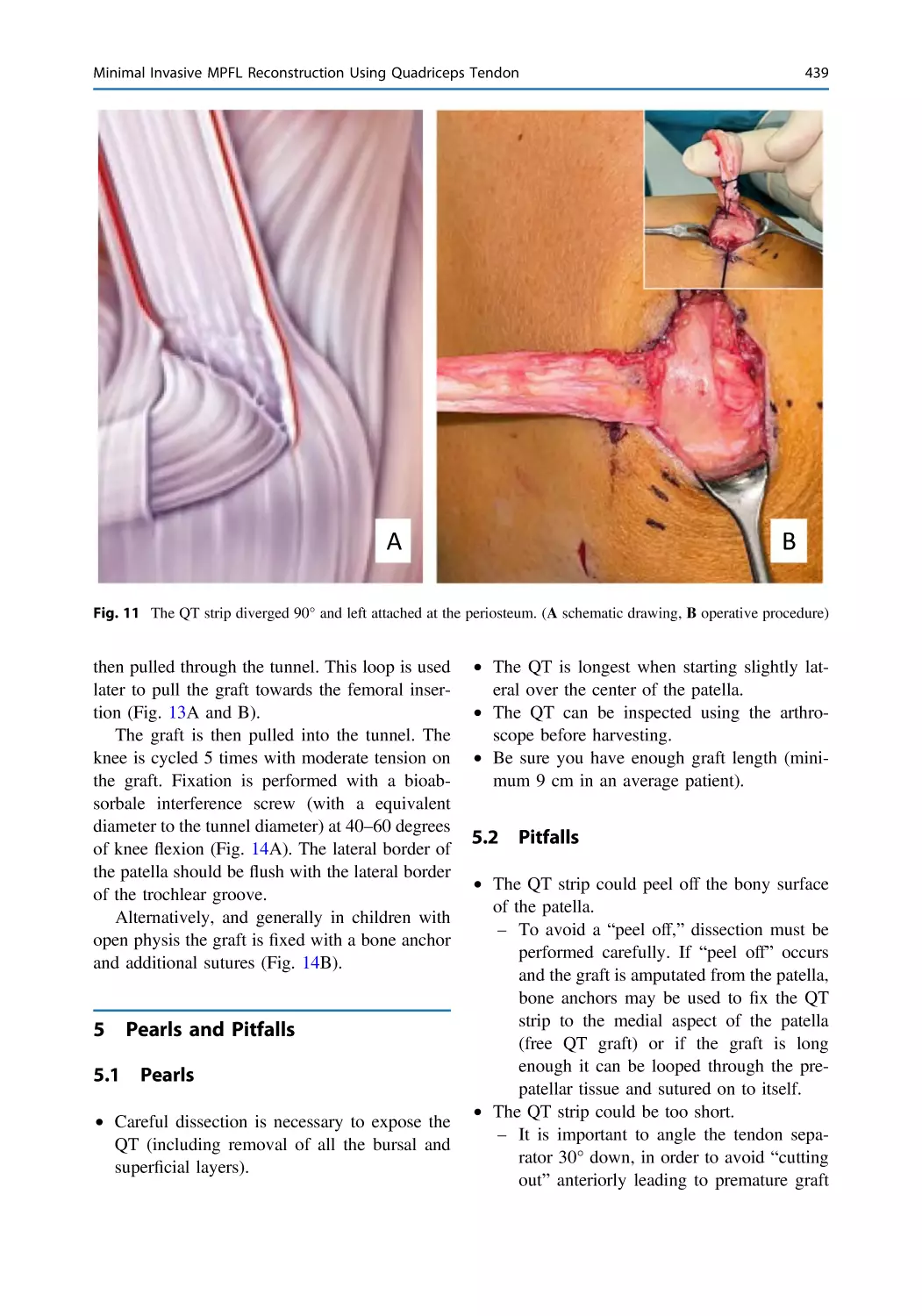
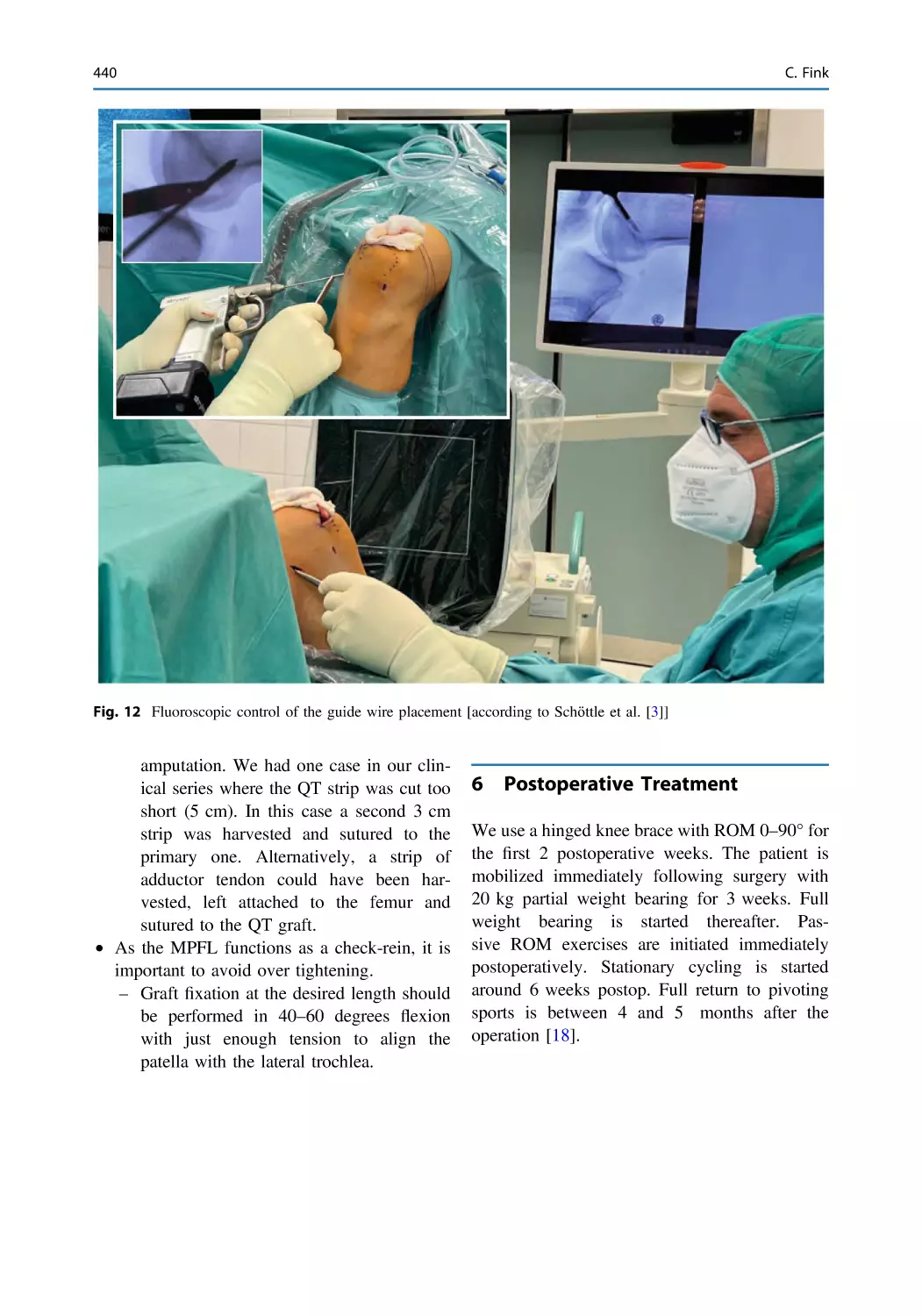
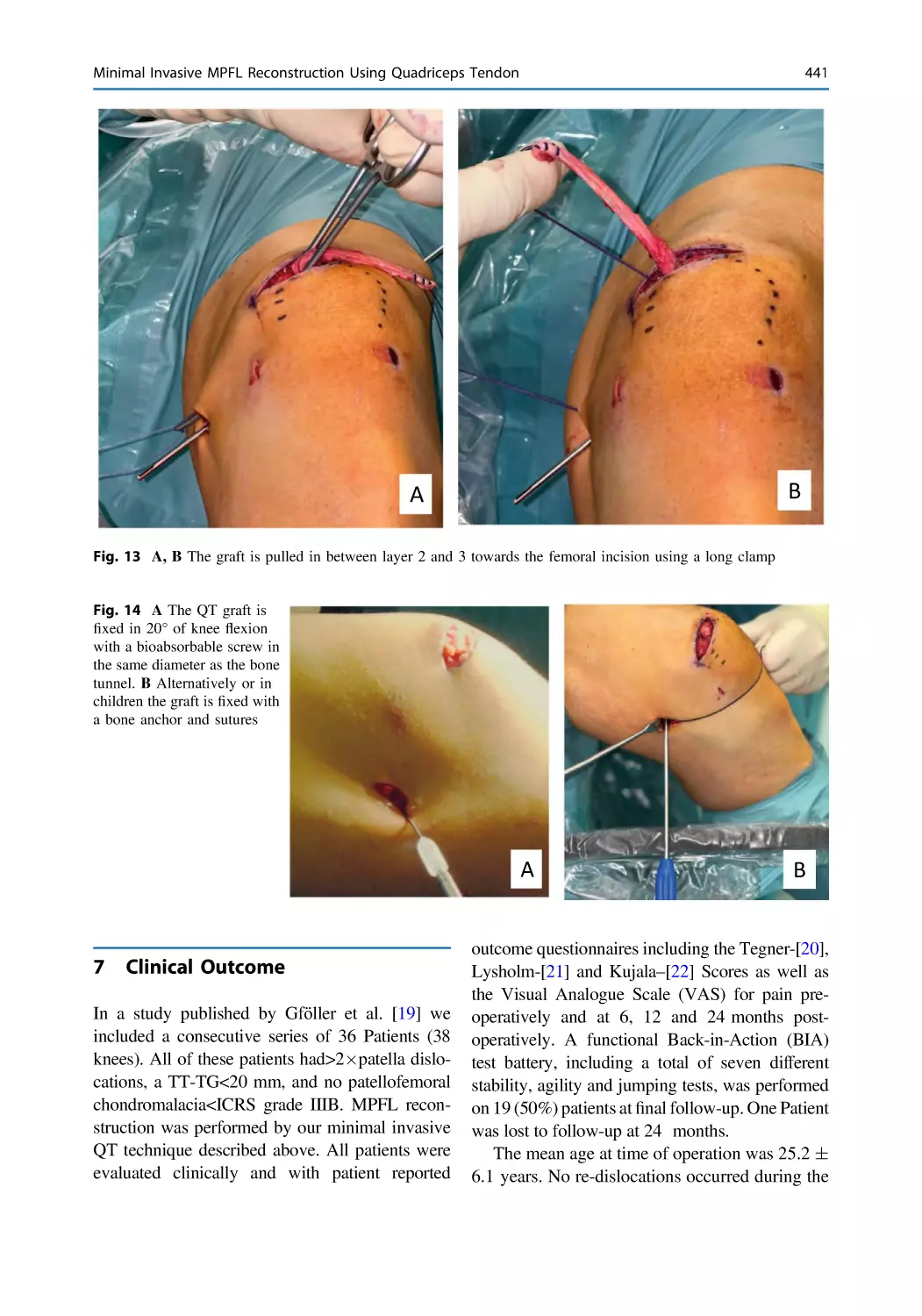
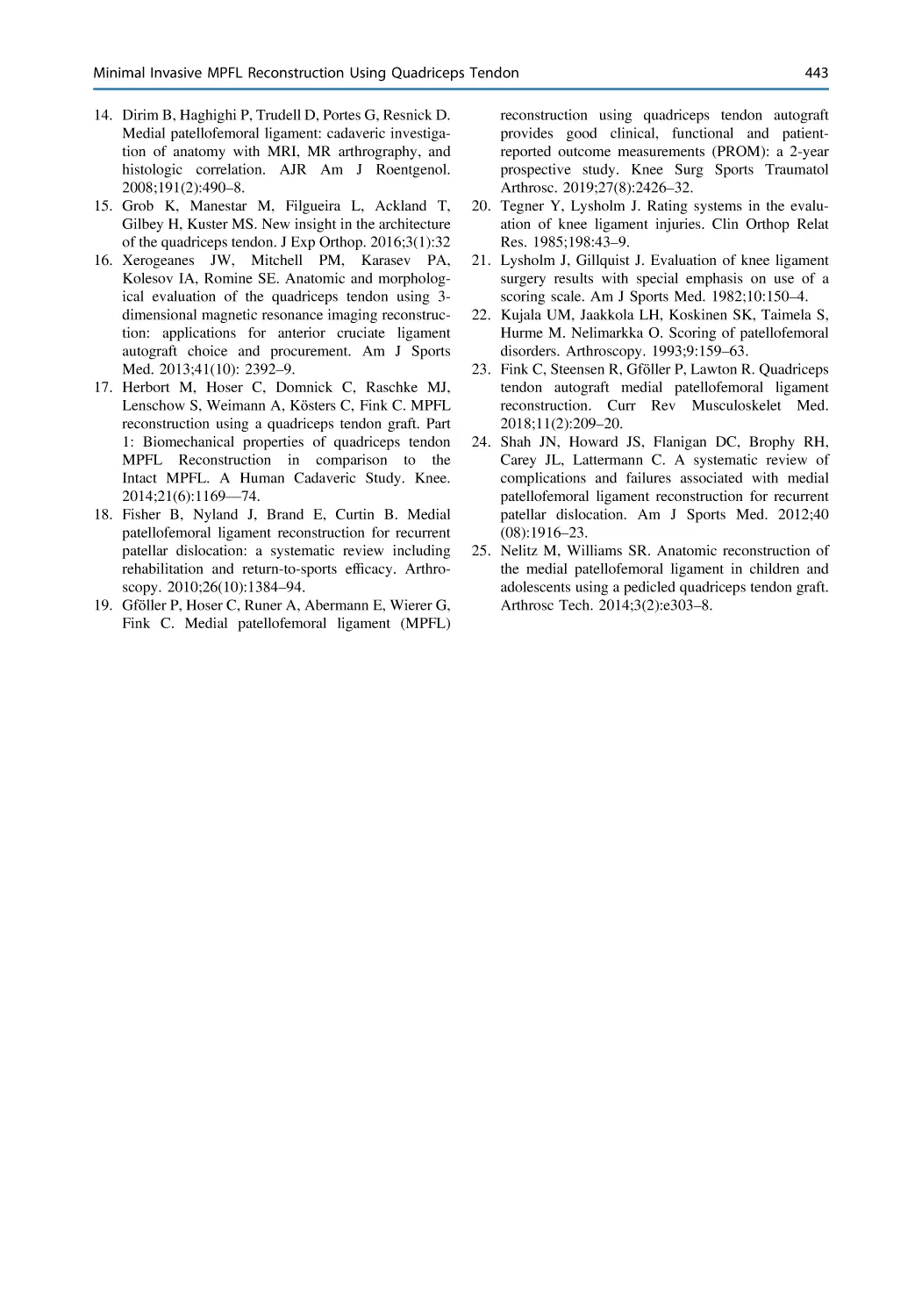
Minimal Invasive MPFL Reconstruction Using Quadriceps
Tendon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 431
Christian Fink
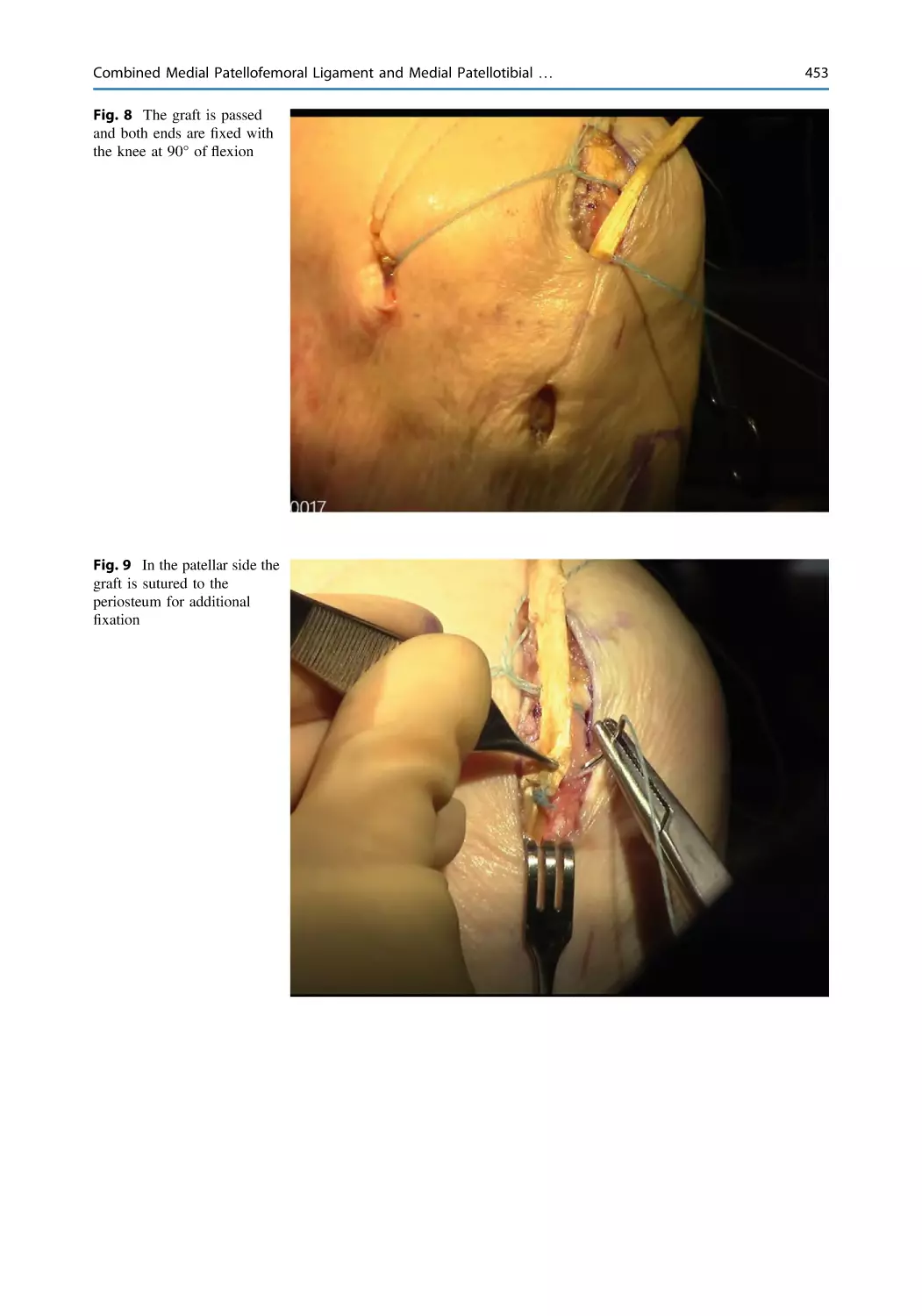
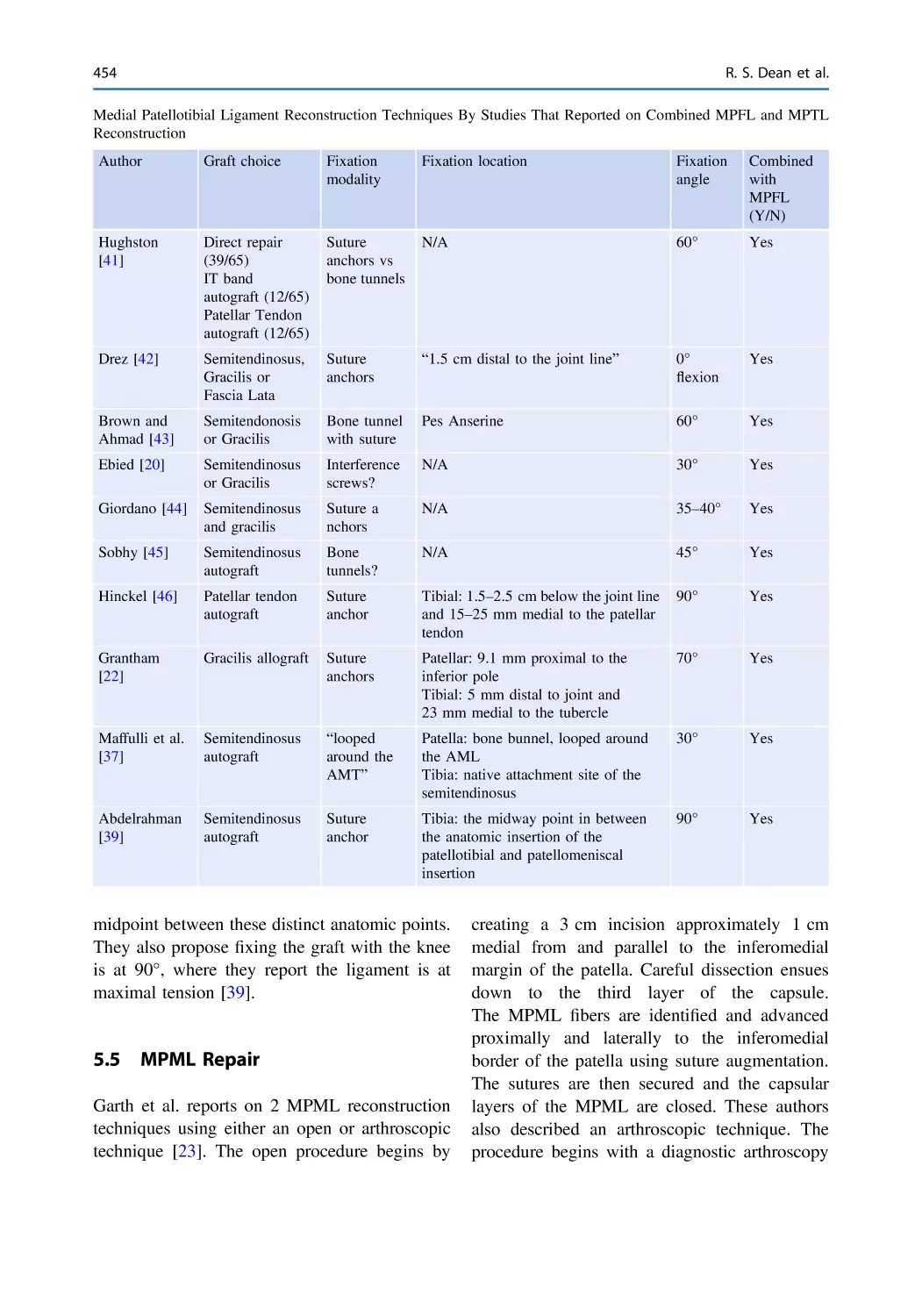
Combined Medial Patellofemoral Ligament and Medial
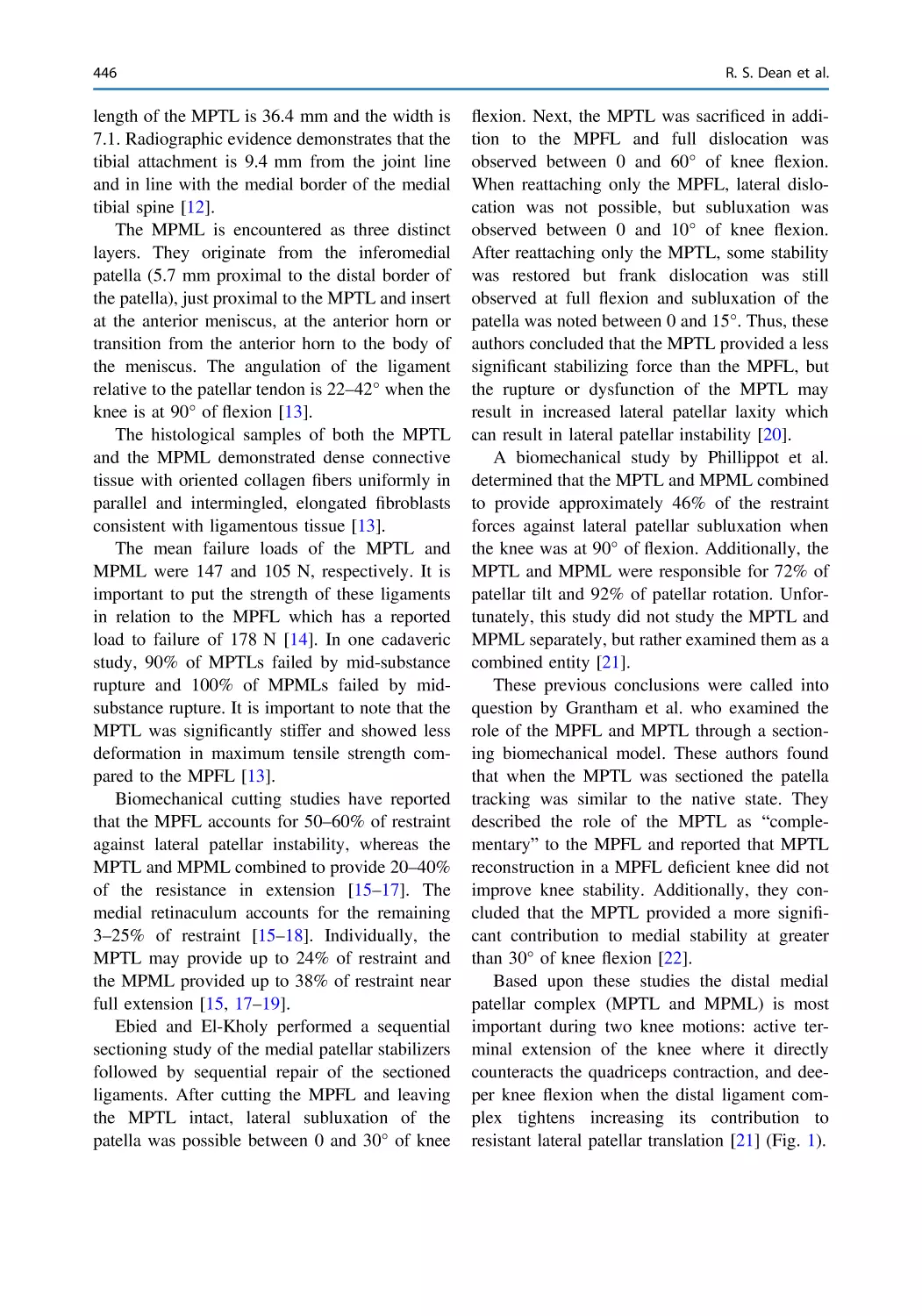
Patellotibial Ligament Reconstruction . . . . . . . . . . . . . . . . . . . . . . . 445
Robert S. Dean, Betina B. Hinckel, and Elizabeth A. Arendt
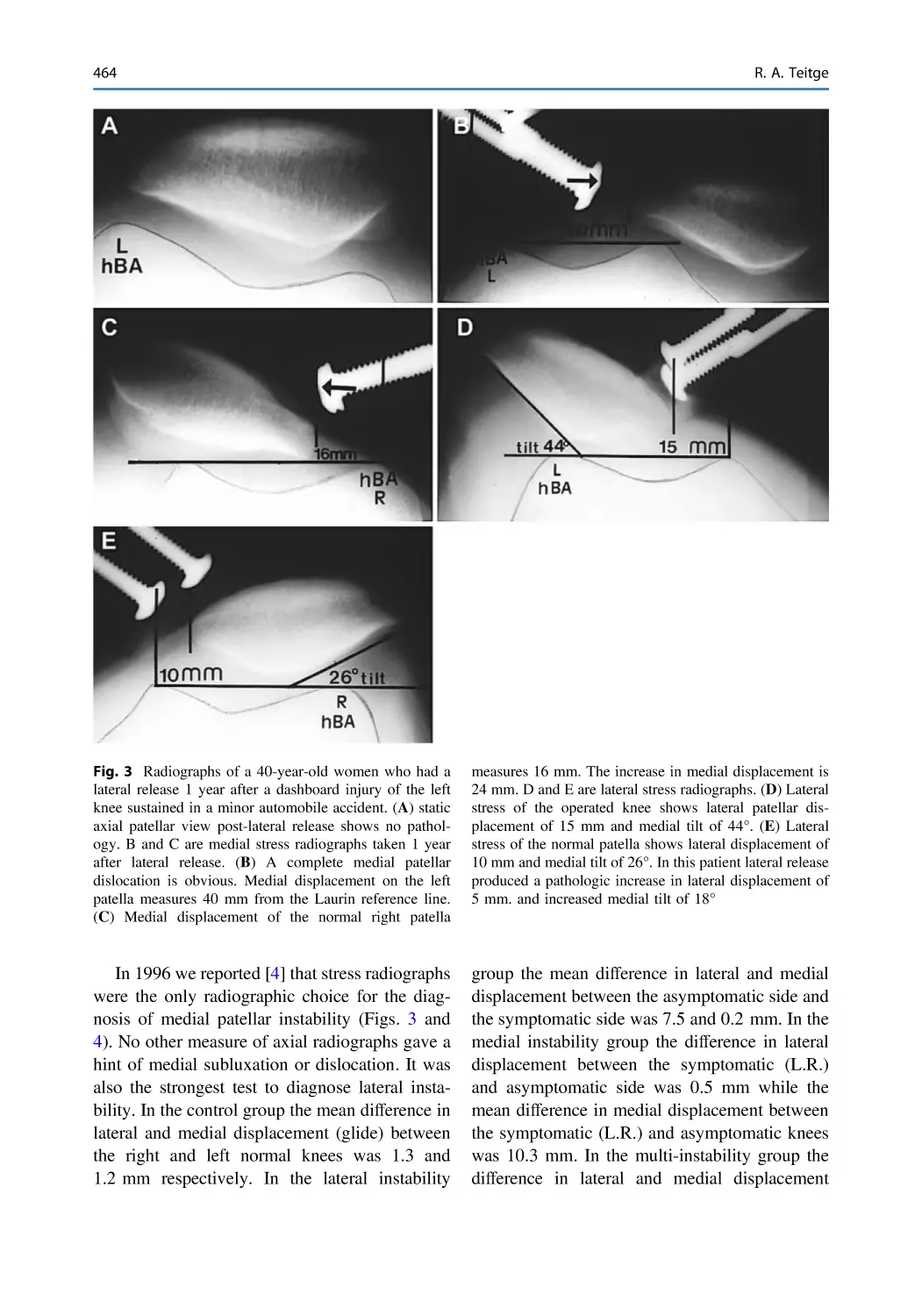
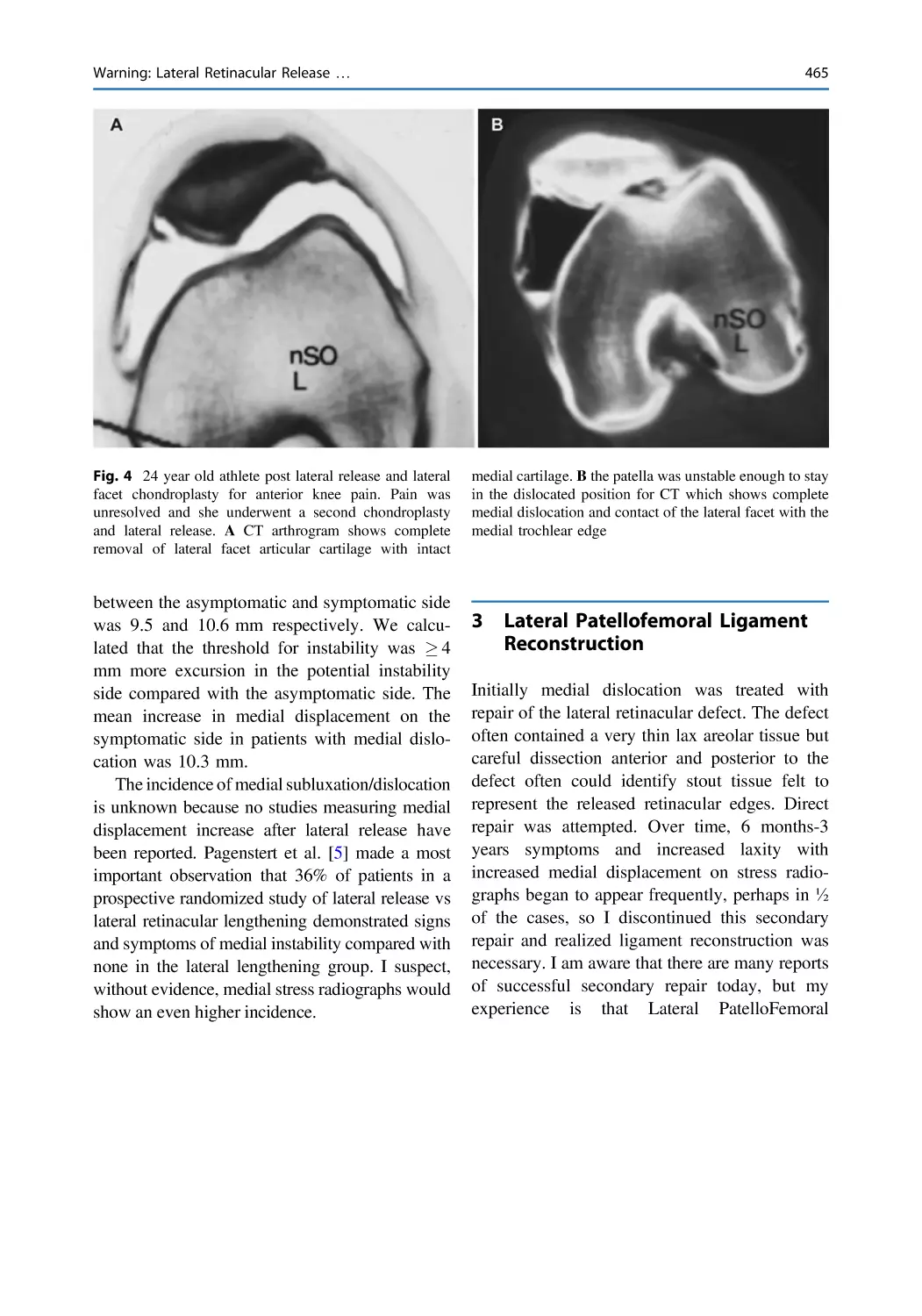
Warning: Lateral Retinacular Release Can Cause Medial
Patellar Dislocation—Lateral Patellofemoral Ligament
Reconstruction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 461
Robert A. Teitge
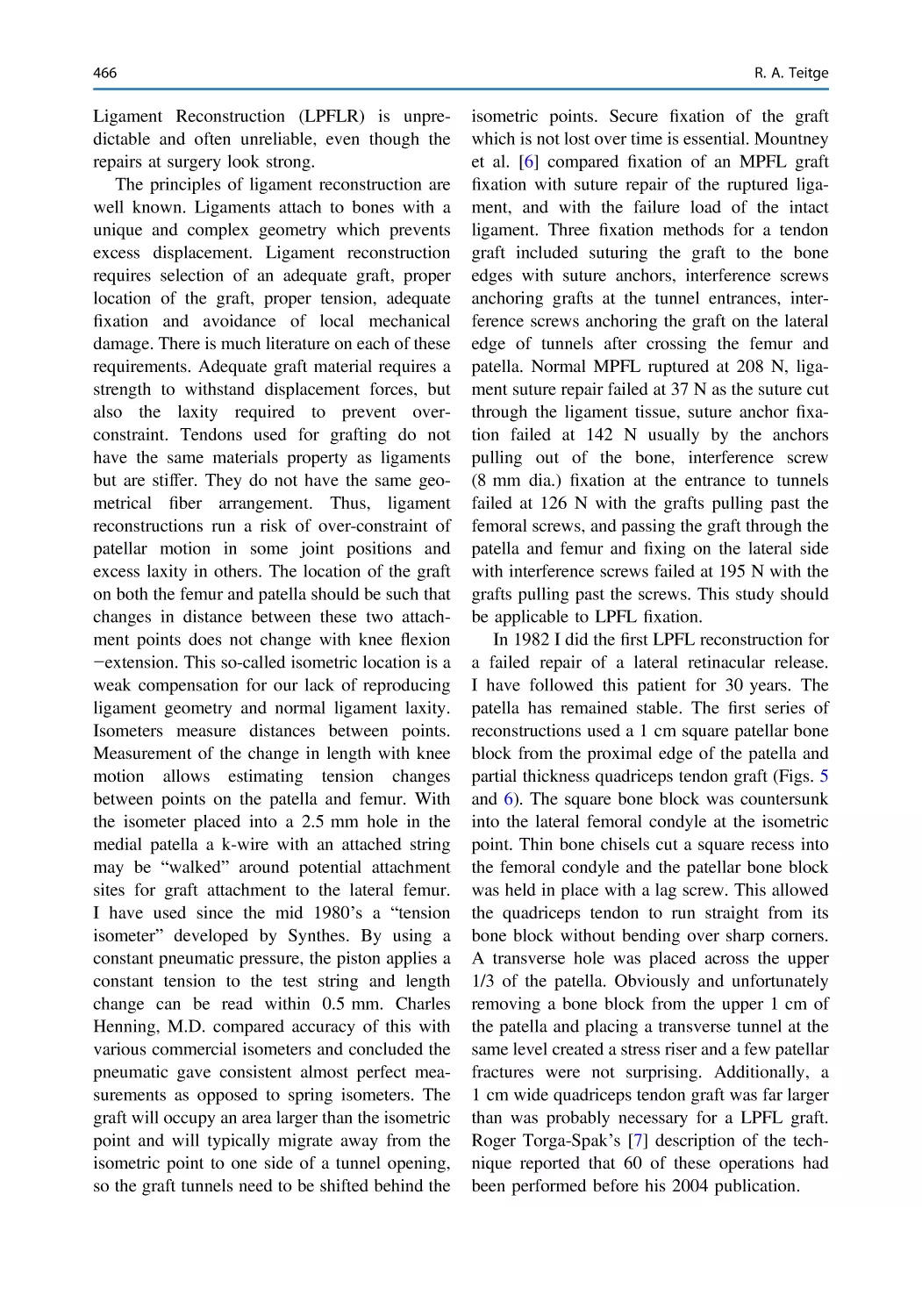
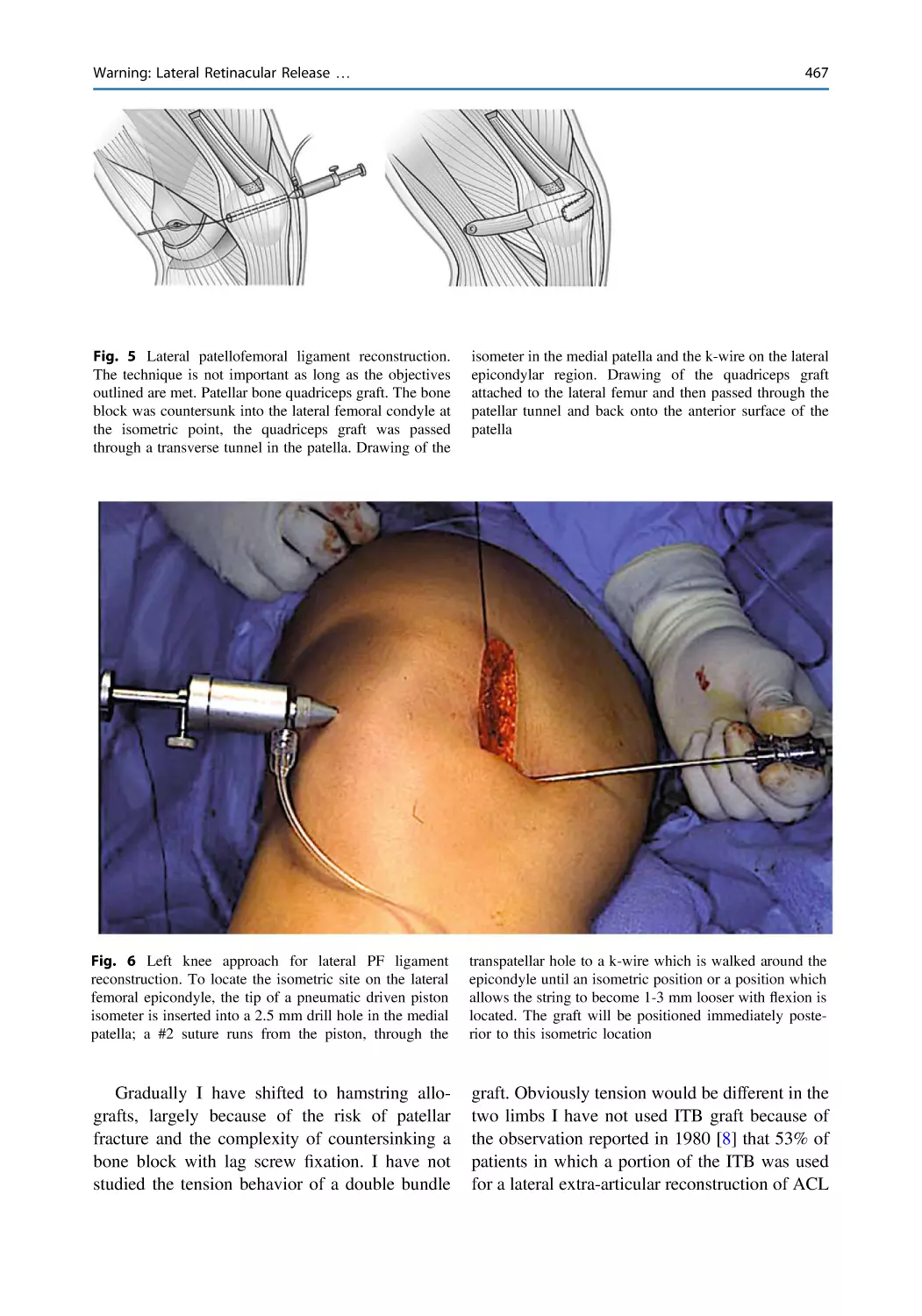
Reconstruction of the Lateral Patellofemoral Ligament . . . . . . . . . 469
David S. Zhu and Lutul D. Farrow
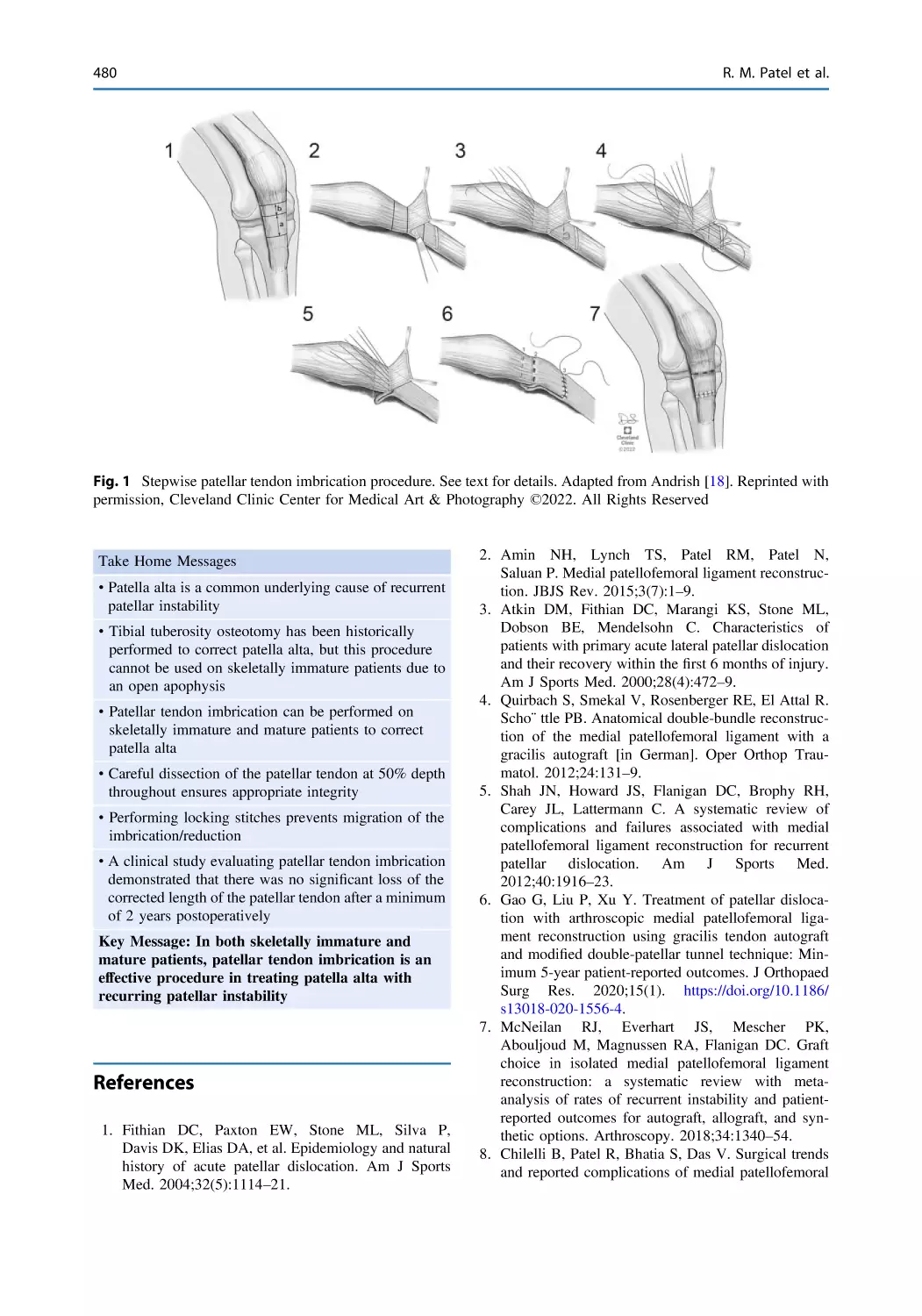
Patellar Tendon Imbrication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 477
Ronak M. Patel, Sneh Patel, and Jack Andrish
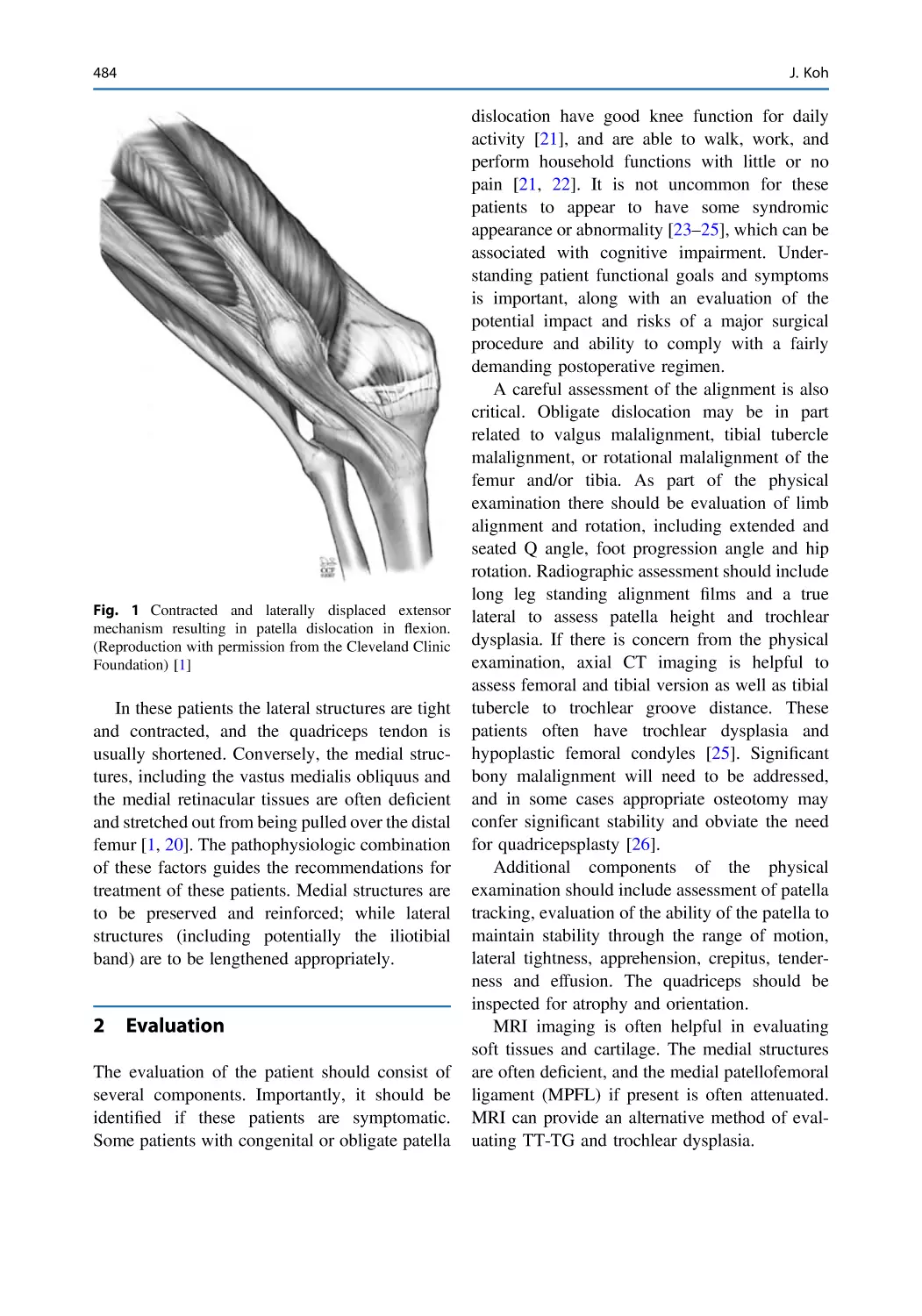
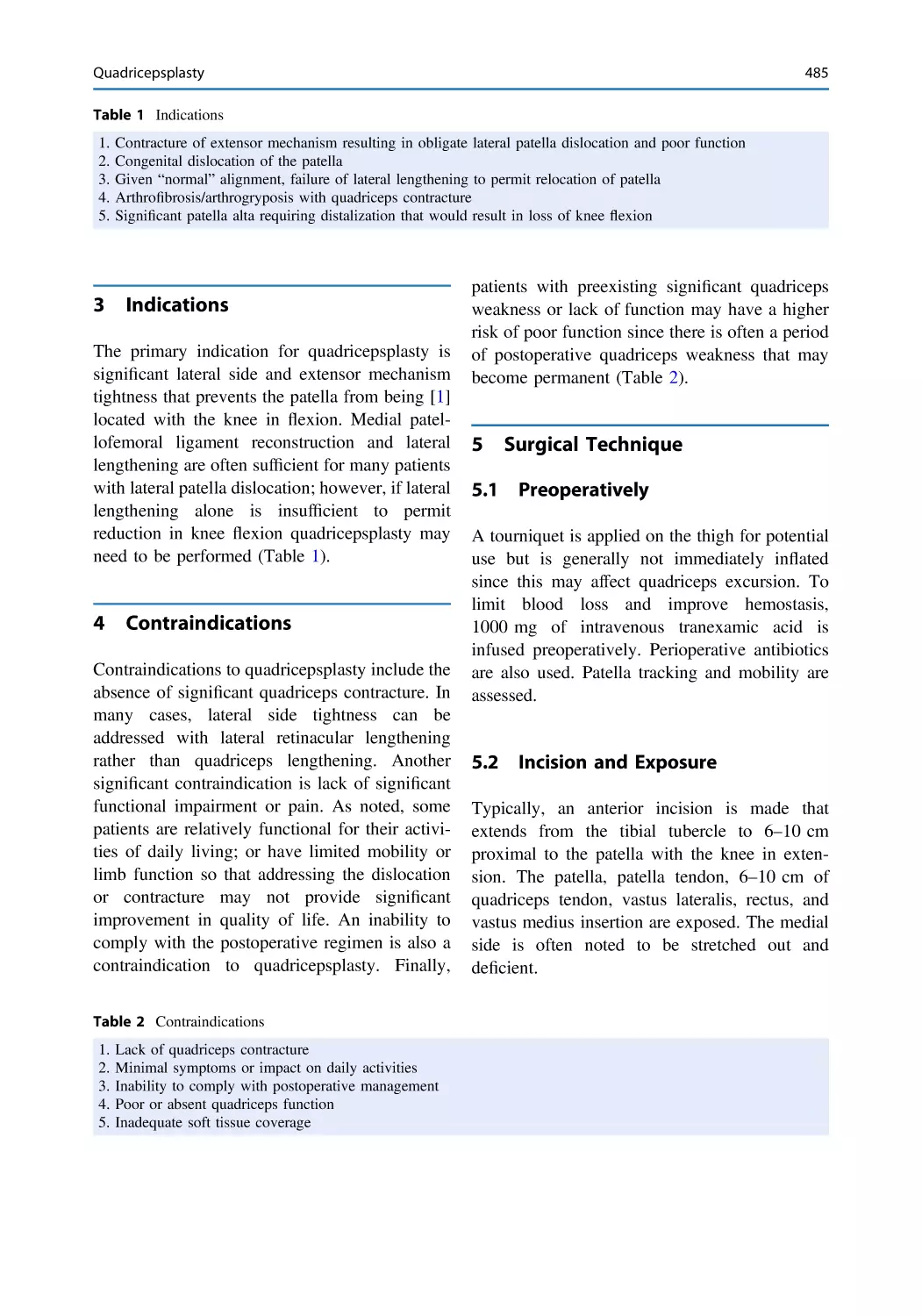
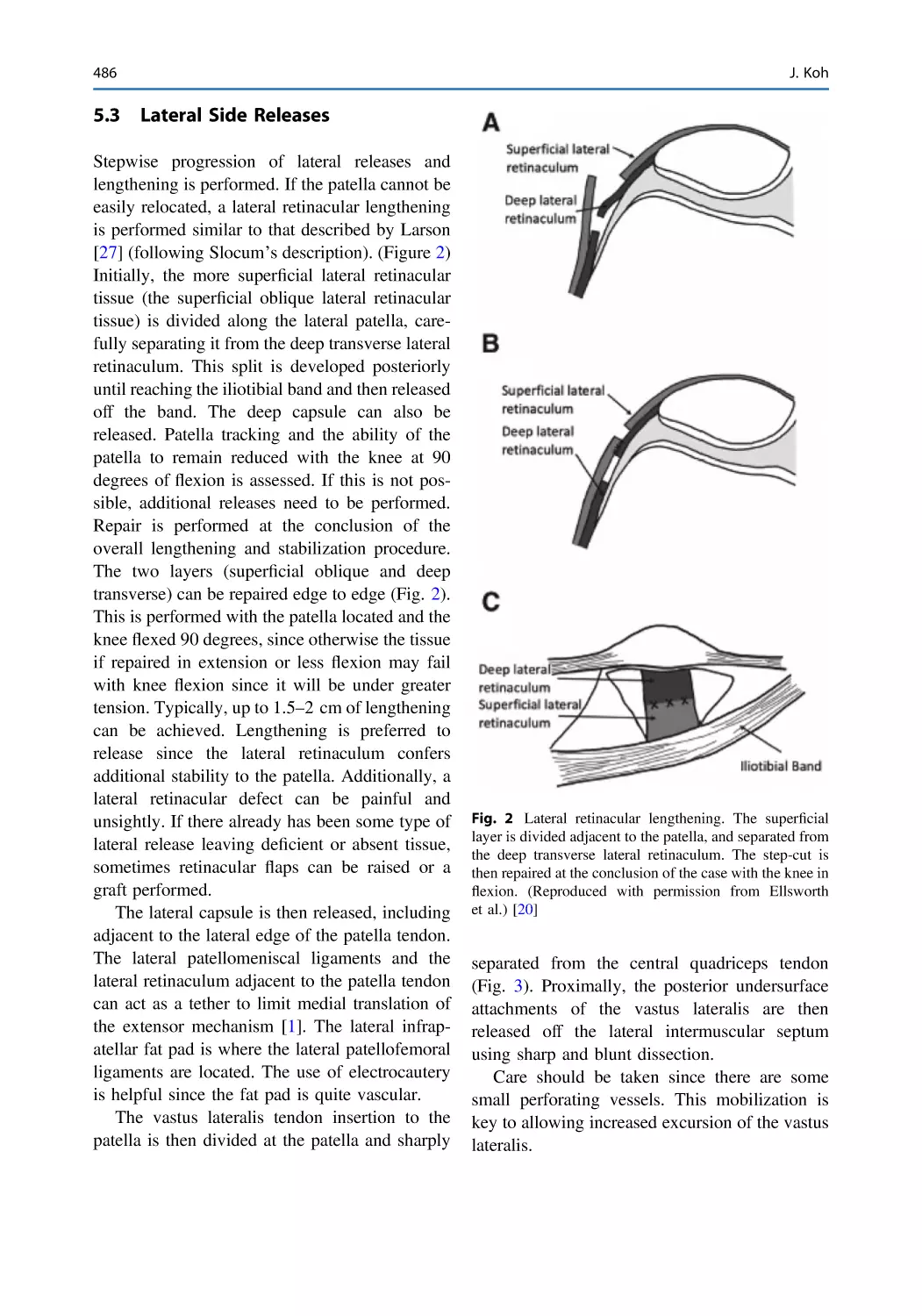
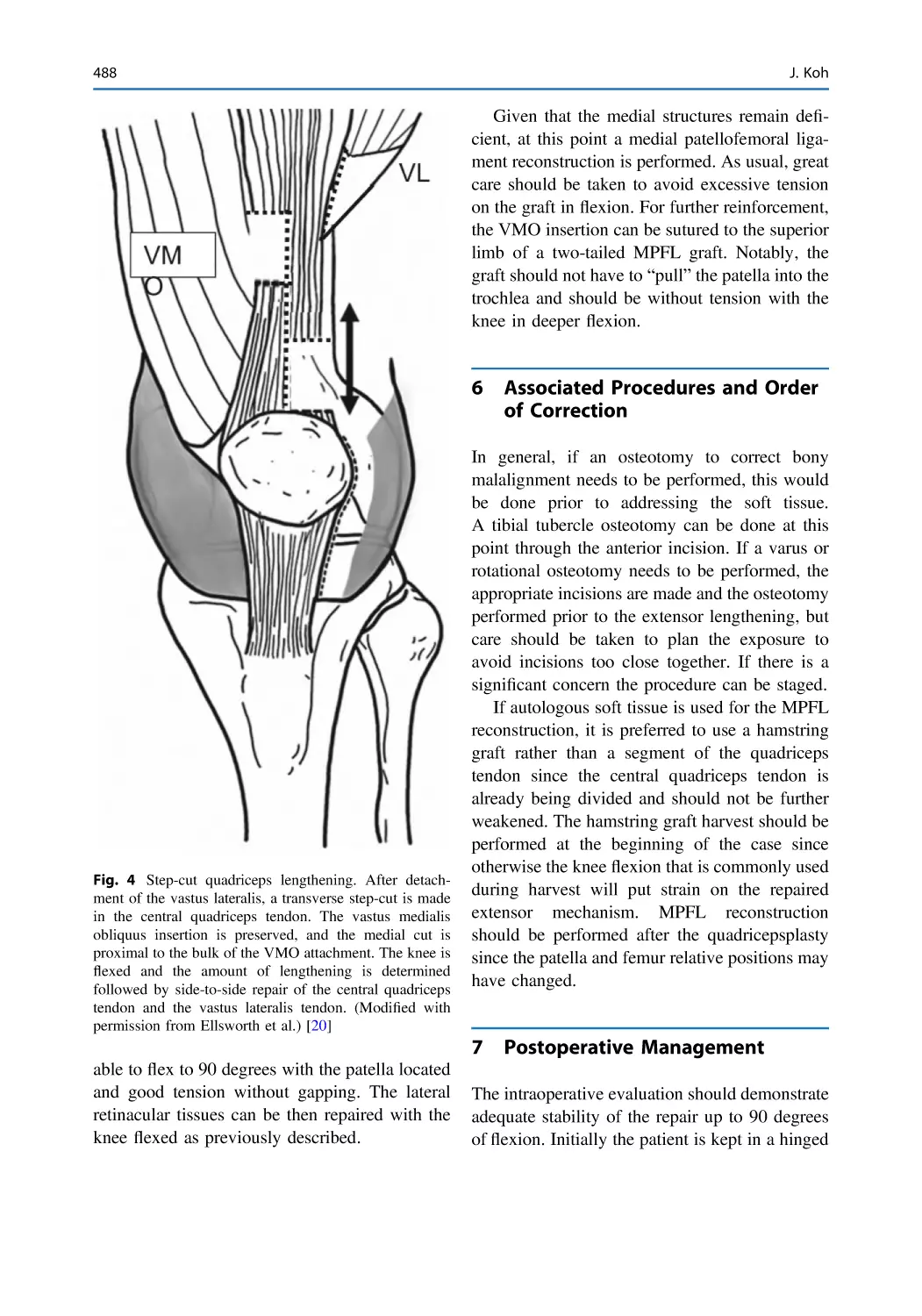
Quadricepsplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 483
Jason Koh
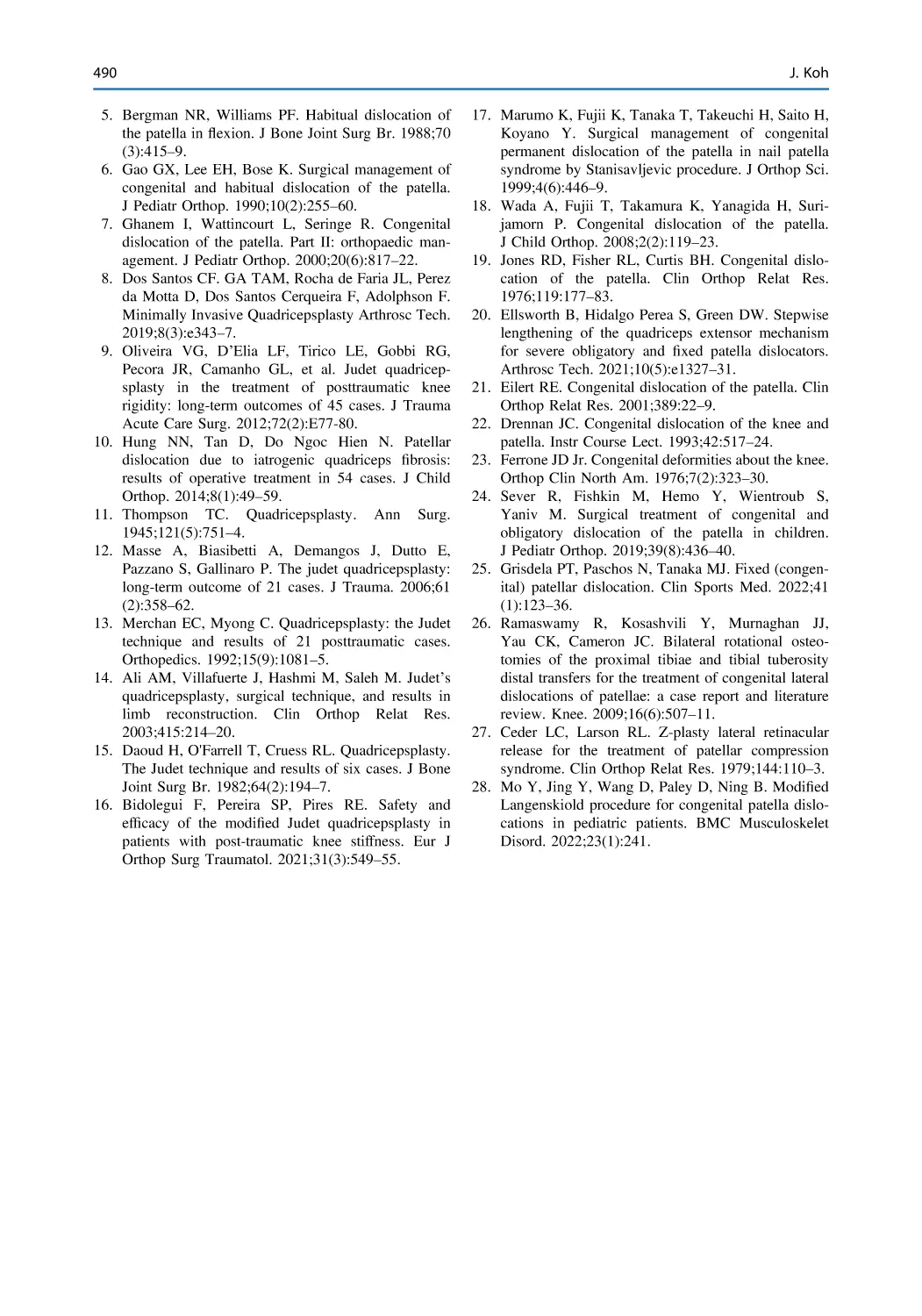
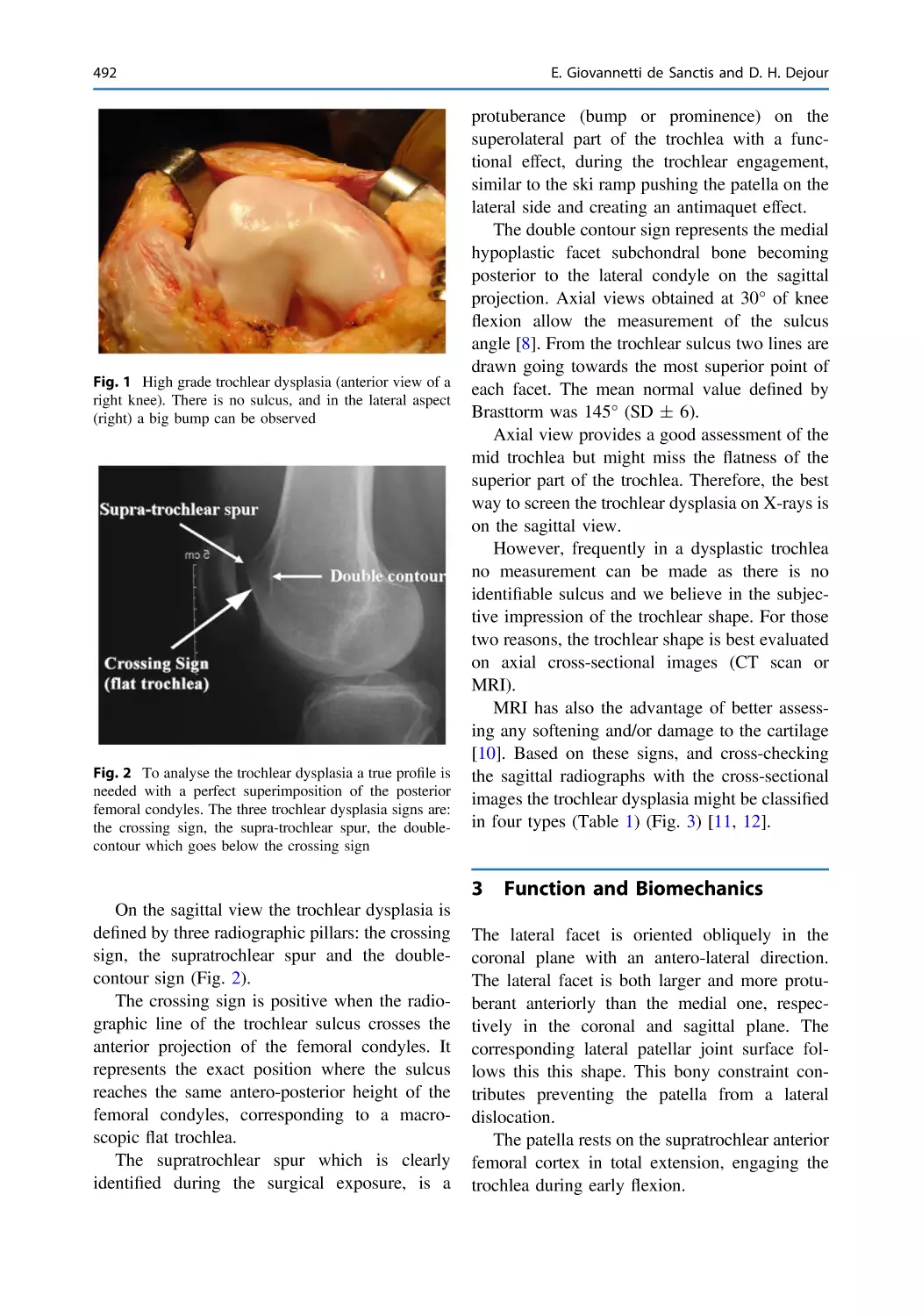
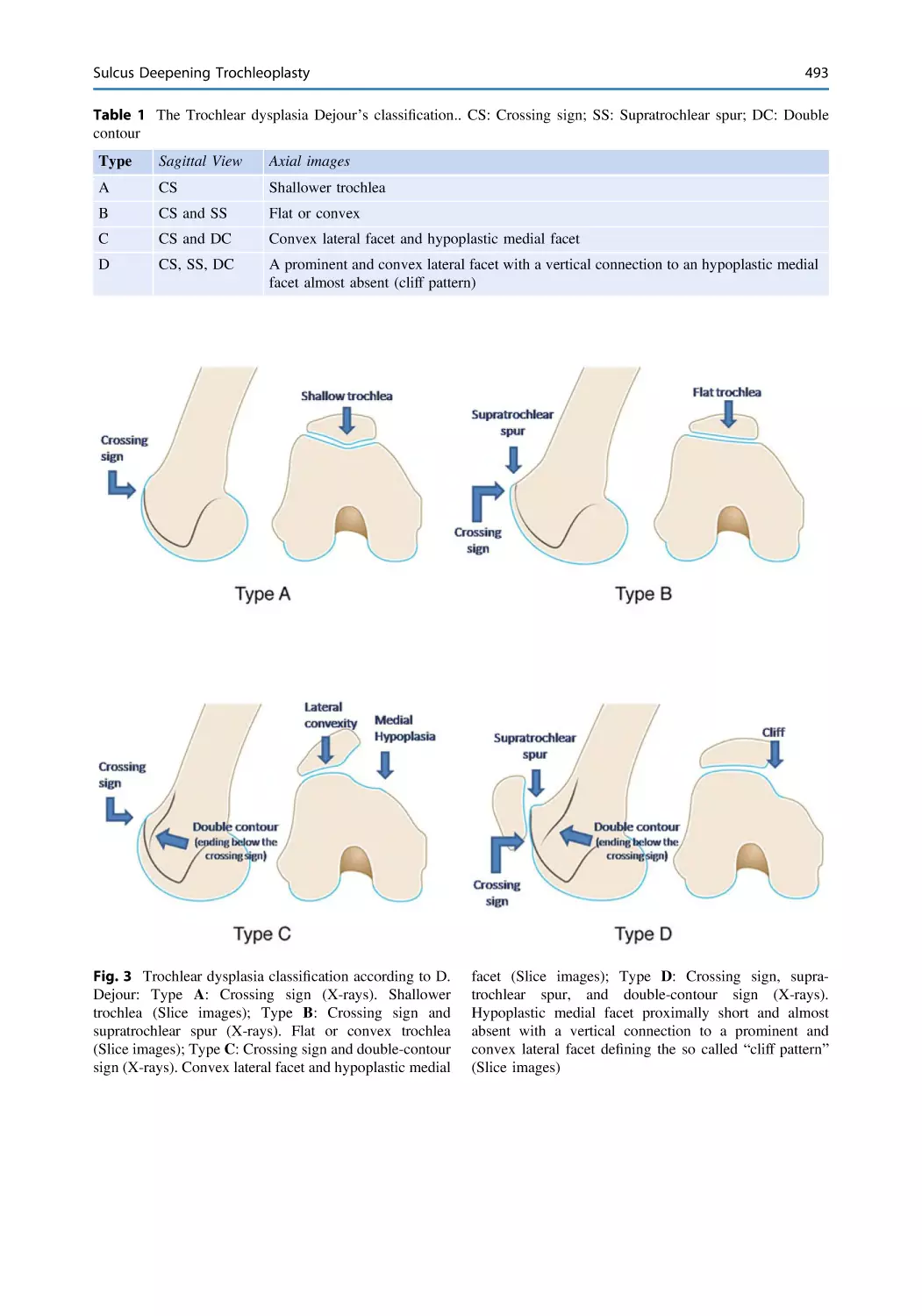
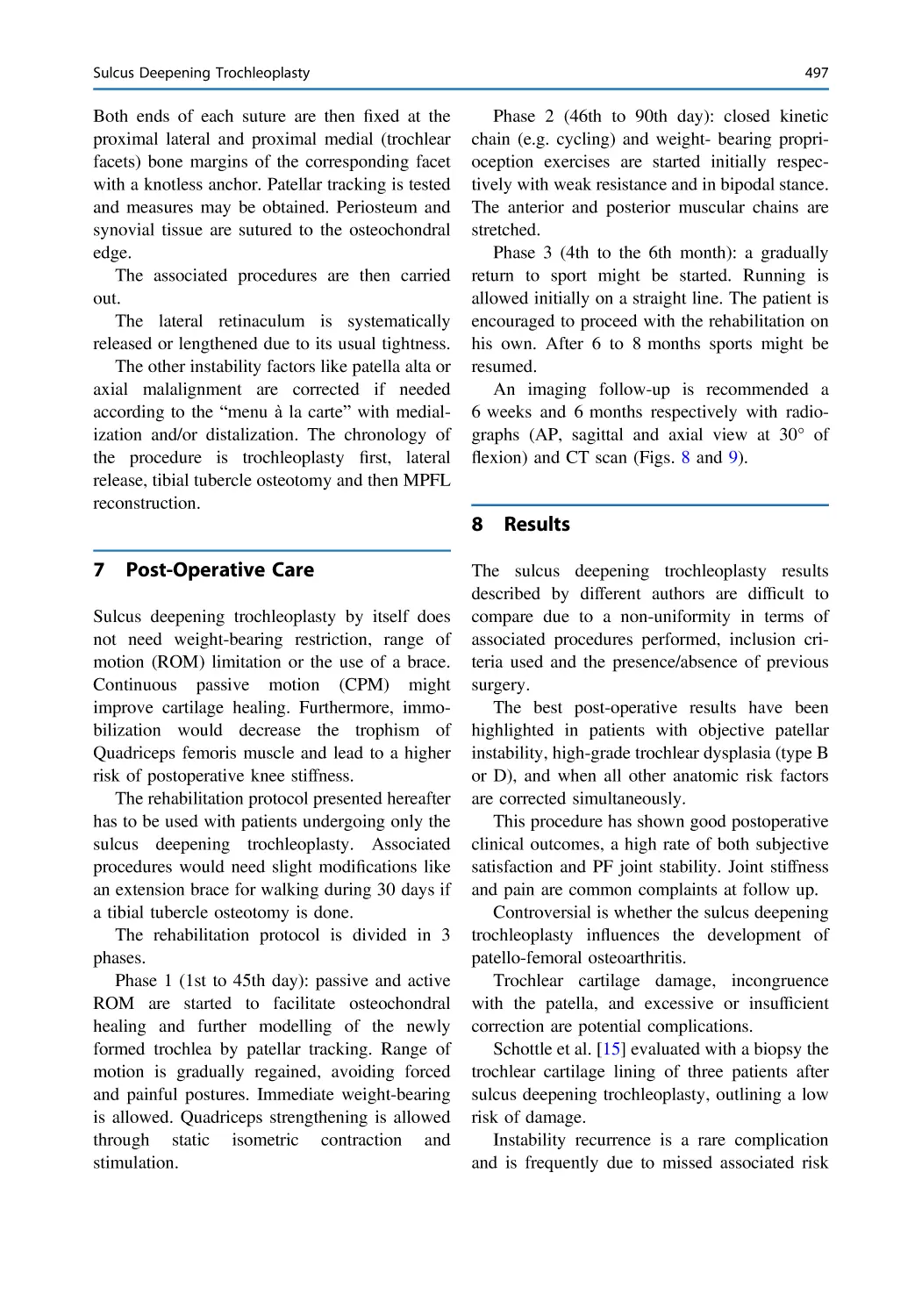
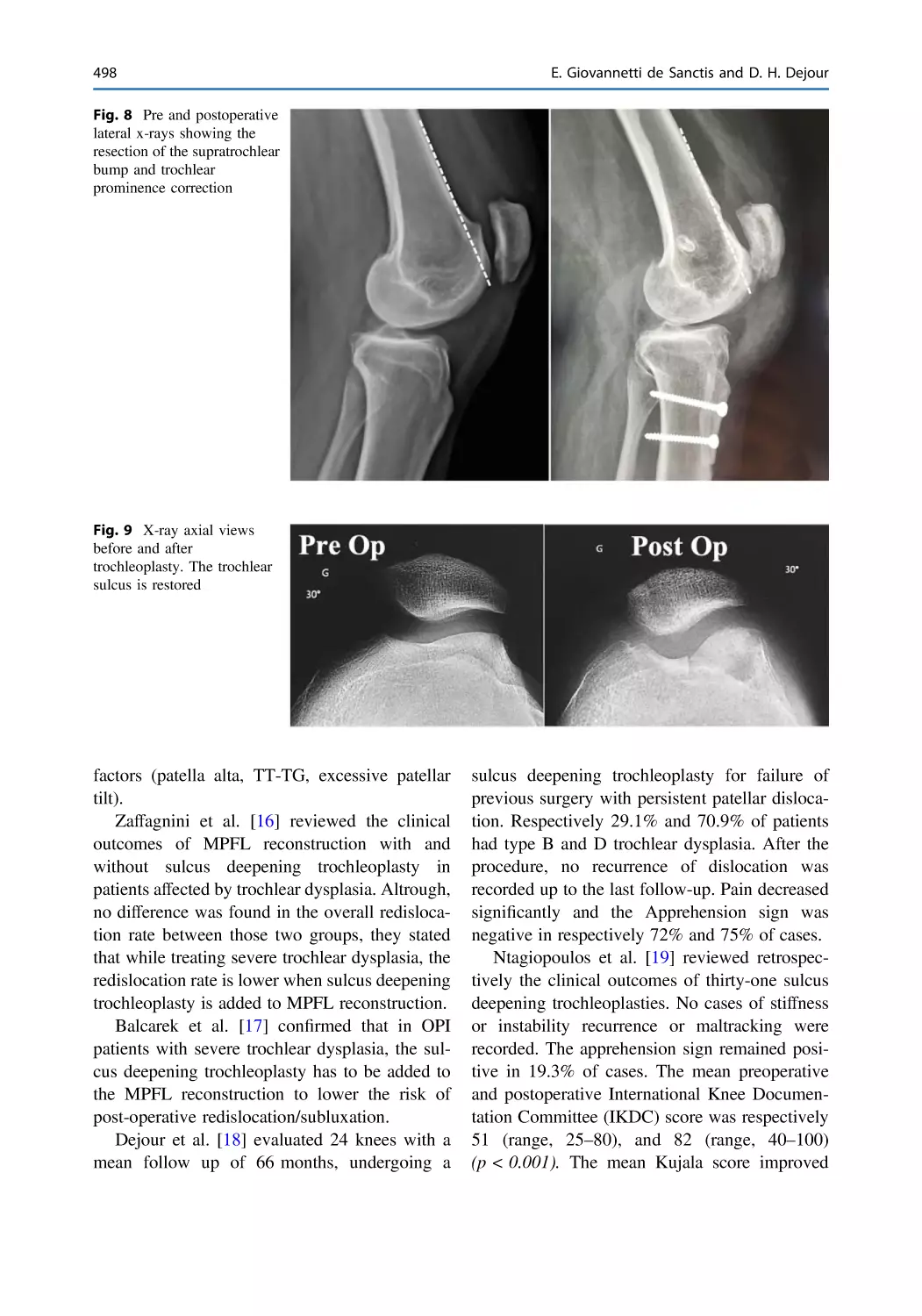
Sulcus Deepening Trochleoplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . 491
Edoardo Giovannetti de Sanctis and David H. Dejour
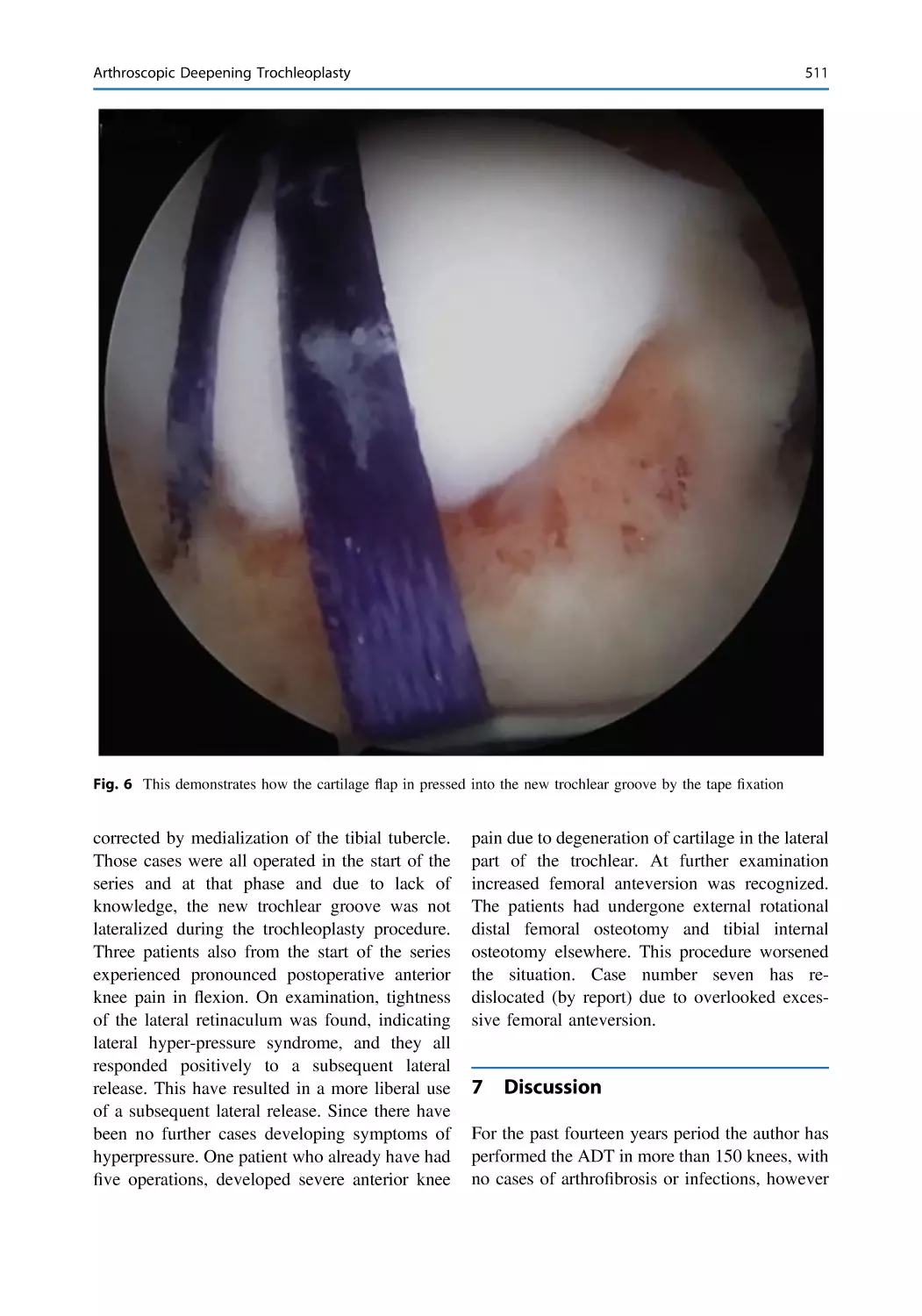
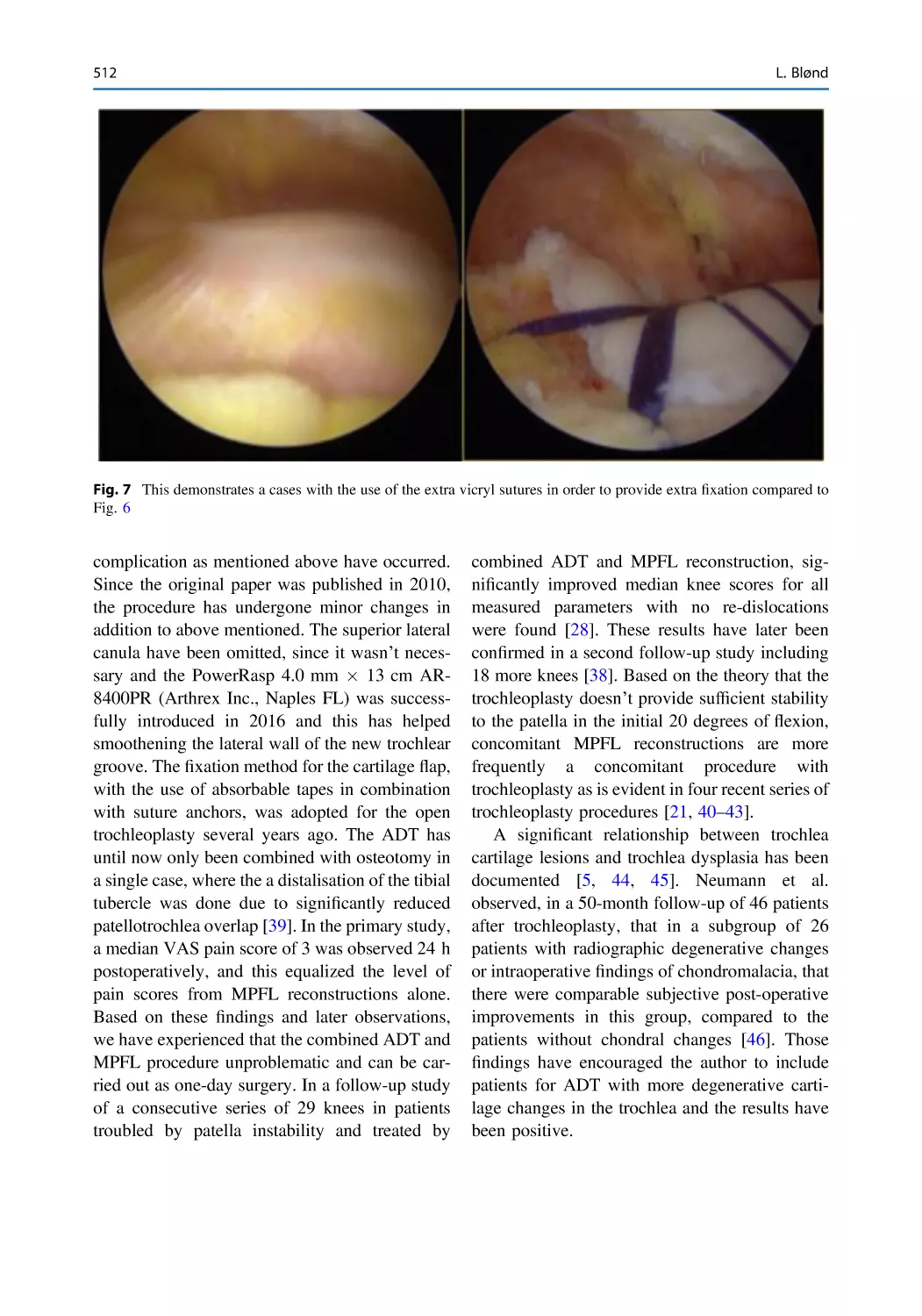
Arthroscopic Deepening Trochleoplasty. . . . . . . . . . . . . . . . . . . . . . 503
Lars Blønd
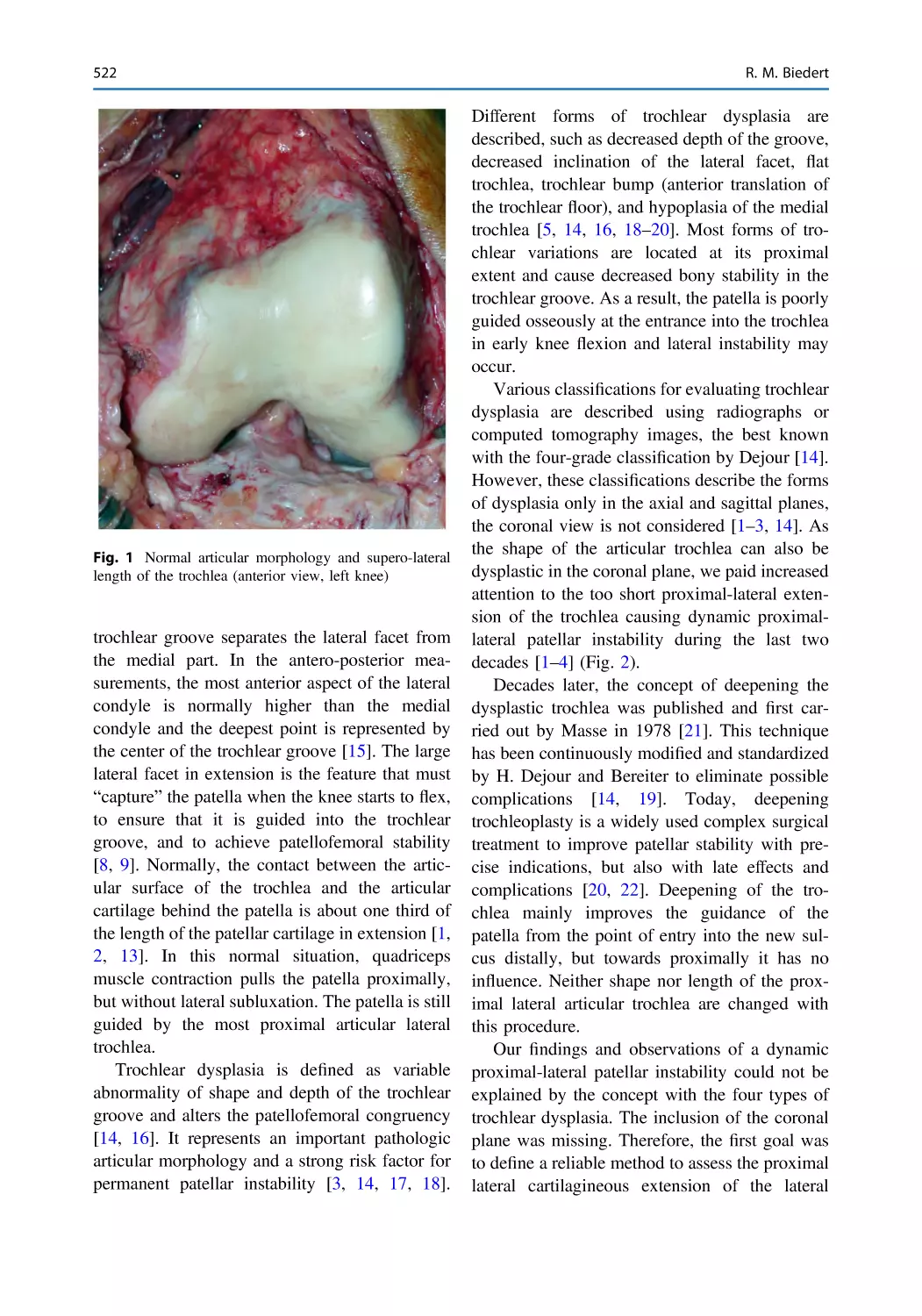
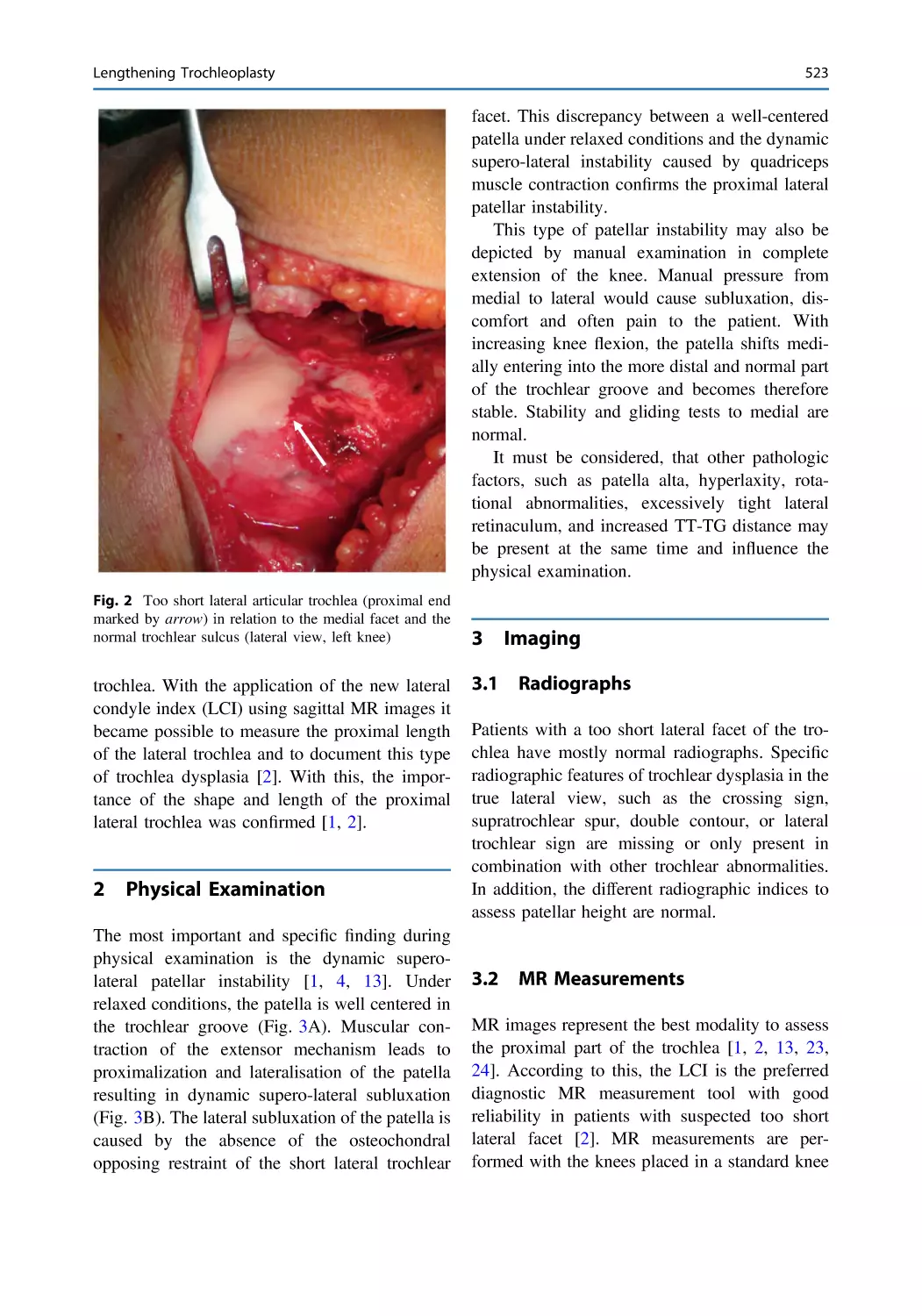
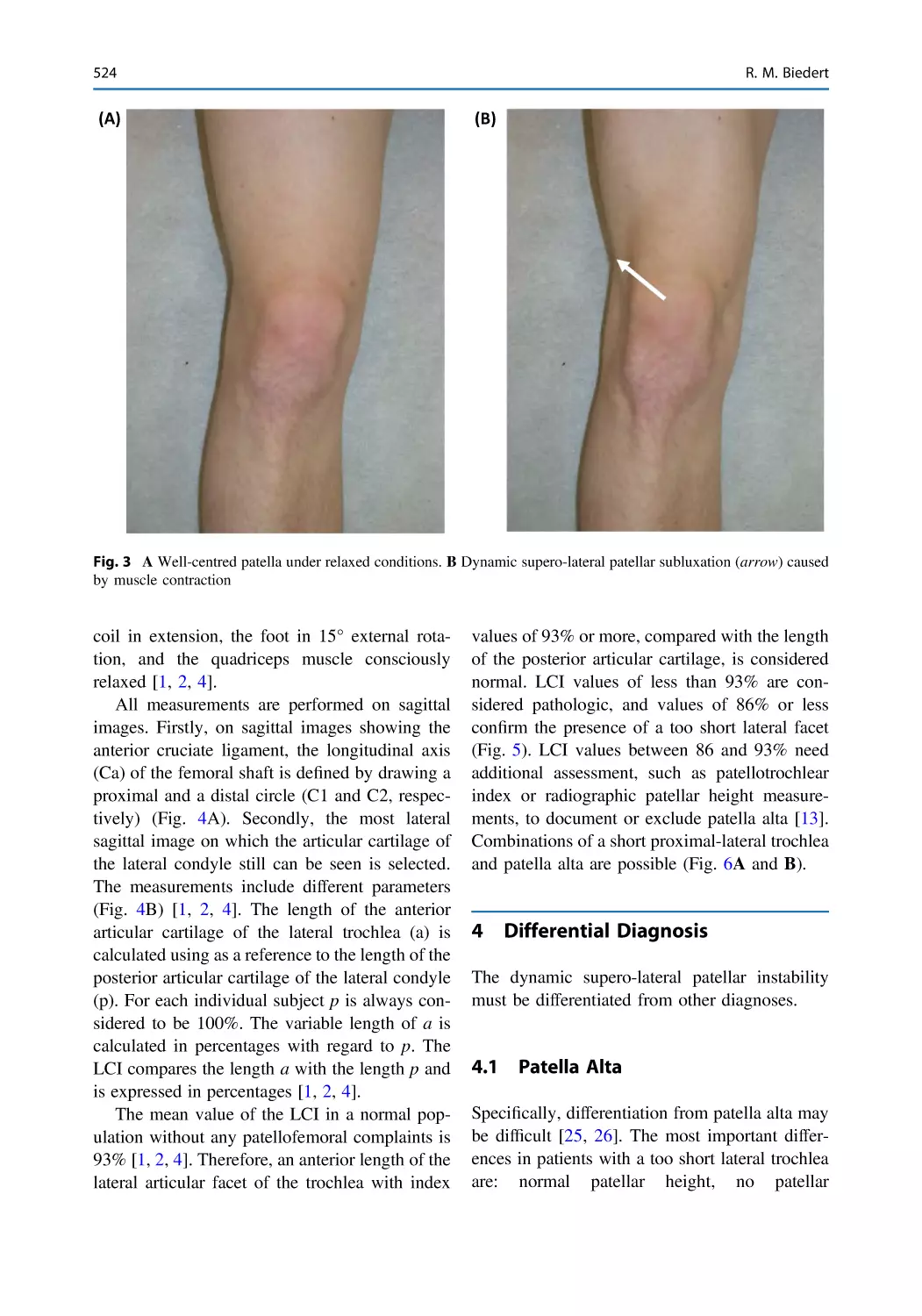
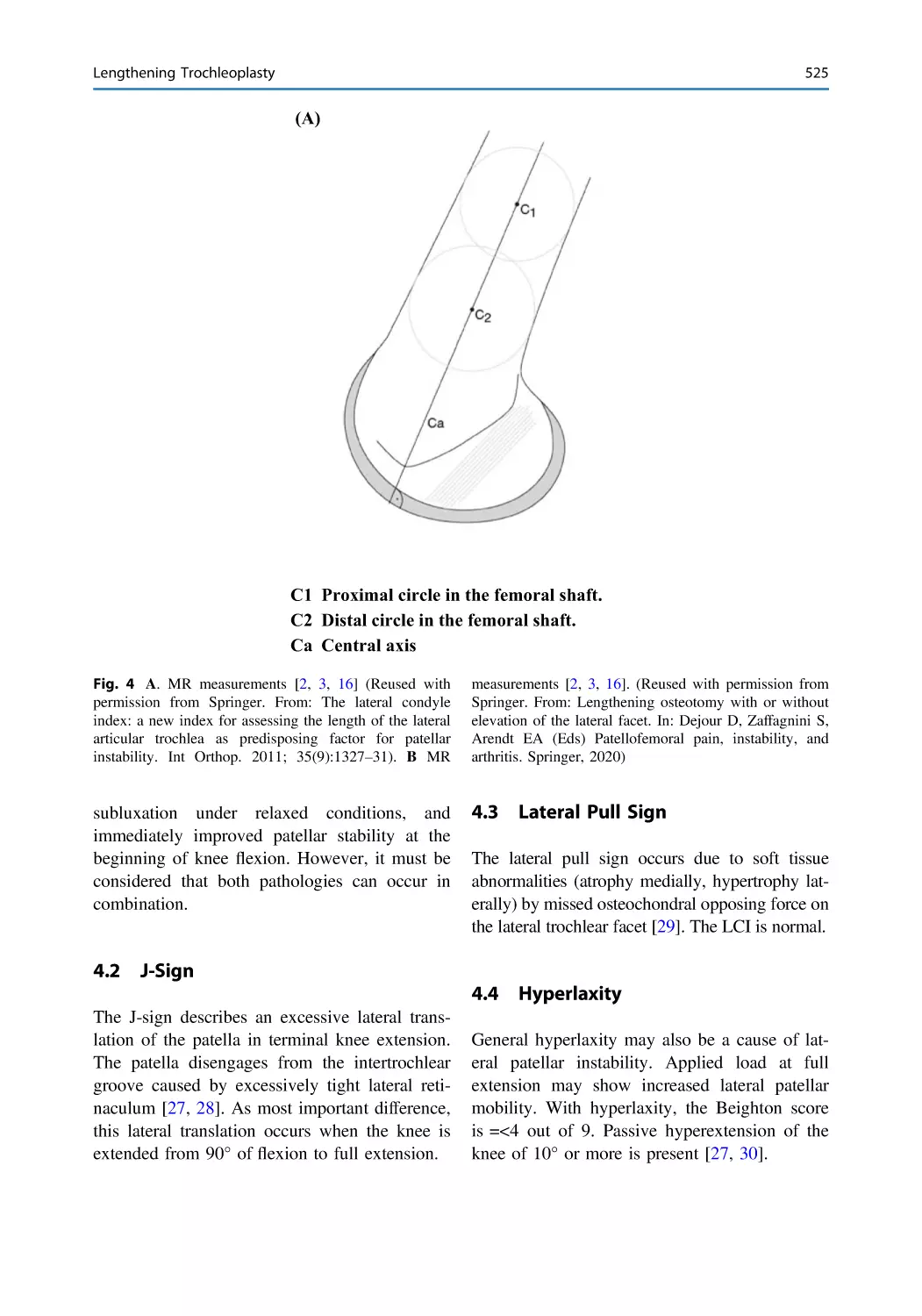
Lengthening Trochleoplasty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 521
Roland M. Biedert
Tibial Tubercle Osteotomy in Patients with Patella Supera
or Infera . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 533
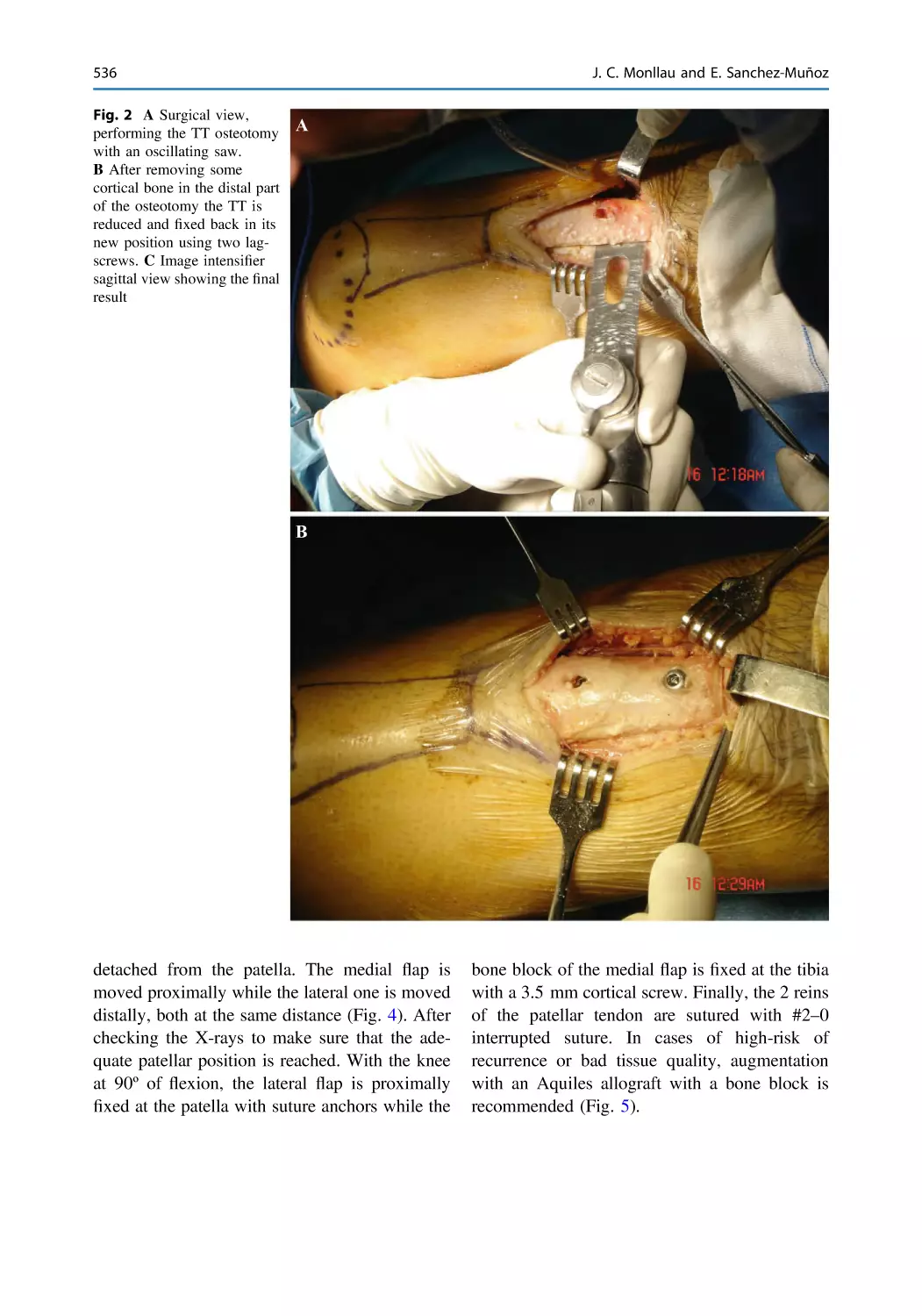
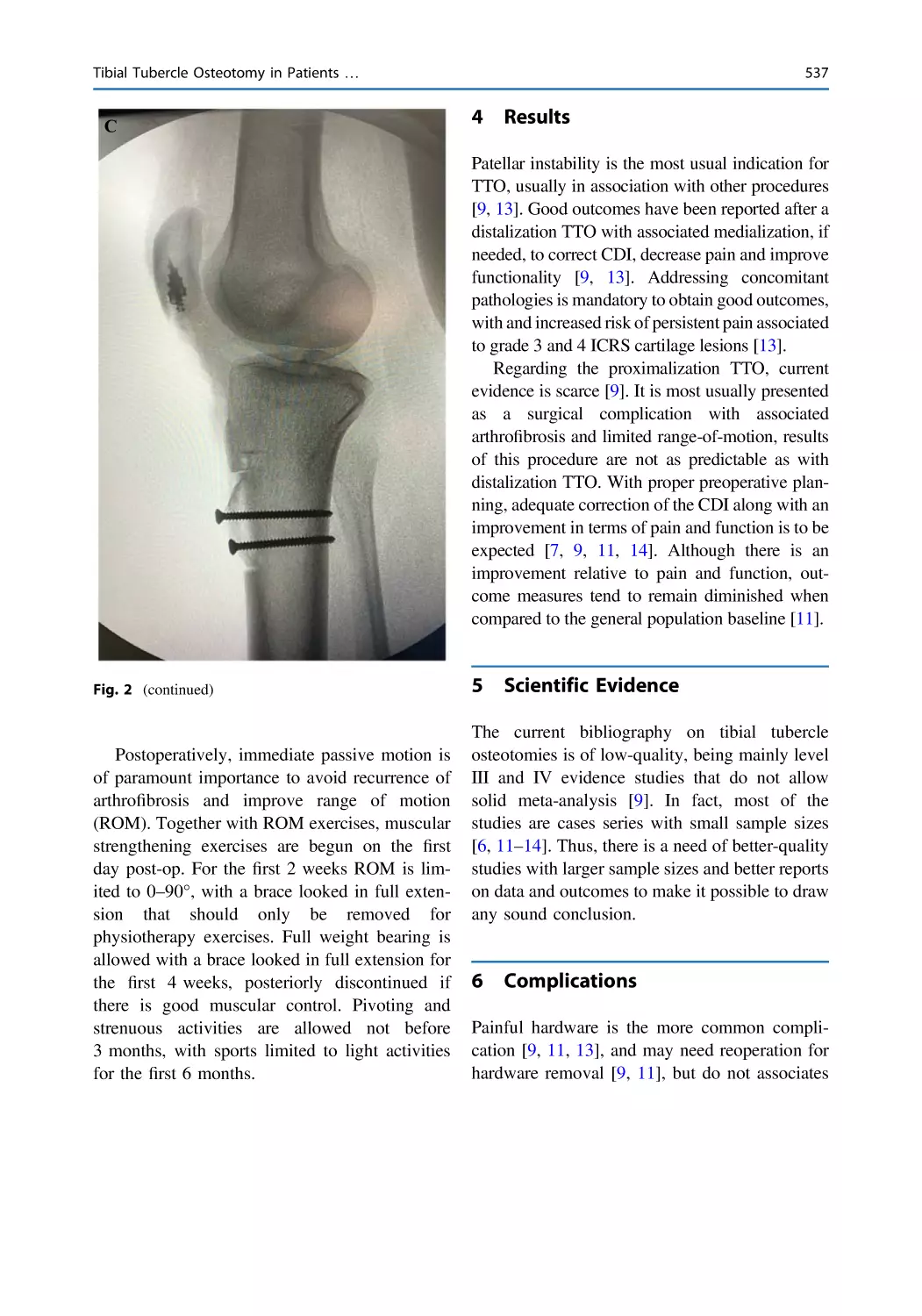
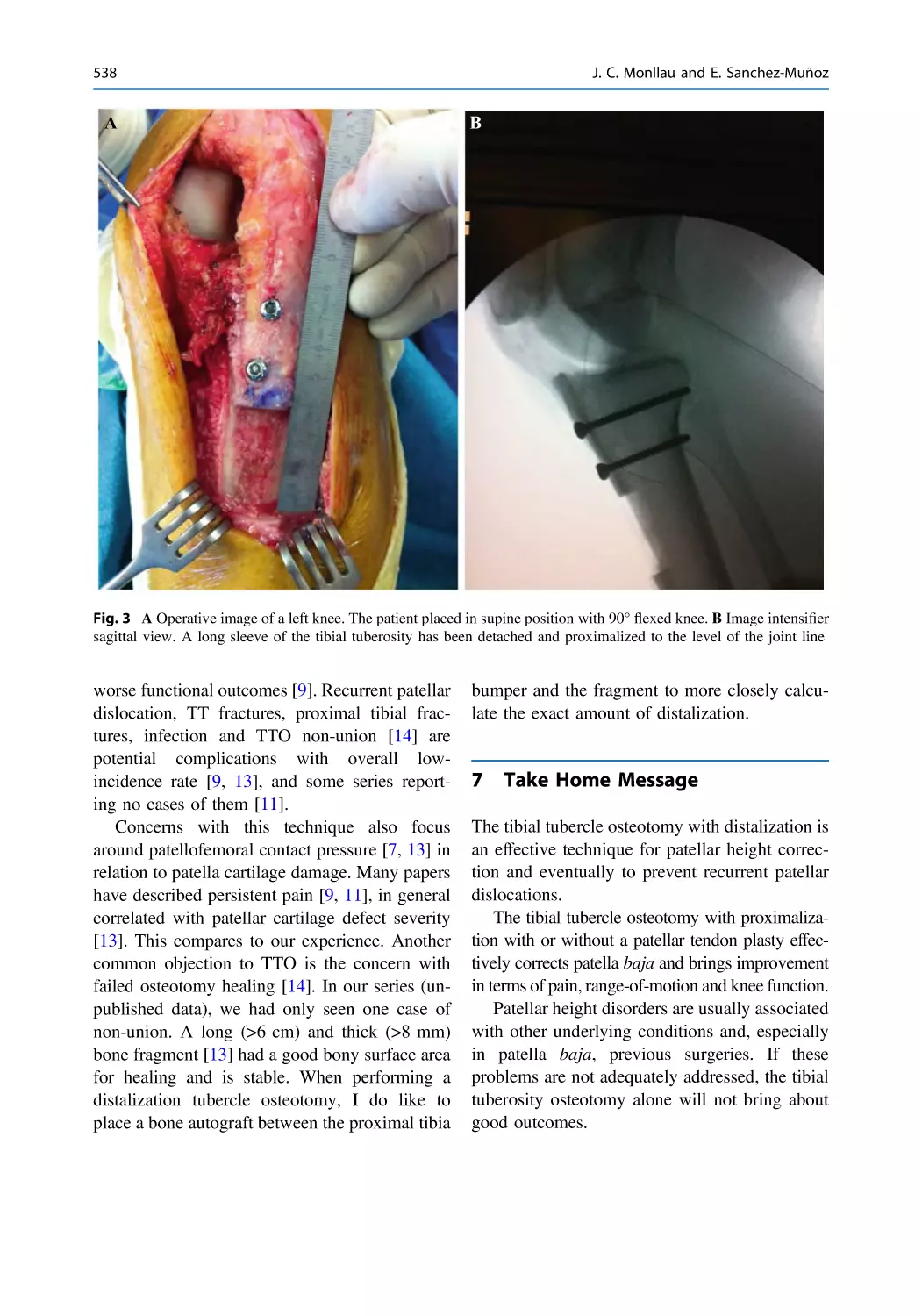
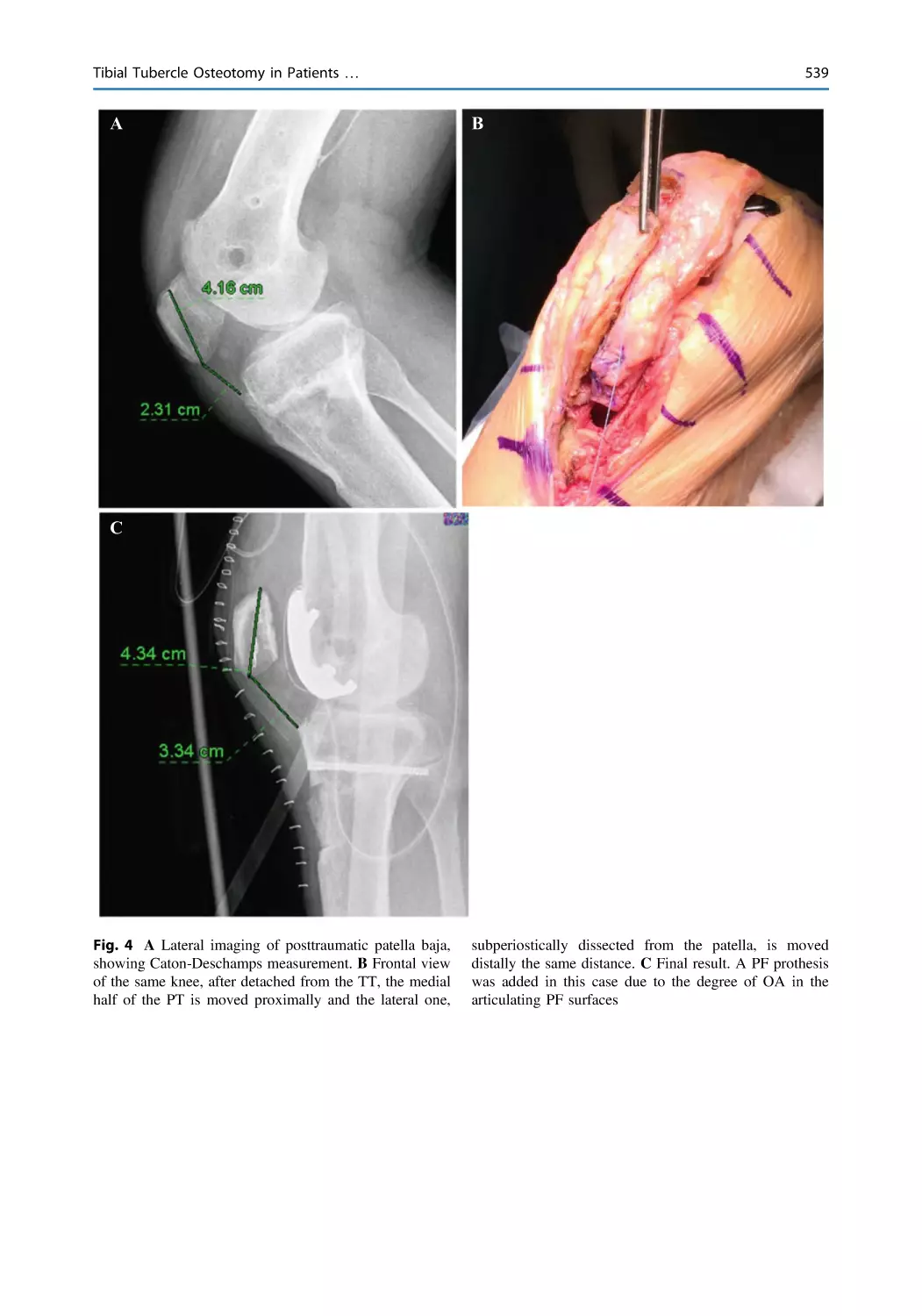
Joan Carles Monllau and Enrique Sanchez-Muñoz
xxiv
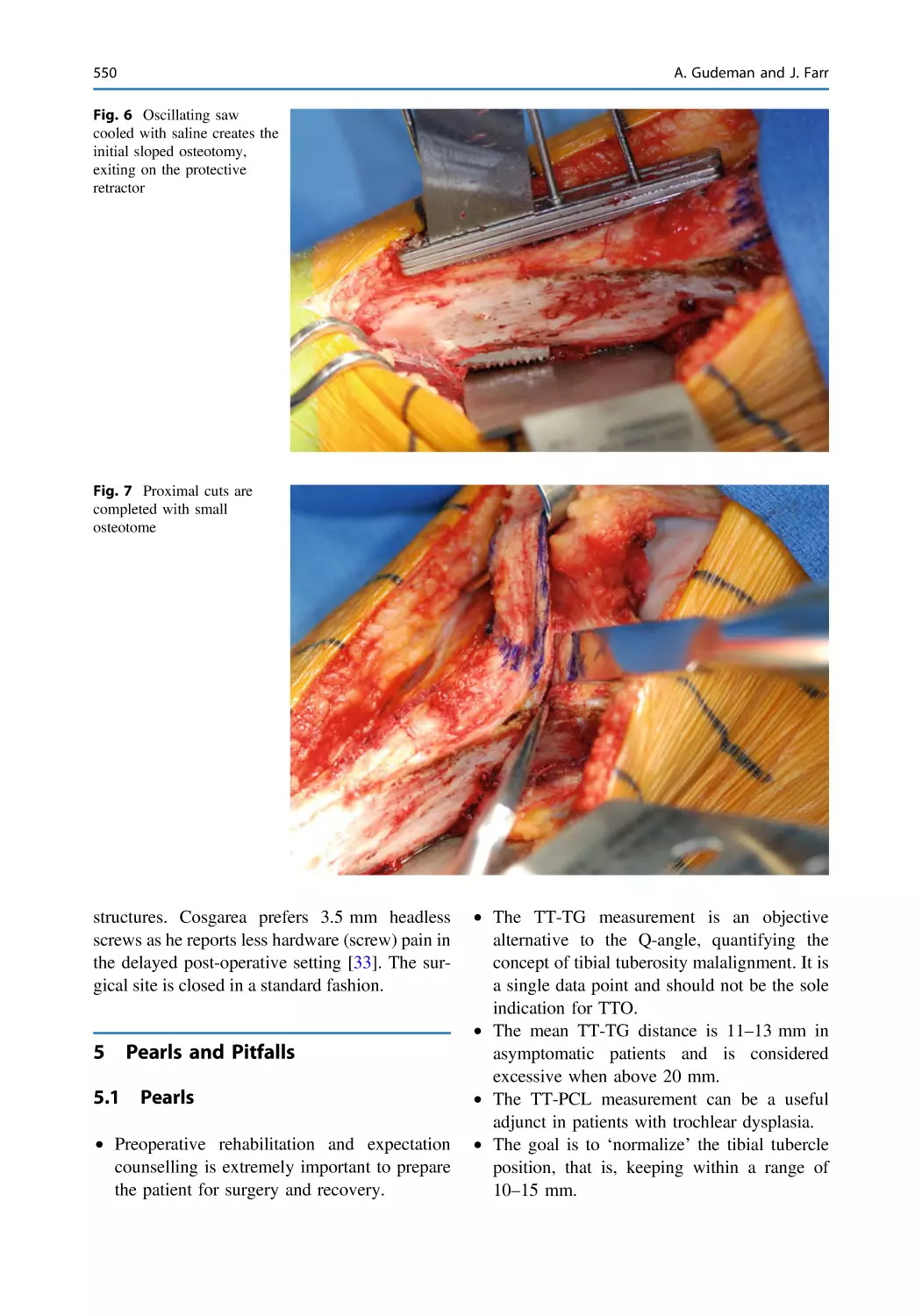
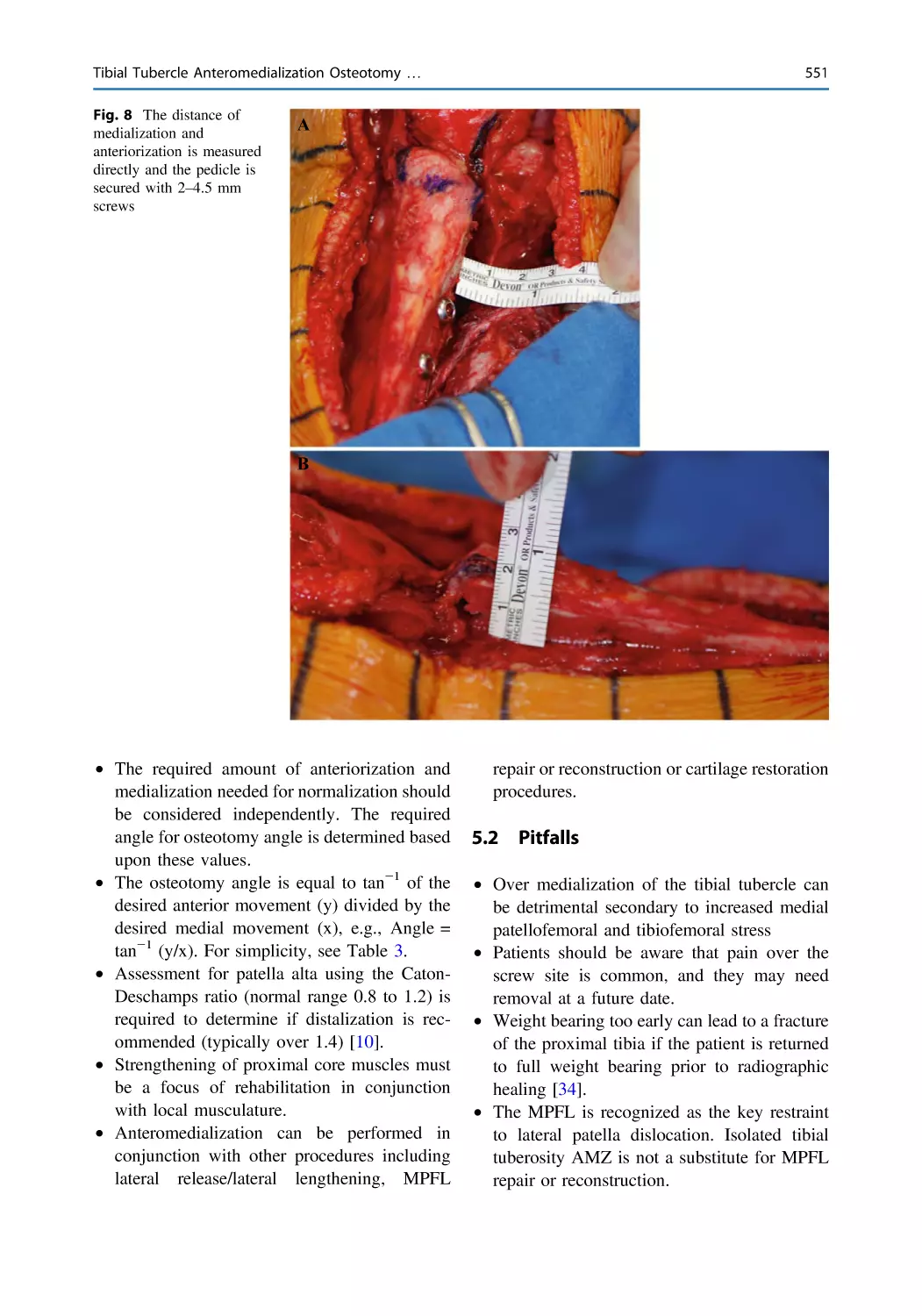
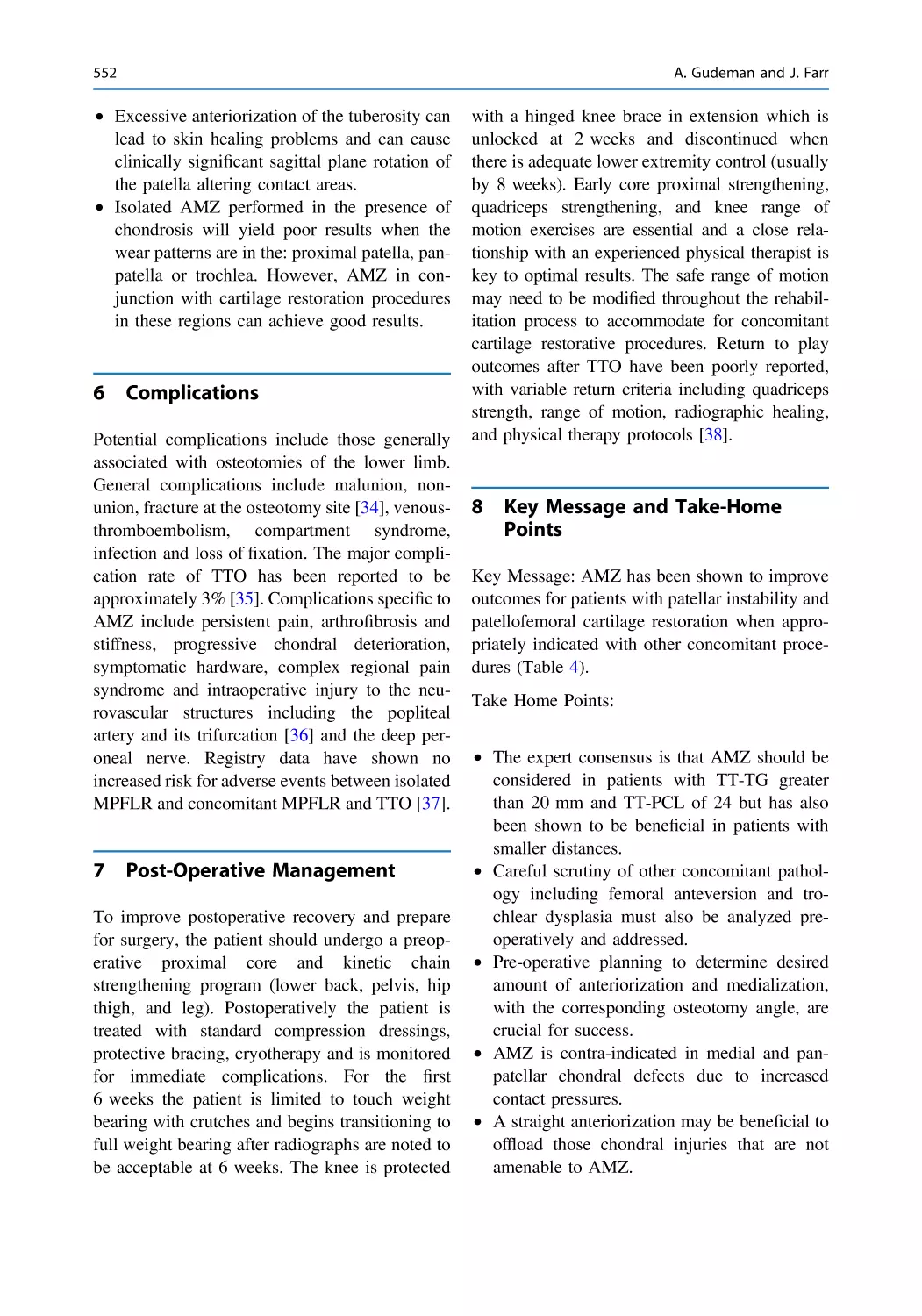
Tibial Tubercle Anteromedialization Osteotomy
(Fulkerson Osteotomy) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 543
Andrew Gudeman and Jack Farr
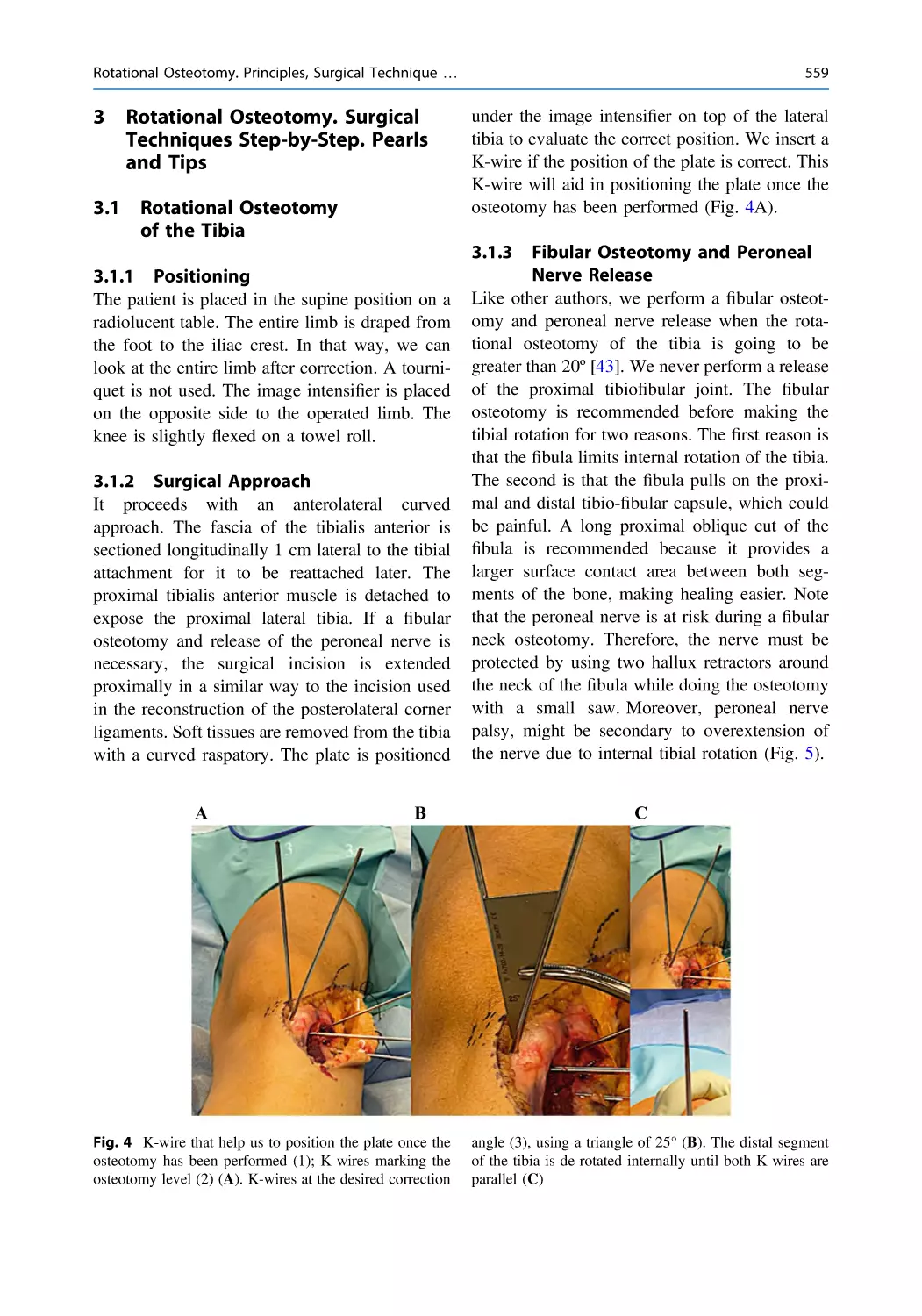
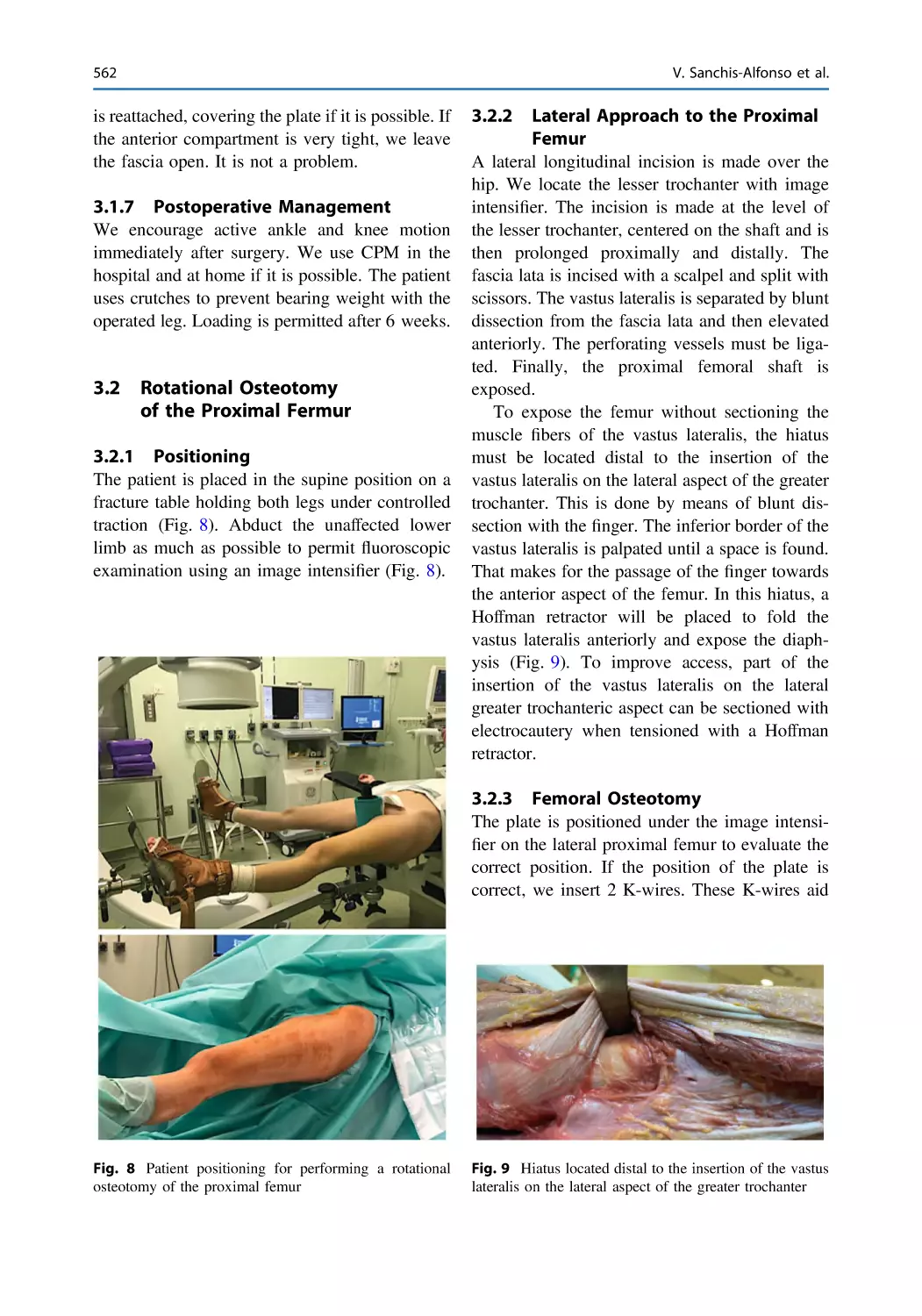
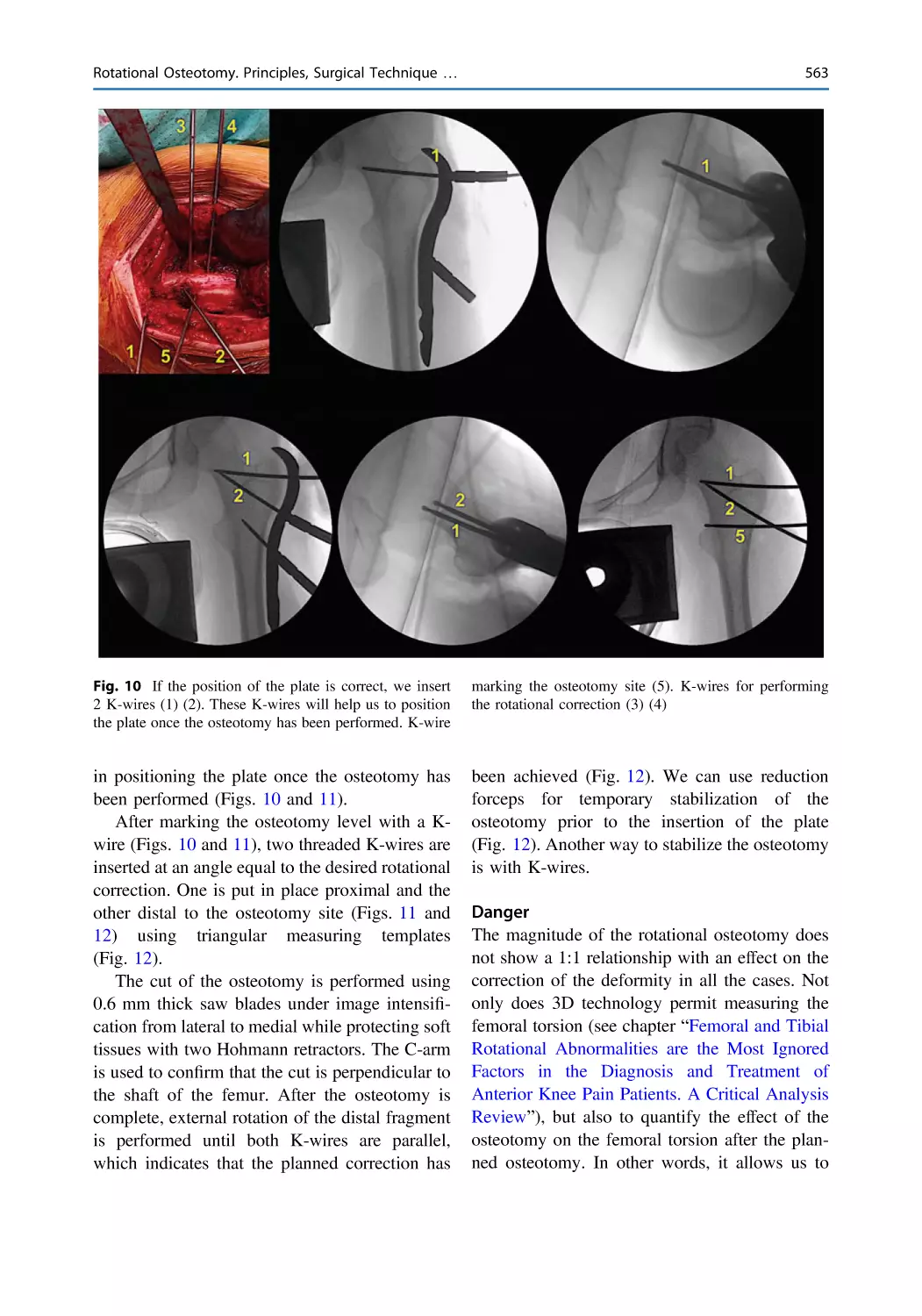
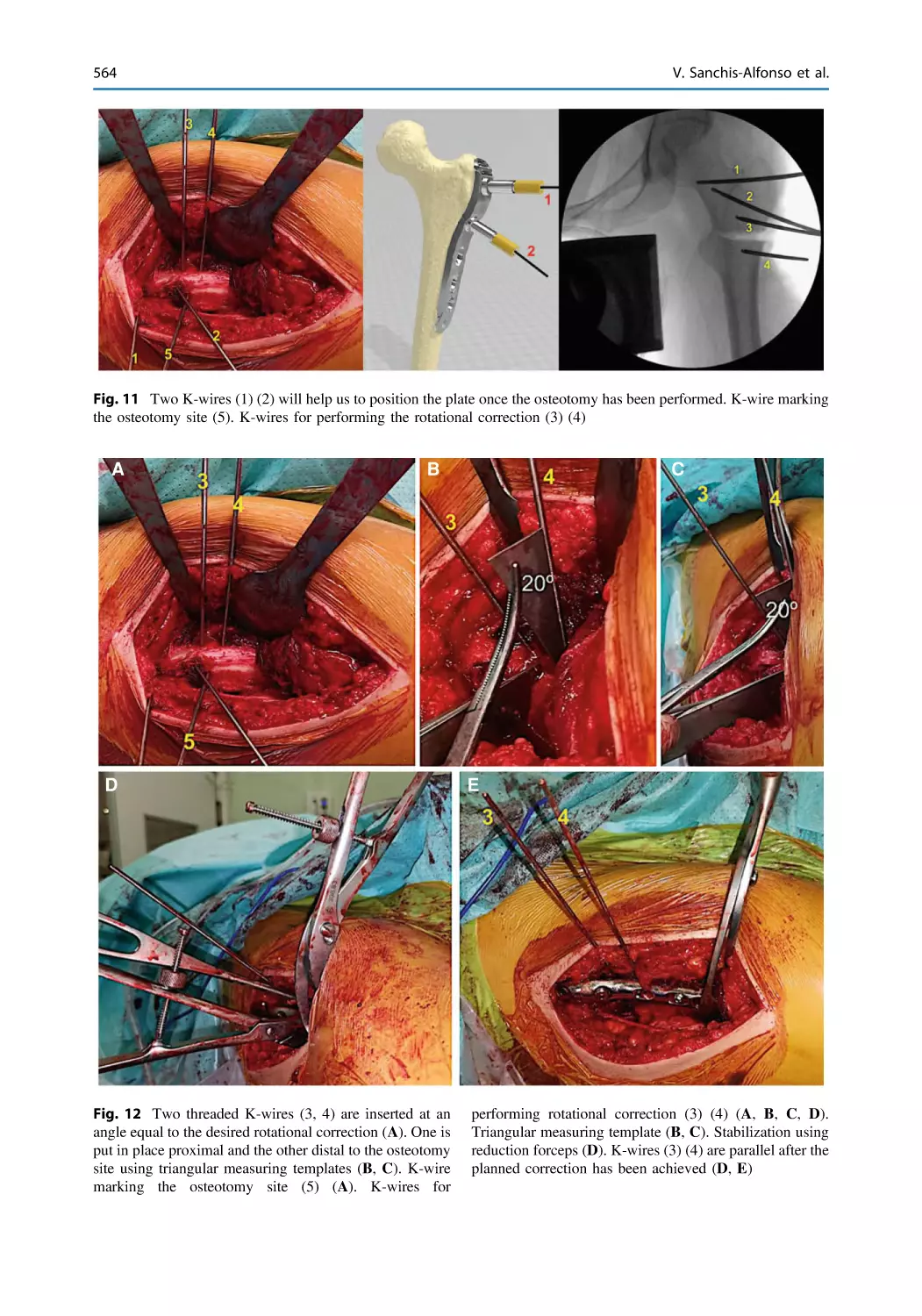
Rotational Osteotomy. Principles, Surgical Technique,
Outcomes and Complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555
Vicente Sanchis-Alfonso, Alejandro Roselló-Añón,
Cristina Ramírez-Fuentes, and Robert A. Teitge
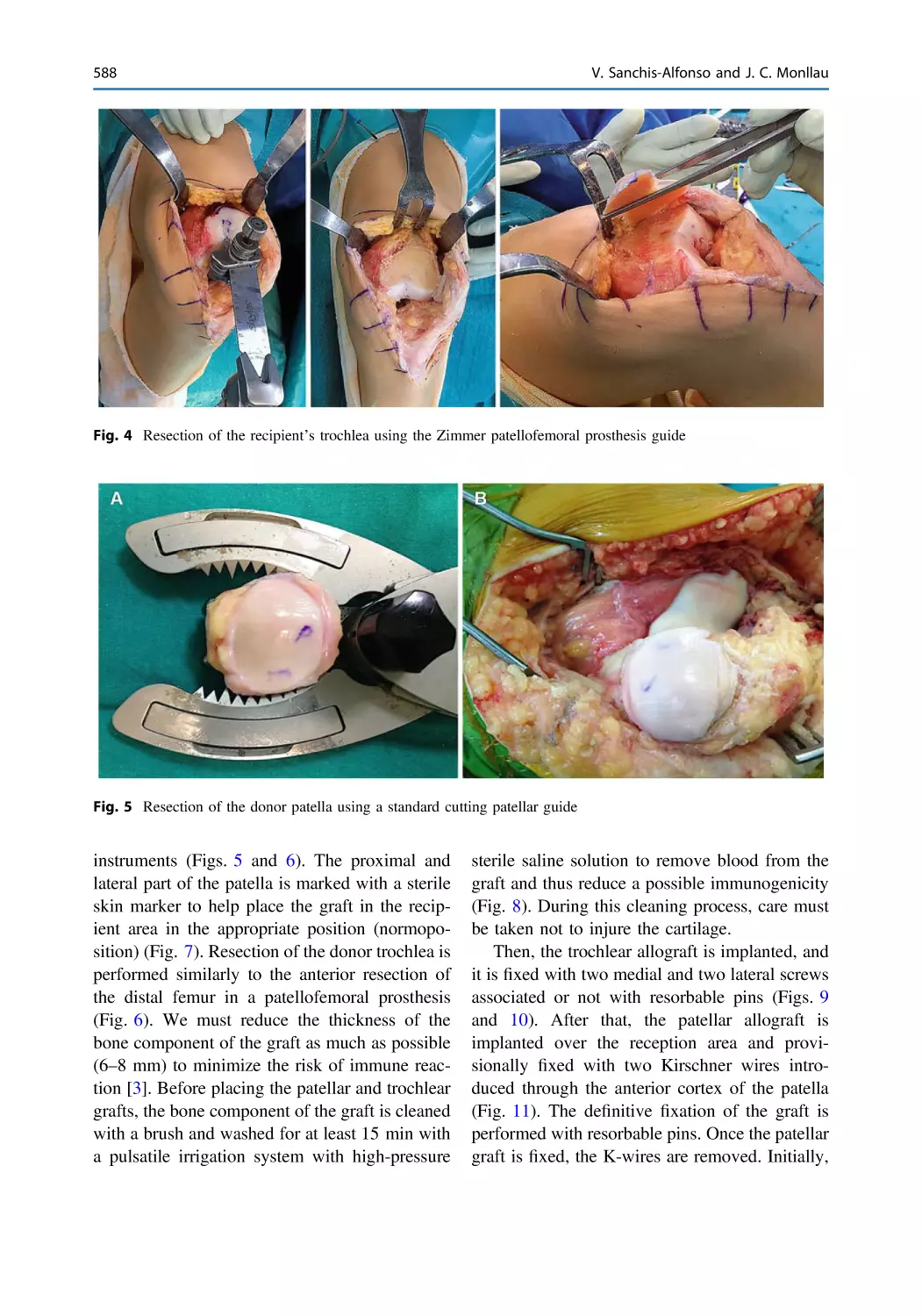
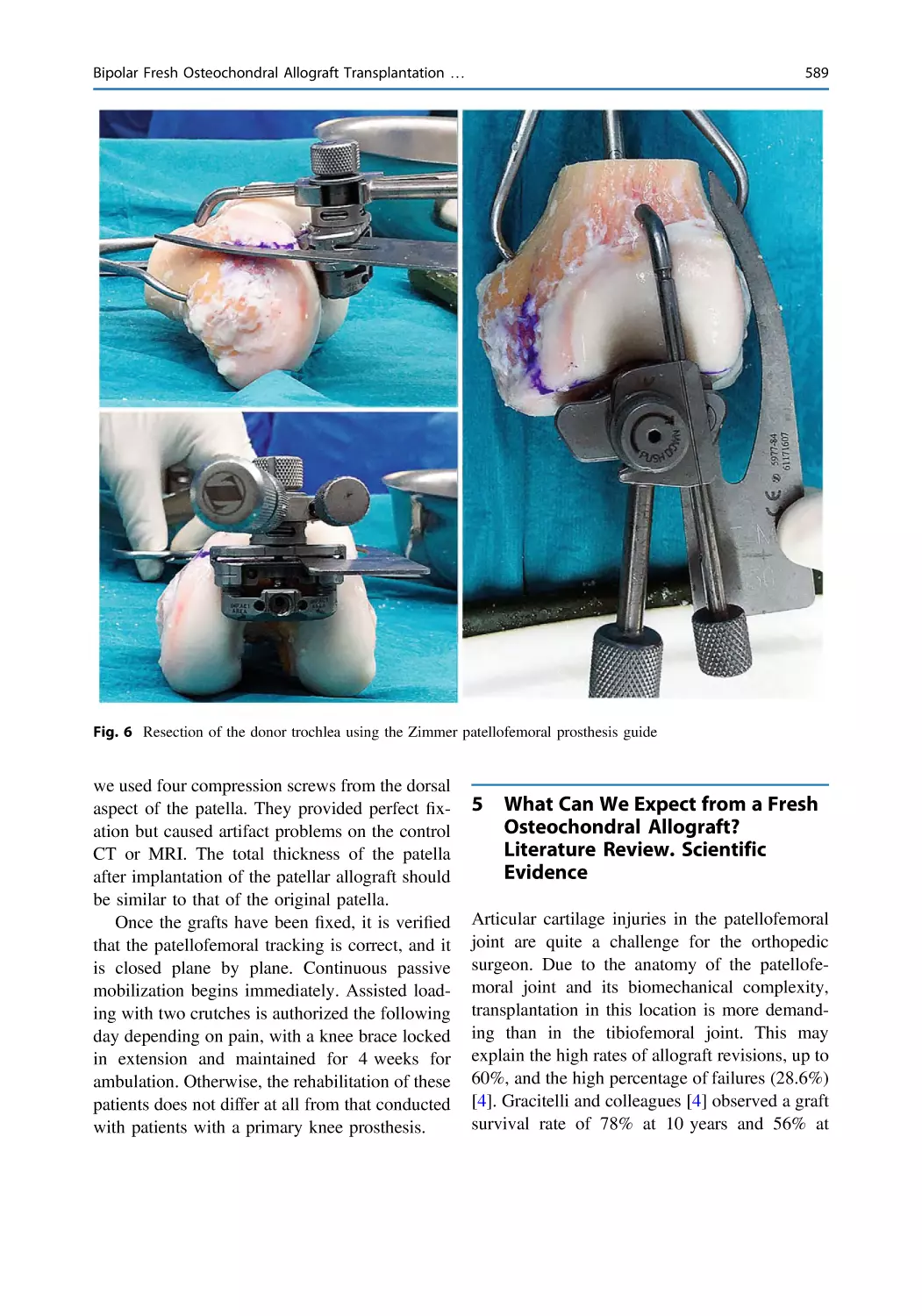
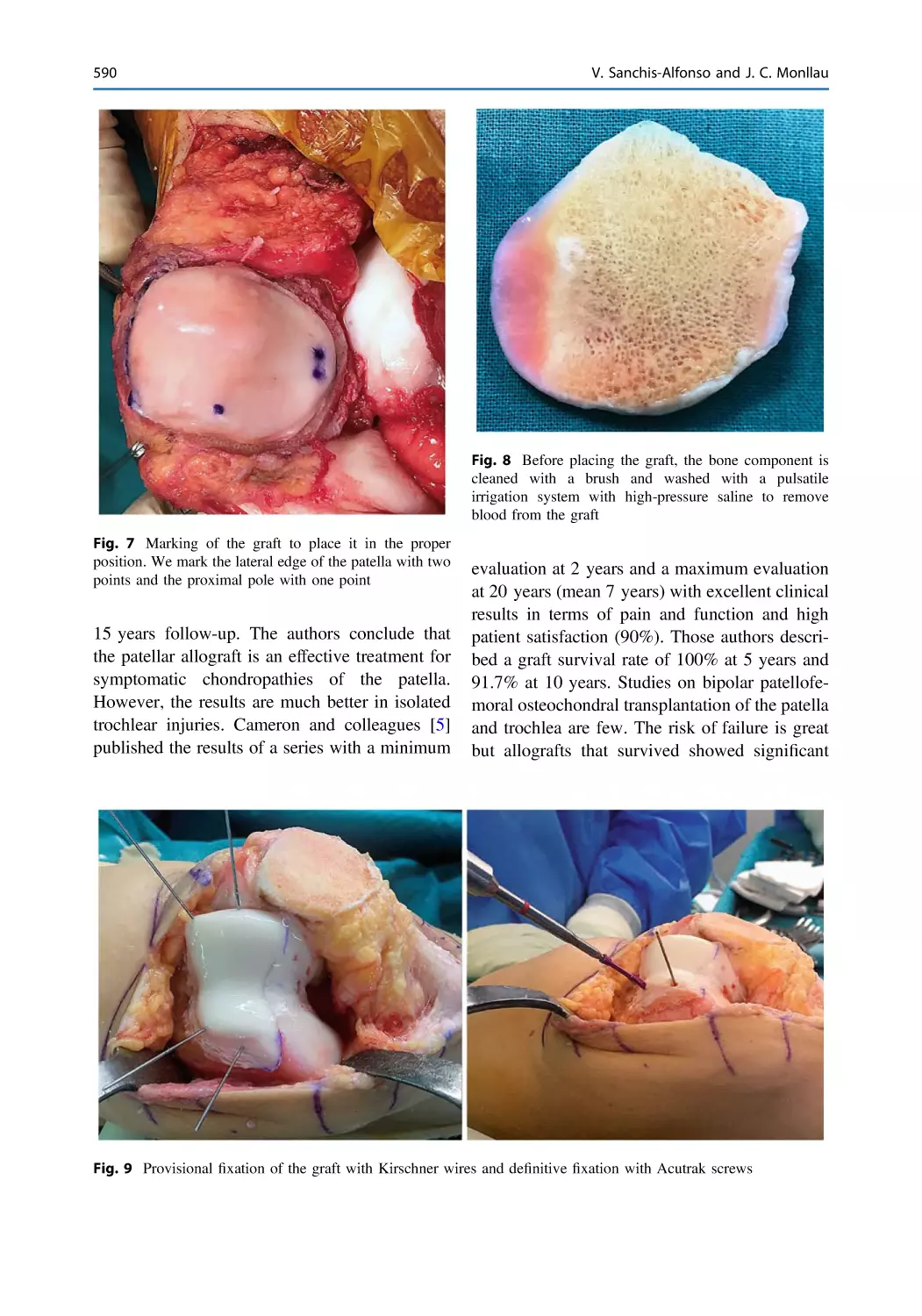
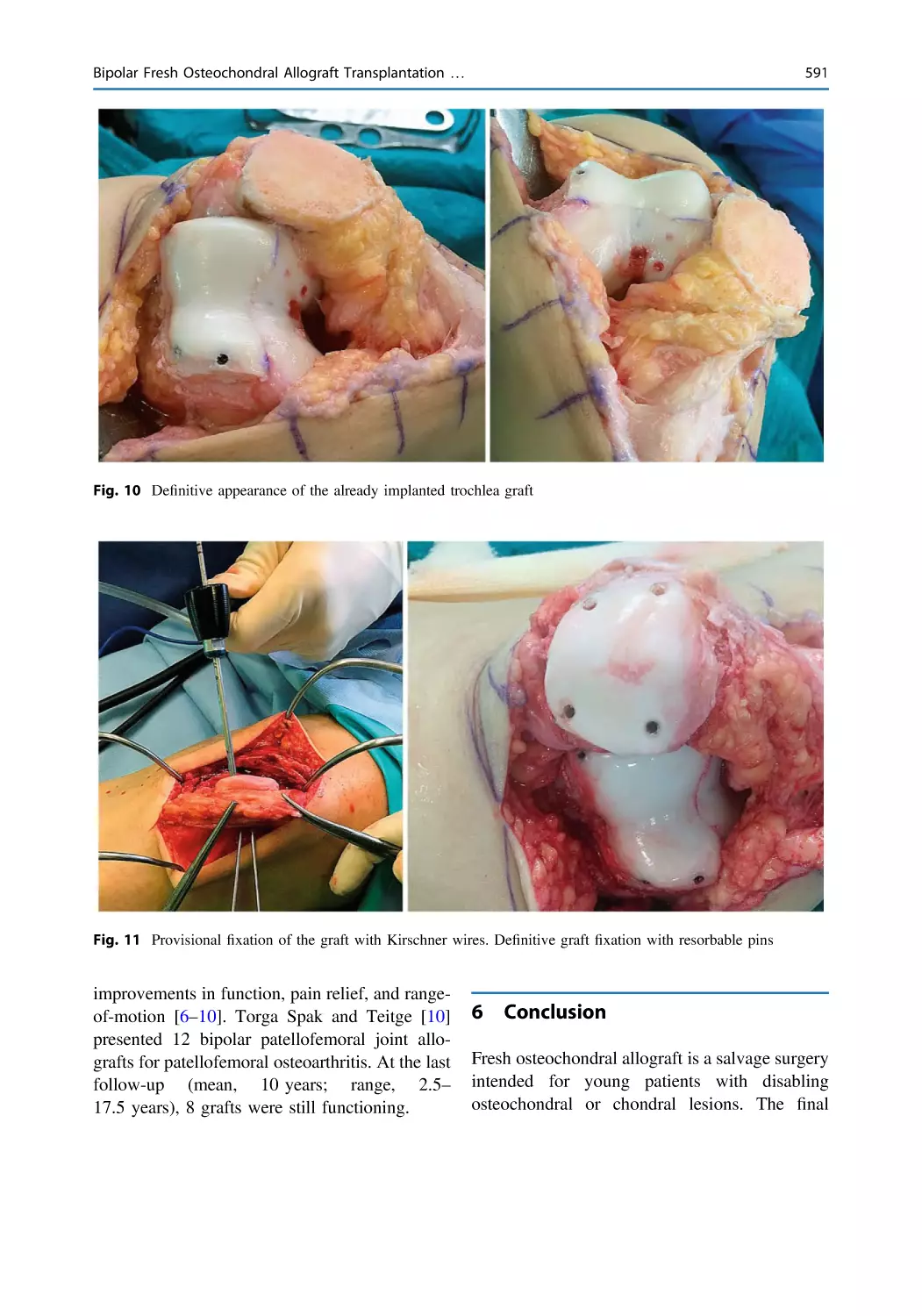
Bipolar Fresh Osteochondral Allograft Transplantation
of the Patellofemoral Joint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 585
Vicente Sanchis-Alfonso and Joan Carles Monllau
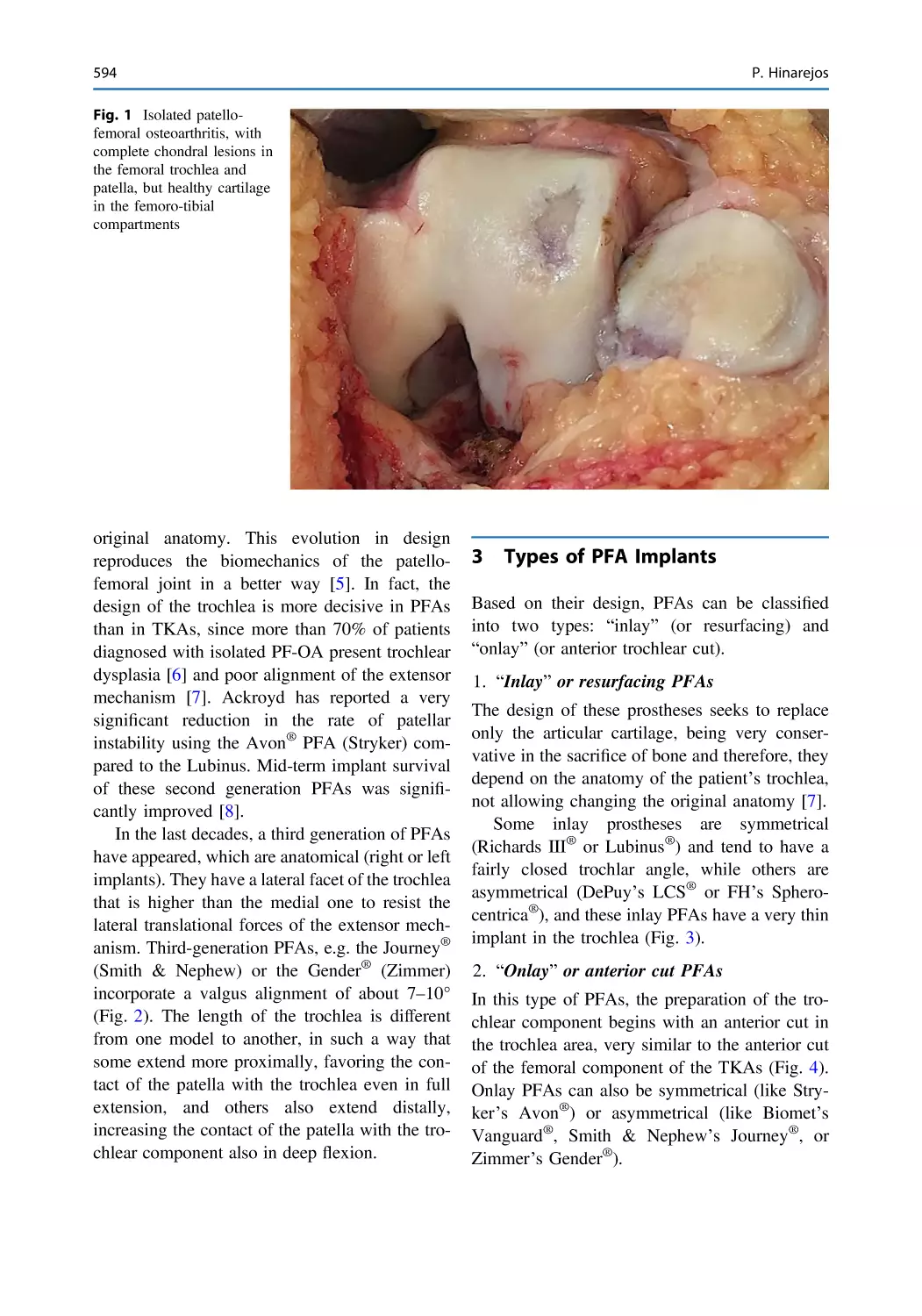
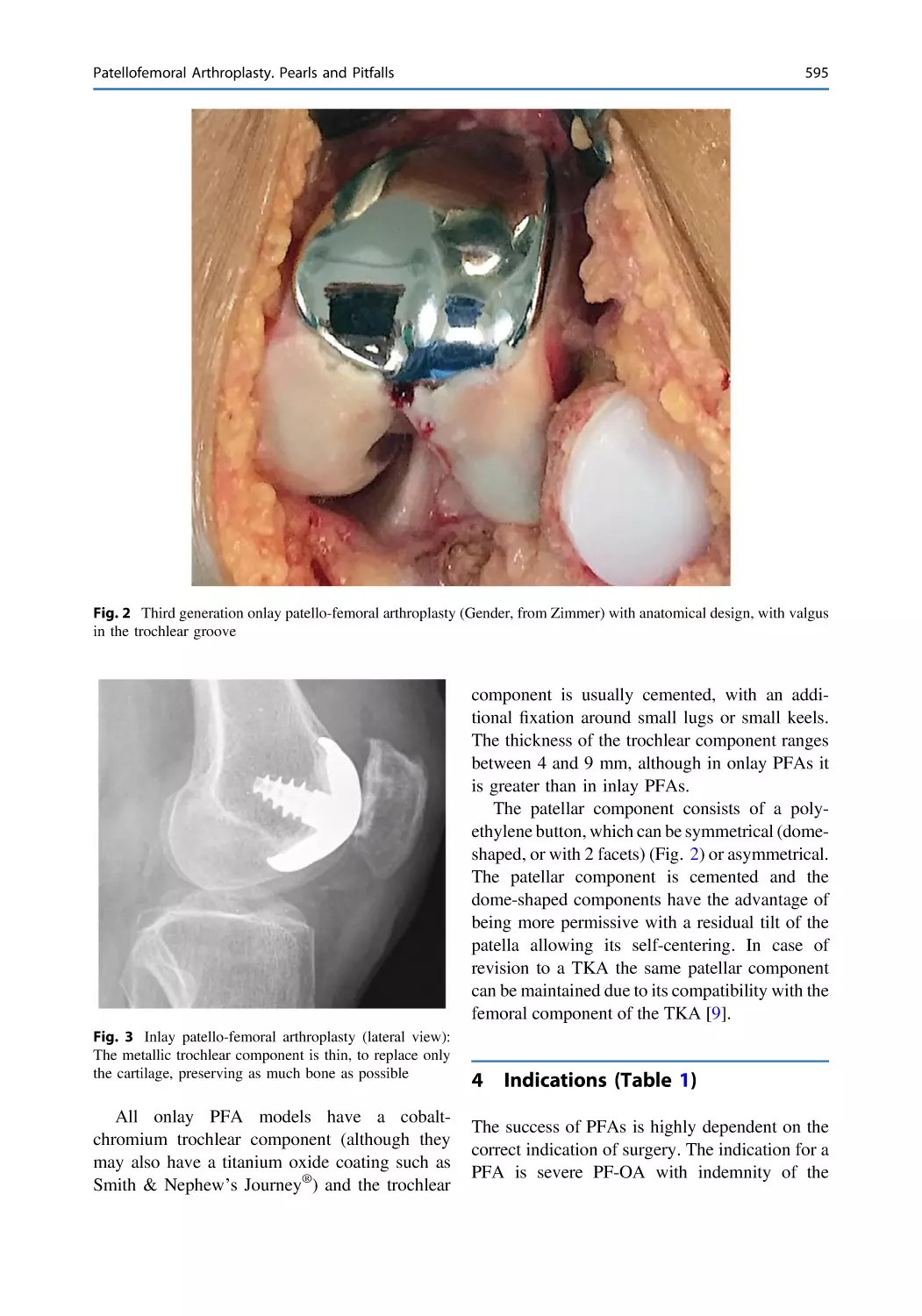
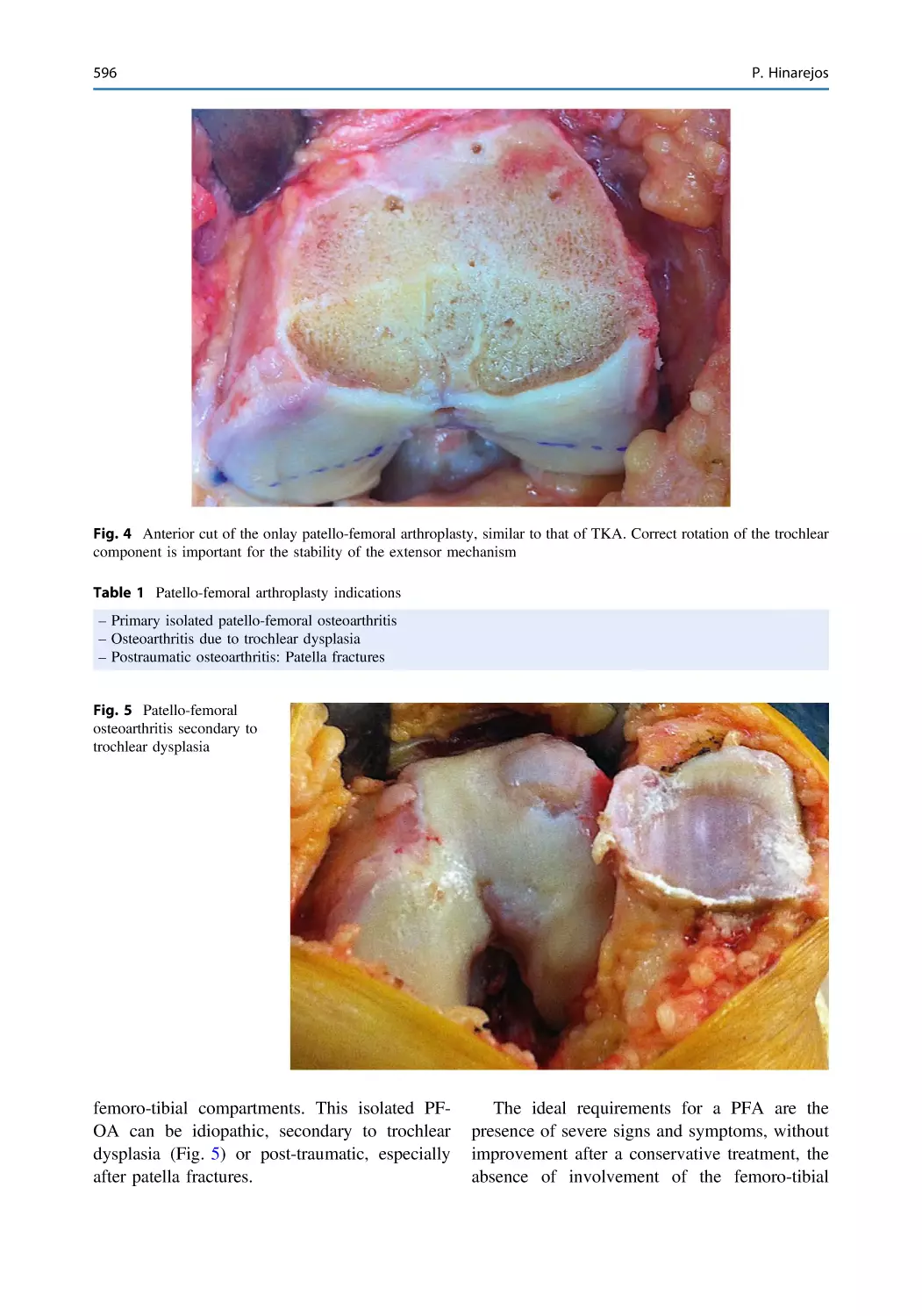
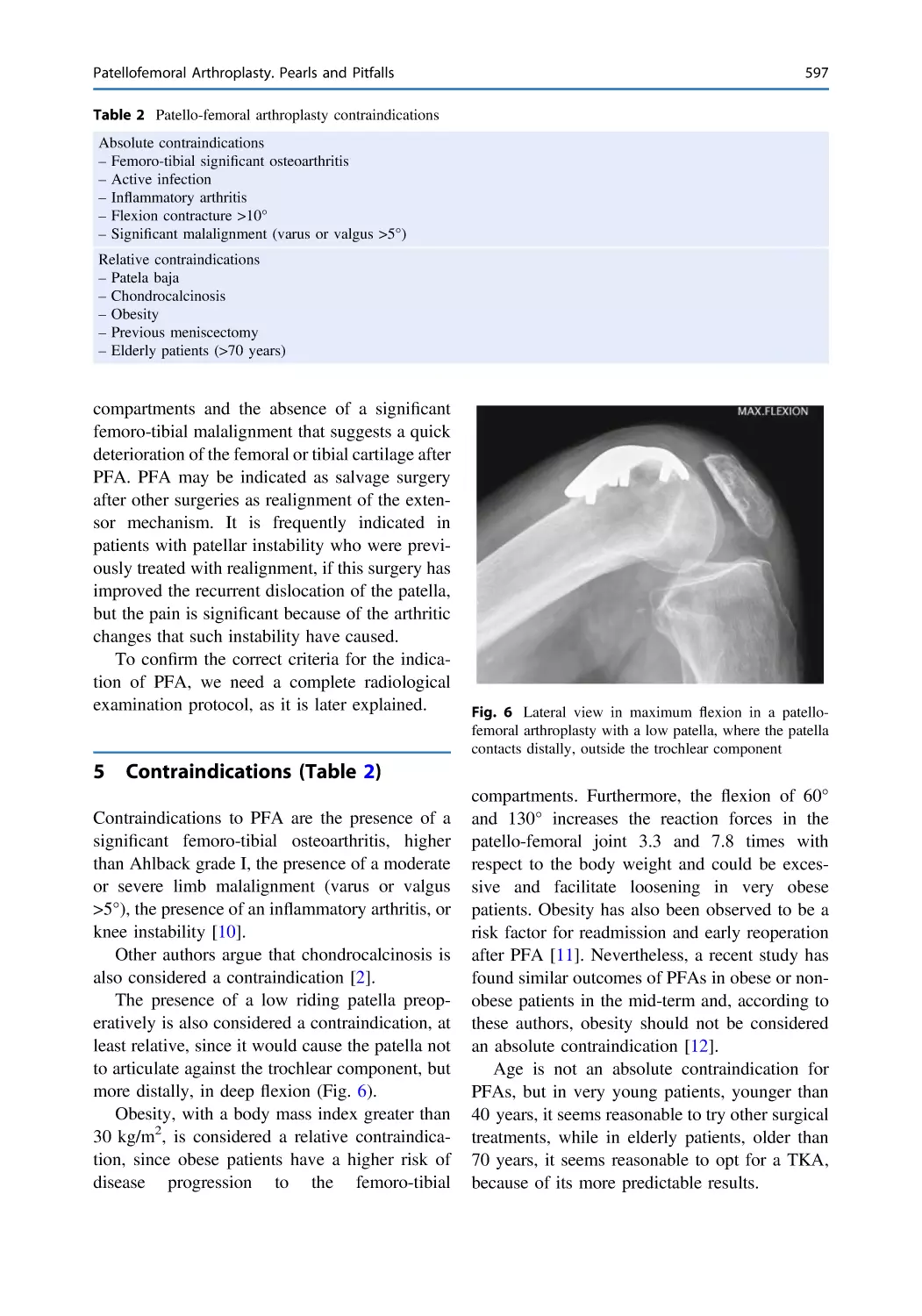
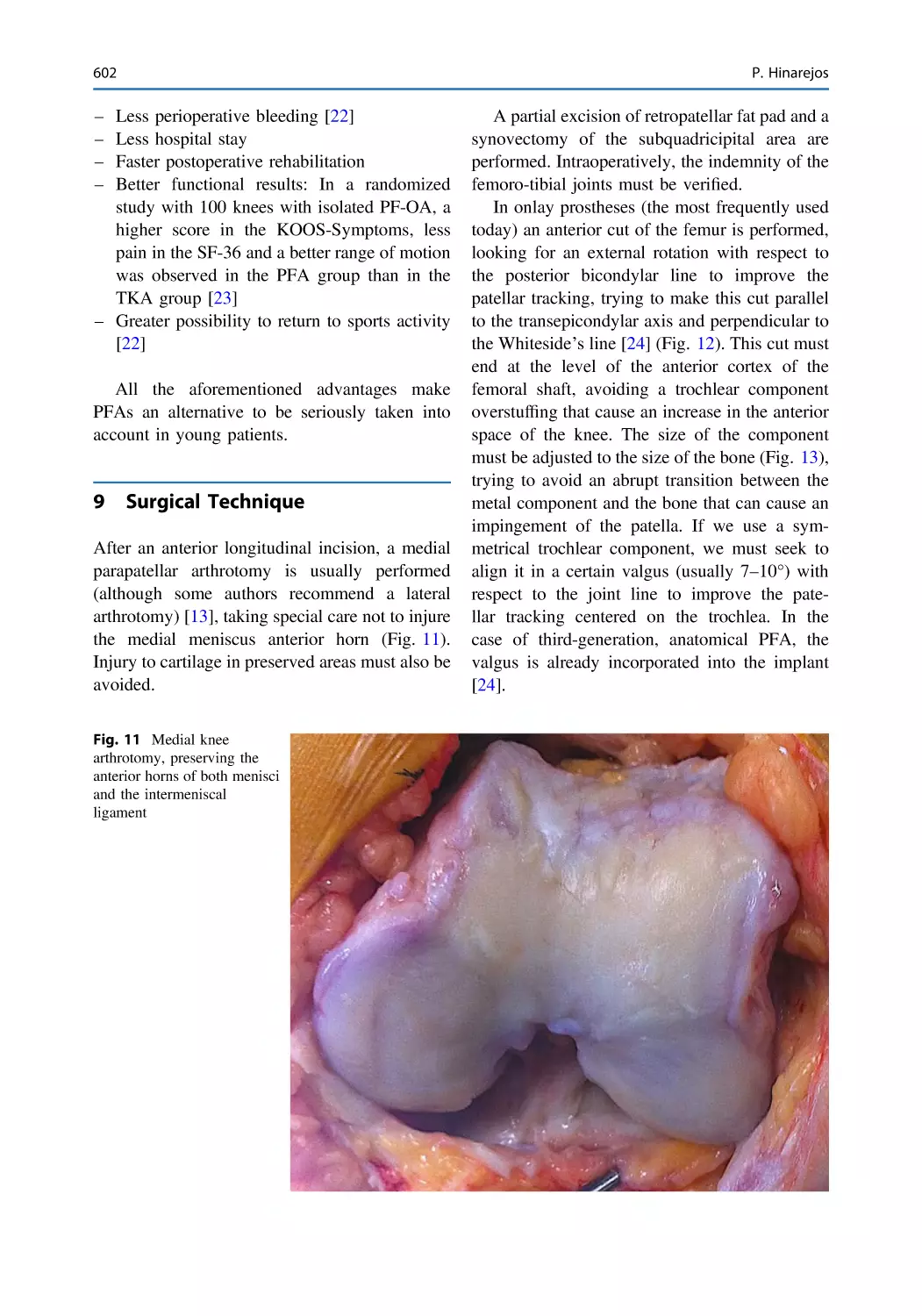
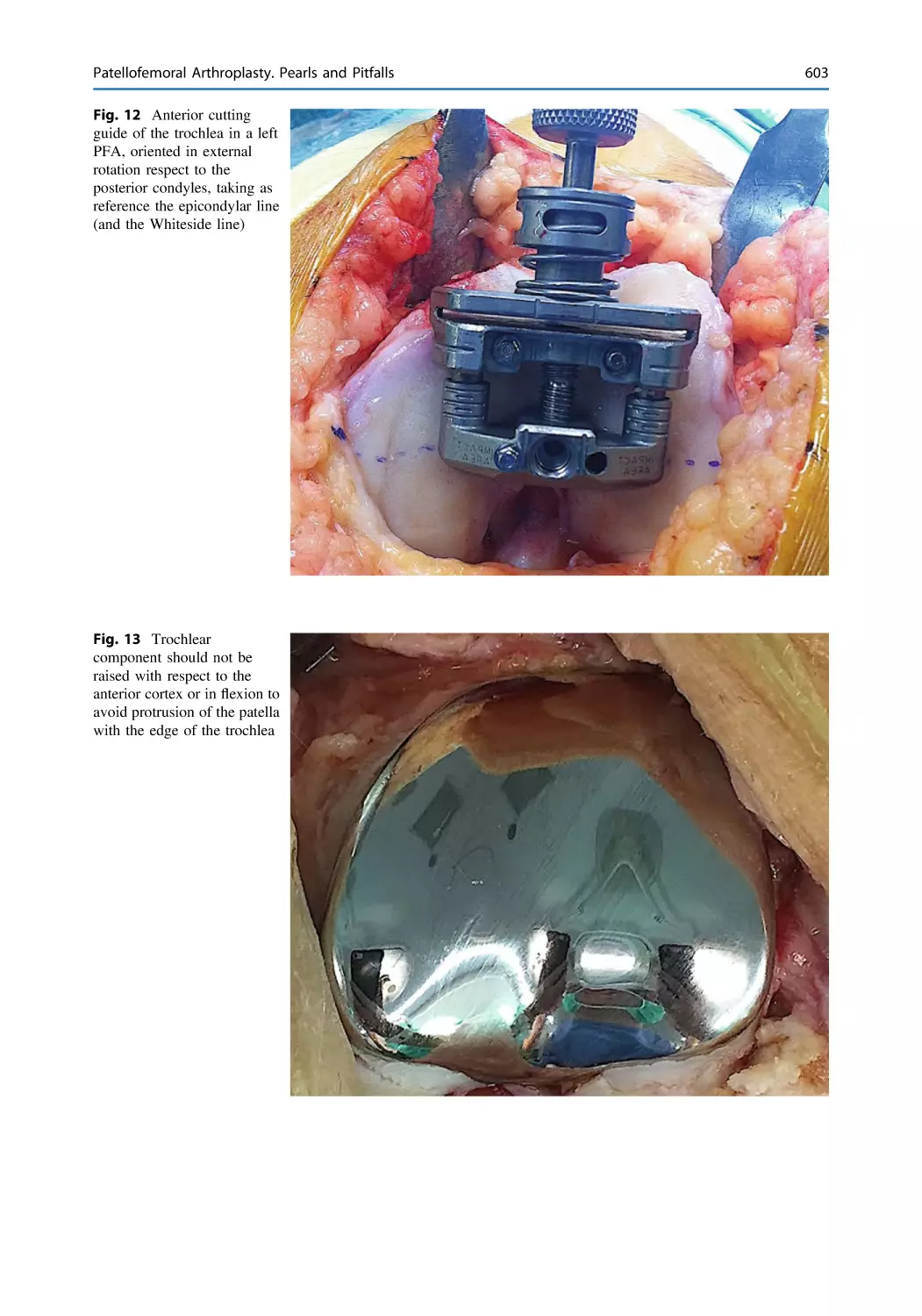
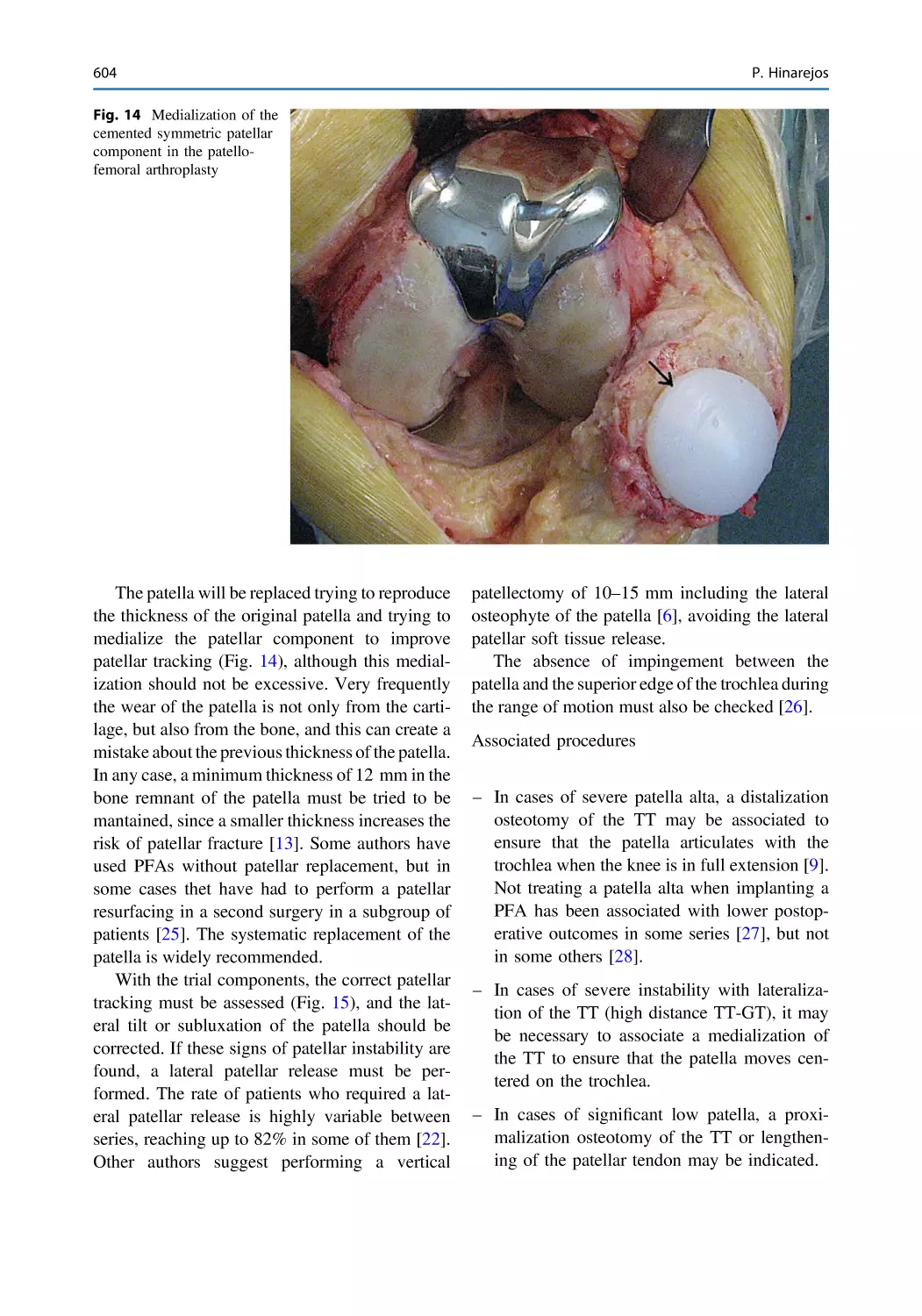
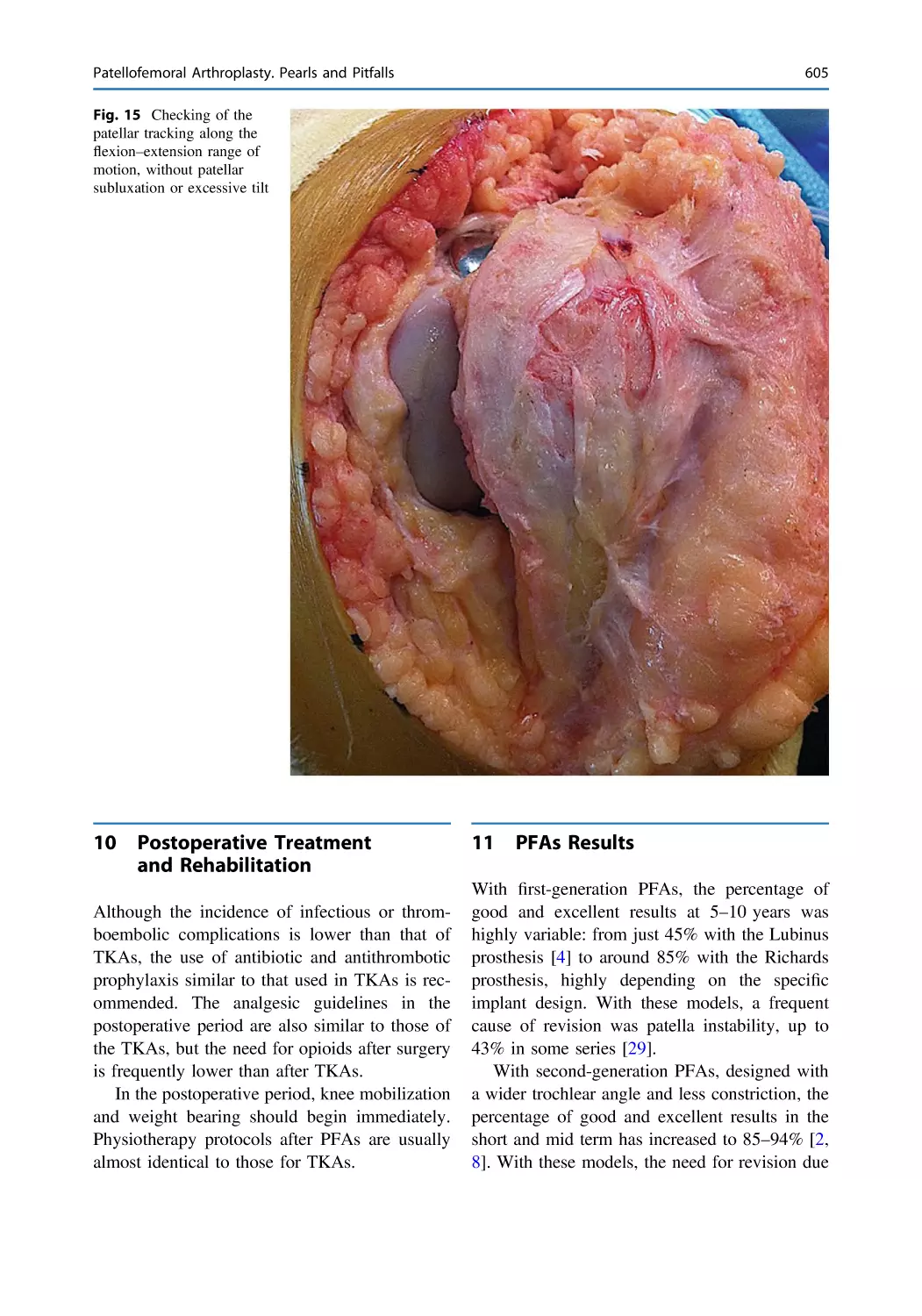
Patellofemoral Arthroplasty. Pearls and Pitfalls . . . . . . . . . . . . . . . 593
Pedro Hinarejos
Clinical Cases—Primary and Revision Patellofemoral Surgery
Patellofemoral Joint Preservation Surgery A Case-Based
Approach
Case # 1: Disabling Anterior Knee Pain After Failed MPFL
Reconstruction in a Patient with Patellar Chondropathy,
Femoral Anteversion and External Tibial Torsion . . . . . . . . . . . . . 615
Vicente Sanchis-Alfonso and Alejandro Roselló-Añón
Case # 2: Disabling Anterior Knee Pain Recalcitrant to
Conservative Treatment in a Patient with Patellofemoral
Osteoarthritis and Structural Femoral Retrotorsion
and Genu Varum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 623
Vicente Sanchis-Alfonso and Alejandro Roselló-Añón
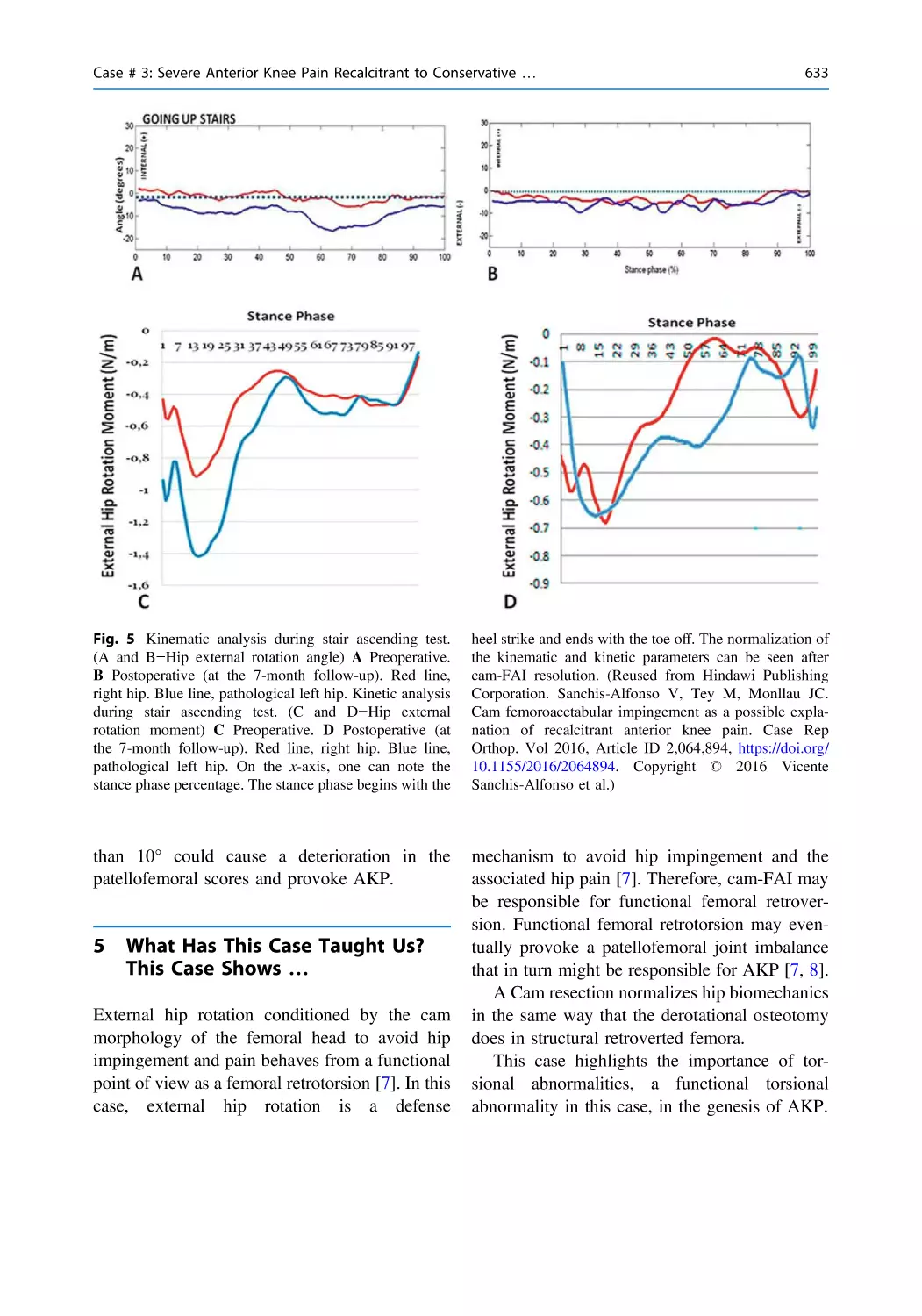
Case # 3: Severe Anterior Knee Pain Recalcitrant
to Conservative Treatment in a Patient with Functional
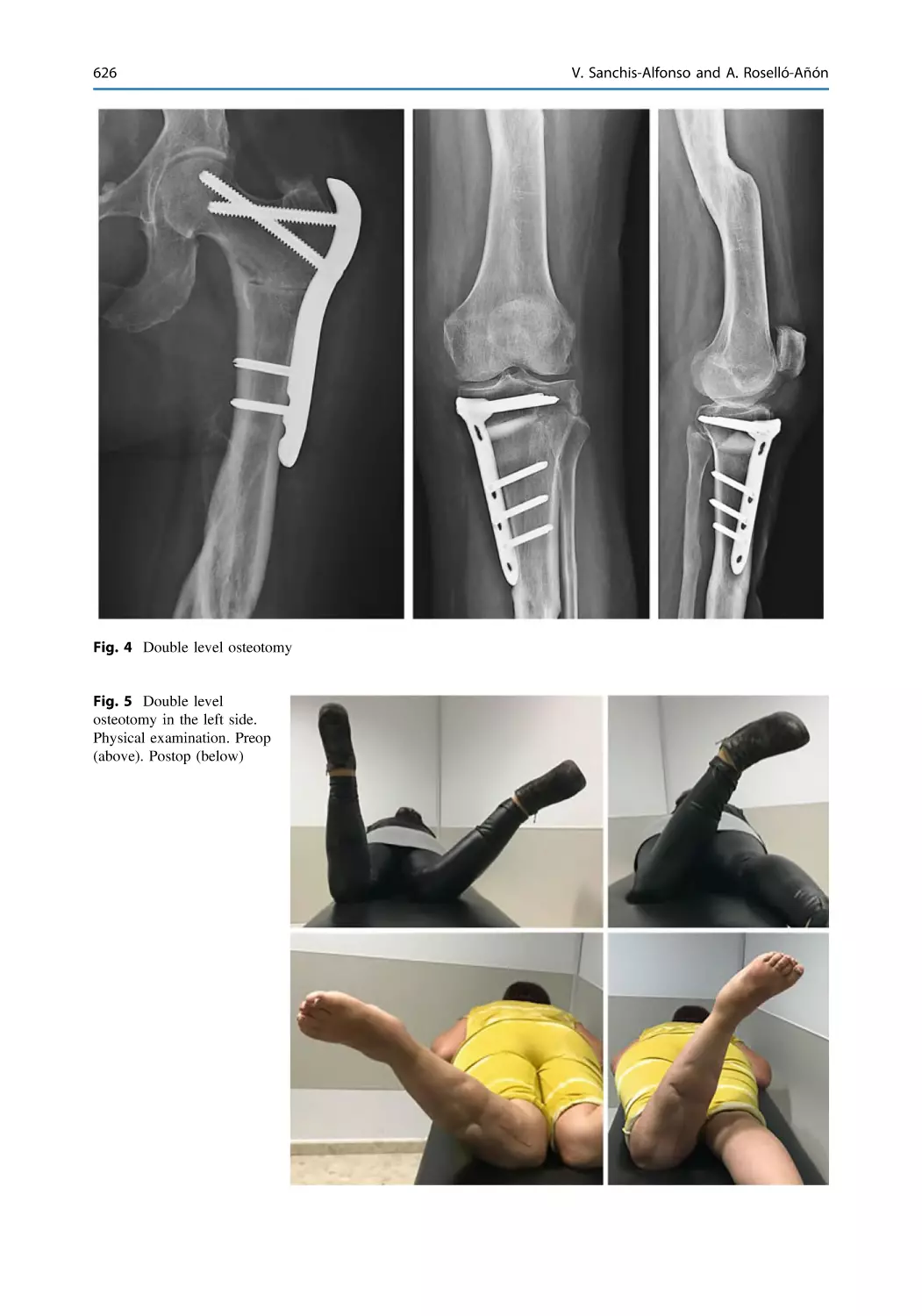
Femoral Retrotorsion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 629
Vicente Sanchis-Alfonso, Marc Tey-Pons, and Joan Carles Monllau
Case # 4: Disabling Anterior Knee Pain in a Multi-operated
Young Patient with Severe Patellofemoral Osteoarthritis
and Medial Patellar Instability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 635
Vicente Sanchis-Alfonso
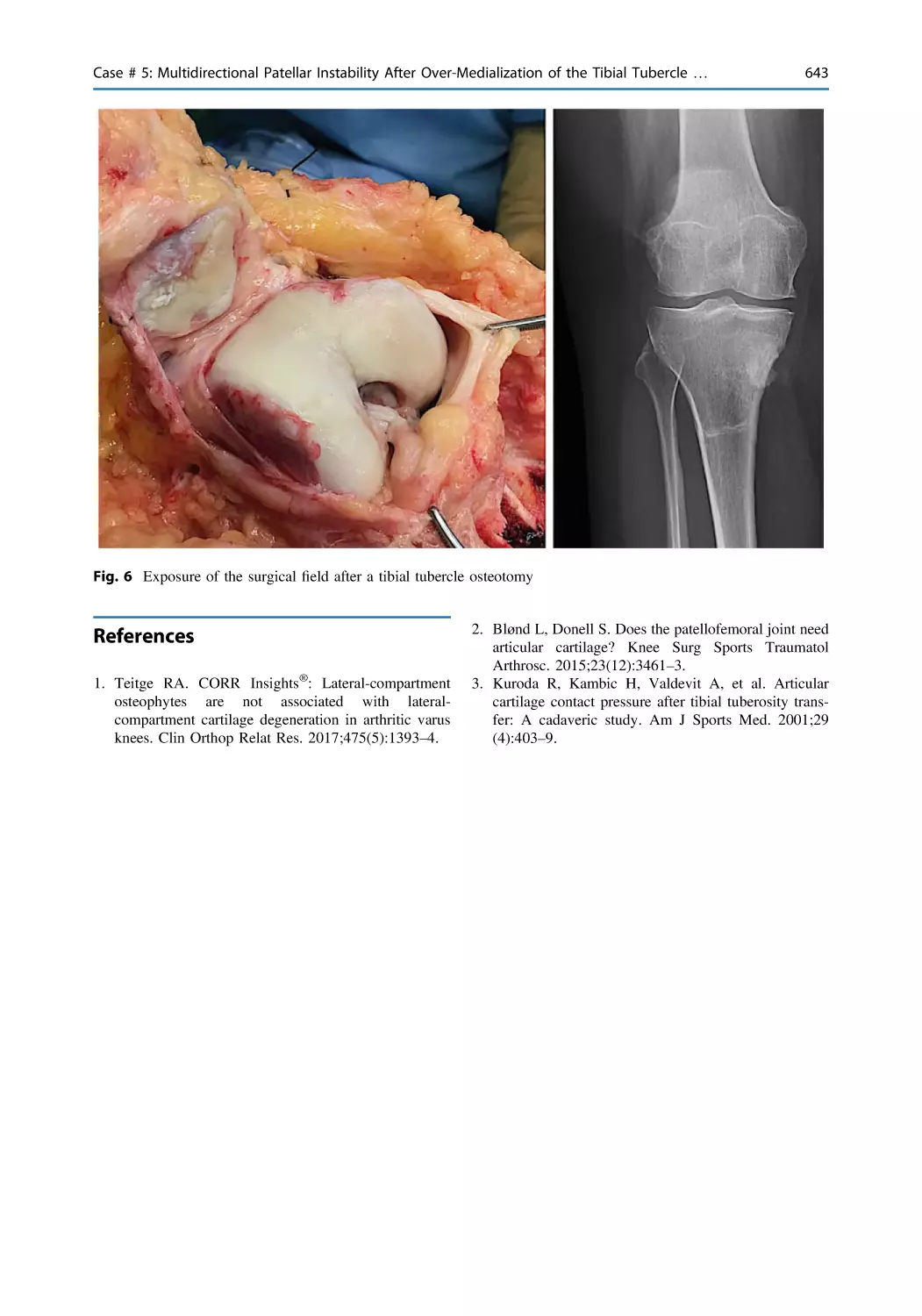
Case # 5: Multidirectional Patellar Instability After
Over-Medialization of the Tibial Tubercle in a Patient
with Severe Trochlear Dysplasia and Patella Alta . . . . . . . . . . . . . 639
Vicente Sanchis-Alfonso
Case # 6: Failed MPFL Reconstruction in a Patient with Severe
Trochlear Dysplasia and Malpositioning of the Femoral
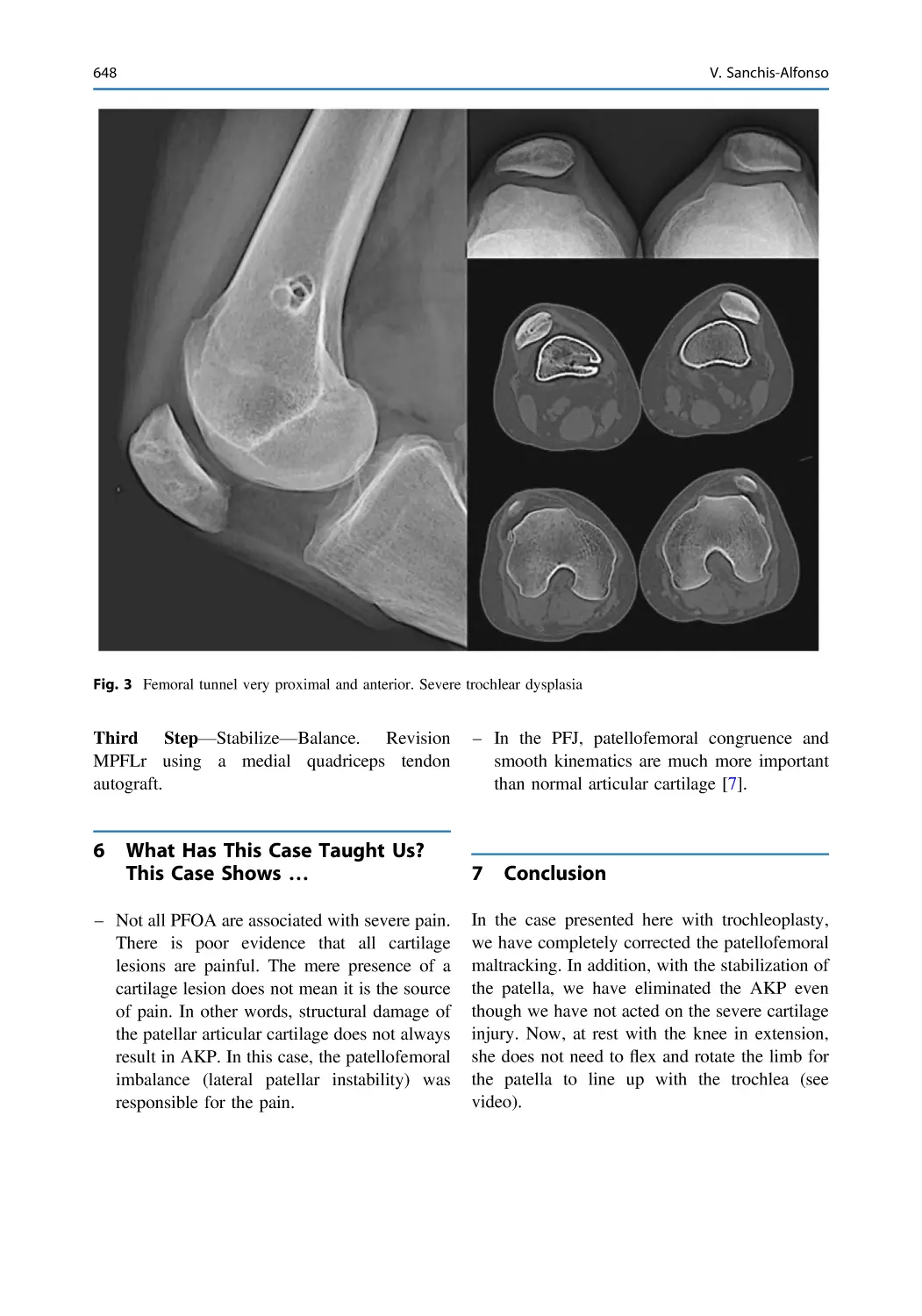
Attachment Point. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 645
Vicente Sanchis-Alfonso
Contents
Contents
xxv
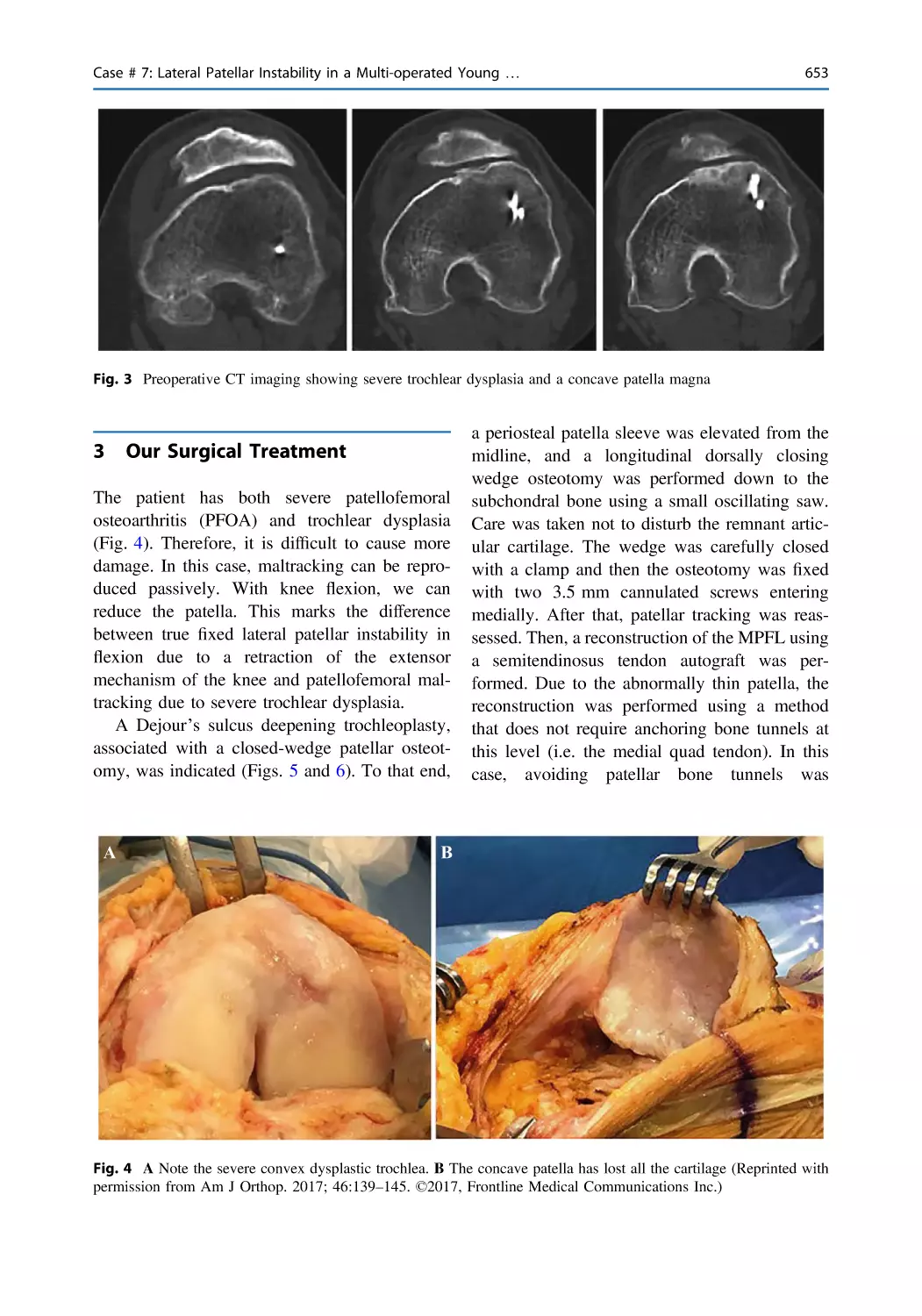
Case # 7: Lateral Patellar Instability in a Multi-operated Young
Patient with Severe Patellofemoral Osteoarthritis and Severe
Trochlear Dysplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 651
Vicente Sanchis-Alfonso and Joan Carles Monllau
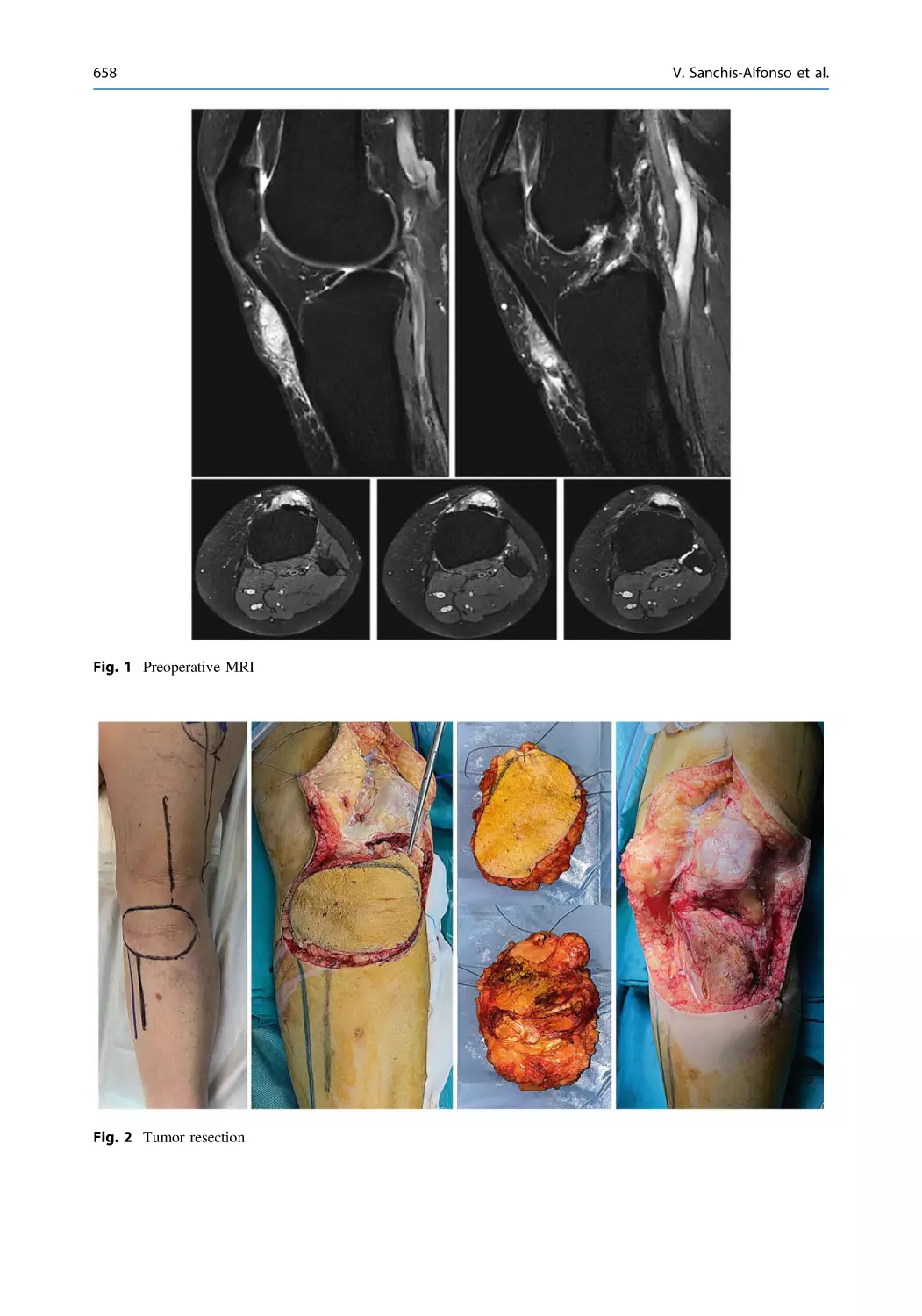
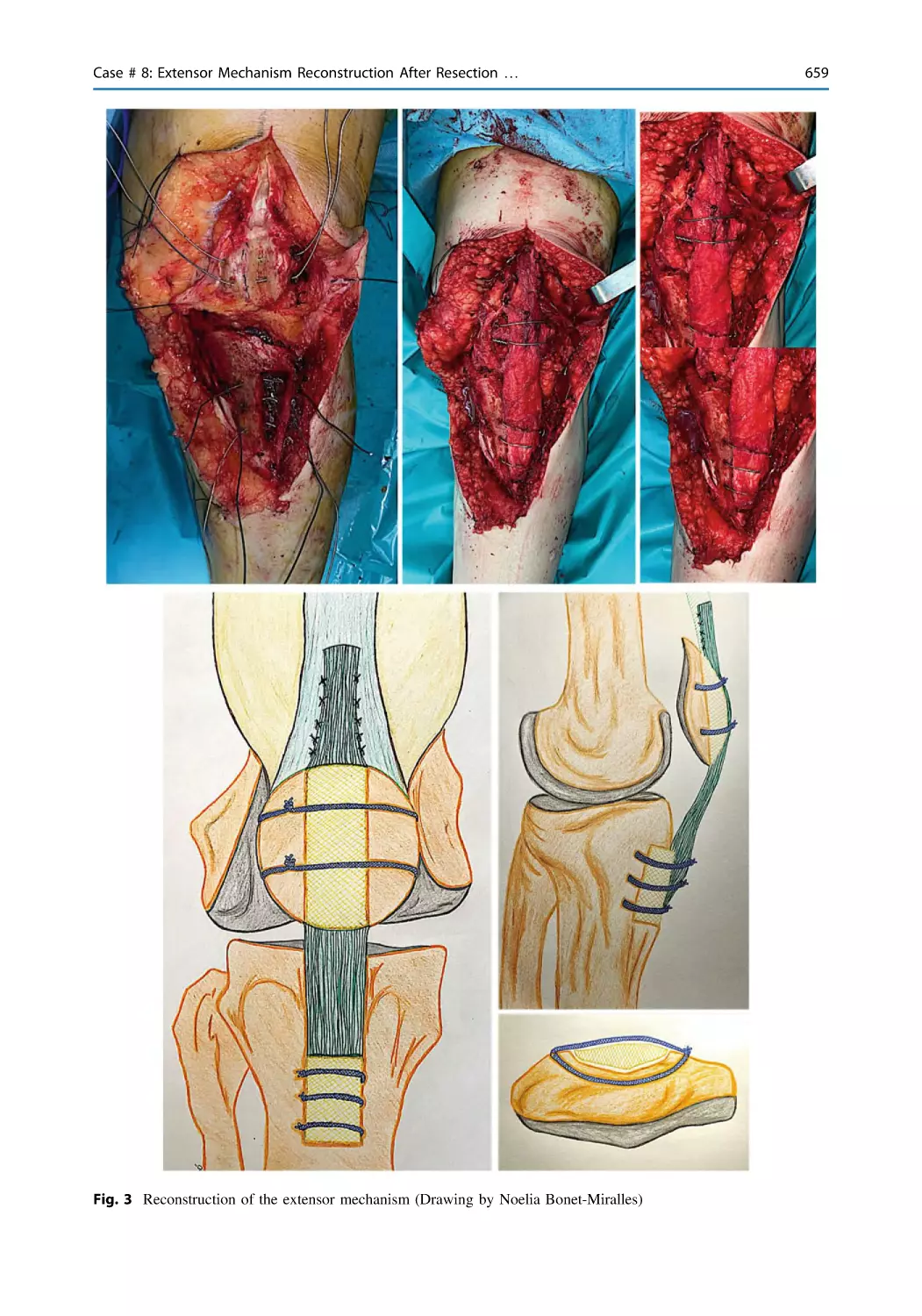
Case # 8: Extensor Mechanism Reconstruction After Resection
of a Soft Tissue Sarcoma that Infiltrates the Patellar Tendon . . . . 657
Vicente Sanchis-Alfonso, Alejandro Roselló-Añón,
Eloisa Villaverde-Doménech, Onofre Sanmartin,
and Juan Pablo Aracil-Kessler
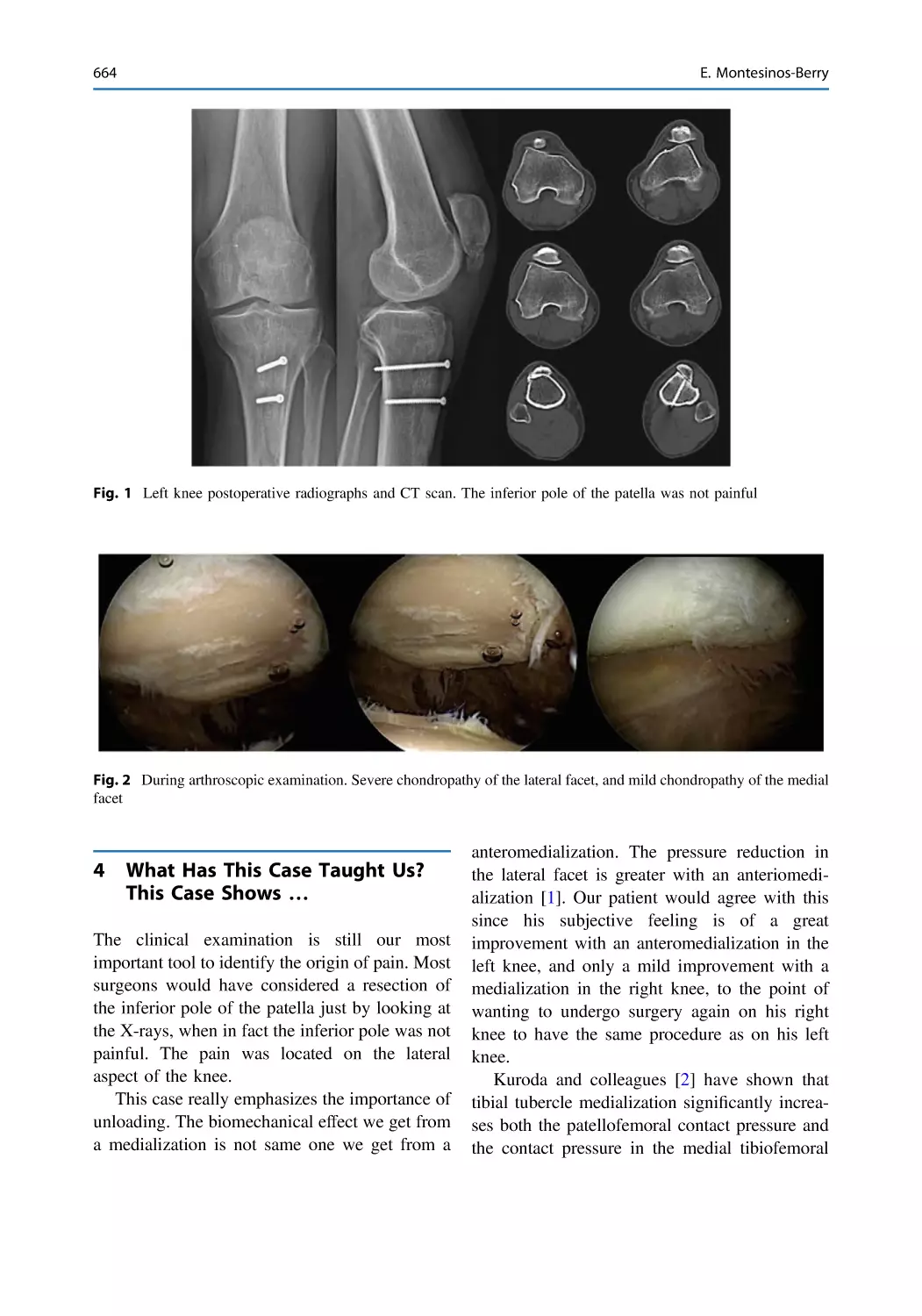
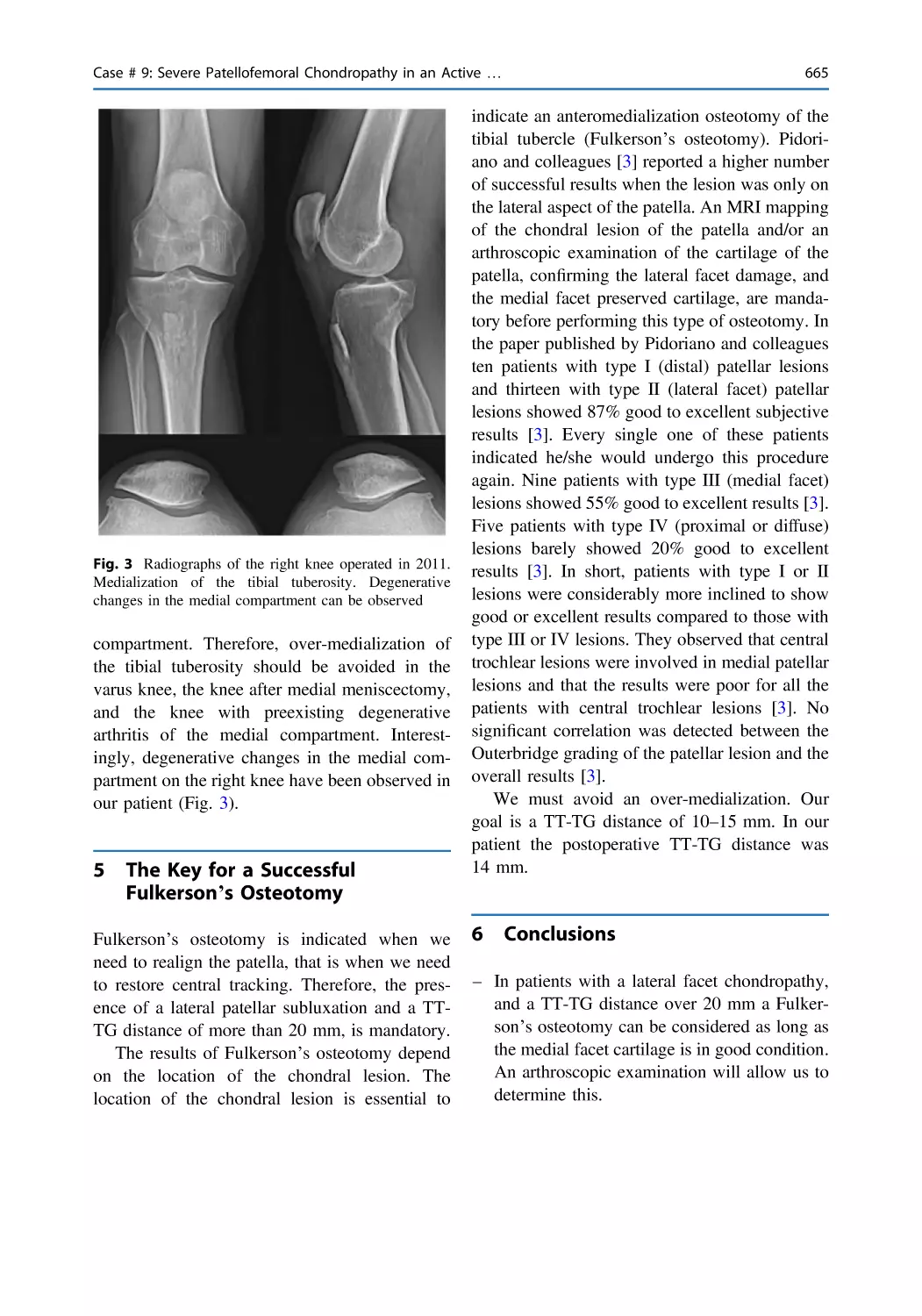
Case # 9: Severe Patellofemoral Chondropathy in an Active
47-Year-Old Patient . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 663
Erik Montesinos-Berry
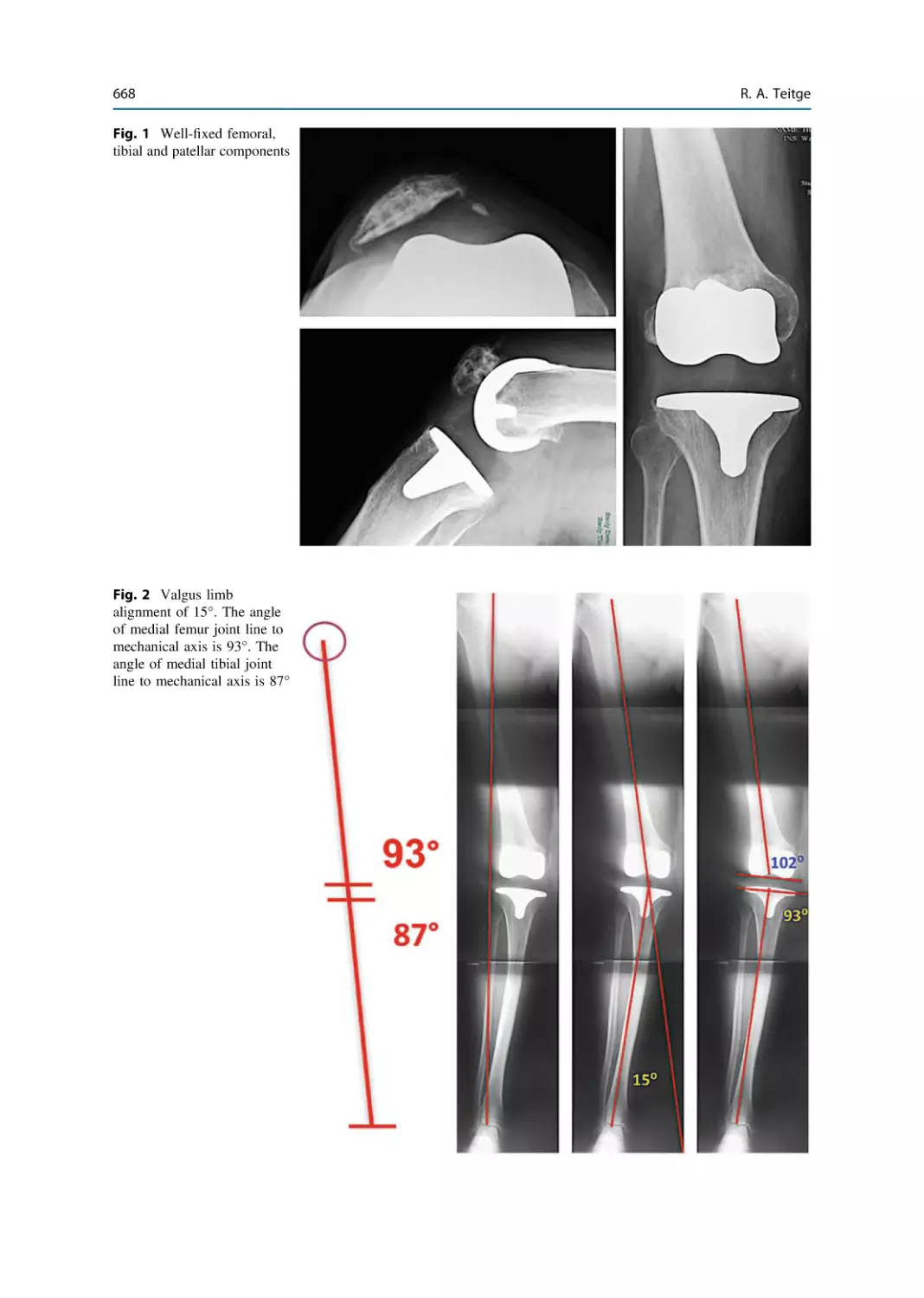
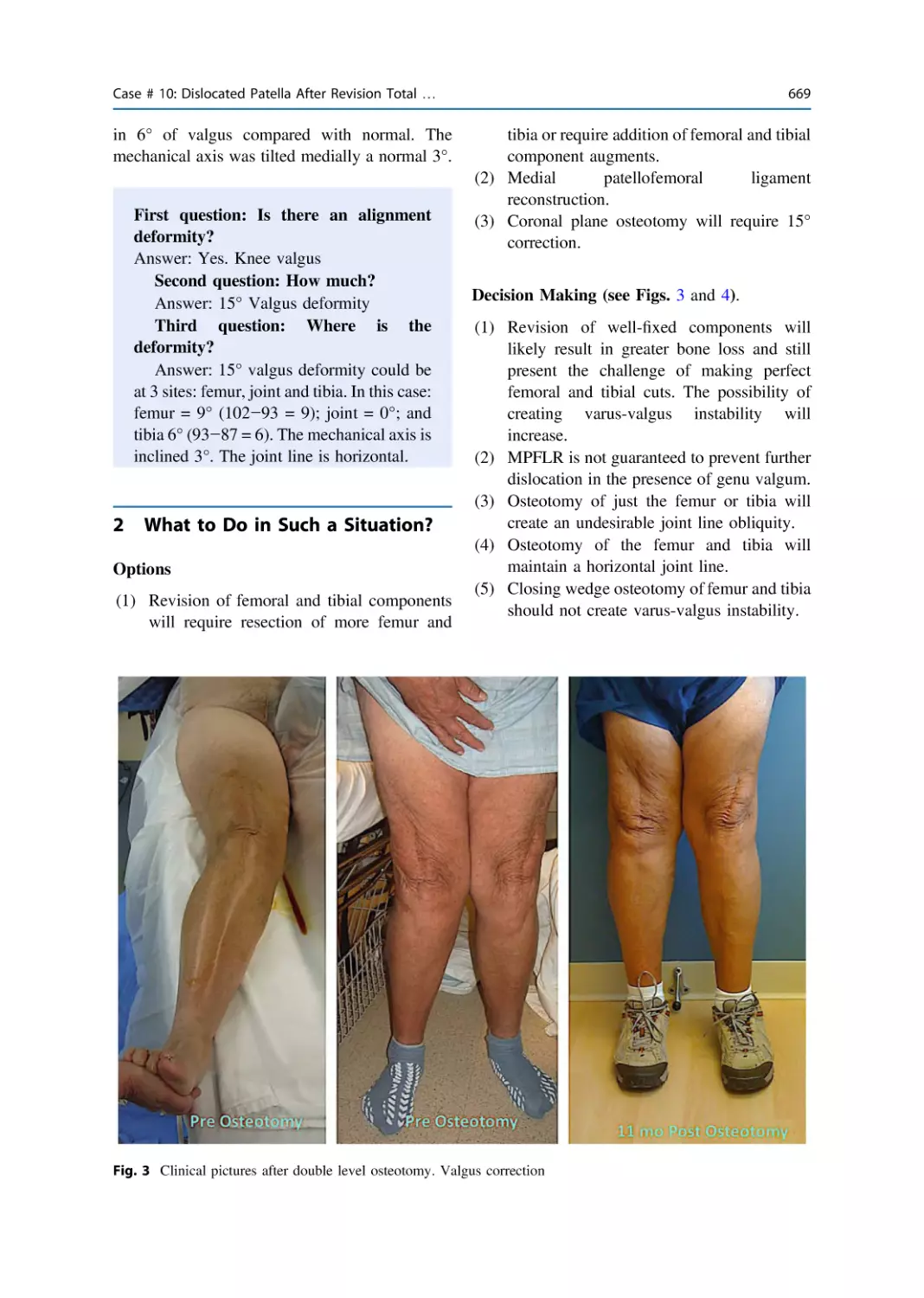
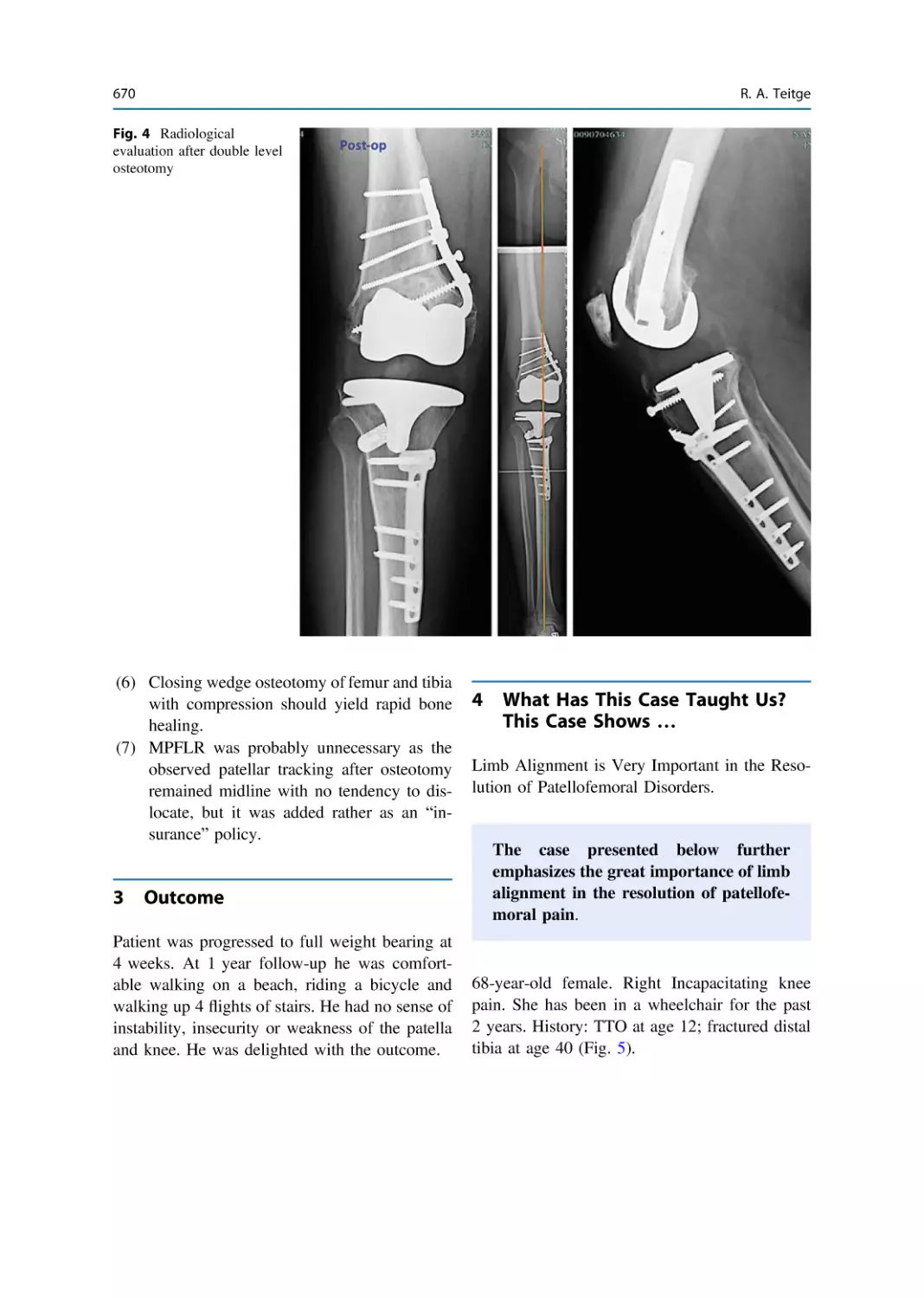
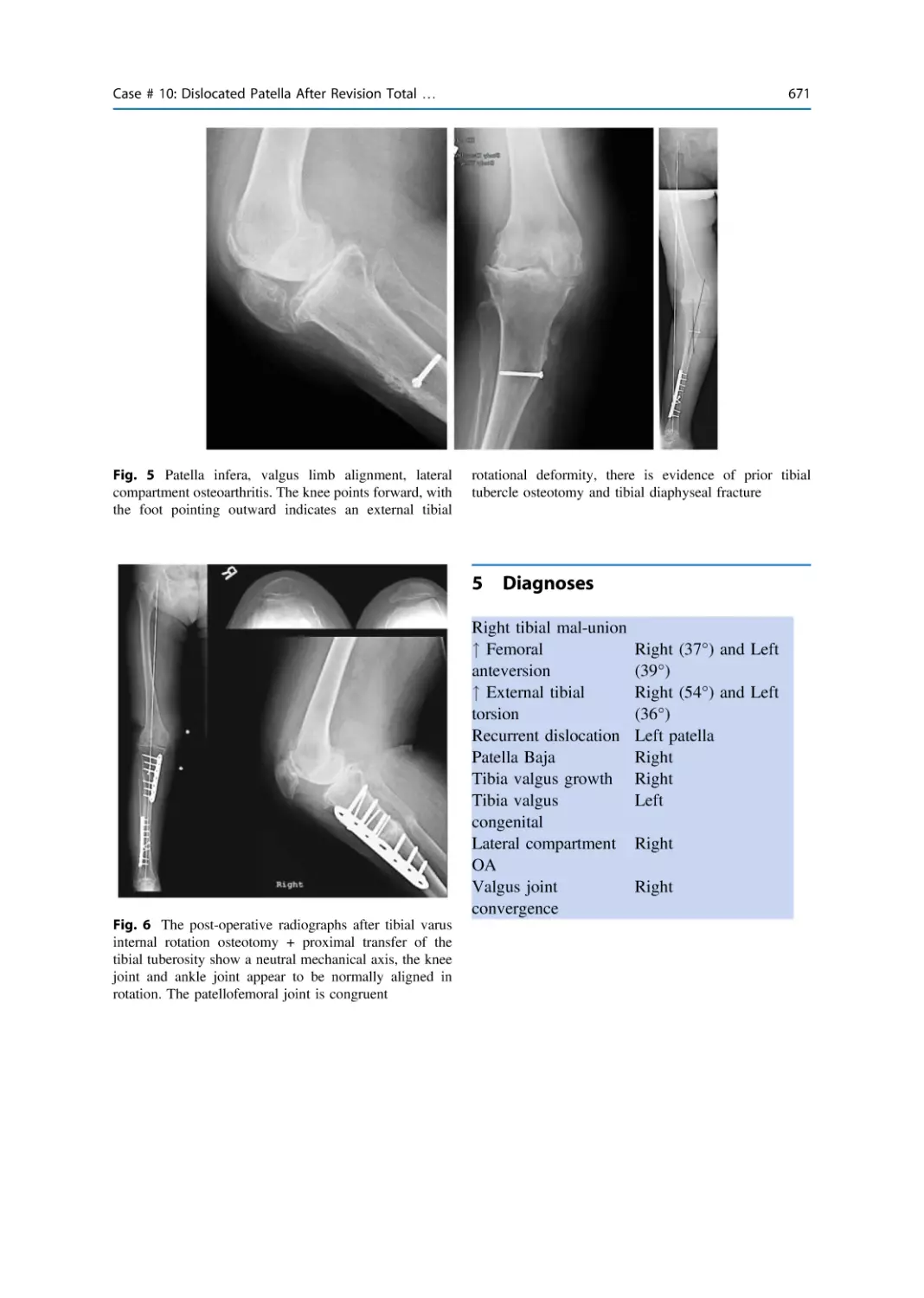
Case # 10: Dislocated Patella After Revision Total Knee
Arthroplasty. Case # 11: Patella Baja and Valgus Limb
56 Years After Tibial Tubercle Transfer . . . . . . . . . . . . . . . . . . . . . 667
Robert A. Teitge
New Frontiers in Anterior Knee Pain, Patellar Instability
and Patellofemoral Osteoarthritis Evaluation and Treatment
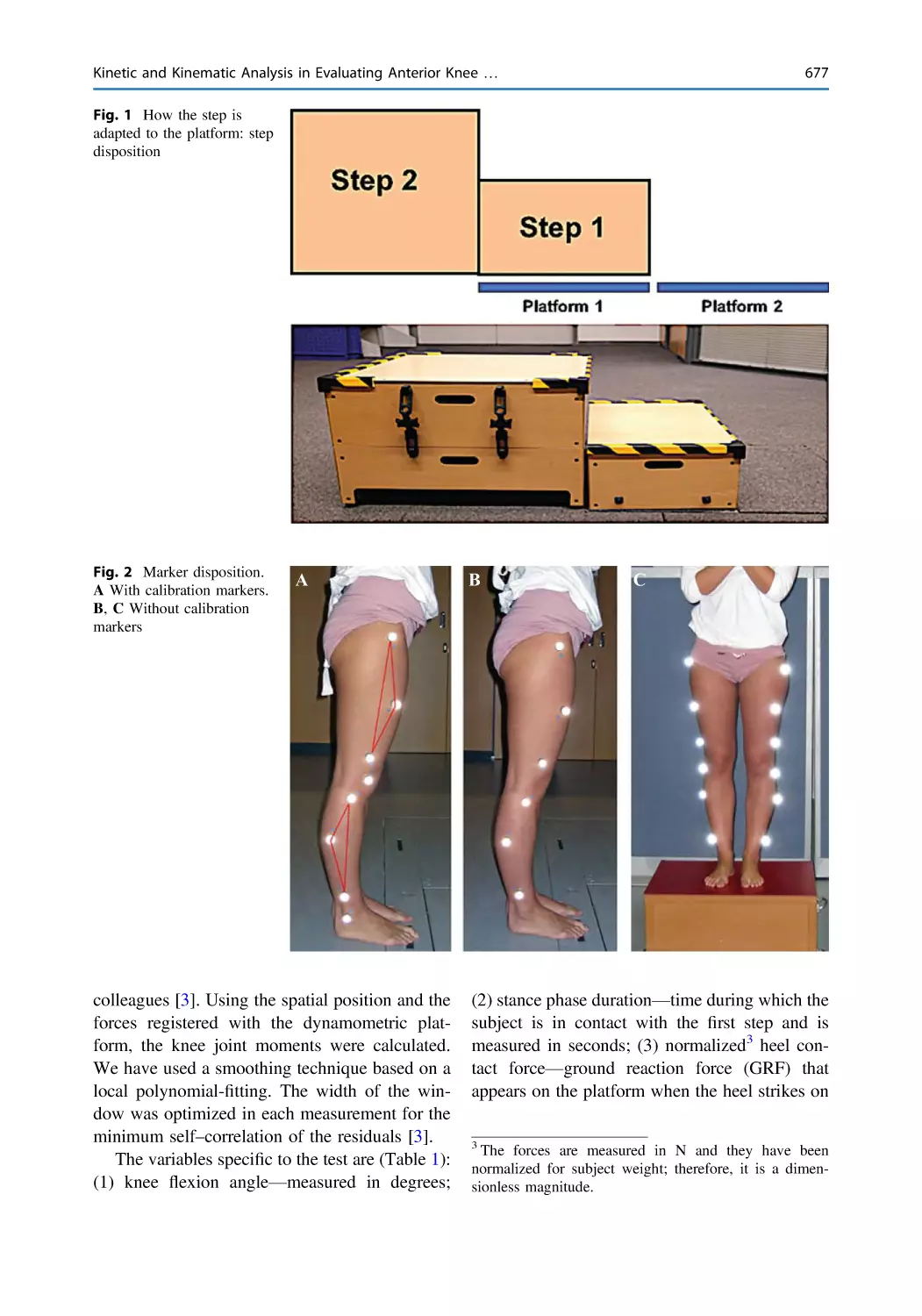
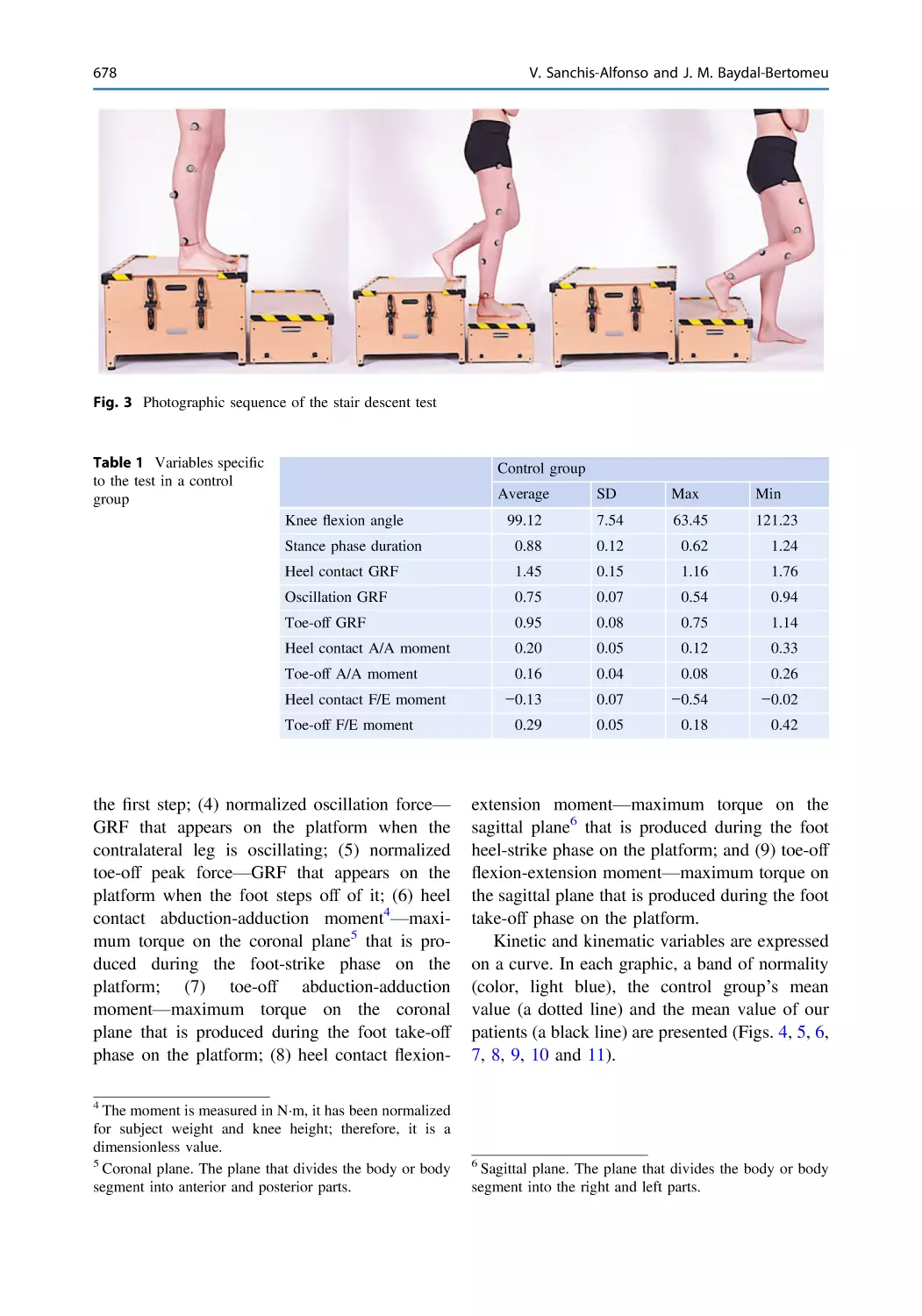
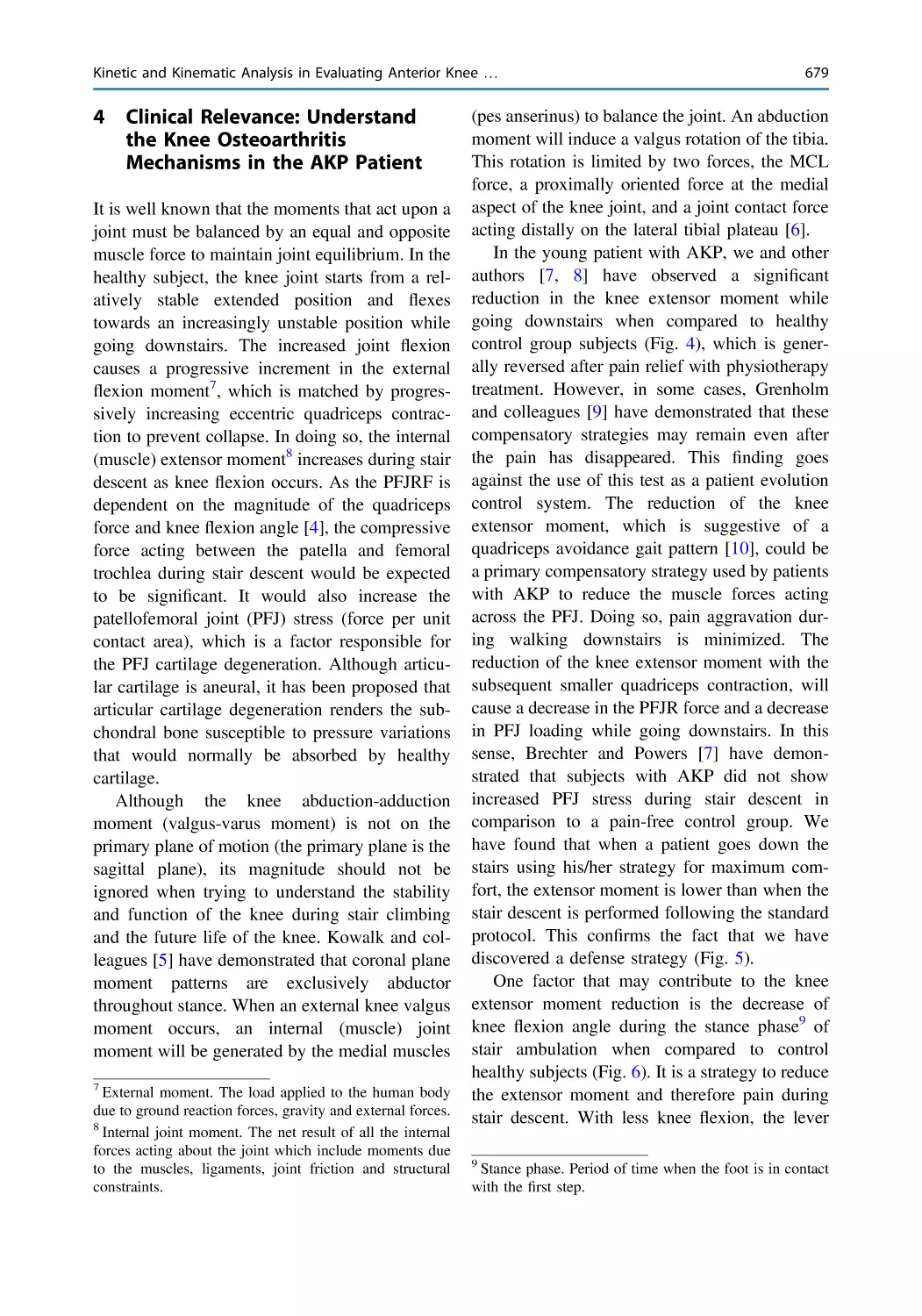
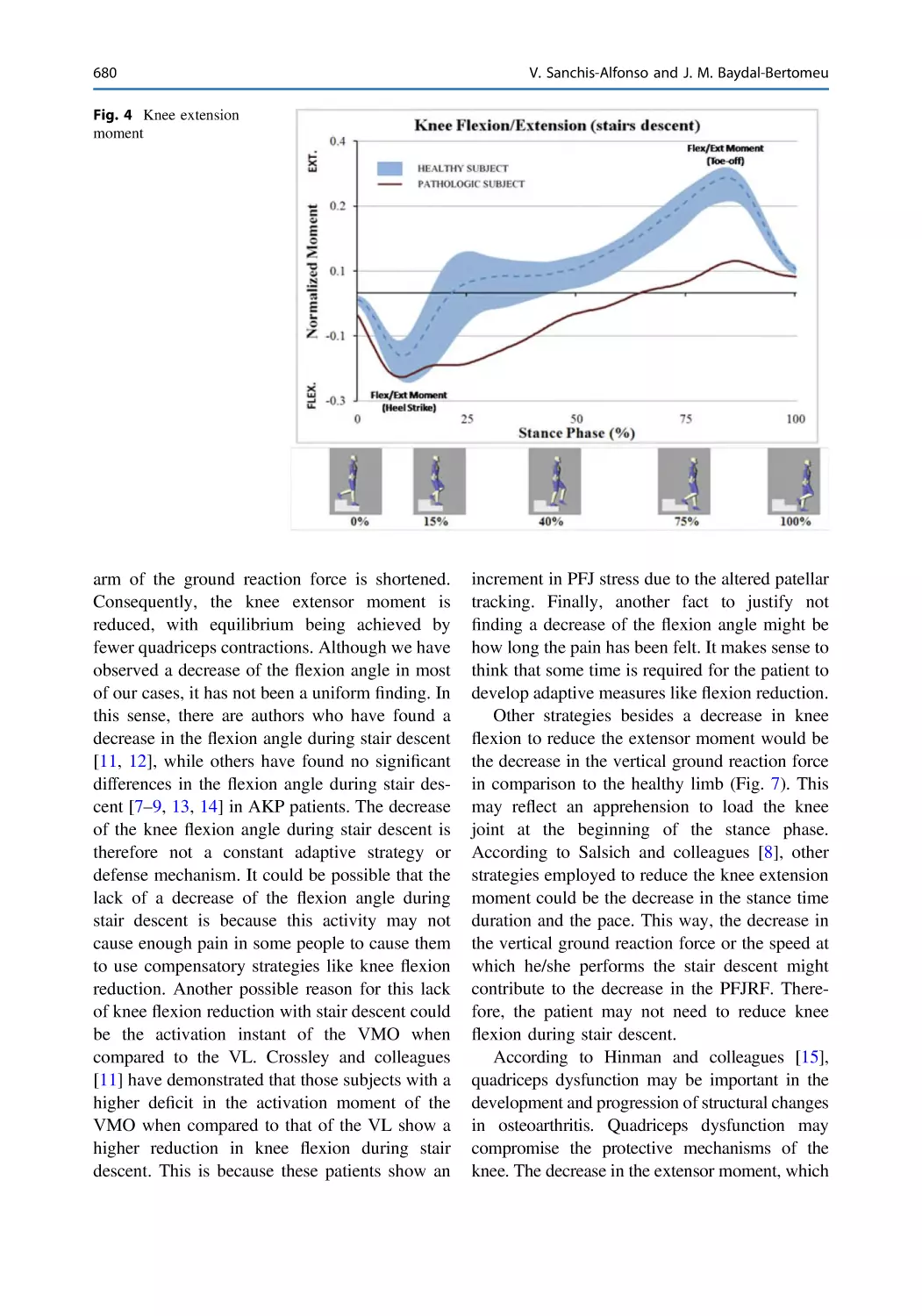
Kinetic and Kinematic Analysis in Evaluating Anterior Knee
Pain Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 675
Vicente Sanchis-Alfonso and Jose María Baydal-Bertomeu
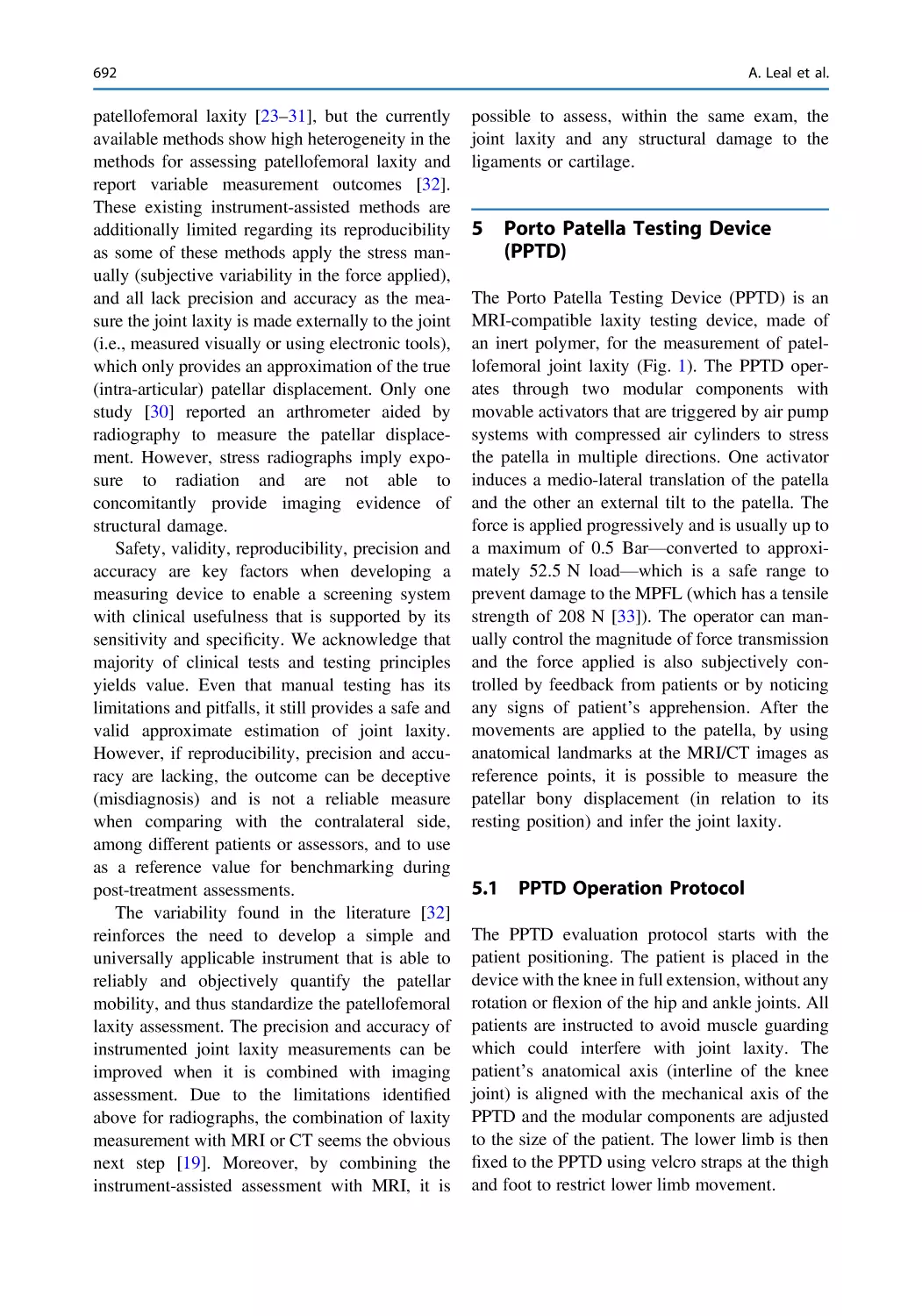
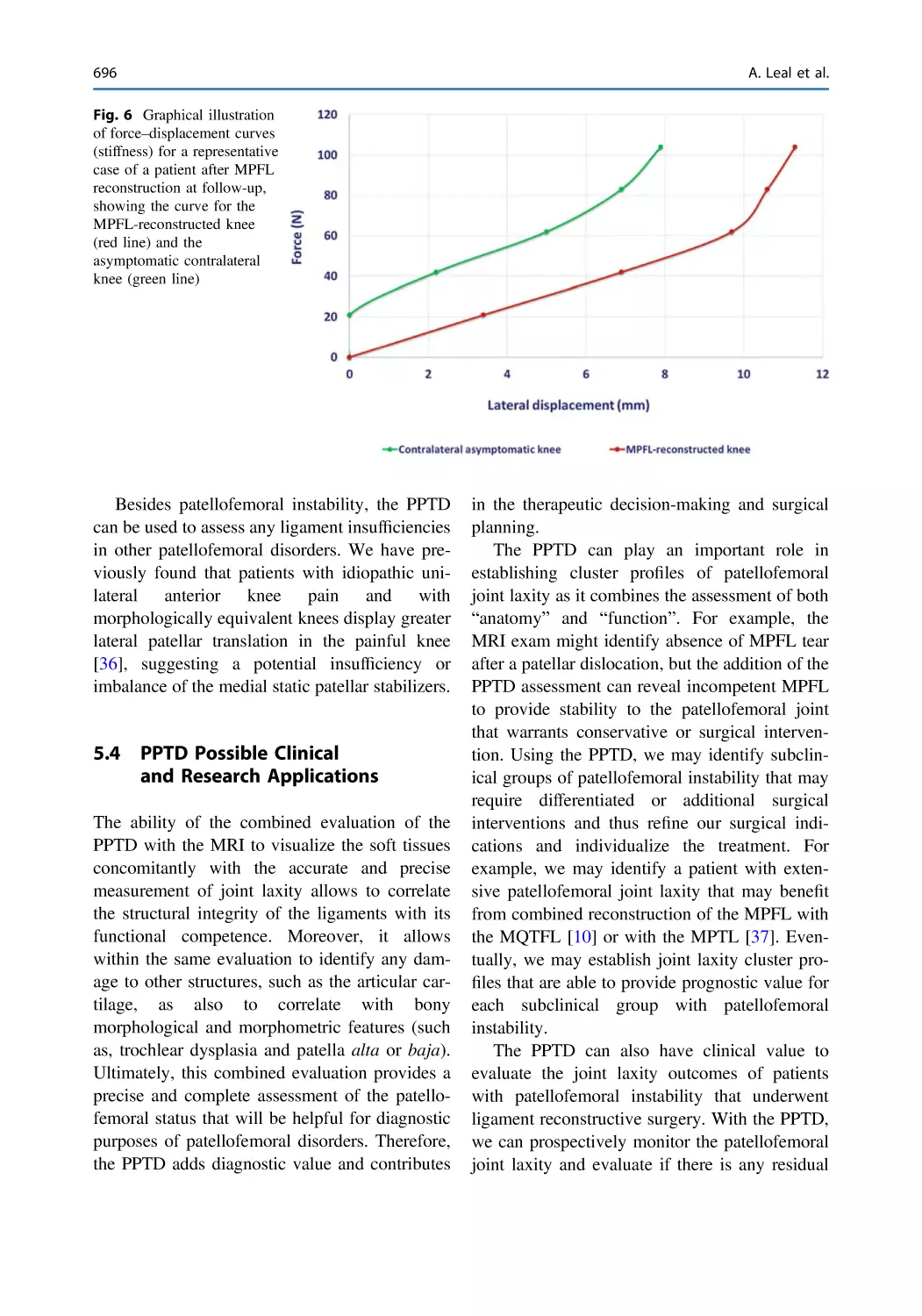
Patellofemoral Instrumented Stress Testing . . . . . . . . . . . . . . . . . . 689
Ana Leal, Renato Andrade, Cristina Valente, André Gismonti,
Rogério Pereira, and João Espregueira-Mendes
Anterior Knee Pain and Functional Femoral Maltorsion
in Patients with Cam Femoroacetabular Impingement . . . . . . . . . . 699
Marc Tey-Pons, Vicente Sanchis-Alfonso, and Joan Carles Monllau
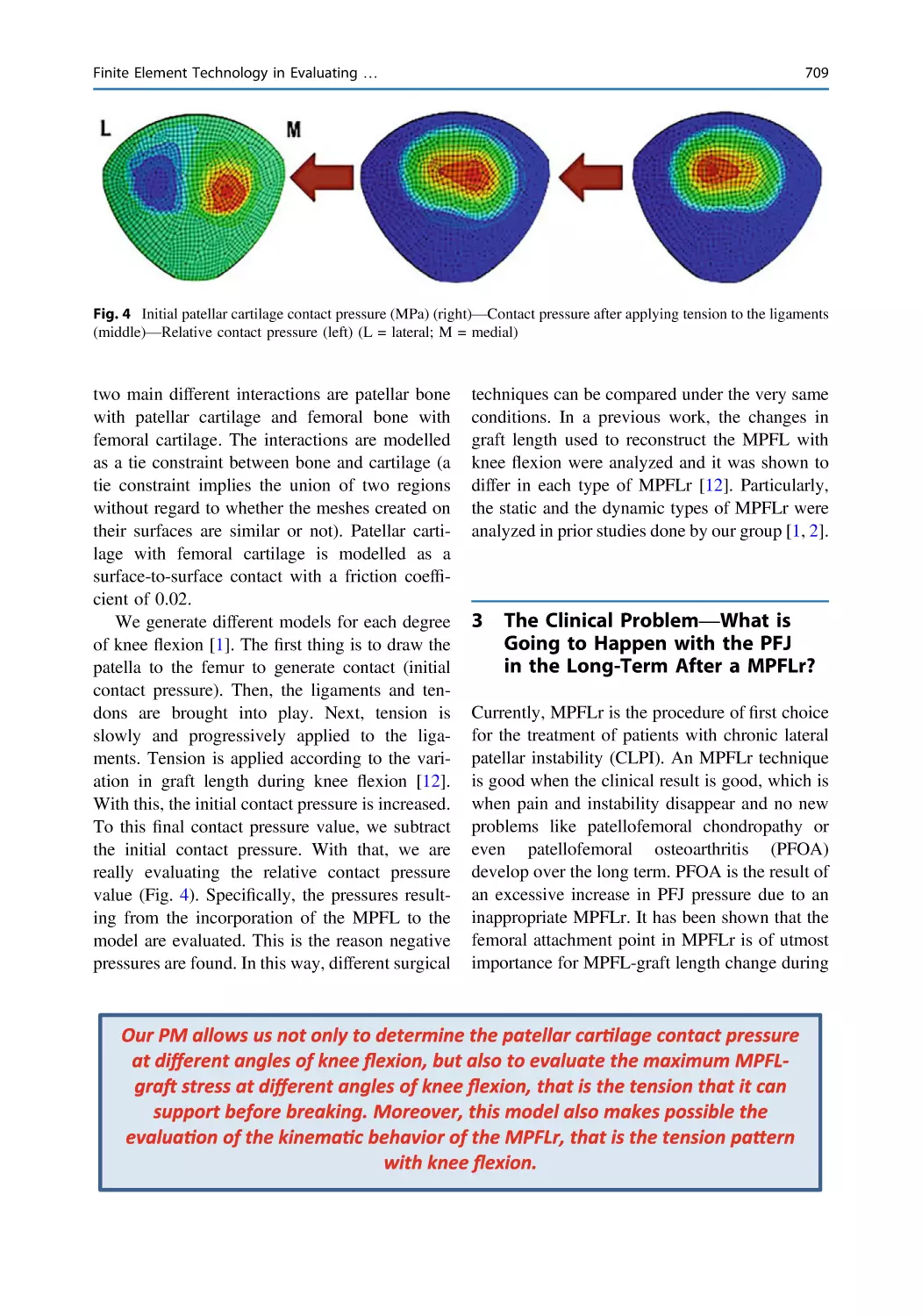
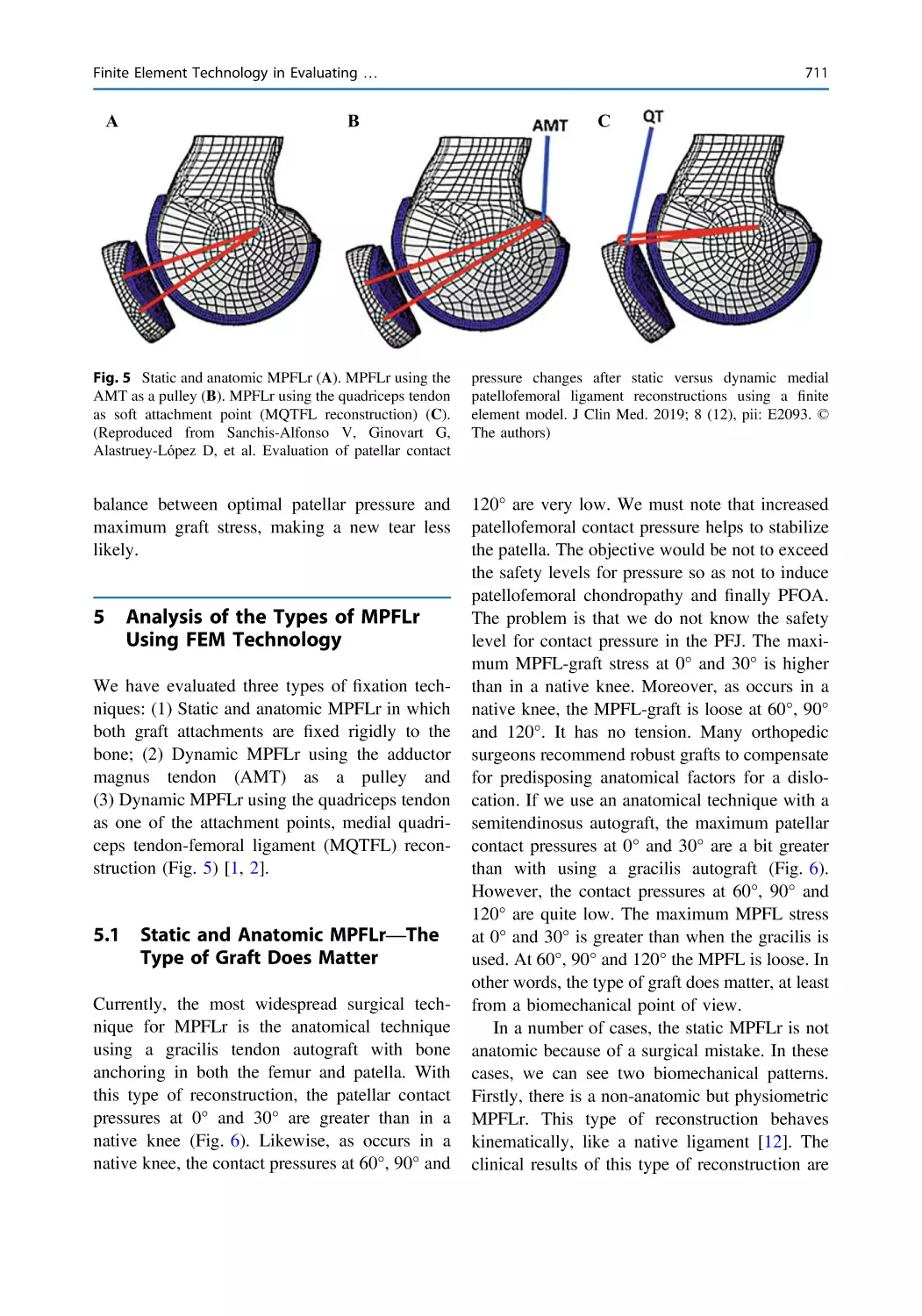
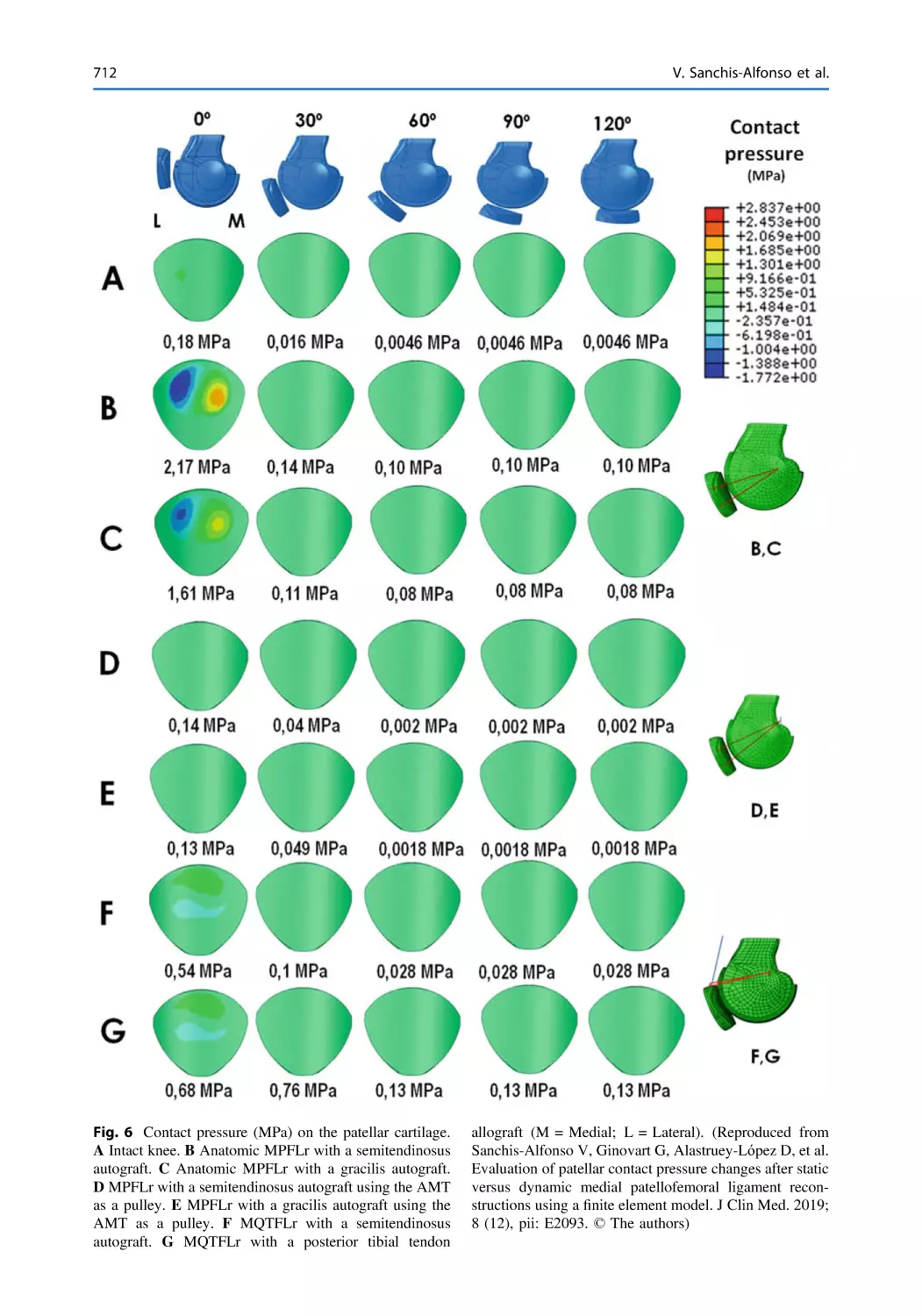
Finite Element Technology in Evaluating Medial Patellofemoral
Ligament Reconstruction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 705
Vicente Sanchis-Alfonso, Diego Alastruey-López,
Cristina Ramirez-Fuentes, Erik Montesinos-Berry, Gerard Ginovart,
Joan Carles Monllau, and María Angeles Perez
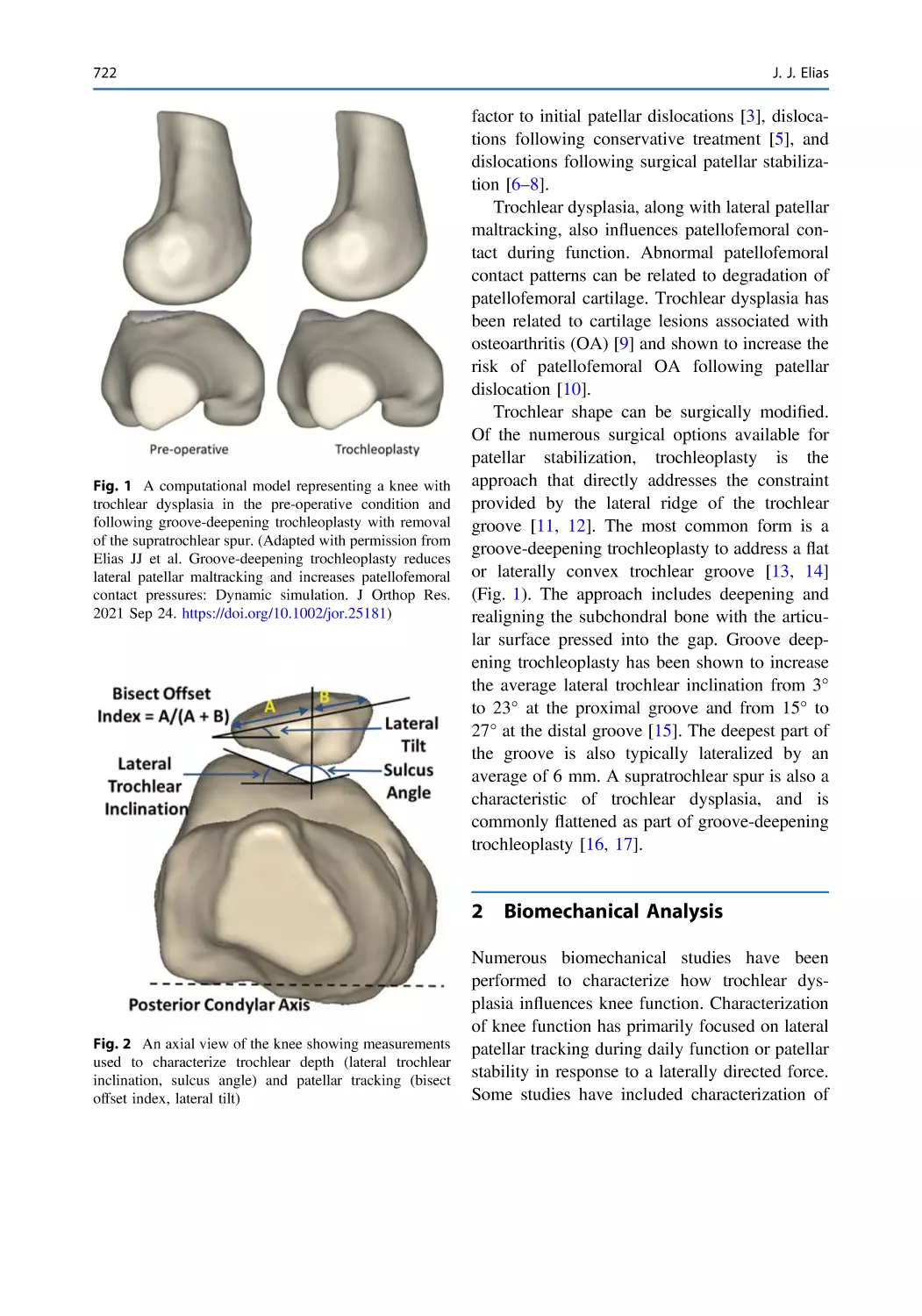
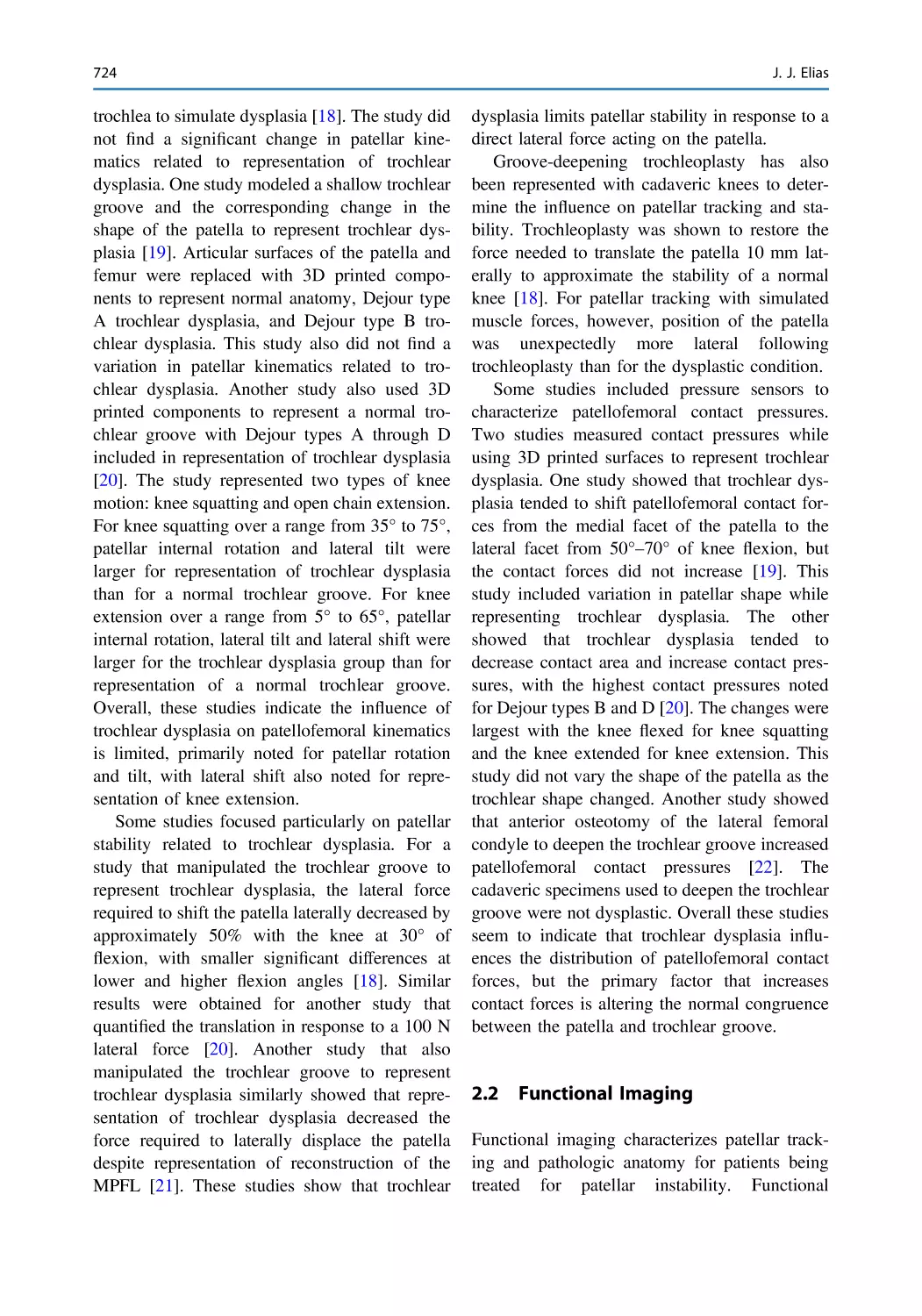
Biomechanical Analysis of the Influence of Trochlear Dysplasia
on Patellar Tracking and Pressure Applied to Cartilage . . . . . . . . 721
John J. Elias
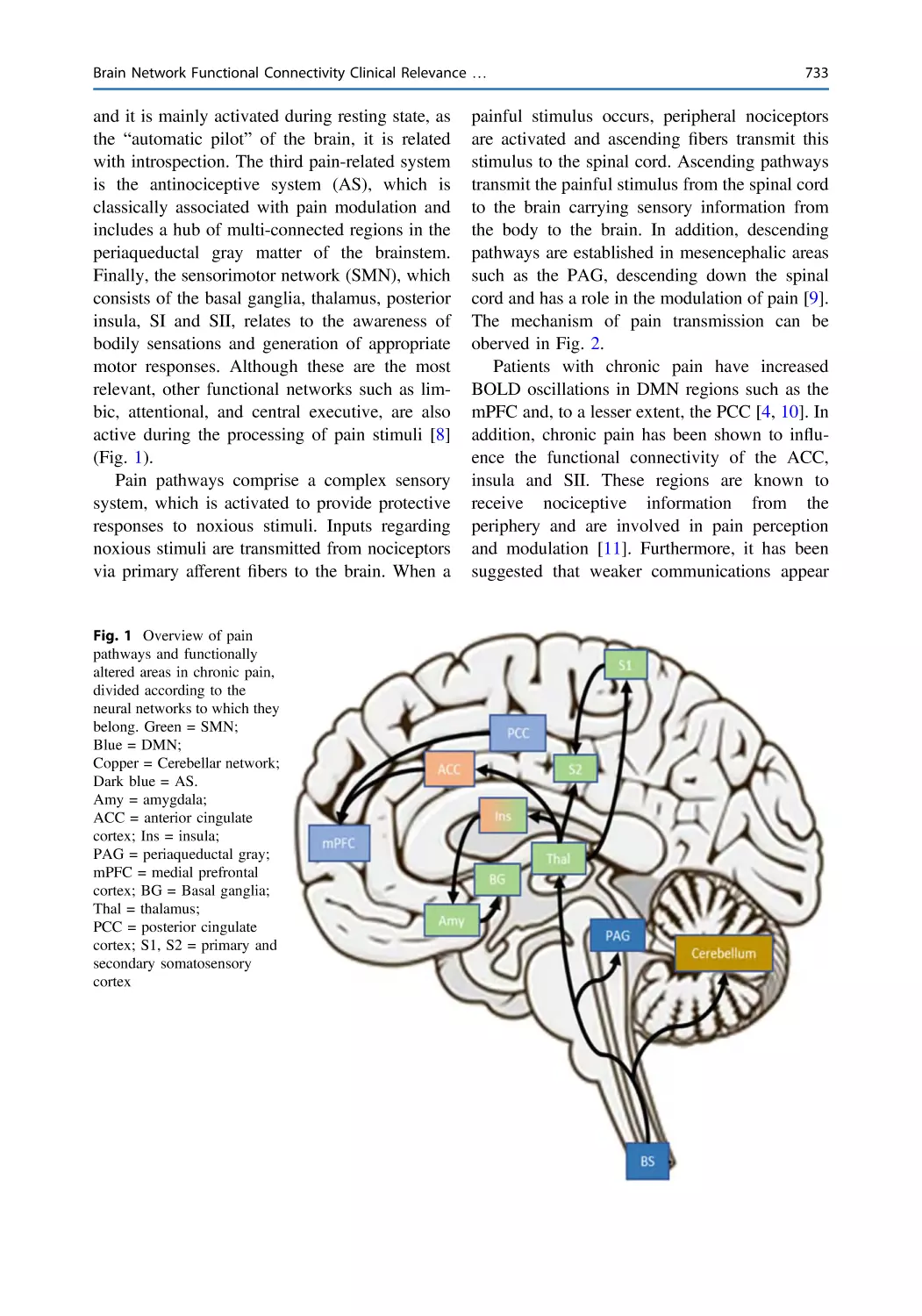
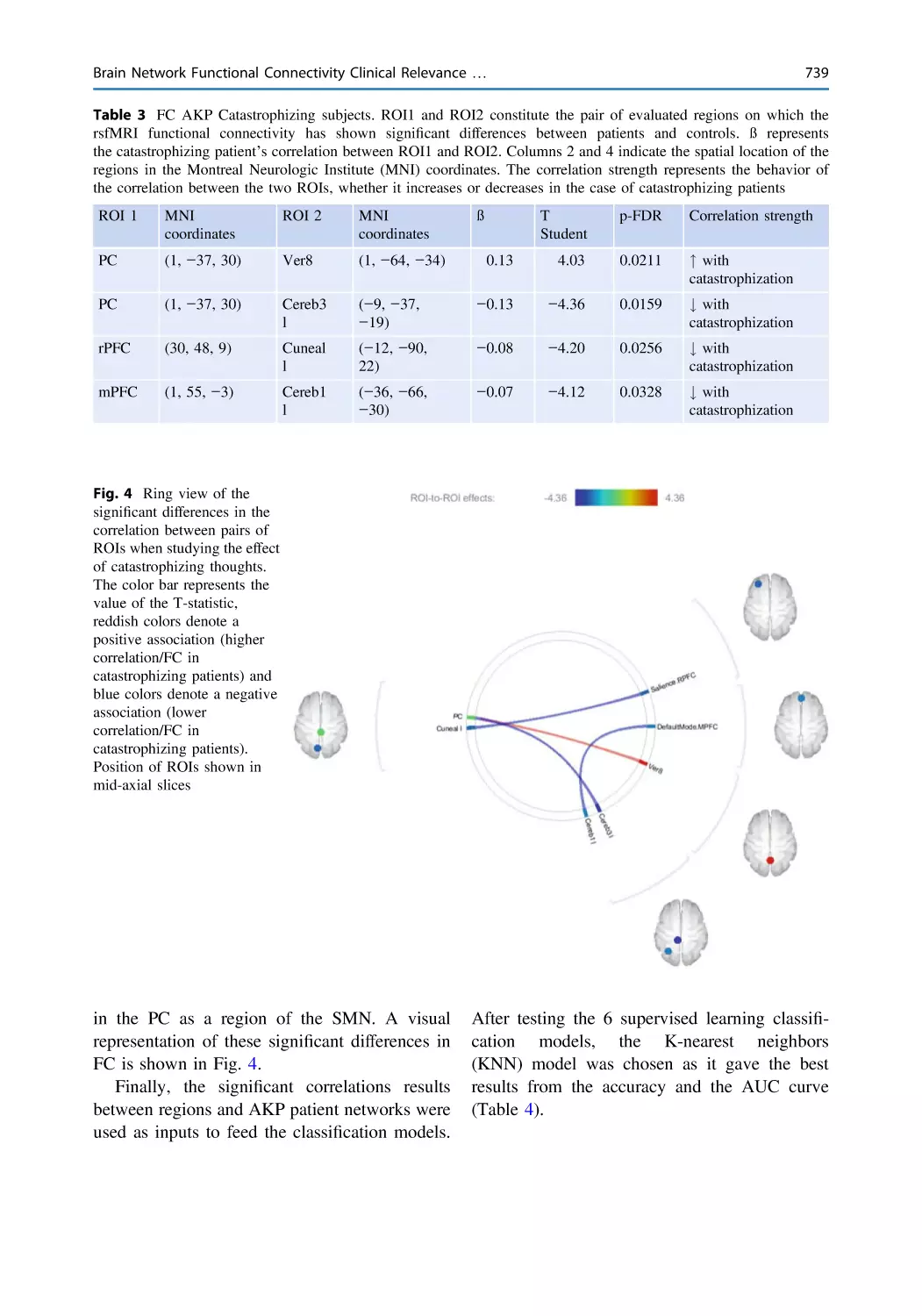
Brain Network Functional Connectivity Clinical Relevance
and Predictive Diagnostic Models in Anterior Knee Pain
Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 731
María Beser-Robles, Vicente Sanchis-Alfonso,
and Luis Martí-Bonmatí
xxvi
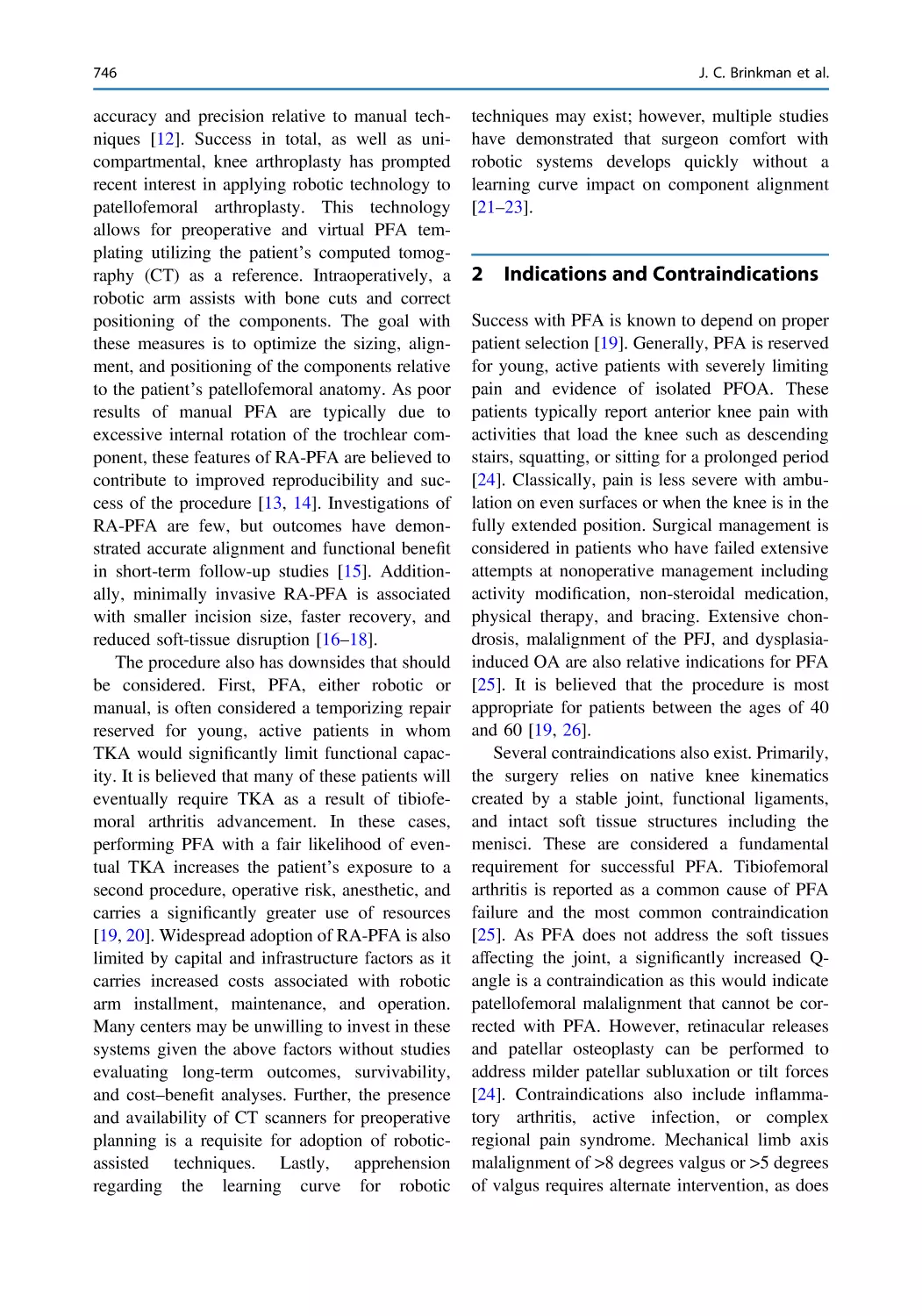
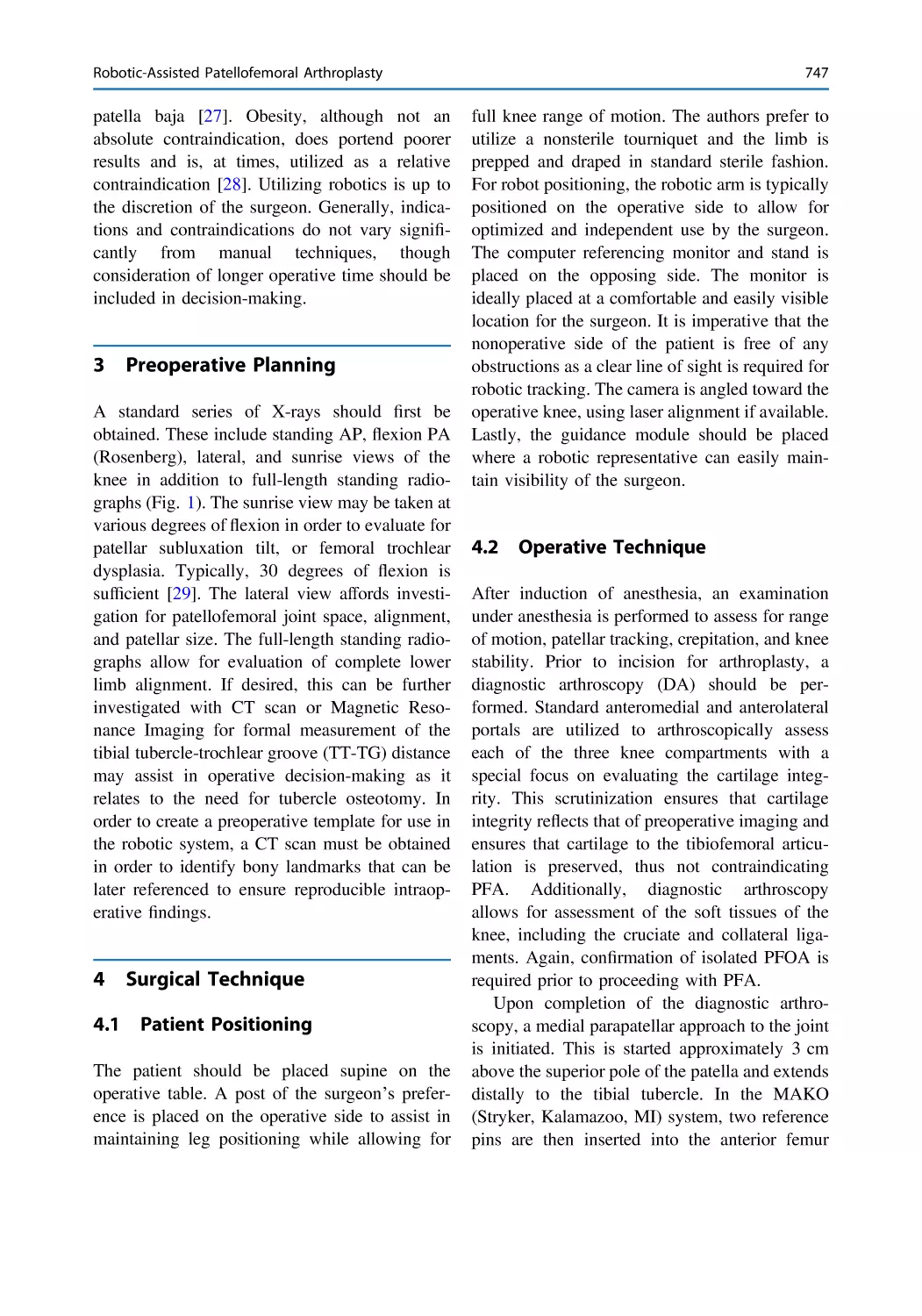
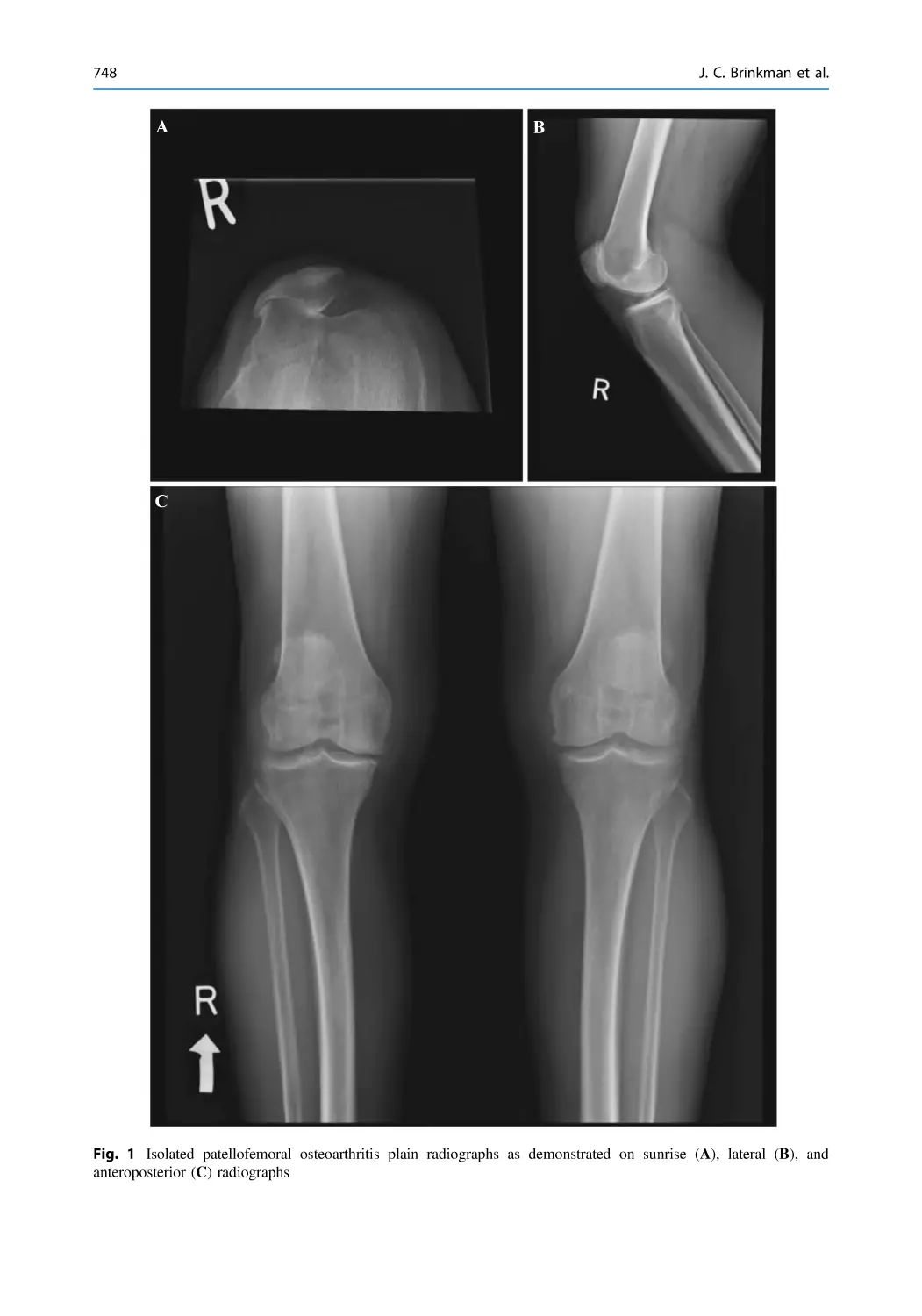
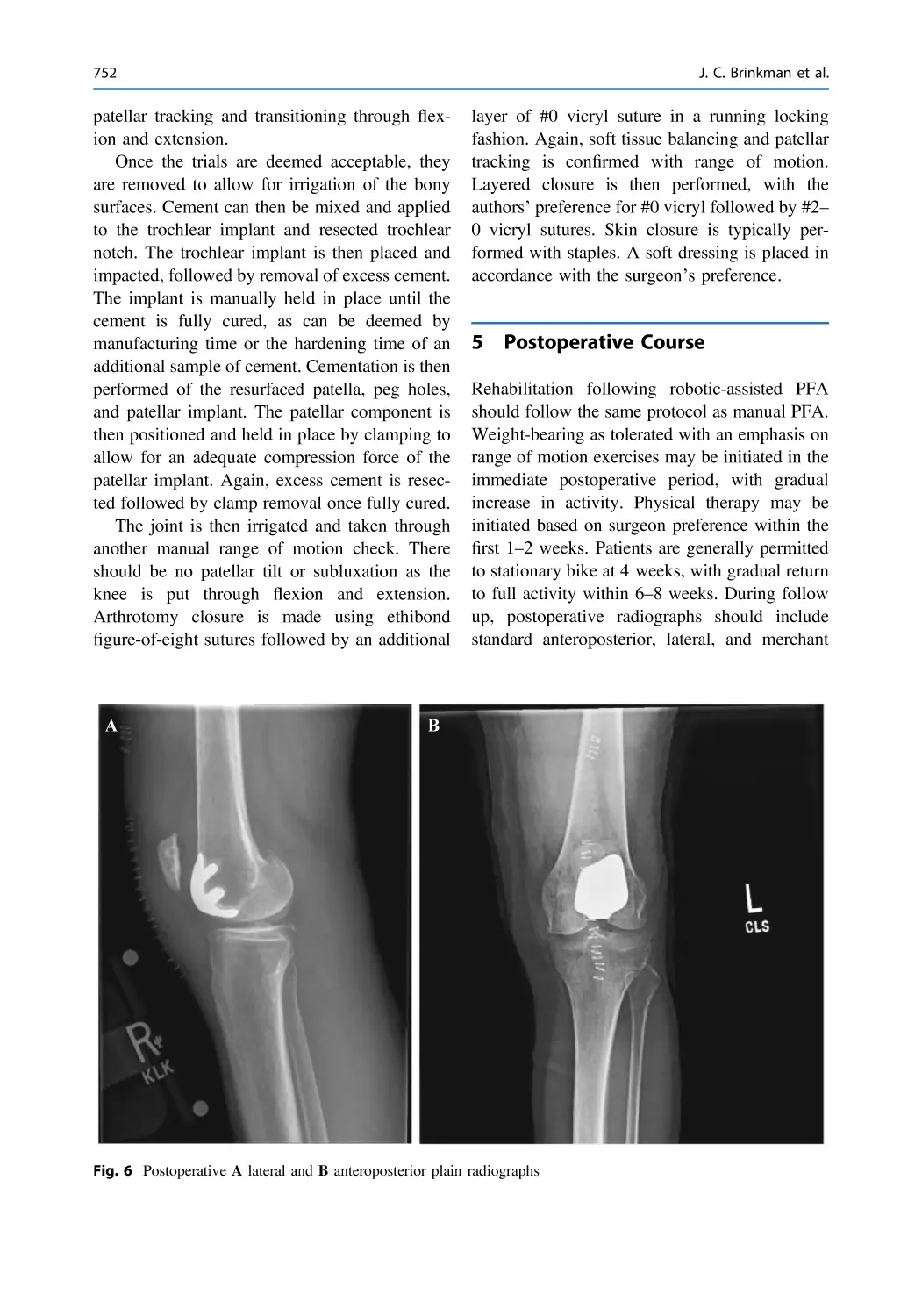
Robotic-Assisted Patellofemoral Arthroplasty . . . . . . . . . . . . . . . . . 745
Joseph C. Brinkman, Christian Rosenow, Matthew Anastasi,
Don Dulle, and Anikar Chhabra
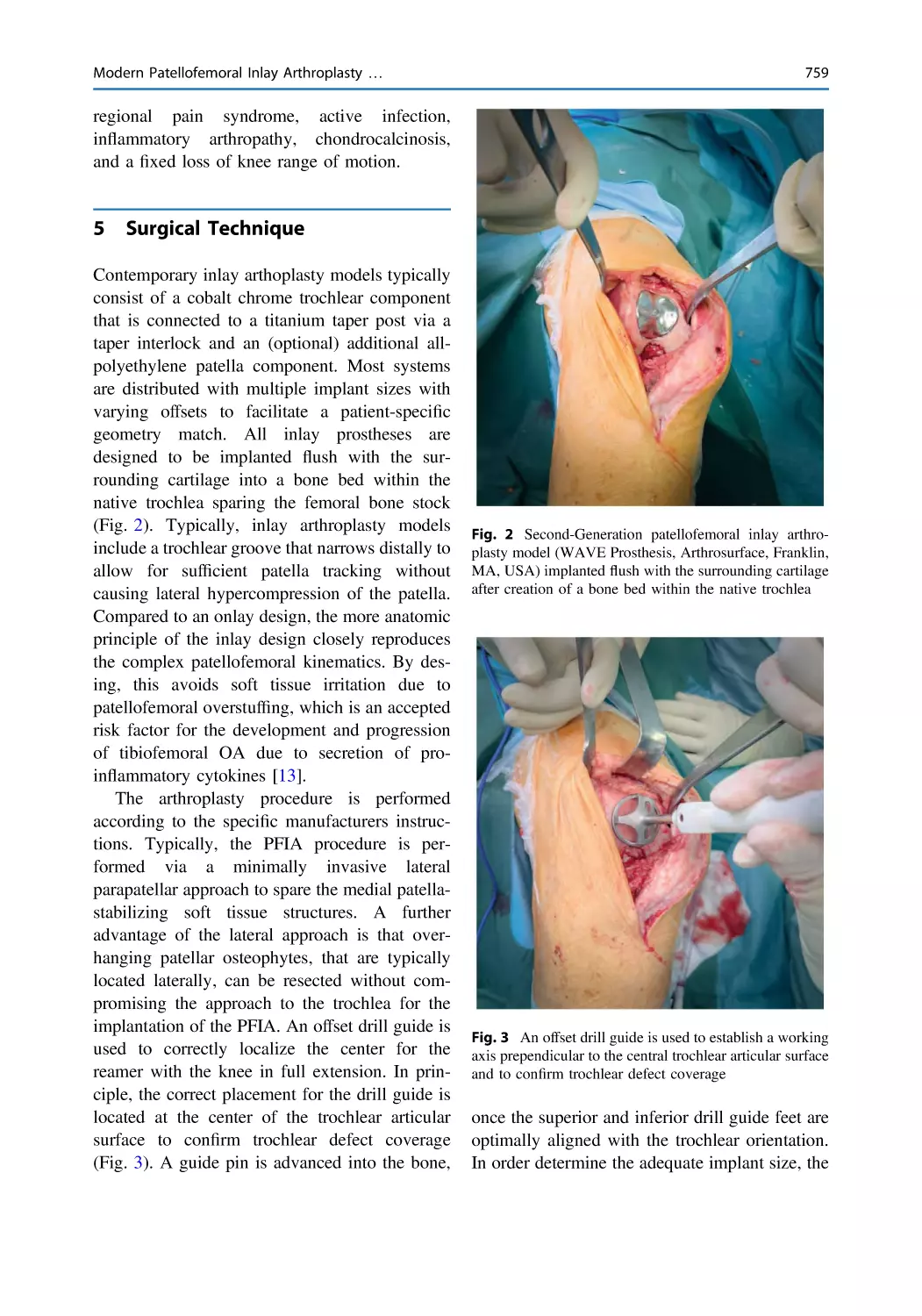
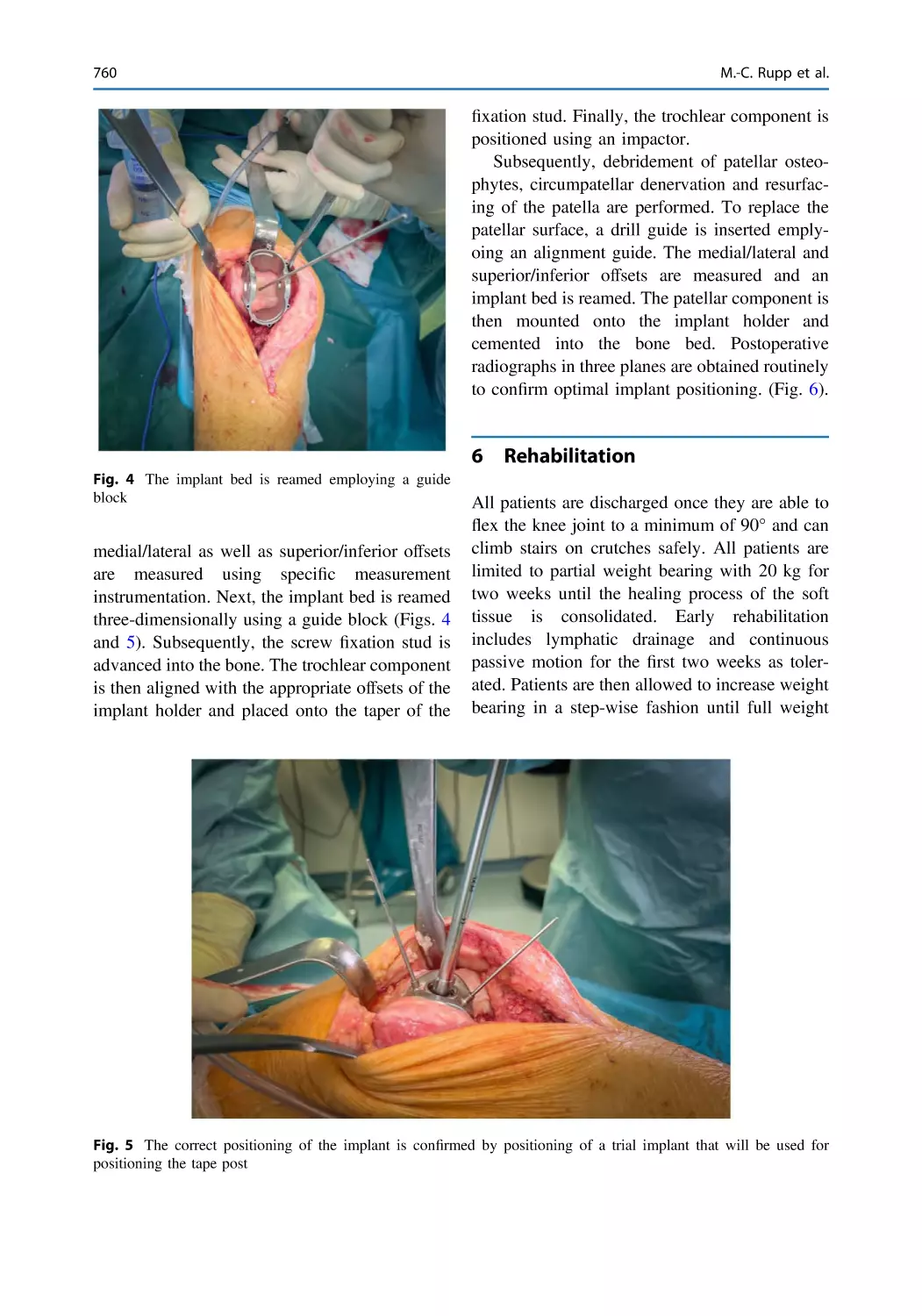
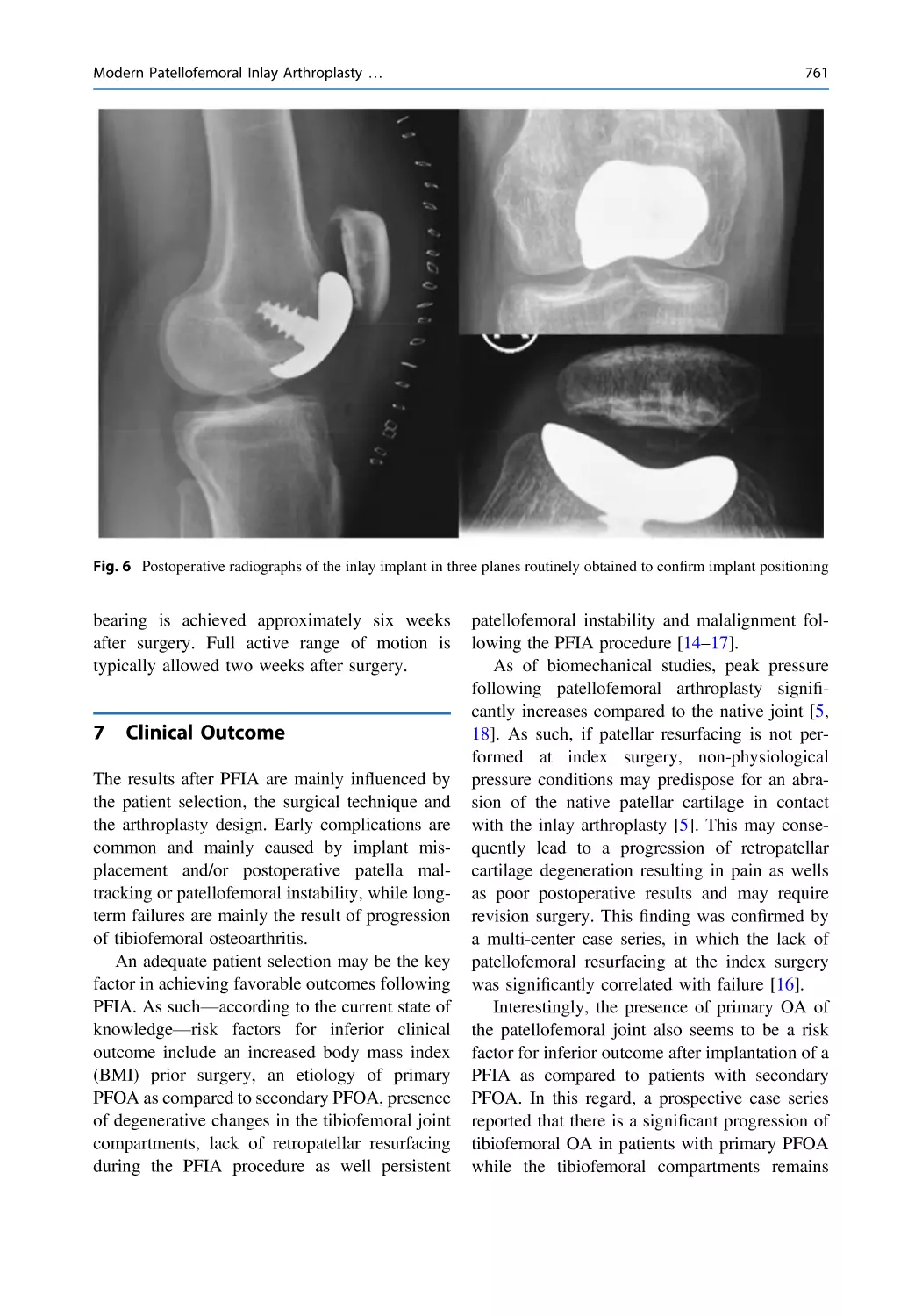
Modern Patellofemoral Inlay Arthroplasty—A Silver Lining
in the Treatment of Isolated Patellofemoral Arthritis . . . . . . . . . . . 757
Marco-Christopher Rupp, Jonas Pogorzelski, and Andreas B. Imhoff
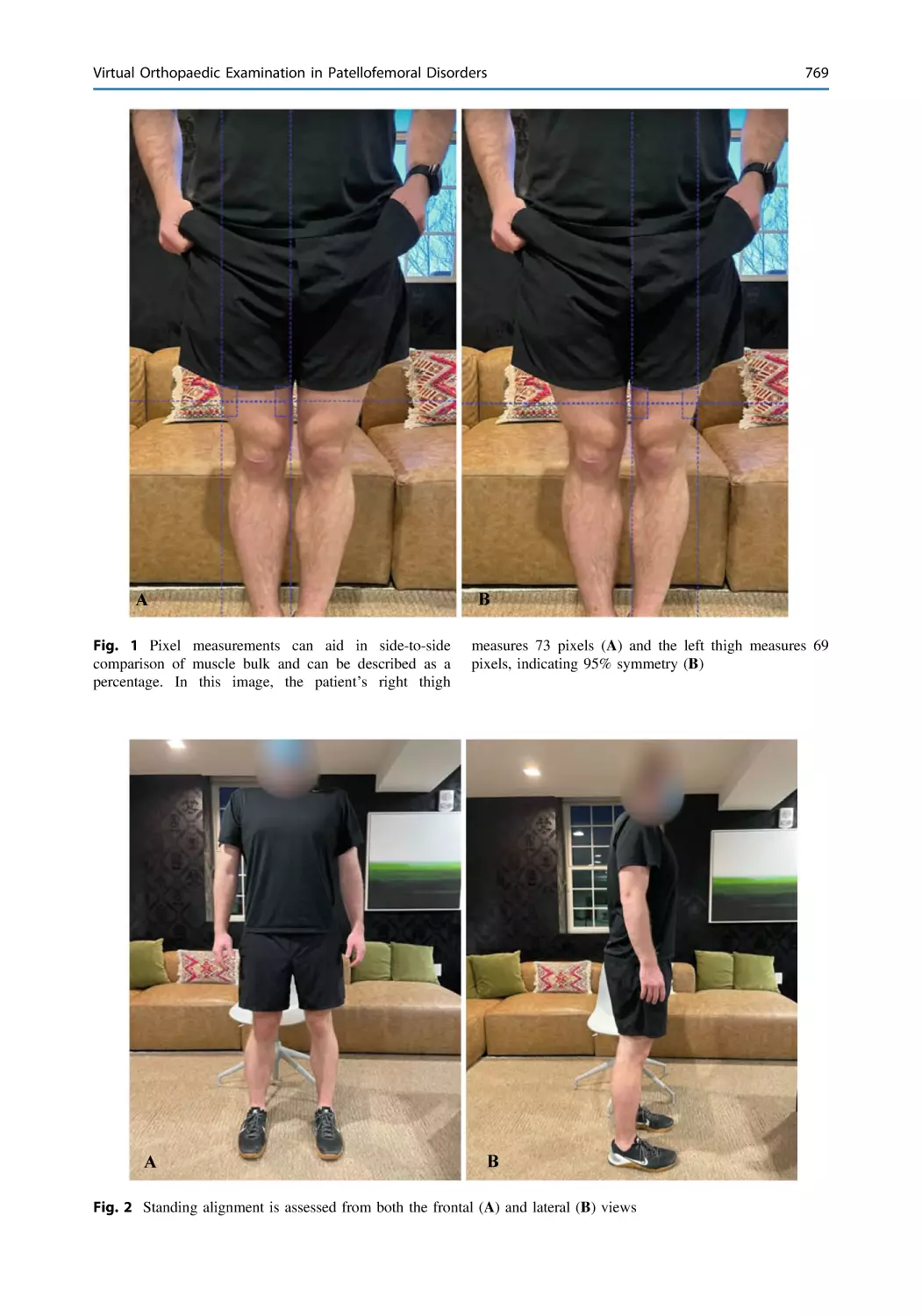
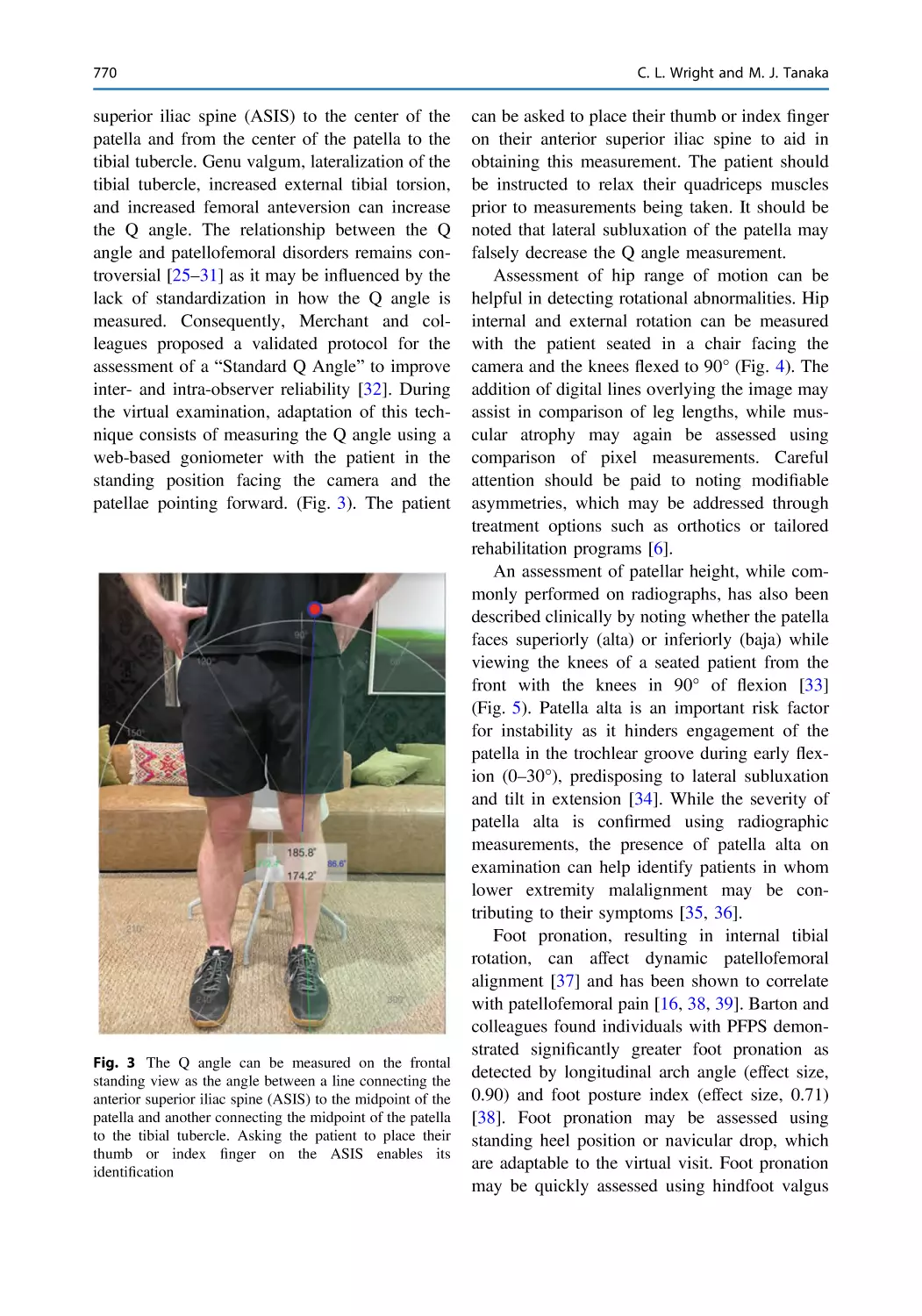
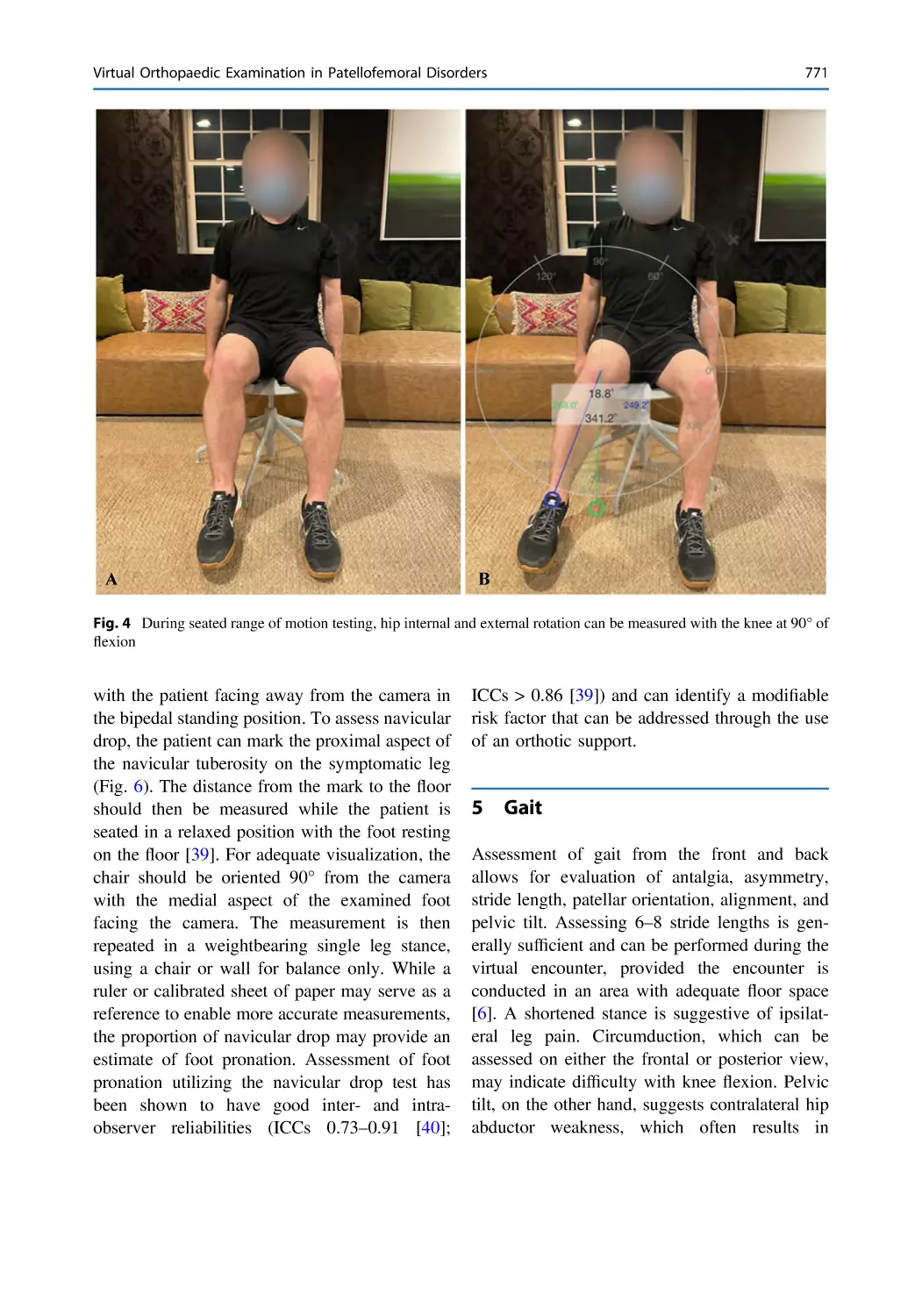
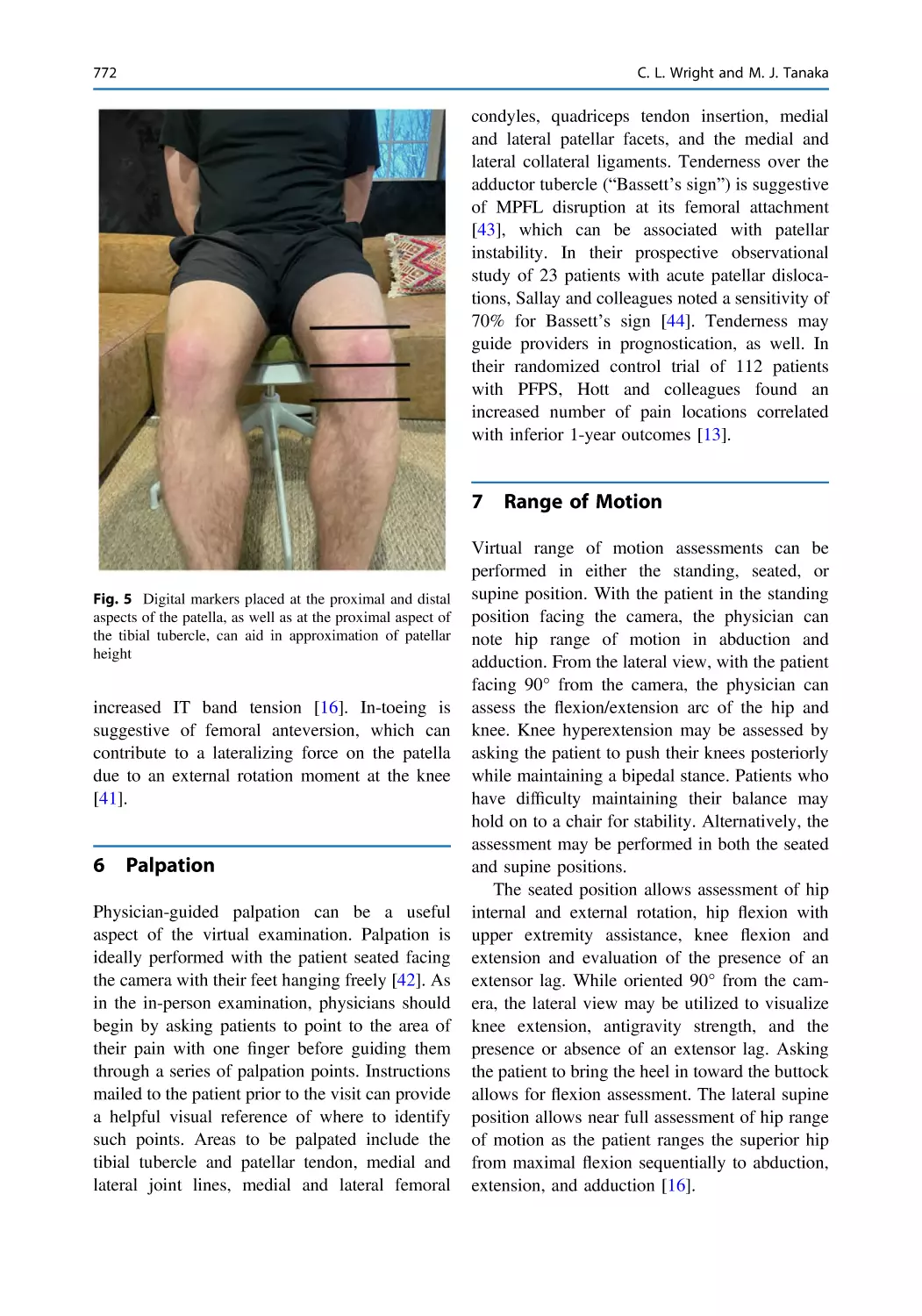
Virtual Orthopaedic Examination in Patellofemoral
Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 765
Casey L. Wright and Miho J. Tanaka
Epilogue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 781
Contents
Contributors
Ferran Abat ReSport Clinic Barcelona. Blanquerna-Ramon Llull University School of Health Science. Rosselló, Barcelona, Spain
Diego Alastruey-López Instituto de Investigación en Ingeniería de Aragón
(I3A), Instituto de Investigación Sanitaria Aragón (IIS Aragón), Multiscale in
Mechanical and Biological Engineering, University of Zaragoza, Zaragoza,
Spain
Håkan Alfredson Department of Community Medicine and Rehabilitation,
Sports Medicine, Umeå University, Umeå, Sweden
Jorge Amestoy Department of Orthopaedic Surgery, Hospital del Mar,
Barcelona, Spain;
Catalan Institute of Traumatology and Sports Medicine (ICATME), Hospital
Universitari Dexeus, Barcelona, Spain;
Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
Matthew Anastasi Department of Orthopaedic Surgery, Mayo Clinic,
Phoenix, AZ, USA;
Department of Sports Medicine, Mayo Clinic, Tempe, Phoenix, AZ, USA;
Alix School of Medicine, Mayo Clinic, Phoenix, AZ, USA
Renato Andrade Dom Henrique Research Centre, Porto, Portugal;
Clínica Espregueira - FIFA Medical Centre of Excellence, Porto, Portugal;
Porto Biomechanics Laboratory (LABIOMEP), Faculty of Sports, University
of Porto, Porto, Portugal
Jack Andrish The Cleveland Clinic Foundation, Cleveland, OH, USA
Juan Pablo Aracil-Kessler Plastic and Reconstructive Surgery Department,
Hospital Provincial de Castellón, Castellón, Spain
Elizabeth A. Arendt University of Minnesota, Minneapolis, MN, USA
Doug W. Bartels Department of Orthopaedic Surgery, Stanford University,
Stanford, CA, USA
Cécile Batailler Albert Trillat Center, Lyon North University Hospital,
Lyon, France
Jose María Baydal-Bertomeu Instituto de Biomecánica de Valencia (IBV),
Valencia, Spain
xxvii
xxviii
María Beser-Robles Biomedical Imaging Research Group at Health
Research Institute, Valencia, Spain
Roland M. Biedert Sportsclinic 1, Wankdorf Center, Bern, Switzerland
Lars Blønd Department of Orthopaedic Surgery, The Zealand University
Hospital, Koege, Denmark;
Department of Orthopaedic Surgery, Aleris-Hamlet, Copenhagen, Denmark
Michelle C. Boling Clinical and Applied Movement Sciences, Brooks
College of Health, University of North Florida, Jacksonville, USA
Joseph C. Brinkman Department of Orthopaedic Surgery, Mayo Clinic,
Phoenix, AZ, USA;
Department of Sports Medicine, Mayo Clinic, Tempe, Phoenix, AZ, USA;
Alix School of Medicine, Mayo Clinic, Phoenix, AZ, USA
William Bugbee Department of Orthopaedic Surgery, Scripps Clinic, La
Jolla, CA, USA
Jorge Chahla Department of Orthopaedic Surgery, Rush University
Medical Center, Chicago, IL, USA
Anikar Chhabra Department of Orthopaedic Surgery, Mayo Clinic,
Phoenix, AZ, USA;
Department of Sports Medicine, Mayo Clinic, Tempe, Phoenix, AZ, USA;
Alix School of Medicine, Mayo Clinic, Phoenix, AZ, USA
Jill Cook La Trobe University, Melbourne, Australia
Kevin Credille Midwest Orthopedics at Rush University Medical Center,
Chicago, IL, USA
Dhanur Damodar Midwest Orthopedics at Rush University Medical
Center, Chicago, IL, USA
Antonio Darder-Prats Department of Orthopaedic Surgery, Hospital
Arnau de Vilanova, Valencia, Spain
Antonio Darder-Sanchez Department of Orthopaedic Surgery, Hospital
Clínico Universitario, Valencia, Spain
Suhas P. Dasari Department of Orthopaedic Surgery, Rush University
Medical Center, Chicago, IL, USA
Robert S. Dean Beaumont Health, Royal Oak, MI, USA
David H. Dejour Lyon-Ortho-Clinic: Clinique de La Sauvegarde, Lyon,
France
Julio Doménech-Fernández Department of Orthopaedic Surgery, Hospital
Arnau de Vilanova, Valencia, Spain
Contributors
Contributors
xxix
Don Dulle Department of Orthopaedic Surgery, Mayo Clinic, Phoenix, AZ,
USA;
Department of Sports Medicine, Mayo Clinic, Tempe, Phoenix, AZ, USA;
Alix School of Medicine, Mayo Clinic, Phoenix, AZ, USA
Scott F. Dye University of California San Francisco, San Francisco, CA,
USA
John J. Elias Department of Health Sciences, Cleveland Clinic Akron
General, Akron, OH, USA
João Espregueira-Mendes Dom Henrique Research Centre, Porto,
Portugal;
Clínica Espregueira - FIFA Medical Centre of Excellence, Porto, Portugal;
3B’s Research Group–Biomaterials, Biodegradables and Biomimetics,
Headquarters of the European Institute of Excellence on Tissue Engineering
and Regenerative Medicine, AvePark, Parque de Ciência e Tecnologia, Zona
Industrial da Gandra, University of Minho, Barco, Guimarães, Portugal;
ICVS/3B’s–PT Government Associate Laboratory, Braga/Guimarães,
Portugal;
School of Medicine, University of Minho, Braga, Portugal
Jack Farr Knee Preservation and Cartilage Restoration Center, OrthoIndy,
Indianapolis, IN, USA
Lutul D. Farrow Cleveland Clinic Orthopaedic and Rheumatologic Institute, Cleveland, OH, USA;
Cleveland Clinic Lerner College of Medicine, Cleveland Clinic Sports Health
Center, Ohio, USA
Christian Fink Gelenkpunkt Sport and Joint Surgery, Innsbruck, Austria;
Research Unit for Orthopedic Sports Medicine and Injury Prevention, UMIT
Hall, Tirol, Austria
Donald C. Fithian Senta Clinic, San Diego, CA, USA
Gaspard Fournier Albert Trillat Center, Lyon North University Hospital,
Lyon, France
Christopher S. Frey Department of Orthopaedic Surgery, Stanford
University, Stanford, CA, USA
John P. Fulkerson Department of Orthopaedics and Rehabilitation, Yale
School of Medicine, New Haven, CT, USA
Gerard Ginovart Department of Orthopaedic Surgery, Hospital Terres de
l’Ebre, Tortosa, Spain
Edoardo Giovannetti de Sanctis Lyon-Ortho-Clinic: Clinique de La
Sauvegarde, Lyon, France
André Gismonti Clínica Espregueira - FIFA Medical Centre of Excellence,
Porto, Portugal
xxx
Contributors
Neal R. Glaviano Department of Kinesiology, College of Agriculture,
Health and Natural Resources, University of Connecticut, Mansfield, USA
Ronald P. Grelsamer The Icahn School of Medicine at the Mount Sinai
Medical Center, New York, NY, USA
Andrew Gudeman Indiana University School of Medicine, Indianapolis,
IN, USA
Safa Gursoy Department of Orthopaedic Surgery, Rush University Medical
Center, Chicago, IL, USA
Mahad Hassan University of Minnesota, Minneapolis, MN, USA
Pedro Hinarejos Consorci Parc de Salut Mar. Barcelona Universitat
Pompeu Fabra, Barcelona, Spain
Betina B. Hinckel Beaumont Health, Royal Oak, MI, USA
Maximiliano Ibañez ICATME, Hospital Universitari Dexeus, UAB,
Barcelona, Spain
Andreas B. Imhoff Department of Orthopaedic Sports Medicine, Hospital
Rechts der Isar, Technical University of Munich, Munich, Germany
Andrew E. Jimenez Department of Orthopaedics and Rehabilitation, Yale
School of Medicine, New Haven, CT, USA
Augustine W. Kang Stanford School of Medicine, Stanford, CA, USA
Rochelle Kennedy La Trobe University, Melbourne, Australia
Jason Koh Department of Orthopaedic Surgery, NorthShore University
HealthSystem, Skokie, IL, USA
Ana Leal CMEMS—Center for MicroElectroMechanical
University of Minho, Guimarães, Portugal
Systems,
Kenneth Lin Department of Orthopaedic Surgery, Stanford University,
Stanford, CA, USA
Laura López-Company Department of Rehabilitation and Physical Therapy, Hospital Arnau de Vilanova, Valencia, Spain
Sebastien Lustig Albert Trillat Center, Lyon North University Hospital,
Lyon, France
Bhargavi Maheshwer Department of Orthopaedic Surgery, Rush University Medical Center, Chicago, IL, USA
Enzo S. Mameri Department of Orthopaedic Surgery, Rush University
Medical Center, Chicago, IL, USA
Luis Martí-Bonmatí Medical Imaging Department and Biomedical Imaging Research Group at Hospital, Universitario y Politecnico La Fe and Health
Research Institute, Valencia, Spain
Jenny McConnell Private Practice, Sydney, NSW, Australia
Contributors
xxxi
David A. Molho Department of Orthopaedics and Rehabilitation, Yale
School of Medicine, New Haven, CT, USA
Joan Carles Monllau Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain;
Catalan Institute of Traumatology and Sports Medicine (ICATME), Hospital
Universitari Dexeus, Barcelona, Spain;
Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
Erik Montesinos-Berry ArthroCentre–Agoriaz, Riaz and Clinique CIC
Riviera, Montreux, Switzerland
Lee Pace Children’s Health Andrews Institute, Plano, TX, USA
Ronak M. Patel Illinois Center for Orthopaedic Research and Education,
Hinsdale, IL, USA
Sneh Patel University of Illinois College of Medicine at Chicago, Chicago,
IL, USA
Rogério Pereira Dom Henrique Research Centre, Porto, Portugal;
Clínica Espregueira - FIFA Medical Centre of Excellence, Porto, Portugal;
Faculty of Sports, University of Porto, Porto, Portugal;
Health Science Faculty, University Fernando Pessoa, Porto, Portugal
María Angeles Perez Instituto de Investigación en Ingeniería de Aragón
(I3A), Instituto de Investigación Sanitaria Aragón (IIS Aragón), Multiscale in
Mechanical and Biological Engineering, University of Zaragoza, Zaragoza,
Spain
Daniel Pérez-Prieto Department of Orthopaedic Surgery, Hospital del Mar,
Barcelona, Spain;
Catalan Institute of Traumatology and Sports Medicine (ICATME), Hospital
Universitari Dexeus, Barcelona, Spain;
Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
Jonas Pogorzelski Department of Orthopaedic Sports Medicine, Hospital
Rechts der Isar, Technical University of Munich, Munich, Germany
William R. Post Mountaineer Orthopedic Specialists, LLC, Morgantown,
WV, USA
Cristina Ramírez-Fuentes Medical Imaging Department,
Universitario y Politecnico La Fe, Valencia, Spain
Hospital
Alejandro Roselló-Añón Department of Orthopaedic Surgery, Hospital
Arnau de Vilanova, Valencia, Spain
Esther Roselló-Sastre Department of Pathology, Hospital General de
Castellón, Castellón, Spain
xxxii
Christian Rosenow Department of Orthopaedic Surgery, Mayo Clinic,
Phoenix, AZ, USA;
Department of Sports Medicine, Mayo Clinic, Tempe, Phoenix, AZ, USA;
Alix School of Medicine, Mayo Clinic, Phoenix, AZ, USA
Marco-Christopher Rupp Department of Orthopaedic Sports Medicine,
Hospital Rechts der Isar, Technical University of Munich, Munich, Germany
Enrique Sanchez-Muñoz Knee Unit, Department of Trauma and Orthopaedic Surgery, Toledo University Hospital, Toledo, Spain
Vicente Sanchis-Alfonso Department of Orthopaedic Surgery, Hospital
Arnau de Vilanova, Valencia, Spain
Onofre Sanmartin IVO’s Dermatology Department, Instituto Valenciano
de Oncología (IVO), Valencia, Spain
Christopher A. Schneble Department of Orthopaedics and Rehabilitation,
Yale School of Medicine, New Haven, CT, USA
James Selfe Faculty of Health and Education, Department of Health Professions, Manchester Metropolitan University, Manchester, UK;
Visiting Academic in Physiotherapy Studies, Satakunta University of
Applied Sciences, Pori, Finland
Elvire Servien Albert Trillat Center, Lyon North University Hospital, Lyon,
France
Jobe Shatrov Albert Trillat Center, Lyon North University Hospital, Lyon,
France;
Sydney Orthopedic Research Institute, St. Leonard’s, Sydney, NSW,
Australia
Seth L. Sherman Department of Orthopaedic Surgery, Stanford University,
Stanford, CA, USA
Benjamin E. Smith Physiotherapy Outpatients, University Hospitals of
Derby and Burton NHS Foundation Trust, Derby, UK
Pablo Sopena-Novales Department of Nuclear Medicine, Hospital Vithas 9
Octubre, Valencia, Spain
Miho J. Tanaka Department of Orthopaedic Surgery, Massachusetts
General Hospital, Harvard Medical School, Boston, MA, USA
Robert A. Teitge Department of Orthopaedic Surgery, Wayne State
University, Detroit, MI, USA
Marc Tey-Pons Department of Orthopaedic Surgery, Hospital del Mar,
Barcelona, Spain;
Department of Orthopaedic Surgery, iMove orthopaedics, Hospital Mi Tres
Torres, Barcelona, Spain
Marc Tompkins University of Minnesota, TRIA Orthopedic Center, Minneapolis, MN, USA
Contributors
Contributors
xxxiii
Cristina Valente Dom Henrique Research Centre, Porto, Portugal;
Clínica Espregueira - FIFA Medical Centre of Excellence, Porto, Portugal
Eloisa Villaverde-Doménech Plastic and Reconstructive Surgery Department, Hospital Provincial de Castellón, Castellón, Spain
Zachary Wang Midwest Orthopedics at Rush University Medical Center,
Chicago, IL, USA
Casey L. Wright Department of Orthopaedic Surgery, Massachusetts
General Hospital, Harvard Medical School, Boston, MA, USA
Adam Yanke Midwest Orthopedics at Rush University Medical Center,
Chicago, IL, USA
David S. Zhu Cleveland Clinic Orthopaedic and Rheumatologic Institute,
Cleveland, OH, USA
Etiopathogenic Bases, Prevention
and Therapeutic Implications
Patellofemoral Pain: An Overview
Vicente Sanchis-Alfonso and Ronald
P. Grelsamer
That those who know her, know her less, the nearer her they get.
Emily Elizabeth Dickinson
1
Anterior Knee Pain—So Common
a Symptom, so Misunderstood
Patellofemoral pain (PFP) or anterior knee pain
(AKP) is defined as “pain around or behind the
patella, which is aggravated by at least one
activity that loads the patellofemoral joint (PFJ)
during weight-bearing on a flexed knee (e.g.,
squatting, stair ambulation, jogging/running,
hopping/jumping)” [1]. The best available test is
“anterior knee pain elicited during a squatting
manoeuvre: PFP is evident in 80% of people who
are positive on this test” [1]. According to the
International patellofemoral pain research retreat
“people with a history of dislocation, or who
report perceptions of subluxation, should not be
included in studies of PFP, unless the study is
specifically evaluating these subgroups” [1].
Although it typically occurs in physically active
people lesser than 40 years, it also affects people
of all activity levels and ages [2].
In a systematic review with meta-analysis,
Smith and colleagues [3] have recently found
high incidence and prevalence levels for
AKP. Subjects were excluded “if the study
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
R. P. Grelsamer
The Icahn School of Medicine at the Mount Sinai
Medical Center, New York, NY, USA
population was selected from a specific disease
area (e.g. diabetes, rheumatoid arthritis,
osteoarthritis); if the study population comprised
of participants with other knee pathology (e.g.
knee ligamentous instability, history of patella
dislocations, true knee locking or giving way,
patella or iliotibial tract tendinopathy,
osteoarthritis)”. The results of that systematic
review confirmed that AKP is a common
pathology among adolescents and adults. That is
the case in both the general population as well as
those who practice sports or perform physically
demanding activities such as those performed by
the military. The prevalence in the general population is reported to stand at 23%, in professional cyclists at 35.7% and in the general
adolescent population at 30% [3]. Moreover, a
woman is twice as likely to develop AKP than a
man [3]. The mean prevalence of low-back pain
in the general population is 18% and goes up to
20% among runners [4]. Overall, the prevalence
of knee osteoarthritis (OA) has been found to be
16% [5]. Although the prevalence of these three
pathological entities is very similar, the interest
they arouse in researchers is very different: There
have been more than 14,000 articles on knee OA
indexed on MEDLINE in the last 20 years.
Compare that to only 1,500 indexed articles on
AKP [3]. It seems clear that PFP or AKP is of
less interest than other conditions of the musculoskeletal system. Despite its high incidence and
prevalence, AKP is the most neglected, the least
understood, and the most problematic pathological knee condition.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_1
3
4
2
V. Sanchis-Alfonso and R. P. Grelsamer
The Problem. Anterior Knee
Pain—A Paradigm of Aversion
Towards a Diagnosis
Implicated factors in AKP include the loss of
homeostasis as well as functional, mechanical
and structural alterations (see chapters “Pathophysiology of Anterior Knee Pain”, “Femoral
and Tibial Rotational Abnormalities are the Most
Ignored Factors in the Diagnosis and Treatment
of Anterior Knee Pain Patients. A Critical Analysis Review” and “Why is Torsion Important in
the Genesis of Anterior Knee Pain?”). The etiology of AKP is multifactorial with not only
local (e.g., knee) factors but also proximal (e.g.,
hip and trunk) and distal ones (e.g., foot and
ankle). In fact, the primary cause of AKP in
many patients does not lie within the PFJ. There
are several subgroups within the AKP population. Therefore, the optimum treatment must be
tailored to the individual patient (see chapter
“Targeted Treatment in Anterior Knee Pain
Patients According to Subgroups Versus Multimodal Treatment”).
Among all the subsets of patients with AKP,
the most challenging type of AKP, from a therapeutic point of view, is neuropathic. Rathleff
and colleagues [6] have shown that young female
adults with long-standing AKP demonstrated
impaired conditioned pain modulation, meaning
that AKP might have important central components that need to be further studied.
Another challenge we face is patellar
nomenclature. The study of the PFJ is complicated by the use of terms that have different
meanings depending on who reads them (The
Tower of Babel) [7]. There are terms that must be
clarified such as the terms patellar malalignment
and skeletal malalignment of the lower limb.
There are other terms that should be abandoned,
such as “chondromalacia patellae” and “patellofemoral pain syndrome.”
AKP is a nemesis to both the patient and the
treating physician, creating chronic disability,
limited participation in sports, diminished quality
of life, psychological impairment, and the basis
for sick leave. Collins and colleagues [8] showed
that 40% of AKP patients had a less-thanfavorable recovery at 12 months from the time
of diagnosis. AKP negatively influences the
quality of life of the patient in the same way as
knee OA, another affection that is considered
more serious. However, since AKP affects
younger populations, it can have a greater impact
on their lives than knee OA [9]. The World
Health Organization (WHO) defines disability as
“a limitation of function that compromises an
individual’s ability to perform an activity within
the range considered normal”. Because AKP
frequently occurs in young working adults, it has
an important societal impact due to absenteeism
from work and lowered productivity as well as
the economic expense of treating these patients
[10]. Moreover, people including friends and
family might consider AKP patients to be
malingering, which only makes things worse.
Furthermore, making this worse, we must
point out that it is a source of iatrogenic pathology (e.g., medial patellar instability) [11]. We
must be very cautious when recommending surgical treatment for AKP patients (see chapter
“The Failed Patella. What Can We Do?”). This
caution is particularly directed to those “wellmeaning trigger-happy orthopedic surgeons” (a
term coined by Scott F. Dye, MD) educated in a
purely structural/biomechanical view of this
pathology. These surgeons base their surgical
decisions solely on Computed tomography
(CT) or Magnetic resonance imaging (MRI)
findings. This approach is misguided. The
patient who began with just mild, intermittent
symptoms may get even worse. We must note
that the vast majority of AKP patients only need
non-operative treatment. The current best
evidence-based non-surgical treatment for AKP
is multimodal therapy. The core components of
this approach include a diverse mix of exercise
therapies (e.g., strengthening, stretching), patellar
taping or bracing and foot orthoses depending on
the sub-group that the patient falls into. There is
limited evidence supporting the long-term outcomes of any single approach. Over the years,
there have been many attempts to define subgroups within the AKP population. Despite these
Patellofemoral Pain: An Overview
efforts, there is currently no consensus on what
the optimal treatments are for the various subgroups. Nonetheless, there is emerging evidence
that tailoring treatments to each subgroup can
improve the treatment outcomes when compared
to currently common multimodal approaches (see
chapter “Targeted Treatment in Anterior Knee
Pain Patients According to Subgroups Versus
Multimodal Treatment”). Finally, we are convinced that the so-called biopsychosocial model
currently used in chronic lumbar pain will soon
be applied to AKP patients. According to this
model, anatomic, biological and biomechanical
factors as well as psychological and social factors
must be considered (see chapter “Evaluation of
Psychological Factors Affecting Anterior Knee
Pain Patients: The Implications for Clinicians
Who Treat These Patients”). Among all the
psychological factors that have been analyzed in
the AKP patient, the most relevant one is catastrophizing (exaggerated worrying), which relates
to pain and disability (see chapter “Evaluation of
Psychological Factors Affecting Anterior Knee
Pain Patients: The Implications for Clinicians
Who Treat these Patients”). Consequently, cognitive behavioral interventions that have brought
on a reduction of catastrophizing pain in patients
with arthritis or lumbar pain may also be helpful
in patients suffering from AKP (see chapter
“Evaluation of Psychological Factors Affecting
Anterior Knee Pain Patients: The Implications
for Clinicians Who Treat these Patients”).
Therefore, treatments for this should be incorporated into conventional approaches. Of course,
catastrophizing can come from repeated doctors’
failures to diagnose and treat (see chapter “Evaluation of Psychological Factors Affecting
Anterior Knee Pain Patients: The Implications
for Clinicians Who Treat these Patients”).
Unfortunately, the criteria for proper treatment
of the AKP patient have largely been anecdotal.
More studies with a high level of evidence are
needed. These patients bring to the office “a bag
full of MRIs or CTs” in which the radiologist
reports a patellar subluxation or a patellar tilt. As
a last resort, they have been advised to undergo
surgery to correct a supposed “lateral displacement of the patella” or the “lateral tilt” diagnosed
5
with the MRI or CT alone. This can be problematic when no adequate physical examination
has been performed. The malalignment theory,
which is strongly supported by many orthopedic
surgeons, has enormously damaged many AKP
patients and has given this pathology a bad reputation. Of course, a structural anomaly can be
responsible for AKP. For example, a rotational
osteotomy ought to be considered for that AKP
patient with a significant torsional deformity
(transverse plane) of the limb (see chapters
“Femoral and Tibial Rotational Abnormalities are
the Most Ignored Factors in the Diagnosis and
Treatment of Anterior Knee Pain Patients.
A Critical Analysis Review”, “Why is Torsion
Important in the Genesis of Anterior Knee Pain?”,
“Surgical Treatment of Anterior Knee Pain.
When is Surgery Needed?” and “Rotational
Osteotomy. Principles, Surgical Technique, Outcomes and Complications”). We must note that
this biomechanical approach is compatible with
the biological perspective (“Tissue Homeostasis
Theory”) (see chapter “Pathophysiology of
Anterior Knee Pain”). We should not be distracted by structural findings manifested on an
MRI—but neither should we ignore them. Van
der Heijden and colleagues [12] have shown that
the structural abnormalities of the PFJ seen on
MRIs are not automatically associated with
AKP. Thus, AKP patients often undergo treatments with little scientific basis. A number of
patients receive intra-articular injections of
platelet-rich-plasma (PRP). A plethora of treatment options with different levels of agreement
have been described. The great number of variables associated with AKP, most of which lack
valid measurement tools, can explain this
confusion.
All of this makes this pathology an urgent
research priority. Moreover, this all explains why
many orthopedic surgeons have an aversion to
treating AKP patients. Doctors do not want to
spend the time evaluating these patients—it’s just
not cost-effective. They order an MRI and read
the report. Moreover, in some parts of the world,
radiologists do not appreciate patellar pathology
unless it is extreme; therefore, orthopedists
relying completely on the MRI report also miss
6
V. Sanchis-Alfonso and R. P. Grelsamer
structural issues. Not uncommonly, AKP patients
are quickly shunted off to orthopedic surgeons
with a particular interest in the topic.
3
Patellofemoral Pain—A
Pathologic Condition with Many
Clichés and False Beliefs
There are many myths surrounding this condition, false collective beliefs that are transmitted
from generation to generation. One of these
myths is that the AKP patient is a person with
peculiar psychological traits that are responsible
for the genesis of pain. This belief is reinforced
by the fact that many patients have very disabling
pain but insignificant radiological findings and
unremarkable physical signs. The psychological
explanation as the cause of pain could not be
further from the truth. Psychological factors in
AKP patients are only modulators of pain and
disability and should be addressed in combination with the search for structural causes (see
chapter “Evaluation of Psychological Factors
Affecting Anterior Knee Pain Patients: The
Implications for Clinicians Who Treat these
Patients”).
Another misconception is that AKP is always
a self-limiting and benign condition, which is
why some physicians believe that an active
treatment is unnecessary. It is frequently said to
that AKP is related to growth. Therefore, symptoms will disappear once the patient reaches
adulthood. For this reason, some physicians recommend “expectation”. That approach is a great
mistake. Collins and colleagues [8] have shown
that success in treating the AKP patient depends
on how early the treatment starts. Patients with
pain of less than 2 months duration have a better
prognosis than those who have had pain for more
than 2 months. Rathleff and colleagues [13] have
shown that AKP is not a self-limiting knee condition. Those authors observed that adolescents
with PFP were more likely to reduce or stop
participation in sports compared to adolescents
with other types of knee pain. They also found
that a majority of their AKP patients had been
symptomatic for more than two years, suggesting
that it is not a self-limited condition. In other
words, early detection and treatment are advisable. In addition, when possible it is essential to
implement prevention measures during adolescence. This will help us prevent years of pain and
functional impairment as well as considerable
health care expenditures. Given the importance
we attach to prevention, we dedicate four chapters
in the first section of this book to this topic
(chapters “Risk Factors for Patellofemoral Pain.
Prevention Programs”, “Anterior Knee Pain After
Arthroscopic Meniscectomy. Risk Factors, Prevention and Treatment”, “Anterior Knee Pain
Prevalence After Anterior Cruciate Ligament
Reconstruction. Risk Factors and Prevention” and
“Patellar Tendinopathy. Risk Factors, Prevention,
and Treatment”). Furthermore, AKP in an adolescent has a high potential for becoming chronic.
Between 70 and 90% of individuals with AKP
have recurrent or chronic pain [14]. Conchie and
colleagues [15] brought into question the traditional belief that AKP in adolescence is a benign
pathology by showing that it is associated with
patellofemoral osteoarthritis (PFOA) in adulthood. An individual is 7.5 times more likely to
develop PFOA if they have suffered from adolescent AKP. The results of this study are perhaps
debatable, as it was a retrospective study rather
than a longitudinal one. Moreover, the follow-up
time for a longitudinal study of this type should
be 50 years and this is impossible. Furthermore,
the diagnosis of AKP was based on mailed
questionnaires with all their limitations. The
paper by Conchie and colleagues [15] nevertheless questions the traditional belief that adolescent
AKP is a benign pathology. Thus, AKP and
PFOA may form a continuum of disease. Sadly,
many orthopedic surgeons do not focus enough
attention on this pathology, which reflects their
limited understanding.
A very common symptom of great concern to
AKP patients is patellofemoral crepitation (a.k.a.
crepitus). Johnson and colleagues [16] published
a paper in Arthroscopy in 1998 on the assessment of asymptomatic knees. Indeed, patellofemoral crepitation has a high incidence rate in
asymptomatic women (94% in females vs. 45%
in males). Patellofemoral crepitation has been
Patellofemoral Pain: An Overview
associated with the lateral subluxation of the
patella. However, Johnson and colleagues [16]
have observed that lateral subluxation of the
patella (radiographic finding) in asymptomatic
people is more common in males than in females
(35% and 19%, respectively). It leads some to
think that crepitus is not of major importance.
We currently know that this is not the case.
Crepitus is an important symptom: Women with
AKP and pain-free controls with knee crepitus
had lower functional performance compared to
pain-free controls without knee crepitus. This is
an indication that both pain and crepitus may
negatively influence function [17]. Crepitus is a
poorly understood sign and symptom that creates
negative emotions (no one likes a noisy joint),
inaccurate etiological theories, and ultimately
leads to fear-avoidance behaviors (see chapter
“Evaluation of Psychological Factors Affecting
Anterior Knee Pain Patients: The Implications
for Clinicians Who Treat these Patients”) [18].
4
Chondromalacia Patellae.
A Symbol of Our Helplessness
in Regards to a Diagnosis
and Our Ignorance on AKP
Proof that AKP is not well understood is that an
obsolete diagnosis like chondromalacia is still
used by many doctors and physical therapists
today for any pain in the anterior aspect of the
knee. More than a century (116 years) has passed
since the term chondromalacia was coined, and
this term is still used by clinicians, by the staff in
charge of codifying the different pathologies for
our hospital databases, as well as on private
health insurers’ lists of covered services. The
term “Chondromalacia Patellae” continues in use
in the “International Statistical Classification of
Diseases and Related Health Problems (ICD-10,
Version 2019)”, its code being M22.4 (Table 1)
[19].
AKP has historically been associated with the
terms “internal derangement of the knee” and
“chondromalacia patellae”. Surprisingly, the
term “internal derangement of the knee” also
continues in use in the “International Statistical
7
Classification of Diseases and Related Health
Problems (ICD-10, Version 2019)”, its code
M23.9 [19]. The expression “internal derangement of the knee” was coined in 1784 by the
British surgeon from Leeds, William Hey [20].
This term was later discredited by the German
school surgeon Konrad Büdinger, Dr Billroth’s
assistant in Vienna. It was he who described
fissuring and degeneration of the patellar articular cartilage of spontaneous origin in 1906 and
similar lesions of traumatic origin in another
paper in 1908 [21, 22]. Büdinger considered that
the expression “internal derangement of the
knee” was a “wastebasket” term. He was right
since the expression lacks any etiological, therapeutic or prognostic significance.
Until the end of the 1960s, AKP was attributed
to chondromalacia patellae. However, not all the
patients with AKP suffer from “chondromalacia
patellae”, and at the same time many patients with
“chondromalacia patellae” do not have AKP. In
1978, Leslie and Bentley [23] reported that only
51% of patients with a clinical diagnosis of
“chondromalacia” had changes on the patellar
surface when examined by means of arthroscopy.
In 1991, Royle and colleagues [24] published a
study in Arthroscopy, with special reference
made to the PFJ, in which they analysed 500
arthroscopies performed over a 2- period. In those
patients with pain thought to have its origin in this
joint, 63% had “chondromalacia patellae” compared with a 45% incidence in those with
meniscal pathological findings at arthroscopy.
They concluded that AKP patients do not always
have patellar articular changes, and patellar
pathology is often asymptomatic. Consistent with
this, Scott F. Dye did not feel any pain during
arthroscopic palpation of his extensive lesion of
the patellar cartilage without intraarticular anesthesia [25]. In this regard, it should be remembered that the articular cartilage is devoid of nerve
fibres and, therefore, cannot cause pain. Van der
Heijden and colleagues [26] have not detected
any differences in the composition of the patellofemoral cartilage between AKP patients and
healthy controls. Moreover, even patients with
severe patellofemoral chondropathy may not
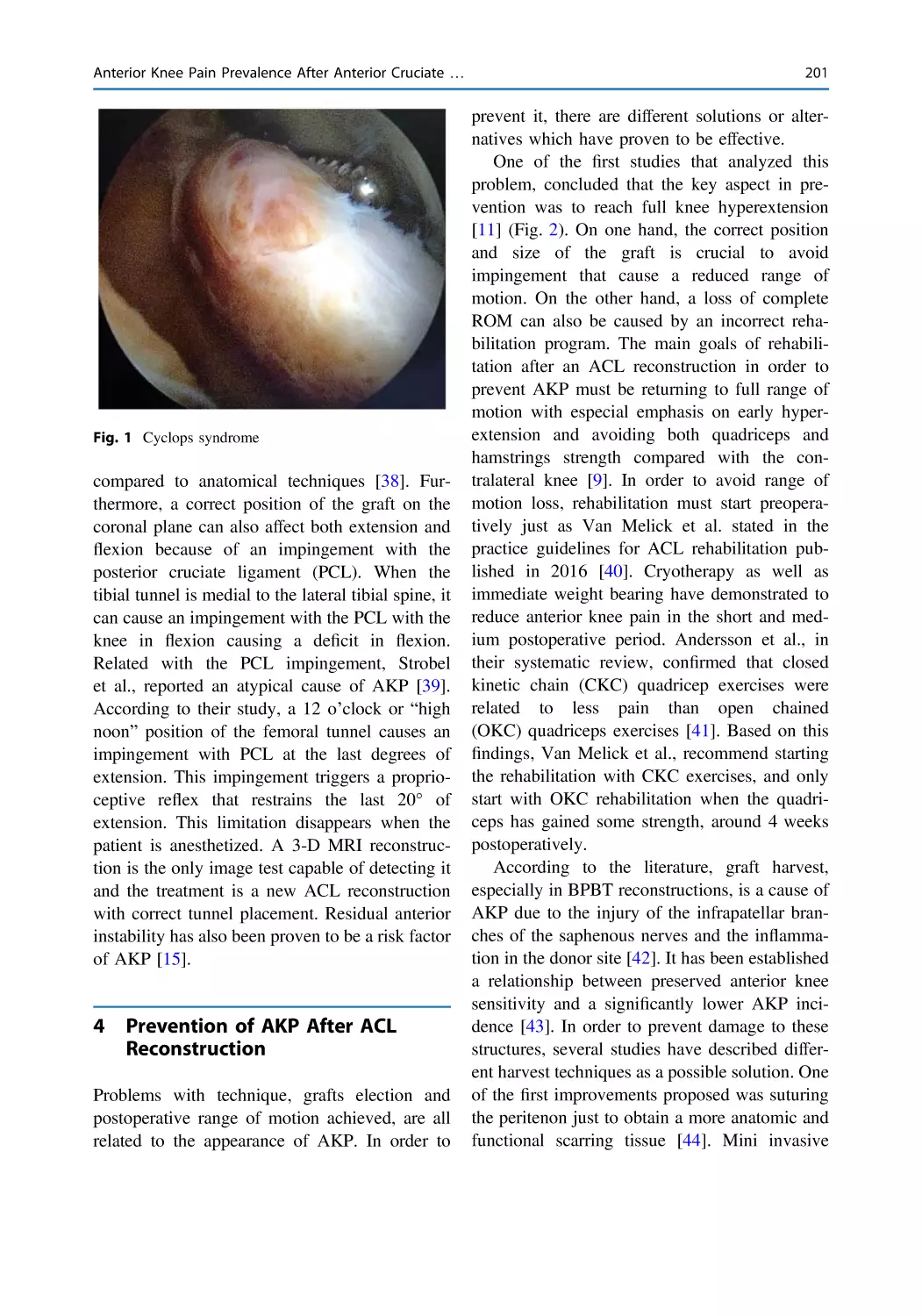
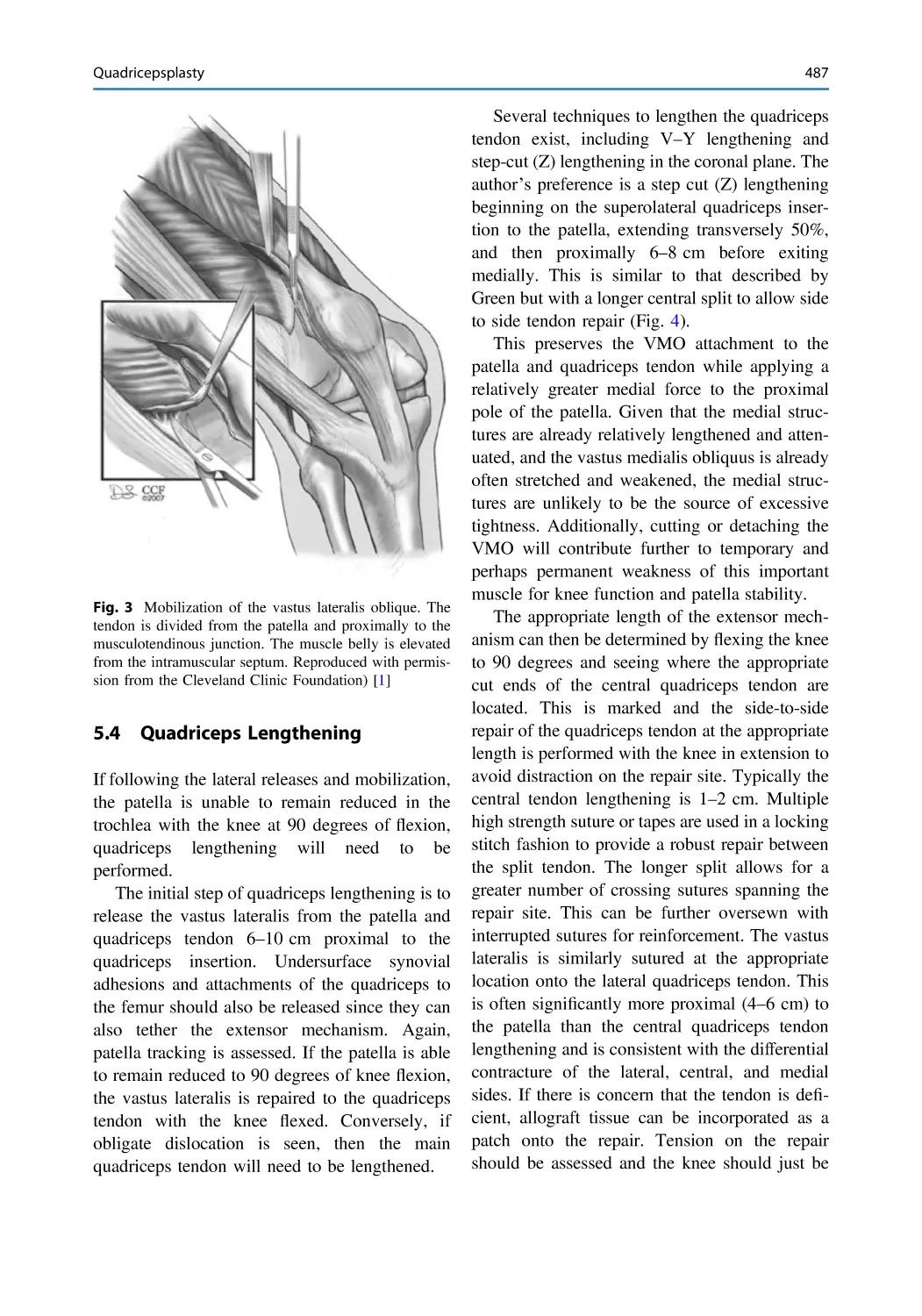
suffer from AKP (Fig. 1).
8
V. Sanchis-Alfonso and R. P. Grelsamer
Table 1 Codification of
patellofemoral disorders by
the International Statistical
Classification of Diseases
and Related Health
Problems in 2019 [19]
M22
Disorders of patella Excl.: Dislocation of patella (S83.0)
M22.0
Recurrent dislocation of patella
M22.1
Recurrent subluxation of patella
M22.2
Patellofemoral disorders
M22.3
Other derangements of patella
M22.4
Chondromalacia patellae
M22.8
Other disorders of patella
M22.9
Disorder of patella, unspecified
A
B
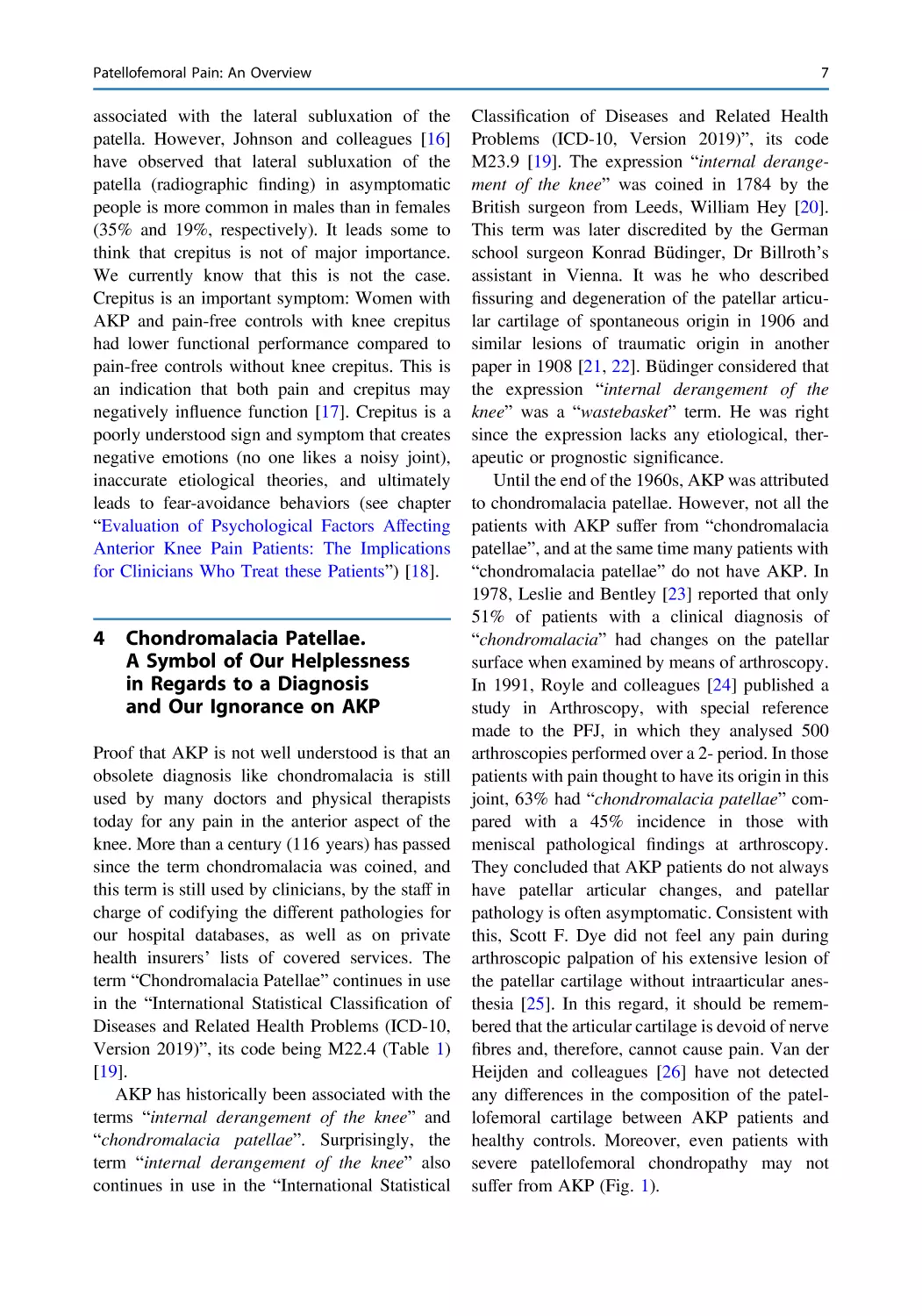
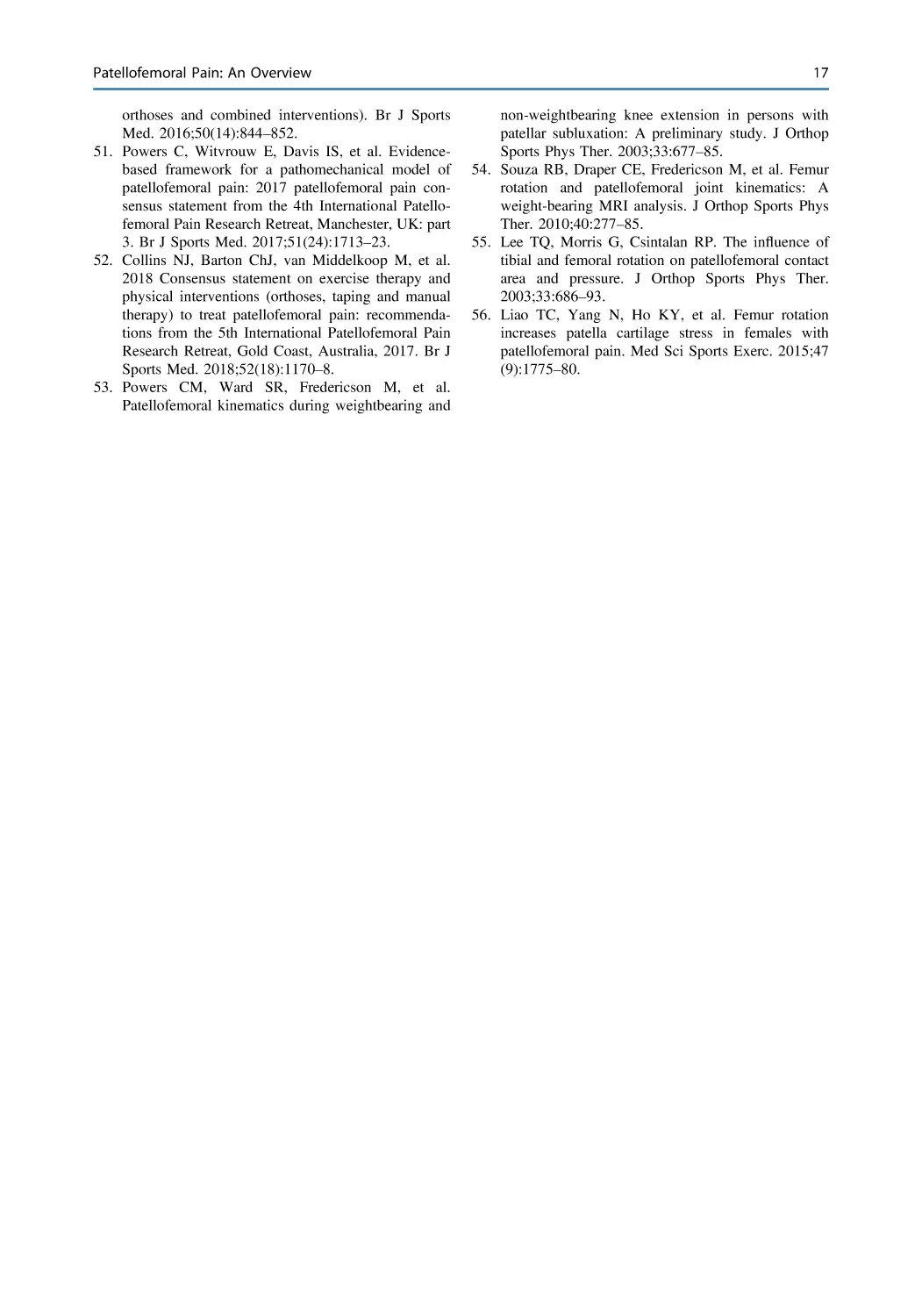
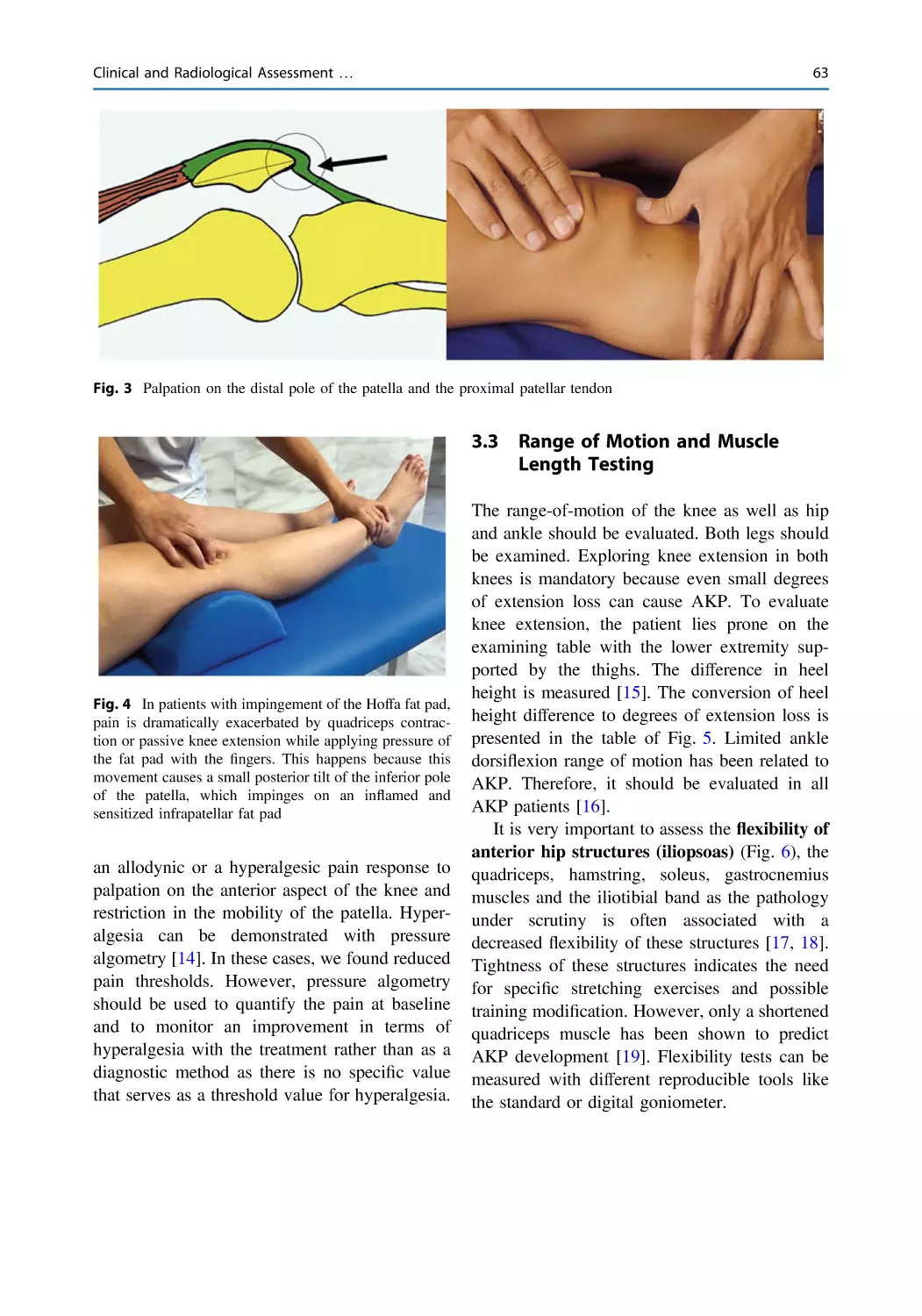
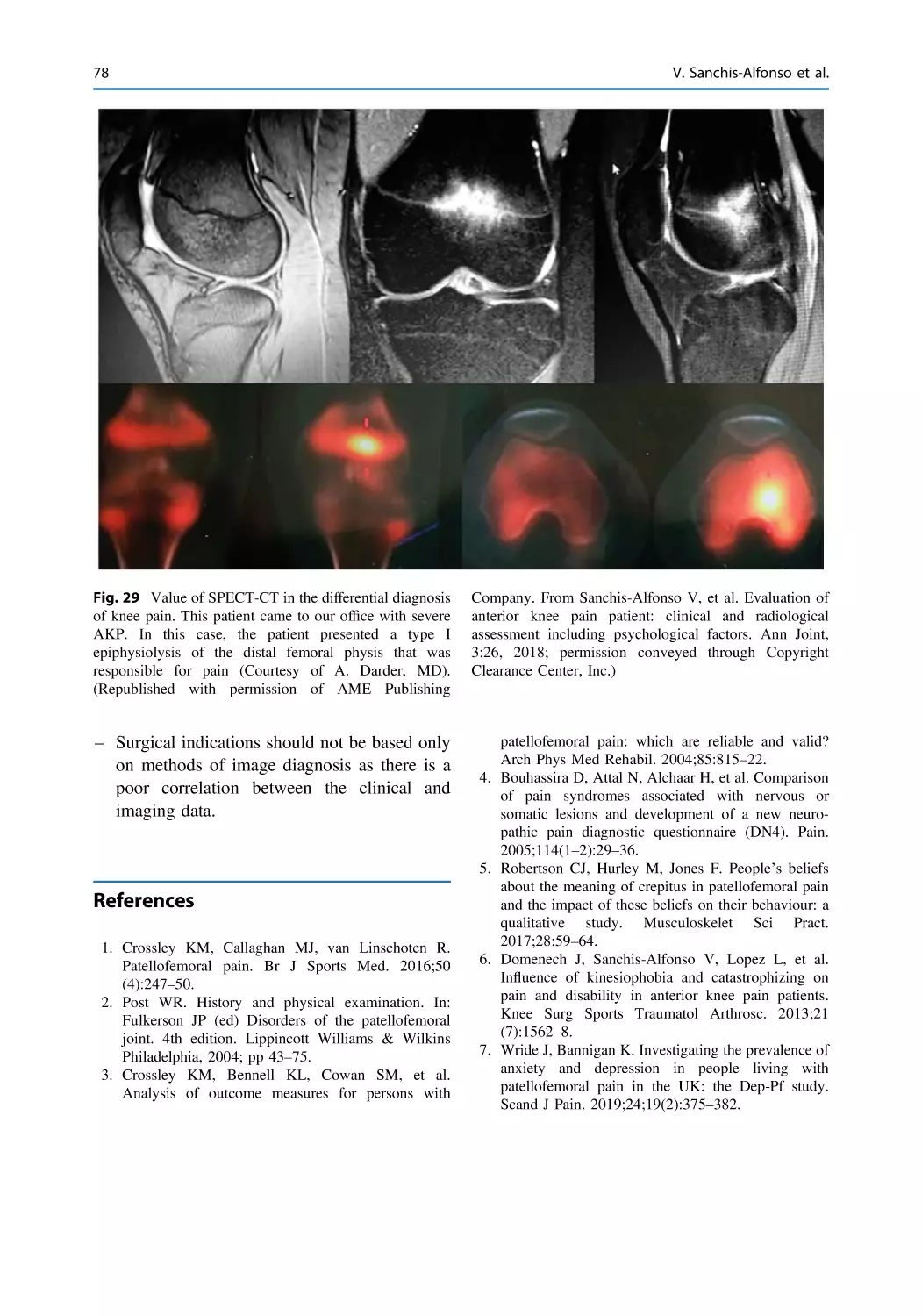
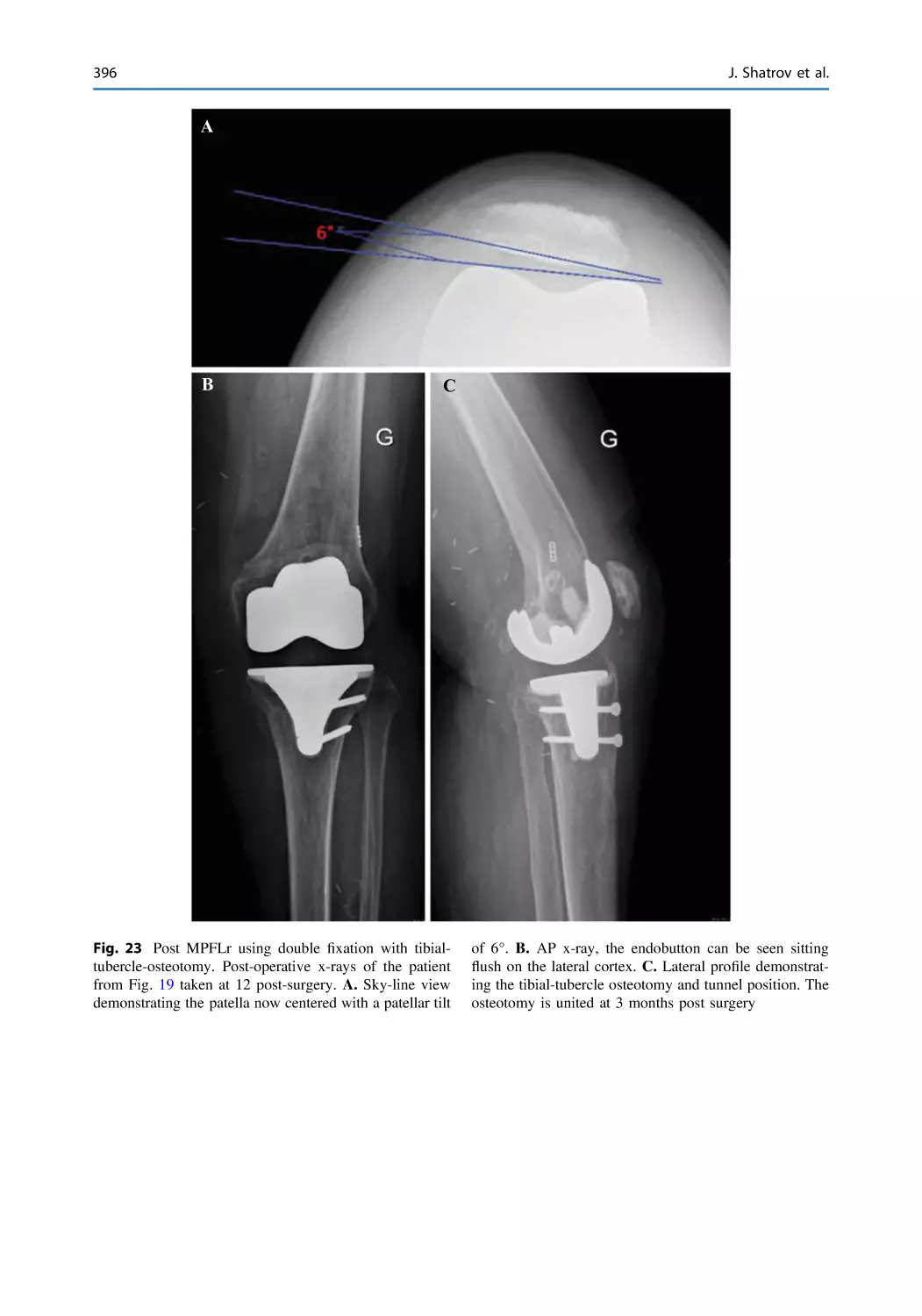
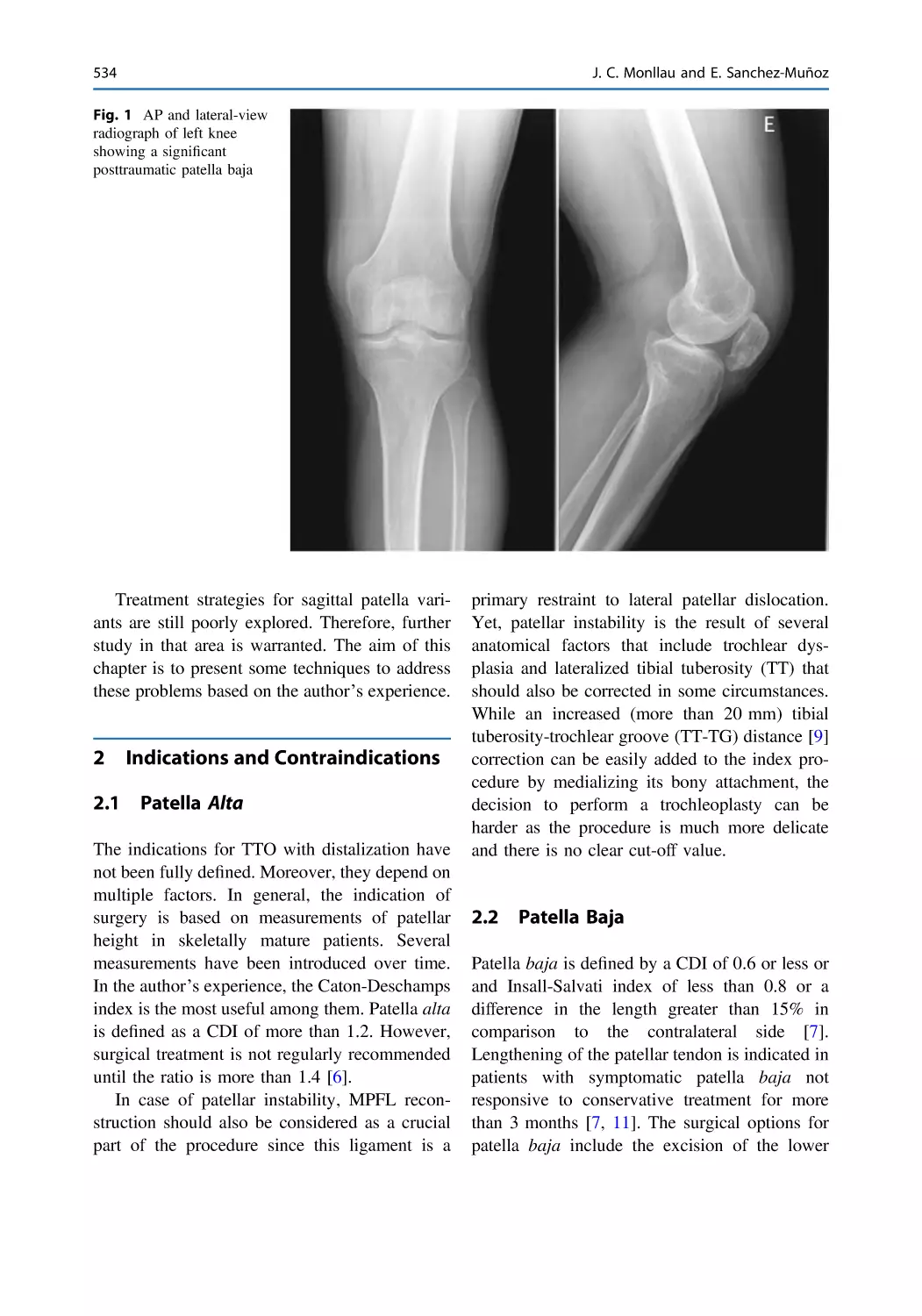
Fig. 1 The intensity of preoperative pain is not related to
the severity or the extension of the chondral lesion found
during surgery. The most serious cases of chondromalacia
arise in patients with a recurrent patellar dislocation who
feel little or no pain between their dislocation episodes
(A). Chondral lesion of the patella with fragmentation and
fissuring of the cartilage in a patient with AKP (B).
(Reprinted by permission from Springer Nature, Anterior
Knee Pain and Patellar Instability by Vicente SanchisAlfonso, 2011)
Consequently, the International Patellofemoral Study Group (IPSG) advises against using
chondromalacia as a diagnosis and suggests the
term “anterior knee pain” as it is only descriptive
without implying a specific diagnosis. Chondromalacia should not be used to describe a clinical
condition. It is merely a descriptive term for
morphological softening of the patellar articular
cartilage. The term “chondromalacia” comes
from the Greek “chondros” and “malakia” and
means “softened articular cartilage”. In conclusion, this is a finding that can be made only upon
palpation with open surgery or by arthroscopic
means, and it is irrelevant. In short, chondromalacia patellae is not synonymous with PFP or
AKP. Although traditions die hard, the term
“chondromalacia patellae” should be excluded
from the clinical terminology for the reasons we
have stated.
The following unfavorable 1908 comment of
Büdinger about “internal derangement of the
knee”, might be applied to “chondromalacia
patellae”: “[It] will simply not disappear from
the surgical literature. It is the symbol of our
helplessness in regard to a diagnosis and our
ignorance of the pathology” [27]. The term
chondromalacia is a twentieth century mistake.
Unfortunately, we always make the same mistakes, as evidenced by the expression “patellofemoral pain syndrome” having replaced
“chondromalacia patellae.” Thus, one nonsense
has been replaced by another.
Patellofemoral Pain: An Overview
5
Patellar Malalignment Versus
Skeletal Lower Limb
Malalignment
9
In the 1970s, AKP was correlated with the
presence of patellar malalignment (PM). PM “is
the abnormal positioning of the patella in any
plane” (Fig. 2) [28]. The most common type of
patellar malalignment is patellar tilt [27]. Moreover, a lateralized tibial tuberosity is included in
the patellar malalignment category because it
leads to a lateral force vector on the patella that
might be responsible for pain and/or lateral displacement of the patella.
In 1968, Jack C. Hughston (Fig. 3) published
an article on subluxation of the patella that represented a major turning point in the recognition
and treatment of patellofemoral disorders [29]. In
1974, Al Merchant (Fig. 4), in an attempt to
better understand patellofemoral biomechanics,
introduced his version of the patellofemoral axial
radiograph [30]. The same author suggested, also
in 1974, the open lateral retinacular release as a
way of treating recurrent patellar subluxation
[31]. In 1975, the French orthopedist Paul Ficat
popularized the concept of patellar tilt, always
associated with increased tightness of the lateral
retinaculum, which causes excessive pressure on
the lateral facet of the patella leading to the
“lateral patellar compression syndrome”
(“Syndrome d’Hyperpression Externe de la
Rotule”) [32]. In fact, the excessive lateral pressure syndrome represents a type of PM.
According to Ficat, the lateral patellar compression syndrome causes hyperpressure in the lateral
patellofemoral compartment and hypopressure in
the
medial
patellofemoral compartment.
Hypopressure and the disuse of the medial
patellar facet cause malnutrition and early
degenerative cartilage changes. This may explain
the early cartilage degeneration found in the
medial patellar facet. Hyperpression also leads to
cartilage degeneration, thus the degeneration of
the lateral cartilage.
In 1977, Ficat and Hungerford published
“Disorders of the Patellofemoral Joint.” It is a
classic of knee extensor mechanism surgery and
the first book in English devoted exclusively to
the extensor mechanism of the knee [27]. In the
preface of the book, these authors refer to the PFJ
as “the forgotten compartment of the knee”
reflecting the situation through the 1970s. In fact,
only two diagnoses were used relating to AKP or
patellar instability before the 1970s: chondromalacia patellae and recurrent dislocation of the
patella. What’s more, the initial designs for knee
arthroplasties ignored the PFJ. In Fig. 5, you can
see the logo of the International Knee Society in
the late 1980s. There is no patella. In 1995, in
Hong Kong, the International Society of the
Fig. 2 CT at 0º of a patient with AKP and functional
patellofemoral instability in the right knee. However, the
left knee was completely asymptomatic. The PM was
symmetric in both knees. (Reprinted by permission from
Springer Nature, Anterior Knee Pain and Patellar Instability by Vicente Sanchis-Alfonso, 2011)
10
Fig. 3 Jack C. Hughston, MD (1917–2004). One of the
founding fathers of Sports Medicine (The Hughston
Foundation, Inc. © 2022)
V. Sanchis-Alfonso and R. P. Grelsamer
Knee (ISK) and the International Arthroscopy
Association (IAA) merged to found ISAKOS.
Curiously, the ISAKOS logo, which is relatively
modern, does not show the patella either. The
same goes for the logos of ESSKA and of the
Asia–Pacific Knee Arthroscopy Sports Medicine
Society. This reflects the little importance knee
surgeons have placed on the PFJ.
In 1979, John Insall published a paper on the
“patellar malalignment syndrome” and his
proximal patellar realignment technique used to
treat this “syndrome” [33, 34]. According to
Insall, lateral loading of the patella is increased in
the malalignment syndrome. In some cases, this
causes “chondromalacia patellae” but this does
not correlate with the presence/absence of pain.
Accordingly, Insall and colleagues [35] reported
in 1983 that AKP correlates better with
malalignment rather than with the severity of
cartilage changes found at surgery. Fulkerson
and colleagues have also emphasized the
importance of PM and an excessively tight lateral
Fig. 4 John Fulkerson (left) and Alan C Merchant (right), IPSG Meeting, Boston, MA, USA, 2006
Patellofemoral Pain: An Overview
Fig. 5 Logo of the International Knee Society. 6th
Congress of the International Society of the Knee, Rome,
8th-12th May 1989—Cavalieri Hilton Hotel
retinaculum as a source of AKP [36, 37].
Moreover, John Fulkerson (Fig. 4) popularized
the anteromedialization (AMZ) of the tibial
tuberosity in 1983 to address pain from patellofemoral chondropathy with patellofemoral tilt
and/or chronic patellar subluxation [38]. This
technique is indicated when restoring normal
patellar tracking. This widely appreciated procedure is not only used for isolated PFOA but for
chronic lateral patellar instability.
For many years, PM has been widely accepted
as an explanation for the genesis of AKP in the
young patient. Moreover, this theory had a great
influence on orthopedic surgeons who developed
several surgical procedures to “correct the
malalignment.” Unfortunately, PM has too often
been treated surgically. Many surgical treatments
have been described yielding extremely variable
results. Consequently, the PM concept is currently questioned, and is not universally accepted
as a source of AKP. In fact, the number of
realignment surgeries performed has dropped
dramatically in recent years, at least in Spain, due
to a reassessment of this paradigm. To think of
AKP as somehow being necessarily tied to PM is
an oversimplification that has stultified progress
toward better diagnosis and treatment. Overreliance on PM as a diagnosis leads to misguided
surgical procedures that can aggravate a patient’s
condition.
At the end of 1970s, skeletal malalignment of
the lower limb was suggested as one of the
causes of AKP in some young patients [39]. It
must be acknowledged that skeletal malalignment is not an abnormal Q-angle or an increased
11
TT-TG distance [40]. It is also not the position of
the patella in the trochlea. Neither is it its
increased shift (subluxation) or increased tilt
[40]. Skeletal malalignment is malalignment of
the limb measured on the transverse, coronal, and
sagittal planes [40]. For example, the presence of
femoral torsion, excessive external tibial torsion,
or increased varus or valgus abnormalities have a
great impact on PFJ biomechanics. Rotational
abnormalities are particularly important [40–42].
In 1979, Stan James presented a comprehensive
review of AKP in which the condition of “miserable malalignment” was described, being
increased femoral anteversion and increased
external tibial torsion [39]. In 1995, he reported
on seven patients with “miserable malalignment”
who had been treated with internal tibial rotational osteotomy over an 18-year period [43].
Several years earlier, in 1990, Cooke and colleagues described internal proximal tibial rotational osteotomy in seven patients presenting
with AKP and drew attention to the inwardly
pointing knee (“squinting patella”) as an unrecognized cause of AKP [44]. However, the concept of skeletal malalignment was almost
unnoticed and has had extremely little influence
on orthopedic surgeons even until a few years
ago. In fact, very few publications refer to
skeletal malalignment as a cause of AKP. From
1990 to June of 2021, only 22 published papers
in English in which the association between
patellofemoral disorders in young patients and in
which torsional abnormalities of the femur and/or
tibia are analyzed from a clinical point of view
could be found [45]. One of the world's greatest
exponents of the skeletal malalignment theory in
the genesis of patellofemoral pain is Robert A.
Teitge, MD (Fig. 6), one of the prominent
members of the International Patellofemoral
Study Group (IPSG).
In short, structural abnormalities predispose to
pain but are not automatically the source of pain
in any given patient. If you have flat feet and foot
pain, your foot pain does not necessarily relate to
your flat feet. Structural abnormalities are only a
predisposing factor just as hypertension predisposes to strokes—even though not everyone with
hypertension suffers from a stroke.
12
V. Sanchis-Alfonso and R. P. Grelsamer
Fig. 6 Vicente SanchisAlfonso (left) and Robert A.
Teitge (right), IPSG Meeting,
Banff, Canada, 2019
(Courtesy of
Ronald P. Grelsamer, MD)
6
Tissue Homeostasis Theory.
An Alternative
to the Structural/Biomechanic
Paradigm
In the 1990s, Scott F. Dye (Fig. 7), of the
University of California, San Francisco, and his
research group came up with the tissue homeostasis theory [46, 47]. The initial observation
that led to the development of the tissue homeostasis theory of patellofemoral pain was made
by Dye when a patient with complaints of AKP
without evidence of chondromalacia or
malalignment underwent a technetium 99 m
methylene diphosphonate bone scan evaluation
of the knees. It was an attempt to assess the
possible presence of covert osseous pathology;
and indeed, the bone scan of that individual
manifested an intense diffuse patellar uptake
despite normal radiographic images.
The tissue homeostasis theory states that
joints are more than mechanical structures; they
are living metabolically active systems. This
theory attributes pain to a physiopathological
mosaic of causes such as increased osseous
remodelling, increased intraosseous pressure, or
peripatellar synovitis that leads to a decrease in
what he called the “Envelope of Function” (or
“Envelope of Load Acceptance”). The “Envelope
of Function” describes a range of loading and
energy absorption that is compatible with tissue
homeostasis of an entire joint system; that is,
with the mechanisms of healing and maintenance
Fig. 7 Scott F. Dye, IPSG Meeting, San Diego, CA,
USA, 2011 (Courtesy of Ronald P. Grelsamer, MD)
of normal tissues. Obviously, the Envelope of
Function for a young athlete will be greater than
that of sedentary elderly individual. Within the
Envelope of Function is the region termed Zone
of Homeostasis. Loads that exceed the Envelope
of Function but are insufficient to cause a
macrostructural failure are termed the Zone of
Supraphysiologic Overload. If sufficiently great
forces are put on the patellofemoral system,
macrostructural failure can occur.
For Dye [46], the following four factors
determine the Envelope of Function or Zone of
Homeostasis: (1) anatomic factors (the morphology, structural integrity and biomechanical
characteristics of tissue); (2) kinematic factors
(dynamic control of the joint involving proprioceptive sensory output, cerebral and cerebellar
Patellofemoral Pain: An Overview
sequencing of motor units, spinal reflex mechanisms, and muscle strength and motor control);
(3) physiological factors (the genetically determined mechanisms of molecular and cellular
homeostasis that determine the quality and rate of
repair of damaged tissues); and (4) treatment
factors (type of rehabilitation or surgery
received).
According to Dye, the loss of both osseous and
soft tissue homeostasis is more important in the
genesis of AKP than structural characteristics. To
him, it matters little which specific structural
factors may be present (i.e., patellar cartilage
lesions, PM, etc.) if the joint is being loaded
within its Envelope of Function and is therefore
asymptomatic. He suggests that patients with
AKP are often symptomatic due to supraphysiological loading of anatomically normal
knee components [47]. In fact, AKP patients
often lack an easily identifiable structural abnormality to account for the symptoms. The Envelope of Function frequently diminishes after an
episode of injury to the point where previously
well-tolerated activities of daily living (e.g., stair
climbing, sitting down in and arising out of
chairs, pushing the clutch of a car) become supraphysiological loads for that patient, leading to
ineffective tissue healing and continued symptoms. Bringing loads down within the newly
diminished Envelope of Function allows for the
normal tissue healing processes to go forward.
7
Creation of Study Groups:
An Inflection Point
in the Knowledge
of Patellofemoral Pain
We are therefore faced with a very prevalent
symptom with multiple possible etiologies. This
is fertile ground for a study group.
In 1994, Jean Yves Dupont from France,
travelled to Farmington, Connecticut in the USA
to visit John Fulkerson. They decided to gather
“a group of friends” from different countries with
a proven interest in the academic study of
patellofemoral problems. They would meet
13
informally to take stock of their patellofemoral
opinions. Dr. Fulkerson served as the first secretary and organizer of the study group and set
up an initial meeting in Orlando, Florida on
February 17, 1995. Thus was born the International Patellofemoral Study Group (IPSG). The
second meeting of the IPSG was held near
Dupont’s home in beautiful Benodet in Brittany
(France) in the fall of 1995 (Fig. 8). Each participant was encouraged to speak on a patellofemoral topic of his choice, and the group was
encouraged to discuss, debate, and critique.
Around this time, Joan and Al Merchant
designed the logo for the IPSG. Patellofemoral
pain is of such complexity that even within this
group there are opposing approaches and theories
with surgeons, therapists and engineers often
holding dogmatic positions. Perhaps less dogmatic over time.
Moreover, in 2003, John Fulkerson created
with the help of Eric Dahlinger, Dr. Peter Jokl,
and tennis legend Ivan Lendl, the Patellofemoral
Foundation (www.patellofemoral.org). to stimulate research efforts, education, and fundraising.
The Patellofemoral Foundation sponsors the
“Patellofemoral Research Excellence Award” to
encourage outstanding PF research. Moreover,
this foundation sponsors the “Patellofemoral
Traveling Fellowship” to stimulate global patellofemoral communication. Finally, the Patellofemoral Foundation awards the “Patellofemoral
Lifetime Achievement Award” every year in
recognition of those surgeons who have dedicated their career to the understanding and
treatment of patients with patellofemoral disorders along with organizing the “Comprehensive
Patellofemoral Online Education Course.”
In 2009, the International Patellofemoral
Research Network (iPFRN), a group of
researchers and clinicians with a specific interest
in patellofemoral pain, was founded. The iPFRN
was established by five global leaders in patellofemoral pain research. They are Irene Davis,
Chris Powers, Kay Crossley, Jenny McConnell
and Erik Witvrouw. This group has published 7
consensus statements in high impact journals
since 2009 [1, 14, 48–52].
14
V. Sanchis-Alfonso and R. P. Grelsamer
Fig. 8 IPSG Meeting, Benodet, France, Fall 1995. (Courtesy of Ronald P. Grelsamer, MD)
8
The “Proximal Control”
Concept—A Turning Point
Historically, the patella has been considered a
mobile structure that sits on a fixed structure that
is the femur. That thinking is based on kinematic
studies done without weight-bearing or in studies
in which the femur has been considered a fixed
structure.
In the 2000s, Chris Powers, of the University
of Southern California, Los Angeles, and his
working group conducted studies of the PFJ with
weight-bearing and suggested that the main
factor contributing to patella tilt and lateral displacement during weight-bearing is the internal
rotation of the femur. Powers and colleagues
[53] published a study in 2003 in which the
objective was to compare PFJ kinematics during
non-weight-bearing and weight-bearing knee
extension in people with AKP and lateral
patellar subluxation. They demonstrated that
lateral patellar displacement was more pronounced during non-weight-bearing (open chain)
compared to weight-bearing (closed chain) knee
extension. However, PFJ kinematics during nonweight-bearing was characterized by the rotation
of the patella on the femur, while it was characterized by the femur rotating underneath the
patella during weight-bearing. In 2010, Chris
Powers and colleagues published another study
comparing PFJ kinematics, femoral rotation, and
patella rotation between females with AKP and
pain-free controls using weight-bearing kinematic MRI [54]. The results of that study suggest
that the control of femur rotation may be
important to restoring normal PFJ kinematics.
That is, the problem of PM is not in the patella
but in the femur. In other words, the primary
contributor to lateral patellar subluxation and
patellar tilt is the internal rotation of the femur
underneath the patella. Therefore, control of the
rotation of the femur is fundamental to guaranteeing normal patellofemoral kinematics. This
theory supposes a change in mentality relative to
the concept of PM. It is a true turning point.
These findings suggest that control of the rotation
of the femur is essential to restoring the normal
Patellofemoral Pain: An Overview
kinematics of the PFJ. In addition, normalizing
femoral rotation can affect the tension of peripatellar soft structures, including the lateral retinaculum, and can also affect patellofemoral
pressures. Lee and colleagues [55] have demonstrated that femoral rotation results in an increase
in PFJ contact pressures on the contralateral facet
of the patella (i.e., lateral PFJ during internal
rotation of the femur and vice versa). Using a
finite element model, Liao and colleagues [56]
have demonstrated that internal rotation of the
femur provokes an increment in PFJ stress.
We are thus facing a paradigm shift. It has
been shown that excessive internal rotation of the
femur can cause (1) a decrease in the patellofemoral contact area and therefore an increase in
patellofemoral pressure and (2) tightness of the
lateral retinaculum. Thus, a new concept was
born: the “proximal control” concept that is
currently fundamental to understanding the
physiotherapeutic treatment of an important
subgroup of AKP patients. Therefore, a treatment
that addresses the control of femoral motion may
play a crucial role in the treatment of some AKP
patients. This way of thinking is diametrically
opposed to the one that had been maintained
until this moment, which was to consider patella
tracking as the relative motion of the patella on a
fixed femur.
9
Take Home Message
To summarize, the high incidence and prevalence
of AKP along with its high associated disability,
its high potential for becoming chronic, and its
association with PFOA in adulthood makes PFP
an urgent research priority.
References
1. Crossley KM, Stefanik JJ, Selfe J, et al. Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat,
Manchester. Part 1: Terminology, definitions, clinical
examination,
natural
history,
patellofemoral
osteoarthritis and patient-reported outcome m. Br J
Sports Med 2016;50:839–843.
15
2. Crossley KM, Callaghan MJ, van Linschoten R.
Patellofemoral pain. Br J Sports Med. 2016;50
(4):247–50.
3. Smith BE, Selfe J, Thacker D, et al. Incidence and
prevalence of patellofemoral pain: a systematic
review and meta-analysis. PLoS ONE. 2018;13(1):
e0190892.
https://doi.org/10.1371/journal.pone.
0190892.
4. Maselli F, Storari L, Barbari V, et al. Prevalence and
incidence of low back pain among runners: a
systematic review. BMC Musculoskelet Disord.
2020;21(1):343.
5. Wallace IJ, Worthington S, Felson DT, et al. Knee
osteoarthritis has doubled in prevalence since the
mid-20th century. Proc Natl Acad Sci USA.
2017;114(35):9332–6.
6. Rathleff MS, Petersen KK, Arendt-Nielsen L, et al.
Impaired conditioned pain modulation in young
female adults with long-standing patellofemoral pain:
a single blinded cross-sectional study. Pain Med.
2016;17(5):980–8.
7. Grelsamer RP. Patellar nomenclature. The tower of
babel revisited. Clin Orthop. 2005;436:60–65.
8. Collins NJ, Bierma-Zeinstra SM, Crossley KM, et al.
Prognostic factors for patellofemoral pain: a multicentre observational analysis. Br J Sports Med.
2013;47(4):227–33.
9. Reijnders L, van de Groes SA. The quality of life of
patients with patellofemoral pain—a systematic
review. Acta Orthop Belg. 2020;86(4):678–87.
10. Tan SS, van Linschoten RL, van Middelkoop M,
et al. Cost-utility of exercise therapy in adolescents
and young adults suffering from the patellofemoral
pain syndrome. Scand J Med Sci Sports.
2010;20:568–79.
11. Sanchis-Alfonso V, Merchant AC. Iatrogenic medial
patellar instability: an avoidable injury. Arthroscopy.
2015;31(8):1628–32.
12. van der Heijden RA, de Kanter JL, Bierma-Zeinstra
SM, et al. Structural abnormalities on magnetic
resonance imaging in patients with patellofemoral
pain: A cross-sectional case-control study. Am J
Sports Med. 2016. pii: 0363546516646107.
13. Rathleff MS, Rathleff CR, Olesen JL, et al. Is knee
pain during adolescence a self-limiting condition?
Prognosis of patellofemoral pain and other types of
knee pain. Am J Sports Med. 2016;44(5):1165–71.
14. Powers CM, Bolgla LA, Callaghan MJ, et al.
Patellofemoral pain: proximal, distal, and local
factors, 2nd International Research Retreat.
J Orthop Sports Phys Ther. 2012;42:A1-54.
15. Conchie H, Clark D, Metcalfe A, et al. Adolescent
knee pain and patellar dislocations are associated
with patellofemoral osteoarthritis in adulthood: A
case control study. Knee. 2016. https://doi.org/10.
1016/j.knee.2016.04.009.
16. Johnson, LL. van Dyk E, Green JR et al. Clinical
assessment of asymptomatic knees: comparison of
men and women. Arthroscopy. 1998;14:347–359.
16
17. De Oliveira SD, Barton C, Crossley K, et al.
Implications of knee crepitus to the overall clinical
presentation of women with and without patellofemoral pain. Phys Ther Sport. 2018;33:89–95.
18. Robertson CJ, Hurley M, Jones F. People’s beliefs
about the meaning of crepitus in patellofemoral pain
and the impact of these beliefs on their behaviour: a
qualitative study. Musculoskelet Sci Pract.
2017;28:59–64.
19. International Statistical Classification of Diseases and
Related Health Problems 10th Revision (ICD-10)WHO Version 2019.
20. Levay D. The history of orthopaedics. New Jersey:
The Parthenon Publishing Group; 1990.
21. Budinger K. Üeber ablösung von gelenkteilen und
verwandte prozesse. Dtsch Z Chir. 1906;84:311–65.
22. Budinger K. Üeber traumatische knorpelrisse im
kniegelenk. Dtsch Z Chir. 1908;92:510.
23. Leslie IJ, Bentley G. Arthroscopy in the diagnosis of
chondromalacia patellae. Ann Rheum Dis.
1978;37:540–7.
24. Royle SG, Noble J, Davies DR, et al. The significance of chondromalacic changes on the patella.
Arthroscopy. 1991;7:158–60.
25. Dye SF, Vaupel GL, Dye CC. Conscious neurosensory mapping of the internal structures of the human
knee without intra-articular anesthesia. Am J Sports
Med. 1998;26:773–7.
26. van der Heijden RA, Oei EHG, Bron EE, et al. No
difference on quantitative magnetic resonance imaging in patellofemoral cartilage composition between
patients with patellofemoral pain and healthy controls. Am J Sports Med. 2015;44(5):1172–8.
27. Ficat P, Hungerford DS. Disorders of the PatelloFemoral Joint. Baltimore: Williams & Wilkins; 1977.
28. Grelsamer R. Patellar malalignment: current Concepts Review. J Bone Joint Surg. 2000;82A:1639–
50.
29. Hughston JC. Subluxation of the patella. J Bone Joint
Surg. 1968;50-A: 1003–1026.
30. Merchant AC, Mercer RL, Jacobsen RH et al.
Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg. 1974; 56-A: 391–1396.
31. Merchant AC, Mercer RL. Lateral release of the
patella: a preliminary report. Clin Orthop.
1974;103:40.
32. Ficat P, Ficat C, Bailleux A. Syndrome d’hyperpression externe de la rotule (S.H.P.E). Rev Chir
Orthop. 1975;61: 39–59.
33. Insall J. “Chondromalacia Patellae”: Patellar
malalignment syndrome. Orthop Clin North Am.
1979;10:117–27.
34. Insall J, Bullough PG, Burnstein AH. Proximal
“tube” realignment of the patella for chondromalacia
patellae. Clin Orthop. 1979;144:63–9.
35. Insall JN, Aglietti P, Tria AJ Jr. Patellar pain and
incongruence. II: Clinical application. Clin
Orthop. 1983;176:225–232.
V. Sanchis-Alfonso and R. P. Grelsamer
36. Fulkerson JP. The etiology of patellofemoral pain in
young, active patients: a prospective study. Clin
Orthop. 1983;179:129–33.
37. Fulkerson JP, Tennant R, Jaivin JS. Histologic
evidence of retinacular nerve injury associated with
patellofemoral
malalignment.
Clin
Orthop. 1985;197:196–205.
38. Fulkerson JP. Anteromedialization of the tibial
tuberosity for patellofemoral malalignment. Clin
Orthop Relat Res. 1983;177:176–81.
39. James, S.L. Chondromalacia of the Patella in the
Adolescent. In: Kennedy JC. editor. The Injured
Adolescent Knee. Baltimore: The Williams &
Wilkins Company, 1979.
40. Teitge RA. Patellofemoral disorders correction of
rotational malalignment of the lower extremity. In:
Noyess, knee disorders: surgery, rehabilitation, clinical outcomes, Elsevier, 2017.
41. Teitge RA. Does lower limb torsion matter? Tech
Knee Surg. 2012;11:137–46.
42. Teitge RA. The power of transverse plane limb malalignment in the genesis of anterior knee pain—
clinical relevance. Ann Joint. 2018;3:70.
43. Meister K, James SL. Proximal tibial derotation
osteotomy for anterior knee pain in the miserably
malaligned extremity. Am J Orthop (Belle Mead NJ).
1995;24:149–55.
44. Cooke TD, Price N, Fisher B. The inwardly pointing
knee. An unrecognized problem of external rotational
malalignment. Clin. Orthop Relat. 1990;56–60.
45. Sanchis-Alfonso V, Domenech-Fernández J, FerràsTarragó J, et al. The incidence of complications after
derotational femoral and/or tibial osteotomies in
patellofemoral disorders in adolescents and active
adult patients. A Systematic Review with MetaAnalysis. (In press).
46. Dye SF. The knee as a biologic transmission with an
envelope of function: a theory. Clin Orthop.
1996;325:10–8.
47. Dye SF, Staubli HU, Biedert RM, et al. The mosaic
of pathophysiology causing patellofemoral pain:
therapeutic implications. Operative Techn Sports
Med. 1999;7:46–54.
48. Davis IS, Powers C. Patellofemoral pain syndrome:
proximal, distal, and local factors—an international
research retreat: April 30–May 2, 2009, Fells Point,
Baltimore. MD J Orthop Sports Phys Ther. 2010;40
(3):A1–48.
49. Witvrouw E, Callaghan MJ, Stefanik JJ, et al.
Patellofemoral pain: consensus statement from the
3rd International Patellofemoral Pain Research
Retreat held in Vancouver. Br J Sports Med.
2014;48(6):411–4.
50. Crossley KM, van Middelkoop M, Callaghan MJ,
et al. 2016 Patellofemoral pain consensus statement
from the 4th International Patellofemoral Pain
Research Retreat, Manchester. Part 2: recommended
physical interventions (exercise, taping, bracing, foot
Patellofemoral Pain: An Overview
orthoses and combined interventions). Br J Sports
Med. 2016;50(14):844–852.
51. Powers C, Witvrouw E, Davis IS, et al. Evidencebased framework for a pathomechanical model of
patellofemoral pain: 2017 patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester, UK: part
3. Br J Sports Med. 2017;51(24):1713–23.
52. Collins NJ, Barton ChJ, van Middelkoop M, et al.
2018 Consensus statement on exercise therapy and
physical interventions (orthoses, taping and manual
therapy) to treat patellofemoral pain: recommendations from the 5th International Patellofemoral Pain
Research Retreat, Gold Coast, Australia, 2017. Br J
Sports Med. 2018;52(18):1170–8.
53. Powers CM, Ward SR, Fredericson M, et al.
Patellofemoral kinematics during weightbearing and
17
non-weightbearing knee extension in persons with
patellar subluxation: A preliminary study. J Orthop
Sports Phys Ther. 2003;33:677–85.
54. Souza RB, Draper CE, Fredericson M, et al. Femur
rotation and patellofemoral joint kinematics: A
weight-bearing MRI analysis. J Orthop Sports Phys
Ther. 2010;40:277–85.
55. Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. J Orthop Sports Phys Ther.
2003;33:686–93.
56. Liao TC, Yang N, Ho KY, et al. Femur rotation
increases patella cartilage stress in females with
patellofemoral pain. Med Sci Sports Exerc. 2015;47
(9):1775–80.
Pathophysiology of Anterior Knee
Pain
Vicente Sanchis-Alfonso, Esther Roselló-Sastre,
Scott F. Dye, and Robert A. Teitge
1
Introduction
Anterior knee pain (AKP) is the most common
reason for adolescents, adults, and physically
active people to consult with an orthopedic surgeon who specializes in the knee. Despite the
high incidence and prevalence of AKP and an
abundance of clinical and basic science research,
the etiology of this condition is not well-known.
This chapter synthesizes a review of the literature
and our research and clinical experience on
pathophysiology of AKP in the young patient.
2
Theories on the Genesis of AKP
Until the end of the 1960s, AKP was attributed to
chondromalacia patellae, a concept from the
early twentieth century [1] that has no clinical
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
E. Roselló-Sastre
Department of Pathology, Hospital General de
Castellón, Castellón, Spain
S. F. Dye
University of California San Francisco, San
Francisco, CA, USA
R. A. Teitge
Wayne State University, Detroit, MI, USA
value because it offers no specific diagnostic,
therapeutic, or prognostic implications. In fact,
many authors have failed to find a clear connection between AKP and chondromalacia
patellae [2, 3].
In the 1970s AKP was related to the presence
of patellar malalignment (PM) [4–8]. For many
years, PM has been widely accepted as an
explanation for the genesis of AKP in the young
patient. Currently, the PM concept is questioned
and is not universally accepted as an underlying
factor in AKP. An obvious problem with the PM
concept is that not all patellar malalignments,
even those of significant proportions, are symptomatic (Fig. 1). A person with PM may not
experience pain if the joint is never stressed to
the extent that the tissues are irritated. Such
individuals probably learn early that “my knee
hurts when I do sports” and therefore stop being
active. Further, only one knee may be symptomatic, even though the underlying patellar
malalignment is entirely symmetrical in both
knees (Fig. 1). In addition, patients with normal
patellar alignment on computed tomography
(CT) can also experience AKP. Therefore,
although the patellar malalignment theory is
biomechanically appealing, it has failed to
explain the presence of AKP in many patients.
We must also remember that significant differences have been demonstrated between subchondral bone morphology and the geometry of
the articular cartilage surface of the patellofemoral joint (PFJ), in both the axial and sagittal
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_2
19
20
V. Sanchis-Alfonso et al.
Fig. 1 Disabling AKP and patellar instability of the left
knee. The right knee was asymptomatic in spite of the fact
that PM was symmetric in both knees. A Preop CT at 0°,
B Postop CT at 6 months of proximal realignment
surgery, C CT of the right knee, D CT of the left knee
at 13 years of follow-up—the patient is completely
asymptomatic in spite of the presence of a visible PM.
(A-Reused with permission from Thieme. From: SanchisAlfonso V. American Journal of Knee Surgery. Volume
7, Issue 2. Usefulness of computed tomography in
evaluating the patellofemoral joint before and after
Insall’s realignment. Thieme: New York. 1994, www.
thieme.com)
planes [9]. Therefore, a radiographical PM may
not be real, and realignment surgery to correct
the nonexistent problem could lead to a worsening of preoperative symptoms.
At the end of 1970s, skeletal malalignment
of the limb was suggested as the genesis of AKP
in some cases [10]. Skeletal malalignment, which
is not the same as PM, is the malalignment of the
limb measured in the transverse, coronal, and
sagittal planes. The presence of excessive
femoral anteversion, excessive external tibial
torsion, or increased varus or valgus abnormalities has a definite effect on the PFJ [11]. James in
1979 presented a comprehensive review of AKP
in which he described the condition of “miserable malalignment”, that is, increased femoral
anteversion and increased external tibial torsion
[10]. In 1995 he reported on seven patients with
miserable malalignment who had been treated
with internal rotational tibial osteotomy during
an 18-year period [12]. Several years earlier,
Cooke and colleagues [13] described internal
rotational proximal tibial osteotomy in seven
patients presenting with AKP and drew attention
to the inwardly pointing knee as an unrecognized
cause of AKP. Unlike the concept of PM, however, the concept of skeletal malalignment was
almost unnoticed and has had very low influence
on orthopedic surgeons. In fact, very few publications refer to skeletal malalignment as a cause
of AKP.
In the 1990s, Scott F. Dye and his research
group at the University of California, San Francisco, proposed the tissue homeostasis theory
[14, 15]. According to this theory, joints are not
simply mechanical structures; they are systems
that are alive and metabolically active [14]. Pain
arises from a physiopathological mosaic of causes, including increased osseous remodeling,
increased intraosseous pressure, or peripatellar
synovitis leading to a reduced “envelope of
function” (or “envelope of load acceptance”)
(Fig. 2) [2, 14, 15]. This envelope of function is
defined by the range of loading and energy
absorption that coexists with normal tissue
healing and maintenance (i.e., tissue homeostasis). According to Dye, in the vast majority of
AKP cases, the loss of homeostasis of both osseous (Fig. 3) and soft tissue in the peripatellar
region is more important than biomechanical/
structural issues in the genesis of AKP. He suggests that AKP patients are often symptomatic
because of supraphysiologic loading of anatomically normal knee components [2, 14, 15]. In
fact, patients with AKP often lack an easily
identifiable structural abnormality to account for
their symptoms. According to Dye’s theory of
envelope of load acceptance, overuse or cyclical
overload of soft tissue or bone areas may explain
AKP in many patients. However, it should be
noted that this biological perspective is compatible with the biomechanical approach. The
Pathophysiology of Anterior Knee Pain
21
Fig. 2 The envelope of function theory. (Reused with permission from SAGE. From Sanchis-Alfonso V, Dye SF.
“How to Deal with Anterior Knee Pain in the Active Young Patient” Sports Health. 2017; 9(4):346–351)
Fig. 3 SPECT-CT in a patient with disabling left AKP
due to excessive external tibial torsion showing the loss of
osseous homeostasis
rotation of the femur [16, 17]. That is to say, the
primary contributor to lateral patellar subluxation
and patellar tilt is the internal rotation of the
femur below the patella. Therefore, control of the
rotation of the femur is fundamental to guaranteeing normal patellofemoral kinematics. Thus, a
new concept was born. It is the “proximal control” that is currently considered fundamental to
understanding the physiotherapeutic treatment of
an important subgroup of AKP patients. Lee and
colleagues [18] have demonstrated that femoral
rotation results in an increase in PFJ contact
pressures on the contralateral facet of the patella
(i.e., lateral PFJ during internal rotation of the
femur and vice versa).
3
diagnostic challenge is to find the cause of the
loading which is “in excess of the envelope of
function or load acceptance”.
Finally, in the 2000s, Chris Powers and his
working group conducted weight-bearing studies
of the PFJ and suggested that the main factor
contributing to patella tilt and lateral displacement during weight-bearing is the internal
A Critical Analysis of Realignment
Surgery for PM
After wide usage of certain surgical techniques,
surgeons may come to question the basic tenets
justifying the procedures and devise clinical
research to test the underlying hypotheses.
Realignment surgery for treating PM is no
exception. In 2005, Sanchis-Alfonso and
22
colleagues [19] retrospectively evaluated 40
Insall’s proximal realignments (IPRs) performed
on 29 patients, with an average postsurgical
follow-up of 8 years (range: 5–13 years). One of
the objectives of this study was to analyze
whether a relationship existed between the presence of PM and that of AKP. In this study, IPR
was found to provide a satisfactory centralization
of the patella into the femoral trochlea in the
short-term follow-up and the surgery was associated with resolution of AKP [19, 20]. This
outcome appears to support the PM theory;
however, the success of realignment surgery may
have been due to factors independent of the relative patellofemoral position, such as denervation of the patella, extensive postoperative rest
(unload), and postoperative physical therapy.
Unfortunately, the satisfactory centralization of
the patella observed at the short-term follow-up
was lost by the long-term follow-up in almost
57% of the cases, based on CT scans [19]. That
is, IPR did not provide a permanent correction of
patellofemoral congruence in all cases.
Nonetheless, this loss of centralization did not
correlate with a worsening of clinical results. In
short, a relation between the result (satisfactory
versus non-satisfactory) and the presence or
absence of postoperative PM was not found in
the long term [19].
Out of 29 patients in the study, 12 presented
with unilateral symptoms. In nine of these
patients, the contralateral asymptomatic knee
presented a PM, and there was a satisfactory
centralization of the patella into the femoral trochlea in only three cases [19]. If the presence of
PM is crucial in the genesis of AKP, how can we
account for unilateral symptoms in patients with
similar morphologic characteristics between both
patellofemoral joints? With regard to unilateral
pain in the presence of bilateral PM, patients are
known to preferentially load one limb more than
the other (usually the dominant limb) in highly
demanding activities, such as sports. This loading difference could be enough to cause
V. Sanchis-Alfonso et al.
unilateral pain, but we did not find a relationship
between the lateral dominance and the affected
side in cases with unilateral pain [21]. Further, in
six patients with bilateral symptoms who
received surgery on the knee with the most
severe symptoms, the contralateral knee was
pain-free at follow-up. Therefore, if the presence
of PM is crucial in the genesis of AKP, why do
symptoms disappear without any change in the
patellofemoral alignment? Loss of both tissue
and bone homeostasis may be more important
than structural characteristics in the genesis of
AKP.
Viewing AKP as being necessarily tied to PM
is an oversimplification that has impeded progress toward better diagnosis and treatment. The
great danger in using PM as a diagnosis is that
the unsophisticated or unwary orthopedic surgeon may think that he or she can correct it with
surgical procedures. Pursuing this misguided
path very often makes the patients’ pain worse.
The worst cases of AKP, at least in my series (V.
S-A), occur in patients that have had multiple
PM-oriented operative procedures for symptoms
that initially were only mild and intermittent. We
have observed that not all patellofemoral malaligned knees show symptoms, which is not surprising, because asymptomatic anatomic
variations are not uncommon. Moreover, we
have demonstrated that PM is not a sufficient
condition for the onset of symptoms, given that
many patients with AKP do not have PM. We
can conclude that the pain does not arise from the
PM. That is, pain does not arise from the malposition of the patella on the trochlea. Thus, no
imaging study should give us an indication for
surgery. PM diagnosed with plain x-ray, CT or
MRI is only an instant in time and does not
describe the dynamics of motion. Moreover, we
do not have adequate proof of the definition of
normal alignment. History, physical exam, and
differential injection must point towards surgery,
with imaging only being used to confirm clinical
impression.
Pathophysiology of Anterior Knee Pain
4
The Key Question: Is There
a Mechanical Overload of the PFJ
Behind AKP and What is the Role
of Patellofemoral Imbalance
in the Genesis of AKP?
Multiple approaches have been taken to determine the genesis of AKP, from the more traditional structural/biomechanical view to the newer
tissue homeostasis perspective. Despite their
differences, all potential explanations include
joint loading as an important factor. This commonality is not surprising because the PFJ is very
sensitive to stress.
Certain activities that highly load the PFJ,
such as going down stairs or inclines or experiencing prolonged flexion while a person is sitting, kneeling, or squatting, are strongly
associated with the genesis and persistence of
AKP. In addition, a direct blow to the patella in a
fall to the ground or with dashboard contact in an
automobile accident can also cause pain that may
persist for an extended time, even without an
overt radiographically identifiable fracture. How
can pain be explained in such cases by the tissue
homeostasis perspective? The PFJ is one of the
most highly loaded joints in the human body [22]
as well as one of the most difficult musculoskeletal systems in terms of restoration of
functionality after an injury and the subsequent
loss of tissue homeostasis [23]. Joint reaction
forces that are created within the PFJ with certain
activities can be many times the body weight
[24]. These high loads have been estimated to be
3.3 times the body weight with activities such as
climbing up or down stairs, 7.6 times the body
weight with squatting, and in excess of 20 times
the body weight with jumping activities [25, 26].
In addition to the load applied to the joint, the
actual stresses generated within the PFJ also
depend on the surface areas of the patella and
femur that may be in contact at any given
moment [19]. Such high forces can easily result
in loads that may exceed the safe load acceptance
capacity of musculoskeletal tissues, leading to
symptomatic damage and inducing a mosaic of
pathophysiologic processes causing AKP [2, 15].
23
Further, patellofemoral overload could be secondary to inappropriate physiotherapy in some
cases of AKP. Attempting to strengthen the
quadriceps through open kinetic chain exercises
will unacceptably overload the PFJ if the exercises are performed between 0 and 45 degrees of
flexion [27]. Likewise, closed kinetic chain
exercises performed between 45 and 90 degrees
of flexion will also overload the PFJ [27].
Although there may be no obvious structural
alteration, the PFJ can be overloaded and AKP
can be triggered.
In some cases, PFJ overloading is secondary
to structural anomalies, such as trochlear dysplasia [28]. Patients with AKP are more likely to
have trochlear dysplasia compared to pain-free
individuals [29]. Moreover, in patients with a
trochlear bump (severe trochlear dysplasia) and
AKP, both hydrostatic pressure and water content increase in the patella [30]. Such increases
potentially provoke episodes of tissular ischemia
and mechanical stimulation of nociceptors,
which are both associated with pain [31]. Along
these lines, Barton and colleagues [32] have
demonstrated that the patella contains an
intraosseous nerve network that is the densest in
the medial and central portions of the patella and
significantly sparser laterally. Moreover, growing
evidence shows that in the subgroup of patients
with patellofemoral chondral lesions, some of
their pain is related to such lesions due to the
overload of the richly innervated subchondral
bone interface [31]. Such subchondral bone
overload is secondary to damaged cartilage and
the loss of its capacity as a shock absorber.
However, of all the structural factors that can
cause an overload of the PFJ, the most powerful
is the skeletal malalignment of the lower limb
(limb alignment in the three planes), specifically
torsional alterations (femoral anteversion and/or
external tibial torsion) [33, 34]. With regard to
malalignment, Albert van Kampen [35] has
demonstrated that patellar tracking is highly
susceptible to tibial rotations. Therefore, patellar
tracking biomechanical studies must take tibial
rotation into account. However, the classic PM
theory does not take tibial and femoral torsion
24
into consideration, which represents another
weak point in the PM theory.
Limb alignment appears to very strongly
influence the quadriceps vector [33, 34]. An
abnormal quadriceps vector is an important
contributor to AKP, and abnormal limb alignment is the underlying cause of the incorrect
quadriceps vector [33, 34]. The direction of the
quadriceps vector is likely more important than
its magnitude [33, 34]. It should be noted that
skeletal malalignment is not an abnormal Qangle or an increased TT-TG distance, nor is it an
increased tilt or increased shift of the patella. It
instead involves the alignment of the limb in all
three spatial planes—coronal, sagittal, and
transverse. During a normal gait, the knee joint
axis moves straight forward with minimal
amounts of internal or external rotation, and the
quadriceps force is directed posteriorly, compressing the patella into the trochlea. With
abnormal limb torsion, the knee joint axis often
moves forward in a manner that is oblique to the
direction of motion. Such movement generates
abnormal shear forces between the patella and
the femur that will eventually cause tissue failure.
If the force is not perfectly aligned, it can lead to
an unbalanced distortion of the soft tissues surrounding the patella. It is very likely that one of
the sources of AKP is in the peripatellar soft
tissues due to the stress that the soft tissues
undergo. However, we do not know the strain
levels that must be reached to trigger the pain.
Some patients with torsional deformities have
unilateral AKP, despite the deformity being
symmetric. Why one side is symptomatic and the
other is not remains an enigma. It is probable that
most people limit their activity to avoid overuse
or injury to the PFJ and thus AKP. Many of these
patients are symptomatic only when they attempt
an activity that causes increased loading; therefore, many select their activities based on what is
comfortable. Once an injury (soft tissue lesion)
or overuse (soft tissue strain) develops, quick
recovery does not occur because of the underlying mechanical inefficiency. This situation may
explain why disabling pain may occur on one
side, while the opposite side remains
V. Sanchis-Alfonso et al.
asymptomatic. Moreover, the lack of symptoms
on one side may be relative. In some cases,
patients have asked for surgery on the asymptomatic side after the symptomatic side has been
corrected because “they never knew what it was
like to feel normal”.
In short, according to Robert A. Teitge, it is
the excess of force in the PFJ that exceeds tissue
homeostasis
which
is
responsible
for
AKP. However, the problem is not a question of
leaving the load acceptance envelope, but rather
knowing what the envelope size limits are and
why the excess force is excessive. If this is true,
then the problem in diagnosing AKP is determining the source of the excess force. Robert A.
Teitge puts forward a simile to understand the
etiopathogenesis of AKP. To build a bridge, one
must be knowledgeable of several factors. They
include: (a) the required load limit, meaning the
envelope; (b) the design of the bridge parts,
which is the skeletal alignment; and (c) what
materials the bridge is made of, connoting the
response of those materials to the load. In the
following sections, we will look at the biological
response to a mechanical stimulus. The question
we must ask ourselves is whether it is possible
that all the neuroanatomical factors that we are
going to discuss below are secondary to an
excess of force. In other words, is the excess
force the precipitating event? We do not have an
answer to these questions.
5
Neuroanatomical Bases for AKP
in the Young Patient: Neural
Model
Sanchis-Alfonso and colleagues have developed
the neural model as an explanation for the genesis of AKP in young patients [36]. The origin of
AKP can be in the lateral retinaculum (LR),
medial retinaculum, infrapatellar fat pad, synovium, or subchondral bone [37–39]. Studies by
Sanchis-Alfonso and colleagues on AKP pathophysiology have mainly focused on the LR
retrieved during patellofemoral realignment surgery in patients with a diagnosis of PM [40–43].
Pathophysiology of Anterior Knee Pain
5.1 Morphologic Neural Changes
in the Lateral Retinaculum
Some studies have implicated neural damage in
the LR as a possible source of AKP in the young
patient. In 1985, Fulkerson and colleagues
described for the first time, nerve damage (demyelination and fibrosis) in the LR of patients
with intractable patellofemoral pain requiring
lateral retinacular release or realignment of the
PFJ [44]. The changes in the retinacular nerves
observed by these authors resembled the
histopathologic picture of Morton's interdigital
neuroma. Later, in 1991, Mori and colleagues
found degenerative neuropathy in the LR in AKP
patients [45].
Sanchis-Alfonso and colleagues have also
observed nonspecific, chronic degenerative
changes in nerve fibers, including myxoid
degeneration of the endoneurium, retraction of
the axonal component, and perineural fibrosis, in
the LR in many cases (Fig. 4A) [42, 43]. Moreover, Sanchis-Alfonso and colleagues have found
that a smaller group of specimens presented
nerve fibers mimicking amputation neuromas
seen elsewhere in the body (Fig. 4B) [42, 43].
A clear relationship has been demonstrated
between the presence of neuromas and AKP;
however, a similar relationship between neural
Fig. 4 A Myxoid degeneration in the nerve fibers. No
inflammatory cells are seen, B Microneuroma next to a
rich vascular area (HE). (B-Reused with permission from
SAGE. From: “Quantitative analysis of nerve changes in
25
myxoid degeneration and pain has not been
found [43].
Nerve damage occurs diffusely in the affected
LR, and one must therefore consider the possibility of multiple neurologic sequelae in the
peripatellar region. A possible consequence of
such damage could be an altered proprioceptive
innervation [43]. For example, Baker and colleagues observed an abnormal sense of the knee
joint position (proprioception) in subjects with
AKP [46]. Current research shows the importance of proprioceptive information from joint
mechanoreceptors for proper knee function.
Connective tissues, in addition to their mechanical function, play an important role in transmitting specific somatosensory afferent signals to
the spinal and cerebral regulatory systems. Thus,
the giving-way in AKP patients can be
explained, at least in part, by the alteration or loss
of joint afferent information with regard to proprioception due to nerve damage in the ascendant
proprioception pathway or a decrease of healthy
nerve fibers capable of transmitting proprioceptory stimuli. It seems likely that, to a certain
degree, the instability of the PFJ in patients with
AKP arises not only from mechanical factors but
also neural factors [47, 48]. Such factors center
on a proprioceptive deficit both in the sense of
position and in the slowing or diminution of
the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment” Am J Sports Med.
1998; 26:703–709)
26
stabilizing and protective reflexes. In addition,
Jensen and colleagues reported abnormal sensory
function in the painful and nonpainful knee in
some subjects with long-term unilateral AKP
[49].
5.2 Hyperinnervation into the Lateral
Retinaculum and AKP
Several studies have implicated hyperinnervation
of the LR as a possible source of AKP in the
young patient, with higher innervation in those
with severe pain compared with those with
moderate or mild pain [43]. Moreover, the LR of
patients with pain as the predominant symptom
has been shown to have a higher innervation
pattern than the medial retinaculum or the LR of
patients with patellar instability [43]. This nerve
ingrowth consisted of myelinated and
Fig. 5 A Free nerve endings
immersed in the connective
tissue, B Hot spot of free
nerve endings forming a
microneuroma, C Nerve
endings entering the arterial
wall. (Neurofilament NF).
(Reused with permission from
SAGE. From:
“Immunohistochemical
analysis for neural markers of
the lateral retinaculum in
patients with isolated
symptomatic patellofemoral
malalignment” Am J Sports
Med. 2000; 28: 725–731)
V. Sanchis-Alfonso et al.
unmyelinated nerve fibers with a predominant
nociceptive component (Fig. 5) [40].
The nociceptive properties of at least some of
these nerves were shown by their substance P
(SP) immunoreactivity (Fig. 6) [40]. SP, which is
found in primary sensory neurons and C fibers
(slow-chronic pain pathway), is involved in the
neurotransmission pathways of nociceptive signals [50–62]. SP was detected in the axons of big
nerve fibers, in free nerve endings, and in the
vessel walls in some patients with pain as the
predominant symptom [40]. Nociceptive fibers
(i.e., neural fibers with intraaxonal SP) were
fewer in number than NF fibers, indicating that
not all the tiny perivascular or interstitial nerves
were nociceptive [40]. Interestingly, the finding
that SP fibers are more abundant in the LR than
in its medial counterpart reinforces the role of the
LR as the main source of pain in some AKP
patients. Moreover, the number of these
Pathophysiology of Anterior Knee Pain
Fig. 6 A Substance P, a marker of sensory fibers, is
expressed in the nerve fibers in a granular pattern,
B Neuromas are rich in nociceptive axons, as can be
demonstrated studying substance P. (Reused with permission from SAGE. From: “Immunohistochemical analysis for neural markers of the lateral retinaculum in
patients with isolated symptomatic patellofemoral
malalignment” Am J Sports Med. 2000; 28: 725–731)
nociceptive fibers has been observed to be higher
in patients experiencing pain as the main symptom relative to those with instability as the predominant symptom (with little or no pain
between instability episodes) [40].
Nerve ingrowth, is mostly located within and
around blood vessels (Fig. 7) [40, 43]. Thus,
within the LR of AKP patients, S-100 positive
fibers in the adventitia and within the muscular
layer of medium and small arteries resemble a
necklace. S-100 protein is a good marker of nerves
because it permits identification of the Schwann
cells in the myelinated parts of axons. Myelinated
fibers typically lose their myelin sheath before
they enter the muscular arterial wall, but this was
found to not be the case in AKP patients. In a study
of myelinated fibers by S-100 immunostaining,
we were surprised by the identification of S-100positive fibers within the muscular layer of medium and small arteries given that the myelin sheath
27
was expected to be lost before the nerve entered
the muscular arterial wall [43]. Vascular innervation has been demonstrated to be more prominent
(94%) in patients with severe pain, whereas this
type of hyperinnervation has been found in only
30% of the patients with light or moderate pain
[42]. These findings are in agreement with the
statement of Byers, who postulated in 1968 that
pain in an osteoid osteoma could be generated and
transmitted by vascular pressure-sensitive autonomic nerves [63]. In reviewing the literature, we
have seen that hyperinnervation is also a factor
implicated in the pathophysiology of pain in other
orthopedic abnormalities, such as chronic back
pain and jumper’s knee [54, 55, 64, 65]. On the
other hand, pain has also been related with vascular innervation in some pathologies, as is the
case in osteoid osteoma, in which an increase in
perivascular innervations has been found in all the
cases, leading the authors to postulate that pain
was more closely related to this innervation than to
the release of prostaglandin E2 [66]. Grönblad and
colleagues have reported similar findings in the
lumbar pain of facet syndrome [67]. Finally,
Alfredson and colleagues related pain in Achilles
tendinosis with vasculo-neural ingrowth [64].
Hyperinnervation has been demonstrated to be
associated with the release of neural growth
factor (NGF), a polypeptide that stimulates
axonogenesis [41]. NGF has two biologically
active precursors: a long form with a molecular
weight of approximately 34 kD and a short form
of 27 kD [68]. The 34 kD precursor has been
found in the LR of AKP patients [41]. Since
some of the nerve fibers of the LR express NGF,
these nerve fibers must still be in a proliferative
phase. As expected, NGF expression is higher in
PM patients with pain that in those with instability as the main symptom (Fig. 8) [41]. Gigante
and colleagues [69] have also found NGF and
TrkA (the NGF receptor) expression in the LR of
patients with PM, but not in patients with jumper’s knee or meniscal tears. Interestingly, NGF
is related not only to neural proliferation in
vessels and perivascular tissue but also to the
release of neuroceptive transmitters, such as
SP [70].
28
Fig. 7 Lateral retinaculum vessels are richly innervated
in some of our patients. The myelinated innervation enters
the muscular wall from the adventitial tissue, forming a
necklace. (S-100). (Reused with permission from SAGE.
V. Sanchis-Alfonso et al.
From: “Quantitative analysis of nerve changes in the
lateral retinaculum in patients with isolated symptomatic
patellofemoral malalignment” Am J Sports Med. 1998;
26:703–709)
Fig. 8 Immunoblotting
detection of NGF showing a
thicker band in cases with
AKP (4,5,6,7) compared with
cases of instability without
pain (1,2,3)
In short, in symptomatic PM patients with
pain as the main symptom, there are detectable
levels of NGF that cause hyperinnervation and
stimulate SP release, whereas in patients with
instability as the predominant symptom, there are
lower levels of local NGF release, less neural
proliferation, and less nociceptive stimulus [41].
Consequently, there must be some factors acting
on a PM that make the patient has pain or
instability as the main symptom. PM may in fact
not have anything to do with the presence of
pain. In other words, symptoms appear to be
related to multiple factors with variable clinical
expression, and our imperfect understanding of
Pathophysiology of Anterior Knee Pain
these factors may explain the all-too-frequent
failure to achieve adequate symptom relief with
the use of realignment procedures. The question
is, what are the mechanisms that stimulate NGF
release in these patients? We hypothesize that
periodic short episodes of ischemia could be the
primary mechanism of NGF release and hyperinnervation, and therefore could be implicated in
pain, at least in a subgroup of AKP patients.
5.3 Role of Ischemia in the Genesis
of AKP: Loss of Vascular
Homeostasis
Despite numerous publications on AKP, the
mechanism underlying the pain is controversial.
The loss of vascular homeostasis has been proposed as an intrinsic pain mechanism in a subgroup of AKP patients.
5.3.1 Basic Science
According to some authors, ischemia can induce
NGF synthesis [70–72]. Moreover, NGF has
been shown to stimulate neural sprouting and
hasten neural proliferation in blood vessel walls
[73, 74], which is the same pattern of hyperinnervation that is seen in the LR of some AKP
patients [40, 42, 43]. Similar changes have been
studied in animal models and are present in the
coronary innervation of patients with myocardial
infarcts and brain ischemia [71, 72, 74]. Thus,
short episodes of tissular ischemia due to vascular torsion or vascular bending have been
hypothesized as the main problem in painful
patellofemoral imbalance [40, 42]. Vascular
bending could be induced mechanically by
medial traction over the retracted LR with knee
flexion [38].
Sanchis-Alfonso and colleagues have
demonstrated histologic retinacular changes
associated with hypoxia in painful PM [42].
They have found lesions that can lead to tissular
anoxia, such as arterial vessels with obliterated
lumina and thick muscular walls, and other
lesions that can arise from ischemia, such as
infarcted foci of the connective tissue, myxoid
stromal degeneration, and ultrastructural findings
29
related with anoxia (degenerated fibroblasts with
autophagic intracytoplasmic vacuoles, endothelial cells with reduplication of the basal lamina,
young vessels with endothelial cells containing
active nuclei and conspicuous nucleoli, and
neural sprouting) (Fig. 9) [75].
Another phenomenon related to ischemia is
angiogenesis. Chronic ischemia leads to release
of vascular endothelial growth factor (VEGF), a
potent hypoxia-inducible angiogenic factor that
causes hypervascularization [76]. This hypervascularization creates blood vessels to supply
the nutrient needs of the tissue. Sanchis-Alfonso
and colleagues have performed a quantitative
analysis of vascularization in the LR excised
during surgical patellofemoral realignments,
using a pan-vascular marker, anti-Factor VIIIrelated antigen [42]. They have found an increase
in the number of blood vessels in the LR of
patients with painful PM, with the severe pain
group having greater numbers compared with
those of moderate or mild pain group [42].
Moreover, as expected, they found a positive
linear correlation between the number of blood
vessels and number of nerves [42]. Tissular
ischemia induces VEGF release by fibroblasts,
synovial cells, mast cells, or even endothelial
cells [77–80]. Based on these principles,
Sanchis-Alfonso and colleagues performed a
study of VEGF expression in the LR of patients
with PM, using immunohistochemistry and
immunoblot analysis [42]. VEGF release begins
8 h after hypoxia, and the peptide disappears in
24 h if the ischemic crisis has ended [42].
Therefore, VEGF positivity reflects the presence
of an ischemic process, or better said, 8–24 h has
elapsed since the onset of the transitory ischemic
episode. However, given that the average duration of VEGF is very short, its absence has no
significance regarding whether a transitory
ischemic process is occurring. Although this
process has been well documented in joints
affected by rheumatoid arthritis and osteoarthritis
[79–81], it has never been documented in AKP
until the study by Sanchis-Alfonso and colleagues [42]. They have shown VEGF production in stromal fibroblasts, vessel walls, certain
endothelial cells, and even nerve fibers, including
30
V. Sanchis-Alfonso et al.
A
B
C
E
D
F
G
Fig. 9 A Arterial vessel in the retinacular tissue can show
a prominent and irregular endothelium and thick muscular
walls or even an irregular reduction of the vascular lumen.
(Hematoxylin–Eosin stain). B Infarcted foci in the
connective tissue showing a degenerative pattern of the
collagen fibers, with loss of the fibrillar component and
accumulation of myxoid material in the interstitium,
(Masson’s Trichrome stain). C Myxoid stromal
degeneration in the middle of the fibrous retinacular
tissue (Hematoxylin–Eosin stain). D Degenerative
changes in fibroblasts (increased autophagic vacuoles—
asterisk–) secondary to hypoxia (TEM). E Young vessels
with endothelial cells containing active nuclei and conspicuous nucleoli. F Neural sprouting is detected ultrastructurally as a bunch of tiny axons immersed in the
Schwann cell cytoplasm. G Neural sprouting detail
similar levels in axons as in perineurium
(Fig. 10) [42]. Their immunohistochemical findings were confirmed by immunoblot analysis.
VEGF levels were higher in patients with severe
pain than in those with mild to moderate pain; the
protein was barely detectable in two cases with
mild pain (Fig. 11) [42]. VEGF expression is
absent in normal joints, although inflammatory
Pathophysiology of Anterior Knee Pain
31
Fig. 10 A VEGF, the factor promoting vascular proliferation, is present in smalls vessels (wall and endothelium) and
in perivascular fibroblasts. B Some cases have VEGF expression in the perineural shift and inside the axons (VEGF)
Fig. 11 Immunoblotting detection of VEGF showing a
thicker band in cases with severe AKP (2,3,10) compared
with cases with moderate pain (1,5,8) or light pain
(4,6,7,9)
processes can stimulate its release [81, 82]. In
such cases, synovial hypoxia secondary to articular inflammation is assumed to trigger VEGF
production [82]. However, inflammatory changes
have not been observed in the LR of AKP
patients [42, 43]. Furthermore, peripheral nervous system hypoxia has been reported to be able
to simultaneously trigger VEGF and NGF synthesis via neurons [83], or inflammatory or
stromal cells [71, 72]. VEGF induces hypervascularization, and NGF induces hyperinnervation.
Both occurrences have been observed in AKP
patients [42, 43]. In conclusion, ischemia could
be the main trigger for pain in at least a subgroup
of AKP patients.
5.3.2 Clinical Studies
The role of vascular insufficiency in AKP has not
been studied extensively from a clinical point of
view. In fact, only a few clinical papers have
alluded to the possibility of hypoxia as a factor in
the pathogenesis of AKP.
Sandow and Goodfellow [84] investigated the
natural history of AKP in adolescents. In a study
sample of 54 adolescent girls, the researchers
observed that 9 out of 54 (16.7%) had pain that
was aggravated by cold weather. According to
Selfe and colleagues [85] the proximal part of the
rete patellae is very superficial and is therefore
vulnerable to thermal environmental stress,
resulting in greater hypoxia during cold weather.
More recently, Selfe and colleagues [86] studied
clinical outcomes in a sample of AKP patients
categorized as hypoxic, that is to say, with “cold
knees” (his or her legs felt cold even in warm
surroundings). Fourteen out of 77 (18.2%) of the
patients were categorized as “cold sufferers,” a
percentage very similar to that reported by Sandow and Goodfellow [84]. Selfe and colleagues
[86] studied local hypothermia by means of
infrared thermography and concluded that patients
categorized as hypoxic reported greater pain levels
and had poorer response to an exercise-based
treatment than non-hypoxic patients. Gelfer and
colleagues [87], using single photon emission
computed tomography (SPECT), also found a
relationship between transient patellar ischemia
after total knee replacement and the clinical
symptoms of AKP. Similarly, using photoplethysmography, which is a reliable technique for
estimating blood flow in bone tissue, Naslund also
observed that an ischemic mechanism (decreased
32
V. Sanchis-Alfonso et al.
blood flow in the patellar bone) is involved in the
pathogenesis of AKP [88]. Moreover, in half of
the AKP studied patients, Naslund observed
accelerated bone remodeling in bony compartments of the knee joint, which may have been due
to a dysfunctioning sympathetic nervous system
and caused intermittent ischemia and pain. Selfe
and colleagues [85] classified AKP patients into
three groups: hypoxic, inflammatory, and
mechanical. However, ischemia may be the painprovoking factor in all three groups, given that
inflammatory changes can develop not only after
ischemia but also after mechanical damage to the
vascular system. Ischemia could be caused by
higher intraosseous pressure, redundant axial
loading, or decreased arterial blood flow.
6
The Role of the Peripheral
and/or Central Nervous System
in the Pathophysiology of
AKP—“Central
Sensitization”—“The
Neuromatrix Model”
AKP is a paradigm of chronic pain. Chronic pain is
a multidimensional phenomenon composed of
sensitive, cognitive-evaluative and affectivemotivational domains. The central nervous system, both the brain and spinal cord, is where pain is
produced and modulated. Several brain and spinal
cord areas work together (the pain neuromatrix) in
response to corporal stimuli to create the multidimensional experience of pain. Interestingly,
Damasio and colleagues [89] observed an overlap
between the cerebral activity areas related to
chronic pain and those related to cognition and
emotions. This finding suggests that chronic pain,
cognition, and emotions are interrelated. Moreover, it has been shown that AKP is not only related
to structural anomalies but also to altered central
neural processes along with alterations in central
nociceptive processing [90, 91]. Slutsky-Ganesh
and colleagues [92] indicate that the posterior
cerebellum could be a key modulator in cognitive
assessment of pain in patellofemoral pain across
the cortico-cerebellar loops, possibly leading to
consequences on motor function downstream.
As we will see in chapter “Evaluation of
Psychological Factors Affecting Anterior Knee
Pain Patients: The Implications for Clinicians
Who Treat these Patients”, AKP patients have a
high incidence of anxiety, depression, kinesiophobia (the belief that movement will create
additional injury or re-injury and pain) and
catastrophizing (the belief that pain will worsen,
and one is helpless to deal with it) [93–95].
Psychological factors play an important role as
pain modulators. Even in cases with clear structural findings that justify pain, psychological
factors influence and modify pain sensation as
well as subsequent impairment. Therefore, they
can be barriers to recovery after the appropriate
surgical treatment. Catastrophizing is not only
responsible for the chronification of pain due to a
psychological mechanism but may also influence
the neurophysiology of pain modulation. In a
functional MRI study of patients with chronic
pain, Gracely and colleagues [96] showed that
catastrophizing ideas were associated with a
higher degree of brain activity not only in the
pain regions but also in the cortical regions
associated with attention, anticipation of pain and
emotional aspects of pain. Catastrophizing may
play a role as a facilitator of the pain perception
process. It also has been suggested that pain
catastrophizing interfere with descending paininhibitory systems and may facilitate neuroplastic changes in the spinal cord during repeated
painful stimulation, thereby promoting sensitization in the central nervous system.
Impaired “conditioned pain modulation,”
defined as the endogenous pain inhibition ability
of a subject, has been demonstrated in young
women with long-standing AKP [97]. Central
sensitization (CS) has been defined by the
International Association for the Study of Pain
(IASP) as “increased responsiveness of nociceptive neurons in the central nervous system to
their normal or subthreshold input” [98]. In other
words, there is ineffective pain modulationinhibition in the central nervous system. That is
to say, there is a process of amplification of the
afferent signal that arrives from the periphery.
For all that, the malfunctioning of the descending
pain-inhibiting mechanisms is another of the
Pathophysiology of Anterior Knee Pain
mechanisms involved in CS. From a clinical
standpoint, we can suspect that there is CS when
the patient presents with allodynia or hyperalgesia. A significant number AKP patients present
more signs of CS when compared to healthy
pain-free individuals. Interestingly, it has been
demonstrated that pain sensitization may be
amenable to treatment through exercises, pharmacological therapy, and surgery [99]. In AKP
patients, there is “central sensitization,” meaning
an increased responsiveness of the central nervous system to a variety of stimuli [100–102].
Rathleff and colleagues [101] suggested that
adolescent females with AKP have both localized and distal hyperalgesia (a reduced pressure
pain threshold), which can be determined
through pressure algometry. This hyperalgesia
may signal altered central processing of nociceptive information.
Jensen and colleagues [49] have shown that
some patients with unilateral AKP have neuropathic pain, which suggests damage in the
peripheral and/or central nervous system that
causes pain signals without a specific cause. In
this way, many AKP patients have alterations in
the central nervous system that might play an
important role both in the magnitude and persistence of pain after suitable conservative or
surgical treatment. Lefaucheur and colleagues
[103] found a link between chronic neuropathic
pain and motor cortex disinhibition. The current
data suggest that repetitive transcranial magnetic
stimulation of the motor cortex corresponding to
the patient’s site of pain may be a complementary treatment modality for patients with chronic
neuropathic AKP [104]. Motor cortex stimulation may produce analgesic effects by restoring
missing or impaired intracortical inhibitory processes [103].
As we can see in chapter “Brain Network
Functional Connectivity Clinical Relevance and
Predictive Diagnostic Models in Anterior Knee
Pain Patients”, AKP patients have brain functional connectivity changes compared to healthy
controls. That is especially the case between the
brain areas involved in cognitive stimulus processing and the regions involved in pain
33
modulation. This widespread impact on overall
brain function could play an important role in
explaining the magnitude, experience and persistence of pain after suitable conservative or
surgical treatment.
7
Authors’ Proposed AKP
Pathophysiology
A subgroup of patients with AKP have a skeletal
malalignment of the limb, especially in the
transverse plane (femoral and/or tibial rotational
malalignment) [33, 34]. This malalignment of the
lower limb could provoke pain due to the
abnormal stress on tissue which is not of sufficient magnitude or direction to result in instability. It is likely that nerve changes or ischemia
may be due to chronic repetitive stretch of soft
tissue
(retinaculum).
Moreover,
skeletal
malalignment could provoke patellofemoral
instability due to a failure of the ligaments that
stabilize the PFJ, and it will also lead to the
development of patellofemoral cartilage lesions
due to the increased patellofemoral compression
forces (Fig. 12). However, in most cases, the
abnormal femoral rotation is functional due to a
deficit of the proximal control [105]. This situation will lead to a patellofemoral imbalance as it
occurs in the structural skeletal malalignment of
the lower limb.
We hypothesize that short and repetitive episodes of tissular ischemia, potentially due vascular torsion or vascular bending induced by a
patellofemoral imbalance, could trigger release
of NGF and VEGF in the peripatellar soft tissues.
Once NGF is present in the tissues, it induces
hyperinnervation, attracts mastocytes, and triggers substance P release by free nerve endings
(Fig. 13) [70]. In addition, VEGF induces
hypervascularization and plays a role in
increasing neural proliferation.
Free nerve endings, slowly adapting receptors
that mediate nociception, are activated in
response to deformation of tissues. In the knee,
such deformation results from abnormal tensile
and compressive forces generated during flexo-
34
V. Sanchis-Alfonso et al.
Fig. 12 Pathways to pain in patients with torsional abnormalities. Force out of balance is the culprit, and force out of
the balance is due to the limb out of alignment
Fig. 13 Pathophysiology of
AKP
extension of the joint or in response to chemical
agents such as histamine, bradykinin, prostaglandins, and leukotrienes [57, 106, 107].
Therefore, SP is released from peripheral endings
of nociceptive afferents as a result of noxious
chemical or mechanical stimulation. The nociceptive information relayed by these free nerve
endings is responsible, at least in part, for the
pain.
Once SP is liberated in the connective tissue,
it induces the release of prostaglandin E2, one of
the biochemical agents known to stimulate
nociceptors (Fig. 13) [50]. The activation of
nociceptive pathways by prostaglandins could be
one of the many mechanisms involved in the
transmission of pain in AKP patients. Moreover,
SP stimulates mast cells, facilitating a
degranulation process that can liberate histamine,
another non-neurogenic pain mediator (Fig. 14)
[56]. Numerous mast cells have been identified in
the LR of AKP patients [19]. Mast cells are also
associated with the release of NGF [40, 108],
contributing to the hyperinnervation and indirectly provoking more pain. Furthermore, SP has
been shown to induce the release of collagenase,
interleukin-1, and tumor necrosis factor-alpha
(TNF-a) from synoviocytes, fibroblasts, and
macrophages [50, 52]. These factors could contribute to the genesis of patellar instability
through degradation of soft tissues. SP, NGF and
mast cells have also recently been implicated in
bone resorption in both in vitro and in vivo
experiments, which could explain, at least in part,
the osteoporosis found in many cases of AKP
Pathophysiology of Anterior Knee Pain
35
A
B
Fig. 14 Mast cells are abundant in the stroma (arrow),
mainly in a perivascular disposition. Some of them show a
degranulation process (activated mast cells) (A), (Giemsa
stain). Ultrastructural image of a mast cell of the lateral
retinaculum with its cytoplasm full of chemotactic
granules, (TEM) (B). (A)-(Reused with permission from
SAGE. From: “Immunohistochemical analysis for neural
markers of the lateral retinaculum in patients with isolated
symptomatic patellofemoral malalignment” Am J Sports
Med. 2000; 28: 725–731)
[109]. Finally, SP and VEGF stimulate
endothelial cell proliferation and migration [53],
which are essential to the development of a new
vascular network that may promote tissue repair,
but indirectly maintain a vicious cycle.
Woolf [110] described four types of pain from
a clinical point of view: (1) nociceptive pain,
which is transient pain in response to noxious
stimulus; (2) homeostatic pain, which is pain that
promotes the healing of injured tissue (i.e., the
cascade of events toward re-establishing homeostasis); (3) neuropathic pain, which is spontaneous pain and hypersensitivity to stimulus in
association with damage to the nervous system;
and (4) functional pain, which is pain resulting
from abnormal central processing of normal
input. All these mechanisms appear to be
involved in the pathophysiology of pain in AKP
patients.
orthopedic pathologies from a clinical point of
view.
AKP obliges us to “think out of the box”, to
look deeper into the anatomy, biomechanics,
biology, anatomic pathology, physiopathology, and psychology. AKP is a great stimulus
for orthopedic intellectual development.
Chondromalacia patellae is not synonymous
with AKP. It is not the underlying problem.
Very often, patellofemoral malalignment
(patellar tilt/lateral patellar subluxation) is not
the problem.
In a subgroup of AKP patients, skeletal
malalignment of the limb is responsible for
disabling AKP due to both patellofemoral
overload and patellofemoral imbalance.
Understanding the biomechanics is crucial—
orthopedic surgery is very much a mechanical
engineering discipline. At this time, from the
biomechanical viewpoint, the most powerful
treatment effect in treating AKP comes from
limb re-alignment.
In the vast majority of AKP cases, the loss of
both soft tissue (peripatellar synovitis and
others soft tissue impingements such as synovial hypertrophy around the inferior pole of
8
–
–
–
–
Take Home Messagess
– Currently, much remains to be learned about
the cause of AKP. Our understanding is limited. AKP is one of the most intriguing
–
36
–
–
–
–
9
V. Sanchis-Alfonso et al.
the patella) and osseous (intraosseous edema,
osseous hypertension) homeostasis is more
important in the genesis of AKP than local
structural anomalies (patellar till, lateral
patellar displacement, and patellofemoral
chondropathy). However, we do not know
how often is AKP present in a structurally
perfect limb, except for overtraining. It is
likely that the loss of homeostasis can be
mechanical with an as yet unrecognized
structural anomaly.
There is a neuroanatomical basis for AKP in
the young patient. A dysfunction of the
peripheral and/or the central nervous system
may cause neuropathic pain in some individuals with AKP.
Periodic short episodes of ischemia, secondary to a mechanical stimulus, could be
implicated in the pathogenesis of AKP by
triggering neural proliferation of nociceptive
axons (SP-positive nerves), mainly in a
perivascular location. These findings are in
line with the homeostasis perspective. Loss of
vascular homeostasis in the knee region (e.g.,
hypervascularity, ischemia, osseous hypertension) may be associated with AKP.
It is possible that all of the neuroanatomical
factors involved in the genesis of AKP and
the loss of vascular homeostasis are due to an
excess of force that would be the precipitating
event.
Chronic pain is a multidimensional phenomenon composed by sensitive, cognitiveevaluative and affective-motivational domains.
The neuromatrix model can explain the multidimensional pain experience in AKP patients.
Key Message
– We hypothesize that it is the force (magnitude
or direction) which determines whether one is
in or out of Dye’s envelope. In short, the
diagnostic challenge is determining the source
of excess force which overcomes tissue
homeostasis. We are a long way from determining why excess force is excess.
References
1. Büdinger K. Üeber ablösung von gelenkteilen und
verwandte prozesse. Dtsch Z Chir. 1906;84:311–65.
2. Dye SF. The pathophysiology of patellofemoral
pain: a tissue homeostasis perspective. Clin Orthop
Relat Res. 2005;436:100–10.
3. Royle SG, Noble J, Davies DR, et al. The
significance of chondromalacic changes on the
patella. Arthroscopy. 1991;7:158–60.
4. Ficat P, Ficat C, Bailleux A. Syndrome d’hyperpression externe de la rotule (S.H.P.E). Rev Chir
Orthop. 1975;61:39–59.
5. Ficat P, Hungerford DS. Disorders of the PatelloFemoral Joint. Baltimore: Williams & Wilkins;
1977.
6. Hughston JC. Subluxation of the patella. J Bone
Joint Surg. 1968;50–A:1003–1026.
7. Insall J. “Chondromalacia Patellae”: Patellar
malalignment syndrome. Orthop Clin North Am.
1979;10:117–27.
8. Merchant AC, Mercer RL. Lateral release of the
patella: a preliminary report. Clin Orthop Relat Res.
1974;103:40.
9. Staeubli HU, Bosshard C, Porcellini P, et al.
Magnetic resonance imaging for articular cartilage:
cartilage-bone mismatch. Clin Sports Med.
2002;21:417–33.
10. James SL. Chondromalacia of the Patella in the
adolescent. In: Kennedy JC. editor. The injured
adolescent knee. Baltimore: The Williams &
Wilkins Company, 1979.
11. Orthopaedic Knowledge Update 3 Home Study
Syllabus Published by American Academy of
Orthopaedic Surgeons, Park Ridge, Illinois, January
1990, pp 563–567.
12. Meister K, James SL. Proximal tibial derotation
osteotomy for anterior knee pain in the miserably
malaligned extremity. Am J Orthop (Belle Mead
NJ). 1995;24:149–55.
13. Cooke TD, Price N, Fisher B, et al. The inwardly
pointing knee. An unrecognized problem of external
rotational malalignment. Clin Orthop Relat Res.
1990;56–60.
14. Dye SF. The knee as a biologic transmission with
an envelope of function: a theory. Clin Orthop Relat
Res. 1996;325:10–8.
15. Dye SF, Staubli HU, Biedert RM, et al. The mosaic
of pathophysiology causing patellofemoral pain:
therapeutic implications. Oper Techni Sports Med.
1999;7:46–54.
16. Powers CM, Ward SR, Fredericson M, et al.
Patellofemoral kinematics during weightbearing
and non-weightbearing knee extension in persons
with patellar subluxation: a preliminary study.
J Orthop Sports Phys Ther. 2003;33:677–85.
17. Souza RB, Draper CE, Fredericson M, et al. Femur
rotation and patellofemoral joint kinematics: a
Pathophysiology of Anterior Knee Pain
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
weight-bearing MRI analysis. J Orthop Sports Phys
Ther. 2010;40:277–85.
Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. J Orthop Sports Phys Ther.
2003;33:686–93.
Sanchis-Alfonso V. Anterior Knee Pain and Patellar
Instability. London: Springer; 2011.
Sanchis-Alfonso V, Gastaldi-Orquín E, MartinezSanJuan V. Usefulness of computed tomography in
evaluating the patellofemoral joint before and after
Insall’s realignment. Correlation with short-term
clinical results. Am J Knee Surg. 1994;7:65–72.
Sanchis-Alfonso V, Roselló-Sastre E, MartinezSanJuan V. Pathogenesis of anterior knee pain
syndrome and functional patellofemoral instability
in the active young. A review Am J Knee Surg.
1999;12:29–40.
Dye SF. Functional anatomy and biomechanics of
the patellofemoral joint. In: Scott WN, editor. The
Knee. St. Louis: Mosby; 1994. p. 381–9.
Dye SF. Forward. In Fulkerson JP. Disorders of the
Patellofemoral Joint. Ed 4. Philadelphia, Lippincott
Williams and Wilkins xi–xii, 2004.
Hungerford DS, Barry M. Biomechanics of the
patellofemoral joint. Clin Orthop. 1979;144:9–15.
Reilly DT, Martens M. Experimental analysis of the
quadriceps muscle force and patellofemoral joint
reaction force for various activities. Acta Orthop
Scand. 1972;73:146–137.
Smith AJ. Estimates of muscle and joint force at the
knee and ankle during jumping activities. J Hum
Movement Stud. 1975;1:78–86.
Steinkamp LA, Dillinghan MF, Markel MD, et al.
Biomechanical considerations in patellofemoral
joint rehabilitation. Am J Sports Med.
1993;21:438–44.
Van Haver A, De Roo K, De Beule M, et al. The
effect of trochlear dysplasia on patellofemoral
biomechanics: a cadaveric study with simulated
trochlear deformities. Am J Sports Med. 2015;43
(6):1354–61.
Powers CM. Patellar kinematics, part II: the
influence of the depth of the trochlear groove in
subjects with and without patellofemoral pain. Phys
Ther. 2000;80(10):965–78.
Ho KY, Hu HH, Colletti PM, et al. Recreational
runners with patellofemoral pain exhibit elevated
patella water content. Magn Reson Imaging.
2014;32(7):965–8.
Sanchis-Alfonso V. Holistic approach to understanding anterior knee pain. Clinical implications.
Knee Surg Sports Traumatol Arthrosc. 2014;22
(10):2275–2285.
Barton RS, Ostrowski ML, Anderson TD, et al.
Intraosseous innervation of the human patella: a
histologic
study.
Am
J
Sports
Med.
2007;35:307–11.
37
33. Teitge RA. Patellofemoral syndrome a paradigm for
current surgical strategies. Orthop Clin N Am.
2008;287–311.
34. Teitge RA. Does lower limb torsion matter? Tech
Knee Surg. 2012;11:137–46.
35. van Kampen A, Huiskes R. The three-dimensional
tracking pattern of the human patella. J Orthop Res.
1990;8(3):372–82.
36. Sanchis-Alfonso V, Roselló-Sastre E. Anterior knee
pain in the young patient—what causes the pain?
“Neural model.” Acta Orthop Scand. 2003;74:697–
703.
37. Biedert RM, Sanchis-Alfonso V. Sources of anterior
knee pain. Clin Sports Med. 2002;21:335–47.
38. Fulkerson JP. The etiology of patellofemoral pain in
young active patients: a prospective study. Clin
Orthop Relat Res. 1983;179:129–33.
39. Kasim N, Fulkerson JP. Resection of clinically
localized segments of painful retinaculum in the
treatment of selected patients with anterior knee
pain. Am J Sports Med. 2000;28:811–4.
40. Sanchis-Alfonso V, Roselló-Sastre E. Immunohistochemical analysis for neural markers of the lateral
retinaculum in patients with isolated symptomatic
patellofemoral malalignment. A neuroanatomic
basis for anterior knee pain in the active young
patient. Am J Sports Med. 2000;28:725–731.
41. Sanchis-Alfonso V, Roselló-Sastre E, Revert F.
Neural growth factor expression in the lateral
retinaculum in painful patellofemoral malalignment.
Acta Orthop Scand. 2001;72:146–9.
42. Sanchis-Alfonso V, Roselló-Sastre E, Revert F,
et al. Histologic retinacular changes associated with
ischemia in painful patellofemoral malalignment.
Orthopedics. 2005;28:593–9.
43. Sanchis-Alfonso V, Roselló-Sastre E, MonteagudoCastro C, et al. Quantitative analysis of nerve
changes in the lateral retinaculum in patients with
isolated symptomatic patellofemoral malalignment.
A preliminary study. Am J Sports Med.
1998;26:703–709.
44. Fulkerson JP, Tennant R, Jaivin JS, et al. Histologic
evidence of retinacular nerve injury associated with
patellofemoral malalignment. Clin Orthopn Relat
Res. 1985;197:196–205.
45. Mori Y, Fujimoto A, Okumo H, et al. Lateral
retinaculum release in adolescent patellofemoral
disorders: its relationship to peripheral nerve injury
in the lateral retinaculum. Bull Hosp Jt Dis Orthop
Inst. 1991;51:218–29.
46. Baker V, Bennell K, Stillman B, et al. Abnormal
knee joint position sense in individuals with
patellofemoral pain syndrome. J Orthop Res.
2002;20(2):208–14.
47. Jerosch J, Prymka M. Knee joint propioception in
patients with posttraumatic recurrent patella dislocation. Knee Surg, Sports Traumatol Arthrosc.
1996;4:14–8.
38
48. Wilson AS, Lee HB. Hypothesis relevant to defective position sense in a damaged knee. J Neurol
Neurosurg Psychiatry. 1986;49:1462–3.
49. Jensen R, Hystad T, Kvale A, et al. Quantitative
sensory testing of patients with long lasting
patellofemoral pain síndrome. Eur J Pain.
2007;11:665–76.
50. Ahmed M, Bergstrom J, Lundblad H, et al. Sensory
nerves in the interface membrane of aseptic loose hip
prostheses. J Bone Joint Surg. 1998;80-B:151–155.
51. Ashton IK, Ashton BA, Gibson SJ, et al. Morphological basis for back pain: the demonstration of
nerve fibers and neuropeptides in the lumbar facet
joint capsule but not in ligamentum flavum.
J Orthop Res. 1992;10:72–8.
52. Ashton IK, Roberts S, Jaffray DC. Neuropeptides in
the human intervertebral disc. J Orthop Res.
1994;12:186–92.
53. Ashton IK, Walsh DA, Polak JM, et al. Substance P
in intervertebral discs. Binding sites on vascular
endothelium of the human annulus fibrosus. Acta
Orthop Scand. 1994;65:635–639.
54. Coppes MH, Marani E, Thomeer RT, et al. Innervation of “painful” lumbar discs. Spine.
1997;22:2342–9.
55. Freemont AJ, Peacock TE, Goupille P, et al. Nerve
ingrowth into diseased intervertebral disc in chronic
back pain. Lancet. 1997;350:178–81.
56. Grönblad M, Korkala O, Konttinen YT, et al. Silver
impregnation and immunohistochemical study of
nerves in lumbar facet joint plical tissue. Spine.
1991;16:34–8.
57. Kocher MS, Fu FH, Harner ChD. Neuropathophysiology. In: Fu FH, Harner ChD, Vince KG, editors.
Knee Surgery. Baltimore: Williams and Wilkins;
1994. p. 231–49.
58. Konttinen YT, Grönblad M, Antti-Poika I, et al.
Neuroimmunohistochemical analysis of peridiscal
nociceptive neural elements. Spine. 1990;15:383–6.
59. Korkala O, Grönblad M, Liesi P, et al. Immunohistochemical demonstration of nociceptors in the
ligamentous structures of the lumbar spine. Spine.
1985;10:156–7.
60. Palmgren T, Grönblad M, Virri J, et al. Immunohistochemical demonstration of sensory and autonomic nerve terminals in herniated lumbar disc
tissue. Spine. 1996;21:1301–6.
61. Witonski D, Wagrowska-Danielewicz M. Distribution of substance-P nerve fibers in the knee joint in
patients with anterior knee pain syndrome. Knee
Surg Sports Traumatol Arthrosc. 1999;7:177–83.
62. Wojtys EM, Beaman DN, Glover RA, et al. Innervation of the human knee joint by substance-P
fibers. Arthroscopy. 1990;6:254–63.
63. Byers PD. Solitary benign osteoblastic lesions of
bone. Osteoid osteoma and benign osteoblastoma
Cancer. 1968;22:43–57.
V. Sanchis-Alfonso et al.
64. Alfredson H, Ohberg L, Forsgren S. Is vasculoneural ingrowth the cause of pain in chronic
Achilles tendinosis? An investigation using ultrasonography and colour Doppler, immunohistochemistry, and diagnostic injections. Knee Surg
Sports Traumatol Arthrosc. 2003;11:334–8.
65. Sanchis-Alfonso V, Roselló-Sastre E, Subías-López
A. Neuroanatomic basis for pain in patellar tendinosis (“jumper’s knee”): A neuroimmunohistochemical study. Am J Knee Surg. 2001;14:174–7.
66. Hasegawa T, Hirose T, Sakamoto R, et al. Mechanism of pain in osteoid osteomas: an immunohistochemical study. Histopathology. 1993;22:487–91.
67. Grönblad M, Weinstein JN, Santavirta S. Immunohistochemical observations on spinal tissue innervation. A review of hipothetical mechanisms of
back pain. Acta Orthop Scand. 1991;62:614–622.
68. Dicou E, Pflug B, Magazin M, et al. Two peptides
derived from the nerve growth factor precursor are
biologically active. J Cell Biol. 1997;136:389–98.
69. Gigante A, Bevilacqua C, Ricevuto A, et al.
Biological aspects in patello-femoral malalignment.
11th Congress European Society of Sports Traumatology, Knee Surgery and Arthroscopy. Book of
Abstracts. Athens 5–8 May, 2004.
70. Malcangio M, Garrett NE, Cruwys S, et al. Nerve
growth factor- and neurotrophin-3-induced changes
in nociceptive threshold and the release of substance
P from the rat isolated spinal cord. J Neurosci.
1997;17:8459–67.
71. Abe T, Morgan DA, Gutterman DD. Protective role
of nerve growth factor against postischemic dysfunction of sympathetic coronary innervation. Circulation. 1997;95:213–20.
72. Lee TH, Kato H, Kogure K, et al. Temporal profile
of nerve growth factor-like immunoreactivity after
transient focal cerebral ischemia in rats. Brain Res.
1996;713:199–210.
73. Isaacson LG, Crutcher KA. The duration of
sprouted cerebrovascular axons following intracranial infusion of nerve growth factor. Exp Neurol.
1995;13:174–9.
74. Kawaja MD. Sympathetic and sensory innervation
of the extracerebral vasculature: roles for p75NTR
neuronal expression and nerve growth factor.
J Neurosci Res. 1998;52:295–306.
75. Society for Ultrastructural Pathology. Handbook of
diagnostic electron microscopy for pathologists-intraining. New York-Tokyo: Igaku-Shoin Medical
Publishers Committee; 1995.
76. Shweiki D, Itin A, Soffer D, et al. Vascular
endothelial growth factor induced by hypoxia may
mediate hypoxia-initiated angiogenesis. Nature.
1992;359:843–5.
77. Liu Y, Cox SR, Morita T, et al. Hypoxia regulates
vascular endothelial growth factor gene expression
Pathophysiology of Anterior Knee Pain
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
in endothelial cells. Identification of a 5’ enhancer.
Circ Res. 1995:77:638–643.
Minchenko A, Bauer T, Salceda S, et al. Hypoxic
stimulation of vascular endothelial growth factor
expression in vitro and in vivo. Lab Invest.
1994;71:374–9.
Nagashima M, Yoshino S, Ishiwata T, et al. Role of
vascular endothelial growth factor in angiogenesis
of
rheumatoid
arthritis.
J
Rheumatol.
1995;22:1624–30.
Yamada T, Sawatsubashi M, Yakushiji H, et al.
Localization of vascular endothelial growth factor
in synovial membrane mast cells: examination with
“multilabelling subtraction immunostaining.” Virchows Arch. 1998;433:567–70.
Pufe T, Petersen W, Tillmann B, et al. The splice
variants VEGF121 and VEGF189 of the angiogenic
peptide vascular endothelial growth factor are
expressed in osteoarthritic cartilage. Arthritis
Rheum. 2001;44:1082–8.
Jackson JR, Minton JAL, Ho ML, et al. Expression
of vascular endothelial growth factor in synovial
fibroblasts is induced by hipoxia and interleukin 1ß.
J Rheumatol. 1997;24:1253–9.
Calzà L, Giardino L, Giuliani A, et al. Nerve growth
factor control of neuronal expression of angiogenetic and vasoactive factors. Proc Natl Acad
Sci USA. 2001;98:4160–5.
Sandow MJ, Goodfellow JW. The natural history of
anterior knee pain in adolescents. J Bone Joint Surg.
1985;67-B:36–38.
Selfe J, Karki A, Stevens D. A review of the role of
circulatory deficit in the genesis of patellofemoral
pain. Phys Therapy Rev. 2002;7:169–72.
Selfe J, Harper L, Pedersen I, et al. Cold legs: a
potential indicator of negative outcome in the
rehabilitation of patients with patellofemoral pain
syndrome. Knee. 2003;10:139–43.
Gelfer Y, Pinkas L, Horne T, et al. Symptomatic
transient patellar ischemia following total knee
replacement as detected by scintigraphy. A prospective, randomized, double-blind study comparing the
mid-vastus to the medial para-patellar approach.
Knee. 2003;10:341–345.
Naslund J. Patellofemoral pain syndrome. Clinical
and pathophysiological considerations. Thesis.
Karolinska Institutet, Stockholm, 2006.
Damasio AR, Grabowky TJ, Bechara A, et al.
Subcortical and cortical brain activity during the
feeling of self-generated emotions. Nat Neurosci.
2000;3:1049–56.
Diekfuss JA, Grooms DR, Nissen KS, et al. Does
central nervous system dysfunction underlie patellofemoral pain in young females? Examining brain
functional connectivity in association with patientreported outcomes. J Orthop Res. 2022;40
(5):1083–96.
Foss KDB, Slutsky-Ganesh AB, Diekfuss JA, et al.
Brain activity during experimental knee pain and its
relationship with kinesiophobia in patients with
39
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
patellofemoral pain: a preliminary functional magnetic resonance imaging investigation. J Sport
Rehabil. 2022;12:1–10. https://doi.org/10.1123/jsr.
2021-0236.
Slutsky-Ganesh AB, Diekfuss JA, Grooms DR, et al.
A preliminary investigation of the effects of patellar
displacement on brain activation and perceived pain
in young females with patellofemoral pain. J Sci
Med Sport. 2022;31;S1440–2440(22)00030–5.
https://doi.org/10.1016/j.jsams.2022.01.006.
Domenech J, Sanchis-Alfonso V, López L, et al.
Influence of kinesiophobia and catastrophizing on
pain and disability in anterior knee pain patients.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(7):1562–8.
Doménech J, Sanchis-Alfonso V, Espejo B.
Changes in catastrophizing and kinesiophobia are
predictive of changes in disability and pain after
treatment in patients with anterior knee pain. Knee
Surg Sports Traumatol Arthrosc. 2014;22
(10):2295–300.
Sanchis-Alfonso
V,
Montesinos-Berry
E,
Domenech J. Catastrophic thinking is a new puzzle
piece in understanding anterior knee pain. Orthopaedics Today Europe Official Newspaper of
EFORT. 2014;17(2):44–50.
Gracely RH. Pain catastrophizing and neural
responses to pain among persons with fibromyalgia.
Brain. 2004;127:835–43.
Rathleff MS, Petersen KK, Arendt-Nielsen L, et al.
Impaired conditioned pain modulation in young
female adults with long-standing patellofemoral
pain: a Single Blinded Cross-Sectional Study. Pain
Med. 2016;17(5):980–8.
IASP terminology. International Association for the
Study of Pain Web site. https://www.iasp-pain.org/
terminology.
Sigmund KJ, Hoeger Bement MK, Earl-Boehm JE.
Exploring the pain in patellofemoral pain: a
systematic review and meta-analysis examining
signs of central sensitization. J Athl Train.
2021;56(8):887–901.
De Oliveira SD, Rathleff MS, Petersen K, et al.
Manifestations of pain sensitization across different
painful knee disorders: a systematic review including meta-analysis and metaregression. Pain Med.
2019;20(2):335–58.
Rathleff MS, Roos EM, Olesen JL, et al. Lower
mechanical pressure pain thresholds in female
adolescents with patellofemoral pain syndrome.
J Orthop Sports Phys Ther. 2013;43(6):414–21.
Rathleff MS, Roos EM, Olesen JL, et al. Selfreported recovery is associated with improvement in
localized hyperalgesia among adolescent females
with patellofemoral pain: results from a cluster
randomized trial. Clin J Pain. 2016;32(5):428–34.
Lefaucheur JP, Drouot X, Ménard-Lefaucheur I,
et al. Motor cortex rTMS restores defective intracortical inhibition in chronic neuropathic pain.
Neurology. 2006;67:1568–74.
40
104. Young NA, Sharma M, Deogaonkar M. Transcranial magnetic stimulation for chronic pain. Neurosurg Clin N Am. 2014;25(4):819–32.
105. Powers CM, Bolgla LA, Callaghan MJ, et al.
Patellofemoral pain: proximal, distal, and local
factors, 2nd International Research Retreat.
J Orthop Sports Phys Ther. 2012;42:A1-54.
106. Soifer TB, Levy HJ, Soifer FM, et al. Neurohistology of the subacromial space. Arthroscopy.
1996;12:182–6.
107. Solomonow M, D’Ambrosia R. Neural reflex arcs
and muscle control of knee stability and motion. In:
Scott WN, ed. Ligament and extensor mechanism
V. Sanchis-Alfonso et al.
injuries of the knee: Diagnosis and treatment. St.
Louis: Mosby-Year Book, 1991; pp 389–400.
108. Nilsson G, Forsberg-Nilsson K, Xiang Z, et al.
Human mast cells express functional TrkA and are a
source of nerve growth factor. Eur J Immunol.
1997;27:2295–301.
109. Sherman BE, Chole RA. A mechanism for
sympathectomy-induced bone resorption in the
middle ear. Otolaryngol Head Neck Surg.
1995;113:569–81.
110. Woolf CJ. Pain: moving from symptom control
toward mechanism-specific pharmacologic management. Ann Intern Med. 2004;140:441–51.
Femoral and Tibial Rotational
Abnormalities Are the Most Ignored
Factors in the Diagnosis
and Treatment of Anterior Knee Pain
Patients. A Critical Analysis Review
Vicente Sanchis-Alfonso
and Robert A. Teitge
1
Introduction
At the end of 1970s, skeletal malalignment of the
limb was suggested as one of the causes of
anterior knee pain (AKP) in some young patients
[1]. It must be acknowledged that skeletal
malalignment is not an abnormal Q-angle or an
increased TT-TG distance. Skeletal malalignment is also not the position of the patella on the
trochlea. Neither is it its increased shift (subluxation) or increased tilt. Skeletal malalignment
is malalignment of the limb measured on the
transverse, coronal, and sagittal planes. The
presence of excessive femoral anteversion,
excessive external tibial torsion, or increased
varus or valgus abnormalities has a great impact
on the patellofemoral joint (PFJ) biomechanics.
In particular, rotational abnormalities are important [2, 3]. In 1979, Stan James presented a
comprehensive review of AKP in which the
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_3.
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
R. A. Teitge
Wayne State University, Detroit, MI, USA
condition of “miserable malalignment” was
described, being increased femoral anteversion
and increased external tibial torsion [1]. In 1995,
he reported on seven patients with “miserable
malalignment” who had been treated with internal tibial rotational osteotomy over an 18-year
period [4]. Several years earlier, Cooke and
colleagues [5] described internal proximal tibial
rotational osteotomy in seven patients presenting
with AKP and drew attention to the inwardly
pointing knee as an unrecognized cause of
AKP. However, the concept of skeletal
malalignment was almost unnoticed and has had
extremely little influence on orthopedic surgeons
even until today. In fact, very few publications
refer to skeletal malalignment as a cause of
AKP. From 1990 to June of 2021, only 22
published papers in English in which the association between patellofemoral disorders in
young patients and in which torsional abnormalities of the femur and/or tibia are analyzed
from a clinical point of view could be found [6].
This scarcity of published papers may be
indicative that symptomatic torsional abnormalities are a rare condition. However, in our daily
clinical practice, surgery to correct torsional
abnormalities in young AKP patients is frequent.
Obviously, this elevated incidence in our clinical
practice may be biased by the fact that numerous
patients are referred to both of us for many
patellofemoral disorders. The aim of this chapter
is to analyze why so little importance is given to
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_3
41
42
V. Sanchis-Alfonso and R. A. Teitge
this problem in the specialized medical literature.
Why do we ignore torsional abnormalities in the
diagnosis and especially in the treatment of the
AKP patient? It is a fundamental question to
delve into. We will attempt to answer it.
2
There is no Agreement on How
to Measure Torsion
We fully understand the scarce interest knee
surgeons have in rotational osteotomies. The
main reason is the diagnostic uncertainty. Limb
alignment on the transverse plane is hard to see
and difficult to measure. Currently, there is no
consensus on how to measure torsion [7–9].
Obviously, accurate measurement of torsion is
essential to diagnosing, correct surgical decisionmaking and the preoperative planning of a rotational osteotomy (i.e., the amount of correction
needed).
The first problem that is faced when we see a
patient with a torsional abnormality is to objectify and quantify the magnitude of the torsion and
therefore determine whether it is pathological or
not. Many times, the values the radiologist provides do not match with the clinical findings.
This mismatch generates doubt and uncertainty
Fig. 1 Evaluation in prone
position in a patient with
excessive left femoral
anteversion
in the orthopedic surgeon who is going to treat
those patients. This is especially true when it
comes to femoral anteversion or femoral torsion.
Currently, there are 28 methods to measure
femoral neck anteversion [7]. Figure 1 shows the
case of a patient with a pathological left femoral
anteversion in which the CT study using the
Jeanmart's method [10] (classic method), which
is the most widespread, reveals a value of 20°
that can be considered as normal. Therefore,
there is a contradiction between the physical
examination and the image in this case. How is it
possible that the imaging shows a normal value?
Without a doubt, something does not work here.
This something is the fact that the radiological
method used to evaluate femoral anteversion is
not adequate.
Murphy and colleagues have shown that the
traditional methods may underestimate the actual
femoral anteversion by a mean 13° and as much
as 18° [11]. In the same way, Kaiser and colleagues have shown a significant difference in
measurement techniques of even up to 11° [12].
Unfortunately, the current tendency is to trust the
images more and more and devalue or mistrust
the physical examination. It is a big mistake.
The CT method that we use to evaluate
femoral anteversion is the one described by
Femoral and Tibial Rotational Abnormalities …
A
C
43
B
D
Fig. 2 A, B Measurement of femoral anteversion using
the Jeanmart's method (classic method). C, D Measurement
of femoral anteversion according to the technique
described by Murphy. Draw a circle on the femoral head
(red circle) and another circle centered in the femoral shaft
below the lesser trochanter (green circle). Then, draw a
line connecting the center of these two circles. This line
defines the femoral neck axis on the transverse plane.
Next, draw a line tangent to the posterior aspect of the
femoral condyles (posterior condylar line). The angle
between these two lines represents the femoral anteversion. The line that is used as the axis of the femoral neck in
the method described by Jeanmart is not the true axis of the
femoral neck
Murphy in 1987 (Fig. 2) [11]. Murphy’s method
comes closest to defining the reality as it started
with the physical measurement of anatomic
specimens. His method of anteversion measurement correlates well with the physical examination. In the patient in Fig. 1, the measurement of
femoral anteversion with Murphy’s method
reveals a value of 39°, which is clearly pathological and coincides with what the physical
examination reveals.
Interestingly, Schmaranzer and colleagues
[13] have observed that the differences between
the classic and Murphy’s method become more
evident in patients with a clinical diagnosis of
femoral torsional abnormality. It has been shown
that the difference in femoral torsion between the
classic method and Murphy’s method increased
from 3° in a patient with normal femoral torsion
to 17° in a patient with excessive femoral torsion
upon physical examination [14]. Furthermore,
44
the more significant the increase in femoral torsion, the greater the differences between the two
methods was also observed [14]. In other words,
the differences between the two methods increase
progressively with the increase in femoral torsion, the relationship between the two methods
being trigonometric and not linear [14]. This
must be considered especially when planning a
rotational osteotomy in patients with severe
femoral torsional abnormalities to avoid mistakes
in preoperative planning.
Once it is known that there is a pathological
torsional abnormality that must be corrected, the
next step is to determine at what level the correction must be made. It may be at the proximal,
mid-diaphysis or distal level. In theory, the ideal
would be to perform the osteotomy at the site
where the deformity originates. If we do it at
another level, we can create a new deformity on
the coronal or sagittal plane even though the total
angle is going to be corrected adequately [15].
Some authors [16–18] have used conventional
imaging studies in an attempt to define where the
torsion occurs along the length of the femur.
Femoral anteversion is defined by the angle
formed by the intersection of 2 reference lines:
one proximal that represents the axis of the
femoral neck, and one distal that is tangential to
the posterior aspect of the femoral condyles and
approximates the knee joint axis. Since this angle
of torsion is defined between these 2 lines, it is
not possible to specify the level of this torsional
alteration. Defining the location of a torsional
abnormality between these 2 primary lines will
require creation of an additional 3 or 4 references
lines. Herzberg and colleagues [19] measured the
anteversion angle of the femoral neck and the
“retrotorsion” angle of the lesser trochanter in 52
female and 34 male femora taken from 46 human
cadavers (age at death 80.3 ± 8.67 years). These
authors showed that the lesser trochanter is a
well-defined landmark between the proximal and
distal femur, and its location follows a linear
correlation with femoral anteversion. Therefore,
the lesser trochanter is a landmark for separating
proximal version and distal femoral torsion.
Archibald and colleagues [15] evaluated 1210
paired adult femora from a well-preserved
V. Sanchis-Alfonso and R. A. Teitge
osteological collection. They have shown that
both the femoral neck and femoral shaft substantially contribute to femoral version. Kim and
colleagues [16] showed that femoral torsion
could occur in the supratrochanteric, infratrochanteric region, or in both sites. Seitlinger
and colleagues [17] have demonstrated that the
neck, mid and distal femur contribute to the total
femoral torsion. Sanchis-Alfonso and colleagues
[20] have shown that pathological FAV in the
AKP patient depends on both the neck and the
shaft. However, Waisbrod and colleagues [18]
have proposed that femoral torsion is a subtrochanteric deformity. Ferràs-Tarragó and colleagues [21, 22] have used three-dimensional
(3D) technology and advanced techniques to
assess similarities between volumetric structures
in order to evaluate the site where the deformity
originates. It might be a good method for planning rotational femoral osteotomy in patients
with unilateral torsional femur abnormalities
(Fig. 3) (See Videos 1 and 2). In short, there is
no universally accepted method that allows us to
determine the origin of the deformity. Therefore,
it is difficult to decide at what level to perform
the rotational osteotomy.
In summary, the fact that there is no consensus as to how to measure torsion leaves the
orthopedic surgeon in doubt about the confirmation of the diagnosis and, more importantly, in
doubt about the surgical planning. The easiest
thing to do in this situation is not to recommend
surgical treatment. If we do not correct the torsion enough, the pain will persist and the pain
will persist if we correct more than necessary. It
has been shown that a difference of 10° during
rotational osteotomy causes a considerable
increase in PFJ pressure (Fig. 4) [23]. In the
same way, Karaman and colleagues [24] showed
that both external and internal rotational
malalignment greater than or equal to 10° after
closed intramedullary nailing of femoral shaft
fractures provoked AKP while climbing stairs.
Finally, Yildirim and colleagues [25] observed
that an external rotation deformity of the femur
greater than 10° could cause a deterioration in the
patellofemoral scores and provoke AKP. Considering the possible iatrogenesis that we can
Femoral and Tibial Rotational Abnormalities …
Fig. 3 3D technology and advanced techniques to assess
similarities between volumetric structures in order to
evaluate the site where the deformity originates. In this
case, the right femur (yellow femur) has an excessive
femoral anteversion (39°). However, the left femur (blue
femur) has a normal femoral anteversion. In this patient,
there is severe right hip pain and disabling right
AKP. However, the lower left limb is completely asymptomatic. The left femur is reverted as it was a mirror vision.
Then we place the blue femur over the yellow femur to see
45
the degree of similarity between them. That is, we overlap
both femurs. The differences between both femurs are
represented in a color code. The intensity of the blue and
red colors represents the magnitude of the positive and
negative differences between both femurs. The green color
represents the absence of differences. In this case, there is a
high similarity in all the femur except in the proximal
part. Thus, we can conclude that the torsional deformity in
this particular case originates in the proximal part of the
femur
Fig. 4 Finite elements analysis in the preop and after intertrochanteric external rotational femoral osteotomy of 5° and
15° (From reference 23). (Courtesy of M.A. Perez, PhD)
46
V. Sanchis-Alfonso and R. A. Teitge
cause in a young patient if we make a hypercorrection of the torsion along with the scarce
literature that supports this technique, it is
understandable why it is not a common technique
among orthopedic surgeons.
3
Not All Torsional Abnormalities
are Symptomatic
Another reason for the scarce interest knee surgeons have shown in rotational osteotomies
would be the fact that there are patients with clear
torsional anomalies that are completely asymptomatic. There are patients with bilateral torsional abnormalities who are completely
asymptomatic (Fig. 5). The only explanation is
that their level of activity is low enough not to
apply sufficient stress to bone and or peripatellar
soft tissues. In other cases, the maltorsion is
symmetrical but only one side is symptomatic
and the other one is completely asymptomatic.
This fact increases uncertainty and discourages
the surgeons from recommending a rotational
osteotomy. We must take note that an abnormal
anatomy is only a risk factor for developing AKP
[26]. However, the length of time and magnitude
of stress on bone and/or soft tissues that are
necessary to initialize the physio-pathological
mechanisms that lead to pain and makes for a
patient are not known.
In AKP patients with torsional abnormalities,
knee pain and disability are highly variable.
Furthermore, the incidence of psychological
affectation is high in AKP patients, and the AKP
patient with a torsional abnormality is not an
exception. The prevalence of anxiety and
depression in AKP patients is higher than those
found in the general population [27, 28]. The fact
that there are patients with a lot of pain and
others with less as well as patients with a lot of
pain and little disability with the same magnitude
of pathological torsion, makes the importance of
the torsional anomaly doubtful with regard to the
symptoms. It is understandable that many
orthopedic surgeons may think that the main
problem is psychological.
According to Robert A. Teitge, the main
player in patellofemoral disease is the force
which traumatizes the PFJ tissues. That force
may act on the cartilage and bone, being
responsible for cartilage breakdown and pain. It
may also place excess tension in the patellar
ligaments, being responsible for instability and
pain. Of all the structural factors causing overload of the PFJ, the most powerful is the skeletal
Fig. 5 Asymptomatic bilateral torsional abnormality (Courtesy of R. Teitge, MD)
Femoral and Tibial Rotational Abnormalities …
malalignment, especially the torsional [3]. When
the skeleton is not normal, the quadriceps force
acting on the PFJ is not normal either. A change
in the quadriceps lateral vector may result from
an increase in femoral anteversion or an increase
in limb valgus. Additionally, it may just as well
be due to an increase in the external rotation of
the tibia on the femur or an actual lateral placement of the tibial tuberosity (TT) on the proximal
tibia that will provoke an increment of the TTTG distance. Of all the factors influencing the
lateral vector, the most important is femoral
anteversion. For example, the lateral vector
increases more than 112% if a person has an
internal torsion of the femur of 30° above the
normal value. Maltorsion may cause a maldistribution of force on the PFJ which probably
acts on both the subchondral bone and all surrounding ligaments. Bone overload is detectable
using SPECT-CT. In some patients with torsional
abnormalities, the SPECT-CT study reveals an
uptake increment in the lateral aspect of the PFJ
that allows us to justify the pain in these patients.
Therefore, SPECT-CT helps to make a correct
surgical indication. But in other cases, the
SPECT-CT is negative in spite of the presence of
a symptomatic torsional abnormality. This raises
uncertainty when it comes to blaming torsional
abnormality for the pain. This fact discourages
the surgeons from putting forward a rotational
osteotomy.
4
Lack of Agreement Regarding
Surgical Technique. Fear
of Internal Fixation Failure
and Other Complications
Another reason for the scarce interest knee surgeons have shown in rotational osteotomies is the
lack of agreement when it comes to the choice of
surgical technique. This means that if five different surgeons were asked about the best way to
proceed, it is highly probable each of them would
come up with a totally different solution
(osteotomy level, open vs percutaneous osteotomy, type of osteotomy fixation, combined procedures: release of the peroneal nerve vs. non-
47
release, fibular osteotomy vs non-osteotomy).
This would leave an inexperienced surgeon
rather confused.
There are a few unanswered questions in
osteotomy surgery. One is about knowing how
much to correct. From a practical point of view,
we always prefer undercorrecting to overcorrecting when performing rotational osteotomy.
Another debatable issue is the level of osteotomy. For example, our proposal in rotational
tibial osteotomy is an osteotomy distal to the TT.
However, other orthopedic surgeons suggest a
supra-tuberosity osteotomy. Then again, there are
others who are inclined toward a mid-shaft or
distal (supramalleolar) osteotomy. Recently,
Winkler and colleagues [29] have shown that
increased external tibial torsion is an
infratuberositary deformity and is not correlated
with a lateralized position of the tibial tuberosity.
Regarding the surgical technique, take note
that it is difficult to achieve a highly precise
osteotomy and keep it perfectly in place during
healing. With a fracture or an osteotomy, the
stress of moving the limb does not reach the
bone ends but it does concentrate at the
fracture/osteotomy site as strain (displacement)
[30]. Relative to a fracture, the more comminuted
it is, the less strain is concentrated at the fracture
line. This is because it is divided between the
number of fracture segments and the length of the
fracture. On the contrary, a straight transverse
osteotomy causes the greatest strain concentration. Thus, the internal fixation must be more
rigid to share the stress and reduce strain to an
acceptable level. Greater stability results from the
increased compression of fragments. If there is
no motion at the osteotomy site and the gap
between fragments is less than 0.5 mm, then
bone cutting cones pass across the gap and new
osteons are produced without the need for a
callus. If the gap is 0.5 mm and there is
motion, the motion of the bone ends up crushes
the cutting cones and primary bone healing will
not occur. It is well known that if you see a callus
developing after internal fixation, you know the
fixation is unstable. IM nails do not normally
provide sufficient rigid fixation. Therefore, they
are classified as “internal splints”. Inadequate
48
stabilization by means of internal fixation results
in failure when the strain is too great: plates
break, screws bend or pull out or delayed healing. Without a doubt, the fear of internal fixation
failure might be another reason for the scarce
interest knee surgeons have shown in rotational
osteotomies.
A more widespread surgical technique for
treating AKP patients is the TT osteotomy, which
has undoubtedly overshadowed the rotational
osteotomy. We do not intend to deny the validity
of this technique, but rather to broaden our
horizon in order to treat AKP patients. At this
point, it would be interesting to make some
observations on the surgery of the TT in the
patient with torsional abnormality. Mani and
colleagues [31] have demonstrated that TT
medialization increases tibial external rotation.
Therefore, greater AKP could triggered if we
perform a medialization of the TT in a patient
with excessive external tibial torsion. Moreover,
Tensho and colleagues [32] have shown that TTTG distance is affected more by knee rotation
than by tubercle malposition. For that reason, the
measurement of the TT-TG distance in patients
with torsional abnormalities is not reliable.
Franciozi and colleagues [33] have seen diminished results from TT osteotomies in patients
with increased femoral anteversion. In the same
way, Zhang and colleagues [34] evaluated 144
consecutive patients with recurrent patellar
instability. Patients were assigned into three
groups: group A (femoral anteversion <20°),
group B (femoral anteversion 20°–30°) and
group C (femoral anteversion >30°). They have
demonstrated that patients with an increased
femoral anteversion angle (>30°) had inferior
postoperative clinical outcomes and a higher rate
of residual J-sign after medial patellofemoral
ligament reconstruction combined with TT
osteotomy. That is, the TT osteotomy does not
prevent the negative effect of femoral anteversion
on PFJ. Therefore, the best available evidence
supports not performing TT osteotomy in
patients with torsional abnormalities. On the
other hand, the frequency and types of complications seen in rotational osteotomy surgery are
similar to those of the TT osteotomy. We have
V. Sanchis-Alfonso and R. A. Teitge
followed the same definition as Payne and colleagues [35] to compare the total percentage of
major complications in rotational osteotomy
surgery and TT osteotomy surgery. Major complications were defined as non-union, fracture,
infections and wound complications requiring
return to the operating room, and DVT or PE.
Payne and colleagues [35], in a systematic
review, found an overall risk of major complications after TT osteotomy of 3.0%. In our systematic review, the overall risk of major
complications after rotational osteotomy was of
3.3% [6].
5
“Orthopedics is All About
Anatomy … Plus A Little Bit
of Common Sense”
We believe that a logical approach to surgical
treatment should be based on restoring native
anatomy and repairing what is damaged. This
was clearly reflected by Jack Hughston in his
well-known sentence: “Orthopedics is all about
anatomy … plus a little bit of common sense”.
Therefore, it would be logical to correct them
surgically if we observe an obvious pathological
torsional alteration in the femur or tibia. You
should strive to restore normal anatomy, because
that will create a better biomechanical environment for the tissue. If you repair a failed tissue
that can be bone, ligament or cartilage and ignore
the mechanics that caused the tissue failure, you
will usually have a failed result.
In cases of combined femoral anteversion and
excessive external tibial torsion, there is a question. What is more important in the genesis of
AKP, femoral anteversion or external tibial torsion? From an anatomical standpoint, the best
option to treat a patient with combined excessive
femoral internal torsion and excessive external
tibial torsion would be a combination of a rotational femoral and a tibial osteotomy. Another
option would be to operate on the bone with the
greatest variance from normal, the femoral
anteversion in the case of Fig. 6. In the case of
Fig. 6, we performed a 25° proximal femoral
external rotational osteotomy with a good result
Femoral and Tibial Rotational Abnormalities …
Fig. 6 Intra-operative x-Rays. Preoperative (left). The
patella is well centered on the distal femur after an
external rotational femoral osteotomy of 25°. Mechanical
axis (MA)
but there was a recurrence of the symptoms at
9 months. For that reason, a rotational tibial
osteotomy was performed that gave a good clinical result. This case highlights the importance of
restoring completely the normal anatomy. In short,
we must understand biomechanics because
orthopedic surgery is a mechanical engineering
discipline. A complete physical examination
attempts to uncover all of the anatomic abnormalities, of which there are often many. When you
uncover any abnormal anatomy you must then
answer the question: how does this change the
normal biomechanics? This is the key question.
6
The Keys to Increasing Adherence
to Rotational Osteotomy
by a Knee Surgeon. Future
Studies
The first step in attracting orthopedic surgeons to
the field of rotational osteotomy is to give them
the means to arrive at diagnostic certainty. In this
aspect, the SPECT-CT to objectify the origin of
pain can help. The SPECT-CT reveals the
49
metabolic and geographic pattern of bone
homeostasis (Fig. 7). It can evidence overloaded
osseous areas.
However, the most important contribution to
rotational osteotomy being definitively incorporated into daily clinical practice by the knee
surgeon is the implementation of a methodology
that simplifies preoperative surgical planning and
allows for the pre-visualization of the results of
surgical interventions on our computers. For this,
the working group of the first author of this
chapter (V.S-A) uses 3D technology (see Video
Case # 1). The imaging dataset used for surgical
planning is based on a CT of the patient. Our 3D
method, is open Access, that is, it is accessible to
any orthopedic surgeon at no economic cost.
Furthermore, it not only allows for the quantification of the femoral torsion (Fig. 8) but also
carrying out virtual surgical planning. Interestingly, with 3D technology, we have shown that
the magnitude of the intertrochanteric rotational
femoral osteotomy does not present a 1:1 relationship with the effect on the correction of the
deformity (see Video Case # 1). Moreover,
rotational osteotomy surgery using 3D
printed surgical guides might improve surgical
accuracy.
In the long run, surgeons will perform rotational osteotomies if they obtain good results. To
that end, the selection of the appropriate patient
is essential. To obtain a satisfactory result, it is
important to analyze patient expectations with
regard to the results of the surgery. Moreover,
whether it is really feasible to achieve a “Minimal Clinically Important Difference” (MCID)
after surgery should be considered. Despite a
statistically significant improvement in functional scores after rotational osteotomy in a torsional abnormality, not all patients perceive a
MCID in every functional domain of the score.
Defining a MCID value for Patient-Reported
Outcome Measures (PROMs) is crucial to
determining the effectiveness of a surgical procedure and therefore the indication for surgery. It
would be interesting to determine the best scores
to evaluate patients with torsional abnormalities
and ascertain the MCID for this pathology.
50
V. Sanchis-Alfonso and R. A. Teitge
Fig. 7 SPECT/CT in an AKP patient with right external
tibial torsion. The scintigraphic uptake is markedly high
in the right patella. Disabling right AKP. The left knee
was asymptomatic in spite of the fact that external tibial
torsion was symmetric in both knees
Fig. 8 Femoral anteversion measurement. Left: Transparency has been added to the proximal femur to identify
landmarks for the center of the femoral head and the base
of the femoral neck. The junction of the center of the ball
of the femoral head and the center of the circumference at
the base of the neck define the plane of inclination of the
neck (red). The plane tangent to the posterior condyles
and posterior region of the greater trochanter is the
femoral bearing plane (purple). Right: Femoral anteversion measurement based on Murphy’s method, between
the neck inclination plane (red) and the femoral support
plane (purple)
7
Take Home Messages
– Skeletal torsional abnormalities, especially
abnormal femoral torsion, are the most
ignored factors not only in the diagnosis but
even more so in the treatment of AKP
patients.
– The “collective consciousness”, that is the
beliefs shared by the majority of orthopedic
surgeons, conveys the idea that rotational
osteotomy is a complex procedure with a high
Femoral and Tibial Rotational Abnormalities …
risk of severe complications. It seems overly
aggressive to cut the femur or the tibia of a
young “healthy” person that only “complains
of pain”. Nothing could be further from the
truth. Rotational osteotomy is a very welltolerated surgery with a low complication rate
and, in many cases, the results are immediate
relative to eliminating pain.
– Changing the limb alignment by means of
osteotomy is the single most powerful and
underutilized treatment available. The quadriceps is responsible for the force acting on the
patella. Osteotomy changes the quadriceps
direction and therefore the force acting on the
patella. If one operates on the traumatized tissue (bone, ligament or cartilage) without
changing the force which produced the trauma,
one should expect a failed result.
References
1. James SL. Chondromalacia of the Patella in the
Adolescent. In: Kennedy JC. editor. The Injured
Adolescent Knee. Baltimore: The Williams &
Wilkins Company, 1979.
2. Teitge RA. Does lower limb torsion matter? Tech
Knee Surg. 2012;11:137–46.
3. Teitge RA. The power of transverse plane limb malalignment in the genesis of anterior knee pain—
clinical relevance. Ann Joint. 2018;3:70.
4. Meister K, James SL. Proximal tibial derotation
osteotomy for anterior knee pain in the miserably
malaligned extremity. Am J Orthop (Belle Mead NJ).
1995;24:149–55.
5. Cooke TD, Price N, Fisher B. The inwardly pointing
knee. An unrecognized problem of external rotational
malalignment. Clin Orthop 1990;56–60.
6. Sanchis-Alfonso V, Domenech-Fernández J, FerrasTarrago J, et al. The incidence of complications after
derotational femoral and/or tibial osteotomies in
patellofemoral disorders in adolescents and active
adult patients. A Systematic Review with MetaAnalysis. (In press).
7. Scorcelletti M, Reeves ND, Rittweger J, et al.
Femoral anteversion: significance and measurement.
J Anat. 2020;237(5):811–26. https://doi.org/10.1111/
joa.13249.
8. Stephen JM, Teitge RA, Williams A, et al. A validated, automated, 3-Dimensional method to reliably
measure tibial torsion. Am J Sports Med. 2021;49
(3):747–56.
51
9. Snow M. Tibial torsion and patellofemoral pain and
instability in the adult population: current concept
review. Curr Rev Musculoskelet Med. 2021;14
(1):67–75.
10. Jeanmart L, Baert AL, Wackenheim A. Computer
tomography of neck, chest, spine and limbs. Atlas of
pathologic computer tomography, vol 3. Springer,
Berlin Heidelberg New York, 1983; pp 171–177.
11. Murphy SB, Simon SR, Kijewski PK, et al. Femoral
anteversion. J Bone Joint Surg Am. 1987;69
(8):1169–76.
12. Kaiser P, Attal R, Kammerer M, et al. Significant
differences in femoral torsion values depending on
the CT measurement technique. Arch Orthop Trauma
Surg. 2016;136(9):1259–64.
13. Schmaranzer F, Lerch TD, Siebenrock KA. Differences in femoral torsion among various measurement
methods increase in hips with excessive femoral
torsion. Clin Orthop Relat Res. 2019;477(5):
1073–83.
14. Ferràs-Tarragó J. Planificación quirúrgica tridimensional de las osteotomías femorales en el dolor
anterior de rodilla. Doctoral Thesis. University of
Valencia, 2021.
15. Archibald HD, Petro KF, Liu RW. An anatomic
study on whether femoral version originates in the
neck or the shaft. J Pediatr Orthop. 2019;39:e50–3.
16. Kim HY, Lee SK, Lee NK, et al. An anatomical
measurement of medial femoral torsion. J Pediatr
Orthop B. 2012;21(6):552–7.
17. Seitlinger G, Moroder P, Scheurecker G, et al. The
contribution of different femur segments to overall
femoral torsion. Am J Sports Med. 2016;44(7):1796–
800.
18. Waisbrod G, Schiebel F, Beck M. Abnormal femoral
antetorsion—a subtrochanteric deformity. J Hip Preserv Surg. 2017;4(2):153–8.
19. Herzberg W, Meitz R, Halata Z. Antetorsion of the
femur neck. A variable of the trochanter minor?
Unfallchirurg 1991;94:168–171.
20. Sanchis-Alfonso V, Domenech-Fernández J, BeserRobles M, et al. Pathological femoral anteversion in
the anterior knee pain patient depends on both the
neck and the shaft (Submitted).
21. Ferràs-Tarragó J, Sanchis-Alfonso V, RamírezFuentes C, et al. A 3D-CT analysis of femoral
symmetry—surgical implications. J Clin Med.
2020;9:3546.
22. Ferràs-Tarragó J, Sanchis-Alfonso V, RamírezFuentes C, et al. Locating the origin of femoral
maltorsion using 3D volumetric technology—the
hockey stick theory. J Clin Med. 2020;9:3835.
23. Gracia-Costa C. Análisis por elementos finitos de las
presiones femoropatelares previas y posteriores a
osteotomía desrrotadora. Trabajo de Fin de Grado.
Escuela de Ingeniería y Arquitectura: University of
Zaragoza; 2019.
24. Karaman O, Ayhan E, Kesmezacar H, et al. Rotational malalignment after closed intramedullary
52
25.
26.
27.
28.
29.
V. Sanchis-Alfonso and R. A. Teitge
nailing of femoral shaft fractures and its influence on
daily life. Eur J Orthop Surg Traumatol. 2013;24
(7):1243–7.
Yildirim AO, Aksahin E, Sakman B. The effect of
rotational deformity on patellofemoral parameters
following the treatment of femoral shaft fracture.
Arch Orthop Trauma Surg. 2013;133(5):641–8.
Erkocak OF, Altan E, Altintas M, et al. Lower
extremity rotational deformities and patellofemoral
alignment parameters in patients with anterior knee
pain. Knee Surg Sports Traumatol Arthrosc. 2016;24
(9):3011–20.
Wride J, Bannigan K. Investigating the prevalence of
anxiety and depression in people living with
patellofemoral pain in the UK: the Dep-Pf Study.
Scand J Pain. 2019;19(2):375–82.
Domenech J, Sanchis-Alfonso V, Lopez L, et al.
Influence of kinesiophobia and catastrophizing on
pain and disability in anterior knee pain patients.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(7):1562–8.
Winkler PhW, Lutz PM, Rupp MC, et al. Increased
external tibial torsion is an infratuberositary deformity and is not correlated with a lateralized position
of the tibial tuberosity. Knee Surg, Sports Traumatol,
Arthroscopy. 2021;29:1678–85.
30. Muller ME, Allgower M, Schneider R, et al. Manual
of internal fixation. Third Edition. Springer. 1991.
31. Mani S, Kirkpatrick MS, Saranathan A, et al. Tibial
tuberosity osteotomy for patellofemoral realignment
alters tibiofemoral kinematics. Am J Sports Med.
2011;39(5):1024–31.
32. Tensho K, Akaoka Y, Shimodaira H, et al. What
components comprise the measurement of the tibial
tuberosity-trochlear groove distance in a patellar
dislocation population? J Bone Joint Surg Am.
2015;97(17):1441–8.
33. Franciozi CE, Ambra LF, Albertoni LJ, et al.
Increased femoral anteversion influence over surgically treated recurrent patellar instability patients.
Arthroscopy. 2017;33(3):633–40.
34. Zhang ZZ, Zhang H, Song GY, et al. Increased
femoral anteversion is associated with inferior clinical outcomes after MPFL reconstruction and combined tibial tubercle osteotomy for the treatment of
recurrent patellar instability. Knee Surg Sports Traumatol Arthrosc. 2020;28(7):2261–9.
35. Payne J, Rimmke N, Schmitt LC, et al. The incidence
of complications of tibial tubercle osteotomy: a
systematic review. Arthroscopy. 2015;31(9):1819–25.
Why is Torsion Important
in the Genesis of Anterior Knee Pain?
Robert A. Teitge
Femoral Anteversion and Tibial Torsion are listed in many of the patellofemoral publications
over the past 60–80 years as risk factors or
associated factors for anterior knee pain, but
discussion stops after making the list and is
almost never to be reconsidered. Why? I believe
this is because we don’t know why torsion
should matter, we don’t know why it there, we
don’t know how to measure it, we don’t know
how to fix it and even those intrepid surgeons
who are willing to operate to alter it, have really
no guide as where they are starting and where
they are going. It is a daunting challenge to know
nothing. I wish here to present how interest in
these questions grew and propose a rationale for
why it matters to anterior knee pain.
A challenge to me came from Robert Kerlan MD in 1976 who said to me “Bob, no one has
studied foot problems in professional athletes,
why don’t you see what you can learn.” The
podiatrists were known to be providing “orthotics” but that was almost the limit of studies.
I stumbled across The Running Foot Doctor [1]
by Steven Subotnick D.P.M. and in it I discovered a drawing of a limb with Chondromalacia of
the Knee which was said to result from a pronated
foot which was increasing the Q-Angle from 15°
R. A. Teitge (&)
Department of Orthopaedic Surgery, Wayne State
University, Detroit, MI, USA
e-mail: rteitge@med.wayne.edu
to 30° and creating an abnormal quadriceps pull.
I left Dr. Kerlan and moved to Seattle where
Sigvard (Ted) Hansen, Jr. M.D. said “Bob, You
have to get to know Stan Newell, D.P.M.” Stan
Newell was the artist who had produced all of the
drawings for The Running Foot Doctor. Stan was
making all the orthotics for the professional athletes in Seattle skirting around the orthopaedic
community. Stan told me “Bob, I can cure more
than 50% of all athletic knee pain with orthotics,
even though I have no idea why.” An interesting
thought. The recreational running craze was just
beginning, Nike was just starting and Stan Newell
and Stan James, M.D. in Eugene, Oregon became
the consultants to Nike Shoes as the orthopaedic
world became interested in running and anterior
knee pain. Stan James was working with many
world-class runners in Eugene and being asked to
lecture on “Runner’s Knee” at various professional society meetings. In 1979 he contributed a
chapter “Chondromalacia of the Patella in the
Adolescent” to Jack Kennedy’s book The Injured
Adolescent Knee [2]. This chapter almost summarizes what we know today and contains the
brilliant description of Miserable Malalignment.
So, beginning in 1980 and using what I learned
from the two Stans, I have examined every knee
patient with both the standard knee examination
and the runner’s exam and concluded torsion is
important.
The correlation of physical examination with
clinical assessment of femoral or tibial torsion is
modest to poor. Consequently, awareness of
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_4
53
54
R. A. Teitge
torsional excess is often overlooked. Special
imaging is mandatory. To understand lower
extremity kinematics requires knowing where the
axis of motion is for all the joints in the chain
including hip, knee, ankle and subtalar joint.
Variations in joint geometry will change the axis
of a particular joint, which will change the
kinematics of that limb. Correlating anatomic
landmarks with imaging is not standardized and
despite modern imaging there is still controversy
in locating with precision the axes of these 4
joints. It may not be possible to define an axis of
joint motion by studying a single bone. Two
points near the ends of the bones are selected and
lines between the two points are used to define
the axis. Different investigators have selected
different points, thus different lines are proposed
to reflect the same axes. It is common that axes
from different investigators may vary by 100%
for the hip, knee, ankle and subtalar joint. Kaiser
et al. [3] found the difference between the mean
of 2 commonly used measurement techniques
was 97% and in one single specimen the difference was 140%. These variations in measurement technique makes comparing studies difficult
Fig. 1 A The maximum
quadriceps efficiency is with
knee joint facing forward in
the direction the body is
moving (Joint axes are red
lines). 1 B With normal
femoral anteversion the
greater trochanter is posterior
when the knee faces straight
forward
A
and even these selected lines may have nothing
to do with joint motion.
The action of a muscle in moving a joint is
most efficient when it’s line of action is perpendicular to the joint axis. The quadriceps controls
knee flexion. It is most efficient when working in
the sagittal plane with the knee axis ⊥ to the
sagittal plane and with the knee joint moving
straight forward in the direction the body mass is
moving. Levens et al. [4] as long ago as 1948,
reported the knee joint axis normally moves
directly forward during gait in line of the body
motion with only a minimal amount of rotation in
the transverse plane (Fig. 1).
Anterior knee pain is usually the result of an
abnormal force. A knee joint in which no force is
acting is seldom painful. The abnormal force
may be an excessive force or a mal-directed
force. A reduction in force generally results
in reduction of pain, but usually with some
associated loss of function. Most of the quadriceps muscle force is exerted as a vector in the
sagittal plane pushing the patella against the
trochlea to maintain of control knee flexion–extension. (Fig. 2).
B
Why is Torsion Important in the Genesis …
Fig. 2 A The resultant of the
quadriceps force vector and
the patellar tendon force
vector creates the
patellofemoral joint reaction
force. It is this force which
keeps the knee from
collapsing and controls its
position of flexion–extension.
B This force is maximum
when it is perpendicular to the
knee joint axis and is in the
sagittal plane with the knee
axis in the coronal plane
55
B
A
But the knee joint is unusual because it must
have a tibio-femoral valgus. The tibio-femoral
valgus is needed to move the knee joint closer to
the midline under the center of mass. Placing the
knee joint closer to the center of body mass
reduces bending forces in the femur and tibia and
allows us to balance on one foot, a requirement
for bipedal gait.
The tibiofemoral angle, however, means the
quadriceps does not act perpendicular to the knee
joint axis, but is deviated in the lateral direction,
thus in addition to the major posterior vector
component, there is a lateral component (Fig. 3).
It is assumed that the lateral vector is counterbalanced by the lateral trochlear inclination. As
the knee internally rotates during flexion the
tibial tuberosity moves medially so the direction of the quadriceps force is more medial and
the lateral vector of this quadriceps force
decreases.
The femur and tibia are both normally twisted.
The biomechanical purpose of the twist is
unclear. It is an assumption that “normal” twist is
optimal for “normal” function such as walking.
Femoral twist is measured as the angle in the
transverse plane between the axis of the hip and
knee.
If there is an abnormal inward twist in femur
so the knee joint points medially, the knee joint
can be placed facing forward only by external
rotation of the hip joint. The acetabulum may
limit the degree of external rotation needed to
place the knee axis forward, or it may place the
external rotators of the hip in such a shortened
position they cannot provide stability. It is
common in such cases, that fatigue of the hip
rotators allows the femur to rotate inward so the
knee joint axis faces medially. If the patella is
pointing medially the quadriceps force will be
more in the lateral direction and the lateral
56
Fig. 3 The valgus
tibiofemoral angle acts
to move the knee joint
closer to the center of
mass of the body. This
tibiofemoral angle deviates the quadriceps
insertion laterally which
produces
a
lateral
quadriceps vector in
addition to the major
posterior vector
quadriceps vector increases at the expense of the
posterior vector which decreases (Fig. 4). To
maintain knee flexion stability, the total force
must increase to prevent knee collapse. One
cause of anterior knee pain is thought to be this
excess lateral quadriceps vector. As the knee
joint rotates out of the sagittal plane the posterior
vector becomes less effective so the total
quadriceps force must increase to maintain stability. As the posterior vector decreases the lateral vector increases so articular shear is
increased which shifts the center of force in the
PFJ as well as altering tension in the retinacular
ligaments. Altering the direction of the quadriceps vector may also alter the tibiofemoral rotation orientation. This is probably best measured
today with weight-bearing CT scanning for
transverse plane alignment.
R. A. Teitge
If there is an abnormal outward twist of the
femur, femoral retroversion, the opposite effect
occurs, the quadriceps medial vector will
increase obviously shifting the center of force
medially in the PFJ (Fig. 5).
If there is an increase in external tibial torsion
and the knee joint is facing forward the foot will
face more laterally. The body weight vector will
push on the side of the outward pointing foot
resulting in excess pronation, stretch of the
medial arch, bunions, posterior tibial tendon
strain, shortening of the Achilles tendon and
lateral ankle impingement. Landing from a jump
requires the ankle joint axis to be perpendicular
to the direction of landing so dorsiflexion
can absorb excess energy. Since gait on an outward facing foot can be uncomfortable or
fatiguing the limb is often internally rotated
placing the foot its optimal functional position
but causing the knee joint axis to face medially
which again increases the lateral quadriceps
vector and requiring more total quadriceps force
required to stabilizing knee flexion.
An increase in internal tibial torsion has the
opposite effect with the primary complaint being
of increased tripping, lateral ankle sprains and
increased loading of the medial plafond.
The normal angular relationship of the hip
joint, knee joint, ankle joint and subtalar joint
axes when viewed in the transverse plane allows
for normal kinematics and with normal distribution of forces transferring the body weight to the
ground. Precise location of these axes is necessary for limb kinematic and gait studies.
Torsional abnormalities in the femur or tibia
obviously can only be corrected by transverse
plane osteotomy.
A simple coronal plane vector diagram of the
Q angle including its lateral component vector in
a normal aligned limb suggests a 5 mm medial
transfer of the tibial tuberosity may reduce the
lateral quadriceps vector by 27%, but a reduction
Why is Torsion Important in the Genesis …
A
57
B
Fig. 4 The Quadriceps direction is changed with a
change in limb torsion. The quadriceps force is generally
in line with the femur. A with normal anteversion the knee
joint faces forward and the majority of the quadriceps is
posterior which produces the PF Joint reaction force. B If
the knee points inward, the quadriceps pulls more laterally
so the lateral vector is increased while the posterior vector
is decreased. The reduction in posterior force means the
total quadriceps force must increase to control knee
stability. The black arrows represent the quadriceps force
and its posterior and lateral vectors. The quadriceps force
is normally in line with the femur, the posterior force
vector is indicated on the left and the lateral force vector is
indicated on the right. A medial pointing knee may occur
if there is increased femoral anteversion, if there is more
internal rotation of the hip joint or if there is more external
tibial torsion and the foot is then placed facing forward
of 30° excess femoral anteversion may reduce
the lateral quadriceps vector by 112%.
Precise biomechanical studies investigating
the effect of changing skeletal geometry on force
transmission are needed to estimate when
pathologic values are reached. These studies
must include the changing of force provided by
altered skeletal geometry, contracting muscles,
body weight, limb length, hip, and foot and ankle
positions. Until then we can only assume that the
population normal is a reasonable goal for torsion correction.
58
R. A. Teitge
References
1. The Running Foot Doctor by Steven I. Subotnick, D.
P.M, World Publications, Mt View, California ©
1977.
2. James SL. Chondromalacia of the Patella in the
Adolescent, p205–251 in The Injured Adolescent
Knee Ed. J.C. Kennedy, Williams & Wilkins Co.
Baltimore, © 1979.
3. Kaiser P, et al. Significant differences in femoral
torsion values depending on the CT measurement
technique. Arch Orthop Trauma Surg. 2016;136
(9):1259–64.
4. Levens AS, et al. Transverse rotation of the segments
of the lower extremity in locomotion. J Bone Joint
Surg. 1948;30(4):859–72.
Fig. 5 Computer simulation of the skeleton in a patient
landing from a jump. Both knees are equally flexed. She
has 50° of femoral anteversion on the right and has had an
external rotation proximal femoral osteotomy of 35° on
the left. The right knee is pointed inward so the
quadriceps is not acting in the sagittal plane. She does
not have a valgus alignment, the apparent valgus is due to
the combination of knee flexion and an inward pointing
knee. This produces a very large lateral component to the
quadriceps force. On the left, the knee is flexing in the
sagittal plane, the patella is facing forward and because
the tibia internally rotates in flexioin there is no lateral
vector to the left quadriceps
Clinical and Radiological Assessment
of the Anterior Knee Pain Patient
Vicente Sanchis-Alfonso, Cristina Ramírez-Fuentes,
Laura López-Company, and Pablo Sopena-Novales
1
Introduction
Anterior knee pain (AKP), which is pain behind
or around the patella, is one of the most common
reasons for consultation with an orthopedic surgeon specializing in the knee among teenagers
and young adults. Although it typically occurs in
physically active people less than 40 years of
age, it does indeed affect people of all activity
levels and ages [1]. A careful clinical history and
physical examination along with imaging studies
are crucial to obtaining an accurate diagnosis.
They will be the cornerstone for a correct
treatment.
The objective of this chapter is to come to an
understanding of how AKP patients should be
evaluated during consultation to obtain a whole
picture for each patient. Doing so will aid in
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
C. Ramírez-Fuentes
Medical Imaging Department, Hospital Universitario
y Politecnico La Fe, Valencia, Spain
L. López-Company
Department of Rehabilitation and Physical Therapy,
Hospital Arnau de Vilanova, Valencia, Spain
P. Sopena-Novales
Department of Nuclear Medicine, Hospital Vithas 9
Octubre, Valencia, Spain
identifying potentially modifiable factors to personalize treatment and achieve better outcomes.
We want to emphasize that the physical examination must not be limited to the knee. The entire
limb must be evaluated. Moreover, we must
always assess the psychological status and central sensitization of all patients with AKP,
including those with severe structural anomalies
that may justify the pain.
2
Clinical History—“Listen
to the Patient”
Talking with the patient is fundamental but is too
often neglected. We must listen very carefully to
our patients as they will usually tell us, in their
own words, what is wrong. It is our mistake if we
fail to truly understand them and assume we
know better.
The first diagnostic step is a thorough clinical
history. This is where we uncover the main clue
for an exact diagnosis. For instance, the absence
of a traumatic episode or presence of bilateral
symptoms should lead towards a patellofemoral
pathology and away from a meniscal pathology
in the young patient. It is common to have
symptoms in both knees that may change from
one knee to the other over time. This is a tip-off
for a patellofemoral problem. On the contrary,
the presence of effusion, more than patellofemoral pain, suggests an intra-articular pathology
(e.g., meniscal rupture, pathologic plicae,
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_5
59
60
osteochondral or chondral lesions or synovial
pathology). Nevertheless, a small effusion may
be present in AKP patients. However, polyarthralgia is not a part of the pathology we are
now dealing with.
Generally, the onset of symptoms is insidious.
It reflects an overuse condition or an underlying
malalignment. Overuse can be the result of a new
activity or of the increase in the time, frequency
or intensity of a previous work or sports activity.
In these cases, getting the history should be oriented to determining which supraphysiologic
loading activity or activities are of importance in
the origin of AKP. The identification and rigorous control of the activities associated with the
initiation and persistence of symptoms is crucial
for treatment success. For example, patients with
left AKP should avoid driving a car with a clutch
for prolonged periods of time because it aggravates the symptoms. In these cases, patient education is crucial to preventing recurrence. In
other cases, the symptoms can be secondary to a
direct knee trauma (e.g., automobile accident in
which the anterior knee strikes the dashboard
[“dashboard knee”]) or an indirect knee trauma.
One must not forget the possibility of AKP
secondary to a posterior cruciate ligament
(PCL) deficiency when there has been a knee
trauma. This is a well-known cause for AKP
given that PCL tears increase patellofemoral joint
(PFJ) reaction force through posterior displacement of the tibial tuberosity [2]. It is also
important to examine the integrity of the anterior
cruciate ligament (ACL) as AKP is present in
20–27% of patients with a chronic ACL insufficiency [2].
The main symptom AKP patients experience
is pain. That pain can be retropatellar or peripatellar. The pain is often described as dull with
occasional sudden episodes of sharp pain. When
asked to locate the pain, it is often difficult for the
patient to pinpoint the area of pain while placing
his or her hand over the anterior aspect of the
knee. However, the pain can also be medial,
lateral or popliteal. Generally, patients have
multiple painful sites with different degrees of
pain intensity. Pain related to the extensor
mechanism is typically aggravated by activities
V. Sanchis-Alfonso et al.
like climbing and descending stairs, squatting,
using the clutch when driving a vehicle with
manual transmission (left AKP), wearing highheeled shoes. It is also worsened after prolonged
sitting with knee flexion, for instance during a
long trip by car or prolonged sitting in a cinema
(“movie sign” or “theater sign”). It improves by
extending the knee. A constant and severe pain
way out of proportion to physical findings that
has a sudden onset after a knee injury or surgery
should make us think of psychological issues or
Reflex sympathetic dystrophy (RSD) or Complex
regional pain syndrome (CRPS). This is true
even when the classic vasomotor findings are
absent. It is classified as neuropathic pain.
Finally, constant burning pain indicates a neuromatous origin. To quantify the pain, we use the
Visual analogue scale (VAS). It is a sensitive
outcome measure for AKP, with a difference of
2 cm being considered clinically relevant [3]. To
screen for neuropathic pain, we advocate for the
use of the Douleur Neuropathique 4 scale (DN4)
[4]. The sensitivity and specificity of the DN4
stands at around 95% and 97% [4].
Other symptoms of AKP are a giving-way
sensation and crepitus. Determining whether the
patient’s pain is associated with a lateral patellar
instability is very important because both the
treatment and the prognosis are very different in
patients with AKP secondary to patellar instability when compared to those without patellar
instability. “Giving-way” episodes due to ACL
deficiency are brought on by rotational activities.
On the other hand, “giving-way” episodes related
to patellofemoral problems are associated with
activities that do not imply rotational strains. It is
a consequence of a sudden reflex inhibition
and/or atrophy of the quadriceps muscle. Patients
sometimes report locking of the knee, which is
usually only a catching sensation. However, they
can actively unlock the knee. Therefore, this type
of locking should not be confused with the one
experienced by patients with meniscal lesions.
Finally, another symptom is crepitus. It should
not be mistaken for the snapping sensation more
consistent with a pathological plica. Crepitus is
common but is clinically irrelevant in most cases.
However, crepitus creates negative emotions,
Clinical and Radiological Assessment …
inaccurate etiological beliefs and finally leads to
fear-avoidance behavior and lower functional
performance [5].
Apart from pain, AKP patients present disability to a great or lesser degree. The World
Health Organization defines disability as “a
limitation of function that compromises an individual’s ability to perform an activity within the
range considered normal”. Regardless of how
intense the pain is, AKP patients show different
degrees of disability in their everyday life. A way
to objectify and quantifying disability is by
means of self-administered scales like the International Knee Documentation Committee evaluation (IKDC) and the Kujala score. It is also
important to know the patient’s activity level
prior to the treatment and what he or she wants to
achieve through treatment to be able to offer
realistic goals.
Patients with AKP have a high incidence of
anxiety, depression, kinesiophobia (the fear that
physical activity will cause more injury or a reinjury and subsequent pain) and catastrophizing
(the belief that pain will worsen and cannot be
relieved) [6]. Over half of people living with
AKP experience anxiety and/or depressive
symptoms. The levels of anxiety and depressive
symptoms in AKP patients are much higher than
those found in the general population (anxiety
symptoms: 49.5% vs. 5.9–7.8%, respectively;
depressive symptoms: 20.8 vs. 3.3–7.8%,
respectively) [7, 8]. Therefore, recognizing and
quantifying the presence of these psychological
factors are important to getting a whole picture of
the patient and to planning the best treatment.
Self-administered screening tests for anxiety and
depression (Hospital Anxiety and Depression
Scale), catastrophizing (Pain Catastrophizing
Scale), and kinesiophobia (Tampa Scale for
Kinesiophobia) should be incorporated into the
clinical history in all the cases [6]. Moreover,
signs of central sensitization are present in AKP
patients in a high percentage of cases [9].
Therefore, it would be very interesting to recognize and quantify it using a self-administered
Central sensitization score.
Finally, we must ask about previous knee
surgeries. For example, one of the causes of
61
disabling AKP after surgery is iatrogenic medial
patellar instability (IMPI) secondary to an “extensive” lateral retinacular release. Inappropriate
physiotherapy could also be responsible for
iatrogenic AKP. Therefore, it is essential that the
patient describe exercises that are being or have
been done with the physiotherapist or in the gym.
3
Physical Examination
The second diagnostic step is a thorough and
careful physical examination. It is essential. Its
primary goal is to locate the painful zone and to
reproduce the symptoms. The location of the
pain can indicate which structure is injured. This
is extremely helpful to making the diagnosis and
to planning the treatment. The most important
diagnostic tool is the “finger”.
3.1 Tests to Locate the Painful Zone
and Reproduce the Pain
The lateral retinaculum should be felt and
assessed carefully. Tenderness anywhere over
the lateral retinaculum, especially where the
retinaculum inserts into the patella, is a very
frequent finding (90%) in AKP patients [10]. We
perform the patellar glide test to evaluate lateral
retinacular tightness. This test is performed with
the knee flexed at 30º and the quadriceps relaxed.
The patella is divided into four longitudinal
quadrants and is displaced medially (Fig. 1).
A medial translation of one quadrant or less is
suggestive of excessive lateral tightness [2]. With
this test, pain is elicited over the lateral retinaculum. The patellar tilt test can also detect a tight
lateral retinaculum. It should always be done. In
a normal knee, the patella can be lifted from its
lateral edge farther than the transepicondylar
axis, with a fully extended knee. On the contrary,
a patellar tilt of 0º or less indicates a tight lateral
retinaculum. Lateral retinacular tightness is very
common in AKP patients. Furthermore, it is the
hallmark of the excessive lateral pressure syndrome described by Ficat [11]. In those cases
with AKP after ACL reconstruction, we
62
Fig. 1 Patellar glide test. The patellofemoral joint is
mentally divided into quadrants and patellar mobility is
assessed in both directions
passively “tilt” the inferior pole of the patella
away from the anterior tibial cortex to rule out
pretibial patellar tendon adhesions.
The axial compression test of the patella (or
patellar grind test) should be part of the systematic examination as it elicits AKP originating
in the patellofemoral articular surfaces (patellar
and/or trochlear subchondral bone). To perform
the axial compression test, we compress the
patella against the trochlea with the palm of the
hand at various angles of knee flexion (Fig. 2). In
addition, this test makes for determining the
location of the lesion in the patellar articular
cartilage. With knee flexion, the patellofemoral
contact zone is displaced proximally in the
V. Sanchis-Alfonso et al.
patella and distally in the femur. Thus, proximal
lesions will yield pain and crepitation at
approximately 90º of knee flexion. On the contrary, distal lesions are tender in the early degrees
of knee flexion. We also perform the sustained
knee flexion test. When it is positive (the
appearance of pain), it means that the patella is
the origin of the pain. It is caused by an increase
in intraosseous pressure [12]. For the sustained
knee flexion test, the patient lies supine on an
examination table with his or her knee extended
and relaxed. The knee is then flexed fully and
kept firmly in a sustained flexion for up to 45s.
The test is positive if the patient complains of
increasing pain after a pain-free interlude of 15 to
30s.
Allen and colleagues [13] found a significant
association between proximal patellar tendinosis
and abnormal patellar tracking in AKP patients.
Therefore, palpation of the inferior pole of the
patella ought to be carried out in all cases to
rule-out patellar tendinopathy. To perform this
test, press downward on the proximal patella. In
this way, the inferior pole of the patella tilts
anteriorly. This maneuver permits palpation of
the proximal patellar tendon attachment (Fig. 3).
However, there is quite often mild tenderness at
the attachment of the patellar tendon at the
inferior pole of the patella in individuals who
play sports. Thus, only moderate and severe pain
should be considered pathological. Moreover,
Hoffa’s fat pad should always be felt as it can be
a source of pain as well (Hoffa’s test) (Fig. 4).
Finally, existing scars should be palpated and
Tinel’s sign performed to detect neuromas. Pain
improvement after an infiltration of the painful
area with local anesthesia or after unloading the
area with functional taping provides evidence for
the origin of pain.
3.2 Pressure Algometry
Fig. 2 Axial compression patellar test
The clinical examination is crucial to identifying
the neuropathic AKP subgroup. This is important
to know the prognosis of the patient that is to
undergo treatment. A patient with CRPS presents
with skin changes like erythema and edema with
Clinical and Radiological Assessment …
63
Fig. 3 Palpation on the distal pole of the patella and the proximal patellar tendon
3.3 Range of Motion and Muscle
Length Testing
Fig. 4 In patients with impingement of the Hoffa fat pad,
pain is dramatically exacerbated by quadriceps contraction or passive knee extension while applying pressure of
the fat pad with the fingers. This happens because this
movement causes a small posterior tilt of the inferior pole
of the patella, which impinges on an inflamed and
sensitized infrapatellar fat pad
an allodynic or a hyperalgesic pain response to
palpation on the anterior aspect of the knee and
restriction in the mobility of the patella. Hyperalgesia can be demonstrated with pressure
algometry [14]. In these cases, we found reduced
pain thresholds. However, pressure algometry
should be used to quantify the pain at baseline
and to monitor an improvement in terms of
hyperalgesia with the treatment rather than as a
diagnostic method as there is no specific value
that serves as a threshold value for hyperalgesia.
The range-of-motion of the knee as well as hip
and ankle should be evaluated. Both legs should
be examined. Exploring knee extension in both
knees is mandatory because even small degrees
of extension loss can cause AKP. To evaluate
knee extension, the patient lies prone on the
examining table with the lower extremity supported by the thighs. The difference in heel
height is measured [15]. The conversion of heel
height difference to degrees of extension loss is
presented in the table of Fig. 5. Limited ankle
dorsiflexion range of motion has been related to
AKP. Therefore, it should be evaluated in all
AKP patients [16].
It is very important to assess the flexibility of
anterior hip structures (iliopsoas) (Fig. 6), the
quadriceps, hamstring, soleus, gastrocnemius
muscles and the iliotibial band as the pathology
under scrutiny is often associated with a
decreased flexibility of these structures [17, 18].
Tightness of these structures indicates the need
for specific stretching exercises and possible
training modification. However, only a shortened
quadriceps muscle has been shown to predict
AKP development [19]. Flexibility tests can be
measured with different reproducible tools like
the standard or digital goniometer.
64
V. Sanchis-Alfonso et al.
Fig. 5 Evaluation of knee extension. (Table from Dale Daniel et al. Raven Press, 1990) [15]
A
B
C
Fig. 6 Evaluation of the flexibility of anterior hip structures. A, B Normal subject. C Shortening of the iliopsoas
Clinical and Radiological Assessment …
To test quadriceps flexibility, the patient lies
prone, and the knee is passively flexed with one
hand while stabilizing the pelvis with the other
hand to prevent compensatory hip flexion
(Fig. 7). We can measure quadriceps tightness as
degrees of prone knee flexion. Suggestions for
quadriceps retraction are: (1) asymmetry, a different flexion of one knee compared to the other,
(2) the feeling of tightness in the anterior aspect
of the thigh, and (3) elevation of the pelvis due to
flexion of the hip. It is important to assess
quadriceps contracture as this can increase the
contact pressure between patella and femur in a
direct way.
To test hamstring flexibility, the patient lies
supine with the hip at 90º of flexion. The patient
is then asked to straighten his or her knee
(Fig. 8). If complete extension is not possible,
there is a hamstring contracture, and its amount is
measured by the popliteal angle. Most young
athletic individuals have popliteal angles
between 160º and 180º [2]. Hamstring tightness
implies an increase in the quadriceps force necessary to extend the knee, which augments the
PFJ reaction force.
Gastrocnemius and soleus flexibility is
evaluated by measuring the amount of active
ankle dorsiflexion while the physical therapist
stabilizes the subtalar joint. Gastrocnemius flexibility is evaluated with the knee extended and
we evaluate soleus flexibility with the knee
flexed at 90º (Fig. 9). Tightness of the
65
gastrocnemius, in the same way as hamstrings
tightness, increases the PFJ reaction force,
keeping the knee in a flexed position. Moreover,
limited ankle dorsiflexion results in increased
subtalar joint pronation. It causes an increment of
tibial internal rotation with deleterious effects on
PFJ biomechanics [2].
The iliotibial band (ITB) is often tight in AKP
patients. This causes lateral patellar displacement
and tilt as well as weakness of the medial patellar
retinaculum. We use Ober’s test to assess ITB
flexibility. To perform this test, the patient lies
on the side opposite the affected leg with the hip
and knee of the bottom leg fully flexed to eliminate the lumbar lordosis. Then, the examiner
flexes the affected knee and hip at 90º. After that,
he/she passively abducts the affected hip as far as
possible and extends the thigh so that it is in line
with the rest of the body (neutral position), which
places the ITB on maximal stretch. Palpation of
the ITB just proximal to the lateral femoral
condyle during maximal stretch will cause severe
pain in patients who have excessive ITB tightness. At this position, the patient is told to relax,
and then the thigh is adducted passively. If the
thigh remains suspended off the table, the test is
positive (shortened ITB). If the thigh drops into
an adducted position, the test is negative (normal
ITB).
Finally, Thomas’s test (Figs. 10 and 11) is a
good method to evaluate both the iliopsoas and
iliotibial band tightness. The patient holds the
non-test limb with the hip at 90° of flexion while
the physician stabilizes the pelvis of the test limb
from the anterior superior iliac spine. The free leg
is allowed to fall in the extension direction to the
point where the pelvis begins to move.
3.4 Assessment of Muscle Strength
Fig. 7 Evaluation of quadriceps flexibility
It has been demonstrated that hip abductors and
external rotation weakness are associated with
AKP [20, 21]. Therefore, it is crucial to evaluate
the strength of these muscles in AKP patients to
address muscle imbalances. Traditional manual
muscle testing or a handheld dynamometer could
be used depending on availability (Fig. 12).
66
Fig. 8 Evaluation of hamstrings flexibility. (Republished
with permission of AME Publishing Company. From
Sanchis-Alfonso V, et al. Evaluation of anterior knee pain
A
V. Sanchis-Alfonso et al.
patient: clinical and radiological assessment including
psychological factors. Ann Joint, 3:26, 2018; permission
conveyed through Copyright Clearance Center, Inc.)
B
Fig. 9 Evaluation of grastrocnemius (A) and soleus
(B) flexibility. (Republished with permission of AME
Publishing Company. From Sanchis-Alfonso V, et al.
Evaluation of anterior knee pain patient: clinical and
radiological assessment including psychological factors.
Ann Joint, 3:26, 2018; permission conveyed through
Copyright Clearance Center, Inc.)
3.5 It is Mandatory to Look Beyond
the Patellofemoral Joint
between torsional abnormalities [excessive
external tibial torsion (Fig. 13) and femoral
anteversion (Fig. 14)] and AKP.
It is very important to evaluate skeletal
malalignment, the malalignment of the limb on
the transverse, coronal, and sagittal planes. With
the patient standing, barefoot, with their feet
together, we assess (Fig. 13): (1) the alignment
Many orthopedic surgeons focus only on the
knee when evaluating an AKP patient. This
approach is a great mistake because there are
other causes of AKP that are at a distance from
the knee. For example, a clear relation exists
Clinical and Radiological Assessment …
67
Fig. 10 Thomas’s test in a normal subject
A
B
C
Fig. 11 Thomas’s test in a pathological case. A Shortening of the iliotibial band. Hip abduction occurs when the hip
goes in extension. B Shortening of the iliopsoas. C Shortening of the rectus femoris
68
Fig. 12 A Hip abductor strength measurement. B Hip
external rotator strength measurement. (Republished with
permission of AME Publishing Company. From SanchisAlfonso V, et al. Evaluation of anterior knee pain patient:
V. Sanchis-Alfonso et al.
clinical and radiological assessment including psychological factors. Ann Joint, 3:26, 2018; permission conveyed
through Copyright Clearance Center, Inc.)
Fig. 13 External tibial torsion (right limb). Pseudo-varus (right limb). Squinting patella (right knee)
Clinical and Radiological Assessment …
69
Fig. 14 Femoral anteversion
on the coronal plane (valgus/varus), (2) patella
orientation (neutral, squinting patella), and
(3) the morphology of the forefeet (pronatus,
hallux valgus). From the back, we evaluate:
(1) the varus or valgus alignment of the knee and
(2) a varus or valgus alignment of the calcaneus.
Finally, we evaluate genu recurvatum or flexum
of the knees from the side. When the patient
stands with the feet parallel, the patella should be
facing forward. In patients with excessive external tibial torsion, a squinting patella and a genu
varum can be seen. The varus in patients with
external tibial rotation may be real, or it may be a
reflection of the tibial torsion (thus pseudovarus). The combination of increased femoral
anteversion and increased external tibial torsion
has been termed miserable malalignment syndrome that includes the squinting patella, genu
varum, genu recurvatum and the pronated foot.
In the prone position, the proportion of internal
to external rotation of the hips in extension must
be measured. If internal rotation exceeds external
rotation by more than 30º, there is increased
femoral anteversion (Fig. 14). In cases with isolated excessive external tibial torsion, internal
and external rotation are similar.
In a previous study, we observed that there is
an association between Cam femoroacetabular
impingement (FAI) and AKP [22]. Therefore, an
evaluation of Cam FAI should be performed
during the physical examination of AKP patients,
especially in patients with normal knee imaging
studies when the pain continues after appropriate
conservative treatment. In this case, AKP is
secondary to functional femoral external rotation
as a defense mechanism to avoid hip pain.
Finally, examination of the feet is essential as
pronated feet play an important role in the origin
of AKP. A functional hallux limitus may be a
predisposing factor for AKP [23]. Functional
hallux limitus consists of a loss of dorsal flexion
of the first metatarsophalangeal joint with the
ankle in dorsal flexion. Limited ankle dorsiflexion range-of-motion has been linked with AKP
and has also been related to altered kinematics of
the knee. The implication is that this may be
involved in the pathogenesis of AKP. Therefore,
ankle dorsiflexion should be evaluated in all
AKP patients (Fig. 15) [24].
3.6 Functional Tests
The current trend in evaluating AKP patients is
using functional tests to detect inapt body
movement patterns that might be responsible for
70
V. Sanchis-Alfonso et al.
Fig. 15 Measurement of ankle joint dorsiflexion range.
(Republished with permission of AME Publishing Company. From Sanchis-Alfonso V, et al. Evaluation of
anterior knee pain patient: clinical and radiological
assessment including psychological factors. Ann Joint,
3:26, 2018; permission conveyed through Copyright
Clearance Center, Inc.)
the pain symptomatology. The final objective
would be to retrain these inapt movements and
thereby reduce the pain.
Fig. 16 Single-leg squat test.
A Correct neuromuscular
control. B Poor
neuromuscular control
A
The most frequently used functional tests are:
(1) the single-leg squat (Fig. 16); (2) the stepdown test (Fig. 17) and (3) the hop down test
(Fig. 18). The three tests explore the same thing
but with different levels of demand. Therefore,
we will use the most appropriate for each patient,
which depends on the disability that the patient
has.
During these tests, many AKP patients have
excessive functional knee valgus. This functional
knee valgus is mainly secondary to femoral
adduction. Some AKP patients show lower limb
abnormalities secondary to muscle weakness
with the subsequent lack of dynamic control of
the lower extremity. It may have an influence on
the normal patellofemoral tracking and bring on
patellofemoral imbalance. This has important
implications for patient rehabilitation. The
malalignment of the patella is secondary to
functional knee valgus and abnormal movements
of the femur. Such abnormalities are (1) femoral
adduction (secondary to weakness of hip
abductors—gluteus medius, upper fibers of gluteus maximus and tensor fascia latae), (2) internal
rotation of the femur secondary to weakness of
B
Clinical and Radiological Assessment …
A
71
B
Fig. 17 Step-down test. During this test, the limb going down only brushes the floor with the heel and then goes back
to full knee extension. A Correct neuromuscular control. B Poor neuromuscular control
the hip external rotators, (3) internal rotation of
the tibia, and (4) tibial abduction secondary to
(5) excessive pronation of the foot. We must note
that a lack of dynamic control of the lower limb
does not depend on the degree of physical
activity of the patient [25]. That is, most physically active adolescents do not necessarily have
better lower limb control [25].
other knee conditions that could simulate patellofemoral pathology.
There are three categories of imaging studies
in patellofemoral pathology: (1) structural
imaging (radiographs, computed tomography
[CT], magnetic resonance imaging [MRI]),
(2) metabolic imaging (technetium scintigraphy),
and (3) a combination of both.
4
4.1 Standard Radiography
Imaging Studies
Imaging studies are the second diagnostic step
and cannot replace the first step. Overlooking this
rule can lead to diagnostic errors that is followed
by failed treatment and iatrogenic morbidity.
A surgical indication should never be based
solely on imaging techniques since the correlation between clinical and image data is not good.
The history and physical examination are the
fundamental elements in the evaluation of the
AKP patient. Nothing can replace the history and
clinical examination. The aim of the imaging
studies is to quantify the pathology and rule out
The majority of patients with patellofemoral pain
will only require standard radiography (standing
anteroposterior view, a true lateral view, and the
low flexion angle axial view [Merchant]). Generally, imaging studies beyond standard radiography are not indicated.
The weight-bearing whole-limb anteroposterior view radiograph allow us to evaluate limb
alignment on the coronal plane (varus, valgus),
and joint space narrowing (Fig. 19). The lateral
view allows one to evaluate the recurvatum and
flexion contracture. It also aids in evaluating the
72
A
V. Sanchis-Alfonso et al.
B
C
Fig. 18 A, B, C Hop down test. B Correct neuromuscular control. C Poor neuromuscular control. Excessive
knee valgus when landing from a drop. Femoral
adduction and tibial abduction are contributing to this
knee position. Knee valgus increases lateral compressive
forces in the PFJ
Fig.
19 Weightbearing
whole-limb
anteroposterior
view
radiograph in a patient
with external tibial torsion. Bilateral varus
alignment and squinting
patella
patellar height. Is there a high-riding patella or
patella alta or a low-riding patella or patella baja?
Moreover, a true lateral X-ray (overlapping of
the posterior borders of the femoral condyles)
allows one to assess trochlear dysplasia (defined
by the crossing sign and quantitatively expressed
by the trochlear bump and the trochlear depth),
and patellar tilt (Fig. 20). Axial views can
demonstrate patellofemoral maltracking (i.e., tilt,
shift, or both) when this happens beyond 30º of
knee flexion, the sulcus angle, loss of joint space,
subchondral sclerosis, and the shape of the
patella. In addition to this, an axial view can
detect secondary clues of earlier dislocation
episodes. For example, medial retinacular calcification is sometimes observed in axial views and
may occur in association with recurrent
subluxation.
Finally, a standard X-ray allows one to rule
out associated and potentially serious bony conditions like tumors or infections. In cases in
Clinical and Radiological Assessment …
Fig. 20 Lateral X-ray. Patellar tilt
which medial patellar instability is suspected, the
stress axial radiography is essential to identifying
and quantifying medial patellar instability [26].
When the patient response to conservative
treatment is not adequate, other imaging techniques such as computed tomography (CT),
magnetic resonance imaging (MRI) and singlephoton
emission
computed
tomography
(SPECT)-CT are indicated.
4.2 Computed Tomography
The CT allows for the measurement of knee
parameters like the tibial tubercle-trochlear
groove (TT-TG) distance, which is widely used
to indicate and plan distal realignment surgeries.
However, it must be noted that the value of the
TT-TG distance is a controversial issue [16]. The
TT-TG distance is influenced by multiple factors
like tibial torsion, knee joint rotation, the slices
selected, and the landmarks of the distal femur
and tibial tuberosity established by the radiologist. However, no pathological distance or index
should be interpreted in isolation. Clinical correlation is requisite in all cases.
Moreover, the CT allows for the evaluation of
torsional abnormalities (Fig. 21). In our clinical
practice, we use the technique described by
Murphy and colleagues in 1987 to measure
femoral torsion [27]. This is the most anatomic,
accurate and reproducible method for evaluating
73
femoral anteversion (high intra- [ICC: 0.95–0.98]
and inter-observer agreement [ICC: 0.93]) [28].
Murphy and colleagues reported that the common
method of running a line along the femoral neck
on a CT image underestimated the actual anteversion by a mean 13º [27]. Moreover, the line that
is used in the most common method, like the axis
of the femoral neck, is not the true axis of the
femoral neck. External tibial torsion is measured
as the angle between the posterior aspect of the
tibial metaphysis and the ankle joint line. Our
normal reference values are femoral anterversion
of 13° for both sexes and external tibial torsion of
21° in males and 27° in females [29, 30].
4.3 Magnetic Resonance Imaging
MRI is useful for evaluating intraosseous edema
(Fig. 22), soft tissue impingement (Figs. 23 and
24), Hoffa fat pad edema (Fig. 25), and patellar
cartilage damage even though this structural
damage may not necessarily be the cause of
AKP. In addition, it also detects possible concomitant lesions. Moreover, MRI often shows
low-grade effusions associated with symptomatic
peripatellar synovitis, which is an underdiagnosed pathological condition of the knee.
4.4 Technetium Scintigraphy
and Single-Photon
Emission Computed
Tomography (SPECT)—CT
Bone scintigraphy using 99mTc hydroxyl ethylene diphosphonate (99mTc-HDP) may be useful
in selected cases. The bone scintigraphy in the
three-dimensional and the conventional CT can
be fused in a single (SPECT/CT) hybrid imaging
procedure which overcomes the limitations of the
CT and SPECT as separate techniques (Fig. 26).
The intensity and distribution of the tracer uptake
correlate with the etiological mechanism and has
been accepted as an effective diagnostic tool in
the orthopedic field [31–34].
If the patella is hot, this suggests that it is the
source of pain, but it does not provide a diagnosis
74
Fig. 21 CT evaluation of femoral anteversion (A, B, C,
D) and external tibial torsion (E). Measurement of femoral
anteversion. Technique described by Murphy (A, B, C).
Draw a circle on the femoral head (B) and another circle
centered in the femoral shaft below the lesser trochanter
(C). Then, draw a line connecting the center of these two
circles (A). This line defines the femoral neck axis on the
transverse plane. Next, draw a line tangent to the posterior
Fig. 22 Intraosseous edema
in a patient with AKP
V. Sanchis-Alfonso et al.
aspect of the femoral condyles (posterior condylar line)
(A). The angle between these two lines represents the
femoral anteversion. (D) Commonly used method
described by Jeanmart (classic method). The line that is
used as the axis of the femoral neck (yellow line) is not
the true axis of the femoral neck connection to the femoral
shaft
Clinical and Radiological Assessment …
A
B
Fig. 23 A Peripatellar synovitis in a patient with AKP
(white arrow). B Quadriceps fat pad impingement
syndrome in a patient with AKP (white arrow). (“Republished with permission of Springer Nature BV, from
A
75
B
Holistic approach to understanding anterior knee pain,
Sanchis-Alfonso V, Knee Surg Sports Traumatol
Arthrosc, 22, 2275–2285, 2014; permission conveyed
through Copyright Clearance Center, Inc.”)
C
Fig. 24 A, B 25-year-old woman with AKP. Morphologic changes of the fat pad observed frequently in
patients with Hoffa’s fat pad impingement: edema localized in the superior and posterior part of the fat pad, deep
infrapatellar bursitis (directly posterior to the distal part of
the patellar tendon, just proximal to its insertion on the
tibial tubercle) and non-visualization of intrahoffatic
clefts. Moreover, we can see a patellar intraosseous
edema. C Normal knee. (“Republished with permission of
Springer Nature BV, from Holistic approach to understanding anterior knee pain, Sanchis-Alfonso V, Knee
Surg Sports Traumatol Arthrosc, 22, 2275–2285, 2014;
permission conveyed through Copyright Clearance Center, Inc.”)
(Figs. 26, 27 and 28). Dye and Boll [35]
observed that about one-half of their patients
with AKP presented increased patellar uptake in
comparison with 4% of the control group. Biopsy
demonstrated that this increased patellar uptake
was secondary to the increased remodelling
activity of the bone. Bone scintigraphy can detect
loss of osseous homeostasis, and often correlates
well with the presence of patellar pain and its
resolution. According to Dye and Boll [35] the
bone scan commonly reverted to normal at an
average time of 6.2 months (range, 3–
14 months), which is interpreted as restoration of
osseous homeostasis. Naslund and colleagues
[36] showed that nearly 50% of AKP patients
show diffuse bone uptake in one or more compartments of the knee (Fig. 28). Not only has a
relationship between hyper-uptake and pain been
demonstrated, but also between pain intensity
and greater uptake (Fig. 28) [37, 38]. Ro and
76
V. Sanchis-Alfonso et al.
and colleagues [40], SPECT bone scintigraphy is
highly sensitive in the diagnosis of patellofemoral abnormalities. For those authors, SPECT
significantly improves the detection of maltracking of the patella and the ensuing increased
lateral patellar compression syndrome. They
conclude that this information could be used to
treat patellofemoral problems more effectively.
SPECT bone scans may be overlaid onto an MRI
or CT (fusion) to correlate bone activity with the
specifics of anatomy (Figs. 26, 27 and 28). It
reveals the metabolic and geographic pattern of
bone homeostasis, which is the normal osseous
metabolic status of the joint.
5
Fig. 25 Post-traumatic Hoffa fat pad edema. (“Republished with permission of Springer Nature BV, from
Holistic approach to understanding anterior knee pain,
Sanchis-Alfonso V, Knee Surg Sports Traumatol
Arthrosc, 22, 2275–2285, 2014; permission conveyed
through Copyright Clearance Center, Inc.”)
colleagues [39] have seen a higher degree of
uptake in the patella in cases with a poorer
response to conservative management.
Scintigraphy may be especially useful in cases
of difficult diagnosis (Fig. 29) and in patients
with injuries related to workers’ compensation
cases in which the physician wishes to establish
objective findings. According to Lorberboym
Take Home Messages
– There is no substitute for a thorough history
and a complete and careful physical examination. The history and physical examination
remain the first step, more than any diagnostic
imaging technique, to come to an accurate
diagnosis of AKP.
– Most orthopedic surgeons only focus on the
knee when they explore a patient with
AKP. This approach is a great mistake
because other important etiological factors
that are at a distance from the knee may be
responsible for the pain. We should examine
the entire lower extremity.
– Imaging studies are a second step and can
never replace the former.
Fig. 26 SPECT-CT overcomes the limitations of the CT and SPECT as separate techniques. It reveals the metabolic
and geographic pattern of bone homeostasis. That is, it correlates bone activity with the specifics of anatomy
Clinical and Radiological Assessment …
A
B
77
C
Fig. 27 SPECT/CT in an AKP patient with right femoral anteversion and external tibial torsion. A Fused SPECT/CT
MIP, B, C fused axials. The scintigraphic uptake is markedly high in the patella’s articular face
Fig. 28 SPECT-CT in a symptomatic patient with
bilateral AKP with much more pain in the left knee.
(Republished with permission of AME Publishing Company. From Sanchis-Alfonso V, et al. Evaluation of
anterior knee pain patient: clinical and radiological
assessment including psychological factors. Ann Joint,
3:26, 2018; permission conveyed through Copyright
Clearance Center, Inc.)
78
V. Sanchis-Alfonso et al.
Fig. 29 Value of SPECT-CT in the differential diagnosis
of knee pain. This patient came to our office with severe
AKP. In this case, the patient presented a type I
epiphysiolysis of the distal femoral physis that was
responsible for pain (Courtesy of A. Darder, MD).
(Republished with permission of AME Publishing
Company. From Sanchis-Alfonso V, et al. Evaluation of
anterior knee pain patient: clinical and radiological
assessment including psychological factors. Ann Joint,
3:26, 2018; permission conveyed through Copyright
Clearance Center, Inc.)
– Surgical indications should not be based only
on methods of image diagnosis as there is a
poor correlation between the clinical and
imaging data.
patellofemoral pain: which are reliable and valid?
Arch Phys Med Rehabil. 2004;85:815–22.
Bouhassira D, Attal N, Alchaar H, et al. Comparison
of pain syndromes associated with nervous or
somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain.
2005;114(1–2):29–36.
Robertson CJ, Hurley M, Jones F. People’s beliefs
about the meaning of crepitus in patellofemoral pain
and the impact of these beliefs on their behaviour: a
qualitative study. Musculoskelet Sci Pract.
2017;28:59–64.
Domenech J, Sanchis-Alfonso V, Lopez L, et al.
Influence of kinesiophobia and catastrophizing on
pain and disability in anterior knee pain patients.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(7):1562–8.
Wride J, Bannigan K. Investigating the prevalence of
anxiety and depression in people living with
patellofemoral pain in the UK: the Dep-Pf study.
Scand J Pain. 2019;24;19(2):375–382.
4.
5.
References
1. Crossley KM, Callaghan MJ, van Linschoten R.
Patellofemoral pain. Br J Sports Med. 2016;50
(4):247–50.
2. Post WR. History and physical examination. In:
Fulkerson JP (ed) Disorders of the patellofemoral
joint. 4th edition. Lippincott Williams & Wilkins
Philadelphia, 2004; pp 43–75.
3. Crossley KM, Bennell KL, Cowan SM, et al.
Analysis of outcome measures for persons with
6.
7.
Clinical and Radiological Assessment …
8. McManus S, Bebbington P, Jenkins R, Brugha T,
editors. Mental health and well-being in England:
Adult psychiatric morbidity survey 2014. Leeds:
NHS Digital, 2016.
9. Sigmund KJ, Hoeger Bement MK, Earl-Boehm JE.
Exploring the pain in patellofemoral pain: a systematic
review and meta-analysis examining signs of central
sensitization. J Athl Train. 2021;56(8):887–901.
10. Fulkerson JP. The etiology of patellofemoral pain in
young, active patients: a prospective study. Clin
Orthop. 1983;179:129–33.
11. Ficat P, Ficat C, Bailleux A. [External hypertension
syndrome of the patella. Its significance in the
recognition of arthrosis] Rev Chir Orthop Reparatrice
Appar. 1975;Mot 61:39–59.
12. Hejgaard N, Arnoldi CC. Osteotomy of the patella in
the patellofemoral pain syndrome. The significance
of increased intraosseous pressure during sustained
knee flexion. Int Orthop. 1987;8:189–194.
13. Allen GM, Tauro PG, Ostlere SJ. Proximal patellar
tendinosis and abnormalities of patellar tracking.
Skeletal Radiol. 1999;28:220–3.
14. Rathleff MS, Roos EM, Olesen JL, et al. Lower
mechanical pressure pain thresholds in female adolescents with patellofemoral pain syndrome. J Orthop
Sports Phys Ther. 2013;43(6):414–21.
15. Daniel D, Akeson W, O’Connor J. Knee Ligaments.
Structure, Function, Injury and Repair. Raven Press,
1990.
16. Sanchis-Alfonso V, Coloma-Saiz J, Herrero-Herrero
M, et al. Evaluation of anterior knee pain patient:
clinical and radiological assessment including psychological factors. Ann Joint. 2018;3:26.
17. Sanchis-Alfonso V, McConnell J, Monllau JC, et al.
Diagnosis and treatment of anterior knee pain.
JISAKOS, 2016. https://doi.org/10.1136/jisakos2015-000033.
18. Piva SR, Goodnite EA, Childs JD. Strength around
the hip and flexibility of soft tissues in individuals
with and without patellofemoral pain syndrome.
J Orthop Sports Phys Ther. 2005;35(12):793–801.
19. Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic
risk factors for the development of anterior knee pain
in an athletic population. A 2-year prospective study.
Am J Sports Med 2000;28(4):480–489.
20. Rathleff MS, Rathleff CR, Crossley KM, et al. Is hip
strength a risk factor for patellofemoral pain? A
systematic review and meta-analysis. Br J Sports
Med. 2014;48:1088.
21. Giles LS, Webster KE, McClelland JA, et al. Does
quadriceps atrophy exist in individuals with patellofemoral pain? A systematic literature review with
meta-analysis. J Orthop Sports Phys Ther.
2013;43:766–76.
22. Sanchis-Alfonso V, Tey M, Monllau JC. A Novel
Association between Femoroacetabular Impingement
79
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
and Anterior Knee Pain. Pain Res Treat. 2015;2015:
937431.
Vallotton J, Echeverri S. Clinical examination of the
patellofemoral patient. In: Zaffagnini S, Dejour D,
Arendt EA, editors. Patellofemoral Pain, Instability,
and Arthritis. Berlin Heidelberg: Springer; 2010.
p. 41–9.
Rabin A, Portnoy S, Kozol Z. The association of
ankle dorsiflexion range of motion with hip and knee
kinematics during the lateral step-down test. J Orthop
Sports Phys Ther. 2016;46:1002–9.
Herrero-Herrero M, García-Massó X, MartínezCorralo C, et al. Relationship between the practices
of physical activity and quality of movement in
adolescents: a screening tool using self-organizing
maps. Phys Sportsmed. 2017;45(3):271–9.
Teitge RA, Faerber WW, Des Madryl P. Stress
radiographs of the patellofemoral joint. J Bone Joint
Surg. 1996;78-A:193–203.
Murphy SB, Simon SR, Kijewski PK, et al. Femoral
anteversion. J Bone Joint Surg Am. 1987;69
(8):1169–76.
Kaiser P, Attal R, Kammerer M, et al. Significant
differences in femoral torsion values depending on
the CT measurement technique. Arch Orthop Trauma
Surg. 2016;136(9):1259–64.
Yoshioka Y, Cooke TD. Femoral anteversion:
assessment based on function axes. J Orthop Res.
1987;5(1):86–91.
Yoshioka Y, Siu DW, Scudamore RA, et al. Tibial
anatomy and functional axes. J Orthop Res. 1989;7
(1):132–7.
Mucha A, Dordevic M, Testa EA, et al. Assessment
of the loading history of patients after high tibial
osteotomy using SPECT/CT–a new diagnostic tool
and algorithm. J Orthop Surg Res. 2013;8:46.
Hirschmann MT, Iranpour F, Davda K, et al.
Combined single-photon emission computerized
tomography and conventional computerized tomography (SPECT/CT): clinical value for the knee
surgeons? Knee Surg Sports Traumatol Arthrosc.
2010;18:341–5.
Sim JA, Na YG, Lee BK, et al. Alignment changes
after open-wedge high tibial osteotomy result in
offloading in the patellofemoral joint: a SPECT/CT
analysis. Knee Surg Sports Traumatol Arthrosc.
2020. https://doi.org/10.1007/s00167-020-06115-0.
Braun M, Cachovan M, Kaul F, et al. Accuracy
comparison of various quantitative [99mTc]Tc-DPD
SPECT/CT reconstruction techniques in patients with
symptomatic hip and knee joint prostheses. EJNMMI
Res.
2021.https://doi.org/10.1186/s13550-02100794-7
Dye SF, Boll DA. Radionuclide imaging of the
patellofemoral joint in young adults with anterior
knee pain. Orthop Clin North Am. 1986;17:249–62.
80
36. Näslund JE, Odenbring S, Näslund UB, et al.
Diffusely increased bone scintigraphic uptake in
patellofemoral pain syndrome. Br J Sports Med.
2005;39(3):162–5.
37. Draper CE, Fredericson M, Gold GE, et al. Patients
with patellofemoral pain exhibit elevated bone
metabolic activity at the patellofemoral joint.
J Orthop Res. 2012;30(2):209–13.
38. Dye SF. The pathophysiology of patellofemoral pain:
a tissue homeostasis perspective. Clin Orthop Relat
Res. 2005;436:100–10.
V. Sanchis-Alfonso et al.
39. Ro DH, Lee HY, Chang CB, et al. Value of SPECTCT imaging for middle-aged patients with chronic
anterior knee pain. BMC Musculoskelet Disord.
2015;16:169.
40. Lorberboym M, Ami DB, Zin D, et al. Incremental
diagnostic value of 99mTc methylene diphosphonate
bone SPECT in patients with patellofemoral pain
disorders. Nucl Med Commun. 2003;24:403–10.
Evaluation of Psychological Factors
Affecting Anterior Knee Pain
Patients: The Implications
for Clinicians Who Treat These
Patients
Vicente Sanchis-Alfonso, Julio Doménech-Fernández,
Benjamin E. Smith, and James Selfe
1
Introduction
Anterior knee pain (AKP) is one of the most
common reasons why physically active people
consult an orthopedic surgeon specializing in the
knee. It can be challenging to manage. Despite its
high prevalence and the abundance of research
the etiopathogenesis of AKP is not well known.
Therefore, there are many myths surrounding this
condition, false collective beliefs that are transmitted from generation to generation. One of
these myths is that the AKP patient is a person
with peculiar psychological traits that are
responsible for the genesis of pain. It could not
be further from the truth.
Many AKP patients have insignificant clinical
and radiological findings. However, they have
severe pain and an important disability. Moreover, some AKP patients have allodynia (pain in
V. Sanchis-Alfonso (&) J. Doménech-Fernández
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
B. E. Smith
Physiotherapy Outpatients, University Hospitals of
Derby and Burton NHS Foundation Trust, Derby,
UK
J. Selfe
Department of Health Professions, Faculty of Health
and Education, Manchester Metropolitan University,
Manchester, UK
the presence of a non-noxious stimulus), primary
hyperalgesia, (pain hypersensitivity in the knee)
or secondary hyperalgesia (pain hypersensitivity
in uninjured tissues beyond the affected area).
We can thus understand that many orthopedic
surgeons, who do not know this condition well,
may think that the main problem is psychological. Furthermore, the absence of structural
pathology leads to cataloging these patients as
somatizers in many cases even though there is no
evidence to justify this.
It is important to note that acute pain does not
have anything to do with chronic pain. Chronic
pain can have significant psychological effects on
the sufferers, and we must note that AKP is a
paradigm of chronic pain. Chronic pain is a
multidimensional experience with sensitive,
cognitive and affective domains [1]. Functional
Magnetic Resonance Imaging (MRI) has identified many pain centres in the brain that work
together as a network. This pain neuromatrix can
account for the multidimensional experience of
pain [2]. Interestingly, Damasio and colleagues
[3] observed an overlap between the cerebral
activity areas related to chronic pain and those
related to cognition and emotion. This finding
suggests that chronic pain, cognition, and emotion are interrelated [3]. Patients with AKP have
a high incidence of anxiety, depression, kinesiophobia (the fear that physical activity will
cause more injury or a re-injury and subsequent
pain) and catastrophizing (the belief that pain
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_6
81
82
V. Sanchis-Alfonso et al.
will worsen and cannot be relieved) [4]. However, ascribing AKP only to psychological
problems is a crude excuse to hide our ignorance
as to the cause of pain in these patients. What it is
true is that psychological disorders are the result
of the pain severity but not the cause of the pain
and disability. We have all seen AKP patients
that have been operated on several times with
completely inappropriate surgical indications and
that were obviously quite affected with painrelated fear.
AKP is usually considered a biomechanical
paradigm hence the literature is dominated by
biomechanical studies that overlook social and
psychological factors. Until recently, the role of
psychological factors involved in AKP have
received little attention. Even so, psychological
factors are increasingly recognized for their role
in chronic pain conditions. Most of the papers in
which AKP is analyzed from a psychological
perspective (the human side of the patellofemoral
pain) have been published in the last 5 years. The
objective of this chapter in to analyze the psychological factors affecting AKP patients in
depth. Moreover, we are going to review the
experience of living with AKP. This chapter is
about expanding our horizons, that is, the options
for treating AKP patients. What this chapter is
not about is negating any other existing paradigm
(the homeostasis paradigm and structural/
anatomic/biomechanical paradigm). From a
biopsychosocial perspective, psychological factors are not an isolated cause of pain, but rather
interact with biological and structural factors.
The key message of this chapter is that psychological factors are modulators of pain and disability. Throughout this chapter, we will work to
justify this statement.
a direct and sequential relation between tissue
damage and pain, and between pain and disability. Therefore, the doctor’s task would be to
repair the damaged tissue and eradicate the pain,
making the functional impairment and disability
disappear. This model has worked well for some
conditions (e.g., meniscal tears). However, for
some conditions that develop with chronic pain
such as AKP, which is a paradigm of chronic
pain, this classic biomedical model is not enough
to understand the pathophysiology of the pain
and determine adequate treatment. Regardless of
how intense the pain is, patients with AKP show
different degrees of disability in their everyday
life. Furthermore, no significant correlation
between structural alterations of the patellofemoral joint and disability have been observed. In
fact, some cases with important anatomic alterations (patellar subluxation, patellar tilt, pathologic external tibial torsion, and severe patellar
and/or trochlear chondropathy) are painless [5–
8]. Therefore, not only must we consider anatomic, biological and biomechanical factors to
understand AKP, but also the psychological and
social ones. This approach was proposed by the
American pathologist and psychiatrist George
Engel. In 1977, the Journal “Science” published
his paper “The need for a new medical model: A
challenge for biomedicine”, introducing the term
“Biopsychosocial Model” (Fig. 1) [9]. This
model allows for the development of more adequate therapeutic strategies than the biomedical
model. However, very few studies currently
focus on the patient with AKP from a psychological and social perspective in comparison with
other conditions such as low back pain (LBP),
knee osteoarthritis, fibromyalgia or rheumatoid
arthritis.
2
3
Biopsychosocial Model
in Anterior Knee Pain—An
Alternative to the Classic
Biomedical Disease Model
Currently, the biomedical disease model is the
dominant one used by physicians in the diagnosis
and treatment of diseases. This model establishes
Fear-Avoidance Model in Anterior
Knee Pain. Kinesiophobia
To try to explain how and why some individuals
with musculoskeletal pain develop chronic pain,
Lethem and colleagues [11] introduced the socalled “fear-avoidance” model in 1983 (Fig. 2).
The central concept of their model is fear of pain.
Evaluation of Psychological Factors …
83
Fig. 1 The Biopsychosocial
model of chronic pain and
disability. International
Classification of Functioning
Disability and Health, World
Health Organization
(Modified from Waddell [10])
“Confrontation” and “avoidance” are the two
opposite responses to this fear. The former
response leads to a reduction of fear over time
with the patient being able to cope with it satisfactorily, continue their usual activities and
achieve full recovery. On the other hand, patients
who interpret pain in an exaggerated or catastrophic way, develop fear of pain and associated
behaviors like hypervigilance and avoidance in
search of security. Although these behaviors can
be adaptive when coping with acute pain, they
can worsen the patient’s condition if the pain is
chronic, because they favor disuse, depression
and increased disability. The fear-avoidance
model is framed within the biopsychosocial disease model, the patient being trapped in a vicious
circle of pain, disability and suffering (Fig. 2).
Asmudson and colleagues [12] added the pain
anxiety component to this model as an aggravating factor in the avoidance behavior generating circuit (Fig. 2). Avoidance behavior not only
includes limiting one’s movements, but also
avoiding social interactions and recreational
activities, which increase the pain and suffering
in these patients. Crombez and colleagues [13]
have even stated that “the fear of pain is more
disabling that pain itself”.
In many studies, fear and avoidance behaviors
have been strongly associated with the disability
present in patients with low back pain
(LBP) [15–18]. Also, in LBP longitudinal studies, changes in fear-avoidance beliefs were good
predictors of disability [19–24]. The fear of pain
and the catastrophic vision of pain also occur in
pain free people. Therefore, these beliefs can
play an important role in the development of new
episodes of pain. In studies performed on subjects without LBP [25–28], it was observed that
fear of pain increased the risk of suffering episodes of LBP, and so the risk of disability was
increased. Picavet and colleagues [29], in 2002,
studied whether pain catastrophizing and fear of
movement/(re)injury (kinesiophobia) are important in the etiology of chronic LBP and the
associated disability. For patients with LBP at
baseline, a high level of catastrophizing predicted
chronic LBP, in particular severe LBP and LBP
with disability. Moreover, a high level of kinesiophobia showed similar associations. For those
subjects without LBP at baseline, a high level of
catastrophizing or kinesiophobia predicted LBP
with disability during follow-up. They concluded
that catastrophizing and kinesiophobia were
good predictors for the chronification of pain and
disability. In another study, Carragee and colleagues [19] performed a five-year follow-up
study on a group of 100 subjects with mild LBP
by means of MRI and a discography, measuring
their fear-avoidance beliefs with a FABQ (FearAvoidance Beliefs Questionnaire). Surprisingly,
84
V. Sanchis-Alfonso et al.
Fig. 2 The fear-avoidance model of chronic pain based on the fear-avoidance model of Vlaeyen and Linton [14] and
the fear-anxiety-avoidance model of Asmudson and colleagues [12]
the severe LBP cases and disabilities had no
relation with structural anomalies found in the
MRI or discography. It was the presence of fear
and avoidance behaviors that turned out to be the
strongest predictor in LBP and disability.
AKP shares with non-specific LBP a low
correlation between the symptoms and structural
anomalies found in imaging studies. Moreover,
both conditions tend to become chronic and
cause disability. The World Health Organization
defines disability as “a limitation of function that
compromises an individual’s ability to perform
an activity within the range considered normal”.
AKP patients show different degrees of disability
in their everyday life, regardless of how intense
the pain is. In some cases, there is severe pain
and little disability. In other cases, the pain is
severe and the disability, too. Piva and colleagues [30] studied whether changes in fearavoidance behaviors (measured with the FABQ
modified for the knee) influenced disability in a
group of patients with AKP undergoing conventional physical therapy treatment. They found
that those patients who lowered their levels of
fear and avoidance of physical activity and work
saw decreased levels of pain and disability at the
end of the treatment. Jensen and colleagues [31]
studied a group of AKP patients by measuring
the degree of pain with the VAS scale and disability with the Cincinnati Knee Rating System
(CKRS) questionnaire and found a weak correlation between the level of pain and disability,
one that was not statistically significant. Therefore, we can reason that AKP causes pain on one
hand and disability on the other, being both
independent dimensions with a poor correlation.
Domenech and colleagues [4] evaluated the
ideas of fear and avoidance with the Tampa
Kinesiophobia Scale (TSK) and have found a
moderate statistically significant correlation with
the patient’s referred disability measured with the
Lysholm Score (Table 1) [4]. The greater the fear
and avoidance beliefs, the greater the disability
perceived by the patient. It is interesting to
highlight that the correlation between kinesiophobia and disability was higher than the one
between pain and disability (Table 1) [4]. Obviously, not all the AKP patients have
Evaluation of Psychological Factors …
Table 1 Spearman
correlation between pain,
disability and the
psychological variables.
(“Republished with
permission of Springer
Nature BV, from Influence
of kinesiophobia and
catastrophizing on pain and
disability in anterior knee
pain patients, Domenech J
et al., Knee Surg Sports
Traumatol Arthrosc, 21,
1562–1568, 2013;
permission conveyed
through Copyright
Clearance Center, Inc.”)
85
Pain (VAS)
Pain (VAS)
a
Disability (Lysholm)
0.49**
Coping Strategies (CSQ)
0.21
−0.01
Reinterpreting pain sensation
0.18
−0.16
Ignoring pain sensations
0.08
0.06
Coping self-statements
0.08
−0.01
Praying or hoping
0.35*
−0.38**
Catastrophizing
0.48**
−0.59**
Increasing activity level
0.01
Anxiety (HAD)
0.46**
0.57**
Depression (HAD)
0.44**
−0.61**
Kinesiophobia (TSK)
0.26*
−0.53**
Catastrophizing (PCS)
0.43**
−0.53**
Diverting attention
0.15
Subscale PCS rumination
0.39**
−0.49**
Subscale PCS magnification
0.41**
−0.47**
Subscale PCS hopelessness
0.46**
−0.56**
VAS (Visual Analogue Scale), CSQ (Coping Strategies Questionnaire), HAD (Hospital
Anxiety and Depression inventory), TSK (Tampa Scale for Kinesiophobia), and PCS
(Pain Catastrophizing Scale)
* p < 0.01; ** p < 0.001
a
Correlation between pain and disability was performed after deleting the subscale pain
of the Lysholm questionnaire to avoid colinearity
kinesiophobia. However, its presence is very
important because it has clinical relevance. If
kinesiophobia is present, then the levels of the
pain and the disability soar (Table 2). In many
cases, AKP patients also exhibit catastrophizing.
Domenech and colleagues [4] evaluated catastrophizing through the Catastrophizing Coping
Scale Questionnaire (CSQ) and through the Pain
Catastrophizing Scale (PCS) and found a moderate statistically significant correlation with the
patient’s disability (Table 1). When the perception of pain is more catastrophic, the patients
perceive greater disability. Moreover, pain and
disability show a moderate but significant correlation even though it is lower than that
observed with catastrophizing or kinesiophobia
[4]. Therefore, there are other factors besides
pain that contribute to disability. It has been
shown that what is mainly responsible for disability is not the pain, but the associated psychological factors. Pain explains only 24% of the
variance in disability whereas catastrophizing
and depression account for 56% of the variance
in disability [4]. There are other factors besides
pain that contribute to disability. It seems plausible that psychological factors contribute to it.
There are complex cultural beliefs about many
aspects of health including the potential iatrogenic effect of healthcare itself. The pain experience is a good example where there is great
cultural complexity for example the fearavoidance model of pain cautions against exercise and activity, which in an acute injury state
may be helpful and common sense but in a
chronic pain state has a negative impact on outcomes [32]. Crepitus is another example where
painless noises from the knee can create negative
emotions, inaccurate etiological beliefs and
finally leads to fear-avoidance behavior and
lower functional performance [33].
Maclachlan and colleagues [34] showed that
there were no significant differences in TSK,
PCS or HADS between less-severe pain patients
and controls. However, more severe AKP
86
V. Sanchis-Alfonso et al.
Table 2 T test comparison of mean values in pain and disability between patients with high or low levels of anxiety,
depression, kinesiophobia and catastrophizing. (“Republished with permission of Springer Nature BV, from Influence
of kinesiophobia and catastrophizing on pain and disability in anterior knee pain patients, Domenech J et al., Knee Surg
Sports Traumatol Arthrosc, 21, 1562–1568, 2013; permission conveyed through Copyright Clearance Center, Inc.”)
Pain
Disability
Anxiety
High level ( 11) n = 29
8.2 (1.1)
Low level (<11) n = 68
6.9 (1.7)
P < 0.0001
30.3 (17.0)
P < 0.0001
53.8 (18.5)
Depression
High level ( 11) n = 16
8.3 (1.4)
Low level (<11) n = 81
6.8 (1.7)
P = 0.009
23.0 (11.3)
P < 0.0001
51.1 (19.4)
Kinesiophobia
High level ( 40) n = 80
7.2 (1.6)
Low level (<40) n = 17
5.8 (2.2)
P = 0.009
44.7 (20.0)
P = 0.002
61.6 (16.6)
Catastrophizing
High level ( 24) n = 35
7.7 (1.5)
Low level (<24) n = 62
6.5 (1.8)
P = 0.001
patients had significantly higher HADS-D and
PCS scores than the controls. Moreover, the
more severe AKP group also had significantly
worse scores for the TSK, HADS-D and PCS
than the less severe AKP group [34]. Among all
the factors, the greatest difference in prevalence
was observed for kinesiophobia, which was 27%
more prevalent in the more-severe AKP group
[34]. This means kinesiophobia seems to be an
important factor in the experience of AKP,
because it was elevated in the AKP group, significantly differed between the AKP sub-groups
(more-severe vs. less-severe) and contributed to
explaining disability [34]. Curiously, Maclachlan
and colleagues [35] emphasize that clinicians
should not assume that kinesiophobia is always
linked to avoidance behaviors and disability.
Therefore, reported high levels of activity should
not preclude the evaluation of kinesiophobia.
Selhorst and colleagues [36] found a significant and negative association between psychological impairment in adolescents with AKP and
the self-reported function, being the fearavoidance beliefs the most associated variable.
Pain related fear and non pain catastrophizing
were significantly associated with some aspects
35.1 (16.2)
P < 0.0001
54.8 (19.1)
of objective function such as quadriceps strength,
hip abduction and single leg hop distance.
4
Relationship Between Cognitions
and Anterior Knee Pain.
Catastrophizing
4.1 Coping Strategies
Understanding individual pain coping strategies
is one of the most important aspects in comprehending the consequences of chronic pain on
patient health. Patients see their pain as a source
of stress for which they develop cognitive and
behavioral strategies that are constantly changing
to minimize the impact of pain and disability. On
certain occasions, these coping strategies are
positive, improving tolerance to reduce the perception of pain and disability. Then, on other
occasions, these coping strategies are maladaptative and worsen the clinical course of the
disease.
The Coping Strategies Questionnaire
(CSQ) [37] measures the frequency with which
patients use different coping strategies. It is
Evaluation of Psychological Factors …
comprised of seven subscales, six cognitive
(distraction, reinterpreting pain sensation, ignoring pain sensation, coping self-assertion, prayer or
hope, and catastrophizing), and a behavioral subscale (increase in the activity level and the
behaviors that reduce the feeling of pain). Thomeé
and colleagues [38] studied the coping strategies
in a group of 50 Swedish patients with chronic
AKP using the CSQ and found that the scores in
the different coping subscales where in accordance
with the results published in other patients with
chronic pain. The most commonly used strategy
was the coping self-statements and the least used
was reinterpreting pain sensations [38].
Domenech and colleagues [4], found similar
results relative to the frequency with which the
different coping strategies are used, regardless of
the cultural differences between people in different
studies. The most used strategies were the increase
in behavioral activities and the coping selfstatements [4]. The least used was reinterpreting
pain sensations [4]. Domenech and colleagues [4]
also analyzed the relationship between the pain
coping subscales and pain and disability. Both
subscales, the catastrophic vision and prayer-hope,
showed significant correlation with the patient’s
disability [4]. Additionally, all of the coping
strategies except the prayer-hope one had a significant relationship with the hospital anxiety and
depression (HAD) scale [4]. However, none of the
coping strategies showed a significant relationship
with the degree of pain [4].
4.2 The Role of Catastrophizing
Catastrophizing is the exaggerated interpretation
of the negative consequences of pain. It is a
multidimensional construct with elements of
magnification (heightened perception of pain),
rumination (excessive focus on pain), and helplessness (beliefs that the control of pain is beyond
one’s ability). AKP patients have a high prevalence of catastrophizing. Obviously, not all AKP
87
patients catastrophize. However, its presence is
very important because it has clinical relevance. If
catastrophizing is present, then the levels of pain
and disability increase dramatically [4].
Catastrophizing plays a key role in pain
modulation. However, the exact mechanisms by
which catastrophizing affects the experience of
pain is not well known. Goodin and colleagues
[39] have shown that the heightened pain
reported by individuals that exhibit extreme pain
catastrophizing may be related to a disruption in
the endogenous pain-inhibitory modulation processes of pain. In a study using functional MRI in
patients with chronic pain, it was seen that
catastrophizing was not only associated with a
greater degree of activity in the brain’s pain
processing areas but also in the cortical areas
related to attention, the anticipation of pain, and
emotional aspects of pain [40]. In healthy subjects in whom pain was caused by heat, higher
levels of catastrophizing were related to a greater
degree of pain as well as a longer duration of the
heat related pain [41]. This suggests that catastrophizing plays a facilitating role in the pain
perception process.
Catastrophizing in chronic pain and disability
has been widely studied in musculoskeletal
conditions such as rheumatoid arthritis, knee
osteoarthritis, or LBP [42–47]. There is growing
evidence that the catastrophic vision of pain is
related not only to the pain patients report but
also to other aspects that influence the course of
the illness. Some studies show that patients with
musculoskeletal pain with these ideas have a
greater degree of disability [48], increased use of
health resources [49] and medication [50, 51],
and a worse recovery after knee arthroplasty
surgery [52]. Many studies confirm a strong
association between catastrophizing and the
patient’s disability in several conditions with
chronic pain, mainly in musculoskeletal pain
[53–56]. Besides the association with disability,
catastrophizing has been related to the degree of
pain. Patients with significant catastrophizing
88
reported greater degrees of pain both in acute and
chronic pain conditions [49, 54, 56, 57].
Thomeé and colleagues [58] studied pain
coping strategies in a group of AKP patients. The
catastrophizing subscale showed a very high
score in the patients with AKP, more than double
the score found in rheumatoid arthritis patients.
Domenech and colleagues [4] studied the
relationship between catastrophizing, measured
on the catastrophizing subscale of the CSQ or by
means of the PCS, and disability in a group of
AKP patients. A statistically significant correlation was found between the disability, measured
using the Lysholm scale score, and the score
obtained from the PCS questionnaire [4]. However, there was a poorer correlation with the
degree of pain [4]. Catastrophizing was also
found to be a widely used coping strategy in
chronic AKP patients [4].
There is controversy about whether catastrophizing is a stable construct, like a personality
trait that predisposes a patient with AKP to the
chronification of pain and disability, or whether it
is a dynamic attribute that can be modified. If the
first premise is correct, then catastrophizing
could be an obstacle to recovery. We believe that
the second premise is correct since we have
observed that catastrophizing is reduced when
patients feel a reduction in pain after a classic
biomedical treatment (physical therapy) [59].
This finding is clinically important because it
contradicts the common belief that AKP patients
are patients with pre-existing psychological
problems that are responsible for pain. Another
relevant finding is that a change in catastrophizing is the strongest predictor of changes in both
pain and disability after treatment (Table 3) [59].
A reduction in catastrophizing explains by itself
the 48% of the variance of the changes in the
degree of pain (Table 4) [59]. The reduction of
catastrophizing and anxiety explains 56% of the
variance in disability (Table 4) [59].
What is very important is that catastrophizing
is a cognition and therefore it is a modifiable
factor. Therefore, cognitive-behavioral therapy
(CBT) focused on reducing fear-avoidance
V. Sanchis-Alfonso et al.
behaviors and the catastrophizing may influence
the clinical state of AKP patients in a positive
manner.
5
Psychological Involvement
in AKP Patients. Depression
and Anxiety
As measured by HADS over half of people living
with AKP experience anxiety and/or depressive
symptoms. The levels of anxiety and depressive
symptoms in AKP patients are much higher than
those found in the general population (anxiety
symptoms: 49.5% vs. 5.9–7.8%; depressive
symptoms 20.8 vs. 3.3–7.8%) [60, 61]. Nevertheless, these figures must be viewed with caution
due to the potential for the HADS to overestimate
anxiety and depression [62]. High levels of anxiety and depression are found in several musculoskeletal conditions. In a systematic review,
Stubbs and colleagues [63] found figures of
around 20% for both anxiety and depression in
osteoarthritis. Similar figures have also been
reported in low back pain [64]. This suggests that
the figures in AKP are realistic, despite concerns
regarding the accuracy of the HADS as a measurement tool. We have found similar rates of
anxiety (30%) and depression (16%) in people
with AKP (n = 97) in a tertiary setting [4].
Obviously, not all AKP patients have painrelated fear. However, the presence of painrelated fear is very important because it has
clinical relevance. For example, if depression is
present, then the levels of the pain and disability
soar [4]. The same goes for anxiety [4]. If there is
psychological involvement, disability and pain
are greater (Fig. 3) [4].
5.1 Relationship Between Anxiety
and Anterior Knee Pain
Anxiety and stress are normal emotional reactions in certain situations. Both anxiety and stress
in a mild or moderate form are healthy and even
p < 0.001
−0.59**
−0.43**
Disability
posttreatment
**
0.54**
0.41**
Pain posttreatment
p < 0.05;
−0.59**
−0.49**
Disability
pretreatment
*
0.30*
0.39**
Depression
Pain pretreatment
Anxiety
0.24
−0.03
−0.04
−0.12
0.28
−0.25
0.44**
−0.21
−0.02
0.12
Ignoring
pain
Reinterpreting
pain
0.19
0.02
Diverting
attention
0.02
0.15
0.25
−0.19
Coping
selfstatements
0.08
0.01
−0.38**
0.40**
Praying
or
hoping
Pain Coping Strategies (CSQ)
−0.50**
0.50**
−0.62**
0.48**
Catastrophizing
0.30*
−0.26
0.33*
−0.41**
Increasing
activity
level
−0.41**
0.35*
−0.55**
0.35*
Kinesiophobia
−0.57**
0.59**
−0.49**
0.47**
Catastrophizing
Table 3 Spearman correlation coefficients of pain intensity and disability level with the psychometric variables before and after treatment. (“Republished with permission of
Springer Nature BV, from Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in patients with anterior knee pain,
Domenech J et al., Knee Surg Sports Traumatol Arthrosc, 22, 2295–2300, 2014; permission conveyed through Copyright Clearance Center, Inc.”)
Evaluation of Psychological Factors …
89
90
V. Sanchis-Alfonso et al.
Table 4 Hierarchical regression explaining pain and disability. (“Republished with permission of Springer Nature BV,
from Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in
patients with anterior knee pain, Domenech J. et al., Knee Surg Sports Traumatol Arthrosc, 22, 2295–2300, 2014;
permission conveyed through Copyright Clearance Center, Inc.”)
Explanatory variables (Change scores)
R2
Corrected R2
Model predicting pain intensity
Catastrophizing (PCS)
0.49
0.48
0.13 (0.09, 0.17)
0.70
0.001
Model predicting disability
Catastrophizing (PCS)
Anxiety
0.58
0.56
–0.92 (–1.42, –0.41)
–2.26 (–3.85, –0.67)
–0.47
–0.37
0.001
0.006
B (95% IC)
Beta
P
Fig. 3 If there is psychological involvement, disability and pain are greater
beneficial because they motivate a person to
prepare a response, either to remain vigilant or to
serve as a warning when in danger. However, it
occasionally becomes dysfunctional when anxiety levels are too high or it lasts too long,
becoming pathological. Anxiety expresses itself
differently in patients, sometimes in emotional
and cognitive manners (tension, fear, edginess,
discomfort, nervousness), behavioral or motor
aspects (immobility, avoidance, restlessness).
Anxiety is also accompanied by vegetative
reactions such as perspiration, palpitations, dry
mouth, shaking, dizziness or nausea on occasion.
Patients with chronic pain perceive pain as a
situation that generates prolonged stress. The
presence of anxiety influences the symptoms in
these patients bidirectionally. High degrees of pain
can sometimes predict anxiety symptoms [65] and
conversely, anxiety increases the painful
experience [66]. One of the most studied mechanisms of the effects of maladaptative anxiety in
chronic pain patients is a tendency towards
hypervigilance and catastrophization [12]. These
tendencies amplify the perception of pain and cause
behaviors that lead to increased disability [67].
Clark and colleagues [68] performed a RCT to
determine the efficacy of physiotherapy for
AKP. The four treatment groups were: (1) exercise, taping and education; (2) taping and education; (3) exercise and education; and (4) education
alone. They found that 27% of patients with AKP
showed anxiety symptoms measured with the
HAD questionnaire. After receiving treatment,
those symptoms improved. Thomee and colleagues [58] also found high levels of anxiety in a
group of patients with AKP using the STAI
questionnaire (State Trait Anxiety Inventory),
finding similar scores to those published for
Evaluation of Psychological Factors …
rheumatoid arthritis. Carlsson and colleagues [69]
measured distress/anxiety using the Rorschach
test in patients with AKP and in a control group of
mainly physical therapy students and found that
patients had high anxiety levels but with no difference from the control group. That may have
been because the students also have a high level of
distress. Piva and colleagues [30] studied a group
of AKP patients with at least 4 weeks pain and an
average numeric pain rating scale score of 3.6.
They found a correlation between disability and
level of anxiety measured with the Beck questionnaire, suggesting that patients with more limitations in physical function had higher anxiety
levels. Domenech and colleagues [4] have shown
that if anxiety is present in chronic AKP patients
with important symptoms, then levels of pain and
disability increase (Table 2).
5.2 Relationship Between Depression
and Anterior Knee Pain
The importance of this association lies in the
fact that both conditions, chronic pain and
depression, can interact to intensify their effects.
A meta-analysis of 83 studies has shown that the
severity of depression is related not only to the
presence of chronic pain, but also to its duration, the degree of pain and the number of
painful areas [70]. Regarding its influence on
disability, several studies show that depression
reduces the functional capacity of patients with
osteoarthritis and rheumatoid arthritis [71–73].
Furthermore, in patients with depression and
chronic pain, the depression symptoms improve
if the pain is reduced [70, 74, 75]. The relationship between depression and pain is reinforced by the fact that antidepressant drugs have
an analgesic effect on musculoskeletal pain
patients even without depression [76].
Although the relationship between chronic
pain and depression has been widely studied in
other musculoskeletal conditions, very few studies analyze this relationship in AKP patients.
Carlsson and colleagues [69] used the Rorschach
test on a group of patients with AKP while
comparing it to a control group. Patients with
91
AKP were different to control patients in that they
showed a higher depression index (DEPI > 4).
Comparison with a group of psychiatric outpatients showed a higher depression rate in patients
with AKP. However, Witonski [77], using the
Beck Depression Inventory (BDI), found no differences between a group of 20 AKP patients with
a mean age of 18 and a control group of similar
age. It is possible that the difference in the results
is because the last group was too young, a mean
age of 18, or because of the different type of
measurement tool. Clark and colleagues [68]
performed a clinical trial with 81 AKP patients,
assigning them randomly to four types of physical
therapy treatments. Prior to this treatment, 15% of
the patients had borderline depression symptoms
or a well-established depression measured with
the HAD questionnaire scale. Interestingly, the
levels of depression, pain and disability improved
after 3 months and after 12 months of treatment
in the 4 groups. Domenech and colleagues [59]
analyzed a sample of 54 patients with chronic
AKP. They measured the presence of depressive
symptoms with the HAD questionnaire. They
demonstrated that if anxiety is present, then levels
of pain and disability rise drastically (Table 2).
In conclusion, in a chronic AKP patient it is
important to identify the presence of depression
for several reasons. The most important fact is
that depression increases disability as well as
the degree of pain. Therefore, it prolongs the
condition. Another reason is that undiagnosed
and untreated depression has been related to a
poor response to physical therapy or surgery. It
is essential to perform a special evaluation
aimed at ruling out the coexistence of hidden
depression in these patients.
6
The Experience of Living
with Anterior Knee Pain
As has been discussed so far in this chapter, psychological factors, such as fear and catastrophizing, can modulate the pain response in people with
AKP. This in turn can act as a barrier to successful
rehabilitation and further modulate the physiological responses to pain with the development
92
and maintenance of chronic persistent pain.
However, the main stay of the research demonstrating this is quantitative. Advocates of qualitative research methods, however, suggest that
qualitative research can disclose the experience of
people with pain, and can therefore be used to
better understand patients’ behaviors and perspectives. Qualitative research gives rich insights
into the sociocultural context of pain.
6.1 Pain-Related Fear
In 2017 (published 2018) the first known qualitative research study investigating the lived
experience of AKP was conducted by Smith and
colleagues [78]. A convenience sample of ten
patients aged between 18 and 40 years with AKP
were recruited prior to starting physiotherapy.
The mean duration of symptoms was 78 months,
and the mean age of the participants was
30.6 years old. These patient characteristics are
comparable to those of other studies recruiting
from the National Health Service (NHS) in the
UK. Interviews were designed to cover the following topics of the lived experience of AKP:
living with knee pain; past healthcare management; interpretation of causation of pain; beliefs,
attitudes and behavior concerning pain; and
expectations for the future.
Participants offered a rich and detailed
account of the impact and lived experience of
AKP; the first theme that emerged from the data
were labelled (1) impact on self. It described the
participants’ sense of loss in relation to their self
and self-identity. The loss of physical ability was
profound and considerable. As one patient
described it, “I struggle at work, bending down
to get the bottom shelf and getting back up, I
literally have to hold onto the table to pull myself
up. I can’t do it off just my knees”.
The further four themes described how participants dealt with this loss in a climate of uncertainty, what they understood and how they made
decisions about their knee pain, these were labelled
(2) uncertainty, confusion and sense making;
(3) exercise and activity beliefs; (4) behavioral
coping strategies and (5) expectations of the future.
V. Sanchis-Alfonso et al.
Participants expressed intense confusion
around their pain and symptoms, resulting in
specific beliefs regarding barriers to exercise and
activity, with all the participants included
describing fear-avoidant, or kinesiophobic,
behaviors with strong ‘damage’ beliefs. “If
something hurts it is because your body’s telling
you if you do that, you’re going to cause more
injury”.
Also, low expectation for the future and low
self-efficacy was demonstrated by most of the
participants included, which could be conceptualized as ‘catastrophizing’. One participant
described negative feelings about the future and
their prognosis, “it does concern me that it’s
going to be every day for the rest of my life I’m
going to be struggling to walk upstairs. And then
I think about getting old, and I think I’m going to
end up with a stairlift and living downstairs”.
The research also identified judgmental attitudes from colleagues, friends or family, and loss
of meaningful activity, acting as moderators to
low moods and feelings of loss of self-identity.
For example, one participant described work
colleagues as “saying that I’m a grandma. They
say, ‘Yeah. If you were a horse, they’d put you
down”, 26-year-old.
6.2 Distress from Joint Noises
Audible joint noises, such as ‘grinding’, ‘creaking’, ‘clunking’ are common features of AKP
and are often referred to as crepitus. Crepitus in
AKP should be considered a normal rather than a
pathological finding on assessment, although
more common in females. For example, in a
1998 cohort study of 210 pain-free adults 94% of
females (mean age 47), with no lifetime history
of knee pain reported crepitus [6]. In comparison,
in the same study they found only 45% of males
(mean age 48) reported crepitus.
Crepitus was found to be a source of distress
and confusion by Smith and colleagues and this
was corroborated in further qualitative research
published by Robertson and colleagues [79].
Robertson aimed to understand people’s beliefs
and understanding of joint crepitus and recruited
Evaluation of Psychological Factors …
eleven participants with a history of AKP, conducting interviews focusing on the participants’
joint noises. Both Smith and colleagues and
Robertson and colleagues identified that joint
noises were often accompanied by negative
emotions and inaccurate aetiological beliefs, such
as a sign of premature ageing or damage beliefs.
This often led to fear-avoidance of the activities
the patients associated with the joint noises, such
as running, squatting, stairs, sitting, and kneeling, with a negative cycle of fear of degenerative
changes and subsequent reduced physical activity. A participant in Smith’s study described the
emotional anxiety associated with the joint
noises, “It was the noise that was concerning me
more than the pain.” Although crepitus seems
normal, time should be taken to explain this to
patients carefully so that they can focus on their
rehabilitation.
6.3 Responding to Treatment
Following Smith’s initial qualitative study, the
research team conducted a feasibility RCT with
60 participants investigating a biopsychosocial
approach to physiotherapy (a holistic approach
that attempts to include patients’ behaviors,
thoughts and feelings into a comprehensive
rehabilitation program) for AKP compared to
usual physiotherapy, in a large UK based teaching hospital [80]. The experimental exercise
program was a novel physiotherapy lead intervention based on pain education and exercise
prescription, where a single exercise was
designed to gradually expose the participant to
the activities they had been avoiding, coupled
with self-management strategies aiming to facilitate improvements in physical activity levels.
Further to this, the study team conducted interviews with a subset of ten patients (five from
both intervention arms) to understand potential
barriers and facilitators to the implementation of
the intervention [80].
The quantitative data collected with the feasibility RCT was not powered to detect any statistical significance in outcome data, and indeed
there was no difference between the two groups
93
at 6-months follow in terms of the global rating
of change (GROC), the visual analogue scale
(VAS) for pain, the Tampa Scale for Kinesiophobia (TSK), the ‘Pain Catastrophizing Scale’
(PCS), the General Self Efficacy Scale (GSES),
and the generic health outcome Euro-QOL (UK
dataset) (EQ-5D-5 L). However, there was some
difference when analyzing the qualitative data.
Self-efficacy and locus of control was a theme
discussed with all participants, however, patients
in the experimental intervention group described
narratives that were conceptualized as greater
self-efficacy and greater internal locus of control,
compared with patients in the usual physiotherapy group. Locus of control and self-efficacy are
inter-related psychological constructs related to
the power of thinking in achieving treatment
outcomes and goals [81]; to put it another way,
it’s how much an individual believes that have
the capability to carry out a specific activity to
achieve their goals [82]. Smith and colleagues
suggested that improvements in pain and function may have been mediated, in some part, by
greater self-efficacy and locus of control.
In conclusion, quantitative methods dominate
AKP research, and have focused on pain and
biomechanics. Qualitative research can offer an
insight into the experience of individuals living
with AKP that cannot be measured with numbers. For example, this qualitative research suggest future intervention development and
research is warranted into biopsychosocial targeted interventions that are aimed to address the
pain-related fear identified.
7
Implications of Psychological
Factors for Clinicians Who Are
Treating AKP Patients
People with severe AKP and psychological
impairment may benefit from therapeutic strategies that target both the physical and nonphysical aspects of this pathological condition.
Selhorst and colleagues [83] have shown that
better functional results and better reduction of
pain compared to a traditional approach in the
short-term follow-up will occur if we address
94
V. Sanchis-Alfonso et al.
psychosocial and physical impairments in the
treatment algorithm of AKP patients. However,
at six months follow-up, the majority of patients
in both groups (sequential cognitive and physical
approach group vs non-sequential physical
impairment-based approach group) reported high
levels of function, but 43% of patients still
reported pain [83]. Moreover, we significantly
reduce pain-related fear, pain catastrophizing,
fear-avoidance beliefs, and improve function if
we incorporate a brief one-time psychologically
informed video into the standard physical therapy protocol [84, 85]. Priore and colleagues [86]
have demonstrated that a knee brace is effective
at reducing kinesiophobia. Therefore, the use of a
knee brace could be a good strategy to improve
exercise compliance by reducing kinesiophobia.
De Oliveira Silva and colleagues [87] have
shown that kinesiophobia may be a potential
psychological mediator of pain and disability
outcomes in AKP patients. The moderate relationship of kinesiophobia with self-reported pain
and disability indicates that addressing kinesiophobia during treatment may be important to
improve clinical outcomes. Kinesiophobia may
play a more important role in the self-reported
pain and disability than PFJ loading during stair
ambulation.
Future research should try to determine whether interventions targeting reductions in psychologic factors can effectively optimize
rehabilitation and reduce the high rate of people
with AKP reporting unfavorable outcomes in the
long-term.
–
–
–
–
9
status of all patients with AKP, including
those with severe structural anomalies.
Our data shows that the presence of psychological factors is a limitation to recovery. That
is, psychological factors are barriers to recovery.
Patients with high levels of pain-related fear
with pathology get back to normal or are at
least much better mentally after effective
treatment. Therefore, we should not ignore
them. We need to look hard for pathology and
help them, even if it takes more patience and
tender loving care from the provider.
Cognitive-behavioral therapy focused on
reducing fear-avoidance behaviors and catastrophizing may influence the clinical state of
AKP patients in a positive manner. Therefore,
psychological therapies might be able to work
together with physical therapy and surgical
therapies in the treatment of AKP patients.
The change in catastrophizing is the strongest
predictor of changes in both pain and disability after treatment.
Key Message
– Psychological factors in AKP patients are
modulators of pain and disability and should
be addressed in combination with the search
of structural causes.
References
8
Take Home Messages
– Chronic pain and disability in AKP patients
are the result of a combination of biomechanical, anatomic and biological factors, as
well as the social environment, psychological
distress, and attitudes and beliefs, such as
catastrophizing and kinesiophobia.
– The clinical interest in addressing the whole
picture is to identify the potentially modifiable
factors to achieve better outcomes. Therefore,
we must always evaluate the psychological
1. Melzack R, Casey KL. Sensory, motivational, and
central control determinants of pain: a new conceptual model. In: Kenshalo D, editor. The skin senses.
Springfield: CC Thomas; 1968. p. 423–39.
2. Moayedi M. All roads lead to the insula. Pain.
2014;155(10):1920–1.
3. Damasio AR, Grabowky TJ, Bechara A, et al.
Subcortical and cortical brain activity during the
feeling of self-generated emotions. Nat Neurosci.
2000;3:1049–56.
4. Domenech J, Sanchis-Alfonso V, Lopez L, et al.
Influence of kinesiophobia and catastrophizing on pain
and disability in anterior knee pain patients. Knee Surg
Sports Traumatol Arthrosc. 2013;21:1562–8.
Evaluation of Psychological Factors …
5. Dye SF, Vaupel GL, Dye CC. Conscious neurosensory mapping of the internal structures of the human
knee without intraarticular anesthesia. Am J Sports
Med. 1998;26(6):773–7.
6. Johnson LL, van Dyk GE, Green JR 3rd, et al.
Clinical assessment of asymptomatic knees: comparison of men and women. Arthroscopy. 1998;14
(4):347–59.
7. Kaplan LD, Schurhoff MR, Selesnick H, et al.
Magnetic resonance imaging of the knee in asymptomatic professional basketball players. Arthroscopy.
2005;21(5):557–61.
8. MacIntyre NJ, Hill NA, Fellows RA, et al. Patellofemoral joint kinematics in individuals with and
without patellofemoral pain syndrome. J Bone Joint
Surg Am. 2006;88(12):2596–605.
9. Engel GL. The need for a new medical model: a
challenge for biomedicine. Science. 1977;196
(4286):129–36.
10. Waddell G, Newton M, Henderson I, et al. A fear
avoidance beliefs questionnaire and the role of fear
avoidance beliefs in chronic low back pain and
disability. Pain. 1993;52:157–68.
11. Lethem J, Slade PD, Troup JDG, et al. Outline of
fear-avoidance model of exaggerated pain perceptions. Behav Res Ther. 1983;21:401–8.
12. Asmudson GJ, Norton PJ, Vlaeyen JWS. Fear
avoidance models of chronic pain: an overview.
In GJ Asmudson, JWS Vlaeyen, G Crombez
(Eds) Understanding and treating fear of pain.
Oxford University Press. Oxford. 2004; pp 3–24
13. Crombez G, Vlaeyen JW, Heuts PH, et al. Pain
related fear is more disabling than pain itself:
evidence on the role of pain related fear in chronic
low back pain disability. Pain. 1999;80:329–39.
14. Vlaeyen JWS, Linton SJ. Fear avoidance and its
consequences in chronic musculoskeletal pain: a state
of the art. Pain. 2000;85:317–32.
15. Al-Obaidi SM, Beattie P, Al-Zoabi B, et al. The
relationship of anticipated pain and fear avoidance
beliefs to outcome in patients with chronic low back
pain who are not receiving workers’ compensation.
Spine. 2005;30:1051–7.
16. Keeley P, Creed F, Tomenson B, et al. Psychosocial
predictors of health-related quality of life and health
service utilisation in people with chronic low back
pain. Pain. 2008;135:142–50.
17. Waddell G, Pilowsky I, Bond MR. Clinical assessment and interpretation of abnormal illness behaviour
in low back pain. Pain. 1989;39:41–53.
18. Woby SR, Watson PJ, Roach NK, et al. Adjustment
to chronic low back pain—the relative influence of
fear avoidance beliefs, catastrophizing and appraisals
of control. Behav Res Ther. 2004;42:762–74.
19. Carragee EJ, Alamin TF, Miller JL, et al. Disographic, MRI and psychosocial determinants of low
back pain disability and remission: a prospective
study in subjects with benign persistent back pain.
Spine J. 2005;5:24–35.
95
20. Fritz JM, George S, Delitto A. The role of fear
avoidance beliefs in acute low back pain: relationship
with current and future disability and work status.
Pain. 2001;94:7–15.
21. George SZ, Fritz JM, McNeil DW. Fear avoidance
beliefs as measured by the fear avoidance beliefs
questionnaire: change in fear avoidance beliefs
questionnaire is predictive of change in self report
of disability and pain intensity for patients with acute
low back pain. Clin J Pain. 2006;22:197–203.
22. Grotle M, Vollestad NK, Brox JI. Clinical course and
impact of fear avoidance beliefs in acute low back
pain. Spine. 2006;31:1038–46.
23. Swinkels-Meewise IEJ, Roelofs J, Shouten EGW,
et al. Fear of movement/(Re)injury predicting chronic
disabling low back pain: a prospective inception
cohort study. Spine. 2006;31:658–64.
24. Woby SR, Watson PJ, Roach NK, et al. Are changes
in fear avoidance beliefs, catastrophizing and appraisal of control, predictive of changes in chronic low
back pain and disability? Euro J Pain. 2004;8:201–
10.
25. Linton SJ, Boersma K, Jansson M, et al. Are fear
avoidance beliefs related to the inception of an
episode of back pain? A prospective study Psychol
Health. 1999;14:1051–9.
26. Linton SJ, Boersma K, Jansson M, et al. The effects
of cognitive behavioural and physical therapy preventive interventions on pain related sick leave.
A randomized controlled trial. Clin J Pain
2005;21:109–119.
27. Jensen JN, Albertsen K, Borg V, et al. The predictive
effect of fear-avoidance beliefs on low back pain
among newly qualified health care workers with and
without previous low back pain: a prospective cohort
study. BMC Musculoskelet Disord. 2009;24
(10):117.
28. Van Nieuwenhuyse A, Somville PR, Crombez G,
et al. The role of physical workload and pain related
fear in the development of low back pain in young
workers: evidence from the BelCoBack study: results
after one year of follow up. Occup Envirom Med.
2006;63:247–57.
29. Picavet HSJ, Vlaeyen JWS, Schouten SAG. Pain
catastrophizing and kinesiophobia: predictors of
chronic low back pain. Am J Epidemiol.
2002;156:1028–34.
30. Piva SR, Fitzgerald GK, Wisniewski S, et al.
Predictor of pain and function outcome after rehabilitation in patients with patellofemoral pain syndrome. J Rehab Med. 2009;41:604–12.
31. Jensen R, Hystad T, Baerheim A. Knee function and
pain related to psychological variables in patients
with long-term patellofemoral pain syndrome.
J Orthop Sports Phys Ther. 2005;35:594–600.
32. Smith BE, Hendrick P, Bateman M, et al. Current
management strategies for patellofemoral pain: an
online survey of 99 practising UK physiotherapists.
BMC Musculoskelet Disord. 2017;18(1):181.
96
33. Robertson CJ, Hurley M, Jones F. People’s beliefs
about the meaning of crepitus in patellofemoral pain
and the impact of these beliefs on their behaviour: A
qualitative study. Musculoskelet Sci Pract.
2017;28:59–64.
34. Maclachlan LR, Matthews M, Hodges PW, et al. The
psychological features of patellofemoral pain: a
cross-sectional study. Scand J Pain. 2018;18
(2):261–71.
35. Maclachlan LR, Collins NJ, Hodges PW, et al.
Psychological and pain profiles in persons with
patellofemoral pain as the primary symptom. Eur J
Pain. 2020;24(6):1182–96.
36. Selhorst M, Fernández-Fernández A, Schmitt L, et.
Al. Adolescent psychological believes, but not parent
beliefs, associated with pain and function in adolescents with patellofemoral pain. Phys Therapy Sport.
2020;45:155–160.
37. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to
patient characteristics and current adjustment. Pain.
1983;17:33–44.
38. Thomeé R, Renstrom P, Karlsson J, et al. Patellofemoral pain syndrome in young women. I. A clinical
analysis of alignment, pain parameters, common
symptoms and functional activity level. Scand J Med
Sci Sports 1995;5:237–244.
39. Goodin BR, McGuire L, Allshouse M, et al. Associations between catastrophizing and endogenous
pain-inhibitory processes: sex differences. J Pain.
2009;10(2):180–90.
40. Gracely RH, Geisser ME, Giesecke T, et al. Pain
catastrophizing and neural responses to pain among
persosns with fibromyalgia. Brain. 2004;127:835–43.
41. Edward RR, Smith MT, Stonerock G, et al. Painrelated catastrophizing in healthy women is associated with greater temporal summation of and reduced
habituation to thermal pain. Clin J Pain.
2006;22:730–7.
42. Keefe FJ, Caldwell DS, Queen KT, et al. Pain coping
strategies in osteoarthritis patients. J Consult Clin
Psychol. 1987;55:208–12.
43. Keefe FJ, Brown Gk, Wallston KA et al. Coping with
rheumatoid arthritis pain: Catastrophizing as a maladaptative strategy. Pain. 1989;37:51–56.
44. Keefe FJ, Affleck G, Lefebvre JC, et al. Pain coping
strategies and coping efficacy in rheumatoid arthritis:
a daily process analysis. Pain. 1997;69:35–42.
45. Forsythe ME, Dumbar MJ, Henningar AW, et al.
Prospective relation between catastrophizing and
residual pain following knee arthroplasty: two-year
follow-up. Pain Res Manag. 2008;13:335–41.
46. Sommers T,Keefe Fj, Pells J, et al. Pain catastrophizing and pain-related fear in osteoarthritis
patients: relationships to pain and disability J Pain
Symptom Manag. 2009;37:863–72.
47. Meyer K, Tschopp A, Sprott H, et al. Association
between catastrophizing and self-rated pain and
disability in patients with chronic low back pain.
J Rehabil Med. 2009;41:620–5.
V. Sanchis-Alfonso et al.
48. Martin M, Bradley L, Alexander R, et al. Coping
strategies predict disability in patients with primary
fibromyalgia. Pain. 1996;68:45–53.
49. Severeijns R, Vlaeyen JW, van den Hout MA, et al.
Pain catastrophizing predicts pain intensity, disability, and psychological distress independent of the
level of physical impairment. Clin J Pain.
2001;17:165–72.
50. Bedard GB, Reid GJ, McGrath PJ. Coping and selfmedication in a community sample of junior high
school students. Pain Res Manag. 1997;2:151–6.
51. Jacobson NS, Butler R. Relation of cognitive coping
and catastrophizing to acudte ain and analgesic use
following breast cancer surgery. J Behav Med.
2000;19:17–29.
52. Kendell K, Saxby B, Farrow M, et al. Psychological
factors associated with short term recovery from total
knee replacement. Br J Health Psychol. 2001;6:41–
52.
53. Peters ML, Vlaeyen JWS, van Drunen C. Do
fibromyalgia patients display hypervigiance for
innocuous somatosensory stimulus? Application of
a body scanning reaction time paradigm. Pain.
2000;86:283–92.
54. Severeijns R, Vlaeyen JWS, Van Den Hout MA,
et al. Pain catastrophizing is associated with health
indices in musculoskeletal pain: a cross-sectional
study in the dutch community. Health Psychol.
2004;23:49–57.
55. Sullivan MJ, Neish N. The effects of disclosure on
pain during dental hygiene treatment: the moderating
role of catastrophizing. Pain. 1999;79:155–63.
56. Turner JA, Mancl L, Aaron LA. Pain-related catastrophizing: a daily process study. Pain.
2004;110:103–11.
57. Buer N, Linton SJ. Fear-avoidance beliefs and
catastrophizing: occurrence and risk factor in back
pain and ADL in the general population. Pain.
2002;99:485–91.
58. Thomeé P, Thomeé R, Karlsson J. Patellofemoral
pain syndrome: pain, coping strategies and degree of
well-being. Scand J Med Sci Sports. 2002;12:276–
81.
59. Domenech J, Sanchis-Alfonso V, Espejo B. Changes
in catastrophizing and kinesiophobia are predictive of
changes in disability and pain after treatment in
patients with anterior knee pain. Knee Surg Sports
Traumatol Arthrosc. 2014;22(10):2295–300.
60. Wride J, Bannigan K. Investigating the prevalence of
anxiety and depression in people living with
patellofemoral pain in the UK: the Dep-Pf Study.
Scand J Pain. 2019 24;19(2):375–382.
61. McManus S, Bebbington P, Jenkins R, Brugha T,
editors. Mental health and well-being in England:
Adult Psychiatric Morbidity Survey 2014. Leeds:
NHS Digital, 2016.
62. Cameron IM, Cardy A, Crawford JR, et al. Measuring depression severity in general practice: discriminatory performance of the PHQ-9, HADS-D, and
BDI-II. Br J Gen Pract. 2011;61:419–26.
Evaluation of Psychological Factors …
63. Stubbs B, Aluko Y, Myint PK, et al. Prevalence of
depressive symptoms and anxiety in osteoarthritis: a
systematic review and meta-analysis. Age Ageing.
2016;45:228–35.
64. Currie SR, Wang J. Chronic back pain and major
depression in the general Canadian population. Pain.
2004;107:54–60.
65. Soderlin MK, Hakala M, Nieminen P. Anxiety and
depression in a community-based rheumatoid arthritis population. Scand J Rheumatol. 2000;29:177–83.
66. Varni JW, Rapoff MA, Waidron SA, et al. Effects of
perceived stress on pediatric chronic pain. J Behav
Med. 1996;19:515–28.
67. McCracken LM, Faber SD, Janeck AS. Pain-related
anxiety predicts non-specific physical complaints in
persons with chronic pain. Behav Res Ther.
1998;36:621–30.
68. Clark DI, Downing N, Mitchell J, et al. Physiotherapy for anterior knee pain: a randomized controlled
trial. Ann Rheum Dis. 2000;59:700–4.
69. Carlsson AM, Warner S, Mattlar CE, et al. Personality in patients with long term patellofemoral pain
syndrome. Knee Surg Sports Traumatol Arthrosc.
1993;1:178–83.
70. Fishbain DA, Cutler R, Rosomoff HL, et al. Chronic
pain-associated depression: antecedent or consequence of chronic pain? a review Clin J Pain.
1997;13:116–37.
71. Axford J, Heron C, Ross F, et al. Management of
knee osteoarthritis in primary care: pain and depression are the major obstacles. J Psychosom Res.
2008;64:461–7.
72. Kojima M, Kojima T, Suzuki S, et al. Depression,
inflammation, and pain in patients with rheumatoid
arthritis. Arthritis Rheum. 2009;61:1018–24.
73. Peck JR, Smith TW, Ward JR et al. Disability and
depression in rheumatoid arthritis. A multi-trait,
multi-method investigation. Arthritis Rheum.
1989;32:1100–1106.
74. Kroenke K, Bair MJ, Damush TM, et al. Optimized
antidepressant therapy and pain self-management in
primary care patients with depression and musculoskeletal pain: a randomized controlled trial. JAMA.
2009;301:2099–110.
75. Wallis BJ, Lord SM, Bogduk M. Resolution of
psychological distress of whiplash patients following
treatment by radiofrequency neurotomy. A randomized double blind placebo controled trial. Pain.
1997;73:15–22.
76. Staiger TO, Gaster B, Sullivan MD, et al. Systematic
review of antidepressants in the treatment of chronic
low back pain. Spine. 2003;28:2540–5.
77. Witonski D. Anterior knee pain syndrome. Int
Orthop. 1999;23:341–4.
97
78. Smith BE, Moffatt F, Hendrick P, et al The
experience of living with patellofemoral pain—loss,
confusion and fear-avoidance: a UK qualitative
studyBMJ Open 2018;8:e018624. https://doi.org/10.
1136/bmjopen-2017-018624.
79. Robertson CJ, Hurley M, Jones F. People’s beliefs
about the meaning of crepitus in patellofemoral pain
and the impact of these beliefs on their behaviour: a
qualitative study. Musculoskeletal Sci Pract.
2017;28:59–64.
80. Smith BE, Moffatt F, Hendrick P, et al Barriers and
facilitators of loaded self-managed exercises and
physical activity in people with patellofemoral pain:
understanding the feasibility of delivering a multicentred randomised controlled trial, a UK qualitative
study. BMJ Open 2019;9:e023805. https://doi.org/
10.1136/bmjopen-2018-023805.
81. Myers AM, Powell LE, Maki BE, et al. Psychological indicators of balance confidence: relationship to
actual and perceived abilities. J Gerontol A Biol Sci
Med Sci. 1996;51:M37–43. https://doi.org/10.1093/
gerona/51A.1.M37.
82. Self-Efficacy: the exercise of control. Bandura,
Albert | Freeman, W. H. | Lightsey, Richard.
J Cognitive Psychotherapy 13(2). https://doi.org/10.
1891/0889-8391.13.2.158.
83. Selhorst M, Rice W, Jackowski M, et al. A sequential
cognitive and physical approach (SCOPA) for
patellofemoral pain: a randomized controlled trial in
adolescent patients. Clin Rehabil. 2018;32(12):1624–
35.
84. Selhorst M, Hoehn J, Degenhart T, et al.
Psychologically-informed video reduces maladaptive
beliefs in adolescents with patellofemoral pain. Phys
Ther Sport. 2020;41:23–8.
85. Selhorst M, Fernandez-Fernandez A, Schmitt L, et al.
Effect of a psychologically informed intervention to
treat adolescents with Patellofemoral Pain: a randomized controlled trial. Arch Phys Med Rehabil.
2021;102(7):1267–73.
86. Priore LB, Lack S, Garcia C, et al. Two weeks of
wearing a knee brace compared with minimal
intervention on kinesiophobia at 2 and 6 weeks in
people with patellofemoral pain: a randomized
controlled trial. Arch Phys Med Rehabil. 2020;101
(4):613–23.
87. De Oliveira SD, Willy RW, Barton CJ, et al. Pain and
disability in women with patellofemoral pain relate to
kinesiophobia, but not to patellofemoral joint loading
variables. Scand J Med Sci Sports. 2020;30:2215–21.
Management of Anterior Knee Pain
from the Physical Therapist’s
Perspective
Jenny McConnell
Anterior knee pain is a complex and interesting
disorder for clinicians to manage. Various soft
tissue structures of the knee can generate neurosensory signals that result in conscious pain
perception. It behooves the clinician to determine, where possible, the source of the symptoms and the underlying causative factors so the
patient receives appropriate management for their
anterior knee pain problem. Pain has biopsychosocial components, so the clinician is in an
ideal position to determine how to effectively
help the patient improve and manage their
symptoms.
As the patellofemoral joint is essentially a soft
tissue joint, the clinician needs to examine the
complex interaction of the dynamic loading and
control of the lower limb, as well as the relative
flexibility of various soft tissue structures to
ascertain the appropriate management of the
anterior knee pain symptoms. This requires a
thorough understanding not only of the lower
limb anatomy and mechanics, but also the neural
innervation of the various soft tissue structures
Supplementary Information The online version
contains supplementary material available at
https://doi.org/10.1007/978-3-031-09767-6_7.
J. McConnell (&)
Private Practice, Sydney, NSW, Australia
e-mail: jenny@mcconnell-institute.com
around the knee, and the effect of pain on muscle
activation. This chapter will explore these issues
to guide the clinician through an evidence based,
clinical reasoned management approach to
empower the patient to self-manage their
symptoms.
1
Sources of Pain
The tissue-based structures that can be a potential
source of knee pain are the synovium, lateral
retinaculum, subchondral bone, and the infrapatellar fat pad (IFP), with the articular cartilage
because it is aneural, providing only an indirect
source, perhaps either through synovial irritation
or increasing bone stress [1–3]. As histologic
changes in the synovium of patients with patellofemoral (PF) are only moderate, peripatellar
synovitis is a possible but less likely source of
knee pain symptoms. Histologic changes have
also been found in some patients with PF pain in
the lateral retinaculum with an increased number
of myelinated and unmyelinated nerve fibres,
neuroma formation and nerve fibrosis, providing
evidence that in some individuals, a laterally
tilted patella compromising the lateral retinacular
structures, may be the source of the symptoms
[2]. Additionally, increased intraosseous pressure
of the patella has been found in patients with PF
pain who complain of pain on prolonged sitting
(movie goers’ knee), possibly secondary to a
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_7
99
100
J. McConnell
transient venous outflow obstruction [3]. But the
structure which possibly has the greatest impact
on pain around the knee is the infrapatellar fat
pad (Hoffa’s pad). Superolateral fat pad oedema
is a frequent finding with patellar mal-tracking
and may precede clinically significant chondrosis
[1, 4, 5].
The IFP is a potent source of pain owing to its
rich innervation and relationship with the highly
innervated synovium [1, 5]. The IFP and the
medial retinaculum of PF patients have a higher
number of substance P fibers than the same
structures of individuals without PF pain [5].
The IFP is a dynamic structure, displacing significantly during knee motion, which is, therefore, vulnerable to interference from trauma or
repetitive overload [6]. The IFP stabilizes the
patella in extremes of knee motion (that is less
than 20° and greater than 100° of knee flexion),
increases tibial external rotation and facilitates
the distribution of synovial fluid [7]. Experimentally inducing knee pain by injecting hypotonic saline into the fat pad of asymptomatic
individuals causes severe infrapatellar pain, as
well as retro patellar pain, with some experiencing medial thigh and even groin pain [8].
2
Effect of Pain
The presence of pain will certainly decrease
muscle activity, timing and endurance as well as
alter movement patterns [9]. Experimental vastus
medialis muscle pain has been found to reduce
the EMG activity in the VM and VL muscles as
well as attenuate the loading response phase peak
knee extensor moments in gait [9, 10]. The
observed changes persist when the pain disappears. So, muscle pain modulates the function of
the quadriceps muscle, resulting in impaired knee
joint control and joint instability during walking,
which is a similar finding to patients with knee
pain. This loss of joint control during and subsequent pain may leave the knee joint prone to
injury and potentially participate in the chronicity
of musculoskeletal problems [10]. Experimentally inducing pain in the IFP of asymptomatic
individuals causes a decrease in both VMO and
VL activity, but when a painful electric shock is
randomly and intermittently applied to the knee,
mimicking the fear of pain state experienced by
PF pain patients, only VMO activity is decreased
[9]. Thus, pain is a cortical experience, where
extrinsic factors such as fear of pain, stress,
anxiety, and depression can amplify the pain
experience for the patient, so the contribution of
these factors must be understood if we are to
satisfactorily improve the rehabilitation of individuals with anterior knee pain.
Depression typically affects 5% of the general
population, but among patients with chronic
pain, 30%–45% experience depression. Studies
have shown that the relationship between
depression and pain is bidirectional: depression
is a positive predictor of the development of
chronic pain, and chronic pain increases the risk
of developing depression [11]. Neuroimaging
suggests an anatomic overlap in the pathway of
chronic pain and depression. Hence, positive
psychological factors, such as hope, optimism,
and pain acceptance may improve persistent and
chronic pain [11]. In a study of 710 chronic low
back pain sufferers, self-confidence to manage
pain was the most commonly perceived selfmanagement barrier, with 40% of these individuals feeling they were not involved as equal
partners in decision making and goal setting
related to their care [12]. It is therefore essential
for the clinician to develop a positive therapeutic
relationship with the patient, so the pain
chronicity and intensity may diminish with the
patient’s improved understanding of how to
manage their knee symptoms. In a recent study
examining the psychological features of PF pain,
no difference was found between PFP and painfree groups. However, when the PF groups were
sub-grouped into severe and less severe, there
were higher levels of psychological impairment
in the more-severe PFP-related disability group
compared with the less severe cases. Kinesiophobia was the most significant psychological
factor followed by depression and catastrophizing [13].
To help unpack the complexity of patellofemoral pain and minimise the risk of established
chronicity, an understanding of the knee joint
Management of Anterior Knee Pain from the Physical …
anatomy and the inter-relationship of the
dynamic lower limb mechanics is required, so an
individually tailored treatment can be designed
for the patient.
3
Anatomy and Biomechanics
The patella articulates with the femoral trochlea
during knee flexion and extension. The lateral
aspect of the femoral trochlea extends further
anteriorly than the medial aspect to provide
inherent stability for the patella, once the patella
is within the confines of the trochlea (from 2030o− knee flexion). Prior to this point, there is no
bony support for the patella, and passive stability
is provided by the medial and lateral retinaculum
and the joint capsule [14]. The stability of the
patella is also affected by the starting position of
the femur [15]. Femoral anteversion changes the
interrelationship of the patella and the femur.
Passive stability for the patella in the first 20°
of knee flexion is provided by the medial and
lateral retinaculum and the joint capsule. The
lateral side of the knee is made up of various
fibrous layers from the iliotibial band and vastus
lateralis to form the superficial and deep lateral
retinaculum [14]. As most of the lateral retinaculum arises from the iliotibial band, tightness of
the band, which has its greatest influence at 20°
of knee flexion, will contribute to lateral tracking
and tilt of the patella [15]. The retinacular support is stronger on the lateral side than it is on the
medial side.
Passive medial patellar stability is poor, so
medial patellar stability needs to be achieved
actively, which occurs through the muscular
attachment of the medial quadriceps into the
patella. The vastus medialis is commonly divided
into the oblique portion, the VMO, and the more
vertical component, the vastus medialis longus
(VML) [16, 17] While there is often difficulty
accurately distinguishing the VMO and VML as
separate entities, most authors agree that they act
as two distinct functional units due to their fibre
orientation and attachments, and thus angle of
force on the patella [18]. The VMO has significantly shorter mean fibre bundle length, greater
101
mean pennation angle, and smaller mean physiological cross-sectional area than VML. Sarcomere lengths of VMO and VML are
comparable. The VMO, being more obliquely
aligned (50 to 55° medially in the frontal plane)
than the VML (15 to 18° medially in the frontal
plane) [19], is more likely to contribute to medial
patellar stabilization, whereas VML, with a larger relative excursion and force-generating
capability, to the extension of the knee [19,
20]. It has been found on ultrasonography that
athletic individuals have an even higher VMO
fiber angle of 67.8°, providing a stronger medial
stabilizing force on the patella, than sedentary
individuals where it was 53.6° [21].
On the lateral side, the VL is oriented 12 to
15° laterally in the frontal plane with the obliquity of the distal fibres being greater. The VMO
opposes the lateral vector force of the VL,
allowing a more efficient extensor moment at the
knee. Senavongse and Amis found in a cadaver
study that relaxation of VMO caused a 30%
reduction in lateral stability of the patella [14].
This is supported by the work Sheehan et al.
[22], who found in asymptomatic individuals
during a dynamic cine- phase contrast MRI that
after motor branch block to the VMO, there was
a lateral shift of the patella of up to 1.8 mm, a
tibiofemoral lateral shift of up to 2.1 mm, and a
tibiofemoral external rotation 3.7°; concluding
that VMO weakness is a major factor in, but not
the sole source of, altered PF kinematics in PF
pain subjects.
VMO is active throughout knee extension to
keep the patella centred in the trochlea of the
femur. Thus, the synergistic relationship between
the medial and lateral vastii is important in
maintaining the alignment of the patella within
the femoral trochlea. Electromyographic
(EMG) studies have demonstrated that the muscle activity of VMO and VL in the general
asymptomatic population is relatively balanced
in terms of activation, magnitude, and timing in a
wide variety of static, dynamic, weightbearing
and non-weightbearing activities [23, 24]. This
synergistic relationship between the VMO and
VL should maintain the alignment of the patella
in the femoral trochlea in the first 30° of knee
102
flexion, before the patella is fully engaged in the
trochlea. It has been proposed that this balanced
activation of the VMO and VL is disrupted in
patients with PFPS. The issue of whether the
disruption could be a motor control dysfunction
has been investigated by Mellor and Hodges [24,
25] who found that synchronization of motor unit
action potentials, is reduced in PFP subjects
(38%) compared with controls (90%). However,
the evidence to support an imbalance in the
activation of the vastii (either decreased activation of VMO or enhanced activation of VL) is
contentious, as was examined in the systematic
review by Smith et al. [26]. Differences in
methodology (particularly with respect to the use
of EMG) and the inherent heterogeneity in the
PFPS population may account for some of the
inconsistencies in study results. This prompted
an impassioned plea by Grant el [27] to establish
methodological uniformity in the PF field (albeit
in this paper the concern was about measurement
of maltracking), with specific standards for anatomic and outcome measures, as the large
methodological variability across the literature
not only hinders the generalization of results, but
it mitigates understanding of the underlying
mechanisms of PF pain.
While there is inconclusive evidence to support or refute an imbalance in the magnitude of
vastii activation in patients with PFPS, disrupted
activation of the vastii may take the form of
delayed activation of the VMO relative to the
VL. It is hypothesized that the VMO, which has
a smaller cross-sectional area than the VL, must
receive a feedforward enhancement of its excitation level to track the patellar optimally. Many
studies examining individuals with PFP have
supported this hypothesis, by demonstrating that
the EMG activity and reflex onset time of the
VMO relative to the VL is delayed, when compared with asymptomatic individuals [23–25]. It
seems that most PF sufferers have a delayed
onset of VMO relative to VL on a stair stepping
task (67% concentrically, 79% eccentrically), but
it is apparent in some PFP patients there is no
delay of VMO [23]. Additionally, in some
asymptomatic individuals there is a delay in
onset of VMO relative to VL (46%
J. McConnell
concentrically and 52% eccentrically) [23]. So,
one could pose the hypothetical question, are
these individuals at risk of developing PF pain in
the future, if their activity level changes? Only a
longitudinal study would determine the answer to
this hypothetical question. What is apparent from
the study by Cowan et al. [23] is the need for
subgrouping of patients with PF pain and tailoring an individual program to their specific
needs. If a delayed onset of VMO is detected, a
treatment aim would be to facilitate a balance
between medial and lateral structures, so the load
through the joint could be distributed as evenly
as possible.
The control of the proximal segment by the
pelvic muscles, particularly the gluteals, is critical for dynamically positioning the femur and
hence the orientation of the trochlea. However, a
recent systematic review to investigate the association between hip muscle strength and dynamic
knee valgus found the relationship between hip
muscle strength, including abductors, extensors,
and external rotators and dynamic knee valgus
conflicting [28]. Some studies have concluded
that men with PFP show muscular weakness of
the hip [29], whereas others have found no difference in hip strength in women between PFP
sufferers and asymptomatic individuals [30].
Additionally, prospective studies indicate that
hip weakness is not a risk for development of
patellofemoral pain [31, 32]. In some clinical
trials strength training of the gluteal muscles
promotes improvement in symptoms in PF
patients but does not alter the kinematics [33,
34]. These findings demonstrate that not all
individuals suffering from PFP present with
dynamic knee valgus and that perhaps only it is
only a subgroup of patients that require
strengthening of the hip musculature [33] or
perhaps the problem is more an issue of control,
timing, and endurance rather than just strength.
There is also evidence that restricted ankle
dorsiflexion range of motion may alter lowerextremity landing mechanics, whereby a smaller
amount of ankle dorsiflexion displacement during landing is associated with less knee flexion
displacement, greater ground reaction forces, and
greater knee valgus displacement [35]. A meta-
Management of Anterior Knee Pain from the Physical …
analysis by Lima et al. [36] confirms the relationship between reduced ankle dorsiflexion and
increased dynamic knee valgus. These authors
concluded that the assessment of dynamic ankle
dorsiflexion in the clinical setting was important.
It has been found during the step-down test, that
individuals who have 17° or less of ankle
dorsiflexion range of motion (ROM) display
significantly greater hip adduction ROM than
those with more than 17° of dorsiflexion [37].
When the heel is elevated in the step-down test,
the same participants with limited dorsiflexion
ROM showed a significant reduction in hip
adduction ROM [37]. Thus, ankle dorsiflexion
and midfoot mobility should be considered when
assessing patients with aberrant frontal plane
lower limb alignment.
If ankle dorsiflexion is restricted then the
subtalar and midfoot joints can compensate by
pronating, provided the foot has sufficient
mobility to allow this. The pronation allows
further movement to occur at the foot and can
cause an increase in dynamic knee valgus and hip
adduction. A meta-analysis on the relationship
between foot posture as a risk factor for overuse
injuries showed very limited evidence that a
pronated foot posture was a risk factor for
patellofemoral pain development [38]. Kedroff
and Amis [39] have recently found no relationship between foot posture and kinematics in PFP
participants, thus questioning the use of orthoses
to correct pronation. A recent study by Matthews
et al. [40] confirmed there was no difference in
success rates between foot orthoses versus hip
exercises in those with high or low midfoot
width mobility. These authors concluded that
there was no association between midfoot width
mobility and treatment outcome, and in their
randomised controlled trial, there was no difference in success rate between foot orthoses and
hip exercises in patients with PF pain [40].
However, some studies have indicated the benefit
of using orthoses in the management of individuals with PF pain, particularly those who wear
less supportive footwear, report lower levels of
103
pain, exhibit less ankle dorsiflexion range of
motion, and report an immediate reduction in
pain with foot orthoses [41, 42].
4
Load and Frequency
Forces in the PF joint are a function of the
quadriceps and patellar tendon forces, which
compress the patella against the femur. The PFJ
Reaction Force (PFJRF) is equal and opposite to
this resultant force and acts perpendicular to the
articular surfaces and increases with increasing
flexion, as the angle between the patellar tendon
and the quadriceps becomes more acute. During
normal daily activities the PFJ becomes exposed
to force values between 0.5 (walking) to 9.7
(squatting and running) x body weight, whilst
sporting activities create force values that
approach up to 20 body weight [43].
It is apparent that not one factor is responsible
for anterior knee pain symptoms (Table 1), but it
is often the cumulative effect of too much load or
too great a frequency of load, as has been well
described by Dye in his seminal 1996 paper ‘The
knee as a biologic transmission with an envelope
of function: a theory’ [44], which hypothesizes
that anterior knee pain is a consequence of an
individual being taken out of their envelope of
function (which differs from individual to individual), breaching their threshold, thus not being
maintained in homeostasis, so soft tissues are
overloaded and the individual experiences pain.
Once pain is provoked, the individual can do less
and less. Dye has identified four factors that
influence an individual’s envelope of function.
These are: (1) anatomic factors which relate to an
individual’s inherent morphology, structural
integrity & biomechanical characteristics (that is
the parents they chose!); (2) kinematic factors
which signify the dynamic control of the joint,
that is the cerebral sequencing of motor units,
indicating neural control of the limb and segment; (3) physiological factors which are the
genetically determined mechanisms controlling
104
J. McConnell
Table 1 Predisposing Factors for PF pain
overuse
patellar malposition
abnormal foot mechanics
poor VMO timing
PF PAIN
tight lateral structures
poor pelvic mechanics
poor pelvic control
training errors
quality and rate of repair and [4] the type of
rehabilitation or surgery, which can be either
beneficial or detrimental to recovery [44].
5
History
The initial part of the examination of the patient
involves obtaining a detailed history, so a differential diagnosis can be proposed. The diagnosis is later confirmed or modified by the
physical findings. In the history, the clinician
needs to elicit, the area of pain, the type of
activity precipitating the pain, the history of the
onset of the pain, the behaviour of the pain and
any associated clicking, giving way, or swelling
[45]. This gives an indication of the structure/s
involved and the likely diagnosis; for example, if
the type of activity that precipitated the patient’s
pain is one that involves eccentric loading, such
as jumping in basketball or increased hill work
during running, patellar tendinopathy would be
suspected. On the other hand, if the athlete
reports pain following tumble turning or vigorous kicking in swimming, or on delivery of a fast
ball in cricket on the landing leg, an irritated fat
pad would be suspected, as it is the rapid,
forceful, end range extension of the knee, causing the inferior pole of the patella to jam suddenly into the nociceptive IFP [1]. In both these
conditions the athlete complains of inferior
patellar pain. The patient with an irritated fat pad
is aggravated by straight leg raise exercises
(SLR), so it is essential the clinician recognises
the condition so appropriate management can be
implemented to enhance, rather than, impede
recovery. The clinical diagnosis of fat pad irritation may be confirmed on MRI on a T2
weighted image where inflammation of the fat
pad may be visualised. Patellar tendinopathy can
be confirmed on diagnostic ultrasound, particularly using colour doppler or with MRI.
It is crucial as a treating clinician, once you
have listened to the patient’s history to give the
patient some knowledge about why they have
pain, where their pain is coming from, and what
is the expected length of time it may take for
recovery. Knowledge is power and it is the
clinician’s responsibility to empower the patient
to manage their problem, and to emphasise that
musculoskeletal problems are managed, not
cured [46]. The importance of education for
conceptual understanding (e.g., musculoskeletal
diagnosis, pain), for physical performance (e.g.,
rehabilitative exercise, postural correction), and
for behavioural change (e.g., modifying load) in
patient management is paramount [45]. By
enhancing the patient’s knowledge about their
problem(s) and how to ‘self-manage’ it, they are
empowered to increasingly take control of the
situation and minimise the impact on their lifestyle. Education to improve understanding can
Management of Anterior Knee Pain from the Physical …
lead to a decrease in patient fear, greater compliance, and a concurrent improvement in pain
experienced and movement impairments [46].
This can be done by explaining Dye’s [44] model
of homeostasis and envelope of function (which
should be drawn sitting next to the patient) to
help the patient have an idea as to why their knee
pain started. Informing the patient about the
effect of loading the knee with activities is
important (such as 05 body weight goes
through the knee with level walking, this
increases to 3–4 body weight with stairs and
8–10 with running). Additionally, discussing
with the patient the effect pain and fear of pain
has on quadriceps muscle activity enhances the
understanding of their problem. This summary is
a helpful tool for the patient to take home and
give them time to absorb the information.
Knee pain !# quads ! more knee pain !
fear of pain !# VMO ! maltracking of patella
! more knee pain !" hamstrings and gastrocs
activity !# ability to lengthen !" relative
flexibility in lumbar spine and midfoot, when:
(i) lifting !# knee flexion !" flexion of spine
!" stress on spine.
(ii) descending steps !# dorsiflexion !"
pronation !" knee collapsing in !" knee
pain.
6
Symptoms of Patellofemoral Pain
The patient usually complains of a diffuse ache in
the anterior knee, which is exacerbated by stair
climbing. For many, the knee will ache when
they’re sitting for prolonged periods with the
knee flexed—the movie sign. However, patients
with an irritated fat pad have pain with prolonged
standing rather than prolonged sitting. Some
patients will have crepitus, which is often a
source of concern for them because they feel, that
the crepitus is indicative of “arthritis”. This creates negative emotions, inaccurate etiological
beliefs and ultimately leads to altered behaviour
[47]. However, the crepitus is mostly due to tight
deep lateral retinacular structures and can be
improved with treatment.
105
Some patients may experience “giving way”
or a buckling sensation of their knee. This occurs
during walking or stair climbing i.e., movements
in a straight line, and is a reflex inhibition of the
quadriceps muscle. It must be differentiated from
the giving way experienced when turning, which
is indicative of an anterior cruciate deficient knee
or patellofemoral instability. Locking is another
symptom, which must be differentiated from
intra-articular pathology. Patellofemoral locking
is usually only a catching sensation where the
patient can actively unlock the knee; unlike loose
body or meniscal locking, where the patient is
either, unable to unlock, or can only passively
unlock, the knee. Mild swelling due to synovial
irritation may also occur with patellofemoral
problems. Mild swelling causes an asymmetric
wasting of the quadriceps muscle, whereby the
VMO is inhibited before the VL and rectus
femoris (RF) [48]. So, an individual, who has
primary intra- articular pathology, such as a
meniscal or ligamentous injury and is recovering
from knee surgery where quadriceps wasting is
common, may have great difficulty resolving the
subsequent secondary patellofemoral problem,
particularly if it is not identified [49, 50].
When considering the possible differential
diagnoses, the clinician must remember that the
lumbar spine and the hip can refer symptoms to
the knee. For example, the prepubescent male
with a slipped femoral epiphysis may present
with a limp and AKP so can initially be misdiagnosed as having PF pain.
Neural tissue may also be a source of symptoms around the PF joint. Lack of mobility of the
L5 and S1 nerve roots and their derivatives can
give rise to posterior or lateral thigh pain, and
dermatomal distribution of anterior thigh pain
coming from the L3 nerve root. Symptoms from
neural tissue can be relatively easily differentiated from PF symptoms because the pain will be
exacerbated in sitting, particularly when the leg
is straight rather than in the classic movie sign
position of a flexed knee. The slump sitting test
or prone knee band will quickly verify the neural
tissue as being a source of the symptoms. Similarly, a peripheral nerve may scar down or
become entrapped following arthroscopic
106
J. McConnell
surgery. The commonest example is the infrapatellar branch of the saphenous nerve. Symptoms
are sharp pain inferomedially with/without
slightly altered sensation laterally. The symptoms can be reproduced on deep bend and
jumping so they are frequently confused with
patellar tendinopathy symptoms because of the
proximity to the tendon. The clinician can usually reproduce this pain with the patient prone,
flexing the knee to 90° and externally rotating the
tibia, to put the nerve on stretch [45].
7
Physical Examination
The physical examination confirms the diagnosis
and helps determine the underlying causative
factors of the patient’s symptoms so the appropriate treatment can be implemented. By examining the patient’s standing position, the clinician
should have a fair indication of how the patient
will move. The clinician observes the patient
from the front, the side and from behind, noting
femoral orientation, foot posture, knee position
and muscle bulk. For example, femoral internal
rotation, a common finding in patients with
patellofemoral pain, is often associated with a
tight iliotibial band and poor hip muscle control,
which can adversely affect the articulation of the
patellofemoral joint and foot position. In weight
bearing, if a pronated foot position is seen, this
could be due to the foot compensating for many
proximal deformities or the foot itself may have
intrinsic issues causing pronation. The static foot
position influences lower limb control and
dynamic knee valgus. Additionally, if the patient
is standing with hyperextended or ‘locked back’
knees, this can irritate the IFP, a potential source
of diffuse knee pain symptoms and be indicative
that inner range (0–20° flexion) quadriceps control of the knee is poor.
Once the clinician has examined the patient in
standing, the clinician then observes the patient
during dynamic activities, commencing with the
least stress activity of walking and progressing to
stairs, squatting, and jumping if necessary. During
this process, the clinician is evaluating the effect of
muscle action on the limb mechanics. Table 2
summarises the dynamic implications of the static
findings. However, the prime aim of the dynamic
examination is to reproduce the patient’s symptoms, so if the symptoms are reproduced (>3 on
visual analogue scale (VAS) with walking, there is
no need to do further strenuous dynamic testing,
but if the symptoms are not reproduced, then the
clinician systematically increases the functional
load until they have a valid objective reassessment
activity to determine the effectiveness of their
Table 2 Dynamic implications of static findings
Foot
– Callus medial aspect great toe
– Enlarged 1st MTP
– Morton’s toe
Medial heel whip (unstable push off)
–
–
–
–
!
!
!
!
Stiff 1st MTP
Talus prominent medial
Straight calcaneum
Tight gastrocnemius
early heel off
prolonged pronation
stiff subtalar joint " subtalar pronation
early heel off
Knee
– Genu valgum
– Hyperextended/locked back
– Tight hamstrings
!" pronation
!# shock absorption
!# dorsiflexion !" pronation
Hip
– Internal femoral rotation
– Tight psoas
!# hip extension & external rotation
!# step length
Pelvis
– Anterior tilt
– Posterior tilt
– sway back
!# hip ext & ER, # step length, " LS rotation
!" pelvic tilt, poor glut med
! combination tilt & rotation
Management of Anterior Knee Pain from the Physical …
107
Table 3 Observation conclusions prior to analysing gait
•
•
•
•
•
•
•
•
If
If
If
If
If
If
If
If
hallux valgus or enlarged MTP ! unstable push off
talus prominent medial and straight or inverted calcaneum ! # shock absorption ! " pelvic instability
hyperextended/ locked back knees ± pudgy fat pads ! " pelvic instability
internal femoral rotation ! # hip extension and external rotation ! " pelvic rotation
anterior tilt pelvis ! # hip extension and external rotation ! " pelvic rotation
posterior tilt ! " lateral tilt of the pelvis
sway back ! combination of lateral tilt & rotation of pelvis
base of support > pelvis width ! lateral shift of trunk
treatment. Table 3 describes the analysis the
clinician performs before observing the patient’s
gait. When examining athletes often these
dynamic activities are not strenuous enough to
reproduce their symptoms, as longer duration
activities, such as running 15 kms, provoke
symptoms. In this situation the clinician can
evaluate the control of the one leg squat to determine the effect of treatment outcome.
On the examination table, the clinician aims to
reproduce the patient’s symptoms by palpating
the around knee, including joint lines IFP and
patella, as well as passively flexing and extending the knee with gentle overpressure. The clinician then examines the passive position of the
patella relative to the femur, the flexibility of
certain soft tissues such as anterior hip structures,
hamstrings, gastrocnemius, and iliotibial band, as
well as the relative strength of various muscles
such as hip rotators, quadriceps, and tibialis
posterior. It has been found however, that traditional nonweight-bearing (NWB) hip-strength
assessments may not directly translate to functional strength during weight-bearing (WB) activity [51]. Thus, the clinician is advised to
examine these muscles in a weight bearing
position, so they have an idea of the relative
control the muscle has over the lower extremity.
8
Treatment
Most patellofemoral conditions are successfully
managed with non-operative treatment. The aims
of the treatment are to unload the painful structures around the PF joint, so the patient realises
there is hope that their symptoms can be
improved; to improve the lower limb mechanics
to allow the patient to have long term control
over managing their symptoms; and to empower
the patient to self-manage their condition,
emphasising that the condition is managed not
cured. If, in the first treatment, the clinician can
decrease the patient’s symptoms by at least 50%,
the clinician has the patient’s buy-in, so compliance with treatment is almost always assured.
Load modification, particularly for the athletic
individual, may be necessary at the onset of
symptoms to minimize pain flares. Table 4 provides a decision-making algorithm for treatment
direction. For a more detailed picture of individualized clinically reasoned patient management, the reader is referred to the chapter ‘A
Multifaceted Presentation of Knee Pain in a
Forty-Year-Old Woman’ in Clinical reasoning in
musculoskeletal practice by Mark A Jones and
Darren A Rivett [46].
8.1 Unloading Pain
The immediate reduction in symptoms can be
achieved by unloading the painful structures
using tape (Fig. 1). Painful, inflamed tissue does
respond well to stretch, so the principle of
unloading painful tissue is to shorten the tissue,
so there is an opportunity for the inflammation to
decrease, promoting optimal repair. In this situation the most appropriate tape is a rigid nonstretch tape, as it provides support to the tissue,
but still allows knee joint movement. It has been
found in asymptomatic individuals, using elastography (supersonic shear imaging to measure
muscle shear elastic modulus), that unloading
tape reduces stress in the region underlying the
tape [52].
108
J. McConnell
Table 4 Decision making algorithm for treatment direction
1. # pain
(i) tape to unload painful tissues. Tape must make an immediate 50% decrease in symptoms
(ii) if patient is walking with knee flexed, as too painful to straighten knee, indicates inflamed IFP, so must unload—
no quads sets or SLRs as will increase pain and delay recovery
2. If knee is locking back or hyperextending during walking, then poor inner range quads control
(i) if condition irritable small ROM knee bends (0–30°), with soft, not locked back knees
(ii) progress to walk standing position, symptomatic knee in front, small ROM knee bends
(iii) show strategy of walking up and down stairs with a forward trunk lean- i.e., hip flexed position
(iv) to facilitate VMO activity, can inhibit VL and TFL with tape and tape patella medially
3. If dynamic knee valgus on step down
(i) check pelvic control (dynamic weight bearing gluteal control)—give subtle gluteal and trunk control training with
slight knee bend, in weight bearing simulating walking position
(ii) check dorsiflexion ROM (knee to wall test), If # then mobilise talocrural joint in WB
(iii) check navicular position, if foot excessively pronated, then may need orthotics, improved footwear with adequate
midfoot support (make sure laces are tied firmly), and foot exercises for tibialis posterior in WB ± intrinsic foot
muscles. Could tape to control midfoot position—helps decision for orthotics
4. If tight soft tissue structures
(i) anterior hip structures tight then prone Fig. 4 stretch
(ii) If hamstrings tight, then seated hamstrings stretch, sit tall with LS in neutral
(iii) if tight lateral structures, then STM lateral retinaculum, tilt tape
(iv) if tight gastrocnemius, then standing stretch off step control foot position
(v) if RF tight, then quads stretch care not to over-flex knee, as can aggravate symptoms
5. If you suspect CRPS
(i) explanation to patient about pain and central sensitisation
(ii) show patient how to desensitise area with different textures, do not focus on the knee
A
Fig. 1 Unloading the IFP. The patient is in supine with
the leg relaxed, if there is too much pain for the patient to
have their leg straight, then a small rolled up towel may be
placed under the knee. After tilting the patella out of the
IFP by commencing the tilt and glide tape half up on the
patella from the inferior pole. The clinician lifts the soft
B
tissue on the medial side of the tibial tubercle, to the
medial epicondyle (A) lifting the soft tissue towards the
patella to shorten the tissues and on the lateral side to the
lateral side of the joint, lifting the tissues towards the
patella. The clinician is aiming for a ‘muffin top’ effect
Management of Anterior Knee Pain from the Physical …
Taping the patella should be individualised to
each patient, so the optimal reduction in symptoms can be achieved. In many cases the patient’s
IFP is inflamed, so the clinician needs to ensure
that the inferior pole of the patella is tilted away
from the IFP so as not to further aggravate the
symptoms. This component must always be
identified and corrected first, usually with a
correction of a lateral tilt tape, so the patient’s
symptoms are not aggravated by positioning the
tape too low on the patella. If the patella is laterally tilted then the patella won’t be able to
engage well in the trochlea, so a lateral tilt correction must be performed before a glide correction. For effective sustained symptom
reduction, the tape needs to remain on the knee
and changed when it loosens. If the patient is
fairly sedentary, one taping application may last
a week, even with showering. However, if the
patient is playing sport and the skin becomes
sweaty, the tape may only last until the end of a
run or the game before it needs to be reapplied.
Thus, the patient needs to be taught how to tape
their own knee. This is done with the patient
sitting on the edge of a chair, leg extended and
relaxed, foot resting on the floor, so the patella is
mobile and can be more easily moved (Fig. 2).
The evidence in the literature about the
effectiveness of tape is mixed, whether using
Fig. 2 Self-tape. A The
patient sits on the edge of a
chair with the leg extended
and the knee relaxed, so they
can move the patella B The
patient is taught how to tape
their own knee
A
109
rigid or elasticised tape [53]. However, taping is
a means to an end, and as such, is an adjunct to
treatment. It was never meant to be used in isolation; it is part of the symptom management
program. If the tape does not reduce the symptoms by at least 50%, then the clinician needs to
consider whether: (1) the tape positioning was
correct—it could be too low on the patella,
causing an irritation of the fat pad; (2) the tape
application was poor—too much tension, resulting in skin breakdown or not enough tension,
resulting in taping that is ineffective and may as
well not be there; (3) the tape was applied in too
much knee flexion—if the knee is flexed >30°
then the patella is already lodged in the trochlea,
albeit not well aligned; (4) tape was not appropriate for that patient—you should not put tape
on the knee of anyone you suspect has complex
regional pain syndrome (CRPS), as it will make
them worse, or tape is inappropriate for someone
whose symptoms are only mild, and therefore,
aren’t bad enough to warrant taping.
An understanding of the effect of creep on
collagenous tissue helps explain some of the
rationale behind certain taping techniques. Creep
is the tendency of a viscoelastic material to
elongate during a sustained low load. So, if the
lateral retinacular tissues are tight, causing a tilt
of the patella, tilt tape can be used to provide a
B
110
J. McConnell
sustained low load on those tissues to progressively elongate them, while at the same time
shortening the medial structures to promote a
more effective VMO activation. Additionally,
tape can be used to facilitate muscle activity by
shortening the muscle and taping in the direction
of the muscle fibres, as well as to minimise
excessive muscle activity, by taping firmly across
the muscle belly. This can expedite symptom
improvement. Examples would be the use of tape
to facilitate external femoral rotation to decrease
dynamic knee valgus, taping the gluteals to
enhance gluteal activation, taping the mid foot to
facilitate tibialis posterior activity and taping
firmly across the VL and TFL to encourage
VMO and gluteal activity [54, 55]. Figure 3
demonstrates tape to minimise activity in TFL
and VL.
The clinician needs to be aware that tape use
can cause some skin problems: (1) namely
A
Fig. 3 A Inhibiting VL and distal ITB—firm tape across
the VL, just above the lateral patella—from posterior to
anterior thigh, making a pucker in the skin to squash the
muscle. May do another tape in the same direction higher
friction rub, which usually occurs on the medial
aspect of the knee, so even tension with the
application of tape and the careful removal of the
tape will minimize the risk; and (2) less commonly an allergic reaction where the use of
hypoallergenic creams or sprays to protect the
skin beneath the tape will decrease the possibility
of a skin rash.
8.2 Improving Dynamic Lower Limb
Loading
Focussing on a quadriceps strategy, a hip strategy, or a foot strategy in rehabilitation is unrealistic for the PF patient, as muscles work
synergistically to control the limb in weight
bearing and it is this subtle muscle control that
the patient has lost that needs to be restored. The
patient needs to realise that they are requiring
B
up the thigh, B Inhibiting TFL. On the muscle belly of
TFL, firmly taping across from anterior to posterior, again
making a pucker in the skin to squash the muscle
Management of Anterior Knee Pain from the Physical …
subtle changes in the motor program (body
management strategies) and as such it is not
necessarily strength changes, they need but the
right muscles at the right time. The clinician
needs to improve the synergistic patterning of the
lower limb muscles, so these muscles respond
quickly and dynamically to a new motor program. In individuals with pain, particularly in the
chronic situation, an abnormal motor pattern
becomes the normal, such that the strong muscles
become stronger, and the weak muscles stay
weak, as the strong will overpower the weak,
which will further enhance the imbalance and
increase the loading on the painful tissues. Hence
the need for the clinician to implement subtle
changes in the way the muscles are working
dynamically i.e., brain training. Synergic control
can be learned and modified. When learning a
new skill or modifying a previously learned skill,
cognitive processes contribute to the planning of
the movement performance; perception guides
the action; and synergies form between different
body components to allow flexible, yet stable
movement control [56]. It is only through
extensive practice that goal- relevant movement
solutions are established, so performance and
learning improve. Therefore, new movement
patterns are shaped by practice, as well as by
contextual factors where the practice takes place
[57]. So, practicing motor skills needs to be in
the specific context in which the behaviour is
intended to apply. Perception develops differently depending on the contextual properties in
which a motor skill is practiced, and generally
motor skills learned in the laboratory or lying on
the treatment table in a clinic transfer poorly to
contexts outside the controlled environment of
the lab or the clinic (i.e., the learned behaviour is
not functional to requirements outside the controlled environment) [58]. For example, for an
individual with PFP who is experiencing pain on
load bearing in an upright position, the training
needs to be performed in this context specific
position to ensure a change in the synergistic
patterning of the lower limb muscles to allow the
appropriate muscles to be strengthened (Fig. 4),
rather than lying on the table and lifting their leg
111
up in the air (i.e., doing SLRs), often with a
weight around the ankle.
It has been found that WB or closed kinetic
chain (CKC) training is more effective than open
chain exercises (OKC), as it promotes a more
simultaneous onset of EMG activity of the four
different muscle portions of the quadriceps
compared with OKC [58]. In OKC, RF activates
earliest, while the VMO is activated last with
smaller amplitude than in CKC, so CKC exercise
promotes a more balanced initial quadriceps
activation and increases the thickness of the
VMO, than OKC exercises [59]. Additionally,
CKC training allows simultaneous training not
only of the vasti but also the gluteals and trunk
muscles to control the limb position in WB [58].
In performing CKC squat exercises, the range
should be restricted to the inner range, not greater
than 45° of knee flexion to minimize PFJ stress
[60], but preferably only to 30° to enhance VMO
activation and improve the seating of the patella
in the trochlea. While performing these squats,
the patient needs to concentrate on their limb
alignment, as well as the control of the movement concentrically and eccentrically.
Improving control of lower limb mechanics
should therefore be individualised to each patient
depending on what was found on assessment.
Barton el al. [61] concluded that ‘an individually
tailored multimodal intervention programme
including gluteal and quadriceps strengthening,
patellar taping and an emphasis on education and
activity modification should be prescribed for
patients with PFP’. This has been validated in a
study by Keays et al. [62] who found that individualized treatment supplementing local standard physiotherapy for PFP lead to greater
improvement in symptoms. These authors felt
that recognition of different subgroups may guide
treatment that should include both local and
deficit-targeted global treatment. So, for example
if a patient exhibiting dynamic knee valgus on
stair decent is given hip strengthening exercises
without the clinician evaluating their dynamic
talocrural ROM, which if found to be restricted
on knee to wall test, the patient’s symptoms on
stairs will not change until the clinician mobilises
112
A
J. McConnell
B
C
Fig. 4 Training the standing leg to improve synergistic
control for walking, stairs and running. A To commence
the patient stands 45o to the wall, the NWB leg is bent up
with the knee touching the wall, for balance no pushing.
The patient’s weight is fully on the standing leg, with the
weight back through the heel, the knee slightly bent, and
the pelvis tucked under slightly. The patient stands tall
and externally rotates the standing leg thigh slightly
without moving the hip or the foot. The patient should
feel the standing leg gluteal is working. The patient holds
this position for 15 s. B This exercise can be progressed
by getting the patient to stand on a pillow, simulating an
unstable surface or rough ground, C The exercise can also
be progressed by adding an elasticised band, knotted and
then jammed in the door, tying a loop around the other
end for the NWB (unaffected) ankle. The patient pulls the
band forward and back, while maintaining the position
described in 4a to simulate running
the talocrurual joint in weight bearing to increase
the dynamic dorsiflexion range (Fig. 5). The
clinician can help the patient maintain the range
by showing the patient how to self-mobilise
using a seat belt and giving the patient foot
exercises to improve the control of the foot.
Addition of an intervention program consisting
of short foot exercises has been shown to have
positive effects on knee pain, navicular position,
and rearfoot posture [63]. Kısacık et al. [63]
suggested that the increase in the strength of the
hip extensors could be associated with improved
stabilization afforded by the foot musculature.
Alternatively, the clinician could give the patient
a heel raise to decrease the amount of dorsiflexion required, or an orthosis to decrease the
compensatory pronation. In this case, the clinician has made the ground different to the foot,
whereas mobilising the talocrural joint or training
the foot musculature makes the foot look different to the ground. Each can be effective- one is
dynamic control; the other is passively changing
the starting position.
Thus, an evidence-based, holistic approach
should include a graded exposure to load with
the patient’s activities and exercise, as well as
consider other factors such as diet to additionally
decrease load, sleep quality and quantity, and
external stressors (psychosocial factors). So perhaps, when clinicians are assessing who will
benefit from what strategy, clinicians also need to
examine patient compliance and motivation to do
the exercise program (daily strategies). Compliance to exercise is poor, if the patient experiences
increased pain during exercise therefore, strategies to decrease initial pain are important. As
some patients may not be as motivated as others,
perhaps they would do better in the longer term,
Management of Anterior Knee Pain from the Physical …
A
113
B
Fig. 5 A Mobilising the talocrural joint in weight bearing with a seat belt. B Self mobilisation
with an orthosis rather than do foot exercises or a
knee brace rather than do weight bearing functional exercises, as using an external device is
simple, taking little time or effort. However,
compliance can be an issue with orthotic use,
with comfort of the orthotic a key factor in
improving compliance.
When examining the effectiveness of randomized controlled trials, patients are most
compliant in the initial period, so effectiveness of
physiotherapy intervention should be evaluated
at the end of the physio intervention [64]. At
follow up the majority of patients are partially
compliant, but the treatment effect is diluted by
those who were not compliant [64]. Campbell
et al. [64] suggest that clinicians should move
away from viewing patients as either compliers
or non-compliers with therapy, but to include
them as partners in rational decisions about
therapy. This would be particularly true of the
adolescent age group, who are notoriously noncompliant with exercise. Continued compliance
is an interplay between the condition (knee pain),
perception about the cause of the pain and the
underlying consequence of persistent chronic
pain with catastrophizing, kinesiophobia,
depression, and belief that the intervention could
be effective, as well as the motivation, willingness, and ability to incorporate the exercises into
everyday life. This is why, in a maintenance
program, the exercises must be easy to do, need
no equipment, not be too many (maximum of 4),
taking no more than 5 min, so they can be
incorporated into everyday life. Empowering the
patient to self-manage and have control is critical
to the success of PFP management or any chronic
musculoskeletal condition for that matter.
The most compliant patients want some further input from the physiotherapist, rather than
just being discharged (i.e., a body service every
6 months, just like a car service) [64]. A recent
study of a 6-week internet-based exercise program for PF pain without seeing a clinician,
resulted in only 8% of enrolled participants
completing the program (860 initially, 70 completed), highlighting the need for a therapist
involved approach for patients with PF pain [65].
8.3 Treatment Progression
Once the patient’s day to day symptoms are more
under control, the clinician needs to help the
patient incorporate increased knee loading and
endurance into their activity program. This will
necessitate establishing what activities the patient
likes to do, whether it be walking, running,
cycling, or swimming. Some patients enjoy and
114
benefit from the routine and camaraderie of a
group exercise class, whether it be aquarobics,
Pilates, yoga, boxing or a spin or pump class.
Participation in the class should be encouraged,
provided the patient can learn to pace themselves
i.e., don’t do too many classes in a week; and
learn to minimize the extremes of range and load
in the exercise, as well as to recognize the
warning signs of overdoing it, such as when the
muscles are fatiguing. Organized exercises classes have huge benefits for mental health, and as
such can help minimize some of the psychosocial
effects of the patient’s symptoms.
As many patients experience pain during stair
ascent and descent, one of the aims of treatment is
to improve the patient’s ability to negotiate stairs
without reproducing symptoms. The patients
need to practice stepping up and down, initially
using a small step, perhaps with a forward trunk
lean and flexed hips to minimize the stress on the
PF joint, then they can progress to a more upright
position, practicing in front of a mirror so that
changes in limb alignment can be observed and
deviations can be observed and corrected. Some
patients may be able to do only a small number of
repetitions with correct lower limb alignment.
Since inappropriate practice can be detrimental to
learning, using a small number of exercises with
correct alignment is sufficient until the patient can
perform larger numbers, pain-free and with correct lower limb alignment. Initially, a small
number of exercises should be performed frequently throughout the day. The number of repetitions should be increased as the symptoms
decrease, and the endurance improves. For further
progression, the patient can move to a larger step,
initially decreasing the number of contractions
and then slowly increasing them again. As the
control improves, the patient can alter the speed
of their stepping activity and may vary the place
on descent where they stop going down. To
increase the load, the addition of weights in the
hands or in a backpack on the back may gradually
be introduced, but with the addition of increased
weight, repetitions and movement speed should
J. McConnell
be decreased, then as control and symptoms
improve built back up again.
The aim of retraining is to make the transition
from functional exercises to functional activities.
When advising about power walking or running,
the clinician can suggest to the patient to imagine
that someone is pushing them forward in the
shoulder blade area. This results in a more mid to
forefoot strike pattern, which should decrease PF
joint stress [66]. Implementation of forefoot
strike training programs has been found to be
helpful in the treatment of runners with patellofemoral pain [66]. However, it is suggested that
the transition to a forefoot strike pattern should
be completed in a graduated manner, as this
strike pattern can overload the Achilles tendon
[66]. Training should also be applicable to the
patient’s activities/sport, so that a jumping athlete, for example, should have jumping incorporated in the program. Plyometric routines such
as bounding, jumping and turning, jumping off
boxes, are an important part of rehabilitation for
the high-performance athlete before they return
to their sport.
Once a more balanced activation pattern of the
quadriceps has been established, an extremely
beneficial method of improving quadriceps
strength is cycling, as this does not load the PF
joint as much as running sports, particularly if the
activity of the VL is minimized, so a more even
quadriceps loading can be attained. Quadriceps
strength deficits, particularly medial quadriceps,
have been implicated in the research on causes of
PF pain [32, 48] and the development of knee
osteoarthritis [67].
Endurance training is also essential to ensure
more resilience for the patient. The number of
repetitions performed by the patient at a training
session depends upon the onset of muscle fatigue.
Initially, it is important to emphasize quality and
not quantity, progressing to increase the number
of repetitions before the onset of fatigue. Patients
should be taught to recognize muscle fatigue or
quivering, so that they do not train through the
fatigue and risk exacerbating their symptoms.
Management of Anterior Knee Pain from the Physical …
9
Conclusion
To effectively help a patient manage their PF
symptoms, the clinician initially needs to explain
to patient (1) why they have pain and where their
symptoms are coming from; (2) to understand the
patient’s goals; and (3) to help manage their
expectations. In treatment, it is imperative that
the clinician helps the patient manage their
symptoms by showing them how to unload their
painful structures and improve dynamic limb
loading which involves weight bearing hip, knee,
and foot muscle training. The clinician needs to
emphasise that PFP is not cured but is managed
by ensuring that the exercise regime is incorporated into the patient’s daily routine. The exercises should only take five minutes otherwise the
patient is unlikely to continue with the exercises.
The patient needs to realise that to keep the knee
in “good health”, these exercises are like cleaning their teeth—essential part of body maintenance. No more than four, but preferably three
exercises should be given as maintenance training, where no equipment is needed so the patient
can do the exercises at any time and place. The
patient should be encouraged to participate in
regular other exercise that they enjoy, as it is a
prudent way of ensuring ongoing knee and
general wellness. Patients need advice on how to
stand, so as not to overload their soft tissue
structures (modified ballet 3rd position (Fig. 6),
except for patients with large genu varum, as
they cannot get their legs to touch) and how to
get out of a chair without using their hands,
keeping their knees over their feet. The clinician
needs to encourage the patient to be actively
engaged in their rehabilitation. A follow up every
6 or 12 months for wellness maintenance
demonstrates to the patient that you, the clinician, are part of their team and are wanting a
continued, successful outcome for them.
10
115
Take-Home Messages
(1) AKP is managed, not cured, and
requires ongoing maintenance to prevent
recurrences.
Fig. 6 Modified ballet 3rd position, legs touching, soft
knees
(2) Understand the patient’s goals and expectations and help manage their expectations.
(3) Knowledge is power, so you need to give an
appropriate explanation to the patient about
where their symptoms are coming from, the
causative factors, and what they can do to
help.
(4) Provide an individualized management
program tailored to each patient, based on
assessment of their issues.
116
J. McConnell
(5) Emphasize that you and the patient are a
team, and your role is to empower the
patient to self-manage.
(6) You need to keep seeing the patient every 6
or 12 months, as part of a continued management plan, to ensure their continued
well-being.
11
Key-Message
(1) AKP is managed, not cured, and requires
ongoing
maintenance
to
prevent
recurrences.
References
1. Dragoo JL, Johnson C, McConnell J. Evaluation and
treatment of disorders of the infrapatellar fat pad.
Sports Med. 2012;42:51–67.
2. Sanchis-Alfonso V, Rosello-Sastre E. Immunohistochemical analysis for neural markers of the lateral
retinaculum in patients with isolated symptomatic
patellofemoral malalignment. Am J Sport Med.
2000;28:725–31.
3. Dye SF, Chew MH. The use of scintigraphy to detect
increased osseous metabolic activity about the knee.
J Bone Joint Surg (Am). 1993;75A:1388–1406.
4. Leese J, Davies D. An investigation of the anatomy
of the infrapatellar fat pad and its possible involvement in anterior pain syndrome: a cadaveric study.
J Anat. 2020;237(1):20–28.
5. Bohnsack M, Meier F, Walter GF, Hurschler C,
Schmolke S, Wirth CJ, Rühmann O. Distribution of
substance-P nerves inside the infrapatellar fat pad
and the adjacent synovial tissue: a neurohistological
approach to anterior knee pain syndrome. Arch
Orthop Trauma Surg. 2005;125(9):592–7.
6. Stephen JM, Sopher R, Tullie S, Amis AA, Ball S,
Williams A. The infrapatellar fat pad is a dynamic
and mobile structure, which deforms during knee
motion, and has proximal extensions which wrap
around the patella. Knee Surg Sports Traumatol
Arthrosc. 2018;26(11):3515–3524.
7. Bohnsack M, Hurschler C, Demirtas T, Rühmann O,
Stukenborg-Colsman C, Wirth CJ. Infrapatellar fat
pad pressure and volume changes of the anterior
compartment during knee motion: possible clinical
consequences to the anterior knee pain syndrome.
Knee Surg Sports Traumatol Arthrosc. 2005;13
(2):135–41.
8. Bennell K, Hodges P, Mellor R, Bexander C,
Souvlis T. The nature of anterior knee pain following
injection of hypertonic saline into the infrapatellar fat
pad. J Orthop Res. 2004;22(1):116–21.
9. Hodges PW, Mellor R, Crossley K, Bennell K. Pain
induced by injection of hypertonic saline into the
infrapatellar fat pad and effect on coordination of the
quadriceps muscles. Arthritis Rheum. 2009;61:70–7.
10. Henriksen M, Alkjaer T, Lund H, Simonsen EB,
Graven-Nielsen T, Danneskiold-Samsøe B, Bliddal H. Experimental quadriceps muscle pain impairs
knee joint control during walking. J Appl Physiol
(1985). 2007;103(1):132–9.
11. Vadivelu N, Kai AM, Kodumudi G, Babayan K,
Fontes M, Burg MM. Pain and psychology-a reciprocal relationship. Ochsner J Summer. 2017;17
(2):173–80.
12. Mann EG, Harrison MB, LeFort S, VanDenKerkhof
EG. What are the barriers and facilitators for the selfmanagement of chronic pain with and without
neuropathic characteristics? Pain Manag Nurs
2017;18(5):295–308.
13. Maclachlan LR, Collins NJ, Hodges PW, Vicenzino B. Psychological and pain profiles in persons
with patellofemoral pain as the primary symptom.
Eur J Pain. 2020;24(6):1182–1196.
14. Senavongse W, Amis AA. The effects of articular,
retinacular, or muscular deficiencies on patellofemoral joint stability: a biomechanical study in vitro.
J Bone Joint Surg Br. 2005;87(4):577–82.
15. McConnell J. Promoting effective segmental
alignment. In Key issues in musculoskeletal physiotherapy, Eds Crosbie J. McConnell J. Oxford, Butterworth—Heinemann; 1993.
16. Amis AA, Senavongse W, Bull AM. Patellofemoral
kinematics during knee flexion-extension: an in vitro
study. J Orthop Res. 2006;24(12):2201–11.
17. Grob K, Manestar M, Filgueira L, Kuster MS,
Gilbey H, Ackland T. The interaction between the
vastus medialis and vastus intermedius and its
influence on the extensor apparatus of the knee joint.
Knee Surg Sports Traumatol Arthrosc. 2018;26
(3):727–738.
18. Smith TO, Nichols R, Harle D, Donell ST. Do the
vastus medialis obliquus and vastus medialis longus
really exist? A systematic review. Clin Anat. 2009;22
(2):183–99.
19. Rajput HB, Rajani SJ, Vaniya VHJ. Variation in
morphometry of vastus Medialis Muscle. Clin Diagn
Res. 2017;11(9)–24.
20. Castanov V, Hassan SA, Shakeri S, Vienneau M,
Zabjek K, Richardson D, et al. Muscle architecture of
vastus medialis obliquus and longus and its functional implications: a three-dimensional investigation. Clin Anat. 2019;32(4):515–523.
21. Benjafield AJ, Killingback A, Robertson CJ,
Adds PJ. An investigation into the architecture of
the vastus medialis oblique muscle in athletic and
Management of Anterior Knee Pain from the Physical …
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
sedentary individuals: an in vivo ultrasound study.
Clin Anat. 2015;28(2):262–8.
Sheehan FT, Borotikar BS, Behnam AJ, Alter KE.
Alterations in in vivo knee joint kinematics following
a femoral nerve branch block of the vastus medialis:
Implications for patellofemoral pain syndrome. Clin
Biomech. 2012;27(6):525–31.
Cowan SM, Bennell KL, Hodges PW, Crossley KM,
McConnell J. Delayed onset of electromyographic
activity of vastus medialis obliquus relative to vastus
lateralis in subjects with patellofemoral pain syndrome. Arch Phys Med Rehabil. 2001;82(2):183–9.
Mellor R, Hodges P. Motor unit synchronization
between medial and lateral vasti muscles. Clin
Neurophysiol. 2005;116(7):1585–95.
Mellor R, Hodges PW. Motor unit synchronization is
reduced in anterior knee pain. J Pain. 2005;6
(8):550–8.
Chester R, Smith TO, Sweeting D, Dixon J, Wood S,
Song F. The relative timing of VMO and VL in the
aetiology of anterior knee pain: a systematic review
and meta-analysis. BMC Musculoskelet Disord.
2008;9:64.
Grant C, Fick CN, Welsh J, McConnell J, Sheehan
FT. A word of caution for future studies in
patellofemoral pain: a systematic review with metaanalysis. Am J Sports Med. 2021;49(2):538–551.
Alzahrani AM, Alzhrani M, Alshahrani SN,
Alghamdi W, Alqahtani M, Alzahrani. Is hip muscle
strength associated with dynamic knee valgus in a
healthy adult population? a systematic review. H. Int
J Environ Res Public Health. 2021;18(14):7669.
Hoglund LT, Burns RO, Stepney AL. Do males with
patellofemoral pain have posterolateral muscle weakness Jr. Int J Sports Phys Ther. 2018;13(2):160–170.
O’Sullivan K, Herbert E, Sainsbury D, McCreesh K,
Clifford AJ. No difference in gluteus medius activation in women with mild patellofemoralpain. Sport
Rehabil. 2012;21(2):110–8.
Rathleff MS, Rathleff CR, Crossley KM, Barton CJ. Is
hip strength a risk factor for patellofemoral pain? A
systematic review and meta-analysis.Br J Sports
Med. 2014;48(14):1088.
Neal BS, Lack SD, Lankhorst NE, Raye A, Morrissey D, van Middelkoop M. Risk factors for
patellofemoral pain: a systematic review and metaanalysis. Br J Sports Med. 2019;53(5):270–281.
Rabelo NDDA, Lucareli PRG. Do hip muscle
weakness and dynamic knee valgus matter for the
clinical evaluation and decision-making process in
patients with patellofemoral pain? Braz J Phys Ther.
2018;22(2):105–9.
Baldon Rde M, Serrão FV, Scattone Silva R,
Piva SR. Effects of functional stabilization training
on pain, function, and lower extremity biomechanics
in women with patellofemoral pain: a randomized
clinical trial. J Orthop Sports Phys Ther. 2014;44
(4):240–251.
Fong CM, Blackburn JT, Norcross MF, McGrath M,
Padua DA Ankle-dorsiflexion range of motion and
117
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
landing biomechanics. J Athl Train. 2011;46
(1):5–10.
Lima YL, Ferreira VMLM, de Paula Lima PO,
Bezerra MA, de Oliveira RR, Almeida GPL. The
association of ankle dorsiflexion and dynamic knee
valgus: a systematic review and meta-analysis. Phys
Ther Sport. 2018;29:61–69.
Bell-Jenje T, Olivier B, Wood W, Rogers S,
Green A, McKinon W. The association between loss
of ankle dorsiflexion range of movement, and hip
adduction and internal rotation during a step down
test. Man Ther. 2016;21:256–61.
Neal BS, Griffiths IB, Dowling GJ, Murley GS,
Munteanu SE, Franettovich Smith MM, et al. Foot
posture as a risk factor for lower limb overuse injury:
a systematic review and meta-analysis. Foot Ankle
Res. 2014;7(1):55.
Kedroff L, Galea Holmes MN, Amis A,
Newham DJ. Effect of patellofemoral pain on foot
posture and walking kinematics. Gait Posture.
2019;70:361–369.
Matthews M, Rathleff MS, Claus A, McPoil T,
Nee R, Crossley KM, et al. Does foot mobility affect
the outcome in the management of patellofemoral
pain with foot orthoses versus hip exercises? A
randomised clinical trial. Br J Sports Med. 2020;54
(23):1416–1422.
Barton CJ, Menz HB, Crossley KM. Clinical
predictors of foot orthoses efficacy in individuals
with patellofemoral pain. Med Sci Sports Exerc.
2011;43(9):1603–10.
Hart HF, Crossley KM, Bonacci J, Ackland DC,
Pandy
MG,
Collins
N.
Immediate effects of foot orthoses on gait biomechanics in individuals with persistent patellofemoral pain. J. Gait
Posture. 2020;77:20–28.
Schindler OS, Scott WN Basic kinematics and
biomechanics of the patello-femoral joint. Part 1:
The native patella. Acta Orthop Belg. 2011;77
(4):421–31.
Dye S. The knee as a biologic transmission with an
envelope of function: a theory. Clin Orthop.
1996;325:10–8.
McConnell J. The physical therapist’s approach to
patellofemoral disorders.Clin Sports Med. 2002;21
(3):363–87.
McConnell J, Rivett D. A multifaceted presentation
of knee pain in a forty-year-old female in Jones M,
Rivett D, Clinical Reasoning in Musculoskeletal
Practice. 2nd ed. London: Elesvier; 2019.
Robertson CJ, Hurley M, Jones F. People’s beliefs
about the meaning of crepitus in patellofemoral pain
and the impact of these beliefs on their behaviour: a
qualitative study. Musculoskelet Sci Pract.
2017;28:59–64.
Spencer JD, Hayes KC. Alexander I Knee joint
effusion and quadriceps reflex inhibition in man.
J Arch Phys Med Rehabil. 1984;65(4):171–7.
Tayfur B, Charuphongsa C, Morrissey D, Miller SC.
Neuromuscular function of the knee joint following
118
50.
51.
52.
53.
54.
55.
56.
57.
58.
J. McConnell
knee injuries: does it ever get back to normal? a
systematic review with meta-analyses. Sports Med.
2021;51(2):321–338.
Amestoy J, Pérez-Prieto D, Torres-Claramunt R,
Sánchez-Soler JF, Leal-Blanquet J, Ares-Vidal J,
et al. Patellofemoral pain after arthroscopy: muscle
atrophy is not everything. Orthop J Sports Med.
2021;9(6):1–8.
Freemyer BG, Urbi A, Torigoe T, Stickley C.
Weight-bearing versus traditional strength assessments of the hip musculature. J Athl Train. 2021;56
(2):191–6.
Hug F, Ouellette A, Vicenzino B, Hodges PW,
Tucker K. Deloading tape reduces muscle stress at
rest and during contraction. Med Sci Sports Exerc.
2014;46(12):2317–25.
Logan CA, Bhashyam AR, Tisosky AJ, Haber DB,
Jorgensen A, Roy A, Provencher MT. Systematic
review of the effect of taping techniques on
patellofemoral pain syndrome. Sports Health.
2017;9(5):456–461.
Song CY, Huang HY, Chen SC, Lin JJ, Chang AH.
Effects of femoral rotational taping on pain, lower
extremity kinematics, and muscle activation in
female patients with patellofemoral pain. J Sci Med
Sport. 2015;18(4):388–93.
Kilbreath SL, Perkins S, Crosbie J, McConnell.
Gluteal taping improves hip extension during stance
phase of walking following stroke. J.Aust J Physiother. 2006;52(1):53–6.
Latash ML. Understanding and synergy: a single
concept at different levels of analysis? Front Syst
Neurosci. 2021;15:735406.
Oppici L, Grütters K, Garofolini A, Rosenkranz R,
Narciss S. Deliberate practice and motor learning
principles to underpin the design of training interventions for improving lifting movement in the
occupational sector: a perspective and a pilot study
on the role of augmented feedback. Front Sports Act
Living. 2021;3:746142.
Stensdotter AK, Hodges PW, Mellor R, Sundelin G,
Hager-Ross C. Quadriceps activation in closed and in
open kinetic chain exercise. Med Sci Sports Exerc.
2003;35(12):2043–7.
59. Cheon S, Lee JH, Jun HP, An YW, Chang E. Acute
effects of open kinetic chain exercise versus those of
closed kinetic chain exercise on quadriceps muscle
thickness in healthy adults. Int J Environ Res Public
Health. 2020;17(13):4669.
60. Powers CM, Ho KY, Chen YJ, Souza RB, Farrokhi S.
Patellofemoral joint stress during weight-bearing and
non-weight-bearing quadriceps exercises. J Orthop
Sports Phys Ther. 2014;44(5):320–7.
61. Barton CJ, Lack S, Hemmings S, Tufail S, Morrissey D. The ‘best practice guide to conservative
management of patellofemoral pain’: incorporating
level 1 evidence with expert clinical reasoning. Br J
Sports Med. 2015;49(14):923–34.
62. Keays SL, Mason M, Newcombe PA. Individualized
physiotherapy in the treatment of patellofemoral
pain. Physiother Res Int. 2015;20(1):22–36.
63. Kısacık P, Tunay VB, Bek N, Atay ÖA, Selfe J,
Karaduman AA. Short foot exercises have additional
effects on knee pain, foot biomechanics, and lower
extremity muscle strength in patients with patellofemoral pain. J Back Musculoskelet Rehabil. 2021;34
(6):1093–104.
64. Campbell R, Evans M, Tucker M, Quilty B,
Dieppe P, Donovan JL. Why don’t patients do their
exercises? Understanding non-compliance with physiotherapy in patients with osteoarthritis of the knee.
J Epidemiol Community Health. 2001;55(2):132–8.
65. Kim TWB, Gay N, Khemka A, Garino J. Internetbased exercise therapy using algorithms for conservative treatment of anterior knee pain: a pragmatic
randomized controlled trial. JMIR Rehabil Assist
Technol. 2016;3: e12.
66. Vannatta CN, Kernozek TW. Patellofemoral joint
stress during running with alterations in foot strike
pattern. Med Sci Sports Exerc. 2015;47(5):1001–8.
67. Wang Y, Wluka AE, Berry PA, Siew T, Teichtahl AJ,
Urquhart DM, et al. Increase in vastus medialis crosssectional area is associated with reduced pain, cartilage
loss, and joint replacement risk in knee osteoarthritis.
Arthritis Rheum. 2012;64(12):3917–25.
Targeted Treatment in Anterior Knee
Pain Patients According
to Subgroups Versus Multimodal
Treatment
James Selfe
1
Introduction and Background
The current best evidence-based non-surgical
treatment for patellofemoral pain (PFP) is multimodal therapy, core components of this
approach include, but are not limited to, a diverse
mix of exercise therapy (e.g. strengthening,
stretching); patellar taping or bracing; foot
orthoses [1]. However, multimodal therapy is not
uniformly applied either in clinical practice or
across research studies [1, 2] and there is limited
evidence supporting the longer-term outcomes of
this approach [3–6]. In view of the reported poor
long-term success of the non-surgical multimodal
approach, alternative solutions have been sought,
and support for developing stratified care using
diagnostic subgrouping with matched interventions for PFP has grown. This mirrors a broader
trend in the management of other musculoskeletal conditions such as, low back pain
where stratified care has proved effective for
optimising patient outcomes [7, 8]. Currently,
J. Selfe (&)
Faculty of Health and Education, Department of
Health Professions, Manchester Metropolitan
University, Manchester, UK
e-mail: J.Selfe@mmu.ac.uk
Visiting Academic in Physiotherapy Studies,
Satakunta University of Applied Sciences, Pori,
Finland
however, within the field of PFP there is limited
evidence as to whether a stratified care approach
improves patient outcomes. This is mostly due to
there being no consensus on what the most
important diagnostic subgroups are from a nonsurgical clinical perspective. This chapter
reviews the current state of knowledge for
PFP subgrouping and introduces readers to
some of the modern methodological approaches
employed to derive subgroups.
2
Complex PFP Stratification
Frameworks
Although interest in personalised medicine and
stratified care has risen in recent years and the
associated methodological approaches to stratified care and subgroup identification have
advanced considerably, the concept of identifying subgroups within the PFP population is not
new. For example, Holmes and Clancy in 1998
(p. 299), (14) when discussing the management
of PFP patients [9], argued that:
an adequate classification system should aid in
proper diagnosis and treatment of specific problems. If properly devised, it should also aid in the
comparison of results between different treatment
centres. In addition, it should be a system that is
simple and useful in the clinical setting with
minimal use of complicated imaging techniques.
However, it can be seen in Table 1 that many
attempts at producing stratification frameworks
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_8
119
120
J. Selfe
Table 1 Complex stratification frameworks containing multiple PFP subgroups (Adapted from Selfe et al. [10])
Author/s
Groups and subgroups
Merchant [11]
5 major groups
• Trauma
• Patellofemoral dysplasia
• Idiopathic chondromalacia patellae
• Osteochondritis dissecans
• Synovial plicae
Subgroups described for each of these specific conditions
(Total = 38 subgroups)
Wilk et al. [12]
8 major groups
• Patellar compression syndromes
• Patellar instability
• Biomechanical dysfunction
• Direct patellar trauma
• Soft tissue lesions
• Overuse syndromes
• Osteochondritis diseases
• Neurologic disorders
Subgroups described for some of these specific conditions
Treatment suggestions for each of the 8 major groups briefly discussed
(Total = 26 subgroups)
Holmes and Clancy
[9]
3 Major groups
• Patellofemoral instability
• PFP with malalignment but no episodes of instability
• PFP without malalignment
Subgroups described for each of these specific conditions
(Total = 60 subgroups)
Witvrouw et al. [13]
2 Major groups
5 Minor groups
• Malalignment
– Malalignment of entire leg
– Malalignment of Patellofemoral Joint (PFJ)
• Muscular dysfunction
– Strength deficit
– Neuromuscular dysfunction
–Flexibility
Subgroups described for some of these specific conditions
Evidence-based treatment recommendations presented
(Total = 13 subgroups)
Powers et al. [14]
3 Major groups
4 Minor groups
• Reduced cartilage thickness
• Decreased PFJ contact area
–Patella malalignment or tracking
• Increased PFJ reaction forces
– Altered tibiofemoral joint kinematics
– Muscle tightness
– Altered tibiofemoral joint kinetics
Literature review and international expert consensus statement on the evidence supporting
each subgroup
(Total = 15 subgroups)
Targeted Treatment in Anterior Knee Pain Patients According …
for PFP, have resulted in complex systems,
generating multiple subgroups that often rely on
using specialist high-cost equipment for identification. These complex stratification frameworks
may be very useful in highly specialised clinical
settings and they may also be good for guiding
research activity but in routine clinical practice a
stratification framework with a double-digit
number of PFP subgroups is unlikely to be
readily adopted.
Recent methodological frameworks on
designing subgrouping studies provide further
understanding on why many of the attempts to
subgroup patients in PFP have not translated well
into clinical practice, some of these are discussed
in the next section. The PROGRESS partnership
[15] provides some broad recommendations and
the Medical Research Council (MRC) [16] provides a framework on development, design and
analysis in stratification research (Fig. 1).
An important issue stressed in both the
PROGRESS recommendations [15] and the
MRC framework [16] is the consideration
throughout the research process of the clinical
relevance, especially if the purpose of the
121
identification of subgroups is to improve treatment outcomes. Therefore, researchers need to
consider the feasibility and acceptability of
implementing the test and the treatment from
both patient and health professional perspectives.
This helps direct the choice of how many and
which tests to use, test thresholds or cut point
scores for allocation of patients to subgroups and
the overall number of subgroups. Table 1 highlighted one of the key limitations in the search
for PFP subgroups to date i.e., each of these
stratification frameworks has generated a doubledigit number of subgroups the complexity of
which limits their clinical utility.
3
Simple PFP Stratification
Frameworks
Table 2 presents six PFP papers that have proposed much simpler stratification frameworks
resulting in either 3 or 4 subgroups.
Although employing differing methodologies
and including slightly different and heterogenous
populations there are some notable areas of
Fig. 1 Key steps in stratification and subgrouping research based on PROGRESS partnership recommendations [15]
and MRC [16] framework
122
Table 2 Simple
stratification frameworks
containing low numbers of
PFP subgroups (Adapted
from Selfe et al. [10])
J. Selfe
Author/s
Groups and Subgroups
Post [17]
2 Major groups
• Unstable PFJ (surgery required)
• Stable PFJ
– Extremity alignment
– Soft tissue mobility/flexibility
– Dynamic control
(Total = 4 subgroups)
Selhorst et al. [18]
Elevated fear avoidance
Decreased muscle flexibility
Functional malalignment
Decreased muscle strength
(Total = 4 subgroups)
Keays et al. [19]
Hypermobility
Hypomobility
Faulty movement pattern
Osteoarthritis
(Total = 4 subgroups)
Selfe et al. [20]
Strong
Weak and Tight
Weak and Pronated
(Total = 3 subgroups)
Drew et al. [21]
Strong
Pronation and Malalignment
Weak
Flexible
(Total = 4 subgroups)
Willy et al. [22]
Overuse/Overload
Muscle Performance deficits
Movement coordination deficits
Mobility impairments (hyper/hypomobile)
(Total = 4 subgroups)
Also need to consider
– Tissue Irritability
– Psychological Factors
overlap in the proposed subgroups in Table 2
with all papers suggesting a subgroup related to
abnormal muscle length/flexibility. The key
muscles of interest are the lower limb biarticular
muscles.
• Rectus femoris
• Hamstrings group
• Gastrocnemius
During gait there is a simultaneous concentric
and eccentric contraction at the opposite ends of
these biarticular muscles which is overlayed
onto and coordinated with uniarticular muscle
contraction to enable smooth locomotion.
The sophistication and complexity of the
neurophysiological control mechanism that
enables this to occur is remarkable and so it is
therefore unsurprising that these muscles are
often implicated in PFP. With respect to the
PROGRESS recommendations [15] and
the MRC framework [16] (Fig. 1) muscle length
tests represent good candidates to include in a
PFP subgrouping model. As described above
there is a strong mechanobiologic rational for
including them, there are objective data on
important clinimetric properties such as validity,
reliability and there are thresholds/cut points to
define excess tightness or excess flexibility
which could help guide subgroup allocation. In
Targeted Treatment in Anterior Knee Pain Patients According …
addition, from a clinical perspective muscle
length tests are feasible and acceptable to both
patients and clinicians, they are routine tests
familiar to most clinicians, they are quickly
performed and they require very low-cost measurement tools such as goniometers or tape
measures to collect the relevant data.
Most of the papers in Table 2 also refer to a
muscle strength subgroup usually including the
quadriceps femoris and various combinations of
the muscles around the hip that provide proximal
control of the femur. The majority of the preceding points supporting the candidacy of muscle
length as a potentially important clinical subgroup of PFP also apply to muscle strength. The
main difference is that the tools for measuring
muscle strength in clinical environments such as
hand-held dynamometers although overall not
high cost are more expensive than those required
to measure muscle length and are therefore not as
readily available in all clinical settings.
The other main area of consensus is the
emergence of a ‘kinematic’ subgroup, which is
referred to by a variety of descriptive nonscientific names i.e. dynamic control [17], functional mal-alignment [18], faulty movement pattern [19], movement coordination [22]. As
physiotherapy sits firmly within an exercise and
movement paradigm it is not surprising to see the
emergence of a kinematic subgroup and from a
clinical perspective many clinicians would
expect to see a movement related subgroup of
PFP patients. However, whilst there may be a
high degree of ecological validity and clinical
acceptability for a kinematic subgroup there are
currently a number of technical challenges to
establishing this as a viable PFP subgroup. These
relate mostly to Stage 3 in Fig. 1 which refers to
test measurement properties such as what is the
level of validity and reliability of the tests used to
assess kinematic deficit? and what thresholds/cut
points should be used to define the extent of the
deficit? In the field of measuring kinematics
complex and expensive three-dimensional
motion analysis systems may provide some
answers [23] but these are unlikely to become
routinely used in clinical practice. Simple to use,
low-cost clinical systems have yet to be well
123
developed, and although there is promising work
around the use of mobile digital technology such
as phones and tablets [24, 25], these approaches
have not yet been subjected to large scale testing.
It is also important to consider what the interrelationships may be between kiniesiophobia,
faulty kinematics and muscle strength. For
example it would be anticipated patients who are
‘weak’ would demonstrate poor kinematics but
equally in those patients who are strong it may be
important to remember the famous Pirelli tyre
advertisement that stated.
Power is nothing without control.
Virtually all the subgroups listed in Tables 1
and 2 are based on physical or biomechanical
factors. Only one paper [18] lists a specific
psychosocial subgroup and only one other [22]
mentions that psychosocial factors should be
considered. It is also interesting to consider that
no papers refer to any physiological subgroups,
only one paper [22] mentions that tissue irritability should be considered. In light of the wellestablished Tissue Homeostasis Model [26, 27]
and its extension the Neural Model [28] it is
perhaps surprising to see no potential physiological subgroups listed in either Table 1 or 2.
Step 2 in Fig. 1 probably explains the reason for
this, as defining specific relevant physiological
variables that would be relatively easy to measure from a clinical perspective is challenging.
4
Targeted Intervention
for Patellofemoral Pains (TIPPs)
As previously stated few subgrouping studies in
PFP have followed the PROGRESS partnership
[15] and the Medical Research Council
(MRC) [16] guidance on stratification research.
Selfe et al. [20] and Drew et al. [21] are exceptions to this, both studies based their approaches
on rigorous statistical methods and adopted
hypothesis-driven approaches initially using data
to identify clinically important subgroups and
then explored the prognostic effect attributed to
subgroup membership [29]. The TIPPs programme of work [20, 30] has also in line with the
124
J. Selfe
Potenal
Subgroups
Simple low
cost evidence
based clinical
test
Published
threshold for
test?
Evidence
based
matched
intervenon
Potenal
subgroups
Fig. 2 Process for identifying appropriate clinical tests and potential subgroups
MRC framework [16] adopted an iterative
approach consisting of multiple phases (Fig. 1)
in order to identify and validate potential subgroups within the PFP population using readily
available, low cost, easy to use tools found in
routine clinical practice.
We conducted a series of literature searches to
draw up an initial ‘long list’ of potential subgroups. One of the key documents guiding this
phase of our work was the First International PFP
Research Retreat [31]. This consensus proposed
three subgroups based on the global anatomical
region thought to be responsible for the problem
i.e., proximal, local, distal. In order to facilitate
implementation into clinical settings, assessments were deemed appropriate when they were:
based on evidence of diagnostic performance;
applicable to be used in a wide range of clinical
settings; easy to learn and administer; free to use
or available at a low cost; linked to reported
thresholds; matched to a credible evidence-based
treatment intervention (Fig. 2). Through this
process, seven assessments were identified
(Table 3).
We then conducted a feasibility study to
investigate if these assessments could be performed in routine clinical practice, if they could
identify clinically relevant subgroups and what
the optimum test thresholds for subgroup
allocation might be within a UK population. Four
National Health Service (NHS) physiotherapy
clinics, serving the general population, in the UK
recruited 130 people with PFP. Participants were
between 18 and 40 years old, experienced uni- or
bilateral PFP for at least three months, and had
not yet started physiotherapy treatment. Additional study details and eligibility criteria are
presented in Selfe et al. [20, 30].
Participants completed demographic, clinical,
and psychosocial questionnaires related to
aspects of PFP and were clinically assessed using
the seven tests. Baseline demographics, such as,
sex and age, were in line with those reported by
others [36, 37]. A causal pathway diagram, based
on the broader literature review, specific consensus documents and expert opinion around the
proximal, local and distal subgroups informed
the analytical approach. Both hierarchical
agglomerative cluster analysis and latent profile
analysis were used to explore the existence of
subgroups within the sample. Surprisingly, the
Hamstrings length test mean scores were similar
across all subgroups identified by preliminary
analyses and so this was excluded from further
analysis. Three subgroups were found and are
illustrated in Fig. 3.
Both weak subgroups were consistent with
expectations, however, the strong subgroup was
Table 3 Seven assessments mapped to the appropriate evidence-based matched treatment option (Adapted from Selfe
et al. [30])
Assessments
Evidence based matched treatment option
Hand held dynamometry for hip abductor strength (Nm/kg) [32]
Hip Abductor strengthening
Hand held dynamometry for quadriceps strength (Nm/kg) [32]
Quadriceps strengthening
Medial–lateral patellar mobility test (mm) [33]
Patella stabilisation or mobilisation
Foot Posture Index (FPI) [34]
Foot orthotics
)
Rectus femoris length test (degrees) [33]
Hamstrings length test (degrees) [35]
Gastrocnemius length test (degrees) [33]
Muscle stretching
Targeted Treatment in Anterior Knee Pain Patients According …
STRONG (22%)
WEAK AND TIGHT (39%)
Strong leg
muscles
Weak leg muscles
Higher level of
function and
Quality of Life
Lower level of
Activity and
Function
More males
Higher BMI
Oldest group
Highest level of
neuropathic pain
and longest pain
duration
Hypomobile
patella
Tight leg muscles
125
PRONATED AND WEAK (39%)
Pronated feet
(FPI>6)
Weak leg
muscles
Youngest
group
Shortest pain
duration
Hypomobile patella
More females
Fig. 3 TIPPs subgroups adapted from Janssen 2017 [38]
a novel previously unrecognised group that fell
outside normal clinical expectation for PFP as no
weakness in muscle strength was identified. The
people in this subgroup reported high levels of
function, therefore it is currently our hypothesis
that this group could be overloading their patellofemoral joint, this is in line with previous
frameworks [12, 14, 22], which refer to an
overload/overuse problem associated with the
patellofemoral joint.
5
Verification of TIPPs Subgroups
The TIPPS classification system has yet to be
applied to patients to determine its efficacy in
guiding treatment and improving outcomes [22].
This is beginning to change and the following
section provides a brief summary of TIPPs verification papers (Stage 5 Fig. 1) and other papers
that have explored the application of TIPPs in
patient populations.
Normative test score results have been
explored between ethnicities and sex from TIPPs
clinical assessments conducted on 89 New
Zealanders (34% Maori, 45% female), in addition the inter-rater reliability of each test was
assessed [39]. Females were significantly weaker
than males in normalised strength measures
(p < 0.001), and had lower FPI. Mean differences between testers for all measures were small
and not significant, except for FPI which had a
2.0 point median difference (p = 0.021). HébertLosier et al. [39] concluded that sex is an
important factor worth considering within the
TIPPs subgrouping approach, more than ethnicity, especially for normalised strength measures;
the sub-optimal reliability of FPI may warrant
reconsideration of its inclusion within future
TIPPs studies. Greuel et al. [40] confirmed the
existence of a strong group of PFP patients. They
reported that there were no differences in strength
between healthy subjects and a strong group of
PFP patients. However, they did report an
increased level of muscle inhibition in the strong
PFP patients, suggestive of a motor control
problem. Drew et al. [41] recruited seventy PFP
patients and identified 4 PFP subgroups that
showed potentially different outcomes at
12 months. They identified ‘Strong’, ‘Pronation
& Malalignment’, ‘Weak’ and ‘Flexible’ subgroups. Furthermore, the natural prognosis of
these subgroups was established. By adjusting
for known covariates, they reported, compared to
126
a ‘Strong’ subgroup, a substantive directional
trend that the’ Weak’ subgroup was the least
likely (31% [7/22]; odds ratio [OR] 0.30; 95% CI
0.07, 1.36) and the ‘Flexible’ subgroup most
likely (63% [7/11]; OR 1.24, 95% CI 0.20, 7.51)
to report a favourable outcome at 12 months
follow up [41]. Yosmoaglu et al. [42] validated
the TIPPs subgroups in a Turkish PFP population
with sixty-one participants and conducted a
prospective crossover intervention study. All
patients received standardised multimodal treatment three times a week for 6 weeks, nonresponders were then classified into one of the 3
TIPPs subgroups. Non-responders were subsequently administered a further 6 weeks of matched intervention designed according to TIPPs
subgroup characteristics. Thirty six percent of the
patients (n = 21) demonstrated recovery following the first phase of multimodal treatment and
were discharged. In the second phase over 70%
(29 patients) of the non-responders demonstrated
recovery after treatment matched to subgroup. Kısacık et al. [43] recruited 30 PFP
patients specifically from the weak and pronated
foot subgroup. Patients were randomised to
either a control group or a short foot exercise
(SFE) group with concealed allocation and
blinding to group assignment. Both groups
received hip and knee strengthening and
stretching exercises and performed the training
protocol under supervision twice per week for
6 weeks. The intervention group received additional SFE. Both groups reported decreased knee
pain, but this was only significant in the SFE
group. Navicular position, rearfoot posture and
hip extensor strength all significantly improved
in the SFE intervention group compared to the
control group.
None of the individual results of the papers
presented in this section provide a definitive
answer to the question “Does Tipps classification
and matched subgroup intervention lead to
improved patient outcomes?” However, collectively they are important in contributing to a
growing evidence base supporting the TIPPs
subgrouping approach and are in line with
J. Selfe
specific components of the robust methodological approaches suggest by PROGRESS partnership [15] and the MRC framework [16] outlined
in Fig. 1.
6
Future Directions
Tables 1 and 2 highlight that most of the work on
developing stratified care using diagnostic subgrouping with matched interventions for PFP has
focussed on the Physical domain and in particular biomechanics. However, there is a growing
recognition that with respect to potentially
important PFP subgroups the Psychosocial and
Physiological domains have been under
investigated.
6.1 Psychosocial Domain
The Psychosocial domain has recently received a
lot of attention with the publication of the 2021
consensus statement on research priorities on
pain and psychological features in individuals
who have patellofemoral pain [44]. Coping
skills, anxiety, and kinesiophobia were considered research priorities. Pain catastrophising,
fear-avoidance beliefs (pain-related fear of
movement) and pain self-efficacy were considered important clinically and should be considered when undertaking a clinical examination
and designing a treatment plan (Fig. 4). Chapter
“Evaluation of Psychological Factors Affecting
Anterior Knee Pain Patients: The Implications
for Clinicians Who Treat these Patients” presents
a comprehensive overview of these important
psychological factors. These factors are all consistent with elements of the fear avoidance model
for persistent musculoskeletal pain and as such
may therefore also lend weight to the justification
of there being a Kinematic subgroup in the
Physical domain. We have previously demonstrated that people with knee pain have elevated
scores on the conscious motor processing subscale of the movement-specific reinvestment
Targeted Treatment in Anterior Knee Pain Patients According …
Psychosocial
Fear avoidance?
(Pain-related fear of
movement)
Physical
Muscle strength
Muscle length
Foot Posture
Kinematic?
Physiological
Vascular /
Ischaemic?
Fig. 4 Potential PFP subgroups within each of the 3 key
domains
scale [45]. This means they have concerns about
moving effectively or safely, which is also consistent with fear-avoidance models. In future
stratification and subgrouping research it will be
interesting to explore the relationship between
the objective measurement of lower limb kinetics
and the degree of self-reported kiniesiophobia to
potentially define a kinematic subgroup of
PFP. The key challenges will be around which
tests to use, test thresholds or cut point scores for
allocation of patients to a Kinematic subgroup
and what the matched treatment interventions
should be. In terms of potential matched treatment interventions for a kiniesiophobia/kinetic
subgroup; PFP patients with elevated scores on
the conscious motor processing subscale of the
movement-specific reinvestment scale may
respond well to implicit rehabilitation strategies.
Implicit rehabilitation targets unconscious
aspects of movement through trial and error
without thinking specifically about how to move,
whereas explicit strategies target the conscious
aspects of movement [45].
6.2 Physiological Domain
Compatible with the theory of Tissue Homeostasis
[26, 27] and central to the Neural Model [28] is
that physiological factors, such as vascularisation
of the knee, could play an important role in PFP
127
and that in some patients with PFP pain may be
induced by ischemia [28, 46, 47]. There is a strong
biologically plausible link between vasularisation,
ischaemia and knee temperature which supports
the candidacy of a vascular/ischaemic subgroup of
PFP as a potentially important clinical subgroup
Figs. 1 and 4. In addition to this laboratory evidence there is also clinical evidence suggesting a
variety of circulatory issues may result in pain and
altered temperature profiles around the patella and
sensitivity to cold surroundings is a commonly
reported clinical feature in PFP [48–56]. In the
2021 consensus statement on research priorities
on pain and psychological features [44] the role of
Quantitative Sensory Testing (QST) was discussed in assessing neural components of
PFP. One of the parameters QST can assess is
thermal pain thresholds (hot/cold), however, in the
consensus thermal pain thresholds did not emerge
as clinically important or as research priorities.
The challenge therefore appears to be around
which are the appropriate clinical tests to use to
explore a potential vascular/ischaemic subgroup
of PFP patients that may have a thermal component to their problem Fig. 1. It is currently unclear
if QST is the appropriate test to investigate this
subgroup. We have conducted a series of studies
investigating a cold knee group as a potential PFP
subgroup [52–54]. On baseline assessment ‘cold’
PFP patients had worse scores on the Modified
Functional Index Questionnaire (MFIQ) and time
to pain onset on an inclined walking treadmill test
compared to PFP patients with ‘nornmal’ skin
temperature (Tsk). Following a standardised
course of multimodal therapy, three months post
discharge the ‘normal Tsk’ PFP patients scores had
improved by greater than minimum clinically
important change whereas the ‘cold Tsk’ PFP
patients had not improved at all [53]. To investigate this more objectively we initially used state of
the art high-cost thermal imaging cameras but
have now validated a low-cost hand-held digital
thermometer as an alternative which would be
more suitable for routine clinical use [55] Fig. 5.
In a sample of 58 healthy participants and 232
PFP patients we used finite mixture models to
examine the presence of PFP temperature subgroups and receiver operating characteristic
128
J. Selfe
clinicians will have access even to a low-cost
digital thermometer. So we have also investigated the utility of four simple clinical questions
which may provide an initial clinical screening to
alert clinicians to the possibility of the presence
of a vascular/ischaemic disorder [53]
Fig. 5 Hand-held digital thermometer measurement of
patellar skin temperature (Tsk)
(ROC) curves to estimate optimal patella Tsk
thresholds for allocation into subgroups [54]. In
contrast to healthy participants, participants with
PFP patella Tsk had an obvious bimodal distribution. The fitted finite mixture model suggested
three temperature subgroups (cold, normal and
hot) with discrimination cut-off thresholds for
subgroup membership based on ROC analysis of
Cold = 29.9 °C; Normal 30.0–35.2 °C;
Hot 35.3 °C (Fig. 6).
As objective measurement of Tsk is not routine musculoskeletal practice we recognise not all
Fig. 6 Histogram showing
distribution of patella Tsk and
suggested thresholds or cut
point scores for allocation of
patients to subgroups
• Do your knees feel cold even on a warm day
• Does cold weather affect your knees
• Do you wear extra tights/long johns in winter
(because of your knees)
• Would you prefer a hot-water bottle or ice
pack on your knee
Of these the last question often provokes an
interesting response, in cases of ‘cold knees’.
Don’t you dare come anywhere near my knee with
that ice pack!
this is quite a strong and negative reaction to
the ice pack. This area work needs further validation to define the potential subgroup and formal investigation as to what the appropriate
matched treatment interventions should be for
this potential subgroup, treatment suggestions
based on clinical experience are presented elsewhere [56].
Targeted Treatment in Anterior Knee Pain Patients According …
7
Conclusion
129
Figure 7 proposes a clinical pathway for the
assessment of a new patient referred with PFP,
highlighting the three overarching domains,
potentially important subgroups and areas where
there is still uncertainty.
Our experience has highlighted some of the
challenges in undertaking subgrouping research
in PFP. One is small sample size, which precludes many of the more complex, statistical
methods for classifying subgroups and/or optimising thresholds. In the Selfe et al. study [20], it
also precluded cross-validation studies for internal verification requiring reliance on using two
different statistical methods instead. Given sample size is a difficulty in many PFP studies,
consideration should be given to establishing
large prospective datasets, which may require
collaboration across institutions and countries.
Such an initiative requires a core dataset of
putative markers, such as the TIPPs clinical tests
This chapter has reviewed a number of proposed
stratification frameworks for PFP and some of
the methodological considerations which guide
stratification research. With the exception of
TIPPs [30] PFP stratification frameworks have
not been developed in line with rigorous
methodological guidelines and therefore have a
number of limitations. The chief limitation particularly of early stratification frameworks is the
double-digit number of subgroups which restricts
their clinical utility. More recently however there
appears to be an emerging evidence base and
consensus that there a relatively small number
PFP subgroups worth considering from a matched treatment perpective. It is probable that
these overlap and /or interact with each other,
however the exact nature how they overlap and
interact with each other are as yet unknown.
Fig. 7 Proposed clinical
pathway for managing
subgroups
Pre-Clinical screening
quesonnaires
Psychosocial Domain
Physiological Domain
Fear Avoidance (e.g. TSK)
Ischaemic (e.g. 4 Cold Quesons)
Physical Domain
Clinical assessment
Objecve Measure of
TsK
Lower Limb
Kinemacs?
Muscle
Strength
Strong
Muscle
Length
Weak and Tight
Cold subgroup?
Foot
Posture
Weak and Pronated
130
J. Selfe
described earlier, but also others for which there
may be emerging evidence of their prognostic
impact, e.g., psychosocial factors [57] and a core
set of outcome measures. While progress is being
made on the latter with the development of the
KOOS-PF [58] there remains a bewildering
variety of different tests used to measure the
same clinical phenomenon; some are more
practical to use than others. The recently published Report PF [59] which is hosted on the
Equator Network provides a clearly defined, and
widely accepted set of agreed standards for
reporting of quantitative PFP research and represents a useful step forwards in terms of standardisation. It consists of 31 items (11 strongly
recommended, 20 recommended), covering
(i) demographics; (ii) baseline symptoms and
previous treatments; (iii) outcome measures;
(iv) outcomes measure description; (v) clinical
trial methodology and (vi) reporting study
results. Finally, we also need carefully collected
normative data on key measures to allow for
appropriate interpretation of comparative test
data in PFP patients. Despite an emerging evidence base and some consensus, to date no
definitive RCTs have been conducted to evaluate
the potential benefits of matched interventions
for PFP subgroups in terms of improved patient
outcomes so this continues to warrant further
research.
8
Take-Home Messages
1. There is limited evidence supporting the
longer-term outcomes of a multimodal
approach to therapy.
2. There have been many attempts at producing
PFP stratification frameworks and defining
subgroups, however no consensus on these
has been reached.
3. Robust methodological frameworks for
guiding stratification and subgrouping
research have been produced but these have
yet to be applied fully to PFP.
4. Three overarching domains need consideration within a subgrouping model for PFP:
Physical; Psychosocial; Physiological.
5. Within the Physical domain consensus
appears to emerging around the importance
of: Muscle strength, Muscle length, Foot
Posture, Kinematics. The Psychosocial and
Physiological domains are under investigated.
6. Candidature for subgroups requires
a. a strong mechanobiologic rational
b. objective data on test measurement properties such as validity and reliability
c. thresholds/cut points to define subgroup
allocation
d. tests that are feasible and acceptable to
both patients and clinicians (e.g. quickly
performed and requiring low cost measurement tools to collect relevant data).
9
Key-Message
There have been many attempts at defining
subgroups within the PFP population, despite
these efforts, currently there is no consensus on
the optimal subgroups, however there is emerging evidence that a subgrouping approach may
improve patients outcomes compared to a multimodal approach to treatment.
References
1. Barton CJ, Lack S, Hemmings S, et al. The ‘best
practice guide to conservative management of
patellofemoral pain’: incorporating level 1 evidence
with expert clinical reasoning. Br J Sports Med.
2015:1–13.
2. Smith B, Hendrick P, Bateman M, et al. Current
management strategies for patellofemoral pain: an
online survey of 99 practising UK physiotherapists.
BMC Musculoskelet Disord. 2017;18:181.
3. Crossley KM, Macri EM, Cowan SM, et al. The
patellofemoral pain and osteoarthritis subscale of the
KOOS (KOOS-PF): development and validation
using the COSMIN checklist. Br J Sports Med.
2017;52:1130–6.
Targeted Treatment in Anterior Knee Pain Patients According …
4. Whittingham M, Palmer S, Macmillan F. Effects of
taping on pain and function in patellofemoral pain
syndrome: a randomized controlled trial. J Orthop
Sports Phys Ther. 2004;34:504–10.
5. Dixit S, DiFiori JP, Burton M, et al. Management of
patellofemoral pain syndrome. Am Fam Physician.
2007;15:194–202.
6. Blond L, Hansen L. Patellofemoral pain syndrome in
athletes. Acta Orthop Belg. 1998;64:393–400.
7. Brennan GP, Fritz JM, Hunter SJ, et al. Identifying
subgroups of patients with acute/subacute “nonspecific” low back pain: results of a randomized clinical
trial. Spine. 2006;31:623–31.
8. Hill JC, Whitehurst D, Lewis M, et al. Comparison of
stratified primary care management for low back pain
with current best practice (STarT Back): a randomised
controlled trial. The Lancet. 2011;378:1560–2157.
9. Holmes SW Jr, Clancy WG Jr. Clinical classification
of patellofemoral pain and dysfunction. J Orthop
Sports Phys Ther. 1998;28:299–306.
10. Selfe J, Janssen J, Drew B, et al. Anterior Knee Pain
Subgroups: The First Step Towards a Personalized
Treatment. Annals of Joint Special edition on
Patellofemoral Pain. Edited by Sanchis-Alfonso V
and Dye S. 2018;3:32.
11. Merchant AC. Classification of patellofemoral disorders. Arthroscopy. 1988;4:235–40.
12. Wilk KE, Davies GJ, Mangine RE, et al. Patellofemoral disorders: a classification system and clinical
guidelines for nonoperative rehabilitation. J Orthop
Sports Phys Ther. 1998;28:307–22.
13. Witvrouw E, Werner S, Mikkelsen C, et al. Clinical
classification of patellofemoral pain syndrome:
guidelines for non-operative treatment. Knee Surg
Sports Traumatol Arthrosc. 2005;13:122–30.
14. Powers CM, Witvrouw E, Davis IS, et al. Evidencebased framework for a pathomechanical model of
patellofemoral pain: 2017 patellofemoral pain consensus statement from the 4th International patellofemoral pain research retreat, Manchester, UK: part
3. Br J Sports Med. 2017;51:1713–23.
15. Hingorani AD, van der Windt DA, Riley RD, et al.
Prognosis research strategy (PROGRESS) 4: stratified medicine research. BMJ. 2013;346: e5793.
16. Medical Research Council. The MRC Framework for
the Development, Design and Analysis of Stratified
Medicine Research. Swindon: Medical Research
Council; 2018.
17. Post WR. Current concepts clinical evaluation of
patients with patellofemoral disorders. Arthroscopy.
1999;15:841–51.
18. Selhorst M, Rice W, Degenhart T, et al. Evaluation
of a treatment algorithm for patients with patellofemoral pain syndrome: a pilot study. Int J Sports Phys
Ther. 2015;10:178–88.
19. Keays S, Mason M, Newcombe P. Individualised
physiotherapy in the treatment of patellofemoral
pain. Physiother Res Int. 2015;20:22–36.
20. Selfe J, Dey P, Callaghan M, et al. Are there three
main subgroups within the patellofemoral pain
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
131
population? A detailed characterisation study of
127 patients to help develop targeted Intervention
(TIPPs). Br J Sports Med. 2016;50:873–80.
Drew B, Conaghan P, Smith T, et al. Development of
data-driven diagnostic subgroups for people with
patellofemoral pain using modifiable clinical, biomechanical and imaging features. J Orthop Sports Phys
Ther. 2019;49:536–47.
Willy R, Hoglund L, Barton C, et al. Patellofemoral
pain clinical practice guidelines linked to the international classification of functioning, disability and
health. From the academy of orthopaedic physical
therapy of the american physical therapy association.
J Orthop Sports Phys Ther. 2019;49: 623–681.
Dierks T, Manal K, Hamill J, et al. Lower extremity
kinematics in runners with patellofemoral pain
during a prolonged run. Med Sci Sports Exerc.
2011;43:693–700.
Richards J, Selfe J, Kelly S, et al. Are there
differences in Knee Stability between patients with
patellofemoral pain and healthy subjects during a
slow step descent task? PRM+. 2018;1:67–70.
Callaghan M, Richards J, Atkins LT, et al. Medial
and lateral knee deviation angular measurements to
assess knee instability using smart phone video
technology. Can J Biomed Res Tech. 2020;3:3–4.
Dye SF, Vaupel GL. The pathophysiology of
patellofemoral pain. Sports Med Arthrosc Rev.
1994;2:203–10.
Dye S, Staubli HU, Biedert RM, et al. The mosaic of
pathophysiology causing patellofemoral pain: therapeutic implcations. Oper Techn Sports Med.
1999;7:46–54.
Sanchis-Alfonso V. Pathophysiology of anterior knee
pain. In: Zaffagnini S, Dejour D, Arendt EA
(eds) Patellofemoral pain, instability, and arthritis.
Berlin: Springer; 2010.
Kent P, Keating JL, Leboeuf-Yde C. Research
methods for subgrouping low back pain. BMC Med
Res Methodol. 2010;10:62.
Selfe J, Callaghan M, Witvrouw E, et al. Study
Protocol: Targeted Interventions for Patellofemoral
Pain (TIPPs): classification of clinical sub-groups.
BMJ Open. 2013;3: e003795. https://doi.org/10.
1136/bmjopen-2013-003795.
Davis I, Powers C. Patellofemoral pain syndrome:
proximal, distal, and local factors. an international
retreat. J Orthop Sports Phys Ther. 2010;40:A1–48.
Maffiuletti NA. Assessment of hip and knee muscle
function in orthopaedic practice and research. J Bone
Joint Surg Am. 2010;92:220–9.
Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic
risk factors for the development of anterior knee pain
in an athletic population: a two year prospective
study. Am J Sports Med. 2000;28:480–9.
Redmond AC, Crane YZ, Menz HB. Normative
values for the foot posture index. J Foot Ankle Res.
2008;1:1–9.
Youdas JW, Krause DA, Hollman JH, et al. The
influence of gender and age on hamstring muscle
132
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
J. Selfe
length in healthy adults. J Orthop Sports Phys Ther.
2005;35:246–52.
Syme G, Rowe P, Martin D, et al. Disability in
patients with chronic patellofemoral pain syndrome:
a randomised controlled trial of VMO selective
training versus general quadriceps strengthening.
Man Ther. 2009;14:252–63.
Brown J. Physiotherapists knowledge of patellofemoral pain syndrome. Br J Ther Rehabil.
2000;7:346–53.
Janssen J, Selfe J, Callaghan M, et al. Patellofemoral
pain subgroups: a critical first step towards personalised
clinical intervention. Lower Extremity Review. 2017;
https://lermagazine.com/cover_story/patellofemoralpain-subgroups-a-critical-first-step-towardpersonalized-clinical-intervention.
Hébert-Losier K, Hanzlíkováa I, Ghadikolaeia S,
et al. An exploration of normative values in New
Zealand to inform the targeted interventions for
patellofemoral pain approach (TIPPs). Musculoskeletal Science and Practice. 2021;54.
Greuel H, Herrington L, Liu A, et al. How does acute
pain influence biomechanics and quadriceps function
in individuals with patellofemoral pain? Knee.
2019;26:330–8.
Drew BT, Conaghan PG, Smith TO, et al. The effect
of targeted treatment on people with patellofemoral
pain: a pragmatic, randomised controlled feasibility
study. BMC Musculoskelet Disord. 2017;18:338.
Yosmaoglu B, Sonmezer E, Ezgisahin I, et al.
Targeted treatment protocol in patellofemoral pain
(TIPPs): does treatment designed according to subgroups improve clinical outcomes in patients unresponsive to multimodal treatment? Sports Health.
2019. https://doi.org/10.1177/1941738119883272.
Kısacık P, Tunay V, Bek N, et al. Short foot
exercises have additional effects on knee pain, foot
biomechanics, and lower extremity muscle strength
in patients with patellofemoral pain. J Back Musculoskelet Rehabil. 2021. https://doi.org/10.3233/
BMR-200255.
Vicenzino B, Rathleff MS, Holden S, et al. Developing clinical and research priorities on pain and
psychological features in individuals who have
patellofemoral pain: An international consensus
process with health care professionals. J Orthop
Sports Phys Ther. 2021.
Selfe J, Dey P, Richards J, et al. An exploration of
the association between the reporting of musculoskeletal pain in the knee and the propensity for
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
conscious control of movement. Clin Rehabil.
2015;29:95–100.
Arnoldi CC. The patellar pain syndrome. Acta
Orthop Scand. 1991;62(Suppl244):1–29.
Naslund J, Walden M, Lindberg LG. Decreased
pulsatile bloodflow in the patella in patellofemoral
pain syndrome. Am J Sports Med. 2007;35:1668–73.
Ben-Eliyahu DJ. Infrared thermographic imaging in
the detection of sympathetic dysfunction in patients
with patellofemoral pain. J Manip Physiol Therapeutics. 1992;15:164–70.
Sandow MJ, Goodfellow JW. The natural history of
anterior knee pain in adolescents. J Bone Jt Surg
(Br). 1985;67:36–8.
Price AJ, Jones J, Allum R. Chronic traumatic
anterior knee pain. Injury. 2000;31:373–8.
McConnell J Chapter 2: Patients emotional states and
expectations. In: Selfe J, Janssen J, Callaghan M, eds.
Patellofemoral Pain: An evidence-based clinical
guide. New York: Nova Science; 2017.
Selfe, J Harper L, Pedersen I, et al. Cold legs: A
potential indicator of negative outcome in the
rehabilitation of patients with patellofemoral pain
syndrome? Knee. 2003;10:139–143.
Selfe J, Sutton C, Hardaker N, et al. Anterior knee
pain and cold knees: a possible association in
women. Knee. 2010;17:319–23.
Janssen J, Selfe J, Gichuru P, et al. Hot and cold
knees: exploring differences in patella skin temperature in patients with patellofemoral pain. Physiotherapy. 2020;108:55–62.
Erande R, Dey M, Richards J, et al. An investigation
of the relationship between thermal imaging and
digital thermometer testing at the knee. Physiotherapy Pract Res. 2016;37:41–7.
Selfe J. Patellofemoral pain: myths. truths; future
directions Physiotherapy Ireland. 2010;31:16–8.
Maclachlan L, Collins N, Matthews M, et al. The
psychological features of patellofemoral pain: a
systematic review. Br J Sports Med. 2017;51:732–42.
Crossley KM, Macri EM, Cowan SM, et al. The
patellofemoral pain and osteoarthritis subscale of the
KOOS (KOOS-PF): development and validation
using the COSMIN checklist. Br J Sports Med.
2018;52:1130–6.
Barton CJ, De Oliveira SD, Morton S, et al.
REPORT-PFP: a consensus from the International
Patellofemoral Research Network to improve
REPORTing of quantitative PatelloFemoral Pain
studies. Br J Sports Med. 2021;55:1135–43.
Surgical Treatment of Anterior Knee
Pain. When is Surgery Needed?
Vicente Sanchis-Alfonso
and Robert A. Teitge
1
Introduction
Anterior knee pain (AKP) continues to be challenging for the orthopedic surgeon. It is widely
accepted that the vast majority of AKP patients
only need conservative treatment and do not need
a surgery [1–3]. However, the results of conservative treatment for AKP are often frustrating.
Some 40% of AKP patients have an unsatisfactory recovery with conservative treatment at
12 months after the initial diagnosis [4]. The
high percentage of undesirable outcomes may be
due to the fact that some of them actually need
surgical treatment. However, they do not receive
it because the doctor lacks the adequate knowledge to make a precise diagnosis.
The patient with AKP is at high risk of
undergoing surgical treatment with little or no
scientific basis simply because AKP is a musculoskeletal pathologic entity with a poorly understood etiopathogenesis. Therefore, in more cases
than is acceptable, the AKP patient’s condition
worsens after surgical treatment [5]. In fact, many
surgeries performed on AKP patients are undertaken to address complications, or the unsatis-
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
R. A. Teitge
Wayne State University, Detroit, MI, USA
factory results of previous poorly performed or
badly indicated surgeries intended to treat AKP
[5]. The patellofemoral joint (PFJ) does not really
tolerate surgical procedures that do not respect its
unique anatomical, biological and biomechanical
characteristics [6]. For that reason, AKP surgery
is currently performed infrequently.
This chapter focuses on the patient with AKP
without patellofemoral osteoarthritis as the cause
of pain. Consequently, techniques such as the
anteromedialization of the tibial tubercle (Fulkerson’s osteotomy), fresh allograft transplantation or patellofemoral arthroplasty are not
analyzed here. This chapter analyzes the current
state of knowledge around the surgical treatment
of AKP patients, emphasizing the importance of
the diagnosis and treatment of torsional alterations of the lower limb. The surgical techniques
used include minimally invasive procedures,
such as peripatellar synovectomy or resection of
synovial hypertrophy around the inferior pole of
the patella and major surgical techniques such as
osteotomies. Indeed, osteotomy must be seriously considered a part of the armamentarium for
treating AKP patients.
2
General Principles in the Surgical
Management of AKP Patients
For AKP patients who might benefit from surgery, a knowledgeable surgeon and a correct
diagnosis are crucial factors. A careful history, a
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_9
133
134
complete physical examination and the use of
imaging must be included. The surgeon must
determine which surgical procedure, if any, has
the potential to improve the patient´s condition
and, most importantly, does them no harm.
2.1 A Right Diagnosis is Paramount—
Listen to the Patient
Conversation with the patient and a complete
physical examination are fundamental, but are
too often neglected. This, in turn, triggers a failed
patellofemoral surgery. We must listen very
carefully to our patients because they will usually
tell us what is wrong in their own words. It is our
mistake if we fail to understand them and assume
we somehow know better than what they are
trying to tell us. To reiterate, a complete physical
examination is prerequisite. This is an attempt to
uncover all of the anatomic abnormalities, of
which there are often many. When any abnormal
anatomy is uncovered then the following question must be answered. How does this change the
normal biomechanics?
To arrive at a correct diagnosis, answers are
also needed to the following questions: (1) Is
AKP secondary to patellar instability, or does it
arise from bone rubbing or tension in the soft
tissues?; (2) Does the patient have a neutral
mechanical axis, or is varus or valgus present?;
(3) Does he or she have abnormal torsion (i.e.,
considerable external tibial rotation or pathological internal rotation of the femur)?; and (4) Is the
quadriceps too tight? A critical factor to consider
when treating AKP patients is whether patellofemoral instability is present concurrently.
Treatment of underlying patellar instability in
these patients should be undertaken with caution
and the patients must know that surgical patellar
stabilization may not relieve AKP. Moreover, a
careful assessment of the limb alignment is an
essential part of the physical evaluation of the
AKP patient.
V. Sanchis-Alfonso and R. A. Teitge
2.2 Treat Patients, Not Images
Unfortunately, many orthopedic surgeons operate based on what computed tomography (CT) or
magnetic resonance imaging (MRI) shows. That
might be chondropathy, lateral patellar subluxation, patellar tilt, or an increment in the tibial
tuberosity-trochlear groove (TT-TG) distance. It
seems as though they are operating on an image
instead of a person. Using this information as the
basis for surgery is a critical error—and it is
responsible for the poor reputation of AKP surgery. In the hands of the wrong orthopedic surgeon, the MRI becomes a license to operate.
The MRI does not tell us what hurts.
Poor results of surgery in AKP patients may
arise either because the diagnosis is inaccurate or
because of physio-pathological premises on
which surgery are based (i.e., “pathological” TTTG distance) are incorrect. Therefore, the treatment is also incorrect. Many orthopedic surgeons base their surgical indication for
patellofemoral surgery on a TT-TG distance
greater than 20 mm. The use of this parameter as
the deciding factor is a critical mistake because it
can be a source of surgical failure and iatrogenic conditions. We must not use imaging
numbers to treat a patient. Physical examination
is the key part of assessing AKP. Tensho
and colleagues [7] have proven that knee rotation
affects the TT-TG distance more than tubercle
malposition does. For this reason, it should not be
used as a surgical indicator for tibial tubercle
transfer. However, the TT-TG distance is currently widely used as an indicator for medialization of the tibial tubercle in the AKP patient.
Historically, great importance has been given
to the presence of a lateral patellar subluxation in
the CT or in the MRI, which is attributed to
excessive traction of the lateral retinaculum
(LR) in the AKP patient. However, the LR does
not pull the patella laterally—it prevents it from
moving too far medially. Lateral patellar subluxation may be due to inadequate lateral
Surgical Treatment of Anterior Knee Pain …
135
Fig. 1 SPECT-CT in an AKP patient with 40° of external left tibial rotation. External tibial rotation increases pressure
on the lateral side of the PFJ. This patient had disabling left AKP recalcitrant to conservative treatment
trochlear inclination, genu valgum, or abnormal
femoral anteversion. If lateral subluxation of
the patella is present, the patellar tendon
approaches the tibial tuberosity from a more
lateral direction. Specifically, most of its force
through the patellar tendon is diverted into pulling the tuberosity laterally when the quadriceps
contracts, causing the tibia to rotate more externally on the femur. Therefore, using a lateral
retinaculum release (LRR) to correct lateral
patellar subluxation is inappropriate. We must
treat the underlying cause, for example, excessive femoral anteversion.
2.3 Identify if AKP is Related to Focal
Overload of the PFJ
A key step in surgical decision-making is to
identify whether AKP is related to patellofemoral
overload. Pain related to it is generally localized,
and worsened or improved depending on the
load applied to the PFJ. Patients with localized
load-related pain may be more amenable to
successful surgical treatment while diffuse constant pain generally does not improve with
surgery.
A true skeletal malalignment of the lower
limb might be responsible for focal overload in
the PFJ [8–13]. In those cases, imaging studies
like single-photon emission computed tomography (SPECT)-CT can reveal overloaded areas
(Fig. 1). We should strive to restore the normal
anatomy because that will create a better
biomechanical environment for the tissue. Rotational osteotomies may be used to unload bone
and peripatellar soft tissue and create an adequate
environment for a return to homeostasis. As
suggested by Post and Dye, “Think of surgery as
a tool used to create an environment in which
homeostasis may be restored” [1].
2.4 If You Repair Failed Tissue (Bone,
Ligament or Cartilage)
and Ignore the Mechanics
Which Caused the Tissue
Failure, You Will Usually
Have a Failed Result
Addressing the involved structures (trochlea, cartilage, and ligaments) does not address the cause of
the abnormal force that produces focal overload
and the subsequent damage to the tissues.
136
V. Sanchis-Alfonso and R. A. Teitge
Osteotomy is quite able to change the direction of the force. This ability is particularly
important when abnormal limb alignment
(transverse or coronal plane or combination) is
present. If the cartilage is repaired but the
mechanics that caused its failure are ignored,
failure is the likely outcome.
It appears to be appropriate to place the trochlear groove under the patella instead of forcing
the latter over the trochlear groove. In short,
think about limb alignment, not patellar alignment (Fig. 2).
A
C
Fig. 2 Normal knee (A). The rotating movement of the
femur underneath the patella in the transverse plane leads
to abnormal patellar tracking (lateral patellar subluxation
and patellar tilt (1) and therefore patellofemoral imbalance) (B). The patella maintains a horizontal position,
while the femur internally rotates. Therefore, the patellar
subluxation during weight-bearing conditions is not the
result of patella moving on the femur, but of the result of
the femur rotating underneath the patella. It would be the
rationale for rotational osteotomy surgery. Retracted
lateral retinaculum (2), tension increases in the medial
retinaculum (3), compression in the lateral patellofemoral
2.5 Identify if There Are Associatted
Psychological Factors
and Central Sensitization
Our data shows that the presence of psychological factors is a limitation to recovery (see
chapter “Evaluation of Psychological Factors
Affecting Anterior Knee Pain Patients: The
Implications for Clinicians Who Treat these
Patients”). Therefore, we should not ignore them.
However, the presence of psychological impairment is not a contraindication for surgery.
B
D
joint increases (4), inward twisting of the knee (5). The
final result: ‘‘patellofemoral imbalance’’. (D) Patellar
maltracking after two previous failed distal femoral
osteotomies. (C) Postoperative CT. After external femoral
rotational osteotomy, we achieve a greater surface of
contact and therefore a decrease in patellofemoral joint
pressure. (“Republished with permission of Springer
Nature BV, from Holistic approach to understanding
anterior knee pain, Sanchis-Alfonso V, Knee Surg Sports
Traumatol Arthrosc, 22, 2275–2285, 2014; permission
conveyed through Copyright Clearance Center, Inc.”)
Surgical Treatment of Anterior Knee Pain …
“Crazy” patients with a real pathology get back
to normal or are at least much better mentally
after effective treatment. A reduction in psychological impairment after a correct surgical treatment that has reduced or eliminated the pain has
been seen. What is more, we have observed a
reduction in central sensitization after successful
surgical treatment. In “crazy” patients, we need
to look hard for a real pathology and help them
even if it takes more patience and tender loving
care from the provider.
2.6 In Short …
We must always evaluate the following:
(1) skeletal limb alignment (including the trochlea); (2) ligaments (i.e., the presence of
hypermobility and its cause and location);
(3) articular cartilage (i.e., complete or partial
loss, location of the loss, possibility to shift
contact to intact cartilage); and (4) muscle (i.e.,
symmetrical atrophy versus gross imbalance).
3
Minimally Invasive Surgical
Procedures
Some orthopaedic surgeons consider minimally
invasive surgical procedures like LRR and
arthroscopic focal synovectomy as minor riskfree surgical procedures. However, we agree with
Ronald Grelsamer in that “There is no such thing
as minor surgery—only minor surgeons”.
137
arthroscopic procedures. They showed a need for
revision surgery in 12% of the cases after a 52month follow-up. Then again, they did emphasize that the surgical procedure is necessary in
less than 15% of AKP patients. Nevertheless, the
authors drew attention to the need for randomized clinical trials to assess the advantages of this
procedure when treating AKP.
However, experienced knee surgeons with a
special interest in the PFJ rarely perform isolated
LRR [16]. In a study [17] that analyzed the
current trends in LRR procedures from 2010
through 2017 using a large USA database, the
authors showed an incidence for LRR of 481.9
per 100,000 orthopedic surgeries in 2010 that
significantly decreased to 186.9 per 100,000
orthopedic surgeries in 2017. LRRs were more
commonly performed in younger female patients
for a diagnosis of pain with the most common
concomitant procedure being meniscectomy,
synovectomy, or a microfracture.
Iatrogenic medial patellar instability has been
described after excessive LRR or in the setting of
an LRR performed in cases of patellar tilt without
a tight LR or in patients with severe trochlear
dysplasia [18]. Lateral retinacular lengthening
has been reported as an alternative to LRR to
prevent its eventual complications [14].
Moreover, releasing the painful retinaculum in
a limited way in a very selected group of AKP
patients may relieve pain [19]. Finally, arthroscopic LRR of a symptomatic type III bipartite
patella without excision of the accessory bone
fragment is related to excellent AKP relief and an
early return to sport activities [20].
3.1 Lateral Retinaculum Release
LRR has a long history. It has often been used to
treat AKP recalcitrant to conservative treatment
in very selected patients with a patellar tilt and a
tight LR, which is demonstrated by an inability
to evert the lateral patella to a neutral position on
physical examination [14]. In a systematic
review of literature, Lattermann and colleagues
[15] demonstrated that the isolated LRR for AKP
yielded good results in 76% of the cases with no
significant difference between open or
3.2 Arthroscopic Focal Synovectomy.
Patellar Decompression
When a focal soft tissue source of AKP refractory to appropriate conservative treatment can be
identified (Fig. 3), arthroscopic debridement of
this pathological tissue can relieve the pain [21–
23]. The most frequent sources of pain would be
synovial hypertrophy around the inferior pole of
the patella, Hoffa fat pad impingement and
peripatellar synovitis (Fig. 3). Other patients may
138
V. Sanchis-Alfonso and R. A. Teitge
Fig. 3 Peripatellar synovitis
require removal of a chronically tender synovial
band of tissue or plica. Moreover, it has been
suggested that the ligament mucosum (i.e.,
infrapatellar plica) potentially plays a role in the
pathogenesis of AKP [23]. Release or resection
of the infrapatelar plica, which tethers the Hoffa
fat pad, significantly improves AKP in these
patients [23].
Use of a superomedial portal may help to
prevent potential errors arising from viewing the
anterior compartment from a peripatellar tendon
portal [2]. These minimally invasive surgical
procedures should not be approached lightly. It is
essential
to
circumvent
postoperative
hemarthrosis, which can be very painful and set
back restoration of homeostasis [1, 2]. Therefore,
intraoperative hemostasis must be meticulous,
and 24-h drainage through one of the arthroscopic portals of the patient’s knee is advised.
Soft tissue impingement may also be associated with osseous hypertension, which can produce transitory ischemia and mechanical
stimulation of nociceptors and the ensuing pain.
Patients with an intraosseous hypertension of the
patella with a positive pain provocation test (i.e.,
pain reproduced by raising intrapatellar pressure)
might be good candidates for extra-articular
arthroscopic patellar decompression (Fig. 4)
[24]. Finally, in patients with AKP recalcitrant to
conservative treatment for more than 6 months
with no associated structural anomalies, patellar
denervation may be an option [25].
4
Major Surgical Procedures—
Osteotomies
Skeletal malalignment of the limb (i.e.,
malalignment on the transverse, coronal, and
sagittal planes) is one of the causes of AKP in
some young patients. The presence of excessive
femoral anteversion, excessive external tibial
torsion, or increased varus or valgus abnormalities has a great impact on PFJ biomechanics. In
particular, rotational abnormalities are important
[11–13].
4.1 Derotational Osteotomies
(Transverse Plane)
One of the most powerful causes of AKP that
both doctors and the literature forget to mention
is the pain resulting from torsional alterations of
the lower limb. However, tibio-femoral rotation
has yet to be integrated into our thinking. In fact,
most of the current literature discusses patellar
alignment in association with AKP as a problem
of the patella itself (increased tilt or increased
shift of the patella). However, in many cases, the
problem is not in the patella but in the femur.
Thus, it is of a vital importance to assess the
rotational profiles of the femur and tibia in an
AKP patient. As far back as in 1995, Flandry and
Huhgston [26] showed that the most frequent
Surgical Treatment of Anterior Knee Pain …
139
Fig. 4 Pain with knee
hyperflexion. Intraosseous
hypertension of the patella
Patellar decompression
cause of failure of an extensor mechanism
realignment surgery was the existence of an
underlying torsional alteration not diagnosed and
therefore not treated. Stevens and colleagues [27]
have demonstrated clinical improvement after
osteotomies of the femur and/or tibia in patients
with a previous failed surgery (tibial tubercle
osteotomy, LRR or arthroscopic debridement) to
treat AKP in those whom torsional abnormalities
of the lower limb had gone unnoticed. Those
authors state that many orthopedic surgeons only
focus on the knee when they see an AKP patient.
Torsional abnormalities often go unrecognized.
4.1.1 Rationale
Limb alignment appears to have a very powerful
influence on the quadriceps vector [13]. If an
abnormal quadriceps vector is an important
contributor to AKP and skeletal malalignment of
the lower limb explains the offending quadriceps
vector, then any torsion or coronal correction is
important [13]. It is important to note that small
alterations in the skeletal alignment of the lower
limb can result in significant alterations in PFJ
stresses. Osteotomy has a great ability to change
the direction of the force and therefore treat these
patients.
140
Lee and colleagues [8, 9, 28] have demonstrated that femoral rotation results in an increase
in PFJ contact pressures on the contralateral facet
of the patella (i.e., lateral PFJ during internal
rotation of the femur and vice versa). Furthermore, tibial rotation results in an increase in PFJ
contact pressures on the ipsilateral facet of the
patella. Lee and colleagues have demonstrated
that tibial rotation not only has an influence on
PFJ contact pressures and areas but also on strain
in the peripatellar retinaculum [28]. More
recently, Passmore and colleagues [10] have
shown that idiopathic lower-limb torsional
deformities of the femur and tibia in children and
adolescents are associated with gait impairments
as well as an increase in loading on the hip and
PFJ. Thus, idiopathic lower-limb torsional
deformities are not a purely cosmetic issue.
Using a finite element model, Liao and colleagues [29] have demonstrated that internal
rotation of the femur provokes an increment in
PFJ stress.
4.1.2 Clinical Evaluation
Four types of torsional alteration of the lower
limb are possible: (1) femoral anteversion,
(2) femoral retroversion, (3) excessive external
tibial torsion, and (4) excessive femoral anteversion associated with an increased external tibial
torsion.One of the questions yet to be answered,
biomechanically, in the last type is whether
excess tibial torsion and excess of femoral
anteversion are of equal mechanical importance?
Then again, does tibial or femoral torsion have a
greater negative mechanical influence? The
importance of different maltorsions is unclear.
When the patient stands with their feet parallel, the patella should be facing forward. In
patients with excessive external tibial torsion, we
can see a squinting patella and a genu varum
(Figs. 5 and 6). The varus in patients with
external tibial rotation may be real, or it may be a
reflection of the tibial torsion (thus pseudovarus). In the same way, we can observe a
“pseudo-valgus” in patients with pathological
femoral anteversion (Fig. 7). Evidently, we must
only correct the transverse deformity in these
cases, not the coronal one. The combination of
V. Sanchis-Alfonso and R. A. Teitge
increased femoral anteversion and increased
external tibial torsion has been termed miserable
malalignment syndrome that includes squinting
patella, genu varum, genu recurvatum and pronated foot (Fig. 8).
In the prone position, the proportion of
internal to external rotation of the hips in
extension must be measured [30]. If internal
rotation exceeds external rotation by more than
30 degrees, there is increased femoral anteversion (Fig. 9). In cases with isolated excessive
external tibial torsion, internal and external
rotation are similar (Fig. 10).
Furthermore, it is important to evaluate the
foot progression angle. The “foot progression
angle” should be neutral when walking [31, 32].
Excessive femoral anteversion is manifested by a
gait pattern with an internal foot progression
angle (in-toeing) (Fig. 11) and external tibial
torsion by out-toeing. However, if excessive
femoral anteversion is associated with excessive
external tibial torsion (i.e., pan genu torsion or
miserable malalignment), the foot progression
angle will be neutral, and this combined longbone deformity may be concealed to the unwary
observer. It is therefore important to have a
patient appropriately unclad and note that the
knee progression angle is inward.
4.1.3 Measuring Torsion
In our clinical practice, we use the technique
described by Murphy and colleagues in 1987 to
measure femoral torsion [33]. This is the most
anatomic, accurate and reproducible method for
evaluating femoral anteversion (high intra- [ICC:
0.95–0.98] and inter-observer agreement [ICC:
0.93]) [34]. Murphy and colleagues reported that
the common method of running a line along the
femoral neck on a CT image underestimated the
actual anteversion by a mean 13° [33]. The line
that is used in the most common method, like the
axis of the femoral neck, is not the true axis of
the femoral neck. External tibial torsion is measured as the angle between the posterior aspect of
the tibial metaphysis and the ankle joint line. Our
normal reference values are femoral anterversion
of 13º for both sexes and external tibial torsion of
21º in males and 27° in females [35, 36].
Surgical Treatment of Anterior Knee Pain …
A
141
B
C
D
Fig. 5 A, B Squinting patella in a patient with excessive
external tibial torsion. C Normal skeletal alignment in the
transverse plane. Female with femoral anteversion of 13º
and external tibial torsion of 27º. D Female with an increase
in external tibial torsion. To keep the foot progression angle
normal, the knee joint points inward causing increased
strain on the knee. The hip appears internally rotated with
the greater trochanter pointing somewhat anteriorly. (A, B
—Republished with permission of AME Publishing
Company. From Sanchis-Alfonso V, et al. Evaluation of
anterior knee pain patient: clinical and radiological assessment including psychological factors. Ann Joint, 3:26,
2018. C, D—Republished with permission of Elsevier
Science & Technology Journals. From Teitge RA. Patellofemoral Disorders Correction of Rotational Malalignment
of the Lower Extremity. In: Noyes´s Knee Disorders:
Surgery, Rehabilitation, Clinical Outcomes, 2017; permission conveyed through Copyright Clearance Center, Inc.”)
4.1.4 Surgical Considerations
Rotational osteotomies are often performed
according to the experience of the surgeon. Since
torsion is the angle measured between the joints,
a change in torsion of the femur may be anywhere between the hip joint and the knee joint.
There is no evidence that the proximal, mid-shaft
or distal location of the osteotomy is preferable.
The authors prefer femoral rotational osteotomy
at the intertrochanteric level to prevent any
scarring to the quadriceps muscle in the region of
the knee. However, the correction must be made
near the knee joint, usually in the supracondylar
region, if there is an associated varus or valgus
deformity. The situation is similar in the tibia. It
matters little whether a rotational correction for
maltorsion is performed in the proximal, mid or
distal tibia except that it should be performed
below the level of the tibial tubercle. Recently,
Winkler and colleagues [37] have shown that
142
V. Sanchis-Alfonso and R. A. Teitge
4.2 Coronal Plane Osteotomy
for Genu Valgum
Fig. 6 Physical findings in a patient with excessive
external tibial torsion
increased external tibial torsion is an
infratuberositary deformity and is not correlated
with a lateralized position of the tibial tuberosity.
The surgeon may select any internal (or external)
fixation device which allows for maintaining the
correction.
Fig. 7 “Pseudo-valgus” in a
patient with pathological
femoral anteversion. In this
case, the valgus was not real.
It was due to the inward
position of her flexed knee,
that is, in this case it was
secondary to a femoral
anteversio of 51º. (Courtesy
of Robert A. Teitge, MD)
Both torsional deformities and coronal plane
deformities are associated with AKP patients in
many cases. The most common multiplanar
deformity in AKP patients is internal femoral
torsion and genu valgum (Fig. 12) [13]. A valgus
limb with the mechanical axis passing through
the knee lateral to its normal position increases
the lateral component of the quadriceps vector
creating an imbalance in forces acting on the
patella. Multiplanar deformity appears to add the
effects from each separate deformity [13]. In
these cases, both deformities must be corrected
[13]. We must combine both varus and external
rotation (Fig. 12) [13]. Multiplanar correction is
somewhat more challenging than monoplanar
correction but very beneficial. Precision surgery
is the key to success.
It is a common misconception that a valgus
deformity should always be corrected with a
distal femoral osteotomy. The crucial question in
osteotomy surgery is about where the deformity
is located. The answer to this question is very
important because we must put the osteotomy
where the deformity is. In contrast with the
widespread belief that valgus malalignment is
caused by a femoral deformity, Eberbach and
colleagues [38] have demonstrated that the valgus knee is secondary to a tibial deformity in a
great number of the cases (41%). Moreover, a
combined femoral- and tibial-based deformity
Surgical Treatment of Anterior Knee Pain …
A
B
143
C
D
E
Fig. 8 A, B, C Miserable malalignment syndrome.
D Female with 30º increase in femoral anteversion. The
knee joint points in the same direction, slightly inward, as
in the normal female, but the greater trochanter points
posteriorly. At some point, the hip cannot externally rotate
enough to keep the knee joint pointed forward. E Female
with a 30º increase in both femoral anteversion and
external tibial torsion. Note the trochanter is pointed more
anterior than normal, and with the foot progression angle
normal, the knee joint axis points markedly inward. (D, E
—Republished with permission of Elsevier Science &
Technology Journals. From Teitge RA. Patellofemoral
Disorders Correction of Rotational Malalignment of the
Lower Extremity. In: Noyes´s Knee Disorders: Surgery,
Rehabilitation, Clinical Outcomes, 2017; permission
conveyed through Copyright Clearance Center, Inc.”)
(Fig. 12) is more frequent than an isolated
femoral-based deformity (27% vs. 23.6%). The
clinical relevance of the paper by Eberbach and
colleagues [38] is that varus osteotomies to treat
genu valgum must be performed at the proximal
tibial site in 41% of the cases or as a double-level
osteotomy in a relevant number of patients
(45.5% of cases) to avoid an oblique joint line
(Fig. 12). The ideal osteotomy site was the distal
femur in only 13.6% of cases.
One of the most frequent symptoms of genu
recurvatum is AKP. In these cases, continuous
hyperextension of the knee will provoke a
hyperpressure on the anterior cartilage of the
tibial plateau on the one hand and infrapatellar fat
pad impingement on the other [39]. Fat pad
impingement will cause chronic inflammation of
the infrapatellar fat pad through repetitive
microtrauma [39]. All of this will be accountable
for the pain. When the angle of recurvatum is
greater than 15º, it is considered pathological
[40].
Non-operative treatment consisting of muscle
strength training and anti-hyperextension bracing
is the first step of treatment. After the failure of
non-operative treatment, we must consider surgical treatment. There are several options for
surgical treatment:
4.3 Osteotomies in the Sagittal Plane
—Genu Recurvatum
The term genu recurvatum describes a knee with
hyperextension of the tibia on the femur
(Fig. 13).
144
V. Sanchis-Alfonso and R. A. Teitge
Fig. 9 Evaluation of a
patient with excessive right
femoral anteversion in the
prone position
(1) Opening wedge osteotomy (Fig. 14). One
cut from anterior to posterior and then a
wedge of bone graft anteriorly with a plate
anteriorly with compression of the graft.
Healing with the bone wedge is not so
rapid, which is one complaint. With this
osteotomy, we will gain length.
(2) Closing wedge posteriorly. This is a much
larger dissection and there is more risk of
moving the soft tissues away. The wedge
may be cut from the side rather than straight
posteriorly. The leg is obviously shortened.
The correction depends on the accuracy of
planning and the removal of the wedge.
Placing a sufficiently long plate on the
posterior tibia is not so easy as the space is
tight.
(3) Philipp Lobenhoffer has proposed a crescentic osteotomy using the Synthes crescent
saws usually used for veterinary cases
referred to as TPLO (tibial plateau leveling
osteotomy). There is minimal bone loss and
a very broad surface area. The trick is to
locate the center of rotation and place a K-
Surgical Treatment of Anterior Knee Pain …
145
wire exactly on the correct coronal and
sagittal plane. We can approach the tibia
laterally by moving the anterior compartment distally. Then you would not have to
move the pes and MCL. This type of
osteotomy would be of help in cases with a
minus variant of the tibial tubercle in which
it would be difficult to make a good
osteotomy of the TT (Figs. 15, 16 and 17).
5
Fig. 10 Evaluation of a patient with normal femoral
anteversion in the prone position. This patient had an
excessive external tibial torsion measured with CT
Fig. 11 The patients are always aware of what is wrong
with them. The doctor only has to listen to what they say.
Here, this girl was asked to walk as she normally walks
and then to exaggerate the way she thinks she walks. We
Take Home Messages
– The gold standard in the treatment of AKP is
physical therapy within the patient’s envelope
of function.
– Surgery for AKP is a last resort, and it is very
often not needed. Surgical treatment must be
considered only when well-documented
anomalies amenable to a specific targeted
can clearly see how the patient rotates the limb internally
during gait. An excessive femoral anteversion is manifested by an in-toeing gait
146
Fig. 12 Left valgus deformity (22º) in a patient with
disabling AKP and lateral patellar instability. Left CD
index 1.5. This patient also had a left femoral anteversion
of 54º and a left external tibial torsion of 56º. Intraoperative X-rays after lateral supracondylar open wedge
Fig. 13 Genu recurvatum. Anterior subluxation of the
femur on the tibia related to the recurvatum deformity
V. Sanchis-Alfonso and R. A. Teitge
varus rotational osteotomy of the femur (7º of varus and
35º of external femoral rotation) and a medial closed
wedge varus rotational osteotomy of the tibia below the
tibial tuberosity (15º varus and 30º internal rotation) was
performed
intervention are present, especially when there
is evidence of focal patellofemoral overload.
– Certain surgical procedures in a carefully
selected patient can significantly improve
AKP resistant to all non-operative alternatives. Every surgical treatment ought to be
tailor-made just because every person is different. For example, when focal pathology,
such as synovial hypertrophy around the
inferior pole of the patella or peripatellar
synovitis can be identified, procedures to
debride the inflammatory foci in the synovium
can be very successful.
– Finally, in some cases, major surgery like the
osteotomy to correct abnormal femoral and
tibial torsion may be essential for the optimal
treatment of AKP. In our experience, AKP
patients with an underlying torsional abnormality respond very well to derotational corrective osteotomies.
Surgical Treatment of Anterior Knee Pain …
Fig. 14 Genu recurvatum. Opening wedge osteotomy
Fig. 15 Genu recurvatum.
Crescentic osteotomy above
of the patellar tendon
insertion
147
148
Fig. 16 Genu recurvatum. Crescentic osteotomy. Preop versus Postop
Fig. 17 Genu recurvatum. Crescentic osteotomy. Preop versus Postop
V. Sanchis-Alfonso and R. A. Teitge
Surgical Treatment of Anterior Knee Pain …
6
Key Message
– We must operate on a patient with AKP when
an appropriate conservative treatment has
failed, and the patient has severe pain and a
significant limitation in their daily life and
there is an objective cause of the pain that is a
candidate for surgery with predictably good
results. The best way to avoid a patellofemoral surgery that will lead to an unsuccessful
result is to stick to operations that come off
with a high-degree of success.
References
1. Post WR, Dye SF. Patellofemoral Pain: an enigma
explained by homeostasis and common sense. Am J
Orthop (Belle Mead NJ). 2017;46(2):92–100.
2. Post WR. “Conservative” surgical treatment for
anterior knee pain. Ann Joint. 2018;3:68.
3. Sanchis-Alfonso V, McConnell J, Monllau JC, et al.
Diagnosis and treatment of anterior knee pain.
JISAKOS. 2016. https://doi.org/10.1136/jisakos2015-000033.
4. Collins NJ, Bierma-Zeinstra SM, Crossley KM, et al.
Prognostic factors for patellofemoral pain: a multicentre observational analysis. Br J Sports Med.
2013;47(4):227–33.
5. Sanchis-Alfonso V. Treating complications of operative management for patellofemoral pain. Ann Joint.
2018;3:27.
6. Dye SF. The pathophysiology of patellofemoral pain:
a tissue homeostasis perspective. Clin Orthop Relat
Res. 2005;436:100–10.
7. Tensho K, Akaoka Y, Shimodaira H, et al. What
components comprise the measurement of the tibial
tuberosity-trochlear groove distance in a patellar
dislocation population? J Bone Joint Surg Am.
2015;97(17):1441–8.
8. Lee TQ, Anzel SH, Bennett KA, et al. The influence
of fixed rotational deformities of the femur on the
patellofemoral contact pressures in human cadaver
knees. Clin Orthop. 1994;302:69–74.
9. Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. J Orthop Sports Phys Ther.
2003;33:686–93.
10. Passmore E, Graham HK, Pandy MG, et al. Hip and
patellofemoral joint loading during gait are increased
in children with idiopathic torsional deformities. Gait
Posture. 2011;63:228–35.
149
11. Teitge RA. Patellofemoral syndrome a paradigm for
current surgical strategies. Orthop Clin N Am.
2008;287–311.
12. Teitge RA. Does lower limb torsion matter? Tech
Knee Surg. 2012;11:137–46.
13. Teitge RA. The power of transverse plane limb malalignment in the genesis of anterior knee pain—
clinical relevance. Ann Joint. 2018;3:70.
14. Sanchis-Alfonso V, Montesinos-Berry E. Is lateral
retinacular release still a valid surgical option? From
release to lengthening. Ann Transl Med. 2015;3
(19):301.
15. Lattermann C, Drake GN, Spellman J, et al. Lateral
retinacular release for anterior knee pain: a systematic review of the literature. J Knee Surg. 2006;19
(4):278–84.
16. Fithian DC, Paxton EW, Post WR, et al. International
Patellofemoral Study Group. Lateral retinacular
release: a survey of the International Patellofemoral
Study Group. Arthroscopy. 2004;20(5):463–468.
17. Huddleston HP, Drager J, Cregar WM, et al. Trends
in lateral retinacular release from 2010 to 2017.
J Knee Surg. https://doi.org/10.1055/s-0041-1731457
18. Sanchis-Alfonso V, Merchant AC. Iatrogenic medial
patellar instability: an Avoidable Injury. Arthroscopy. 2015;31(8):1628–32.
19. Kasim N, Fulkerson JP. Resection of clinically
localized segments of painful retinaculum in the
treatment of selected patients with anterior knee pain.
Am J Sports Med. 2000;28:811–4.
20. Felli L, Formica M, Lovisolo S, et al. Clinical
outcome of arthroscopic lateral retinacular release for
symptomatic bipartite patella in athletes. Arthroscopy. 2018;34(5):1550–8.
21. Maier D, Bornebusch L, Salzmann GM, et al. Midand long-term efficacy of the arthroscopic patellar
release for treatment of patellar tendinopathy unresponsive to nonoperative management. Arthroscopy.
2013;29(8):1338–45.
22. Rooney A, Wahba AJ, Smith TO, et al. The surgical
treatment of anterior knee pain due to infrapatellar fat
pad pathology: a systematic review. Orthop Traumatol Surg Res. 2015;101(4):469–75.
23. Smallman TV, Portner OT, Race A, et al. Arthroscopic untethering of the fat pad of the knee: Release
or resection of the infrapatellar plica (Ligamentum
Mucosum) and related structures for anterior knee
pain. Arthrosc Tech. 2018;30;7(5):e575-e588.
24. Miltner O, Siebert CH, Schneider U, et al. Patellar
hypertension syndrome in adolescence: a three-year
follow up. Arch Orthop Trauma Surg. 2003;123
(9):455–9.
25. Vega J, Golanó P, Pérez-Carro L. Electrosurgical
arthroscopic patellar denervation Arthroscopy.
2006;22(9):1028.e1-1028.e3.
26. Flandry F, Hughston JC. Complications of extensor
mechanism surgery for patellar malalignment. Am J
Orthop (Belle Mead NJ). 1995;24(7):534–43.
150
27. Stevens PM, Gililland JM, Anderson LA, et al.
Success of torsional correction surgery after failed
surgeries for patellofemoral pain and instability.
Strategies Trauma Limb Reconstr. 2014;9(1):5–12.
28. Lee TQ, Yang BY, Sandusky MD, et al. The effects
of tibial rotation on the patellofemoral joint: assessment of the changes in in situ strain in the peripatellar
retinaculum and the patellofemoral contact pressures
and areas. J Rehabil Res Dev. 2001;38:463–9.
29. Liao TC, Yang N, Ho KY, et al. Femur rotation
increases patella cartilage stress in females with
patellofemoral pain. Med Sci Sports Exerc. 2015;47
(9):1775–80.
30. Carson WG Jr, James SL, Larson RL, et al.
Patellofemoral disorders: physical and radiographic
evaluation. Part I: Physical examination. Clin Orthop
Relat Res. 1984;(185):165–177.
31. Staheli LT. Torsion-treatment indications. Clin
Orthop Relat Res. 1989;247:61–6.
32. Staheli LT, Corbett M, Wyss C, et al. Lowerextremity rotational problems in children. Normal
values to guide management. J Bone Joint Surg Am.
1985;67(1):39–47.
33. Murphy SB, Simon SR, Kijewski PK, et al. Femoral
anteversion. J Bone Joint Surg Am. 1987;69
(8):1169–76.
V. Sanchis-Alfonso and R. A. Teitge
34. Kaiser P, Attal R, Kammerer M, et al. Significant
differences in femoral torsion values depending on
the CT measurement technique. Arch Orthop Trauma
Surg. 2016;136(9):1259–64.
35. Yoshioka Y, Cooke TD. Femoral anteversion:
assessment based on function axes. J Orthop Res.
1987;5(1):86–91.
36. Yoshioka Y, Siu DW, Scudamore RA, et al. Tibial
anatomy and functional axes. J Orthop Res. 1989;7
(1):132–7.
37. Winkler PhW, Lutz PM, Rupp MC, et al. Increased
external tibial torsion is an infratuberositary deformity and is not correlated with a lateralized position
of the tibial tuberosity. Knee Surg Sports Traumatol
Arthroscopy. 2021;29:1678–85.
38. Eberbach H, Mehl J, Feucht MJ, et al. Geometry of
the valgus knee: Contradicting the dogma of a
femoral-based deformity. Am J Sports Med. 2017;45
(4):909–14.
39. van Raaij TM, de Waal MJ. Anterior opening wedge
osteotomy of the proximal tibia for anterior knee pain
in
idiopathic
hyperextension
knees.
Int
Orthop. 2006;30(4):248–52.
40. Moroni A, Pezzuto V, Pompili M, et al. Proximal
osteotomy of the tibia for the treatment of genu
recurvatum in adults. J Bone Joint Surg Am.
1992;74:577–86.
The Failed Patella. What Can We Do?
Vicente Sanchis-Alfonso, Julio Domenech-Fernandez,
and Robert A. Teitge
1
Introduction
The title of this chapter has been borrowed from
the world of spinal surgery (“The Failed Spine”).
It is a term that we are going to use to describe
the situation of those patients who did not have a
successful outcome after a surgery that was carried out to resolve Anterior knee pain (AKP). It
resulted in the pain worsening considerably in
most of the patients. That does not necessarily
mean that the surgery was botched. Even with
the best surgeon and with the best indication,
patellofemoral surgery to treat AKP might fail. In
this case, the failure is the consequence of a
surgical complication, that is, an adverse event
caused by factors that are outside the orthopedic
surgeon’s control. Obviously, it is a consequence
of a wrong diagnosis or an incomplete diagnosis
on some occasions. In other cases, it is a result of
an error in the surgical indication or in the surgical technique that will create a new pathology.
A good example of a “Failed Patella” consequence of a poorly performed or badly indicated
surgery for AKP is Iatrogenic medial patellar
instability (IMPI). Finally, we must not forget
V. Sanchis-Alfonso (&) J. Domenech-Fernandez
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
R. A. Teitge
Wayne State University, Detroit, MI, USA
that other cause of a failed patella, inadequate
physical therapy after surgery.
Complications in surgery can occur regardless
of the quality of care or competence of the
orthopedic surgeon. Obviously, all surgical procedures carry risks of complications. Thus, it is
important to prevent unnecessary surgeries to
diminish the number of complications. Some
types of patellofemoral surgeries are more predictable in alleviating or eliminating pain than
others. For instance, in our personal experience, a
rotational osteotomy is much more predictable in
alleviating AKP than other surgeries. Therefore,
a way to avoid a failed patella is to perform only
operations with a confirmed high degree of success. Therefore, caution is necessary when recommending surgical treatment for AKP,
particularly for “well-meaning, trigger-happy
orthopedic surgeons”.
The patient with severe pain after a patellofemoral surgery whose objective was to remove
pain represents a real challenge for the orthopedic surgeon specialized in the knee. In our
experience, most AKP surgeries are done to
rectify the complications or bad results from
previous, poorly performed or badly indicated
AKP surgeries. The goals of this chapter are:
(1) to give diagnostic advice for evaluating the
failed patellofemoral surgery patient, (2) to provide best practices for avoiding complications
around patellofemoral surgery in AKP treatment,
and (3) to present operative salvage procedures
to treat these cases.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_10
151
152
2
V. Sanchis-Alfonso et al.
General Principles
in the Management of Failed
Patella
Having a knowledgeable surgeon and a correct
diagnosis of the failure are crucial to solving a
“Failed Patella”. The key question we must ask
ourselves is: Why did the previous surgery fail?
If we do not find an answer to this question, we
will not be able to resolve the pain that our
patient presents.
2.1 Correct Diagnosis—Listen
to the Patient
Each patient with a “failed patella” is different.
A careful history must be taken, with close
attention being paid to what the patient reports.
Speaking to a patient is crucial because they will
usually tell us, in their own words, what is
wrong. It is always important to talk with the
patient and especially listen to them. Quite possibly, it is even much more important in the
patient with a surgical failure. Moreover, a good
physical examination and imaging are also very
important. We are particularly surprised by the
low quality of imaging studies that we see in
patients who are referred to us for patellofemoral
revision surgery.
2.2 Rule Out Inappropriate Physical
Therapy
It is not always the surgeon who is responsible
for the failure. We must not forget the damage
that the physiotherapist can do during postoperative rehabilitation. Sometimes pain aggravation
after surgery is a consequence of inappropriate
postoperative physical therapy. For instance,
strengthening of the musculature should be performed in a “safe range of flexion–extension” to
avoid patellofemoral overload. Steinkamp and
colleagues [1] have demonstrated that between 0
and 45° closed kinetic chain exercises cause
smaller moments, lesser reaction forces, and less
pressure in the patellofemoral joint (PFJ). Due to
that, they are less harmful to the patient. Nevertheless, beyond 45°, the open chain exercises are
the ones with smaller moment, lesser reaction
forces, and less pressure. If we do not follow
these premises, we run the risk of causing
patellofemoral overload that will result in the
appearance of pain in the anterior aspect of the
knee. This is just one of the many examples that
can cited relative to the damage that the physiotherapist can cause.
2.3 Rule Out Central Sensitization
Pain persistence in an operated AKP patients may
be the result of central sensitization (CS) [2]. One
of the mechanisms that can explain the transition
from acute to chronic pain is the phenomenon of
CS. It is defined as the “increased responsiveness
of nociceptive neurons in the central nervous
system” [3]. According to Woolf [3], the hallmarks of central sensitization include: (1) allodynia (that is, pain in the presence of a non-noxious
stimulus); (2) primary hyperalgesia, (that is, pain
hypersensitivity at the affected site) and (3) secondary hyperalgesia (that is, pain hypersensitivity
in uninjured tissues beyond the affected area). CS
is the neurophysiological phenomenon in which
the persistent transmission of pain produces a
reorganization of the transmission mechanisms in
the central nervous system (CNS). It is what
makes the perception of pain permanent [3]. In a
situation of sustained chronic pain, the facilitatory
and inhibitory modulatory circuits are reorganized, creating new synapses and producing
changes in excitability at the central level. The
increase in peripheral nociceptive afferences and
the increase in activity at the level of the spinal
cord produces an alteration in the processing of
pain transmission at the level of the spinal cord
and brain. That perpetuates the painful sensation
even though the peripheral lesion that initially
produced the pain has disappeared. It is noteworthy that there is no injury to the nerve structures in CS, but rather a physiological change that
makes the painful sensation persist.
The Failed Patella. What Can We Do?
The phenomenon of pain centralization is
frequent in different musculoskeletal conditions
that present with chronic pain [4, 5]. Thus, it has
been estimated that centralization of pain occurs
in 30% of cases of osteoarthritis and in close to
100% of patients with fibromyalgia and whiplash
syndrome. It has been suggested that it appears in
a third of patients with chronic low back pain and
in all patients with failed back surgery syndrome.
The Central Sensitization Inventory (CSI) is a
self-report instrument designed to identify
patients who have pain characteristics related to
CS. This questionnaire is the most widely
method used in clinical setting. Patients are asked
25 questions aimed at assessing CS symptoms.
The patient scores each answer on a Likert scale
from 0 (never) to 4 (always). A score of more
than 40 indicates the presence of CS [6].
Sanchis-Alfonso and colleagues [7] studied
the presence of CS using the CSI questionnaire.
It was done with a sample of 44 patients with
chronic AKP that were compared to a group of
44 healthy subjects matched for age and sex.
They found a prevalence of central pain sensitization of 36% in AKP patients versus 4% in the
healthy population. The study also explored the
participation of CS in both pain and disability as
well as in a list of psychological variables that
earlier studies have demonstrated as having an
influence on the clinical severity of AKP (i.e.,
depression, anxiety, kinesiophobia and catastrophizing). No differences were found in the level
of pain measured with VAS between patients
with or without centralized pain. Patients with
pain centralization had the same intensity of pain
as patients without centralization. However, AKP
patients with CS had significantly greater disability than patients without centralization as
measured with the Kujala scale (41.6 vs. 53.6,
respectively; p < 0,05). This difference coincides
with the value of 12 that is considered Minimal
clinically important differences (MCIDs) when
using the Kujala scale [8]. These findings suggest
that pain chronification in AKP patients that is
mediated by the phenomenon of CS is more
disabling even though their pain intensity may
not be greater. In accordance with studies in
other musculoskeletal pathologies, the values on
153
the CSI scale correlated with the levels of anxiety
and depression, as occurs in our sample of
patients. Nevertheless, the CSI score did not
correlate with levels of catastrophizing and
kinesiophobia, suggesting that they are independent constructs. Catastrophizing and kinesiophobia are psychological variables that have
been shown to be associated with disability in
AKP patients [9, 10]. CS is a neurophysiological
phenomenon in which pain modulation is altered
by its facilitatory and inhibitory mechanisms in
chronic pain conditions. In some AKP patients,
CS is revealed as an explaining factor that
influences disability independently of catastrophizing and kinesiophobia.
Further research is needed to evaluate the
prognostic capabilities of CS and its relationship
with therapeutic management. However, we
believe that the presence of CS should not be the
justification for not continuing to evaluate the
patient and send her to a “Pain Unit”. There are
patients with high values in the CS score who have
objective structural causes that provide an explanation for the pain and that had gone undetected.
Once that pain is treated to improve or eliminate it,
it causes the CS score to drop drastically.
2.4 Do Not Forget the Psychological
Evaluation
One must not forget the psychological evaluation
of the patient. Our data (see chapters “Evaluation
of Psychological Factors Affecting Anterior Knee
Pain Patients: The Implications for Clinicians
Who Treat these Patients”) shows that the presence of psychological factors in these patients is a
limitation to recovery. That is, psychological
factors are barriers to recovery. Once again, the
presence of those factors should not be the excuse
for not continuing to study the patient and refer
him to the psychiatrist. “Crazy” patients with a real
pathology get back to normal or are at least much
better mentally after effective treatment. Therefore, they should not be ignored. We need to look
hard for a real pathology and try to help them, even
if it takes more patience and tender loving care
from the provider.
154
2.5 Do Not Ignore the Mechanics
Which Caused the Tissue
Failure, if so, Another
Failed Result Ensues
We must do a complete physical examination to
uncover all of the anatomic abnormalities, of
which there are often many. You should strive to
restore the normal anatomy, because that will
create a better biomechanical environment for the
tissue. When any abnormal anatomy is uncovered, a question must be answered. How does
this change the normal biomechanics? Biomechanics is crucial. Orthopedic surgery is a
mechanical engineering discipline. If you repair a
failed tissue (bone, ligament or cartilage) and
ignore the mechanics which caused the tissue
failure, you will usually have a failed result.
2.6 In Short …
We must look for, identify and quantify injuries
or anatomical anomalies that can be corrected.
Moreover, we must have the conviction that they
are the most responsible for the pain that the
patient we are evaluating has. Find the pain
generator is crucial to the success of a surgery.
We must always evaluate the following:
(1) skeletal alignment (i.e., Does the patient have
a neutral mechanical axis, or is varus or valgus
present?; Does he or she have abnormal femoral
and/or tibial torsion?; Does the patient have a
genu recurvatum or genu flexum?); (2) the ligaments (i.e., Does the patient have excessive lateral displacement of the patella or excessive
medial displacement or both?); (3) the articular
cartilage (i.e., complete or partial loss, location of
the loss, possibility to shift contact to intact
cartilage); and (4) the muscle (i.e., symmetrical
atrophy versus gross imbalance).
The surgeon must determine what surgical
procedure, if any, has the potential to improve
the patient’s condition and, most importantly, not
harm them. We, as orthopedic surgeons, must
never forget the principles of Hippocratic medicine: “Primum non nocere”. We must not do
harm or make a poor situation much worse. We
V. Sanchis-Alfonso et al.
must make the patients stop saying the typical: “I
wish I hadn’t been operated on.”
We must note that a failed patella does not
necessarily require more surgeries. In some
cases, repetitive transcranial magnetic stimulation, radiofrequency neurotomy, spinal cord
stimulation or implantable pumps that supply
medication to control the pain could be necessary. However, these techniques are beyond the
scope of this chapter.
Confronting the failed patella of the patient
provides a great stimulus for intellectual activity.
It provides an opportunity for new observations. It
is an opportunity to learn something new each day.
3
Iatrogenic Medial Patellar
Instability and Multidirectional
Patellar Instability
Iatrogenic medial patellar instability (IMPI) is a
good example of a new pathology created by the
orthopedic surgeon as a result of a poorly performed or badly indicated surgery. IMPI is an
objective condition with its own personality that
causes disabling AKP and severe disability [11,
12]. In all the cases of the series of the authors of
this chapter, there was a previous surgical procedure consisting of an “extensive” isolated lateral retinaculum release (LRR) or an inadequate
selection of the patient on whom LRR was performed [11, 12]. Sometimes, LRR has been
associated with a proximal and/or distal realignment to treat AKP resistant to conservative
treatment or to treat lateral patellar instability
[12]. Regarding “extensive” LRR, the first author
is weary of hearing this nonsense, “The previous
surgeon did not release of the lateral retinaculum.
So, I am going to complete this release like it
should have been done”. It is a great mistake.
Often, the pain and disability from IMPI are
much worse and distinct than the preoperative
symptoms for which the operation was performed, causing important psychological problems [12]. The percentage of patients with
anxiety, depression catastrophizing and kinesiophobia is greater in patients with IMPI than in the
more “typical” AKP patients. The figures are as
The Failed Patella. What Can We Do?
follows: kinesiophobia (100% vs. 80%), catastrophizing (41% vs. 37%), anxiety (59% vs.
37%), and depression (24% vs. 11%) [12]. Frequently, psychological involvement is overlooked by the orthopedic surgeon. However, it is
an important issue because psychological factors
are barriers to recovery (See chapter “Evaluation
of Psychological Factors Affecting Anterior
Knee Pain Patients: The Implications for Clinicians Who Treat these Patients”).
IMPI is more frequent than we had thought. It
might be underdiagnosed because it is still not a
well-known entity. Most of these patients go
from one doctor to another until they find a
doctor who gives a correct diagnosis and an
appropriate solution to their problem. These
patients have frequently visited several physicians who had told them that there was nothing
that could be done to solve their problem. Then,
the patient comes to our office with a large folder
full of radiological studies (MRI, CT scan, Xrays) that are identified as normal or as “lateral
patellar subluxation” or “chondromalacia patellae”, at the most. There is question we should ask
ourselves. Are these radiologically “normal” tests
enough to rule out an objective condition that
justifies the severe pain the patients suffer? The
answer is an emphatic no.
Diagnosis of IMPI. Medial Patellar Instability
sees you. Do you see it?
The first step in diagnosing a pathological condition is to know that it exists. This was clearly
stated by Jack Hughston in his well-known sentence: “You may not have seen it, but maybe it has
seen you”. In our series, many patients have had
to visit more than three doctors before obtaining a
diagnosis and an appropriate treatment. This
demonstrates that it is a clinical condition that
most orthopedic surgeons do not know about.
Therefore, we believe that there is a need to
communicate the diagnostic procedures for recognizing this clinical condition far and wide.
The most important findings for diagnosing
IMPI are (1) pain and tenderness at the site of the
LR defect; (2) increased passive medial patellar
mobility when compared with the contralateral
normal knee; (3) pain and apprehension when
155
medial stress is applied to the patella; and (4) a
positive Fulkerson relocation test [13]. To perform this test, the patella is held slightly in a
medial direction with the knee extended. Then,
we flex the knee while letting go of the patella,
which causes the patella to go into the femoral
trochlea. In patients with medial subluxation, this
test reproduces the patient’s symptom.
In patients with IMPI, there is significant pain
relief with a “reverse” McConnell taping
(Fig. 1). Similarly, the application of a patellar
brace with the buttress pad or strap on the medial
side will minimize or eliminate symptoms (e.g.,
Trupull brace, DJ Orthopedics, Vista, California,
USA). This is a good way to confirm our diagnosis before indicating a surgical treatment.
Multidirectional Patellar Instability
On some occasions, IMPI is associated with
lateral patellar instability due to a deficiency of
the medial patellofemoral ligament (MPFL). We
must remember that another restraint to medial
patellar displacement, apart from the lateral retinaculum, is the MPFL (Fig. 2). In these cases,
we are faced with a multidirectional instability of
patella.
Figure 3 Belongs to a patient operated on for
lateral patellar instability with an LRR. The
patient had severe trochlear dysplasia. The
patient developed an IMPI that was associated
with her previous situation of lateral patellar
stability. We are therefore facing a typical case of
multidirectional patellar instability in which a
sulcus sign similar to that seen in multidirectional
shoulder instabilities can be seen (Fig. 4).
Evaluation of IMPI
Ideally, we should evaluate AKP patients, and
IMPI should not be an exception, during dynamic
activities that trigger or aggravate the symptoms.
This should be done under realistic loading conditions, for example, the stair descending test. In
patients with IMPI, kinematic analysis demonstrates a stair descending pattern with knee
extension (Fig. 5). The knee extension could be a
strategy to avoid instability and therefore pain.
The patella goes from medial to lateral with knee
flexion. This provokes a sudden giving way that
156
A
c
Fig. 1 Technique for application of reverse McConnell
taping on a patient’s right knee. A Protective tape. B,
C Application of tape. D Definitive tape in place. (L,
lateral; M, medial; P, patella). “Reprinted from
V. Sanchis-Alfonso et al.
B
d
Arthroscopy, 31(8): 1628–1632, 2015, Sanchis-Alfonso
V and Merchant AC. Iatrogenic medial patellar instability:
An avoidable injury, with permission from Elsevier”
is much more disabling than a true lateral subluxation. So, the patient will avoid knee flexion to
avoid giving way and so avoid pain.
Finally, the stress radiograph [14] (Fig. 6) or
stress CT [15] (Fig. 7) will document and
quantify IMPI objectively. A comparison of the
normal side with the pathological side is more
important than the absolute amount of displacement. In some cases, IMPI is obvious without
stress studies (Fig. 8). In many cases IMPI is
associated with cartilage lesions on the lateral
patellar facet (Fig. 9).
Fig. 2 With medial displacement of the patella the MPFL
becomes tight. MPFL is a restraint to medial patellar
displacement. (Reused with permission from Baishideng
Publishing Group Inc. From Sanchis-Alfonso V, et al.
Failed medial patellofemoral ligament reconstruction:
Causes and surgical strategies. World J Orthop, 2017; 8
(2): 115–129)
How to Prevent IMPI?
Extensive LRR, or over-release with transection
of the vastus lateralis tendon, is a major cause of
IMPI (Fig. 10). Moreover, IMPI can be a result
The Failed Patella. What Can We Do?
Fig. 3 Multidirectional patellar instability. A Pathological
medial displacement of the patella. B, C Pathological
lateral displacement. Sulcus sign (black arrow). (Republished with permission of AME Publishing Company.
157
From V Sanchis-Alfonso, Treating complications of
operative management for patellofemoral pain, Ann Joint,
3:27, 2018)
osteotomy of the tibial tubercle. When it is done,
we must do careful preoperative planning. Kelman and colleagues [16] have shown, in a
cadaver study, that tibial tubercle medialization
does not pull the patella medially as much as it
pulls the tibia laterally. In these cases, we must
perform a lateral transfer of the tibial tubercle as
the first step of revision surgery, that is a reosteotomy of the TT.
Treating IMPI
Fig. 4 Sulcus sign in a patient with multidirectional
shoulder instability
of the release of a LR that was lax, showing poor
patient selection (Fig. 11A). An isolated LRR
should never be performed in the face of trochlear dysplasia (Fig. 11B), patella alta, or
hyperelasticity. If the LR is not tight, the surgeon
should not release it.
Another source of IMPI is the overmedialization of the tibial tuberosity as in the
case of Figs. 12, 13 and 14. We must be very
cautious when indicating a medialization
Reconstructive surgery includes direct ligament
repair or reconstruction of the lateral patellofemoral ligament. According to Teitge and Torga
[17], IMPI reappears after the first postoperative
year after lateral retinacular repair and imbrication. For this reason, the most logical approach
should be to reconstruct the lateral patellar
retinaculum.
The preference of the first author of this chapter
is the technique described by Jack Andrish [18]
(see video in Arthrosc Tech 2015; 4(3) e245-249)
because it is very anatomic (Fig. 15) and allows
for fine-tuning of the graft tension by adding
sutures to further tighten the graft (Fig. 16). As in
reconstruction of the MPFL, the surgeon should
tension the lateral reconstruction with the patella
engaged within the trochlea with the knee flexed at
30°. The purpose of this technique is to reconstruct
the deep transverse layer of the lateral retinaculum
158
V. Sanchis-Alfonso et al.
Fig. 5 Knee joint angle during stair descent
Table 1 Clinical outcome assessments after reconstruction of the deep transverse layer of the lateral retinaculum [12]
(Fig. 15) and not the lateral patellofemoral ligament. The deep layer of the lateral patellar retinaculum is reconstructed using a central strip of
the iliotibial band leaving it attached proximally
and attaching it to the midpoint of the patella [18].
We must note that it is a “salvage” procedure. It
does not address the original source of complaint.
Moreover, it cannot improve or reverse the
symptoms of osteoarthritis or bony malalignment.
Patients with symptomatic IMPI have chronic pain
and the etiology of chronic pain is multifactorial
with a different pathoneurophysiology than acute
pain, including psychological factors like pain
modulators. The reconstruction of the LR is a good
treatment for this difficult group of severely disabled patients (Table 1 and Fig. 17) [12].
The Failed Patella. What Can We Do?
159
A
B
C
Fig. 6 A 24-year-old woman with severe AKP (10/10—
VAS), a disabling disability (4/100—Kujala score), and
patellar instability in the left knee distinct and much worse
than the previous instability, anxiety, depression, catastrophizing ideas with pain and kinesiophobia. Left knee
was operated on 2 years ago, performing an Insall
proximal realignment and LRR due to lateral patellar
instability. She came to our office with conventional
radiographs, which were normal (A), and a CT at 0° that
showed correct radiological patellofemoral congruence
(B). The right knee was asymptomatic despite the patellar
However, we must note that the mere fact that the
patient can sublux and even dislocate their patella
medially is no guarantee that their pain and disability are directly due to the instability.
In cases of IMPI secondary to extensive LRR
and over-medialization of the tibial tuberosity,
the first step would be to perform a lateralization
of the tibial tubercle. After that, a reconstruction
of the lateral retinaculum is done.
D
subluxation and patellar tilt (B). The Fulkerson relocation
test for medial subluxation was positive. An axial stress
radiograph of the left knee allowed us to detect an
iatrogenic medial subluxation of the patella (medial
displacement of 15 mm) (C). Axial stress radiograph of
the asymptomatic right knee (D). Arrows represent the
force applied to displace the patella medially. The
symptoms disappeared after an isolated surgical correction of the medial subluxation of the patella using
iliotibial band and patellar tendon for repairing the lateral
stabilizers of the patella
4
Iatrogenic Patella Infera
Patella infera or patella baja is a devastating
complication after surgical treatment of AKP or
lateral patellar instability. It can provoke disabling
AKP and a severe restriction of knee range-ofmotion and can have significant effects on patient
function and lifestyle. Weale and colleagues [19]
160
V. Sanchis-Alfonso et al.
Fig. 7 A Axial stress CT of right knee. B An axial stress
CT of the left knee allows us to detect iatrogenic medial
subluxation of the patella (medial displacement of
13 mm). Arrows represent the force applied to displace
the patella medially. “Reprinted from Arthroscopy, 31(8):
1628–1632, 2015, Sanchis-Alfonso V and Merchant AC.
Iatrogenic medial patellar instability: An avoidable injury,
with permission from Elsevier”
Fig. 8 IMPI after lateral partial patellar facetectomy. In this
case, a patellofemoral prosthesis was put in place that did
away with the retropatellar pain but the patient continued
with a disabling pain and disability. A reconstruction of the
deep layer of the lateral retinaculum according to Andrish’s
tecnique was performed with a good result
Fig. 9 You can note an
evident medial displacement
of the patella when we apply a
force that displaces the patella
medially. Moreover, you can
see a chondral lesion of the
lateral facet of the patella
The Failed Patella. What Can We Do?
Fig. 10 Frequently found in IMPI patients; a sectioned
vastus lateralis tendon (red arrow) (A). B Reconstruction
of lateral retinaculum with iliotibial band (black arrow)
and reattachment of vastus lateralis (green arrow).
Fig. 11 A Patellar tilt in a
patient with non-tight lateral
retinaculum. B Severe
trochlear dysplasia. In both
cases an LRR was performed
resulting in IMPI
A
have demonstrated that there is a one-degree of
loss of knee flexion for each millimeter of patellar
tendon shortening. Moreover, if proper treatment
is delayed, early patellofemoral osteoarthritis
(PFOA) can present itself [20].
Patella infera may be a complication of
patellofemoral surgery or a consequence of a
surgical planification technique mistake. It often
occurs in association with arthrofibrosis following knee surgery. However, it is secondary to
distal realignment surgery in some cases. An
example is the distal tubercle transfer procedure
161
“Reprinted from Arthroscopy, 31(8): 1628–1632, 2015,
Sanchis-Alfonso V and Merchant AC. Iatrogenic medial
patellar instability: An avoidable injury, with permission
from Elsevier”
B
for patella instability in patients with patella alta
(Fig. 18). Other less frequent causes are patellar
tendon contracture after arthroscopic denervation
of the inferior pole of the patella (Fig. 19) or
after tourniquet paralysis of the quadriceps
(Fig. 20).
How to Avoid a Patella Infera?
Adequate preoperative planning is crucial.
Intraoperative visualization before tibial tubercle
fixation, and early restoration of quadriceps
activation are mandatory.
162
V. Sanchis-Alfonso et al.
Fig. 12 Stress axial radiography showing medial left
patellar instability. The arrow indicates the direction of
the force that displaces the patella medially. (Republished
with permission of AME Publishing Company. From V
Sanchis-Alfonso, Treating complications of operative
management for patellofemoral pain, Ann Joint, 3:27,
2018)
Fig. 13 Medial left patellar instability secondary to an
over-release of the LR (white arrow) associated with an
over-medialization of the tibial tuberosity. Overmedialization of the tibial tubercle can be avoided by
means of an intraoperative evaluation of the tubercle
sulcus angle. The intraoperative goal should be a tubercle
sulcus angle of 0°. (Republished with permission of AME
Publishing Company. From V Sanchis-Alfonso, Treating
complications of operative management for patellofemoral pain, Ann Joint, 3:27, 2018)
The Failed Patella. What Can We Do?
163
Fig. 14 In this case, we performed a reconstruction of
the deep layer of the lateral retinaculum and a lateral
transfer of the tibial tubercle. Here you can see the correct
postop patellofemoral congruence. There was a severe
patellar chondropathy. Despite the correct congruence and
kinematics of the PFJ, pain persisted in the anterior aspect
of the knee. Therefore, a patellofemoral arthroplasty was
performed with a good clinical result. (Republished with
permission of AME Publishing Company. From V
Sanchis-Alfonso, Treating complications of operative
management for patellofemoral pain, Ann Joint, 3:27,
2018)
Fig. 15 Anatomy of the lateral retinaculum. Patella (P),
deep lateral retinaculum (DLR), superficial lateral retinaculum (SLR), iliotibial band (ITB), and vastus lateralis
(VL). The true lateral patellofemoral ligaments are
thickenings of the lateral capsule. There is a lateral
epicondylopatellar ligament described and present in
some individuals, to varying degrees of frequency, but
the superficial oblique and deep transverse retinacular
layers are more consistent. The superficial oblique
retinaculum is quite thin. The deep transverse retinaculum
is stout, oriented in an optimal direction to restrain the
patella and attached to the lateral boarder of the patella
and the deep surface of the iliotibial band
164
A
V. Sanchis-Alfonso et al.
B
Fig. 16 Surgical technique. A The iliotibial band
(ITB) is detached from Gerdy’s tubercle and B then
reflected proximally beyond the lateral femoral epicondyle to be attached to the lateral border of the junction
of the middle and proximal thirds of the patella by
suturing to the remaining peripatellar retinacular tissue or
by using a suture anchor. To adjust tension, a series of
sutures are placed reattaching the posterior border of the
transferred tendon to the anterior border of the remaining
intact iliotibial band. “Reprinted from Arthroscopy, 31:
422–427, 2015, Sanchis-Alfonso V et al. Results of
isolated lateral retinacular reconstruction for iatrogenic
medial patellar instability, with permission from Elsevier”
Fig. 17 A 25-year-old female came to our institution with
a history of chronic severe anterior right knee pain, severe
disability, and patellofemoral instability refractory to
conservative treatment, for about 5 years. The Kujala
preoperative score was 36 points. The patient underwent
an Insall’s proximal realignment with LRR procedure at
the age of 18 due to recurrent lateral patellar dislocation.
Computed tomography (CT) examination at 0° extension
and quadriceps contraction shows lateralization of the
patella (A). Documentation of medial patellar instability
(B). Preoperative gait analysis revealed a significant
increment of the vertical heel contact peak force as a
result of a knee extension gait pattern (C). Follow-up CT
scan at 0° extension with quadriceps contraction demonstrates similar lateral displacement of the patella in both
knees (D), and stress CT revealed medial patellar stability
(E). Four months after surgery, she was symptom free.
Gait analysis was performed at this time to evaluate the
effects of surgical reconstruction of the lateral retinaculum
on gait parameters. No significant differences were seen
when compared to the contralateral limb, the gait pattern
being normal (F). At the time of surgery, an arthroscopy of
the right knee was performed. All the intra-articular
structures were intact, except for a patellar chondropathy
grade III, according to the Outerbridge classification,
located medially and a peripatellar synovitis. We did not
perform chondroplasty or peripatellar synovectomy. After
the arthroscopy, we performed an open reconstruction of
the lateral patellotibial ligament according to the technique
described by Hughston using the iliotibial band and the
patellar tendon. “Reprinted from The Knee, 14: 484–488,
2007, Sanchis-Alfonso V et al. Gait pattern normalization
after lateral retinaculum reconstruction for iatrogenic
medial patellar instability, with permission from Elsevier”
The Failed Patella. What Can We Do?
165
Fig. 18 This is the case of a PFOA in a patient with
severe iatrogenic patella infera after TT distalization
surgery. In this case, the patellar tendon is of normal
length. (Courtesy of JC Monllau, MD) (Republished with
permission of AME Publishing Company. From V
Sanchis-Alfonso, Treating complications of operative
management for patellofemoral pain, Ann Joint, 3:27,
2018)
Fig. 19 Patella infera following a patellar tendon contracture after arthroscopic denervation of the inferior pole of the
patella to treat disabling AKP. A Pre-operative MRI.
B Magnetic resonance image 1.5 years after arthroscopic
denervation of the inferior pole of the patella. (Republished
with permission of AME Publishing Company. From V
Sanchis-Alfonso, Treating complications of operative management for patellofemoral pain, Ann Joint, 3:27, 2018)
166
V. Sanchis-Alfonso et al.
Fig. 20 24-year-old woman operated on for AKP
recalcitrant to conservative treatment. An LRR was
performed. She presented a paralysis of the quadriceps
as a consequence of femoral nerve damage by the
ischemia cuff. Note the lowering of the left patella
(A) when compared with the height of the contralateral
healthy limb patella (B). (Republished with permission of
AME Publishing Company. From V Sanchis-Alfonso,
Treating complications of operative management for
patellofemoral pain, Ann Joint, 3:27, 2018)
Treating Patella Infera
for 8 weeks. Rehabilitation begins at week 8.
Burnett and colleagues [24] evaluated two techniques of reconstruction of the extensor mechanism of the knee using an extensor mechanism
allograft. There was Group I with the allograft
minimally tensioned and Group II with the allograft tightly tensioned in full extension. They
demonstrated that the results of surgery depend
on the initial tensioning of the allograft.
A loosely tensioned allograft results in a persistent extension lag and clinical failure. Allografts
that are highly tensioned in full extension can
restore active knee extension and result in clinical success. They concluded that an extensor
mechanism allograft transplantation will be successful only if the graft is initially tensioned
tightly in full extension [24].
Surgery is indicated when the Caton–Deschamps
ratio is less than or equal to 0.6 [21]. There are
two surgical options. If patella infera is the result
of a distalization of the tibial tubercle we should
perform an osteotomy of proximalization of the
tibial tuberosity (Fig. 18) [22]. If it has resulted
from the shortening of the patellar tendon, a Zlengthening of the patellar tendon would be the
prefer option (Figs. 19 and 21) [23]. In exceptional cases, the treatment of a patella infera
requires an extensor mechanism allograft transplantation. Figure 22 corresponds to a patient
with a patella infera at 10 years of performing an
extensor mechanism allograft. You can observe a
severe degeneration of the patellar tendon.
Therefore, it is not feasible to perform a Zlengthening of the patellar tendon. Considering
that, a decision was taken to make a new
extensor mechanism allograft. There was a good
functional result. A crucial technical aspect for
the success of this surgery is not to flex the knee
intraoperatively to evaluate the result of the
reconstruction [24]. After surgery, immobilization with the knee in full extension is put in place
5
The Failed Cartilage Surgery
We sometimes see patients operated on due to
patellofemoral pain who have undergone surgery
on the cartilage of the patella or the femoral
trochlea with poor results. The patient usually
The Failed Patella. What Can We Do?
Fig. 21 Patella infera with a shortened patellar tendon.
Lengthening of the patellar tendon by means of a Z-plasty
associated with patellofemoral arthroplasty. A reconstruction of the LR also was performed (white arrow).
167
(Courtesy of JC Monllau, MD) (Republished with permission of AME Publishing Company. From V SanchisAlfonso, Treating complications of operative management
for patellofemoral pain, Ann Joint, 3:27, 2018)
Fig. 22 Correction of the patella infera using an extensor mechanism allograft transplantation
168
has more severe pain than before surgery. If we
study the patient in detail, an underlying pathological torsion abnormality is detected in most of
the cases. In this case, the reason for the failure
of the surgery is a badly indicated surgery.
An inward pointing of the knee increases the
lateral direction of pull of the quadriceps.
Therefore, the pull on the MPFL and also medial
retinaculum and medial meniscopatellar ligament
is increased and the direction of pressure on the
patella is altered. This causes an increased compression on the lateral facet and a decrease on the
medial facet of the patella (Figs. 23 and 24). It
may be what is behind the persistence of pain
and the surgical failure of the cartilage surgery.
How to Avoid Failed Cartilage Surgery?
To avoid a cartilage surgery failure, the restoration of the normal anatomy is crucial as that will
create a better biomechanical environment for the
tissue. In this case, we are referring to the cartilage. If you repair failed tissue and ignore the
mechanics which caused the tissue failure, you
will usually have a failed result.
Furthermore, only correcting the torsional
abnormality will make the pain disappear in many
cases even if we do not treat the cartilage injury.
We must note that not all PFOA cases are associated with severe pain. In the PFJ, patellofemoral
Fig. 23 A If the knee joint moves forward, the compression on the PFJ and ligaments tensioned are balanced. B If
the knee joint twists inward from beneath the patella, the
MPFL is placed under increased tension, the compression
beneath the lateral facet increases, and the compression
V. Sanchis-Alfonso et al.
congruence and smooth kinematics are much
more important than normal articular cartilage.
Treating Failed Cartilage Surgery
The great problem after failed cartilage surgery
lies not in the lesion itself but in the age of the
patients, who are too young for “metal and
plastic”. In these cases, fresh allograft transplantation should be considered as a salvage
treatment procedure (Figs. 25 and 26).
Before any resurfacing technique, the PFJ and
the skeletal mal-alignment of the extremity must
be optimized to obtain satisfactory results.
A resurfacing technique is not a substitute for
skeletal realignment. In cases where the patellar
tracking and skeletal alignment of the extremity
are correct, an isolated resurfacing technique can
be performed (Figs. 25 and 26).
6
Rotational Osteotomy. A Game
Changer in the Treatment
of “Failed Patella”
What is a game changer? It might be a sudden
strategy that the usually winning opponent has
never imagined being used by the underdog team
to win the game. We really believe that rotational
osteotomy is a game changer in the treatment of
beneath the medial facet decreases. (Reused with permission from Elsevier. From Teitge RA. Patellofemoral
Disorders Correction of Rotational Malalignment of the
Lower Extremity. In: Noyes’s Knee Disorders: Surgery,
Rehabilitation, Clinical Outcomes, 2017)
The Failed Patella. What Can We Do?
169
Fig. 24 If the knee joint twists inward because the femur
twists inward, the lateral displacement pull on the patella
is increased, the strain on the MPFL is increased, the
compression on the lateral patellar facet is increased, and
the compression on the medial patellar facet is decreased.
The treatment must be to decrease the inward twist on the
knee joint, not to move the tubercle medially. A similar
increase of inward pointing of the knee joint occurs in the
presence of excess external tibial torsion when the foot is
pointed forward. (Reused with permission from Elsevier.
From Teitge RA. Patellofemoral Disorders Correction of
Rotational Malalignment of the Lower Extremity. In:
Noyes’s Knee Disorders: Surgery, Rehabilitation, Clinical
Outcomes, 2017)
the “failed patella”. The patient in Fig. 27 had
severe chronic patellofemoral pain with extensive
and severe involvement of the patellar cartilage in
both knees. In addition, she presented an external
tibial torsion of 49° in the left knee and 45° in the
right knee. A bipolar fresh patellofemoral allograft procedure was performed on her right knee
with a good result in the short term. Due to
problems of availability of fresh allografts in the
tissue bank, a decision was taken to perform an
internal rotational tibial osteotomy on her left
knee. The results were very good. The patient is
happier with her left knee than with her right one,
which is now the bad knee for her (Fig. 28).
As far back as 1995, Flandry and Huhgston
[25] showed that the most frequent cause of
failure of an extensor mechanism realignment
surgery was the existence of an underlying
undiagnosed torsional alteration that, of course,
had gone untreated.
In 2009, Paulos and colleagues [26] compared
two surgical techniques in a cohort of patients
with patellar instability and limb malalignment.
In one group, they performed a proximal
170
V. Sanchis-Alfonso et al.
Fig. 25 Severe diffuse patellar chondropathy in a 40year-old woman with disabling AKP after two previous
failed surgeries performed to treat AKP. A Surgical image
of the chondral lesion. B Patellar fresh allograft in situ.
C Anteroposterior radiograph D Lateral radiograph and
E Axial radiograph at the 5-year follow-up. (Republished
with permission of AME Publishing Company. From V
Sanchis-Alfonso, Treating complications of operative
management for patellofemoral pain, Ann Joint, 3:27,
2018)
realignment associated with a rotational tibial
osteotomy. In the other one, a Elmslie-TrillatFulkerson proximal–distal realignment was done.
They concluded that rotational abnormality correction produced significantly better results than
conventional proximal–distal realignment.
Stevens and colleagues [27], in 2014, analyzed
16 consecutives patients (23 knees) with a failed
knee surgery (tibial tubercle osteotomy in 12
knees and arthroscopic debridement in 9) before
which a femoral or tibial torsional abnormality
was recognized and subsequently treated by
means of rotational osteotomy. They demonstrated clinical improvement after osteotomies of
the femur and/or tibia in these patients. Those
authors state that many orthopedic surgeons only
focus on the knee when they see an AKP patient.
Torsional abnormalities often go unrecognized.
These authors observed that addressing rotational
abnormalities in the index surgery provides better
clinical results than osteotomies performed after
previous knee surgeries for treating AKP and/or
patellar instability.
Drexler and colleagues [28] evaluated 15
knees (12 patients) in 2013 in which a rotational
tibial osteotomy proximal to the tibial tuberosity
associated with a tibial tubercle transfer was performed based on a diagnosis of recurrent patella
subluxation secondary to excessive external tibial
torsion. The authors showed a satisfactory clinical
outcome at a median follow-up of 84 months
(range 15–156). The high number of patients with
previous failed surgeries in this series provides
some evidence that tibial tubercle medialization
associated with soft tissue plication is not sufficient to correct patellar instability in patients with
excessive external tibial torsion.
Finally, Franciozi and colleagues [29] evaluated 48 patients who underwent an MPFLr
associated with a tibial tubercle osteotomy due to
recurrent patellar dislocation. They classified the
patients in 2 groups. One was with excessive
The Failed Patella. What Can We Do?
171
Fig. 26 CT of the same case from Fig. 25
Fig. 27 Patient with bilateral AKP and similar structural
changes in both knees including pathologic excessive
external tibial torsion. A bipolar patellofemoral fresh
allograft procedure was done on the right knee. Some
2 years later, a rotational tibial osteotomy was carried out
on the left knee
172
V. Sanchis-Alfonso et al.
Fig. 28 In these images of the same patient as in Fig. 27,
the deterioration of the fresh bipolar allograft was
observed as the months went by. This deterioration was
due to the disadvantageous biomechanical environment
into which the graft was implanted and which had not been
corrected. In other words, we did not correct the pathological external tibial torsion that this patient presents. The
external tibial torsion will lead to an augmentation of the
lateral vector of the quadriceps femoris muscle and
therefore to a mechanical overload on the lateral aspect
of the patellofemoral joint with the ulterior development of
a severe patellofemoral chondropathy, as in fact is
observed on the CT images. It is absolutely essential to
correct the anomalous biomechanical environment in order
to avoid the surgical failure performed on the cartilage. Do
not ignore the mechanics which caused the tissue failure, if
so, another failed result ensues
femoral anteversion (FAV) and the other one
with normal FAV. The patients with increased
FAV had significantly lower functional scores
than the patients without FAV. We can conclude
that increased FAV can negatively affect the
postoperative prognosis. Femoral rotational
osteotomy combined with MPFLr should be
considered for the treatment of recurrent patellar
dislocation associated with FAV.
– Ideally, treating a complication should
address the problem that led to the primary
surgery and the damage caused by the failed
surgical procedure.
– A poorly indicated or poorly performed surgical treatment can be disastrous for the patient.
Orthopedic surgeons must never forget the
principles of Hippocratic medicine: “Primum
non nocere”. We must not cause harm or make
an already bad situation much worse.
7
Take Home Messages
– The best way to avoid a patellofemoral surgery that will lead to an unsuccessful result is
to stick to operations that have shown a high
degree of success.
– By reducing the large number of unnecessary
surgeries to treat AKP and by paying attention
to technical details, we also can considerably
reduce the number of surgical complications.
– We must be sure that an anatomic lesion that
is amenable to surgical correction is identified
preoperatively.
References
1. Steinkamp LA, Dillingham MF, Markel MD, et al.
Biomechanical considerations in patellofemoral joint
rehabilitation. Am J Sports Med. 1993;21:438–44.
2. Sigmund KJ, Hoeger Bement MK, Earl-Boehm JE.
Exploring the pain in patellofemoral pain: a systematic review and meta-analysis examining signs of
central sensitization. J Athl Train. 2021;56(8):887–
901.
3. Woolf CJ. Central sensitization: Implications for the
diagnosis and treatment of pain. Pain. 2011;152(3
Suppl):S2.
The Failed Patella. What Can We Do?
4. Schuttert I, Timmerman H, Petersen KK, et al. The
definition, assessment, and prevalence of (human
assumed) central sensitisation in patients with
chronic low back pain: a systematic review. J Clin
Med. 2021;10(24):5931.
5. Neblett R, Hartzell MM, Cohen H, et al. Ability of
the central sensitization inventory to identify central
sensitivity syndromes in an outpatient chronic pain
sample. Clin J Pain. 2015;31:323–32.
6. Mayer TG, Neblett R, Cohen H, et al. The development and psychometric validation of the Central
Sensitization Inventory (CSI). Pain Pract. 2012;12
(4):276–85.
7. Sanchis-Alfonso V, Domenech-Fernandez J, BeserRobles M, et al. Influence of central sensitization on
pain, disability and psychological impairment in
anterior knee pain patients. A prospective crosssectional observational study. (In press).
8. Agarwalla A, Liu JN, Wu HH, et al. Return to work
following tibial tubercle osteotomy for patellofemoral osteoarthritis and pain [published online April
22, 2020]. Cartilage. 1947603520916544.
9. Domenech J, Sanchis-Alfonso V, Espejo-Tort B.
Influence of kinesiophobia and catastrophizing on
pain and disability in anterior knee pain patients. Knee
Surg Sports Traumatol Arthrosc. 2013;21:1562–8.
10. Domenech J, Sanchis-Alfonso V, Espejo-Tort B.
Changes in catastrophizing and kinesiophobia are
predictive of changes in disability and pain after
treatment in patients with anterior knee pain. Knee
Surg Sports Traumatol Arthrosc. 2014;22(10):2295–
300.
11. Sanchis-Alfonso V, Merchant AC. Iatrogenic medial
patellar instability: an avoidable injury. Arthroscopy.
2015;31(8):1628–32.
12. Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC, et al. Results of isolated lateral retinacular
reconstruction for iatrogenic medial patellar instability. Arthroscopy. 2015;31(3):422–7.
13. Fulkerson JP. A clinical test for medial patella
tracking. Tech Orthop. 1997;12:165–9.
14. Teitge RA, Faerber WW, Des MP. Stress radiographs
of the patellofemoral joint. J Bone Joint Surg Am.
1996;78:193–203.
15. Biedert RM. Computed tomography examination. In:
Biedert RM, ed. Patellofemoral disorders. Diagnosis
and treatment. West Sussex: Wiley, 2004;101–111.
16. Kelman GJ, Focht L, Krakauer JD, et al. A cadaveric
study of patellofemoral kinematics using a
173
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
biomechanical testing rig and gait laboratory motion
analysis. Orthop Trans. 1989;13:248–9.
Teitge RA, Torga SR. Lateral patellofemoral ligament
reconstruction. Arthroscopy. 2004;20:998–1002.
Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC, et al. Deep transverse lateral retinaculum
reconstruction for medial patellar instability.
Arthrosc Tech. 2015;4(3):e245-249.
Weale AE, Murray DW, Newman JH, et al. The
length of the patellar tendon after unicompartmental
and total knee replacement. J Bone Joint Surg Br.
1999;81(5):790–5.
Caton J, Deschamps G, Chambat P, et al. Patella
infera. Apropos of 128 cases. Rev Chir Orthop
Reparat- rice Appar Mot. 1982;68(5):317–325.
Caton J. Method of measuring the height of the
patella. Acta Orthop Belg. 1989;55:385–6.
Drexler M, Dwyer T, Marmor M, et al. The treatment
of acquired patella baja with proximalization of the
tibial tuberosity: surgical technique and six-year
clinical outcome. Arthroscopy. 2013;29: e155.
Dejour D, Levigne C, Dejour H. Postoperative low
patella. Treatment by lengthening of the patellar
tendon. Rev Chir Orthop Reparatrice Appar Mot
1995;81: 286–295.
Burnett SJ, Berger RA, Paprosky WG, et al. Extensor
mechanism allograft reconstruction after total knee
arthroplasty. A comparison of two techniques.
J Bone Joint Surg Am. 2004;86(12):2694–2699.
Flandry F, Hughston JC. Complications of extensor
mechanism surgery for patellar malalignment. Am J
Orthop (Belle Mead NJ). 1995;24(7):534–43.
Paulos L, Swanson SC, Stoddard GJ, et al. Surgical
correction of limb malalignment for instability of the
patella: a comparison of 2 techniques. Am J Sports
Med. 2009;37(7):1288–300.
Stevens PM, Gililland JM, Anderson LA, et al.
Success of torsional correction surgery after failed
surgeries for patellofemoral pain and instability.
Strategies Trauma Limb Reconstr. 2014;9(1):5–12.
Drexler M, Dwyer T, Dolkart O, et al. Tibial
rotational osteotomy and distal tuberosity transfer
for patella subluxation secondary to excessive external tibial torsion: surgical technique and clinical
outcome. Knee Surg Sports Traumatol Arthrosc.
2014;22(11):2682–9.
Franciozi CE, Ambra LF, Albertoni LJ, et al.
Increased femoral anteversion influence over surgically treated recurrent patellar instability patients.
Arthroscopy. 2017;33(3):633–40.
Risk Factors for Patellofemoral Pain:
Prevention Programs
Michelle C. Boling and Neal R. Glaviano
1
Epidemiology of PFP
Patellofemoral pain (PFP) is one of the most
common knee injuries among those who are
physically active. It is a challenging condition to
manage due to the exacerbation of symptoms
during tasks that require weight-bearing knee
flexion, which is common during activities of
daily living. While conservative treatment is the
cornerstone to PFP management, long-term outcomes are less optimal [1]. Therefore, identifying
those at greater risk for PFP and implementing
prevention programs are essential to minimizing
the long-term sequelae associated with PFP.
To fully appreciate the risk factors for PFP, it
is essential to consider the epidemiology across
various populations. The epidemiology of PFP is
commonly measured with prevalence and incidence. Prevalence is the proportion of a population reporting PFP regardless of the initial
diagnosis, while incidence is the number of new
cases of PFP during a specific period of time.
M. C. Boling (&)
Clinical and Applied Movement Sciences, Brooks
College of Health, University of North Florida,
Jacksonville, USA
e-mail: m.boling@unf.edu
N. R. Glaviano
Department of Kinesiology, College of Agriculture,
Health and Natural Resources, University of
Connecticut, Mansfield, USA
Prevalence and incidence rates have been measured across numerous populations who commonly experience PFP.
The prevalence of PFP varies greatly among
sampled populations, ranging from 7.2 to 45.3%
[2–5]. The prevalence of PFP has been reported
to be 25% in patients attending a sports medicine
clinic [6], 22.7% in a university community [3],
13.5% in military cadets [7], and 20.7% in the
general Chinese population [5]. The prevalence
of PFP among runners has a greater range, with
recreational runners in the United Kingdom
having a prevalence of 16.7% [8] and amateur
runners in Nigeria having a prevalence of 45.3%
[4]. Furthermore, the point prevalence among a
pooled adolescent cohort has been reported to be
7.2% [2], while the annual prevalence has been
reported to be as high as 28.9% [9].
The incidence of PFP also varies considerably
based on the sampled population. Within military
cadets the incidence of PFP has been reported to
range from 9.7 to 571.4 cases per 1000 personyears. Among female novice recreational runners, the incidence rate over a 10-week period
was reported as 1080.5 cases per 1000 personyears [2, 10]. Furthermore, in an adolescent
population participating in physical education
classes, the incidence rate for PFP was reported
to be 42.6 cases per 1000 person-years [11].
Patellofemoral pain has also been suggested to
impact females more commonly than males.
Evidence supports females are at a 2-times
greater risk for developing PFP across the
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_11
175
176
M. C. Boling and N. R. Glaviano
general population [3], adolescent population
[12] and military cadets [7]. The high prevalence
and incidence rates for PFP among various
populations, and the increased risk among
females, highlight the need for clinicians to
understand the risk factors for PFP to implement
specific prevention programs to target those at
the greatest risk for developing this chronic
condition.
2
Risk Factors
Patellofemoral pain is considered a multifactorial
condition in which various intrinsic factors, such
as altered movement patterns, muscle strength,
and postural alignment could predispose an
individual to the development of PFP. It is
important to consider extrinsic factors, (i.e.
training load) as well, and how this may lead to
the development of PFP. Overall, factors that can
influence loading of the patellofemoral joint have
been investigated in prospective cohort studies,
as abnormal loading of the patellofemoral joint is
theorized to be the underlying cause of PFP [13].
The following paragraphs summarize risk factors
assessed in prospective cohort investigations.
3
Intrinsic Risk Factors
Altered Movement Patterns
Prospective investigations have assessed lower
extremity kinematics during various functional
tasks as risk factors for the development of
PFP. The influence of lower extremity joint
motion on patellofemoral joint contact forces and
loading of the patellofemoral joint provides the
theoretical foundation for the investigation of
lower extremity kinematics as risk factors for the
development of PFP [13].
Patellofemoral pain is a prevalent condition
among runners and therefore, this population is
frequently included in prospective investigations.
Noehren et al. [14] assessed gait mechanics in
female runners to determine if there were any
lower extremity kinematics during running gait
that increased the risk for the development of
PFP. Based on their findings, female runners who
developed PFP displayed greater hip adduction
throughout the stance phase of running when
compared to those who did not develop
PFP. Transverse plane motion at the hip and
rearfoot angles at the ankle were not found to be
risk factors for PFP in female runners.
Three prospective cohort investigations have
assessed lower extremity movement patterns
during a jump-landing task as risk factors for the
development of PFP [15–17]. In two of these
studies (one study was a follow up investigation
to the initial study), three-dimensional lower
extremity kinematics during a jump-landing task
were evaluated in male and female military
cadets. In the initial study, military cadets who
displayed an increased hip internal rotation angle
and decreased peak knee flexion angle during the
jump-landing task were at an increased risk for
developing PFP. In the follow up study, Boling
et al. [15] analyzed risk factors separately for
male and female military cadets during the same
jump-landing task. In female military cadets,
decreased hip abduction angle and increased
knee internal rotation angle when landing from a
jump increased the risk for developing PFP. In
male military cadets, decreased knee flexion
angle and increased hip external rotation angle
increased the risk for developing PFP.
In another prospective study, two-dimensional
knee valgus displacement during a landing task
was assessed as a risk factor for the development
of PFP in adolescent females. Increased twodimensional knee valgus angle displacement was
associated with an increased risk of developing
PFP in adolescent females [17]. Holden et al.
[17] reported knee valgus displacement 10.6°
predicted PFP development in adolescent
females with a sensitivity of 75% and specificity
of 85%. It is important to note that frontal and
transverse plane motion at the hip likely
Risk Factors for Patellofemoral Pain: Prevention Programs
contributes to the measurement of twodimensional knee valgus displacement in this
investigation. Therefore, the findings from this
investigation are further supported by the previous
prospective
investigations
reporting
increased frontal and transverse plane motion at
the hip as risk factors for the development of PFP
[14, 15].
An additional prospective investigation
assessed performance on the Y-balance test and
frontal plane knee projection angle during a
single leg squat as risk factors for the development of PFP in male military recruits [18].
Asymmetry 4.08 cm in the posterolateral
reach on the Y-balance test and frontal plane
knee projection angle 4.81° during a single leg
squat were significant predictors for the development of PFP in this population.
In summary, altered lower extremity movement patterns appear to play a role in the
development of PFP in males and females.
Increased frontal plane and transverse plane
motion, most notably at the hip and knee, have
been reported in multiple studies during various
dynamic tasks as potential risk factors for the
development of PFP in both males and females.
When assessing individuals who may be at risk
for the development of PFP, clinicians should
pay particular attention to increased frontal and
transverse plane motion during dynamic tasks
and address these altered movement patterns to
potentially decrease the risk for future PFP
development.
Muscle Strength
Both isometric and isokinetic strength of lower
extremity muscle groups have been investigated
as risk factors for the development of PFP. Due
to the influence of hip musculature on the ability
to control lower extremity movements, strength
of the hip musculature has been investigated as a
risk factor for PFP. Furthermore, quadriceps
strength has been investigated as a risk factor for
the development of PFP due to the quadriceps
serving as the main dynamic stabilizer of the
patella.
Prospective investigations have assessed isometric strength of the hip flexors, extensors,
177
abductors, adductors, internal rotators and
external rotators in male and female military
cadets [15, 16], male and female high school
runners [19], female high school basketball
players [20], and female adult runners [10]. None
of these studies reported an association between
decreased isometric strength of the hip musculature and an increased risk of developing
PFP. Interestingly, increased isometric strength
of the hip external rotators was associated with
an increased risk of developing PFP in male and
female military cadets [16]. However, in a larger
cohort as a follow-up study to this previous
investigation, no isometric hip strength measures
were found to be associated with an increased
risk of developing PFP in male or female military
cadets [15]. Specific to male and female high
school runners [19] and female high school
basketball players [20], increased isometric
strength of the hip abductors was associated with
an increased risk for the development of
PFP. A systematic review with meta-analysis
pooled the data from prospective studies and
regardless of cohort population, strength of the
hip musculature was not found to be a risk factor
for the development of PFP [21].
Both isometric and isokinetic measures of
quadriceps strength have been included in
prospective investigations of risk factors for PFP
in various populations. Three investigations have
assessed isometric quadriceps strength in military
cadets [15, 16, 22]. In a combined cohort of male
and female military cadets, decreased isometric
quadriceps strength was associated with an
increased risk for the development of PFP [16].
However, when male and female military cadets
were analyzed separately, isometric quadriceps
strength was not found to be a risk factor for the
development of PFP [15]. Isometric strength of
the quadriceps has also been investigated in
female high school basketball players and was
not reported as a risk factor for the development
of PFP [20]. Based on the three prospective
investigations assessing isokinetic torque of the
quadriceps, decreased isokinetic torque of the
quadriceps was not a risk factor for the development of PFP in male and female physical
education students [11] but was found to increase
178
the risk of development PFP in male military
cadets [23] and female military recruits [24].
When pooling the data from all studies assessing
strength of the quadriceps musculature, regardless of cohort and type of measurement (isometric or isokinetic), decreased strength of the
quadriceps was found to be a risk factor for the
development of PFP [21].
Postural Alignment
Q-angle is the angle formed by force vectors of
the quadriceps musculature and the patellar tendon [25]. A larger Q-angle is proposed to
increase the lateral force vector placed on the
patella by the quadriceps and therefore, cause
lateral tracking of the patella [26]. Three
prospective cohort investigations have assessed
Q-angle in female and male military recruits [16],
novice female runners [10], and male and female
physical education students [11]. All three studies reported static Q-angle is not a risk factor for
the development of PFP.
Foot Posture
Excessive pronation at the foot has been associated with increased frontal and transverse plane
motion up the kinetic chain [27, 28]. Because
motion at the foot and ankle may influence the
mechanics at the patellofemoral joint, excessive
pronation has been theorized to predispose individuals to PFP.
Various plantar pressure measures during gait
have been assessed as risk factors for the development of PFP. During walking, a more laterally
directed pressure at initial contact, slower
movement of the center of pressure from lateral
to medial, and shortened time to maximal pressure on the fourth metatarsal were found to be
associated with an increased risk of developing
PFP in military cadets [29]. During running,
increased vertical peak force under the second
metatarsals and a shortened time to peak vertical
force at the lateral heel were associated with an
increased risk for the development of PFP in
novice female runners [30]. In a systematic
review with meta-analysis, data for time to peak
force measures were pooled and no significant
M. C. Boling and N. R. Glaviano
associations were found between these measures
and risk of developing PFP [21].
Static measures of foot posture have also been
investigated as risk factors for the development
of PFP; however, no studies have used the same
measure. Witvrouw et al. [11] reported measures
of foot arch on a podograph, lower leg-heel
alignment, and heel-forefoot alignment were not
risk factors for the development of PFP in
physical education students. Thijs et al. [30]
investigated static foot posture using the foot
posture index (FPI) in recreational runners. They
reported measurements of FPI were not associated with the risk of developing PFP. Boling
et al. [16] investigated foot posture using the
navicular drop assessment. Increased navicular
drop was identified as a risk factor for the
development of PFP. However, in a follow up
study on gender specific risk factor profiles in a
larger cohort of military cadets, navicular drop
was not a risk factor for the development of PFP
in males or females [15]. Based on the current
data available, foot posture does not appear to
predispose individuals to the development of
PFP.
4
Extrinsic Risk Factors
Overload/Overtraining
The envelope of function can be used to understand how excessive loading of the patellofemoral joint may lead to the development of PFP
[31]. Dye et al. [32] describes how supraphysiologic loading of an otherwise normal patellofemoral joint could cause the loss of homeostasis
within the joint tissues. This loss of tissue
homeostasis can lead to pain and loss of function.
Repetitive loading of the patellofemoral joint is
common during military recruit training and thus,
many prospective studies have investigated risk
factors for PFP in this population. In two
prospective investigations conducted during
basic military training, the majority of cases of
PFP were reported within the first four weeks of
training [33, 34]. It may be speculated that the
Risk Factors for Patellofemoral Pain: Prevention Programs
individuals who developed PFP had lower levels
of physical activity prior to basic training and
underwent a significant increase in training load
in the first few weeks of training (operating
outside of the envelope of function) leading to a
loss of tissue homeostasis. When developing
prevention programs, it is important to consider
training load along with intrinsic risk factors for
the development of PFP.
5
Prevention of PFP
One of the most common injury prevention
models was developed by van Mechelen et al.
[35]. This injury prevention model includes four
steps: establishing the incidence of an injury,
establishing the etiology of the injury, implementing a preventative program, and assessing the
effectiveness of the program. The injury incidence
following the intervention is compared to the initial injury incidence rate to determine the effectiveness. The model is continuous, as step four
leads into step one, repeating the process (Fig. 1).
Optimizing injury prevention requires the
programs to be adopted into clinical practice,
placing a significant focus on implementation.
Finch [36] modified the initial van Mechelen
179
model [35] to the Translating Research into
Injury Prevention Practice (TRIPP). The TRIPP
model includes two additional steps, evaluating
the prevention measure in ideal scientific conditions and evaluating the program’s feasibility in
clinical practice by describing the intervention
context to inform implementation strategies
(Fig. 1). The two other steps recognize the value
of implementation. They also demonstrate one of
the challenges of the current prevention programs
within the patellofemoral pain literature, as most
studies have been conducted within military
settings.
While many risk factors have been evaluated
in the PFP literature, altered movement patterns
and decreased knee extensor strength have
emerged as specific intrinsic risk factors. There is
limited evidence of implementing a prevention
program to mitigate the risk of developing
PFP. Foot orthoses and footwear, knee braces,
and combined stretching and strengthening
exercises have been implemented to reduce the
incidence of PFP, with most being conducted in a
military population.
Muscle Strength
Decreased isometric and isokinetic knee extensor
strength is a risk factor for PFP, suggesting
Fig. 1 Comparison of van Mechelen injury prevention model [35] and translating research into injury prevention
practice framework [36]
180
strength-based interventions that focus on the
quadriceps would be a viable intervention. Three
randomized control trials have evaluated the
effect of a strength-focused program on preventing PFP, two in military recruits [33, 37] and
a third in elite volleyball players [38].
A randomized controlled trial of 1020 Army
recruits was the first prevention program to
investigate an intervention with the goal of
reducing the occurrence of PFP [33]. A 12-week
program that combined strengthening and
stretching was implemented three times a week,
compared to a control group that completed
upper extremity exercises. Those allocated to the
prevention program had improvements in their
running fitness assessment but the program did
not reduce the risk of developing PFP in the
Army recruits.
The second randomized control trial was a 16week prevention program on an elite volleyball
team over a single season [38]. The prevention
program included isometric open kinetic chain
exercises, isometric closed kinetic chain exercises, sports specific or plyometric exercises, and
eccentric exercises. The program was conducted
two times a week, with exercises adjusted
weekly, and integrated into the regular volleyball
training. The control group maintained their
regular training program, with no additional
exercises. After the volleyball season, there was
no reduction in PFP risk among those completing
the prevention program compared to the control
group.
The third prevention program was a randomized control trial of 1502 military recruits over
14-weeks [37]. Individuals in the prevention
group completed four lower extremity strengthening exercises as a warm-up to military training
and four lower extremity stretching exercises
during the session warm-down. In contrast, the
control group completed their regular training.
The prevention program was completed on
average seven times per week, which was the
highest number of completed sessions in a week
across the three randomized controlled trials.
This prevention program effectively reduced the
risk of developing PFP by 75% compared to the
control group.
M. C. Boling and N. R. Glaviano
The three randomized controlled trials included a wide range of exercises within the prevention program, but all included a squat and
lunge task (Table 1). Brushoj et al. [33] included
a squat and lunge task to target the quadriceps,
with both exercises being prescribed only in
weeks 5–8. Cumps et al. [38] included three
exercises per week that targeted the quadriceps,
hamstrings, and gluteal muscles. Coppack et al.
[37] included isometric hip abduction, lunge,
step-down, and squatting tasks. With evidence
supporting knee extension strength as a risk
factor for the development of PFP, each of these
studies likely targeted the quadriceps with the
prescribed exercises. However, none of the
studies measured strength pre-and postintervention. The inability to objectively assess
strength is essential to determine the prevention
program’s effectiveness. Future randomized
control trials are necessary to determine the
prevention program’s effectiveness at improving
knee extension strength and reducing the risk of
PFP.
Altered Movement Patterns
Altered frontal and sagittal plane kinematics,
assessed in three-dimensional and twodimensional motion analysis, increase the risk
of developing PFP. Implementing an intervention
program to decrease hip adduction and internal
rotation, and increase knee flexion may reduce
the risk of developing PFP among physically
active individuals. Motor learning and gait
retraining have demonstrated promise at reducing
frontal plane kinematics in females with PFP [39,
40]; however, no studies have evaluated these
interventions to prevent the development of
PFP. There is a need for randomized controlled
trials to determine if movement patterns can be
altered and if this reduces the risk for developing
PFP.
Other Prevention Programs
Previous studies have identified various foot
posture impairments in those with PFP, supporting early prevention program interventions.
Three studies, ranging between 9 and 14 weeks,
have evaluated the effect of orthoses and
Population
Military
cadets
Elite
volleyball
players
Authors
Brushoj
et al. [33]
Cumps
et al. [38]
16-weeks 2x/week
12-weeks
15-min
3x/week
Duration/frequency
Month 2:
Isometric strength
in CKC
• Oscillating
squat: 3 20 s
• SLS circles:
3 10
• Oscillating
hamstrings:
3 20 s
• Quad sets:
3 10 at 7 s
• Oscillating quad:
3 20 s
• Oscillating
lunge: 3 20 s
• Co-Contraction:
3 10 7 s
• Oscillating
lunge: 3 20 s
• Oscillating
hamstrings:
3 20 s
• Quad sets:
3 10 at 7 s
• Oscillating quad:
3 20 s
• SLR: 3 10 at
7s
• Quad sets:
3 10 at 7 s
• Co-Contraction:
3 10 at 7 s
• SLR: 3 10 at
7s
• Quad sets:
3 10 at 7 s
• Oscillating quad:
3 20 s
• SLR abduction:
3 10 at 7 s
Week 1
Week 2
Week 3
Squat/lunge: 3 10–20
Hip ABD/ER: 3 12–20
Forefoot lift: 3 5–15
Coordination: 3 10–15
Quadriceps stretch: 3 15 s
Month 1:
Isometric strength
in OKC
•
•
•
•
•
Exercises with load
Table 1 Summary of exercises included in injury prevention programs
• Jump lunge
3 10
• Oscillating drop
jump: 3 30 s
• Bilateral squat:
3 20
• Drop squat 3 10
• Front step up & down:
3 10
• Lunge: 3 10
(continued)
•Drop squat:
3 12
•Shuffle
sideways: 3 20
•Jump and reach:
3 15
• Unilateral squat:
3 10
• Lateral step up
& down:
3 10
• Oscillating
jump lunge:
3 20 s
Month 4:
Eccentric load
• Bilateral squat: 3 10
Oscillating lunge:
3 20 s
• Lateral step up & down:
3 10
• Oscillating squat:
3 20 s
• Oscillating hamstring:
3 20 s
• Bilateral squat: 3 10
Month 3: Sports specific &
plyometric
Risk Factors for Patellofemoral Pain: Prevention Programs
181
Military
cadets
Coppack
et al. [37]
14-weeks each physical
training session (mean =
7/week)
Duration/frequency
•
•
•
•
•
• SLR abduction:
3 10 at 7 s
• Oscillating
squat: 3 20 s
• Oscillating
lunge: 3 20 s
• SLR abduction: 3 10 at
7-sec
• Bilateral squat: 3 10
• Shuffle sideways: 3 20
Isometric hip abduction: 3 10–20
Forward lunge: 3 10–14
SL step-down: 3 10–14
SLS squat: 3 10–14
Quadriceps, iliotibial band, hamstring, and calf stretch: 3 20 s each
• Quad sets:
3 10 at 7 s
• Oscillating quad:
3 20 s
• Co-contraction:
3 10 7 s
Exercises with load
Week 4
Note ABD = abduction, ER = external rotation, SL = single leg, SLS = single leg squat
Population
Authors
Table 1 (continued)
• Oscillating drop
jump: 4 30 s
• Front step up &
down: 3 10
• Unilateral squat:
3 10
182
M. C. Boling and N. R. Glaviano
Risk Factors for Patellofemoral Pain: Prevention Programs
183
footwear in military recruits [41–43]. Prescribing
orthoses and footwear did not reduce the risk of
developing PFP in any of these investigations.
The use of knee braces with patellar support
has also been investigated in reducing the risk of
developing PFP. Two studies, ranging from 6 to
8 weeks, compared the use of a knee brace to no
knee brace on PFP risk [44, 45]. When compared
to the individuals not wearing a brace, both
studies reported those wearing a knee brace had a
reduced risk (ranging from 50 to 74%) of
developing PFP. The findings from these studies
suggest the use of knee braces with patellar
support may be effective in reducing the risk of
developing PFP.
past decade, additional research is needed to
better understand how these risk factors may
differ by gender and sampled population. Based
on the available evidence, increased frontal and
transverse plan motion of the lower extremity
during dynamic tasks, asymmetry in the posterolateral reach of the Y-balance test and
decreased strength of the quadriceps may be
considered intrinsic risk factors for the development of PFP. Gaining a better understanding of
risk factors for PFP will help to inform future
studies investigating the effectiveness of prevention programs in reducing the risk for developing PFP.
Overload or Overtraining
7
Prevention programs for PFP have primarily
targeted intrinsic risk factors; however, extrinsic
risk factors may be an additional avenue.
Increases in physical activity that exceed the
envelope of function is likely a common occurrence in military recruits as they initiate basic
training. Advancements in technology allow for
quantification of external load with subjective
measures, such as the rate of perceived exertion
scale, and objective measures with accelerometers or global positioning systems. Future studies
could measure the external load of military
cadets before basic training and during the initial
few weeks to understand how this may play a
role in the development of PFP among military
cadets. Additionally, studies could investigate the
effects of altering external loading based on the
risk of developing PFP during the initial weeks
of basic training.
6
Take-Home Messages
• Patellofemoral pain is a prevalent condition
among physically active individuals.
• The incidence of patellofemoral pain is
reported to be the highest among recreational
runners and military cadets.
• Altered lower extremity movement patterns in
the frontal and transverse planes during
dynamic tasks, such as running and landing
from a jump, likely increase the risk for
developing patellofemoral pain.
• Decreased strength of the quadriceps musculature is a risk factor for the development of
patellofemoral pain.
• Increased levels of training leading to overloading of the patellofemoral joint likely
increase the risk for developing patellofemoral
pain.
• There is limited evidence for effective injury
prevention programs targeting risk factors for
the development of patellofemoral pain.
Conclusions
Patellofemoral pain is a prevalent knee condition
affecting individuals who are physically active,
with the highest incidence among recreational
runners and military cadets. Although there has
been an increase in the number of prospective
studies investigating risk factors for PFP over the
8
Key-Message
• Risk factors for the development of patellofemoral pain include altered frontal and
transverse plane motion at the hip and knee
184
during dynamic tasks and decreased knee
extensor strength. More research is needed to
gain a better understanding of risk factors for
patellofemoral pain, which can then inform
the development effective injury prevention
programs.
References
1. Lankhorst NE, van Middelkoop M, Crossley KM,
Bierma-Zeinstra SM, Oei EH, Vicenzino B, et al.
Factors that predict a poor outcome 5–8 years after
the diagnosis of patellofemoral pain: a multicentre
observational analysis. Br J Sports Med. 2016;50
(14):881–6.
2. Smith BE, Selfe J, Thacker D, Hendrick P, Bateman M, Moffatt F, et al. Incidence and prevalence of
patellofemoral pain: a systematic review and metaanalysis. PLoS One. 2018;13(1): e0190892.
3. Dey P, Callaghan M, Cook N, Sephton R, Sutton C,
Hough E, et al. A questionnaire to identify
patellofemoral pain in the community: an exploration
of measurement properties. BMC Musculoskelet
Disord. 2016;17:237.
4. Akodu A, Nwakalor N. Patellofemoral pain syndrome: prevalence and coping strategies of amateur
runners in Lagos state. Medicina Sportiva: J
RomanSports Med Soc. 2018;14(2):3059–67.
5. Xu X, Yao C, Wu R, Yan W, Yao Y, Song K, et al.
Prevalence of patellofemoral pain and knee pain in
the general population of Chinese young adults: a
community-based questionnaire survey. BMC Musculoskelet Disord. 2018;19(1):165.
6. Devereaux MD, Lachmann SM. Patello-femoral
arthralgia in athletes attending a Sports Injury Clinic.
Br J Sports Med. 1984;18(1):18–21.
7. Boling M, Padua D, Marshall S, Guskiewicz K,
Pyne S, Beutler A. Gender differences in the
incidence and prevalence of patellofemoral pain
syndrome. Scand J Med Sci Sports. 2010;20
(5):725–30.
8. Yusuf M, Dey P, Callaghan M, Relph N, Gichuru P,
Pinner S, et al. Validation and utilisation of a digital
version of the survey instrument for natural history,
Aetiology and Prevalence of Patellofemoral pain
studies (eSNAPPS). Phys Ther Sport. 2021;50:82–8.
9. Fairbank JC, Pynsent PB, van Poortvliet JA,
Phillips H. Mechanical factors in the incidence of
knee pain in adolescents and young adults. J Bone
Joint Surg Br. 1984;66(5):685–93.
10. Thijs Y, Pattyn E, Van Tiggelen D, Rombaut L,
Witvrouw E. Is hip muscle weakness a predisposing
factor for patellofemoral pain in female novice
runners? A prospective study. Am J Sports Med.
2011;39(9):1877–82.
M. C. Boling and N. R. Glaviano
11. Witvrouw E, Lysens R, Bellemans J, Cambier D,
Vanderstraeten G. Intrinsic risk factors for the
development of anterior knee pain in an athletic
population. A two-year prospective study. Am J
Sports Med. 2000;28(4):480–9.
12. Molgaard C, Rathleff MS, Simonsen O. Patellofemoral pain syndrome and its association with hip,
ankle, and foot function in 16- to 18-year-old high
school students: a single-blind case-control study.
J Am Podiatr Med Assoc. 2011;101(3):215–22.
13. Powers CM, Witvrouw E, Davis IS, Crossley KM.
Evidence-based framework for a pathomechanical
model of patellofemoral pain: 2017 patellofemoral
pain consensus statement from the 4th international
patellofemoral pain research retreat, Manchester,
UK: part 3. Br J Sports Med. 2017;51(24):1713–23.
14. Noehren B, Hamill J, Davis I. Prospective evidence
for a hip etiology in patellofemoral pain. Med Sci
Sports Exerc. 2013;45(6):1120–4.
15. Boling MC, Nguyen AD, Padua DA, Cameron KL,
Beutler A, Marshall SW. Gender-specific risk factor
profiles for patellofemoral pain. Clin J Sport Med.
2021;31(1):49–56.
16. Boling MC, Padua DA, Marshall SW, Guskiewicz K,
Pyne S, Beutler A. A prospective investigation of
biomechanical risk factors for patellofemoral pain
syndrome: the Joint Undertaking to Monitor and
Prevent ACL Injury (JUMP-ACL) cohort. Am J
Sports Med. 2009;37(11):2108–16.
17. Holden S, Boreham C, Doherty C, Delahunt E. Twodimensional knee valgus displacement as a predictor
of patellofemoral pain in adolescent females. Scand J
Med Sci Sports. 2015.
18. Nakagawa TH, Dos Santos AF, Lessi GC,
Petersen RS, Scattone Silva R. Y-balance test
asymmetry and frontal plane knee projection angle
during single-leg squat as predictors of patellofemoral pain in male military recruits. Phys Ther Sport.
2020;44:121–7.
19. Finnoff JT, Hall MM, Kyle K, Krause DA, Lai J,
Smith J. Hip strength and knee pain in high school
runners: a prospective study. PM R. 2011;3(9):792–
801.
20. Herbst KA, Barber Foss KD, Fader L, Hewett TE,
Witvrouw E, Stanfield D, et al. Hip strength is greater
in athletes who subsequently develop patellofemoral
pain. Am J Sports Med. 2015;43(11):2747–52.
21. Neal BS, Lack SD, Lankhorst NE, Raye A, Morrissey D, van Middelkoop M. Risk factors for
patellofemoral pain: a systematic review and metaanalysis. Br J Sports Med. 2019;53(5):270–81.
22. Milgrom C, Finestone A, Eldad A, Shlamkovitch N.
Patellofemoral pain caused by overactivity.
A prospective study of risk factors in infantry
recruits. J Bone Joint Surg Am. 1991;73(7):1041–3.
23. Van Tiggelen D, Witvrouw E, Coorevits P,
Croisier J, Roget P. Analysis of isokinetic parameters
in the development of anterior knee pain syndrome: a
prospective study in a military setting. Isokinet Exer
Sci. 2004;12:223–8.
Risk Factors for Patellofemoral Pain: Prevention Programs
24. Duvigneaud N, Bernard E, Stevens V, Witvrouw E,
Van Tiggelen D. Isokinetic assessment of patellofemoral pain syndrome: a prospective study in female
recruits. Isokinet Exer Sci. 2008;16(4):213–9.
25. Livingston LA. The quadriceps angle: a review of the
literature. J Orthop Sports Phys Ther. 1998;28
(2):105–9.
26. Schulthies SS, Francis RS, Fisher AG, Van de
Graaff KM. Does the Q angle reflect the force on the
patella in the frontal plane? Phys Ther. 1995;75
(1):24–30.
27. McClay I, Manal K. A comparison of threedimensional lower extremity kinematics during running between excessive pronators and normals. Clin
Biomech (Bristol, Avon). 1998;13(3):195–203.
28. Tiberio D. The effect of excessive subtalar joint
pronation on patellofemoral mechanics: a theoretical
model. J Orthop Sports Phys Ther. 1987;9(4):160–5.
29. Thijs Y, Van Tiggelen D, Roosen P, De Clercq D,
Witvrouw E. A prospective study on gait-related
intrinsic risk factors for patellofemoral pain. Clin J
Sport Med. 2007;17(6):437–45.
30. Thijs Y, De Clercq D, Roosen P, Witvrouw E. Gaitrelated intrinsic risk factors for patellofemoral pain in
novice recreational runners. Br J Sports Med.
2008;42(6):466–71.
31. Dye SF. The knee as a biologic transmission with an
envelope of function: a theory. Clin Orthop Relat
Res. 1996;325:10–8.
32. Dye SF. The pathophysiology of patellofemoral pain:
a tissue homeostasis perspective. Clin Orthop Relat
Res. 2005;436:100–10.
33. Brushoj C, Holmich P, Nielsen MB, Albrecht-Beste
E. Acute patellofemoral pain: aggravating activities,
clinical examination, MRI and ultrasound findings.
Br J Sports Med. 2008;42(1):64–7; discussion 7.
34. Wills AK, Ramasamy A, Ewins DJ, Etherington J. The incidence and occupational outcome of
overuse anterior knee pain during army recruit
training. J R Army Med Corps. 2004;150(4):264–9.
35. van Mechelen W, Hlobil H Fau-Kemper HC, Kemper HC. Incidence, severity, aetiology and prevention
of sports injuries. A review of concepts. Sports Med.
1992;14:82–9.
185
36. Finch C. A new framework for research leading to
sports injury prevention. J Sci Med Sport. 2006;9(1–
2):3–9.
37. Coppack RJ, Etherington J, Wills AK. The effects of
exercise for the prevention of overuse anterior knee
pain: a randomized controlled trial. Am J Sports
Med. 2011;39(5):940–8.
38. Cumps E, Verhagen EA, Duerinck S, Devillé A,
Duchene L, Meeusen R. Effect of a preventive
intervention programme on the prevalence of anterior
knee pain in volleyball players. Eur J Sport Sci.
2008;8(4):183–92.
39. Noehren B, Scholz J, Davis I. The effect of real-time
gait retraining on hip kinematics, pain and function in
subjects with patellofemoral pain syndrome. Br J
Sports Med. 2011;45(9):691–6.
40. Willy RW, Scholz JP, Davis IS. Mirror gait retraining for the treatment of patellofemoral pain in female
runners. Clin Biomech (Bristol, Avon). 2012;27
(10):1045–51.
41. Bonanno DR, Murley GS, Munteanu SE, Landorf KB, Menz HB. Effectiveness of foot orthoses
for the prevention of lower limb overuse injuries in
naval recruits: a randomised controlled trial. Br J
Sports Med. 2018;52(5):298–302.
42. Schwellnus MP, Jordaan G, Noakes TD. Prevention
of common overuse injuries by the use of shock
absorbing insoles. A prospective study. Am J Sports
Med. 1990;18(6):636–41.
43. Milgrom C, Finestone A, Shlamkovitch N, Wosk J,
Laor A, Voloshin A, et al. Prevention of overuse
injuries of the foot by improved shoe shock attenuation. A randomized prospective study. Clin Orthop
Relat Res. 1992(281):189–92.
44. Van Tiggelen D, Witvrouw E, Roget P, Cambier D,
Danneels L, Verdonk R. Effect of bracing on the
prevention of anterior knee pain–a prospective randomized study. Knee Surg Sports Traumatol
Arthrosc. 2004;12(5):434–9.
45. BenGal S, Lowe J, Mann G, Finsterbush A, Matan Y.
The role of the knee brace in the prevention of
anterior knee pain syndrome. Am J Sports Med.
1997;25(1):118–22.
Anterior Knee Pain After
Arthroscopic Meniscectomy: Risk
Factors, Prevention and Treatment
Jorge Amestoy, Daniel Pérez-Prieto,
and Joan Carles Monllau
1
General Considerations
The menisci are essential to the normal functioning and biomechanics of the knee. Their
functions include shock absorption, load transmission, stability, and proprioception [1, 2].
Meniscal injuries are common conditions in the
knee joint, particularly in sports medicine. They
can be classified mainly as either traumatic or
degenerative injuries. It depends on the mechanism of injury, the pattern of rupture, the age of
the patient and the previous state of the meniscal
tissue [3–5].
A better understanding of the role of meniscus
anatomy, its biomechanics and pathogenesis led
to the development of the “meniscus preservation” concept over recent decades. Nevertheless,
arthroscopic resections of parts of the menisci
probably continue to be the most common surgical procedures around the knee [3, 5–8].
Depending on the type of tear, the time of evo-
J. Amestoy (&) D. Pérez-Prieto J. C. Monllau
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
e-mail: jamestoyramos@gmail.com
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
lution since the injury and the patient profile,
partial meniscectomy is the treatment of choice
in many cases [9–12]. In those cases, arthroscopic surgery is an elegant procedure that often
results in a remarkable improvement in joint line
pain [13]. However, a non-negligible number of
patients have developed characteristic and usually temporary anterior knee pain after the surgical procedure.
This phenomenon has also been seen in
patients that have undergone distinct types of
knee surgery, namely anterior cruciate ligament
(ACL) reconstruction or total knee arthroplasty
[14, 15]. The incidence of postoperative PFP
after arthrocopic partial meniscectomy in patients
who did not previously have this pain is 23.8% at
6 weeks after the surgery [16]. That percentage is
quite similar to the incidence in patients who
have pain after ACL reconstruction (22–24%)
[17].
Patellofemoral pain after knee arthroscopy
usually appears around the sixth postoperative
week, which is just the moment when the patient
begins to return to their usual sports activities
after an arthroscopic partial meniscectomy [18,
19]. It is at this point that the patient should be
able to fully activate the quadriceps femoris
muscle [20]. Despite referring to improvement in
the discomfort at the level of the knee joint
interline, the patients with postoperative PFP
describe the appearance of a generally nonspecific pain that is sometimes located directly
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_12
187
188
J. Amestoy et al.
anterior to the knee. They will often place a hand
over the anterior knee when asked about the
location of their pain. They often complain with
anterior pain with prolonged sitting that it is
usually relieved by passive extension as well as
worsening pain when going downstairs. Noisy
knees are common and not necessarily a cause of
concern in the postoperative period [21]. Crepitus or a rubbing sensation under the kneecap that
hurts could be pathological if associated with
chondral lesions in the patellofemoral joint.
However, the excess synovial fluid still present in
the knee after arthroscopic meniscectomy may
also be the cause of this patellar crepitation.
2
Risk Factors for Patellofemoral
Pain After Knee Arthroscopy
The cause of anterior knee pain that has been
extensively described in this book is likely to be
multifactorial, which means a wide range of
factors are involved in its etiopathogenesis.
Neuromuscular, anatomic, mechanical, and even
psychological factors have all been suggested as
causative [22–24], which explains the unpredictable results of treatment.
In the case of patellofemoral pain that appears
after arthroscopic partial meniscectomy, there are
several specific risk factors that may influence
the development of this pain during the postoperative period.
2.1 Postoperative Quadriceps Muscle
Atrophy
Classically, one of the suggested etiopathogenesis factors of anterior knee pain was a muscle
imbalance between the vastus medialis (VM) and
the vastus lateralis (VL) of the quadriceps
femoris muscle. It was assumed that hypotrophy
or lack of neuromuscular activity of the VM,
particularly its oblique fibers (VMO), caused a
lateral patellar tilt and abnormal patellofemoral
tracking that led to excessive compressive stress
on the patellar facets and anterior knee pain.
However, Chester et al. have found that the
VM/VL imbalance is not present in all patients
experiencing PFP [25]. They stated that some
other agents must be causative.
Quadriceps muscle hypotrophy that occurs
following knee surgery contributes to persistant
muscle weakness [26, 27] due to alterations in
muscle architecture [28], selective fibre atrophy
[29, 30], or even neural deficits like quadriceps
activation failure [31]. It might also cause postoperative patellofemoral pain.
Amestoy and colleagues studied 120 patients
who underwent arthroscopic partial meniscectomy. In the study, an MRI of the thigh, surface
electromyography and isokinetic tests were performed before and after surgery. They observed
that patients who developed PFP at 6 weeks after
the surgery showed a greater decrease in muscle
thickness (5.11 cm2 for VL15 cm, 6.80 cm2 for
VM15 cm, and 7.80 cm2 for VM3.75 cm or
VMO) with respect to patients who did not
develop this anterior knee pain (1.38, 2.28, and
2.69 cm2, respectively) at 6 weeks after surgery
(P < 0.001 for all) [16]. This decrease in muscle
thickness was much more noticeable in the VM
than in the VL muscle.
The weakness of the hip abductor and external
rotator muscles might also influence the appearance of this post-operative patellofemoral pain.
Weakness of said muscles allows the femur to
abduct/internally rotate more than normal,
thereby increasing lateral patellar contact pressure and causing subsequent increased anterior
knee pain [32–35]. No study has evaluated the
atrophy of these muscles after knee arthroscopy.
However, it is logical to think that arthrogenic
inhibition after knee surgery will be more notable
in the quadriceps muscle group than in the gluteal muscle group due to the greater proximity of
the knee.
2.2 Delayed Quadriceps Activation
Activation failure is the inability to completely
volitionally contract the muscle due to alterations
in neural signalling. It is common following any
type of knee surgery [36, 37]. Quadriceps activation failure occurs due to alterations in neural
Anterior Knee Pain After Arthroscopic Meniscectomy …
signalling caused by a reduction in alpha motor
neuron pool recruitment and/or the firing rate
[38]. It is not simply an isolated local phenomenon related to atrophy. If left untreated,
quadriceps activation failure can significantly
impede strength gains by only allowing portions
of the muscles to be volitionally utilized during
active exercise [39]. In the same way as after
knee arthroscopy, decreased quadriceps activation has also been observed in the acute stage of
an ACL injury and in patients with ACLdeficient knees who experience instability (noncopers) [40, 41].
In addition to muscle atrophy, delay in the
activation of the quadriceps femoris muscle
could be another risk factor in the development
of patellofemoral pain after knee arthroscopy.
A deficiency of the VMO weakens the medial
quadriceps vector, thereby allowing greater
pulling of the lateral quadriceps vector with a
resultant increase in the dynamic Q-angle. Due to
this loss of the medial force, the patella is pulled
laterally out of its normal tracking. Additionally,
studies have shown more delayed activation of
the VMO in comparison to the VL, at 15, 30, and
45 degrees of knee extension, using electromyography [42].
In their study, Amestoy and colleagues
observed that the electrical contractility of the
queadriceps femoris muscle evaluated by means
of surface electromyography (sEMG) decreased
to a greater extent in patients that developed
patellofemoral pain at 6 weeks after the surgery
(804.25 mV in the VL and 1250.80 mV in the
VM) than in patients that did not develop this
pain (486.95 and 680.82 mV) (P = 0.036 and
P < 0.001, respectively) [16]. This decrease in
muscle activation was again much more noticeable in the VM than in the VL muscle (Fig. 2).
Briani and colleagues described similar differences in the activation of the quadriceps heads
during contraction among adolescent female
patients with anterior knee pain when compared
with healthy controls [43, 44].
Therefore, patients who develop PFP after
APM not only have greater loss of muscle
thickness but also a greater decrease in the
electrical contractility of the quadriceps femoris.
189
Thus, this should be considered as an independent risk factor for the development of anterior
knee pain after meniscus surgery.
Some studies have demonstrated that tourniquet use resulted in a significantly decreased
thigh circumference as well as significant negative electromyographic changes at 3 weeks after
ACL reconstruction [45]. In this sense, intraoperative tourniquet use may be detrimental to the
quadriceps femoris muscle after knee arthroscopy. No significant differences were found in
muscle strength or in the functional results
between patients on whom a tourniquet was used
and patients on whom it was not used.
2.3 Postoperative Quadriceps Muscle
Weakness
In addition to quadriceps muscle hypotrophy and
quadriceps activation failure, postoperative
strength deficit has been identified as another
independent risk factor in the development of
patellofemoral pain after arthroscopic partial
meniscectomy.
Amestoy and colleagues observed that patients
who developed anterior knee pain in the postoperative period of meniscal knee surgery had lower
quadriceps muscle strength than patients who did
not develop this pain (12.27 kg vs. 20.02 kg
respectively, P < 0.001). Both groups started
from comparable levels of strength before surgery
[16]. To assess the muscle strength values, an
isokinetic test (Biodex dynamometer) was performed both pre-surgically and 6 weeks postsurgically. It provided data on muscular strength
through range-of-motion at 60°/s.
2.4 Preoperative Quadriceps Muscle
Thickness
Despite the important role that the quadriceps
muscle plays in this pathology, no study had
studied the influence of preoperative quadriceps
femoris muscle thickness on the development of
patellofemoral pain after knee arthroscopy until
now.
190
J. Amestoy et al.
In a recent study, the Monllau and colleagues
study group observed that there is a direct correlation between the preoperative muscle thickness of the quadriceps femoris muscle and its
neuromuscular activation in the postoperative
period of knee arthroscopy [18]. The results
suggest that patients who have less VL muscle
thickness and especially the VM preoperatively
have a greater risk of developing patellofemoral
pain around the sixth week after APM. On the
other hand, they also suggest that the delayed
onset of electromyographic activity of the
quadriceps femoris muscle, regardless of muscle
thickness prior to surgery, could be considered a
risk factor for the development of patellofemoral
pain. This is of great importance, because they
establish a direct relationship between preoperative muscle thickness, which is relatively easy to
assess and quantify clinically, and the risk of
developing patellofemoral pain in the arthroscopic meniscal surgery postoperative period.
3
Prevention
For all this, achieving early activation of the
quadriceps femoris with an early recovery of its
muscle thickness and strength after arthroscopic
partial meniscectomy would be beneficial in
preventing postoperative anterior knee pain. In
this way, monitoring the neuromuscular activation of the quadriceps and its muscle thickness
may facilitate the identification of patients at risk
of developing this postoperative complication. It
would also allow them to start an early treatment.
Recently, research has focused on developing
specific disinhibitory interventions to improve
voluntary quadriceps activation. Neuromuscular
electrical stimulation (NMES) has been shown to
improve quadriceps function and strength, as
well as decrease its atrophy in the ACL surgery
postoperative period [39, 46]. Five of the seven
studies included in a systematic review found a
significant improvement in quadriceps strength
with the application of NMES following knee
arthroscopy [47–49]. Moreover, high intensity
NMES resulted in more strength recovery than
low intensity or no application of NMES
6 weeks following surgery (p < 0.05) [50].
Eccentric exercise, whereby the muscle is
lengthened and an external force exceeds that
produced by the muscle, has been shown to be
more effective than traditional concentric
strengthening at minimizing muscle atrophy and
improving muscle force production [51]. The
ability to eccentrically contract the quadriceps is
critical to optimal knee range-of-motion during
the weight-acceptance phase of gait [52, 53],
which is necessary in the early phase of rehabilitation after meniscal surgery [19, 54–56].
The combination of NMES with eccentric
exercises in the postoperative rehabilitation protocol after meniscal surgery may improve early
activation of the quadriceps femoris muscle.
Therefore, they may aid in preventing the
development of anterior knee pain even in those
patients with poor quadriceps muscle thickness.
Based on the current evidence, sEMG application should be considered in postoperative
protocols following arthroscopic surgery. Some
studies that assessed the effect of sEMG following arthroscopic knee surgery reported a
benefit in terms of quadriceps strength measured
by muscle force, knee range-of-motion and
functional knee scores when compared to standard rehabilitation alone [57–59]. Among these
studies, the sEMG group had greater VM and VL
muscle activity and maximum contraction values
when compared to NMES or rehabilitation alone
(p < 0.05).
It has recently been shown that there is a
direct relationship between the preoperative
muscle thickness of the quadriceps femoris and
neuromuscular activation and muscle strength at
6 weeks after arthroscopic partial meniscectomy
[18]. Therefore, having the quadriceps femoris
muscle in a correct preoperative state might be
protective against the development of postoperative patellofemoral pain. In this sense, a progressive rehabilitation program that is mainly
focused on strengthening the quadriceps femoris
of subjects who have undergone meniscal
Anterior Knee Pain After Arthroscopic Meniscectomy …
surgery leads to improved knee function and
prevents the developement of PFP. Much the
same happens in patients who have undergone
ACL reconstruction [46, 60, 61].
4
Treatment
An ideal meniscal rehabilitation protocol should
consider the size, tear pattern, location, quality of
the repaired tissue and any concomitant procedures. Proper postoperative rehabilitation of the
meniscetomized knee is essential, not only to
prevent the development of anterior knee pain
but specially to return to regular sports activities.
The return would also include running or jumping at approximately 6 weeks [21, 62].
The mainstay of treatment for postoperative
PFP after APM is currently the strengthening of
the quadriceps femoris muscle, abductor and
external rotator hip muscles and core muscles.
Additional measures include gait retraining, the
passive correction of patellar maltracking with
bracing and taping or hyaluronic acid or plateletrich plasma injections.
It is well known that knee pain and effusion
can lead to quadriceps dysfunction and atrophy.
This is particularly true in the setting of a
meniscal tear, both preoperatively and postoperatively [20]. Strengthening exercises for PFP
management originally focused on strengthening
the knee via quadriceps strengthening as VM
weakness is a known factor in the etiology of
PFP. The return of full quadriceps function and
strength is often hard won on the road to
recovery. So, it is prudent to have early
strengthening included in a patient’s rehabilitation protocol [21].
The American College of Sports Medicine
recommends a resistance training load of 70–
85% of the one repetition maximum to promote
muscle hypertrophy [63]. It is often challenging
for postoperative patients to achieve these loads
early in the recovery process after an arthroscopic surgery. Blood flow restriction therapy
(BFRT) has become a growing part of the preoperative and postoperative rehabilitation regimen of arthroscopy to combat this difficult
191
problem [62]. This therapy results in the development of an anaerobic environment along with
the subsequent release of growth factors. It is the
release of these growth factors that promotes
muscle hypertrophy [64–66]. The beauty of
BFRT is that it can stimulate an anaerobic
environment using loads that are much lower
than the traditional 70–85% of the one repetition
maximum. According to a recent meta-analysis,
strength and muscle hypertrophy were significantly greater in the groups performing exercise
with BFR 2–3 days per week when compared to
those exercising 4–5 days per week without BFR
[66]. The use of this therapy may be beneficial in
those patients who developed PFP pain after
arthroscopic meniscal surgery because it would
cause greater quadriceps muscle growth with
lower loads and less overload of the patellofemoral joint.
In recent years, the importance of hip abductors and external rotators strengthening has been
identified as an important pillar in the management of PFP. Two recent systematic reviews that
investigated the importance of hip and knee
strengthening as compared to knee strengthening
alone. Both reviews found that the combination
therapy significantly reduced pain in patients
with PFP [67]. Core strengthening has also been
recently revealed to be an important component
to add to postoperative anterior knee pain treatment regimens [68, 69]. In addition, they are
exercises that can be easily performed from the
first postoperative weeks after a simple knee
arthroscopy [70].
Patellar bracing has shown some short-term
benefit in PFP in small studies [71]. According to
a systematic review by Saltychev, of the 37
studies included in their review, only 7 demonstrate a significant benefit with patellar bracing
[72]. Kinesio taping of the VMO has been shown
to decrease pain and improve quadriceps function in athletes with PFP. However, these results
were seen among only 15 patients with PFP,
limiting the power of the results [73]. Probably
knee taping and patellar bracing may be beneficial in reducing PFP after meniscus surgery, but
only as an adjunct to targeted strengthening
therapy.
192
J. Amestoy et al.
Surgical treatment for postoperative PFPS is
very uncommon and is reserved for cases due to
femoropatellar chondral lesions refractory to
conservative treatment, or severe osseous and
ligamentous abnormalities that prevent normal
patellar tracking despite non-operative treatment
programs.
5
Summary
– PFP after APM affects almost 1 in 4 patients.
Its appearance can be prevented with a series
of preventive measures that are relatively easy
to apply.
– Muscle atrophy, late neuromuscular activation
and early non-recovery of muscle strength are
identifiable risk factors in the development of
PFP after simple knee arthroscopy. A thinner
quadriceps femoris muscle prior to arthroscopic knee surgery is directly correlated with
less neuromuscular activation of the same in
the postoperative period. VM seems to have a
greater influence than VL on the development
of this pathology.
– The main preventive strategy is to strengthen
the quadriceps femoris muscle prior to surgery
through a pre-rehabilitation program until an
adequate muscle thickness of the quadriceps
femoris is achieved. Promoting early neuromuscular activation, recovering the thickness
and muscle strength of the quadriceps femoris
should also be preventive strategies for patellofemoral pain after arthroscopy. For this
purpose, the combination of NEMS, sEMG
and eccentric exercises might be a good
option.
– Recovering good functionality of the quadriceps femoris muscle is the main objective of
the treatment of PFP after knee arthroscopy,
for which BFRT has become a very usefull
tool. The strengthening of the hip abductors
and core muscles should not be forgotten in
the treatment of this pathology. They are
exercises that can be easily performed from
the first postoperative weeks after knee
arthroscopy.
References
1. Greis PE, Bardana DD, Holmstrom MC, Burks RT.
Meniscal injury: I. Basic science and evaluation. J Am
Acad Orthopaedic Surg. 2002;10:168–76. https://doi.
org/10.5435/00124635-200205000-00003.
2. Walker PS, Erkman MJ. The role of the menisci in
force transmission across the knee. Clin Orthop Relat
Res. 1975;109:184–92.
3. Abram SGF, Hopewell S, Monk AP, Bayliss LE,
Beard DJ, Price AJ. Arthroscopic partial meniscectomy for meniscal tears of the knee: a systematic
review and meta-analysis. Br J Sports Med.
2020;54:652–63.
https://doi.org/10.1136/bjsports2018-100223.
4. Verdonk P, Vererfve P. Traumatic lesions: stable
knee, ACL knee. In: The meniscus. Springer;2010.
pp. 45–51.
5. Boyer T, Dorfmann H, Podgorski A. Degenerative
lesions-meniscal cyst. Springer; 2010. pp. 51–61.
6. Feeley BT, Lau BC. Biomechanics and clinical
outcomes of partial meniscectomy. J Am Acad
Orthop Surg. 2018;26:853–63. https://doi.org/10.
5435/JAAOS-D-17-00256.
7. Gauffin H, Tagesson S, Meunier A, Magnusson H,
Kvist J. Knee arthroscopic surgery is beneficial to
middle-aged patients with meniscal symptoms: a
prospective, randomised, single-blinded study.
Osteoarthritis Cartilage. 2014;22:1808–16. https://
doi.org/10.1016/j.joca.2014.07.017.
8. Wesdorp MA, Eijgenraam SM, Meuffels DE,
Bierma-Zeinstra
SMA,
Kleinrensink
G-J,
Bastiaansen-Jenniskens YM, Reijman M. Traumatic
meniscal tears are associated with meniscal degeneration. Am J Sports Med. 2020;48:2345–52. https://
doi.org/10.1177/0363546520934766.
9. Matsusue Y, Thomson NL. Arthroscopic partial
medial meniscectomy in patients over 40 years old:
a 5- to 11-year follow-up study. Arthroscopy.
1996;12:39–44. https://doi.org/10.1016/s0749-8063
(96)90217-0.
10. Paxton ES, Stock MV, Brophy RH. Meniscal repair
versus partial meniscectomy: a systematic review
comparing reoperation rates and clinical outcomes.
Arthroscopy. 2011;27:1275–88. https://doi.org/10.
1016/j.arthro.2011.03.088.
11. Seil R, Becker R. Time for a paradigm change in
meniscal repair: save the meniscus! Knee Surg Sports
Traumatol Arthrosc. 2016;24:1421–3. https://doi.org/
10.1007/s00167-016-4127-9.
12. Stein T, Mehling AP, Welsch F, von Eisenhart-Rothe
R, Jäger A. Long-term outcome after arthroscopic
meniscal repair versus arthroscopic partial meniscectomy for traumatic meniscal tears. Am J Sports Med.
2010;38:1542–8. https://doi.org/10.1177/03635465
10364052.
13. Fayard JM, Pereira H, Servien E, Lustig S,
Neyret
P.
Meniscectomy
global
results-
Anterior Knee Pain After Arthroscopic Meniscectomy …
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
complications. In: The meniscus. Springer;2010.
pp. 177–91.
Wünschel M, Leichtle U, Obloh C, Wülker N, Müller
O. The effect of different quadriceps loading patterns
on tibiofemoral joint kinematics and patellofemoral
contact pressure during simulated partial weightbearing knee flexion. Knee Surg Sports Traumatol
Arthrosc. 2011;19:1099–106. https://doi.org/10.
1007/s00167-010-1359-y.
Goicoechea N, Hinarejos P, Torres-Claramunt R,
Leal-Blanquet J, Sánchez-Soler J, Monllau JC. Patellar denervation does not reduce post-operative anterior knee pain after primary total knee arthroplasty
with patellar resurfacing. Knee Surg Sports Traumatol Arthrosc. 2021;29:3346–51. https://doi.org/10.
1007/s00167-020-06164-5.
Amestoy J, Pérez-Prieto D, Torres-Claramunt R,
Sánchez-Soler JF, Leal-Blanquet J, Ares-Vidal J,
Hinarejos P, Monllau JC. Patellofemoral pain after
arthroscopy: muscle atrophy is not everything.
Orthop J Sports Med. 2021;9:232596712110130.
https://doi.org/10.1177/23259671211013000.
Culvenor AG, Øiestad BE, Holm I, Gunderson RB,
Crossley KM, Risberg MA. Anterior knee pain
following anterior cruciate ligament reconstruction
does not increase the risk of patellofemoral
osteoarthritis at 15- and 20-year follow-ups.
Osteoarthr Cartil. 2017;25:30–3. https://doi.org/10.
1016/j.joca.2016.09.012.
Amestoy J, Pérez-Prieto D, Torres-Claramunt R,
Sánchez-Soler JF, Solano A, Leal-Blanquet J,
Hinarejos P, Monllau JC. Preoperative muscle
thickness influences muscle activation after arthroscopic knee surgery. Knee Surg Sports Traumatol
Arthrosc. 2021. https://doi.org/10.1007/s00167-02106820-4.
Becker R, Kopf S, Seil R, Hirschmann MT, Beaufils P, Karlsson J. From meniscal resection to
meniscal repair: a journey of the last decade. Knee
Surg Sports Traumatol Arthrosc. 2020;28:3401–4.
https://doi.org/10.1007/s00167-020-06316-7.
Akima H, Furukawa T. Atrophy of thigh muscles
after meniscal lesions and arthroscopic partial menisectomy. Knee Surg Sports Traumatol Arthrosc.
2005;13:632–7. https://doi.org/10.1007/s00167-0040602-9.
Brelin AM, Rue J-PH. Return to play following
meniscus surgery. Clin Sports Med. 2016;35:669–78.
https://doi.org/10.1016/j.csm.2016.05.010.
Sanchis-Alfonso V. Holistic approach to understanding anterior knee pain. Clinical implications. Knee
Surg Sports Traumatol Arthrosc. 2014;22:2275–85.
https://doi.org/10.1007/s00167-014-3011-8.
Sanchis-Alfonso V, Dye SF. How to deal with
anterior knee pain in the active young patient. Sports
Health. 2017;9:346–51. https://doi.org/10.1177/
1941738116681269.
Witvrouw E, Lysens R, Bellemans J, Cambier D,
Vanderstraeten G. Intrinsic risk factors for the
193
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
development of anterior knee pain in an athletic
population: a two-year prospective study. Am J
Sports Med. 2000;28:480–9. https://doi.org/10.1177/
03635465000280040701.
Chester R, Smith TO, Sweeting D, Dixon J, Wood S,
Song F. The relative timing of VMO and VL in the
aetiology of anterior knee pain: a systematic review
and meta-analysis. BMC Musculoskelet Disord.
2008;9:64. https://doi.org/10.1186/1471-2474-9-64.
Krishnan C, Williams GN. Factors explaining
chronic knee extensor strength deficits after ACL
reconstruction. J Orthop Res. 2011;29:633–40.
https://doi.org/10.1002/jor.21316.
Williams GN, Buchanan TS, Barrance PJ, Axe MJ,
Snyder-Mackler L. Quadriceps weakness, atrophy,
and activation failure in predicted noncopers after
anterior cruciate ligament injury. Am J Sports Med.
2005;33:402–7.
https://doi.org/10.1177/03635465
04268042.
Bleakney R, Maffulli N. Ultrasound changes to
intramuscular architecture of the quadriceps following intramedullary nailing. J Sports Med Phys
Fitness. 2002;42:120–5.
Lorentzon R, Elmqvist LG, Sjöström M, Fagerlund M, Fuglmeyer AR. Thigh musculature in
relation to chronic anterior cruciate ligament tear:
muscle size, morphology, and mechanical output
before reconstruction. Am J Sports Med.
1989;17:423–9. https://doi.org/10.1177/0363546589
01700318.
Lopresti C, Kirkendall DT, Street GM, Dudley AW.
Quadriceps Insufficiency following repair of the
anterior cruciate ligament. J Orthop Sports Phys
Ther. 1988;9:245–9. https://doi.org/10.2519/jospt.
1988.9.7.245.
Palmieri-Smith RM, Thomas AC, Wojtys EM. Maximizing quadriceps strength after ACL reconstruction. Clin Sports Med. 2008;27(405–424):vii–ix.
https://doi.org/10.1016/j.csm.2008.02.001.
Vora M, Curry E, Chipman A, Matzkin E, Li X.
Patellofemoral pain syndrome in female athletes: a
review of diagnoses, etiology and treatment options.
Orthop Rev (Pavia). 2018;9. https://doi.org/10.4081/
or.2017.7281.
Nakagawa TH, Moriya ÉTU, Maciel CD, SerrãO FV.
Trunk, Pelvis, hip, and knee kinematics, hip strength,
and gluteal muscle activation during a single-leg
squat in males and females with and without
patellofemoral pain syndrome. J Orthop Sports Phys
Ther. 2012;42:491–501. https://doi.org/10.2519/
jospt.2012.3987.
Mascal CL, Landel R, Powers C. Management of
patellofemoral pain targeting hip, pelvis, and trunk
muscle function: 2 case reports. J Orthop Sports Phys
Ther. 2003;33:647–60. https://doi.org/10.2519/jospt.
2003.33.11.647.
Ferber R, Bolgla L, Earl-Boehm JE, Emery C,
Hamstra-Wright K. Strengthening of the hip and core
versus knee muscles for the treatment of
194
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
J. Amestoy et al.
patellofemoral pain: a multicenter randomized controlled trial. J Athl Train. 2015;50:366–77. https://
doi.org/10.4085/1062-6050-49.3.70.
Hart JM, Pietrosimone B, Hertel J, Ingersoll CD.
Quadriceps activation following knee injuries: a
systematic review. J Athl Train. 2010;45:87–97.
https://doi.org/10.4085/1062-6050-45.1.87.
Ingersoll CD, Grindstaff TL, Pietrosimone BG,
Hart JM. Neuromuscular consequences of anterior
cruciate ligament injury. Clin Sports Med. 2008;27
(383–404):vii. https://doi.org/10.1016/j.csm.2008.03.
004.
Hart HF, Ackland DC, Pandy MG, Crossley KM.
Quadriceps volumes are reduced in people with
patellofemoral joint osteoarthritis. Osteoarthr Cartil.
2012;20:863–8. https://doi.org/10.1016/j.joca.2012.
04.009.
Lepley LK, Wojtys EM, Palmieri-Smith RM. Combination of eccentric exercise and neuromuscular
electrical stimulation to improve quadriceps function
post-ACL reconstruction. Knee. 2015;22:270–7.
https://doi.org/10.1016/j.knee.2014.11.013.
Knoll Z, Kocsis L, Kiss RM. Gait patterns before and
after anterior cruciate ligament reconstruction. Knee
Surg Sports Traumatol Arthrosc. 2004;12:7–14.
https://doi.org/10.1007/s00167-003-0440-1.
Shanbehzadeh S, Mohseni Bandpei MA, Ehsani F.
Knee muscle activity during gait in patients with
anterior cruciate ligament injury: a systematic review
of electromyographic studies. Knee Surg Sports
Traumatol Arthrosc. 2017;25:1432–42. https://doi.
org/10.1007/s00167-015-3925-9.
Akkurt E, Salli A, Ozerbil OM, Ugurlu H. The effect
of isokinetic exercise on symptoms, functional status,
and EC activation onset time of the vastus medialis
oblique and vastus lateralis in female patients with
patellofemoral pain syndrome. Isokinet Exerc Sci.
2010;18:157–61.
Briani RV, De Oliveira SD, Flóride CS, Aragão FA,
de Albuquerque CE, Magalhães FH, de
Azevedo FM. Quadriceps neuromuscular function
in women with patellofemoral pain: influences of the
type of the task and the level of pain. PLoS One.
2018;13: e0205553. https://doi.org/10.1371/journal.
pone.0205553.
Carry PM, Kanai S, Miller NH, Polousky JD.
Adolescent patellofemoral pain: a review of evidence
for the role of lower extremity biomechanics and core
instability. Orthopedics. 2010;33:498–507. https://
doi.org/10.3928/01477447-20100526-16.
Kuo L-T, Yu P-A, Chen C-L, Hsu W-H, Chi C-C.
Tourniquet use in arthroscopic anterior cruciate
ligament reconstruction: a systematic review and
meta-analysis of randomised controlled trials. BMC
Musculoskelet Disord. 2017;18:358. https://doi.org/
10.1186/s12891-017-1722-y.
Johnston PT, Feller JA, McClelland JA, Webster KE.
Knee strength deficits following anterior cruciate
ligament reconstruction differ between quadriceps
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
and hamstring tendon autografts. Knee Surg Sports
Traumatol Arthrosc. 2021. https://doi.org/10.1007/
s00167-021-06565-0.
Gatewood CT, Tran AA, Dragoo JL. The efficacy of
post-operative devices following knee arthroscopic
surgery: a systematic review. Knee Surg Sports
Traumatol Arthrosc. 2017;25:501–16. https://doi.org/
10.1007/s00167-016-4326-4.
Feil S, Newell J, Minogue C, Paessler HH. The
effectiveness of supplementing a standard rehabilitation program with superimposed neuromuscular
electrical stimulation after anterior cruciate ligament
reconstruction: a prospective, randomized, singleblind study. Am J Sports Med. 2011;39:1238–47.
https://doi.org/10.1177/0363546510396180.
Rebai H, Barra V, Laborde A, Bonny J-M,
Poumarat G, Coudert J. Effects of two electrical
stimulation frequencies in thigh muscle after knee
surgery. Int J Sports Med. 2002;23:604–9. https://
doi.org/10.1055/s-2002-35525.
Snyder-Mackler L, Delitto A, Bailey SL, Stralka SW.
Strength of the quadriceps femoris muscle and
functional recovery after reconstruction of the anterior cruciate ligament. A prospective, randomized
clinical trial of electrical stimulation. J Bone Joint
Surg Am. 1995;77(8):1166–73.
Gerber JP, Marcus RL, Dibble LE, Greis PE,
Burks RT, LaStayo PC. Effects of early progressive
eccentric exercise on muscle structure after anterior
cruciate ligament reconstruction. J Bone Joint Surg
Am. 2007;89:559–70. https://doi.org/10.2106/JBJS.
F.00385.
Harkey MS, Gribble PA, Pietrosimone BG. Disinhibitory interventions and voluntary quadriceps activation: a systematic review. J Athl Train.
2014;49:411–21. https://doi.org/10.4085/1062-605049.1.04.
Torry MR, Decker MJ, Viola RW, O’Connor DD,
Steadman JR. Intra-articular knee joint effusion
induces quadriceps avoidance gait patterns. Clin
Biomech (Bristol, Avon). 2000;15:147–59. https://
doi.org/10.1016/s0268-0033(99)00083-2.
Kopf S, Beaufils P, Hirschmann MT, Rotigliano N,
Ollivier M, Pereira H, Verdonk R, Darabos N,
Ntagiopoulos P, Dejour D, Seil R, Becker R. Management of traumatic meniscus tears: the 2019
ESSKA meniscus consensus. Knee Surg Sports
Traumatol Arthrosc. 2020;28:1177–94. https://doi.
org/10.1007/s00167-020-05847-3.
Capin JJ, Khandha A, Zarzycki R, Manal K,
Buchanan TS, Snyder-Mackler L. Gait mechanics
after ACL reconstruction differ according to medial
meniscal treatment. J Bone Joint Surg Am.
2018;100:1209–16. https://doi.org/10.2106/JBJS.17.
01014.
Lepley LK, Lepley AS, Onate JA, Grooms DR.
Eccentric exercise to enhance neuromuscular control.
Sports Health. 2017;9:333–40. https://doi.org/10.
1177/1941738117710913.
Anterior Knee Pain After Arthroscopic Meniscectomy …
57. Akkaya N, Ardic F, Ozgen M, Akkaya S, Sahin F,
Kilic A. Efficacy of electromyographic biofeedback
and electrical stimulation following arthroscopic
partial meniscectomy: a randomized controlled trial.
Clin Rehabil. 2012;26:224–36. https://doi.org/10.
1177/0269215511419382.
58. Rice DA, McNair PJ. Quadriceps arthrogenic muscle
inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum. 2010;40:250–66.
https://doi.org/10.1016/j.semarthrit.2009.10.001.
59. Kirnap M, Calis M, Turgut AO, Halici M, Tuncel M.
The efficacy of EMG-biofeedback training on quadriceps muscle strength in patients after arthroscopic
meniscectomy. 2005.
60. Eitzen I, Holm I, Risberg MA. Preoperative quadriceps strength is a significant predictor of knee
function two years after anterior cruciate ligament
reconstruction. Br J Sports Med. 2009;43:371–6.
https://doi.org/10.1136/bjsm.2008.057059.
61. Failla MJ, Arundale AJH, Logerstedt DS, SnyderMackler L. Controversies in knee rehabilitation. Clin
Sports Med. 2015;34:301–12. https://doi.org/10.
1016/j.csm.2014.12.008.
62. Sherman SL, DiPaolo ZJ, Ray TE, Sachs BM,
Oladeji LO. Meniscus injuries. Clin Sports Med.
2020;39:165–83. https://doi.org/10.1016/j.csm.2019.
08.004.
63. Ratamess N, Alvar BA, Evetoch TK, Housh TJ. Progression models in resistance training for healthy
adults. Med Sci Sports Exer. 2009;41:687–708.
https://doi.org/10.1249/MSS.0b013e3181915670.
64. Day B. Personalized blood flow restriction therapy:
how, when and where can it accelerate rehabilitation
after surgery? Arthrosc: J Arthrosc Related Surg.
2018;34:2511–3.
https://doi.org/10.1016/j.arthro.
2018.06.022.
65. DePhillipo NN, Kennedy MI, Aman ZS, Bernhardson AS, O’Brien LT, LaPrade RF.) The role of blood
flow restriction therapy following knee surgery:
expert opinion. Arthrosc: J Arthrosc Related Surg.
2018;34:2506–10. https://doi.org/10.1016/j.arthro.
2018.05.038.
66. Loenneke JP, Wilson JM, Marín PJ, Zourdos MC,
Bemben MG. Low intensity blood flow restriction
195
67.
68.
69.
70.
71.
72.
73.
training: a meta-analysis. Eur J Appl Physiol.
2012;112:1849–59. https://doi.org/10.1007/s00421011-2167-x.
Nascimento LR, Teixeira-Salmela LF, Souza RB,
Resende RA. Hip and knee strengthening is more
effective than knee strengthening alone for reducing
pain and improving activity in individuals with
patellofemoral pain: a systematic review with metaanalysis. J Orthop Sports Phys Ther. 2018;48:19–31.
https://doi.org/10.2519/jospt.2018.7365.
Motealleh A, Kordi Yoosefinejad A, Ghoddosi M,
Azhdari N, Pirouzi S. Trunk postural control during
unstable sitting differs between patients with patellofemoral pain syndrome and healthy people: a crosssectional study. Knee. 2019;26:26–32. https://doi.
org/10.1016/j.knee.2018.10.002.
Foroughi F, Sobhani S, Yoosefinejad AK, Motealleh A.
Added value of isolated core postural control training on
knee pain and function in women with patellofemoral
pain syndrome: a randomized controlled trial. Arch
Phys Med Rehabil. 2019;100:220–9. https://doi.org/10.
1016/j.apmr.2018.08.180.
Zazulak BT, Hewett TE, Reeves NP, Goldberg B,
Cholewicki J. Deficits in neuromuscular control of
the trunk predict knee injury risk: prospective
biomechanical-epidemiologic study. Am J Sports
Med. 2007;35:1123–30. https://doi.org/10.1177/
0363546507301585.
Sinclair JK, Selfe J, Taylor PJ, Shore HF,
Richards JD. Influence of a knee brace intervention
on perceived pain and patellofemoral loading in
recreational athletes. Clin Biomech. 2016;37:7–12.
https://doi.org/10.1016/j.clinbiomech.2016.05.002.
Saltychev M, Dutton R, Laimi K, Beaupré G,
Virolainen P, Fredericson M. Effectiveness of conservative treatment for patellofemoral pain syndrome: a systematic review and meta-analysis.
J Rehabil Med. 2018;50:393–401. https://doi.org/
10.2340/16501977-2295.
Aghapour E, Kamali F, Sinaei E. Effects of Kinesio
Taping® on knee function and pain in athletes with
patellofemoral pain syndrome. J Bodyw Mov Ther.
2017;21:835–9. https://doi.org/10.1016/j.jbmt.2017.
01.012.
Anterior Knee Pain Prevalence After
Anterior Cruciate Ligament
Reconstruction: Risk Factors
and Prevention
Antonio Darder-Sanchez, Antonio Darder-Prats,
and Vicente Sanchis-Alfonso
1
Introduction
Anterior cruciate ligament (ACL) tears are
nowadays one of the most prevalent knee injuries
with an estimated incidence of 68.6 per 100,000
person-years [1]. Surgical treatment through
ligament reconstruction accounts approximately
for 100,000 procedures each year in the United
States [2]. Although the results are considered
satisfactory as 90% of the patients have a normal
knee function restored, ACL reconstructions
have been linked to various complications [3].
Anterior knee pain (AKP) is one of the most
frequent postoperative complications in this type
of surgeries [4–6]. Several causes have been
described to be responsible of AKP such us
patellar tendinopathies, Hoffa´s disease, postoperative flexure contracture, quadriceps weakness
donor site morbidity or injuries to the infrapatellar branches of the saphenous nerves [7–9].
However, the exact origin and pathophysiology
is still unknown.
A. Darder-Sanchez (&)
Department of Orthopaedic Surgery, Hospital
Clínico Universitario, Valencia, Spain
e-mail: toni-9486@hotmail.com
A. Darder-Prats V. Sanchis-Alfonso
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
2
Prevalence
There is an important variability in the literature
when it comes to determine the exact prevalence
of AKP after an ACL reconstruction. The general
estimation, rates the prevalence of AKP between
5 and 40%. This variability may appear, on one
hand, due to the differences in the type of
patients, grafts or techniques used, and on the
other hand, because some studies talk exclusively
about AKP while others refer to donor site
morbidity, a wider term, which includes other
symptoms such as numbness.
Some classic reviews estimate a prevalence of
AKP ranging from 5 to 19% [10] while others
talk about 40–60% of patients experiencing
AKP, disturbance in anterior knee sensitivity or
inability to kneel [11]. In 2012, a retrospective
comparative study on 171 patients, showed an
overall prevalence of 42% at 3 months which fall
to a 11% at 2 years postoperatively [7]. Moreover, according to the results, 95% of the patients
who presents AKP at 2 years also presented it at
3 months, meaning that the origin of AKP is
acute in the vast majority of cases.
Some years later, Kanamoto et al. conducted a
prospective study on 57 patients who underwent
anatomic double bundle ACL reconstruction
with hamstring tendon (HT) graft. Six months
postoperatively, 32 out of 57 patients referred
anterior knee symptoms using the Kujala patellofemoral score, which reflects a total incidence
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_13
197
198
A. Darder-Sanchez et al.
of 56.1% [6]. More recently, Rousseau et al.
confirmed a 16% of AKP prevalence (130 of
811) during the 2 years after the intervention of
ACL reconstruction [4]. According to this study,
patellar tendinopathies represented 40% of these
cases whereas the other 60% was due to nonspecific causes not linked to patellar tendinopathies [4]. Most of the study periods include the
first 2 years after surgery, and it is a frequent
conclusion in the bibliography that AKP
decreases within these 2 years. Corry et al.
demonstrated an important decrease of AKP over
time, detecting a 55% prevalence of AKP at
1 year whereas at 2 years the prevalence was
31% [12]. In 2019, in the study mentioned
before, the prevalence reduced to a 2.7% after a
correct rehabilitation at the end of the 2-year
study period [4].
3
Risk Factors for AKP After ACL
Reconstruction
The origin of AKP after ACL reconstruction is
multifactorial and a clear cause has not been
identified yet. Different aspects regarding range
of motion, type of graft or technical errors during
surgery are involved in the appearance of AKP. It
is important to take into account this risk factors
in order to reduce the incidence of AKP.
3.1 Range of Motion (ROM) Deficits
Shelbourne and Trumper highlighted the importance of regaining full hyperextension to avoid
the appearance of AKP, stablishing in their study
there was a relationship between AKP and
extension deficits [11]. Sachs et al., years before
had stablished flexion contracture as an important factor of AKP [13]. In 2001, Kartus et al.,
reinforced this association, confirming there is
consensus in literature about the importance of
recovering hyperextension when it comes to
reducing AKP [9]. Recently, in 2020, da Silva
Marques et al. detected that the presence of knee
extension deficit increased the probability of
suffering from AKP by 5.3 times [14]. Moreover,
Niki et al. concluded that different factors where
related to the time of appearance of AKP [7].
Donor site morbidity and knee extension deficits
were related to early AKP whereas decreased
quadriceps strength and a poor Lysholm score
associated with late AKP. On the other hand,
flexion deficits generate controversy between
authors. While some older studies stated that the
loss of flexion was related to AKP [15], recent
studies did not find statistical differences between
groups despite a 5°–15° flexion deficit [7].
3.2 Type of Graft
Most of the studies about AKP stablish a relation
between the type of graft used in the ACL
reconstruction and its prevalence. According to
the bibliography, donor site morbidity is a crucial
factor and it is directly related to the technique
and the type of graft chosen. Classically, bone
patellar tendon bone (BPTB) graft has been
known as a risk factor for AKP. But, does the
evidence nowadays support this? How does the
appearance of new grafts affect the prevalence of
AKP? Do anatomical or double bundle techniques decrease AKP?
BPTB graft has been one of the most used and
reliable techniques for ACL reconstruction
despite some drawbacks such as postoperative
AKP, patellar fracture risk or patellar tendon
rupture [16, 17]. An important meta-analysis
back in 2003, comparing BPTB grafts and
hamstring (HT) grafts concluded that although
there were no statistically differences between
both groups in relation to loss of extension, there
was a slightly higher incidence of it in the BPTP
group (1.9 vs. 0.7%) [18]. Moreover, this study
demonstrated that the BPTB group presented a
higher rate of AKP compared to HT patients with
significant differences (17.4 vs. 11.5%).
According to Freedman et al., surgical damage to
the extensor mechanism during graft harvest is
the main responsible [18].
Webster et al., in a randomized clinical trial
with a 15 year follow up period described significant differences in AKP between both groups
at 8 months postoperatively (BPTB group 73%
Anterior Knee Pain Prevalence After Anterior Cruciate …
vs. HT group 35%) and at 2 years postoperatively (BPTB group 52% vs. HT group 17%)
[19]. However, the study found out that at
15 years postoperatively there were no significance differences between both groups (BPTB
group 38% vs. HT group 27%). The authors
concluded that donor site morbidity differences
between both groups found after 3 years [19],
were not present in a 15 year follow up. Moreover, according to this study, although the incidence of AKP was high, the severity of pain was
low with a mean of 3 on the BPTB group and 2.3
on the HT group on a 10-point scale. These
findings, are similar to those described in previous studies [20−21]. Recently, in a new metaanalysis, five studies reported results on anterior
knee pain prevalence in BPTB and HT groups
[22]. The statistical results showed that HT group
had advantages in AKP and kneeling pain on the
short and medium-term postoperative period as
the incidence of AKP in the BPTB group was
significantly higher.
Da Silva Marques et al., who studied 438
patients in order to predict the main variables
causing AKP after ACL reconstruction, found a
higher incidence in the BPBT group compared to
the HT group (9.7 vs. 2.7%) with a 3.4 odds ratio
between both groups [14]. The authors refer that
this happens because closing the defect of the
patellar tendon can lower the patella leading to
AKP and hypersensitivity specially when the
patellofemoral joint suffers extra pressure, for
example during squatting.
All these findings lead us to the conception
that BPTB graft is related to a higher incidence in
AKP. Contrary to this general idea, in 2009, an
important systematic review conducted by
Samuelsson et al. evaluated that, out of 16 articles analyzing AKP, 9 studies found no difference between both graft groups [23]. The other 7
articles found a higher incidence of AKP in the
BPTB group between the third and eighth
months after surgery, but this difference
decreased thereafter. Another interesting fact
analyzed was that there was no association
between different functional scores or clinical
variables and a higher occurrence in AKP.
199
According to the bibliography reviewed, AKP
is generally more frequent in patients treated with
BPTB grafts, but the fact that some studies have
not found difference, suggests that as we mentioned before there are other factors affecting the
appearance of AKP.
Currently, single-bundle technique is the most
frequently used in ACL reconstruction. However, studies comparing it with a double-bundle
technique are frequent, due to the theoretical
advantage of the latter of reproducing more
exactly the ACL anatomy. Aga et al., studied
quality of life parameters, including AKP, in
double-bundle and single-bundle reconstructions
[24]. They found no differences between both
groups. In 2010, another study published similar
conclusions [25]. In cadaveric studies, the
reconstruction of the posterolateral bundle
(PLB) causes an increased control of rotational
stability [26]. Considering this, an excessive
tension of the PLB could generate too much
constrain on tibial rotation affecting negatively to
the patellofemoral joint and consequently anterior knee pain. However, there are no studies to
this day that conclude there is a higher incidence
of anterior knee pain in double-bundle reconstructions. Further studies, focusing of patellofemoral tracking symptoms and anterior knee
pain are needed.
In the last years, with the desire to prevent
some of the morbidities caused by the graft
harvest, alternative grafts are being used.
Quadricipital tendon (QT) was first introduced
by Blauth et al. as it was thought it could reduce
donor site morbidity caused by traditional grafts
[27]. Studies have demonstrated good clinical
results with QT in ACL reconstruction when
compared to BPBT showing less incidence of
pressure pain, pain associated to knee flexion or
kneeling [28, 29]. Furthermore, a better extension capacity has also been noticed. However, in
this study, the authors found a higher postoperative level of activity in the BPTB group.
In 2016, Jon Kyu Lee et al. compared the
functional outcomes of a bone QT graft and a
double-bundle HT graft [30]. The study proved
that the BQT graft was not significantly different
200
from the HT graft in terms of knee stability and
functional outcomes. In order to evaluate AKP,
the Shelbourne and Trumper questionnaire [11]
was analyzed, and no significant difference was
found between both groups. There was not a
single item of the test were the BQT was superior
to HT group. Furthermore, the BQT showed a
better knee flexor muscle recovery, fact that has
also been reported in other studies [31].
Regarding knee extensor recovery no differences
were detected.
Recently a meta-analysis comparing the three
main graft types was published [32]. When it
comes to AKP, six studies compared donor site
pain between 439 patients in the QT graft group
and 287 patients in the BPTB group. They found
a significant difference, as the QT graft group
presented less incidence of AKP (risk ratio for
QT vs. BPTB group, 0.25; 95% CI, 0.18–0.36;
P < 0.00001). Besides that, four studies compared AKP between 136 patients who underwent
ACL reconstruction with QT graft and 135
patients with HT grafts. No significance differences were found between them. It has also been
described that QT patients achieve similar levels
of quadriceps isokinetic strength at 1-year postoperatively [33]. Other advantages reported of
the QT autograft include less pain and analgesic
use than with an HT reconstruction and the earlier capacity to achieve complete knee extension
and range of motion compared with BPTB
reconstruction [34].
Taking into account the bibliography
reviewed, the type of graft used influences the
appearance of AKP. Nevertheless, it is not the
only factor. Evidence nowadays support that
BPBT is the graft associated with a higher incidence of AKP. Although QT grafts, which are
popular lately, present similar risk of AKP when
compared to HT grafts, more quality studies need
to be conducted in order to evaluate all the
clinical outcomes of this graft in an ACL
reconstruction compared to more traditional
grafts.
A. Darder-Sanchez et al.
3.3 Intraoperative Technical Errors
There is a wide variety of technical errors that
can modify the normal biomechanics of the knee
causing patellofemoral symptoms. Arthrofibrosis
and more specifically the well-known cyclops
syndrome (Fig. 1), are complications after ACL
reconstruction which can limit the knee range of
motion, especially the knee hyperextension.
Therefore, they can cause the appearance of
AKP. In a recent study, 9% of the patients after
an ACL reconstruction presented an extension
deficit [4]. Half of this cases were caused by a
cyclops syndrome. The authors found no significant differences on the rate of cyclops syndrome
between the HT graft group and the BPTB group
[4]. Cyclops syndrome has been related to a too
anterior placement of the graft as well as to an
insufficient resection of the native ACL possible
remnants [35]. The most accepted treatment in
these cases is the arthroscopic resection of the
anterior fibrosis. Another type of arthrofibrosis is
the appearance of pretibial patellar tendon
adhesions. According to Stedman et al., this
scarring of the patellar tendon to the anterior face
of the tibia causes pain during the last degrees of
extension, a reduced mobility of the patella and a
patella infera due to traction of the tibial adhesions [36]. This traction modifies the force vector
and the angle between the quadriceps and the
patellar tendon, increasing the load to the patellofemoral joint, causing therefore AKP [36−37].
The treatment in this case, just as with the
cyclops syndrome, consists on arthroscopic
resection.
A correct graft placement is vital in order to
recover a full range of motion. When the tibial
tunnel is done too anterior, it causes an
impingement in the intercondylar notch in the
last degrees of extension. Moreover, an anterior
femoral tunnel will also produce a lack of
extension and consequently AKP. Evidence
shows that transtibial techniques are related with
higher incidences of knee extension deficits
Anterior Knee Pain Prevalence After Anterior Cruciate …
Fig. 1 Cyclops syndrome
compared to anatomical techniques [38]. Furthermore, a correct position of the graft on the
coronal plane can also affect both extension and
flexion because of an impingement with the
posterior cruciate ligament (PCL). When the
tibial tunnel is medial to the lateral tibial spine, it
can cause an impingement with the PCL with the
knee in flexion causing a deficit in flexion.
Related with the PCL impingement, Strobel
et al., reported an atypical cause of AKP [39].
According to their study, a 12 o’clock or “high
noon” position of the femoral tunnel causes an
impingement with PCL at the last degrees of
extension. This impingement triggers a proprioceptive reflex that restrains the last 20° of
extension. This limitation disappears when the
patient is anesthetized. A 3-D MRI reconstruction is the only image test capable of detecting it
and the treatment is a new ACL reconstruction
with correct tunnel placement. Residual anterior
instability has also been proven to be a risk factor
of AKP [15].
4
Prevention of AKP After ACL
Reconstruction
Problems with technique, grafts election and
postoperative range of motion achieved, are all
related to the appearance of AKP. In order to
201
prevent it, there are different solutions or alternatives which have proven to be effective.
One of the first studies that analyzed this
problem, concluded that the key aspect in prevention was to reach full knee hyperextension
[11] (Fig. 2). On one hand, the correct position
and size of the graft is crucial to avoid
impingement that cause a reduced range of
motion. On the other hand, a loss of complete
ROM can also be caused by an incorrect rehabilitation program. The main goals of rehabilitation after an ACL reconstruction in order to
prevent AKP must be returning to full range of
motion with especial emphasis on early hyperextension and avoiding both quadriceps and
hamstrings strength compared with the contralateral knee [9]. In order to avoid range of
motion loss, rehabilitation must start preoperatively just as Van Melick et al. stated in the
practice guidelines for ACL rehabilitation published in 2016 [40]. Cryotherapy as well as
immediate weight bearing have demonstrated to
reduce anterior knee pain in the short and medium postoperative period. Andersson et al., in
their systematic review, confirmed that closed
kinetic chain (CKC) quadricep exercises were
related to less pain than open chained
(OKC) quadriceps exercises [41]. Based on this
findings, Van Melick et al., recommend starting
the rehabilitation with CKC exercises, and only
start with OKC rehabilitation when the quadriceps has gained some strength, around 4 weeks
postoperatively.
According to the literature, graft harvest,
especially in BPBT reconstructions, is a cause of
AKP due to the injury of the infrapatellar branches of the saphenous nerves and the inflammation in the donor site [42]. It has been established
a relationship between preserved anterior knee
sensitivity and a significantly lower AKP incidence [43]. In order to prevent damage to these
structures, several studies have described different harvest techniques as a possible solution. One
of the first improvements proposed was suturing
the peritenon just to obtain a more anatomic and
functional scarring tissue [44]. Mini invasive
202
A. Darder-Sanchez et al.
Fig. 2 Knee hyperextension
harvest techniques using a double incision have
been proposed by some authors [42, 45]. Tsuda
et al. assert that the use of horizontal incisions
reduces the possible damage to the nervous
structures mentioned before and allows better
access to the tibial tunnel and the graft width
[45]. However, most of the authors use vertical
incisions just as exposed by Beaufils et al. [42].
According to them, graft harvest is done with the
knee at 90° of flexion. Two vertical incisions
each of approximately two centimeters are made.
The distal one is done just on the anterior tibial
tubercle while the proximal incision is done just
above the apex of the patella which allows not
damaging neither the peritenon nor the nervous
branches. In their study they observed a
decreased sensory morbidity as well as a lower
incidence in anterior knee pain in the double
incision group with a significant difference (19
vs. 58%) [42]. Gaudot et al. found similar results
in their study, strongly recommending this double incision harvesting technique [46].
Moreover, it has also been observed a
decrease in AKP with the filling of autologous
bone or beta-tricalcium phosphate (BTCP) to
reduce the bone defect in the harvesting site.
Higuchi et al., observed morphologically and
histologically that BTCP helped and accelerated
bone and patellar tendon remodeling [47]. One
year later Argawalla et al., described this technique and exposed that the main advantages of
using BTCP instead of autologous bone was the
absence of donor site morbidity and a bigger
graft availability [48]. Kato et al. who also
studied the use of BTCP concluded that the
protrusion of the BTCP graft had no adverse
effects and still reduced AKP [49].
Recently, a new graft harvesting incision has
been exposed with encouraging results [50].
Janani et al. described a small incision which
allowed a mobile window to both harvest the
graft and use it to drill the tibial tunnel. They use
an oblique incision of about four to five centimeters done with the knee at 30° of flexion over
the patellar tendon with the proximal border on
the lateral side with a distal and medial direction.
With the help of retractors, they create a rectangular window. The patellar tendon is harvested
with the knee at 100–120° while the tibial
tuberosity bone plug is obtained with the knee at
30º of flexion. Finally with the knee in complete
extension, the patellar bone plug is harvested. In
this study, Janani compared the incidence of
AKP between patients who underwent this
technique and people who underwent ACL
reconstructions with HT grafts. They concluded
there were no differences between both groups,
the incidence at 3 months was 28.9% and 25.5%
respectively while at 18 months was 6.59% and
6.05% respectively.
The use of the contralateral autograft patellar
tendon is not common between surgeons due to
the donor site morbidity caused in a completely
healthy knee. Nevertheless, Shelbourne et al. a
few years ago studied the IKDC and the
quadriceps muscle strength using either
Anterior Knee Pain Prevalence After Anterior Cruciate …
ipsilateral or contralateral patellar tendon [51].
After surgery, a rehabilitation protocol based on
antagonistic exercises on both knees was used:
rehabilitation on the donor site knee was focused
on recovering strength while the main goal in the
ACL reconstructed knee was gaining range of
motion. The results showed that in the contralateral knee group both knees showed significantly more quadriceps strength than the ACL
reconstructed knee in the ipsilateral group after a
2-year follow-up period. Although a better
quadriceps strength has been related to less AKP,
this study showed no differences on subjective
symptoms such as kneeling pain or range of
motion between groups. More studies correlating
contralateral patellar grafts with symptoms such
as AKP must be done to evaluate if there really
exists any benefit.
The infrapatellar fat pad (IPFP) is known to
have a relevant role in the patellofemoral
pathophysiology as it has a biomechanical
function and it is responsible for modulating the
inflammatory response at this level. Therefore, it
has been hypothesized it could be a source of
AKP. Kanamoto et al., added as an independent
risk factor for AKP after an ACL reconstruction,
the increased blood flow in the IPFP measured by
ultrasounds [6]. This finding took other authors
to study if a smaller resection of the IFP in the
ACL footprint resulted in a decrease of
AKP. Recently, Asai et al. concluded that
removing the IFP had no effects on clinical outcomes after ACL reconstruction including AKP
[52]. Further studies may elucidate what is the
exact role of the IPFP in the appearance of AKP.
In the last years, biological treatments such us
platelet rich plasma (PRP) or plasma rich in
growth factors (PRGF) have been used in a wide
variety of pathologies in orthopedic surgery to
try to accelerate the maturation of different tissues. When it comes to ACL surgery, several
studies have investigated its effects on the harvesting site, especially with the BPTB graft
technique in order to reduce the AKP that
appears due to the donor site gap. Walters et al.,
hypothesized that PRP in the donor site could
reduce AKP [53]. They concluded that there
were no differences between groups neither in
203
kneeling pain nor in AKP with the daily activities
at 12 weeks and 6 months postoperatively.
These results contradict a previous study which
confirmed a decrease in subjective pain at
twelve-month follow-up in the group treated with
PRP [54]. Therefore, more studies must be conducted in order to elucidate the real effect of PRP
in AKP. Seijas et al., carried a randomized
prospective trial, measuring with ultrasound if
PRGF accelerated maturity of the patellar tendon
[55]. The results showed significant differences
exclusively in the fourth month of follow-up but
not in the rest of follow-up times. However,
studies investigating if there is a correlation
between a faster regeneration and a decrease in
the occurrence of AKP need to be conducted.
To sum up, in order to prevent the appearance
of AKP we can act both over rehabilitation and
technical aspects of the surgery. When it comes
to rehabilitation, gaining muscle strength as well
as complete range of motion are key points,
especially early complete hyperextension. A delicate surgical technique is also fundamental. On
one hand, a correct placement of the femoral
tunnel is vital to avoid notching and loss of
extension. On the other hand, orthopedic surgeons must try to use harvesting techniques that
reduce morbidity on the donor site.
5
Take Home Messages
• AKP is one of the most frequent complications after ACL reconstruction. Although the
severity of the symptoms is usually not much,
its prevalence is really high specially during
the first two years after surgery.
• The risk factors are multiple and the phisiopathological mechanism is still unclear but
literature agrees that a loss of range of motion,
the graft harvesting site and the surgical
technique have a direct relation with the
occurrence of AKP.
• A loss of hyperextension and BPTB graft
seem to be associated with a higher incidence
of AKP. The popular QT graft has demonstrated less donor site morbidity than the
BPBT and no differences when compared
204
with HT graft, therefore it may be a good
alternative.
• In order to prevent AKP different solutions
have been proposed: specified rehabilitation
protocols, modifications of the graft harvesting technique, the use of bone to fill de donor
site gap or the possible effectiveness of
orthobiological techniques.
• More studies need to be conducted in order to
define what are the exact causes of AKP after
ACL reconstruction and consequently reduce
both the incidence and prevalence of this
frequent complication.
References
1. Sanders TL, Maradit Kremers H, Bryan AJ, et al.
Incidence of anterior cruciate ligament tears and
reconstruction: a 21-year population-based study.
Am J Sports Med. 2016;44(6):1502–7.
2. Campbell W, Canale S, Beaty J, et al. Campbell’s
operative orthopaedics. Philadelphia: Elsevier; 2017.
3. Ardern CL, Taylor NF, Feller JA, et al. Fifty-five per
cent return to competitive sport following anterior
cruciate ligament reconstruction surgery: an updated
systematic review and meta-analysis including
aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543–52.
4. Rousseau R, Labruyere C, Kajetanek C, et al.
Complications after anterior cruciate ligament reconstruction and their relation to the type of graft: a
prospective study of 958 cases. Am J Sports Med.
2019;47(11):2543–9.
5. Samuelsen BT, Webster KE, Johnson NR, et al.
Hamstring autograft versus patellar tendon autograft
for ACL reconstruction: is there a difference in graft
failure rate? A meta-analysis of 47,613 patients. Clin
Orthop Relat Res. 2017;475(10):2459–68.
6. Kanamoto T, Tanaka Y, Yonetani Y, et al. Anterior
knee symptoms after double-bundle ACL reconstruction with hamstring tendon autografts: an ultrasonographic and power Doppler investigation. Knee Surg
Sports Traumatol Arthrosc. 2014;23(11):3324–9.
7. Niki Y, Hakozaki A, Iwamoto W, et al. Factors affecting
anterior knee pain following anatomic double-bundle
anterior cruciate ligament reconstruction. Knee Surg
Sports Traumatol Arthrosc. 2012;20:1543–9.
8. Ogilvie-Harris DJ, Giddens J. Hoffa’s disease:
arthroscopic resection of the infrapatellar fat pad.
Arthroscopy. 1994;10:184–7.
9. Kartus J, Movin T, Karlsson J. Donor-site morbidity
and anterior knee problems after anterior cruciate
ligament reconstruction using auto-grafts. Arthroscopy. 2001;17(9):971–80.
A. Darder-Sanchez et al.
10. Sachs RA, Daniel DM, Stone ML, et al. Patellofemoral problems after anterior cruciate ligament
reconstruction. Am J Sports Med. 1989;17:760–5.
11. Shelbourne KD, Trumper RV. Preventing anterior
knee pain after anterior cruciate ligament reconstruction. Am J Sports Med. 1997;25:41–7.
12. Corry IS, Webb JM, Clingeleffer AJ, et al. Arthroscopic reconstruction of the anterior cruciate ligament: a comparison of patellar tendon autograft and
four-strand hamstring tendon auto-graft. Am J Sports
Med. 1999;27(4):444–54.
13. Sachs RA, Daniel DM, Stone ML, et al. Patellofemoral problems after anterior cruciate ligament
reconstruction. Am J Sports Med. 1989;17:760–5.
14. Marques F, Barbosa P, Alves P, et al. Anterior knee
pain after anterior cruciate ligament reconstruction.
Orthop J Sports Med. 2020;8(10):232596712096108.
15. Kartus J, Magnusson L, Stener S, et al. Complications following arthroscopic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol
Arthrosc. 1999;7(1):2–8.
16. Tsuda E, Okamura Y, Ishibashi Y, et al. Techniques
for reducing anterior knee symptoms after anterior
cruciate ligament reconstruction using a bone-patellar
tendon-bone autograft. Am J Sports Med.
2001;29:450–6.
17. Slone HS, Romine SE, Premkumar A, et al. Quadriceps tendon auto-graft for anterior cruciate ligament
reconstruction: a comprehensive review of current
literature and systematic review of clinical results.
Arthroscopy. 2015;31(3):541–54.
18. Freedman KB, D’Amato MJ, Nedeff DD. Arthroscopic anterior cruciate ligament reconstruction: a
meta-analysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med. 2003;31
(1):2–11.
19. Webster KE, Feller JA, Hartnett N, et al. Comparison
of patellar tendon and Hamstring tendon anterior
cruciate ligament reconstruction: a 15-year follow-up
of a randomized controlled trial. Am J Sports Med.
2016;44:83–90.
20. Feller JA, Webster KE. A randomized comparison of
patellar tendon and hamstring tendon anterior cruciate ligament reconstruction. Am J Sports Med.
2003;31:564–73.
21. Holm I, Oiestad BE, Risberg MA, et al. No
differences in prevalence of osteoarthritis or function
after open versus endoscopic technique for anterior
cruciate ligament reconstruction: 12-year follow-up
report of a randomized controlled trial. Am J Sports
Med. 2012;40(11):2492–8.
22. Zhao L, Lu M, Deng M, et al. Outcome of bone–
patellar tendon–bone vs hamstring tendon autograft
for anterior cruciate ligament reconstruction. Medicine. 2020;99(48): e23476.
23. Samuelsson K, Andersson D, Karlsson J. Treatment
of anterior cruciate ligament injuries with special
reference to graft type and surgical technique: an
assessment of randomized controlled trials. Arthroscopy. 2009;25:1139–74.
Anterior Knee Pain Prevalence After Anterior Cruciate …
24. Aga C, Risberg M, Fagerland M, et al. No difference
in the KOOS Quality of life subscore between
anatomic double-bundle and anatomic single-bundle
anterior cruciate ligament reconstruction of the knee:
a prospective randomized controlled trial with 2
years’ follow-up. Am J Sports Med. 2018;46
(10):2341–54.
25. Aglietti P, Giron F, Losco M, et al. Comparison
between single- and double-bundle anterior cruciate
ligament reconstruction. Am J Sports Med. 2009;38
(1):25–34.
26. Belisle AL, Bicos J, Geaney L, et al. Strain pattern
comparison of double- and single-bundle anterior
cruciate ligament reconstruction techniques with the
native anterior cruciate ligament. Arthroscopy.
2007;23:1210–7.
27. Blauth W. 2-strip substitution-plasty of the anterior
cruciate ligament with the quadriceps tendon [in
German]. Unfallheilkunde. 1984;87(2):45–51.
28. Gorschewsky O, Klakow A, Putz A, et al. Clinical
comparison of the autologous quadriceps tendon
(BQT) and the autologous patella tendon (BPTB) for
the reconstruction of the anterior cruciate ligament.
Knee Surg Sports Traumatol Arthrosc. 2007;15
(11):1284–92.
29. Slone HS, Romine SE, Premkumar A, et al. Quadriceps tendon auto-graft for anterior cruciate ligament
reconstruction: a comprehensive review of current
literature and systematic review of clinical results.
Arthroscopy. 2015;31(3):541–54.
30. Lee JK, Lee S, Lee MC. Outcomes of anatomic
anterior cruciate ligament reconstruction: bonequadriceps tendon graft versus double-bundle hamstring tendon graft. Am J Sports Med. 2016;44
(9):2323–9.
31. Cavaignac E, Coulin B, Tscholl P, et al. Is quadriceps
tendon autograft a better choice than hamstring
autograft for anterior cruciate ligament reconstruction? A comparative study with a mean follow-up of
3.6 years. Am J Sports Med. 2017;45(6):1326–32.
32. Mouarbes D, Menetrey J, Marot V, et al. Anterior
cruciate ligament reconstruction: a systematic review
and meta-analysis of outcomes for quadriceps tendon
autograft versus bone-patellar tendon–bone and
hamstring-tendon autografts. Am J Sports Med.
2019;47(14):3531–40.
33. Han HS, Seong SC, Lee S. Anterior cruciate ligament
reconstruction: quadriceps versus patellar autograft.
Clin Orthop Relat Res. 2008;466:198–204.
34. Joseph M, Fulkerson J, Nissen C, et al. Short-term
recovery after anterior cruciate ligament reconstruction: a prospective comparison of three autografts.
Orthopedics. 2006;29(3):243–8.
35. Jackson DW, Schaefer RK. Cyclops syndrome: loss
of extension following intra-articular anterior cruciate
ligament reconstruction. Arthroscopy. 1990;6:171–8.
36. Steadman JR, Dragoo JL, Hines SL, et al. Arthroscopic release for symptomatic scarring of the
anterior interval of the knee. Am J Sports Med.
2008;36:1763–9.
205
37. Ahmad CS, Kwak SD, Ateshian GA, et al. Effects of
patellar tendon adhesion to the anterior tibia on knee
mechanics. Am J Sports Med. 1998;26:715–24.
38. Kopf S, Forsythe B, Wong AK, et al. Nonanatomic
tunnel position in traditional transtibial single-bundle
anterior cruciate ligament reconstruction evaluated
by three-dimensional computed tomography. J Bone
Joint Surg Am. 2010;926:1427–31.
39. Strobel MJ, Castillo RJ, Weiler A. Reflex extension
loss after anterior cruciate ligament reconstruction
due to femoral “high noon” graft placement. Arthroscopy. 2001;17:408–11.
40. Van Melick N, van Cingel R, Brooijmans F, et al.
Evidence-based clinical practice update: practice
guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br J Sports Med. 2016;50
(24):1506–15.
41. Andersson D, Samuelsson K, Karlsson J. Treatment
of anterior cruciate ligament injuries with special
reference to surgical technique and rehabilitation: an
assessment of randomized controlled trials. Arthroscopy. 2009;25:653–85.
42. Beaufils P, Gaudot F, Drain O, et al. Mini-invasive
technique for bone patellar tendon bone harvesting:
its superiority in reducing anterior knee pain following ACL reconstruction. Curr Rev Musculoskelet
Med. 2011;4(2):45–51.
43. Kartus J, Magnusson L, Stener S, et al. Complications following arthroscopic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol
Arthrosc. 1999;7(1):2–8.
44. Berg P, Mjoberg B. A lateral skin incision reduces
peripatellar dysaesthesia after knee surgery. J Bone
Joint Surg Br. 1991;73:374–6.
45. Tsuda E, Okamura Y, Ishibashi Y, et al. Techniques
for reducing anterior knee symptoms after anterior
cruciate ligament reconstruction using a bone-patellar
tendon-bone autograft. Am J Sports Med. 2001;29
(4):450–6.
46. Gaudot F, Leymarie JB, Drain O, et al. Doubleincision mini-invasive technique for BTB harvesting:
its superiority in reducing anterior knee pain following ACL reconstruction. Orthop Traumatol Surg Res.
2009;95:28–35.
47. Higuchi H, Kobayashi A, Ikeda K, et al. Efficacy of
b-tricalcium phosphate graft into the bone defects
after bone-patellar tendon-bone anterior cruciate
ligament reconstruction. J Knee Surg. 2017;30:467–
73.
48. Agarwalla A, Puzzitiello R, Garcia GH, et al.
Application of a beta-tricalcium phosphate graft to
minimize bony defect in bone–patella tendon–bone
anterior cruciate ligament reconstruction. Arthrosc
Tech. 2018;7(7):e725-9.
49. Kato Y, Chavez J, Yamada S, et al. Beta-tricalcium
phosphate block for donor site morbidity of the
patella in anterior cruciate ligament reconstruction
using bone-patellar tendon-bone graft. Knee Surg
Relat Res. 2019;31(2):113–9.
206
50. Janani G, Suresh P, Prakash A, et al. Anterior knee
pain in ACL reconstruction with BPTB graft—Is it a
myth? Comparative outcome analysis with hamstring
graft in 1,250 patients. J Orthop. 2020;22:408–13.
51. Shelbourne K, Beck M, Gray T. Anterior cruciate
ligament reconstruction with contralateral autogenous patellar tendon graft. Am J Sports Med.
2014;43(3):648–53.
52. Asai K, Nakase J, Oshima T, et al. Partial resection of
the infrapatellar fat pad during anterior cruciate
ligament reconstruction has no effect on clinical
outcomes including anterior knee pain. Arch Orthop
Trauma Surg. 2020;140(11):1751–7.
53. Walters B, Porter D, Hobart S, et al. Effect of
intraoperative platelet-rich plasma treatment on
A. Darder-Sanchez et al.
postoperative donor site knee pain in patellar tendon
autograft anterior cruciate ligament reconstruction: a
double-blind randomized controlled trial. Am J
Sports Med. 2018;46(8):1827–35.
54. Cervellin M, deGirolamo L, Bait C, et al. Autologous
platelet-rich plasma gel to reduce donor site morbidity after patellar tendon graft harvesting for anterior
cruciate ligament reconstruction: a randomized, controlled clinical study. Knee Surg Sports Traumatol
Arthrosc. 2012;20(1):114–20.
55. Seijas R, Rius M, Ares O, et al. Healing of donor site
in bone-tendon-bone ACL reconstruction accelerated
with plasma rich in growth factors: a randomized
clinical trial. Knee Surg Sports Traumatol Arthrosc.
2015;23(4):991–7.
Patellar Tendinopathy: Risk Factors,
Prevention, and Treatment
Rochelle Kennedy and Jill Cook
1
Introduction
Patellar tendinopathy is an overuse injury characterised by localised pain at the inferior pole of
the patella during activities that mechanically
load the tendon [1]. It is most common in young,
athletic males participating in sports that place
substantial demands on the knee extensors.
Activities such as jumping or changing direction
are often most provocative, as these tasks require
large amounts of energy storage and release in
the patellar tendon [2].
Patellar tendinopathy can be a chronic and
debilitating condition, which can result in prolonged absence from sport and may be career
threatening [3]. Previous research has found that
more than one third of athletes presenting for
management of patellar tendinopathy were
unable to return to sport at 6-month follow-up
[4], and more than 50% were forced to retire
from sport altogether [5]. Research in sub-elite
athletes reported that patellar tendinopathy is
most common in volleyball and basketball athletes, with prevalence rates reported to be 14.4%
and 11.8% respectively [6]. The National Bas-
R. Kennedy (&) J. Cook
La Trobe University, Melbourne, Australia
e-mail: Rochelle.Kennedy@latrobe.edu.au
J. Cook
e-mail: j.cook@latrobe.edu.au
ketball Association (NBA) also reported that
0.8% of missed games annually were attributable
to patellar tendon injury, however this time-loss
definition of injury may not capture those athletes who continue to play despite patellar tendon
pain [7].
Tendinopathy is the clinical term for persistent tendon pain and loss of function related to
mechanical load [1]. This is distinct from tendinosis, which is a pathological term used to
describe tendon pathology [1]. A high proportion
of physically active individuals who have no
history of lower limb tendinopathy will demonstrate abnormalities on tendon imaging, with
nearly one in five physically active individuals
demonstrating asymptomatic Achilles or patellar
tendon changes [8]. Careful interpretation of
imaging findings is critical, as asymptomatic
tendon changes can co-exist with other painful
conditions. For example, 32–72% of individuals
with patellofemoral joint pain also exhibit
asymptomatic patellar tendon abnormalities,
confusing an already complex clinical picture [9,
10]. It is important to highlight that tendinopathy
is principally a clinical diagnosis and imaging is
not required as part of the diagnosis.
Clinicians should be aware of the high
prevalence of asymptomatic pathology on
imaging and interpret any imaging findings in
accordance with the clinical presentation. Patellar
tendinopathy presents a significant diagnostic
challenge, with much clinical overlap with other
conditions of the anterior knee such as
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_14
207
208
patellofemoral joint pain [11]. Common diagnostic criteria include palpation tenderness,
reproduction of symptoms during pain provocation testing and imaging abnormality [12].
However, these tests are non-specific and may
aggravate other structures of the anterior knee
[12], and the prevalence of asymptomatic imaging abnormalities is high [8]. Current evidence
suggests the combination of pain provocation
tests with localised pain under load increases
diagnostic accuracy [12]. A recent study of
anterior knee pain in basketball players found
that although diffuse anterior knee pain was very
common, pain localised to the inferior pole of the
patella, a key diagnostic criterion for patellar
tendinopathy, was not [12].
Additionally, the types of movements that
aggravate the patellar tendon may differ from
those that aggravate other structures of the
anterior knee. The patellar tendon is exposed to
the highest magnitude of tensile load when being
used like a spring to store and release energy
[13]. This movement must be fast, as the tendon
is viscoelastic, therefore slower movements do
not result in energy storage [14]. In the case of
the patellar tendon, tensile load is the primary
consideration, as there are no friction or compressive loads on the patellar tendon. Clinicians
should pay close attention to the types of activities that cause aggravation, and if these are of
low tensile load such as slow heavy resistance,
this should raise suspicion of a non-tendon cause
of pain. Therefore, it is important that both the
pain location and the type of provocative load is
considered during the clinical reasoning process.
Despite numerous hypotheses regarding the
aetiology and pathogenesis of patellar tendon
pathology, the exact pathoaetiology remains
unknown. The continuum model of tendon
pathology is based on a cell-driven response and
describes four primary states of pathology;
reactive, dysrepair, degenerative and reactive on
degenerative [15]. It is important to note that
although the model is described in discrete
stages, it is a continuum, and therefore there is
fluidity between the stages [15].
Several changes occur within the tendon as
pathology progresses along the continuum.
R. Kennedy and J. Cook
Tenocytes are upregulated, there is an increase
in large proteoglycan content and bound water
infiltration, matrix changes, collagen disorganisation and a progressive loss of hierarchical
structure [16]. As pathology becomes degenerative, there may be vascular infiltration [16].
These changes may be reversible with load
modification and exercise early in the continuum,
but as pathology progresses to the degenerative
stage, changes become largely irreversible and
this region of the tendon is unlikely to be able to
transmit tensile load [16]. Critically, these
changes usually occur in a localised region
within the tendon, and there is usually significant
volume of normal tendon surrounding the
degenerative area [17]. Therefore, despite
degenerative changes being irreversible, there is
still capacity to load the tendon and change
symptoms [17]. Reactive on degenerative
pathology refers to reactive tendinopathy within
the normal part of a degenerative tendon [15]. As
degenerative regions of a tendon are unable to
transmit load due to the loss of matrix structure,
this may result in overload of the normal part
of the tendon if loads are not managed appropriately [15]. As with reactive tendon
pathology, this state is reversible if overload is
addressed.
The relationship between tendon pathology
and pain is not absolute, however the presence of
pathology is a risk factor for an individual
becoming symptomatic [18]. In professional
football players, an association has been found
between ultrasound detected patellar tendon
abnormalities at the beginning of the season and
increased risk of developing symptoms
throughout the season [19]. Furthermore, a
cohort study of professional dancers showed that
the presence of focal hypoechoic changes was
associated with the future development of
tendon-related pain [20]. Conversely, in Australian football players, pre-season imaging was
not able to predict the development of symptoms
in-season, whereas simply asking the players
whether they had experienced symptoms previously had greater predictive value [21]. This
tenuous relationship between pathology and
symptoms suggest that clinicians should be more
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
concerned with aberrant loading patterns as
opposed to the presence of pathological changes
within the tendon.
2
Clinical Presentation
Subjective Examination
Patellar tendinopathy pain increases in a dose
dependent manner with increasing patellar tendon load but remains localised to the inferior
pole of the patella [3]. Typically, individuals
with patellar tendinopathy present with gradual
onset, localised pain at the inferior pole of the
patella, which began following changes in their
training load or intensity [3]. Patellar tendon pain
is mechanical in nature and occurs when the
tendon is loaded, ceasing or reducing when
loading stops [22]. The ‘warm-up phenomenon’
is a common and misleading feature of tendon
pain, whereby pain decreases throughout a
loading bout but is often worse after activity or
the next morning [22]. Consequently, the early
warning signs of tendinopathy are frequently
ignored, as the importance of this initial pain is
often underestimated.
3
Risk and Associated Factors
Changes in Load
While load is essential to maintain tendon
structure, mechanical properties and capacity,
excess load is linked to pathology and pain.
Tendon pain is commonly preceded by rapid
changes in demand on the tendon to store and
release energy [22]. The increased prevalence of
patellar tendinopathy during the pre-season period is indicative of this, as this time of the season
is characterised by rapid increases in load after a
period of relative unloading [23]. Clinicians
should identify and address any relevant changes
in load preceding the development of symptoms,
as this forms a key component of effective
management and prevention.
209
Age
The onset of patellar tendon pathology may
occur earlier than in other tendons. While
pathology in other tendons has been linked to
load accumulation [14], patellar tendinopathy is
highly prevalent in young, jumping athletes,
primarily aged between 14 and 18 [24]. Furthermore, longitudinal research has indicated that
pathology in the patellar tendon is less likely to
develop after adolescence [25]. The maturation
process of the patellar tendon differs from other
tendons as it does not have an apophysis, and
instead matures through a cartilage plate at both
the proximal [20] and distal ends [26]. A mature
tendon bone attachment is reached approximately
2 years after peak height velocity [20]. Exposure
to repetitive, high magnitude tendon load during
this maturation period may disrupt the developing bone-tendon junction [20, 26], leading to
pathological changes indistinguishable from
tendon pathology seen later in life [27]. This is
clinically important as patellar tendon pathology
that develops during adolescence will remain
throughout life [25]. However, whether an individual will develop symptoms associated with
this pathology is related to aberrant loading
patterns.
Quadriceps/Calf Strength
Atrophy or reduced strength in anti-gravity
muscles including gluteus maximus, quadriceps
and calf is often observed in longstanding cases
of patellar tendinopathy [3]. Patellar tendinopathy has been linked with significant motor cortex
inhibition [28], which may explain the persistent
atrophy sometimes present in chronic cases.
Additionally, persistent pain with mechanical
loads in patellar tendinopathy may result in
profound unloading, as the individual quickly
learns the movements to unload the tendon.
Clinically, atrophy in the calf muscle complex
may be just as substantial as quadriceps wasting,
and it is therefore important to examine the entire
lower limb kinetic chain to identify relevant
deficits.
210
Biomechanical Factors
Biomechanical factors associated with PT
include restricted ankle dorsiflexion range of
movement and a rigid, supinated foot [29, 30]. It
has been found that having less than 45° of ankle
dorsiflexion is associated with patellar
tendinopathy [29]. This is likely due to decreased
shock-absorption at the ankle when landing that
leads to increased knee loading during take-off
[29]. Therefore, it may be important to be aware
of both inherent restrictions of dorsiflexion range
of movement, as well as other confounding factors that may reduce dorsiflexion range, such as
recent or repeated ankle inversion injuries or
anterior ankle impingement [29].
Sex
Patellar tendinopathy is more prevalent in men
compared to women, men have twice the
prevalence of women across different sports [2,
31]. It is proposed that this is due to a reduced
force-generating capacity of the knee extensors
in women, thereby reducing the amount of force
transmitted through the patellar tendon [2].
Additionally, an observational study of male and
female volleyball players found that women have
a substantially lower average jump frequency
compared to men [32]. Investigations of the
jumping and landing kinematics of both male and
female volleyball players found that when participants were matched for jump height, they
generated similar patellar tendon loads irrespective of sex [33]. Clinically, women with patellar
tendinopathy tend to be elite jumping athletes,
who can transmit exceptionally high forces
through their patellar tendon. It is therefore likely
that that sex-based differences in prevanlence
R. Kennedy and J. Cook
rates are attributable to the force generating
capacity of the knee extensors.
Jumping Ability
Excellent jumping ability has also been identified
as a risk factor for the development of patellar
tendinopathy. Prospective studies have found
that those athletes who had a better jumping
ability were more likely to develop patellar
tendinopathy [34]. This phenomenon is known as
the ‘jumper’s knee paradox’ [34]. It has been
proposed that this may be due to the amount of
force these athletes are able to transmit through
the patellar tendon [34].
Level of Sporting Participation
Patellar tendinopathy prevalence seems to
increase with level of sporting participation.
Athletes competing at an international level have
been shown to be up to three times more likely to
develop patellar tendinopathy when compared to
their sub-elite counterparts [35]. This association
may be related to the ‘jumper’s knee paradox’, or
the high training loads associated with elite level
sport [35]. Comparison of the landing kinematics
and patellar tendon loads has found no significant
differences between elite and sub-elite players,
indicating that training load may be the primary
contributing factor to the difference between
these groups [35] (Table 1).
4
Athletes with patellar tendinopathy should be able
to indicate with one finger the location of their
pain. Pain is localised to the inferior pole of the
Table 1 Risk and associated factors for patellar tendinopathy
Young males
Jumping athlete
Decreased ankle dorsiflexion range of movement
Natural jumping ability
Level of sporting participation
Changes in load
Physical Examination/Differential
Diagnosis
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
211
Table 2 Progressive loading test for the patellar tendon
Progressive loading test for patellar tendon
Double leg squat or double leg decline board squat
Single leg squat or single leg decline squat
Double leg jump
Single leg jump
Stop jump
patella and does not move or spread with load [3].
It is important to ask the athlete to indicate the
location of their pain under load, as opposed to
tenderness on palpation, as palpation has been
shown to have low clinical utility when diagnosing patellar tendinopathy [36]. As normal tendons
may be tender to palpate, the absence of palpation
tenderness may be more useful clinically, as it may
indicate a non-tendon diagnosis [36].
Patellar tendon pain should increase in a dosedependent manner in response to increases in
patellar tendon load. Examination should begin
with low patellar tendon load activities and progress towards tasks requiring greater energy storage and release in the patellar tendon (Table 2).
For example, assessment should commence with a
low load task such as a double leg squat, and
progress towards double and single leg jumps.
Throughout this progressive loading test, the
individual is asked to indicate the location of their
pain under load, which should remain localised,
and rate the intensity of pain on a numerical pain
rating scale. Pain consistent with patellar tendon
origin should increase in a dose-dependent manner throughout the progressive loading test. It is
also important to be aware of any aberrant
movement patterns during assessment. For
example, individuals with patellar tendinopathy
often demonstrate poorer lower leg power with
jumping and hopping tasks and avoid deeper
ranges of knee flexion when hopping. Hip
mechanics during hopping are often relatively
good, especially when compared with those
commonly demonstrated by individuals with other
conditions of the anterior knee such as patellofemoral pain syndrome.
The decline squat (Fig. 1) is a useful pain
provocation test for diagnosing patellar
tendinopathy [37], and when combined with pain
location [12], can be useful to differentiate it
from other conditions of the anterior knee. High
levels of pain will be experienced early in range,
and this can be used to assess the degree of
tendon irritability. The knee flexion angle when
pain is first experienced should be recorded, and
this can be used as an outcome measure
throughout rehabilitation [38].
5
Differential Diagnosis
Numerous conditions can cause anterior knee
pain, and it can be a diagnostic challenge to
distinguish between several pain-producing
structures (Table 3). These structures include
the patellofemoral joint, fat pad, bursae, or plica.
Patellofemoral Pain Syndrome
The patellofemoral joint is a common source of
anterior knee pain [39]. It is primarily a diagnosis
of exclusion, as there are no sensitive or specific
clinical tests to confirm the diagnosis [39].
Patellofemoral joint pain can be diffusely located
around the patella including inferiorly over the
tendon and is aggravated by tasks requiring
weight-bearing knee flexion, such as running,
squatting and stair-climbing [39]. In contrast to
those with patellar tendinopathy, individuals with
212
R. Kennedy and J. Cook
Fig. 1 Decline board squat
Table 3 Differential diagnosis
Differential diagnosis for patellar tendinopathy
Differential diagnosis
Defining characteristics
Patellofemoral joint pain
– Diffuse anterior knee pain
– Aggravated by weight-bearing knee flexion
Quadriceps tendinopathy
– Located superior/superolateral to the patella
– Older athlete
– Aggravated by deep knee flexion tasks such as squatting
Distal patellar tendinopathy (OsgoodSchlatter disease)
– Younger athlete (10–15)
– Localised pain and swelling around the tibial tuberosity
Fat pad syndrome
– Often initiated by knee hyperextension injury
– Aggravated by end of range knee extension
– Hoffa’s fat pad tender to palpate
Pre/infrapatellar bursitis
– Superficial swelling anterior aspect of the knee
– Pre-patellar bursitis often initiated by direct trauma to the anterior
knee or repetitive kneeling
Plica
– Sharp pain and snapping sensation around the superior aspect of the
patellar
– Thickened band may be palpable medial to the patellofemoral joint
patellofemoral joint pain often demonstrate
poorer hip control and greater knee flexion with
hopping tasks [40] and will have lower levels of
pain deeper into range with the decline squat test
[38]. Taping may reduce patellofemoral joint
pain during provocative manoeuvres such as the
squat or lunge. The diamond taping method
(Fig. 2) can be used clinically to assist in differentiating patellofemoral joint pain from
patellar tendinopathy. Pain during provocative
movements should significantly decrease with
the use of tape in cases of patellofemoral joint
pain, whereas patellar tendon pain remains largely unchanged.
Fat Pad Syndrome
Hoffa’s fat pad can become painful and swollen
following an acute traumatic hyperextension
injury to the knee or after repetitive, end of range
knee extension [41]. Pain is diffusely located
around the anterior to inferior aspect of the knee
and is aggravated by knee hypertension or direct
palpation of the fat pad [41].
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
213
Fig. 2 Patellofemoral joint
diamond taping
Pre-and Infra-patellar Bursitis
Pre-patellar bursitis is typically characterised by
superficial swelling at the anterior aspect of the
knee [42]. It is aggravated by direct trauma, or by
kneeling for extended periods. Although
uncommon, infective bursitis can occur if a
wound is present, and this requires immediate
medical management [42].
Infra-patellar bursitis is less common and is
located at the tibial insertion of the patellar tendon
and can be associated with tendon pathology at this
insertion. Pain is typically more variable in both
nature and location when compared with patellar
tendinopathy. Imaging may be of assistance if
history and clinical examination are equivocal.
Plica
Although it more closely mimics quadriceps
tendinopathy, synovial plica may cause sharp
pain and a snapping sensation around the superior aspect of the patella [43]. A tender, thickened
band may be palpable around the medial aspect
of the patellofemoral joint [43]. MRI can assist in
the differentiation between quadriceps or patellar
tendinopathy and a synovial plica irritation [3].
Quadriceps Tendinopathy
Quadriceps tendinopathy is characterised by pain
at the superior/superolateral aspect of the patella
[44]. Comparatively few studies have investigated quadriceps tendinopathy, perhaps due to
relatively low prevalence rates, which are
estimated to be between 0.2 and 2% in athletic
populations [44]. This condition is often aggravated by a deep squat, where the tendon becomes
compressed against the femoral condyle [44].
The combination of the tendon being used like a
spring from a position of compression is most
provocative, such as at the bottom of a squat
during weightlifting movements. As quadriceps
tendon pathology is a load accumulation condition, quadriceps tendinopathy is more common
in older athletes, particularly those involved in
sports such as weightlifting that require deep
squatting, or if the athlete uses a deep knee
flexion strategy when decelerating or changing
direction [44]. It is managed in a similar manner
to patellar tendinopathy, with the avoidance of
deep knee flexion in the early stages of rehabilitation until the tendon is tolerant of these loads.
Distal Patellar Tendinopathy
In younger athletes (typically aged between 10 and
15), repetitive and excessive traction at the distal
attachment between the patellar tendon and the
tibial tuberosity can result in Osgood-Schlatter
disease [45]. This is characterised by localised pain
and swelling around the tibial tuberosity and
changes in the tendon and bone can persist into
adulthood [45]. These changes predispose the
individual to tendinopathy in adulthood. The
management is like that of all tendinopathies, with
load management and strengthening exercises
forming the cornerstones of management.
214
6
R. Kennedy and J. Cook
Outcome Measures
The Victorian Institute of Sport Assessment scale
for the patellar tendon (VISA-P) is a validated
outcome measure that can be used to assess
severity of symptoms and monitor outcomes
[46]. The VISA-P is scored out of 100, with
higher scores representing better function and
less pain. The minimum clinically important
difference is 13-points [46]. It is best used at
monthly intervals as it is less sensitive to small
changes in clinical presentation. It is recommended to be used in conjunction with a daily
24 h response test, such as the decline squat, to
evaluate shorter-term changes in pain and function, and to determine tolerance to rehabilitation.
The 24 h response test should be completed at a
similar time each day, and the amount of pain
recorded using a numerical pain rating scale.
This can be used to assess the effect of activity on
the tendon from the previous day.
7
Role of Imaging
Patellar tendinopathy is a principally a clinical
diagnosis, and imaging is not required to confirm
the diagnosis. While imaging can provide clinically useful information it is mostly unnecessary
and potentially harmful. Imaging has the potential to identify clinically unimportant incidental
findings that may lead to unnecessary escalation
of treatment. Additionally, appropriate communication of imaging findings is crucial, as the use
of more medicalised terminology to describe
imaging findings is associated with increased
anxiety and perceived severity, and may lead to a
preference for more invasive treatments [47].
Therefore, it is important to be discerning as to
when to request imaging and to understand its
potential benefits and limitations.
Both ultrasound and MRI can show focal
patellar tendon abnormalities. However, there is
a high prevalence of tendon pathology on
imaging, and there is little association between
this pathology and reduced function or pain [8].
Tendon abnormality on imaging does not
confirm that pain and dysfunction are generated
by the tendon, however, a pristine tendon on
imaging may exclude it as a potential source of
pain [8]. Additionally, as degenerative pathological changes are likely irreversible, the serial
imaging of tendons is not recommended, as
pathology is unlikely to change despite changes
in functionality and pain [17]. With these limitations in mind, imaging should not be used to
confirm a patellar tendinopathy diagnosis or to
monitor improvement, but rather used to rule out
coexisting pathology or provide an alternate
diagnosis.
8
Management
Exercise and load management form the cornerstones of patellar tendinopathy management.
A four-stage, progressive tendon-loading exercise program is proposed (Table 4), with the aims
of developing load tolerance of the tendon itself,
the musculoskeletal unit, and the rest of the
kinetic chain. This approach has been shown to
be more effective than traditional eccentric
exercise protocols [48], and involves progression
through isometric, heavy slow resistance, energy
storage and sport-specific exercises.
Isometric exercises are indicated to reduce
tendon pain, improve the mechanical stiffness of
the tendon and to commence loading of the
musculotendinous unit when pain limits the
ability to complete isotonic exercises [3]. They
are stage 1 of the four-stage program when
required for these purposes. Research has shown
that isometric exercise of the quadriceps can
result in pain-relief and a reduction in cortical
inhibition in individuals with patellar
tendinopathy [28], and can also improve the
mechanical properties of the tendon by increasing tendon stiffness [49]. It is preferable that this
is completed single leg, using a leg extension
machine in mid-range (60° knee flexion) (Fig. 3).
However, if equipment is not available, the
Spanish squat exercise has also been shown to be
effective (Fig. 4) [50]. The most evidence exists
for a 5 45 s protocol at 70% of maximal
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
215
Table 4 Four-stage progressive loading program
Isometrics
– Isometrics on leg extension machine, 5 45 secs at 70% MVIC with 2 min recovery
– Spanish squat 5 30-secs if equipment not available
Heavy slow resistance
–
–
–
–
Functional endurance
– Walking lunges
– Stair climbing on toes
Energy storage
– Stair running
– Jump into lunge
– Split squats
Sport-specific
– Deceleration
– Jumping
– Change of direction drills
Fig. 3 Single leg knee
extension
Fig. 4 Spanish squat
Leg extension
Leg press
Seated calf raise
Standing calf raise
216
voluntary isometric contraction (MVIC), with 2min rest between repetitions to allow for muscle
and cortical recovery [28]. The aim of this stage
of the 4-stage program is to provide sufficient
pain-relief for the individual to commence heavy,
slow resistance exercises. Therefore, this stage of
the program is the shortest in duration, and rarely
completed in isolation. Isometrics should be used
to gain control of pain, reduce cortical inhibition,
and to allow the individual to commence their
strength program.
The second stage of the program involves
heavy slow resistance exercises and should be
commenced as soon as feasible. What constitutes
a ‘heavy’ load is highly individual, however, as
most people with patellar tendinopathy are
young, athletic men, it is likely that sufficient
loading will require weighted, gym-based exercises. It is crucial that exercises are completed
single leg, and that each muscle and leg is loaded
maximally and independently, so deficits are not
hidden within the kinetic chain. Exercises should
be completed on both sides, as the strength of the
affected side can be enhanced by improvements
of the unaffected side, a phenomenon known as
cross education [51, 52]. Loads for each side may
differ initially, with the aim of achieving symmetry by the end of rehabilitation. It is important
to target the affected musculotendinous unit in
isolation initially, before introducing exercises to
incorporate the rest of the kinetic chain. Exercises should be completed slowly, and the use of
Fig. 5 Single leg press
R. Kennedy and J. Cook
a metronome to externally pace exercises may
assist in modulating excitatory and inhibitory
control of the muscle [53]. The key exercises
during this phase include the leg extension, leg
press (Fig. 5), seated and standing and seated
calf raises (Figs. 6 and 7), all completed single
leg. Calf strengthening is an essential and often
overlooked component of this phase of rehabilitation. The soleus muscle is a key contributor
during both deceleration and change of direction
manoeuvres, as it decelerates the tibia and
attenuates load through the anterior knee, while
gastrocnemius is important for both jumping and
sprinting. As all these movements are provocative for patellar tendinopathy, targeted strengthening of both gastrocnemius and soleus is
crucial. These exercises should be commenced at
plantar-grade, and dorsiflexion range can be
increased as strength improves. Sessions during
this phase are ideally completed 2–3 times per
week on non-consecutive days. Once a strength
base has been established, a functional endurance
program including exercises such as stair
climbing or walking lunges can be commenced.
The third phase of rehabilitation involves the
re-introduction of energy storage and release
loads in the patellar tendon. This is the first time
the tendon is exposed to provocative load during
rehabilitation. The rate of loading is increased,
using exercises such as low-level skipping,
jumping, hopping and deceleration (Figs. 8, 9
and 10). These exercises should be completed
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
217
Fig. 6 Single leg seated calf
raise
with bodyweight loads only, as increasing the
rate of loading increases the load on the tendon
substantially. If possible, energy storage should
be introduced prior to energy storage and release.
Exercises should be completed every 2–3 days,
as it can take up to 72 h for tendon structure to
return to baseline following a loading bout [54].
Weighted, gym-based exercises from phase two
are continued concurrently throughout this stage.
Symptoms should be carefully monitored with a
24 h load response test such as the decline squat
the next morning, to determine if the tendon has
tolerated the increase in load. If pain remains low
and stable, these drills can be progressed in
quantity and intensity.
The final phase of rehabilitation is characterised by the gradual re-introduction to sport
specific drills. This phase is highly specific and
depends on the chosen sport of the athlete. Stage
three drills are ceased during this phase and
replaced by more sport specific drills, to avoid
overload of the tendon. Specific, gym-based
strength exercises as per phase two must be
maintained twice per week. High patellar tendon
load activities such as jumping, deceleration and
change of direction must be carefully quantified
and graduated throughout the training block.
Return to play may be considered when the
athlete can sustain repeated high patellar tendon
load activities without an increase in symptoms
the following day.
9
In-Season Rehabilitation
Depending on the severity of symptoms, some
athletes may be able to continue to train and play
whilst managing patellar tendinopathy. As
improving and maintaining strength are the
cornerstones of patellar tendinopathy management, a gym program must be maintained
throughout the season. The removal of some
provocative loads during training such as agility
drills may be required to control symptoms. It
may be necessary to limit training to three times
per week during this stage. Isometrics may be
used prior to training and games for analgesia
and to reduce cortical inhibition. Adjunct treatments may be considered if they allow the athlete
to load the tendon, however, treatments that
directly target tendon pathology are generally
invasive and are discouraged.
10
Adjuncts
Various adjunct treatments for patellar
tendinopathy have been investigated. Extracorporeal shockwave therapy (ESWT) has been
shown to provide no additional benefit over
placebo for the in-season management of jumping athletes with patellar tendinopathy [55].
A further randomised controlled trial compared
218
Fig. 7 Single leg standing
calf raise
R. Kennedy and J. Cook
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
Fig. 8 Skipping
Fig. 9 Jumping
Fig. 10 Hopping
219
220
the use of focused or radial shockwave therapy,
found no significant difference between groups
[56]. Interestingly, both of these groups
improved significantly, but it was concluded that
this change was unlikely to be clinically worthwhile [56]. The addition of ESWT to an eccentric
exercise program has also been studied, finding
no additional benefit compared to eccentric
exercise alone [57].
The use of a patellar strap or sports tape has
also been investigated. Both patellar taping and a
patellar strap have been found to decrease pain in
the short term, however neither method was more
effective than a placebo taping method [58].
Various injection therapies have been proposed to be of benefit in patellar tendinopathy.
A systematic review of injection therapies found
that a steroid injection decreased pain in the
short-term, however symptoms relapsed at
longer-term follow-up [59]. Various other injection therapies have also been studied, but insufficient evidence was available to determine
superiority of one over the other, or over placebo
treatment [59]. As adjunct treatments do not
address muscle, tendon, or kinetic chain dysfunction, it is not recommended that they are
used in isolation. They may be considered in
cases when the use of an adjunct treatment
enables the athlete to complete their rehabilitation program and there is no evidence of potential harm.
Surgery for resistant patellar tendinopathy
may be considered if pain persistently disrupts
training and playing and when adequate conservative rehabilitation has failed. Traditional surgical treatment for patellar tendinopathy involves
open patellar tenotomy and excision of the
pathological region [60], and is associated with a
prolonged recovery period and poorer outcomes
[61]. Surgical techniques that remain external to
the tendon, such as arthroscopic shaving, are
recommended over more invasive procedures.
Surgery is performed under ultrasound guidance
on the region of neovascular ingrowth on the
dorsal aspect of the tendon, adjacent to the
pathological region, with minor resection of
Hoffa’s fat pad [60]. Disruption of the fat pad-
R. Kennedy and J. Cook
tendon interface and the anterior peritendon
decreases nociception, and may enable an earlier
return to sport [60]. Rehabilitation after surgery
involves immediate weight-bearing, followed by
a structured rehabilitation period, with return to
play in 2–4 months [60].
11
Prevention
Many of the same principles apply for both the
prevention and management of patellar
tendinopathy. These principles include appropriate load management, the maintenance of
sufficient strength and addressing individual risk
and associated factors as required.
Appropriate load monitoring and management
is essential, as large fluctuations in load can be
provocative for the tendon especially in those
with a history of patellar tendinopathy. It is
particularly important to be cognisant of high
patellar tendon load activities such as jumping,
deceleration and change of direction, and to
monitor the volume of these activities. Recent
decreases and subsequent increases in training
load due to other injuries is also relevant, especially in the case of injuries that affect ankle
dorsiflexion range and calf strength such as
inversion ankle sprains, as this can increase
patellar tendon load.
The maintenance of strength, particularly of
the knee extensors and calf complex is crucial.
A formal gym program targeting these muscle
groups should be completed at least twice weekly
as a key preventative strategy for athletes competing in sports requiring high patellar tendon
load. This program should consist of single leg
press, single leg extension, seated and standing
single leg calf raises.
Pre-season screening for patellar tendinopathy
risk and associated factors may assist in preventing the development of symptoms throughout the season. Screening for previous selfreported patellar tendon pain is a stronger predictor of in-season tendinopathy than ultrasound
imaging findings [21], and this information may
be used to inform individualised training
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
program design with the aim of addressing any
relevant deficits or factors, such as lack of
dorsiflexion range.
Finally, it is important to act early if the tendon becomes symptomatic. The early signs of
tendinopathy are often ignored, due to the warmup phenomenon and the fact that many athletes
can often continue to train and play in the early
stages of tendinopathy. Addressing load early
often prevents the sequelae of pain and disability
associated with severe patellar tendinopathy.
12
Take Home Messages
1. Patellar tendinopathy is characterised by
localised pain at the inferior pole of the
patella, which increases in a dose-dependent
manner with increasing demand on the knee
extensors.
2. Patellar tendinopathy presents a significant
diagnostic challenge, with much clinical
overlap with other conditions of the anterior
knee. It is critical to determine the exact
location of pain during pain provocation tests
to increase diagnostic accuracy.
3. The relationship between patellar tendon
pathology and pain is limited. The prevalence
of imaging abnormalities in sporting populations is high, and these abnormalities are not
always associated with pain or loss of function.
4. Patellar tendinopathy is a clinical diagnosis,
imaging is not required to make the diagnosis.
Imaging can be of assistance when ruling out
co-existing pathology or an alternate diagnosis, but clinicians should be discerning as to
its use.
5. While load is essential to maintain tendon
structure and capacity, excess load is linked
to pathology and pain. The development of
patellar tendon symptoms is preceded by a
change in loading patterns, usually an
increase in tensile load being transmitted
through the patellar tendon.
6. Exercise and load management are the
cornerstones of patellar tendinopathy management. A four-stage, tendon-loading
221
exercise program has been shown to be
more effective than traditional eccentric
loading protocols.
13
Key Message
– It is crucial to distinguish patellar tendinopathy from other common conditions of the
anterior knee. Patellar tendinopathy is found
almost exclusively in young, athletic men
participating in sports that place significant
demands on the knee extensors. Pain is localised to the inferior pole of the patellar and
does not move or spread. Pain increases in a
dose-dependent manner with increasing tensile load being transmitted by the patellar
tendon. Diagnosis can be difficult due to significant clinical overlap with other anterior
knee conditions, but the combination of pain
location and the use of common pain provocation tests may assist with the clinical reasoning process. A four-stage tendon loading
exercise program is recommended for management, with the aim of increasing the load
tolerance of the tendon itself, musculotendinous unit, and the rest of the kinetic chain.
References
1. Scott A, Squier K, Alfredson H, Bahr R, Cook JL,
Coombes B, et al. Icon 2019: international scientific
tendinopathy symposium consensus: clinical terminology. Br J Sports Med. 2020;54(5):260–2.
2. Lian ØB, Engebretsen L, Bahr R. Prevalence of
jumper’s knee among elite athletes from different
sports: a cross-sectional study. Am J Sports Med.
2005;33(4):561–7.
3. Malliaras P, Cook J, Purdam C, Rio E. Patellar
tendinopathy: clinical diagnosis, load management, and
advice for challenging case presentations. J Orthopaedic
Sports Phys Therapy. 2015;45(11):887–98.
4. Cook J, Khan K, Harcourt P, Grant M, Young D,
Bonar S. A cross sectional study of 100 athletes with
jumper’s knee managed conservatively and surgically. The Victorian Institute of Sport Tendon Study
Group. Br J Sports Med. 1997;31(4):332–6.
5. Kettunen JA, Kvist M, Alanen E, Kujala UM. Longterm prognosis for Jumper’s knee in male athletes:
prospective follow-up study. Am J Sports Med.
2002;30(5):689–92.
222
6. Zwerver J, Bredeweg SW, van den Akker-Scheek I.
Prevalence of Jumper’s knee among nonelite athletes
from different sports: a cross-sectional survey. Am J
Sports Med. 2011;39(9):1984–8.
7. Drakos MC, Domb B, Starkey C, Callahan L,
Allen AA. Injury in the National Basketball Association: a 17-year overview. Sports Health. 2010;2
(4):284–90.
8. Docking SI, Ooi CC, Connell D. Tendinopathy: is
imaging telling us the entire story? J Orthopaedic
Sports Phys Therapy. 2015;45(11):842–52.
9. van der Heijden RA, De Kanter JL, Bierma-Zeinstra
SM, Verhaar JA, van Veldhoven PL, Krestin GP,
et al. Structural abnormalities on magnetic resonance
imaging in patients with patellofemoral pain: a crosssectional case-control study. Am J Sports Med.
2016;44(9):2339–46.
10. Esculier J-F, Bouyer LJ, Dubois B, Leblond J,
Brisson M, Chau L, et al. Predictors of clinical
success in runners with patellofemoral pain: secondary analyses of a randomized clinical trial. J Sci
Med Sport. 2018;21(8):777–82.
11. Rio E, Girdwood M, Thomas J, Garofalo C, Fortington LV, Docking S. Pain mapping of the anterior
knee: injured athletes know best. Scand J Pain.
2018;18(3):409–16.
12. Hannington M, Docking S, Cook J, Edwards S,
Rio E. Self-reported jumpers’ knee is common in
elite basketball athletes–but is it all patellar
tendinopathy? Phys Therapy Sport. 2020;43:58–64.
13. Alexander RM. Energy-saving mechanisms in walking and running. J Exp Biol. 1991;160(1):55–69.
14. Kujala UM, Sarna S, Kaprio J. Cumulative incidence
of achilles tendon rupture and tendinopathy in male
former elite athletes. Clin J Sport Med. 2005;15
(3):133–5.
15. Cook J, Rio E, Purdam C, Docking S. Revisiting the
continuum model of tendon pathology: what is its
merit in clinical practice and research? Br J Sports
Med. 2016;50(19):1187–91.
16. Cook J, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical
presentation of load-induced tendinopathy. Br J
Sports Med. 2009;43(6):409–16.
17. Docking S, Rosengarten S, Daffy J, Cook J. Treat the
donut, not the hole: the pathological Achilles and
patellar tendon has sufficient amounts normal tendon
structure. J Sci Med Sport. 2014;18: e2.
18. Comin J, Cook JL, Malliaras P, McCormack M,
Calleja M, Clarke A, et al. The prevalence and clinical
significance of sonographic tendon abnormalities in
asymptomatic ballet dancers: a 24-month longitudinal
study. Br J Sports Med. 2013;47(2):89–92.
19. Fredberg U, Bolvig L. Significance of ultrasonographically detected asymptomatic tendinosis in the
patellar and achilles tendons of elite soccer players: a
longitudinal study. Am J Sports Med. 2002;30
(4):488–91.
20. Rudavsky A, Cook J, Docking S. Quantifying
proximal patellar tendon changes during adolescence
R. Kennedy and J. Cook
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
in elite ballet dancers, a 2-year study. Scand J Med
Sci Sports. 2018;28(11):2369–74.
Docking SI, Rio E, Cook J, Carey D, Fortington L.
Quantification of Achilles and patellar tendon structure on imaging does not enhance ability to predict
self-reported symptoms beyond grey-scale ultrasound and previous history. J Sci Med Sport.
2019;22(2):145–50.
Rio E, Moseley L, Purdam C, Samiric T, Kidgell D,
Pearce AJ, et al. The pain of tendinopathy: physiological or pathophysiological? Sports Med. 2014;44
(1):9–23.
Docking SI, Rio E, Cook J, Orchard J, Fortington LV.
The prevalence of Achilles and patellar tendon
injuries in Australian football players beyond a
time-loss definition. Scand J Med Sci Sports.
2018;28(9):2016–22.
Cook J, Khan K, Kiss Z, Griffiths L. Patellar
tendinopathy in junior basketball players: a controlled clinical and ultrasonographic study of 268
patellar tendons in players aged 14–18 years. Scand J
Med Sci Sports. 2000;10(4):216–20.
Gisslén K, Gyulai C, Nordström P, Alfredson H.
Normal clinical and ultrasound findings indicate a
low risk to sustain jumper’s knee patellar tendinopathy: a longitudinal study on Swedish elite junior
volleyball players. Br J Sports Med. 2007;41
(4):253–8.
Ducher G, Cook J, Spurrier D, Coombs P,
Ptasznik R, Black J, et al. Ultrasound imaging of
the patellar tendon attachment to the tibia during
puberty: a 12-month follow-up in tennis players.
Scand J Med Sci Sports. 2010;20(1):e35–40.
Maffulli N, Longo UG, Spiezia F, Denaro V. Sports
injuries in young athletes: long-term outcome and
prevention strategies. Phys Sports Med. 2010;38
(2):29–34.
Rio E, Kidgell D, Purdam C, Gaida J, Moseley GL,
Pearce AJ, et al. Isometric exercise induces analgesia
and reduces inhibition in patellar tendinopathy. Br J
Sports Med. 2015;49(19):1277–83.
Malliaras P, Cook JL, Kent P. Reduced ankle
dorsiflexion range may increase the risk of patellar
tendon injury among volleyball players. J Sci Med
Sport. 2006;9(4):304–9.
Kaufman KR, Brodine SK, Shaffer RA, Johnson CW,
Cullison TR. The effect of foot structure and range of
motion on musculoskeletal overuse injuries. Am J
Sports Med. 1999;27(5):585–93.
Hägglund M, Zwerver J, Ekstrand J. Epidemiology
of patellar tendinopathy in elite male soccer players.
Am J Sports Med. 2011;39(9):1906–11.
Bahr MA, Bahr R. Jump frequency may contribute to
risk of jumper’s knee: a study of interindividual and
sex differences in a total of 11 943 jumps video
recorded during training and matches in young elite
volleyball players. Br J Sports Med. 2014;48
(17):1322–6.
Janssen I, Brown N, Munro BJ, Steele JR. Variations
in jump height explain the between-sex difference in
Patellar Tendinopathy: Risk Factors, Prevention, and Treatment
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
patellar tendon loading during landing. Scand J Med
Sci Sports. 2015;25(2):265–72.
Visnes H, Aandahl HÅ, Bahr R. Jumper’s knee
paradox—jumping ability is a risk factor for developing jumper’s knee: a 5-year prospective study. Br J
Sports Med. 2013;47(8):503–7.
Janssen I, Steele JR, Munro BJ, Brown NAT.
Previously identified patellar tendinopathy risk factors differ between elite and sub-elite volleyball
players. Scand J Med Sci Sports. 2015;25(3):308–14.
Cook JL, Khan K, Kiss ZS, Purdam CR, Griffiths L.
Reproducibility and clinical utility of tendon palpation to detect patellar tendinopathy in young basketball players. Br J Sports Med. 2001;35(1):65–9.
Purdam CR, Cook JL, Hopper DM, Khan KM,
Group VTS. Discriminative ability of functional
loading tests for adolescent jumper’s knee. Phys
Therapy Sport. 2003;4(1):3–9.
Zwerver J, Bredeweg SW, Hof AL. Biomechanical
analysis of the single-leg decline squat. Br J Sports
Med. 2007;41(4):264–8.
Crossley KM, van Middelkoop M, Barton CJ, Culvenor AG. Rethinking patellofemoral pain: prevention, management and long-term consequences. Best
Pract Res Clin Rheumatol. 2019;33(1):48–65.
Barton CJ, Levinger P, Menz HB, Webster KE.
Kinematic gait characteristics associated with patellofemoral pain syndrome: a systematic review. Gait
Posture. 2009;30(4):405–16.
Dragoo JL, Johnson C, McConnell J. Evaluation and
treatment of disorders of the infrapatellar fat pad.
Sports Med. 2012;42(1):51–67.
Baumbach SF, Lobo CM, Badyine I, Mutschler W,
Kanz K-G. Prepatellar and olecranon bursitis: literature review and development of a treatment algorithm. Arch Orthopaedic Trauma Surg. 2014;134
(3):359–70.
Schindler OS. ‘The Sneaky Plica’revisited: morphology, pathophysiology and treatment of synovial
plicae of the knee. Knee Surg Sports Traumatol
Arthrosc. 2014;22(2):247–62.
Sprague A, Epsley S, Silbernagel KG. Distinguishing
quadriceps tendinopathy and patellar tendinopathy:
Semantics or significant? J Orthopaedic Sports Phys
Therapy. 2019;49(9):627–30.
Circi E, Atalay Y, Beyzadeoglu T. Treatment of
Osgood-Schlatter disease: review of the literature.
Musculoskeletal Surg. 2017;101(3):195–200.
Hernandez-Sanchez S, Hidalgo MD, Gomez A.
Responsiveness of the VISA-P scale for patellar
tendinopathy in athletes. Br J Sports Med. 2014;48
(6):453–7.
Nickel B, Barratt A, Copp T, Moynihan R, McCaffery K. Words do matter: a systematic review on how
different terminology for the same condition influences management preferences. BMJ Open. 2017;7
(7): e014129.
Breda SJ, Oei EH, Zwerver J, Visser E, Waarsing E,
Krestin GP, et al. Effectiveness of progressive
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
223
tendon-loading exercise therapy in patients with
patellar tendinopathy: a randomised clinical trial.
Br J Sports Med. 2021;55(9):501–9.
Kubo K, Ishigaki T, Ikebukuro T. Effects of plyometric and isometric training on muscle and tendon
stiffness in vivo. Physiol Rep. 2017;5(15): e13374.
Rio E, Purdam C, Girdwood M, Cook J. Isometric
exercise to reduce pain in patellar tendinopathy inseason: is it effective “on the Road”? Clin J Sport
Med. 2019;29(3):188–92.
Green LA, Gabriel DA. The cross education of
strength and skill following unilateral strength training in the upper and lower limbs. J Neurophysiol.
2018;120(2):468–79.
Lee M, Carroll TJ. Cross education. Sports Med.
2007;37(1):1–14.
Rio E, Kidgell D, Moseley GL, Gaida J, Docking S,
Purdam C, et al. Tendon neuroplastic training: changing
the way we think about tendon rehabilitation: a narrative
review. Br J Sports Med. 2016;50(4):209–15.
Rosengarten SD, Cook JL, Bryant AL, Cordy JT,
Daffy J, Docking SI. Australian football players’
Achilles tendons respond to game loads within 2
days: an ultrasound tissue characterisation (UTC)
study. Br J Sports Med. 2015;49(3):183–7.
Zwerver J, Hartgens F, Verhagen E, van der Worp H,
van den Akker-Scheek I, Diercks RL. No effect of
extracorporeal shockwave therapy on patellar
tendinopathy in jumping athletes during the competitive season: a randomized clinical trial. Am J Sports
Med. 2011;39(6):1191–9.
van der Worp H, Zwerver J, Hamstra M, van den
Akker-Scheek I, Diercks RL. No difference in
effectiveness between focused and radial shockwave
therapy for treating patellar tendinopathy: a randomized controlled trial. Knee Surg Sports Traumatol
Arthrosc. 2014;22(9):2026–32.
van Leeuwen MT, Zwerver J, van den Akker-Scheek
I. Extracorporeal shockwave therapy for patellar
tendinopathy: a review of the literature. Br J Sports
Med. 2009;43(3):163–8.
de Vries A, Zwerver J, Diercks R, Tak I, van
Berkel S, van Cingel R, et al. Effect of patellar strap
and sports tape on pain in patellar tendinopathy: a
randomized controlled trial. Scand J Med Sci Sports.
2016;26(10):1217–24.
van Ark M, Zwerver J, van den Akker-Scheek I.
Injection treatments for patellar tendinopathy. Br J
Sports Med. 2011;45(13):1068–76.
Willberg L, Sunding K, Forssblad M, Fahlström M,
Alfredson H. Sclerosing polidocanol injections or
arthroscopic shaving to treat patellar tendinopathy/
jumper’s knee? A randomised controlled study. Br J
Sports Med. 2011;45(5):411–5.
Bahr R, Fossan B, Løken S, Engebretsen L. Surgical
treatment compared with eccentric training for patellar tendinopathy (jumper’s knee): a randomized,
controlled trial. JBJS. 2006;88(8):1689–98.
Pathophysiology of Patellar
Instability
William R. Post
Effective and rational treatment depends upon a
clear understanding of all the factors that go into
patellofemoral instability. How can you solve a
problem without understanding the contributing
factors? Some of these will be able to be modified surgically. Some cannot and depend on
muscle strength and control. Some pertinent
morphological features such as rotational deformities and trochlear dysplasia are well known to
be familial [1, 2].
Before we can meaningfully discuss the
pathophysiology of patellofemoral instability, we
must clearly define our understanding of patellofemoral stability.
Patellofemoral stability has previously been
defined as “constraint by passive soft tissue
tethers and chondral/bony geometry that, together with muscular forces, guide the patella into
the trochlear groove and keep it engaged within
the trochlear groove as the knee flexes and
extends” [3].
Let us first consider each of these factors
separately
There are important soft tissue constraints on
both the medial and lateral aspect of the patella.
The anatomy and function of these structures has
W. R. Post (&)
Mountaineer Orthopedic Specialists, LLC,
Morgantown, WV, USA
e-mail: wpost@wvortho.com
been well defined in multiple publications [4–8].
The medial patellar restraints include the medial
patellofemoral ligament which is a very important structure extending from the medial femoral
condyle to the upper third of the medial border of
the patella. Although medial patellofemoral
ligament reconstruction is commonly discussed
as the treatment for patellar instability one must
realize that the medial patellofemoral ligament
complex includes much more than just the
medial patellofemoral ligament alone. There is a
proximal extension of the medial patellofemoral
retinaculum into the distal quadriceps tendon and
the more distal portions of the medial patellofemoral complex include the medial patellotibial
and patellomeniscal ligaments [5]. The more
proximal portions of the medial soft tissue constraints have more influence on patellar constraint early in knee flexion while the more distal
portions of the medial soft tissue constraints exert
more of their influence when the knee is in
greater flexion [4]. As our understanding of the
specific characteristics of each of these portions
of the medial soft tissues expands, we must take
this into consideration as we refine our understanding of patellofemoral stability.
Not only do the medial soft tissues contribute
to constraint of the patella but the lateral soft
tissues also play a key role. The lateral tissues
certainly restrain the patella from displacement in
the medial direction but they also contribute to
preventing lateral displacement of the patella
with respect to the trochlea. This has been
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_15
225
226
W. R. Post
demonstrated in the laboratory [9] and also is
evident in clinical results reported for lateral
release which can exacerbate lateral instability in
certain clinical situations [10–12]. When considering the true effects of the medial and lateral
soft tissue restraints, it is important to realize that
there is a very significant posterior component to
the anatomical position (Fig. 1A).
The articular shape of the patella and the
trochlea also have a strong influence on stability.
The deeper the concavity of the trochlea is, the
more stable the patellofemoral articulation will
be. This is especially true in the proximal portion
of the trochlea where the patella enters the trochlea in early flexion. If the proximal portion of
the trochlea is flat or even convex it is more
difficult for the patella to be well-contained
within the trochlea. In this regard it is important
to consider not only how flat the proximal portion of the trochlea is but to evaluate at which
degree of flexion the distal patella begins to enter
he proximal (hopefully concave) portion of the
trochlea. Once the patella has entered the concave trochlea weightbearing and quadriceps force
Fig. 1 A Note the prominent
posterior vector associated
with both the medial and
lateral soft tissue constraints
(yellow arrows). B In the knee
with normal alignment and
anatomy the compression
resulting from weightbearing
and quadriceps force
increases patellar stability (red
arrow)
A
increase patellar stability (Fig. 1B). We must
consider how far proximally the trochlea itself
extends on the distal femur and also the relative
height of the patella itself when we consider at
which degree of flexion engagement of the
patella within the trochlea begins [13]. This is an
important source of variability among patients.
Neither patella alta itself, nor trochlear morphology should be logically considered separately considering that the critical issue is the
interaction and stability of the patella and the
trochlea in early flexion.
Axial and coronal plane skeletal alignment
also play crucial roles in patellofemoral biomechanics. For example the lower extremity with a
significant valgus alignment at the knee increases
the lateral vector of quadriceps force, causing
lateral displacement of the patella unless it is
appropriately controlled by soft tissue constraints
and the articular shape and alignment of the
patellofemoral articulation (Fig. 2). One factor
that can contribute to increasing the valgus angle
and resultant lateral vector of quadriceps force is
an abnormally lateral position of the tibial
Pathophysiology of Patellar Instability
Fig. 1 (continued)
227
B
tuberosity. It is for this reason historically that
medial tuberosity transfer has been proposed
when the patellar tendon insertion at the tibial
tuberosity can be proven to be abnormally lateral.
This is most commonly considered clinically
when the excessive lateral quadriceps vector is
severe enough to result in lateral translation of
the patella on axial imaging studies. There are
several methods of measuring this clinically by
comparing the axial position of the tibial
tuberosity to either the center of the trochlear
groove (TT-TG distance) or the PCL insertion
site (TT-PCL distance). Most commonly the
depth of the trochlea is the reference point,
although it still remains uncertain which measurement is more clinically reproducible and
important [14].
Similarly rotational alignment of the extremity
plays a critical role in positioning the trochlea
underneath the patella [15]. Excessive internal
rotation of the femur relative to the patella
essentially moves the trochlea anteromedially
away from the patella (Fig. 3). Excessive internal
rotation of the femur can result from excessive
femoral anteversion as well as relative weakness
of the hip external rotators producing dynamic
valgus. Since as a profession we have typically
discussed patellofemoral tracking as keeping the
patella over the trochlea we might misunderstand
this very important point. Sometimes it is just as
important or even more important to consider
putting the trochlea back under the patella by
externally rotating the femur. In this case we are
not putting the train back on the track, but rather
putting the track back underneath the train
(Figs. 4A and B). Clinically it is not always
purely one or the other.
Internal rotation of the trochlea away from the
patella can result from bony rotational abnormalities of the femur with excessive femoral
anteversion or from lack of strong hip external
rotation and pelvic stability which can produce
relative dynamic internal rotation of the trochlea
even in the absence of bony abnormality. It is
this dynamic loss of control that is referred to as
a functional valgus knee which can be easily
diagnosed on physical examination. Hyperpronation of the foot can also produce internal
228
Fig. 2 Valgus alignment of the knee resulted in a lateral
vector on the patellofemoral joint (yellow arrow). Relative
contributions to the quadriceps vector come from the
medial and lateral portions of the quadriceps (red arrows).
Constraint to resist this lateral vector must come from
medial and lateral soft tissue constraints (orange arrows)
as well as the medial component of the quadriceps vector
rotation of the lower extremity resulting in the
same unhealthy internal rotation of the trochlea
relative to the patella [16].
W. R. Post
Each of these previous factors can affect the
ability of muscular forces to be a positive influence on patellar stability. The effect of weightbearing and muscular contraction compresses the
patella to the trochlea. Assuming that the patella
has a stable environment by virtue of soft tissue
constraints and articular constraint the compression resulting from muscular and weightbearing
forces increases stability of the joint. The concept
here is identical to that discussed in the glenohumeral joint where concavity compression is a
recognized factor in joint stability [17, 18].
However if the patella is not adequately constrained by soft tissue and/or the articular surfaces muscular and weightbearing forces can
produce instability. For example if the patella is
just starting to enter the trochlea and the trochlea
is nicely concave, a strong contraction even in a
valgus knee will produce compression of the
patella into the groove thus increasing stability
(Fig. 5a). However, if the patella either has not
entered the trochlea by this point due to patella
alta, if the soft tissue constraints are not adequate
to guide the patella into the groove, if the trochlea is internally rotated away from the patella
and/or if the proximal portion of the groove is not
actually concave but rather convex (such as is the
case with severe trochlear dysplasia), muscular
contraction can become part of the problem
instead of part of the solution (Fig. 5b). When
one takes away the concavity there is no
concavity/compression affect.
The practical application of the role of muscle
strength and control is in non-operative treatment
of patellofemoral instability when one must focus
on neuromuscular control of the core and the
entire lower extremity to improve dynamic control of femoral position. Increased quadriceps
strength will improve stability by increasing the
concavity/compression effect. Patellar taping or
bracing may add to patellar constraint and possibly provide helpful proprioceptive feedback.
Now that we have developed an understanding of the factors which contribute to patellofemoral stability, we need to consider exactly what
we mean by patellofemoral instability. The same
authors that defined patellofemoral stability as
Pathophysiology of Patellar Instability
Fig. 3 Internal rotation of
the femur moves the trochlea
posterior medially away from
the patella (white curved
arrow). Such internal rotation
can be from excessive
anteversion of the femoral
neck and/or relative weakness
of the hip external rotators
producing dynamic valgus
Fig. 4 A In a normally
aligned patellofemoral joint
with normal articular
congruity the train is on the
track. B. When there is
pathological bony deformity
causing femoral internal
rotation it makes more sense
to put the track back
underneath the train as
opposed to trying to move the
patella (the train) to the
trochlea (the track). In this
situation femoral osteotomy
should be considered
A
229
230
Fig. 4 (continued)
W. R. Post
B
above define patellofemoral instability as
“symptomatic deficiency of the aforementioned
passive constraint (patholaxity) such that the
patella may escape partially or completely from
its asymptomatic position with respect to the
femoral trochlea under the influence of displacing force. Such displacing force could be generated by muscle tension, movement and/or
externally applied forces” [3].
To think precisely about this problem it is
important to further define several key words.
Laxity when used biomechanically is a word
which refers to passive displacement under load.
As an example an excessively lax medial patellofemoral ligament complex would allow excessive lateral translation under load. This can be
seen in such cases during physical examination
by applying lateral pressure to the patella in
different degrees of flexion. Such a finding can
also be imaged by stress radiography although
this is not widely done [19]. So if the ligament
does not have the physical capacity to adequately
constrain the joint to which it is attached we say
that there is patholaxity of the joint. This can
occur after trauma or may exist in the setting of
hyperlaxity syndromes such as Ehlers-Danlos
syndrome.
Laxity itself should not be confused with
instability. Instability is more properly used to
define a symptom. For example, patients may
lack normal intact soft tissue constraints and be
without actual symptoms of instability. In other
words though the ligaments are lax, other stability factors such as neuromuscular control,
activity level and articular alignment may be
sufficient to allow the patient to remain asymptomatic. In this setting with findings of laxity on
clinical evaluation, it is not appropriate to say
Pathophysiology of Patellar Instability
Fig. 5 A In this CT image in
full extension the posterior
weightbearing and quadriceps
force vector produces
stability. B With trochlear
dysplasia and a convex
proximal trochlea the convex
patella articulates with a
convex trochlea and the
quadriceps vector may
produce instability if
composite forces are even
slightly lateral to the convex
trochlea
A
B
231
232
W. R. Post
that this patient has patellofemoral instability
since instability itself is a symptom and not a
physical finding. Indeed the symptom of patellofemoral instability is most often episodic even
in the presence of severe patholaxity of the soft
tissue constraints.
To summarize, factors which cause displacement of the patella are a combination of muscle
forces, insufficient articular congruency, skeletal
alignment variables, dynamic positioning of the
extremity as well as direct or indirect trauma.
Patellofemoral instability injuries most often
result from non-contact injuries by excessive
internal rotation of the femur relative to the
patella with significant muscular forces causing
lateral displacement resulting in failure of the
medial soft tissue constraints. If underlying laxity
of the soft tissue constraints exists from either
congenital hypermobility or previous injury, less
force is required to produce the pathological
displacement. MRI studies have consistently
shown disruption of the medial soft tissues with
acute dislocation [20].
The key clinical question is to begin to understand which of the variables must be addressed
clinically by surgery or nonoperative management
to assure normal function in the absence of
recurrent instability episodes which can produce
severe articular injury resulting in posttraumatic
osteoarthritis and recurrent disability.
1
Using Pathophysiology
to Understand Different Types
of Patellofemoral Instability
Given our understanding of factors affecting the
pathophysiology of patellar instability, we can
now address different types of patellofemoral
instability. The most common type of patellofemoral instability involves dislocation of the
patella laterally with respect to the trochlea in
early flexion (<45°). This is essentially a failure
of the patella under load to enter the trochlea and
remain in the trochlea as the knee flexes. While
this is far and away the most common type of
patellofemoral instability, it is not the only type.
Clinical studies have consistently revealed trochlear dysplasia, patella alta and increased TTTG distance in patients with lateral instability to
be factors which make recurrent dislocation more
likely [21–23]. As such information evolves,
patient selection for treatment after primary dislocation will become more objective.
Less common types of patellofemoral instability include lateral patellar instability with
flexion. In this situation referred to as obligate
lateral dislocation the patella enters the trochlea
normally but with further flexion suddenly dislocates lateral to the trochlea. This typically
occurs each time the patient goes from full
extension to full flexion. In order to understand
the situation we can apply the same principles
addressed above. In this situation there is
excessive lateral tightness as well as concomitant
relative deficiency of the lateral aspect of the
trochlea. In some cases there may be shortening
of the extensor mechanism exacerbating the lateral tightness and contributing to obligate lateral
dislocation in flexion. Understanding these factors, lateral release with possible lengthening of
the quadriceps mechanism is the mainstay of
such treatment with elevation of the lateral trochlea as an additional component of the repair.
In addition to these 2 types of lateral patellofemoral instability, medial patellar instability
also occurs. This problem is usually iatrogenic
related to prior surgery with excessive lateral
release and sometimes surgical injury to the
vastus lateralis tendon. In this case the root
causes are less than appropriate lateral soft tissue
constraints as well as imbalance of the quadriceps related to the vastus lateralis weakness. One
must also be aware when planning treatment for
medial patellar instability that any pathologic
factors present contributing to the original lateral
instability may still need to be effectively treated.
Restoring medial and lateral soft tissue constraints along with considering possible treatment
of pre-existing issues such as trochlear dysplasia
Pathophysiology of Patellar Instability
or patella alta is a logical approach based on
understanding of pathophysiological principles.
In addition to the 2 types of lateral patellofemoral instability and the usually iatrogenic medial
patellar instability, patients may experience multidirectional instability of the patella. In this setting all the potential factors known to contribute
to patellofemoral instability must again be carefully evaluated. Pathologic laxity may exist and
be either traumatic, iatrogenic, congenital or a
combination of all three. Underlying bony
alignment issues and potential deficiencies of
dynamic control are also common factors in
patients who truly have multidirectional instability. This does not mean that all these factors need
to be addressed by surgery in each patient. Such
patients are highly complex with multifactorial
pathology creating difficult decision making. One
must always carefully balance potential morbidity
of surgical intervention with proven efficacy.
2
Conclusion
A good understanding of the pathophysiology of
patellofemoral instability is essential for any
clinician treating such patients. Such knowledge
must be combined with ongoing clinical research
to treat patients wisely. Careful evaluation of all
known pathophysiological elements is indicated
before surgical decision making. As a profession
we have much to learn about how much surgery
and what surgery is necessary in any given
clinical scenario. Recent consensus suggests
avoiding a cookbook approach of operating on
every identified factor (trochlear dysplasia,
patella alta, pathologic laxity, tibial tuberosity
position, femoral and tibial rotational deformities) [3]. As always, risks and benefits must be
considered and we must always remember: primum non nocere—first do no harm.
233
References
1. Chan CJ, Chau YJ, Woo SB, Luk HM, Lo IF.
Familial patellar dislocation associated with t(15;20)
(q24;q13.1). J Orthop Surg (Hong Kong). 2018;26
(2):2309499018777026.
2. Rebolledo BJ, Nam D, Cross MB, Green DW,
Sculco TP. Familial association of femoral trochlear
dysplasia with recurrent bilateral patellar dislocation.
Orthopedics. 2012;35(4):e574-9.
3. Post WR, Fithian DC. Patellofemoral instability: a
consensus statement from the AOSSM/PFF patellofemoral instability workshop. Orthop J Sports Med.
2018;6(1):2325967117750352.
4. Hinckel BB, Gobbi RG, Demange MK,
Pereira CAM, Pecora JR, Natalino RJM, et al.
Medial patellofemoral ligament, medial patellotibial
ligament, and medial patellomeniscal ligament:
anatomic, histologic, radiographic, and biomechanical study. Arthroscopy. 2017;33(10):1862–73.
5. Tanaka MJ, Chahla J, Farr J 2nd, LaPrade RF,
Arendt EA, Sanchis-Alfonso V, et al. Recognition of
evolving medial patellofemoral anatomy provides
insight for reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019;27(8):2537–50.
6. Shah KN, DeFroda SF, Ware JK, Koruprolu SC,
Owens BD. Lateral patellofemoral ligament: an
anatomic study. Orthop J Sports Med. 2017;5
(12):2325967117741439.
7. Capkin S, Zeybek G, Ergur I, Kosay C, Kiray A. An
anatomic study of the lateral patellofemoral ligament.
Acta Orthop Traumatol Turc. 2017;51(1):73–6.
8. Reider B, Marshall JL, Koslin B, Ring B, Girgis FG.
The anterior aspect of the knee joint. J Bone Joint
Surg Am. 1981;63(3):351–6.
9. Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human
knee. Am J Sports Med. 1998;26(1):59–65.
10. Betz RR, Magill JTd, Lonergan RP. The percutaneous lateral retinacular release. Am J Sports Med
1987;15(5):477–82.
11. Dandy DJ, Desai SS. The results of arthroscopic
lateral release of the extensor mechanism for recurrent dislocation of the patella after 8 years. Arthroscopy. 1994;10(5):540–5.
12. Christensen F, Soballe K, Snerum L. Treatment of
chondromalacia patellae by lateral retinacular release
of the patella. Clin Orthop. 1988;234:145–7.
13. Biedert RM, Albrecht S. The patellotrochlear index:
a new index for assessing patellar height. Knee Surg
Sports Traumatol Arthrosc. 2006;14(8):707–12.
234
14. Brady JM, Sullivan JP, Nguyen J, Mintz D,
Green DW, Strickland S, et al. The tibial tubercleto-trochlear groove distance is reliable in the setting
of trochlear dysplasia, and superior to the tibial
tubercle-to-posterior cruciate ligament distance when
evaluating coronal malalignment in patellofemoral
instability. Arthroscopy. 2017;33(11):2026–34.
15. Post WR, Teitge R, Amis A. Patellofemoral
malalignment: looking beyond the viewbox. Clin
Sports Med. 2002;21(3):521–46, x.
16. Imhoff FB, Cotic M, Dyrna FGE, Cote M, Diermeier T, Achtnich A, et al. Dynamic Q-angle is
increased in patients with chronic patellofemoral
instability and correlates positively with femoral
torsion. Knee Surg Sports Traumatol Arthrosc.
2021;29(4):1224–31.
17. Halder AM, Kuhl SG, Zobitz ME, Larson D, An KN.
Effects of the glenoid labrum and glenohumeral
abduction on stability of the shoulder joint through
concavity-compression: an in vitro study. J Bone
Joint Surg Am. 2001;83(7):1062–9.
18. Lippitt SB, Vanderhooft JE, Harris SL, Sidles JA,
Harryman DT 2nd, Matsen FA 3rd. Glenohumeral
W. R. Post
19.
20.
21.
22.
23.
stability from concavity-compression: a quantitative
analysis. J Shoulder Elbow Surg. 1993;2(1):27–35.
Teitge RA, Faerber WW, Des Madryl P, Matelic TM.
Stress radiographs of the patellofemoral joint. J Bone
Joint Surg Am. 1996;78(2):193–203.
Sallay PI, Poggi J, Speer KP, Garrett WE. Acute
dislocation of the patella. A correlative pathoanatomic study. Am J Sports Med. 1996;24(1):52–60.
Huntington LS, Webster KE, Devitt BM, Scanlon JP,
Feller JA. Factors associated with an increased risk of
recurrence after a first-time patellar dislocation: a
systematic review and meta-analysis. Am J Sports
Med. 2020;48(10):2552–62.
Jaquith BP, Parikh SN. Predictors of recurrent
patellar instability in children and adolescents after
first-time dislocation. J Pediatr Orthop. 2017;37
(7):484–90.
Arendt EA, Askenberger M, Agel J, Tompkins MA.
Risk of redislocation after primary patellar dislocation: a clinical prediction model based on magnetic
resonance imaging variables. Am J Sports Med.
2018;46(14):3385–90.
Evaluation of the Patient
with Patellar Instability: Clinical
and Radiological Assessment
Andrew E. Jimenez, Lee Pace,
and Donald C. Fithian
1
Introduction
The initial evaluation of a patient with patellar
instability relies heavily on a detailed history and
physical examination. These two pieces of the
evaluation are vitally important. The use of
radiologic evaluation and advanced imaging
studies are also key components that act as an
adjunct to the history and physical. As will be
discussed in this chapter, the etiology of patellar
instability is often due to anatomic risk factors
and can at times be multifactorial in nature. The
initial evaluation should serve to properly identify these etiologies.
Patellofemoral instability is a common
orthopaedic problem and is among the most
frequent acute knee injuries in pediatric and
adolescent age groups with an annual incidence
between 23 and 43 per 100,000 [1]. Typically,
patellofemoral instability is due to anatomic
abnormalities in the lower extremity that lead to
A. E. Jimenez (&)
Department of Orthopaedics and Rehabilitation,
Yale School of Medicine, New Haven, CT, USA
L. Pace
Children’s Health Andrews Institute, Plano, TX,
USA
D. C. Fithian
Senta Clinic, San Diego, CA, USA
medial retinacular deficiency. Multiple risk factors have been associated with recurrent patellar
instability. Most of these risk factors are anatomic in nature and include trochlear dysplasia,
patella alta, genu valgum, femoral anteversion
and ligamentous laxity. Other identified risk
factors include skeletal immaturity, history of a
contralateral dislocation, and participation in
sport. While these non-anatomic factors have
been identified, it is unclear if they are true risk
factors or are coincident to the underlying anatomic abnormalities. As a result, recurrence rates
have been described from as little as 34% to as
high as 88% depending on the presence of risk
factors [2]. The use of a detailed history, physical
examination, and imaging allows for proper
evaluation of these variables and thus allows the
clinician to best guide the patient in shared
decision making. It is helpful to think of patellar
instability as the symptom of the underlying
pathoanatomy. Evaluating the patient from this
perspective helps the clinician to identify the
underlying problem(s) most effectively.
2
History
The history is the first component of any patient
presenting with patellar instability and often is
the key component of establishing a diagnosis.
There are several ways in which a patient with
patellar instability can present. The classic scenario in which a patient sustained a traumatic
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_16
235
236
dislocation that required relocation is typically
self-explanatory. However, there are several
other ways in which a patient with instability can
present. Some patients present with atraumatic
recurrent subluxations while others may at best
describe multiple episodes of buckling or giving
way. Conversely, other patients may describe
pain as a large component of their symptoms. For
these more subtle cases, it is important to keep
instability on the differential diagnosis.
Despite the oft cited example of a twisting
injury in sports, a good percentage of instability
events happen at random, and subluxations can
be a common instability episode. It is helpful to
establish the total number of instability events,
age at first instability event, post instability
swelling and if manual reduction of the dislocation was necessary [3, 4]. Additionally, prior
treatments or surgery should be noted along with
a relevant family history of patellofemoral
instability [5]. Noting the presence of pain is also
important as some patients may cite pain as their
presenting complaint but their examination and
imaging will uncover that instability has been the
source of the problem. While it is normal to have
pain during and after an instability event, some
patients, particularly those with severe anatomic
risk factors, may often have pain in between
episodes which may represent concomitant cartilage injury. Pain should not be totally separated
out from instability.
Noting symptoms or dislocation events on the
contralateral knee is also valuable. A history of a
contralateral patellar dislocation greatly increases
the risk of recurrence and may be influential in
establishing an appropriate treatment plan [6].
Reporting of mechanical symptoms such as
locking or catching combined with a history of
significant swelling after dislocation episodes
may be related to osteochondral injury and loose
bodies which may indicate timely surgical
intervention. Reviewing any prior surgery and
knowing the specific procedures performed can
help provide a complete picture of the patient’s
pathology. If possible, prior operative reports and
operative pictures should be reviewed.
A. E. Jimenez et al.
3
Physical Examination
After obtaining a detailed history, the next step is
physical examination with the goal of identifying
specific pathology. The examination for patellofemoral instability allows for an efficient yet
complete assessment of the patient, and the details
identified in the history can help to focus the exam.
In addition to a holistic exam of the knee, the exam
should evaluate the four principle anatomic risk
factors: trochlear dysplasia, patella alta, genu
valgum and femoral anteversion. It is important to
keep in mind that these can sometimes coexist.
In the non-acute setting, the exam commences
with an evaluation of coronal plane alignment
with the patient supine on the examining table
and bringing the lower extremities into contact
with one another. If the knees are touching but
the feet do not, a concern for genu valgum is
raised and consideration is given for a standing
hip to ankle radiograph.
Patella alta can be evaluated in two ways.
First, with the patient supine, the presence of a
bulging fat pad distal to the patella is consistent
with patella alta. Also, with the patient seated at
the edge of the examining table with the knees
flexed to 90°, the position of the patella is
assessed. If the patella is high riding in the trochlea and is not engaged in the intercondylar
notch, this is consistent with a long patellar
tendon/patella alta (Fig. 1). Lastly, lateral patellar
apprehension in high degrees of knee flexion is
also consistent with patella alta [7]. This will be
discussed more below as this is seen more often
with trochlear dysplasia.
Femoral anteversion is evaluated in the prone
position with the knee flexed 90°. Two principle
exams can be conducted with the patient in this
position. The first is Craig’s test. This involves
internally and externally rotating the hip until the
examiner can feel the patient’s greater trochanter
at its point of greatest prominence. In this position the angle between the thigh and the leg is
recorded (Fig. 2). If this angle is >30°, there is
concern for pathologic femoral anteversion and a
rotational profile CT scan is considered. In
Evaluation of the Patient with Patellar Instability …
237
Fig. 1 Physical exam finding of patella alta. With the
knee flexed to 90° the position of the patella can be
assessed. In the setting of patella alta, the patella (white
arrow) will not be engaged in the intercondylar notch
(black arrow)
addition, if the total amount of internal hip
rotation is 45° or greater than the total amount of
external rotation, this can also be consistent with
pathologic femoral anteversion [8].
Trochlear dysplasia is by far the most common anatomic risk factor for patellar instability.
There are a couple different ways to evaluate for
this pathology. As all are familiar, patellar
apprehension is the keystone examination to
evaluate for instability [9]. However, this test
should be done in various degrees of knee flexion, not just in full extension. Around 30° of
flexion, the patella begins to engage in the trochlea which, in the absence of dysplasia, is able
to catch the patella and direct it into the trochlear
groove. In the setting of dysplasia, the patella
will still be highly unstable in this position.
Often, it takes up to 60° or more of flexion before
the most proximal aspect of the patella has traversed past the dysplastic portion of the trochlea
and becomes seated and stable. If a patient
Fig. 2 (Reproduced from Magee DJ: Orthopedic
physical assessment, ed 3, Philadelphia, 1997, WB
Saunders) Demonstration of Craig’s Test. The patient is
positioned prone with the hip in neutral and the knee
flexed 90°. The examiner may palpate the position of the
leg where the greater trochanter is most prominent. The
angle between a line down the shaft of the tibia and a
vertical line perpendicular to the examination table
represents the degrees of femoral anteversion
demonstrates continued apprehension up to this
degree of knee flexion, that is consistent with
high grade trochlear dysplasia. As mentioned
above, this can also be consistent with high grade
patella alta as it takes higher degrees of knee
flexion to engage the patella in the trochlea if the
238
A. E. Jimenez et al.
A
B
C
D
Fig. 3 (Reproduced with permission from SanchisAlfonso V., Montesinos-Berry E., Serrano A., MartínezSanjuan V. (2011) Evaluation of the Patient with Anterior
Knee Pain and Patellar Instability. In: Sanchis-Alfonso V.
(eds) Anterior Knee Pain and Patellar Instability.
Springer, London) The moving patellar apprehension test
begins with the knee held in full extension and the patella
is manually translated laterally (black arrow) with the
thumb A. The knee is then flexed to 90° and then brought
back to full extension while the lateral force on the patella
(black arrow) is maintained B. In the second part of the
test, the knee is started in full extension C, brought back
to 90° of flexion D, and then brought back to full
extension while the index finger is used to translate the
patella medially (black arrow). For a positive test, in the
first part, the patient expresses apprehension and may
activate his or her quadriceps in response to the apprehension. However, in the second part of the test, the
patient experiences no apprehension and allows free
flexion and extension of the knee
patellar tendon is pathologically long. Ahmad
et al. described a variation of this evaluation
called the “moving patellar apprehension test”
(Fig. 3) [9]. The moving patellar apprehension
test has demonstrated a sensitivity as high as
100%, specificity of 88.4%, a positive predictive
value of 89.2%, a negative predictive value of
100%, and an accuracy of 94.1%. This dynamic
provocative test is similar to the pivot shift test
for the ACL-deficient knee.
The “J” sign is another exam observation that
can be diagnostic for dysplasia. With the patient
seated on the examination table and the legs
hanging over the side with the knees flexed 90˚,
the patient is asked to extend the knee actively to
a fully extended position (Fig. 4). Normally, the
patella follows a straight line as the knee is
extended. In the setting of trochlear dysplasia,
the patella will be pushed lateral by the flat or
convex trochlea as the knee is extended making
the shape of an inverted “J”. Conversely, as the
knee is flexed, the patella will move from lateral
to midline as it centers in the trochlear groove.
A “lazy J” sign can be seen in the setting of lowgrade dysplasia and patella alta. A “jumping J
sign” is usually found in patients with trochlear
dysplasia and a large supratrochlear spur which
is often irritating to the patient [10].
In addition to these focused exams, the knee
should be evaluated for range of motion, swelling, cruciate and collateral ligament integrity,
joint line tenderness and crepitus. Patients presenting with an acute dislocation often will have
an effusion and tenderness over the medial retinacular structures and may not be amenable to
the entirety of the exam listed above.
Evaluation of the Patient with Patellar Instability …
A
239
B
C
Fig. 4 (Reproduced with permission from SanchisAlfonso V., Montesinos-Berry E., Serrano A., MartínezSanjuan V. (2011) Evaluation of the Patient with Anterior
Knee Pain and Patellar Instability. In: Sanchis-Alfonso V.
(eds) Anterior Knee Pain and Patellar Instability.
Springer, London) The “J” sign. When the knee is
extended from 90° A to 0° C the patella outlines an
inverted J-shaped course. Intermediate positions between
90˚ and 0˚ B
The Quadriceps angle or Q angle has been
commonly referenced in the evaluation of
patients with patellar instability. The Q-angle is
described at the intersection of lines drawn from
the anterior superior iliac spine to the center of
the patella and from the center of the patella to
the tibial tubercle. Normal values have been
reported 10° in men and 15° in women. The Q
angle is mainly of historical interest and is not
routinely necessary to measure or evaluate in
modern day evaluation of patients with patella
instability as it does not provide any information
that drives treatment.
Patients with patellofemoral instability may
also demonstrate elements of hypermobility. It is
therefore important to evaluate the presence of
ligamentous laxity. Patellofemoral instability
patients are six times more likely to have
hyperlaxity compared to age matched controls,
but outcomes of intervention as still promising in
this patient population [11]. Hypermobile
patients may demonstrate excessive skin laxity,
and the presence of Ehlers-Danlos syndrome
should be evaluated especially given the significant systemic pathologies which may be present.
In all patients, generalized ligamentous laxity
should be quantified using the Beighton hypermobility score [12].
Referred pain from the hip should always be a
consideration as well when evaluating these
patients and a basic hip examination for range of
motion and anterior impingement is warranted.
Hip pathologies in younger patients such as
Perthes disease, slipped capital femoral epiphysis, or femoroacetabular impingement syndrome may uncommonly manifest as referred
knee pain.
4
Evaluation of Failed Prior
Stabilization Surgery
Patients who have undergoing previous surgery
and continue to have recurrent patellar instability
fall into one or more categories: improper surgical indication, surgical technical error, or
incorrect assessment and treatment of risk factors
for instability (trochlear dysplasia, patella alta,
femoral anteversion, etc.) [13]. If the patient was
properly indicated and continues to have instability postoperatively, technical errors of the
index surgery or surgeries must be considered in
addition to failure to address other anatomic risk
factors of stability. Parikh et al. [14] reported that
47% of the complications that occurred after
MPFL reconstruction surgery were due to
240
A. E. Jimenez et al.
technical errors, the most common of which was
malposition of the femoral tunnel. The femoral
attachment is critical for the function and kinematics of the reconstructed MPFL graft. In the
normal knee, the MPFL is tighter in extension
than in flexion. If the femoral attachment site of a
reconstructed MPFL is placed too anterior, the
graft will tighten when the knee is flexed, and
patellofemoral overload can occur [15]. Similarly
even with a properly placed femoral tunnel,
excessive graft tension is another technical error
that can lead to failure of reconstructive surgery
[16] and can manifest with a painful and relatively immobile patella.
Crepitus through a range of motion is important to document. Most patients with patellar
instability will have some degree of cartilage
damage. This damage can accelerate if an
improper surgery is performed and some patients
in revision settings may require concomitant
chondral resurfacing. It is important to document
any surgical scars as it will need to be determined
if they can be used for a revision surgery or if
new ones need to be made. In particular, a history
of a prior lateral release reduces lateral restraint
and may increase the risk of iatrogenic medial
instability [17]. Lastly, a history of prior tibial
tubercle osteotomy (TTO) can alter patellofemoral mechanics with over-distalization resulting
in loss of terminal flexion and over medialization
potentially contributing to medial instability [18].
5
Evaluation of Medial Patellar
Instability
The direction of any instability is extremely
important. Most of the time instability is in the
lateral direction; however, some patients may
have medial instability and some patients may
suffer from multidirectional instability. Medial
patellar instability is much less frequent than
lateral patellar instability, but should be suspected, especially in patients who remain symptomatic after any lateral retinacular release
surgery. Medial instability was first described by
Hughston and Deese who reported on medial
patellar subluxation in 54 patients who had previously undergone an overzealous lateral release
[19]. Recent biomechanical finite element analysis has demonstrated that lateral retinacular
release even in the setting of a tibial tuberosity
transfer can result in multidirectional instability
[20]. Less commonly, hyperlaxity, trochlear
dysplasia, and deficient quadriceps can rarely be
associated with medial patellar subluxation
events. Bollier et al. detailed that patients with
medial patellar subluxation can occur in cases
with a malpositioned MPFL graft [21].
Patients with prior surgery should be carefully
examined as medial instability can sometimes be
mistaken for lateral patellar instability. In the
case of medial patellar instability, the patella is
subluxated medially in full extension and then as
the knee flexes, it jumps laterally to center in the
trochlear groove. On exam, static medial patellar
subluxation, vastus lateralis atrophy, or a lateral
patellar void may be seen. Our primary method
for diagnosis of medial patellar subluxation is
Fulkerson’s relocation test (Fig. 5). To perform
this test, we hold the patella slightly in a medial
direction with the knee extended. Then, we flex
the knee while letting go of the patella, which
causes the patella to go into the trochlea. In
patients with medial subluxation this test reproduces the patient’s symptom. Further, the gravity
subluxation test has also been described where
the patient is placed in the lateral decubitus
position with the affected limb supported by the
examiner at the ankle and knee [22]. The knee is
flexed from the extended position. If medial
instability is present, the patient cannot tolerate
passive knee flexion without upward force on the
patella, which reduces the patella and allows it to
enter the groove as the knee is flexed passively
by the examiner. A positive test is indicative of
medial instability and confirms deficiency of the
lateral retinacular constraints. Further evaluation
on imaging should follow the standard protocol for patients with lateral patellar instability,
but additional views such as stress radiographs of
the patellofemoral joint as described by Teitge
et al. can be helpful in establishing a diagnosis
[23].
Evaluation of the Patient with Patellar Instability …
A
B
241
6
Imaging studies are next in the diagnostic algorithm after the history and physical exam. Relying on imaging results prior to consideration of a
history and physical can lead to diagnostic errors
and at times improper treatment. Surgical indications should be based on history, physical
exam findings, and imaging working together in
tandem. Imaging modalities may be used to
confirm the diagnosis established by the history
and physical exam, quantify pathology, and to
identify other concomitant pathologies that may
warrant treatment.
7
C
Fig. 5 (Reproduced with permission from SanchisAlfonso V., Montesinos-Berry E., Serrano A., MartínezSanjuan V. (2011) Evaluation of the Patient with Anterior
Knee Pain and Patellar Instability. In: Sanchis-Alfonso V.
(eds) Anterior Knee Pain and Patellar Instability.
Springer, London) Fulkerson’s relocation test. We hold
the patella slightly in the medial direction (black arrow)
with the knee extended A. Contralateral asymptomatic
knee B. Then, we flex the knee while letting go of the
patella, which causes the patella to go into the femoral
trochlea C
Imaging Studies
Radiographs
Initial imaging for patients with patellofemoral
instability are standard radiographic views
including standing anteroposterior (AP) view, a
45° bent knee posteroanterior Rosenberg vie, and
a true lateral view (defined as <2 mm offset of
the posterior femoral condyles). Weightbearing AP and 45° PA views allow one to evaluate
evidence of joint space narrowing of the medial
or lateral compartment as well as large varus and
valgus deviations. Such deviations would need
further quantification with long leg standing
films if indicated. Of note, with the advent of
advanced axial imaging, the diagnostic utility of
these radiographic views is falling out of favor.
The lateral view is the workhorse view to
qualify anatomic risk factors for patellar instability. However, the x-ray should be used to
support advanced imaging and not as a sole
diagnostic tool. Patellar height (patella alta vs
patella baja) can be quantified using several
methods
including
the
Insall-Salvati,
Blackburne-Peel, and Caton−Deschamps ratio.
The Caton-Deschamps and Balckburne-Peel
ratios are used by many clinicians because the
value remains constant despite minor variations
in knee flexion and can be used for skeletally
immature patients.
242
A perfect lateral view can evaluate for trochlear dysplasia. Radiographic findings such as
the crossing sign, trochlear spur, and double
contour sign are pathognomonic for trochlear
dysplasia. The crossing sign is when the curve of
the trochlear floor crosses the anterior contour of
the lateral femoral condyle, which represents
flattening of the trochlear groove and absence of
trochlear constraint. A trochlear spur (also
described as a trochlear prominence, boss, bump,
or eminence) is when the proximal trochlea
begins to elevate away from the distal femoral
metadiaphysis and can become convex with larger spurs. The spur size can be quantified via the
distance between the most anterior point of the
spur and a line drawn along the distal aspect of
the anterior femoral cortex. The double contour
sign is a double line at the anterior aspect of the
femoral condyles that represents the chondral
outline of a hypoplastic medial trochlea. The
Dejour classification is based on these lateral
radiographic and axial imaging findings [24].
Type A is characterized by a shallow trochlea,
with a crossing sign on the lateral view and a
sulcus angle >145 on the axial view. Type B is
characterized by the appearance of a flat trochlea
on axial radiographs and a supratrochlear spur on
lateral images. Type C has the presence of a
crossing sign and a double contour sign in lateral
radiographs combined with medial hypoplasia
and lateral convexity on axial radiographs.
Type D dysplasia has asymmetry of the trochlear
facets and a cliff between the medial and lateral
facets on the axial view [24]. A summary of
radiographic signs of trochlear dysplasia can be
found in Fig. 6. In patients with a prior MPFL
reconstruction, the femoral tunnel position can be
evaluated on the lateral radiograph (Fig. 7). In
addition, the lateral view can diagnose degenerative changes in the patellofemoral joint.
In a Merchant view of the knee in 45˚ of
flexion, patellofemoral pathoanatomy is often
overlooked because pathology at the proximal
part of the trochlear groove may not be readily
visible, and a supratrochlear spur may be missed.
Alternatively, a Laurin radiograph with the knee
flexed to 20° and the imaging beam directed from
A. E. Jimenez et al.
inferior to superior is better at evaluating trochlear morphology. However, this is still difficult
to obtain at times and a “normal” appearing axial
view does not rule out conditions such as trochlear dysplasia.
The axial radiograph can also be used for
stress images of the patella. In these images, axial
radiographs are obtained while an examiner
applies approximately constant pressure to the
patella in either the medial or lateral direction.
Relaxation of the quadriceps must be maintained
and the displacement can be measured on the
radiograph by a technique described by Laurin
et al. [25]. Lastly, a long leg standing film, or AP
hip to ankle x-ray, is ordered based on physical
exam concerns for coronal plane malalignment.
This imaging study is crucial to quantify varus
and valgus alignment.
8
Magnetic Resonance Imaging
(MRI)
Advanced imaging with MRI is currently the
gold standard to diagnose and quantify pathoanatomy and articular cartilage injuries in patients
with patellar instability. An MRI should be performed before any surgical intervention for
patellar instability and the authors advocate for
MRI examination of all acute, traumatic, first
time dislocations to evaluate for osteochondral or
chondral injuries that may warrant surgical fixation [26]. Axial MRI allows for thorough and
quantitative evaluation of bony and cartilaginous
anatomy and injury as well as patellar height.
While evaluation of bony anatomic risk factors
and chondral injuries are the primary concern,
MRI is also useful for viewing the status of the
MPFL [27].
Axial MRI is key to quantifying trochlear
dysplasia. Given that trochlear dysplasia is the
most common anatomic risk factor associated
with patellar instability, it must be diagnosed and
assessed for in every patient. Historically, dysplasia has been categorized via the Dejour classification scheme on axial MRI, however, there
has been poor inter-rater reliability with this
Evaluation of the Patient with Patellar Instability …
243
Fig. 6 (Reproduced with permission from Dejour D,
Saggin PRF: Sulcus-deepening trochleoplasty in
Scott WN, ed: Insall and Scott Surgery of the Knee, ed
5. Philadelphia PA, Elsevier, 2012, pp 688−695) Illustrations of the knee joint demonstrating the appearance of
various types of trochlear dysplasia on the lateral and
axial radiographic imaging. A Dejour Type A, the
crossing sign is visible on lateral views and the trochlea
appears shallower than normal but still symmetric and
concave. B Dejour Type B, the crossing sign and trochlear
spur are visible on lateral imaging. On axial views the
trochlea appears flat, with prominence of the entire
trochlea. C Dejour Type C, the crossing stign and
double-contour sign are visible on the lateral view, but
no prominence is visible. On the axial view, the lateral
facet appears convex and the medial facet is hypoplastic.
D Dejour Type D, the crossing sign, supratrochlear spur,
and doubler-contour sign are visible. On the axial view,
there is clear symmetry of the height of the facets, which
is known as a cliff pattern
approach and better reliability has been shown by
a binary classification of low-grade (Dejour A)
and high-grade (Dejour B-D) dysplasia.
Recent literature has documented the value of
lateral trochlear inclination (LTI) to help quantify
trochlear morphology [28]. Currently, as described by Joseph et al. LTI is measured using a twoimage technique on axial MRI sequences at the
levels of the most proximal extent of the trochlear cartilaginous surface and the posterior
femoral condyles (Fig. 8). An LTI value that is
positive denotes that there is some degree of a
trochlear groove at the most proximal extent of
the trochlea. An LTI of 0° represents a flat
proximal trochlea and a negative LTI represents a
convex proximal trochlea. LTI has been used
extensively to quantitatively evaluate trochlear
dysplasia in the setting of patellar instability. LTI
as measured on MRI can better characterize the
proximal trochlea than radiographic imaging
which has been traditionally used for the Dejour
classification [29, 30]. Carrillon, et al. (using a
single image technique) have established that an
LTI <11° is associated with a 95% specificity of
having patellar instability secondary to trochlear
dysplasia [31] although this number has not been
reassessed since the advent of the two-image
technique.
Patellar height is also evaluated on MRI via
sagittal imaging. MRI is currently considered to
be more reliable than x-ray for measuring patellar
height due to inconsistencies in the angle of the
244
Fig. 7 Lateral radiograph of a patient status-post medial
patellofemoral ligament reconstruction with recurrent
instability. Femoral tunnel position is indicated by the
yellow arrow and patellar tunnels are indicated by the
white arrows
Fig. 8 [28] (Reproduced from Joseph et al., Reprinted
with permission from SAGE Publishing) Measurement
technique for 2-image lateral trochlear inclination (LTI).
A An angular measurement was taken on an axial MRI
image between the most proximal aspect of the lateral
trochlear cartilaginous surface and a horizontal reference
line represented by the red lines. This angle measured 15°.
This angle’s apex was medial, so it was assigned a
positive value. B An angle was measured between the
A. E. Jimenez et al.
x-ray beam, and all the indices mentioned above
can be measured on MRI as well as x-ray. Further, one can measure the patellotrochlear index
(PTI) on MRI (Fig. 9). This measures the amount
of cartilaginous overlap between the patella and
the trochlea and is thought to be a more functional representation of patellar height. While
there is no scientific data to say at what point a
PTI value represents pathologic patella alta,
expert opinion puts it between 0.1 and 0.25.
Biedert et al. showed the mean value in a normal
population was 0.31 with a 95% CI of 0.125
−0.50 [32]. Of note the values established on
MRI by Biedert et al. were with the knee in full
extension, but many knee MRIs, particularly in
the United States, are obtained with the knee in
10° of flexion. This discrepancy should be kept in
mind when interpreting the results.
The tibial tubercle-trochlear groove (TT-TG)
distance is a popular and well-known measure for
patients with patellar instability. It has, by and
large, replaced the Q angle as a measure of
malalignment and may be helpful in guiding
decision making for tubercle osteotomies. While
posterior condyles and a horizontal line represented by the
red lines. This angle measured 2°. It was assigned a
positive value because the apex of the angle was medial.
The 2-image LTI was determined by subtracting the angle
of the posterior femoral condyles relative to the horizontal
from the angle of the proximal lateral trochlea relative to
the horizontal. In this example, the LTI calculation was
15°−2° = 13°
Evaluation of the Patient with Patellar Instability …
245
9
Fig. 9 [32] (Reproduced from Biedert et al., Reprinted
with permission from Springer Publishing) Patellotrochlear index measurement. BL(P) Baseline patella (2
superior most aspect of articular cartilage to 3 inferior
most aspect); BL(T) Baseline trochlea (length of trochlear
articular surface from 1 superior most aspect with respect
to 3 the inferior most aspect of the articular patellar
cartilage using a right angle and parallell lines); The ratio
is BL(T)/BL(P); LT Length of trochlear cartilage (superior
most aspect to inferior most aspect of trochlea using a
vertical line)
recommendations vary, most surgeons consider a
TT-TG value >20 mm to be an indication for a
tibial tubercle osteotomy. However, recent work
has challenged the concept that an elevated TT-TG
is a sole representation of a lateralized tibial
tubercle. Rather, the TT-TG looks to be a multifactorial measure that is influenced by trochlear
groove anatomy and tibial rotation [33, 34]. As a
result, the notion of a pathologically lateral tibial
tubercle is not as common as previously thought.
If there is still concern for a lateralized tibial
tubercle, some have argued that measurement of
the tibial tubercle-posterior cruciate ligament distance (TT-PCL) offers a better measure of tubercle
lateralization because both points are referenced
from the tibia [35–37]. For this reason, TT-PCL
distance is independent of tibiofemoral rotation as
well as the position of the groove. It can be useful
to measure both TT-TG and TT-PCL in order to
assess whether TT-TG might be falsely elevated
due to rotation or an abnormal groove.
Computed Tomography (CT)
CT scans are less commonly utilized in the
evaluation of patellofemoral instability than
radiographs and MRI. They are preferred by
some for TT-TG measurements, and they are
central to quantifying torsional deformities of the
lower extremities. In this setting, the decision to
obtain a CT scan is typically not routine but
instead dictated by physical exam findings consistent with increased femoral anteversion or
external tibial torsion (8). Further applications of
CT scans include three-dimensional CT (3D-CT)
scans which have been used to show realistic
volumetric representations of the patella and
trochlea. The complex geometry of the trochlea
can be challenging to interpret on 2 dimensional
images and the addition of 3D-CT can help
provide a qualitative evaluation and may be
useful for preoperative planning for some surgeons [38] (Fig. 10).
10
Ultrasound
The advancement of high-definition ultrasound
devices has allowed for an expansion of its
clinical application including the evaluation of
trochlear morphology [39]. Due the limitations of
image acquisition with ultrasound as compared
with MRI, most notably the inability to visualize
the posterior condyles of the femur, most ultrasound evaluations have focused on measurements of trochlear depth and sulcus angle
measurements. Despite these shortcomings,
ultrasound has been used as a cost effective way
to evaluate the prevalence of trochlear dysplasia
in a general population of patients [40]. A particular advantage of ultrasound is that it can
evaluate the trochlea along the curvature of the
distal femur, while maintaining an orthogonal
alignment to the trochlear groove. This is in
contrast with MRI, where the angle of the image
acquired must be set beforehand and maintained
over the area of interest. The role for ultrasound
may continue to evolve in the evaluation of
patients with patellar instability but further
246
A
A. E. Jimenez et al.
B
C
E
D
F
Fig. 10 (Reproduced with permission from SanchisAlfonso V., Montesinos-Berry E., Serrano A., MartínezSanjuan V. (2011) Evaluation of the Patient with Anterior
Knee Pain and Patellar Instability. In: Sanchis-Alfonso V.
(eds) Anterior Knee Pain and Patellar Instability.
Springer, London) 3D-CT reconstruction of the
patellofemoral joint. Axial plane showing degenerative
changes of the articular cartilage of the medial patellar
facet A, frontal plane B, and sagittal plane C. 3D-CT
shows great fidelity of the surface anatomy D, E, but it is
unable to show undersurface detail which is clearly shown
by conventional CT scans F or MRI
Evaluation of the Patient with Patellar Instability …
research is warranted to develop ultrasoundspecific criteria for trochlear dysplasia rather than
using MRI obtained values.
11
Summary
The evaluation and treatment of patients with
patellofemoral instability requires an in-depth
knowledge and consideration of all potential
contributing pathologies through the history,
physical examination, and imaging studies.
Properly identifying patients with recurrent
patellar instability using provocative clinical tests
and appropriate imaging is critical in identifying
patients who would benefit from surgical intervention. Advanced imaging modalities can
identify patients with loose bodies, chondral
fractures which will require concomitant treatment. The assimilation of all this information
helps the treating surgeon counsel the patient on
treatment options and select the ideal intervention to address their instability.
12
Take Home Messages
• MRI is a key component of a diagnostic
workup and should be obtained on every
patient prior to surgical intervention and in all
patients
• Trochlear dysplasia is the most common
anatomic risk factor associated with patellar
instability, and it should be assessed for every
patient
13
Key Message
• A careful history, detailed physical examination, and focused imaging studies are the key
components of establishing and accurate
diagnosis and developing a properly indicated
treatment plan.
247
References
1. Sanders TL, Pareek A, Hewett TE, Stuart MJ,
Dahm DL, Krych AJ. Incidence of first-time lateral
patellar dislocation: a 21-Year population-based
study. Sports Health. 2018;10(2).
2. Jaquith BP, Parikh SN. Predictors of recurrent
patellar instability in children and adolescents after
first-time dislocation. J Pediatr Orthop. 2017;37(7).
3. Grimm NL, Levy BJ, Jimenez AE, Crepeau AE, Lee
Pace J. Traumatic patellar dislocations in childhood
and adolescents. Orthop Clin N Am. 2020;51(4).
4. Chotel F, Bérard J, Raux S. Patellar instability in
children and adolescents. Orthop Traumatol Surg
Res OTSR. 2014;100(1 Suppl).
5. Post WR, Fithian DC. Patellofemoral instability: a
consensus statement from the AOSSM/PFF patellofemoral instability workshop. Orthop J Sport Med.
2018;6(1).
6. Fithian DC, Paxton EW, Stone ML, Silva P,
Davis DK, Elias DA, et al. Epidemiology and natural
history of acute patellar dislocation. Am J Sport Med.
2004;32(5).
7. Colatruglio M, Flanigan DC, Harangody S,
Duerr RA, Kaeding CC, Magnussen RA. Identifying
patients with patella alta and/or severe trochlear
dysplasia through the presence of patellar apprehension in higher degrees of flexion. Orthop J Sport
Med. 2020;8(6).
8. Kozic S, Gulan G, Matovinovic D, Nemec B,
Sestan B, Ravlic-Gulan J. Femoral anteversion
related to side differences in hip rotation. Passive
rotation in 1,140 children aged 8–9 years. Acta
orthopaedica Scandinavica. 1997;68(6).
9. Ahmad CS, McCarthy M, Gomez JA, Shubin
Stein BE. The moving patellar apprehension test for
lateral patellar instability. Am J Sport Med. 2009;37
(4).
10. Diduch DR, Kandil A, Burrus MT. Lateral patellar
instability in the skeletally mature patient: evaluation
and surgical management. J Am Acad Orthop Surg.
2018;26(12).
11. Hiemstra LA, Kerslake S, Kupfer N, Lafave MR.
Generalized joint hypermobility does not influence
clinical outcomes following isolated MPFL reconstruction for patellofemoral instability. Knee Surg
Sports Traumatol Arthroscopy Offic J ESSKA.
2019;27(11).
12. Beighton P, Solomon L, Soskolne CL. Articular
mobility in an african population. Ann Rheum Dis.
1973;32(5).
13. Sanchis-Alfonso V, Montesinos-Berry E, RamirezFuentes C, Leal-Blanquet J, Gelber PE, Monllau JC.
Failed medial patellofemoral ligament reconstruction: causes and surgical strategies. World J
Orthop. 2017a;8(2).
248
14. Parikh SN, Nathan ST, Wall EJ, Eismann EA.
Complications of medial patellofemoral ligament
reconstruction in young patients. Am J Sport Med.
2013;41(5).
15. Sanchis-Alfonso V, Ramirez-Fuentes C, MontesinosBerry E, Domenech J, Martí-Bonmatí L. Femoral
insertion site of the graft used to replace the medial
patellofemoral ligament influences the ligament
dynamic changes during knee flexion and the clinical
outcome. Knee Surg Sports Traumatol Arthroscopy
Offic J ESSKA. 2017b;25(8).
16. Sanchis-Alfonso V. Guidelines for medial patellofemoral ligament reconstruction in chronic lateral
patellar instability. J Am Acad Orthop Surg.
2014;22(3).
17. Sanchis-Alfonso V, Merchant AC. Latrogenic medial
patellar
instability:
an
avoidable
injury.
Arthroscopy J Arthroscop Relat Surg. 2015;31(8).
18. Merican AM, Kondo E, Amis AA. The effect on
patellofemoral joint stability of selective cutting of
lateral retinacular and capsular structures. J Biomech.
2009;42(3).
19. Hughston JC, Deese M. Medial subluxation of the
patella as a complication of lateral retinacular release.
Am J Sport Med. 1988;16(4).
20. Salvatore G, Berton A, Orsi A, Egan J, Walley KC,
Johns WL, et al. Lateral release with tibial tuberosity
transfer alters patellofemoral biomechanics promoting
multidirectional
patellar
instability.
Arthroscopy J Arthroscop Relate Surg. 2021.
21. Bollier M, Fulkerson J, Cosgarea A, Tanaka M.
Technical failure of medial patellofemoral ligament
reconstruction. Arthroscopy J Arthroscop Relat Surg.
2011;27(8).
22. Nonweiler DE, DeLee JC. The diagnosis and treatment of medial subluxation of the patella after lateral
retinacular release. Am J Sport Med. 1994;22(5).
23. Teitge RA, Faerber WW, Des Madryl P, Matelic TM.
Stress radiographs of the patellofemoral joint. J Bone
Jt Surg Am Vol. 1996;78(2).
24. Dejour D, Le Coultre B. Osteotomies in patellofemoral instabilities. Sports medicine and arthroscopy review. 2007;15(1).
25. Laurin CA, Dussault R, Levesque HP. The tangential
x-ray investigation of the patellofemoral joint: x-ray
technique, diagnostic criteria and their interpretation.
Clin Orthop Relat Res. 1979(144).
26. Fones L, Jimenez AE, Cheng C, Chevalier N,
Brimacombe MB, Cohen A, et al. Trochlear dysplasia as shown by increased sulcus angle is associated with osteochondral damage in patients with
patellar instability. Arthroscopy J Arthroscop Relat
Surg. 2021.
27. Zhang GY, Ding HY, Li EM, Zheng L, Bai ZW,
Shi H, et al. Incidence of second-time lateral patellar
dislocation is associated with anatomic factors, age
A. E. Jimenez et al.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
and injury patterns of medial patellofemoral ligament
in first-time lateral patellar dislocation: a prospective
magnetic resonance imaging study with 5-year
follow-up. Knee Surg Sports Traumatol Arthroscopy
Offic J ESSKA. 2019;27(1).
Joseph SM, Cheng C, Solomito MJ, Pace JL. Lateral
trochlear inclination angle: measurement via a 2Image technique to reliably characterize and quantify
trochlear dysplasia. Orthop J Sport Med. 2020;8(10).
Paiva M, Blønd L, Hölmich P, Steensen RN,
Diederichs G, Feller JA, et al. Quality assessment
of radiological measurements of trochlear dysplasia;
a literature review. Knee Surg Sports Traumatol
Arthroscopy Offic J ESSKA. 2018;26(3).
Stepanovich M, Bomar JD, Pennock AT. Are the
current classifications and radiographic measurements for trochlear dysplasia appropriate in the
skeletally immature patient? Orthopaed J Sports
Med. 2016;4(10).
Carrillon Y, Abidi H, Dejour D, Fantino O,
Moyen B, Tran-Minh VA. Patellar instability:
assessment on MR images by measuring the lateral
trochlear inclination-initial experience. Radiology.
2000;216(2).
Biedert RM, Albrecht S. The patellotrochlear index:
a new index for assessing patellar height. Knee Surg
Sports Traumatol Arthroscopy Offic J ESSKA.
2006;14(8).
Paiva M, Blønd L, Hölmich P, Barfod KW. Effect of
medialization of the trochlear groove and lateralization of the tibial tubercle on TT-TG Distance: a
cross-sectional study of dysplastic and nondysplastic
knees. Am J Sport Med. 2021;49(4).
Tensho K, Shimodaira H, Akaoka Y, Koyama S,
Hatanaka D, Ikegami S, et al. Lateralization of the
tibial tubercle in recurrent patellar dislocation: verification using multiple methods to evaluate the tibial
tubercle. J Bone Jt Surg Am Vol. 2018;100(9).
Seitlinger G, Scheurecker G, Högler R, Labey L,
Innocenti B, Hofmann S. Tibial tubercle-posterior
cruciate ligament distance: a new measurement to
define the position of the tibial tubercle in patients with
patellar dislocation. Am J Sport Med. 2012;40(5).
Anley CM, Morris GV, Saithna A, James SL, Snow M.
Defining the role of the tibial tubercle-trochlear groove
and tibial tubercle-posterior cruciate ligament distances in the work-up of patients with patellofemoral
disorders. Am J Sport Med. 2015;43(6).
Dong C, Zhao C, Li M, Fan C, Feng X, Piao K, et al.
Accuracy of tibial tuberosity-trochlear groove distance and tibial tuberosity-posterior cruciate ligament
distance in terms of the severity of trochlear dysplasia. J Orthop Surg Res. 2021;16(1).
Fuchs A, Feucht MJ, Dickschas J, Frings J, Siegel M,
Yilmaz T, et al. Interobserver reliability is higher for
assessments with 3D software-generated models than
Evaluation of the Patient with Patellar Instability …
with conventional MRI images in the classification of
trochlear dysplasia. Knee Surg Sports Traumatol
Arthroscopy Offic J ESSKA. 2021.
39. Øye CR, Holen KJ, Foss OA. Mapping of the
femoral trochlea in a newborn population: an ultrasonographic study. Acta Radiol. 2015;56(2).
249
40. DeVries CA, Bomar JD, Pennock AT. Prevalence of
trochlear dysplasia and associations with patellofemoral pain and instability in a skeletally mature
population. J Bone Jt Surg Am Vol. 2021;103(22).
Evolving Management of Acute
Dislocations of the Patella
Vicente Sanchis-Alfonso, Erik Montesinos-Berry,
and Marc Tompkins
1
Background
The acute lateral dislocation of the patella or
First-time lateral patellar dislocation (FTLPD) is
a relatively frequent injury in the young physically active population. Its incidence in the
general population is 42 cases (95% CI 37−47)
per 100,000 person-years and it is 108 cases
(95% CI 101−116) per 100,000 in female
patients aged 10−17 [1]. Furthermore, the possibility of a recurrence of the dislocation is relatively high in the general population, 22.7%
(95% CI 22.2−23.2) at a mean of 10 years.
Young females, aged 10−17, show the greatest
risk at 36.8% (95% CI 35.5−38.0) [1]. Therefore,
this is a frequent knee pathology that causes
chronic instability in an important number of
patients. Perhaps even more important than the
abovementioned facts, is that the dislocation of
the patella is a significant risk factor for the
development of patellofemoral osteoarthritis
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
E. Montesinos-Berry
ArthroCentre–Agoriaz, Riaz & Clinique CIC
Riviera, Montreux, Switzerland
M. Tompkins
University of Minnesota, TRIA Orthopedic Center,
Minneapolis, MN, USA
(PFOA) in the young adult and the physical
limitations that accompany early PFOA [2].
Sanders and colleagues [2] have shown an
accumulated incidence of PFOA of 1.2% at 5
years, 2.7% at 10 years, 8.1% at 15 years, 14.8%
at 20 years, and 48.9% at 25 years. Moreover, it
is thought that 71% of patients with an FTLPD
will develop either a chondral injury or an
osteochondral injury [3]. In 2017, Salonen and
colleagues observed that 70% of patients with an
FTLPD sustained cartilage injuries in the patellofemoral joint (PFJ) that were visible on MRI
[4]. At a mean 8 years of follow-up, patellofemoral cartilage deterioration was visible in 100%
of the patients with a single FTLPD with nonsurgical treatment [4]. Redislocation was not
related to the severity of the cartilage damage [4].
It is interesting to highlight the fact that an
osteochondral injury, recurrent patellar instability
and trochlear dysplasia are associated with the
development of PFOA [2].
FTLPD is thus a frequent pathology that is not
self-limiting and furthers the development of
early-onset PFOA which can result in anterior
knee pain (AKP) and a decrease in the level of
physical activity and quality of life. Since one of
the factors that favors the appearance of PFOA at
long-term, with no good solution in the young
patient, is the recurrence of the dislocation, an
effort must be made to implement therapeutic
strategies to minimize the risk of recurrence and
the consequent future complications.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_17
251
252
V. Sanchis-Alfonso et al.
A
B
Fig. 1 Evident MPFL disruption. MPFL injury pattern
assessment by MRI. A Coronal view. B Axial view.
Laterally subluxated patella. The contralateral patella has
a normal alignment. (Republished with permission of
AME Publishing Company. From Sanchis-Alfonso V and
Montesinos-Berry E. Acute dislocation of the patella:
should these patients be operated on more often? Ann
Joint, 3:20, 2018)
Currently, there is a controversy regarding the
best treatment for FTLPD despite the high incidence of this pathological condition. Classically,
it was thought that these patients were candidates
for non-surgical treatment in the majority of
cases. The exceptions were when the dislocation
was irreducible, in cases with an evident disruption of the medial patellar stabilizers (Fig. 1),
in the presence of osteochondral fragments secondary to a dislocation that behave like intraarticular loose bodies (Fig. 2), or when there is a
large and displaced bone avulsion facture off the
medial aspect of the patella (Fig. 3).
Interestingly, 84% of patellar avulsion fractures
affect the inferomedial border of the patella,
which is the zone where the medial patellotibial
ligament and the medial patellomeniscal ligament are attached [5]. The avulsion site is very
important because 20% of patients with inferomedial border fractures showed recurrence
compared with 0% of superior patellar avulsion
fracture patients after acute surgical repair [5].
Therefore, fixation of the avulsion fracture may
not be sufficient in these cases, and some of these
patients may require an MPFL reconstruction
(MPFLr) [5].
A
B
Fig. 2 MRI signs of FTLPD: contusions of the anterior
portion of the lateral femoral condyle and of the medial
patellae, osteochondral defects (black thick arrow), intra-
C
articular bodies (white thick arrow), and joint effusions
(asterisk). A & B Axial FSE PDW Fat Sat MR images.
C Coronal FSE PDW Fat Sat MR image
Evolving Management of Acute Dislocations of the Patella
253
A
B
Fig. 3 A large, displaced bone avulsion fracture of the
MPFL. A Surgical image. B CT-3D image. (Republished
with permission of AME Publishing Company. From
Classic dogma suggests that these patients “do
well” with non-surgical treatment. However,
current scientific evidence puts the classic standard of treatment in doubt and suggests that an
FTLPD should be treated surgically more often
than it is normally done [6]. The aim of this
chapter is to describe the present-day indications
clearly and concisely for the surgical or nonsurgical treatment after an FTLPD. The treatment
of this injury should be personalized as we will
see throughout this chapter. We consistently
speak about non-surgical treatments instead of
referring to them as conservative treatments, but
it is important to note that any treatment of the
PFJ, whether surgical or non-surgical, should be
as conservative as possible. Treatment for the
PFJ should include whatever is necessary for
appropriate treatment, no more, no less.
Sanchis-Alfonso V and Montesinos-Berry E. Acute
dislocation of the patella: should these patients be
operated on more often? Ann Joint, 3:20, 2018)
2
Who Needs Early Surgery?–
Factors Affecting
Decision-Making
Medical providers for patients with patellofemoral pathology need to keep themselves up to
date with the current literature on the particular
patellofemoral pathology they are treating,
including randomized clinical trials (RCTs) and
systematic reviews with a meta-analysis.
There are several studies that analyze surgical
versus non-surgical treatment for FTLPD [7–17].
In some of them, the recurrence rates of patellar
dislocation reported were lower in the surgical
treatment group [7–11]. Nonetheless, other authors
did not find differences in recurrence rates between
surgical and non-surgical treatment [12–17].
254
The functional results were similar in both
modalities of treatment in most of the studies,
suggesting that surgical treatment does not
improve the outcomes [8–17]. However, there
are several key issues to acknowledge if we
analyze the above papers in-depth. The first is
that the follow-up times and ages are very
heterogeneous, therefore, the recurrence rates as
well as ages are not comparable in all the studies.
The small number of patients in these papers is a
limiting factor that could lead to non-detection of
statistically significant differences between the
groups. Finally, the conservative treatment protocol is not the same in all studies, and the types
of surgical treatment are also different (realignment surgery, MPFL repair and MPFLr). Consequently, it is difficult to draw conclusions when
doing systematic reviews with a meta-analysis
using these studies.
Pagliazzi and colleagues [18], in a metaanalysis of RCTs, showed a greater redislocation
rate in non-surgical patients after an FTLPD.
Better clinical outcomes were found with surgical treatment up to the 6-year follow-up, but the
results were similar in both groups, surgical and
non-surgical, at longer term follow-up. In 2020,
Migliorini and colleagues [19] recommend up
front surgical treatment after an FTLPD in a
systematic review of randomized and nonrandomized clinical trials with meta-analysis.
Better function is achieved with the therapeutic
approach proposed by these authors, as demonstrated by higher values in the Kujala score as
well as a significant reduction in redislocations
and persistent feelings of instability in comparison with non-surgical treatment. In 2020, Fu and
colleagues [20] conducted a systematic review
with a meta-analysis of solely RCTs and concluded the same as Migliorini and colleagues
[19], that surgical treatment is better than nonsurgical treatment in patients with an FTLPD. It
is important to note that these systematic reviews
include both MPFL repairs and MPFL reconstructions within the surgical treatment group and
we must bear in mind that the results of a repair
are not the same as those of a reconstruction. In
2018, Askenberger and colleagues [21] published their results of a randomized controlled
V. Sanchis-Alfonso et al.
trial in which they compare the non-surgical
treatment of the FTLPD (knee brace for 4 weeks
and physical therapy) with surgical treatment
(arthroscopic-assisted repair of the MPFL with
anchors followed by 4 weeks of immobilization
and physical therapy). The authors conclude that
the percentage of redislocations is significantly
less in the surgical group than in the non-surgical
group (22 vs. 43%), but the overall function was
not different between groups and the majority of
patients in both groups were satisfied with the
function of the knee. Although there are no differences with regard to patient function, the fact
that the number of dislocations is reduced with
surgical treatment is clinically relevant because
the recurrence of dislocation is a factor that
favors PFOA, as we have already stated. The
take-home message might be that surgical treatment has a lower recurrence rate and better shortterm clinical outcomes but a higher rate of
complications and similar clinical outcomes in
the long-term.
We can conclude that the currently available
evidence is not sufficiently conclusive to recommend one treatment over the other. That is,
the results of these papers are not enough to
answer the relevant question as to who needs
early surgery. To answer this question for each
individual patient, it is necessary to keep other
issues in mind, ones that we will analyze next.
2.1 First-Time Patellar Dislocation
with an Associated Loose
Body
Even though the current standard treatment for
FTLPD is non-surgical, an operation would be
considered to fix the osteochondral fragment if
the patient presents with an osteochondral injury
and an associated loose body. If it cannot be
fixed, then generally the loose body is excised
arthroscopically. According to Pedowitz and
colleagues, if the treatment of an osteochondral
injury is not pared with an MPFL repair or
MPFLr, the percentage of recurrent instability is
61% [22]. If we compare the cases in which an
MPFLr is performed to those cases in which the
Evolving Management of Acute Dislocations of the Patella
MPFL is repaired or nothing at all is done, then
we see that there is a lower rate of recurrent
instability (10 vs 58.7%), a higher percentage of
return to sports activity (66.7 vs 38.1%), and an
even smaller risk of a second surgery (56.7 vs
47%) with MPFLr [23]. Given this body of literature, it would be reasonable to perform an
MPFLr on all adolescents with an FTLPD with
an associated loose body.
2.2 Pathoanatomy−Risk Factors
for Recurrence After
an FTLPD−Predictive
Models Analysis
The decision-making with regard to either surgical or non-surgical treatment can be based on
the risk of recurrence after non-surgical treatment. The key question is whether recurrent
patellar dislocation be predicted after an FTLPD.
The idea is to identify those risk factors that can
predict the failure of non-surgical treatment and
to design predictive models of recurrent dislocation after an FTLPD treated non-surgically.
Predictive models may assist in the decisionmaking process aimed at achieving better clinical
outcomes as well as reducing costs [24]. The end
point of using predictive models in the FTLPD
population is to identify individuals at high risk
for recurrent patellar instability that might benefit
from early surgical treatment.
Several scoring systems to assess the risk of
recurrence after an FTLPD have been published.
An analysis of this literature demonstrates that
the redislocation risk can only be assessed using
combined risk factors. In 2013, Lewallen and
colleagues [25] analyzed the factors that predict a
lateral patellar dislocation recurrence in pediatric
patients and adolescents with a mean age of 15
years (ranging from 9 to 18 years). They discovered that successful conservative treatment
after an FTLPD was 62% and that around half of
the patients with recurrent lateral patellar dislocation need surgical treatment. The most important risk of dislocation recurrence appeared in
skeletally immature patients with trochlear
255
dysplasia. The combination of both factors (trochlear dysplasia and skeletal immaturity) conferred a risk of 69% at 5 years. The results of this
study are in accordance with those of Askenberger and colleagues [26] who recognized that
trochlear dysplasia is the main anatomic patellar
instability risk factor in skeletally immature
children. Balcarek and colleagues [27] developed
the Patellar instability severity score (PISS)
which was the first multivariable scoring system.
This score might allow us to differentiate
between responders and non-responders to nonsurgical treatment after an FTLPD. PISS has six
factors. They are age, the bilaterality of the
instability, trochlear dysplasia severity, patella
alta, tibial tuberosity-trochlear groove (TT-TG)
distance, and patellar tilt. Jaquith and Parikh [28]
also presented a predictive score to calculate the
risk of recurrence. According to these authors,
trochlear dysplasia, skeletal immaturity (age of
14 years or less), Caton-Deschamps index
(CDI) > 1.45, and a history of contralateral
patellar dislocation were all significant risk factors for recurrence after an FTLPD. The presence
of all 4 risk factors had a predicted recurrence
risk rate of 88%. The presence of any 3 risk
factors had a predicted risk of about 75% and the
presence of any 2 risk factors had a predicted risk
of about 55%. Arendt and colleagues [29] evaluated sixty-one patients out of 145 with FTLPD
that had had a recurrent dislocation within 2
years of follow-up. Stepwise logistic regression
analysis demonstrated that skeletal immaturity,
the sulcus angle and Insall-Salvati ratio were
significant predictors of redislocation. The cut
points were determined to be a sulcus angle
154° and Insall-Salvati ratio 1.3. The probability of redislocation was of 5.8% with no
factors present and 22.7% with any 1 factor
present, increasing to 78.5% if all 3 factors were
present. Natural history studies of recurrent lateral instability show that the mean time to
recurrence is 3.7 years [29]. For this reason,
Hevesi and colleagues [30] chose a minimum
follow-up time of 4 years in their study, in contrast to previous studies [25–27]. They developed
a model to predict the risk of recurrence after an
256
FTLPD that is entitled “Recurrent Instability of
the Patella Score” (RIP Score). This score is
based on age (<25 years old), skeletal immaturity, trochlear dysplasia (A-D according to the
Dejour classification) and TT-TG/PL ratio
0.5 (TT-TG, tibial tubercle to trochlear groove
distance; PL patellar length). This score gives a
maximum of 5 points and a minimum of zero; if
the patient is under 25 years of age, the score will
be 2; the remaining items score 1. According to
the score obtained, the risk of recurrent instability is low (0−1 points), intermediate (2−3) or
high (4−5). In low-risk patients, there were no
further dislocation episodes at 1, 2, 5, and 10
years. In intermediate-risk patients the percentages of recurrent instability-free patients were 83,
72, 69 and 69% respectively. These figures are
84, 62, 34 and 21% in the same time periods in
the high-risk group. In 2020, Huntington and
colleagues demonstrated in a systematic review
with meta-analysis that the key risk factors for
recurrence were younger age, open physes, trochlear dysplasia, radiographic patella alta, and an
elevated TT-TG distance, while sex and MPFL
injury pattern were not predictive. The presence
of 3 factors increased the recurrence risk to over
70% [31]. In 2022, Wierer and colleagues [32]
proposed the “The Patellar Instability Probability
Calculator” to estimate the individual risk of
early recurrence after FTLPD. They have shown
that at 16 years of age with a FTLPD, trochlear dysplasia (Dejour type B-D; lateral trochlear inclination 12°) and history of
contralateral instability are significant risk factors
for recurrent lateral patellar dislocation within 2
years after FTLPD. The prediction accuracy
including these 3 risk factors was 79%. However,
patella alta, an increased TT-TG distance, and
patellar tilt did not have an association with
increased recurrence rates or an influence on
prediction accuracy of recurrent lateral patellar
dislocation either.
In summary, predictive models can help us to
predict which patients are most likely to redislocate after FTLPD treated conservatively. This
approach helps us with our decision-making for
V. Sanchis-Alfonso et al.
the optimum treatment of a patient with an
FTLPD. It can also be useful when we want to
inform patients and their families about the
prognosis after an FTLPD.
2.3 Patient’s Goals–Return to Sports
at a Pre-Injury Level
When we consider a therapeutic indication, be it
surgical or non-surgical, it must not only be
based on the best available scientific evidence,
pathophysiological arguments and predictive
models, but also on the patient´s expectations
and wishes. These three elements constitute the
three cornerstones of evidence-based medicine.
There are patients for whom sports is important
for leisure or professional reasons. We have to
offer the treatment with the greatest guarantees of
making it possible for them to return to their
sports activity of choice.
In 2017 Magnussen and colleagues [6] showed
that those patients in whom there is no recurrence
of the dislocation after non-surgical treatment of
an acute dislocation are quite limited by this injury
up to three years after the FTLPD. Interestingly,
patient-reported outcomes of non-surgical treatment without recurrence are not different from
those non-operated with dislocation recurrence
[6]. It is important to note that only 26.4% of
patients without further dislocations were able to
practice their sport again with no limitations at a
pre-injury level [6]. These studies demonstrate
that the absence of recurrent dislocation as an
isolated finding may not be sufficient to evaluate
the outcomes of a patient after an FTLPD. In
contrast, Regalado and colleagues [11] showed, in
2014, that 80% of adolescent patients who were
treated surgically after an FTLPD attain an
excellent result with regard to the return to sports
at a pre-injury level. This percentage was only
47% for patients who were treated conservatively.
These studies suggest that surgery increases the
likelihood of returning to sports at a pre-injury
level compared with a non-surgical treatment for
athletic adolescents.
Evolving Management of Acute Dislocations of the Patella
2.4 Economic Decision Model
Nwachukwu and colleagues [33] used a costeffectiveness model to compare non-surgical
treatment to surgical treatment of recurrent dislocations and surgical treatment done immediately after an FTLPD. In their analysis, the
authors describe both the direct and the indirect
costs of each therapeutic strategy. Direct costs
include direct medical costs, cost of surgery, and
physical therapy. Indirect costs were calculated
based on the lost productivity associated with
caregiver (parental) work absenteeism. Effectiveness was expressed in quality-adjusted life
years (QUALYs). The authors found that both
immediate surgical treatment as well as delayed
surgery are cost-effective treatment options.
However, with a perspective of 10 years,
immediate surgery offers the most QUALY
gains. As a result, the conclusion was that early
operative intervention was the most cost-effective
treatment. These findings are important considerations for therapeutic decision-making when
we see a patient with an FTLPD.
3
Take Home Messages
– The FTLPD patient may benefit from operative intervention more often than has generally been indicated previously.
– Non-operative management is recommended
in patients with an FTLPD with no significant
risk factors for recurrence and no osteochondral fracture.
– The isolated MPFL repair may not be adequate for stabilizing the patella.
– The risk of recurrent dislocation after an
FTLPD is increased by a number of factors
and to a greater extent, when multiple risk
factors are present. Published stratification
models allow for an evaluation of the individual risk profile. Low-risk patients may be
treated non-surgically while surgery should be
considered for high-risk patients. Moreover,
we should include individual preferences
(patient´s goals such as sports) in the decision
protocols.
257
– The optimization of the treatment of the
FTLPD will improve short-term disability
from the dislocation and will reduce the longterm risk of PFOA from repeated chondral
injuries.
– High quality clinical trials are obviously
needed to further refine what FTLPD patients
would benefit from surgical intervention and
which patients can be managed nonoperatively.
References
1. Gravesen KS, Kallemose T, Blønd L, et al. High
incidence of acute and recurrent patellar dislocations:
a retrospective nationwide epidemiological study
involving 24.154 primary dislocations. Knee Surg
Sports Traumatol Arthrosc. 2018;26(4):1204−9.
2. Sanders TL, Pareek A, Johnson NR, et al. Patellofemoral arthritis after lateral patellar dislocation: a
matched population-based analysis. Am J Sports
Med. 2017;45(5):1012–7.
3. Stanitski CL, Paletta GA Jr. Articular cartilage injury
with acute patellar dislocation in adolescents. Arthroscopic and radiographic correlation. Am J Sports
Med. 1998;26(1):52–5.
4. Salonen EE, Magga T, Sillanpaa PJ, et al. Traumatic
patellar dislocation and cartilage injury: a follow-up
study of long-term cartilage deterioration. Am J
Sports Med. 2017;45:1376–82.
5. Mochizuki T, Tanifuji O, Watanabe S, et al. The
majority of patellar avulsion fractures in first-time
acute patellar dislocations included the inferomedial
patellar border that was different from the medial
patellofemoral ligament attachment. Knee Surg
Sports Traumatol Arthrosc. 2020;28(12):3942–8.
6. Maggnussen RA, Verlage M, Stock E, et al. Primary
patellar dislocations without surgical stabilization or
recurrence: how well are these patients really doing?
Knee Surg Sports Traumatol Arthrosc. 2017;25
(8):2352–6.
7. Camanho GL, Viegas Ade C, Bitar AC, et al.
Conservative versus surgical treatment for repair of
the medial patellofemoral ligament in acute dislocations of the patella. Arthroscopy. 2009;25(6):620–5.
8. Sillanpää PJ, Mattila VM, Mäenpää H, et al. Treatment with and without initial stabilizing surgery for
primary traumatic patellar dislocation. A prospective
randomized study. J Bone Joint Surg Am. 2009;91
(2):263–73.
9. Bitar AC, Demange MK, D’Elia CO, et al. Traumatic
patellar dislocation: nonoperative treatment compared with MPFL reconstruction using patellar
tendon. Am J Sports Med. 2012;40(1):114–22.
258
10. Bitar AC, D’Elia CO, Demange MK, et al. Randomized prospective study on traumatic patellar dislocation: conservative treatment versus reconstruction of
the medial patellofemoral ligament using the patellar
tendon, with a minimum of two years of follow-up.
Rev Bras Ortop. 2015;46(6):675–83.
11. Regalado G, Lintula H, Kokki H, et al. Six-year
outcome after non-surgical versus surgical treatment
of acute primary patellar dislocation in adolescents: a
prospective randomized trial. Knee Surg Sports
Traumatol Arthrosc. 2016;24(1):6–11.
12. Nikku R, Nietosvaara Y, Kallio PE, et al. Operative
versus closed treatment of primary dislocation of the
patella. Similar 2-year results in 125 randomized
patients. Acta Orthop Scand. 1997;68(5):419−23.
13. Buchner M, Baudendistel B, Sabo D, et al. Acute
traumatic primary patellar dislocation: long-term
results comparing conservative and surgical treatment. Clin J Sport Med. 2005;15(2):62–6.
14. Christiansen SE, Jakobsen BW, Lund B, et al.
Isolated repair of the medial patellofemoral ligament
in primary dislocation of the patella: a prospective
randomized study. Arthroscopy. 2008;24(8):881–7.
15. Palmu S, Kallio PE, Donell ST, et al. Acute patellar
dislocation in children and adolescents: a randomized
clinical trial. J Bone Joint Surg Am. 2008;90
(3):463–70.
16. Apostolovic M, Vukomanovic B, Slavkovic N, et al.
Acute patellar dislocation in adolescents: operative
versus nonoperative treatment. Int Orthop. 2011;35
(10):1483–7.
17. Petri M, Liodakis E, Hofmeister M, et al. Operative
vs conservative treatment of traumatic patellar dislocation: results of a prospective randomized controlled
clinical trial. Arch Orthop Trauma Surg. 2013;133
(2):209–13.
18. Pagliazzi G, Napoli F, Previtali D, et al. A metaanalysis of surgical versus nonsurgical treatment of
primary patella dislocation. Arthroscopy. 2019;35
(8):2469–81.
19. Migliorini F, Driessen A, Quack V, et al. Surgical
versus conservative treatment for first patellofemoral
dislocations: a meta-analysis of clinical trials. Eur J
Orthop Surg Traumatol. 2020;30(5):771–80.
20. Fu Z, Zhu Z, Chen H, et al. Surgical treatment is
better than non-surgical treatment for primary patellar dislocation: a meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg. 2020;140
(2):219–29.
21. Askenberger M, Bengtsson E, Ekstrom W, et al.
Operative repair of medial patellofemoral ligament
injury versus knee brace in children with an acute
first-time traumatic patellar dislocation: a randomized
controlled trial. Am J Sports Med. 2018;46
(10):2328–40.
V. Sanchis-Alfonso et al.
22. Pedowitz JM, Edmonds EW, Chambers HG, et al.
Recurrence of patellar instability in adolescents
undergoing surgery for osteochondral defects without
concomitant ligament reconstruction. Am J Sports
Med. 2019;47(1):66–70.
23. Gurusamy P, Pedowitz JM, Carroll AN, et al. Medial
patellofemoral ligament reconstruction for adolescents with acute first-time patellar dislocation with an
associated loose body. Am J Sports Med. 2021;49
(8):2159–64.
24. Vogenberg FR. Predictive and prognostic models:
implications for healthcare decision-making in a
modern recession. Am Health Drug Benefits. 2009;2
(6):218–22.
25. Lewallen LW, McIntosh AL, Dahm DL. Predictors
of recurrent instability after acute patellofemoral
dislocation in pediatric and adolescent patients. Am J
Sports Med. 2013;41(3):575–81.
26. Askenberger M, Janarv PM, Finnbogason T, et al.
Morphology and anatomic patellar instability risk
factors in first-time traumatic lateral patellar dislocations: a prospective magnetic resonance imaging
study in skeletally immature children. Am J Sports
Med. 2017;45(1):50–8.
27. Balcarek P, Oberthur S, Hopfensitz S, et al. Which
patellae are likely to redislocate? Knee Surg Sports
Traumatol Arthrosc. 2014;22:2308–14.
28. Jaquith BP, Parikh SN. Predictors of recurrent
patellar instability in children and adolescents
after first-time dislocation. J Pediatr Orthop.
2017;37:484–90.
29. Arendt EA, Askenberger M, Agel J, et al. Risk of
redislocation after primary patellar dislocation: a
clinical prediction model based on magnetic resonance imaging variables. Am J Sports Med. 2018;46
(14):3385–90.
30. Hevesi M, Heidenreich MJ, Camp ChL, et al. The
recurrent instability of the patella score: a statistically
based model for prediction of long-term recurrence
risk after first-time dislocation. Arthroscopy. 2019;35
(2):537–43.
31. Huntington LS, Webster KE, Devitt BM, et al.
Factors associated with an increased risk of recurrence after a first-time patellar dislocation: a systematic review and meta-analysis. Am J Sports Med.
2020;48(10):2552–62.
32. Wierer G, Krabb N, Kaiser P, et al. The patellar
instability probability calculator: a multivariate-based
model to predict the individual risk of recurrent
lateral patellar dislocation. Am J Sports Med.
2022;50(2):471–7.
33. Nwachukwu BU, So C, Schairer WW, et al. Economic decision model for first-time traumatic patellar
dislocations in adolescents. Am J Sports Med.
2017;45(10):2267–75.
How to Deal with Chronic Patellar
Instability
Vicente Sanchis-Alfonso and Erik Montesinos-Berry
1
Introduction
Patellar displacement is limited by passive retinacular tethers and the chondral/bony geometry
of the trochlea and patella. Together, they guide
the patella into the trochlear groove and keep it
engaged in the groove throughout knee range-ofmotion [1]. Patellar instability is defined as a
symptomatic deficiency of the abovementioned
constraints, either alone or in combination.
Thereby, the patella can escape partially or
completely from its normal position with respect
to the femoral trochlea under the influence of a
displacing force [1]. Out of all the anatomic
factors that play a role in the pathogenesis of
patellar instability, the most important are the
medial patellofemoral ligament (MPFL) and the
trochlea. Currently, no one doubts that the major
soft-tissue stabilizer of the patella is the MPFL.
Moreover, trochlear dysplasia is the main risk
anatomic factor for lateral patellar instability [2–
5]. However, Diederichs and colleagues [6] have
recently analyzed rotational limb alignment in
patients with non-traumatic patellar instability
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
E. Montesinos-Berry
ArthroCentre–Agoriaz, Riaz and Clinique CIC
Riviera, Montreux, Switzerland
and in controls using Magnetic resonance imaging (MRI). They have found that patellar instability patients have greater internal femoral
rotation, greater knee rotation, and a tendency to
genu valgum in comparison to healthy controls.
They conclude that rotational malalignment may
be a primary risk factor in patellar instability that
has so far been underestimated.
As there are many types of patellar instability,
it is necessary to be familiar with all of them to
provide the right treatment. To classify the
patellar instability, several factors must be considered. The factors are the direction of the
instability and degree of knee flexion at which
there is instability. In terms of the direction of the
instability, it could be lateral, medial (usually
iatrogenic) or multidirectional (lateral and medial). Based on the degree of flexion, it could be
lateral instability in the first 30° (the most common type of patellar instability), lateral instability
in the first 30° and beyond 30° and lateral
instability in flexion. Then, we must consider the
pathoanatomic variables that favor instability.
Here, one sees that there are many varieties of
instability and, therefore, several subpopulations
of patients with chronic patellar instability. Lateral instability is found with or without the
concomitant risk factors for instability like trochlear dysplasia, patella alta, and rotational
malalignments such as medial femoral torsion or
external tibial torsion.
Therefore, not all patellar instabilities are
equal. The etiology of the disorder is
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_18
259
260
V. Sanchis-Alfonso and E. Montesinos-Berry
multifactorial. Knowing this, a clear understanding of the cause of instability is crucial for
appropriate surgical treatment. The goal of this
chapter is to identify how to best treat patellar
instability to achieve good outcomes and prevent
future patellofemoral osteoarthritis (PFOA).
2
Lateral Patellar Instability During
the Early Arc of Knee Flexion
It is during the early arc (0°–30°) knee flexion
when most cases of lateral patellar instability
typically occur. It accounts for 70% of the cases
of lateral instability in our series. Moreover, the
vast majority of patients who have chronic lateral
patellar instability also have cartilage damage in
their patellofemoral joint (PFJ).
A
Fig. 1 A Medial knee anatomy. Adductor tubercle (AT),
medial patellofemoral ligament (MPFL), medial quadriceps tendon femoral ligament (MQTFL), superficial
medial collateral ligament (sMCL) and vastus medialis
obliquus (VMO). B Articular-sided view of proximal
medial patellar restraints. Attachments of the MPFL on
2.1 What to Do–Rationale
Various anatomic and biomechanical studies
have shown that the MPFL (Fig. 1) is the most
important limitation to lateral patellar displacement between 0° and 30° of knee flexion [7–9].
In this subset of patients with lateral patellar
instability, the MPFL deficiency is thought to be
the all-important lesion [10].
The present surgical approach, in this subgroup
of patients who have had a minimum of two
documented patellar dislocations, is to stabilize
the patella by means of an anatomic MPFL
reconstruction (MPFLr). In that reconstruction, a
mini-open technique and a graft that is stronger
that the native MPFL are employed [11]. This
approach is used to compensate for the underlying
predisposing factors to patellar instability [11].
B
the patella, and the MQTFL on the quadriceps tendon.
(“Republished with permission of Springer Nature BV,
from Recognition of evolving medial patellofemoral
anatomy provides insight for recognition, Tanaka MJ,
et al., 27, 2537–2550, 2019; permission conveyed through
Copyright Clearance Center, Inc.”)
How to Deal with Chronic Patellar Instability
The decisive steps to guarantee a successful
outcome after MPFLr are the suitable graft
positioning on the femur and the right tension on
the graft [11]. A lot less attention has been given
to the patellar attachment of the MPFL than to
the femoral attachment [11].
According to Mochizuki and colleagues [12]
the MPFL mainly attaches to the vastus intermedius tendon (Fig. 1). Therefore, some surgeons propose a medial quadriceps tendon
femoral ligament (MQTFL) reconstruction
(Fig. 1) [13].
261
Not only does the MPFLr prevent further
patellar dislocation but it might also detain the
progression of knee osteoarthritis [15]. With
second-look arthroscopy, the effect of MPFLr on
articular cartilage in the PFJ showed that the
status of the patellofemoral chondral was only
modified at the central ridge of the patella [16].
Consequently, it is not necessary to treat chondral lesions in most cases even though it is a
good idea to remove loose bodies in some
(Figs. 3 and 4).
3
2.2 The Treatment of Associated
Chondral Lesions
If the patellar instability has gone on for a long
time, the probability and the extent of patellofemoral chondral injuries will be greater [14]. Of
patients with recurrent lateral patellar instability,
58% have patellar lesions and trochlear lesions
have been observed in 13% (Fig. 2) [14].
Fig. 2 The severity of
chondral injury in patients
with lateral patella instability
is highly variable. Even in the
most severe cases the isolated
MPFLr is sufficient to
eliminate the pain
Lateral Patellar Instability
Persisting Beyond 30° of Knee
Flexion
This condition accounts for 25% of the cases of
lateral instability in our series. Lateral patellar
instability beyond 30° of knee flexion suggests
severe trochlear dysplasia (grade C or D) or a
pathological femoral anteversion associated with
a deficient MPFL (Fig. 5). It is not enough to
262
V. Sanchis-Alfonso and E. Montesinos-Berry
Fig. 3 Loose body in a
patient with lateral patellar
instability
Fig. 4 Loose bodies and
severe patellar chondropathy
in a patient with chronic
lateral patellar instability. The
isolated MPFLr was sufficient
to eliminate the pain
have an isolated MPFL or a MQTFL reconstruction to achieve good clinical results when
treating this type of instability. The predisposing
anatomic factors for instability should be corrected along with the MPFLr. Step one is to
correct the patellofemoral maltracking (J-sign) to
neutralize the lateral displacing forces. In step
two, only when the patellofemoral joint is realigned, do we stabilize the joint. That means to
restore the passive restraining elements to get
good patellofemoral balance. This restoration is
achievable by doing an MPFL or an MQTFL
reconstruction. One should never use the
MPFL/MQTFL reconstruction to pull the patella
medially because it will give rise to an overload
on the PFJ and cause future PFOA.
3.1 The Medial and Anteromedial
Tibial Tuberosity Transfer
According to several authors, a medialization of
the tibial tuberosity (TT) must be done when the
TT-TG distance is more than 20 mm [17]. However, there is not any strong evidence in the medical literature to support this recommendation. The
TT-TG distance depends on weight-bearing and
joint size [18–20]. Moreover, the intra and interobserver reliability for TT-TG distance measurements is seen less in patients with severe trochlear
dysplasia when compared to those with a lowgrade trochlear dysplasia [20]. Some authors have
also demonstrated that there are no differences in
TT-TG distance between the stable and the
How to Deal with Chronic Patellar Instability
263
Fig. 5 Lateral patellar instability persisting beyond 30° of knee flexion in a patient with pathological femoral
anteversion
unstable knee in patients with unilateral patellar
instability [21]. Other authors have not found any
differences in the outcomes of isolated MPFL
reconstructions in the setting of a TT-TG
index >20 mm when compared to those with a
TT-TG distance <20 mm [22].
As a result of what was previously described,
prudence should be exercised when interpreting
the TT-TG distance. In other words, the TT-TG
distance alone is not a good enough indicator for
a TT osteotomy. Other factors ought to be considered. Examples include a prominent J-sign,
the circumstances around the initial and posterior
dislocation episodes (traumatic vs atraumatic),
bilaterality, level of activity as well as patient
expectations.
An anteromedialization of the TT (Fulkerson
osteotomy) for patients with distal patellar articular damage could be indicated. This will not only
correct the maltracking, but it will also unload the
distal pole of the patella and consequently reduce
or eliminate the anterior knee pain.
3.2 Patellar Distalization
by Osteotomy or Patellar
Tendon Imbrication
According to several authors, we must perform a
distalization of the TT (Fig. 6) when the CatonDeschamps index is more than 1.2 [17]. However, there is no strong evidence to support this
recommendation in the medical literature. Controversy exists as to how to measure patellar
height [23]. Moreover, TT distalization is not a
panacea. TT distalization always implies some
degree of medialization [24]. Additionally, distalization is risky in patients with chondral
lesions of the distal pole of the patella because it
provokes an overload of this area in initial flexion. Yang and colleagues [25] have demonstrated
that excessive patellar distalization can cause
increased patellofemoral contact pressures during
early flexion at 0° and 10°. Finally, we must take
into consideration that MPFLr brings about a
descent of the patella [26, 27].
264
V. Sanchis-Alfonso and E. Montesinos-Berry
Fig. 6 Patella alta in a patient with lateral patellar
instability. A distalization osteotomy of the anterior tibial
tubercle followed by a double bundle MPFLr, using an
anatomic femoral tunnel. 5 years after his surgery he is
still a professional dancer. The result of his surgery is
excellent despite a patellar tilt of 29°, a severe trochlear
dysplasia and a TT-TG distance of 33 mm
A pathological ratio or index is not enough to
indicate a tibial tubercle distalization. A prominent J-sign, the circumstances relative to the
initial and posterior dislocation episodes (traumatic vs atraumatic), bilaterality, the level of
activity, and patient expectations are other factors
that should be taken into consideration. Patellar
tendon imbrication is a useful alternative to
osteotomy in the skeletally immature patient.
D) was considerably more frequent in the surgical failure group (89%) than in the control group
(21%) [2]. Even so, no statistical differences in
the patellar height ratio (Insall-Salvati index) or
the TT-TG distance were observed between the
two groups [2]. Trochlear dysplasia seems to be
an important risk factor for the failure of operative stabilization of the recurrent patellar dislocation [2]. There is a correlation between high
degrees of trochlear dysplasia and a poor clinical
outcome. This is because the MPFL graft may be
overloaded because of the increased instability
present in dysplastic situations [3]. A more tailored operative procedure along with the MPFLr
and a trochleoplasty would be advisable.
When there are cases with high degrees of
trochlear dysplasia, a trochleoplasty should be
considered. An acceptable revision option for the
surgical treatment of patients with persistent
3.3 Trochleoplasty
Trochlear dysplasia seems to be the most
important of all the main risk factors for the
development of chronic lateral patellar instability
[2–5]. Incidentally, in an analysis of failed surgery for patellar instability, it has been shown
that a severe trochlear dysplasia (Dejour type B-
How to Deal with Chronic Patellar Instability
patellar dislocation and high-grade trochlear
dysplasia is the sulcus-deepening trochleoplasty
[5]. Trochleoplasty is a widely used and reliable
surgical technique to treat patellofemoral instability in patients who have a dysplastic trochlea.
Nonetheless, while improved stability can be
predicted, pain is less predictable and could even
increase after surgery. The overall results depend
on the type of dysplasia, types B and D having a
significantly better clinical outcome [28]. With
reference to trochleoplasty, there is concern
about the long-term consequences to healthy
cartilage. Even so, the vast majority of patients,
candidates for trochleoplasty, present severe
chondropathy. However, many patients with
trochlear dysplasia will go on to develop PFOA
at some point in the future [17].
When assessing the indications for trochleoplasty, caution is called for. In our clinical
experience, it is a valuable tool only in a small
subset of patients with lateral patellar instability.
This is the case when there is a severe trochlear
dysplasia, when the patella dislocates not only
during the first 30° of knee flexion but also at
higher degrees of knee flexion, and when there is
a positive J-sign. In a consensus statement from
the AOSSM/PFF about patellar instability, the
Deepening trochleoplasty is considered when all
the following are present: a positive J-sign, a
boss or 5 mm supratrochlear spur, and a convex
proximal trochlea [1].
In a systematic review with a meta-analysis
published in 2021, Leclerc and colleagues [29]
determined that trochleoplasty is an effective
surgical procedure to stabilize the patella. The
deepening trochleoplasty, described by Dejour,
was the most effective among all the trochleoplasty techniques with only 1 recurrence out of
349 knees (0.28%). Nevertheless, we should
point out that the trochleoplasty in general is not
a problem-free technique. Leclerc and colleagues
[29] have shown that patellar instability without
dislocation occurred in 82 out of 754 knees (8%
[95% CI: 3–14%]), PFOA in 117 out of 431
knees (27%), knee stiffness in 59 out of 642
knees (7% [95% CI: 3–12%]) and the need for
subsequent surgery in 151 out of 904 knees
265
(17%). Therefore, we must be cautious when we
decide to perform a trochleoplasty as the surgical
procedure.
3.4 The Rotational Femoral
Osteotomy And The
Femoral Varization
Osteotomy Versus Growth
Modulation
Lateral patellar instability originates from a
deficient MPFL that may have become incompetent due to trochlear dysplasia, patella alta,
genu valgum, abnormal limb torsion or a combination of these factors [30]. The MPFL might
not be strong enough to withstand the normal
lateral pull of the quadriceps when the trochlea is
dysplastic. In the same way, when abnormal limb
torsion is present, the lateral displacement force
acting upon the patella will be increased, and the
ligament will most likely fail. This leads to lateral
patellar instability (Fig. 7) [30]. Kaiser and colleagues [31] highlight the importance of internal
femoral torsion in the etiopathogenesis of lateral
patellar instability. They have shown that 20° of
increased internal femoral torsion is a significant
risk factor for patellar instability in a knee with
an intact MPFL. However, with an insufficient
MPFL, 10° of increased internal femoral torsion
is a significant risk factor for patellar instability.
When the limb is realigned, the lateral displacement force acting upon the patella will be
decreased, which eliminates lateral patellar
instability [30]. Excessive external tibial torsion
as well as a pathological femoral anteversion
have been correlated with chronic patellofemoral
instability. We consider rotational osteotomies
along with an MPFLr in those cases with severe
rotational deformity (femoral anteversion >40°,
external tibial torsion > 40°) and a positive Jsign. Milinkovic and colleagues [32] have shown
that a high-grade J-sign and an increased body
mass index (BMI) are the most relevant parameters influencing the quality of life in patients
with lateral patellar instability measured using
the Banff Patella Instability Instrument (BPII 2.0
266
V. Sanchis-Alfonso and E. Montesinos-Berry
Fig. 7 Lateral patellar instability persisting beyond 30°
of knee flexion. Haglund excavation on the patella with
sclerotic edges in a patient with valgus and left femoral
anteversion. According to Robert A. Teitge, MD abnormal sclerotic joint surfaces suggests abnormal loading.
A rotational supracondylar femoral osteotomy was performed. After osteotomy, coronal plane alignment was
evaluated. A normal mechanical axis is near the medial
tibial spine, not in the middle of the knee joint
score). Nelitz and colleagues [33] as well as Lee
and colleagues [34] have shown that femoral
rotational osteotomies may result in an increment
of knee valgus. Therefore, the assessment of
coronal plane alignment is crucial after a femoral
rotational osteotomy performed for treating
patellar instability.
In the author´s clinical practice, knee valgus is
often associated with femoral torsional abnormalities in cases of chronic lateral patellar
instability. If there is genu valgum, the treatment
will depend upon the stage of maturation of the
patient. In patients with an open physis, a therapeutic option is growth modulation (hemiepiphysiodesis). In skeletally mature patients, a
therapeutic option to correct the valgus is the
open or closed osteotomy of the distal femur. In
skeletally mature patients with genu valgum
( zone II or a mechanical lateral distal femoral
angle (mLDFA) <83º) and patellar instability
(Fig. 8), Palmer and colleagues [35] recommend
performing a distal femoral osteotomy. In both
cases, that is to say, in skeletally immature and
mature patients these authors proposed the
MPFL reconstruction as a second surgery, since
in 80% of the cases with the genu valgum correction it is sufficient to resolve the patellar
instability. The first study in which the use of the
femoral varus osteotomy is described in patients
with lateral patellar instability and genu valgum
dates back to 2009 [36]. The objective of the
varus osteotomy is to reduce the lateral vector
applied to the patella. In a systematic review with
a meta-analysis published in 2019 assessing the
outcomes of a distal femoral varus osteotomy
performed to treat patellar instability in patients
with genu valgum, Tan and colleagues [37]
concluded that this type of osteotomy was useful
in the management of this subset of patellar
instability patients. The problem is that out of the
5 studies analyzed in this systematic review, in 4
of them the varus osteotomies are performed
along with other associated procedures. For this
reason, we cannot know for sure if the good
clinical result achieved with this particular procedure is due to the varus osteotomy or to any of
the other associated surgeries, or even to all the
surgical procedures as a whole. The only study of
the 5 included in this systematic review in which
the osteotomy is analyzed as an isolated
How to Deal with Chronic Patellar Instability
267
Fig. 8 Evaluation of the magnitude of the genu valgum with the quadrant method
procedure was published by Wilson and colleagues in 2018 [38]. These authors [38]
observed a disappearance of lateral patellar
instability in most of the cases after an isolated
osteotomy of the distal femur without any other
associated surgical procedures. They analyzed 10
patients, out of which 2 (20%) presented new
episodes of instability. This shows how important genu valgum is in the etiopathogenesis of
lateral patellar instability. Therefore, a logical
approach would be to treat genu valgum and in a
second procedure, if necessary, do an MPFLr.
On the contrary, in the other 4 studies no recurrences of instability are reported. This systematic
review also evaluates the performance of a
closing wedge osteotomy or an opening wedge
osteotomy. The results obtained with both types
of osteotomies are similar. Nevertheless, the
authors draw attention to the fact that the opening
wedge osteotomy lowers the Caton-Deschamps
index, something that did not occur with the
closing wedge osteotomy. The clinical relevance
of this finding is that patients with a normal
height patella or with a low-riding patella may
profit from a closing wedge osteotomy in order to
prevent patella infera. On the other hand, patients
with a high-riding patella, which is a well-known
risk factor for the appearance of lateral patellar
instability, may profit from an opening wedge
osteotomy because it will distalize the patella.
Therefore, it is essential to evaluate preoperatively the height of the patella before deciding
between a closing or opening wedge osteotomy.
3.5 Additional Surgery on the Lateral
Retinaculum
Isolated lateral retinacular release (LRR) is not
recommended to treat patellar instability [1].
Isolated Lateral release or lengthening is only
necessary in rare cases. Biomechanical studies by
Amis and Merican [39] have shown that the
lateral retinaculum (LR) actually contributes to
268
resisting lateral patellar displacement. It is a
restraint on lateral patellar displacement. Therefore, lateral patellar instability increases after
LRR. Moreover, to guide the patella towards the
trochlear sulcus during the first degrees of knee
flexion, both the MPFL and the LR must interplay in a harmonious way. Both ligaments
behave similarly to the reins of a horse. Both
reins must have some degree of tension. They are
not very tense but they are not loose either. If one
of the reins is completely loose the horse is
inclined towards the opposite direction, as occurs
in the patella. This will provoke a patellofemoral
imbalance that could be responsible for iatrogenic anterior knee pain.
In cases with severe patellar tilt where, in
theory, we could consider LRR or lengthening,
we always find severe trochlear dysplasia. In
these cases, trochleoplasty automatically relaxes
the deep layer of the LR and therefore LRR or
lengthening can be avoided. Likewise, we must
avoid LRR in trochlear dysplasia. An LRR in a
patient with trochlear dysplasia will provoke
medial patellar instability (MPI) [40]. Our advice
is not to perform an LRR but a lengthening. It
has the same effect as the LRR relative to the
elimination of hypercompression on the lateral
side. Moreover, LR lengthening is an individually adapted technique. Finally, it prevents the
secondary complications of LRR such as MPI.
A surgical procedure on the LR is an intraoperative decision [41]. To decide, it is helpful to
perform the intraoperative patella tilt test [41].
V. Sanchis-Alfonso and E. Montesinos-Berry
This is done by putting a transverse K wire
through the proximal patella, from medial to
lateral. The K wire must be parallel to the operating table with the knee in full extension and at
20° of flexion [41]. If the K wire is tilted (positive test), one should consider doing a lateral
patellar retinaculum lengthening or think about
an LRR.
4
Fixed Lateral Patellar Instability
in Knee Flexion
This type of lateral patellar instability is the least
frequent. It accounts for 5% of the cases of lateral
instability in our series. It may be congenital or
acquired. In this type of instability, the patella is
centered or almost centered on the femoral trochlea when the knee is in extension or almost in
extension (Figs. 9, 10 and 11). But in flexion, the
patella is always dislocated and making contact
with the lateral surface of the external femoral
condyle (Figs. 9, 10 and 11).
The natural history of this type of instability
consists in the development of severe trochlear
dysplasia and finally PFOA (Figs. 12 and 13).
Therefore, an early diagnosis is important as is
early surgical correction so that the trochlea can
develop correctly. In this way, late-onset sequelae, including osteoarthritis can be held back.
The pathophysiology of this type of lateral
instability is diametrically opposed to the two
types analyzed previously. The quadriceps is
Fig. 9 Fixed lateral patellar instability in knee flexion. The patella is well-centered in extension, but in flexion is
dislocated and cannot be reduced to the midline due to severe quadriceps retraction
How to Deal with Chronic Patellar Instability
A
269
C
B
Fig. 10 Fixed lateral patellar instability in knee flexion.
The patella is well-centered A on the femoral trochlea
when the knee is in extension. In flexion, the patella is
dislocated and contacting B, C the lateral surface of the
external femoral condyle. (A, B. Reused with permission
Fig. 11 Fixed lateral patellar
instability in knee flexion. (C,
D, E. Reused with permission
from Baishideng Publishing
Group Inc. From SanchisAlfonso V, et al. Failed
medial patellofemoral
ligament reconstruction:
Causes and surgical strategies.
World J Orthop, 2017; 8(2):
115–129)
from Baishideng Publishing Group Inc. From SanchisAlfonso V, et al. Failed medial patellofemoral ligament
reconstruction: Causes and surgical strategies. World J
Orthop, 2017; 8(2): 115–129)
A
C
short and is displaced laterally (Fig. 14) [42].
Therefore, the extensor mechanism becomes a
flexor and external rotator of the knee. Moreover,
a flat lateral condyle is seen around the sulcus
B
D
E
terminals [43]. These factors collectively lead to
an MPFL insufficiency. The patella is permanently dislocated in flexion and cannot be
reduced manually.
270
V. Sanchis-Alfonso and E. Montesinos-Berry
Fig. 12 Fixed lateral patellar instability in knee flexion. Severe trochlear dysplasia and severe PFOA
Fig. 13 Fixed lateral patellar instability in knee flexion.
Severe PFOA. (Republished with permission of AME
Publishing Company. From V Sanchis-Alfonso, Treating
complications of operative management for patellofemoral pain, Ann Joint, 3:27, 2018)
Currently, the standard surgical approach in
patients with fixed lateral patellar instability in
knee flexion involves Lateral retinaculum
lengthening, the release of the vastus lateralis
from the superolateral border of the patella, and
Quadriceps tendon lengthening on the coronal
plane after isolating the central tendon of the
quadriceps from the vastus medialis and lateralis
(Fig. 15). Afterwards, a side-to side repair of the
quadriceps tendon is performed (Figs. 15). Then,
a side-to side repair of the vastus lateralis and
vastus medialis is carried out. If needed, the
lateral condyle may be raised. The final step is an
MPFLr. In order to calculate the length necessary
for quadriceps tendon lengthening it is essential
to achieve 90º of flexion or more by maintaining
the patella reduced. Once this objective has been
achieved, end-to-end suture of the quadriceps
tendon is performed. We use a brace postoperatively for 6 weeks with weight bearing
How to Deal with Chronic Patellar Instability
271
Fig. 14 Fixed lateral patellar instability in knee flexion. The quadriceps is short and displaced laterally with knee
flexion
immediately after surgery depending on the tolerance. The brace is locked in 0º of knee extension for ambulation. At the third week, the brace
is unlocked allowing flexion increments from 10
to 20º per week. The return to full activity varies
from 6 to 12 months.
In 2019 Song and colleagues [44] presented a
novel surgical technique to lengthen the extensor
mechanism of the knee in skeletally mature
patients with fixed lateral patellar instability in
knee flexion. The authors perform a tibial
tubercle proximalization (“bony release”) associated with a lateral retinaculum release, tibial
tubercle medialization and a MPFL reconstruction. The objective is to avoid the possibility of
extensor lag during the postoperative rehabilitation after quadriceps lengthening. This technique
allows early postoperative rehabilitation. However, a possible problem with this surgical technique is the patella alta, which is a well-known
risk factor for patellar instability. Nevertheless,
we must note that this surgical technique is
always associated with a MPFL reconstruction
that provokes a descent of the patella. Moreover,
the patellar height is evaluated before definitive
fixation.
5
Medial Patellar Instability
and Multidirectional Patellar
Instability
Medial patellar instability (MPI) is an objective
condition with its own characteristics that frequently brings on disabling anterior knee pain,
significant disability as well as important psychological problems [40]. In most cases, it is
secondary to an “extensive” LRR [40, 45]. In
other cases, it is due to the release of the LR in
patients with trochlear dysplasia or hyperelasticity [40]. It can also be attributable to the
release of a previously lax LR, which shows poor
patient selection [39]. Typically, the patient feels
new pain and new instability that are different
and much worse than that prior to surgery.
The first step in diagnosing a pathological
condition is to know that it exists. This was
clearly reflected by Jack Hughston in his well-
272
V. Sanchis-Alfonso and E. Montesinos-Berry
Fig. 15 Lengthening of the quadriceps tendon on the coronal plane. Side-to side repair of the quadriceps tendon
known sentence: ``You may not have seen it, but
maybe it has seen you''. Normally, MPI appears
in the first 30º of knee flexion. It is frequently
missed because patients complain of the patella
moving laterally with early knee flexion. In our
series, many patients have had to visit more than
three doctors before obtaining a diagnosis and an
appropriate treatment. This demonstrates that it is
a clinical condition that most orthopedic surgeons do not know about. Therefore, we believe
that there is a need to spread the word about the
diagnostic procedures for recognizing this clinical condition.
The physical findings are crucial to the diagnosis. The most important are pain and tenderness at the site of the LR defect, an increment in
passive medial patellar mobility, especially when
compared with the opposite normal knee. There
are also the issues of pain and apprehension
when we apply medial stress to the patella and a
positive “Fulkerson relocation test” (Fig. 16)
[46].
Moreover, all our patients experienced significant relief from their pain with a “reverse”
McConnell taping [40]. We believe that it is a
good and useful diagnostic approach to take.
When the standard radiological studies are normal, it puts the orthopedic surgeon on the
defensive when seeing this kind of patient. Stress
axial radiography [47] or stress axial CT scans
[48] allow for the objective documentation and
quantification of MPI.
At the present time, our preference for
reconstructing the lateral retinaculum is the
technique described by Jack Andrish because it is
very anatomic and allows us to fine tune the
graft-tension by adding sutures to further tighten
the graft [49]. He uses a central strip or an
How to Deal with Chronic Patellar Instability
273
A
B
C
D
Fig. 16 Fulkerson relocation test A, B. A The patella is
held medially in extension (arrow) and B then released on
abrupt knee flexion. It is a provocative test, and therefore
reproduction of symptomatology with this maneuver
strongly suggests medial patellar instability. Sulcus sign
C. Excessive medial displacement of the patella D
anterior strip of the iliotibial band, leaving it
attached proximally and attaching it to the midpoint of the patella. The objective of this technique is to reconstruct the deep transverse layer
of the LR. The lateral reconstruction must be
tensioned with the patella engaged within the
trochlea with the knee at 30º of knee flexion.
Take note that it is a “salvage” procedure. It does
not address the original source of pain. Moreover, it cannot improve symptoms from
osteoarthritis, malalignment, or lateral instability
due to a deficient MPFL. This may explain the
satisfactory results of only 65% in isolated
reconstructions [45].
The LR is a restraint on medial patellar displacement. Another restraint on medial patellar
displacement is the MPFL. The MPFL tightens
with medial displacement of the patella.
Therefore, we must reconsider medial instability
after the MPFLr in cases of multidirectional
instability. If the MPI is corrected after
the MPFLr, it is not necessary to reconstruct the
LR.
6
Take Home Messages
– Not all the patients with chronic patellar
instability are equal.
– The etiology of chronic patellar instability is
multifactorial. Therefore, its treatment must
be personalized. Let’s call it “bespoke treatment.” This is the only way to avoid failures
and subsequent operations.
274
References
1. Post WR, Fithian DC. Patellofemoral instability: a
consensus statement from the AOSSM/PFF patellofemoral instability workshop. Orthop J Sports Med.
2018;30;6(1):2325967117750352. https://doi.org/10.
1177/2325967117750352.eCollection.
2. Nelitz M, Theile M, Dornacher D, et al. Analysis of
failed surgery for patellar instability in children with
open growth plates. Knee Surg Sports Traumatol
Arthrosc. 2012;20:822–8.
3. Wagner D, Pfalzer F, Hingelbaum S, et al. The
influence of risk factors on clinical outcomes
following anatomical medial patellofemoral ligament
(MPFL) reconstruction using the gracilis tendon.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(2):318–24.
4. Kita K, Tanaka Y, Toritsuka Y, et al. Factors
affecting the outcomes of double-bundle medial
patellofemoral ligament reconstruction for recurrent
patellar dislocations evaluated by multivariate analysis. Am J Sports Med. 2015;43(12):2988–96.
5. Dejour D, Byn P, Ntagiopoulos PG. The Lyon’s
sulcus-deepening trochleoplasty in previous unsuccessful patellofemoral surgery. Int Orthop. 2013;37
(3):433–9.
6. Diederichs G, Kohlitz T, Kornaropoulos E, et al.
Magnetic resonance imaging analysis of rotational
alignment in patients with patellar dislocations. Am J
Sports Med. 2013;41(1):51–7.
7. Conlan T, Garth WP Jr, Lemons JE. Evaluation of
the medial soft-tissue restraints of the extensor
mechanism of the knee. J Bone Joint Surg Am.
1993;75:682–93.
8. Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human
knee. Am J Sports Med. 1998;26:59–65.
9. Hautamaa PV, Fithian DC, Kaufman KR,
Daniel DM, Pohlmeyer AM. Medial soft tissue
restraints in lateral patellar instability and repair.
Clin Orthop Relat Res. 1998;349:174–82.
10. Nomura E. Classification of lesions of the medial
patello-femoral ligament in patellar dislocation. Int
Orthop. 1999;23:260–3.
11. Sanchis-Alfonso V. Guidelines for medial patellofemoral ligament reconstruction in chronic lateral
patellar instability. J Am Acad Orthop Surg.
2014;22:175–82.
12. Mochizuki T, Nimura A, Tateishi T, et al. Anatomic
study of the attachment of the medial patellofemoral
ligament and its characteristic relationships to the
vastus intermedius. Knee Surg Sports Traumatol
Arthrosc. 2013;21:305–10.
13. Fulkerson JP, Edgar C. Medial quadriceps tendonfemoral ligament: surgical anatomy and reconstruction technique to prevent patella instability. Arthrosc
Tech. 2013;2:e125–8.
V. Sanchis-Alfonso and E. Montesinos-Berry
14. Franzone JM, Vitale MA, Shubin Stein BE, et al. Is
there an association between chronicity of patellar
instability and patellofemoral cartilage lesions? An
arthroscopic assessment of chondral injury. J Knee
Surg. 2012;25:411–6.
15. Nomura E, Inoue M, Kobayashi S. Long-term followup and knee osteoarthritis change after medial patellofemoral ligament reconstruction for recurrent patellar
dislocation. Am J Sports Med. 2007;35:1851–8.
16. Kita K, Tanaka Y, Toritsuka Y, et al. Patellofemoral
chondral status after medial patellofemoral ligament
reconstruction using second-look arthroscopy in
patients with recurrent patellar dislocation. J Orthop
Sci. 2014;19:925–32.
17. Arendt EA, Dahm DL, Dejour D, et al. Patellofemoral joint: from instability to arthritis. Instr Course
Lect. 2014;63:355–68.
18. Izadpanah K, Weitzel E, Vicari M, et al. Influence of
knee flexion angle and weight bearing on the tibial
tuberosity–trochlear groove (TTTG) distance for
evaluation of patellofemoral alignment. Knee Surg
Sports Traumatol Arthrosc. 2014;22:2655–61.
19. Hingelbaum S, Best R, Huth J, et al. The TT-TG
index: a new knee size adjusted measure method to
determine the TT-TG distance. Knee Surg Sports
Traumatol Arthrosc. 2014;22:2388–95.
20. Dornacher D, Reichel H, Kappe T. Does tibial
tuberosity–trochlear groove distance (TT-TG) correlate with knee size or body height. Knee Surg Sports
Traumatol Arthrosc. https://doi.org/10.1007/s00167015-3526-7.
21. Caplan N, Lees D, Newby M, et al. Is tibial
tuberosity-trochlear groove distance an appropriate
measure for the identification of knees with patellar
instability? Knee Surg Sports Traumatol Arthrosc.
2014;22:2377–81.
22. Matsushita T, Kuroda R, Oka S, et al. Clinical
outcomes of medial patellofemoral ligament reconstruction in patients with an increased tibial
tuberosity-trochlear groove distance. Knee Surg
Sports Traumatol Arthrosc. 2014;22:2438–44.
23. Biedert RM, Albrecht S. The patellotrochlear index:
a new index for assessing patellar height. Knee Surg
Sports Traumatol Arthrosc. 2006;14:707–12.
24. Servien E, Verdonk PC, Neyret P. Tibial tuberosity
transfer for episodic patellar dislocation. Sports Med
Arthrosc Rev. 2007;15:61–7.
25. Yang JS, Fulkerson JP, Obopilwe E, et al. Patellofemoral contact pressures after patellar distalization:
a biomechanical study. Arthroscopy. 2017;33
(11):2038–44.
26. Fabricant PD, Ladenhauf HN, Salvati EA, et al.
Medial patellofemoral ligament (MPFL) reconstruction improves radiographic measures of patella alta in
children. Knee. 2014;21:1180–4.
27. Hiemstra LA, Kerslake S, Lafave MR, et al. Patella
alta is reduced following MPFL reconstruction but
has no effect on quality-of-life outcomes in patients
How to Deal with Chronic Patellar Instability
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
with patellofemoral instability. Knee Surg Sports
Traumatol Arthrosc. 2021;29(2):546–52.
Fucentese SF, Zingg PO, Schmitt J, et al. Classification of trochlear dysplasia as predictor of clinical
outcome after trochleoplasty. Knee Surg Sports
Traumatol Arthrosc. 2011;19:1655–61.
Leclerc JT, Dartus J, Labreuche J, et al. Complications and outcomes of trochleoplasty for patellofemoral instability: a systematic review and metaanalysis of 1000 trochleoplasties. Orthop Traumatol
Surg Res. 2021;107(7): 103035. https://doi.org/10.
1016/j.otsr.2021.103035.
Teitge RA. Osteotomy in the treatment of patellofemoral instability. Tech Knee Surg. 2006;5:2–18.
Kaiser P, Schmoelz W, Schoettle P, et al. Increased
internal femoral torsion can be regarded as a risk
factor for patellar instability—a biomechanical study.
Clin Biomech. 2017;47:103–9.
Milinkovic DD, Jovandic I, Zimmermann F, et al. The
J-sign and the body mass index determine the diseasespecific quality of life in patients with lateral patellar
instability. Knee Surg Sports Traumatol Arthrosc.
2021. https://doi.org/10.1007/s00167-021-06705-6.
Nelitz M, Wehner T, Steiner M, et al. The effects of
femoral external derotational osteotomy on frontal
plane alignment. Knee Surg Sports Traumatol
Arthrosc. 2014;22:2740–6. https://doi.org/10.1007/
s00167-013-2618-5.
Lee SY, Jeong J, Lee K, et al. Unexpected angular or
rotational deformity after corrective osteotomy. BMC
Musculoskelet Disord. 2014;15:175. https://doi.org/
10.1186/1471-2474-15-175.
Palmer RC, Podeszwa DA, Wilson PL, et al. Coronal
and transverse malalignment in pediatric patellofemoral instability. J Clin Med. 2021;8;10(14):3035.
https://doi.org/10.3390/jcm10143035.
Omidi-Kashani F, Hasankhani IG, Mazlumi M, et al.
Varus distal femoral osteotomy in young adults with
valgus knee. J Orthop Surg Res. 2009;4:15.
Tan SHS, Hui SJ, Doshi C, et al. The outcomes of
distal femoral varus osteotomy in patellofemoral
instability: a systematic review and meta-analysis.
J Knee Surg. 2020;33(5):504–12.
Wilson PL, Black SR, Ellis HB, et al. Distal femoral
valgus and recurrent traumatic patellar instability: is
275
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
an isolated varus producing distal femoral osteotomy
a treatment option? J Pediatr Orthop. 2018;38:
e162–7.
Merican AM, Sanghavi S, Iranpour F, et al. The
structural properties of the lateral retinaculum and
capsular complex of the knee. J Biomech. 2009;42
(14):2323–9.
Sanchis-Alfonso V, Merchant AC. Iatrogenic medial
patellar instability: an avoidable injury. Arthroscopy.
2015;31(8):1628–32.
Arendt EA. Lateral-sided surgery with MPFL reconstruction: when is this needed? In: Bonnin M,
Servien E, Demey G, Dejour D, editors. La Patella.
Montpellier, France: Sauramps Medical; 2012.
p. 119–23.
Andrish J. Surgical options for patellar stabilization
in the skeletally immature patient. Sports Med
Arthrosc. 2007;15:82–8.
Biedert RM. Patellar instability with increased knee
flexion due to lateral femoral condyle distal dysplasia: a report of two cases. Knee. 2012;19:140–3.
Song GY, Feng H, Zhang H, et al. Tibial tubercle
proximalization: a novel technique to lengthen the
extensor mechanism in skeletally mature patients
with lateral habitual patellar dislocations. Orthop J
Sports Med. 2019;21;7(3):2325967119831642.
https://doi.org/10.1177/2325967119831642.
Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC, et al. Results of isolated lateral retinacular
reconstruction for iatrogenic medial patellar instability. Arthroscopy. 2015;31:422–7.
Fulkerson JP. A clinical test for medial patella
tracking. Tech Orthop. 1997;12:165–9.
Teitge RA, Faerber WW, Des MP. Stress radiographs
of the patellofemoral joint. J Bone Joint Surg Am.
1996;78:193–203.
Biedert RM. Computed tomography examination. In:
Biedert RM, editor. Patellofemoral disorders. Diagnosis and treatment. West Sussex: Wiley;2004.
p. 101–111.
Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC, et al. Deep transverse lateral retinaculum
reconstruction for medial patellar instability.
Arthrosc Tech. 2015;4(3):e245-249.
Limitations of Patellofemoral
Surgery in Children
Mahad Hassan and Marc Tompkins
1
Rehabilitation Challenges
in Children with Patellofemoral
Instability
Patellofemoral instability is a common knee
pathology in the acute injury setting within the
pediatric population [1–4]. Recurrence can be as
high as 75% in patients with open physes who
also have risk factors present such as patella alta
and trochlear dysplasia [5]. In addition to anatomic and surgical considerations outlined later
in this chapter, rehabilitation poses a challenge in
this population. Pediatric patients can have difficulty adhering to post-surgical restrictions and
rehabilitation programs. This can result in inadequate healing of bony or soft tissue realignment
or reconstruction procedures. Availability of
physical therapists with experience to treat children, especially therapists with experience treating patellofemoral pediatric patients, may impact
the management of the patient following surgery.
This may result in inadequate restoration of
musculoskeletal function or inability to address
underlying biomechanical issues that predisposed
the patient to injury in the first place. Parental
M. Hassan M. Tompkins (&)
University of Minnesota, Minneapolis, MN, USA
e-mail: mtompkin@umn.edu
engagement, as well as availability to provide
transport to rehabilitation facilities, are important
challenges unique to this population.
2
Anatomic Considerations
There are several anatomic risk factors for
patellofemoral instability to consider when
treating pediatric patients with open physes.
Patella alta is poor overlap, or engagement, of
the patella and the trochlea [6]. The risk of
instability in patella alta occurs because there is a
delayed engagement of the patella on the trochlear sulcus as the knee goes from extension
into flexion. This decreases the trochlea’s function as primary restraint to lateral displacement
of the patella potentially resulting in the patella
moving lateral to the trochlea. In adults, patella
alta is addressed surgically with tibial tubercle
distalization. This is not recommended in pediatric patients with open physes because violation
of the tibial tubercle apophysis can result in its
arrest and resultant recurvatum deformity.
Extensor mechanism malalignment creates an
angle at the patellofemoral joint resulting in a
laterally directed force vector on the patella,
which puts the patella at risk of lateral instability.
In adults, this can be addressed with a anteromedialization tibial tubercle osteotomy. Similar
to tibial tubercle distalization, this will put the
patient at risk of apophyseal arrest [7].
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_19
277
278
M. Hassan and M. Tompkins
Trochlear dysplasia is a risk factor for patellofemoral instability because the poorly formed,
or medialized, sulcus increases the lateral tracking of the patella and risk for lateral instability
[5]. Various procedures have been described to
address dysplasia and increase the effective depth
of the trochlea [7–11]. However, these procedures have been contraindicated in skeletally
immature patients as they can damage the distal
femoral physis [7].
Genu valgum can contribute to patellar
instability because it also creates a laterally
directed force vector on the patella. In skeletally
immature patients, the physis can be utilized to
correct this deformity via guided growth [1, 12].
Coronal plane abnormalities can also be addressed with osteotomies, but the physis must be
considered when performing an osteotomy.
Increased femoral version and/or tibial torsion
can cause poor overlap of the patella and trochlea
in the axial plane resulting in lateralizing of the
patella relative to the trochlea increasing the risk
of lateral instability. In adults, axial plane
abnormalities can be addressed at the proximal,
midshaft, or distal aspects of the femur or tibia.
Midshaft osteotomies are typically fixed with an
intramedullary nail which is difficult in skeletally
immature patients because most nailing systems
approach the intramedullary canal in a manner
which penetrates through the physis [13, 14].
3
Surgical Techniques
Due to the aforementioned anatomic considerations, surgical techniques unique to the pediatric
population have been devised.
For skeletally immature patients with patella
alta, a patellar tendon shortening procedure can
be done in lieu of a distalizing tibial tubercle
osteotomy in skeletally immature patients. This
is performed by using sutures to imbricate the
tendon with the aim of improving the engagement between the patella and trochlea [15, 16].
There a few limitations to this technique and care
should be taken with the sequence of performing
concomitant procedures such as medial imbrication and MPFL reconstruction. Ligament
isometry is significantly altered following patellar tendon shortening and could necessitate
rebalancing if these procedures are performed
prior to the patellar tendon shortening. Complications from this technique can arise and patella
baja may result as it can in a distalizing osteotomy. This can result in significantly increased
contact pressures in the patellofemoral joint
throughout early flexion [15, 16], Patellar tendon
rupture through the imbrication site can also
occur. Subsequent repair can be done but may
lead to worse outcomes and extended recovery
[15, 16].
Multiple techniques have been described in
the past to address extensor mechanism
malalignment. The Roux-Goldthwait procedure
was originally described over one hundred years
ago and involves longitudinally dividing the
patellar tendon and transferring the lateral limb
deep and medial to the medial limb [17, 18].
Galeazzi described a tenodesis technique in the
1920s in which the semitendinosus tendon is
harvested and secured to the medial patella in an
oblique manner while keeping its insertion intact
[19]. When performed in isolation, the outcomes
of this procedure are variable when recurrent
dislocation and knee function are considered.
While the original description of the procedure
and follow up studies showed good results with
lower than 10% recurrent instability rates, a
recent long term follow up study showed a
greater than 80% redislocation with approximately 40% of those patients requiring surgical
stabilization [19–21].
Treating trochlear dysplasia with a deepening
trochleoplasty has been described in skeletally
immature patients, but only in those who are
close to skeletal maturity [22]. There are currently no descriptions or indications for performing trochleoplasty in very skeletally
immature patients as this will put the anterior
distal femoral physis at risk of injury and subsequent growth disturbance.
Genu valgum can be addressed surgically via
hemi-epiphysiodesis or guided growth. Guided
growth in this case is the temporary slowing of
the medial distal femoral physis until the
patient’s mechanical axis is corrected to the
Limitations of Patellofemoral Surgery in Children
center of the knee [12]. Limitations with this
approach include undercorrection if not enough
growth remains or overcorrection if not followed
closely. Hence, the patient must be followed
closely to monitor for correction and the patient
and family must be prepared for further surgery
to remove hardware.
Axial plane correction can be performed surgically with a plate and screws at any level:
proximal, midshaft, or distal. Midshaft requires
more dissection and soft tissue disruption than
would be done in adults with intramedullary
nailing. With proximal and distal osteotomies,
the physis must be taken into account and protected when performing these osteotomies.
3.1 Medial Patellofemoral Ligament
Reconstruction
Medial patellofemoral ligament (MPFL) reconstruction can be a powerful operation to decrease
the dislocation risk in patients with patellar
instability, but requires adjustment in surgical
technique for skeletally immature patients. The
attachment of the MPFL on the femur is in close
proximity to the physis, so in some patients it is
not possible to place the fixation on the femur in
a perfect anatomic position [23]. If the MPFL is
not in an anatomic location, it can affect the
tracking of the patella and result in instability or
overconstraint [24]. Care must therefore be taken
to place the MPFL as close to anatomic as possible, while also protecting the physis.
MPFL reconstruction has been shown to
decrease dislocation risk even in patients with
anatomic risk factors such as patella alta and
trochlear dysplasia [25]. However, further procedures may still be necessary at skeletal maturity such as addressing the trochlear dysplasia
which would be contra-indicated in patients with
an open distal femoral physis. As such, it is
important to counsel parents and patients that
279
when there are anatomic risk factors present
which cannot be adequately addressed during
skeletal growth, an MPFL reconstruction may be
a temporizing procedure and there may be a need
to perform additional procedures as the child
achieves skeletal maturity.
4
Risk of Recurrence and Return
to Activity
Failure of surgical patellar stabilization is
believed to be due to many reasons, but includes:
(1) technical failure of the primary stabilization
method, (2) unaddressed static and dynamic
pathoanatomy and (3) intrinsic risk factors such
as collagen disorders and ligamentous laxity
[26]. Age at the time of surgery has been shown
in multiple studies to affect risk of recurrence
following surgery, with younger patients at
higher risk [27, 28]. This is something in which
patients should be counseled at the time of the
surgical discussion. The greater the presence of
anatomic risk factors at the time of surgery also
increases the risk of further instability [29]. All of
the anatomic risk factors, therefore, that can be
addressed must at least be considered for intervention at the time of surgery.
There is limited literature on return to play
after patellar stabilization surgery in pediatric
patients [26, 30]. A systematic review on return
to play highlighted a lack of objective guidelines
for return to play. Moreover, there was a wide
range of timing and criteria in the studies identified in the review [30]. Return to play timeframes are varied and can range from 3 to 8
months. The variation in return to play timeline
also depends on concurrent procedures performed [26, 30]. A recent review recommended
using the criteria for return consisting of no pain,
full motion, no effusion, no objective patellofemoral instability on exam, near symmetric
strength and excellent dynamic stability [31].
280
5
M. Hassan and M. Tompkins
Summary
Patellofemoral surgery in children is multifaceted and complex. It is possible to stabilize
the patellofemoral joint and achieve good clinical
outcomes, but there are many limitations that
must be understood when planning surgery for
these patients.
References
1. Hennrikus W, Pylawka T. Patellofemoral instability
in skeletally immature athletes. J Bone Joint Surg
Am. 2013;95(2):176–83.
2. Weeks KD 3rd, Fabricant PD, Ladenhauf HN,
Green DW. Surgical options for patellar stabilization
in the skeletally immature patient. Sports Med
Arthrosc. 2012;20(3):194–202.
3. Khormaee S, Kramer DE, Yen YM, Heyworth BE.
Evaluation and management of patellar instability in
pediatric and adolescent athletes. Sports Health.
2015;7:115–23.
4. Fithian DC, Paxton EW, Stone ML, Silva P,
Davis DK, Elias DA, White LM. Epidemiology and
natural history of acute patellar dislocation. Am J
Sports Med. 2004;32:1114–21.
5. Arendt EA, Askenberger M, Agel J, Tompkins MA.
Risk of redislocation after primary patellar dislocation: a clinical prediction model based on magnetic
resonance imaging variables. Am J Sports Med.
2018;46(14):3385–90.
6. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc.
1994;2(1):19–26
7. Dejour D, Saggin P. The sulcus deepening trochleoplasty−the Lyon’s procedure. Int Orthop.
2010;34:311–6.
8. Kuroda R, Kambic H, Valdevit A, et al. Distribution
of patellofemoral joint pressures after femoral
trochlear osteotomy. Knee Surg Sports Traumatol
Arthrosc. 2002;10:33–7.
9. Masse Y. Trochleoplasty. Restoration of the intercondylar groove in subluxations and dislocations of
the patella. Rev Chir Orthop Reparatrice Appar Mot.
1978;64:3–17.
10. Bereiter HG, Gautier E. Die trochleoplastik ale
chirurgishe therapie der rezidivierenden patellauxation bei trochleodysplasie des femurs. Arthroskopie.
1994;7:281–6.
11. Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human
knee. Am J Sports Med. 1998;26(1):59–65.
12. Kearney SP, Mosca VS. Selective hemiepiphyseodesis for patellar instability with associated genu
valgum. J Orthop. 2015;12(1):17–22.
13. Pandya NK, Edmonds EW. Immediate intramedullary flexible nailing of open pediatric tibial shaft
fractures. J Pediatr Orthop. 2012;32:770–6.
14. Metaizeau JD, Denis D. Update on leg fractures in
paediatric patients. Orthop Traumatol Surg Res.
2019;105:S143-51.
15. Andrish J. Surgical options for patellar stabilization
in the skeletally immature patient. Sports Med
Arthrosc. 2007;15:82–8.
16. Parvaresh KC, Huddleston HP, Yanke AB. Patellar
tendon shortening for treatment of patella alta in
skeletally immature patients with patellar instability.
Arthrosc Tech. 2021;10(8):e1979-84.
17. Marsh JS, Daigneault JP, Sethi P, Polzhofer GK.
Treatment of re- current patellar instability with a
modification of the roux−goldthwait technique.
J Pediatr Orthop. 2006;26(4):461–5.
18. Vahasarja V, Kinnunen P, Lanning P, Serlo W.
Operative realign−ment of patellar malalignment in
children. J Pediatr Orthop. 1995;15(3):281–5.
19. Letts RM, Davidson D, Beaule P. Semitendinosus
tenodesis for repair of recurrent dislocation of the
patella in children. J Pediatr Orthop. 1999;19
(6):742–7.
20. Hall JE, Micheli LJ, McManama GB Jr. Semitendinosus tenodesis for recurrent subluxation or dislocation of the patella. Clin Orthop Relat Res.
1979;144:31–5.
21. Grannatt K, Heyworth BE, Ogunwole O, Micheli LJ,
Kocher MS. Galeazzi semitendinosus tenodesis for
patellofemoral instability in skeletally immature
patients. J Pediatr Orthop. 2012;32(6):621–5.
22. Nelitz M, Dreyhaupt J, Williams SRM. No growth
disturbance after trochleoplasty for recurrent patellar
dislocation in adolescents with open growth plates.
Am J Sports Med. 2018;46(13):3209–16.
23. Shea KG, Martinson WD, Cannamela PC, Richmond CG, Fabricant PD, Anderson AF,
Polousky JD, Ganley TJ. Variation in the medial
patellofemoral ligament origin in the skeletally
immature knee: an anatomic study. Am J Sports
Med. 2018;46(2):363–9.
24. Burrus MT, Werner BC, Conte EJ, Diduch DR.
Troubleshooting the femoral attachment during
medial patellofemoral ligament reconstruction: location, location, location. Orthop J Sports Med. 2015;3
(1):2325967115569198.
25. Schlumberger M, Schuster P, Hofmann S, Mayer P,
Immendörfer M, Mayr R, Richter J. Midterm results
after isolated medial patellofemoral ligament reconstruction as first-line surgical treatment in skeletally
immature patients irrespective of patellar height and
trochlear dysplasia. Am J Sports Med. 2021;49
(14):3859–66.
Limitations of Patellofemoral Surgery in Children
26. Vellios EE, Trivellas M, Arshi A, Beck JJ. Recurrent
patellofemoral instability in the pediatric patient:
management and pitfalls. Curr Rev Musculoskelet
Med. 2020;13(1):58–68. https://doi.org/10.1007/
s12178-020-09607-1.
27. Hiemstra LA, Kerslake S. Age at time of surgery but
not sex is related to outcomes after medial patellofemoral ligament reconstruction. Am J Sports Med.
2019;47(7):1638–44.
28. Hiemstra LA, Kerslake S, Kupfer N, Lafave M.
Patellofemoral stabilization: postoperative redislocation and risk factors following surgery. Orthop J
Sports Med. 2019;7(6).
29. Nelitz M, Theile M, Dornacher D, Wölfle J,
Reichel H, Lippacher S. Analysis of failed surgery
281
for patellar instability in children with open growth
plates. Knee Surg Sports Traumatol Arthrosc.
2012;20(5):822–8.
30. Zaman S, White A, Shi WJ, Freedman KB, Dodson CC. Return−to−play guidelines after medial
patellofemoral ligament surgery for recurrent patellar
instability: a systematic review. Am J Sports Med.
2017;363546517713663.
31. Menetrey J, Putman S, Gard S. Return to sport after
patellar dislocation or following surgery for patellofemoral instability. Knee Surg Sports Traumatol
Arthrosc. 2014;22(10):2320–6.
The Failed Medial Patellofemoral
Ligament Reconstruction. What Can
We Do?
Vicente Sanchis-Alfonso and Cristina Ramírez-Fuentes
1
Introduction
A torn medial patellofemoral ligament (MPFL) is
considered the focal lesion in chronic lateral
patellar instability (CLPI). Therefore, it is logical
that the most frequently performed surgery to
treat CLPI is MPFL reconstruction (MPFLr).
Failed MPFLr is the term that we are going to use
to describe the situation of those patients who
have not seen a successful outcome after a surgery that was done to resolve CLPI. As a result,
the patient will have a recurrence, anterior knee
pain (AKP) and a limitation in knee range-ofmotion. The three complaints can be present in
combination or in isolation. Note that a “failed”
MPFLr does not necessarily mean that the surgery was botched. It may be the consequence of a
surgical complication, that is an adverse event
caused by factors that are outside the orthopedic
surgeon’s control. However, it is a consequence
of an error in surgical indication or in the surgical
technique on most occasions. Schneider and
colleagues [1] reported a reoperation rate of 3.1%
(95% CI, 1.1–5.0%) after an isolated MPFLr.
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
C. Ramírez-Fuentes
Medical Imaging Department, Hospital Universitario
y Politecnico La Fe, Valencia, Spain
The objectives of this chapter are four-fold. They
are (1) to analyze the causes of failure,
(2) to describe how to avoid surgical failure,
(3) to explain how to solve the problem and
(4) to analyze the outcomes after MPFL surgery
revision.
2
Causes of Revision Surgery—
MPFLr Failure Etiology
The reasons revision surgery is called for after
MPFLr are varied. They include (1) an incorrect
surgical indication, (2) a technical failure, (3) a
failure to recognize and correct an existing
pathoanatomy, (4) intrinsic risk factors like collagen disorders and (5) a patellar fracture.
2.1 Incorrect Surgical Indication
The first requisite for a successful MPFLr is
appropriate patient selection. The ideal indication
for an isolated MPFLr would be: (1) a patient
with CLPI with at least two documented episodes
of dislocation and confirmation of dislocation
with examination under general anesthesia, (2) a
TT-TG distance <20 mm, a positive apprehension test until 30º of knee flexion, a patellar
Caton-Deschamps index of <1.2, and trochlear
dysplasia grade A [2]. An MPFLr should not be
performed if the patella cannot be laterally dislocated. The objective of an MPFLr is not to pull
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_20
283
284
the patella to its proper position within the trochlear groove but to stabilize it once the patellofemoral tracking (J-sign) has been corrected.
Therefore, an isolated MPFLr is not indicated to
eliminate the J-sign. In this way, Zhang and
colleagues [3] have demonstrated that a preoperative high-grade J-sign is associated with
residual graft laxity after isolated MPFLr.
2.2 Technical Mistakes and Surgical
Technique Issues
According to Parikh and colleagues [4] 47% of
the complications that occur after MPFLr are
related to technical errors.
2.2.1 Incorrect Femoral Attachment
Point
The most frequent serious technical error that can
lead to MPFLr failure is the incorrect location of
the femoral attachment point (Figs. 1, 2, 3, 4, 5
and 6). Walker and colleagues [5] analyzed
MPFLr revision surgeries in a systematic review
that was done as recently as 2021. In it, the authors
showed that the most frequent cause for revision
surgery is the malposition of the femoral attachment point (38%). The femoral attachment point is
crucial as it determines the length change behavior
of the graft and thereby the graft tension at different angles of knee flexion [6]. It is determinant
in the kinematic behavior of the graft [6].
How to avoid an incorrect femoral attachment
point?
To accurately locate the femoral attachment
point, Schoettle and colleagues [7] recommended
using intra-operatory fluoroscopy. Having a true
intra-operative lateral image is indispensable
when this radiological method is used. However,
various authors have demonstrated that Schoettle's radiological method, which is accepted as
the gold standard, is no guarantee of a true
anatomical attachment point [8–11]. Therefore,
the radiological method is only an approximation. It should not be used as the sole way of
locating the femoral attachment point. To locate
the real anatomical attachment point most
V. Sanchis-Alfonso and C. Ramírez-Fuentes
accurately, make an incision that is large enough
to identify the most relevant anatomical landmark, the adductor magnus tendon (AMT).
The AMT is easily identifiable and leads right to
the origin of the MPFL on the femur. It is situated 10.6 ± 2.5 mm distal to the apex of the
adductor tubercle (AT) and parallel to the long
axis of the femur [12]. The great variability in the
location of the AT (Fig. 7) is behind the variability in the location of the femoral insertion of
the MPFL. This explains the large number of
errors when Schoettle's method is used to identify the femoral fixation point during MPFLr.
But, is the anatomic femoral tunnel position so
relevant in MPFLr?
A poor outcome is not always seen with femoral
tunnel malpositioning. In our experience, those
ligaments with a non-anatomical femoral fixation
point that behave kinematically like an anatomical MPFL have excellent clinical outcomes at
long-term follow-up [6]. However, those nonanatomical grafts that do not show physiological
kinematic behavior are those that have a poor
clinical outcome [6]. What should we do in those
cases? We believe every MPFL graft should be
placed anatomically, because an anatomical
femoral tunnel position maximizes outcomes and
provides the best chance of excellent short-term
and long-term success. In summary, an anatomical MPFLr is a fast and reproducible way to
achieve an MPFL that is long enough to act as an
isometric “leash” from 0º to 30º and becoming
loose after 30º of knee flexion (Fig. 8). In conclusion, the relevant anatomy and biomechanics
must be identified and restored to avoid
complications.
2.2.2 Excessive Graft Tension
Another technical error that can lead to surgical
failure is excessive graft tension. The concept of
‘‘tensioning’’ the MPFL graft is not correct from
a conceptual point of view because the MPFL is
not under constant tension in its native state. It
only comes under tension when a lateral force
acts on the patella to displace it laterally. Philip
Schoettle makes a very intelligent simile, comparing the MPFL to a dog leash. The leash is
The Failed Medial Patellofemoral Ligament …
285
Fig. 1 CASE # 1. A 19-year-old male patient presented
with severe AKP and CLPI. He had undergone an MPFLr
with a single bundle semitendinosus tendon graft some
3 years earlier. Upon physical examination, no patellofemoral tracking disorder was detected (negative J-sign).
The patient was first placed under general anesthesia.
During the procedure, it was determined that dislocation
beyond 40° of knee flexion was not possible. The femoral
tunnel of the MPFLr was seen excessively anterior. It is a
significant error. Severe chondropathy of the articular
surface of the patella was also observed. Moreover, the
distance between the patellar fixation point and the
femoral fixation point increased with knee flexion.
Clinically speaking, it results in increased patellofemoral
pressure during knee flexion, which may have been the
origin of the patient’s severe patellar chondropathy. The
resolution was found in the anatomic MPFLr in which the
contralateral semitendinosus tendon with a double-bundle
technique was used. (Reused with permission from
Baishideng Publishing Group Inc. From SanchisAlfonso V, et al. Failed medial patellofemoral ligament
reconstruction: Causes and surgical strategies. World J
Orthop, 2017; 8(2): 115–129)
loose most of the time, except when the dog (the
patella) wants to run away (dislocate), and then it
becomes tight. If the leash (the MPFL) were tight
all the time, it would choke the dog. Continuing
with our simile, it would create patellofemoral
pressure that would be great enough to lead to
chondropathy and finally PFOA. In vivo studies
of the kinematics of the MPFL have shown that
the greatest distance between the femoral and
patellar attachment points is between 0 and 60º of
knee flexion (the greatest at 30º) and that this
distance decreases significantly from 60º to 120º
of flexion [6]. With this, we make it such that
excessive compression forces are not produced in
the patellofemoral joint during high degrees of
knee flexion. Finally, it is important to note that
286
Fig. 2 CASE # 2. A 28-year-old female patient came to
us with very severe AKP and CLPI. A clear case of
patellofemoral maltracking was seen in the physical
examination (positive J-sign). Moreover, we were able
to dislocate the patella laterally beyond 60° of knee
flexion. She had been operated on various times over the
previous 8 years. She had undergone a lateral retinacular
release, proximal realignment, osteotomy for medialization of the tibial tubercle and MPFLr. It was noted that the
femoral tunnel was overly proximal and anterior. With
knee flexion, the space between the patellar and the
femoral fixation points increases a great deal. Clinically, it
V. Sanchis-Alfonso and C. Ramírez-Fuentes
brings about a significant increase in patellofemoral
pressure during knee flexion. It was considered a possible
explanation for the patient’s severe case of patellofemoral
osteoarthritis (PFOA). In this specific instance, the pain
went away after a sulcus deepening trochleoplasty. After
carrying out an anatomic double-bundle MPFLr with a
semitendinosus tendon graft, the CLPI also totally
disappeared. (Reused with permission from Baishideng
Publishing Group Inc. From Sanchis-Alfonso V, et al.
Failed medial patellofemoral ligament reconstruction:
Causes and surgical strategies. World J Orthop, 2017; 8
(2): 115–129)
The Failed Medial Patellofemoral Ligament …
287
A
B
C
D
Fig. 3 CASE # 3. This clinical case highlights the
importance of the femoral attachment point in MPFLr
outcomes. Both knees were operated on, the left with an
excellent result B, D and the right with a bad result A,
C. In this case, there are no confusion variables that can
influence the result. There is no patellar tilt, no patella
alta, no severe trochlear dysplasia, and the TT-TG
distance is normal. Therefore, the only variable that
counts is the femoral attachment point and therefore we
are able to compare the failed operated knee with the
contralateral successful knee. The right knee was reoperated on performing a new reconstruction with a new
femoral attachment (blue arrow) with an excellent result.
Finally, we must note that the patient is an athlete and
therefore she is more demanding and a surgical procedure
that is not 100% perfect will be more noticeable in an
athlete than in a sedentary person. In short, the only
difference between both knees was the femoral attachment
point. (C, D. Reused with permission from Baishideng
Publishing Group Inc. From Sanchis-Alfonso V, et al.
Failed medial patellofemoral ligament reconstruction:
Causes and surgical strategies. World J Orthop, 2017; 8
(2): 115–129)
288
V. Sanchis-Alfonso and C. Ramírez-Fuentes
Fig. 4 CASE # 3. Here we analyze the knee with an
excellent outcome. This knee was operated on performing
a double-bundle MPFLr with semitendinosus. In the
graphs on the right you can see the kinematics of the
reconstructed MPFL in vivo. The blue lines represent the
reconstructed MPFL. The femoral attachment point is
clearly non-anatomic (blue arrow). The red dot represents
the anatomic femoral attachment. The red lines represent
the virtual anatomic MPFLr that we have drawn using an
anatomic femoral attachment (red dot). We can see that
the length of the MPFL-graft (the blue line) is quite
similar to the length of the virtual anatomic MPFL (the
red line). Anatomic and reconstructed MPFL are isometric
from 0 to 30° of knee flexion, that is there is less than
5 mm of length change throughout this range of motion.
In conclusion, the MPFL-graft behaves physiologically,
that is, it is isometric from 0 to 30º of knee flexion
the MPFL is not tight when the patella is not
subject to a lateral displacing force. In a state of
rest, the MPFL is not under tension.
attachment points is greatest [6]. If the fixation
were made in the flexion range in which the two
anchor points are closer, we would be subjecting
the graft to excessive tension when we flex the
knee further. Therefore, it would cause a significant increase in patellofemoral pressure that
would result in the future development of a
patellofemoral chondropathy and pain. To prevent excessive tension, do not pull the graft tight
at the time of fixation. If the other knee is
How to avoid excessive tension on the graft?
When we go to fix the graft, the assistant should
keep the patella well-centered in the femoral
trochlea with the knee at 30º of flexion. We do it
at 30º because it is at this knee flexion angle that
the distance between the femoral and patellar
The Failed Medial Patellofemoral Ligament …
A
289
B
Fig. 5 CASE # 3. Now, we are going to analyze the knee
with a bad result (right knee). In this knee, you can also
observe a clearly non-anatomic femoral attachment point.
It is too anterior A. However, in this knee unlike the left
one the graft does not behave physiologically. It was
isometric from 0 to 120° of knee flexion B. (B, Reused
with permission from Baishideng Publishing Group Inc.
From Sanchis-Alfonso V, et al. Failed medial patellofemoral ligament reconstruction: Causes and surgical
strategies. World J Orthop, 2017; 8(2): 115–129)
asymptomatic, the aim is to reproduce the degree
of patellar mobility of the healthy contralateral
knee. We must note that tighter is never better in
MPFL reconstruction surgery.
revision MPFLr surgery is unaddressed trochlear
dysplasia (18.4%).
While an isolated MPFLr is sufficient in the
group of patients with patellar instability from 0
to 30º, this might fail to control instability in the
group with instability beyond 30º [14]. Thus,
surgical failure in MPFLr might be due to not
considering risk factors for patellar instability
such as trochlear dysplasia or pathologic femoral
anteversion. Apprehension that is relieved at 30°
of knee flexion suggests a good clinical result
with an isolated MPFLr. An apprehension
beyond 30° of knee flexion suggests severe trochlear dysplasia, a significant femoral anteversion or both. With that, an associated surgical
procedure such as trochleoplasty and/or femoral
rotational osteotomy might be necessary [14, 15].
If the trochlear geometry is insufficient to
provide restraint, osteotomy to change the shape
of the trochlea has proven its value. Nelitz and
colleagues [16] performed an analysis of failed
surgery for patellar instability. They observed
that severe trochlear dysplasia (Dejour type BD) was significantly more frequent in the surgical failure group (89%) than in the non-surgical
failure group (21%). However, they did not find
2.2.3 Single Versus Double-Bundle
Patellar Graft Insertion
Migliorini and colleagues [13] performed a systematic review in which the isolated singlebundle (SB) was compared to the double-bundle
(DB) graft for recurrent lateral patellar instability.
In the DB group, there was more improvement in
function and a reduction of overall complications
when compared to the SB group. The authors
concluded that the current scientific evidence
support the use of the DB tendon graft for the
isolated MPFLr.
2.3 Failure to Recognize and Correct
Concomitant Risk Factors
for Instability
In a 2021 systematic review analyzing MPFLr
revision surgery by Walker and colleagues [5],
the authors showed that the second cause for
290
V. Sanchis-Alfonso and C. Ramírez-Fuentes
A
B
C
D
Fig. 6 CASE # 3. Right knee after revision surgery.
After a quasi-anatomical MPFLr the pain disappeared.
Femoral tunnel excessively anterior (blue arrow). New
femoral attachment (red arrow). The new ligament is
isometric from 0 to 30º of knee flexion C, D. That is, the
graft behaves physiologically. An interesting finding was
that the pain disappeared completely in spite of the fact
that the severe patellar chondral lesion was left alone. We
can conclude that femoral tunnel position is crucial for a
successful MPFLr. (A, B. Reused with permission from
Baishideng Publishing Group Inc. From Sanchis-Alfonso
V, et al. Failed medial patellofemoral ligament reconstruction: Causes and surgical strategies. World J Orthop,
2017; 8(2): 115–129)
differences relative to the patellar height ratio and
the TT-TG distance between the two groups. In
the same way, Wagner and colleagues [17] also
found that high degrees of trochlear dysplasia
correlate with poor clinical outcomes because the
MPFL graft might be overloaded given that there
is more instability in dysplastic situations. Similarly, Kita and colleagues [18] reported that
severe trochlear dysplasia is the most important
predictor of residual patellofemoral instability
after an isolated MPFLr. They have shown that a
combination of severe trochlear dysplasia with an
increased TT-TG distance was more likely to
affect the outcomes of MPFLr. We can conclude
that considering that high degree trochlear
dysplasia seems to be a major risk factor for
failure of isolated MPFLr, an associated
trochleoplasty might be considered in such cases
(Fig. 9). Moreover, trochlear dysplasia seems to
be a major risk factor for failure of MPFLr for
recurrent patellar dislocation in children and
adolescents [16]. These results in children are in
agreement with the literature in adults.
Dejour and colleagues [19] have shown that
the sulcus-deepening trochleoplasty is a good
revision option for the surgical treatment of
patients with persisting patellar dislocation after
MPFLr and high-grade trochlear dysplasia.
Similarly, Fucentese and colleagues [20] have
demonstrated that trochleoplasty is a useful and
The Failed Medial Patellofemoral Ligament …
Fig. 7 The anatomic variability of the adductor tubercle
may explain the anatomic variability of the MPFL femoral
fixation point. (Reused with permission from Baishideng
Publishing Group Inc. From Sanchis-Alfonso V, et al.
Failed medial patellofemoral ligament reconstruction:
Causes and surgical strategies. World J Orthop, 2017; 8
(2): 115–129)
reliable surgical technique to improve patellofemoral instability in patients with a dysplastic
trochlea. However, the same is not the case with
pain even though the significant improvement in
Fig. 8 A normal MPFL is
tighter in extension (C) than
in flexion (A, B). Beyond 60º
the graft is loose
A
291
stability after trochleoplasty is highly predictable.
The pain may even increase after surgery. In
conclusion, severe trochlear dysplasia can be
successfully treated with a trochleoplasty. The
trochleoplasty procedure not only corrects the
trochlear dysplasia, but also the increased TT-TG
distance.
Another risk factor that has been given great
importance is the pathological TT-TG distance
(>20 mm). Matsushita and colleagues [21]
demonstrated that isolated MPFL reconstructions
performed in CLPI with a TT-TG distance
greater than 20 mm yielded similar clinical outcomes to those performed with a TT-TG under
20 mm. Moreover, there were no re-dislocations
in either group. They concluded that a TT-TG
distance greater than 20 mm may not be an
absolute indication for medialization of the tibial
tubercle. Less and less importance is being given
to the TT-TG distance when indicating a surgery.
What is now emerging more and more
strongly is the importance of torsional alterations
in the genesis of patellar instability, specifically
B
C
292
V. Sanchis-Alfonso and C. Ramírez-Fuentes
Fig. 9 CASE # 4. Chronic lateral patellar instability in a
patient with grade D trochlear dysplasia (positive J-sign).
We note that the patella dislocates beyond 40° of knee
flexion. She had been operated on performing a proximal
realignment surgery. Lateral patellar instability resolved
after a MPFLr associated with a sulcus deepening
trochleoplasty. (Reused with permission from Baishideng
Publishing Group Inc. From Sanchis-Alfonso V, et al.
Failed medial patellofemoral ligament reconstruction:
Causes and surgical strategies. World J Orthop, 2017; 8
(2): 115–129)
the increment in femoral anteversion. Diederichs
and colleagues [22] have analyzed rotational
limb alignment in patients with non-traumatic
patellar instability and in controls using magnetic
resonance imaging (MRI). They found that
patellar instability patients have greater internal
femoral rotation, greater knee rotation, and a
tendency for genu valgum when compared to
healthy controls (Figs. 10, 11, 12 and 13). They
conclude that rotational malalignment may be a
primary risk factor in patellar instability that has
so far been underestimated. Cao and colleagues
[23] have shown that increased femoral anteversion along with a high-grade J sign is associated with MPFLr failure. These authors have
shown that MPFLr revision surgery by means of
rotational distal femoral osteotomy associated
with MPFLr provides satisfactory clinical outcomes in patients with increased femoral anteversion along with a high-grade J sign. Finally,
Zhang and colleagues [3] evaluated 15 patients
who presented with MPFL-graft laxity. A preoperative high-grade J-sign was identified in 66.7%
of these patients in comparison to 13.3% in the
control group with no graft laxity. Moreover,
they demonstrated that the presence of a preoperative high-grade J-sign and femoral tunnel
malposition were independent risk factors associated with residual graft laxity after MPFLr.
Both torsional deformities and coronal plane
deformities are associated with patellar instability
in some patients. The most common multiplanar
deformity is internal femoral torsion and genu
valgum.
The Failed Medial Patellofemoral Ligament …
293
Fig. 10 CASE # 5. This is the case of a 19-year-old male
patient who came to my office due to left lateral
patellofemoral instability. You can observe instability
beyond 30º. At the age of 12 years and 11 months, he
underwent surgery on his left knee (MPFLr + hemitransfer of the patellar tendon following the Goldthwait
technique + lateral retinaculum release). His lower-left
extremity showed significant valgus malalignment and
pathological femoral anteversion. At the age of 14 years
and 10 months, his right knee was operated on
(MPFLr + hemitransfer of the patellar tendon according
to Goldthwait technique). Both knees were bad but the
one that really disabled him was the left one (positive Jsign). In short, the patient is looking for a solution to the
left patellar instability, which is what really limited him.
He would have never bothered to go to the doctor because
of the right side as he was able to live with it. This case
highlights the importance of the knee valgus and femoral
anteversion in the genesis of patellar instability
2.4 Intrinsic Risk Factors Such
as Collagen Disorders
2.5 Patellar Fracture. How to Avoid It
Generalized joint hypermobility (4 or more
points on the Beighton score) has frequently been
considered a risk factor for patellar instability
(Fig. 14). However, Hiemstra and colleagues
[24] have shown that the presence of generalized
joint hypermobility has no influence on diseasespecific quality-of-life, physical symptoms score
or functional outcomes after MPFLr. Patients
with Ehlers-Danlos syndrome (Fig. 15) are prone
to patellar instability. In these patients, it is
important to consider the use of allografts for
MPFLr given the problems we may have with
autografts in this patient population [25]. Additionally, patients with Ehlers-Danlos suffer from
combined medial and lateral patellar instability
that requires reconstruction of both the MPFL
and the lateral patellofemoral ligament to achieve
adequate stability [26].
In a systematic review analyzing MPFLr revision
surgery performed by Walker and colleagues [5]
in 2021, the authors showed that the third cause
for revision surgery is a patellar fracture (11.8%).
Fulkerson and Edgar [27] described the medial
quadriceps tendon-femoral ligament -MQTFLreconstruction. This surgical technique avoids
the risk of patella fracture.
3
Reasons for Consultation
in a Patient with Failed MPFLr
Those patients who have a failed MPFLr are
going to consult for three reasons: (1) recurrence
of instability, (2) AKP, (3) limitation of the range
of motion of the knee or a combination of them.
294
V. Sanchis-Alfonso and C. Ramírez-Fuentes
Fig. 11 CASE # 5. X-rays show left-limb malalignment
on the coronal plane (knee valgus). Valgus 10º (4º
femur + 4º joint deformity + 2º tibia) (Mechanical axis—
red line). The patella is subluxed externally. In X-rays, we
can see a curvature of the left femur which represents the
normal anterior bow of the femur. This is highly
suggestive of internal rotation of the femur. It would
suggest a femoral anteversion. CT study: LEFT–femoral
anteversion = 43º (According to Murphy´s method)/
TT-TG distance = 26 mm/external tibial torsion = 25º/
tibio-femoral rotation (knee rotation) = 29º/Trochlear
inclination 3º; RIGHT–femoral anteversion = 26º/TTTG distance = 25 mm/external tibial torsion = 30º/knee
rotation = 25º/trochlear inclination 5º
3.1 Re-dislocation or Persistence
of Apprehension Without
Dislocation
tear again due to an indirect trauma to the knee. If
we add the high frequency of return to sports
practice, and the ensuing possibility of a new
knee trauma to the fact that more and more
MPFL are reconstructed, we can infer that the
number of re-dislocations after MPFLr will be
greater each time even though it is not as much as
we might think because only 31% of graft ruptures are due to knee trauma [29].
In most cases, re-dislocation after an isolated
MPFLr is non-traumatic (69%) [29]. In the rest
of the cases, it is secondary to an obvious trauma
(31%) [29]. In both cases, it can be due to a
femoral tunnel malposition or the presence of
anatomic risk factors. There are numerous risk
factors such as (1) trochlear dysplasia (types B
through D), (2) patella alta (CD index >1.2),
(3) genu valgum (>5º), (4) TT-TG distance
Schneider and colleagues [1] reported an instability recurrence rate of 1.2% (95% CI, 0.3–
2.1%) and a rate of apprehension persistence of
3.6% (95% CI, 0–7.2%) after isolated MPFLr for
the treatment of CLPI. However, Shah and colleagues [28] showed that recurrent apprehension
represents 32% of all the complications found in
MPFLr. Instability might be due to a rupture of
the MPFL graft, or could be secondary to the
failure to recognize associated risk factors for
instability. It has been reported that 84.1% (95%
CI, 71.1–97.1%) of patients return to sports after
an isolated MPFLr [1]. Thus, the return to sports
puts the reconstructed ligament at risk and so its
The Failed Medial Patellofemoral Ligament …
Fig. 12 CASE # 5.
Intraoperative X-rays. The
patella is well centered on the
distal femur after biplanar
supracondylar osteotomy
(lateral supracondylar open
wedge varus and rotational
osteotomy of the femur)
Fig. 13 CASE # 5. 3D
model. The patella is well
centered on the distal femur
after biplanar supracondylar
osteotomy (lateral
supracondylar open wedge
varus and rotational
osteotomy of the femur)
295
296
V. Sanchis-Alfonso and C. Ramírez-Fuentes
Fig. 14 Beighton score
greater than 20 mm and (5) torsional abnormalities (femoral anteversion greater than 25º and
external tibial torsion greater than 35º). Of all
these factors, the most prevalent in re-dislocation
cases are trochlea dysplasia (50%) and valgus
malalignment (35%) [29]. In atraumatic redislocations, 2 or more risk factors are present
in 65% of cases [29]. Sappey-Marinier and colleagues [30] have evaluated the importance of
the J-sign prior to isolated MPFLr surgery and
have observed that it is a risk factor for predicting surgical failure. Furthermore, they have
shown that a CDI > 1.3 is also another risk factor
for surgical failure. Cregar and colleagues [31]
have found that severe trochlear dysplasia (types
C and D) and a femoral tunnel malposition
(10 mm from Schottle's point) appear to be
responsible for the increased prevalence of
recurrent dislocation as well as worse patientreported outcomes. Despite this, the role of
concomitant bony procedures along with MPFLr
to correct the pathoanatomy remains unknown.
An incorrect femoral/patellar attachment point
can also lead to the excessive obliquity of the
The Failed Medial Patellofemoral Ligament …
297
might lead to graft laxity in extension and graft
tension in flexion with a clinical presentation of
AKP and loss of flexion. Moreover, excessive
graft tension with knee flexion could stretch the
graft and lead to its failure, predisposing the
patient to re-dislocation even though the tendon
graft used for MPFLr is substantially stronger
than the native MPFL. In contrast, an excessively
distal femoral attachment point may lead to graft
tension in extension and laxity in flexion. Its
clinical presentation would be an extension lag.
The femoral attachment point should mimic the
native anatomy as closely as possible to avoid the
problems cited. Therefore, it is essential to
accurately check the femoral tunnel placement
intra-operatively.
4
Fig. 15 Skin laxity in Ehlers-Danlos syndrome
graft, making it ineffective in preventing excessive lateral patellar displacement in the first 30º of
knee flexion (Fig. 16). This might explain a persistent lateral dislocation of the patella sometimes
seen with a healthy graft (Fig. 16). In this case,
remedying the instability can be achieved simply
by modifying the attachment points (Fig. 16).
3.2 Knee Pain and Limitation
of the Range of Motion
Medial knee pain after MPFLr is estimated to
occur in 30% of cases [32]. A normal MPFL is
tighter in extension than in flexion [6]. When the
femoral fixation point is placed too anteriorly, the
graft tightens when the knee is flexed [6]. At the
mid-term, it might provoke a severe patellar
chondropathy as well as PFOA in the long-term.
Thaunat and Erasmus [33] suggested that an
overly far proximal femoral attachment point
Revision Surgery After Failed
MPFLr
4.1 How Should We Plan It?
To plan a revision surgery on a patient with a
failed MPFLr, a dynamic 3D-CT study at 0º, 30º,
60º, 90º and 120º of knee flexion is performed
[6]. The objectives are to locate the femoral
attachment point and to evaluate the kinematic
behavior of the graft in vivo. Evaluation of the
length change behavior of the graft with knee
flexo-extension is very important because it
indirectly allows us to know whether the graft is
taut in flexion or not [6].
Take note that a non-anatomic femoral fixation point is not necessarily associated with a
failed reconstruction. In other words, the expected long-term clinical result should be good if an
MPFLr has a non-anatomic femoral fixation
point but in the in vivo kinematic study it has an
adequate change of length pattern and an optimal
isometry from 0 to 30º [6]. Hence, the persistent
pain and instability could not be attributed to this
non-anatomic femoral fixation point. Thus, causes of graft failure other than the choice of the
femoral fixation point should be highlighted.
298
V. Sanchis-Alfonso and C. Ramírez-Fuentes
Fig. 16 CASE # 6. A 30-year-old female patient
suffering from very severe left AKP had had an MPFLr
done. It had been carried out with a partial thickness
quadriceps tendon. Clinically, there was no evidence of
patellofemoral tracking disorders (negative J-sign).
Despite having an intact MPFL, the patella could be
dislocated laterally while the patient was under general
anesthesia. In her case, the instability was caused by an
inappropriate graft length change pattern during knee
flexion and extension. The lateral patellar instability and
the pain completely went away following an anatomic
double-bundle MPFLr with a semitendinosus tendon
graft. (Reused with permission from Baishideng Publishing Group Inc. From Sanchis-Alfonso V, et al. Failed
medial patellofemoral ligament reconstruction: Causes
and surgical strategies. World J Orthop, 2017; 8(2): 115–
129)
4.2 General Principles
in the Management
of Failed MPFLr
question, we will not be able to find a solution to
the problem that our patients present.
A knowledgeable surgeon and a correct diagnosis of the failure are crucial factors to resolve a
“Failed MPFLr”. There is a key question that we
must ask ourselves. Why did the previous surgery fail? If we do not find an answer to this
4.2.1 Confirm Diagnosis
Stress X-rays can confirm the diagnosis. We
must apply force for medial and lateral displacement of the patella. Then, we measure the
displacement, compare it with the contralateral
normal knee, and record it.
The Failed Medial Patellofemoral Ligament …
4.2.2 Define the Deficient Restraints
Which Caused the
Instability—Reconstruction
of the Deficient Restraints
and Limb Realignment
When It is Grossly
Abnormal
What causes patellar instability? That is the key
question when we indicate surgery to a patient
with CLPI. Patellar Instability is the result of a
failure of the patellar restraints (MPFL, lateral
retinaculum and trochlear geometry) and an
increment of the lateral vector of the quadriceps.
This vector is increased by knee valgus,
increased internal torsion of the femur and
increased external torsion of the tibia (abnormal
limb alignment). Instability occurs in the range
between 0º and 30º of knee flexion in approximately 70% of the cases. In this range-of-motion,
patellar stability depends mainly on the MPFL
[14]. Beyond 30º of knee flexion, patellar stability mainly depends on the bony anatomy of
the femoral trochlea and femoral anteversion
[14]. The primary soft tissue restraint to lateral
patellar dislocation is the MPFL. That is the
reason why MPFLr is very important. Trochlear
dysplasia will cause stress on the MPFL for
which this ligament is not designed. The lateral
retinaculum prevents lateral displacement of the
patella. Therefore, an increment in lateral patellar
instability is expected after LRR.
4.3 Steps In Revision MPFLr Surgery
4.3.1 Correction of Patellofemoral
Tracking
When there is a maltracking (positive J-sign), the
first step would be to correct it. In my series, the
most frequent cause of patellar maltracking is
severe trochlear dysplasia. However, in some
cases, the patellar maltracking is secondary to
excessive femoral anteversion. Trochleoplasty
should be only performed when the patella dislocates at high degrees of knee flexion, mostly in
revision surgeries. When the maltracking can be
detected only actively, selective epidural
299
analgesia can help to evaluate intraoperatively the
active patellar excursion after realignment surgery. After realignment, the anesthesiologist
wakes the patient and we ask her to flex the knee
(see Video Case # 6). In this way, we can observe
the correction of the patellofemoral tracking after
sulcus deepening trochleoplasty before fixing the
MPFL.
4.3.2 Stabilization of the Patella
Once the patellofemoral maltracking has been
corrected, we stabilize the patella by performing
an MPFLr. In some infrequent cases, once the
MPFL has been reconstructed, patellar tilt may
still be abnormal. In these cases, a third surgical
step in the lateral retinaculum (LR) may be necessary to achieve good patellofemoral balance.
The decision to operate or not on the lateral
patellar retinaculum is an intraoperative decision
based on the patella tilt test [34]. To do this test, a
transverse K wire is placed in the proximal patella,
from medial to lateral. With the knee in full
extension and at 20º of flexion, the K wire should
be parallel to the surgery table. If the K wire is
tilted (positive test) within this range-of-motion,
lateral patellar retinaculum lengthening is needed.
In cases of multidirectional patellar instability,
the LR reconstruction should be the final
step. The reason we perform LR reconstruction
as the last step is because MPFLr not only stabilizes the patella laterally but also medially.
To guide the patella towards the trochlear
sulcus during the first degrees of knee flexion,
both the MPFL and the LR must interplay in a
harmonious way. Both ligaments behave similarly to the reins of a horse. Both reins must have
some degree of tension. They are not very tense
but they are not loose either. If one of the reins is
completely loose, the horse is inclined towards
the opposite direction as occurs in the patella.
This patellofemoral imbalance may be responsible for pain. Following the same simile, we can
compare the patella with the mouthpiece and the
trochlea with the tongue. If we tense the reins
very much we will nail the mouthpiece into the
tongue and that hurts the horse. Similarly, if we
tense both ligaments during surgery, we will
300
increase the patellofemoral joint reaction and it
will provoke a patellar overload and patellar
chondropathy and PFOA in the long-term.
4.3.3 Patellar Chondropathy. What Can
We Do?
Patellar condropathy is very common in cases of
CLPI (Figs. 17 and 18). We only remove
unstable cartilage flaps, but other cartilage
lesions are not addressed. Patellar chondropathy
could be responsible for AKP in the patient with
CLPI. However, in the vast majority of the cases,
once the patella has been stabilized, the pain
disappears even though the chondral lesion is left
alone. Loose bodies are removed.
Fig. 17 Patellofemoral chondropathy after an inadequate
MPFLr. In this case, the cartilage lesion was left alone,
and only patellofemoral balance was corrected by means
of a new anatomic MPFLr and an LR lengthening
procedure. The patient is pain-free even though nothing
was done to the cartilage. Moreover, the patellar tilt was
V. Sanchis-Alfonso and C. Ramírez-Fuentes
4.4 Complex Revision Cases—MPFLr
Without Bone Tunnels
In multi-operated patients, revision surgery might
be a real challenge because we have found
multiple tunnels and implants in both the patellar
insertion area as well as in the femoral insertion
area. Therefore, there may be an increased risk of
patella fractures as well as tunnel collisions that
may compromise the fixation. In these cases, we
might consider surgical techniques without bone
tunnels. One option would be to use an autologous quadriceps tendon graft along with its
native patellar insertion site and using the AMT
not completely corrected. A Preop-CT. B Iatrogenic
patellar chondropathy. C Postop-CT. (Republished with
permission of AME Publishing Company. From V
Sanchis-Alfonso, Treating complications of operative
management for patellofemoral pain, Ann Joint, 3:27,
2018)
Fig. 18 Patellofemoral chondropathy after an inadequate MPFLr. In this case, the cartilage lesion was left alone, and
only a new anatomic MPFLr was performed. The patient is pain-free even though nothing was done to the cartilage
The Failed Medial Patellofemoral Ligament …
as an elastic femoral fixation. With this technique, we avoid a two-stage procedure.
4.5 Outcomes After Revision Surgery
Chatterton and colleagues [35] have reported
acceptable patellar stability after revision surgery. However, knee pain and subjective outcomes do not improve significantly. In this sense,
Zimmermann and colleagues [36] have observed
better outcomes when revision surgery is performed to solve recurrent instability than when it
is performed for patellofemoral pain or limitation
of the range of mobility.
5
Take Home Messages
– An MPFLr should not be performed if the
patella cannot be laterally dislocated.
– An MPFLr does not work to pull the patella
into position. Its role is only to stabilize the
patella once the patellofemoral tracking has
been corrected.
– An anatomic femoral fixation point is an easy
and reproducible way to achieve the optimal
length change behavior of the graft with knee
flexo-extension to obtain satisfactory longterm clinical results.
– To avoid a failed MPFLr, we must respect the
anatomy.
– Not all patients with lateral patellar instability
are equal. The etiology of lateral patellar
instability is multifactorial. Therefore, there
are several subsets of patients with lateral
patellar instability. In that light, treatment
must be tailor-made.
– In cases of multidirectional instability, we
must first correct the maltracking. Second, we
must reconstruct the MPFL. The final step is
to reconstruct the LR.
301
6
Key Message
– A failed MPFLr can be more disabling than
primary patellar instability. Some patients
who have experienced more than one patellar
dislocation are still highly functional and may
not need surgery. Only when patients are
significantly limited in their daily living
activities should the MPFLr be considered.
We must be extreme care with recommending
surgery.
References
1. Schneider DK, Grawe B, Magnussen RA, et al.
Outcomes after isolated medial patellofemoral ligament reconstruction for the treatment of recurrent
lateral patellar dislocations: a systematic review and
meta-analysis. Am J Sports Med. 2016;44:2993–
3005.
2. Sanchis-Alfonso V. Guidelines for medial patellofemoral ligament reconstruction in chronic lateral
patellar instability. J Am Acad Orthop Surg.
2014;22(3):175–82.
3. Zhang Z, Song GY, Zheng T, et al. The presence of a
preoperative high-grade J-sign and femoral tunnel
malposition are associated with residual graft laxity
after MPFL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2021;29(4):1183–90.
4. Parikh SN, Nathan ST, Wall EJ, et al. Complications
of medial patellofemoral ligament reconstruction in
young patients. Am J Sports Med. 2013;41
(5):1030–8.
5. Walker M, Maini L, Kay J, et al. Femoral tunnel
malposition is the most common indication for
revision medial patellofemoral ligament reconstruction with promising early outcomes following revision reconstruction: a systematic review. Knee Surg
Sports Traumatol Arthrosc. 2021. https://doi.org/10.
1007/s00167-021-06603-x.
6. Sanchis-Alfonso V, Ramírez-Fuentes C, MontesinosBerry E, et al. Femoral insertion site of the graft used
to replace the medial patellofemoral ligament influences the ligament dynamic changes during knee
flexion as well as clinical outcome. Knee Surg Sports
Traumatol Arthrosc. 2017;25:2433–41.
302
7. Schoettle PB, Schmeling A, Rosenstiel N, et al.
Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. Am J Sports Med. 2007;35(5):801–4.
8. Ziegler CG, Fulkerson JP, Edgar C. Radiographic
reference points are inaccurate with and without a
true lateral radiograph: the importance of anatomy in
medial patellofemoral ligament reconstruction. Am J
Sports Med. 2016;44(1):133–42.
9. Sanchis-Alfonso V, Ramirez-Fuentes C, MontesinosBerry E, et al. Radiographic location does not ensure
a precise anatomic location of the femoral fixation
site in medial patellofemoral ligament reconstructions. Orthop J Sports Med. 2017. https://doi.org/10.
1177/2325967117739252.
10. Chen J, Han K, Jiang J, et al. Radiographic reference
points do not ensure anatomic femoral fixation sites
in medial patellofemoral ligament reconstruction: a
quantified anatomic localization method based on the
saddle sulcus. Am J Sports Med. 2021;49(2):435–41.
11. Ishikawa M, Hoo C, Ishifuro M, et al. Application of
a true lateral virtual radiograph from 3D-CT to
identify the femoral reference point of the medial
patellofemoral ligament. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3809–17.
12. Fujino K, Tajima G, Yan J, et al. Morphology of the
femoral insertion site of the medial patellofemoral
ligament. Knee Surg Sports Traumatol Arthrosc.
2015;23(4):998–1003.
13. Migliorini F, Trivellas A, Colarossi G, et al. Singleversus double-bundle patellar graft insertion for
isolated MPFL reconstruction in patients with
patellofemoral instability: a systematic review of
the literature. Arch Orthop Trauma Surg. 2020;140
(6):769–76.
14. Sanchis-Alfonso V. How to deal with chronic
patellar instability: what does the literature tell us?
Sports Health. 2016;8(1):86–90.
15. Imhoff FB, Cotic M, Liska F, et al. Derotational
osteotomy at the distal femur is effective to treat
patients with patellar instability. Knee Surg Sports
Traumatol Arthrosc. 2019;27(2):652–8.
16. Nelitz M, Theile M, Dornacher D, et al. Analysis of
failed surgery for patellar instability in children with
open growth plates. Knee Surg Sports Traumatol
Arthrosc. 2012;20:822–8.
17. Wagner D, Pfalzer F, Hingelbaum S, et al. The
influence of risk factors on clinical outcomes
following anatomical medial patellofemoral ligament
(MPFL) reconstruction using the gracilis tendon.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(2):318–24.
18. Kita K, Tanaka Y, Toritsuka Y, et al. Factors
affecting the outcomes of double-bundle medial
patellofemoral ligament reconstruction for recurrent
patellar dislocations evaluated by multivariate analysis. Am J Sports Med. 2015;43(12):2988–96.
19. Dejour D, Byn P, Ntagiopoulos PG. The Lyon’s
sulcus-deepening
trochleoplasty
in
previous
V. Sanchis-Alfonso and C. Ramírez-Fuentes
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
unsuccessful patellofemoral surgery. Int Orthop.
2013;37(3):433–9.
Fucentese SF, Zingg PO, Schmitt J, et al. Classification of trochlear dysplasia as predictor of clinical
outcome after trochleoplasty. Knee Surg Sports
Traumatol Arthrosc. 2011;19(10):1655–61.
Matsushita T, Kuroda R, Oka S, et al. Clinical
outcomes of medial patellofemoral ligament reconstruction in patients with an increased tibial
tuberosity-trochlear groove distance. Knee Surg
Sports Traumatol Arthrosc. 2014;22(10):2438–44.
Diederichs G, Kohlitz T, Kornaropoulos E, et al.
Magnetic resonance imaging analysis of rotational
alignment in patients with patellar dislocations. Am J
Sports Med. 2013;41(1):51–7.
Cao Y, Zhang Z, Shen J, et al. Derotational distal
femoral osteotomy yields satisfactory clinical outcomes in pathological femoral rotation with failed
medial patellofemoral ligament reconstruction. Knee
Surg Sports Traumatol Arthrosc. 2021. https://doi.
org/10.1007/s00167-021-06739-w.
Hiemstra LA, Kerslake S, Kupfer N, et al. Generalized joint hypermobility does not influence clinical
outcomes following isolated MPFL reconstruction
for patellofemoral instability. Knee Surg Sports
Traumatol Arthrosc. 2019;27(11):3660–7.
Williams J, Hutt J, Rickman M. Anterior cruciate
ligament reconstruction in Ehlers-Danlos syndrome.
Case Rep Orthop. 2015;2015:1–3.
Shubert DJ, McDonough EB. Bilateral medial and
lateral patellofemoral ligament reconstruction in a
patient with hypermobility type Ehlers-Danlos syndrome: a case report. JBJS Case Connect. 2019;9(3):
e0359.
Fulkerson JP, Edgar C. Medial quadriceps tendonfemoral ligament: surgical anatomy and reconstruction technique to prevent patella instability. Arthrosc
Tech. 2013;12,2(2):e125–8.
Shah JN, Howard JS, Flanigan DC, et al. A systematic review of complications and failures associated
with medial patellofemoral ligament reconstruction
for recurrent patellar dislocation. Am J Sports Med.
2012;40(8):1916–23.
Feucht MJ, Mehl J, Forkel P, et al. Failure analysis in
patients with patellar redislocation after primary
isolated medial patellofemoral ligament reconstruction. Orthop J Sports Med. 2020. https://doi.org/10.
1177/2325967120926178.
Sappey-Marinier E, Sonnery-Cottet B, O´Loughlin P,
et al. Clinical outcomes and predictive factors for
failure with isolated MPFL reconstruction for recurrent patellar instability: a Series of 211 reconstructions with a minimum follow-up of 3 years. Am
J Sports Med. 2019;47(6):1323–30.
Cregar WM, Huddleston HP, Wong SE, et al.
Inconsistencies in reporting risk factors for medial
patellofemoral ligament reconstruction failure: a
systematic review. Am J Sports Med. 2021. https://
doi.org/10.1177/03635465211003342.
The Failed Medial Patellofemoral Ligament …
32. Enderlein D, Nielsen T, Christiansen SE, et al.
Clinical outcome after reconstruction of the medial
patellofemoral ligament in patients with recurrent
patella instability. Knee Surgery, Sport Traumatol
Arthrosc. 2014;22(10):2458–64.
33. Thaunat M, Erasmus PJ. The favourable anisometry:
an original concept for medial patellofemoral ligament reconstruction. Knee. 2007;14(6):424–8.
34. Arendt EA. Lateral-sided surgery with MPFL reconstruction: when is this needed? La Patella, Sauramps
Medical, Montpellier;2012. p. 119–123.
303
35. Chatterton A, Nielsen TG, Sorensen OG, et al.
Clinical outcomes after revision surgery for medial
patellofemoral ligament reconstruction. Knee Surg
Sports Traumatol Arthrosc. 2018;26(3):739–45.
36. Zimmermann F, Milinkovic DD, Bortlein J, et al.
Revision surgery for failed medial patellofemoral
ligament reconstruction results in better diseasespecific outcome scores when performed for recurrent
instability than for patellofemoral pain or limited range
of motion. Knee Surg Sports Traumatol Arthrosc.
2021. https://doi.org/10.1007/s00167-021-06734-1.
Surgical Treatment of Recurrent
Patellar Instability: History
and Current Concepts
Christopher A. Schneble,
David A. Molho, and John P. Fulkerson
1
Introduction: Background
and History
Treatment for recurrent patella instability in the
1970s and 1980s centered around two main
schools of thought: John Insall’s viewpoint,
which advocated for an aggressive lateral
advancement of the medial soft tissue [1], and the
collective position of Hauser, Southwick, Trillat
and Elmslie who supported the use of a standalone tibial tubercle transfer [2–4]. Both schools
of thought were effective in preventing recurrent
patella dislocation [5–9]. Despite short term
success, both the imbrication type procedures
and the posteromedial tibial tubercle transferring
osteotomies (TTOs) eventually often led to
medial patellofemoral arthritis [7, 10, 11]. Many
of the stand-alone tibial tubercle transfers, notably the Hauser procedure, resulted in movement
of the patella quite far medially, distally, and
posteriorly along the proximal tibia. This often
would induce altered articular loading, eventually leading these patients to develop arthritis
C. A. Schneble D. A. Molho J. P. Fulkerson (&)
Department of Orthopaedics and Rehabilitation,
Yale School of Medicine, New Haven, CT, USA
e-mail: john.fulkerson@yale.edu
C. A. Schneble
e-mail: Christopher.schneble@yale.edu
D. A. Molho
e-mail: david.molho@yale.edu
from persistent overload [2, 12]. Around the
same time, Maquet proposed anteriorization of
the tibial tuberosity to unload an arthritic patellofemoral joint [13, 14]. The Maquet procedure
became an effective option for alleviating
arthritic patellofemoral pain, but anteriorization
alone fell short in resolving patellofemoral
instability [15].
During the late 1970s when surgical treatments for patellar instability were continuing to
evolve, John Fulkerson was receiving his training under Wayne Southwick. Southwick’s
approach for surgically addressing recurrent
patellar instability often involved a dovetailed
patellar tendon transfer that moved the tibial
tuberosity medially [3]. The insight that Fulkerson gathered from these experiences led him to
consider tibial tuberosity transfers as his preferred technique for patella stabilization. For the
rest of his career he sought the optimal implementation of TTOs in the treatment of recurrent
patella instability.
In 1983, John Fulkerson first described the
anteromedial tibial tuberosity transferring
osteotomy (AMTTO) for the treatment of patellar
malalignment [16], as well as for lateral patellofemoral arthritis, which at the time was called
excessive lateral pressure syndrome by Paul Ficat
[17–19]. The AMTTO combined the benefits of
articular unloading with those of improved
extensor mechanism vector alignment [16]. This
also came with the added benefit of bone-to-bone
healing at the osteotomy site without distraction
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_21
305
306
C. A. Schneble et al.
Fig. 1 A, B Bilateral Merchant axial radiographs of a
patient with recurrent right patellar instability and recurrent dislocations. On subsequent follow-up examinations
she exhibited persistent lateral tracking. The top row of
images (1A) was immediately after the first dislocation
event for the right knee, showing increased lateral
subluxation and tilting in comparison to the nonsymptomatic left side. The bottom row of images (1B)
were acquired a few years later following multiple repeat
dislocations on the right, while the left side remained
asymptomatic. Progression of lateral patellar tilting and
lateral subluxation can be seen. It is important to note that
the magnitude of patellar tilt and subluxation can be be
dampened on axial radiographs with knee flexion beyond
30 degrees
across the osteotomy site as seen in a Maquet
procedure [20, 21]. AMTTO was effective in
minimizing the likelihood of medial patellofemoral overload and subsequent arthritis due to
over medialization, posteromedialization or distalization during the previously described patellar
tendon transfers [22–24]. Fulkerson was a strong
advocate for using AMTTO procedures to treat
lateral patellar instability for almost 20 years,
finding the procedure to work remarkably well
for both recurrent patellar instability and the
prevention of overload induced arthritis [11, 25–
27]. Jack Farr, William Post, Brian Cole, John
Albright, Seth Sherman and others have all
contributed towards our understanding of how
effective an AMTTO can be [19, 28–32].
A salient lesson gathered from Fulkerson’s
experiences was that the correction of a laterally
tracking extensor mechanism was rather effective
at preventing recurrent instability. Even without
medial patellofemoral reconstruction, anteromedialization (AMZ) of the tibial tuberosity surfaced as
a viable solution for restoring patellar stability in
most patients who had evidence of a laterally
tracking patella on Merchant view axial
radiographs [16, 25, 27] (Fig. 1A, B). The notion
that correction of a laterally tracking vector alone
can often result in adequate stability became an
important principle in John Fulkerson’s practice.
Despite the utility of a TTO, restoring soft tissue
support can improve success rates, particularly in
patients with trochlea dysplasia, while adding little
additional risk when done properly [33–36]. In
contrast, failure to balance lateral tracking, by
either a medial or anteromedial TTO, can leave a
patient vulnerable to late patellofemoral arthritis
secondary to lateral focal overloading (Fig. 2A–C).
Apart from the tibial tubercle, other osseous
locations can be osteotomized for treatment of
patellofemoral instability. Robert Teitge correctly pointed out that patellar instability can be
related to femoral rotation problems, including
excessive femoral anteversion that results in a
more lateralized extensor mechanism vector [37].
He went on to suggest that a femoral derotational osteotomy would be an appropriate
treatment option [37]. Performing a compensatory TTO, however, proves to be a much more
benign and consistently effective treatment, so
few orthopedic surgeons do femoral de-rotation
Surgical Treatment of Recurrent Patellar Instability …
A
B
307
C
Fig. 2 A–C Radiographic and arthroscopic images of a
patient who developed lateral focal articular overloading
from persistent lateral patellofemoral instability. Figure A shows a 30-degree Merchant axial radiograph with
joint space narrowing laterally, osteophyte formation, and
slight lateral patellar tilting and translation. Figure B shows an MRI of the same knee, however this
was acquired in 20° of knee flexion. The magnitude of
lateral patellar tilting and translation is more accentuated
in this early flexion range. Articular cartilage wear and
thinning along the lateral patellar facet is present.
Figure C shows an intra-articular view of the lateral
patellofemoral compartment as viewed from the anterolateral portal. The lateral patellar facet exhibits chondral
fibrillation, fissuring and cartilage loss has extended down
to nearly the level of the subchondral bone
osteotomies for the treatment of patellar instability, even in the presence of excessive femoral
anteversion, with an exception being if anteversion were to need correction for other reasons, in
which case it will usually be done bilaterally.
Since the time of Insall, an increased understanding of the intricate patellofemoral stabilizing anatomy has led to advancements in soft
tissue stabilization procedures. João Ellera
Gomes first described the notion of medial
patellofemoral ligament (MPFL) reconstruction
for the treatment of recurrent lateral patella
instability in 1992 [38]. Subsequently, Don
Fithian popularized the technique in the United
States and referred to the MPFL as the primary
restraint to lateral dislocation of the patella [39,
40]. In an attempt to translate the anatomical
location of the MPFL to its corresponding
radiographic position, Schöttle developed radiographic criteria that could be used to identify the
femoral origin of the MPFL [41]. These criteria
have proved helpful in MPFL reconstruction
procedures, however others, like SanchisAlfonso, have emphasized the importance of an
open dissection to assure precise, anatomical
placement of the femoral tunnel in every case
[42, 43]. MPFL reconstructions became very
popular given they were, and continue to be, very
effective procedures for treating recurrent instability [44].
Thanks to Mochizuki, Smigielski, Tanaka,
Baldwin, Hinckel, Chahla, and others, the complex anatomy of the medial patellofemoral
restraints have been further elucidated [45–50].
Their work identified the MPFL as only a portion
of a much more intricate medial patellofemoral
complex (MPFC), a term coined by Miho Tanaka
[51, 52]. In a quest to understand the intricate
medial patellofemoral anatomy, Tanaka described the midpoint of the proximal MPFC, located
at the junction of the MPFL and the medial
quadriceps tendon-femoral ligament (MQTFL)
(Fig. 3A, B) [52]. With the MQTFL being
roughly equivalent to the MPFL in resisting lateral patellar translation and dislocation, there has
been an increased interest in reconstructing this
portion of the complex [53–56]. Despite
advancements in our understanding of the MPFC
and the MQTFL, more time is still needed for
long-term outcome studies to surface regarding
MQTFL or combined reconstructions. Thus far,
MQTFL reconstructions have shown promise as
a viable option for restoring medial soft tissue
restraint [56] (Fig. 4A, B).
In addition to proximal patellofemoral
restraints, there are also more distally located
patellotibial and patellomeniscal restraints.
Hinckel found that the distal medial restraints are
primarily responsible for maintaining patellar
stability in flexion [49, 57].
308
Fig. 3 A, B Figures 3A and 3B show are an artist
rendition of the medial patellofemoral restraints. Figure A illustrates the medial side of the knee, with the
medial patellofemoral complex (MPFC) marked by a gold
star. Figure B illustrates an anterior view of the distal
femur, and the bony undersurface of a reflected patella.
The MPFC is outlined in light blue, extending from the
medial femur to its insertion on the medial quadriceps
A
Fig. 4 A, B Axial right knee MRI slices of an adolescent
patient with recurrent patellar instability and dislocations.
The left image (A) was acquired after a traumatic
dislocation that resulted in a medial patella osteochondral
flap. She was treated with a medial patellofemoral
ligament (MPFL) reconstruction and debridement of this
osteochondral flap. Her instability unfortunately recurred
C. A. Schneble et al.
tendon (medial quadriceps tendon femoral ligament) and
the medial osseous patella (medial patellofemoral ligament). AMT = Adductor magnus tendon; VMO = Vastus
medialis obliquus; R = Rectus femoris; QT = quadriceps
tendon; PT = patellar tendon; MCL = Medial collateral
ligament; SM = Tibial insertion of semimembranosus;
MQTFL = Medial quadriceps tendon femoral ligament;
MPFL = Medial patellofemoral ligament
B
and two years later she presented with worsened patellar
tilt and subluxation, which is exhibited in the MRI image
on the right (B). Her physes were not yet closed, and she
was successfully treated with a medial quadriceps tendonfemoral ligament (MQTFL) reconstruction without recurrence of instability
Surgical Treatment of Recurrent Patellar Instability …
In recent years with MPFL reconstructions
becoming more frequently performed, outcomes
data has become more available. In 2018, Liu and
Shubin Stein demonstrated that isolated MPFL
reconstruction was effective at restraining the
patella from lateral dislocation, even in patients
with Dejour B and D dysplastic trochleae [58].
Further, MPFL reconstruction was shown to be
effective in the setting of high TT-TG measurements, raising further questions about when a
TTO of any sort is appropriate [58].
The concept of trochleoplasty was first raised
by Albee [59], then Masse [60], being subsequently popularized by Schöttle, Dejour, Bereiter, Diduch, and others [61–66]. Often being
performed to address patellar instability in
Dejour B or D patients, little popularity was
adopted in the United States because of the
potential adverse effects on articular cartilage, the
magnitude of the surgery, potential long-term
consequences, and evidence suggesting a successful stabilization could be obtained without
the need for trochleoplasty [63, 67–72]. While
Hiemstra has indicated trochleoplasty is an
acceptable procedure for instability in patients
with high-grade dysplasia, outcomes data stems
from lower evidence studies with substantial
heterogeneity amongst study populations [63, 72,
73]. Additionally, Rouanet has noted concerningly high rates of arthritis occurring 15 years
post-trochleoplasty [72].
Distalization of the extensor mechanism has
been proposed for patients with patella alta to
facilitate earlier engagement of the patella into
the deeper distal portion of the trochlea [74, 75].
A distalizing TTO (DTTO), can achieve this,
however it carries an increased risk of non-union
that occurs as a result of the increased load
experienced across the osteotomy site with knee
flexion [76].
Although lateral instability is exceedingly
more common, medial patellar instability can also
occur. Sanchis-Alfonso described the risks and
symptoms of medial patellar instability, often
iatrogenic in nature, and suggested this diagnosis
must be considered in patients with recurrent
symptoms of instability after surgery [77].
309
2
Putting It All Together: What
Does Fulkerson Do Now?
For patients with recurrent patellar instability,
Fulkerson’s approach is a distillation of the work
of many patellofemoral scholars. Ultimately, the
goal is to design an optimal procedure, or combination of procedures, to maximize stability,
function, and long-term joint preservation. Surgical planning for patellar instability can be
complex particularly given the dynamic forces
seen across the patellofemoral joint and the
complex three-dimensional (3D) morphology of
the trochlea. Traditional two-dimensional (2D)
imaging gives only a glimpse of the whole
multidimensional problem, limiting one’s ability
to assess the confluence of factors that affect
patellar stability. Cross sectional imaging provides a limited depiction of the trochlear topography that drives patellar instability. In many
cases, however, this often adequate to successfully develop a treatment plan.
An understanding of the dynamic plane of
patellar tracking over the dysplastic trochlea,
however, is often necessary to develop an optimal reconstruction plan in more complex cases.
In most cases, instability is derived from several
influencing factors. Treatments should be
designed using information from the history and
clinical examination, along with observations
from gait and imaging. For instance, a patient
with recurrent patellar dislocations, minimal Jsign, central tracking, a normal gait pattern, and
mild to moderate trochlear dysplasia will likely
do very well with a medial patellofemoral complex reconstruction alone, and further diagnostic
studies likely are not needed. The majority of
patients with recurrent patellar dislocations happen to fall in this category.
Deciding when to add a TTO is challenging in
some cases, making the history and physical
examination even more critical. If there is
increased ligamentous laxity, valgus, or internal
rotation during gait, a more prominent J sign,
obvious clinical lateral maltracking, or a history
of failed prior surgery, one should consider a
TTO and the potential benefit it may confer.
310
A good primary screening tool for deciding when
to add a TTO is a properly done neutral rotation
30-degree knee flexion axial radiograph, known
as a Merchant view, which can generally be
acquired in the office. If the patella sits laterally
on this view (see Fig. 1a, b) adding a TTO may
be in the patient’s best interest. Other traditional
radiographic measurements like the CatonDeschamps ratio (C-D ratio), the tibial tubercletrochlear groove (TT-TG) distance, the lateral
trochlear inclination (LTI) angle, and the Dejour
classification are also helpful in surgical decision
making. With these clinical and radiographic
parameters, one gains a general overview of the
collective problem and whether a TTO will
provide added benefit.
Three-dimensional imaging can be very
helpful when one is unsure about whether to
perform a TTO. Using 3D images one can better
discern the obliquity and curvilinearity of the
trochlea, thereby providing an appreciation for
the expected path of patellar tracking (Fig. 5a–c).
In particular, one can infer the entry point for the
patella as it enters the trochlea, and its coronal
plane distance from the central trochlea. Threedimensional reformats from a 20-degree knee
flexion weight bearing CT yields a very helpful
depiction of how the patella engages with trochlea in early knee flexion. This early interaction
of engagement is important in instability patients
when considered in the context of a dysplastic
trochlea and the aforementioned factors.
Deciding whether to add a TTO also comes
down to risk and reward for each patient. As part
of this assessment the surgeon should gauge the
following:
1. What is the projected risk of redislocation
without a TTO?
2. What is the likelihood of developing lateral
patellofemoral arthritis if a TTO is not done?
3. What is the patient’s healing and rehabilitation potential?
Over time, certain findings have consistently
influenced the likelihood that Fulkerson would
C. A. Schneble et al.
perform a TTO in a given patient, however no
single finding was ever considered as absolute or
in isolation. These findings are:
1. A prominent J sign with evidence of a lateral
patella entry point
2. A TT-TG over 15–20 mm (causes consideration for the need to medialize the tibial
tubercle)
3. C-D ratio > 1.3 (causes consideration for the
need to distalize the tibial tubercle)
4. A curvilinear dysplastic trochlea
5. The presence of a connective tissue disorder,
or ligamentous laxity
6. Evidence of excessive femoral anteversion
7. Evidence of patellofemoral articular damage
that would benefit from the unloading effects
of an AMTTO.
It is important to synthesize the magnitude of
contribution from each factor, and the risks
associated with their correction. Not all forms of
malalignment need be corrected when identified,
but when found to confer a sizeable influence
towards persistent instability they will often need
to be addressed for successful treatment. Tibial
tubercle transfer can serve as a powerful procedure, when indicated, with the potential to provide improved extensor mechanism tracking
while also off-loading painful or progressive
articular lesions.
Compared to a TTO, trochleoplasty has been
quite uncommon in Fulkerson’s approach to
patellar instability over the years. Nonetheless, in
selected cases, recession of a prominent proximal
medial trochlear ridge or spur, usually done
arthroscopically, has been performed occasionally, usually done to facilitate patellar entry into
the femoral trochlea at the time of a concomitant
distalizing tibial tubercle transfer, as recommended by Rush and Diduch [64].
In summary, recurrent instability of the patella
can often be treated successfully by reconstruction of the medial patellofemoral complex
(MPFC) in most patients, without additional
procedures. If lateral maltracking is a definable
Surgical Treatment of Recurrent Patellar Instability …
311
Fig. 5 A–C From left to right, the top row depicts
progressively distal axial MRI slices of a right distal
femur afflicted with trochlear dysplasia and recurrent right
patellar instability and dislocations. Prior medial patellofemoral ligament (MPFL) reconstruction was unsuccessful in preventing recurrence. The second row, from left to
right, shows progressively distal axial CT scan slices.
Both the MRI and CT images shown reveal a flattening of
the trochlea consistent with dysplasia, however the nadirs
of the trochlea at each slice level can be difficult to
synthesize in order to garner a fluid understanding of what
patellar tracking path would result in the most optimal
bony constraint. The bottom series of images are 3Dimensional CT reformats that were created using ScanIP
(Synopsys, Mountain View, CA). The red lines reveal the
estimated deepest points of the trochlea along its entirety.
Visualizing the trochlea in this manner, while also
considering the extent of lateral bony constraint, can help
one to understand and validate plans for tibial tubercle
transferring osteotomies. It provides a more digestible,
tangible depiction of the vector corrections necessary to
result in the optimal pathway for patellar tracking
problem, particularly when associated with a
J-sign, a laterally curved trochlea, a distal or
lateral articular lesion on the patella, ligamentous
laxity, or patella alta, moving the tibial tubercle
in addition to medial reconstruction is often
indicated. Trochleoplasty is uncommon and is
often reserved for unusual cases in which a
prominent proximal medial ridge or spur exists
or when a severely deformed trochlea requires
alteration to facilitate tracking. This is typically
less than 1% of all patella instability surgeries.
References
1. Insall JN, Aglietti P, Tria AJ, Jr. Patellar pain and
incongruence. II: clinical application. Clin Orthop
Relat Res. 1983;(176):225–32.
2. Hauser ED. Total tendon transplant for slipping
patella: a new operation for recurrent dislocation of
the patella. 1938. Clin Orthop Relat Res.
2006;452:7–16.
3. Southwick WO, Becker GE, Albright JA. Dovetail
patellar tendon transfer for recurrent dislocating
patella. Jama. 1968;204(8):665–9.
312
4. Trillat A, Dejour H, Couette A. Diagnosis and
treatment of recurrent dislocations of the patella.
Rev Chir Orthop Reparatrice Appar Mot.
1964;50:813–24.
5. DeCesare WF. Late results of Hauser procedure for
recurrent dislocation of the patella. Clin Orthop Relat
Res. 1979;140:137–44.
6. Fondren FB, Goldner JL, Bassett FH, 3rd. Recurrent
dislocation of the patella treated by the modified
Roux-Goldthwait procedure. A prospective study of
forty-seven knees. J Bone Joint Surg Am. 1985;67
(7):993–1005.
7. Zeichen J, Lobenhoffer P, Bosch U, Friedemann K,
Tscherne H. Interim results of surgical therapy of
patellar dislocation by Insall proximal reconstruction.
Unfallchirurg. 1998;101(6):446–53.
8. Brown DE, Alexander AH, Lichtman DM. The
Elmslie-Trillat procedure: evaluation in patellar dislocation and subluxation. Am J Sports Med. 1984;12
(2):104–9.
9. Hawkins RJ, Bell RH, Anisette G. Acute patellar
dislocations. The natural history. Am J Sports Med.
1986;14(2):117–20.
10. Rantanen J, Paananen M. Modified Hauser operation
for patellar instability. Immediate mobilization of 35
knees, a 5–8 year follow-up study. Acta Orthop
Scand. 1996;67(5):455–8.
11. Longo UG, Rizzello G, Ciuffreda M, Loppini M,
Baldari A, Maffulli N, et al. Elmslie-Trillat, Maquet,
Fulkerson, Roux Goldthwait, and other distal realignment procedures for the management of patellar
dislocation: systematic review and quantitative synthesis of the literature. Arthroscopy. 2016;32
(5):929–43.
12. Hampson WG, Hill P. Late results of transfer of the
tibial tubercle for recurrent dislocation of the patella.
J Bone Joint Surg Br. 1975;57(2):209–13.
13. Maquet P. A biomechanical treatment of femoropatellar arthrosis: advancement of the patellar tendon.
Rev Rhum Mal Osteoartic. 1963;30:779–83.
14. Maquet P. Advancement of the tibial tuberosity. Clin
Orthop Relat Res. 1976;115:225–30.
15. Schmid F. The Maquet procedure in the treatment of
patellofemoral osteoarthrosis. Long-term results. Clin
Orthop Relat Res. 1993;294:254–8.
16. Fulkerson JP. Anteromedialization of the tibial
tuberosity for patellofemoral malalignment. Clin
Orthop Relat Res. 1983;177:176–81.
17. Ficat P, Philippe J, Cuzacq JP, Cabrol S,
Belossi J. The syndrome of external hyperpressure
of the patella. A radioclinical entity. J Radiol Electrol
Med Nucl. 1972;53(12):845–9.
18. Sherman SL, Humpherys J, Farr J. Optimizing
patellofemoral cartilage restoration and instability
with tibial tubercle osteotomy. Arthroscopy. 2019;35
(8):2255–6.
19. Sherman SL, Erickson BJ, Cvetanovich GL,
Chalmers PN, Farr J 2nd, Bach BR Jr, et al. Tibial
tuberosity osteotomy: indications, techniques, and
outcomes. Am J Sports Med. 2014;42(8):2006–17.
C. A. Schneble et al.
20. Radin EL. The Maquet procedure–anterior displacement of the tibial tubercle. Indications, contraindications, and precautions. Clin Orthop Relat Res. 1986
(213):241–8.
21. Radin EL, Pan HQ. Long-term follow-up study on the
Maquet procedure with special reference to the causes
of failure. Clin Orthop Relat Res. 1993;290:253–8.
22. Chrisman OD, Snook GA, Wilson TC. A long-term
prospective study of the Hauser and RouxGoldthwait procedures for recurrent patellar dislocation. Clin Orthop Relat Res. 1979;144:27–30.
23. Cox JS. Evaluation of the Roux-Elmslie-Trillat
procedure for knee extensor realignment. Am J
Sports Med. 1982;10(5):303–10.
24. Fielding JW, Liebler WA, Wilson S, Puglisi A.
Tibial tubercle transfer: a long-range follow-up
study. Clin Orthop Relat Res. 1979;144:43–4.
25. Klinge SA, Fulkerson JP. Fifteen-year minimum
follow-up of anteromedial tibial tubercle transfer for
lateral and/or distal patellofemoral arthrosis. Arthroscopy. 2019;35(7):2146–51.
26. Pidoriano AJ, Weinstein RN, Buuck DA, Fulkerson JP. Correlation of patellar articular lesions with
results from anteromedial tibial tubercle transfer.
Am J Sports Med. 1997;25(4):533–7.
27. Buuck DA, Fulkerson JP. Anteromedialization of the
tibialtubercle: a 4- to 12-year follow-up. Operat Tech
Sports Med. 2000;8(2):131–7.
28. Farr J, Schepsis A, Cole B, Fulkerson J,
Lewis P. Anteromedialization: review and technique.
J Knee Surg. 2007;20(2):120–8.
29. Farr J. Autologous chondrocyte implantation
improves patellofemoral cartilage treatment outcomes. Clin Orthop Relat Res. 2007;463:187–94.
30. Post WR, Fulkerson JP. Distal realignment of the
patellofemoral joint. Indications, effects, results, and
recommendations. Orthop Clin North Am. 1992;23
(4):631–43.
31. Crebs DT, Anthony CA, McCunniff PT, Nieto MJ,
Beckert MW, Albright JP. Effectiveness of Fulkerson
osteotomy with femoral nerve stimulation for
patients with severe femoral trochlear dysplasia.
Iowa Orthop J. 2015;35:34–41.
32. Edwards A, Larson E, Albright J. Correlation of
radiographic patellofemoral indices with tibial tubercle transfer distance in Fulkerson osteotomy procedures. Iowa Orthop J. 2014;34:24–9.
33. Hadley CJ, Tucker BS, Lombardi NJ, Eck B,
Pepe MD, Frederick RW, et al. Combined MPFL
reconstruction and tibial tubercle osteotomy for
patellar instability: a retrospective review of 23
patients. J Orthop. 2021;28:49–52.
34. Su P, Liu X, Jian N, Li J, Fu W. Clinical outcomes
and predictive factors for failure with MPFL reconstruction combined with tibial tubercle osteotomy
and lateral retinacular release for recurrent patellar
instability. BMC Musculoskelet Disord. 2021;22
(1):632.
35. Allen MM, Krych AJ, Johnson NR, Mohan R,
Stuart MJ, Dahm DL. Combined tibial tubercle
Surgical Treatment of Recurrent Patellar Instability …
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
osteotomy and medial patellofemoral ligament reconstruction for recurrent lateral patellar instability in
patients with multiple anatomic risk factors. Arthroscopy. 2018;34(8):2420-6.e3.
Franciozi CE, Ambra LF, Albertoni LJB, Debieux P,
Granata GSM Jr, Kubota MS, et al. Anteromedial
tibial tubercle osteotomy improves results of medial
patellofemoral ligament reconstruction for recurrent
patellar instability in patients with tibial tuberositytrochlear groove distance of 17 to 20 mm. Arthroscopy. 2019;35(2):566–74.
Teitge RA. Patellofemoral syndrome a paradigm for
current surgical strategies. Orthop Clin North Am.
2008;39(3):287–311, v.
Ellera Gomes JL. Medial patellofemoral ligament
reconstruction for recurrent dislocation of the patella:
a preliminary report. Arthroscopy. 1992;8
(3):335–40.
Hautamaa PV, Fithian DC, Kaufman KR,
Daniel DM, Pohlmeyer AM. Medial soft tissue
restraints in lateral patellar instability and repair.
Clin Orthop Relat Res. 1998;349:174–82.
Arendt EA, Fithian DC, Cohen E. Current concepts
of lateral patella dislocation. Clin Sports Med.
2002;21(3):499–519.
Schöttle PB, Schmeling A, Rosenstiel N, Weiler A.
Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. Am J Sports Med. 2007;35(5):801–4.
Sanchis-Alfonso V, Ramirez-Fuentes C, MontesinosBerry E, Aparisi-Rodriguez F, Martí-Bonmatí L.
Does radiographic location ensure precise anatomic
location of the femoral fixation site in medial
patellofemoral ligament surgery? Knee Surg Sports
Traumatol Arthrosc. 2016;24(9):2838–44.
Sanchis-Alfonso V, Ramírez-Fuentes C, MontesinosBerry E, Elía I, Martí-Bonmatí L. Radiographic
location does not ensure a precise anatomic location
of the femoral fixation site in medial patellofemoral
ligament reconstruction. Orthop J Sports Med.
2017;5(11):2325967117739252.
Post WR, Fithian DC. Patellofemoral instability: a
consensus statement from the AOSSM/PFF patellofemoral instability workshop. Orthop J Sports Med.
2018;6(1):2325967117750352.
Chahla J, Smigielski R, LaPrade RF, Fulkerson JP. An
updated overview of the anatomy and function of the
proximal medial patellar restraints (Medial patellofemoral ligament and the medial quadriceps tendon
femoral ligament). Sports Med Arthrosc Rev.
2019;27(4):136–42.
Tanaka MJ, Chahla J, Farr J 2nd, LaPrade RF,
Arendt EA, Sanchis-Alfonso V, et al. Recognition of
evolving medial patellofemoral anatomy provides
insight for reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019;27(8):2537–50.
Mochizuki T, Nimura A, Tateishi T, Yamaguchi K,
Muneta T, Akita K. Anatomic study of the attachment of the medial patellofemoral ligament and its
characteristic relationships to the vastus intermedius.
313
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(2):305–10.
Baldwin JL. The anatomy of the medial patellofemoral ligament. Am J Sports Med. 2009;37
(12):2355–61.
Hinckel BB, Gobbi RG, Demange MK,
Pereira CAM, Pécora JR, Natalino RJM, et al.
Medial patellofemoral ligament, medial patellotibial
ligament, and medial patellomeniscal ligament:
anatomic, histologic, radiographic, and biomechanical study. Arthroscopy. 2017;33(10):1862–73.
Ge Y, Chen S, Kato T, Zdanowicz U, Smigielski R.
A polygon-shaped complex appearance of medial
patellofemoral ligament with dynamic functional
insertion based on an outside-in and inside-out
dissection technique. Knee Surg Sports Traumatol
Arthrosc. 2018;26(12):3754–61.
Tanaka MJ. The anatomy of the medial patellofemoral complex. Sports Med Arthrosc Rev. 2017;25
(2):e8-11.
Tanaka MJ, Voss A, Fulkerson JP. The anatomic
midpoint of the attachment of the medial patellofemoral complex. J Bone Joint Surg Am. 2016;98
(14):1199–205.
Espregueira-Mendes J, Andrade R, Bastos R,
Joseph S, Fulkerson JP, Silva LD. Combined soft
tissue reconstruction of the medial patellofemoral
ligament and medial quadriceps tendon-femoral
ligament. Arthrosc Tech. 2019;8(5):e481-8.
Spang R, Egan J, Hanna P, Lechtig A, Haber D,
DeAngelis JP, et al. Comparison of patellofemoral
kinematics and stability after medial patellofemoral
ligament and medial quadriceps tendon-femoral
ligament reconstruction. Am J Sports Med. 2020;48
(9):2252–9.
Joseph SM, Fulkerson JP. Medial quadriceps tendon
femoral ligament reconstruction technique and surgical anatomy. Arthrosc Tech. 2019;8(1):e57-64.
Fulkerson JP, Edgar C. Medial quadriceps tendonfemoral ligament: surgical anatomy and reconstruction technique to prevent patella instability. Arthrosc
Tech. 2013;2(2):e125-8.
Hinckel BB, Gobbi RG, Kaleka CC, Camanho GL,
Arendt EA. Medial patellotibial ligament and medial
patellomeniscal ligament: anatomy, imaging, biomechanics, and clinical review. Knee Surg Sports
Traumatol Arthrosc. 2018;26(3):685–96.
Liu JN, Brady JM, Kalbian IL, Strickland SM,
Ryan CB, Nguyen JT, et al. Clinical outcomes after
isolated medial patellofemoral ligament reconstruction for patellar instability among patients with
trochlear dysplasia. Am J Sports Med. 2018;46
(4):883–9.
Albee FH. The bone graft wedge in the treatment of
habitual dislocation of the patella. Med Record.
1915;88:257–9.
Masse Y. Trochleoplasty. Restoration of the intercondylar groove in subluxations and dislocations of
the patella. Rev Chir Orthop Reparatrice Appar Mot.
1978;64(1):3–17.
314
61. Dejour H, Walch G, Neyret P, Adeleine P. Dysplasia
of the femoral trochlea. Rev Chir Orthop Reparatrice
Appar Mot. 1990;76(1):45–54.
62. Dejour D, Saggin P. The sulcus deepening
trochleoplasty-the Lyon’s procedure. Int Orthop.
2010;34(2):311–6.
63. von Knoch F, Böhm T, Bürgi ML, von Knoch M,
Bereiter H. Trochleaplasty for recurrent patellar
dislocation in association with trochlear dysplasia.
A 4- to 14-year follow-up study. J Bone Joint Surg
Br. 2006;88(10):1331–5.
64. Rush J, Diduch D. When is trochleoplasty a rational
addition? Sports Med Arthrosc Rev. 2019;27
(4):161–8.
65. Bereiter H, Gautier E. Die Trochleaplastik als
chirurgische Therapie der rezidivierenden Patellaluxation bei Trochleadysplasie des Femurs. Arthroskopie. 1994;7:281–6.
66. Carstensen SE, Feeley SM, Burrus MT, Deasey M,
Rush J, Diduch DR. Sulcus deepening trochleoplasty
and medial patellofemoral ligament reconstruction
for patellofemoral instability: a 2-year study.
Arthrosc J Arthrosc Relat Surg. 2020;36(8):2237–45.
67. Zaffagnini S, Previtali D, Tamborini S, Pagliazzi G,
Filardo G, Candrian C. Recurrent patellar dislocations: trochleoplasty improves the results of medial
patellofemoral ligament surgery only in severe
trochlear dysplasia. Knee Surg Sports Traumatol
Arthrosc. 2019;27(11):3599–613.
68. Dejour DH, Deroche É. Trochleoplasty: indications
in patellar dislocation with high-grade dysplasia.
Surgical technique. Orthop Traumatol Surg Res.
2021:103160.
69. Fucentese SF, Zingg PO, Schmitt J, Pfirrmann CWA,
Meyer DC, Koch PP. Classification of trochlear
dysplasia as predictor of clinical outcome after
trochleoplasty. Knee Surg Sports Traumatol
Arthrosc. 2011;19(10):1655–61.
C. A. Schneble et al.
70. Longo UG, Vincenzo C, Mannering N, Ciuffreda M,
Salvatore G, Berton A, et al. Trochleoplasty techniques provide good clinical results in patients with
trochlear dysplasia. Knee Surg Sports Traumatol
Arthrosc. 2018;26(9):2640–58.
71. Thaunat M, Bessiere C, Pujol N, Boisrenoult P,
Beaufils P. Recession wedge trochleoplasty as an
additional procedure in the surgical treatment of
patellar instability with major trochlear dysplasia:
Early results. Orthop Traumatol Surg Res. 2011;97
(8):833–45.
72. Rouanet T, Gougeon F, Fayard JM, Rémy F,
Migaud H, Pasquier G. Sulcus deepening trochleoplasty for patellofemoral instability: A series of 34
cases after 15 years postoperative follow-up. Orthop
Traumatol Surg Res. 2015;101(4):443–7.
73. Hiemstra LA, Peterson D, Youssef M, Soliman J,
Banfield L, Ayeni OR. Trochleoplasty provides good
clinical outcomes and an acceptable complication
profile in both short and long-term follow-up. Knee
Surg Sports Traumatol Arthrosc. 2019;27
(9):2967–83.
74. Simmons E Jr, Cameron JC. Patella alta and recurrent
dislocation of the patella. Clin Orthop Relat Res.
1992;274:265–9.
75. Palmer SH, Servant CT, Maguire J, Machan S,
Parish EN, Cross MJ. Surgical reconstruction of
severe patellofemoral maltracking. Clin Orthop Relat
Res. 2004;419:144–8.
76. Johnson AA, Wolfe EL, Mintz DN, Demehri S,
Shubin Stein BE, Cosgarea AJ. Complications after
tibial tuberosity osteotomy: association with screw
size and concomitant distalization. Orthop J Sports
Med. 2018;6(10):2325967118803614.
77. Sanchis-Alfonso V, Merchant AC. Iatrogenic medial
patellar instability: an avoidable injury. Arthroscopy.
2015;31(8):1628–32.
Chondral and Osteochondral Lesions
in the Patellofemoral Joint
Kevin Credille, Dhanur Damodar,
Zachary Wang, Andrew Gudeman,
and Adam Yanke
1
Introduction to Focal Cartilage
Defects
Focal cartilage defects may be associated with
impaired quality of life in a similar manner to
osteoarthritis. Patients can present with limited
activity due to severe pain, recurrent effusions,
dysfunction, and the eventual progression of
joint degeneration [1, 2]. This is clinically
important as between 30,000 and 100,000 procedures are performed each year in the United
States to help treat and alleviate symptoms secondary to cartilage lesions in the knee [2].
Symptomatic lesions can present acutely as a
result of trauma after anterior cruciate ligament
(ACL) tears or patellar dislocations or chronically from repetitive patellofemoral stress often
with a component of genetic predisposition. On
the other hand, asymptomatic lesions can also
occur and may be found incidentally at the time
of MRI or arthroscopy and are NOT an indication for surgical intervention [3]. Regardless of
the etiology, these defects may progress in light
K. Credille D. Damodar Z. Wang A. Yanke (&)
Midwest Orthopedics at Rush University Medical
Center, Chicago, IL, USA
e-mail: adam.yanke@rushortho.com
A. Gudeman
Indiana University School of Medicine, Indianapolis,
IN, USA
of the known poor regenerative properties of
hyaline articular cartilage. In a subset of patients
these focal lesions may eventually progress to
osteoarthritis [4].
2
Modified Outerbridge
Classification / International
Cartilage Repair Society (ICRS)
Classification
The two major cartilage lesion categorizations
are the Modified Outerbridge Classification and
the International Cartilage Repair Society (ICRS)
Classification. The Outerbridge Classification
was developed in 1961 and is based on inspection of the cartilage surface through arthroscopy
and also through an open approach. Grade 0 is
normal cartilage, grade 1 is cartilage softening,
grade 2 are partial thickness fissures less than
1.5 cm, grade 3 are fissures greater than 1.5 cm
with a full thickness fissure, and grade 4 is
complete cartilage loss with exposed subchondral
bone. The Modified Outerbridge Classification
separated the dimensions from Grades 2 and 3.
That is, the grades are as before except Grade 2 is
now for lesions less than 50% in depth and Grade
3 lesion are from 50% to full thickness with the
dimensions of the lesion reported independently.
The ICRS Classification is also based on visual
inspection of the cartilage surface. Grade 0 is
normal cartilage, grade 1 lesions have softening,
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_22
315
316
K. Credille et al.
blistering, and/or fissures, grade 2 lesions are
fissures <50% of cartilage depth, grade 3 lesions
are >50% cartilage depth, and grade 4 lesions are
full-thickness lesions with exposure and
involvement of the subchondral bone.
3
General Isolated Cartilage Lesion
Evaluation
At the time of presentation, patients do not report
a chondral lesion. Rather, patients complain of
pain and, at times, associated swelling, diminished motion, stiffness, and mechanical symptoms such as catching or locking [3]. Of note,
knee effusions persisting after an aggravating
event are one of the most important clinical
indicators suggestive of an underlying cartilage
injury. This type of effusion progresses slowly as
opposed to acute effusions seen with cruciate
ligament injuries or patellar dislocations. These
slow, latent effusions are reflective of the insidious nature of chondral lesions. When a chondral
defect of the knee is suspected, patients are
questioned and examined for malalignment, knee
instability, patellar instability, and other
pathologies [3]. In patients with acute pain from a
cartilage lesion, radiographs do not show
pathology other than an effusion or loose body
[5]. However, standard weight bearing knee
radiographic views (AP and PA flexed) as well as
standing long leg limb alignment films are
required to rule out coronal plane malalignment
as malignment in any plane may contribute to a
failed cartilage restoration procedure [6]. MRI is
also ordered to evaluate the location, size, and
depth of cartilage defects and any concomitant
ligamentous or meniscal pathology. Once a
chondral lesion is identified as the root cause of a
patient’s symptoms, non-operative treatment
consisting
of
rest,
non-steroidal
antiinflammatory drugs (NSAIDs), steroid and hyaluronic acid injections, and physical therapy
needs to be trialed for six weeks to six months
before considering surgical options [3]. For
lesions that fail conservative management,
arthroscopic evaluation can be considered.
Importantly, higher failure rates of cartilage
restoration procedures occur when coexisting
pathologies go unaddressed [6]. Therefore, ligament reconstruction, meniscal repair, or meniscal
allograft transplant should precede or be addressed concomitantly with any cartilage defect repair
procedures to minimize the excessive stress in the
patellofemoral joint PFJ and increase the chances
of a successful cartilage treatment [5]. Select
patients may also need treatment concomitantly
with a distal femoral osteotomy, proximal tibial
osteotomy, or tibial tubercle osteotomy.
4
Evaluation of the Patient
with Patellofemoral Specific
Lesions
Patellofemoral patients typically present with
anterior knee pain with activities such as walking, stairs, squatting, jumping, or running as
these increase contact pressures in the knee
during flexion due to mechanical loading. While
posterior knee pain can also be present, this is
often secondary to an effusion and most patients
will still localize their pain just deep to their
patella. A subset will have patellar or trochlear
chondral lesions. Locking and catching symptoms can also occur but are associated with
chondral flaps. Clinicians should pay particular
attention to acute and/or chronic nature of the
patient’s patellofemoral instability and whether
they are experiencing apprehension, subluxation,
or full dislocations. It is important to uncover
whether the patient’s pain is transient and occurs
secondary to an acute subluxation or dislocation
event or if it is a result of a persistent chondral
defect stemming from chronic instability or
malalignment [3].
At the time of physical and radiographic
examination of patellofemoral lesions, focus
should be paid to lower extremity alignment, the
patient’s gait, and the patient’s Q angle. The Q
angle is increased by a lateralized tibial tubercle,
and valgus alignment and may appear decreased
by chronic subluxation of the patella until it is
reduced into the central trochlear groove. That is,
the most accurate Q angle measurement needs to
be made while the patella is in the trochlear
Chondral and Osteochondral Lesions in the Patellofemoral Joint
groove and a Merchant extended goniometer
extends to the ASIS. The knee should also be
evaluated for effusion, patellar displacement in
quadrants, patellar tracking during flexion and
extension and evaluation for a J sign. Concomitant ligamentous injury should also be ruled out
[3]. One should also perform the patellar grind
exam by applying direct compression to the
patella with translation. This may signify an
underlying chondral lesion or stress overload. To
best interpret the results of this test, it should also
be performed on the contralateral knee [7]. If
history and physical examination suggest the
possibility of a patellofemoral cartilage defect,
Merchant and lateral knee views will aid in the
diagnose patella alta or patella baja via the
Caton-Deschamps index [8], patellar tilt and
subluxation, and bony contour indicative of trochlear dysplasia [9, 10].
MRI is essential to evaluate chondral and/or
osteochondral lesions of the PFJ and other factors such as trochlear dysplasia [3]. While MRI is
a helpful tool in the evaluation of chondral
lesions, it may underestimate true lesion size by
up to 60% and does not provide lesion structural
or edge stability data like diagnostic arthroscopy
[11]. However, it is important for identifying
meniscal pathology, ligamentous injuries, subchondral bone edema, and patellar height and
tibial tubercle to trochlear groove (TT-TG) distance which can be associated with developing
cartilage defects [12]. One should also consider a
CT arthrogram as an adjunct for patients with
poorly visualized chondral lesions on MRI and
significant patellar maltracking to help assess
tibial version, plan osteotomies, and further
evaluate bony anatomy (in cases with suspected
axial malalignment, MRI or CT hip/knee/ankle
assessment is indicated) [13].
If major anatomic factors placing the patient
at increased risk for patellar dislocation or excess
patellofemoral stresses are identified, the patient
may end up needing concomitant procedures
including, but not limited to a tibial tubercle
osteotomy (TTO), medial patellofemoral ligament reconstruction, and lateral retinacular
lengthening. These procedures serve to correct
317
pathologic anatomy that may have contributed
the initial cartilage lesion and to decrease the
contact stresses through mechanical offloading.
An anteromedialization (AMZ) TTO is an
example of a procedure that reduces the lateral
force vector by moving the tubercle medially and
reducing patella contact pressures by moving the
patella tendon attachment anteriorly [5].
5
General Indications for Cartilage
Restoration Procedures
In general, surgical treatment of full thickness
cartilage lesions is reserved for persistently
symptomatic patients who have failed conservative treatment or those with cartilage flaps and
unstable osteochondral fragments. Full thickness
lesions can be treated with a variety of surgical
options including chondroplasty/debridement,
open reduction and internal fixation (ORIF) of
osteochondral fragments, microfracture, osteochondral autograft transfer (OAT), osteochondral
allograft transplantation (OCA), and various cellbased techniques such as autologous chondrocyte
implantation (ACI), matrix induced autologous
chondrocyte implantation (MACI), and particulated juvenile allograft cartilage (PJAC) [3, 5].
For smaller lesions less than 2 cm2, debridement/
chondroplasty, microfracture, and OAT are the
preferred treatment choices. OCA is preferable
for larger lesions >2–4 cm2. Cell-based therapies
like MACI and PJAC are also excellent for larger
lesions, but are limited to lesions with minimal
subchondral bone loss [14]. Deeper subchondral
bone loss is better treated with OATs and OCAs,
although bone grafting can be used with cellbased therapies in the setting of defects 8 mm
at the time of cartilage restoration [15]. Patients
younger than <55 generally qualify for cartilage
restoration procedures versus total knee arthroplasty, but the primary criteria for this may
depend upon how much healthy cartilage
remains [16]. A person with several large lesions
throughout the knee is more consistent with
osteoarthritis and may fare better with a total
knee or patellofemoral arthroplasty [5].
318
6
K. Credille et al.
Debridement/Chondroplasty
Chondroplasty is by definition a cartilage
debridement and is one of the most commonly
performed cartilage procedures [17]. In this
procedure, a loose cartilage flap is debrided to a
stable edge to reduce mechanical symptoms and
prevent further propagation of the lesion from
mechanical stress, as seen in Fig. 1. While this
procedure is best suited for lesions smaller than 2
cm2, it can also be the first stage of cell-based
cartilage procedures such as ACI, MACI, and
PJAC [18]. While it is important to for debridement to create stable vertical walls, the negative
effects of aggressively debriding tissue beyond
areas of cartilage instability remains controversial [19], and it is crucial to avoid creating an
uncontained lesions or exposing subchondral
bone [20].
Clinical outcomes and proper characterization
of cartilage debridement in the PFJ remain limited in the orthopedic literature. A case series
performed by Anderson et al. in 2017 retrospectively identified 86 patients undergoing isolated cartilage debridement in the knee, with
58.5% of patients having lesions in the PFJ with
Fig. 1 Arthroscopic image
of a cartilage flap
ICRS grades of 2–4 and mean size of 3.3 cm2.
The authors found chondroplasty success was
correlated with baseline presurgical PRO scores,
male sex, and ICRS grade. On the other hand,
lesion size, patient age, and obesity had no effect
on surgical outcome [21]. In another retrospective case series performed by Federico and
Ryder, 36 patients with patellar chondromalacia
without a history of instability or malalignment
who underwent patellar chondroplasty were
examined and followed for an average of
59 months. Thirty-two (89%) of the patients
reported the surgery had a beneficial effect and
there was only a slight deterioration of results
found at final follow up. Further, of the 29
patients playing sports preoperatively, 27 (93%)
were able to return to play [22]. This indicates
that chondroplasty has the potential to provide
durable long term outcomes in the PFJ.
7
Bone Marrow Stimulation
Bone marrow stimulation is achieved through a
variety of techniques such as drilling, using K
wires, and the microfracture technique which
Chondral and Osteochondral Lesions in the Patellofemoral Joint
uses angulated awls. The goal of marrow stimulation is to promote fibrocartilage formation via
migration of mesenchymal stem cells to the
cartilage defect from subchondral bone [23, 24].
The threshold for performing bone marrow
stimulation is restricted in the PFJ and should be
2 cm2 or less, due to the higher sheer stresses
experienced in this joint compartment. It should
be avoided in uncontained lesions altogether
[25]. The authors advocate that bone marrow
stimulation plays little to no role in the PFJ regardless of lesion size.
Regardless of the marrow stimulation technique used, it is essential to perform a chondroplasty through the calcified cartilage to
subchondral bone while creating stable vertical
walls [19]. The bony perforations made with this
technique must be perpendicular to the bone
surface, which can be difficult to achieve for the
patella via arthroscopy of the PFJ [3]. Sometimes
a small arthrotomy is necessary for proper visualization, instrument angulation, and counter
pressure that is necessary for lesions on the
patella. For classic “micro fracture” each perforation must be at least 3 mm deep and spaced
3–4 mm apart from the others as seen in Fig. 2.
Newer marrow stimulation techniques attempt as
little bony injury as possible with very small
(e.g., 1 mm) drill bits and drill to a depth of
6–10 mm to access more marrow derived cells.
The injury to the bone surface will promote
Fig. 2 Shows bony
perforations spaced
appropriately at
approximately 3–4 mm apart
from each other at the bed of a
cartilage lesion
319
inflammation, bleeding, clot formation, and
mesenchymal stem cell migration to the site of
injury. It should be noted that while these cells
will produce collagen and cartilage to repair the
cartilage defect, it is fibrocartilage, which
biomechanically inferior to the native hyaline
cartilage typically found at the bone surfaces of
joints [19].
Most of the outcome studies related to bone
marrow stimulation combine data from both the
tibiofemoral joint (femoral condyles) and PFJ, as
there is limited data available on isolated patellar
microfracture. The majority of these studies
demonstrate low failures rates in the short-term at
2 years follow up in lower demand patients with
smaller defects, with increases in long-term
failure rates after 2–5 years of follow up
[25–27]. Kreuz et al. evaluated full thickness
cartilage lesions in 85 patients in different anatomic locations in the knee including the femoral
condyle, tibia, trochlea, and patella. Patient
reported outcomes were strong at 6-months and
18-months but started to deteriorate at the 2-year
mark and MRI measured defect filling deteriorating at 36-months, with the trochlear and
patellar patients declining more rapidly than the
other groups [28]. Additionally, it has been
shown that microfracture can negatively impact
the success rates of subsequent cartilage
restoration procedures. Minas et al. demonstrated
an ACI failure rate of 26% after a prior marrow
320
K. Credille et al.
stimulation procedure compared to a primary
ACI failure rate of only 8%. The authors concluded that limiting bone marrow procedures in
the PFJ to chondral lesions smaller than 2 cm2
and limiting it to the trochlea would maximize
the chance of achieving a successful outcome if
subsequent procedures were needed [29].
8
Osteochondral Autograft
Transplant (OAT)/Mosiacplasty
Osteochondral autograft transplant is a cartilage
restoration technique reserved for smaller osteochondral lesions <2–3 cm2 that involves harvesting 6–15 mm cylindrical cartilage plugs from
non-weight-bearing portions of the ipsilateral
knee such as the peripheral margins of the
Fig. 3 Shows an OAT plug
after harvest in the top part of
the image and a smooth
articular surface after plug
implantation
trochlea, posterior condyles, or intercondylar
notch, and re-implanting them in the weight
bearing chondral defect. For larger defects,
numerous plugs are used in a mosaic pattern to
provide lesion coverage [5, 19]. A harvested
OAT plug is shown in Fig. 3. The plugs offer the
advantage of transferring a native hyaline cartilage surface attached to underlying subchondral
bone in a single-stage procedure, which facilitates healing. If any cartilage gaps are still present after autograft plug transfer, fibrocartilage
will end up filling in the periphery of the autografts and augment the transferred native cartilage. The procedure is typically performed
through an open arthrotomy, however newer
techniques have evolved to allow this procedure
to be performed arthroscopically [5]. Stable fixation is typically achieved without hardware as
Chondral and Osteochondral Lesions in the Patellofemoral Joint
the autografts are often press fit after preparation
of the cartilage defect [30]. While OAT is an
autograft and avoids immunologic complication
risks, there are still concerns for donor site
morbidity, which limits the use of OAT in larger
lesions >2–3 cm2 that may require mosaicplasty
[31]. Additionally, creating a surface that matches the native cartilage contour is essential for
achieving successful outcomes and is especially
difficult with larger lesions [5]. It has been shown
that autograft prominence as little as 1 mm can
lead to catching and locking symptoms months
after the procedure. For the PFJ, interface mismatch is more common and complicated by the
unique anatomy of the trochlea and patella coupled with the patella having the thickest cartilage
of any recipient site in the knee [19].
Outcomes studies for OAT in the PFJ report
inconsistent success rates. Hongody et al. reported a 79% rate of good to excellent outcomes
after mosaicplasty in the PFJ at long term 10-year
follow up [32]. However, another prospective
study by Baltzer et al. of 112 patients with
chronic chondral lesions of the knee demonstrated retropatellar defect location (n = 25) as
the strongest predictor of poor outcomes. However, this study failed to take into account the
effects of PFJ malalignment [33]. Many authors
believe that malalignment of the PFJ impacts the
outcome in OAT. As an example, a study by
Astur et al. found significantly improved clinical
outcomes at 1 and 2-years follow up of <2.5 cm2
full-thickness cartilage lesions when PFJ
malalignment patients were excluded [34]. This
is further supported by recent research. For
example, Emre et al. recently performed a study
of isolated OAT in the PFJ with all 33 patients
reporting improved outcomes at a mean followup of 19.3 month [35]. In another recent study,
Yabumoto et al. examined isolated OAT in the
PFJ with all patient reported outcomes showing
improvement at a mean follow up of
46.9 months [36]. Both Emre et al. and Yabumoto et al. concluded that OAT is particularly
effective even in the long-term when meticulous
attention is paid to achieving a high surface
congruity.
9
321
Osteochondral Allograft
Transplantation (OCA)
Osteochondral allograft transplantation (OCA) is
indicated for large cartilage defects >2–4 cm2
with or without damage to underlying subchondral bone, as its use in pure chondral lesions is
increasing [37]. It is arguably the most complex
cartilage procedure of the PFJ. Indications
include treatment of contained or uncontained
cartilage lesions, meaning it can be used whether
the lesion has surrounding articular cartilage or
not [5]. Additionally, OCA can serve to treat
bipolar lesions and as a salvage procedure after
other cartilage restoration techniques have failed
to provide pain relief and delay arthroplasty in
younger patient populations [38, 39]. Relative
contraindications include smoking, steroid use,
and obesity as high failure rates have been
demonstrated in these patients [5]. The surgical
technique shares a lot of similar principles to
OAT, being that it requires press fitting of a
harvested implant and that surface topography
matching is integral to procedure success. It is
also a single-stage procedure but unlike OAT it
does not carry any donor site morbidity as it is an
allograft donor. However, a downside to OCA is
the logistical constraints to matching a donor to
the patient and scheduling surgery accordingly.
Newer technologies such as cryopreserved OCAs
have been invented to circumvent these constraints [40]. OCA requires an arthrotomy to
place a size and topography matched donor
allograft that press fits into a well-prepared defect
that has been debrided down to a health stable
rim as seen in Fig. 4. Its use in the PFJ is likewise complicated by the complex anatomy of the
patella and trochlea and patellar cartilage thickness. Since this technique uses an allograft, fresh
OCAs are harvested within 24 hours of a donor’s
death and preserved for up to 28 days at 39°
Fahrenheit [19].
Overall, the OCA failure rates have been
demonstrated to be higher in the PFJ than the
tibiofemoral joint space. A systematic review
performed in 2016 by Assenmacher et al. showed
success rates of 76% in the tibiofemoral joint
322
K. Credille et al.
Fig. 4 Shows an OCA press
fitted into a previously well
prepared and debrided lesion
with topography matching.
space versus 50% in the PFJ at a mean follow-up
of 12.3 years. In this study, the PFJ group had a
reoperation rate of 83% compared to 34% for
defects involving the tibial plateau or femoral
condyles [41]. Unfortunately, there is a paucity
of randomized control trials examining patellofemoral OCA. There are, however, several cohort
studies reporting on patellofemoral outcomes for
trochlear and patella OCA. A retrospective case
series performed by Gracitelli et al. studied 28
knees with patellar lesions that underwent OCA
with a mean follow up of 9.7 years and found
78.1% graft survivorship at 5 and 10 year follow
up and 55.8% graft survivor ship at 15 years
follow up. In another retrospective case series by
Cameron et al. evaluating trochlear OCA on 29
knees with a mean follow up of 7 years, the
authors found 100% graft survivor ship at
5 years and 91.7% graft survivorship at 10 years
with improvement of all patient reported outcomes [42]. In addition, both studies showed an
overall patient satisfaction rate of 89%. Thus,
both studies demonstrate good 10-year outcomes
for OCA in the PFJ and highlight its potential use
as a salvage procedure prior to arthroplasty for
large, isolated chondral defects.
10
Matrix Induced Autologous
Chondrocyte Implantation
(MACI) / Autologous
Chondrocyte Implantation (ACI)
Matrix induced autologous chondrocyte implantation (MACI) is a two-stage procedure that
treats full thickness cartilage defects that are
typically >2 cm2 without bony involvement. This
procedure and its predecessor ACI allow for
much easier topography matching in the PFJ than
OAT or OCA [3]. Initially, healthy chondrocytes
are typically harvested arthroscopically at the
time of an initial staging and debridement procedure. The chondrocytes are then colony
expanded in culture, and subsequently attached
to a collagen membrane. Then, in a second procedure, the defect is debrided down to the calcified cartilage level and stable vertical walls are
created typically and a mini parapatellar arthrotomy is used to enhance visualization. Then the
membrane custom trim fitted into the debrided
cartilage defect. This can be achieved by using a
free hand technique by using pre-shaped cutting
tools [43]. The implant is secured in the defect
Chondral and Osteochondral Lesions in the Patellofemoral Joint
Fig. 5 Demonstrates a successful implant of the MACI
membrane after fibrin glue has been applied and cured
using a layer of fibrin glue in the defect bed and
then another thin layer also placed above the
membrane and given time to cure as seen in
Fig. 5. One can also use sutures or suture anchors
if needed for membrane fixation. Eventually, the
goal is for the healthy autologous implanted
chondrocytes to incorporate into the exposed
bone and migrate/expand to fill the defect evenly.
Due to the nature of this surgical technique, it has
the advantage of fitting into lesions of a variety of
different shapes and sizes, which is particularly
useful in the PFJ [5].
The first-generation autologous chondrocyte
implantation (ACI) was born out of the 1990s in
the effort to supplant and improve upon the outcomes being achieved with microfracture and
other cartilage restoration techniques. It grew in
popularity due in large part to its ability to
regenerate native hyaline cartilage and repair full
thickness cartilage defects. Eventually, ACI was
found to produce what researchers and clinicians
alike desired: better long-term clinical outcomes
with a more cost-effective technology than
microfracture [44]. Since the inception of ACI, a
second-generation technology has been developed using bi-layer collagen membranes and
323
MACI, the third-generation technology, was created by seeding chondrocytes onto matrices of
collagen [45]. It should be noted that a common
complication of MACI/ACI is graft hypertrophy
given the cell-based nature of the technology [46].
As for MACI outcomes, Brittberg et al. performed a large scale prospective, multicenter,
randomized trial comparing MACI and
microfracture in lesions >3 cm2. The authors
found improvements in patient reported outcomes at 2 and 5 years of follow up of MACI as
compared to microfracture [47]. MACI/ACI has
been well studied in the PFJ in contrast to many
other cartilage restoration techniques and initially
reports of ACI in this region were disappointing.
However, with the emergence of better understanding of PFJ biomechanics and concomitant
treatment of malalignment, ACI outcomes
improved even in the mid to long term [48, 49].
A prospective cohort study by Keudell et al.
examined patients with isolated patellar chondral
lesions treated by ACI and found a 90% success
rate at 15 years with 83% of patients reporting
good to excellent outcomes at that time point
[50]. A recent systematic review of 58 studies by
Andriolo et al. found an overall failure rate of
14.9% for ACI/MACI mostly occurring within
the first 5 years of follow up with no differences
found between ACI and MACI [51]. In another
systematic review by Schuette et al. of patients
undergoing MACI of the knee joint, the authors
found a 12.4% failure rate in the tibiofemoral
joint versus 4.7% in the PFJ [52]. These results
suggest that MACI/ACI are potentially better
longer term treatments for chondral lesions in the
PFJ, especially when PFJ malalignment is concomitantly treated. This is further supported by a
recent meta-analysis by Hinckell et al. showing a
success rate of 96.1% for 1274 cell-based cartilage restoration procedures, 1229 of which were
MACI/ACI. Lastly, while MACI/ACI are both
expensive, they may end up being similarly costeffective to other cartilage procedures given that
they delay other costly procedures such as
arthroplasty [19].
324
11
K. Credille et al.
Particulated Juvenile Allograft
Cartilage
Particulated juvenile allograft cartilage (PJAC) is
another cell-based cartilage restoration technique
used for full-thickness chondral lesions 1–6 cm2
and ICRS grade 3 or higher without bony
involvement [19]. PJAC is used preferentially in
the PFJ but can still be utilized in the TFJ. Akin
to MACI/ACI, this technique evolved from
research efforts to expand the chondral lesion
treatment arsenal for orthopedic surgeons and
offers the same ease of surface contour matching.
An additional benefit of PJAC compared to
MACI/ACI is that it is a one-stage procedure.
PJAC shares graft hypertrophy as a common
complication with MACI/ACI as they are both
cell-based techniques [46]. PJAC is initially
harvested from the femoral condyles of pediatric
donors, with a viable shelf life of 45 days.
Each PJAC package contains 30–200 cubes of
minced graft tissue and one package is capable of
treating a full-thickness cartilage lesion up to 2.5
cm2, with larger lesions treated with multiple
PJAC packages [2]. Mincing the graft allows
chondrocytes to migrate from extracellular
matrix and form native hyaline cartilage [53].
Furthermore, the advantage of using pediatric
cartilage rather than adult tissue is that juvenile
chondrocytes are capable of producing more
extracellular matrix and proteoglycan content
and thus have a more favorable cartilage gene
expression profile [54, 55].
For implanting the graft, a similar defect
preparation is used to that of MACI/ACI. The
defect is debrided down to the calcified cartilage
level and stable vertical walls are created typically via a mini arthrotomy similar to
MACI/ACI. Once the defect is prepared, the
minced PJAC cubes can be placed directly into
the defect or prepared extra-articularly. Regardless of the method used, cubes should be spaced
1–2 mm apart in one layer and the top layer
needs to be 1 mm below the periphery of the
cartilage defect [2]. This ensures minimization of
the shear stress and compressive biomechanical
loading on the graft that might occur if the
implant sits proud to the defect perimeter [56]. If
the lesion is uncontained and there are concerns
for excessive biomechanical sheer and compressive stresses, commercial collagen can be sutured
or anchored to the cartilage wall defect extensions. This technique for treating uncontained
lesions can also be applied to other cell-based
techniques like MACI/ACI [57] (see Fig. 6).
However, outcomes studies for PJAC remain
sparse, are limited to case series or case reports
and most of the PJAC research has been focused
on lesions in the talus. Regardless, there is still
some existing data. Recently, there was a
prospective case series performed by Wang et al.
of 27 patients treated for patellofemoral cartilage
defects with an average of 3.84 years of followup. Patients in this study experienced statistically
significant improvements in patient reported
outcomes. Additionally, at the 2-year follow up
MRI, nearly 70% of patients had more than twothirds of their defect filled [46]. Several other
single arm studies have shown similarly favorable results for patients with patellar and trochlear cartilage lesions in the short-term and
medium-term follow up [58–61]. Future studies
will need to focus on long-term outcomes and
head-to-head comparisons with other cartilage
restoration techniques.
12
Post-operative Rehabilitation
Cartilage restoration procedures have a variety of
protocols aimed at protecting their repair. Range
of motion exercises are usually started within the
first week post-operatively to encourage cartilage
healing and prevent stiffness. Weight bearing
varies based on the procedure type and surgeon
preference. Chondroplasty, for example, will be
weight bearing as tolerated immediately while
full weight bearing in extension is often the case
for one or two weeks after patellofemoral cartilage procedures with the exception of marrow
stimulation, MACI, and PJAC. The latter three
procedures require six weeks of protected weight
bearing before progression to full weight bearing
to give time for a mature cartilage surface to
Chondral and Osteochondral Lesions in the Patellofemoral Joint
325
Fig. 6 Shows properly
spaced minced PJAC cubes
1–2 mm apart sitting more
than 1 mm below the
periphery of the cartilage
lesion
form. For OCA, there is generally a slightly
faster return to weight bearing before six weeks
depending on physician preference [62].
13
Conclusion
As a patient is evaluated for a chondral defect in the
PFJ, surgeons should comprehensively assess all
factors that impact the etiology of a presenting
lesion. Anatomic factors including PFJ alignment,
concomitant meniscal or ligamentous injury, lesion
size and depth, involvement of subchondral bone,
and the amount of remaining cartilage in the
PFJ overall should be evaluated. With the appropriate indications, good to excellent outcomes can
be achieved. Chondroplasty and OAT can help
treat patients with small lesions <2 cm2. Larger
lesions will require OCA, MACI, or PJAC. Further
head-to-head comparisons of these restoration
procedures will be needed to fully determine the
most cost-effective and efficacious procedures
available for patients.
14
Key Message
Treatment of chondral lesions in the PFJ requires
a multifaceted approach as it involves management of the higher biomechanical stress of the
PFJ, addressing malalignment issues concomitantly, anatomical differences such as thicker
cartilage of the patella and complex anatomy of
the patella and trochlea. Treatment choice
requires careful consideration as differing outcomes studies exist between the PFJ compared to
the tibiofemoral joint (TFJ).
15
Seven Take Home Messages
1. It is important to not immediately focus on
the chondral lesion. The key to successful
management is to first identify all the potential pain generators. As cartilage is aneural,
“assigning the pain” to the cartilage lesion is a
diagnosis by exclusion.
326
2. As a patient is evaluated for a chondral defect
in the PFJ, surgeons should comprehensively
assess all factors that impact the etiology of a
presenting lesion: PFJ alignment, meniscal
and ligamentous status, lesion size, depth, and
location, involvement of subchondral bone,
and amount of remaining cartilage in the PFJ.
3. Associated patellofemoral malalignment and
instability can be addressed with concomitant
mechanical procedures such as tibial tubercle
osteotomy, medial patellofemoral ligament
reconstruction, and lateral retinacular
lengthening.
4. Small chondral lesions <2 cm2 that have
failed nonsurgical management should be
considered for chondroplasty, osteochondral
autograft transplant (OAT), or particulated
juvenile allograft cartilage (PJAC)
5. Larger chondral lesions >2–4 cm2 require
osteochondral allografts (OCA), matrix
induced autologous chondrocyte implantation
(MACI/ACI) or even PJAC.
6. Larger lesions >2 cm2 with subchondral bone
loss 6–10 cm2 = OAT or OCA and represent
a strong opportunity to be a salvage procedure prior to the necessitation of arthroplasty.
PJAC and MACI/ACI are contraindicated
without addressing bony involvement.
7. MACI/ACI and PJAC provide easier topography matching than OCA or OAT.
References
1. Heir S, Nerhus TK, Røtterud JH, et al. Focal cartilage
defects in the knee impair quality of life as much as
severe osteoarthritis: a comparison of knee injury and
osteoarthritis outcome score in 4 patient categories
scheduled for knee surgery. Am J Sports Med.
2010;38(2). https://doi.org/10.1177/0363546509352
157.
2. Riboh JC, Cole BJ, Farr J. Particulated articular
cartilage for symptomatic chondral defects of the
knee. Curr Rev Musculoskelet Med. 2015;8(4).
https://doi.org/10.1007/s12178-015-9300-0.
K. Credille et al.
3. Yanke AB, Cole BJ. Joint preservation of the knee: a
clinical casebook. 2019. https://doi.org/10.1007/9783-030-01491-9.
4. Guermazi A, Hayashi D, Roemer FW, et al. Brief
Report: Partial- and full-thickness focal cartilage
defects contribute equally to development of new
cartilage damage in knee osteoarthritis: the multicenter osteoarthritis study. Arthr Rheumatol 2017;69
(3). https://doi.org/10.1002/art.39970.
5. Krych AJ, Saris DBF, Stuart MJ, Hacken B. Cartilage injury in the knee: assessment and treatment
options. J Am Acad Orthop Surg. 2020;28(22).
https://doi.org/10.5435/JAAOS-D-20-00266.
6. Krych AJ, Hevesi M, Desai VS, Camp CL, Stuart MJ,
Saris DBF. Learning from failure in cartilage repair
surgery: an analysis of the mode of failure of primary
procedures in consecutive cases at a tertiary referral
center. Orthop J Sports Med. 2018;6(5). https://doi.
org/10.1177/2325967118773041.
7. Dixit S, DiFiori JP, Burton M, Mines B. Management of patellofemoral pain syndrome. Am Fam
Phys. 2007;75(2).
8. Caton J, Deschamps G, Chambat P, Lerat JL,
Dejour H. [Patella infera. Apropos of 128 cases].
Revue de chirurgie orthopedique et reparatrice de
l’appareil moteur. 1982;68(5).
9. Grelsamer RP, Bazos AN, Proctor CS. Radiographic
analysis of patellar tilt. J Bone Joint Surg Ser B.
1993;75(5). https://doi.org/10.1302/0301-620x.75b5.
8376449.
10. Dejour H, Walch G, Neyret P, Adeleine P. [Dysplasia
of the femoral trochlea]. Revue de chirurgie orthopedique et reparatrice de l’appareil moteur. 1990;
76(1).
11. Gomoll AH, Yoshioka H, Watanabe A, Dunn JC,
Minas T. Preoperative measurement of cartilage
defects by MRI underestimates lesion size. Cartilage.
2011;2(4).
https://doi.org/10.1177/194760351039
7534.
12. Mehl J, Feucht MJ, Bode G, Dovi-Akue D, Südkamp
NP, Niemeyer P. Association between patellar cartilage defects and patellofemoral geometry: a
matched-pair MRI comparison of patients with and
without isolated patellar cartilage defects. Knee Surg
Sports Traumatol Arthrosc 2016;24(3). https://doi.
org/10.1007/s00167-014-3385-7.
13. Johnston JD, Masri BA, Wilson DR. Computed
tomography topographic mapping of subchondral
density (CT-TOMASD) in osteoarthritic and normal
knees: methodological development and preliminary
findings. Osteoarthr Cartil. 2009;17(10). https://doi.
org/10.1016/j.joca.2009.04.013.
14. Farr J, Cole BJ, Sherman S, Karas V. Particulated
articular cartilage: CAIS and DeNovo NT. J Knee
Surg. 2012;25(1). https://doi.org/10.1055/s-00311299652.
15. Jones KJ, Cash BM. Matrix-induced autologous
chondrocyte implantation with autologous bone
grafting for osteochondral lesions of the femoral
Chondral and Osteochondral Lesions in the Patellofemoral Joint
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
trochlea. Arthrosc Tech. 2019;8(3):e259-66. https://
doi.org/10.1016/J.EATS.2018.10.022.
Moran CJ, Pascual-Garrido C, Chubinskaya S, et al.
Restoration of articular cartilage. J Bone Joint Surg
Ser A. 2014;96(4). https://doi.org/10.2106/JBJS.L.
01329.
Montgomery SR, Foster BD, Ngo SS, et al. Trends in
the surgical treatment of articular cartilage defects of
the knee in the United States. Knee Surg Sports
Traumatol Arthrosc. 2014;22(9). https://doi.org/10.
1007/s00167-013-2614-9.
Grieshober JA, Stanton M, Gambardella R. Debridement of articular cartilage: the natural course. Sports
Med Arthrosc Rev. 2016;24(2). https://doi.org/10.
1097/JSA.0000000000000108.
Mestriner AB, Ackermann J, Gomoll AH. Patellofemoral cartilage repair. Curr Rev Musculoskelet Med.
2018;11(2).
https://doi.org/10.1007/s12178-0189474-3.
Galloway MT, Noyes FR. Cystic degeneration of the
patella after arthroscopic chondroplasty and subchondral bone perforation. Arthrosc J Arthrosc Relat
Surg. 1992;8(3). https://doi.org/10.1016/0749-8063
(92)90070-R.
Anderson DE, Rose MB, Wille AJ, Wiedrick J,
Crawford DC. Arthroscopic mechanical chondroplasty of the knee is beneficial for treatment of
focal cartilage lesions in the absence of concurrent
pathology. Orthop J Sports Med. 2017;5(5). https://
doi.org/10.1177/2325967117707213.
Federico DJ, Reider B. Results of isolated patellar
debridement for patellofemoral pain in patients with
normal pateliar alignment. Am J Sports Med.
1997;25(5). https://doi.org/10.1177/036354659702
500513.
Steadman JR, Rodkey WG, Briggs KK. Microfracture to treat full-thickness chondral defects: surgical
technique, rehabilitation, and outcomes. J Knee Surg.
2002;15(3).
Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture:
surgical technique and rehabilitation to treat chondral
defects. In: Clinical orthopaedics and related
research, vol. 391; 2001. https://doi.org/10.1097/
00003086-200110001-00033.
Mithoefer K, Mcadams T, Williams RJ, Kreuz PC,
Mandelbaum BR. Clinical efficacy of the microfracture technique for articular cartilage repair in the
knee: an evidence-based systematic analysis. Ame J
Sports Med. 2009;37(10). https://doi.org/10.1177/
0363546508328414.
Gobbi A, Karnatzikos G, Kumar A. Long-term
results after microfracture treatment for fullthickness knee chondral lesions in athletes. Knee
Surg Sports Traumatol Arthrosc. 2014;22(9). https://
doi.org/10.1007/s00167-013-2676-8.
Goyal D, Keyhani S, Lee EH, Hui JHP. Evidencebased status of microfracture technique: a systematic
review of Level I and II studies. Arthrosc J Arthrosc
Relat Surg. 2013;29(9). https://doi.org/10.1016/j.
arthro.2013.05.027.
327
28. Kreuz PC, Steinwachs MR, Erggelet C, et al. Results
after microfracture of full-thickness chondral defects
in different compartments in the knee. Osteoarthr
Cartil. 2006;14(11). https://doi.org/10.1016/j.joca.
2006.05.003.
29. Minas T, Gomoll AH, Rosenberger R, Royce RO,
Bryant T. Increased failure rate of autologous
chondrocyte implantation after previous treatment
with marrow stimulation techniques. Am J Sports
Med. 2009;37(5). https://doi.org/10.1177/036354650
8330137.
30. Rowland R, Colello M, Wyland DJ. Osteochondral
autograft transfer procedure: arthroscopic technique
and technical pearls. Arthrosc Tech. 2019;8(7).
https://doi.org/10.1016/j.eats.2019.03.006.
31. Ambra LF, de Girolamo L, Mosier B, Gomoll AH.
Review: interventions for cartilage disease: current
state-of-the-art and emerging technologies. Arthr
Rheumatol. 2017;69(7). https://doi.org/10.1002/art.
40094.
32. Hangody L, Ráthonyi GK, Duska Z, Vásárhelyi G,
Füles P, Módis L. Autologous osteochondral mosaicplasty. Surgical technique. J Bone Joint Surg Am.
2004;86-A Suppl 1.
33. Baltzer AWA, Ostapczuk MS, Terheiden HP,
Merk HR. Good short- to medium-term results after
osteochondral autograft transplantation (OAT) in
middle-aged patients with focal, non-traumatic osteochondral lesions of the knee. Orthop Traumatol Surg
Res. 2016;102(7). https://doi.org/10.1016/j.otsr.
2016.06.004.
34. Astur DC, Arliani GG, Binz M, et al. Autologous
osteochondral transplantation for treating patellar
chondral injuries. J Bone Joint Surg. 2014;96(10).
https://doi.org/10.2106/jbjs.m.00312.
35. Emre TY, Atbasi Z, Demircioglu DT, Uzun M,
Kose O. Autologous osteochondral transplantation
(mosaicplasty) in articular cartilage defects of the
patellofemoral joint: retrospective analysis of 33
cases. Musculoskelet Surg. 2017;101(2). https://doi.
org/10.1007/s12306-016-0448-6.
36. Yabumoto H, Nakagawa Y, Mukai S, Saji T. Osteochondral autograft transplantation for isolated patellofemoral osteoarthritis. Knee. 2017;24(6). https://
doi.org/10.1016/j.knee.2017.07.016.
37. Zouzias IC, Bugbee WD. Osteochondral allograft
transplantation in the knee. Sports Med Arthrosc
Rev. 2016;24(2). https://doi.org/10.1097/JSA.00000
00000000109.
38. Meric G, Gracitelli GC, Görtz S, de Young AJ,
Bugbee WD. Fresh osteochondral allograft transplantation for bipolar reciprocal osteochondral
lesions of the knee. Am J Sports Med. 2015;43(3).
https://doi.org/10.1177/0363546514562549.
39. Tschon M, Veronesi F, Giannini S, Fini M. Fresh
osteochondral allotransplants: outcomes, failures and
future developments. Injury. 2017;48(7). https://doi.
org/10.1016/j.injury.2017.05.006.
40. Bennett CH, Nadarajah V, Moore MC, et al. Cartiform implantation for focal cartilage defects in the
328
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
K. Credille et al.
knee: a 2-year clinical and magnetic resonance
imaging follow-up study. J Orthop. 2021;24.
https://doi.org/10.1016/j.jor.2021.02.025.
Assenmacher AT, Pareek A, Reardon PJ,
Macalena JA, Stuart MJ, Krych AJ. Long-term
outcomes after osteochondral allograft: a systematic
review at long-term follow-up of 12.3 years.
Arthrosc J Arthrosc Relat Surg. 2016;32(10).
https://doi.org/10.1016/j.arthro.2016.04.020.
Cameron JI, Pulido PA, McCauley JC, Bugbee WD.
Osteochondral allograft transplantation of the
femoral trochlea. Am J Sports Med. 2016;44(3).
https://doi.org/10.1177/0363546515620193.
Hevesi M, Krych AJ, Saris DBF. Treatment of
cartilage defects with the matrix-induced autologous
chondrocyte implantation cookie cutter technique.
Arthrosc Tech. 2019;8(6). https://doi.org/10.1016/j.
eats.2019.01.022.
Mistry H, Connock M, Pink J, et al. Autologous
chondrocyte implantation in the knee: systematic
review and economic evaluation. Health Technol
Assess. 2017;21(6). https://doi.org/10.3310/hta21060.
Marlovits S, Zeller P, Singer P, Resinger C, Vécsei
V. Cartilage repair: generations of autologous chondrocyte transplantation. Eur J Radiol. 2006;57(1).
https://doi.org/10.1016/j.ejrad.2005.08.009.
Wang T, Belkin NS, Burge AJ, et al. Patellofemoral
cartilage lesions treated with particulated juvenile
allograft cartilage: a prospective study with minimum
2-year clinical and magnetic resonance imaging
outcomes. Arthrosc J Arthrosc Relat Surg. 2018;34
(5). https://doi.org/10.1016/j.arthro.2017.11.021.
Brittberg M, Recker D, Ilgenfritz J, Saris DBF. Matrixapplied characterized autologous cultured chondrocytes
versus microfracture: five-year follow-up of a prospective randomized trial. Am J Sports Med. 2018;46(6).
https://doi.org/10.1177/0363546518756976.
Vanlauwe JJE, Claes T, van Assche D, Bellemans J,
Luyten FP. Characterized chondrocyte implantation
in the patellofemoral joint: an up to 4-year follow-up
of a prospective cohort of 38 patients. Am J Sports
Med. 2012;40(8). https://doi.org/10.1177/03635465
12452712.
Gobbi A, Kon E, Berruto M, et al. Patellofemoral
full-thickness chondral defects treated with secondgeneration autologous chondrocyte implantation.
Am J Sports Med. 2009;37(6). https://doi.org/10.
1177/0363546509331419.
von Keudell A, Han R, Bryant T, Minas T. Autologous
chondrocyte implantation to isolated patella cartilage
defects: two- to 15-year follow-up. Cartilage. 2017;8
(2). https://doi.org/10.1177/1947603516654944.
Andriolo L, Merli G, Filardo G, Marcacci M, Kon E.
Failure of autologous chondrocyte implantation.
Sports Med Arthrosc Rev. 2017;25(1):10–8. https://
doi.org/10.1097/JSA.0000000000000137.
Schuette HB, Kraeutler MJ, McCarty EC. Matrixassisted autologous chondrocyte transplantation in
the knee: a systematic review of mid- to long-term
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
clinical outcomes. Orthop J Sports Med. 2017;5(6).
https://doi.org/10.1177/2325967117709250.
Frisbie DD, Lu Y, Kawcak CE, Dicarlo EF,
Binette F, Mcilwraith CW. In Vivo evaluation of
autologous cartilage fragment-loaded scaffolds
implanted into equine articular defects and compared
with autologous chondrocyte implantation. Am J
Sports Med. 2009;37(1_suppl). https://doi.org/10.
1177/0363546509348478.
Bonasia DE, Martin JA, Marmotti A, et al. Cocultures of adult and juvenile chondrocytes compared
with adult and juvenile chondral fragments: in vitro
matrix production. Am J Sports Med. 2011;39(11).
https://doi.org/10.1177/0363546511417172.
Adkisson HD, Martin JA, Amendola RL, et al. The
potential of human allogeneic juvenile chondrocytes for
restoration of articular cartilage. Am J Sports Med.
2010;38(7).
https://doi.org/10.1177/03635465103
61950.
Farr J, Cole B, Sherman S, Karas V. Particulated
articular cartilage: CAIS and DeNovo NT. J Knee
Surg. 2012;25(01):023–30. https://doi.org/10.1055/s0031-1299652.
Gomoll AH, Probst C, Farr J, Cole BJ, Minas T. Use of
a Type I/III bilayer collagen membrane decreases
reoperation rates for symptomatic hypertrophy after
autologous chondrocyte implantation. Am J Sports
Med. 2009;37(1_suppl).https://doi.org/10.1177/03635
46509348477.
Farr J, Tabet SK, Margerrison E, Cole BJ. Clinical,
radiographic, and histological outcomes after cartilage repair with particulated juvenile articular cartilage: a 2-year prospective study. Am J Sports Med.
2014;42(6).
https://doi.org/10.1177/03635465145
28671.
Tompkins M, Hamann JC, Diduch DR, et al.
Preliminary results of a novel single-stage cartilage
restoration technique: particulated juvenile articular
cartilage allograft for chondral defects of the patella.
Arthrosc J Arthrosc Relat Surg. 2013;29(10). https://
doi.org/10.1016/j.arthro.2013.05.021.
Buckwalter JA, Bowman GN, Albright JP, Wolf BR,
Bollier M. Clinical outcomes of patellar chondral
lesions treated with juvenile particulated cartilage
allografts. Iowa Orthop J. 2014;34.
Dawkins BJ, Shubin Stein BE, Mintz DN, et al.
Patellofemoral joint cartilage restoration with particulated juvenile allograft in patients under 21 years
old. Knee. Published online 2021. https://doi.org/10.
1016/j.knee.2021.07.006.
Hurley ET, Davey MS, Jamal MS, Manjunath AK,
Alaia MJ, Strauss EJ. Return-to-play and rehabilitation protocols following cartilage restoration procedures of the knee: a systematic review. Cartilage.
2021;13(1_suppl). https://doi.org/10.1177/19476035
19894733.
Patellofemoral Arthritis
Christopher S. Frey, Augustine W. Kang,
Kenneth Lin, Doug W. Bartels, Jack Farr,
and Seth L. Sherman
1
Background
Patellofemoral arthritis (PF OA) is a common
degenerative disease of the joint surface between
the patella and trochlea that may exist in isolation
or as part of a larger multi-compartmental
disease-state. It is a common pathology with
annual incidence between 0.6% to 3.1% [1].
About half of those with symptomatic knee
osteoarthritis were found to have patellofemoral
involvement [2]. Isolated disease is reportedly
found in 9% of symptomatic knees in patient
over 40 [3]. Rates were similar between women
and men; however, in symptoms-based cohorts,
females twice the prevalence compared to males
(43% vs 23%) [2].
Considering the prevalence of patellofemoral
arthritis, it is no surprise that the disease poses a
significant burden on society. A 2018 systematic
review of studies examining quality of life
among patients with patellofemoral pain reported
C. S. Frey K. Lin D. W. Bartels
S. L. Sherman (&)
Department of Orthopaedic Surgery, Stanford
University, Stanford, CA, USA
e-mail: shermans@stanford.edu
A. W. Kang
Stanford School of Medicine, Stanford, CA, USA
J. Farr
Knee Preservation and Cartilage Restoration Center,
OrthoIndy, Indianapolis, IN, USA
that relative to pain-free controls population
norms, patients with patellofemoral pain had
worse Knee Injury and Osteoarthritis Outcome
Score-Quality of Life scores and physical and
mental functioning scores [4]. There is also an
economic impact. It is thought that knee
osteoarthritis treatment costs well over $27 billion in annual healthcare costs alone. At 9%
patellofemoral OA costs are not inconsequential.
When surgery is indicated for PF OA, a recent
study found that among younger patients, knee
arthroplasty and subsequent procedures approach
$50,000 [5]. It should be noted that patellofemoral arthroplasty has cheaper implants and was
found to have better quality-adjusted life year
gains Moreover, disability and time off work has
financial repercussions as well. In fact, for generalized OA, there is an estimated $4,835 loss in
productivity per year [6]. This can be attributed
to reduced productivity, long-term sick leave,
unemployment, and early retirement [7–9]. In
those undergoing arthroplasty before 60 years of
age, the cost of salvage procedures in the event
of failure should also be taken into account. For
this, patellofemoral arthroplasty proves easier as
it can simply be easily converted to a primary
total knee replacement.
Although often overlooked, isolated patellofemoral arthritis is a significant healthcare issue.
The goal of this chapter is to provide an overview
of the common causes, workup, and treatment of
PF OA.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_23
329
330
2
C. S. Frey et al.
Anatomy
The patellofemoral joint is a unique and morphologically complex structure involving the
posterior surface of the patella and the trochlea.
The posterior surface of the patella is typically
covered by articular cartilage up to 7 mm thick
[10]. It is made up of multiple facets, primarily
the lateral, medial, and odd facets as well as a
central ridge that has some variation in its position [11]. The trochlea consists of a groove surrounded by a medial and lateral facet which
forms a concave trough for the patella to glide
through. Normal trochlear morphology has a
lateral facet that is higher than the medial
facet allowing it to buffer against lateralization of
the patella.
The patella acts as a mechanical pulley for
extensor mechanism, and is particularly critical
in the last 30° of knee extension [12]. Passive
alignment of the patella is maintained by both
bony and soft features. The shape of the patella
and trochlea guides the patella throughout much
of the arc of motion. Passive soft tissue constraints consist of medial and lateral ligamentous
and retinacular complexes [13]. Medially there is
the medial patellar complex consisting of the
medial patellofemoral ligament (MPFL), medial
quadriceps tendon–femoral ligament (MQTFL),
medial patellomeniscal ligament (MPML), and
medial patellotibial ligament (MPTL) which
collectively work to prevent lateralization
throughout the full arc of patellar tracking [14].
On the lateral side, there are the superficial lateral
retinaculum and deeper patellotibial and epicondylopatellar bands [11]. Dynamic alignment
is largely dictated by the quadriceps, hip external
rotators, and core [11]. Specifically, the vastus
medialis oblique (VMO) is a primary restraint to
lateral subluxation of the patella and its weakening may be a significant cause of “giving
way”, if not frank instability. If the pull of the
quadriceps vector is excessively lateral, this may
increase the lateral PF contact pressure and
contribute to instability [15]. The intricate balance of these factors keeps the patella centered
through its excursion in a healthy knee.
As the patella tracks, it is subject to a dynamic
range of force vectors. In full extension, there is
almost no posterior force and thus minimal joint
reactive force. As flexion of the knee increases
the patella begins to engage the trochlea. The
force vectors of the patellar and quadriceps tendons become more posteriorly oriented and
generate a cumulative posterior force [16].
Therefore, as the knee approaches 90° the joint
reactive forces increase. At the same time, the
contact area of the patella increases until about
60° of flexion, decreasing pressure [17]. It is
associated with a general shift in contact from
distal to proximal in the patella and from proximal to distal in the trochlea.
3
Pathophysiology and Risk Factors
Patellar instability is the most common cause of
cartilage injury and subsequent degenerative
change in isolated PF OA, constituting about one
in three cases [18]. Upon initial dislocation, up to
95% of knees may sustain articular cartilage
damage to the patella [19]. Moreover, over ¾ of
these injuries will involve an osteochondral
defect. This highlights the importance of
obtaining an MRI after patellar dislocations.
After the initial dislocation, it appears that there
is a significantly positive correlation between the
number of dislocations and prevalence of PF OA
on MRI [20]. In fact, nearly all (97%) of chronic
dislocators were found to have cartilage lesions
of the PF joint. Any significant alteration to the
previously mentioned mechanisms of stability
can result in maltracking or dislocation. For
example, patients with trochlear dysplasia have a
significantly higher risk of arthritis [18]. Patients
with a trochlear boss (aka, spur, in which a
proximal focal bony prominence is relatively
anterior) have significantly greater risk of PF OA
and the greater the dysplasia, the more risk for
degeneration [18].
Another common mechanism of patellofemoral cartilage injury is blunt trauma. Excluding
dislocations, traumatic etiology is thought to be
responsible for about 9% of isolated PF arthritis
Patellofemoral Arthritis
in some cohorts [18]. Injuries with fractures
involving the articular surfaces of the patella or
trochlea will likely pose the same risks of
arthritis as most intra-articular fractures. In these
cases, direct force transmission as well as chronic
elevations in contact forces from joint incongruity leads to chondrocyte death [21]. For tibial
plateau fractures, the incidence of secondary
osteoarthritis may be nearly 50% [22]. Even
without fractures, energy delivered is thought to
manifest in delayed chondral damage. In other
words, chondrocyte death occurs with impacts
insufficient to cause bone fracture. In an in vitro
rabbit model, cell death was detected at 20 Mpa
impacts while frank matrix damage was found at
30 Mpa impacts [23]. With no living chondrocytes, the articular cartilage matrix deteriorates
over time. Chondrocyte overload may also be a
result of diminished trochlea-patella congruence
or disturbed joint homeostasis.
Ligamentous injuries are also associated with
PF OA. A common association is with anterior
cruciate ligament (ACL) injuries. One systematic
review reported that PF OA is associated with
ACL injury, especially in cases of reconstruction
[24]. Bone-patellar tendon-bone graft, singlebundle reconstruction, and delayed operation
time reported a higher prevalence of PF OA
within this subset. In fact, the prevalence of
PF OA at 15 years status post ACL reconstruction may be nearly 50% [25]. The mechanism is
poorly understood, but loss of terminal extension
and reduced patellar mobility may play a role.
Quadriceps weakness and an overall inflammatory state may be additional contributing factors.
Osteochondritis dissecans (OCD) is a condition involving focal subchondral bone impairment, necrosis, collapse, and destabilization of
overlying articular cartilage. Although the vast
majority occur in the medial femoral condyle and
less commonly in the lateral femoral condyle, it
sometimes occurs in the patellofemoral joint
[26]. Most of these patients were competitive
athletes at some point. One longitudinal study of
skeletally immature patients reported that 2/42
331
nonoperatively treated and 4/53 operatively
treated children with OCD lesions ultimately
developed symptomatic arthritis [27].
Our knowledge of the genetic component of
osteoarthritis is still limited and epigenetics is
even more limited. It has been estimated that the
heritability of osteoarthritis may be 50% or more
[28]. Some genes reported to be associated
include VDR, AGC1, IGF-1, ER alpha, TGF beta,
CRTM, CRTL, and collagen II, IX, and XI. Genes
that have been identified to lead to patellar
anomalies when altered include TBX4 and
LMX1B [29]. In general, these are associated with
nail patella syndrome, small patella syndrome,
and isolated patella aplasia. These conditions can
lead to patellar dysplasia and instability which
will ultimately contribute to PF OA.
4
Presentation
It is crucial to understand the underlying
pathology that links chondrosis to pain. Cartilage
is considered an aneural tissue. Thus, the actual
pain generator needs elucidation before planning
treatment [30]. This can be from surrounding soft
tissue, bone or rarely referred pain.
Typically, the patient with PF OA will present
with chronic anterior knee pain that is aggravated
with flexion and activities such as lunges and
stairs. [3] When isolated, they will often tolerate
ambulating on level ground, but avoid stairs or
squats. Patients may experience swelling and
stiffness as well, especially with flares.
In addition to pain, patients may also experience mechanical symptoms. This can consist of
subjective sensations of grinding, popping, or
clicking, likely from the increased friction
between patella and trochlea. This should not be
associated with frank locking, however, this can
be associated with other pathology-like displaced
meniscus tear or chondral flap [31]. The patient
may also complain of patellar instability, which
often, as discussed above, is a risk factor but not
prerequisite for PF OA [18].
332
5
C. S. Frey et al.
Examination
It is helpful to examine the patient standing/
walking, sitting, and in supine. This allows for a
thorough assessment of leg alignment, kinematics, patellar mechanics, and provocative testing.
Observing the patient while standing offers
much information about their limb alignment.
Aberrations impacting patellar alignment such as
genu valgum, femoral anteversion, external tibial
torsion, or pes planus can be observed. Gait
evaluation may yield characteristic stance
abnormalities such as anterior pelvic tilt through
stance phase on the affected side and lateral
pelvic tilt on the contralateral side. There may
also be increased hip adduction and lower hip
extension during stance phase [32].
Having the patient sit with knees bent over the
examination table makes it easy to assess patellar
tracking. The patella should track more or less
midline with active knee extension, but may
track laterally. This is referred to as the “J” sign
which may be associated with trochlear dysplasia
or soft tissue conditions that are associated with
instability [33]. The “jumping J” sign, an exaggerated form of the “J” sign, may be indicative of
bony abnormality such as a supratrochlear spur
implying soft tissue surgery alone may not be
helpful [33].
In the supine position it is easy to inspect and
palpate the knee and surrounding anatomy. Some
commonly described findings include quadriceps
atrophy, effusion, and patellofemoral crepitus
[34]. Quadriceps atrophy seems to impact all
components, not just the VMO [35]. Patellar tilt,
patella alta, apprehension, and active instability
tests have all been described. In brief, lateral
patellar tilt is the angle the patella can be
manipulated to by pressing on the medial patella
and pulling on the lateral edge. This represents
relative lateral tightness and loading. The patella
alta test involves pressure over the inferior pole
of the patella while the knee moves from extension to flexion and is positive with pain. Patellar
apprehension involves a laterally directed force
to the patella tested in an arc of knee flexion and
extension. It is considered positive if painful or
this is apprehension or guarding. Although it is
often considered a test for instability, it may also
be associated with PF OA. The active instability
test involves assessing isometric quadriceps
contraction in slight knee flexion (*15°) with
the lower extremity in a neutral position. It is
considered positive if there is lateral movement
of the patella. Although specific, these tests may
lack sensitivity in diagnosing PF OA [36]. In
addition, the patellar grind test, or Clarke Test
involves the patient contracting their quadriceps
muscle while the provider resists proximal
movement of the patella with counterforce. Pain
is considered a positive finding.
The Q angle can also be measured while
supine to understand the direction of the force
vector. It is measured as the angle between the
line from the anterior superior iliac spine to the
center of the patella and the line from the center
of the patella to the tibial tubercle. The normal
value is typically 10–15° for men and 15–20° for
women There is some concern for poor intra and
inter-observer reliability, but may have improved
accuracy when performed using a goniometer in
the clinic [37].
6
Imaging
Radiographs remain important in the evaluation
of PF OA. Radiographic signs of arthritis include
joint space narrowing, cyst development, subchondral sclerosis, and osteophyte formation.
There are multiple views that allow for inspection of various aspects of the knee.
The low flexion angle axial view (Merchant,
Laurin, etc.) is helpful for directly assessing
advanced degenerative change in the joint. If full
thickness chondral defects are not present at this
angle, the joint space may appear near normal.
The most common grading system is the Iwano
grade, which consists of four stages as follows
[38]. Stage I involves a remodeling joint line,
Stage II depicts joint narrowing less than 3 mm,
Stage III is narrowing over 3 mm, but no bony
contact, and Stage IV describes bone on bone
contact. Some of the commonly implemented
Patellofemoral Arthritis
parameters include: sulcus angle, congruence
angle, and the lateral patellofemoral angle.
Specifically, the sulcus angle measures trochlear
depth. It is calculated as the angle between peaks
of MFC and LFC and the nadir of the intracondylar sulcus. Greater values indicate trochlear
dysplasia, with 145° often being cited as the
cutoff [39]. The congruence angle, which uses
the angle between the patellar articular ridge and
apex of the sulcus angle, measures patellar subluxation. Normal subjects have an average angle
of 16° (medial to the congruence line), and an
angle over 16° is typically associated with subluxation [40]. Lastly, the lateral patellofemoral
angle assesses patellar tilt. This parameter is
measured as the angle between the line along the
lateral facet and along the anterior condyles. If
these lines are parallel or converge, it is indicative of increased tilt or subluxation and is associated with more severe chondromalacia [41, 42].
It is important to note that absolute values cannot
be used in isolation. One should consider the
whole picture when evaluating radiographs in
PF OA.
In the context of evaluating PF OA, the
standing flexed PA, also known as the Rosenberg
or skier view, as well as the classic AP, primarily
aid in evaluation of the tibiofemoral joint.
The PA view is considered to be more sensitive
for catching medial/lateral compartment arthritis
and may capture this before standard AP films
[43]. However, a subset of patients with more
anterior TF OA will have joint space narrowing
only on the AP view.
The true lateral view (femoral condyles are
superimposed and confluent) allows for direct
visualization of degenerative change in the
patellofemoral joint as well as morphologic features that may predispose to arthritis there. While
it visualizes the same hallmarks of PF OA as
suggested by axial views, the lateral view has
been found to have lower diagnostic accuracy
[44]. Using these true lateral images, the classic
signs of trochlear dysplasia may be detected as
described by Dejour [39]. In short, the crossing
sign appears when the line of the trochlear
groove intersects the anterior border of the
femoral condyle. The supratrochlear spur is seen
333
as a prominence just proximal to the trochlea and
illustrates a prominence of the trochlea that
works like a ramp to push off the patella. Lastly,
the double contour consists of the radiographic
line adjacent to the crossing sign and represents a
hypoplastic medial condyle. 96% of patients with
patellar instability were found to have these
radiographic signs of dysplasia [39]. The Dejour
classification was developed based upon various
combinations of these findings and dysplasia is
assigned to 4 main types to aid in operative
planning. However, 3D reconstruction from MRI
and/or CT have demonstrated a more nuanced
continuum of dysplasia.
Patellar height is another important factor
measured on these lateral views. Patella alta may
be associated with patellofemoral osteoarthritis
[45]. This is related to multiple factors. Patients
with this abnormal positioning of the patella have
been found to have decreased contact surfaces of
the patellofemoral joint, which increases the
pressure on the cartilage interface and can
directly lead to chondral injury [46]. Patella alta
can also result in patellar instability, which can
be a driving factor of degeneration [47]. On the
other hand, patella baja is associated with anterior knee pain, decreased range of motion, and
extensor tendon weakness [48]. This is less
common and may be associated with prior
intervention. Patella height factors into preoperative planning to decide whether or not the
patellar component will be engaged in the trochlea component at full quad active extension.
Although there may be some proponents of
the Insall-Salvati, the most commonly used
measurement by patellofemoral experts is the
Caton-Deschamps Index (CDI) [49, 50]. It is
calculated by dividing the distance from the
anterosuperior articular margin of the tibia to the
inferior articular margin of the patella/articular
surface patella. Thus, it changes after tibial
tubercle osteotomies, but stays constant with
various degrees of knee flexion. This may be of
value in corrective TTOs to assess for restoration
of more “regular” parameters. Values over 1.2
are typically associated with patella alta. In
addition, the patella overlap with the trochlea
yields another assessment of patellar height.
334
The three compartments of the knee should
not be viewed in isolation. For a complete picture
of the knee, bilateral full hip to ankle radiographs
are crucial to better characterize the anatomic and
mechanical axes of the limb. This view will
depict aberrations in contact forces and therefore,
joint degeneration patterns. It will also assist in
surgical planning. Knowledge of alignment will
direct one to the most appropriate soft and/or
bony intervention for a mechanically sound knee.
Advanced imaging is particularly useful for
patellofemoral joint evaluation. Computed
tomography (CT) is an excellent tool for
depicting bony morphology. It can be used to
assess trochlear dysplasia, patellar height, and the
tibial tubercle-trochlear groove (TT-TG) distance. TT-TG measurement captures malalignment in the axial plain, specifically the
lateralization of the tibial tubercle relative to the
trochlea. Values over 20 mm are often described
as pathologic and an indication for intervention
[39]. One should note the limitations of this
measurement, however. It has been shown to
positively vary with age and patient height. [51]
This would need to be taken into consideration
for patients at either end of the height spectrum.
CT can also be used to evaluate the direct effects
of degenerative change on the joint. Although
cartilage is not best visualized with standard CT
imaging, subchondral bone can easily be scrutinized. In fact, this imaging modality has superior
resolution of underlying bony structure when
compared to MRI [52]. Considering many
patients will have an MRI and full XR series
already, CT is not always worth the additional
risk.
Unlike CT, MRI is useful for directly evaluating articular cartilage. Considering how thin
and structurally contoured this tissue is, high
quality imaging is required. T1-weighted images
are limited in delineating the boundary between
joint effusion and cartilage surface [53]. This
offers basic anatomic details but is not useful for
focal defects or delamination. T2-weighted
imaging provides better contrast resolution of
this interface, but has the limitation of poor
internal cartilage signal. For these reasons,
C. S. Frey et al.
proton density-weighted sequences are often
most accurate in evaluating cartilage defects [54].
Findings can be classified with the modified
Outerbridge classification, which has been
adapted to MRI use. It consists of seven stages
starting with mere signal heterogeneity and
ending with full thickness cartilage loss.
In addition to cartilage, MRI is useful for
picking up changes in underlying bone. Common
changes in subchondral bone include cyst formation, sclerosis, and marrow edema. Although
fairly nonspecific, focal areas of edema may be
indicative of overlying cartilage defects [55].
There may also be classic bone bruising patterns
of patellofemoral instability at the medial patellar
facet and lateral femoral condyle. These findings
are helpful for guiding pre-operative planning;
however, arthroscopy is still considered the gold
standard [56]. After operative repair, MRI may
be used for monitoring healing. There exist
several detailed scoring systems such as
MOCART and OCAMRISS, however, the data
is mixed regarding correlation with clinical outcomes and at this time, this is largely applied in
the setting of research [57].
Similar to CT, MRI offers evaluation of axial
alignment. MRI is an accurate modality for
measuring TT-TG, with good inter-rater reliability [58]. However, it appears to consistently
yield higher values; 3.8 mm on average according to one study. Thus, the calculated values
from CT and MRI are not interchangeable. With
the ability to visualize soft tissue, MRI allows
one to measure TT-PCL as well. Similarly,
20 mm may be used as a cutoff for pathologic
lateralization [51]. However, there exist some
key differences between TT-TG and TT-PCL that
must be noted. By utilizing points in the femur
and tibia, TT-TG measures gross femorotibial
rotation as a result of factors such as femoral
torsion, tibial torsion, lateralized tibial tubercle,
and medialized groove. It is, therefore, more
sensitive to knee flexion as well, through the
“screw home mechanism”. By only using points
on the tibia, TT-PCL isolates tibial pathology. By
combining the two metrics, one can pinpoint the
cause of the malalignment.
Patellofemoral Arthritis
7
Conservative Treatment
Once PF OA is determined to be the cause of the
patient’s symptoms, it is important to understand
the driving force behind the pathology. For
example, patellar instability due to malalignment
or trochlear dysplasia may be treated with different methods than an isolated osteochondritis
dissecans lesion or prior trauma. Regardless, a
specific treatment plan must be developed to
address their predisposing mechanical factors
and corresponding chondral pathology.
Conservative management is performed first
and consists of many different techniques.
Supervised physical therapy (PT) is an often
implemented first line intervention. Benefits may
be derived from general exercise and wellness or
even weight loss. Much of the literature regarding PT and osteoarthritis comes from tricompartmental literature, but it has shown modest
improvement in outcomes with little risk [59].
For these reasons, it is often recommended as a
first line intervention. The most recent AAOS
guidelines also strongly recommend selfmanagement and patient education programs to
empower patients to best help themselves [60].
Regarding patellofemoral joint arthritis specifically, a “core to floor” program is often implemented. The addition of core and hip
strengthening to standard therapy focusing on the
afflicted extremity has been shown to have
additive effects with pain and strength [61, 62].
McConnell tape was developed as a means of
noninvasive restraint to prevent lateralization of
the patella. By improving alignment, joint forces
can be improved across the patellofemoral joint.
MRI has shown that taping can significantly
restore alignment in knees with PF OA [63]. Pain
was also reduced with squatting. One small study
found patellar taping to be associated with a 25%
reduction in knee pain [64]. This may be attributed to the improved alignment, but it is difficult
to parse out the impact of placebo.
Bracing works in a similar fashion as taping to
improve pain. Most patella stabilizing braces are
designed to hold the patella medially. It was
found that brace use during the day was
335
associated with decreased pain and bone marrow
edema [65]. Moreover, it appears that bracing
may also help to improve alignment and kinematics with walking, but not stairs [66, 67]. By
increasing the contact area, stress is decreased
which may alleviate the injury to underlying
tissue. Interestingly one study found that the
realigning strap may not provide additional value
in decreasing the pain scores [68]. This may be
because external alignment of the patella does
not improve pain over the simple comfort of
bracing despite adjusting the contact forces. This
study also used one specific brace and these
results may be more reflective of that particular
brace.
Offloading implements may be another option
in relieving symptoms of PF OA. The most
recent AAOS clinical practice guidelines recommends using canes to improve pain and
function in patients with knee osteoarthritis with
moderate strength [60]. Although not specific to
the patellofemoral compartment, the concept of
decreasing joint reactive forces across the joint is
similar and likely transferable, especially with
activities that bring the knee through flexion.
There are even some companies with braces
designed to decrease PF loading.
Oral or topical medications to relieve the pain
and/or inflammation are another first line intervention for primary OA. Although not specifically directed at PF OA, the most recent OARSI,
AAOS, and ESCEO guidelines provide recommendations on nonoperative management of
knee arthritis with pharmaceuticals [59]. There is
a consensus between the three guidelines in
recommending topical NSAIDs because of
improved pain and function with use. Furthermore, this class benefits from a decreased side
effect profile compared to oral NSAIDs. Interestingly, both ESCEO and OARSI strongly recommend against non-pharmaceutcal forms of
glucosamine or chondroitin sulfate while the
AAOS guidelines do not differentiate by preparation and offer a “limited” recommendation.
ESCEO recommends their use when pharmaceutical grade. The committee claims that this
formulation is stabilized and therefore has
336
physiologically relevant bioavailability which
corresponds to clinical efficacy [69]. The OARSI
and AAOS recommend paracetamol conditionally in the short and long term while the ESCEO
only recommends short term use. Both groups
cite low proof of clinical efficacy and mild hepatotoxicity risk.
If this first-line of medical intervention is
inadequate, both guidelines recommend short
term use of oral NSAIDs [59]. Although effective
in controlling symptoms, this medication class is
limited by cardiovascular, renal, and gastric side
effects. It is recommended to take PPIs with
nonselective NSAIDs to mitigate the gastrointestinal effects.
As a last resort pharmaceutical intervention,
patients can also take opioids. The ESCEO
guidelines recommend short term use of relatively
weak narcotics such as tramadol [59]. This is
attributed to efficacious pain relief. However, the
OARSI and AAOS recommend against this class
of medication, even in the short term because of
unsavory side effects such as addiction, nausea,
constipation, and falls. Alternatively, patients can
take duloxetine, a serotonin-norepinephrine
reuptake inhibitor, which is particularly suited
for cases of central pain sensitization as well as
other chronic pain disorders [70, 71].
The vast majority of injections currently in the
orthopaedist’s armamentarium can be broken
down into three groups: viscosupplementation,
corticosteroids, and biologics. All three guidelines support the use of intra-articular corticosteroids, especially in the short term (<6 weeks)
[59, 60]. This broad class of medications acts
through glucocorticoid receptors to downregulate
the inflammatory cascade. Although recently
downgraded to moderate strength in the AAOS
guidelines, it is still considered an integral component of the treatment algorithm for patients
who do not respond to anti-inflammatories due to
significant relief of symptoms. There is some
concern that these injections may be cytotoxic.
Indeed, there are studies that demonstrate both
tenocyte, synoviocyte, and chondrocyte toxicity
with combination injections, including local
anesthetic and corticosteroids [72, 73]. It appears
that bupivacaine and triamcinolone are the least
C. S. Frey et al.
noxious compounds, but it may be safest to avoid
intra-articular anesthetics. This may be considered diagnostic in some sense, but this interpretation is limited in that injections are not
sequestered to the PF compartment.
Viscosupplementation is thought to work by
augmenting the synovial fluid with additional
glycosaminoglycans. This would have improved
lubrication and shock absorbing qualities with
ultimate mechanical and analgesic effects [74].
Typically, this involves hyaluronic acid with both
high and low molecular weight options available.
One small trial of hyaluronic acid used in patients
with PF OA found significant improvements in
pain with stairs and global assessments [75].
However, it was limited by an 18.6% adverse
event rate, most of which were local site reactions
such as joint effusion. In the context of general
osteoarthritis, this treatment has had mixed outcomes with the AAOS recommending against
hyaluronic acid with moderate strength and both
OARSI and ESCEO recommending its use.
The AAOS guidelines cite a lack of clinically
relevant differences when compared to controls in
more recent analysis, even with the use of high
molecular cross-linked formulations.
Lastly, there are various biologic formulations
currently in use or on the horizon that are being
applied to the degenerative joint. Of these, platelet rich plasma (PRP) is probably the most
described. The technology relies on the concentration of a growth factor payload that is not
completely understood and varies with formulation. In general, leukocyte poor (LP-PRP) is
associated with less of an inflammatory effect as
concentrations of the pro-inflammatory cells is
lower than that of whole blood. This formulation
is often favored out of concern for inflammation
after the injection [76]. Additionally, LP-PRP has
also been found to have a greater ability to preserve cartilage mouse models and functional
outcomes in knee OA trials [76, 77].
Unfortunately, due to this variation, studies
are fairly heterogenous. With respect to the
patellofemoral joint, one publication found that
LR-PRP was associated with an increase in volume of patellofemoral cartilage on 3D MRI
analysis as well as several PROMs [78]. There is
Patellofemoral Arthritis
337
a vastly larger body of evidence for general OA.
Overall, results are quite mixed with multiple
large studies and meta-analyses showing no
significant benefit. Subsequently, the AAOS
guidelines downgraded the recommendation
for its use to limited and OARSI recommends
against its use for OA. The most recent ESCEO
guideline does not delve much into the topic.
Topical antiinflammatory
AAOS
ESCEO
OARSI
Strong for
First line
First line
Oral anti-inflammatory
Strong for
First line
First line
Opioid
Strong
against
Conditional
short term
Strong
against
Intra-articular
corticosteroid
Moderate
short term
Conditional
short term
Conditional
short term
Intra-articular
viscosupplementation
Moderate
against
Conditional
Conditional
Intra-articular PRP
Limited
for
No comment
Strong
against
Glucosamine/Chondroitin
Limited
for
First line
(Pharmaceutical
grade)
Strong
against
8
Surgical Management
of Patellofemoral Arthritis
Once non-operative management fails, there are
multiple surgical options. Several important factors should be considered when deciding on the
best management. Patient factors include age,
medical comorbidities, activity level, and symptomatology. The joint as a whole must be considered, and previous injuries, chondral wear
pattern—both location and severity, and ligamentous pathology or instability should be
incorporated into planning. Perhaps most
importantly, lower limb alignment in both the
coronal and axial or rotational planes is integral
to the treatment algorithm for obtaining optimal
outcome. In general, in more diffuse disease or
older lower demand patients, arthroplasty with or
without additional procedures would likely provide more predictable benefit than pure soft tissue work or restorative cartilage surgery. In the
setting of malalignment, depending on the nature
of the malalignment, corrective osteotomy may
be warranted in order to correct aberrant force
vectors and/or patellar instability.
It should be noted that there is a very limited
role for isolated arthroscopy in patellofemoral
arthritis. Knee arthroscopy with debridement
allows for direct evaluation of the cartilage as well
as other intra-articular pathology such as meniscus
injury to facilitate planning for definitive management. In essence, this serves more as a staging
arthroscopy to take inventory of possible surgical
targets. Chondroplasty can be performed on
unstable lesions. Any loose bodies identified
should be removed. Patients may have some initial
symptomatic relief, especially if there are
mechanical symptoms, but the underlying problem may require further definitive surgery. This
technique may be used definitively in instances of
acute pain, specific localized mechanical symptoms, and no malalignment or intra-articular
pathology in low demand patients [79] One registry study found isolated large cartilage defects to
respond well at one year post-operative follow-up,
as long as there was no associated meniscus
pathology requiring debridement.
If there is isolated lateral trochlear or patellar
disease, lateral retinacular lengthening or release
can be used to decrease lateral retinacular forces
on joint, yet the reduction of PF loading has been
questioned. It may also have theoretical benefit
from denervating the retinaculum to provide pain
relief [80]. This can be done arthroscopically or
open. In the setting of PF OA, lateral retinacular
release had mixed results, with worse outcomes
associated with cases of patellar instability [81,
82]. Typically, lateral lengthening is preferred
over a complete release as the latter results in
greater disruption of lateral stabilizing structures
[83]. This can potentially result in iatrogenic
medial patellar instability, especially in cases
with patellar instability to begin with. Although
there are no direct assessments of lengthening on
isolated PF OA, it likely has a role as an adjunct,
especially with tight lateral structures, or lateral
osteophytes (Fig. 1).
Similarly, lateral facetectomy can both
decompress the tight lateral structures and
remove focal lateral facet OA making up the
338
C. S. Frey et al.
P
R
T
Fig. 1 Lateral retinacular lengthening. After developing the plane superficial to the joint capsule, along the
patellar tendon, a 2-cm lateral retinacular lengthening is
performed, with closure of the lateral tissues at the
retinaculum in a lengthened position to rebalance soft
tissue tension while preventing iatrogenic instability. T:
patellar tendon; P: patella; R: lateral retinaculum in
lengthened position
“kissing” osteophytes that may be contributing to
pain [80]. When used to treat PF OA, often with
lateral release, there were modest short term
results with reoperation free survival of 85% at
5 years and 67.2% at 10 years in one study [84].
Another investigation utilizing lateral release
combined with facetectomy for cases of PF OA
with lateral patellar compression had overall
good results with improved Kujala and satisfaction scores at 5 years out, but had similar reoperation rates [80].
measurement variability, as CT scan and MRI
may produce differing measurements, and knee
flexion angle may affect static measurement of the
dynamic nature of axial malalignment [85].
Additionally, rotational malalignment is affected
by femoral version, tibial torsion, tibiofemoral
rotation through the knee joint and other factors
[86]. While TTO is typically used in the setting of
instability, by nature it alters force vectors across
the patellofemoral joint, and thus, can be used to
decrease contact pressures in areas of chondrosis.
This method of relieving PF OA is most relevant
for young, active patients who are not ready for
arthroplasty. It is of less benefit in cases of more
severe or diffuse disease. TTO can be performed
in conjunction with soft tissue stabilization for
patients with concomitant instability.
The classic anteromedialization osteotomy of
Fulkerson is best suited for cases with distal
lateral patellar chondrosis related to maltracking
refractory to conservative management. It helps
realign the extensor mechanism and improve
patellar contact with the trochlea earlier in the arc
of motion. This shifts the contact area more
proximal on the patella [87]. It serves to offload
the joint and provide relief in patients with
malalignment and lateral disease. In carefully
selected patients, results are fairly promising with
good satisfaction and improvements in Kujala
9
Osteotomy
The tibial tubercle osteotomy (TTO) is the
workhorse of bony alignment procedures for
patellofemoral malalignment and can be used to
manipulate contact forces. In patellofemoral OA,
the optimal use of anteromedialization is distal
and lateral OA of the patella. It is less effective
for bipolar OA, medial, proximal and panpatellar
presentations.
Although a TT-TG > 20 mm is often cited as
a threshold for this procedure in patella instability, indications are more nuanced for differing
underlying pathologies and threshold values may
be lower on case-by-case basis (i.e. TTTG > 15 mm). This is partially due to
Patellofemoral Arthritis
scores [88]. However, failure rates are correlated
with severity of arthritis and patients with
arthritis have earlier deterioration of symptoms.
Typically, it is indicated in younger patients
under 50, however, active older patients may also
benefit [89]. There is no consensus on the degree
of correction. Some suggest a goal TT-TG of 10–
15 mm [90]. It is important not to over-medialize
as this may cause increased medial tibiofemoral
contact forces [91].
Pure anteriorization, known as the Maquet
osteotomy, has been shown to decrease patellofemoral joint forces through changing the lever
arm [92]. It unloads the patella without affecting
alignment. This may be useful for medial patella
cartilage lesions for when anteromedialization is
contraindicated [90]. This technique, as originally described, was marred by infection and
dehiscence, and carried the risk of overload of
the superior pole. Direct medialization, often
described as the Roux-Elmslie-Trillat procedure
helps to address lateralized forces that lead to
maltracking. Long term outcomes show around
54%-64% good or excellent results, with worse
outcomes for patellofemoral pain than instability
[93]. It is limited by bony contact needed for
fixation and rarely indicated [90].
The TTO can be augmented with MPFL
reconstruction to aid in patellar tracking and
patellar contact area. This is typically indicated in
cases of concomitant symptomatic instability and
objective laxity remains after TTO. Although the
MPFL cannot be used to “pull” the patella, it
does offer soft tissue stabilization as a restraint to
lateral subluxation with a native tensile strength
of about 209 N [94]. When MPFL and TTO are
combined for indicated cases, the recurrence
rates of instability appear to be quite low, around
4%–6% [95, 96].
Rotational and coronal plane osteotomies are
used to correct for malalignment in the axial
plane malalignment through the tibia and femur,
and while described, have not been extensively
studied in the setting of PF arthritis. In cases of
increased femoral anteversion, a femoral rotational osteotomy can be performed to redistribute
pressure [97]. External derotation of the distal
339
femur can unload the lateral patella, but at the
cost of increasing medial contact pressure. If the
deformity is related to tibial torsion (typically
external rotation of 40°), the corrective rotational
osteotomy may be made through the proximal
tibia [98]. Prior studies have reported improvement in patellofemoral pain and instability in
patients who have failed prior extensor mechanism operations, but have not focused on treatment of PF arthritis. Pathologic genu valgum can
lead to lateralization of force vectors acting
on the patella and can be treated with varus
producing distal femoral osteotomy [99]. It
should be noted that prior reports of femoral
varus producing or derotational osteotomies
have not focused on PF arthritis, and although
severe patellofemoral osteoarthritis is typically
considered a contraindication, mild to moderate
PF OA is not necessarily [99, 100].
10
Cartilage Surgery
Cartilage restoration is a powerful tool for treating symptomatic focal chondral defects in the
setting of preserved joint space; thus, it is not
considered for advanced or diffuse disease. Considering that hyaline cartilage is relatively avascular and hypocellular, its ability for spontaneous
healing is limited [57]. The cartilage-based
interventions can largely be broken down into
palliative (arthroscopic debridement), reparative
(marrow stimulating), or restorative (osteochondral or cartilaginous). Patients must be indicated
carefully to optimize outcome, as it is accepted
that in general, there is a limited role for these
techniques in cases of patellofemoral arthritis.
Osteochondral transfer is a useful tool for
large defects and has been shown to be effective,
even after failed bone marrow stimulation procedures [101]. However, several patient specific
factors are worth consideration. While age and
cause do not appear to have a significant impact,
female gender, increasing size, patellar lesions,
and bipolar lesions seem to be associated with
worse outcomes [102]. Patients should not have
severely diminished range of motion and
340
C. S. Frey et al.
Fig. 2 Bipolar disease of the patellofemoral joint,
focal, treated with bipolar osteochondral allograft. Top
right—large but focal patellar defect; top right—focal
central defect; bottom left—OCA to the patella showing
good contour match with no step-off; bottom right—OCA
to the trochlea showing restoration of trochlear surface
geometry and no step-off
typically recommended not to have end stage
degenerative disease. As previously mentioned,
maltracking and malalignment must be addressed
as well to optimize outcomes.
In general, the results of osteochondral allograft of the patellofemoral joint are positive,
especially considering the lack of donor morbidity. A recent systematic review found significant improvements in IKDC as well as good
10 year survivorship of 77%, similar to femoral
condyle lesions [103]. However, when applied to
bipolar lesions in more severe disease the results
are not quite as promising. One study found
improvements in IKDC function and pain, but a
five year survival of 64% [104]. However,
another found that ultimately, 8 of 11 patients
were able to delay arthroplasty and many grafts
had survivorship over 10 years [105]. At this
time there is limited applicability for patellofemoral arthritis. Arthroplasty is generally the more
reliable option other than in very young and
active patients (Fig. 2).
There are some measures that can be taken
to maximize outcomes. It is preferable to use
grafts from the same location [102]. This
improves surface congruency for smoother gliding. However, as long as the radius of curvature
is similar, femoral grafts are likely to be of useful size [106]. Advanced imaging and sizing
markers can be useful for templating. Another
consideration when using allograft is maintaining chondrocyte viability. It is known that
fresh allograft has better viability than cryopreserved counterparts and that sooner time
implantation is generally better [107, 108]. It is
also interesting to note that impaction can also
lead to cell inviability [109]. The greater the
impaction from tapping, the greater damage
dealt. This is particularly salient for thick, mismatched plugs.
Patellofemoral Arthritis
11
Arthroplasty
For cases of severe, isolated PF OA that has
failed conservative management, patellofemoral
arthroplasty is the most predictable and reliable
treatment [110]. Traditionally, the ideal patient
tended to be older than 50, but under 65, not
excessively active, and not overweight. However, these boundaries continue to evolve. Recent
literature has cited equivalent patient reported
outcomes in obese and non-obese patients [111].
Contraindications include lack of conservative
management, significant degenerative disease in
the tibiofemoral joint, patellar malalignment or
patellar instability, knee mechanical malalignment, inflammatory arthritis, infection, significant loss of ROM [112]. The senior authors now
use PF arthroplasty in those over 40 and the
elderly as they will likely enjoy the more natural
kinematics compared to a TKA.
Patellofemoral arthroplasty is a powerful tool
that offers several advantages over other procedures for end stage disease. First of all, it resurfaces the patellofemoral joint to remove the
arthritic articulation. Through implant position,
moderate degrees of malalignment can be corrected, and properly centralizing the trochlear
groove center effectively decreases TT-TG. Targeted placement of the patellar button can lower
the patella and medialize the central ridge of the
patella to effectively decrease Q-angle. PF
arthroplasty also spares the medial and lateral
compartment as well as cruciate ligaments,
retaining more natural kinematics and proprioception than total knee replacements [113]. PF
arthroplasty may be performed in conjunction
with soft tissue stabilization for patients with
concomitant instability.
Historically, isolated patellofemoral arthroplasty did not compare favorably to total knee
arthroplasty [114]. Revision was required in 1/3
of the patients and patient satisfaction was poor.
At the time, design was limited by deviations
from trochlear anatomy and susceptibility to
maltracking and wear [115]. Second generation
implants were developed with wider trochlear
surfaces contoured to facilitate patellar tracking.
341
Some have lateralized and/or deepened trochlear
grooves to further improve tracking. With more
modern implants, many of these problems have
been corrected and survivorship has improved.
One recent systematic review cited 10 year survivorship of 83.3% and 20 year survivorship of
66.6% [116].
When used for isolated PF OA, patellofemoral
arthroplasty and total knee arthroplasty have
yielded similar results in recent studies. In one
randomized controlled trial, 1-year WOMAC
functional scores was not significantly different
between the two [117]. Moreover, long term
outcomes for Oxford Knee Score (OKS) and EQ5D quality of life scores were not significantly
different. Complications were similar, yielding a
similar number of superficial infections, but more
secondary interventions in the TKA group. This
was replicated in a recent systematic review
[112]. Although patients did well in both groups
with improvements in PROMs after surgery,
patellofemoral arthroplasty patients had better
functional results and physical activity scores
throughout the first two years postoperatively.
Complications and revision rates were in total,
not significantly different. PF arthroplasty has
been associated with lower blood loss, decreased
tourniquet time, and decreased hospital stay
[118]. Some studies have found higher revision
rates than TKA. PFA may be intentionally used
as a bridge to TKA in younger patients, with a
greater likelihood of higher post-op activity
level, greater implant wear, and more rapid progression of arthritis in the tibiofemoral compartments, which would warrant earlier revision.
Exact techniques for PFA vary based on surgeon preference, patient factors, and implant
system, but the general concepts should be
emphasized. A tourniquet can be placed at the
surgeon’s discretion. The typical skin incision
will be longitudinal from the patella down to the
tibial tubercle, carried through the skin and
subcutaneous tissue. Sometimes the patient will
have scars from prior operations that can be
incorporated into the incision. Several approaches to the knee are viable, including medial and
lateral arthrotomies. The senior author, SS,
342
prefers a medial parapatellar arthrotomy. Next, a
limited synovectomy can be performed to
mobilize the patella. Once adequately mobile, the
patella can be prepared and sized. Patellar and
quadriceps tendon attachments can be used as
reference and a minimum of 12–14 mm of
patella should be left after cutting—in younger
patients, the risk of “stuffing” the joint is overridden by the reward of better bone stock if
revision is needed in the distant future. Rotational alignment of the trochlea can be established with an intra- or extra-medullary system to
prepare for femoral cuts. The native trochlea can
be used to determine varus/valgus orientation.
However, if there is dysplasia one can align the
proximal trochlea groove just lateral to the mid
sagittal plane of the femur [110]. When performing the anterior femoral cut, steps should be
taken to ensure that there will be no notching.
The anterior cut should yield a “modified grand
piano” sign. PFA is a resurfacing. The lateral
facet is normally higher than the medial facet,
therefore, PFA orientation may appear neutral
rather than the external rotation. One can use
direct visualization as well as fluoroscopy to
ensure that there is no notching. The rest of the
femur can be prepared and trochlea sized
according to the system used. Implant position
and patellar tracking should be checked with trial
implants. The patella should engage throughout
its entire excursion. After thorough cleansing and
drying, final implants are cemented in place.
Following final implantation, if there is maltracking, instability, or lateral retinaculum tightness, these can be addressed at this time (Fig. 3).
There are several complications that can result
from incorrect procedural technique. For example, component malpositioning in the sagittal,
coronal, and/or axial planes can lead to maltracking and instability [119]. Excessive external
rotation has been associated with subluxation
while internal rotation leads to impingement.
Patellar fracture has also been known to occur,
up to rates of 9% in some cases [120]. Risk
C. S. Frey et al.
factors for this include low BMI, larger resections, thinner patellas, and large trochlear components. Sometimes, the procedure may be
executed well, but the patient may just have
progression of disease due to activity level,
genetics, or other factors. Notching has the
potential to yield stress concentration and possibly fracture, similarly to TKA. Though not a
“complication”, it is important to have a thorough discussion with those patients who have a
remote history of patellar instability. In the more
recent years, the instability has resolved secondary to the high coefficient of friction (CoF) of
PFA implants and soft tissue contractures associated with OA. With low CoF PFA, the old,
contracted scar of prior MPFL tearing may progressively loosen and lead to functional subluxation or rarer, dislocation. While this is easily
addressed with MPFL reconstruction, a preoperative discussion is important for patient trust
and satisfaction. Alternatively, an MPFL reconstruction may be performed at the index PFA.
However, if the patella is stable intra-operatively,
the risk/reward ratio supports only performing
the PFA to avoid problems with ROM with the
“prophylactic” addition of MPFLR as only a
subset will develop this instability.
Procedure
Indications
Outcomes
Palliative
Arthroscopy
Mechanical
symptoms,
diagnostic workup,
loose body, unstable
chondral lesion
Short term
symptomatic
relief of
mechanical
symptoms
Lateral
Lengthening/Lateral
Facetectomy
Lateral tightness
Short to medium
term pain relief in
select patients
Tibial Tubercle
Osteotomy
Malalignment, lateral
wear pattern,
young/active, mild
disease
Short to medium
term
improvement in
select patients
Patellofemoral
Arthroplasty
Isolated
patellofemoral
degenerative disease
and pain
Good medium to
long term results
in select patients
Total Knee
Arthroplasty
Multicompartmental
degenerative disease
and pain
Good long term
results
Patellofemoral Arthritis
Fig. 3 Intraoperative photographs of patellofemoral
arthroplasty, through a medial parapatellar arthrotomy. Top—diffuse chondrosis of the patella and
12
Conclusion
PF OA is a degenerative condition resulting from
multiple etiologies. It is largely a clinical diagnosis confirmed with imaging. Treatment
343
trochlea. Bottom—final placement of patellar and femoral
trochlea components.
consists of initial nonoperative modalities such as
therapy, oral medications and injections. For
refractory cases, operative management should
be customized to each patient’s presentation,
demands, mechanics and pathology. Orthopaedic
surgeons have multiple tools at their disposal to
344
treat this including palliative, reparative, and
restorative treatments of cartilage, bony and soft
tissue methods of correcting alignment and
patellar loading, as well as arthroplasty.
References
1. Pereira D, Peleteiro B, Araújo J, Branco J, Santos RA, Ramos E. The effect of osteoarthritis
definition on prevalence and incidence estimates: a
systematic review. Osteoarthritis Cartilage. 2011;19
(11):1270–85.
2. Kobayashi S, Pappas E, Fransen M, Refshauge K,
Simic M. The prevalence of patellofemoral
osteoarthritis: a systematic review and meta-analysis.
Osteoarthritis Cartilage. 2016;24(10):1697–707.
3. Walker T, Perkinson B, Mihalko WM. Patellofemoral arthroplasty: the other unicompartmental
knee replacement. J Bone Joint Surg Am. 2012;94
(18):1712–20.
4. Coburn SL, Barton CJ, Filbay SR, Hart HF,
Rathleff MS, Crossley KM. Quality of life in
individuals with patellofemoral pain: a systematic
review including meta-analysis. Phys Ther Sport.
2018;33:96–108.
5. Chawla H, Nwachukwu BU, van der List JP,
Eggman AA, Pearle AD, Ghomrawi HM. Cost
effectiveness of patellofemoral versus total knee
arthroplasty in younger patients. Bone Joint J.
2017;99-B(8):1028–1036.
6. Murphy LB, Cisternas MG, Pasta DJ, Helmick CG,
Yelin EH. Medical expenditures and earnings losses
among US adults with arthritis in 2013. Arthritis
Care Res. 2018;70(6):869–76.
7. Bieleman HJ, Oosterveld FGJ, Oostveen JCM,
Reneman MF, Groothoff JW. Work participation
and health status in early osteoarthritis of the hip
and/or knee: a comparison between the Cohort Hip
and Cohort Knee and the Osteoarthritis Initiative.
Arthritis Care Res. 2010;62(5):683–9.
8. Sharif B, Garner R, Sanmartin C, Flanagan WM,
Hennessy D, Marshall DA. Risk of work loss due to
illness or disability in patients with osteoarthritis: a
population-based cohort study. Rheumatology.
2016;55(5):861–8.
9. Hubertsson J, Petersson IF, Thorstensson CA,
Englund M. Risk of sick leave and disability
pension in working-age women and men with knee
osteoarthritis. Ann Rheum Dis. 2013;72(3):401–5.
10. Grelsamer RP, Proctor CS, Bazos AN. Evaluation
of patellar shape in the sagittal plane. A clinical
analysis. Am J Sports Med. 1994;22(1):61–66.
11. Sherman SL, Plackis AC, Nuelle CW. Patellofemoral anatomy and biomechanics. Clin Sports Med.
2014;33(3):389–401.
C. S. Frey et al.
12. Huberti HH, Hayes WC. Patellofemoral contact
pressures. The influence of q-angle and tendofemoral contact. J Bone Joint Surg Am. 1984;66
(5):715–724.
13. Loudon JK. Biomechanics and pathomechanics of
the patellofemoral joint. Int J Sports Phys Ther.
2016;11(6):820–30.
14. Tanaka MJ, Chahla J, Farr J 2nd, et al. Recognition
of evolving medial patellofemoral anatomy provides insight for reconstruction. Knee Surg Sports
Traumatol Arthrosc. 2019;27(8):2537–50.
15. Aglietti P, Insall JN, Cerulli G. Patellar pain and
incongruence. I: Measurements of incongruence.
Clin Orthop Relat Res. 1983;(176):217–224.
16. Hungerford DS, Barry M. Biomechanics of the
patellofemoral joint. Clin Orthop Relat Res.
1979;144:9–15.
17. White BJ, Sherman OH. Patellofemoral instability.
Bull NYU Hosp Jt Dis. 2009;67(1):22–9.
18. Grelsamer RP, Dejour D, Gould J. The pathophysiology of patellofemoral arthritis. Orthop Clin North
Am. 2008;39(3):269–274, v.
19. Nomura E, Inoue M, Kurimura M. Chondral and
osteochondral injuries associated with acute patellar
dislocation. Arthroscopy. 2003;19(7):717–21.
20. Vollnberg B, Koehlitz T, Jung T, et al. Prevalence
of cartilage lesions and early osteoarthritis in
patients with patellar dislocation. Eur Radiol.
2012;22(11):2347–56.
21. Anderson DD, Marsh JL, Brown TD. The pathomechanical etiology of post-traumatic osteoarthritis
following intraarticular fractures. Iowa Orthop
J. 2011;31:1–20.
22. Honkonen SE. Degenerative arthritis after tibial
plateau fractures. J Orthop Trauma. 1995;9(4):273–7.
23. Milentijevic D, Rubel IF, Liew AS, Helfet DL,
Torzilli PA. An in vivo rabbit model for cartilage
trauma: a preliminary study of the influence of
impact stress magnitude on chondrocyte death and
matrix damage. J Orthop Trauma. 2005;19
(7):466–73.
24. Huang W, Ong TY, Fu SC, Yung SH. Prevalence of
patellofemoral joint osteoarthritis after anterior
cruciate ligament injury and associated risk factors:
a systematic review. J Orthop Translat. 2020;22:14–
25.
25. Culvenor AG, Cook JL, Collins NJ, Crossley KM.
Is patellofemoral joint osteoarthritis an underrecognised outcome of anterior cruciate ligament
reconstruction? A narrative literature review. Br J
Sports Med. 2013;47(2):66–70.
26. Peters TA, McLean ID. Osteochondritis dissecans
of the patellofemoral joint. Am J Sports Med.
2000;28(1):63–7.
27. Hevesi M, Sanders TL, Pareek A, et al. Osteochondritis Dissecans in the knee of skeletally immature
patients: rates of persistent pain, osteoarthritis, and
arthroplasty at mean 14-years’ follow-up. Cartilage.
2020;11(3):291–9.
Patellofemoral Arthritis
28. Spector TD, MacGregor AJ. Risk factors for
osteoarthritis: genetics. Osteoarthritis Cartilage.
2004;12 Suppl A:S39–S44.
29. Bongers EMHF, van Kampen A, van Bokhoven H,
Knoers NVAM. Human syndromes with congenital
patellar anomalies and the underlying gene defects.
Clin Genet. 2005;68(4):302–19.
30. Karuppal R. Current concepts in the articular
cartilage repair and regeneration. J Orthop.
2017;14(2):A1–3.
31. Pihl K, Turkiewicz A, Englund M, et al. Association of specific meniscal pathologies and other
structural pathologies with self-reported mechanical
symptoms: a cross-sectional study of 566 patients
undergoing meniscal surgery. J Sci Med Sport.
2019;22(2):151–7.
32. Crossley KM, Schache AG, Ozturk H, Lentzos J,
Munanto M, Pandy MG. Pelvic and hip kinematics
during walking in people with patellofemoral joint
osteoarthritis compared to healthy age-matched
controls. Arthritis Care Res. 2018;70(2):309–14.
33. Trasolini NA, Serino J, Dandu N, Yanke AB.
Treatment of proximal trochlear dysplasia in the
setting of patellar instability: an arthroscopic technique. Arthrosc Tech. 2021;10(10):e2253–8.
34. Leslie IJ, Bentley G. Arthroscopy in the diagnosis
of chondromalacia patellae. Ann Rheum Dis.
1978;37(6):540–7.
35. Hart HF, Ackland DC, Pandy MG, Crossley KM.
Quadriceps volumes are reduced in people with
patellofemoral joint osteoarthritis. Osteoarthritis
Cartilage. 2012;20(8):863–8.
36. Haim A, Yaniv M, Dekel S, Amir H. Patellofemoral
pain syndrome: validity of clinical and radiological
features. Clin Orthop Relat Res. 2006;451:223–8.
37. Merchant AC, Fraiser R, Dragoo J, Fredericson M.
A reliable Q angle measurement using a standardized protocol. Knee. 2020;27(3):934–9.
38. Iwano T, Kurosawa H, Tokuyama H, Hoshikawa Y.
Roentgenographic and clinical findings of patellofemoral osteoarthrosis. With special reference to its
relationship to femorotibial osteoarthrosis and etiologic factors. Clin Orthop Relat Res. 1990;
(252):190–197.
39. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol
Arthrosc. 1994;2(1):19–26.
40. Merchant AC, Mercer RL, Jacobsen RH, Cool CR.
Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974;56
(7):1391–6.
41. Laurin CA, Lévesque HP, Dussault R, Labelle H,
Peides JP. The abnormal lateral patellofemoral
angle: a diagnostic roentgenographic sign of recurrent patellar subluxation. J Bone Joint Surg Am.
1978;60(1):55–60.
42. Damgacı L, Özer H, Duran S. Patella-patellar
tendon angle and lateral patella-tilt angle decrease
345
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
patients with chondromalacia patella. Knee Surg
Sports Traumatol Arthrosc. 2020;28(8):2715–21.
Rueckl K, Boettner F, Maza N, Runer A, Bechler U,
Sculco P. The posterior-anterior flexed view is
better than the anterior-posterior view for assessing
osteoarthritis of the knee. Skeletal Radiol. 2018;47
(4):511–7.
Heng HYC, Bin Abd Razak HR, Mitra AK.
Radiographic grading of the patellofemoral joint is
more accurate in skyline compared to lateral views.
Ann Transl Med. 2015;3(18):263.
Stefanik JJ, Zhu Y, Zumwalt AC, et al. Association
between patella alta and the prevalence and worsening of structural features of patellofemoral joint
osteoarthritis: the multicenter osteoarthritis study.
Arthritis Care Res. 2010;62(9):1258–65.
Ward SR, Terk MR, Powers CM. Patella alta:
association with patellofemoral alignment and
changes in contact area during weight-bearing.
J Bone Joint Surg Am. 2007;89(8):1749–55.
Magnussen RA, De Simone V, Lustig S, Neyret P,
Flanigan DC. Treatment of patella alta in patients
with episodic patellar dislocation: a systematic
review. Knee Surg Sports Traumatol Arthrosc.
2014;22(10):2545–50.
Perelli S, Ibañez M, Morales-Marin C, et al. Patellar
tendon lengthening: rescue procedure for patella
baja. Arthrosc Tech. 2020;9(1):e1–8.
Verhulst FV, van Sambeeck JDP, Olthuis GS, van
der Ree J, Koëter S. Patellar height measurements:
Insall-Salvati ratio is most reliable method. Knee
Surg Sports Traumatol Arthrosc. 2020;28(3):869–
75.
Anagnostakos K, Lorbach O, Reiter S, Kohn D.
Comparison of five patellar height measurement
methods in 90° knee flexion. Int Orthop. 2011;35
(12):1791–7.
Pennock AT, Alam M, Bastrom T. Variation in
tibial tubercle-trochlear groove measurement as a
function of age, sex, size, and patellar instability.
Am J Sports Med. 2014;42(2):389–93.
Gomoll AH, Madry H, Knutsen G, et al. The
subchondral bone in articular cartilage repair:
current problems in the surgical management. Knee
Surg Sports Traumatol Arthrosc. 2010;18(4):434–
47.
Vallotton JA, Meuli RA, Leyvraz PF, Landry M.
Comparison between magnetic resonance imaging
and arthroscopy in the diagnosis of patellar cartilage
lesions: a prospective study. Knee Surg Sports
Traumatol Arthrosc. 1995;3(3):157–62.
Schaefer FKW, Kurz B, Schaefer PJ, et al. Accuracy and precision in the detection of articular
cartilage lesions using magnetic resonance imaging
at 1.5 Tesla in an in vitro study with orthopedic and
histopathologic correlation. Acta radiol. 2007;48
(10):1131–1137.
Starr AM, Wessely MA, Albastaki U, Pierre-Jerome
C, Kettner NW. Bone marrow edema:
346
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
C. S. Frey et al.
pathophysiology, differential diagnosis, and imaging. Acta radiol. 2008;49(7):771–86.
Azer NM, Winalski CS, Minas T. MR imaging for
surgical planning and postoperative assessment in
early osteoarthritis. Radiol Clin North Am. 2004;42
(1):43–60.
Merkely G, Hinckel BB, Shah N, Small KM,
Lattermann C. Magnetic resonance imaging of the
patellofemoral articular cartilage. In: Dejour D,
Zaffagnini S, Arendt EA, Sillanpää P, Dirisamer F,
editors. Patellofemoral Pain, Instability, and Arthritis: Clinical Presentation, Imaging, and Treatment.
Springer: Berlin Heidelberg; 2020. p. 47–61.
Camp CL, Stuart MJ, Krych AJ, et al. CT and MRI
measurements of tibial tubercle-trochlear groove
distances are not equivalent in patients with patellar
instability. Am J Sports Med. 2013;41(8):1835–40.
Arden NK, Perry TA, Bannuru RR, et al. Nonsurgical management of knee osteoarthritis: comparison of ESCEO and OARSI 2019 guidelines. Nat
Rev Rheumatol. 2021;17(1):59–66.
American Academy of Orthopaedic Surgeons Management of Osteoarthritis of the Knee (NonArthroplasty) Evidence-Based Clinical Practice
Guideline; 2021. https://www.aaos.org/oak3cpg.
Chevidikunnan MF, Al Saif A, Gaowgzeh RA,
Mamdouh KA. Effectiveness of core muscle
strengthening for improving pain and dynamic
balance among female patients with patellofemoral
pain syndrome. J Phys Therapy Sci. 2016;28
(5):1518–23.
Ferber R, Bolgla L, Earl-Boehm JE, Emery C,
Hamstra-Wright K. Strengthening of the hip and
core versus knee muscles for the treatment of
patellofemoral pain: a multicenter randomized controlled trial. J Athl Train. 2015;50(4):366–77.
Crossley KM, Marino GP, Macilquham MD,
Schache AG, Hinman RS. Can patellar tape reduce
the patellar malalignment and pain associated with
patellofemoral osteoarthritis? Arthritis Rheum.
2009;61(12):1719–25.
Cushnaghan J, McCarthy C, Dieppe P. Taping the
patella medially: a new treatment for osteoarthritis
of the knee joint? BMJ. 1994;308(6931):753–5.
Callaghan MJ, Parkes MJ, Hutchinson CE, et al.
A randomised trial of a brace for patellofemoral
osteoarthritis targeting knee pain and bone marrow
lesions. Ann Rheum Dis. 2015;74(6):1164–70.
Powers CM, Ward SR, Chen YJ, der Chan L,
Terk MR. The effect of bracing on patellofemoral
joint stress during free and fast walking. Am J
Sports Med. 2004;32(1):224–31.
Powers CM, Ward SR, Chen YJ, Chan LD,
Terk MR. Effect of bracing on patellofemoral joint
stress while ascending and descending stairs. Clin J
Sport Med. 2004;14(4):206–14.
Hunter DJ, Harvey W, Gross KD, et al. A randomized trial of patellofemoral bracing for treatment of
patellofemoral osteoarthritis. Osteoarthritis Cartilage. 2011;19(7):792–800.
69. Bruyère O, Honvo G, Veronese N, et al. An updated
algorithm recommendation for the management of
knee osteoarthritis from the European society for
clinical and economic aspects of osteoporosis,
osteoarthritis and musculoskeletal diseases (ESCEO).
Semin Arthritis Rheum. 2019;49(3):337–50.
70. Koh IJ, Kim MS, Sohn S, Song KY, Choi NY, In Y.
Duloxetine reduces pain and improves quality of
recovery following total knee arthroplasty in centrally sensitized patients: a prospective, randomized
controlled study. J Bone Joint Surg Am. 2019;101
(1):64–73.
71. Skljarevski V, Zhang S, Iyengar S, et al. Efficacy of
duloxetine in patients with chronic pain conditions.
Curr Drug ther. 2011;6(4):296–303.
72. Nuelle CW, Cook CR, Stoker AM, Cook JL,
Sherman SL. In Vivo Toxicity of local anesthetics
and corticosteroids on supraspinatus tenocyte cell
viability and metabolism. Iowa Orthop J.
2018;38:107–12.
73. Sherman SL, Khazai RS, James CH, Stoker AM,
Flood DL, Cook JL. In vitro toxicity of local
anesthetics and corticosteroids on chondrocyte and
synoviocyte viability and metabolism. Cartilage.
2015;6(4):233–40.
74. Altman RD, Manjoo A, Fierlinger A, Niazi F,
Nicholls M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: a
systematic review. BMC Musculoskelet Disord.
2015;16:321.
75. Clarke S, Lock V, Duddy J, Sharif M, Newman JH,
Kirwan JR. Intra-articular hylan G-F 20 (Synvisc) in
the management of patellofemoral osteoarthritis of
the knee (POAK). Knee. 2005;12(1):57–62.
76. Jayaram P, Liu C, Dawson B, et al. Leukocytedependent effects of platelet-rich plasma on cartilage loss and thermal hyperalgesia in a mouse
model of post-traumatic osteoarthritis. Osteoarthritis
Cartilage. 2020;28(10):1385–93.
77. Riboh JC, Saltzman BM, Yanke AB, Fortier L,
Cole BJ. Effect of leukocyte concentration on the
efficacy of platelet-rich plasma in the treatment of
knee osteoarthritis. Am J Sports Med. 2016;44
(3):792–800.
78. Raeissadat SA, Ghorbani E, Sanei Taheri M, et al.
MRI changes after platelet rich plasma injection in
knee osteoarthritis (Randomized Clinical Trial).
J Pain Res. 2020;13:65–73.
79. Tetteh ES, Bajaj S, Ghodadra NS. Basic science and
surgical treatment options for articular cartilage
injuries of the knee. J Orthop Sports Phys Ther.
2012;42(3):243–53.
80. Paulos LE, O’Connor DL, Karistinos A. Partial
lateral patellar facetectomy for treatment of arthritis
due to lateral patellar compression syndrome.
Arthroscopy. 2008;24(5):547–53.
81. Aderinto J, Cobb AG. Lateral release for patellofemoral arthritis. Arthroscopy. 2002;18(4):399–403.
82. Christensen F, Søballe K, Snerum L. Treatment of
chondromalacia patellae by lateral retinacular
Patellofemoral Arthritis
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
release of the patella. Clin Orthop Relat Res.
1988;234:145–7.
Unal B, Hinckel BB, Sherman SL, Lattermann C.
Comparison of lateral retinaculum release and
lengthening in the treatment of patellofemoral
disorders. Am J Orthop. 2017;46(5):224–8.
Wetzels T, Bellemans J. Patellofemoral osteoarthritis treated by partial lateral facetectomy: results at
long-term follow up. Knee. 2012;19(4):411–5.
Tan SHS, Lim BY, Chng KSJ, et al. The difference
between computed tomography and magnetic resonance imaging measurements of Tibial tubercletrochlear groove distance for patients with or without
patellofemoral instability: a systematic review and
meta-analysis. J Knee Surg. 2020;33(8):768–76.
Lin KM, James EW, Aitchison AH, Schlichte LM,
Wang G, Green DW. Increased tibiofemoral rotation on MRI with increasing clinical severity of
patellar instability. Knee Surg Sports Traumatol
Arthrosc. 2021;29(11):3735–42.
Fulkerson JP. Diagnosis and treatment of patients
with patellofemoral pain. Am J Sports Med.
2002;30(3):447–56.
Rosso F, Rossi R, Governale G, et al. Tibial
Tuberosity Anteromedialization for patellofemoral
chondral disease: prognostic factors. Am J Sports
Med. 2017;45(7):1589–98.
Carofino BC, Fulkerson JP. Anteromedialization of
the tibial tubercle for patellofemoral arthritis in
patients >50 years. J Knee Surg. 2008;21(2):101–5.
Gardner EC, Molho DA, Fulkerson JP. Coronal
Malalignment-when and how to perform a Tibial
tubercle osteotomy. Clin Sports Med. 2022;41
(1):15–26.
Kuroda R, Kambic H, Valdevit A, Andrish JT.
Articular cartilage contact pressure after tibial
tuberosity transfer. A cadaveric study. Am J Sports
Med. 2001;29(4):403–409.
Ferguson AB Jr, Brown TD, Fu FH, Rutkowski R.
Relief of patellofemoral contact stress by anterior
displacement of the tibial tubercle. J Bone Joint
Surg Am. 1979;61(2):159–66.
Grimm NL, Lazarides AL, Amendola A. Tibial
tubercle osteotomies: a review of a treatment for
recurrent patellar instability. Curr Rev Musculoskelet Med. 2018;11(2):266–71.
Amis AA, Firer P, Mountney J, Senavongse W,
Thomas NP. Anatomy and biomechanics of the
medial patellofemoral ligament. Knee. 2003;10
(3):215–20.
Hadley CJ, Tucker BS, Lombardi NJ, et al. Combined MPFL reconstruction and tibial tubercle
osteotomy for patellar instability: a retrospective
review of 23 patients. J Orthop. 2021;28:49–52.
Su P, Liu X, Jian N, Li J, Fu W. Clinical outcomes
and predictive factors for failure with MPFL
reconstruction combined with tibial tubercle osteotomy and lateral retinacular release for recurrent
patellar instability. BMC Musculoskelet Disord.
2021;22(1):632.
347
97. Liska F, von Deimling C, Otto A, et al. Distal
femoral torsional osteotomy increases the contact
pressure of the medial patellofemoral joint in
biomechanical analysis. Knee Surg Sports Traumatol Arthrosc. 2019;27(7):2328–33.
98. Fouilleron N, Marchetti E, Autissier G, Gougeon F,
Migaud H, Girard J. Proximal tibial derotation
osteotomy for torsional tibial deformities generating
patello-femoral disorders. Orthop Traumatol Surg
Res. 2010;96(7):785–92.
99. Sherman SL, Thompson SF, Clohisy JCF. Distal
femoral varus osteotomy for the management of
valgus deformity of the knee. J Am Acad Orthop
Surg. 2018;26(9):313–24.
100. Barnavon T, Odri GA, Vendeuvre T, et al. Medial
closing-wedge distal femoral varus osteotomy:
symptoms and functional impact in cases of associated patellofemoral osteoarthritis. A two-year
follow-up prospective pilot study. Knee. 2020;27
(3):615–623.
101. Riff AJ, Huddleston HP, Cole BJ, Yanke AB.
Autologous chondrocyte implantation and osteochondral allograft transplantation render comparable outcomes in the setting of failed marrow
stimulation. Am J Sports Med. 2020;48(4):861–70.
102. Chahla J, Hinckel BB, Yanke AB, et al. An expert
consensus statement on the management of large
chondral and osteochondral defects in the patellofemoral joint. Orthop J Sports Med. 2020;8
(3):2325967120907343.
103. Chahla J, Sweet MC, Okoroha KR, et al. Osteochondral allograft transplantation in the patellofemoral joint: a systematic review. Am J Sports Med.
2019;47(12):3009–18.
104. Meric G, Gracitelli GC, Görtz S, De Young AJ,
Bugbee WD. Fresh osteochondral allograft transplantation for bipolar reciprocal osteochondral
lesions of the knee. Am J Sports Med. 2015;43
(3):709–14.
105. Spak RT, Teitge RA. Fresh osteochondral allografts
for patellofemoral arthritis: long-term followup. Clin
Orthop Relat Res. 2006;444:193.
106. Du PZ, Markolf KL, Levine BD, McAllister DR,
Jones KJ. Differences in the radius of curvature
between femoral condyles: implications for osteochondral allograft matching. J Bone Joint Surg Am.
2018;100(15):1326–31.
107. Jomha NM, Lavoie G, Muldrew K, Schachar NS,
McGann LE. Cryopreservation of intact human
articular cartilage. J Orthop Res. 2002;20(6):1253–5.
108. Williams SK, Amiel D, Ball ST, et al. Prolonged
storage effects on the articular cartilage of fresh
human osteochondral allografts. J Bone Joint Surg
Am. 2003;85(11):2111–20.
109. Walczak BE, Nies MS, Trask DJ, et al. Osteochondral graft size is significantly associated with
increased force and decreased chondrocyte viability.
Am J Sports Med. 2018;46(3):623–31.
110. Farr J 2nd, Barrett D. Optimizing patellofemoral
arthroplasty. Knee. 2008;15(5):339–47.
348
111. Tishelman JC, Pyne A, Kahlenberg CA,
Gruskay JA, Strickland SM. Obesity does not affect
patient-reported outcomes following patellofemoral
arthroplasty. J Knee Surg. 2022;35(3):312–6.
112. Peng G, Liu M, Guan Z, et al. Patellofemoral
arthroplasty versus total knee arthroplasty for
isolated patellofemoral osteoarthritis: a systematic
review and meta-analysis. J Orthop Surg Res.
2021;16(1):264.
113. Vandenneucker H, Labey L, Vander Sloten J, Desloovere K, Bellemans J. Isolated patellofemoral
arthroplasty reproduces natural patellofemoral joint
kinematics when the patella is resurfaced. Knee Surg
Sports Traumatol Arthrosc. 2016;24(11):3668–77.
114. Blazina ME, Fox JM, Del Pizzo W, Broukhim B,
Ivey FM. Patellofemoral replacement. Clin Orthop
Relat Res. 1979;144:98–102.
115. Strickland SM, Bird ML, Christ AB. Advances in
patellofemoral arthroplasty. Curr Rev Musculoskelet Med. 2018;11(2):221–30.
C. S. Frey et al.
116. van der List JP, Chawla H, Zuiderbaan HA,
Pearle AD. Survivorship and functional outcomes
of patellofemoral arthroplasty: a systematic review.
Knee Surg Sports Traumatol Arthrosc. 2017;25
(8):2622–31.
117. Joseph MN, Achten J, Parsons NR, Costa ML, PAT
Trial Collaborators. The PAT randomized clinical
trial. Bone Joint J. 2020;102-B(3):310–318.
118. Dahm DL, Al-Rayashi W, Dajani K, Shah JP,
Levy BA, Stuart MJ. Patellofemoral arthroplasty
versus total knee arthroplasty in patients with
isolated patellofemoral osteoarthritis. Am J
Orthop. 2010;39(10):487–91.
119. Mofidi A, Veravalli K, Jinnah RH, Poehling GG.
Association and impact of patellofemoral dysplasia
on patellofemoral arthropathy and arthroplasty.
Knee. 2014;21(2):509–13.
120. King AH, Engasser WM, Sousa PL, Arendt EA,
Dahm DL. Patellar fracture following patellofemoral
arthroplasty. J Arthroplasty. 2015;30(7):1203–6.
Fresh Osteochondral Allografts
in Patellofemoral Surgery
Suhas P. Dasari, Enzo S. Mameri,
Bhargavi Maheshwer, Safa Gursoy,
Jorge Chahla, and William Bugbee
1
Introduction
Patellofemoral chondral lesions of the knee are a
particularly challenging subset of chondral
lesions to manage. In addition to difficulties
related to physiological healing, anatomical and
biomechanical derangements that are unique to
the patellofemoral joint must also be addressed
[1]. The morphology of the patella and trochlea
between patients is widely variable, making each
procedure intrinsically challenging for any
operative technique [2]. Biomechanically, the
anterior compartment of the knee experiences
very high loads during daily function that can
exacerbate symptoms and impair healing processes. Concomitant abnormalities, such as
coronal and rotational limb malalignment, patellofemoral maltracking, patella alta, excessive
lateral tilt, and trochlear dysplasia can all contribute to the challenge of managing patellofemoral chondral lesions and must be adequately
addressed to ensure a satisfactory clinical outcome [1].
S. P. Dasari E. S. Mameri B. Maheshwer
S. Gursoy J. Chahla (&)
Department of Orthopaedic Surgery, Rush
University Medical Center, Chicago, IL, USA
e-mail: Jorge.chahla@rushortho.com
Despite their difficult nature, these lesions are
not rare occurrences, and the optimal management of these defects must be understood
when implementing a joint-preserving procedure.
Among patients undergoing knee arthroscopy, a
study by Widuchowski et al. examined 25,124
patients and reported 60% of them had chondral
lesions of the knee with patellar lesions being the
most common [3]. Furthermore, a recent 2017
meta-analysis by Hart et al. demonstrated that up
to 52% of patients with knee pain are diagnosed
with cartilage lesions in the patellofemoral joint
[4]. Thus, the relative incidence of these debilitating lesions, the complex biomechanical environment, and high stress forces experienced in
the PFJ make it critical for surgeons to understand the anatomy, biomechanics, pathophysiology, and treatment modalities available for
appropriately addressing osteochondral lesions of
the PFJ.
The purpose of this chapter is to describe the
key anatomical and biomechanical principles,
pathophysiology, basic science principles,
advantages and disadvantages, indications and
contraindications, operative planning, surgical
techniques, and clinical outcomes of patellofemoral chondral lesions managed with a fresh
osteochondral allograft (OCA) technique.
W. Bugbee
Department of Orthopaedic Surgery, Scripps Clinic,
La Jolla, CA, USA
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_24
349
350
2
S. P. Dasari et al.
Anatomical and Biomechanical
Considerations
Articular cartilage in the PFJ is the thickest in the
human body and is up to 7.5 mm thick on the
patella [5]. The proximal posterior surface of the
patella is covered by thick hyaline articular cartilage and has a midline ridge that is congruous
with the femoral trochlear groove, while the
distal aspect of the patella’s posterior surface is
nonarticulating [6]. The patellar bone is composed of two major articular facets and several
subfacets that vary considerably from patient to
patient. The facets are broadly classified by the
Wiberg scheme into 3 different groups [7, 8].
A type 1 patella will have concave medial and
lateral facets that are approximately equal in size;
this is the rarest phenotype. Type 2 facets will
have a flat or convex medial facet that is much
smaller in size than the lateral facet; this is the
most common subtype in the general population.
A type 3 patella will have a convex medial facet
that is only slightly smaller than the lateral facet
and accounts for 25% of patellae.
The femoral trochlea articulates with the
patella to form the patellofemoral joint. It is a
5.5 mm deep groove in the distal aspect of the
femur that is lined with articular cartilage [6]. It
has a larger lateral facet that extends more
proximally and anteriorly relative to its smaller
medial facet [6]. The articular cartilage at the
body of the trochlea has an average depth of
4 mm [9]. The remainder of the trochlea has a 2
to 3 mm thick cartilage cap that is thinner
medially [6]. The trochlea plays a critical role in
PFJ biomechanics as it provides a lateral buttress
to prevent subluxation of the patella during knee
flexion [7, 8, 10]. It also facilitates painless,
friction-free articulation over a full range of
motion in healthy knees.
Biomechanical forces, contact area, and contact pressure at the PFJ change with varying
degrees of knee flexion. During knee range of
motion, the greatest forces are experienced
between 60° to 90° of flexion [11]. These forces
move proximally along the patella as the angle of
knee flexion increases [11]. Contact area also
reaches a maximum at 90° of flexion, at which
point the proximal patella will come into contact
with the trochlea [6]. Beyond 90° of flexion, the
contact area decreases [6]. Contact pressure is
defined by the ratio of force across the joint and
contact area at a given angle of knee flexion.
Because force increases at a rate that is greater
than the increase in contact area during knee
flexion, the maximum compressive pressures will
occur between 60° to 90° of knee flexion [11].
Clinically, this manifests with patients describing
anterior knee pain during flexion related activities though they can also complain of intermittent
sharp pain if their lesion is unstable. This
increased strain at the PFJ was quantified in a
study by Flynn and Soutas-Little [12]. The
authors demonstrated that the patellofemoral
joint (PFJ) experienced 1.3 times body weight
(BW) while ambulating, 3.3 times BW when
climbing stairs, and 5.6 times BW when running
due to strain associated with increased flexion
angles.
3
Pathophysiology
The pathophysiology of chondral lesions within
the PFJ is multifactorial. Lesions develop from
traumatic or instability events as well as secondary injuries in the setting of aberrant joint
loading [6]. More specifically, common mechanisms that contribute to injury include chronic
repetitive microtrauma from suboptimal extensor
mechanism alignment and acute microtrauma
[13]. Maltracking of the patella can be caused by
a number of conditions and leads to an altered
distribution of pressure, can cause chronic
repetitive stress, and/or contribute to treatment
failures [14]. Increased lateral patellar maltracking, a greatly increased Q angle (or tibial
tuberosity-trochlear groove [TT-TG] index),
abnormal femoral torsion, trochlear dysplasia,
and patellar instability all contribute to abnormal
contact pressures in the PFJ [14, 15]. An acute
dislocation frequently damages the medial soft
tissue constraints and predisposes the patient to
further episodic patellar dislocations, which
Fresh Osteochondral Allografts in Patellofemoral Surgery
eventually lead to chondral damage in the vast
majority of patients [5]. Furthermore, acute
injuries can occur in up to 95% of dislocation
events and lead to osteochondral or chondral
fractures and fissures that occur either at the time
of the injury/dislocation or during the reduction
[5]. Subsequent ongoing chondral damage occurs
via chondroptosis, which is a chondrocyte
specific apoptotic pathway, and via degradation
of the extracellular matrix due to elevated matrix
metalloproteinase expression [5].
Chronic patellar instability is associated with
underlying trochlear dysplasia, increased Q
angles, insufficient medial stabilization, and
increased TT-TG distances [16]. Patellar maltracking is defined as instances where the patella
fails to engage or subsequently disengages from
the trochlear groove [17]. The medial patellofemoral ligament (MPFL), the lateral trochlea, and
the deep sulcus work in a synergistic effect to
maintain normal patellar tracking during the full
range of knee motion [16]. The MPFL is the
primary restraint during the first 70° of knee
flexion; however, the trochlea serves as the primary restraint for the remainder of knee flexion.
Deficiency in either mechanism can lead to
chronic patellar instability, and trochlear dysplasia has been reported to be present in 85% of
patients with recurrent lateral patellar instability
[18]. Joint instability has demonstrated increased
in-vitro peak contact stresses and has correlated
with cartilage degeneration in an animal model
[5, 19, 20]. Furthermore, a study by Jungmann
et al. has reported an association between trochlear dysplasia and severe patellofemoral joint
degradation [21]. This is reflected by the results
of a separate study by Noehren et al., where the
authors identified common risk factors of patellar
instability like trochlear dysplasia, patella alta,
and increased TT-TG distance and reported the
correlation between these risk factors and
advanced early onset degenerative disease in
young patient populations [22].
When addressing PFJ pathology, trochlear
morphology is critical to surgical planning.
A systematic review by Cregar et al. demonstrated that MPFL reconstruction, while effective
in patellar instability cases, was at an increased
351
risk to fail in cases with high grade trochlear
dysplasia [23]. Furthermore, a shallow, dysplastic trochlear groove creates a knee with instability that is comparable to a knee with an
incompetent MPFL. A dysplastic trochlea is
defined as a trochlea with a sulcus angle greater
than 145° on sunrise views of a knee flexed at
30° [17]. The Dejour classification is used to
grade the level of trochlear dysplasia [17].
Dejour outlined radiographic parameters that
define trochlear dysplasia [24]. This included a
trochlear depth less than 4 mm, a patellar tilt
over 20°, a spur height greater than 5 mm, and a
trochlear sulcus angle over 145°. Using these
criteria, the Dejour dysplasia classification was
described with four overarching dysplastic phenotypes (A-D). This was further subclassified
into low-grade dysplasia (type A dysplasia) and
high-grade dysplasia (types B-D dysplasia) [17].
Clinically, this is reflected in the treatment
options recommended as low-grade trochlear
dysplasia does not typically require operative
intervention as these patients are unlikely to
benefit from a trochleoplasty procedure [17].
The complex strain and stress environment at
the PFJ articular surface has made chondral
lesions of the PFJ a notoriously difficult pathological challenge to surgeons [25]. Focal defects
of the patellar cartilage lead to altered biomechanics, debilitating pain, and rapid acceleration
of osteoarthritis when mismanaged [25]. An
understanding of the pathophysiology of patellofemoral osteochondral lesions can guide a
surgeon in determining which combination of
procedures will provide the best long term pain
relief, provide substantial functional improvement, and adequately address the etiology of
aberrant joint loading and instability when
present.
4
Treatment Modalities
Cartilage lesions of the knee can be debilitating
conditions that can worsen overtime and progress
to a diffuse arthritis if left untreated [26, 27].
When managing these lesions, the first-line goals
are conservative modalities that aim to relieve
352
inflammation, control pain, and restore functional
capacity [13]. Typically, nonsteroidal antiinflammatory medications, intra-articular corticosteroids, and hyaluronic acid viscosupplementation are utilized as first-line therapeutic
interventions to manage inflammatory symptoms
[13]. Physical therapy can also play a crucial role
in the early nonoperative management of these
lesions as there is a high incidence of functional
impairment and kinematic derangement in individuals with PFJ cartilage lesions. Muscle
strengthening can improve absorption of physiological loads across the knee, while weight loss
and activity modification can avoid aggravation
of painful symptoms [28, 29]. In general, nonoperative treatment should be trialed prior to
pursuing surgical intervention as many patients
will achieve substantial relief through these
conservative measures, allowing them to potentially avoid a complicated subsequent surgical
procedure [30, 31].
Surgical management is pursued for patients
with persistent, functionally limiting symptoms
that have failed to adequately respond to initial
nonoperative treatment [6]. There are several
effective cartilage repair modalities that have
been described for the management of patellofemoral chondral defects, including bone marrow
stimulation techniques, autologous chondrocyte
implantation (ACI), osteochondral autograft
transplantation (OAT), and osteochondral allograft transplantation (OCA) [1]. When determining the optimal treatment modality, the lesion
size, depth, location, subchondral bone, and
patient demand must be assessed. Due to the
relatively challenging anatomy and increased
biomechanical forces experienced at the PFJ,
these cartilage procedures have consistently
demonstrated inferior clinical outcomes when
implemented at the PFJ relative to other locations
within the knee, regardless of the technique used
[1, 27, 32].
Bone marrow-stimulation techniques, such as
microfracture or subchondral drilling attempt to
stimulate bone marrow to allow cell migration
into the defect area to promote healing [33].
These procedures are limited as they create
fibrocartilage that is physiologically and
S. P. Dasari et al.
biomechanically inferior to hyaline cartilage
[34]. These techniques are also unable to adequately manage larger osteochondral lesions [35,
36]. Additionally, the unique anatomy of the PFJ
makes marrow stimulation techniques challenging and leads to difficulty in creating stable vertical walls [37]. These factors, combined with the
challenging biomechanical environment, limit
the utility and popularity of marrow stimulation
techniques in the PFJ.
Autologous
chondrocyte
implantation
(ACI) utilizes tissue engineering techniques to
regenerate cartilage using cell-based therapy.
While effective, it is a two-stage procedure that
requires harvesting donor cartilage from a nonweightbearing portion of the knee in addition to
an expensive culturing phase. The modality has
been shown to be effective in treating large
chondral lesions and can be implemented using a
sandwich technique, when there is subchondral
bone involvement [38]. Many proponents of ACI
recommend routine use of patellofemoral
unloading and realignment procedures when
using this technique [2, 39, 40].
Osteochondral autograft transfer (OAT) is a
procedure that is effective at managing smaller
symptomatic osteochondral lesions regardless of
underlying subchondral bone involvement [41].
Typically, autografts are harvested from nonweight bearing portions of the knee like the
intercondylar notch before being prepared and
press-fit in a single stage procedure [6]. OATs
have several inherent advantages including the
transfer of mature, physiologic hyaline cartilage
and viable chondrocytes over an intact osseous
bed. Additionally, the technique has no risk of
immunologic reaction [28]. While effective for
smaller lesions, this technique is not without
limitations. For example, the morbidity associated with a donor site of an OAT procedure can
make it an undesirable therapeutic intervention
for patients with defects that are larger than 2.5
cm2 [42]. Additionally, this technique is particularly limited in the management of patellofemoral chondral lesions due to the challenging
anatomy of the PFJ. There is difficulty matching
the surface concavity and convexity of the
patellofemoral articulation when transplanting
Fresh Osteochondral Allografts in Patellofemoral Surgery
autograft plugs from a non-weightbearing portion
of the knee [6]. Moreover, donor grafts from
non-weight-bearing portions of the knee tend to
have thinner articular cartilage than that of the
native patella, which further limits the applicability of this technique for patellofemoral chondral lesions [43]. Finally, the typical donor sites
for graft harvest are often within the same
patellofemoral articulation that is being treated
for symptomatic cartilage disease, which may
compromise the clinical situation. These inherent
limitations suggest that OAT procedures can be
viable modalities for small patellofemoral chondral lesions with subchondral bone involvement
but are limited in their applicability for larger
lesions in the PFJ.
5
Osteochondral Allografts (OCA)
OCAs have numerous advantages relative to
many of the other cartilage repair modalities
when managing lesions of the PFJ (Table 1).
This includes the presence of mature, metabolically active chondrocytes in the graft,
353
immunoprivileged properties, no donor site
morbidity, management of underlying subchondral pathology, and efficacy in large lesions,
unconstrained lesions, and bipolar lesions [44,
45]. Unlike an OAT, the OCA is able to provide
viable cells without the associated concomitant
donor site morbidity that is intrinsic to an autograft technique [27]. This lack of donor site
morbidity can also make an OCA a more viable
treatment option for larger defects, where an
OAT procedure would not be feasible. Thus, the
OCA procedure allows for the management of a
large osteochondral defect using a single procedure without concomitant donor site morbidity
[13, 46].
An additional benefit of the OCA procedure is
that it facilitates the replacement of a defect with
hyaline cartilage overlying an intact osseous bed
[47]. This creates an architecturally stable articular surface with mature hyaline cartilage in the
setting of a large, full-thickness osteochondral
defect [27]. This property allows the graft to
accept full loading as soon as the bone base has
healed, which can expedite the rehabilitation and
recovery process; this is particularly beneficial
Table 1 Advantages and Disadvantages of the Fresh Osteochondral Allograft Technique for Patellofemoral
Osteochondral Lesions
Advantages
Disadvantages
Mature, metabolically active chondrocytes transplanted
in the graft
Graft availability and challenges related to morphology
matching the donor graft with the recipient’s knee
anatomy
No donor site morbidity
Expensive procedure
Relatively immunoprivileged
A risk of disease transmission
Management of underlying subchondral bone
pathology
Technically demanding procedure
Effective option for large lesions, unconstrained
lesions, bipolar lesions
Logistical demands to minimize chondrocyte death
Effective for trochlear dysplasia with high grade
chondromalacia
Can be used as a primary procedure or a secondary
salvage procedure after a failed prior surgical
intervention
Graft survivorship not impacted by prior procedures to
the lesion
Return to weight bearing can begin when bone base
has healed and integrated
354
when managing the lesion in athletes as it can
accelerate their return to activity and weight
bearing [41, 48, 49].
Furthermore, the OCA technique for PFJ
lesions offers a wide range of applicability. The
technique can be implemented in large chondral
lesions with or without subchondral bone
involvement.
Additionally,
transplantation
necessitates removal of the underlying native
subchondral bone, so prior microfracture surgery
does not affect graft survivorship [26]. Another
benefit is that OCAs can be used to treat
unconstrained lesions as they do not need a
continuous border of healthy articular cartilage
for successful repair [41, 50]. The technique can
also be successfully implemented in bipolar
lesions, as a salvage procedure after failed prior
treatment, and in young patients with posttraumatic osteochondral defects after fractures
around the knee joint [13]. For trochlear defects,
an OCA procedure can be implemented as both a
primary and salvage procedure, while it is typically utilized as a salvage procedure for large
patellar lesions to delay arthroplasty in young
patients [13]. Though trochleoplasty is able to
address high grade trochlear dysplasia and provide an osseous restraint to patellar instability, it
does not adequately address any symptomatic
trochlear chondral lesions and is contraindicated
in cases of high grade trochlear chondromalacia
[17, 18]. As a result, in chronic instability cases
with a large chondral lesion and high-grade trochlear dysplasia, a trochlear shell OCA technique
may be a viable surgical option to adequately
address both trochlear pathologies [18]. In cases
of severe dysplasia of both the patella and trochlea, large plug or shell allografts have the
unique ability among cartilage repair techniques
to change structural pathoanatomy.
Disadvantages of an OCA are related to
availability, cost, infection risk, disease transmission, and challenging surgical technique
(Table 1). Cost is a major limitation of the OCA
technique. In 2016, it had been reported that the
average cost of a fresh OCA in the United States
S. P. Dasari et al.
was approximately 11,000 dollars [27]. Part of
this cost is reflected in the rigorous testing that
grafts undergo to minimize the risk of disease
transmission [41]. Despite this testing, there is
still some small risk of communicable disease
transmission associated with OCA transplants
[27].
Graft availability is another relative disadvantage of the OCA technique. Variability
between patellar and trochlear anatomy in the
population can make it difficult to find an
appropriate donor graft [2]. Graft matching is
made further challenging by the unique bony
shape, chondral thickness, and sliding articulation intrinsic to the PFJ [51]. Challenges related
to complex morphology matching are most pronounced when lesions involve the central trochlear groove or median patellar ridge [2]. As a
result, graft availability can be a significant limitation as the ideal graft should be from a donor
of similar or younger age at death and have
similar knee dimensions to the recipient [41].
Location matching and size matching are strategies implemented to offset this challenge, but
graft availability still remains a limiting factor in
the effective implementation of this transplant
technique [2]. To offset this limitation, it is crucial for scheduling flexibility. When a wellmatched donor graft becomes available, the surgeon and patient should agree to perform the
procedure in a time frame that minimizes chondrocyte death (*28 days). While the goal should
be to find a donor graft that matches the morphology of the host joint architecture, a slight
mismatch has been shown to lead to acceptable
clinical results [51].
Another drawback to OCA transplants within
the PFJ is that they are technically challenging
procedures. Precise fitting of the plug and creating a smooth transition between the donor and
recipient is crucial to success with this technique
[13]. The complex topography and variation in
anatomy of the patella and the trochlea contribute
to the challenges associated with the OCA
transplantation procedure [2].
Fresh Osteochondral Allografts in Patellofemoral Surgery
6
Osteochondral Allograft Storage
and Preparation
Chondrocyte viability is critical for graft survival
and resulting mid-to-long term clinical outcomes
[2]. Chondrocyte viability is important for graft
survivorship as these cells maintain the extracellular matrix (ECM) to prevent deterioration
[52]. Viability is dependent on a variety of factors, including preservation technique, timing
from graft harvesting to implantation, and the
technique of implantation. Fresh allografts are
typically harvested within 24 h of the donor’s
death and stored at 4° Celsius until the procedure
[53]. The shelf life of a fresh graft has remained
controversial with current recommendations
suggesting a storage time of up to 28 days [54,
55]. These recommendations have demonstrated
adequate chondrocyte viability for current transplant practices [13].
Storage media and methods have varied
greatly over the past 50 years since the technique
was initially described [52]. As grafts have
become commercially supplied under Food and
Drug Administration (FDA) oversight, they have
become subjected to a prolonged storage interval
to allow for rigorous testing protocols [52].
Under ideal conditions, grafts should be recovered from donors between the age of 15–35 years
of age with macroscopically healthy cartilage and
harvested within 12 to 24 h after a donor’s death
[52]. This period can be extended by approximately 12 h if the donor’s body is cooled within
the first 6 h of death [56]. Prior to storage, the
tissue is subjected to high pressure pulsatile
lavage irrigation, decontamination, dry centrifugation, and centrifugation with sterile phosphatebuffered saline before microbiological tests can
be performed [56]. Stricter guidelines imposed
by the FDA have decreased the risk of disease
transmission allowing OCA transplants to
become an increasingly popular primary or salvage procedure [13].
Because the procedure is heavily dependent
on chondrocyte viability within the graft, there
have been several studies dedicated to optimizing
temperature and storage media conditions [57–
355
61]. Broadly speaking, grafts can be stored as
frozen, cryopreserved, or fresh. Each technique
has variable effects on chondrocyte viability,
graft immunogenicity, and duration of time
where the graft is viable for a transplantation
[52]. Frozen grafts demonstrate a chondrocyte
survivorship of less than 5% but also demonstrate decreased immunogenicity due to the
freezing process [62, 63]. Cryopreservation has
been proposed as a solution to maintain chondrocyte viability during the freezing process by
preventing intracellular ice formation [52]. While
sound in theory, cryopreservation only allows for
viable chondrocytes at the surface of the articular
cartilage layer as the dense extracellular matrix
limits penetration of the cryopreservant to deeper
cellular layers [56, 64]. Additionally, the freezing
process can cause fissures and delamination of
the cartilage [65]. Fresh OCAs have the highest
chondrocyte viability and are placed in tissue
culture medium at 4° Celsius [52]. A study by
Ranawat et al. demonstrated superior histological
and biomechanical properties of fresh allografts
relative to frozen/cryopreserved porcine specimens [66]. A subsequent study by Pallante et al.
demonstrated similar findings in a goat animal
model [67].
In addition to the storage medium and conditions, the time from harvesting to implantation
is critical for maximizing chondrocyte viability at
the time of the procedure. For properly stored
fresh grafts, there is little loss in viability during
the first week after harvesting [68, 69]. Studies
have demonstrated a time dependent decrease in
chondrocyte viability and mechanical properties
of fresh grafts after storage beyond 14 days [44,
70, 71]. By 3 weeks, chondrocyte viability
declines to roughly 70% and is approximately
67% by 7 weeks [44, 57, 60, 61]. While prolonged storage decreases viability, cell density,
and tissue metabolism, it has minimal effects on
the ECM or osseous components [65].
Expedited implantation is made challenging
by the need for tissue banks to store the transplant grafts for a minimum of 7–10 days to
ensure proper microbiologic and serologic testing
[65, 72]. Furthermore, delays for size matching
356
grafts can also prolong the time from harvesting
to implantation. While it is important to perform
the procedure in a timely manner, studies that
have investigated the implantation of fresh OCAs
after prolonged storage demonstrated good efficacy in grafts stored up to 42 days after harvest
despite the corresponding decline in chondrocyte
viability [73, 74]. Based on these findings, current recommendations would suggest that the
transplant procedure be performed within
42 days of graft harvesting [65].
Higher impact loads also adversely affect cell
viability. Prior studies have demonstrated that
less than 50% of cells in the graft survive high
force loads during impaction [75, 76]. It has also
been demonstrated that the load of the impact
plays a larger role in chondrocyte death than the
number of impacts, so multiple low-load taps are
preferred over a single high-load tap if impaction
cannot be avoided [2]. Ideally, impaction should
not be needed and the graft can be press fit into
position such that it is flush and in contact with
the base of the recipient hole regardless of subchondral bone matching [2]. Using this method
allows the surgeon to decrease the subsidence of
the graft, leading to a better restoration of the
contact pressure in that knee compartment [77].
Another potential drawback to an allograft
technique is the risk of potential immunogenicity. Intact hyaline cartilage is a relatively
immunoprivileged tissue because it is avascular
and the chondrocytes of the tissue are embedded
in a dense ECM that is inaccessible to the host
immune system [52]. Despite this, marrow elements in the osseous portion of the graft have
some degree of immunogenicity as the subchondral bone component of the graft is laden
with potentially immunogenic cells and proteins
[65]. Routine pulse lavage of the graft has been
implemented to decrease the concentration of
these marrow elements, mechanically remove
proteins that may trigger a reaction, and thus
reduce immunogenicity of the allograft [78–80].
Studies have demonstrated that larger grafts were
more likely to elicit a systemic immune response
[81]. Because the immunogenicity of the graft is
directly related to the osseous portion of the
graft, reducing the thickness of the subchondral
S. P. Dasari et al.
bone component of an OCA is thought to minimize the risk of potential immunogenicity [13].
Despite this potential risk, larger grafts have not
demonstrated inferior overall survival rates relative to smaller grafts [82].
Graft integration occurs over a gradual process termed creeping substitution. Overtime, the
osseous portion of the graft is gradually replaced
by host bone. This slow process is mediated on
the cellular level by osteoblastic bone formation
and osteoclastic resorption; minimizing the
amount of transplanted bone may reduce the
healing process associated with bone incorporation [83]. The cartilage component is transplanted at a mature stage, does not undergo
interactions with the host, and does not undergo
further healing [65]. When performed appropriately, transplanted OCAs have good survivorship
and retrieved specimens have demonstrated high
donor chondrocyte viability [57, 69].
7
Indications and Contraindications
As a high load joint, symptomatic patellofemoral
osteochondral lesions often require an intervention. When nonoperative treatment measures fail,
surgical intervention should be considered. OCA
is a valid treatment modality for large patellar
and trochlear chondral defects except in patients
with end-stage osteoarthritis [2]. Cases with
subtotal loss or bipolar lesions without significant joint space narrowing can be adequately
addressed by this modality in younger patient
populations [2]. OCA is indicated as a primary
procedure in patients who have large, full
thickness cartilage lesions with abnormal subchondral bone, though it is gaining increasing
implementation in the treatment of pure chondral
lesions as well [13]. OCA is suitable for a wide
range of disease pathologies due to its inherent
osseous structure and multishaping possibilities:
this includes complex reconstruction procedures,
massive osteochondral defects, osteonecrosis,
diseases affecting the subchondral bone, primary
large chondral lesions, and lesions that have
failed a prior cartilage repair technique [52].
Fresh Osteochondral Allografts in Patellofemoral Surgery
Surgical candidates for an OCA transplant
procedure are young active patients with full
thickness, symptomatic focal lesions that are
greater than 2 cm2 in size [41]. Typically, these
patients cannot undergo another restorative procedure like arthroplasty due to their age or an
OAT or ACI procedure due to defect size, depth,
and location [41]. For these younger patients
with cartilage defects, arthroplasty is not an ideal
treatment modality as it leads to functional limitations and a higher rate of revision joint
replacement [84–86]. Unlike joint replacement
procedures, OCA transplantations give this subset of patients the best possibility to return to
athletic activity, especially in those younger than
24 years old with symptoms that are less than a
year old [41]. Another major benefit of OCA
transplants for larger lesions and for patellofemoral lesions is the ability to construct an optimized allograft that matches the size, shape, and
depth of the lesion [53, 65]. This allows it to be a
suitable modality for posttraumatic osteochondral defects, osteonecrosis, and osteochondritis
dissecans, where large lesions that are unamenable to adequate repair by OAT can be
managed [41]. Additionally, unlike ACI, OCA
transplants are single stage procedures that
replace hyaline cartilage and the underlying
subchondral bone without the need for an additional intervention [53, 65, 87]. Another advantage of OCA transplants is that prior treatment
failures do not limit its utilization and it can be
successfully used as a salvage procedure [53].
For bipolar patellofemoral lesions, there is some
controversy over the efficacy of OCA transplants,
with some authors proposing it as an effective
surgical option for large defects, defects with
extensive subchondral bone involvement, or as a
salvage procedure for extensive degenerative
changes in younger patient populations [84].
OCA can be performed in cases of contained
lesions, with the use of the dowel-plug technique,
as well as larger uncontained defects, with the use
of the shell technique [25, 37, 56]. Knee alignment and patellar tracking should be evaluated to
determine the need for any concomitant
357
procedures when pursuing an OCA transplant.
General indications for the procedure include
young, active patients (typically less than
50 years old) with severe discomfort from a focal
chondral or osteochondral lesion (Table 2) [6].
There are several absolute contraindications
where a fresh patellofemoral OCA should not be
pursued (Table 2). These include advanced
osteoarthritis, where patellofemoral arthroplasty
may be a superior treatment option; cases with a
chronic posttraumatic defect; or any patient who
is a poor surgical candidate [41]. Advanced
osteoarthritis and inflammatory arthritis are contraindications for OCA transplant as the failure
rate for the procedure and need for subsequent
total knee arthroplasty in a short span make this
patient population unlikely to benefit from the
intervention [41].
Relative contraindications to the procedure
include obese patients (BMI > 35 kg/m2), concomitant meniscal/ligamentous injuries in the
ipsilateral knee, uncorrectable malalignment of
the knee joint, smoking, or corticosteroid use
(Table 2) [41]. Irreversible damage can occur to
allografts in obese patients, patients who smoke,
and those who chronically use corticosteroids, due
to impaired bone metabolism [41]. For cases with
osteonecrosis, it is recommended that chronic
corticosteroid use is stopped prior to pursuing the
OCA transplant. It is believed that continued
corticosteroid use will interfere with revascularization of the allograft leading to collapse [53, 88].
Higher body mass leads to an increased risk of
failure in obese patients due to aberrant loading of
the graft and the resulting death of viable chondrocytes [89–91]. Normal joint alignment is critical for a successful OCA transplant, and
uncorrectable malalignment can lead to decreased
viability of transplanted chondrocytes [41]. It is
also critical to restore normal intraarticular
biomechanics via addressing any concomitant
meniscal insufficiency or ligamentous instability
during the OCA procedure [41]. Patients with
posterior cruciate ligament deficiency will place
increased stress on the PFJ and are not ideal candidates for this procedure in isolation [25].
358
S. P. Dasari et al.
Table 2 Indications, Absolute Contraindications, and Relative Contraindications of the Fresh Osteochondral Allograft
Technique for Patellofemoral Osteochondral Lesions
Indications
Large chondral/osteochondral lesions (greater than 2 cm2) of the patellofemoral joint that have failed nonoperative
management [41]
Patellar defects, trochlear defects, bipolar defects, and subtotal defects without significant joint space narrowing [2]
Patients with associated subchondral bone pathology [13]
Salvage procedure after failing a prior cartilage repair technique [53]
Young active patients (less than 50 years old) who desire to return to a relatively high level of activity and are willing
to follow postoperative recovery and rehabilitation protocols [41, 84–86]
Absolute Contraindications
End stage osteoarthritis [41]
Chronic post traumatic defects [41]
Poor surgical candidates [41]
Inflammatory arthritis [41]
Relative Contraindications
Obese patients (BMI over 35 kg/m2) [41, 89–91]
Concomitant ligamentous or meniscal injuries (must be addressed before or during the procedure in order to purse an
OCA of the PFJ) [41]
Uncorrected malalignment of the joint (must be addressed before or during the procedure in order to purse an OCA of
the PFJ) [41]
Smoking [41]
Chronic corticosteroid use [53, 88]
8
Pre-Operative Planning
8.1 Imaging
Preoperative imaging of chondral and osteochondral lesions usually begins with plain
radiographs consisting of standing anteroposterior views, lateral views, patellofemoral (sunrise)
views, and long axis weight-bearing [25, 50, 56,
92]. The common standing views are often
paired with a 45° flexion posteroanterior
weightbearing (Rosenberg) view and should be
inspected for pathological changes in all knee
compartments. Bearing in mind the possible
anatomical underlying causes for patellofemoral
disorders, the lateral view also provides information regarding patellar height or trochlear
dysplasia. Further assessment of trochlear morphology, as well as patellar morphology and
additional maltracking features can be noted in
sunrise views. Long axis radiographs should be
inspected for coronal plane mechanical
malalignment.
Advanced imaging studies, including magnetic resonance imaging (MRI) and computed
tomography (CT) should also be conducted
(Fig. 1). MRI is a highly sensitive and specific
modality for the detection of chondral pathology,
with similar accuracy reported for patellar and
trochlear defects [93]. Aside from lesion size and
location, MRI is able to detect subchondral bone
edema or sclerosis [94]. Additionally, MRI is
valuable for assessing associated intra-articular
disorders that would require intervention, such as
meniscal status, ligament status, or the presence
of loose bodies.
CT can be useful as an additional means of
quantifying bone involvement, and bone stock in
the context of massive chondral defects or OCD
patients [50]. TT-TG distance, patellar tilt, and
rotational deformities can also be assessed.
Fresh Osteochondral Allografts in Patellofemoral Surgery
359
Fig. 1 Focal patellar chondral lesion with an uncontained trochlear lesion, disrupted medial patellofemoral ligament,
and concomitant severe trochlear dysplasia seen on an axial T2 MRI (A, B)
8.2 Concomitant Procedures
It is crucial to address any associated knee disorders that could jeopardize cartilage restoration,
either beforehand in a staged approach or concomitant to the OCA [1, 2, 13]. A tibial
tuberosity osteotomy (TTO) is a distal realignment procedure that allows for adjustments in the
coronal, sagittal, and axial planes in order to
redistribute patellar contact pressures and
improve patellar tracking [95]. Anteriorization of
the tibial tubercle will shift contact forces proximally, and medialization of the tubercle will
decrease the lateral force vector [95]. The Fulkerson anteromedialization (AMZ) TTO combines
both mechanisms and was developed to address
patellofemoral pain with concomitant patellar
maltracking [96]. The procedure improves contact mechanics and unloads the patellofemoral
joint, so it is often performed alongside patellofemoral cartilage restoration procedures as it has
been shown to improve the clinical outcomes of
these restoration techniques [95, 97, 98].
The AMZ TTO transfers contact forces from
distal and lateral to proximal and medial on the
patellar articular surface to unload the PFJ and
minimize strain on an OCA. This makes it particularly useful when managing lesions on the
inferior pole or lateral facet [13]. The AMZ TTO
is designed to decrease the Q angle to a more
central position and correct the TT-TG distance
for cases of patellar instability, allowing for
adequate unloading of the patellofemoral compartment during cartilage restoration surgery [6].
This has been shown to significantly decrease
patellofemoral contact pressure [99]. Furthermore, a study by Pidoriano et al. has demonstrated superior outcomes for managing lesions at
the lateral facet or distal pole of the patella relative to patients who did not undergo AMZ TTO
[100]. In the setting of cartilage restoration procedures, the AMZ TTO can be performed as a
concomitant procedure to minimize contact
pressures on the OCA and optimize the biomechanical environment [95]. An unloading
osteotomy is also strongly considered when an
OCA is performed in the setting of bipolar
patellofemoral lesions [2]. Unloading osteotomies can reduce joint surface pressures by up
to 30%, making them crucial for success in this
situation.
Varus or valgus osteotomies for coronal plane
malalignment, lateral retinacular release or
lengthening, vastus medialis advancement,
medial—and rarely lateral—patellofemoral ligament reconstruction, distalization of the patella,
and de-rotation osteotomies should be performed
when necessary [1, 2, 50]. While unloading
osteotomies improve clinical outcomes related to
OCA, they are not without complications and
carry a risk of nonunion, painful hardware, or
iatrogenic overloading of a separate site within
360
the patellofemoral joint [6]. Lastly, bone marrow
aspirate concentrate (BMAC) is also often used
in conjunction with an OCA to enhance graft
integration [13].
8.3 Graft-Matching
Allograft size-matching is a critical step of preoperative planning as creating a smooth articular
surface is key to the success of the procedure
[101]. The traditional prevailing parameter for
donor matching is based on anteroposterior and
lateral radiographs of the recipient corrected for
magnification [102, 103]. Previous studies using
computer modeling and cadaveric specimens
have demonstrated that contact pressures can
significantly increase when there is a graft mismatch leading to a 0.5–1 mm protuberance relative to the neighboring cartilage [77, 104]. MRI
can also be useful in presurgical matching and is
employed by 93% of members of the Metrics of
Osteochondral Allografts (MOCA) expert group
in addition to standard radiography with a sizing
marker for patellofemoral OCA [2, 105]. Previous studies have shown a potential for underestimating defect size when using MRI in
comparison to surgical findings [106, 107].
However, modern equipment and cartilagespecific MRI sequences tend to allow for more
detailed evaluation [25]. Other reported parameters are preoperative CT scan, anthropometric
agreement between donor and recipient, and
Wiberg’s classification for the shape of the
patella [56].
The anatomic complexity of the patellofemoral joint, combined with wide variability for
articular geometry and cartilage thickness, make
donor-matching even more challenging than
OCA procedures for the tibiofemoral compartments. To create a matching system specific to
OCA procedures of the PFJ, Determann et al.
proposed the use of radiographic patellar measurements [108]. The authors demonstrated a
strong correlation for ex vivo patellar angle and
articular length and moderate correlation for lateral facet width, total width and central ridge
S. P. Dasari et al.
height using their technique. While potentially
beneficial, this method still lacks sufficient clinical validation. As a result, to help with surgical
planning, a diagnostic arthroscopy is recommended to further evaluate for the size, location,
and severity of the cartilage defect, and to further
verify patient eligibility for OCA.
9
Surgical Technique and Case
Presentation
9.1 Patient Positioning
and Anesthesia
The patient is placed in the supine position on the
operating table and placed under general anesthesia. The senior author prefers a technique,
where a well-padded high-thigh tourniquet is
placed on the operative side and a bump is placed
under the knee so that it rests at approximately
30° of flexion. The contralateral leg is secured to
the table in full extension with a pneumatic
compression device to help prevent DVT. Preliminary arthroscopy and eventual concomitant
procedures should be performed before the OCA.
An adductor canal block combined with local
infiltration is an effective and safe option for pain
management, without the loss of quadriceps
motor function associated with femoral nerve
blocks.
9.2 Surgical Exposure
A small medial or lateral parapatellar arthrotomy
is performed depending on the location of the
cartilage defect. A medial arthrotomy is generally
preferred as it facilitates patellar mobilization
and exposure of both the patella and trochlea,
which makes it far superior to lateral approaches
for this. Furthermore, the lateral trochlea surface
is directed medially and thus instruments are
more easily positioned from the medial side
with the patella subluxed laterally. Medial
subluxation of the patella for exposure is significantly more difficult. Full exposure of the patella
Fresh Osteochondral Allografts in Patellofemoral Surgery
and trochlea—particularly in cases of bipolar
lesions or large defects requiring the shell technique—may require a sizeable arthrotomy.
9.3 Dowel-Plug OCA Technique
The defect should be identified and templated.
Next, a guide pin is placed in the center of the
defect and the edges of the defect are scored. It is
essential that the guide pin be placed as perpendicular as possible to the joint surface. The defect
is then reamed until bleeding, healthy bone is
encountered, with care not to exceed a maximum
of 7 to 8 mm of overall bone depth. This can be
achieved by frequently checking the calibrated
coring reamer (Arthrex, Inc. Naples, Florida),
along with a final measurement. The recipient
site is then dilated with a smooth cylinder
(Arthrex, Inc. Naples, Florida) several times to
ensure the donor plug can be inserted without the
need to apply too much pressure. In order to
accomplish a perfect fit between the donor graft
and the host socket, a compass reference is created on the prepared defect and measures are
taken
from
each
main
coordinate
(North/South/East/West). These measurements
will be used later at the time of graft trimming.
The whole donor specimen is then secured
within an allograft workstation (Arthrex, Inc.
Naples, Florida) to ensure precision during harvest. The osteochondral donor plug is then harvested from the allograft with use of a coring
reamer. The direction of this reamer relative to
the surface of the allograft should be identical to
the direction that the recipient site was prepared.
This fundamental technique can be challenging
in the complex surface topography of the patella
and trochlea. The subchondral bone of the donor
plug is then trimmed according to previous
measurements to match the corresponding depths
of the host location, and the surfaces are
smoothed with a rasp. The depth of the recipient
site and donor plug is measured several times to
make sure there are no areas that will be too
proud.
Copious irrigation should be used while
reaming the receiving site and graft in order to
361
prevent heat necrosis. Prior to implantation of the
donor bone plug, the subchondral bone is subjected to pulse lavage with an antibiotic solution
to eradicate any remaining bone-marrow elements to minimize the chance of immune reaction [79]. Bone marrow aspirate concentrate is
often used in an effort to augment allograft
integration [109].
The bone plug is then gently press-fit into the
socket to match the exact height of the surrounding articular cartilage. Rotation of the plug
is checked to ensure “best fit.” Impaction of the
graft should be avoided when possible. Consensus among the MOCA expert group points to an
ideal depth of the allograft that is limited to 6 to
10 mm [76]. If proud, the surgeon should consider removal of the plug with a small blunt
elevator and smoothing off the small, elevated
area with a rasp. If the recipient site is too deep,
then remove the allograft and add a deeper layer
of bone graft first. Preference should be given to
matching cartilage surface topography and minimizing peripheral step-off over osseous mismatching [2].
The dowel-plug technique is the preferred
method of patellofemoral OCA when working
with focal, contained chondral defects (Figs. 2
and 3) [2, 37]. The dowel or press-fit technique
fashions a 15–35 mm diameter plug that allows
for press-fit implantation on the recipient site and
obviates the need for implant-fixation. Defects
that are entirely on the medial or lateral facets of
the patella can be addressed with small dowelplugs. Central defects can be treated with a dowel
OCA but are technically more challenging to
match perfectly owing to the complex geometry
of the trochlear groove and patellar median ridge.
Although there is no consensus on the ideal
approach for these cases, options include ACI, a
“mega-OAT” dowel technique, where one uses a
single large plug to resurface almost the entire
patella, or a shell technique [2, 110, 111].
9.4 Shell Technique for the Patella
Common indications for a patellar shell OCA
technique include extensive damage to both
362
S. P. Dasari et al.
A
B
C
D
Fig. 2 Patellar osteochondral lesion treated with a fresh
osteochondral allograft (OCA) using the dowel-plug
technique. A Osteochondral lesion of the patella,
B patellar lesion after removal of the lesion by reaming,
C shaped osteochondral allograft plug, D OCA press-fit
using the dowel-plug technique
patellar facets, damage to the median ridge, and
uncontained lesions [37]. The technique is typically indicated for cartilage defects that are not
eligible for a dowel-plug OCA procedure. In the
clinical setting, other frequent indications include
post-traumatic arthritis (post-patellar fracture)
and osteonecrosis [16, 56].
For patellar shell grafting, a patellar cut is
performed using principles comparable to those
of resurfacing during total knee arthroplasty.
A caliper can be used to obtain the patellar
thickness measurement, in addition to superiorinferior and medial–lateral widths for donor sizematching. The patellar cut is performed either
free-hand or using a “lobster-claw” patellar
clamp. At least 12 mm of the native patellar
thickness should be preserved in order to limit
fracture risk, and no more than about 15 mm
should be preserved in order to avoid overstuffing, which would increase patellofemoral contact
forces and limit flexion [112, 113]. Any resulting
sclerotic bone should be drilled. Donor graft
Fresh Osteochondral Allografts in Patellofemoral Surgery
363
9.5 Shell Technique for the Trochlea
Fig. 3 A focal, contained trochlear osteochondral lesion
treated with a press-fit OCA using the dowel-plug
technique
preparation is carried out in similar fashion. It is
wise to avoid shell grafts that are beyond 10 mm
of subchondral bone thickness as this is the
known threshold for a theoretically higher risk of
immune reaction, although large trochlea graft
often are up to 15 mm at their highest point to
accommodate a minimum thickness (5–6 mm) at
their lowest point [114]. Oversized graft or native
bone margins can be trimmed for ideal matching.
The allograft is placed and temporarily fixed to
the receiving site with Kirschner wires, positioned on the extra-articular dorsal aspect of the
patella. If placement, size, and tracking are
deemed satisfactory, definitive fixation canthen
be performed. Retrograde fixation from the dorsal aspect to the subchondral bone as well as
countersunk headless fixation from the margins
of the articular surface have been described as
typical fixation techniques [37, 56, 111]. Possible
fixation implants include metal screws, bioabsorbable screws or pins.
The trochlear shell OCA technique is typically
indicated for uncontained trochlear lesions as
well as cases with trochlear dysplasia and concomitant high grade chondromalacia [17, 18, 41].
In a recently published technical note, the senior
author described a trochlear shell allograft technique combined with MPFL reconstruction and a
TTO to treat trochlear dysplasia in the setting of
chondral damage and chronic patellar instability
(Fig. 4) [16]. After performing a medial parapatellar incision and dissecting to the joint capsule, a medial patellar arthrotomy is performed.
During this initial stage, it is important that the
incision is large enough to allow complete
visualization and exposure of the trochlea,
patellar surfaces, and tibial tubercle, if a TTO is
indicated. While the knee is positioned in 60° of
flexion, three 2.0 mm Kirschner wires are placed
in parallel in a distal to proximal fashion to serve
as a guide for the oscillating saw when removing
the existing native dysplastic trochlea. Copious
irrigation is utilized during this step to minimize
the risk of thermal necrosis. The remaining bony
surface is then homogenized to facilitate anatomic fixation of the allograft. The donor femur
allograft is prepared on the back table. Three
Kirschner wires are placed: one is central and
superior to the notch while the other two pins are
parallel and just lateral to either side of the central pin. These are used to guide the oscillating
saw. After making the cut, the undersurface of
the graft is shaved and osteophytes are removed
to facilitate anatomic reconstruction of the trochlea. Pulsatile irrigation is performed on the
graft followed by pressurized carbon dioxide
once the curvature of the graft match is confirmed. This is followed by application of bone
marrow aspirate concentrate to the osseous portion of the graft, which is done to maximize
healing and integration of the graft (Fig. 5). The
graft is then placed in its optimal anatomic
position on the patient’s femur and four
364
Fig. 4 Trochlear osteochondral allograft (OCA) shell
technique. A Three Kirschner wires are used to guide an
oscillating saw, which is cutting the trochlea under
constant irrigation. B The cut surface after the trochlear
cap was removed and C the placement of the
Fig. 5 Bone marrow aspirate
concentrate (BMAC) applied
to the osseous portion of the
trochlear OCA. A Aspiration
of bone marrow from the iliac
crest. B Using pressurized
carbon dioxide on the osseous
portion of the graft. C,
D Application of BMAC to
the OCA
S. P. Dasari et al.
osteochondral allograft to ensure an anatomic reconstruction. D Securing the trochlear OCA using four headless
screws. E A lateral fluoroscopic view after the fixation.
F Final view of the anatomically reconstructed trochlea
with an OCA secured using four headless screws
Fresh Osteochondral Allografts in Patellofemoral Surgery
365
Fig. 6 Preoperative (A) and
postoperative (B) axial views
of CT scans demonstrating the
trochlear shell allograft for
trochlear dysplasia with
concomitant trochlear
chondromalacia in a left knee
Table 3 Pearls and Pitfalls of the Fresh Osteochondral Allograft Technique for Patellofemoral Osteochondral Lesions
Pearls
For contained lesions, a dowel-plug technique should be used, while a shell technique should be used for uncontained
lesions alone or when correcting a trochlear lesion in the setting of trochlear dysplasia
Knee alignment and patellar tracking should be evaluated to determine the need for a concomitant procedure like an
anteromedialization tibial tubercle osteotomy, medial patellofemoral ligament reconstruction etc
Preoperative matching of the donor to the recipient in terms of size, shape, curvature, and overall knee morphology is
critical to ensuring a successful outcome
Donor cartilage should be from young patients without obvious chondral disease. The donor should ideally be similar
in age or younger than the recipient
Surgeon and patient schedules must be flexible to facilitate timing of the surgery when a size and shape matched donor
graft becomes available
For the plug technique, bleeding healthy bone should be encountered while reaming the defect. However, the recipient
site should not exceed 7–8 mm of depth. Frequently check the calibrated coring reamer to avoid over-reaming. Using
a graft that is thicker than 8 mm may increase the immunogenicity of the transplanted tissue
For the plug technique, using a smooth dilator after reaming the defect facilitates further insertion of the donor plug
For the plug technique, reduce the size of the original allograft in order to facilitate its manipulation during
osteochondral plug preparation
For the plug technique, use a clockface reference (12/3/6/9) for measuring the depth of the recipient’s bed and have an
assistant outside the surgical field taking notes to precisely prepare the donor plug. This allows the surgeon to ensure
an accurate donor-host curvature match
Multiple trials of shaving the undersurface of the graft should be done to facilitate anatomic reconstruction
Pulsed lavage the osseous component of the graft to minimize the risk of an immunogenic reaction
Bone marrow aspirate concentrate (BMAC) can be used to biologically enhance and expedite graft integration
BMAC should be applied to the osseous component of the graft after pulsed lavage of the graft and after applying
pressurized carbon dioxide to the osseous component of the graft. Pressurized carbon dioxide helps to clean the bone
microarchitecture
Pitfalls
Heat necrosis can occur from high-speed reamers in the edges of the receptor’s bed as well as in the donor plug. It can
also occur when using the oscillating saw for the shell technique. Copiously irrigate cutting surfaces with roomtemperature saline while using reamers and saws to minimize this risk
Failure to address concomitant underlying pathology such as instability related to an insufficient MPFL or a dysplastic
trochlea can ultimately lead to failure of the procedure
(continued)
366
S. P. Dasari et al.
Table 3 (continued)
Inaccurate curvature match can lead to inferior outcomes of the OCA procedure
Ensure a flush fit of the graft; a graft that is too proud will lead to aberrant joint mechanics
Reaming too deep increases the risk of a fracture and also requires the use of an OCA with a thicker osseous
component that could increase the risk of immunogenicity
For the plug technique, minimize impaction of the osteochondral graft while press-fitting it into the receptor’s bed (use
a sponge to cushion the chondral surface and frequent low-force impaction if necessary)
Non-compliance with postoperative rehabilitation can lead to poor results. Do not pursue an osteochondral allograft in
a patient who is unwilling or unable to follow the postoperative rehabilitation and recovery protocol
Kirschner wires are drilled to hold the graft in
place, while four headless screws are used to
secure the graft. The screws are placed either
perpendicularly through the center of the graft or
obliquely from the graft margins. For this case,
the trochlear shell technique (Fig. 6) was followed by a TTO, MPFL reconstruction, and a
dowel-plug technique OCA for a contained
patellar chondral lesion. A list of pearls and pitfalls of the fresh OCA technique for patellofemoral osteochondral lesions is outlined in
Table 3.
encouraged after 6 weeks [37]. From 6 to
12 weeks the patient should be able to regain the
ability to perform functional activities of daily
life. Avoidance of high-impact activities during
the first 6 to 12 months is advised to allow for
complete graft healing and incorporation. A preference for low-impact over high-impact activities
after this period is also encouraged. Athletes
should follow rigorous criteria for return to play,
at the discretion of the treating surgeon [50].
11
10
Rehabilitation
Patients should customarily follow an initial
period of non-weight-bearing during the first
eight weeks for graft protection. Progressive
weightbearing with a knee brace locked in full
extension, has not been shown to excessively load
the patellofemoral joint, and, as a result, it is safe
for patients and often implemented assuming no
associated osteotomy was performed [2, 115].
Supervised rehabilitation should start immediately postoperatively, with a focused emphasis on
quadriceps activation. Early range of motion
exercises are widely considered safe in order to
avoid arthrofibrosis, and a continuous passive
motion (CPM) machine should be implemented
whenever possible [2]. Some authors advocate
limiting knee flexion during the early postoperative phase and allowing for 30° flexion increments biweekly until a full range of motion is
Patient Outcomes
11.1 Clinical Outcomes
The current literature has consistently demonstrated good to excellent outcomes in terms of
survival and function for generalized knee OCA
procedures [50, 52]. However, when compared
to OCAs in the tibiofemoral compartment,
patellofemoral OCA has often been associated
with inferior results, higher failure rates, and
higher reoperation rates [27, 32, 116]. Cameron
et al. retrospectively evaluated patient outcomes
and satisfaction in 28 patients who had OCA to
the femoral trochlea [117]. They found significant improvement in modified d’Aubigné-Postel
score, International Knee Documentation Committee (IKDC) subscores, and Knee Society
Score-Function (KS-F). Furthermore, 89% of
patients were extremely satisfied or satisfied with
their surgical outcome. This was determined
using the OCA patient satisfaction score.
Fresh Osteochondral Allografts in Patellofemoral Surgery
However, these results must be interpreted with
caution due to the small sample size and lack of
comparison with other treatment options.
In 2020, Chahla et al. performed a systematic
review of clinical outcomes after PF OCA with at
least 1.5 years follow up [1]. One hundred and
twenty nine patients were evaluated from eight
clinical studies. The etiologies of the osteochondral lesions included trauma, osteochondritis
dissecans, patellar instability, degenerative
chondral lesions, and osteoarthritis. A total of 16
outcome measures were utilized across these
studies. Significant improvement in at least one of
the following primary clinical outcome measures
was reported in seven of the eight studies. These
primary outcome measures were the IKDC, Knee
Society Score-Function, Lysholm Knee score,
and modified d’Aubigné-Postel score. However,
the apparent heterogeneity in studies’ reporting of
subjective and objective outcomes, as well as the
influence of concomitant pathologies and procedures alongside PF OCA limit the generalizability
of these findings. Additionally, the design of the
included studies precluded the authors from performing a formal meta-analysis of the data.
11.2 Imaging Outcomes
Similar to the clinical outcomes for PFJ OCA,
the imaging outcomes are supportive of the
technique but limited thus far. Spak and Teitge
evaluated radiographs at final follow-up for graft
incorporation, resorption, collapse, cyst formation, and osteophyte formation [1, 118]. At final
follow up, all patients demonstrated an intact
allograft with radiographs exhibiting mild
degenerative changes for six of eight patients,
and no degenerative changes in the remaining
two patients. Jamali et al. also evaluated radiographs of 12 patients for visibility of allografthost junctions, allograft radiodensity, and presence of subchondral cysts [119]. Four patients
did not show signs of PF arthrosis, six had mild
arthrosis, and two patients developed advanced
arthrosis. The allograft-host interface was visible
in three patients. Graft radiodensity was found to
be increased in four patients. Subchondral lysis
367
was seen in four patients; however, three of these
four grafts had good to excellent clinical scores.
Given the limited radiographic analyses performed for PF OCA outcomes, future studies
should focus on imaging outcomes to aid in
validating the success of OCA to treat patellofemoral chondral lesions.
11.3 Survivorship
In the systematic review by Chahla et al., seven
included studies performed Kaplan–Meier survival analysis for PF OCA [1]. Cameron et al.
reported 100% allograft survivorship at 5 years
and 91.7% at 10 years post-operatively [117].
The lowest survivorship was reported by Gracitelli et al. with 55.8% at 15 years follow up [26].
When combining data from all studies, the
weighted mean 5 year survival rate was 87.9%,
the average 10-year survivorship was 77.2%, and
survival rate at 15 years was 55.8%; however,
this 15 year outcome was only reported in one
single study [1].
Amongst these seven clinical studies included
in the systematic review by Chahla et al., graft
failure was not uniformly defined [1]. Three
studies defined graft failure as necessitating graft
revision or conversion to total knee arthroplasty
(TKA) [117, 120, 121]. Another study defined
failure as any reoperation resulting in allograft
removal [26]. Frank et al. defined failure to be
conversion to TKA, revision OCA, or graft failure as observed on second-look arthroscopy [89].
One study included clinical outcome measures as
part of their definition of failure, with clinical
ratings less than 70 points on KSS-F and
Lysholm Knee Score scales [118].
A recent 2019 study by Cotter et al. performed
a survivorship analysis of 50 patients treated with
PF OCA (using either plug or shell technique)
and identified variables associated with graft
failure [37]. In the plug technique group, two
patients (out of 16 patients) failed at an average
of 9.17 years post-operatively. In the shell technique group, 13 patients (out of 34 patients)
failed at an average of approximately 3.81 years
post-operatively. In addition, Kaplan–Meier
368
survival analyses was performed for each
group. The plug technique group was found to
have survival rates of 100% and 66% at 5 and
9.8 years after PF OCA, respectively. The shell
technique group had survival rates of 65.8% at
5 years and 37% at 10.6 years. In this study,
logistic regression analysis was performed to
identify variables associated with PF OCA failure within the entire cohort of patients and within
the shell group specifically (37]. Increased BMI
was found to be associated with graft failure in
the entire cohort as well as within the shell
technique group. Furthermore, a traumatic etiology of the chondral pathology was protective
against graft failure in the entire cohort analysis.
An additional study by Meric et al. reported
on the results from a total of 48 subjects with
bipolar reciprocal osteochondral lesions. Survivorship of the bipolar OCA was 64.1% at
5 years. High reoperation (62%) and failure rates
(46%) were observed, but patients with surviving
allografts showed significant clinical improvement (18-point score, IKDC pain, IKDC function, KS-F). Interestingly, bipolar OCA
transplants in the PFJ have displayed lower
failure rates when compared to bipolar tibiofemoral transplants [111].
S. P. Dasari et al.
11.4 Complications
Complications following PF OCA are relatively
uncommon, and studies reporting on this data are
limited. No intraoperative complications were
identified by Chahla et al.’s systematic review
[1]. In a 2006 study by Spak and Teitge, the
authors reported five minor complications: four
patients developed postoperative anterior knee
pain that was managed conservatively and one
patient developed a post-operative skin rash that
resolved with prednisone [118]. In addition, all
patients had mild synovitis that resolved spontaneously. Cameron et al.’s study of 28 patients
found one patient to have persistent pain, possibly attributed to complex regional pain syndrome, ultimately requiring a total knee
arthroplasty (TKA) (117]. Bakay et al. reported
on one patient developing hyperpressure of the
patellofemoral joint, which did not require
reoperation [122]. Cotter et al. reported no
intraoperative complications, but three patients
developed postoperative complications [37]. One
patient developed a deep infection requiring
arthroscopic irrigation and debridement followed
by intravenous antibiotics. One patient experienced a superficial skin infection that resolved
Table 4 Key Points to “Take-Home”
“Take-Home” Points
Osteochondral lesions of the patellofemoral joint are challenging to treat due to the complex, variable anatomy and
high biomechanical strain experienced at the joint. Despite this, osteochondral allografts can effectively treat patellar
lesions, trochlear lesions, large lesions, unconstrainted lesions, and bipolar lesions at this joint as both a primary and
salvage treatment option
Osteochondral allografts combine mature hyaline cartilage with metabolically active chondrocytes over a stable,
structural osseous base allowing them to address chondral and subchondral pathology
Location matching, size matching, expedition of time from harvest to transplantation, and minimization of impaction
are all critical components to optimizing clinical outcomes with the fresh osteochondral allograft procedure
Concomitant procedures including the Fulkerson anteromedialization tibial tubercle osteotomy, patellofemoral
ligament reconstruction, varus/valgus osteotomies, de-rotation osteotomies, lateral reticular release/lengthening, and
the application of bone marrow aspirate concentrate can all be critical towards satisfactory clinical outcomes for the
application of osteochondral allografts when treating patellofemoral pathology
The dowel plug technique is ideal for focal, contained lesions while shell techniques are preferred for large,
unconstrained lesions or lesions with concomitant trochlear dysplasia
The initial literature has demonstrated inferior outcomes of patellofemoral osteochondral allografts relative to
tibiofemoral osteochondral allografts; however, several studies have reported promising initial clinical improvement
and patient satisfaction with fresh osteochondral allografts at this joint. Additionally, a recent systematic review has
demonstrated good survivorship of the transplanted graft at five- and ten-years follow-up
Fresh Osteochondral Allografts in Patellofemoral Surgery
with oral antibiotic treatment only. One patient
developed pain and stiffness secondary to intraarticular adhesions requiring arthroscopic lysis of
adhesions. Wang et al. reported on three patients
who developed arthrofibrosis post-operatively,
but all were successfully treated with arthroscopic lysis of adhesions and scar excision [120].
Unfortunately, one of these patients subsequently
developed septic arthritis after lysis of adhesions,
which was treated with arthroscopic irrigation
and debridement. This same patient later went on
to undergo TKA nearly four years later.
11.5 Reoperation Rates
The most common reoperation reported after
PF OCA was hardware removal [1, 26, 118–120].
However, it is not clear if this was secondary to the
index PF OCA procedure or due to concomitant
procedures performed during PF OCA (e.g.,
realignment surgeries or osteotomies). Reoperations were also performed for patients who were
deemed to have a failed allograft, subsequently
requiring TKA. Cotter et al. reported five of 16
patients (31.3%) that underwent plug technique
required reoperation approximately 1–2 years
following primary PF OCA [37]. Reasons for
reoperation in this group included medial femoral
condyle chondroplasty, post-operative pain
necessitating second-look arthroscopy, hardware
removal for concomitant high tibial osteotomy,
and irrigation and debridement secondary to
infection. In contrast, 28 of 34 patients (82.4%)
that underwent shell technique PF OCA required
reoperation. The most common reoperation was
patellofemoral arthroplasty and second-look
arthroscopy with chondral debridement (grafts
intact). Six patients required TKA, and four
patients required hardware removal from concomitant osteotomy procedures.
369
12
Conclusion and Key Message
Patellofemoral osteochondral allograft is an
effective procedure used to treat patellofemoral
osteochondral lesions unamenable to conservative measures (Table 4). It can be used as both a
primary procedure or a secondary salvage procedure to treat large lesions, unconstrained
lesions, lesions involving the underlying subchondral bone, and bipolar lesions. Current
clinical literature shows promise in the widespread implementation of this technique. Future
studies should continue to investigate possible
graft-matching parameters specifically tailored
for the patellofemoral joint as well as the longterm outcomes and complications associated with
the patellofemoral OCA surgical technique.
References
1. Chahla
J,
Sweet
MC,
Okoroha
KR,
Nwachukwu BU, Hinckel B, Farr J, et al. Osteochondral allograft transplantation in the patellofemoral joint: a systematic review. Am J Sports Med.
2019;47(12):3009–18.
2. Chahla J, Hinckel BB, Yanke AB, Farr J, Bugbee WD,
Carey JL, et al. An Expert consensus statement on the
management of large chondral and osteochondral
defects in the patellofemoral joint. Orthop J Sports
Med. 2020;8(3):2325967120907343.
3. Widuchowski W, Widuchowski J, Trzaska T. Articular cartilage defects: study of 25,124 knee arthroscopies. Knee. 2007;14(3):177–82.
4. Hart HF, Stefanik JJ, Wyndow N, Machotka Z,
Crossley KM. The prevalence of radiographic and
MRI-defined patellofemoral osteoarthritis and structural pathology: a systematic review and metaanalysis. Br J Sports Med. 2017;51(16):1195–208.
5. Lording T, Lustig S, Servien E, Neyret P. Chondral
Injury in patellofemoral instability. CARTILAGE.
2014;5(3):136–44.
6. Strauss EJ, Galos DK. The evaluation and management of cartilage lesions affecting the patellofemoral joint. Curr Rev Musculoskelet Med. 2013;6
(2):141–9.
370
7. Fox AJ, Wanivenhaus F, Rodeo SA. The basic
science of the patella: structure, composition, and
function. J Knee Surg. 2012;25(2):127–41.
8. Stäubli HU, Dürrenmatt U, Porcellini B, Rauschning W. Anatomy and surface geometry of the
patellofemoral joint in the axial plane. J Bone Joint
Surg Br. 1999;81(3):452–8.
9. Kladny B, Martus P, Schiwy-Bochat KH, Weseloh G,
Swoboda B. Measurement of cartilage thickness in the
human knee-joint by magnetic resonance imaging
using a three-dimensional gradient-echo sequence. Int
Orthop. 1999;23(5):264–7.
10. Tecklenburg K, Dejour D, Hoser C, Fink C. Bony
and cartilaginous anatomy of the patellofemoral
joint. Knee Surg Sports Traumatol Arthrosc.
2006;14(3):235–40.
11. Zwerver J, Bredeweg SW, Hof AL. Biomechanical
analysis of the single-leg decline squat. Br J Sports
Med. 2007;41(4):264–8; discussion 8.
12. Flynn TW, Soutas-Little RW. Patellofemoral joint
compressive forces in forward and backward running. J Orthop Sports Phys Ther. 1995;21
(5):277–82.
13. Mestriner AB, Ackermann J, Gomoll AH. Patellofemoral cartilage repair. Curr Rev Musculoskelet
Med. 2018;11(2):188–200.
14. Grelsamer RP, Dejour D, Gould J. The pathophysiology of patellofemoral arthritis. Orthop Clin North
Am. 2008;39(3):269–74, v.
15. Farr J, Covell DJ, Lattermann C. Cartilage lesions
in patellofemoral dislocations: incidents/locations/
when to treat. Sports Med Arthrosc Rev. 2012;20
(3):181–6.
16. Kerzner B, Gursoy S, Dasari SP, Fortier LM,
Yanke AB, Chahla J. Trochlear osteochondral shell
allograft technique to treat trochlear dysplasia in the
setting of chondral damage and chronic patellar
instability. Arthroscopy Techniques. 2022.
17. Nolan JE, Schottel PC, Endres NK. Trochleoplasty:
indications and technique. Curr Rev Musculoskelet
Med. 2018;11(2):231–40.
18. DePhillipo NN, Kennedy MI, Aman ZS, Moatshe G,
LaPrade RF. Osteoarticular allograft transplantation
of the trochlear groove for trochlear dysplasia: a
case report. JBJS Case Connect. 2018;8(2): e29.
19. McKinley TO, Borrelli J Jr, D’Lima DD, Furman BD, Giannoudis PV. Basic science of intraarticular fractures and posttraumatic osteoarthritis.
J Orthop Trauma. 2010;24(9):567–70.
20. Tochigi Y, Vaseenon T, Heiner AD, Fredericks DC,
Martin JA, Rudert MJ, et al. Instability dependency
of osteoarthritis development in a rabbit model of
graded anterior cruciate ligament transection.
J Bone Joint Surg Am. 2011;93(7):640–7.
21. Jungmann PM, Tham S-C, Liebl H, Nevitt MC,
McCulloch CE, Lynch J, et al. Association of
trochlear dysplasia with degenerative abnormalities
in the knee: data from the Osteoarthritis Initiative.
Skeletal Radiol. 2013;42(10):1383–92.
S. P. Dasari et al.
22. Noehren B, Duncan S, Lattermann C. Radiographic
parameters associated with lateral patella degeneration in young patients. Knee Surg Sports Traumatol Arthrosc. 2012;20(12):2385–90.
23. Cregar WM, Huddleston HP, Wong SE, Farr J,
Yanke AB. Inconsistencies in reporting risk factors
for medial patellofemoral ligament reconstruction
failure: a systematic review. Am J Sports Med.
2021:3635465211003342.
24. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol
Arthrosc. 1994;2(1):19–26.
25. Dekker TJ, Kennedy MI, Grantham WJ,
DePhillipo NN, LaPrade RF. Patellar fresh osteochondral allograft transplantation. Arthrosc Tech.
2019;8(8):e851–4.
26. Gracitelli GC, Meric G, Pulido PA, Görtz S, De
Young AJ, Bugbee WD. Fresh osteochondral
allograft transplantation for isolated patellar cartilage injury. Am J Sports Med. 2015;43(4):879–84.
27. Familiari F, Cinque ME, Chahla J, Godin JA,
Olesen ML, Moatshe G, et al. Clinical outcomes
and failure rates of osteochondral allograft transplantation in the knee: a systematic review. Am J
Sports Med. 2018;46(14):3541–9.
28. Strauss EJ, Fonseca LE, Shah MR, Yorum T.
Management of focal cartilage defects in the knee—
Is ACI the answer? Bull NYU Hosp Jt Dis. 2011;69
(1):63–72.
29. Chiu JKW, Wong Y-m, Yung PSH, Ng GYF. The
effects of quadriceps strengthening on pain, function, and patellofemoral joint contact area in persons
with patellofemoral pain. Amer J Phys Med Rehab.
2012;91(2).
30. Werner S. Anterior knee pain: an update of physical
therapy. Knee Surg Sports Traumatol Arthrosc.
2014;22(10):2286–94.
31. Mosier BA, Arendt EA, Dahm DL, Dejour D,
Gomoll AH. Management of patellofemoral arthritis: from cartilage restoration to arthroplasty. J Am
Acad Orthop Surg. 2016;24(11):e163–73.
32. Brophy RH, Wojahn RD, Lamplot JD. Cartilage
restoration techniques for the patellofemoral joint.
J Am Acad Orthop Surg. 2017;25(5):321–9.
33. Godin JA, Sanchez G, Cinque ME, Chahla J,
Kennedy NI, Provencher MT. Osteochondral allograft transplantation for treatment of medial femoral
condyle defect. Arthrosc Tech. 2017;6(4):
e1239–44.
34. Alford JW, Cole BJ. Cartilage restoration, part 1:
basic science, historical perspective, patient evaluation, and treatment options. Am J Sports Med.
2005;33(2):295–306.
35. Alford JW, Cole BJ. Cartilage restoration, part 2:
techniques, outcomes, and future directions. Am J
Sports Med. 2005;33(3):443–60.
36. Chahla J, LaPrade RF, Mardones R, Huard J,
Philippon MJ, Nho S, et al. Biological therapies for
Fresh Osteochondral Allografts in Patellofemoral Surgery
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
cartilage lesions in the hip: a new horizon. Orthopedics. 2016;39(4):e715–23.
Cotter EJ, Christian DR, Frank RM, Abyar E,
Wischmeier D, Yanke AB, et al. Survivorship of
patellofemoral osteochondral allograft transplantation. Arthroscopy Sports Med Rehab. 2019;1(1):
e25–34.
Bartlett W, Gooding CR, Carrington RW, Skinner JA, Briggs TW, Bentley G. Autologous chondrocyte implantation at the knee using a bilayer
collagen membrane with bone graft. A preliminary
report. J Bone Joint Surg Br. 2005;87(3):330–2.
Vasiliadis HS, Lindahl A, Georgoulis AD, Peterson L. Malalignment and cartilage lesions in the
patellofemoral joint treated with autologous chondrocyte implantation. Knee Surg Sports Traumatol
Arthrosc. 2011;19(3):452–7.
Giuliani JR, Burns TC, Owens BD, Svoboda SJ. Knee cartilage patellofemoral injuries.
Tech Orthop. 2010;25(21W):224.
Cavendish PA, Everhart JS, Peters NJ, Sommerfeldt MF, Flanigan DC. Osteochondral allograft
transplantation for knee cartilage and osteochondral
defects: a review of indications, technique, rehabilitation, and outcomes. JBJS Rev. 2019;7(6): e7.
Chow JCY, Hantes ME, Houle JB, Zalavras CG.
Arthroscopic autogenous osteochondral transplantation for treating knee cartilage defects: A 2- to 5year follow-up study. Arthroscopy J Arthroscopic
Related Surgery. 2004;20(7):681–90.
Gomoll AH, Minas T, Farr J, Cole BJ. Treatment of
chondral defects in the patellofemoral joint. J Knee
Surg. 2006;19(4):285–95.
Pearsall AWt, Tucker JA, Hester RB, Heitman RJ. Chondrocyte viability in refrigerated
osteochondral allografts used for transplantation
within the knee. Am J Sports Med. 2004;32
(1):125–31.
Arnoczky SP. The biology of allograft incorporation. J Knee Surg. 2006;19(3):207–14.
Dean CS, Chahla J, Serra Cruz R, LaPrade RF.
Fresh Osteochondral allograft transplantation for
treatment of articular cartilage defects of the Knee.
Arthrosc Tech. 2016;5(1):e157–61.
Krych AJ, Robertson CM, Williams RJ 3rd. Return
to athletic activity after osteochondral allograft
transplantation in the knee. Am J Sports Med.
2012;40(5):1053–9.
Campbell AB, Pineda M, Harris JD, Flanigan DC.
Return to sport after articular cartilage repair in
athletes’ knees: a systematic review. Arthroscopy.
2016;32(4):651-68.e1.
Nielsen ES, McCauley JC, Pulido PA, Bugbee WD.
Return to sport and recreational activity after
osteochondral allograft transplantation in the Knee.
Am J Sports Med. 2017;45(7):1608–14.
Sherman SL, Garrity J, Bauer K, Cook J, Stannard J,
Bugbee W. Fresh osteochondral allograft transplantation for the knee: current concepts. J Am Acad
Orthop Surg. 2014;22(2):121–33.
371
51. Lin KM, Wang D, Burge AJ, Warner T, Jones KJ,
Williams RJ, 3rd. Osteochondral allograft transplant
of the patella using femoral condylar allografts:
magnetic resonance imaging and clinical outcomes
at minimum 2-year follow-up. Orthopaedic J Sports
Med. 2020;8(10):2325967120960088.
52. Bugbee W, Cavallo M, Giannini S. Osteochondral
allograft transplantation in the knee. J Knee Surg.
2012;25(2):109–16.
53. Torrie AM, Kesler WW, Elkin J, Gallo RA. Osteochondral allograft. Curr Rev Musculoskelet Med.
2015;8(4):413–22.
54. Nuelle CW, Nuelle JA, Cook JL, Stannard JP. Patient factors, donor age, and graft storage
duration affect osteochondral allograft outcomes in
knees with or without comorbidities. J Knee Surg.
2017;30(2):179–84.
55. Schmidt KJ, Tírico LE, McCauley JC, Bugbee WD.
Fresh osteochondral allograft transplantation: is
graft storage time associated with clinical outcomes
and graft survivorship? Am J Sports Med. 2017;45
(10):2260–6.
56. Gelber PE, Perelli S, Ibañez M, Ramírez-Bermejo
E, Fariñas O, Monllau JC, et al. Fresh osteochondral
patellar allograft resurfacing. Arthrosc Tech. 2018;7
(6):e617–22.
57. Williams SK, Amiel D, Ball ST, Allen RT,
Wong VW, Chen AC, et al. Prolonged storage
effects on the articular cartilage of fresh human
osteochondral allografts. J Bone Joint Surg Am.
2003;85(11):2111–20.
58. Allen RT, Robertson CM, Pennock AT, Bugbee WD, Harwood FL, Wong VW, et al. Analysis
of stored osteochondral allografts at the time of
surgical implantation. Am J Sports Med. 2005;33
(10):1479–84.
59. Pennock AT, Robertson CM, Wagner F, Harwood FL, Bugbee WD, Amiel D. Does subchondral
bone affect the fate of osteochondral allografts
during storage? Am J Sports Med. 2006;34
(4):586–91.
60. Pennock AT, Wagner F, Robertson CM, Harwood FL, Bugbee WD, Amiel D. Prolonged storage
of osteochondral allografts: does the addition of
fetal bovine serum improve chondrocyte viability? J
Knee Surg. 2006;19(4):265–72.
61. Pallante AL, Bae WC, Chen AC, Görtz S, Bugbee WD, Sah RL. Chondrocyte viability is higher
after prolonged storage at 37 degrees C than at 4
degrees C for osteochondral grafts. Am J Sports
Med. 2009;37 Suppl 1(Suppl 1):24s-32s.
62. Enneking WF, Mindell ER. Observations on massive retrieved human allografts. J Bone Joint Surg
Am. 1991;73(8):1123–42.
63. Görtz S, Bugbee WD. Allografts in articular
cartilage repair. Instr Course Lect. 2007;56:469–80.
64. Judas F, Rosa S, Teixeira L, Lopes C, Ferreira MA.
Chondrocyte viability in fresh and frozen large
human osteochondral allografts: effect of cryoprotective agents. Transplant Proc. 2007;39(8):2531–4.
372
65. Demange M, Gomoll AH. The use of osteochondral
allografts in the management of cartilage defects.
Curr Rev Musculoskelet Med. 2012;5(3):229–35.
66. Ranawat AS, Vidal AF, Chen CT, Zelken JA,
Turner AS, Williams RJ 3rd. Material properties of
fresh cold-stored allografts for osteochondral
defects at 1 year. Clin Orthop Relat Res.
2008;466(8):1826–36.
67. Pallante AL, Chen AC, Ball ST, Amiel D,
Masuda K, Sah RL, et al. The in vivo performance
of osteochondral allografts in the goat is diminished
with extended storage and decreased cartilage
cellularity. Am J Sports Med. 2012;40(8):1814–23.
68. Sammarco VJ, Gorab R, Miller R, Brooks PJ. Human
articular cartilage storage in cell culture medium:
guidelines for storage of fresh osteochondral allografts. Orthopedics. 1997;20(6):497–500.
69. Gross AE, Shasha N, Aubin P. Long-term followup
of the use of fresh osteochondral allografts for
posttraumatic knee defects. Clin Orthop Relat Res.
2005;435:79–87.
70. Ball ST, Amiel D, Williams SK, Tontz W,
Chen AC, Sah RL, et al. The effects of storage on
fresh human osteochondral allografts. Clin Orthop
Relat Res. 2004;418:246–52.
71. Malinin T, Temple HT, Buck BE. Transplantation
of osteochondral allografts after cold storage.
J Bone Joint Surg Am. 2006;88(4):762–70.
72. Vangsness CT Jr, Garcia IA, Mills CR, Kainer MA,
Roberts MR, Moore TM. Allograft transplantation
in the knee: tissue regulation, procurement, processing, and sterilization. Am J Sports Med.
2003;31(3):474–81.
73. Williams RJ 3rd, Ranawat AS, Potter HG, Carter T,
Warren RF. Fresh stored allografts for the treatment
of osteochondral defects of the knee. J Bone Joint
Surg Am. 2007;89(4):718–26.
74. McCulloch PC, Kang RW, Sobhy MH, Hayden JK,
Cole BJ. Prospective evaluation of prolonged fresh
osteochondral allograft transplantation of the
femoral condyle: minimum 2-year follow-up.
Am J Sports Med. 2007;35(3):411–20.
75. Patil S, Tapasvi SR. Osteochondral autografts. Curr
Rev Musculoskelet Med. 2015;8(4):423–8.
76. Walczak BE, Nies MS, Trask DJ, Hetzel S,
Roney PJ, Squire MW, et al. Osteochondral graft
size is significantly associated with increased force
and decreased chondrocyte viability. Am J Sports
Med. 2018;46(3):623–31.
77. Kock NB, Smolders JMH, van Susante JLC,
Buma P, van Kampen A, Verdonschot N. A cadaveric analysis of contact stress restoration after
osteochondral transplantation of a cylindrical cartilage defect. Knee Surg Sports Traumatology
Arthroscopy: Official J ESSKA. 2008;16(5):461–8.
78. Ibrahim T, Qureshi A, McQuillan TA, Thomson J,
Galea G, Power RA. Intra-operative washing of
morcellised bone allograft with pulse lavage: how
S. P. Dasari et al.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
effective is it in reducing blood and marrow
content? Cell Tissue Bank. 2012;13(1):157–65.
Meyer MA, McCarthy MA, Gitelis ME, Poland SG,
Urita A, Chubinskaya S, et al. Effectiveness of
lavage techniques in removing immunogenic elements from osteochondral allografts. CARTILAGE.
2016;8(4):369–73.
Sun Y, Jiang W, Cory E, Caffrey JP, Hsu FH,
Chen AC, et al. Pulsed lavage cleansing of osteochondral grafts depends on lavage duration, flow
intensity, and graft storage condition. PLoS ONE.
2017;12(5): e0176934.
Bugbee WD, Convery FR. Osteochondral allograft
transplantation. Clin Sports Med. 1999;18(1):67–
75.
Hunt HE, Sadr K, DeYoung AJ, Gortz S, Bugbee WD. The Role of immunologic response in
fresh osteochondral allografting of the Knee. Am J
Sports Med. 2014;42(4):886–91.
Czitrom AA, Keating S, Gross AE. The viability of
articular cartilage in fresh osteochondral allografts
after clinical transplantation. J Bone Joint Surg Am.
1990;72(4):574–81.
Giannini S, Buda R, Ruffilli A, Pagliazzi G,
Ensini A, Grigolo B, et al. Failures in bipolar fresh
osteochondral allograft for the treatment of endstage knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2015;23(7):2081–9.
Vazquez-Vela Johnson G, Worland RL, Keenan J,
Norambuena N. Patient demographics as a predictor
of the ten-year survival rate in primary total knee
replacement. J Bone Joint Surg Br. 2003;85(1):52–6.
Levy YD, Görtz S, Pulido PA, McCauley JC,
Bugbee WD. Do fresh osteochondral allografts
successfully treat femoral condyle lesions? Clin
Orthop Relat Res. 2013;471(1):231–7.
Chui K, Jeys L, Snow M. Knee salvage procedures:
The indications, techniques and outcomes of large
osteochondral allografts. World J Orthop. 2015;6
(3):340–50.
Görtz S, De Young AJ, Bugbee WD. Fresh
osteochondral allografting for steroid-associated
osteonecrosis of the femoral condyles. Clin Orthop
Relat Res. 2010;468(5):1269–78.
Frank RM, Lee S, Levy D, Poland S, Smith M,
Scalise N, et al. Osteochondral allograft transplantation of the knee: analysis of failures at 5 years.
Am J Sports Med. 2017;45(4):864–74.
Shasha N, Aubin PP, Cheah HK, Davis AM,
Agnidis Z, Gross AE. Long-term clinical experience
with fresh osteochondral allografts for articular knee
defects in high demand patients. Cell Tissue Bank.
2002;3(3):175–82.
Pylawka TK, Wimmer M, Cole BJ, Virdi AS,
Williams JM. Impaction affects cell viability in
osteochondral tissues during transplantation. J Knee
Surg. 2007;20(2):105–10.
Fresh Osteochondral Allografts in Patellofemoral Surgery
92. Zouzias IC, Bugbee WD. Osteochondral allograft
transplantation in the Knee. Sports Med Arthrosc
Rev. 2016;24(2):79–84.
93. Harris JD, Brophy RH, Jia G, Price B, Knopp M,
Siston RA, et al. Sensitivity of magnetic resonance
imaging for detection of patellofemoral articular
cartilage defects. Arthroscopy. 2012;28(11):1728–
37.
94. DeFranco MJ, McNickle AG, Cole BJ. Allograft
osteoarticular resurfacing. Paris: Springer Paris,
pp 497–503.
95. Farr J, Schepsis A, Cole B, Fulkerson J,
Lewis P. Anteromedialization—review and technique. J Knee Surg. 2007;20(2):120–8.
96. Fulkerson JP. Anteromedialization of the tibial
tuberosity for patellofemoral malalignment. Clin
Orthop Relat Res. 1983;177:176–81.
97. Fulkerson JP, Becker GJ, Meaney JA, Miranda M,
Folcik MA. Anteromedial tibial tubercle transfer
without bone graft. Am J Sports Med. 1990;18
(5):490–6;discussion 6–7.
98. Trinh TQ, Harris JD, Siston RA, Flanigan DC.
Improved outcomes with combined autologous
chondrocyte implantation and patellofemoral osteotomy versus isolated autologous chondrocyte
implantation. Arthroscopy. 2013;29(3):566–74.
99. Cohen ZA, Henry JH, McCarthy DM, Mow VC,
Ateshian GA. Computer simulations of patellofemoral joint surgery. Patient-specific models for
tuberosity transfer. Am J Sports Med. 2003;31
(1):87–98.
100. Pidoriano AJ, Weinstein RN, Buuck DA, Fulkerson JP. Correlation of patellar articular lesions with
results from anteromedial tibial tubercle transfer.
Am J Sports Med. 1997;25(4):533–7.
101. Gursoy S, Simsek ME, Akkaya M, Kaya O,
Bozkurt M. Local curvature mismatch may worsen
the midterm functional outcomes of osteochondral
allograft transplantation. Knee Surg Sports Traumatol Arthrosc. 2021;29(9):2948–57.
102. LaPrade RF, Botker J, Herzog M, Agel J. Refrigerated osteoarticular allografts to treat articular cartilage defects of the femoral condyles. A prospective
outcomes study. J Bone Joint Surg Am. 2009;91
(4):805–11.
103. Bernstein DT, O’Neill CA, Kim RS, Jones HL,
Noble PC, Harris JD, et al. Osteochondral allograft
donor-host matching by the femoral condyle radius
of curvature. Am J Sports Med. 2017;45(2):403–9.
104. Koh JL, Kowalski A, Lautenschlager E. The effect
of angled osteochondral grafting on contact pressure: a biomechanical study. Am J Sports Med.
2006;34(1):116–9.
105. Du PZ, Markolf KL, Levine BD, McAllister DR,
Jones KJ. Differences in the radius of curvature
between femoral condyles: implications for osteochondral allograft matching. J Bone Joint Surg Am.
2018;100(15):1326–31.
373
106. Gomoll AH, Yoshioka H, Watanabe A, Dunn JC,
Minas T. Preoperative measurement of cartilage
defects by mri underestimates lesion size. Cartilage.
2011;2(4):389–93.
107. Campbell AB, Knopp MV, Kolovich GP, Wei W,
Jia G, Siston RA, et al. Preoperative MRI underestimates articular cartilage defect size compared
with findings at arthroscopic knee surgery. Am J
Sports Med. 2013;41(3):590–5.
108. Determann JR, Fleischli JE, D’Alessandro DF,
Piasecki DP. Patellofemoral osteochondral allografts: can we improve the matching process? J
Knee Surg. 2017;30(8):835–41.
109. Oladeji LO, Stannard JP, Cook CR, Kfuri M,
Crist BD, Smith MJ, et al. Effects of autogenous
bone marrow aspirate concentrate on radiographic
integration of femoral condylar osteochondral allografts. Am J Sports Med. 2017;45(12):2797–803.
110. Gomoll AH, Gillogly SD, Cole BJ, Farr J,
Arnold R, Hussey K, et al. Autologous chondrocyte
implantation in the patella: a multicenter experience. Am J Sports Med. 2014;42(5):1074–81.
111. Hinckel B, Farr J, Gomoll A. Patellofemoral
osteochondral allograft transplantation. Operative
Techniques in Sports Medicine. 2015;23.
112. Bengs BC, Scott RD. The effect of patellar thickness on intraoperative knee flexion and patellar
tracking in total knee arthroplasty. J Arthroplasty.
2006;21(5):650–5.
113. Lynch AF, Rorabeck CH, Bourne RB. Extensor
mechanism complications following total knee
arthroplasty. J Arthroplasty. 1987;2(2):135–40.
114. De Caro F, Bisicchia S, Amendola A, Ding L. Large
fresh osteochondral allografts of the knee: a
systematic clinical and basic science review of the
literature. Arthroscopy. 2015;31(4):757–65.
115. Loudon JK. Biomechanics and pathomechanics of
the patellofemoral joint. Int J Sports Phys Ther.
2016;11(6):820–30.
116. Assenmacher AT, Pareek A, Reardon PJ,
Macalena JA, Stuart MJ, Krych AJ. Long-term
outcomes after osteochondral allograft: a systematic
review at long-term follow-up of 12.3 Years.
Arthroscopy. 2016;32(10):2160–8.
117. Cameron JI, Pulido PA, McCauley JC, Bugbee WD.
Osteochondral allograft transplantation of the
femoral trochlea. Am J Sports Med. 2016;44
(3):633–8.
118. Spak RT, Teitge RA. Fresh osteochondral allografts
for patellofemoral arthritis: long-term followup. Clinical Orthopaedics Related Research®.
2006;444:193–200.
119. Jamali AA, Emmerson BC, Chung C, Convery FR,
Bugbee WD. Fresh osteochondral allografts. Clinical Orthopaedics and Related Research®.
2005;437:176–85.
120. Wang D, Rebolledo BJ, Dare DM, Pais MD,
Cohn MR, Jones KJ, et al. Osteochondral allograft
374
transplantation of the knee in patients with an
elevated body mass index. Cartilage. 2019;10
(2):214–21.
121. Wang D, Kalia V, Eliasberg CD, Wang T, Coxe FR,
Pais MD, et al. Osteochondral allograft transplantation of the knee in patients aged 40 years and
older. Am J Sports Med. 2018;46(3):581–9.
S. P. Dasari et al.
122. Bakay A, Csönge L, Papp G, Fekete L. Osteochondral resurfacing of the knee joint with allograft. Int
Orthop. 1998;22(5):277–81.
Extensor Mechanism Complications
After Total Knee Arthroplasty
Jobe Shatrov, Cécile Batailler, Gaspard Fournier,
Elvire Servien, and Sebastien Lustig
1
Introduction
Extensor mechanism problems in total knee
arthroplasty account for 12% of complications
[41]. Manifestations are broad both in terms of
etiology and impact on the patient. The most
commonly encountered complications are patellar tendon rupture, quadriceps tendon injury,
periprosthetic patella fracture, patellofemoral
instability, soft tissue impingement and
osteonecrosis of the patella. The purpose of this
chapter is to review the incidence, risk factors
and surgical management of the aforementioned
complications.
2
Commonly it is diagnosed on plain imaging
by the presence of sclerotic bone which may
appear smaller than the contralateral side and
may have the appearance of being fractured or
fragmented. In latter stages remodelling may
occur characterised by a periosteal reaction.
Interestingly, the superior pole tends to demonstrate increased radiodensity, and the inferior pole increased radiolucency [47]. CT
imaging typically features a focal area of bone
sclerosis surrounded by a sclerotic demarcation
line. Radionuclide studies can show either
decreased accumulation of the bone-seeking
radiopharmaceutical agent or focal increased
uptake of the radionuclide depending on the
phase of the disease.
Avascular Necrosis of the Patella
2.1 Definition and Epidemiology
The rate of patella osteonecrosis after TKA is
reported to be 1.4% [25]. However many patients are
asymptomatic and the actual incidence is unknown.
J. Shatrov C. Batailler G. Fournier E. Servien
S. Lustig
Albert Trillat Center, Lyon North University
Hospital, Lyon, France
J. Shatrov (&)
Sydney Orthopedic Research Institute, St. Leonard’s,
Sydney, NSW, Australia
e-mail: sebastien.lustig@gmail.com
2.2 Anatomical Considerations
The blood supply to the extensor mechanism is
provided by an anastomotic ring created by 6
branches; descending geniculate artery superior
and inferior medial and lateral geniculate arteries
and a branch from the anterior recurrent tibial
artery. On a left knee the first two arteries
join and enter the ring at 1 o’clock, with the
remaining vessels entering the ring at 3, 5 7
o’clock respectively [30]. It is disrupted as part
of routine exposure to the knee joint [42]. During
a medial parapatellar arthrotomy the descending,
superior and inferior genicular arteries are disrupted. During excision of the lateral meniscus
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_25
375
376
and the infrapatellar fat pad the lateral supply is
disrupted by cutting the recurrent branch of the
anterior tibial artery and inferior lateral geniculate artery. A lateral arthrotomy will disrupt the
superior and inferior lateral geniculate arteries as
well as the anterior tibial recurrent artery leaving
only the superior lateral geniculate artery intact
[36]. Exposure and release of the medial meniscus and plateau will disrupt the inferior medial
geniculate artery, leaving only the superior
medial geniculate artery intact.
2.3 Risk Factors
2.3.1 Surgical Approach
Whilst a medial parapatellar approach reduces
blood flow to the patella by 53% it is generally
considered safe and no difference has been
demonstrated with a sub-vastus approach [38]. If
a lateral release is performed the sole remaining
blood-supply to the patella may be from the
recurrent branch of the anterior tibial artery.
However AVN has been reported in case reports
following isolated medial parapatellar arthrotomy
as well [39]. Given lateral releases are typically
performed to improve patella tracking, the need
to perform such a release may be avoided
through careful component sizing and positioning which have been shown to improve patella
tracking. These include avoiding over-stuffing,
dome shaped patella button, lateralised and
externally rotated femoral component and a lateral arthrotomy in valgus osteoarthritis. In difficult exposures we prefer a tibial tubercle
osteotomy (TTO) as this avoids injury to
quadriceps and the superior geniculate vessels
which can occur with a V–Y turn-down or
quadriceps snip.
2.4 Surgical Management
Asymptomatic cases can be managed nonoperatively with a period of activity modification, monitoring with serial clinical examination
for the presence of an extensor lag and x-rays for
J. Shatrov et al.
fragmentation or fracture. However in the case of
unbearable symptoms, extensor lag, component
loosening or fragmentation surgical intervention
is indicated.
2.4.1 Allograft
In cases of discontinuity of the extensor apparatus, extensor mechanism allograft replacement is
required. Our preference is to perform a complete
extensor mechanism replacement including a
tibial tuberosity bone block, patellar tendon,
patella and quadriceps tendon. Brown et al. have
reported outcomes following complete extensor
mechanism allograft at 10 years, reporting a
failure rate of 38% [8]. For patients not meeting
the criteria for extensor mechanism allograft,
bracing, knee arthrodesis or patellectomy with
muscle transfer are alternative options. A surgical technique for extensor mechanism allograft
reconstruction in TKA is described at the end of
this section.
2.4.2 Muscle Transfer
Transfer of the vastus medialis, vastus lateralis,
and medial head of the gastrocnemius muscle can
be used to fill the defect caused by loss of the
patella and extensor tendon mechanism after
failure and removal of allograft material. However only short—term results have been reported
with this technique and it is generally considered
a salvage procedure after failed reconstruction
[50].
2.4.3 Patellectomy
Patellectomy may be indicated in such cases
where reconstruction of allograft is not possible
(infection, inability to adhere to post-operative
protocol) however it must be recognised that this
reduces the quadriceps strength by 50%, requires
at least 15% more force to straighten the knee and
may result in a progressive recurvatum in a nonconstrained prosthetic knee [49]. Change et al.
followed up 8 patients with unsalvageable patella
fractures with TKA up at 49 months who were
treated with patellectomy. Whilst pain relief was
achieved, 2 could not use stairs, two had quadriceps failure and 50% had an extensor lag [13].
Extensor Mechanism Complications After Total Knee Arthroplasty
2.5 Extensor Mechanism Allograft
Replacement
Contraindications
1. Active infection or repeated unsuccessful
staged re-implantation surgeries with
infection
2. Inability to comply with post-operative
immobilisation (3 months leg in extension)
and rehabilitation
Pre-operative planning
• Fresh frozen, non-irradiated extensor mechanism allograft is available which matches the
affected side
• 10 cm’s of quadriceps tendon is necessary for
sufficient soft tissue fixation and overlap with
the host tissue
• If the allograft tibia is not delivered in its
entirety, a minimum 6 cm of tuberosity bone
length must be available for sufficient distal
fixation
• The allograft should be inspected and deemed
appropriate prior to the patient entering the
operating room
• A constrained prosthesis may be required to
avoid delayed recurvatum and graft failure
377
• Allograft is made slightly larger than the host
insertion site since it can be easily trimmed
down to obtain a press-fit at the time of
insertion. The patellar tendon must be carefully protected during harvest, so it is not
damaged by the oscillating saw
• The host tibial tubercle trough is sized
appropriately and outlined on the anterior
tibial cortex.
• Proximal portion of the tubercle is dovetailed
in a distal/anterior to proximal posterior
fashion, just proximal to the patellar tendon
insertion. The dovetail is outlined with a pen
in a 30–40° angle with a 20–25 mm length.
The allograft is securely stored until ready for
implantation (Fig. 1).
• We recommend a graft that has the following
dimensions
• Quadriceps tendon −10 cm
• Patella—minimum 40 mm in diameter and
25 mm in thickness
• Patellar tendon minimum 50 mm in length
• Tibial tuberosity
• Minimum 6 cm in length, minimum 2 cm in
diameter proximally and distally with 15 mm
thickness
The graft is cleared of any remnant muscle
fibres leaving the quadriceps tendon, patella
tendon, patella and tibial tuberosity intact. The
graft is than fashioned to create two long strips of
quads tendon with a whip stitch (Fig. 2).
The critical step of the trough preparation is to
leave a 1.5 cm bridge proximally to prevent graft
escape, with a so called dove-tail technique. This
is measured and then a small sagittal saw and
lombotte are used to create the desired dimensions to receive the graft. A small medialization
or change in length may be achieved by manipulating placement of the trough. The patella
height should be checked prior to completion of
the trough (Fig. 3).
The tibial tuberosity is first fixed with two
large fragment screws. Each limb of the graft is
then pulvertaft weaved into the quads tendon and
then stitched in extension (Fig. 4).
The patient is managed for minimum
12 weeks locked in extension followed by
graduated flexion. It is critical not to bend the
knee once final fixation and tensioning of the
graft has been achieved.
Graft Preparation
Take home messages
• The tibial tubercle of the allograft is carefully
measured to dimensions of approximately
56 cm of length, 2 cm wide, and 2 cm depth
• Patella osteonecrosis following TKA is a rare
complication
Graft sizing
378
Fig. 1 Whole extensor mechanism allograft preparation
Fig. 2 Tibial preparation for extensor mechanism allograft placement
J. Shatrov et al.
Extensor Mechanism Complications After Total Knee Arthroplasty
379
Fig. 3 Fixation of the extensor mechanism
• Etiology related to multiple incisions disrupting the blood supply as well as remnant
thickness of the patella
• Management is usually non-surgical
• Surgical options vary and are considered salvage options.
3
Patella Clunk Syndrome
3.2 Anatomical Considerations
Patella clunk occurs when a discrete fibrosynovial nodule forms between the superior pole of
the patella and the undersurface of the quadriceps
tendon and becomes entrapped within the intercondylar box of the PS femoral component during knee flexion. Subsequently, when the knee is
extended within 30–45° of full extension, the
nodule dislodges resulting in an audible and
often painful clunk [28].
3.1 Definition and Epidemiology
Patella clunk is a palpable sound which may
range from a painless subtle crepitation to a
painful, catching or audible clunk of the patella
that occurs typically in the range of 20°–45°
flexion [17]. Diagnosis is clinical and it typically
presents 3–12 months post-surgery.
Patella clunk syndrome has been reported in
both CR and PS designed prosthesis and has an
incidence of 0%–18 [17, 28].
3.3 Risk Factors
3.3.1 Prosthesis Type
Most reports are with the use of a PS constrained
implant and this is the greatest risk-factor. PS
femoral prosthesis have a relatively higher trochlear transition zone from the groove of the
prosthesis to the intercondylar box that is
hypothesised to result in increased contact of the
380
J. Shatrov et al.
Fig. 4 Post operatively
distal quadriceps tendon compared to other
prosthesis designs. This is believed the subsequent soft tissue irritation, fibrous hyperplasia
and subsequent clunk [15].
3.3.4 Elevation of the Joint Line
Joint line elevation of more than 8 mm has been
shown to create patella baja that can produce
patella clunk syndrome [21].
3.3.2 Prosthesis Design
PS prosthesis with an intercondylar box ratio of
less than 0.7 have been reported to have no
incidence of patellar clunk [23].
3.3.5 Surgical Technique
Inadequate synovial tissue removal at the junction between the quadriceps tendon and the
superior pole of the patella may also be associated with patella clunk syndrome [26].
3.3.3 Prosthesis Placement
A proximal placement of the patella button,
causing impingement on the quadriceps tendon
[26].
3.4 Surgical Management
Management is ideally non-surgical. In approximately 20–50% of cases resolution occurs with
Extensor Mechanism Complications After Total Knee Arthroplasty
conservative treatment, reassurance and occasionally targeted corticosteroid injection [28].
Arthroscopic debridement of the fibrous nodule
has a success rate of over 80% [32]. In refractory
cases, or cases where arthroscopy is not possible
open peripatellar synovectomy has been shown
to successfully treat clunk syndrome although is
a more morbid procedure than arthroscopic
resection [41].
Take home messages
• Patella clunk syndrome is a clinical diagnosis
• Syndrome is strongly associated with PS
design femoral implants
• 20–50% will
management
resolve
with
non-surgical
• Arthroscopic removal of the fibrous nodule
has a high success rate.
4
Patella Tendon Rupture in Total
Knee Arthroplasty
4.1 Definition and Epidemiology
Patella tendon rupture following TKA is a rare
but devastating complication, occurring in less
than 1% of primary knee arthroplasties. Rupture
can occur intra-operatively or post-operatively.
4.2 Anatomical Considerations
Patella tendon rupture most commonly occurs as
an avulsion from its insertion at the tibial tubercle. A mid-substance tear is less common. The
majority of the patellar tendon fascicles attach to
the distal two thirds of the anterior surface of the
patella, with 60% of their fibres inserting lateral
to the apex of the inferior pole of the patella. It is
thin and flat, tapering slightly distally and being
an average of 6.5 cm in length [4].
381
4.3 Risk Factors
4.3.1 Difficult Exposure
Difficult exposure is the most commonly sited
reason for patella tendon injury intra-operatively
[44]. Situations associated with difficult exposure
include obesity, revision surgery, pre-operative
stiffness and heterotopic ossification and patella
baja.
4.3.2 Previous Tibial Tubercle
Osteotomy
In an early series of patients suffering patellar
tendon injury intra-operatively, nearly half had a
history of previous tibial-tubercle-osteotomy[44].
4.3.3 Joint Line Elevation
Joint line elevation beyond 4 mm is associated
with increased patellofemoral joint contact forces
in walking and during stair climbing [31]. Joint
line elevation typically occurs in revision knee
arthroplasty where there has been distal femoral
bone loss.
4.4 Surgical Management
Surgery should consist of repair with augmentation, reconstruction or replacement. A number of
techniques have been described for augmentation
and reconstruction of patellar tendon ruptures in
TKA. A suggested algorithm[37] that summarises
when these techniques may be used is presented
below (Fig. 5).
4.4.1 Achilles Tendon Allograft
Burnette et al. compared an Achilles tendon
bone-block to a complete extensor mechanism
allograft in 19 patients following TKA and suggested the use of a total extensor mechanism
replacement when the inferior pole of the patella
could not be mobilised to within 2–3 cm of the
joint line [9]. This technique also requires a
stable component and an intact patella in order to
attach the bone block to the tuberosity.
382
J. Shatrov et al.
Fig. 5 Patella tendon rupture in total knee arthroplasty surgical management algorithm
4.4.2 Partial Extensor Mechanism
Allograft Using the ‘HourGlass Technique’
The hourglass variant of the partial allograft
technique is a useful treatment option that can be
used even after patellar resurfacing. An
hourglass-shaped patellar bone block is press-fit
into the native patella. The graft is fixed to both
the patella and the tibia then sutured with the
knee fully extended. Outcomes of this technique
have been reported previously in 5 patients after
at least 24 months’ follow-up. The mean knee
and function Knee Society Scores values were
77.8 and 64.0, respectively. Extension lag was
less than 10 in all 5 patients [22]. The technique
is described later in this section.
4.4.3 Whole Extensor Mechanism
Allograft
Whole extensor mechanism allograft may be
required in cases of chronic patellar tendon rupture when the patella is retracted and cannot be
mobilised to within 1-2 cm of the joint line, or
when bone stock is poor. Both of these situations
are common in this setting. The technique and
outcomes for whole extensor mechanism allograft has been highlighted in an earlier section.
4.4.4 Surgical Technique—Acute
Patellar Tendon Rupture—
Repair
with Semitendinosus
Augmentation
A surgical technique is demonstrated in a
cadaveric dissection below (Figs. 6, 7, 8). Several descriptions of this technique with variations
have been described and published previously
[10, 29].
A mid-substance patellar tendon disruption is
seen (Fig. 6). The patella can be reduced to its
natural position. The semitendinosus tendon is
harvested and detached (Fig. 7). Both free ends
are subsequently whip stitched to facilitate
passing through tunnels.
Two transverse tunnels are created using a
4.5 mm drill. The length of the tendon should be
Extensor Mechanism Complications After Total Knee Arthroplasty
383
Fig. 6 Patellar tendon repair with semtitendinosus autograft augmentation
Fig. 7 Tunnel creation for graft
checked prior to creation of the tibial tunnel to
ensure it is long enough.
The graft is shuttled through the tunnels and
sutured to itself once the tendon has been
repaired end-to-end. Alternative options include
leaving the tendon attached to its insertion
medially and fixing it with an anchor fixation on
the lateral tuberosity, or fixation of both free ends
with the use of anchors.
384
J. Shatrov et al.
Fig. 8 Graft passage and tendon repair
4.4.5 Surgical Technique for Chronic
Patellar Tendon Rupture—
Reconstruction
with a PartialExtensor
Mechanism Allograft—The
“Hour-Glass” Technique
(Fig. 9)
The allograft patella is cut in the coronal plane
to remove the cartilage-covered aspect. The
remaining bone is then cut into an hourglass
shape and press-fit into a groove fashioned in the
native patella (see below). An hourglass shape
that is identical to the shape of the groove in the
patella is critical to ensure primary stability.
A metallic wire 1.2 mm in diameter is threaded
distally through the tibial bone block, which
measures about 6 cm (Fig. 10).
A partial extensor mechanism is fashioned in
the shape of an hour glass being 12 mm wide at
its thinnest point in the patella trough. The tibial
tuberosity bone block is 2 cm wide proximally
and 12 mm wide distally, with a length of 6 cm.
Troughs are created in the patella and tibial
tuberosity to receive the allograft. The patellar
bone block is press-fit into the patellar groove
and firmly fixed using the metallic wire. Primary
stability is enhanced by the hourglass shape of
the bone block, and most of the tendon attachments are preserved. In addition to primary stability, the metallic wires and proximal fixation to
the quadricipital tendon combine to prevent
migration of the patellar bone block (Fig. 11).
The graft is fixed distally with 2–3 cortical
screws and the quadriceps tendon end of the graft
is then pulvertaft weaved through the native
quadriceps tendon with the leg held in extension.
Post operatively the patient is managed with the
knee locked in strict extension for a minimum of
8 weeks followed by a period graduated flexion
Extensor Mechanism Complications After Total Knee Arthroplasty
385
Fig. 9 Chronic patellar
tendon rupture reconstruction
using partial extensor
mechanism allograft—‘Hourglass’ technique
with monitoring via serial x-rays and clinical
examination.
5
Take home messages
5.1 Definition and Epidemiology
• Patellar tendon rupture following TKA is
difficult problem to treat
• Usually occurs as a result of difficult exposure
and revision surgery
• Acute rupture may be repairable, however we
advise augmentation due to high rates of
failure with primary repair
• Chronic ruptures require salvage reconstructive procedures, with allograft options providing the most reliable results in our
institution´s experience.
The rate of quadriceps tendon rupture following
TKA is low, being reported to be 1- 0.1%, with
partial tears being more common than complete
disruption [20, 33].
Quadriceps Tendon Rupture
5.2 Risk Factors
Systemic disorders, that weaken soft tissues,
excessive resection of the patella, lateral release
and a prior quadriceps snip or V–Y turndown
have all been associated with quadriceps tendon
386
J. Shatrov et al.
Fig. 10 Graft and host preparation
rupture in TKA suggesting the aetiology is likely
multifactorial [20, 33, 41].
5.3 Surgical Management
A management algorithm adapted from one
suggested by Nam et al. is presented below that
summarises management of quadriceps tendon
injury in TKA (Fig. 12) [36]. Partial tears can be
managed successfully with non-operative management [20]. When surgery is indicated, primary repair is associated with a high failure rate
(30–100%) thus augmentation with a biological
or synthetic augment is recommended. Augmentation for repairs or quads tendon injuries has
similarly been described using fascia lata and
Achilles tendon allograft, muscle transfer using
sartorius, allograft, hamstring reconstruction and
synthetic material.
Take home messages
• A similar approach for patellar tendon ruptures can be followed for Quadriceps tendon
ruptures
• Non-surgical management for partial injuries
with a minimal lag have good results
• Primary repair should be augmented.
6
Periprosthetic Patella Fracture
6.1 Definition and Epidemiology
The rate of periprosthetic patellar fracture following total knee arthroplasty ranges from 0.68%
to 5.2%, however the rate in unresurfaced patella
is 0.05% [11].
Extensor Mechanism Complications After Total Knee Arthroplasty
387
• II—intact implant but extensor mechanism
disruption
• IIIa—loose implant, with good patellar bone
stock
• IIIb—loose implant, with poor patellar bone
stock.
6.3 Risk Factors
Patient factors
• BMI greater than 30 6.3-fold and 1.7-fold
increases in the risk of loosening and fracture
[35].
• Pre-operative thickness of <18 mm has been
shown to be a risk factor for fracture [24].
• Osteoporosis [36].
• Loosening − 50% of patella fractures have
loosening of the component [37].
Surgical technique factors
• Resurfacing the patella—Unresurfaced patella
have a rate of fracture that is 0.05% (significantly lower than resurfaced patella)
• Lateral release increases 2.7 times the risk for
patella fracture [35].
Fig. 11 Graft fixation and post-operative management
6.2 Anatomical Considerations
Rather than considering the fractured region of
the patella, it is more useful to consider the stability of the implant, the continuity of the extensor mechanism and the remaining bone stock.
Patella fractures can be classified in multiple
ways. The most commonly quoted system was
reported by Ortiguera and Berry [40].
• I—a stable implant and intact extensor
mechanism
• Residual remnant bone thickness for the
patella is recommended to be at least 12 mm
of initial thickness. However results are
inconclusive with some studies showing a
higher rate of fracture < 12 mm [35], and
others no difference [24].
Patella design
• In a study of cementless implants with a
porous tantalum anchoring surface a 20% 2year fracture rate was observed in a study of
30 patients [12].
• Fixation with a single central peg has been
suggested to increase the risk of fracture [35].
388
J. Shatrov et al.
Fig. 12 Algorithm for surgical management of quadriceps tendon rupture following total knee arthroplasty
Fig. 13 Treatment algorithm outlining the management of periprosthetic patellar fracture following total knee
arthroplasty. (Reproduced from: Parker DA, Dunbar MJ, Rorabeck CH. Extensor mechanism failure associated with
total knee arthroplasty: prevention and management. J Am Acad Orthop Surg. 2003 Jul–Aug;11(4):238–47)
6.4 Surgical Management
A management algorithm [41] that is commonly
quoted in the management of periprosthetic
patella fractures is shown above (Fig. 13).
Regardless of management options, complications rate is high when the extensor mechanism is
disrupted. We present a case where the extensor
mechanism has been augmented with a biological semitendinosus autograft. Case details are
provided below.
Type 1—Non-operative management. Good
results [40].
Extensor Mechanism Complications After Total Knee Arthroplasty
389
Fig. 14 Pre-operative x-rays
demonstrating malunited
patella fracture with severe
tricompartmental arthrosis
Type 2–42% reoperation rate, 50% complication
rate, and 58%prevalence of extensor lag postoperatively [11].
Type 3—reoperation rate of 20% and an overall
complication rate of 45% [11].
6.5 Case Example
Images and x-rays of an 82 year old gentleman
who initially presented to our service with a
painful stiff knee after a previous patella fracture
(Fig. 14). Pre-operatively he had a total range of
20°, with a 20° fixed-flexion deformity and only
able to flex to a maximum of 40°. He subsequently
underwent a TKA (Fig. 15) with a rotating hinge
prosthesis with a TTO for exposure which was
uneventful. 3 months following the surgery he fell
and these are his radiographs (Fig. 16).
X-ray following a fall demonstrating a transverse periprosthetic patella fracture and the post
for the hinge mechanism can be seen dislodged
on the lateral view indicating that the post
mechanism was ‘jumped’ during the hyperflexion of the knee during the fall (Fig. 16).
Intra-operative images demonstrating the
prosthesis dislocated in deep flexion as the piston
has ‘jumped’ out of the polyethelene. The patella
390
J. Shatrov et al.
Fig. 15 Post-operative xrays showing an all-cemented
hinge-prosthesis with a
resurfaced patella. Note a
TTO has been performed to
facilitate exposure
post fixation with tension band wire. Note the
extensor mechanism has been augmented with a
semi-tendinosus autograft which has been left
attached to its insertion at the pes anserinus,
tunnel through the patella using a 6 mm transverse tunnel in the superior half and fixed back to
the tibia using the screw from the TTO and a
suture anchor (Fig. 17).
Post op-operative x-rays (Fig. 18) demonstrating patella fracture fixation with a tension
band wire. Note the post of the rotating hinge is
now reduced in the correct position and an
anchor can be seen just below the tibial plateau
on the lateral view. Intra-operatively the patella
prosthesis was noted to be stable and well fixed.
Take home messages
• The critical factors determining management
of patella fractures are the stability of the
implant, the integrity of the extensor mechanism and the quality of the bone-stock
• Surgical management has a high complication
rate
• Augmentation of the extensor mechanism is a
good option to protect internal fixation.
Extensor Mechanism Complications After Total Knee Arthroplasty
391
Fig. 16 Periprosthetic patella
fracture with a dislocated
hinge
7
Patellar Instability in Total Knee
Arthroplasty
7.1 Definition and Epidemiology
Patellofemoral instability (PFI) following TKA is
an uncommon but devastating complication with
incidence ranging from 0.5 to 0.8% [43, 45]. It is
defined as either subluxation or dislocation of the
patella on the femoral component (Fig. 19).
7.2 Risk Factors
Aetiology of PFI following TKA is either
implant, soft tissue related or a combination of
both. The most frequently cited cause is femoral
or tibial component internal rotation [1, 2, 48],
and when present, revision arthroplasty is
recommended [34, 48]. What defines the
threshold for malrotation has not been clearly
defined.
7.2.1 Femoral Component Rotation
Determining the threshold for femoral and tibial
malrotation is difficult. Post-operatively, the PCA
is no longer available for femoral referencing
and therefore most studies have described using
the TEA as a landmark to measure femoral component positioning on CT scans [6, 14]. We set a
threshold to define malrotation of the femoral
component TEA as more than 6° of IR. This is
based on the observation that the PCA is 3.5° to
0.3° IR to the TEA in a normal population [6].
7.2.2 Tibial Rotation
Tibial rotation malrotation is also not well
defined, with variations in definitions and
thresholds varying. Typically the most prominent
392
J. Shatrov et al.
Fig. 17 Intra-operative findings and extensor mechanism augmentation
point or medial third of the tibial tuberosity is
used as a reference point, however it has previously been shown that the interobserver measurement disagreement is more than 3° in 70% of
cases [27]. We set a threshold for tibial rotation
of 20° according to the technique described by
Berger et al. which utilises the most prominent
point of the tibial tuberosity. Using this technique
a range of 18° ± _2.6° was described as a limit.
An inherent issue with measuring tibial rotation
however is the wide variation in the position of
the tibial tuberosity which has previously been
described [16].
7.3 Surgical Management
7.2.3 Femoral-Tibial Rotation
For combined femoral-tibial mal-rotation we set
a limit no more than 3º. Previously it has been
observed that 3°–8° of combined internal rotation
was associated with PFI in TKA [5].
Tibial Tubercle Osteotomy
When implant position is satisfactory, addressing
the soft tissue imbalance is required. The medial
patellofemoral ligament (MPFL) prevents the
patella from subluxing laterally and keeps it
within the trochlear groove in early flexion [18].
Reconstruction of the MPFL has been used
successfully in the treatment of lateral patella
instability in the native knee [3, 7, 19].
A management algorithm is described below
(Fig. 20) and a surgical technique for MPFLr and
TTO at the end of this section.
• TTO should be performed in the following
situations:
• Grade 3 J-sign
Extensor Mechanism Complications After Total Knee Arthroplasty
393
Fig. 18 Post-operatively
• Chronic patella dislocation
• Severe quadriceps shortening or severe patella
baja.
7.3.1 Technique
The TTO is performed using an oscillating saw
to create an osteotomy that is 6 cm in length, 1.5cm deep proximally, tapered distally and hinged
open leaving the lateral side attached to soft tissues. TTO is fixed using two 3.5 mm cortical
screws, or in cases of thin bone, transosseous
cerclage wires can be utilised. Medialisation is
performed up to 10 mm, or until correction of the
J-sign and proximalisation in cases of quadriceps
shortening or severe patella baja. 1.5 cm bone
bridge is preserved proximally to avoid conflict
with the tibial tray.
7.3.2 Medial Patellofemoral Ligament
Reconstruction
A medial sub-vastus approach is performed and
extended if necessary for a TTO. The MPFLr is
performed using a quadriceps tendon autograft
taken from the medial 1/3 of the quadriceps
tendon, leaving the patella attachment undisturbed (Fig. 21).
The graft is whip stitched and passed beneath
the vastus medialis muscle. Next, a femoral
tunnel is drilled starting from the femoral footprint of the MPFL [46] aiming for the metadiaphyseal junction laterally.
Due to the observation of poor bone quality in
the supracondylar region of the femur, an additional cortical fixation is added with the use of an
endobutton. The graft is tensioned with the knee
flexed to approximately 30°- 45° and fixed with
an interference screw but a cortical button is
added laterally to avoid graft slippage (Figs. 22
and 23).
Post operatively the patient is placed into a
range-of-motion knee brace that allows a range
of movement from 0 to 90 degrees flexion. The
patient can fully-weight bear with the brace
locked in full extension. Follow-up consultation
at 6 and 12 weeks is performed with x -rays to
look at patella height, tilt and translation. If a
394
J. Shatrov et al.
A
C
B
Fig. 19 Patellar instability post total knee arthroplasty. Patient with dislocated patella post TKA. A. AP image, B, skyline view and C lateral view
Fig. 20 Suggested management algorithm for patella instability post total knee arthroplasty
Extensor Mechanism Complications After Total Knee Arthroplasty
Fig. 21 Graft harvest and passage
Fig. 22 Tunnel placement and graft double-fixation
395
396
J. Shatrov et al.
A
B
C
Fig. 23 Post MPFLr using double fixation with tibialtubercle-osteotomy. Post-operative x-rays of the patient
from Fig. 19 taken at 12 post-surgery. A. Sky-line view
demonstrating the patella now centered with a patellar tilt
of 6°. B. AP x-ray, the endobutton can be seen sitting
flush on the lateral cortex. C. Lateral profile demonstrating the tibial-tubercle osteotomy and tunnel position. The
osteotomy is united at 3 months post surgery
Extensor Mechanism Complications After Total Knee Arthroplasty
TTO is performed, x-rays are taken until radiographic union is achieved which is usually
12 weeks after surgery.
4.
Take home messages
• Surgery for patellar instability post TKA
either requires revision of components or a
soft tissue procedure, plus or minus a TTO.
• MPFL reconstruction in this population
should utilise a quadriceps tendon autograft.
• Double fixation of the graft that is reinforced
with a cortical button should be used due to
the typically poor bone quality in this region
post TKA.
5.
8
8.
Summary
Extensor mechanism complications following
TKA are common. Fortunately, those with the
most severe impact on the patient are rare,
however their management is difficult and in
many circumstances is considered salvage surgery. Knowledge regarding the relevant anatomy
and risk factors for these main complications will
assist surgeons in avoiding them. Algorithms to
guide management decisions and inform treatment thresholds are presented based on our
institution’s experience and the best available
literature. Furthermore, several surgical techniques are described for various extensor mechanism complications.
6.
7.
9.
10.
11.
12.
13.
References
14.
1. Akagi M, Matsusue Y, Mata T, Asada Y,
Horiguchi M, Iida H, et al. Effect of rotational
alignment on patellar tracking in total knee arthroplasty. Clin Orthop Relat Res. 1999. https://doi.org/
10.1097/00003086-199909000-00019155-163.
2. Anouchi YS, Whiteside LA, Kaiser AD, Milliano MT. The effects of axial rotational alignment
of the femoral component on knee stability and
patellar tracking in total knee arthroplasty demonstrated on autopsy specimens. Clin Orthop Relat Res.
1993:170–177.
3. Astur DC, Gouveia GB, Borges JH, Astur N,
Arliani GG, Kaleka CC, et al. Medial patellofemoral
15.
16.
397
ligament reconstruction: a longitudinal study comparison of 2 techniques with 2 and 5-years follow-up.
Open Orthop J. 2015;9:198–203.
Basso O, Johnson DP, Amis AA. The anatomy of the
patellar tendon. Knee Surg Sports Traumatol
Arthrosc. 2001;9:2–5.
Berger RA, Crossett LS, Jacobs JJ, Rubash HE.
Malrotation causing patellofemoral complications
after total knee arthroplasty. Clin Orthop Relat Res.
1998. https://doi.org/10.1097/00003086-19981100000021144-153.
Berger RA, Rubash HE, Seel MJ, Thompson WH,
Crossett LS. Determining the rotational alignment of
the femoral component in total knee arthroplasty
using the epicondylar axis. Clin Orthop Relat Res.
1993:40–47.
Bouras TUE, Brown A, Gallacher P, Barnett A.
Isolated medial patellofemoral ligament reconstruction significantly improved quality of life in patients
with recurrent patella dislocation. Knee Surg Sports
Traumatol Arthrosc. 2019;27:3513–3517.
Brown NM, Murray T, Sporer SM, Wetters N,
Berger RA, Della Valle CJ. Extensor mechanism
allograft reconstruction for extensor mechanism
failure following total knee arthroplasty. J Bone Joint
Surg Am. 2015;97:279–83.
Burnett RS, Butler RA, Barrack RL. Extensor
mechanism allograft reconstruction in TKA at a
mean of 56 months. Clin Orthop Relat Res.
2006;452:159–65.
Cadambi A, Engh GA. Use of a semitendinosus
tendon autogenous graft for rupture of the patellar
ligament after total knee arthroplasty. A report of
seven cases. J Bone Joint Surg Am. 1992;74:974–9.
Chalidis BE, Tsiridis E, Tragas AA, Stavrou Z,
Giannoudis PV. Management of periprosthetic patellar fractures. A systematic review of literature Injury.
2007;38:714–24.
Chan JY, Giori NJ. Uncemented metal-backed
tantalum patellar components in total knee arthroplasty have a high fracture rate at midterm follow-up.
J Arthroplasty. 2017;32:2427–30.
Chang MA, Rand JA, Trousdale RT. Patellectomy
after total knee arthroplasty. Clin Orthop Relat Res.
2005;440:175–7.
Chauhan SK, Clark GW, Lloyd S, Scott RG, Breidahl W, Sikorski JM. Computer-assisted total knee
replacement. A controlled cadaver study using a
multi-parameter quantitative CT assessment of alignment (the Perth CT Protocol). J Bone Joint Surg Br.
2004;86:818–23.
Clarke HD, Fuchs R, Scuderi GR, Mills EL,
Scott WN, Insall JN. The influence of femoral
component design in the elimination of patellar
clunk in posterior-stabilized total knee arthroplasty.
J Arthroplasty. 2006;21:167–71.
Cobb JP, Dixon H, Dandachli W, Iranpour F. The
anatomical tibial axis: reliable rotational orientation
in knee replacement. J Bone Joint Surg Br.
2008;90:1032–8.
398
17. Conrad DN, Dennis DA. Patellofemoral crepitus
after total knee arthroplasty: etiology and preventive
measures. Clin Orthop Surg. 2014;6:9–19.
18. Dandy DJ. Chronic patellofemoral instability. J Bone
Joint Surg Br. 1996;78:328–35.
19. Deie M, Ochi M, Sumen Y, Adachi N, Kobayashi K,
Yasumoto M. A long-term follow-up study after
medial patellofemoral ligament reconstruction using
the transferred semitendinosus tendon for patellar
dislocation. Knee Surg Sports Traumatol Arthrosc.
2005;13:522–8.
20. Dobbs RE, Hanssen AD, Lewallen DG, Pagnano MW. Quadriceps tendon rupture after total
knee arthroplasty. Prevalence, complications, and
outcomes. J Bone Joint Surg Am. 2005;87:37–45.
21. Figgie HE 3rd, Goldberg VM, Heiple KG, Moller HS
3rd, Gordon NH. The influence of tibialpatellofemoral location on function of the knee in
patients with the posterior stabilized condylar knee
prosthesis. J Bone Joint Surg Am. 1986;68:1035–40.
22. Fiquet C, Schneider A, Ballis R, Servien E, Neyret P,
Lustig S. Reconstructing the chronically disrupted
knee extensor mechanism after total knee arthroplasty: hourglass variant of the original partial
allograft technique. Orthop Traumatol Surg Res.
2017;103:1197–200.
23. Fukunaga K, Kobayashi A, Minoda Y, Iwaki H,
Hashimoto Y, Takaoka K. The incidence of the
patellar clunk syndrome in a recently designed
mobile-bearing posteriorly stabilised total knee
replacement. J Bone Joint Surg Br. 2009;91:463–8.
24. Hamilton WG, Ammeen DJ, Parks NL, Goyal N,
Engh GA, Engh CA Jr. Patellar cut and composite
thickness: the influence on postoperative motion and
complications in total knee arthroplasty. J Arthroplasty. 2017;32:1803–7.
25. Healy WL, Wasilewski SA, Takei R, Oberlander M.
Patellofemoral complications following total knee
arthroplasty. Correlation with implant design and
patient risk factors. J Arthroplasty. 1995;10:197–201.
26. Hozack WJ, Rothman RH, Booth RE, Jr., Balderston RA. The patellar clunk syndrome. A complication of posterior stabilized total knee arthroplasty.
Clin Orthop Relat Res. 1989:203–208.
27. Indelli PF, Graceffa A, Marcucci M, Baldini A.
Rotational alignment of the tibial component in total
knee arthroplasty. Ann Transl Med. 2016;4:3.
28. Ip D, Ko PS, Lee OB, Wu WC, Lam JJ. Natural
history and pathogenesis of the patella clunk syndrome. Arch Orthop Trauma Surg. 2004;124:
597–602.
29. Jarvela T, Halonen P, Jarvela K, Moilanen T.
Reconstruction of ruptured patellar tendon after total
knee arthroplasty: a case report and a description of
an alternative fixation method. Knee. 2005;12:
139–43.
30. Kirschner MH, Menck J, Nerlich A, Walser R,
Buhren V, Hofmann GO. The arterial blood supply
of the human patella. Its clinical importance for the
J. Shatrov et al.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
operating technique in vascularized knee joint transplantations. Surg Radiol Anat. 1997;19:345–51.
Konig C, Sharenkov A, Matziolis G, Taylor WR,
Perka C, Duda GN, et al. Joint line elevation in
revision TKA leads to increased patellofemoral
contact forces. J Orthop Res. 2010;28:1–5.
Lucas TS, DeLuca PF, Nazarian DG, Bartolozzi AR,
Booth RE, Jr. Arthroscopic treatment of patellar
clunk. Clin Orthop Relat Res. 1999;226–229.
Lynch AF, Rorabeck CH, Bourne RB. Extensor
mechanism complications following total knee
arthroplasty. J Arthroplasty. 1987;2:135–40.
Malo M, Vince KG. The unstable patella after total
knee arthroplasty: etiology, prevention, and management. J Am Acad Orthop Surg. 2003;11:364–71.
Meding JB, Fish MD, Berend ME, Ritter MA,
Keating EM. Predicting patellar failure after total
knee arthroplasty. Clin Orthop Relat Res.
2008;466:2769–74.
Nam D, Abdel MP, Cross MB, LaMont LE, Reinhardt KR, McArthur BA, et al. The management of
extensor mechanism complications in total knee
arthroplasty. AAOS exhibit selection. J Bone Joint
Surg Am. 2014;96:e47.
Ng J, Balcells-Nolla P, James PJ, Bloch BV. Extensor mechanism failure in total knee arthroplasty.
EFORT Open Rev. 2021;6:181–8.
Nicholls RL, Green D, Kuster MS. Patella intraosseous blood flow disturbance during a medial or
lateral arthrotomy in total knee arthroplasty: a laser
Doppler flowmetry study. Knee Surg Sports Traumatol Arthrosc. 2006;14:411–6.
Noh JH, Roh YH. Osteonecrosis of bipartite patella
following total knee arthroplasty without lateral
release. Acta Orthop Traumatol Turc. 2019;53:74–6.
Ortiguera CJ, Berry DJ. Patellar fracture after total
knee arthroplasty. J Bone Joint Surg Am.
2002;84:532–40.
Parker DA, Dunbar MJ, Rorabeck CH. Extensor
mechanism failure associated with total knee arthroplasty: prevention and management. J Am Acad
Orthop Surg. 2003;11:238–47.
Pawar U, Rao KN, Sundaram PS, Thilak J, Varghese J. Scintigraphic assessment of patellar viability in
total knee arthroplasty after lateral release. J Arthroplasty. 2009;24:636–40.
Rand JA. The patellofemoral joint in total knee
arthroplasty. J Bone Joint Surg Am. 1994;76:612–20.
Rand JA, Morrey BF, Bryan RS. Patellar tendon
rupture after total knee arthroplasty. Clin Orthop
Relat Res. 1989;233–238.
Scuderi GR, Insall JN, Scott NW. Patellofemoral
pain after total knee arthroplasty. J Am Acad Orthop
Surg. 1994;2:239–46.
Servien E, Fritsch B, Lustig S, Demey G, Debarge R,
Lapra C, et al. In vivo positioning analysis of medial
patellofemoral ligament reconstruction. Am J Sports
Med. 2011;39:134–9.
Extensor Mechanism Complications After Total Knee Arthroplasty
47. Theodorou DJ, Theodorou SJ, Farooki S, Kakitsubata Y, Resnick D. Osteonecrosis of the patella:
imaging features. Clin Imaging. 2001;25:60–5.
48. Warschawski Y, Garceau S, Frenkel Rutenberg T,
Dahduli O, Wolfstadt J, Backstein D. Revision total
knee arthroplasty for patellar dislocation in patients
with malrotated TKA components. Arch Orthop
Trauma Surg. 2020;140:777–83.
399
49. Watkins MP, Harris BA, Wender S, Zarins B,
Rowe CR. Effect of patellectomy on the function of
the quadriceps and hamstrings. J Bone Joint Surg
Am. 1983;65:390–5.
50. Whiteside LA. Surgical technique: Muscle transfer
restores extensor function after failed patella-patellar
tendon allograft. Clin Orthop Relat Res.
2014;472:218–26.
Surgical Techniques: Why, When
and How I Do It
Sonosurgery Ultrasound-Guided
Arthroscopic Shaving
for the Treatment of Patellar
Tendinopathy When Conservative
Treatment Fails
Ferran Abat and Håkan Alfredson
1
Background
Proximal patellar Tendinopathy, commonly
denominated as Jumper´s Knee, is widely considered to be a challenge to treat [1].
The treatment of patellar tendinopathy focuses
on reducing if not eliminating the pain and
improving function. At present, there are a several distinct treatments oriented to that end, and a
“gold-standard” treatment might be in sight [2].
Conservative treatment of chronic patellar
tendinopathy by means of eccentric quadriceps
training has shown good results [3, 4].
The authors put forward the following treatment protocol for patellar tendinopathy (Fig. 1).
It starts from the correct diagnostic positioning
(Fig. 2) and moves on to physiotherapy, rehabilitation as well as biomechanical and behavioral modification. If that approach fails, we
begin with ultrasound-guided procedures outside
the injured region in the tendon, and sometimes
F. Abat (&)
ReSport Clinic Barcelona. Blanquerna-Ramon Llull
University School of Health Science. Rosselló, 102.
08034 Barcelona, Spain
e-mail: abat@resportclinic.com
H. Alfredson
Department of Community Medicine and
Rehabilitation, Sports Medicine, Umeå University,
901 87 Umeå, Sweden
e-mail: hakan.alfredson@umu.se
end with an ultrasound-guided arthroscopic
shaving procedure (Fig. 3).
Conservative treatment should initially consist
of physiotherapy and rehabilitation that progresses with inertial eccentric exercises. Other
functional rehabilitation processes should also be
relied upon [5]. The key for the correct analysis
of the patients will be the biomechanical study of
the patient [6].
Ultrasound-guided electrolysis or USGET
(Ultrasound-Guided Galvanic Electrolysis Technique) is considered when the tendon is in the
chronic phase and physiotherapy treatment has
not been sufficient [1, 2]. This technique makes
use of 0.3 mm acupuncture needles through
which a galvanic current is directed to the injured
area of the tendon (Fig. 4). This technique should
always be utilized under strict ultrasound control
and with the help of local anesthesia to control
pain. USGET acts on the biology of the tendon
that is damaged and that does not heal on its
own. It destroys the degenerating tissue and
triggers the biological response necessary for
repair. In other words, it causes a key inflammatory response in the biological process of
tendon collagen repair [7]. However, causing
inflammation and a biological process to repair
collagen is pointless if it is not done in combination with the application of active work that
correctly directs tendon repair. Therefore, it is
essential that this technique be partnered with
good mechanical stimulus planning.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_26
403
404
F. Abat and H. Alfredson
Fig. 1 Treatment algorithm proposed by the authors
according to the ReSport Clinic methodology for patellar
tendinopathy. Initially, the diagnosis is made by ultrasound, which can be supported by magnetic resonance
imaging (MRI). The conservative physiotherapy protocol
is started as well as the modification of sports and
biomechanical habits. If the result is not satisfactory,
treatment proceeds with ultrasound-guided galvanic electrolysis (USGET) under local anesthesia with or without
platelet-rich plasma support. In the case of hypervascularization, high-volume infiltrations or polidocanol can be
used (the latter is the authors’ preferred option). If this
does not improve the patient's symptoms, sonosurgery is
performed
USGET is non-thermal electrochemical ablation with a cathodic flow to the clinical focus of
tendon degeneration. The treatment brings on a
dissociation of the H2O, salts and amino acid
components, those elements that create new
molecules through ionic instability, of the
extracellular matrix. The organic reaction that is
induced in the tissue encircling the cathodic
needle gives rise to a localized inflammation in
the area to be treated [7]. An immediate activation of an inflammatory response and overexpression of the activated gamma receptor for
peroxisome proliferation (PPAR-gamma) is produced. Moreover, the action of IL-1, TNF and
COX-2, which are mechanisms of tendon
degeneration, are affected by USGET through its
direct inhibitory effect and thereby facilitates
phagocytosis and tendon regeneration [7]. The
application of USGET stimulates the production
of new immature collagen fibers that come to
maturity through eccentric stimulus (Abat et al.
2015). With that application, excellent results are
obtained in the short- and long-term in terms of
pain and function. It must be said that using this
technique without mechanical stimuli results in a
significant loss of the biological effect.
The introduction of Platelet Rich Plasma
(PRP) is another adjunct to USGET in conservative treatment. It is applied by means of
ultrasound-guided infiltrations in the area of
Sonosurgery Ultrasound-Guided Arthroscopic Shaving …
Fig. 2 High-definition ultrasound image of a proximal
patellar tendinopathy. Longitudinal sect with linear probe.
Note the thickened tendon in its proximal portion in
contact with the patella (double arrow) as well as cortical
405
rarefaction of the patella at the insertion of the tendon. An
important intrasubstance rupture (arrow) and the fibrosis
of Hoffa's fat pad stand out
Fig. 3 Positioning in the
operating room for
sonosurgery on the patellar
tendon. The main surgeon
handles the arthroscopic
instruments while the
assistant shows the ultrasound
image. It is important that the
arthroscopic and ultrasound
screens be viewed
simultaneously during the
procedure
tendon injury. To carry it out, blood must be
drawn from the patient and centrifuged to separate the blood components. Then, the Platelet
Rich Plasma (high concentration of platelets) is
collected from it. The PRP is later pushed into
the injured area to try to bring about a stimulatory response. This response helps to reduce pain
and increase function [2, 8, 9]. Although pain
during treatment and in the days immediately
following it seems to increase considerably, it is
406
F. Abat and H. Alfredson
Fig. 4 Ultrasound-guided
galvanic electrolysis
(USGET) procedure under
local anesthesia. The
ultrasound shows the lesion
area within the patellar tendon
and the 0.3 mm needle of the
USGET handpiece applies the
galvanic current directly to
the focus of the lesion
one of the most valid options among the nonsurgical ones to improve function and alleviate
pain in the long-term. it is advisable to rely on
other treatments such as radiofrequency to
address the intermediate pain, but the administration of anti-inflammatories should be avoided.
Thought must be given to the surgical approach
when the conservative options fail.
The open patellar tenotomy and excision of
the region with tendon changes is quite often
included in traditional surgical treatment. On
occasion, ultrasound-guided percutaneous longitudinal tenotomy, curettage, multiple drilling of
the inferior patellar pole, or excision of the distal
patellar tip are also employed [10–12]. The
aftermath of these treatments is always a relatively long rehabilitation period. The clinical
results of classical surgery vary, and the outcomes are often unsatisfactory [13]. In a randomized study in which treatment with eccentric
quadriceps training was compared to traditional
open tenotomy in combination with excision,
similar results were seen. However, there was
only 50% of good clinical results in both groups
[14].
Over recent years, the question as to where the
pain originates in this case and other chronic
painful tendinopathies has been debated [15]. In
some studies that used Color Doppler Ultrasound
in surgery along with immuno-histochemical
analyses of tendon biopsies, high blood flow
[16] and nerves outside the tendon (on the dorsal
side of the proximal patellar tendon) [17, 18]
have been documented. Very few nerves were
seen inside the tendons if any. A temporary cure
for the pain was observed by injecting a local
anesthetic that targeted the region with high
blood flow and nerves outside the tendon. Those
findings were at the root of the push to develop
new treatment methods like sclerosing polidocanol injections [19] and ultrasound-guided
arthroscopic shaving [20]. They put a focus on
treatment outside the dorsal patellar tendon
where high blood flow and nerves have been
detected. Herein, we describe the newly invented
surgical treatment method.
2
Classification and Preoperative
Evaluation
The deep portion of the proximal insertion of the
patellar tendon supports most of the traction
forces that the tendon must withstand. When the
patient has lived with the patellar tendon injury
for a long time, they generally present with
hypotonic atrophy of the quadriceps muscles.
The pain typical of patellar tendinosis can be
triggered by a sudden and rapid contraction of
the quadriceps.
Sonosurgery Ultrasound-Guided Arthroscopic Shaving …
Historically, the Blazina scale [21] of 1973 is
used to classify the degree of injury. It provides a
qualitative description of the injury. Four injury
gradations can be defined:
• Grade I: Pain during sport
• Grade II: Pain at the start of sports activities
that disappears after warming up and reappears when fatigue comes on.
• Grade III: Pain during and after activity,
making the subject unable to participate further in sports activities.
• Grade IV: Complete tendon rupture.
As regards the duration of symptoms, authors
like Kaux [22] characterize the phases of
tendinopathy as:
• Acute (0–6 weeks)
• Sub-Acute (6–12 weeks)
• Chronic (>3 months)
A diagnosis is necessarily acquired by means
of a thorough clinical examination as well as
supplementary
musculoskeletal
ultrasound
(Echo-MSK) and magnetic resonance imaging
(MRI). The ultrasound image of an injured tendon will show a pattern of fibrillar irregularity
with hypoechoic areas. There may even be
intratendinous lesions. The tendon will be
thickened. Moreover, hypervascularizations that
have their origin in Hoffa’s fat pad may be present. In the insertional portion of the patella,
cortical irregularities can be seen.
3
Indications
It is indicated for patients that have lived with
proximal patellar tendon pain during patellar
tendon loading activity for more than 3 months.
They would have also been diagnosed, both
clinically and with ultra–sound and Doppler or
MRI, with patellar tendinopathy/Jumper’s knee.
Furthermore, conservative treatment would have
failed for them.
407
4
Contraindications
The contraindications include chronic inflammatory diseases, other systematic diseases that
affect the joints and/or connective tissue as well
as concomitant knee injuries (ACL, menisci,
cartilage, fractures).
5
Surgical Technique Using
Ultrasound-Guided Arthroscopy
Sonosurgery [2, 20, 23] has shown good clinical
results. It has few complications and makes for a
decrease in tendon thickness along with better
tendon structure over time. The technique is
based on the use of ultrasound simultaneously
with arthroscopy (Fig. 5), thus making it possible
to work on the injured tendon with total security
by combining the two approaches.
Treatment is currently focused mainly on the
exterior of the patellar tendon, that is, its dorsal
part (Fig. 6). It has been demonstrated that it is
where there is the greatest blood flow and new
nerves are being generated over the course of
tendinopathy.
To start, a thorough ultrasound with Color
Doppler examination is performed (Fig. 7).
Then, the main damaged area of the tendon is
analyzed to determine whether there is a patella
tip causing an imprint on the tendon, a rupture or
involvement of the bursa. Later, an arthroscopic
review of the knee will detect possible associated
injuries.
Although some surgeons prefer to use spinal
anesthesia, surgery can be performed under local
anesthesia. Either option is correct. However, not
tightening the ischemia cuff so that hypervascularizations can be seen with ultrasound during
surgery is imperative.
Put the patient in a supine position with the
knee straight and the quadriceps relaxed. The
procedure is started on the ventral/deep part of
the tendon. A standard antero-medial and anterolateral portal and a controlled pressure pump are
used (Fig. 8).
408
F. Abat and H. Alfredson
Fig. 5 Starting position for
sonosurgery on the patellar
tendon. Direct view of the
tendon under ultrasound and
arthroscopy simultaneously
Fig. 6 Longitudinal view
with linear probe and highdefinition ultrasound of a
proximal patellar
tendinopathy. The shaver can
be visualized in the external
dorsal portion of the tendon,
the starting point of the
arthroscopic procedure
Afterwards, the insertion of the patellar tendon in the patella is identified to initiate
debridement using a synoviotome with a 4.5 mm
full radius. Simultaneous longitudinal and crosssectional ultrasound views guide the entire procedure (Fig. 9). Debridement is carefully performed. The goal being the destruction of only
the high blood flow (neovessels) region and the
nerves adjacent to the tendinosis changes on the
dorsal side of the tendon (i.e., separating the
Hoffa fat pad from the patellar tendon). Healthy
tendon tissue is not resected, and the Hoffa fat
pad should be left untouched as much as
possible.
Should a prominent patella peak be encountered (Fig. 10), the recommendation is to resect it
with caution. The tendon must be well explored
in search of intratendinous tears (Fig. 11).
When a lesion is been detected at the level of
the superficial bursa of the patellar prior to surgery, a longitudinal incision in the skin and
resection of the bursa should be carried out
(Fig. 12). The portals are closed with sutures or
tape and a bandage is kept in place for 24 h.
Sonosurgery Ultrasound-Guided Arthroscopic Shaving …
Fig. 7 Pre-surgery ultrasound image with high-definition
ultrasound and linear probe in transverse (left) and
longitudinal (right) views. Note the hypervascularization
409
(single arrow) entering the tendon from Hoffa's fat pad.
Tendon thickening (double-headed arrow) and hypoechoic tendon injury areas (asterisk) are highlighted
Fig. 8 Arthroscopic and
ultrasound positioning during
patellar tendon sonosurgery.
The arthroscope and shaver
will alternately be used
through a standard
anteromedial and an
anterolateral portal
6
Rehabilitation Protocol
Walking with full weightbearing immediately
after treatment is allowed. As intratendinous
surgery is not performed, rehabilitation can begin
immediately and be relatively aggressive and
rapid. Range-of-motion exercises, standing and
walking, cycling, and low-load strength training
begin within the first 3 weeks. Then, there is a
gradual increase in load and the initiation of
more sport-specific training. It depends on the
degree of swelling and pain. Isometric, concentric, and eccentric exercises (Fig. 13) should be
tolerated before starting up plyometric training.
Required rehabilitation periods vary from 2 to
4 months before a return to full tendon loading
sports activity.
Day 1: Here, partial weightbearing with crutches is the start. Then, the patients are given
instructions to begin full non-weightbearing
range-of-motion exercises.
Day 2–7: The next step is to start walking and
do light bicycling. Light concentric as well as
410
Fig. 9 Ultrasound images in transverse (left) and longitudinal (right) views with a linear probe where the
insertion of the patellar tendon in the patella is identified
Fig. 10 Arthroscopic image where a patella with a
prominent beak can be seen. By means of debridement
with the shaver, this prominence is lowered so that it does
not imprint on the tendon
eccentric strength training for the quadriceps
muscles are brought into play.
Day 8–14: In the 2nd week after treatment, the
patients are instructed to increase their tendon
loading activity step-by-step with more sportspecific training.
Extreme jumping, running or weight training
activity is strongly discouraged, or better yet,
disallowed for the first 2 weeks.
Maximum patellar tendon loading activity
(return to sport) could be started two weeks
postoperatively if there are no signs of marked
muscle atrophy.
F. Abat and H. Alfredson
for debridement by means of a 4.5 mm full radius
arthroscopic shaver. Simultaneous transverse and longitudinal ultrasound views guide the entire procedure
Fig. 11 Arthroscopic image where, after careful debridement of the injured patellar tendon and removal of the
patellar beak, an intratendinous tear is observed in the
deep portion of the tendon in its contact with the patella
7
Complications
In general, this procedure is free of serious
complications but, of course, attention must be
paid to the risks that are native to knee
arthroscopy.
When tendon debridement is not done with
sufficient precision and ultrasound control, the
thickness of the tendon can be excessively
compromised. This circumstance possibly sets
the stage for a subsequent rupture.
Sonosurgery Ultrasound-Guided Arthroscopic Shaving …
Fig. 12 Debridement of the superficial bursa of the
patella as the last step in the sonosurgery of the injured
tendon in those cases in which a bursal pathology
411
accompanying the tendon injury had previously been
confirmed. A longitudinal incision is made in the skin and
the bursa is resected
Fig. 13 Progression of exercises after surgery for patellar tendinopathy. From elastic exercises with one and two legs
to the use of inertial devices such as the yoyo multigym or leg extensions in protocolized loading programs
8
Conclusions (Take Home
Message)
Intra-tendinous surgical revision treatment of
proximal patellar tendinopathy seems questionable to us. This assertion is grounded in the poor
clinical results seen with intra-tendinous surgical
approaches and the new research findings gained
from looking at the innervation patterns.
Surgical treatment around the tendon with US
and DP-guided arthroscopic shaving has shown a
great potential to make for a pain-free return,
after a relatively short rehabilitation period, to
sports activities that place a high demand on the
patellar tendon.
412
References
1. Abat F, Sánchez-Sánchez JL, Martín-Nogueras AM,
Calvo-Arenillas JI, Yajeya J, Méndez-Sánchez R,
Monllau JC, Gelber PE. Randomized controlled trial
comparing the effectiveness of the ultrasound-guided
galvanic electrolysis technique (USGET) versus
conventional electro-physiotherapeutic treatment on
patellar tendinopathy. J Exp Orthop. 2016;3(1):34.
https://doi.org/10.1186/s40634-016-0070-4.
2. Abat F, Alfredson H, Cucchiarini M, Madry H,
Marmotti A, Mouton C, Oliveira JM, Pereira H,
Peretti GM, Spang C, Stephen J, van Bergen CJA, de
Girolamo L. Current trends in tendinopathy: consensus of the ESSKA basic science committee. Part II:
treatment options. J Exp Orthop. 2018;5(1):38.
https://doi.org/10.1186/s40634-018-0145-5.
3. Jonsson P, Alfredson H. Superior results with eccentric
compared to concentric quadriceps training in patients
with jumper’s knee: a prospective randomized study.
Br J Sports Med. 2005;39(11):847–50. https://doi.org/
10.1136/bjsm.2005.018630.
4. Purdam CR, Jonsson P, Alfredson H, Lorentzon R,
Cook JL, Khan KM. A pilot study of the eccentric
decline squat in the management of painful chronic
patellar tendinopathy. Br J Sports Med. 2004;38
(4):395–7. https://doi.org/10.1136/bjsm.2003.000053.
5. Abat F, Alfredson H, Cucchiarini M, Madry H,
Marmotti A, Mouton C, Oliveira JM, Pereira H,
Peretti GM, Romero-Rodriguez D, Spang C,
Stephen J, van Bergen CJA, de Girolamo L. Current
trends in tendinopathy: consensus of the ESSKA
basic science committee. Part I: biology, biomechanics, anatomy and an exercise-based approach. J Exp
Orthop.
2017;4(1):18.
https://doi.org/10.1186/
s40634-017-0092-6.
6. Obara K, Chiba R, Takahashi M, Matsuno T,
Takakusaki K. Knee dynamics during take-off and
landing in spike jumps performed by volleyball players
with patellar tendinopathy. J Phys Ther Sci. 2022;34
(2):103–9. https://doi.org/10.1589/jpts.34.103.
7. Abat F, Valles SL, Gelber PE, Polidori F, Stitik TP,
García-Herreros S, Monllau JC, Sanchez-Ibánez JM.
Molecular repair mechanisms using the Intratissue
Percutaneous Electrolysis technique in patellar tendonitis. Rev Esp Cir Ortop Traumatol. 2014;58(4):201–
5. https://doi.org/10.1016/j.recot.2014.01.002.
8. Vander Doelen T, Jelley W. Non-surgical treatment
of patellar tendinopathy: A systematic review of
randomized controlled trials. J Sci Med Sport.
2020;23(2):118–124. https://doi.org/10.1016/j.jsams.
2019.09.008.
9. Chen PC, Wu KT, Chou WY, Huang YC, Wang LY,
Yang TH, Siu KK, Tu YK. Comparative effectiveness of different nonsurgical treatments for patellar
tendinopathy: a systematic review and network metaanalysis. Arthroscopy. 2019;35(11):3117-3131.e2.
https://doi.org/10.1016/j.arthro.2019.06.017.
F. Abat and H. Alfredson
10. Johnson DP. Arthroscopic surgery for patellar tendonitis: A new technique. Arthroscopy. 1998;14:S44.
11. Lee DW, Kim JG, Kim TM, Kim DH. Refractory
patellar tendinopathy treated by arthroscopic decortication of the inferior patellar pole in athletes: midterm outcomes. Knee. 2018;25(3):499–506. https://
doi.org/10.1016/j.knee.2018.02.015.
12. Testa V, Capasso G, Maffulli N, Bifulco G.
Ultrasound-guided percutaneous longitudinal tenotomy for the management of patellar tendinopathy.
Med Sci Sports Exerc. 1999;31(11):1509–15. https://
doi.org/10.1097/00005768-199911000-00003.
13. Coleman BD, Khan KM, Maffulli N, Cook JL,
Wark JD. Studies of surgical outcome after patellar
tendinopathy: clinical significance of methodological
deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J
Med Sci Sports. 2000;10(1):2–11. https://doi.org/10.
1034/j.1600-0838.2000.010001002.x.
14. Bahr R, Fossan B, Løken S, Engebretsen L. Surgical
treatment compared with eccentric training for patellar tendinopathy (Jumper's Knee). A randomized,
controlled trial. J Bone Joint Surg Am. 2006;88
(8):1689–98. https://doi.org/10.2106/JBJS.E.01181.
15. Khan KM, Cook JL, Maffulli N, Kannus P. Where is
the pain coming from in tendinopathy? It may be
biochemical, not only structural, in origin. Br J
Sports Med. 2000;34(2):81–3. https://doi.org/10.
1136/bjsm.34.2.81.
16. Alfredson H, Ohberg L. Neovascularisation in
chronic painful patellar tendinosis–promising results
after sclerosing neovessels outside the tendon challenge the need for surgery. Knee Surg Sports
Traumatol Arthrosc. 2005;13(2):74–80. https://doi.
org/10.1007/s00167-004-0549-x.
17. Forsgren S, Danielson P, Alfredson H. Vascular NK1 receptor occurrence in normal and chronic painful
Achilles and patellar tendons: studies on chemically
unfixed as well as fixed specimens. Regul Pept.
2005;126(3):173–81.
https://doi.org/10.1016/j.
regpep.2004.09.008.
18. Danielson P, Andersson G, Alfredson H, Forsgren S.
Marked sympathetic component in the perivascular
innervation of the dorsal paratendinous tissue of the
patellar tendon in arthroscopically treated tendinosis
patients. Knee Surg Sports Traumatol Arthrosc.
2008;16(6):621–6. https://doi.org/10.1007/s00167008-0530-1.
19. Hoksrud A, Ohberg L, Alfredson H, Bahr R.
Ultrasound-guided sclerosis of neovessels in painful
chronic patellar tendinopathy: a randomized controlled trial. Am J Sports Med. 2006;34(11):1738–46.
https://doi.org/10.1177/0363546506289168.
20. Willberg L, Sunding K, Ohberg L, Forssblad M,
Alfredson H. Treatment of Jumper’s knee: promising
short-term results in a pilot study using a new arthroscopic approach based on imaging findings. Knee Surg
Sports Traumatol Arthrosc. 2007;15(5):676–81. https://
doi.org/10.1007/s00167-006-0223-6.
Sonosurgery Ultrasound-Guided Arthroscopic Shaving …
21. Blazina ME, Kerlan RK, Jobe FW, Carter VS,
Carlson GJ. Jumper’s knee. Orthop Clin North Am.
1973;4(3):665–78.
22. Kaux JF, Forthomme B, Goff CL, Crielaard JM,
Croisier JL. Current opinions on tendinopathy.
J Sports Sci Med. 2011;10(2):238–53.
23. Masci L, Alfredson H, Neal B, Wynter BW.
Ultrasound-guided tendon debridement improves
413
pain, function and structure in persistent patellar
tendinopathy: short term follow-up of a case series.
BMJ Open Sport Exerc Med. 2020;6(1): e000803.
https://doi.org/10.1136/bmjsem-2020-000803.
Medial Patellofemoral Ligament
Reconstruction: Anatomical Versus
Quasi-anatomical Femoral Fixation
Vicente Sanchis-Alfonso, Maximiliano Ibañez,
Cristina Ramirez-Fuentes,
and Joan Carles Monllau
1
Introduction
Chronic lateral patellar instability (CLPI) is a
common finding in the orthopedic knee surgeon´
s daily clinical practice. First-time lateral patellar
dislocation has an incidence rate of 23 per
100,000 person-year [1]. After a first episode,
patellar dislocation recurrence follows in more
than 50% of patients [2].
As likely as not, the etiology of CLPI is
multifactorial. However, the deficiency of the
medial patellofemoral ligament (MPFL) seems to
be the most important factor in the genesis of
instability [3] Over recent years, MPFL recon-
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
M. Ibañez
ICATME, Hospital Universitari Dexeus, UAB,
Barcelona, Spain
C. Ramirez-Fuentes
Medical Imaging Department, Hospital Universitario
y Politecnico La Fe, Valencia, Spain
J. C. Monllau
Hospital del Mar, Barcelona, Spain
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
struction (MPFLr) has come to be recognized as
crucial in its treatment. Resultingly, MPFLr is the
most routinely used surgical intervention for
CLPI. It is possible to carry out MPFLr along
with other surgical techniques that are directed
toward correcting some predisposing factors that
frequently go hand-in-hand with CLPI. They are
anteromedialization of the tibial tubercle, rotational osteotomy or trochleoplasty [4–6].
The first publications on MPFLr date from the
early 1990s [7–9]. Ellera-Gomes [7] published in
1992 in Arthroscopy 58 cases of MPFL reconstructions operated on from September 1986 to
March 1998. One year later Avikainen and colleagues [8] published in Clin Orthop 14 adductor
magnus tenodesis associated to MPFL repair
performed from 1982 to 1984. We could considered this technique as a non-anatomic MPFLr.
Robert A. Teitge began doing MPFL reconstructions in the early 1980s as a consequence of
the good results he had obtained with reconstructions of the lateral patellofemoral ligament
in patients with iatrogenic medial patellar instability. In 1994 Robert Teitge published a paper in
which he described both LPFL and MPFL
reconstructions [9]. But if we dig a little deeper
into this topic we find a 1924 publication by
Gallie and Le Mesurier [10], which seems prophetic, describing not only the reconstruction of
the MPFL (in older literature called “proximal
transverse retinaculum”), but also highlighting
the importance of alignment and bone deformities in the genesis and treatment of
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_27
415
416
V. Sanchis-Alfonso et al.
patellofemoral instability. But as often happens,
this technique fell into oblivion.
In the last 30 years, many variations of these
pioneer techniques in which multiple graft types
and fixation strategies were used have been
published. Overall, the MPFLr techniques can be
grouped in two main types, the static and the
dynamic. The current gold standard seems to
favor the static MPFLr with anatomical bone
attachments at both the femoral and patellar
insertion points. More recently a dynamic nonanatomical MPFLr using the adductor magnus
tendon (AMT) as a pulley, has been again
advocated [11]. This technique may be particularly useful in children as it avoids the risk of
injuring the distal femur growth plate and so a
limb deformity overtime [12].
The objective of this chapter is to describe, in
detail, both static and dynamic MPFL reconstructive techniques as well as the authors’
rational for the treatment used in patients with
CLPI.
2
Aim
The objective of MPFLr is only to stabilize the
patella in the early degrees of knee flexion (i.e.,
the first 30°), but not to correct the patellofemoral
maltracking (J-sign). Isolated MPFLr does not
correct patellar shift and tilt. Therefore, an
MPFLr should be done only after patellofemoral
maltracking has been corrected.
3
Indications
For a successful MPFLr it is crucial to have the
proper selection of the patient. The ideal patients
for an isolated MPFLr would be those with at
least two documented episodes of lateral dislocation with otherwise no advanced signs of
malalignment on any plane (namely, a TT-TG
distance of less than 20 mm, a patellar CatonDeschamps index of less than 1.2 and grade A
trochlear dysplasia) [13]. Patellar dislocation
should be confirmed with physical examination
under anesthesia (Fig. 1).
Fig. 1 Physical examination of the right knee under
anaesthesia. Note the lateral dislocation of the patella.
(“Republished with permission of Elsevier Science &
Technology Journals, from Medial Patellofemoral Ligament Reconstruction, V Sanchis-Alfonso & JC Monllau,
Operative Techniques in Sports Medicine, Vol 27, 4,
2019; permission conveyed through Copyright Clearance
Center, Inc.”)
4
The Bases for a Successful MPFLr
The most important points for a successful
MPFLr are (1) the accurate location and placement of the graft, particularly at its femoral
attachment, and (2) its adequate tensioning.
The MPFL is more like a checkrein that should
not be too tense. For that reason, getting the
correct tension is key to a successful reconstruction. In general, an overly tight graft is
believed to cause overtensioning in the medial
patellofemoral joint (PFJ) and probably patellofemoral osteoarthritis (PFOA) in the long run. In
this chapter, this problem will be further
addressed. Lateral retinacular release (LRR) that
has been used extensively over several years for
the treatment of various extensor mechanism
abnormalities and associated to MPFLr is no
longer recommended as a rule.
4.1 The Femoral Attachment Point
As happens in other ligament reconstructions,
poor graft placement of the MPFLr can cause
severe complications and even disability [13].
The femoral attachment point will determine the
Medial Patellofemoral Ligament Reconstruction …
length change behavior of the graft and therefore
the graft tension at different angles of knee
flexion [14]. Proximal and anterior femoral
attachments points will result in an excessive
stretching of the MPFL-graft at deeper knee
flexion angles as shown by Wang and colleagues
[15]. This will over-constrain the medial PFJ and
increase the cartilage pressures at this level. In
that way, PFOA may be the consequence of
femoral tunnel malposition after MPFLr. Interestingly, the patellar attachment point seems not
to be so important as the femoral attachment
point [14]. It has been demonstrated that MPFL
length changes during knee flexion depend on
the femoral attachment site more than on the
patellar attachment one [14]. In this section, we
will focus on the femoral attachment point.
The current trend in MPFLr is oriented
towards drilling the femoral attachment in the
most anatomic point. An anatomic femoral fixation is the easiest and most reproducible way to
achieve the optimal length-change behavior of
the graft during knee flexion—extension, and
therefore, a satisfactory long-term clinical result
[13, 14]. Yet a strict anatomic femoral attachment point might not be that critical for a successful reconstruction, as has been demonstrated
by Sanchis-Alfonso and colleagues [14]. A nonanatomic MPFL graft that replicates the isometry
and length change pattern of a native MPFL will
also provide satisfactory results [14]. This concept is of paramount importance in children
because of the close anatomical relationship
between the distal femoral physis and the area
where the anatomic tunnel should be drilled. The
actual risk of iatrogenic physeal damage is the
reason the first author performs a quasianatomical MPFLr with gracilis tendon autograft, using the AMT as a pulley for femoral
fixation in skeletically immature patients with
good clinical results. Using this technique, the
kinematic behavior exhibited by the graft is like
that of the native MPFL [16].
In 2007, Schoettle and colleagues [17] published a technique that demonstrated how to find
a reproducible anatomic femoral attachment
point. They used intra-operative fluoroscopy to
determine some radiological coordinates that
417
help the surgeon to reach the right spot.
According to this investigation, an exact lateral
image is needed to locate the anatomic femoral
attachment point. This is currently the most
common technique to determine the femoral
fixation point. The technique permits drilling the
femoral tunnel through a very small and cosmetic
skin approach. However, one may wonder how
accurate this method is insofar as replicating the
anatomic femoral attachment point? In terms of
accuracy, it largely depends on getting a true
lateral knee image with a perfect superposition of
both femoral condyles. Nevertheless, several
authors have questioned the precision of this
radiological method [18–21].
The femoral MPFL attachment site is located
approximately one centimeter distal to the tip of
the adductor tubercle (AT) [22]. However, the
great interindividual anatomical variability in the
location of the AT probably explains the unpredictability relative to the location of the femoral
insertion of the MPFL. This means that the
MPFL is unique for every single individual and
so the optimal femoral position is patient
specific.
More recently, new technologies like 3D-CT
scan (Fig. 2) appeared to help the surgeon in
locating the right spot for femoral MPFL
attachment. Sanchis-Alfonso and colleagues [19]
evaluated 100 patients with CLPI by means of
3D-CT. For each knee, two virtual 7 mm diameter femoral tunnels were created. One tunnel
was shaped based on the AT landmark (the
anatomic tunnel). The second one was created
according to Schoettle’s radiological method
[17]. The ratio of overlapping between the two
tunnels was calculated. An overlapping area
superior to 50% was considered as reasonable.
The goal was achieved in only 38% of cases with
a good intra- and inter-observer reliability values
[19]. Therefore, it was concluded that the radiological method is only an approximation and
should not be the sole basis for safely and
reproducibly drilling an anatomic femoral tunnel
in MPFLr.
Some drawbacks in Schoettle[17] investigation may contribute to understanding this paradox. They analyzed only 8 frozen cadaver knees
418
V. Sanchis-Alfonso et al.
Fig. 2 Location of the AT (red arrow) by means of 3DCT. Medial supracondylar line (white arrow). Medial
femoral epicondyle (blue arrow). Non-anatomical femoral
tunnel placement (black arrow). (“Republished with
permission of Springer Nature BV, from Does
radiographic location ensure precise anatomic location
of the femoral fixation site in medial patellofemoral
ligament surgery?, Sanchis-Alfonso V, et al., 24, 2838–
2844, 2016; permission conveyed through Copyright
Clearance Center, Inc.”)
of unknown age and gender. Additionally, the
presence of trochlear dysplasia was not mentioned or considered. However, CLPI is more
frequent in young females with bony variances
such as trochlear dysplasia. Therefore, the use of
female knees with trochlear dysplasia would be
reasonable in this type of studies. To further
illustrate this concept, in the Sanchis-Alfonso
[19] investigation, 7 out of 12 male patients
without severe trochlear dysplasia showed an
overlap area greater than 50% when using the
method described by Schöettle. Conversely, this
occurred in only 12 out of 40 female patients
with severe trochlear dysplasia [19]. Thus, severe
trochlear dysplasia associated with the female
gender was predictive of overlap of less than 50
in 70% of the cases [19]. In conclusion, in female
knees with a severe trochlear dysplasia, the
radiographic method used to recognise the
femoral anatomic fixation point showed a nonnegligible number of inaccuracies. Since CLPI is
more frequent in females with a severe trochlear
dysplasia, this finding is relevant from the clinical standpoint.
Fluoroscopy is a method that can be very
helpful for the casual surgeon to determine the
femoral attachment point. However, to avoid
mistakes, the fluoroscopic findings should not be
relied upon too greatly due to extreme
interindividual anatomical variability. For that
reason, it is wise to recommend an incision large
enough to permit the correct identification of the
anatomy of the area, including the AMT and the
apex of the AT. The femoral MPFL attachment is
located 10 mm distal to the AT and proximal and
a bit posterior from the medial femoral epicondyle (ME) in a groove midway between the
MFE and the AT (Fig. 3). And so, the AT has
been suggested as a consistent landmark for a
proper location of the femoral tunnel during
MPFLr because the distances between the AT
and the femoral attachment of the MPFL are
uniform, approximately 10 mm distally [22–25].
However, a good option would be to use the 3D-
Medial Patellofemoral Ligament Reconstruction …
419
A
Fig. 3 Anatomic dissection of the left knee showing
medial restraints to lateral patellar translation: medial
patellotibial ligament (MPTL), medial patellomeniscal
ligament (MPML), medial patellofemoral ligamemt
(MPFL). Adductor tubercle (AT) and the medial femoral
epicondyle (ME). Superficial medial collateral ligament
(sMCL), medial meniscus (MM), semimembranosus
tendon (SM), and medial gastrocnemius tendon attachment site (MGT). (“Republished with permission of
Springer Nature BV, from Recognition of evolving
medial patellofemoral anatomy provides insight for
recognition, Tanaka MJ, et al., 27, 2537–2550, 2019;
permission conveyed through Copyright Clearance Center, Inc.”)
CT scan to locate the anatomic femoral attachment point if a minimally invasive and most
cosmetic surgery is considered. This technology
makes for locating the MPFL femoral attachment
point based on the position of the AT. Software
translates the 3D-CT calculated point into 2D
images (Fig. 4). In conclusion, determination of
femoral attachment point location must be based
on anatomy. Just like anterior cruciate ligament
(ACL). The vital thing is to know the anatomy.
As Jack Hughston said, orthopaedic surgery is
above all anatomy plus a bit of common sense.
Once the anatomic femoral attachment point
has been determined, normal isometry of the
graft is automatically expected. The MPFL
shows isometric behaviour in 80% of the cases
from 0° to 60° and in 20% of the cases from 0° to
30° [14]. This is called “favourable anisometry”.
B
Fig. 4 The AT is an important landmark to determine the
location of the MPFL femoral attachment point. Using
software analyses, the point calculated in the 3D-CT
(A) can be translated to a regular 2D x-ray image (B).
Tunnel created using the AT as a landmark—anatomic
tunnel (red circle). Tunnel created in accordance with
Schöttle’s radiological method (yellow circle). Like in our
study, Ishikawa and colleagues [26] demonstrated, on a
virtual true lateral radiograph reconstruction from a threedimensional computed tomography (3D-CT) image,
that in patients with recurrent patellar dislocation the
femoral attachment point of the MPFL is more posterior
and distal to the Schöttle point. (Reused from
SAGE JOURNALS. Sanchis-Alfonso V, RamirezFuentes C, Montesinos-Berry E, et al. Radiographic
location does not ensure a precise anatomic location of
the femoral fixation site in medial patellofemoral ligament
reconstructions. The Orthopaedic Journal of Sports
Medicine, 5(11), 2,325,967,117,739,252. https://doi.org/
10.1177/2325967117739252. ©The Author(s) 2017)
Beyond these degrees of flexion, the graft
slackens. Nevertheless, the idea of ligament
isometry is based on a knee with regular anatomy
should be remembered and the patients with
CLPI are know to have many anatomical knee
abnormalities.
4.2 Graft Tensioning
The MPFL is considered a checkrein, more than
a constraint, that it is not under constant tension
in its native state. It only comes under tension
when a lateral or medial force pushes the patella
either laterally or medially. Schoettle brilliantlly
compared its function to that of a dog leash,
which is loose most of the time. However, when
the dog (namely, the patella) runs away (meaning, dislocates), the leash tightens. Therefore,
420
there is no need to tension the MPFL graft during
its reconstruction. If the graft were tight all the
time, it would bring on an increase in patellofemoral pressure that could lead to PFOA over
time.
4.3 Role of Lateral Retinacular
Release
Lateral retinacular release (LRR) of the patella
has been used extensevely for knee surgeries,
particularly in disorders of the extensor mechanism. However, its current usefulness is under
scrutiny due to its complications and doubtful
outcomes.
In the first author’s opinion, LRR or lengthening has no role in primary CLPI surgery. In a
series of 33 patients evaluated with a minimum
of 12 months, Malatray and colleagues [27]
demonstrated that isolated MPFLr was not inferior to MPFLr associated with arthroscopic LRR
in terms of the IKDC subjective score and
patellar tilt. They conclude that there is no indication for LRR associated to MPFLr in the
treatment of CLPI. Furthermore, Merican and
colleagues [28] conducted a biomechanical
investigation showing that the lateral retinaculum
actually contributes to resisting lateral patellar
displacement. Consequently, lateral patellar
instability will increase after LRR.
To guide the patella towards the trochlear
sulcus during the first degrees of knee flexion,
both the MPFL and the lateral retinaculum must
interplay in a harmonious way. Christian Lattermann states that both ligaments behave similarly to the reins of a horse. Both reins must have
some degree of tension. They are not very tense
but they are not loose either. If one of the reins is
completely loose the horse is inclined towards
the opposite direction as it occurs in the patella.
This will provoke a patellofemoral imbalance
that could be responsible for iatrogenic anterior
knee pain (AKP).
The most usual indication for LRR or
lengthening is severe patellar tilt. However, in
this case, severe trochlear dysplasia is also a
V. Sanchis-Alfonso et al.
common finding that can be addressed by means
of trochleoplasty. This last procedure relaxes the
deep layer of the lateral retinaculum and so LRR
is unnecessary. Additionally, LRR in cases of
trochlear dysplasia might provoke medial patellar
instability.
Only in the rare cases of fixed lateral dislocation in flexion must we consider LRR or
lengthening since in these cases there is a
shortening of the lateral structures. In these
exceptional cases the advice of the first author
(V.S-A) is not to perform a LRR but a
lenghthening (Fig. 5). It has the same effect
regarding the elimination of hypercompression
and hypertension on the lateral side as the LRR.
Moreover, lateral retinaculum lenghthening is a
tecnnique individually adapted. Finally, it avoids
the secondary complications of LRR such as
medial patellar instability.
5
Surgical Technique Step-By-Step.
Pearls and Tips
5.1 Static and Anatomic MPFLr
The first author’s preferred surgical technique is
the anatomic double-bundle static MPFLr using a
semitendinosus autograft. MPFLr can be done
either with single-bundle (SB) or double-bundle
(DB) graft configuration. According to current
evidence, the use of a double-bundle pattern
seems more advisable to better reproduce the
native MPFL function. Better outcomes (i.e.,
Kujala, IKDC, and VAS) and fewer complications, reoperations and re-dislocation rates have
been found in a recent revision of primary isolated DB MPFLr for recurrent patellofemoral
instability [29]. Furthermore, Migliorini and colleagues [30] have shown that isolated MPFLr
with semitendinosus tendon graft performed better than the gracilis. All the scores of interests
(Kujala, Tegner, Lysholm) and range of motion
scored better in the semitendinosus group. Moreover, in favour of the semitendinosus group, a
statistically significant reduction of the revision
surgeries and re-dislocations were evidenced.
Medial Patellofemoral Ligament Reconstruction …
421
A
B
C
D
Fig. 5 Lateral retinaculum lengthening. Technical note
according to RM Biedert, MD. The lateral retinaculum
consists of a superficial oblique and a deep transverse part
(A). Lengthening is started incising longitudinally the
superficial oblique retinaculum about 5 mm from its
attachment to the lateral border of the patella. Then it is
separated from the deep transverse retinaculum (B). The
deep transverse ligament is incised also longitudinally
from its attachment to the iliotibial band and the synovial
layer opened (C). This releases the increased tension of the
lateral structures. The two parts of the lateral retinaculum
are sutured together in 90º of knee flexion (D). This makes
it impossible that the retinaculum is too tight. The mobility
of the patella should be 1–2 quadrants to the medial and
the lateral side in full extension, guaranteeing a normal
balance of the patella in the trochlea
The patient is placed in the supine position on
a standard table. After induction of anesthesia
lateral patellar dislocation must be confirmed
(Fig. 1). Fathalla and colleagues [31] have
assessed the prognostic value of examination
under anesthesia (EUA) prior to MPFLr. They
retrospectively evaluated the outcome of 23
patients who had undergone an isolated MPFLr
for CLPI. Of the 23, 9 failed (39%), all of them
had a dislocating patella at more than 30º of knee
flexion. They concluded that patients in whom
the patella can be dislocated beyond 30º on EUA
are unlikely to benefit from isolated MPFLr.
The leg to be operated on is prepared in the
standard fashion. The use of a tourniquet is
optional. A sterile bump is placed under the knee
to keep it slightly flexed. Although the benefit of
a diagnostic arthroscopy has been questioned
[32], it is routinely performed prior to MPFLr in
the author’s practice (Fig. 6). The main objectives being (1) full evaluation of the status of the
cartilage and (2) to rule out any intraarticular
damage not seen on the preoperative magnetic
resonance imaging.
Then, the semitendinosus tendon is harvested
following the standard technique, prepared and
wrapped in gauze previously soaked in a solution
of 100 ml of saline mixed with 500 mg of vancomycin powder. This last step has been suggested to avoid microbiological contamination of
the graft [33].
Next, an incision is made in the anterior
aspect of the knee, centered over the junction of
the medial and middle thirds of the patella. The
422
V. Sanchis-Alfonso et al.
Fig. 6 Diagnostic
arthroscopy previous to
MPFLr. Note (A) a
chondropathy in the medial
facet of the patella, (B) a
loose body in the subquad
area (axial CT view),
(C) arthroscopic view, an
(D) after its excision.
(“Republished with
permission of Elsevier
Science & Technology
Journals, from Medial
Patellofemoral Ligament
Reconstruction, V SanchisAlfonso & JC Monllau,
Operative Techniques in
Sports Medicine, Vol 27, 4,
2019; permission conveyed
through Copyright Clearance
Center, Inc.”)
medial third of the patella is exposed and subperiosteally dissected with a scalpel. The dissection is carried through medially between
layers 2 and 3. Two 4.5 mm diameter tunnels are
drilled in the anterior cortex of the patella near its
medial aspect (Fig. 7). Special care should be
taken when drilling to avoid penetrating the
subchondral bone and damaging the articular
cartilage. Attention should be paid to leaving at
least 10 mm of bone-bridge between the tunnels
to avoid intraoperative fractures.
Then, a small incision is made over the medial
epicondyle. 3D-CT technology is used to locate
the anatomic femoral attachment point as
explained earlier on. The image intensifier is
used to further check the femoral attachment
point (regularly located 10 mm distal to the AT).
Once the anatomic femoral attachment point is
determined using the 3D-CT method, there is no
need to further check the graft isometry. After
that, the medial patellar and medial femoral
incisions are connected by blunt dissection by
means of a hemostat. Firstly, the graft is passed
through the patellar tunnels (Figs. 7 and 8) and
then between layers 2 and 3 until the femoral
attachment point is reached.
Correct ligament tension is crucial to the
success of MPFLr surgery. Enough tension to put
the graft taut is sufficient. Do not pull the graft
tight at the time of fixation. If done so, it leads to
elevated medial contact pressures and medial
patellar tracking. To avoid excessive graft tension, the graft is fixed at 30° of knee flexion as
the distance between the femoral and patellar
attachments points is greatest at this angle [14].
Graft fixation on the femoral side can be done
with bioabsorbable interference screws or suture
anchors, which is the author’s preferred technique. A biomechanical cadaveric study demonstrated that suture anchor femoral fixation was
not significantly different from interference screw
fixation in terms of load-to-failure [34]. Likewise, the mean load-to-failure values for both
fixation techniques in MPFLr were greater than
the values reported in the medical literature for
the native MPFL [34]. The effect of interference
Medial Patellofemoral Ligament Reconstruction …
Fig. 7 Intraoperative views of the patellar steps of the
surgical procedure. (A) the dissected anterior and medial
sides of the patella. (B) drilling two 4.5 v-shaped tunnels.
(C) and (D) the graft being passed through the tunnels.
(“Republished with permission of Elsevier Science &
423
Technology Journals, from Medial Patellofemoral Ligament Reconstruction, V Sanchis-Alfonso & JC Monllau,
Operative Techniques in Sports Medicine, Vol 27, 4,
2019; permission conveyed through Copyright Clearance
Center, Inc.”)
significantly increases graft tension. If the difference between the diameter of the femoral
tunnel and the graft is 0 or 1 mm, the tension of
the graft increased significantly compared to
when the difference between the diameters is
equal to or greater than 2 mm. Therefore, the
casual surgeon should be aware of the inadvertent increases in graft tension even in low
preloading conditions to palliate the risk of graft
overtensioning.
Fig. 8 Double-bundle MPFLr
screw femoral fixation on MPFL graft tension
has been analyzed by Ackermann and colleagues
[35]. They demonstrated that this type of fixation
5.2 Quasi-Anatonical (Elastic) MPFLr
For this technique (Fig. 9), the homolateral gracilis tendon (GT) autograft is the author’s
(JCM) preferred choice. The harvesting technique consists of a 2 cm long vertical skin
424
Fig. 9 Operative images of a
left knee showing the 3
surgical approaches needed
and the fundamental steps of
the technique. A V-shaped
tunnel is drilled in the medial
aspect of the patella A; the GT
is introduced in the patellar
tunnel B; a traction suture
looped around the adductor
magnus (AM) C; the GT is
then looped around the AM
tendon D. (“Republished with
permission of Springer
Nature BV, from Clinical and
radiological outcomes after a
quasi-anatomical
reconstruction of medial
patellofemoral ligament with
gracilis tendon autografty,
Monllau JC, et al., 25, 2453–
2459, 2017; permission
conveyed through Copyright
Clearance Center, Inc.”)
V. Sanchis-Alfonso et al.
A
B
C
D
incision centered in the upper medial aspect of
the tibia and some 3-fingerbreadths down the
joint line. After dissecting the soft tissue, the
Sartorius fascia is incised horizontally, releasing
the distal attachment of the GT. From there on,
the graft is harvested using a tendon stripper.
When harvesting the tendon, care should be
taken so as not to amputate it before full dissection is made. The graft must be at least
90 mm in length (total graft length 180 mm) to
properly reconstruct the MPFL in a doublebundle pattern. The 2 ends of the graft are prepared with #2 high-strength Krackow mattress
sutures. The prepared graft is then sized and kept
wrapped in vancomycin-soaked gauze to prevent
bacterial contamination [32]. The native MPFL
was found to have a mean tensile strength of
208 N and the mean maximum load for 1 strand
of a GT was found to be 837 ± 138 N [36, 37].
Therefore, the author’s (JCM) opinion is that the
GT is enough in terms of both length and
strength to reconstruct the MPFL.
A second 2 to 3 cm vertical skin approach is
then made over the superior medial border of the
patella to expose its proximal third where the
anatomical footprint of the MPFL is located.
Two convergent 4.5 mm holes are drilled at the
edges of the footprint. The tunnels are made in a
convergent V-shape from the medial cortex to
the cancellous bone of the patella. Attention
should be paid to leaving at least 15 mm of bonebridge between the tunnels to avoid intraoperative fractures or locus minor resistentiae where a
stress fracture could be produced postoperatively. The edges of both drill holes and the inner
angle of the V-shaped tunnels obtained are
smoothed out to avoid any “killer turn”.
A third 2 to 3 cm skin incision is then made
slightly proximal to the ME along the AMT. The
approach is deepened in line with the medial
Medial Patellofemoral Ligament Reconstruction …
intermuscular septum and the AMT is easily
identified, by means of finger palpation under the
crural fascia. The AMT is carefully dissected as
distally as possible in order to reach the closest
point possible to the native MPFL footprint.
A looped suture is placed around the AMT to
later aid in graft passage. The same suture helps
in a proper distal dissection of the AMT with a
pulling and “sawing” movement toward the
femoral insertion. The graft is then passed
through the patellar tunnels and then through the
interval between layers 2 and 3. Attention should
be paid to avoid an intra-articular graft. This is of
particular relevance when the MPFL is reconstructed in combination with other intraarticular
procedures. Finally, the graft is looped around
the AMT, used like a pulley, and back to the
patella. While maintaining the graft under a
slight tension, the knee is cycled several times to
find the correct physiometry and to check patellofemoral tracking. Before proceeding to the last
step, it is important to verify that the patella can
still be manually lateralized some 10 mm to
avoid any over-constraint. Lastly, both graft ends
are tied together at 30° of flexion with highresistance irresorbible #2 sutures. The remaining
tendon end can be cut, or it can also be tied under
the pre-patellar periosteum if it is long enough.
This kind of MPFLr at the femoral side permits securing the graft without any bone drilling,
without hardware, and with an elastic fixation of
the new ligament. Therefore, the procedure is
inexpensive, safe in skeletally immature patients
and less likely to develop the medial patellofemoral over-constraint that is eventually produced
by static femoral fixation [38, 39]. The author’s
accumulated experience as well as a previous
finite element investigation supports this concept
[40]. In addition, the current procedure does not
require the use of an image intensifier. Although
the AMT femoral insertion is not completely
anatomic, as the MPFL anatomically inserts
some 10 mm distally to the AT, it is assumed
that this kind of elastic attachment might compensate for the mismatching.
425
6
Addressing the Associated
Predisposing Factors to Patellar
Dislocation
Patellar chondropathy is a common finding in
cases of CLPI. In general, the authors only
remove unstable cartilage flaps and loose bodies,
other cartilage lesions are not addressed.
Although patellar chondropathy could be
responsible for AKP in patients with CLPI, the
pain disappears even though the eventual chondral lesion is left alone once the patella has been
stabilized.
Medialization of the tibial tuberosity (TT) is
commonly recommended when the TT-TG distance is greater than 20 mm. However, there is
no consensus as to the threshold value of TT-TG
distance for indicating TT osteotomy (TTO) associated with MPFLr for the treatment of recurrent patellar instability. In a retrospective
analysis of 81 patients who underwent either
isolated MPFLr or MPFLr combined with TTO
for recurrent patellar instability with a TT-TG
distance of 15 to 25 mm, Kim and colleagues
[41] observed that both groups had similar satisfactory clinical results with a similar incidence
of MPFLr failure. Interestingly, no differences in
clinical outcomes were observed between the
isolated MPFLr and TTO subgroups (TT-TG 15–
20 versus TT-TG 20–25). The conclusion was
that an isolated MPFLr is a safe and reliable
treatment for patients with recurrent patellar
instability with a TT-TG distance of 15 to
25 mm. Some reasons may contribute to explain
these findings. Firstly, the TT-TG distance
depends on knee flexion, weightbearing, tibiofemoral rotation, and joint size [42]. Secondly,
the intra and interobserver reliability for TT-TG
distance measurements is less in patients with
severe trochlear dysplasia compared to low-grade
trochlear dysplasia [42]. Thirdly, there are no
differences in the TT-TG distance between the
stable and the unstable knee in patients with
unilateral patellar instability [43]. Finally, some
studies have not found differences in the
426
outcomes of isolated MPFLr in the setting of a
TT-TG index>20 mm compared to those with a
TT-TG distance<20 mm [44]. Therefore, it
seems wise to use these measurements with care
when designing the treatment for each individual.
A much more comprehensive approach that
includes the patient’s medical history and physical examination, the etiology of dislocation
(traumatic versus atraumatic), the uni or bilaterality of the process as well as the activity level
and expectations of the patient is advised.
Patellofemoral tracking (J-sign) should also be
taken into consideration. In conclusion, TTO
should be considered in extremely selected cases
when a less invasive alternative is insufficient.
Similarly, there is no consensus on a threshold
value for the Caton-Deschamps index to indicate
TT distalization associated with MPFLr for the
treatment of recurrent patellar instability. In a
recent publication, isolated MPFLr in patients
with patella alta (Caton-Deschamps index 1.2)
and CLPI results in a significant decrease in the
patellar height ratio with the effect size being
greatest in patients with higher pre-operative
Caton-Deschamps index values [45]. In patients
with patella alta, defined as a Caton-Deschamps
index 1.2, normalization of the patellar height
ratio occurred in 59.6% of the cases [45]. Additionally, no differences in clinical outcomes were
encountered in patients with and without patella
alta using de Banff Patellofemoral Instability
Instrument score [45]. Consequently, distalization may not be necessary in most CLPI associated with patella alta if MPFLr provokes a
descent of the patella, at least in those with
Caton-Deschamps Index values between 1.2–1.4
[46]. On the other hand, patients with mild
patella alta report similar outcomes after isolated
MPFLr than patients with normal patella height
[46]. In conclusion, the value of adding TT distalization in patients with patella alta is not clear.
Moreover, TT distalization is not a panacea. TT
distalization always implies some degree of
medialization. Additionally, it may be risky in
patients with chondral lesions of the distal pole
of the patella because the procedure causes an
overload of this area upon initial flexion.
V. Sanchis-Alfonso et al.
Furthermore, the detachment of the TT might
potentially cause a tibial fracture and non-union.
Regarding sulcus deepening trochleoplasty, it
is not a routine surgical procedure. It is a valuable tool only in a small subset of patients,
mostly in revision surgeries. They include severe
trochlear dysplasia, when the patella dislocates
not only during the first 30º of knee flexion but
also at high degrees of knee flexion, and when
there is patellofemoral maltracking (positive Jsign).
The first author (V.S-A) recommends never
performing a trochleoplasty, a femoral osteotomy
or a tibial tubercle osteotomy if there is no
maltraking (J-sign) as isolated MPFLr is likely to
work.
7
Postoperative Management
Pain control is important after surgery; a femoral
nerve block and endovenous analgesics are our
preferred options. A knee brace is recommended
for 4 weeks until the quadriceps is fully activated. Immediate full weightbearing, as tolerated,
with the help of two crutches is encouraged from
the beginning. The principles of MPFLr rehabilitation stress early complete range-of-motion
(ROM) exercises, with the emphasis on extension to prevent scar formation and capsular
retractions, quadriceps strengthening and proximal control of the lower limb (hip abductors and
external rotators strengthening). As knee rotation
places lateral stress on the patella, it is necessary
to refrain from knee rotation until three months
after the operation [47].
In recent years, several investigations have
analyzed the return to sports after ACL reconstruction. Conversely, there is scarce information
on when to start sports after MPFLr. As in the
ACL reconstruction, the timing to return to sports
is not just a matter of time but rather a matter of
meeting some clinical and functional requirements. Ménétrey and colleagues [48] proposed
six clinical criteria for returning to sport after
MPFLr: absence of pain, no effusion, no patellar
instability, full range of motion, symmetrical
Medial Patellofemoral Ligament Reconstruction …
strength (85–90%) in both legs, and excellent
dynamic stability assessed with the use of several
functional tests such as the single-leg squat and
the star excursion balance test (SEBT). Many
sports activities call for changes in direction and
landing from jumps. It is therefore important to
assess these parameters before returning to
sports. Drop and jump test and side hop-test
provide valuable information about those sports
gestures.
8
Clinical Outcomes. Scientific
Evidence
Medial patellofemoral ligament (MPFL) reconstruction is being performed more frequently
each time with good clinical outcomes. SappeyMarinier and colleagues [49] have reported the
clinical outcomes of isolated MPFLr. They conclude that isolated MPFLr is a safe and efficient
surgical procedure with a low failure rate. They
evaluated 211 MPFL reconstructions with a
mean follow-up of 5.8 years (range, 3–
9.3 years). Twenty-seven percent of patients had
a preoperative positive J-sign, and 93% of
patients had trochlear dysplasia (A, 47%; B,
25%; C, 15%; D, 6%). The mean CDI was 1.2
(range, 1.0−1.7); mean tibial tubercle-trochlear
groove distance, 15 mm (range, 5−30 mm); and
mean patellar tilt, 23° (range, 9°-47°). The mean
Kujala score improved from 56.1 preoperatively
to 88.8 in the postop. Recurrent patellar instability requiring surgical revision was reported in
10 cases (4.7%). Preoperative predictive factors
for failure were patella alta (CDI 1.3) and a
preoperative positive J-sign. These results are in
accordance with a recent systematic review with
a meta-analysis to evaluate outcomes after isolated MPFLr for the treatment of recurrent
patellar dislocations. The pooled estimated mean
postoperative Kujala score was 85.8 (95% CI,
81.6–90.0), with 84.1% (95% CI, 71.1–97.1%)
of the patients returning to sports after surgery.
The pooled total risk of recurrent instability after
surgery was 1.2% (95% CI, 0.3–2.1%) with a
positive apprehension sign risk of 3.6% (95% CI,
427
0–7.2%) and a reoperation risk of 3.1% (95% CI,
1.1–5.0%) [50].
Platt and colleagues [51] also meta-analyzed
the overall rate of return to sports after MPFLr.
In their revision, the rate of return to sport was
higher (92.8%) even though only 71.3% return to
their preoperative level of performance. Return to
sport after MPFLr does not differ significantly in
patients with or without an osteotomy (95.4 vs.
86.9%). Moreover, the time to return to play was
seen at approximately 7 months after index surgery. Complications occurred at an overall rate of
8.8%, being the most common recurrence of
instability (1.9%). Another interesting issue is the
characteristics of patients who were unable to
return to play after MPFLr. This subject was
addressed by Hurley and colleagues [52]. They
evaluated the psychological readiness to return to
sport using the MPFL-RSI score. It was concluded that patients that do not return to play
exhibit poor psychological readiness with the
most common reason being fear of re-injury.
Interestingly, only 42.4% of US military servicemembers undergoing primary MPFLr were
able to fully return to unrestricted impact activity
after surgery, bilateral instability being a factor of
poor prognosis [53].
In summary, a high percentage of patients
with CLPI undergoing MPFLr have good clinical
outcomes with a return to sports and a low
incidence of recurrent instability, postoperative
apprehension, and reoperations.
9
Anatomical MPFLr Versus Quasianatomical MPFLr
Marot and colleagues [54] performed a multicenter longitudinal prospective study to compare
the functional outcomes after an isolated MPFLr
using either a quasi-anatomical technique (elastic
femoral fixation) or an anatomical (static femoral
fixation) MPFLr. Patients with trochlear dysplasia types C and D were excluded. The main
evaluation criterion was the Kujala functional
score. The secondary objectives were to compare
the rates of redislocation, range-of-motion and
428
V. Sanchis-Alfonso et al.
subjective patellar instability (Smillie test). The
mean postoperative Kujala was 90.4 (89.4 in
group A and 92.1 in group B). Upon comparing
the mean difference between pre- and postoperative values, no differences were detected
between the two groups. They concluded that an
isolated quasi-anatomical MPFLr using a gracilis
tendon autograft provides outcomes as good as
the isolated anatomical MPFLr at the 2–5 years
follow-up in the selected subgroup of patients
with CLPI.
6.
7.
8.
9.
10
Take Home Messages
– MPFLr has proven to be a safe, reliable and
reproducible technique for the treatment of
CLPI.
– The paramount requirement for a successful
MPFLr is the proper selection of the patient as
well as correct presurgical planning and a
meticulous surgical technique.
– An MPFL reconstruction should not be performed if the patella cannot be laterally
dislocated.
10.
11.
12.
13.
14.
References
1. Sanders TL, Pareek A, Hewett TE, et al. Incidence of
first-time lateral patellar dislocation: a 21-year
population-based study. Sports Health. 2018;10
(2):146–51.
2. Huntington LS, Webster KE, Devitt BM, et al.
Factors associated with an increased risk of recurrence after a first-time patellar dislocation: a systematic review and meta-analysis. Am J Sports Med.
2020;48(10):2552–62.
3. Nomura E. Classification of lesions of the medial
patello-femoral ligament in patellar dislocation. Int
Orthop. 1999;23(5):260–3.
4. Allen MM, Krych AJ, Johnson NR, et al. Combined
tibial tubercle osteotomy and medial patellofemoral
ligament reconstruction for recurrent lateral patellar
instability in patients with multiple anatomic risk
factors. Arthroscopy. 2018;34(8):2420–6.
5. Nelitz M, Dreyhaupt J, Robert S, et al. Combined
supracondylar femoral derotation osteotomy and
patellofemoral ligament reconstruction for recurrent
15.
16.
17.
18.
19.
patellar dislocation and severe femoral anteversion
syndrome: surgical technique and clinical outcome.
Int Orthop. 2015;39(12):2355–62.
Nelitz M, Williams SR. [Combined trochleoplasty
and medial patellofemoral ligament reconstruction
for patellofemoral instability]. [Article in German]
Oper Orthop Traumatol. 2015;27(6):495–504.
Ellera Gomes JL. Medial patellofemoral ligament
reconstruction for recurrent dislocation of the patella:
a preliminary report. Arthroscopy. 1992;8(3):335–40.
Avikainen VJ, Nikku RK, Seppanen-Lehmonen TK.
Adductor magnus tenodesis for patellar dislocation.
Technique and preliminary results. Clin Orthop Relat
Re. 1993;(297):12–16.
Teitge RA. Treatment of complications of patellofemoral joint surgery. Oper Tech Sports Med.
1994;4:317–33.
Gallie WE, Lemesurier AB. Habitual dislocation of
the patella. J Bone J Surg. 1924;6(3):575–82.
Monllau JC, Masferrer-Pino A, Ginovart G, et al.
Clinical and radiological outcomes after a quasianatomical reconstruction of medial patellofemoral
ligament with gracilis tendon autograft. Knee Surg
Sports Traumatol Arthrosc. 2017;25(8):2453–9.
Seitlinger G, Moroder P, Fink C, et al. Acquired
femoral flexion deformity due to physeal injury
during medial patellofemoral ligament reconstruction. Knee. 2017;24(3):680–5.
Sanchis-Alfonso V. Guidelines for medial patellofemoral ligament reconstruction in chronic lateral
patellar instability. J Am Acad Orthop Surg.
2014;22:175–82.
Sanchis-Alfonso V, Ramírez-Fuentes C, MontesinosBerry E, et al. Femoral insertion site of the graft used
to replace the medial patellofemoral ligament influences the ligament dynamic changes during knee
flexion and the clinical outcome. Knee Surg Sports
Traumatol Arthrosc. 2017;25(8):2433–41.
Wang C, Kernkamp WA, Li C, et al. Elongation and
orientation pattern of the medial patellofemoral
ligament during lunging. J Orthop Res. 2021;39
(9):2036–47.
Pérez-Prieto D, Capurro B, Gelber PE, et al. The
anatomy and isometry of a quasi-anatomical reconstruction of the medial patellofemoral ligament. Knee
Surg Sports Traumatol Arthrosc. 2017;25(8):2420–3.
Schöttle PB, Schmeling A, Rosenstiel N, et al.
Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. Am J Sports Med. 2007;35(5):801–4.
Ziegler CG, Fulkerson JP, Edgar C. Radiographic
reference points are inaccurate with and without a
true lateral radiograph: The importance of anatomy in
medial patellofemoral ligament reconstruction. Am J
Sports Med. 2016;44(1):133–42.
Sanchis-Alfonso V, Ramirez-Fuentes C, MontesinosBerry E, et al. Radiographic location does not ensure
a precise anatomic location of the femoral fixation
Medial Patellofemoral Ligament Reconstruction …
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
site in medial patellofemoral ligament reconstructions. Orthop J Sports Med.2017. https://doi.org/10.
1177/2325967117739252.
Chen J, Han K, Jiang J, et al. Radiographic reference
points do not ensure anatomic femoral fixation sites
in medial patellofemoral ligament reconstruction: a
quantified anatomic localization method based on the
saddle sulcus. Am J Sports Med. 2021;49(2):435–41.
Ishikawa M, Hoo C, Ishifuro M, et al. Application of
a true lateral virtual radiograph from 3D-CT to
identify the femoral reference point of the medial
patellofemoral ligament. Knee Surg Sports Traumatol Arthrosc. 2021. https://doi.org/10.1007/s00167020-06403-9.
Fujino K, Tajima G, Yan J, et al. Morphology of the
femoral insertion site of the medial patellofemoral
ligament. Knee Surg Sports Traumatol Arthrosc.
2015;23(4):998–1003.
Viste A, Chatelet F, Desmarchelier R, et al. Anatomical study of the medial patello-femoral ligament:
landmarks for its surgical reconstruction. Surg Radiol
Anat. 2014;36(8):733–9.
Smirk C, Morris H. The anatomy and reconstruction
of the medial patellofemoral ligament. Knee. 2003;10
(3):221–7.
Wijdicks CA, Griffith CJ, LaPrade RF, et al. Radiographic identification of the primary medial knee
structures. J Bone Joint Surg Am. 2009;91(3):521–9.
Ishikawa M, Hoo C, Ishifuro M, et al. Application of
a true lateral virtual radiograph from 3D-CT to
identify the femoral reference point of the medial
patellofemoral ligament. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3809–17.
Malatray M, Magnussen R, Lustig S, et al. Lateral
retinacular release is not recommended in association
to MPFL reconstruction in recurrent patellar dislocation. Knee Surg Sports Traumatol Arthrosc.
2019;27(8):2659–64.
Merican AM, Amis AA: Anatomy of the lateral
retinaculum of the knee. https://www.ncbi.nlm.nih.
gov/pubmed/18378934. J Bone Joint Surg Br.
2008;90(4):527–534.
Migliorini F, Trivellas A, Colarossi G, et al. Singleversus double-bundle patellar graft insertion for
isolated MPFL reconstruction in patients with
patellofemoral instability: a systematic review of
the literature. Arch Orthop Trauma Surg. 2020;140
(6):769–76.
Migliorini F, Trivellas A, Driessen A, et al. Graft
choice for isolated MPFL reconstruction: gracilis
versus semitendinosus. Eur J Orthop Surg Traumatol.
2020;30(5):763–70.
Fathalla I, Holton J, Ashraf T. Examination under
anesthesia in patients with recurrent patellar dislocation: prognostic study. J Knee Surg. 2019;32
(4):361–5.
Shultz CL, Schrader SN, Packard BD, et al. Is
diagnostic arthroscopy at the time of medial
patellofemoral ligament reconstruction necessary?.
429
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
Orthop J Sports Med. 2020;8(8):2325967120945
654.
Pérez-Prieto D, Portillo ME, Torres-Claramunt R,
et al. Contamination occurs during ACL graft
harvesting and manipulation, but it can be easily
eradicated. Knee Surg Sports Traumatol Arthrosc.
2018;26(2):558–62.
Gould HP, Delaney NR, Parks BG, et al. Interference
screw versus suture anchors for femoral fixation in
medial patellofemoral ligament reconstruction: a
biomechanical study. Orthop J Sports Med. 2021.
https://doi.org/10.1177/2325967121989282.
Ackermann J, Mestriner AB, Merkeley G, et al.
Femoral interference screw insertion significantly
increases graft tension in medial patellofemoral
ligament reconstruction. Knee Surg Sports Traumatol
Arthrosc. 2021;29(9):2851–6.
Mountney J, Senavongse W, Amis AA, et al. Tensile
strength of the medial patellofemoral ligament before
and after repair or reconstruction. J Bone Joint Surg
Br. 2005;87(1):36–40.
Stephen JM, Kittl C, Williams A, et al. Effect of
medial patellofemoral ligament reconstruction
method on patellofemoral contact pressures and
kinematics. Am J Sports Med. 2016;44(5):1186–94.
Stephen JM, Lumpaopong P, Deehan DJ, et al. The
medial patellofemoral ligament: Location of femoral
attachment and length change patterns resulting from
anatomic and nonanatomic attachments. Am J Sports
Med. 2012;40(8):1871–9.
Melegari TM, Parks BG, Matthews LS. Patellofemoral contact area and pressure after medial
patellofemoral ligament reconstruction. Am J Sports
Med. 2008;36(4):747–52.
Sanchis-Alfonso V, Ginovart G, Alastruey-Lopez D,
et al. Evaluation of patellar contact pressure changes
after static versus dynamic medial patellofemoral
ligament reconstructions using a finite element
model. J Clin Med. 2019. https://doi.org/10.3390/
jcm8122093.
Kim JM, Sim JA, Yang HY, et al. Clinical comparison of medial patellofemoral ligament reconstruction
with or without tibial tuberosity transfer for recurrent
patellar instability. Am J Sports Med. 2021;49
(12):3335–43.
Sanchis-Alfonso V. How to deal with chronic
patellar instability: What does the literature tell us?
Sports Health: A Multidisciplinary Approach. 2016;8
(1):86–90.
Caplan N, Lees D, Newby M, et al. Is tibial
tuberosity-trochlear groove distance an appropriate
measure for the identification of knees with patellar
instability? Knee Surg Sports Traumatol Arthrosc.
2014;22(10):2377–81.
Matsushita T, Kuroda R, Oka S, et al. Clinical
outcomes of medial patellofemoral ligament reconstruction in patients with an increased tibial
tuberosity-trochlear groove distance. Knee Surg
Sports Traumatol Arthrosc. 2014;22(10):2438–44.
430
45. Hiemstra LA, Kerslake S, Lafave MR, et al. Patella
alta is reduced following MPFL reconstruction but
has no effect on quality-of-life outcomes in patients
with patellofemoral instability. Knee Surg Sports
Traumatol Arthrosc. 2021;29(2):546–52.
46. Bartsch A, Lubberts B, Mumme M, et al. Does
patella alta lead to worse clinical outcome in patients
who undergo isolated medial patellofemoral ligament
reconstruction? A systematic review. Arch Orthop
Trauma Surg. 2018;138(11):1563–73.
47. Fujii Y, Nakagawa S, Arai Y, et al. Clinical
outcomes after medial patellofemoral ligament reconstruction: an analysis of changes in the patellofemoral joint alignment. Int Orthop. 2021;45(5):1215–
22.
48. Menetrey J, Putman S, Gard S. Return to sport after
patellar dislocation or following surgery for patellofemoral instability. Knee Surg Sports Traumatol
Arthrosc. 2014;22(10):2320–6.
49. Sappey-Marinier E, Sonnery-Cottet B, O´Loughlin P,
et al. Clinical outcomes and predictive factors for
failure with isolated MPFL reconstruction for recurrent patellar instability: a series of 211 reconstructions with a minimum follow-up of 3 years. Am J
Sports Med. 2019;47(6):1323–30.
50. Schneider DK, Grawe B, Magnussen RA, et al.
Outcomes after isolated medial patellofemoral ligament reconstruction for the treatment of recurrent
V. Sanchis-Alfonso et al.
51.
52.
53.
54.
lateral patellar dislocations: a systematic review and
meta-analysis. Am J Sports Med. 2016;44(11):2993–
3005.
Platt BN, Bowers LC, Magnuson JA, et al. Return to
sport after medial patellofemoral ligament reconstruction: a systematic review and meta-analysis.
Am J Sports Med. 2021. https://doi.org/10.1177/
0363546521990004.
Hurley ET, Markus DH, Mannino BJ, et al. Patients
unable to return to play following medial patellofemoral ligament reconstructions demonstrate poor
psychological readiness. Knee Surg Sports Traumatol Arthrosc. 2021. https://doi.org/10.1007/s00167021-06440-y.
Moreland CM, SZhaw KA, Burks R, et al. Primary
medial patellofemoral ligament reconstruction in
military service members: can we reliably restore
preinjury function and stability?. Orthop J Sports
Med. 2021.
https://doi.org/10.1177/23259671211
013334.
Marot V, Sanchis-Alfonso V, Perelli S, et al. Isolated
reconstruction of medial patellofemoral ligament
with an elastic femoral fixation leads to excellent
clinical results. Knee Surg Sports Traumatol
Arthrosc. 2021;29(3):800–5.
Minimal Invasive MPFL
Reconstruction Using Quadriceps
Tendon
Christian Fink
1
Historical Perspective
In 2011, as president of the German speaking
Arthroscopy Association (AGA) I was invited as
a guest speaker to the 2nd Balkan Congress of
Arthroscopy, Sport Traumatology, and Knee
Surgery in Ohrid, Macedonia. In a busy period of
my practice, I was not particular keen to go there
initially, but in the end this trip changed the way
of treating my patellofemoral patients up to now.
As one of the first speaker of the meeting Prof.
Matthias Veselko from Ljubljana presented his
technique of MPFL reconstruction using a strip
of quadriceps tendon (QT) [1].
At this time MPFL reconstruction in general
had just become more and more popular replacing the retinacular repairs and duplications as
well as the tibial tubercle transfers, which one or
the other (or both) we have been doing for almost
all the patellar dislocations at that time. Most of
the MPFL reconstruction techniques at this time
used hamstring grafts (HS), commonly the gracilis tendon [2, 3]. This was exactly what I was
doing at this stage.
C. Fink (&)
Gelenkpunkt Sport and Joint Surgery, Innsbruck,
Austria
e-mail: C.fink@gelenkpunkt.com
Research Unit for Orthopedic Sports Medicine
and Injury Prevention, UMIT Hall, Tirol, Austria
However, at the same time I was very interested in the QT for ACL reconstruction. In order
to reduce the morbidity of open tendon harvest I
was working on the development a new instrumentation to allow for a more precise and easier
QT graft harvest.
Following the presentation of Prof. Veselko
my head kept spinning. This strip of QT he used
for his technique looked just so much more like
the natural flat and thin MPFL (Fig. 1) than the
hamstring graft I was currently using. Most of
all, this technique avoided anchors or drill holes a
common worry not only to me, but many of my
surgeons friends. I was wondering why this
technique was not used more commonly around
the globe.
Looking at this presentation (I took a lot of
pictures) again and again on my way back from
Macedonia I thought I discovered a possible
reason. Conventional QT harvest for ACL or
PCL reconstruction requires a fairly extended
longitudinal incision over the thigh. This was
sometimes associated with some ugly scar formation and a possible reason why QT as a primary ACL graft was also not really popular at
this stage (Fig. 2). Competing with a 2 cm incision necessary for HS harvest this was not
exactly making you a popular surgeon especially
within a female patient community.
So, I was convinced about the technique the
first minute I saw it but I realized in order to
make this technique more popular a minimal
invasive harvesting technique for the QT just like
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_28
431
432
C. Fink
A
B
Fig. 1 Anatomical dissection of the native MPFL (A) compared to a reconstructed one using a QT strip (B)
Fig. 2 Example of a scar
following conventional
quadriceps tendon harvest
for reconstruction of the anterior (ACL) or posterior (PCL) cruciate ligament would be helpful.
In the next few months, I went to the anatomy
lab to do some anatomical dissections and also
talked to the engineer I was working with at the
KARL STORZ company to make some modification on the ACL harvesting instruments we were
developing. All we really needed was to define a
new tendon separator of 3 mm thickness instead
of the 5 mm used for ACL/PCL graft harvest.
After a few trials in the lab the new minimal
invasive technique for quadriceps MPFL reconstruction was born [4].
Parallel to these developments I went through
the literature and realized that this technique with
some modification has been around for a few
years already and that very encouraging clinical
results had been published.
The first description of partial-thickness QT
graft MPFL reconstruction was by Burks and
Luker in 1997 [5]. This was a free graft technique, harvesting a strip of QT with a patella bone
block, which was placed into a recessed bony bed
in the femoral epicondyle and secured with a
screw/washer. The QT end of the graft was
secured through a bone tunnel on the patella side.
Minimal Invasive MPFL Reconstruction Using Quadriceps Tendon
Steensen et al. in 2005 [6] were the first to
describe leaving the quadriceps tendon attached
on the patella side. Harvesting a partial thickness
quadriceps tendon graft, they extended dissection
distally over the anterior patella elevating the
thick periosteum. By dissecting further distal
laterally than medially they created a diagonal
hinge point, allowing the graft to fold into position medially on an intact periosteal pedicle.
A 5 cm midline longitudinal incision was made
extending proximally from the superior pole of
the patella. A partial thickness quadriceps tendon
graft, 10–12 mm wide, was harvested from the
central third of the quadriceps tendon.
Shortly after Steensen et al. [6], in 2005
Noyes and Albright [7] published a technique,
also based on an intact graft pedicle on the
patella side. They harvested an 8 70 mm fullthickness graft from the medial (rather than
central) aspect of the QT. This was left attached
at the superomedial border of the patella, passed
medially beneath the medial retinaculum and
sutured to the medial intermuscular septum. Due
to non-anatomical femoral fixation, this is technically not an MPFL reconstruction, but a medial
reinforcement.
On one of the following international Knee
meetings I got to know Prof. Deepak Goyal from
India, who was using a QT MPFL technique for
several years. He published his clinical results
and the technique with bony femoral fixation in
2013 [8]. He harvests the central 10–12 mm of
the QT superficial lamina, via a 7–8 cm longitudinal incision starting at the superior pole of
the patella. The proximal free end of the graft
was tunneled medially between the capsule and
medial retinaculum. No.2 Ethibond® stay sutures
were placed at junction of the medial edge of the
patella and the graft to stabilize the graft-patella
anatomic attachment and finally, the graft is
secured in the distal femur with a biointerference screw rather than transosseus
sutures as described by Steenson et al.[6].
Proudly I presented my “discoveries” and my
technique to friends who I knew being involved
with patellofemoral surgeries for years. They all
used hamstring MPFL techniques at this time.
433
However, there was not only interest but a lot of
skepticisms, most of all questioning the strength
of the patellar graft fixation. Was fixation of a
detached and diverged periosteum strip only with
sutures at the medial edge of the patella really
strong enough to withstand the forces?
There was nothing in the literature about this
topic. So again, I knew if this technique was
about to get more popular, we needed both
biomechanical as well as clinical data.
I knew that a group in Münster Germany had
just published on the biomechanical characteristics of different MPFL fixation methods for
hamstring graft on the patella [9]. This setup
seemed perfect for testing the QT construct and
would also allow for direct comparisons not only
to the characteristics of the natural MPFL but
also in comparison to the commonly used hamstring techniques.
I contacted one of the authors (Prof. Mirco
Herbort) of the paper whom I knew and presented my ideas. He was immediately interested
and soon afterwards we started the biomechanical project. I flew to Münster in order to
demonstrate and train them in the surgical technique. I did not want to be part of the further
procedures and the testing itself in order to avoid
bias.
A few weeks later I got a phone call from
Prof. Herbort late at night. He sounded really
excited. Not only was the maximum pullout
strength equivalent or higher than the natural
MPFL but the stiffness of the construct also
closely resembled that of the natural MPFL.
The biomechanical results and the good clinical impression we got from the first patients
encouraged us to push this technique forward
[10].
2
Anatomy and Considerations
for QT Graft Harvest
The native MPFL is a broad flat structure
approximately 1 mm thick arising from a broad
origin on the femur approximately 9–17 mm in
width and located within a triangle formed by the
434
C. Fink
adductor tubercle, medial femoral epicondyle
and gastrocnemius tubercle [11–14]. It has a
similarly broad insertion on the patella
(24 mm ±5 mm), occupying approximately the
upper half of the length of the patella articular
surface. Hence the native MPFL is morphologically more similar to a broad flat QT graft, than a
tubular HS graft. Interestingly, embryologically,
the MPFL and QT are both formed from the
same origin, ventral mesenchyme, whilst the HT
originates in the dorsal mesenchyme [8].
Given the native QT width (44 mm), harvesting a 10–12 mm wide graft will usually
constitute 20–30% of the QT width. QT thickness increases steadily as aponeurotic layers of
the extensor apparatus join, reaching a maximal
thickness of 7.9 mm distally (range 6.5 to
9.5 mm)[15]. Therefore, a 3 mm deep graft will
constitute less than half the depth distally. Due to
proximal tendon narrowing and thinning, the
graft constitutes a relatively larger proportion of
the volume proximally. However, volumetric
MRI studies have shown that a full thickness
10 mm 80 mm graft constitutes 39% by volume [16]. A 3 mm deep graft therefore is likely
to constitute only around 20% by volume and no
donor site problems have been reported in any
published studies.
3
Biomechanics
Herbort et al. [17], found that in a human
cadaveric model the biomechanical characteristics of a 3 mm thick by 10 mm wide QT strip
[stiffness 33.6 N/mm (±6.8), yield load 147.1 N
(±65.1),maximum load to failure 205 N
(±77.8)] were very similar to that of the native
MPFL [stiffness 29.4 N/mm (±9.8), yield load
167.8 N (±80), maximum load to failure
190.7 N (±82.8)], whilst Lenschow et al. [9]
found that HT constructs are about 3stiffer (87–
100 N/mm). Therefore, QT grafts may more
closely restore native MPFL kinematics and may
be more forgiving of variations in position and
tension. Stiffer HT grafts may be more sensitive
to over-tensioning or malpositioning, which can
lead to increased patellofemoral joint stress
compression forces and lead to restricted motion.
4
Surgical Technique
4.1 Patient Positioning
and Arthroscopy
Patient positioning has to allow free knee motion
between 0° and 120°.
The intraoperative access for the fluoroscope
is important to be kept in mind and ideally
checked prior to draping. We prefer fixation of
the operative leg in an electric leg holder
(Fig. 3A).
An arthroscopy is performed initially, to
inspect the articular cartilage in the patellofemoral joint and to evaluate patella tracking
(Fig. 3B). The latter is best visualized through a
superolateral portal for the arthroscope.
4.2 Graft Harvest
In 90° of knee flexion a 3 cm transverse skin
incision is placed over the superomedial margin
of the patella (Fig. 4A). The prepatellar bursa is
incised longitudinally and the quadriceps tendon
is then carefully exposed. A long Langenbeck
retractor (Fig. 4B) is then introduced and the
quadriceps tendon subcutaneously exposed
proximal to the patella.
Step 1: A double knife (Karl Storz, Tuttlingen) in 10 or 12 mm width is then introduced. It
is pushed proximally to a minimum of 9 cm
(mark on the instrument) (Fig. 5A and B).
Step 2: The thickness of the graft is then
determined with 3 mm by a tendon separator
(Karl Storz, Tuttlingen). The separator is angled
about 30 degree and pushed proximally to the
same mark (minimum 9 cm) (Fig. 6A and B).
Step 3: Finally, the tendon strip is subcutaneously cut using a special tendon cutter (Karl
Storz, Tuttlingen) (Fig. 7A and B).
Minimal Invasive MPFL Reconstruction Using Quadriceps Tendon
A
435
B
Fig. 3 Positioning of the patient. A The operated knee is placed in an electric leg holder. B Arthroscopy is performed
prior to graft harvest
A
B
Fig. 4 A Placement of the skin incision at the superomedial aspect of the patella. B A long Langenbeck retractor is
inserted to allow proper visualization of the quadriceps tendon
436
C. Fink
B
A
Fig. 5 Graft harvest—Step I: Double knife of 10 or 12 mm (KARL STORZ, Tuttlingen) pushed proximally 8—10 cm
above the superior patella boarder (A schematic drawing, B operative procedure)
Fig. 6 Graft harvest—Step 2:
Tendon Separator (3 mm)
(KARL STORZ, Tuttlingen)
pushed proximally to the
same length (8–10 cm)
(A schematic drawing,
B. operative procedure)
A
4.3 Patella Preparation
The free proximal end is sheathed with resorbable sutures (Fig. 8A) in a web-stitch technique
(Fig. 8B). The diameter of the free tendon end is
measured using an ACL graft sizer (Fig. 8C).
Distally the longitudinal cuts are continued in
the same width (10 or 12 mm) with a surgical
knife towards the patella and over the patellar
surface (2 cm-lateral and 1 cm-medial). The
quadriceps tendon strip is than subperiostally
elevated from the surface of the patella (Fig. 9A
B
and B). The proximal 1.5 cm of the medial
patellar border is then exposed.
Using a periosteal elevator the prepatellar tissue
is lifted from the medial patella border (Fig. 10A)
creating a subperiosteal tunnel (Fig. 10B).
A surgical clamp is introduced into the tunnel
from medial to lateral and by grasping the sutures
the graft is passed through. The graft diverged 90°
and left attached to the periosteum (Fig. 11A and
B). It is then secured at the medial boarder of the
medial patellar (equivalent to the attachment of
the natural MPFL) by resorbable No. 1 sutures.
Minimal Invasive MPFL Reconstruction Using Quadriceps Tendon
A
437
B
Fig. 7 Graft harvest—Step 3: The tendon strip is cut at the desired length (8–10 cm) using a special Tendon cutter
(KARL STORZ, Tuttlingen) (A schematic drawing, B operative procedure)
A
B
C
Fig. 8 A The free proximal end is sheathed with resorbable sutures in a B locked web-stitch technique. C the tendon
diameter is measured
438
C. Fink
*
°
A
B
Fig. 9 The preparation of the tendon strip is extended distally on the patella (°lateral 1.5 to 2 cm and *medial 0.5 to
1 cm (A schematic drawing, B operative procedure)
A
B
Fig. 10 The prepatellar tissue is lifted from the medial patella border (Fig. 10A) using a periosteal elevator creating a
subperiosteal tunnel (Fig. 10B)
4.4 Femoral Preparation
A 1.5 cm skin incision is then made over the
adductor tubercle. Under fluoroscopic guidance a
2.4 mm guide pin is drilled into the insertion of
the MPFL (Fig. 12) [3]. It is directed anterolaterally to exit the femur on the lateral cortex
well proximal to the lateral epicondyle. If found
accurate by fluoroscopy the guide pin is over
reamed with a cannulated reamer according to
the diameter of the graft (most commonly 6–
8 mm) to a depth of 30 mm.
Starting at the medial boarder of the patella a
long curved clamp is used to create a tunnel in
the space between the vastus medialis and the
joint capsule (Layer 2 and 3). A suture loop is
Minimal Invasive MPFL Reconstruction Using Quadriceps Tendon
A
439
B
Fig. 11 The QT strip diverged 90° and left attached at the periosteum. (A schematic drawing, B operative procedure)
then pulled through the tunnel. This loop is used
later to pull the graft towards the femoral insertion (Fig. 13A and B).
The graft is then pulled into the tunnel. The
knee is cycled 5 times with moderate tension on
the graft. Fixation is performed with a bioabsorbale interference screw (with a equivalent
diameter to the tunnel diameter) at 40–60 degrees
of knee flexion (Fig. 14A). The lateral border of
the patella should be flush with the lateral border
of the trochlear groove.
Alternatively, and generally in children with
open physis the graft is fixed with a bone anchor
and additional sutures (Fig. 14B).
5
Pearls and Pitfalls
5.1 Pearls
• Careful dissection is necessary to expose the
QT (including removal of all the bursal and
superficial layers).
• The QT is longest when starting slightly lateral over the center of the patella.
• The QT can be inspected using the arthroscope before harvesting.
• Be sure you have enough graft length (minimum 9 cm in an average patient).
5.2 Pitfalls
• The QT strip could peel off the bony surface
of the patella.
– To avoid a “peel off,” dissection must be
performed carefully. If “peel off” occurs
and the graft is amputated from the patella,
bone anchors may be used to fix the QT
strip to the medial aspect of the patella
(free QT graft) or if the graft is long
enough it can be looped through the prepatellar tissue and sutured on to itself.
• The QT strip could be too short.
– It is important to angle the tendon separator 30° down, in order to avoid “cutting
out” anteriorly leading to premature graft
440
C. Fink
Fig. 12 Fluoroscopic control of the guide wire placement [according to Schöttle et al. [3]]
amputation. We had one case in our clinical series where the QT strip was cut too
short (5 cm). In this case a second 3 cm
strip was harvested and sutured to the
primary one. Alternatively, a strip of
adductor tendon could have been harvested, left attached to the femur and
sutured to the QT graft.
• As the MPFL functions as a check-rein, it is
important to avoid over tightening.
– Graft fixation at the desired length should
be performed in 40–60 degrees flexion
with just enough tension to align the
patella with the lateral trochlea.
6
Postoperative Treatment
We use a hinged knee brace with ROM 0–90° for
the first 2 postoperative weeks. The patient is
mobilized immediately following surgery with
20 kg partial weight bearing for 3 weeks. Full
weight bearing is started thereafter. Passive ROM exercises are initiated immediately
postoperatively. Stationary cycling is started
around 6 weeks postop. Full return to pivoting
sports is between 4 and 5 months after the
operation [18].
Minimal Invasive MPFL Reconstruction Using Quadriceps Tendon
441
B
A
Fig. 13 A, B The graft is pulled in between layer 2 and 3 towards the femoral incision using a long clamp
Fig. 14 A The QT graft is
fixed in 20° of knee flexion
with a bioabsorbable screw in
the same diameter as the bone
tunnel. B Alternatively or in
children the graft is fixed with
a bone anchor and sutures
A
7
Clinical Outcome
In a study published by Gföller et al. [19] we
included a consecutive series of 36 Patients (38
knees). All of these patients had>2patella dislocations, a TT-TG<20 mm, and no patellofemoral
chondromalacia<ICRS grade IIIB. MPFL reconstruction was performed by our minimal invasive
QT technique described above. All patients were
evaluated clinically and with patient reported
B
outcome questionnaires including the Tegner-[20],
Lysholm-[21] and Kujala–[22] Scores as well as
the Visual Analogue Scale (VAS) for pain preoperatively and at 6, 12 and 24 months postoperatively. A functional Back-in-Action (BIA)
test battery, including a total of seven different
stability, agility and jumping tests, was performed
on 19 (50%) patients at final follow-up. One Patient
was lost to follow-up at 24 months.
The mean age at time of operation was 25.2 ±
6.1 years. No re-dislocations occurred during the
442
C. Fink
period of investigation. The mean Lysholm Score
improved significantly (p < 0.05) from 79.3 ±
16.1 pre-operatively to 83.2 ± 14.4 at 6 m,
88.1 ± 11.3 at 12 m and to 90.0 ± 9.6 at
24 months follow-up. No change throughout the
study period was observed for the median Tegner
Activity Score (median = 6). The mean Kujala
Score increased from a pre-operative value of
82.0 ± 12.4, to 84.5 ± 8.4 at 6 m, 88.2 ± 5.8 at
12 months up to 88.7 ± 4.5 at 24 months followup. 77.8% of the performed functional BIA tests
were equal or above of the norm for patients of
the corresponding age and activity level.
8
Discussion
QT MPFL reconstruction has been shown to be a
safe technique with high success at preventing
recurrent dislocations and fewer complications
than HT techniques [23, 24]. QT grafts provide a
thin, broad strip of tissue with a continuous
anatomic attachment along the superior half of
the medial border of the patella that is anatomically and biomechanically more similar to the
native MPFL than HT grafts [17, 23]. Maintaining an intact graft pedicle on the patella
means that patella bone tunnel drilling or suture
anchor placement is not necessary, reducing
fracture risk.
Long incisions described for open QT graft
harvesting may have deterred surgeons from
using this technique, however a minimal invasive
QT harvesting techniques offer potentially better
cosmetic results than both open QT and HT
techniques. On the other hand, the option to
harvest QT via a midline incision means that
QT MPFL reconstruction combines well with
trochleaplasty via the same incision.
Overall, QT is a valuable alternative to common HT grafts for primary MPFL reconstruction
in children [25] and adults, and is an important
revision surgery option.
References
1. Macura M, Veselko M. Simultaneous reconstruction
of ruptured anterior cruciate ligament and medial
patellofemoral ligament with ipsilateral quadriceps
grafts. Arthroscopy. 2010;26(9):1258–62.
2. Christiansen SE, Jacobsen BW, Lund B, Lind M.
Reconstruction of the medial patellofemoral ligament
with gracilis tendon autograft in transverse patellar
drill holes. Arthroscopy. 2008;24(1):82–7.
3. Schoettle PB, Schmeling A, Romero J, Weiler A.
Anatomical reconstruction of the medial patellofemoral ligament using a free gracilis autograft. Arch
Orthop Trauma Surg. 2009;129(3):305–9.
4. Fink C, Veselko M, Herbort M, Hoser C. Minimally
invasive reconstruction of the medial patellofemoral
ligament using quadriceps tendon. Arthrosc Tech.
2014;12;3(3): e325—9
5. Burks RT, Luker MG. Medial patellofemoral ligament reconstruction techniques in orthopaedics. 1997.
6. Steensen RN, Dopirak RM, Maurus PB. A simple
technique for reconstruction of the medial patellofemoral ligament using a quadriceps tendon graft.
Arthroscopy. 2005;21(3):365–70.
7. Noyes FR, Albright JC. Reconstruction of the medial
patellofemoral ligament with autologous quadriceps
tendon. Arthroscopy. 2006;22(8):904 e901–907.
8. Goyal D. Medial patellofemoral ligament reconstruction: The superficial quad technique. Am J Sports
Med. 2013;41:1022–9.
9. Lenschow S, Schliemann B, Gestring J, Herbort M,
Schulze M, Kösters C. Medial patellofemoral ligament reconstruction: fixation strength of 5 different
techniques for graft fixation at the patella. Arthroscopy. 2013;29(4):766–73.
10. Fink C, Veselko M, Herbort M, Hoser C. MPFL
reconstruction using a quadriceps tendon graft: Part
2: operative technique and short term clinical results
Knee. 2014;21(6):1175–9.
11. Aframian A, Smith TO, Tennent TD, Cobb JP,
Hing CB. Origin and insertion of the medial
patellofemoral ligament: a systematic review of
anatomy. Knee Surg Sports Traumatol Arthrosc.
2017;25:3755–72.
12. Amis AA, Firer P, Mountney J, Senavongse W,
Thomas NP. Anatomy and biomechanics of the
medial patellofemoral ligament. Knee. 2003;10
(3):215–20.
13. Andrikoula S, Tokis A, Vasiliadis H, Georgoulis A.
The extensor mechanism of the knee joint: an
anatomical study. Knee Surgery, Sport. Traumatol.
Arthrosc. J Article. 2006;14:214–220. Springer,
Berlin.
Minimal Invasive MPFL Reconstruction Using Quadriceps Tendon
14. Dirim B, Haghighi P, Trudell D, Portes G, Resnick D.
Medial patellofemoral ligament: cadaveric investigation of anatomy with MRI, MR arthrography, and
histologic correlation. AJR Am J Roentgenol.
2008;191(2):490–8.
15. Grob K, Manestar M, Filgueira L, Ackland T,
Gilbey H, Kuster MS. New insight in the architecture
of the quadriceps tendon. J Exp Orthop. 2016;3(1):32
16. Xerogeanes JW, Mitchell PM, Karasev PA,
Kolesov IA, Romine SE. Anatomic and morphological evaluation of the quadriceps tendon using 3dimensional magnetic resonance imaging reconstruction: applications for anterior cruciate ligament
autograft choice and procurement. Am J Sports
Med. 2013;41(10): 2392–9.
17. Herbort M, Hoser C, Domnick C, Raschke MJ,
Lenschow S, Weimann A, Kösters C, Fink C. MPFL
reconstruction using a quadriceps tendon graft. Part
1: Biomechanical properties of quadriceps tendon
MPFL Reconstruction in comparison to the
Intact MPFL. A Human Cadaveric Study. Knee.
2014;21(6):1169—74.
18. Fisher B, Nyland J, Brand E, Curtin B. Medial
patellofemoral ligament reconstruction for recurrent
patellar dislocation: a systematic review including
rehabilitation and return-to-sports efficacy. Arthroscopy. 2010;26(10):1384–94.
19. Gföller P, Hoser C, Runer A, Abermann E, Wierer G,
Fink C. Medial patellofemoral ligament (MPFL)
20.
21.
22.
23.
24.
25.
443
reconstruction using quadriceps tendon autograft
provides good clinical, functional and patientreported outcome measurements (PROM): a 2-year
prospective study. Knee Surg Sports Traumatol
Arthrosc. 2019;27(8):2426–32.
Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat
Res. 1985;198:43–9.
Lysholm J, Gillquist J. Evaluation of knee ligament
surgery results with special emphasis on use of a
scoring scale. Am J Sports Med. 1982;10:150–4.
Kujala UM, Jaakkola LH, Koskinen SK, Taimela S,
Hurme M. Nelimarkka O. Scoring of patellofemoral
disorders. Arthroscopy. 1993;9:159–63.
Fink C, Steensen R, Gföller P, Lawton R. Quadriceps
tendon autograft medial patellofemoral ligament
reconstruction. Curr Rev Musculoskelet Med.
2018;11(2):209–20.
Shah JN, Howard JS, Flanigan DC, Brophy RH,
Carey JL, Lattermann C. A systematic review of
complications and failures associated with medial
patellofemoral ligament reconstruction for recurrent
patellar dislocation. Am J Sports Med. 2012;40
(08):1916–23.
Nelitz M, Williams SR. Anatomic reconstruction of
the medial patellofemoral ligament in children and
adolescents using a pedicled quadriceps tendon graft.
Arthrosc Tech. 2014;3(2):e303–8.
Combined Medial Patellofemoral
Ligament and Medial Patellotibial
Ligament Reconstruction
Robert S. Dean, Betina B. Hinckel,
and Elizabeth A. Arendt
1
Introduction
Lateral patellar dislocations (LPD) have a
reported incidence of 23.2 per 100,000 adolescents each year [1], with nearly equal sex distribution [2]. Recurrence is common; a recent
systematic review found the overall rate of
recurrent dislocation following first-time LPD
was 33.6% [3].
There are multiple anatomical considerations
that are risk factors for LPD, both primary and
recurrent [3–5] (ref C). Important anatomic risk
factors include open physis, patellar alta, and
trochlear dysplasia, e.g., Generalized hyperlaxity
including Ehlers-Danlos can increase the risk for
instability/dislocation [6].
The medial patellar ligaments are responsible
for the lateral stability of the patellofemoral joint.
They include three primary structures, the medial
patellofemoral ligament (MPFL), the medial
patellotibial ligament (MPTL) and the medial
patellomeniscal ligament (MPML) [7]. Injuries to
any of these structures can lead to lateral instability events which can incite lack of knee confidence, pain and at times cartilage degeneration
R. S. Dean B. B. Hinckel (&)
Beaumont Health, Royal Oak, MI, USA
e-mail: betinahinckel@gmail.com
E. A. Arendt
University of Minnesota, Minneapolis, MN, USA
[8]. While the MPFL has been the focus of the
majority of biomechanical and clinical studies,
the MPTL and MPML both play an integral role
in patellofemoral stability and warrant further
consideration for patients presenting with lateral
instability [9, 10].
Many surgical techniques and subsequent
outcomes studies have described MPFL reconstruction in detail, but this book chapter aims to
demonstrate the importance of the MPTL and
MPML which collectively are referred as the
distal medial patellar constraints. The anatomy
and biomechanics, clinical work-up, and surgical
techniques will be described, and outcomes of
prior surgical studies.
2
Anatomy and Biomechanics
In 1974, Slocum et al. first described an analogous structure to the MPTL and the MPML
which they described as a single structure. These
authors described it as a single reinforcing band
that arises from the lower margin of the articular
segment of the patella and passed in an oblique
fashion, inferiorly and medially, before inserting
at the anteromedial aspect of the tibia; they also
reported that the band had some attachment to
the medial meniscus [11].
An anatomic study by the current authors
described the MPTL originating 3.6 mm proximal to the distal border of the patella. The course
is 28° relative to the patellar tendon. The average
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_29
445
446
length of the MPTL is 36.4 mm and the width is
7.1. Radiographic evidence demonstrates that the
tibial attachment is 9.4 mm from the joint line
and in line with the medial border of the medial
tibial spine [12].
The MPML is encountered as three distinct
layers. They originate from the inferomedial
patella (5.7 mm proximal to the distal border of
the patella), just proximal to the MPTL and insert
at the anterior meniscus, at the anterior horn or
transition from the anterior horn to the body of
the meniscus. The angulation of the ligament
relative to the patellar tendon is 22–42° when the
knee is at 90° of flexion [13].
The histological samples of both the MPTL
and the MPML demonstrated dense connective
tissue with oriented collagen fibers uniformly in
parallel and intermingled, elongated fibroblasts
consistent with ligamentous tissue [13].
The mean failure loads of the MPTL and
MPML were 147 and 105 N, respectively. It is
important to put the strength of these ligaments
in relation to the MPFL which has a reported
load to failure of 178 N [14]. In one cadaveric
study, 90% of MPTLs failed by mid-substance
rupture and 100% of MPMLs failed by midsubstance rupture. It is important to note that the
MPTL was significantly stiffer and showed less
deformation in maximum tensile strength compared to the MPFL [13].
Biomechanical cutting studies have reported
that the MPFL accounts for 50–60% of restraint
against lateral patellar instability, whereas the
MPTL and MPML combined to provide 20–40%
of the resistance in extension [15–17]. The
medial retinaculum accounts for the remaining
3–25% of restraint [15–18]. Individually, the
MPTL may provide up to 24% of restraint and
the MPML provided up to 38% of restraint near
full extension [15, 17–19].
Ebied and El-Kholy performed a sequential
sectioning study of the medial patellar stabilizers
followed by sequential repair of the sectioned
ligaments. After cutting the MPFL and leaving
the MPTL intact, lateral subluxation of the
patella was possible between 0 and 30° of knee
R. S. Dean et al.
flexion. Next, the MPTL was sacrificed in addition to the MPFL and full dislocation was
observed between 0 and 60° of knee flexion.
When reattaching only the MPFL, lateral dislocation was not possible, but subluxation was
observed between 0 and 10° of knee flexion.
After reattaching only the MPTL, some stability
was restored but frank dislocation was still
observed at full flexion and subluxation of the
patella was noted between 0 and 15°. Thus, these
authors concluded that the MPTL provided a less
significant stabilizing force than the MPFL, but
the rupture or dysfunction of the MPTL may
result in increased lateral patellar laxity which
can result in lateral patellar instability [20].
A biomechanical study by Phillippot et al.
determined that the MPTL and MPML combined
to provide approximately 46% of the restraint
forces against lateral patellar subluxation when
the knee was at 90° of flexion. Additionally, the
MPTL and MPML were responsible for 72% of
patellar tilt and 92% of patellar rotation. Unfortunately, this study did not study the MPTL and
MPML separately, but rather examined them as a
combined entity [21].
These previous conclusions were called into
question by Grantham et al. who examined the
role of the MPFL and MPTL through a sectioning biomechanical model. These authors found
that when the MPTL was sectioned the patella
tracking was similar to the native state. They
described the role of the MPTL as “complementary” to the MPFL and reported that MPTL
reconstruction in a MPFL deficient knee did not
improve knee stability. Additionally, they concluded that the MPTL provided a more significant contribution to medial stability at greater
than 30° of knee flexion [22].
Based upon these studies the distal medial
patellar complex (MPTL and MPML) is most
important during two knee motions: active terminal extension of the knee where it directly
counteracts the quadriceps contraction, and deeper knee flexion when the distal ligament complex tightens increasing its contribution to
resistant lateral patellar translation [21] (Fig. 1).
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
Fig. 1 This image depicts a cadaveric dissection of a left
knee from an anterior viewpoint. It’s important to
appreciate the medial patellotibial ligament (MPTL) and
medial patellomeniscal (MPML) ligament as unique
structures. Medial meniscus (MM), medial femoral
condyle (MFC), medial patellofemoral ligament (MPFL),
lateral femoral condyle (LFC), iliotibial band (ITB)
3
447
A traditional glide test is performed by
applying a medial or lateral force to the patella,
displacement of greater than or equal to 3
quadrants with this test is considered a positive
result. Similarly, the patellar apprehension sign is
observed when forced lateral displacement of the
patella produces anxiety and/or forced resistance
from the patient contracting their quadriceps.
A modified technique can be performed with
the quadriceps completely relaxed and knee at
full extension with the examiner applying an
equal force to both extremities, if one side has a
soft endpoint with increased translation, which
can be identified when the medial femoral trochlea is greater than one half uncovered and can
be palpated, suspicion for a medial patellar stabilizers insufficiency should be raised [23].
A patellar tilt test can be used to assess for
tightness of the lateral. The J sign signifies
patellar mal-tracking [19]. Additionally,
increased lateral patellar translation in deep
flexion suggests increased dependency on the
distal medial patellar stabilizers—MPTL and
MPML, due to insufficient support from the
trochlear groove and/or lack of engagement due
to patellar alta [24].
Tenderness over the anteromedial proximal
tibia in addition to focal tenderness over the
inferior aspect of the patella, at the insertion of
the MPTL or MPML can heighten the suspicion
for lesions to the distal medial patellar structures.
Diagnosis
3.2 Imaging
3.1 Presentation and Physical Exam
It is crucial to perform a thorough physical
examination in order to identify any concomitant
pathologies including ligamentous, muscular,
osseous or cartilaginous pathologies which can
contribute to various findings during the workup
phase of management. Exam features pertinent to
this discussion will be detailed.
Several physical exam maneuvers can be
suggestive of medial patellar stabilizers injury,
however it is essential compare all findings to the
contralateral, healthy, limb for reference.
Imaging of these injuries typically begins with
standard AP and lateral radiographs along with a
low flexion axial view. These images allow
clinicians the opportunity to appreciate any frank
dislocations, increased lateral translations or
avulsion fractures. Additionally, the lateral
radiograph is used evaluate for trochlear dysplasia as well as patellar height. Low flexion
axial views allow one to assess for sulcus depth,
patellar tilt and translation, as well as patellar
morphology. Finally, in some circumstances full
length weight bearing films can be used to
448
R. S. Dean et al.
evaluate limb alignment and are helpful because
valgus tibiofemoral alignment places more strain
on the inferomedial patellofemoral complex
susceptible [25].
MRI should be obtained to evaluate for injury
to the local soft tissues, cartilage and bone
bruising patterns. MRI has been shown to be a
reliable modality for diagnosis of MPFL tears
with a sensitivity of 85% and an accuracy of 80%
when using open exploration of the medial knee
as the “gold standard”. This same study reported
that MRI was a more accurate diagnostic
modality than arthroscopy [26]. While there are
no known studies that report on the accuracy of
advanced imaging for MPTL and MPML, injuries there are several known studies that describe
the visualization of these ligaments on MRI.
These studies reported accurate anatomical
identification of the structures as unique entities
[7, 27, 28]. As such, one can surmise that a
trained eye would likely be able to identify
lesions along the visualized structures. Thawait
et al. reported several cases with isolated injuries
to the inferior pole of the medial retinaculum,
corresponding to the MPTL and MPML, without
lateral patella dislocation or noted MPFL lesions.
They reported that these ligaments can be injured
in isolation through twisting injuries and are
likely associated with medial meniscal or
meniscocapsular lesions [28]. Tompkins et al.
reviewed MRI of primary LPD and a majority
(61%) of patellar chondral lesions were at its
inferomedial aspect; all medial patellar retinacular partial injuries involved the inferomedial
aspect of the patella, consistent with the insertion
of the medial patellotibial ligament [29] (Fig. 2).
4
Treatment Options
The indications for distal medial patella-tibial
reconstruction are evolving. Although we recognize the contribution of both MPML and
MPTL, most surgeons focus on the reconstruction of the MPTL due to the technical challenges
and risk to meniscal stability with reconstruction
of the MPML.
Fig. 2 This image depicts an axial A and sagittal B slice
of an MRI with disruption of the medial patellar
retinaculum. Increased signal intensity in this region is
highly suggestive of a medial patellotibial complex injury
The current authors consider performing
MPTL reconstruction in adjunct to MPFL
reconstruction when there is lateral patellar subluxation with quadriceps contraction with the
knee fully extended, flexion instability (obligate
dislocation in flexion), knee hyperextension
associated to generalized laxity, and/or increased
quadriceps vector due to rotational deformities
[24]. Additionally, it can be used and as adjuvant
procedure in children with significant risk factors
for recurrence of dislocation when bony surgery
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
is limited due to open physes [24]. It should also
be noted that the utilization of MPTL reconstruction in combination with MPFL reconstruction may limit the need for bony procedures
such as tibial tuberosity osteotomy and/or
trochleoplasty in certain patients. Though historically there have been studies utilizing
emphasize an isolated MPTL reconstruction for
surgical patellar stabilization, current practice
supports MPFL reconstruction as primary, and
MPTL as an adjuvant ligament restraint.
The MPTL reconstruction is performed first and
the MPFL second.
5
Isolated Procedures
5.1 Hamstrings Tenodesis
In isolation, MPTL reconstructions can be performed as a hamstring (either gracilis or semitendinosus) tenodesis. The technique was
originally described in 1972 by Baker et al. They
recommended harvesting the semitendinosus and
then mobilizing the patella by releasing the lateral
capsule and fascial band. Next, an oblique hole
was drilled across the patella in the line of the
tenodesis and the tendon was tied back on itself
[30]. Several articles proposed a similar strategy to
the aforementioned technique in children [31, 32].
5.2 Isolated MPTL Reconstruction
Zaffagnini et al. proposed a non-anatomic technique which began with a midline incision when
the knee was at 20° of flexion. The authors then
harvest the patellar tendon, with its associated
bone plug, from the medial third of the tendon.
They recommend repeated dynamic analysis of
patellar tracking in order to identify a reinsertion
point that ensured stability without excessively
tensioning the ligament or patellofemoral joint.
The quality of fixation is assessed subjectively
using direct palpation and observation. When the
correct point is established, a socket is created and
the bone plug is fixed using a cortical screw [33].
449
5.3 Combined “3 or 4 in 1”
Procedures
Myers et al. utilize a patellar tendon autograft in
addition to a lateral release and VMO advancement. After the medial retinaculum is elevated
from the tibia, the medial third of the patellar
tendon is harvested from its tibial attachment.
The graft is then transferred to the superficial
medial collateral ligament (sMCL) so that the
graft has a 40–45° angle with the remaining
patellar tendon. The graft is fixed with the knee
flexed to 30°. At the end of this technique the
VMO is advanced 5–10 mm distally and laterally
[34]. A similar technique was described in a
pediatric population by Oliva et al. A difference
between this newer technique is the fixation
modality; Oliva et al. utilizes 2 metallic suture
anchors to suture the patellar tendon graft to the
medial aspect of the tibia in addition to the
sMCL [35].
In 2007 Joo et al. proposed an adaptation of
the hamstring tenodesis where they avoided
using bone tunnels through the patella by directly
fixing the tendon to the patella using a screw.
This technique was a “4-in-1” that also involved
a lateral release, proximal “tube” realignment of
the patella, and patellar tendon transfer in addition to the hamstring tenodesis. The tendon is
pulled across the surface of the patella and the
portion that was abutting the superolateral corner
of the patella is sutured under tension using a
non-absorbable anchoring screw. The remaining
tendon is sutured to the periosteum with a
running suture, in the line of the tenodesis.
This construct is fixed with the knee at 30° of
flexion [36].
5.4 Combined MPFL and MPTL
Reconstruction
The authors’ preferred MPTL technique utilizes a
soft tissue allograft. When using an anterior tibialis allograft there is often enough width to
divide the graft into 2 parts (Fig. 3). The larger
portion can be used for the MPFL reconstruction
450
R. S. Dean et al.
Fig. 3 Two hamstring
autografts are prepared. Each
graft should be a minimum of
28 cm in length and
whipstitched at both ends
while the smaller graft can be used for the medial
patellotibial complex graft.
The surgeon can identify the inferior-medial
border of the patella at the distal end of the
cartilage border, C-arm can be used as needed.
Careful dissection through each layer of the
medical capsule ensures (Fig. 4). The anatomic
landmarks of the MPTL are identified on the
patella (Figs. 5 and 6). Fixation can be established using a small anchor such as 1.8 mm QFix (Smith and Nephew). If the patella is small or
if there are concerns about bone quality, one can
undermine the periosteum on the dorsal surface
of the patella. Using fluoroscopic guidance, the
appropriate fixation point for the distal medial
patellotibial complex can be identified on the
anteromedial tibia approximately 5–10 mm distal
to the joint line and just medial to the medial
edge of the medial tibial spine [13]. The reconstructed ligament is typically placed at a 25–30°
angle relative to the medial aspect of the patellar
tendon. This angle is equal to a diagonal line
from the inferior medial to superolateral corners
of the patella, which helps resist superolateral
migration of the patella throughout knee range of
motion [13]. Fixation can be established using a
small anchor such as 2.8 mm Q-Fix (Smith and
Nephew) (Fig. 7). The graft is then sutured to the
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
Fig. 4 This figure depicts the
medial capsule of the knee
with the layer reflected
medially
Fig. 5 This image shows the
anatomic placement of the
patellar attachment of the
medial patellofemoral
ligament, between the
proximal and middle thirst of
the patella
Fig. 6 The medial
patellofemoral tunnel is
drilled 1 cm directly lateral to
the previously identified
medial most patellar
attachment
451
452
R. S. Dean et al.
Fig. 7 This image
demonstrates the anatomical
location of the medial
patellotibial ligament, just
medial and proximal to the
distal pole of the patella.
A suture anchor is placed here
for future fixation
periosteum and back upon itself using a free
needle for additional fixation (Fig. 8 and 9). It is
easier to tension the graft in the patellar attachment. Therefore, the graft is fixed first on the
tibia, passed deep to the retinaculum and then
fixed in the patella. The final fixation and tension
should be done with the knee in 90° of flexion.
During fixation the surgeon should confirm
that the tension through the MPTL is similar to
that of the patellar tendon. This is important as to
ensure that there isn’t excessive pressure on the
medial compartment. The knee is then observed
through complete range of motion as well as
medial and lateral forces on the patella as to
assess for the degree of translation [19].
Grantham et al. proposes a slight variation of
the MPTL reconstruction aspect of the technique
using their anatomic studies. They start by
preparing a gracilis graft. From there, they
establish the MPTL patellar attachment 9.1 mm
proximal to the inferior pull with a suture anchor.
Next, they identify the tibial attachment 5 mm
distal to the joint line and 23 mm medial to the
tibial tubercle. The allograft is then tensioned
with the knee at 70° [22].
An additional non-anatomic technique was
described by Maffulli et al. who utilizes a semitendinosus autograft to reconstruct both the
MPFL and MPTL. The authors propose maintaining the native semitendinosus attachment site
and passing the graft through two bone tunnels
on the patella. The fixation is achieved by looping the graft around the adductor magnus tendon
at 30° of flexion [37]. Concerns over this technique were raised by outside authors who questioned the specific distances of the patellar
tunnels, the fixation method of the graft after
being looped around the adductor magnus tendon, in addition to the non-anatomic location of
the semitendinosus on the tibia compared to the
attachment site of the MPTL [38].
Recently, Abdelrahman et al. reports on a
combined MPFL and MPTL reconstruction in
which the MPTL reconstruction is performed
based upon a central approximation of the MPTL
and the MPML. These authors reported that it is
fundamental to identify the individual anatomic
footprint of both the MPTL and the MPML in the
tibia and the meniscus so that to place their
reconstruction with hamstring autograft at the
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
Fig. 8 The graft is passed
and both ends are fixed with
the knee at 90° of flexion
Fig. 9 In the patellar side the
graft is sutured to the
periosteum for additional
fixation
453
454
R. S. Dean et al.
Medial Patellotibial Ligament Reconstruction Techniques By Studies That Reported on Combined MPFL and MPTL
Reconstruction
Author
Graft choice
Fixation
modality
Fixation location
Fixation
angle
Combined
with
MPFL
(Y/N)
Hughston
[41]
Direct repair
(39/65)
IT band
autograft (12/65)
Patellar Tendon
autograft (12/65)
Suture
anchors vs
bone tunnels
N/A
60°
Yes
Drez [42]
Semitendinosus,
Gracilis or
Fascia Lata
Suture
anchors
“1.5 cm distal to the joint line”
0°
flexion
Yes
Brown and
Ahmad [43]
Semitendonosis
or Gracilis
Bone tunnel
with suture
Pes Anserine
60°
Yes
Ebied [20]
Semitendinosus
or Gracilis
Interference
screws?
N/A
30°
Yes
Giordano [44]
Semitendinosus
and gracilis
Suture a
nchors
N/A
35–40°
Yes
Sobhy [45]
Semitendinosus
autograft
Bone
tunnels?
N/A
45°
Yes
Hinckel [46]
Patellar tendon
autograft
Suture
anchor
Tibial: 1.5–2.5 cm below the joint line
and 15–25 mm medial to the patellar
tendon
90°
Yes
Grantham
[22]
Gracilis allograft
Suture
anchors
Patellar: 9.1 mm proximal to the
inferior pole
Tibial: 5 mm distal to joint and
23 mm medial to the tubercle
70°
Yes
Maffulli et al.
[37]
Semitendinosus
autograft
“looped
around the
AMT”
Patella: bone bunnel, looped around
the AML
Tibia: native attachment site of the
semitendinosus
30°
Yes
Abdelrahman
[39]
Semitendinosus
autograft
Suture
anchor
Tibia: the midway point in between
the anatomic insertion of the
patellotibial and patellomeniscal
insertion
90°
Yes
midpoint between these distinct anatomic points.
They also propose fixing the graft with the knee
is at 90°, where they report the ligament is at
maximal tension [39].
5.5 MPML Repair
Garth et al. reports on 2 MPML reconstruction
techniques using either an open or arthroscopic
technique [23]. The open procedure begins by
creating a 3 cm incision approximately 1 cm
medial from and parallel to the inferomedial
margin of the patella. Careful dissection ensues
down to the third layer of the capsule.
The MPML fibers are identified and advanced
proximally and laterally to the inferomedial
border of the patella using suture augmentation.
The sutures are then secured and the capsular
layers of the MPML are closed. These authors
also described an arthroscopic technique. The
procedure begins with a diagnostic arthroscopy
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
followed by a debridement of <1 cm of fatty
tissue in the gutter adjacent to the inferomedial
patella. A PDS suture is then passed from the
inferomedial periosteal border of the patella into
the arthroscopic visual field. A second suture is
passed through the MPML, approximately
1.5 cm distal and medial to the initial needle.
After the suture is passed with the use of this
initial needle placement a second set of needles
was inserted in parallel to the initial set,
approximately 10–15 mm more proximally, near
the proximal margin of the MPML. A 10 mm
incision is then made between the entrance and
exit sites of the respective sutures. An extracapsular tract is created using a hemostat, deep to the
subcutaneous tissue through each incision,
extending to the site at which each suture exited
the capsule. The hemostat is then used to pull
them through the tract to exit the incision. The
sutures are then tied down. In both the open and
arthroscopic technique the authors note that by
advancing the MPML 1 cm, they are able to
prevent pathologic displacement of the central
patellar ridge over the lateral trochlea without
excessive restriction of the patella [23].
There is one known case report that describes
isolated MPTL and MPML avulsion fractures
without evidence of MPFL pathology. On exam,
they stated that the patella rested in a subluxed
position, but wouldn’t dislocate when the knee
was in full extension but dislocated easily when
the knee was flexed to 30°. They reported a
successful repair using nonabsorbable transosseous sutures through the MPTL/MPML to
the insertion on the patella to the medial/inferior
patellar border [40].
5.6 Post-operative Protocol
Depending on concomitant pathology and/or
additional surgeries, patients can be weightbearing as tolerated in a knee brace locked in extension
immediately after surgery. Passively, patients can
focus on early range of motion as tolerated, and
they can also work on isometric quadriceps exercises [22, 39]. After 1–2 weeks patients can begin
455
kinetic closed chain strengthening programs. By
4–6 weeks post-operatively, patients are typically
allowed to start progressive strengthening of
muscles with ultimate return to full activity by
approximately 12 weeks post-op [33].
6
Outcomes
6.1 MPTL Repair/Reconstruction
Without MPFL
Hughston et al. reported on MPTL repair or
reconstruction at mean 54-month follow-up and
showed that 68% reported improvement in their
functional levels and 75% reported subjective
improvements. Eighty percent stated they had a
good/excellent outcome and only 6/65 knees
required a secondary surgery by the latest available follow-up [41]. Using a combination of open
and arthroscopic techniques Zaffagini et al.
reported encouraging clinical and radiographic
results at 6.1 years following MPTL reconstructions. Eighty-three percent of knees were normal
or nearly normal by IKDC scoring, and only 1
knee (3%) was found to have patellar osteoarthritis. They also reported that only 14% of patients
suffered surgical failure, 7% had further dislocation and 7% required a revision surgery [33].
One study reported on outcomes following
semitendinosus tenodesis in a pediatric population and found that at an average of 3.17 year
follow-up, 88% of patients were asymptomatic,
5% developed recurrent subluxations and 5% had
recurrent dislocations, while 14% complained of
recurrent patellofemoral syndrome [31]. Similarly, in a study from 1972 that included 53
patients with mean 5 year follow-up, Baker et al.
reported 3.8% of patients had re-dislocation and
9.4% underwent reoperation following MPTL
reconstruction using a semitendinosus tenodesis.
They also reported that 80.1% of patients reported
good or excellent outcomes [30]. Conversely to
these successful reports, Grannatt et al. reported a
less optimistic longer-term follow-up study on 34
pediatric patients that underwent semitendinosus
tenodesis. They reported 35% reoperation
456
secondary to instability, with 82% reporting
recurrent subluxations or dislocations and 41%
with an IKDC score of less than 70 [32].
Several other studies have reported successful
outcomes with MPTL reconstruction using a
patellar tendon transfer with lateral retinaculum
release and vastus medialis advancement [34, 35,
47]. Myers et al. reported on 42 knees with
minimum 2 year follow-up and reported that
76% had good or excellent results with 12%
reporting poor results; two had recurrent dislocations [34]. Oliva et al. included 25 patients and
8 year follow-up with only 1 patient suffering a
re-dislocation which occurred following a motor
vehicle accident [35].
6.2 MPTL with MPFL Reconstruction
Ebied and Kholy was the first known study that
reported outcomes following combined MPFL
and MPTL reconstruction in 25 knees. They
reported significant improvement in IKDC scores
with no reports of subsequent dislocation events
[20]. Additionally, Drez et al. published and
early report of 15 patients with minimum 2-year
follow-up after combined MPFL/MPTL reconstructions using either semitendinosis, gracilis or
IT band autografts. They reported 93% had good
or excellent outcomes, no rates of re-dislocation
and high patient reported outcome scores [42].
Hetsroni et al. reported on outcomes of combined MPFL and MPTL reconstructions in 23
knees with a minimum of 2-year follow-up. They
demonstrated significant improvements in Kujala
score (86.4 vs 54.9), however activity scores
were not consistently restored compared to preinjury levels [48]. Similarly, Sobhy et al. reported on 33 patients that underwent combined
MPFL and MPTL reconstruction with semitendinosus autograft and reported improved pain
scores (VAS 6.3 vs 1.8) and patient reported
outcomes (Kujala score, 37 vs 91; Lysholm
score, 52 vs 90) [45]. Recently, Hinckel et al.
reported on 7 patients that underwent a combined
MPTL and MPFL reconstruction and reported
high rates of satisfaction with 100% of patients
R. S. Dean et al.
stating they would undergo the procedure again
at a mean of 5.5 months post-operatively [46].
6.3 MPTL with Concomitant
Realignment Procedures
Several studies reported on MPTL reconstruction
with Roux-Goldthwait procedures [36, 49, 50].
Most recently, Niedzielski et al. included 11
patients at 8-year follow-up and had only 1 dislocation, with 10 having normal patellar tracking. Of
note, this study reported a decrease in the maximum quadriceps muscle torque between 60 and
180° compared to the healthy contralateral limb
[49]. Additionally. Joo et al. reported no redislocations and all patients with a Kujala score
greater than 88 at 4.5-year follow-up [36]. Marcacci et al. performed a tibial tuberosity osteotomy
in addition to MPTL reconstruction with a patellar
tendon autograft. In their 18-person study with
5 year follow-up, they reported no re-disclocations
with 83.3% of patients having IKDC A or B
scores, and a mean Kujala score of 88.9% [51].
6.4 Systematic Reviews
Finally, Baumann et al. performed a systematic
review of previous outcome studies describing
MPTL reconstruction which included 403 knees
from 19 studies. Their review included primarily
studies that utilized hamstrings tenodesis (n = 9),
medial transfers of the patellar tendon (n = 5),
and combined MPFL and MPTL reconstructions
using either hamstring autograft or allograft
(n = 5). They showed that despite a variable
degree of study qualities, most studies reported
favorable patient reported outcomes with low
rates of dislocation [52].
7
Conclusions
The distal medial patellar ligamentous complex
(MPTL and MPML) are integral stabilizers of the
patella. Additionally, they have a consistent
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
anatomical and biomechanical profile in preclinical studies. While typically performed in
conjunction with MPFL reconstruction, there are
several described surgical procedures designed to
repair or reconstruct these structures which have
demonstrated reproducible and encouraging
outcomes. Understanding the anatomy and surgical options for managing distal medial patellar
ligamentous complex injuries can offer a
promising option for managing the complexities
of lateral patellar instability in the at risk patient
population.
8
Key Message
While the long-term outcomes are scarcely
described in the literature, the available data
suggests that the addition of a medial patellotibial
ligament reconstruction to a medial patellofemoral ligament reconstruction is effective at
preventing subsequent dislocations or instability
events in select high risk situations, while also
providing pain and functional relief to a young
and active patient population.
References
1. Sanders TL, Pareek A, Hewett TE, Stuart MJ,
Dahm DL, Krych AJ. Incidence of first-time lateral
patellar dislocation: a 21-year population-based
study. Sports Health. 2018;10(2):146–51.
2. Stefancin JJ, Parker RD. First-time traumatic patellar
dislocation: a systematic review. Clin Orthop Relat
Res. 2007;455:93–101.
3. Huntington LS, Webster KE, Devitt BM, Scanlon JP,
Feller JA. Factors associated with an increased risk of
recurrence after a first-time patellar dislocation: a
systematic review and meta-analysis. Am J Sports
Med. 2020;48(10):2552–62.
4. Askenberger M, Arendt EA, Ekström W, Voss U,
Finnbogason T, Janarv PM. Medial patellofemoral
ligament injuries in children with first-time lateral
patellar dislocations: a magnetic resonance imaging
and arthroscopic study. Am J Sports Med. 2016;44
(1):152–8.
5. Arendt EA, England K, Agel J, Tompkins MA. An
analysis of knee anatomic imaging factors associated
with primary lateral patellar dislocations. Knee Surg
Sports Traumatol Arthrosc. 2017;25(10):3099–107.
457
6. Parikh SN, Lykissas MG, Gkiatas I. Predicting risk
of recurrent patellar dislocation. Curr Rev Musculoskelet Med. 2018;11(2):253–60.
7. Hinckel BB, Gobbi RG, Kaleka CC, Camanho GL,
Arendt EA. Medial patellotibial ligament and medial
patellomeniscal ligament: anatomy, imaging, biomechanics, and clinical review. Knee Surg Sports
Traumatol Arthrosc. 2018;26(3):685–96.
8. Salonen EE, Magga T, Sillanpää PJ, Kiekara T,
Mäenpää H, Mattila VM. Traumatic patellar dislocation and cartilage injury: a follow-up study of longterm cartilage deterioration. Am J Sports Med.
2017;45(6):1376–82.
9. Stupay KL, Swart E, Shubin Stein BE. Widespread
implementation of medial patellofemoral ligament
reconstruction for recurrent patellar instability maintains functional outcomes at midterm to long-term
follow-up while decreasing complication rates: a
systematic review. Arthroscopy. 2015;31(7):1372–80.
10. Tanaka MJ, Chahla J, Farr J 2nd, LaPrade RF,
Arendt EA, Sanchis-Alfonso V, et al. Correction to:
recognition of evolving medial patellofemoral anatomy provides insight for reconstruction. Knee Surg
Sports Traumatol Arthrosc. 2019;27(8):2551.
11. Slocum DB, Larson RL, James SL. Late reconstruction of ligamentous injuries of the medial compartment of the knee. Clin Orthop Relat Res.
1974;100:23–55.
12. Gali JC, Junior CA, Nogueira F, Yuri, Nakamichi,
Santos NBd, et al., editors. Medial patellotibial
ligament anatomy and histology. 2017.
13. Hinckel BB, Gobbi RG, Demange MK,
Pereira CAM, Pécora JR, Natalino RJM, et al.
Medial patellofemoral ligament, medial patellotibial
ligament, and medial patellomeniscal ligament:
anatomic, histologic, radiographic, and biomechanical study. Arthroscopy. 2017;33(10):1862–73.
14. LaPrade MD, Kallenbach SL, Aman ZS, Moatshe G,
Storaci HW, Turnbull TL, et al. Biomechanical
evaluation of the medial stabilizers of the patella.
Am J Sports Med. 2018;46(7):1575–82.
15. Panagiotopoulos E, Strzelczyk P, Herrmann M,
Scuderi G. Cadaveric study on static medial patellar
stabilizers: the dynamizing role of the vastus medialis
obliquus on medial patellofemoral ligament. Knee
Surg Sports Traumatol Arthrosc. 2006;14(1):7–12.
16. Hautamaa PV, Fithian DC, Kaufman KR,
Daniel DM, Pohlmeyer AM. Medial soft tissue
restraints in lateral patellar instability and repair.
Clin Orthop Relat Res. 1998;349:174–82.
17. Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human
knee. Am J Sports Med. 1998;26(1):59–65.
18. Conlan T, Garth WP, Lemons JE. Evaluation of the
medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am. 1993;75
(5):682–93.
19. Hinckel BB, Gobbi RG, Demange MK, Bonadio MB,
Pécora JR, Camanho GL. Combined reconstruction
458
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
R. S. Dean et al.
of the medial patellofemoral ligament with quadricipital tendon and the medial patellotibial ligament with
patellar tendon. Arthrosc Tech. 2016;5(1):e79-84.
Ebied AM, El-Kholy W. Reconstruction of the
medial patello-femoral and patello-tibial ligaments
for treatment of patellar instability. Knee Surg Sports
Traumatol Arthrosc. 2012;20(5):926–32.
Philippot R, Boyer B, Testa R, Farizon F, Moyen B.
The role of the medial ligamentous structures on
patellar tracking during knee flexion. Knee Surg
Sports Traumatol Arthrosc Offic J ESSKA. 2012;20
(2):331–6.
Grantham WJ, Aman ZS, Brady AW, Rosenberg SI,
Lee Turnbull T, Storaci HW, et al. Medial patellotibial ligament reconstruction improves patella
tracking when combined with medial patellofemoral
reconstruction: an in vitro kinematic study. Arthroscopy. 2020;36(9):2501–9.
Garth WP Jr, Connor GS, Futch L, Belarmino H.
Patellar subluxation at terminal knee extension:
isolated deficiency of the medial patellomeniscal
ligament. J Bone Joint Surg Am. 2011;93(10):954–
62.
Hinckel BB, Lipinski L, Arendt EA. Concepts of the
distal medial patellar restraints: medial patellotibial
ligament and medial patellomeniscal ligament. Sports
Med Arthrosc Rev. 2019;27(4):143–9.
McWalter EJ, Cibere J, MacIntyre NJ, Nicolaou S,
Schulzer M, Wilson DR. Relationship between
varus-valgus alignment and patellar kinematics in
individuals with knee osteoarthritis. J Bone Joint
Surg Am. 2007;89(12):2723–31.
Balcarek P, Walde TA, Frosch S, Schüttrumpf JP,
Wachowski MM, Stürmer KM. MRI but not
arthroscopy accurately diagnoses femoral MPFL
injury in first-time patellar dislocations. Knee Surg
Sports Traumatol Arthrosc Offic J ESSKA. 2012;20
(8):1575–80.
Dirim B, Haghighi P, Trudell D, Portes G, Resnick D.
Medial patellofemoral ligament: cadaveric investigation of anatomy with MRI, MR arthrography, and
histologic correlation. Am J Roentgenol. 2008;191
(2):490–8.
Thawait SK, Soldatos T, Thawait GK, Cosgarea AJ,
Carrino JA, Chhabra A. High resolution magnetic
resonance imaging of the patellar retinaculum: normal anatomy, common injury patterns, and pathologies. Skeletal Radiol. 2012;41(2):137–48.
Tompkins MA, Rohr SR, Agel J, Arendt EA.
Anatomic patellar instability risk factors in primary
lateral patellar dislocations do not predict injury
patterns: an MRI-based study. Knee Surg Sports
Traumatol Arthrosc. 2018;26(3):677–84.
Baker RH, Carroll N, Dewar FP, Hall JE. The
semitendinosus tenodesis for recurrent dislocation of
the patella. J Bone Joint Surg Br. 1972;54(1):103–9.
Letts RM, Davidson D, Beaule P. Semitendinosus
tenodesis for repair of recurrent dislocation of the
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
patella in children. J Pediatr Orthop. 1999;19(6):742–
7.
Grannatt K, Heyworth BE, Ogunwole O, Micheli LJ,
Kocher MS. Galeazzi semitendinosus tenodesis for
patellofemoral instability in skeletally immature
patients. J Pediatr Orthop. 2012;32(6):621–5.
Zaffagnini S, Grassi A, Marcheggiani Muccioli GM,
Luetzow WF, Vaccari V, Benzi A, et al. Medial
patellotibial ligament (MPTL) reconstruction for
patellar instability. Knee Surg Sports Traumatol
Arthrosc. 2014;22(10):2491–8.
Myers P, Williams A, Dodds R, Bülow J. The threein-one proximal and distal soft tissue patellar
realignment procedure. Am J Sports Med. 1999;27
(5):575–9.
Oliva F, Ronga M, Longo UG, Testa V, Capasso G,
Maffulli N. The 3-in-1 procedure for recurrent
dislocation of the patella in skeletally immature
children and adolescents. Am J Sports Med. 2009;37
(9):1814–20.
Joo SY, Park KB, Kim BR, Park HW, Kim HW. The
“four-in-one” procedure for habitual dislocation of
the patella in children: early results in patients with
severe generalised ligamentous laxity and aplasis of
the trochlear groove. J Bone Joint Surg Br. 2007;89
(12):1645–9.
Maffulli N, Aicale R, D’Addona A, Young DA,
Kader DF, Oliva F. Combined medial patellofemoral
and patellotibial reconstruction with soft tissue
fixation in recurrent patellar dislocation. Injury.
2020;51(8):1867–73.
Kumar A, Haider Y, Jameel J, Qureshi OA. Combined medial patellofemoral and patellotibial reconstruction with soft tissue fixation in recurrent patellar
dislocation: some concerns. Injury. 2020;51
(10):2339.
Abdelrahman T, Moatshe G, Arendt E, Feller J,
Getgood A. Combined medial patellofemoral ligament and medial patellotibial ligament reconstruction
for recurrent lateral patellar dislocation in flexion.
Arthrosc Tech. 2021;10(2):e385-95.
Samelis PV, Papagrigorakis E, Mavrogenis A, Savvidou O, Koulouvaris P. Isolated avulsion fracture of
patellar attachment of medial patellotibial and medial
patellomeniscal ligaments in the presence of trochlear
dysplasia: an indication for acute surgical repair.
Cureus. 2019;11(11): e6205.
Hughston JC, Flandry F, Brinker MR, Terry GC,
Mills JC. Surgical Correction of Medial Subluxation
of the Patella. Am J Sports Med. 1996;24(4):486–91.
Drez D Jr, Edwards TB, Williams CS. Results of
medial patellofemoral ligament reconstruction in the
treatment of patellar dislocation. Arthrosc J Arthrosc
Relat Surg. 2001;17(3):298–306.
Brown GD, Ahmad CS. Combined medial patellofemoral ligament and medial patellotibial ligament
reconstruction in skeletally immature patients. J Knee
Surg. 2008;21(4):328–32.
Combined Medial Patellofemoral Ligament and Medial Patellotibial …
44. Giordano M, Falciglia F, Aulisa AG, Guzzanti V.
Patellar dislocation in skeletally immature patients:
semitendinosous and gracilis augmentation for combined medial patellofemoral and medial patellotibial
ligament reconstruction. Knee Surg Sports Traumatol
Arthrosc. 2012;20(8):1594–8.
45. Sobhy MH, Mahran MA, Kamel EM. Midterm results
of combined patellofemoral and patellotibial ligaments reconstruction in recurrent patellar dislocation.
Eur J Orthop Surg Traumatol. 2013;23(4):465–70.
46. Hinckel BB, Gobbi RG, Bonadio MB, Demange MK,
Pécora JR, Camanho GL. Reconstruction of medial
patellofemoral ligament using quadriceps tendon
combined with reconstruction of medial patellotibial
ligament using patellar tendon: initial experience. Rev
Bras Ortop. 2016;51(1):75–82.
47. Rillmann P, Dutly A, Kieser C, Berbig R. Modified
Elmslie-Trillat procedure for instability of the patella.
Knee Surg Sports Traumatol Arthrosc. 1998;6
(1):31–5.
48. Hetsroni I, Mann G, Dolev E, Nyska M. Combined
reconstruction of the medial patellofemoral and
49.
50.
51.
52.
459
medial patellotibial ligaments: outcomes and prognostic factors. Knee Surg Sports Traumatol Arthrosc.
2019;27(2):507–15.
Niedzielski KR, Malecki K, Flont P, Fabis J. The
results of an extensive soft-tissue procedure in the
treatment of obligatory patellar dislocation in children with ligamentous laxity: a post-operative isokinetic study. Bone Joint J. 2015;97-b(1):129–33.
HALL JE, MICHELI LJ, MCMANAMA GBJ. Semitendinosus tenodesis for recurrent subluxation or
dislocation of the patella. Clin Orthopaed Relat Res.
1979(144):31–5.
Marcacci M, Zaffagnini S, Lo Presti M, Vascellari A,
Iacono F, Russo A (2004) Treatment of chronic
patellar dislocation with a modified Elmslie-Trillat
procedure. Arch Orthop Trauma Surg 124(4):250–
257. https://doi.org/10.1007/s00402-003-0511-2.
Baumann CA, Pratte EL, Sherman SL, Arendt EA,
Hinckel BB. Reconstruction of the medial patellotibial ligament results in favorable clinical outcomes: a
systematic review. Knee Surg Sports Traumatol
Arthrosc Offic J ESSKA. 2018;26(10):2920–33.
Warning: Lateral Retinacular Release
Can Cause Medial Patellar
Dislocation—Lateral Patellofemoral
Ligament Reconstruction
Robert A. Teitge
1
Historic Evolution of Diagnosis
and Treatment
It should be obvious that a joint will not dislocate
without being acted upon by a dislocating force.
An unstable and dislocatable joint when at rest
often resides in a position of normal alignment
and radiographs often show no subluxation and
almost never dislocation. For me, it was perhaps
hearing Losee et al. [1] describe the pivot shift
and Slocum and Larson [2] describe Rotatory
Instability of the Knee which made me appreciate
such maneuvers provide the force required to
displace the tibia from femur. Unfortunately,
neither of these tests can be quantified.
Beginning in 1980, I began seeing many
referred patients with failed patellofemoral surgery. Examining medial and lateral displacement
of the patella, later referred to as glide, was part
of the examination, but it was obvious the neutral
starting position could not be determined. It was
the rule in the 1970’s at Los Angeles County
General Hospital that no patient could have surgery for an unstable joint unless radiographs
provided proof of dislocation. Stress radiographs
when compared with the contralateral stable joint
provided an opportunity to objectively measure
R. A. Teitge (&)
Wayne State University, Detroit, Michigan, USA
e-mail: rteitge@med.wayne.edu
the amount of instability. Likewise, any
improvement resulting from surgery could also
be quantified with stress radiographs. Stress
radiography was the obvious solution to the
problem of determining if an excess patellar
displacement was medial or lateral. Many of
these “failed” patients had had a lateral retinacular release as part of their surgery. Many were
severely disabled much worse than before surgery. In many the PFJ was so sensitive with
patients so apprehensive that meaningful examination was not possible. Routine PF radiographs
were most often not revealing.
2
Stress Radiographs
Stress radiographs proved to be the key to
diagnosis. Trial and error led to a reliable technique. Using positioning for the standard Merchant axial view and an adjustable frame at the
end of the x-ray table, radiographs were repeated
with stress applied in both the medial and lateral
direction of both knees. (Fig. 1). Since the height
of the patella and patellar flexion is different in
different patients, the angle of the x-ray beam to
the table often needs adjustment so the beam is
perpendicular to the tangent point of PF contact
on the trochlea. Following the recommendation
of Laurin et al. [3] we attempted to minimize
knee flexion but were generally unable to obtain
axial radiographs at less than 30° flexion. Initially I used my fingers gripping both sides of the
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_30
461
462
R. A. Teitge
A
Fig. 1 Stress Radiographs A In clinic, the knee is
extended to the maximum and still be able to obtain an
axial view. The knee is supported on one side to prevent
rotation while stress is applied to the opposite side of the
patella B Patient positioning in the operating theater for
stress radiographs C Medial stress being applied
patella to apply the displacement force, before
moving to a padded curved wooden block and
later to a device produced for me by the Medmetric Corporation in San Diego. This Patella
Pusher (Fig. 2) had a gauge to measure force so
an equal force would be applied with each test. It
was obvious that an absolute displacement value
could not be used for all patients because of
differences in generalized soft tissue laxity, trochlear geometry, and patellar height. Therefore,
comparison with the asymptomatic side needed
to be the reference. For those with bilateral
symptomatic knees, the comparison meant little,
but we felt confident the finding of complete
dislocation represented instability.
The presence of complete dislocation on the
symptomatic side contrasted with minimal medial translation on the asymptomatic side was
dramatic evidence of medial instability. (Fig. 3).
It became clear that many patients worse after
lateral release (LR) had patellae which would
dislocate outside the trochlea with medial stress
(Figs. 3 and 4). We then realized we had two
groups of patients with medial dislocation. There
were patients who had a lateral release for pain
but not instability and those who had LR for
instability. Those with LR for pain with medial
dislocation on stress often had lateral displacements slightly greater than normal but would not
dislocate laterally. Those with LR for lateral
Warning: Lateral Retinacular Release …
463
Fig. 2 Patella pusher
instability would often dislocate in both the
medial and lateral direction. These were referred
to as multi-directional instability. It was also
clear that patients with medial dislocation often
were more anxious, depressed, afraid of being
examined, and afraid of pain far in excess of the
presentation of lateral instability patients.
In 1987 I presented a scientific exhibit at the
annual AAOS meeting. Jack Hughston was quite
excited and spent considerable time studying the
cases. In 1991 I presented at AAOS a case series
of 68 patients all worse after LRR, all with
increased medial excursion, all with medial
excursion apprehension and all with a stress
radiographs demonstrating a patella dislocated
medially. The moderator requested I remove this
paper from the program because he did not
believe that radiographs showing medial patellar
dislocation represented true pathology but rather
represented an adequate and appropriate release
and that stress radiographs were not a valid
testing method.
464
R. A. Teitge
A
Fig. 3 Radiographs of a 40-year-old women who had a
lateral release 1 year after a dashboard injury of the left
knee sustained in a minor automobile accident. (A) static
axial patellar view post-lateral release shows no pathology. B and C are medial stress radiographs taken 1 year
after lateral release. (B) A complete medial patellar
dislocation is obvious. Medial displacement on the left
patella measures 40 mm from the Laurin reference line.
(C) Medial displacement of the normal right patella
measures 16 mm. The increase in medial displacement is
24 mm. D and E are lateral stress radiographs. (D) Lateral
stress of the operated knee shows lateral patellar displacement of 15 mm and medial tilt of 44°. (E) Lateral
stress of the normal patella shows lateral displacement of
10 mm and medial tilt of 26°. In this patient lateral release
produced a pathologic increase in lateral displacement of
5 mm. and increased medial tilt of 18°
In 1996 we reported [4] that stress radiographs
were the only radiographic choice for the diagnosis of medial patellar instability (Figs. 3 and
4). No other measure of axial radiographs gave a
hint of medial subluxation or dislocation. It was
also the strongest test to diagnose lateral instability. In the control group the mean difference in
lateral and medial displacement (glide) between
the right and left normal knees was 1.3 and
1.2 mm respectively. In the lateral instability
group the mean difference in lateral and medial
displacement between the asymptomatic side and
the symptomatic side was 7.5 and 0.2 mm. In the
medial instability group the difference in lateral
displacement between the symptomatic (L.R.)
and asymptomatic side was 0.5 mm while the
mean difference in medial displacement between
the symptomatic (L.R.) and asymptomatic knees
was 10.3 mm. In the multi-instability group the
difference in lateral and medial displacement
Warning: Lateral Retinacular Release …
Fig. 4 24 year old athlete post lateral release and lateral
facet chondroplasty for anterior knee pain. Pain was
unresolved and she underwent a second chondroplasty
and lateral release. A CT arthrogram shows complete
removal of lateral facet articular cartilage with intact
between the asymptomatic and symptomatic side
was 9.5 and 10.6 mm respectively. We calculated that the threshold for instability was 4
mm more excursion in the potential instability
side compared with the asymptomatic side. The
mean increase in medial displacement on the
symptomatic side in patients with medial dislocation was 10.3 mm.
The incidence of medial subluxation/dislocation
is unknown because no studies measuring medial
displacement increase after lateral release have
been reported. Pagenstert et al. [5] made a most
important observation that 36% of patients in a
prospective randomized study of lateral release vs
lateral retinacular lengthening demonstrated signs
and symptoms of medial instability compared with
none in the lateral lengthening group. I suspect,
without evidence, medial stress radiographs would
show an even higher incidence.
465
medial cartilage. B the patella was unstable enough to stay
in the dislocated position for CT which shows complete
medial dislocation and contact of the lateral facet with the
medial trochlear edge
3
Lateral Patellofemoral Ligament
Reconstruction
Initially medial dislocation was treated with
repair of the lateral retinacular defect. The defect
often contained a very thin lax areolar tissue but
careful dissection anterior and posterior to the
defect often could identify stout tissue felt to
represent the released retinacular edges. Direct
repair was attempted. Over time, 6 months-3
years symptoms and increased laxity with
increased medial displacement on stress radiographs began to appear frequently, perhaps in ½
of the cases, so I discontinued this secondary
repair and realized ligament reconstruction was
necessary. I am aware that there are many reports
of successful secondary repair today, but my
experience is that Lateral PatelloFemoral
466
Ligament Reconstruction (LPFLR) is unpredictable and often unreliable, even though the
repairs at surgery look strong.
The principles of ligament reconstruction are
well known. Ligaments attach to bones with a
unique and complex geometry which prevents
excess displacement. Ligament reconstruction
requires selection of an adequate graft, proper
location of the graft, proper tension, adequate
fixation and avoidance of local mechanical
damage. There is much literature on each of these
requirements. Adequate graft material requires a
strength to withstand displacement forces, but
also the laxity required to prevent overconstraint. Tendons used for grafting do not
have the same materials property as ligaments
but are stiffer. They do not have the same geometrical fiber arrangement. Thus, ligament
reconstructions run a risk of over-constraint of
patellar motion in some joint positions and
excess laxity in others. The location of the graft
on both the femur and patella should be such that
changes in distance between these two attachment points does not change with knee flexion
−extension. This so-called isometric location is a
weak compensation for our lack of reproducing
ligament geometry and normal ligament laxity.
Isometers measure distances between points.
Measurement of the change in length with knee
motion allows estimating tension changes
between points on the patella and femur. With
the isometer placed into a 2.5 mm hole in the
medial patella a k-wire with an attached string
may be “walked” around potential attachment
sites for graft attachment to the lateral femur.
I have used since the mid 1980’s a “tension
isometer” developed by Synthes. By using a
constant pneumatic pressure, the piston applies a
constant tension to the test string and length
change can be read within 0.5 mm. Charles
Henning, M.D. compared accuracy of this with
various commercial isometers and concluded the
pneumatic gave consistent almost perfect measurements as opposed to spring isometers. The
graft will occupy an area larger than the isometric
point and will typically migrate away from the
isometric point to one side of a tunnel opening,
so the graft tunnels need to be shifted behind the
R. A. Teitge
isometric points. Secure fixation of the graft
which is not lost over time is essential. Mountney
et al. [6] compared fixation of an MPFL graft
fixation with suture repair of the ruptured ligament, and with the failure load of the intact
ligament. Three fixation methods for a tendon
graft included suturing the graft to the bone
edges with suture anchors, interference screws
anchoring grafts at the tunnel entrances, interference screws anchoring the graft on the lateral
edge of tunnels after crossing the femur and
patella. Normal MPFL ruptured at 208 N, ligament suture repair failed at 37 N as the suture cut
through the ligament tissue, suture anchor fixation failed at 142 N usually by the anchors
pulling out of the bone, interference screw
(8 mm dia.) fixation at the entrance to tunnels
failed at 126 N with the grafts pulling past the
femoral screws, and passing the graft through the
patella and femur and fixing on the lateral side
with interference screws failed at 195 N with the
grafts pulling past the screws. This study should
be applicable to LPFL fixation.
In 1982 I did the first LPFL reconstruction for
a failed repair of a lateral retinacular release.
I have followed this patient for 30 years. The
patella has remained stable. The first series of
reconstructions used a 1 cm square patellar bone
block from the proximal edge of the patella and
partial thickness quadriceps tendon graft (Figs. 5
and 6). The square bone block was countersunk
into the lateral femoral condyle at the isometric
point. Thin bone chisels cut a square recess into
the femoral condyle and the patellar bone block
was held in place with a lag screw. This allowed
the quadriceps tendon to run straight from its
bone block without bending over sharp corners.
A transverse hole was placed across the upper
1/3 of the patella. Obviously and unfortunately
removing a bone block from the upper 1 cm of
the patella and placing a transverse tunnel at the
same level created a stress riser and a few patellar
fractures were not surprising. Additionally, a
1 cm wide quadriceps tendon graft was far larger
than was probably necessary for a LPFL graft.
Roger Torga-Spak’s [7] description of the technique reported that 60 of these operations had
been performed before his 2004 publication.
Warning: Lateral Retinacular Release …
467
Fig. 5 Lateral patellofemoral ligament reconstruction.
The technique is not important as long as the objectives
outlined are met. Patellar bone quadriceps graft. The bone
block was countersunk into the lateral femoral condyle at
the isometric point, the quadriceps graft was passed
through a transverse tunnel in the patella. Drawing of the
isometer in the medial patella and the k-wire on the lateral
epicondylar region. Drawing of the quadriceps graft
attached to the lateral femur and then passed through the
patellar tunnel and back onto the anterior surface of the
patella
Fig. 6 Left knee approach for lateral PF ligament
reconstruction. To locate the isometric site on the lateral
femoral epicondyle, the tip of a pneumatic driven piston
isometer is inserted into a 2.5 mm drill hole in the medial
patella; a #2 suture runs from the piston, through the
transpatellar hole to a k-wire which is walked around the
epicondyle until an isometric position or a position which
allows the string to become 1-3 mm looser with flexion is
located. The graft will be positioned immediately posterior to this isometric location
Gradually I have shifted to hamstring allografts, largely because of the risk of patellar
fracture and the complexity of countersinking a
bone block with lag screw fixation. I have not
studied the tension behavior of a double bundle
graft. Obviously tension would be different in the
two limbs I have not used ITB graft because of
the observation reported in 1980 [8] that 53% of
patients in which a portion of the ITB was used
for a lateral extra-articular reconstruction of ACL
468
instability demonstrated medial tilting of the
patella on post-op axial radiographs.
Lateral PF Ligament Reconstruction is a salvage procedure to improve the complication of
medial instability. It cannot be considered a cure
for whatever reason the lateral release was supposed to improve. Since the lateral retinaculum
does provide a resistance to lateral patellar displacement it was observed early that patients with
lateral instability often noted improvement in their
lateral instability with LPFL reconstruction.
Results have held up and I am unaware of any
recurrence of medial dislocation. Lag screws used
for fixation often had to be removed because of
the irritation to the overlying ITB. The clinical
outcome cannot be assessed beyond the patients
report of improvement because of the multiple
variables of their underlying disease. Residual
symptoms may arise from the original undiagnosed cause of pain or from an imbalance between
medial and lateral retinacular tightness. It is generally impossible to diagnose this imbalance. As
Pagenstert [5] reported the group difference
between < 1 quadrant, 1−2 quadrants and 3
quadrants of medial glide was Kujala scores of
57.7, 90.3 and 75.3 (significantly different). This
reflects the potential extreme sensitivity of retinacular imbalance. It must also be acknowledged
the agreement between 5 examiners in the PatelloFemoral Study Group was only 11% for
assessment of patellar glide and 8% for assessment of patellar tilt (kappa = 0.11 and 0.08) [9].
Clearly, assessment of retinacular tension balance
R. A. Teitge
is poor and the decision to improve balance with
lateral release is likely a poor choice. Case
examples shown in Figs. 3 and 4.
References
1. Losee RE, Johnson TR, Southwick WO. Anterior
subluxation of the lateral tibial plateau. A diagnostic
test and operative repair. J Bone Joint Surg Am.
1978;60(8):1015−30.
2. Slocum DB, Larson RL. Pes anserinus transplantation.
A surgical procedure for control of rotatory instability of
the knee. J Bone Joint Surg Am. 1968;50(2): 226−42.
3. Laurin CA, et al. The abnormal lateral patellofemoral
angle: a diagnostic roentgenographic sign of recurrent
patellar subluxation. J Bone Joint Surg Am. 1978;60
(1):55–60.
4. Teitge RA, et al. Stress radiographs of the patellofemoral joint. J Bone Joint Surg Am. 1996;78(2):193–
203.
5. Pagenstert G, et al. Open lateral patellar retinacular
lengthening versus open retinacular release in lateral
patellar hypercompression syndrome: a prospective
double-blinded comparative study on complications
and outcome. Arthroscopy. 2012;28(6):788–97.
6. Mountney J, et al. Tensile strength of the medial
patellofemoral ligament before and after repair or
reconstruction. J Bone Joint Surg Br. 2005;87(1):36–40.
7. Teitge RA, Torga Spak R. Lateral patellofemoral
ligament reconstruction. Arthroscopy. 2004;20(9): 998
−1002.
8. Teitge RA, et al. Iliotibial band transfer for anterolateral rotatory instability of the knee. Summary of 54
cases. Am J Sports Med. 1980; 8(4): 223−7.
9. Smith TO, et al. The intra- and inter-observer reliability of the physical examination methods used to
assess patients with patellofemoral joint instability.
Knee. 2012;19(4):404–10.
Reconstruction of the Lateral
Patellofemoral Ligament
David S. Zhu and Lutul D. Farrow
1
Introduction
Reconstruction of the lateral patellofemoral
ligament (LPFL) is primarily utilized for the
treatment of medial subluxation and dislocation
of the patella. Medial patellar instability is very
rare and is classically considered to be iatrogenic,
typically occurring following extensive lateral
release when performed in the setting of patellofemoral instability and/or patellofemoral pain.
Recently, primary medial instability has been
recognized as a clinical entity that may warrant
LPFL reconstruction. The lateral patellofemoral
ligament is an important anatomic structure and
has secondary role in stability of the patellofemoral joint, resisting lateral displacement of the
patella. A tight LPFL has also been implicated as
a contributor to increased patellofemoral contact
pressures in the setting of patellofemoral pain
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_31.
D. S. Zhu L. D. Farrow (&)
Cleveland Clinic Orthopaedic and Rheumatologic
Institute, Cleveland, OH, USA
e-mail: farrowl@ccf.org
L. D. Farrow
Cleveland Clinic Lerner College of Medicine,
Cleveland Clinic Sports Health Center, 5555
Transportation Blvd, Garfield Heights, Ohio, USA
and chondrosis [1, 2]. Over the past few decades
several studies have helped to describe the
function of the lateral patellofemoral ligament
[3–5]. In a biomechanical study, Desio et al.
demonstrated that the lateral retinaculum contributes ten percent of the total restraining force
opposing lateral displacement of the patella [4].
Another biomechanics study demonstrated that
while lateral release can decrease contact pressures on the lateral patellar facet of the patella, it
also results in increased lateral tracking of the
patella [5]. Finally, Bedi and Marzo showed that
adding a lateral release following medial patellofemoral (MPFL) repair actually decreases the
force necessary to laterally displace the patella
when compared to the MPFL repair without lateral retinacular release [3]. These biomechanical
studies helped to support the LPFL’s contribution
to stability of the patellofemoral joint.
Although it is now known that isolated lateral
retinacular release is contraindicated in the
treatment of patellar instability, the procedure has
long been utilized as a standalone procedure for
patellofemoral instability and also in conjunction
with other procedures for patellofemoral instability such as tibial tubercle osteotomy and
medial patellofemoral ligament reconstruction.
The first description of lateral retinacular release
in the English literature dates back to 1891 when
Pollard described this technique for treatment of
a patient with obligatory dislocation of the patella
[6]. In this report, lateral retinacular release was
utilized in conjunction with a medial retinacular
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_31
469
470
D. S. Zhu and L. D. Farrow
reefing and trochleoplasty to successfully treat
this condition [6]. Since this first report lateral
retinacular release has been utilized for the
treatment of patellar instability but became
increasingly popular following a preliminary
report on its use by Merchant and Mercer and
subsequent positive reports on its use [7, 8].
Lateral release was touted as an effective, simple
and less invasive procedure for the treatment of
lateral patellofemoral instability. Chen and
Ramanathan described a percutaneous approach
to lateral retinacular lengthening that was felt to
eliminate the need for larger open instability
surgeries in most patients [7]. In addition to its
use for the treatment of lateral patellar instability
lateral release has also been utilized for the
treatment of patellofemoral pain. In lateral
patellar hypercompression syndrome (LHPS)
patellofemoral pain was thought to be caused by
a tight lateral retinaculum leading to patellofemoral joint overload, chondral degeneration and
resultant pain [1, 2]. Being relatively quick and
less technically demanding this procedure has
been used by many for the treatment of patellofemoral instability and pain.
Following the widespread adoption and use of
this procedure in the 70’s and 80’s, Hughston
and Deese provided the first report of medial
patellar subluxation as a result of lateral retinacular release [9]. In their series, 50% of knees
referred to the senior author with complications
following lateral release were found to have
developed medial subluxation [9]. This study
demonstrated for the first time that overzealous
lateral retinacular release can result in symptomatic medial subluxation of the patella. Following this initial report, several other authors
have reported on complications following lateral
retinacular release [10–12].
2
Indications (Table 1)
The primary indication for lateral patellofemoral
ligament reconstruction is in cases of medial
patellofemoral ligament instability, both primary
and iatrogenic. Medial instability (subluxation
and dislocation) of the patella has long been
Table 1 Indications
1. Iatrogenic medial patellar instability following prior
lateral release
2. Primary medial patellar instability
3. Refractory lateral parapatellar pain following prior
lateral release
4. During revision patellofemoral stabilization following
prior lateral release
thought to be iatrogenic, only occurring following extensive release of the lateral patellofemoral
ligament. Recently, primary medial instability of
the patella has been described. Loeb et al.
reported on a series of 6 patients with primary
medial patellofemoral instability [13]. Of the 6
patients in this series only one patient required
LPFL reconstruction [13]. Although medial
patellar instability is uncommon, LPFL reconstruction can be important in management of
patients with medial subluxation/dislocation.
3
Contraindications (Table 2)
Lateral patellofemoral ligament reconstruction is
contraindicated in cases with a competent lateral
patellofemoral ligament and in cases without
medial instability. Although rare, LPFL reconstruction should be avoided in cases of prior IT
band surgery. Procedures utilizing IT band (i.e.,
physeal-sparing anterior cruciate ligament surgery in the skeletally immature patient) or
excising IT band (lateral friction syndrome)
might make it difficult or impossible to use the
iliotibial band for LPFL reconstruction. In
patients
with
end-stage
patellofemoral
Table 2 Contraindications
1. Intact and competent lateral patellofemoral
ligament/lateral retinaculum
2. Absence of medial patellar instability
3. Prior IT band surgery (i.e. lateral friction syndrome,
physeal-sparing ACLR, etc.)
4. End-stage patellofemoral osteoarthritis
5. Inflammatory arthropathy
6. Unmanaged complex regional pain syndrome
Reconstruction of the Lateral Patellofemoral Ligament
471
osteoarthritis or inflammatory arthropathy
arthroplasty options should be considered rather
than soft tissue stabilization techniques.
anchor placement and graft healing. The trough
should be placed at the mid-portion of the patella.
The incision for the iliotibial band harvest is
made along the lateral aspect of the thigh. This
incision is started at the lateral epicondyle and
taken proximally 7–8 cm. With mobilization of
the subcutaneous tissues a smaller incision can
be utilized. Sharp dissection is carried down to
expose the iliotibial band. The subcutaneous are
then lifted bluntly to allow for wide visualization
of the iliotibial band. Next, the subcutaneous
tissues at the level of the patella are tunneled
proximally in order to form a subcutaneous
tunnel between the anterior incision and the lateral incision for later passage of our graft. At this
point in time a 10 mm wide 80 mm long strip
of iliotibial band is created. (Fig. 1) The proximal strip is released sharply but the distal base is
maintained. The free end of the graft is whipstitched with a #2 non-absorbable braided suture.
A large, blunt forcep is then tunneled under the
soft tissues just lateral to the patella and passed to
the distal aspect of the opening in the iliotibial
band. The tag sutures are then used to pull the
strip of the iliotibial band anteriorly, bringing the
graft perpendicularly under the iliotibial band.
(Fig. 2) While suture fixation can be utilized to
attach the iliotibial band strip to the lateral patella,
we prefer suture anchor fixation. We utilize and
all suture anchor placed into the groove we previously made at the mid-point of the patella. This
anchor is placed at the hemisphere of the patella.
Typically, only a single anchor is necessary for
fixation. The knee is now placed over a bolster in
order to position it at 20–30°. The patella is
placed in the center of the groove and the suture
from our suture anchor is passed in order to fix the
iliotibial band strip to the lateral aspect of the
patella. (Fig. 2) Any excess iliotibial band strip is
then sutured to the anterior patellar periosteum
with an absorbable #0 suture.
Stability of the patella is then checked in full
extension and at 30 degrees of flexion. The knee
is taken through a full arc of motion to assess
patellar tracking. The goal is 1 quadrant of
medial glide of the patella and the patella should
be able to be everted to neutral when the patella
is centered over the trochlear groove with the
4
Procedure
We perform the procedure under general anesthesia with a regional nerve block. The patient is
positioned supine on an operative table with the
contralateral extremity padded free from pressure. A non-sterile tourniquet is applied high on
the thigh. If we are performing arthroscopy, a
lateral stress post is utilized in order to aid with
application of valgus stress when viewing the
medial compartment. Some authors prefer the
use of a leg holder. We prefer to position the
operative leg free in order to allow full range of
motion of both the hip and knee during surgery
to better assess stability of the patellofemoral
joint. Once positioning is complete, the entire
lower extremity is prepped and draped. The limb
is exsanguinated and the procedure is performed
under tourniquet control.
When addressing iatrogenic medial instability,
preexisting incisions may dictate approach for
reconstruction of the lateral patellofemoral ligament. In the absence of prior surgery and in most
cases of revision surgery we utilize a two incision approach. The goal is to adequately visualize the mid-portion of the iliotibial band and also
visualize the lateral border of the patella. We first
utilize an anterior midline incision to expose the
patella. This incision is typically 5–7 cm in
length. This is taken down through the subcutaneous tissues until the prepatellar fascia is identified. The prepatellar fascia is then incised
longitudinally and lifted laterally in order to
expose the lateral retinaculum. In cases of
extensive iatrogenic medial instability the lateral
retinaculum may be completely absent and the
joint may be open to the subcutaneous tissues. In
most cases the lateral joint is covered by a sheet
of scar tissue. The lateral patellar border is
identified and a cautery knife is utilized to clear
the lateral border of soft tissue. A small rongeur
is then utilized to decorticate the lateral patellar
border and create shallow trough to aid with
472
D. S. Zhu and L. D. Farrow
Fig. 1 A 10 mm wide 80
mm long strip of iliotibial
band is created. Reprinted
with permission, Cleveland
Clinic Foundation ©2022. All
Rights Reserved
knee in full extension. Lateral tilt of the patella is
indicative of over tensioning and should be
avoided. If happy with stability and patellar
tracking the defect in the iliotibial band is then
closed side to side with a running absorbable #0
suture. (Fig. 3) Closing this defect will help to
further tension the iliotibial band reconstruction
of the lateral patellofemoral ligament. At this
time we will typically place the arthroscope back
into the knee in order to confirm proper patellofemoral tracking through the range of motion,
specifically confirming that there is not abnormal
lateral tracking.
At this point in time the tourniquet is deflated
and meticulous hemostasis is obtained prior to
closure. All wounds are closed in layers and the
patient is placed into a sterile compressive bandage. We utilize a motion-control hinged knee
brace. Disposable ice packs or a cryotherapy
device is placed in the operating room.
5
Pearls and Pitfalls
The greatest pearl with respect to management of
the medial patellofemoral dislocator/subluxator is
prevention. Lateral release should be avoided
whenever possible in treatment of lateral patellar
instability, especially in patients with underlying
significant ligamentous laxity. When the lateral
retinaculum is tight and in need of management,
the surgeon should utilize lateral retinacular
lengthening whenever possible. Lateral retincular
lengthening helps to avoid symptomatic medial
instability. Proper diagnosis is also of utmost
importance. Apprehension with medial patellar
glide is often seen with these patients. On occasion, a clunk can also be felt with this maneuver.
This maneuver should be performed on all
patients presenting with complaints of patellofemoral instability.
Reconstruction of the Lateral Patellofemoral Ligament
473
Fig. 2 The iliotibial band
strip is passed under the
anterior iliotibial band in
order to fix it to the lateral
aspect of the patella.
Reprinted with permission,
Cleveland Clinic Foundation
©2022. All Rights Reserved
This procedure is fairly straightforward but
taking an IT band strip which is too short could
make it difficult or impossible to pass the strip to
the lateral aspect of the patella. Generally a 60–
70 mm long strip (as measured from a plumb line
at the level of the mid-patella) will be long
enough to reconstruct the LPFL. Suture irritation
in the IT band has been seen on occasion. Nonabsorbable sutures used to close the harvest
defect can possibly rub on the lateral condyle and
cause pain from friction. Alternatively, thinner
patients may feel the suture in the IT band. In
order to prevent this I utilize an absorbable #0
suture to close the IT band defect. We have seen
no complications with this approach.
6
Postoperative Rehabilitation
Following surgery, the patient is touch-down
weight-bearing until seen by the Physical Therapist. Once properly instructed, the patient may
progress to weight-bearing as tolerated with the
brace locked in full extension. Once the patient is
confident with ambulation while the brace is
unlocked he/she may progress off crutches.
When non-weight-bearing the brace may be
unlocked and motion is allowed. For the first
4 weeks following surgery, the patient is allowed
motion from 0 to 90°. After 4 weeks, range of
motion can be progressed as tolerated. The brace
474
D. S. Zhu and L. D. Farrow
Fig. 3 The defect in the
iliotibial band is closed side to
side. Reprinted with
permission, Cleveland Clinic
Foundation ©2022. All
Rights Reserved
may be unlocked for weight bearing at 4 weeks
post-surgery if quadriceps function and gait
mechanics allow. The brace is discontinued at
6 weeks post-surgery. Expectations are that
patients may begin a running program at
3 months post-surgery. Return to sport may
commence as soon as 4 months post-surgery if
pain and effusion has resolved, range of motion
has fully returned and when the patient has met
return to play criteria as determined by the
Physical Therapist.
7
Outcomes
Due to the rare occurrence of medial patellar
instability there have not been many large studies
evaluating outcomes following lateral patellofemoral ligament reconstruction. Most of the evidence describing lateral techniques to address
medial patellar instability exists as isolated case
reports or case series [13–21]. One of the first
studies evaluating outcomes came from Hughston et al. who evaluated direct repair or reconstruction of the LPFL in 63 patients with
symptomatic patellofemoral instability [9]. At
final follow-up 80% of patients reported good to
excellent results and 6 knees required additional
surgery due to failure to improve [9]. The authors
found this technique was effective in relieving
painful medial subluxation of the patella [9].
In addition to improved functional status following LPFL reconstruction, Sanchis-Alfonso
et al. also evaluated resolution of psychological
variables following reconstruction [18]. As
mentioned previously, patients with medial subluxation of the patella following overzealous
lateral release can present not only with apprehension and instability but also patellofemoral
pain. In the study by Sanchis-Alfonso et al. 24%
Reconstruction of the Lateral Patellofemoral Ligament
475
of patients had signs of depression, 59% had
anxiety, 41% exhibited catastrophizing with
respect to patellofemoral pain and 100% exhibited kinesiophobia [18]. Following LPFL reconstruction depression, anxiety and catastrophizing
was completely resolved in this cohort and only
53% experienced kinesiophobia [18]. This study
outlined the importance of LPFL reconstruction
not only for relieving painful medial subluxation
but also for improving psychological findings in
these patients.
Our own greater than 10-year anecdotal
experience with lateral patellofemoral ligament
reconstruction mirrors the clinical outcomes discussed above. Careful diagnosis is critical to
insure that medial subluxation is the true cause of
patient symptoms. When present, medial patellar
instability can be quite unsettling and even mentally and physically debilitating for the patient.
Lateral patellofemoral ligament reconstruction is
a simple yet extremely effective procedure for
correction of medial patellar instability, both
iatrogenic and primary. Owing to the large width
of the iliotibial band, when proper surgical technique is utilized, there is low risk for morbidity
with this technique. Lateral patellofemoral ligament reconstruction should be in the armamentarium of any surgeon routinely managing
patients with complex patellofemoral pathology.
5. Ostermeier S, Holst M, Hurschler C, Windhagen H,
Stukenborg-Colsman C. Dynamic measurement of
patellofemoral kinematics and contact pressure after
lateral retinacular release: an in vitro study. Knee
Surg Sports Traumatol Arthrosc. 2007;15(5):547–54.
https://doi.org/10.1007/s00167-006-0261-0
Epub
2007 Jan 16 PMID: 17225178.
6. Pollard B. Old dislocation of patella by intra-articular
operation. Lancet. 1891;30(2):1203–4.
7. Chen SC, Ramanathan EB. The treatment of patellar
instability by lateral release. J Bone Joint Surg Br.
1984;66(3):344–8.
https://doi.org/10.1302/0301620X.66B3.6725343 PMID: 6725343.
8. Merchant AC, Mercer RL. Lateral release of the
patella. A preliminary report. Clin Orthop Relat Res.
1974;(103):40–5. https://doi.org/10.1097/00003086197409000-00027. PMID: 4414065.
9. Hughston JC, Deese M. Medial subluxation of the
patella as a complication of lateral retinacular release.
Am J Sports Med. 1988;16(4):383–8. https://doi.org/
10.1177/036354658801600413. PMID: 3189663.
10. Jackson RW, Kunkel SS, Taylor GJ. Lateral retinacular release for patellofemoral pain in the older patient.
Arthroscopy. 1991;7(3):283–6. https://doi.org/10.
1016/0749-8063(91)90128-k PMID: 1750937.
11. Kolowich PA, Paulos LE, Rosenberg TD,
Farnsworth S. Lateral release of the patella: indications and contraindications. Am J Sports Med.
1990;18(4):359–65. https://doi.org/10.1177/036354
659001800405. PMID: 2403183.
12. Miller PR, Klein RM, Teitge RA. Medial dislocation
of the patella. Skeletal Radiol. 1991;20(6):429–31.
https://doi.org/10.1007/BF00191085 PMID: 1925
675.
13. Loeb AE, Farr J, Parikh SN, Cosgarea AJ. Noniatrogenic medial patellar dislocations: case series and
international patellofemoral study group experience
Orthop J Sports Med. 2021;9(2):2325967120985530.
https://doi.org/10.1177/2325967120985530.
PMID:33748301;PMCID:PMC7938389.
14. Ahmad CS, Sinicropi SM, Su B, Puffinbarger WR.
Congenital medial dislocation of the patella. Orthopedics. 2003;26(2):189–90. https://doi.org/10.3928/
0147-7447-20030201-25 PMID: 12597226.
15. Johnson DP, Wakeley C. Reconstruction of the
lateral patellar retinaculum following lateral release:
a case report. Knee Surg Sports Traumatol Arthrosc.
2002;10(6):361–3. https://doi.org/10.1007/s00167002-0309-8 Epub 2002 Sep 11 PMID: 12444515.
16. Nonweiler DE, DeLee JC. The diagnosis and treatment of medial subluxation of the patella after lateral
retinacular release. Am J Sports Med. 1994;22
(5):680–6. https://doi.org/10.1177/0363546594022
00517. PMID: 7810793.
17. Richman NM, Scheller AD Jr. Medial subluxation of
the patella without previous lateral retinacular release.
Orthopedics. 1998;21(7):810–3. https://doi.org/10.
3928/0147-7447-19980701-12 PMID: 9672920.
References
1. Johnson RP. Lateral facet syndrome of the patella.
Lateral restraint analysis and use of lateral resection.
Clin Orthop Relat Res. 1989;148–58. PMID:
2910595.
2. Krompinger WJ, Fulkerson JP. Lateral retinacular
release for intractable lateral retinacular pain. Clin
Orthop Relat Res. 1983;179:191–3 PMID: 6617015.
3. Bedi H, Marzo J. The biomechanics of medial
patellofemoral ligament repair followed by lateral
retinacular release. Am J Sports Med. 2010;38
(7):1462–7. https://doi.org/10.1177/0363546510373
581. PMID:20601605.(B,1891).
4. Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human
knee. Am J Sports Med. 1998;26(1):59–65. https://
doi.org/10.1177/03635465980260012701.
PMID:
9474403.
476
18. Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC, Merchant AC. Results of isolated lateral
retinacular reconstruction for iatrogenic medial patellar instability. Arthroscopy. 2015;31(3):422–7.
https://doi.org/10.1016/j.arthro.2014.09.005
Epub
2014 Nov 4 PMID: 25450418.
19. Yazdi H, Monshizadeh S, Bozorgi Z. Congenital
medial dislocation of the patella with multiple
congenital anomalies: case report and method of
treatment. J Pediatr Orthop B. 2014;23(2):126–9.
https://doi.org/10.1097/BPB.0b013e32836330c6
PMID: 24296651.
D. S. Zhu and L. D. Farrow
20. Saper MG, Shneider DA. Medial patellar subluxation
without previous lateral release: a case report.
J Pediatr Orthop B. 2014;23(4):350–3. https://doi.
org/10.1097/BPB.0000000000000054 PMID: 247
55851.
21. Akşahin E, Yumrukçal F, Yüksel HY, Doğruyol D,
Celebi L. Role of pathophysiology of patellofemoral
instability in the treatment of spontaneous medial
patellofemoral subluxation: a case report. J Med Case
Rep. 2010;22(4):148. https://doi.org/10.1186/17521947-4-148.
PMID:20492715;PMCID:PMC28
83992.
Patellar Tendon Imbrication
Ronak M. Patel, Sneh Patel,
and Jack Andrish
1
Introduction
Lateral patellar dislocations are not uncommon,
with a reported incidence of 30 to 43 per 100,000
[1]. Furthermore, the recurrence rate of patellar
dislocations is reported to be 20 to 80% [1–4].
An increasingly common surgery used to treat
patellofemoral instability is a medial patellofemoral ligament (MPFL) reconstruction [5–7].
Patel et al. analyzed the ABOS Part II database
and reported that the number of MPFL reconstructions performed increased an average of 3%
annually from 2003–2017 [8]. However, in their
systematic review, Shah et al. reported a complication rate of 26.1% for MPFL reconstructions
[5]. The increased percentage of MPFL reconstructions and relatively high complication rate
highlight the need to evaluate for other anatomic
risk factors for recurrent patellar instability.
R. M. Patel (&)
Illinois Center for Orthopaedic Research and
Education, 550 W. Ogden Ave, Hinsdale, IL 60521,
USA
e-mail: r-patel7@md.northwestern.edu
S. Patel
University of Illinois College of Medicine at
Chicago, Chicago, IL, USA
J. Andrish
The Cleveland Clinic Foundation, Cleveland, OH,
USA
One of the most common risk factors for
recurrent patellar instability is patella alta.
Review of radiographic findings in patients with
recurrent patellar instability found patella alta to
be one of the most common underlying pathoanatomic findings related to the recurrence of
patellar disclocations [9]. The exact definition of
patella alta has been up to debate but recently the
patellar articular surface contact with the articular
surface of the trochlea has been used to relate
normal vs abnormal patellar tendon lengths [10].
In patella alta, the increased distance between the
patella and the trochlea leads to delayed
engagement of the patella and trochlea during
flexion, which has been associated with increased
patellofemoral contact forces and greater vulnerability to patellar dislocation [11–14].
A common approach to surgically correcting
patella alta is to perform a tibial tuberosity
osteotomy with a distalization [15]. However, a
tibial tuberosity osteotomy cannot be performed
in a skeletally immature patient because of the
presence of the open tibial tuberosity apophysis.
Additionally, tibial tuberosity osteotomy has
been associated with problems of delayed union
and non-union and hardware irritation and damage [16, 17]. A novel method to treat patella alta
was described in 2007 by the senior author, and it
involves shortening the patellar tendon via
imbrication [18]. Since the imbrication procedure
does not involve the tibial tuberosity, it can be
used in skeletally immature and mature patients.
This chapter discusses the surgical technique for
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_32
477
478
R. M. Patel et al.
the imbrication procedure in the treatment of
patella alta as well as recent results from a
radiographic study.
2
Surgical Indications
Patella alta is typically measured via a validated
height index, including Blackburne-Peele, InsallSalvati, and Caton Deschamps ratios. Patients who
present with radiographically confirmed patella
alta and recurrent patellar dislocations are candidates for the imbrication procedure [10, 19–22].
Since the pathoanatomies are usually multifactorial, the procedure often includes other patellar
stabilization techniques including MPFL reconstruction vs medial retinacular imbrication and
lateral lengthening. Furthermore, if medialization
of the tibial tuberosity is needed, the imbrication
can be combined with a Trillat osteotomy of the
tibial tuberosity, instead of performing a distalmedial transfer of the tuberosity [23].
The imbrication procedure can also be used
for management of anterior knee pain in a patient
with patella alta and patella chondrosis that
involves the distal articular surface. This procedure allows the load to be transferred to the more
proximal articular cartilage, which will result in
the lessening of contact stresses due to a broader
distribution of the load.
3
Surgical Technique
The amount of shortening of the patellar tendon
is first determined by creating a patella tendon
length that will normalize the Insall-Salvati
(IS) Index. An IS ratio of 1:1 is the intended
goal of the imbrication procedure. An exception
to this method is when the patella has a long nonarticular nose. In this case, the amount of shortening is determined by normalizing the modified
IS index or the Canton-Deschamps Index. If a
MPFL reconstruction needs to be completed,
perform the imbrication technique before the
MPFL reconstruction. However, if a medialization osteotomy of the tibial tuberosity is required,
perform the osteotomy before performing the
imbrication technique. A video of the imbrication
procedure is provided in Yalcin et al. [24]. The
surgical technique (Fig. 1) is described below.
Step 1: The amount of shortening is determined
preoperatively through radiographic measurements and marked with a marking pen (a).
A third line is drawn proximally to the dissection
that is one-half the distance of the patella tendon
shortening (b = 1/2a).
Step 2: At the location of the distal marking, the
anterior half of the tendon is elevated by sharp
dissection using a fresh No. 15 blade proximal to
the predetermined level. The dissection follows
the parallel fibers of the tendon. Throughout the
dissection, it is important to stay uniform in
thickness.
Step 3: After detaching the infra-patella fat pad
from the posterior aspect of the patella tendon,
three #1 PDS are placed from the proximal
marking and passed deep to the tendon and
brought midway through the dissected portion of
the tendon. After a locking stitch has been made,
the sutures are again passed deep to the tendon
and returned to the original entry site and left
untied. These sutures will be used to fasten the
redundant flap on the posterior side that results
from the imbrication.
Step 4: Three #2 FiberWire (Arthrex, Naples,
FL) sutures are placed at the proximal apex of the
flap created in Step 2 and passed through the flap
and secured to the original start of the dissection.
Locking stitches are made distally and returned
to the original entry site.
Step 5: The FiberWire sutures are tied, and it is
sometimes helpful to distract the patella distally
as the sutures are tied to facilitate the imbrication.
Patellar Tendon Imbrication
Step 6: The sutures placed in Step 3 are tied,
which imbricates the redundant posterior side of
the tendon. The distal end of the anterior section
of the tendon is repaired in a pants-over-vest
fashion using #0 absorbable sutures.
Step 7: The knee is flexed to 90° to assess for
competence of the sutures. Additionally, the
flexion is used to assess for the need for a
quadriceps lengthening in cases of severe patella
alta or fixed congenital lateral patellar dislocation.
Full flexion is usually obtained after rehabilitation.
4
Postoperative Care
The initial phase of the postoperative care
involves a motion-control brace set at zero to 30
degrees of flexion and touchdown nonweightbearing is allowed. Starting at 2–3 weeks
after surgery, flexion is increased in the brace by
10–20° per week until week 6. At 6 weeks, the
brace can be completely removed. If full
weightbearing is needed prior to 6 weeks after
surgery, the brace can be locked in 0° of extension during ambulation. Starting at 3 weeks, the
brace can be removed to perform heel-slide range
of motion exercises. However, except for performing the exercises, the brace should be worn
full time when ambulating or sleeping.
Patients are encouraged to perform hourly repetitions of quadriceps isometric exercises as well as
focus on ‘pelvifemoral’ conditioning and core stability. After 6 weeks, weightbearing can be
increased gradually and patients can be slowly
weaned off of crutches. Closed chain resistance
exercises can also be started around this time.
However, open chain resistance exercises are
deferred until 4 months. Full weightbearing is usually achieved by 8–12 weeks. Return to full rehabilitation and sport level activity generally is seen
after 6 months but can vary depending on factors
such as age and elimination of strength deficits.
479
5
Discussion
Patellar instability is not uncommon in the
skeletally immature population. The rate of
patellar dislocation was found to be 29% to 43%
in the age range of 10 to 17 years [1, 3, 4]. These
patellar dislocations have been highly associated
with patella alta. However, the most common
procedure to treat patella alta is a tibial tuberosity
osteotomy with distalization, and this procedure
cannot be performed on this patient population
due to an open apophysis. Because of this issue,
the senior author developed the imbrication
method to correct patella alta in skeletally
immature patients that has now been expanded to
adults.
A recent study conducted by Patel et al.
assessed the postoperative radiographic results of
the imbrication procedure [25]. The study evaluated 27 patients (32 knees) with a mean age of
19.8 years (range, 12–35 years) and a mean
follow-up of 4.1 years (range, 2–8.25 years).
The mean patellar length preoperatively was
6.1 cm (range, 5.0–8.0 cm). The mean patellar
length 3 weeks and a minimum of 2 years postoperatively was 5.1 cm (range, 3.4–8.0 cm) and
5.2 cm (range, 3.7–7.1 cm), respectively. On
average there was no significant loss of the corrected length of the patellar tendon postoperatively at a minimum of 2 years. Additionally, the
complications involved in this procedure were
minimal. Parvaresh et al. also described an
imbrication technique that was similar to one
described in this chapter [26]. However, the
paper did not assess the clinical outcomes of their
technique.
In conclusion, the patellar tendon imbrication
is a viable and effective technique in treating
patella alta with recurring patellar instability in
skeletally immature and mature patients.
480
R. M. Patel et al.
Fig. 1 Stepwise patellar tendon imbrication procedure. See text for details. Adapted from Andrish [18]. Reprinted with
permission, Cleveland Clinic Center for Medical Art & Photography ©2022. All Rights Reserved
Take Home Messages
• Patella alta is a common underlying cause of recurrent
patellar instability
• Tibial tuberosity osteotomy has been historically
performed to correct patella alta, but this procedure
cannot be used on skeletally immature patients due to
an open apophysis
• Patellar tendon imbrication can be performed on
skeletally immature and mature patients to correct
patella alta
• Careful dissection of the patellar tendon at 50% depth
throughout ensures appropriate integrity
• Performing locking stitches prevents migration of the
imbrication/reduction
• A clinical study evaluating patellar tendon imbrication
demonstrated that there was no significant loss of the
corrected length of the patellar tendon after a minimum
of 2 years postoperatively
Key Message: In both skeletally immature and
mature patients, patellar tendon imbrication is an
effective procedure in treating patella alta with
recurring patellar instability
References
1. Fithian DC, Paxton EW, Stone ML, Silva P,
Davis DK, Elias DA, et al. Epidemiology and natural
history of acute patellar dislocation. Am J Sports
Med. 2004;32(5):1114–21.
2. Amin NH, Lynch TS, Patel RM, Patel N,
Saluan P. Medial patellofemoral ligament reconstruction. JBJS Rev. 2015;3(7):1–9.
3. Atkin DM, Fithian DC, Marangi KS, Stone ML,
Dobson BE, Mendelsohn C. Characteristics of
patients with primary acute lateral patellar dislocation
and their recovery within the first 6 months of injury.
Am J Sports Med. 2000;28(4):472–9.
4. Quirbach S, Smekal V, Rosenberger RE, El Attal R.
Scho¨ ttle PB. Anatomical double-bundle reconstruction of the medial patellofemoral ligament with a
gracilis autograft [in German]. Oper Orthop Traumatol. 2012;24:131–9.
5. Shah JN, Howard JS, Flanigan DC, Brophy RH,
Carey JL, Lattermann C. A systematic review of
complications and failures associated with medial
patellofemoral ligament reconstruction for recurrent
patellar dislocation. Am J Sports Med.
2012;40:1916–23.
6. Gao G, Liu P, Xu Y. Treatment of patellar dislocation with arthroscopic medial patellofemoral ligament reconstruction using gracilis tendon autograft
and modified double-patellar tunnel technique: Minimum 5-year patient-reported outcomes. J Orthopaed
Surg Res. 2020;15(1). https://doi.org/10.1186/
s13018-020-1556-4.
7. McNeilan RJ, Everhart JS, Mescher PK,
Abouljoud M, Magnussen RA, Flanigan DC. Graft
choice in isolated medial patellofemoral ligament
reconstruction: a systematic review with metaanalysis of rates of recurrent instability and patientreported outcomes for autograft, allograft, and synthetic options. Arthroscopy. 2018;34:1340–54.
8. Chilelli B, Patel R, Bhatia S, Das V. Surgical trends
and reported complications of medial patellofemoral
Patellar Tendon Imbrication
9.
10.
11.
12.
13.
14.
15.
16.
ligament reconstruction among board eligible orthopaedic surgeons: analysis of data over a 15 year
period. Am J Sports Med. Forthcoming.
Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc.
1994;2:19–26.
Biedert RM, Albrecht S. The patellotrochlear index:
a new index for assessing patellar height. Knee Surg
Sports Traumatol Arthrosc. 2006;14:707–12. https://
doi.org/10.1007/s00167-005-0015-4.
Luyckx T, Didden K, Vandenneucker H, Labey L,
Innocenti B, Bellemans J. Is there a biomechanical
explanation for anterior knee pain in patients with
patella alta? Influence of patellar height on patellofemoral contact force, contact area and contact
pressure. J Bone Joint Surg Br. 2009;91:344–50.
Singerman R, Davy DT, Goldberg VM. Effects of
patella alta and patella infera on patellofemoral
contact forces. J Biomech. 1994;27:1059–65.
Stefanik JJ, Zhu Y, Zumwalt AC, et al. Association
between patella alta and the prevalence and worsening of structural features of patellofemoral joint
osteoarthritis: the multicenter osteoarthritis study.
Arthritis Care Res. 2010;62:1258–65.
Ward SR, Terk MR, Powers CM. Patella alta:
association with patellofemoral alignment and
changes in contact area during weight-bearing.
J Bone Joint Surg Am. 2007;89:1749–55.
Mayer C, Magnussen RA, Servien E, Demey G,
Jacobi M, Neyret P, et al. Patellar tendon tenodesis in
association with tibial tubercle distalization for the
treatment of episodic patellar dislocation with patella
alta. Am J Sports Med. 2012;40:346–51. https://doi.
org/10.1177/0363546511427117.
Payne J, Rimmke N, Schmitt LC, Flanigan DC,
Magnussen RA. The incidence of complications of
tibial tubercle osteotomy: a systematic review.
Arthroscopy. 2015;31:1819–25. https://doi.org/10.
1016/j.arthro.2015.03.028.
481
17. Sherman SL. Tibial tubercle osteotomy that includes
distalization has higher reoperation and revision
rates. Healio Medblog; 2018. https://www.healio.
com/news/blogs/%7Bd0aa44d3-00d3-4b42-beef660d11561766%7D/patellofemoral-update/blogtibial-tubercle-osteotomy-that-includesdistalizationhas-higher-reoperation-and-revision-rates.
18. Andrish J. Surgical options for patellar stabilization
in the skeletally immature patient. Sports Med
Arthrosc Rev. 2007;15(2):82–8. https://doi.org/10.
1097/jsa.0b013e31805752d0.
19. Neyret P, Robinson AHN, Le Coultre B, Lapra C,
Chambat P. Patellar tendon length—the factor in
patellar instability? Knee. 2002;9:3–6.
20. Caton J, Deschamps G, Chambat P, Lerat JL,
Dejour H. Patella infera. Apropos of 128 cases.
Rev Chir Orthop Reparatrice Appar Mot.
1982;68:317–25.
21. Blackburne JS, Peel TE. A new method of measuring
patellar height. J Bone Joint Surg Br. 1977;59:241–2.
22. Insall J, Salvati E. Patella position in the normal knee
joint. Radiology. 1971;101:101–4. https://doi.org/10.
1148/101.1.101.
23. Andrish J. Patellar tendon shortening. In: Dejour D,
Zaffagnini S, Arendt E, Sillanpää P, Dirisamer F,
editors. Patellofemoral pain, instability, and arthritis.
2nd ed. Springer; 2020. p. 551–6.
24. Yalcin S, Patel RM, Andrish J, Farrow LD. Patellar
tendon imbrication. Video J Sports Med. 2021;1
(3):263502542110066.
https://doi.org/10.1177/
26350254211006699.
25. Patel RM, Gombosh M, Polster J, Andrish J. Patellar
tendon imbrication is a safe and efficacious technique
to shorten the patellar tendon in patients with patella
alta.
Orthop
J
Sports
Med.
2020;8
(10):232596712095931.
https://doi.org/10.1177/
2325967120959318.
26. Parvaresh KC, Huddleston HP, Yanke AB. Patellar
tendon shortening for treatment of patella alta in
skeletally immature patients with patellar instability.
Arthrosc Techniq. 2021;10(8). https://doi.org/10.
1016/j.eats.2021.04.025.
Quadricepsplasty
Jason Koh
1
Introduction
Quadricepsplasty in the context of anterior knee
pain and instability is primarily required in
patients with congenital or obligate patella dislocation who have a tight or excessively contracted extensor mechanism [1]. In these patients
in order to obtain knee flexion, the contracted
extensor mechanism will seek the shortest distance between the femoral attachment and the
tibial tubercle, and the patella dislocates laterally
rather than remaining on the trochlea (Fig. 1)
[2, 3].
Treating these instability patients without
recognition and treatment of these contractures
will lead to either loss of motion, recurrent dislocation, or both [3–5]. In severe cases, quadricepsplasty to lengthen the tight extensor
mechanism is required to successfully maintain
patella stability [6, 7]. Quadricepsplasty may be
also required for such conditions such as congenital dislocation of the knee [2], arthrogryposis
[2], and congenital or acquired arthrofibrosis or
quadriceps scarring [8–10].
Historically, a number of procedures such as
the Thompson [11] or Judet [12] quadricep-
J. Koh (&)
Department of Orthopaedic Surgery, NorthShore
University HealthSystem, Skokie, IL, USA
e-mail: drjasonkoh@gmail.com
splasty have been described for the treatment of
acquired quadriceps contractures. Typically these
have been related to quadriceps contracture or
adhesions that can occur after trauma [13], but
with the changes in management of femur fractures with internal fixation and rapid mobilization
this has become less commonly required. When
these types of more extensive quadricepsplasties
need to be performed it is more commonly in
those patients who have prolonged use of external fixation and/or immobilization [14]. Key to
those procedures are the progressive release of
intra- and extra-articular adhesions, resection of
fibrous tissue and scar, and sometimes resection
or release of fibrotic or contracted muscle [14,
15]. The results are typically successful in
achieving improvement of range of motion, but
these extensive procedures may have a relatively
high complication rate and a significant rate of
residual quadriceps weakness [2, 9, 13, 16].
In the context of obligate dislocation in flexion, these types of extensive procedures are not
usually necessary. Several authors have proposed
either Z step cut lengthening [6, 7, 18] or V–Y
lengthening [18, 19] of the quadriceps tendon to
allow increased excursion. These reports have
been very small series or case reports in patients
with significant congenital dislocations and often
syndromic conditions. The patients have typically
improved range of motion but there have been a
relatively significant number of complications,
residual quadriceps weakness or recurrences.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_33
483
484
J. Koh
Fig. 1 Contracted and laterally displaced extensor
mechanism resulting in patella dislocation in flexion.
(Reproduction with permission from the Cleveland Clinic
Foundation) [1]
In these patients the lateral structures are tight
and contracted, and the quadriceps tendon is
usually shortened. Conversely, the medial structures, including the vastus medialis obliquus and
the medial retinacular tissues are often deficient
and stretched out from being pulled over the distal
femur [1, 20]. The pathophysiologic combination
of these factors guides the recommendations for
treatment of these patients. Medial structures are
to be preserved and reinforced; while lateral
structures (including potentially the iliotibial
band) are to be lengthened appropriately.
2
Evaluation
The evaluation of the patient should consist of
several components. Importantly, it should be
identified if these patients are symptomatic.
Some patients with congenital or obligate patella
dislocation have good knee function for daily
activity [21], and are able to walk, work, and
perform household functions with little or no
pain [21, 22]. It is not uncommon for these
patients to appear to have some syndromic
appearance or abnormality [23–25], which can be
associated with cognitive impairment. Understanding patient functional goals and symptoms
is important, along with an evaluation of the
potential impact and risks of a major surgical
procedure and ability to comply with a fairly
demanding postoperative regimen.
A careful assessment of the alignment is also
critical. Obligate dislocation may be in part
related to valgus malalignment, tibial tubercle
malalignment, or rotational malalignment of the
femur and/or tibia. As part of the physical
examination there should be evaluation of limb
alignment and rotation, including extended and
seated Q angle, foot progression angle and hip
rotation. Radiographic assessment should include
long leg standing alignment films and a true
lateral to assess patella height and trochlear
dysplasia. If there is concern from the physical
examination, axial CT imaging is helpful to
assess femoral and tibial version as well as tibial
tubercle to trochlear groove distance. These
patients often have trochlear dysplasia and
hypoplastic femoral condyles [25]. Significant
bony malalignment will need to be addressed,
and in some cases appropriate osteotomy may
confer significant stability and obviate the need
for quadricepsplasty [26].
Additional components of the physical
examination should include assessment of patella
tracking, evaluation of the ability of the patella to
maintain stability through the range of motion,
lateral tightness, apprehension, crepitus, tenderness and effusion. The quadriceps should be
inspected for atrophy and orientation.
MRI imaging is often helpful in evaluating
soft tissues and cartilage. The medial structures
are often deficient, and the medial patellofemoral
ligament (MPFL) if present is often attenuated.
MRI can provide an alternative method of evaluating TT-TG and trochlear dysplasia.
Quadricepsplasty
485
Table 1 Indications
1.
2.
3.
4.
5.
3
Contracture of extensor mechanism resulting in obligate lateral patella dislocation and poor function
Congenital dislocation of the patella
Given “normal” alignment, failure of lateral lengthening to permit relocation of patella
Arthrofibrosis/arthrogryposis with quadriceps contracture
Significant patella alta requiring distalization that would result in loss of knee flexion
Indications
The primary indication for quadricepsplasty is
significant lateral side and extensor mechanism
tightness that prevents the patella from being [1]
located with the knee in flexion. Medial patellofemoral ligament reconstruction and lateral
lengthening are often sufficient for many patients
with lateral patella dislocation; however, if lateral
lengthening alone is insufficient to permit
reduction in knee flexion quadricepsplasty may
need to be performed (Table 1).
4
Contraindications
Contraindications to quadricepsplasty include the
absence of significant quadriceps contracture. In
many cases, lateral side tightness can be
addressed with lateral retinacular lengthening
rather than quadriceps lengthening. Another
significant contraindication is lack of significant
functional impairment or pain. As noted, some
patients are relatively functional for their activities of daily living; or have limited mobility or
limb function so that addressing the dislocation
or contracture may not provide significant
improvement in quality of life. An inability to
comply with the postoperative regimen is also a
contraindication to quadricepsplasty. Finally,
Table 2 Contraindications
1.
2.
3.
4.
5.
Lack of quadriceps contracture
Minimal symptoms or impact on daily activities
Inability to comply with postoperative management
Poor or absent quadriceps function
Inadequate soft tissue coverage
patients with preexisting significant quadriceps
weakness or lack of function may have a higher
risk of poor function since there is often a period
of postoperative quadriceps weakness that may
become permanent (Table 2).
5
Surgical Technique
5.1 Preoperatively
A tourniquet is applied on the thigh for potential
use but is generally not immediately inflated
since this may affect quadriceps excursion. To
limit blood loss and improve hemostasis,
1000 mg of intravenous tranexamic acid is
infused preoperatively. Perioperative antibiotics
are also used. Patella tracking and mobility are
assessed.
5.2 Incision and Exposure
Typically, an anterior incision is made that
extends from the tibial tubercle to 6–10 cm
proximal to the patella with the knee in extension. The patella, patella tendon, 6–10 cm of
quadriceps tendon, vastus lateralis, rectus, and
vastus medius insertion are exposed. The medial
side is often noted to be stretched out and
deficient.
486
J. Koh
5.3 Lateral Side Releases
Stepwise progression of lateral releases and
lengthening is performed. If the patella cannot be
easily relocated, a lateral retinacular lengthening
is performed similar to that described by Larson
[27] (following Slocum’s description). (Figure 2)
Initially, the more superficial lateral retinacular
tissue (the superficial oblique lateral retinacular
tissue) is divided along the lateral patella, carefully separating it from the deep transverse lateral
retinaculum. This split is developed posteriorly
until reaching the iliotibial band and then released
off the band. The deep capsule can also be
released. Patella tracking and the ability of the
patella to remain reduced with the knee at 90
degrees of flexion is assessed. If this is not possible, additional releases need to be performed.
Repair is performed at the conclusion of the
overall lengthening and stabilization procedure.
The two layers (superficial oblique and deep
transverse) can be repaired edge to edge (Fig. 2).
This is performed with the patella located and the
knee flexed 90 degrees, since otherwise the tissue
if repaired in extension or less flexion may fail
with knee flexion since it will be under greater
tension. Typically, up to 1.5–2 cm of lengthening
can be achieved. Lengthening is preferred to
release since the lateral retinaculum confers
additional stability to the patella. Additionally, a
lateral retinacular defect can be painful and
unsightly. If there already has been some type of
lateral release leaving deficient or absent tissue,
sometimes retinacular flaps can be raised or a
graft performed.
The lateral capsule is then released, including
adjacent to the lateral edge of the patella tendon.
The lateral patellomeniscal ligaments and the
lateral retinaculum adjacent to the patella tendon
can act as a tether to limit medial translation of
the extensor mechanism [1]. The lateral infrapatellar fat pad is where the lateral patellofemoral
ligaments are located. The use of electrocautery
is helpful since the fat pad is quite vascular.
The vastus lateralis tendon insertion to the
patella is then divided at the patella and sharply
Fig. 2 Lateral retinacular lengthening. The superficial
layer is divided adjacent to the patella, and separated from
the deep transverse lateral retinaculum. The step-cut is
then repaired at the conclusion of the case with the knee in
flexion. (Reproduced with permission from Ellsworth
et al.) [20]
separated from the central quadriceps tendon
(Fig. 3). Proximally, the posterior undersurface
attachments of the vastus lateralis are then
released off the lateral intermuscular septum
using sharp and blunt dissection.
Care should be taken since there are some
small perforating vessels. This mobilization is
key to allowing increased excursion of the vastus
lateralis.
Quadricepsplasty
Fig. 3 Mobilization of the vastus lateralis oblique. The
tendon is divided from the patella and proximally to the
musculotendinous junction. The muscle belly is elevated
from the intramuscular septum. Reproduced with permission from the Cleveland Clinic Foundation) [1]
5.4 Quadriceps Lengthening
If following the lateral releases and mobilization,
the patella is unable to remain reduced in the
trochlea with the knee at 90 degrees of flexion,
quadriceps lengthening will need to be
performed.
The initial step of quadriceps lengthening is to
release the vastus lateralis from the patella and
quadriceps tendon 6–10 cm proximal to the
quadriceps insertion. Undersurface synovial
adhesions and attachments of the quadriceps to
the femur should also be released since they can
also tether the extensor mechanism. Again,
patella tracking is assessed. If the patella is able
to remain reduced to 90 degrees of knee flexion,
the vastus lateralis is repaired to the quadriceps
tendon with the knee flexed. Conversely, if
obligate dislocation is seen, then the main
quadriceps tendon will need to be lengthened.
487
Several techniques to lengthen the quadriceps
tendon exist, including V–Y lengthening and
step-cut (Z) lengthening in the coronal plane. The
author’s preference is a step cut (Z) lengthening
beginning on the superolateral quadriceps insertion to the patella, extending transversely 50%,
and then proximally 6–8 cm before exiting
medially. This is similar to that described by
Green but with a longer central split to allow side
to side tendon repair (Fig. 4).
This preserves the VMO attachment to the
patella and quadriceps tendon while applying a
relatively greater medial force to the proximal
pole of the patella. Given that the medial structures are already relatively lengthened and attenuated, and the vastus medialis obliquus is already
often stretched and weakened, the medial structures are unlikely to be the source of excessive
tightness. Additionally, cutting or detaching the
VMO will contribute further to temporary and
perhaps permanent weakness of this important
muscle for knee function and patella stability.
The appropriate length of the extensor mechanism can then be determined by flexing the knee
to 90 degrees and seeing where the appropriate
cut ends of the central quadriceps tendon are
located. This is marked and the side-to-side
repair of the quadriceps tendon at the appropriate
length is performed with the knee in extension to
avoid distraction on the repair site. Typically the
central tendon lengthening is 1–2 cm. Multiple
high strength suture or tapes are used in a locking
stitch fashion to provide a robust repair between
the split tendon. The longer split allows for a
greater number of crossing sutures spanning the
repair site. This can be further oversewn with
interrupted sutures for reinforcement. The vastus
lateralis is similarly sutured at the appropriate
location onto the lateral quadriceps tendon. This
is often significantly more proximal (4–6 cm) to
the patella than the central quadriceps tendon
lengthening and is consistent with the differential
contracture of the lateral, central, and medial
sides. If there is concern that the tendon is deficient, allograft tissue can be incorporated as a
patch onto the repair. Tension on the repair
should be assessed and the knee should just be
488
J. Koh
Given that the medial structures remain deficient, at this point a medial patellofemoral ligament reconstruction is performed. As usual, great
care should be taken to avoid excessive tension
on the graft in flexion. For further reinforcement,
the VMO insertion can be sutured to the superior
limb of a two-tailed MPFL graft. Notably, the
graft should not have to “pull” the patella into the
trochlea and should be without tension with the
knee in deeper flexion.
6
Fig. 4 Step-cut quadriceps lengthening. After detachment of the vastus lateralis, a transverse step-cut is made
in the central quadriceps tendon. The vastus medialis
obliquus insertion is preserved, and the medial cut is
proximal to the bulk of the VMO attachment. The knee is
flexed and the amount of lengthening is determined
followed by side-to-side repair of the central quadriceps
tendon and the vastus lateralis tendon. (Modified with
permission from Ellsworth et al.) [20]
able to flex to 90 degrees with the patella located
and good tension without gapping. The lateral
retinacular tissues can be then repaired with the
knee flexed as previously described.
Associated Procedures and Order
of Correction
In general, if an osteotomy to correct bony
malalignment needs to be performed, this would
be done prior to addressing the soft tissue.
A tibial tubercle osteotomy can be done at this
point through the anterior incision. If a varus or
rotational osteotomy needs to be performed, the
appropriate incisions are made and the osteotomy
performed prior to the extensor lengthening, but
care should be taken to plan the exposure to
avoid incisions too close together. If there is a
significant concern the procedure can be staged.
If autologous soft tissue is used for the MPFL
reconstruction, it is preferred to use a hamstring
graft rather than a segment of the quadriceps
tendon since the central quadriceps tendon is
already being divided and should not be further
weakened. The hamstring graft harvest should be
performed at the beginning of the case since
otherwise the knee flexion that is commonly used
during harvest will put strain on the repaired
extensor mechanism. MPFL reconstruction
should be performed after the quadricepsplasty
since the patella and femur relative positions may
have changed.
7
Postoperative Management
The intraoperative evaluation should demonstrate
adequate stability of the repair up to 90 degrees
of flexion. Initially the patient is kept in a hinged
Quadricepsplasty
knee brace locked in extension for 2 weeks, and
then progression by allowing 30 degrees additional range of motion every 2 weeks in the brace
until 90 degrees of knee flexion is achieved. With
the brace locked in extension, touch down
weightbearing is permitted with the brace for the
first 2 weeks, then progressed to 50% at 4 weeks
and full at 6 weeks. The brace can be discontinued when quadriceps function allows a
straight leg raise. The initial goal range of motion
is 110 degrees of knee flexion by 3 months.
Progression is slow to allow tissues to heal
without excessive lengthening or stretching out.
489
mechanism, meticulous and strong repair techniques, and rehabilitation that respects the biology of healing. Recurrent instability is related to
improper tensioning and the lack of strong
medial structures to restrain the patella. Reconstruction of the MPFL helps decrease the risk of
instability. In either case, if patients remain
symptomatic, revision repair and reconstruction
would be appropriate.
Other potential issues include wound complications or failure of range of motion.
10
8
Results of Quadricepsplasty
Early results of quadricepsplasty for congenital
or obligate dislocation utilized different techniques of quadriceps lengthening and had relatively good results in terms of keeping the patella
reduced. These procedures did not differentially
lengthen the vastus lateralis compared to the
central and medial quadriceps tendon, and it was
not uncommon to see patients who had an
extensor lag [2, 28].
More recently, Andrish described repairing
the vastus lateralis to the side of a coronal split
central quadriceps tendon. He was able to
achieve good range of motion and patella stability, and good quadriceps function. He did note
that the restoration of quadriceps strength took
up to a year [1].
Green has also described differential repair of
the vastus lateralis to a split quadriceps tendon.
The split cut is similar to that described here with
preservation of the VMO and medial quadriceps
tendon attachment. No extensor lag was noted in
24 patients [20].
9
Complications
Complications of quadricepsplasty are primarily
related to either failure of extensor mechanism
repair resulting in extensor lag, or recurrent
instability. Prevention of failure of the repair is
related to appropriate tensioning of the extensor
Take Home Message
Obligate lateral patella dislocation is primarily
contracture of the lateral more than central or
medial tissues. Lateral release should be meticulous and complete, and begin with retinacular
tissues, the lateral patellotibial ligaments, and
then the vastus lateralis. A step-cut lengthening
of the quadriceps tendon preserving the medial
quadriceps tendon and VMO attachments may
allow for improved quadriceps strength and differential tensioning of the less contracted medial
structures [20]. The repair should be tested
intraoperatively to demonstrate appropriate
patella tracking. Lateral structures should be
repaired at the appropriate tension and the medial
patellofemoral ligament reconstructed to increase
patella stability. With appropriate technique and
rehabilitation, excellent results can be expected.
References
1. Andrish J. Quadricepsplasty for congenital dislocation of the patella and patellar tendon shortening for
patella alta. In: Parikh S, editor. Patella Instability.
Philadelphia: Wolters Kluwer; 2020. p. 353–61.
2. Tercier S, Shah H, Joseph B. Quadricepsplasty for
congenital dislocation of the knee and congenital
quadriceps contracture. J Child Orthop. 2012;6
(5):397–410.
3. Bose K, Chong KC. The clinical manifestations and
pathomechanics of contracture of the extensor mechanism of the knee. J Bone Joint Surg Br. 1976;58-B
(4):478–84.
4. Zeier FG, Dissanayake C. Congenital dislocation of
the patella. Clin Orthop Relat Res. 1980;148:140–6.
490
5. Bergman NR, Williams PF. Habitual dislocation of
the patella in flexion. J Bone Joint Surg Br. 1988;70
(3):415–9.
6. Gao GX, Lee EH, Bose K. Surgical management of
congenital and habitual dislocation of the patella.
J Pediatr Orthop. 1990;10(2):255–60.
7. Ghanem I, Wattincourt L, Seringe R. Congenital
dislocation of the patella. Part II: orthopaedic management. J Pediatr Orthop. 2000;20(6):817–22.
8. Dos Santos CF. GA TAM, Rocha de Faria JL, Perez
da Motta D, Dos Santos Cerqueira F, Adolphson F.
Minimally Invasive Quadricepsplasty Arthrosc Tech.
2019;8(3):e343–7.
9. Oliveira VG, D’Elia LF, Tirico LE, Gobbi RG,
Pecora JR, Camanho GL, et al. Judet quadricepsplasty in the treatment of posttraumatic knee
rigidity: long-term outcomes of 45 cases. J Trauma
Acute Care Surg. 2012;72(2):E77-80.
10. Hung NN, Tan D, Do Ngoc Hien N. Patellar
dislocation due to iatrogenic quadriceps fibrosis:
results of operative treatment in 54 cases. J Child
Orthop. 2014;8(1):49–59.
11. Thompson TC. Quadricepsplasty. Ann Surg.
1945;121(5):751–4.
12. Masse A, Biasibetti A, Demangos J, Dutto E,
Pazzano S, Gallinaro P. The judet quadricepsplasty:
long-term outcome of 21 cases. J Trauma. 2006;61
(2):358–62.
13. Merchan EC, Myong C. Quadricepsplasty: the Judet
technique and results of 21 posttraumatic cases.
Orthopedics. 1992;15(9):1081–5.
14. Ali AM, Villafuerte J, Hashmi M, Saleh M. Judet’s
quadricepsplasty, surgical technique, and results in
limb reconstruction. Clin Orthop Relat Res.
2003;415:214–20.
15. Daoud H, O'Farrell T, Cruess RL. Quadricepsplasty.
The Judet technique and results of six cases. J Bone
Joint Surg Br. 1982;64(2):194–7.
16. Bidolegui F, Pereira SP, Pires RE. Safety and
efficacy of the modified Judet quadricepsplasty in
patients with post-traumatic knee stiffness. Eur J
Orthop Surg Traumatol. 2021;31(3):549–55.
J. Koh
17. Marumo K, Fujii K, Tanaka T, Takeuchi H, Saito H,
Koyano Y. Surgical management of congenital
permanent dislocation of the patella in nail patella
syndrome by Stanisavljevic procedure. J Orthop Sci.
1999;4(6):446–9.
18. Wada A, Fujii T, Takamura K, Yanagida H, Surijamorn P. Congenital dislocation of the patella.
J Child Orthop. 2008;2(2):119–23.
19. Jones RD, Fisher RL, Curtis BH. Congenital dislocation of the patella. Clin Orthop Relat Res.
1976;119:177–83.
20. Ellsworth B, Hidalgo Perea S, Green DW. Stepwise
lengthening of the quadriceps extensor mechanism
for severe obligatory and fixed patella dislocators.
Arthrosc Tech. 2021;10(5):e1327–31.
21. Eilert RE. Congenital dislocation of the patella. Clin
Orthop Relat Res. 2001;389:22–9.
22. Drennan JC. Congenital dislocation of the knee and
patella. Instr Course Lect. 1993;42:517–24.
23. Ferrone JD Jr. Congenital deformities about the knee.
Orthop Clin North Am. 1976;7(2):323–30.
24. Sever R, Fishkin M, Hemo Y, Wientroub S,
Yaniv M. Surgical treatment of congenital and
obligatory dislocation of the patella in children.
J Pediatr Orthop. 2019;39(8):436–40.
25. Grisdela PT, Paschos N, Tanaka MJ. Fixed (congenital) patellar dislocation. Clin Sports Med. 2022;41
(1):123–36.
26. Ramaswamy R, Kosashvili Y, Murnaghan JJ,
Yau CK, Cameron JC. Bilateral rotational osteotomies of the proximal tibiae and tibial tuberosity
distal transfers for the treatment of congenital lateral
dislocations of patellae: a case report and literature
review. Knee. 2009;16(6):507–11.
27. Ceder LC, Larson RL. Z-plasty lateral retinacular
release for the treatment of patellar compression
syndrome. Clin Orthop Relat Res. 1979;144:110–3.
28. Mo Y, Jing Y, Wang D, Paley D, Ning B. Modified
Langenskiold procedure for congenital patella dislocations in pediatric patients. BMC Musculoskelet
Disord. 2022;23(1):241.
Sulcus Deepening Trochleoplasty
Edoardo Giovannetti de Sanctis
and David H. Dejour
1
Introduction
Trochlear dysplasia refers to a genetic pathologic
alteration of the trochlear shape, becoming shallow, flat or even convex sometimes with a
superolateral prominence (Fig. 1). The trochlear
dysplasia, and therefore an incongruency
between trochlear and patellar surfaces, has a
high influence on patellar tilt, subluxation and
lateral displacement, failing to provide an adequate constraint to the normal patellar tracking.
Trochlear dysplasia is the main factor in patellar
dislocation and is found in 96% of the population
with objective patellar dislocation OPI (at least
one true dislocation) [1]. The higher the degree
of trochlear dysplasia, the higher the risk of
instability. We found in the old literature the
Disclosure Statement
E. G. d. S. has nothing to disclose.
D. D.: Royalties ARTHREX.
E. Giovannetti de Sanctis (&) D. H. Dejour
Lyon-Ortho-Clinic: Clinique de La Sauvegarde,
Ramsay Santé, 8, avenue Ben Gourion, 69009 Lyon,
France
e-mail: edoardo.giovannettids@gmail.com
D. H. Dejour
e-mail: corolyon@wanadoo.fr
E. Giovannetti de Sanctis
Lyon Ortho Clinic, 29 Av. des Sources, 69009 Lyon,
France
description of trochleoplasty by Bilton Polar in
1890, but since then it has undergone different
changes. Another publication done by Masse in
1978 [2] describes a sort of trochleoplasty but
was Henri Dejour in 1987 [3] who popularized
and standardized the method and gave the
rational for it. In 2010 David Dejour modified it
to improve the correction of the different features
of the trochlear dysplasia [4]. The procedure’s
main aim is to decrease the trochlear prominence
while creating a new groove with both a normal
depth and orientation.
2
Radiologic Features
and Classification
Standard radiographic views, such as weight
bearing true lateral view, axial view at 30° of knee
flexion, and anteroposterior (AP) view, are
mandatory to start a patellofemoral disorder evaluation [5, 6]. The lateral view has to be performed
by superimposing the two posterior femoral condyles in a monopodal weight-bearing position with
20° of flexion. This projection shows from anterior
to posterior the contour of the facets and the line
representing the trochlear sulcus [5, 7]. The lateral
condyle, and therefore the lateral facet, might be
recognized, having a more visible condylotrochlear groove and a greater radiopacity. The
line representing the trochlear sulcus is in continuity with the Blumensaat line, which is the line
drawn along the roof of the intercondylar notch.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_34
491
492
Fig. 1 High grade trochlear dysplasia (anterior view of a
right knee). There is no sulcus, and in the lateral aspect
(right) a big bump can be observed
Fig. 2 To analyse the trochlear dysplasia a true profile is
needed with a perfect superimposition of the posterior
femoral condyles. The three trochlear dysplasia signs are:
the crossing sign, the supra-trochlear spur, the doublecontour which goes below the crossing sign
E. Giovannetti de Sanctis and D. H. Dejour
protuberance (bump or prominence) on the
superolateral part of the trochlea with a functional effect, during the trochlear engagement,
similar to the ski ramp pushing the patella on the
lateral side and creating an antimaquet effect.
The double contour sign represents the medial
hypoplastic facet subchondral bone becoming
posterior to the lateral condyle on the sagittal
projection. Axial views obtained at 30° of knee
flexion allow the measurement of the sulcus
angle [8]. From the trochlear sulcus two lines are
drawn going towards the most superior point of
each facet. The mean normal value defined by
Brasttorm was 145° (SD ± 6).
Axial view provides a good assessment of the
mid trochlea but might miss the flatness of the
superior part of the trochlea. Therefore, the best
way to screen the trochlear dysplasia on X-rays is
on the sagittal view.
However, frequently in a dysplastic trochlea
no measurement can be made as there is no
identifiable sulcus and we believe in the subjective impression of the trochlear shape. For those
two reasons, the trochlear shape is best evaluated
on axial cross-sectional images (CT scan or
MRI).
MRI has also the advantage of better assessing any softening and/or damage to the cartilage
[10]. Based on these signs, and cross-checking
the sagittal radiographs with the cross-sectional
images the trochlear dysplasia might be classified
in four types (Table 1) (Fig. 3) [11, 12].
3
On the sagittal view the trochlear dysplasia is
defined by three radiographic pillars: the crossing
sign, the supratrochlear spur and the doublecontour sign (Fig. 2).
The crossing sign is positive when the radiographic line of the trochlear sulcus crosses the
anterior projection of the femoral condyles. It
represents the exact position where the sulcus
reaches the same antero-posterior height of the
femoral condyles, corresponding to a macroscopic flat trochlea.
The supratrochlear spur which is clearly
identified during the surgical exposure, is a
Function and Biomechanics
The lateral facet is oriented obliquely in the
coronal plane with an antero-lateral direction.
The lateral facet is both larger and more protuberant anteriorly than the medial one, respectively in the coronal and sagittal plane. The
corresponding lateral patellar joint surface follows this this shape. This bony constraint contributes preventing the patella from a lateral
dislocation.
The patella rests on the supratrochlear anterior
femoral cortex in total extension, engaging the
trochlea during early flexion.
Sulcus Deepening Trochleoplasty
493
Table 1 The Trochlear dysplasia Dejour’s classification.. CS: Crossing sign; SS: Supratrochlear spur; DC: Double
contour
Type
Sagittal View
Axial images
A
CS
Shallower trochlea
B
CS and SS
Flat or convex
C
CS and DC
Convex lateral facet and hypoplastic medial facet
D
CS, SS, DC
A prominent and convex lateral facet with a vertical connection to an hypoplastic medial
facet almost absent (cliff pattern)
Fig. 3 Trochlear dysplasia classification according to D.
Dejour: Type A: Crossing sign (X-rays). Shallower
trochlea (Slice images); Type B: Crossing sign and
supratrochlear spur (X-rays). Flat or convex trochlea
(Slice images); Type C: Crossing sign and double-contour
sign (X-rays). Convex lateral facet and hypoplastic medial
facet (Slice images); Type D: Crossing sign, supratrochlear spur, and double-contour sign (X-rays).
Hypoplastic medial facet proximally short and almost
absent with a vertical connection to a prominent and
convex lateral facet defining the so called “cliff pattern”
(Slice images)
494
E. Giovannetti de Sanctis and D. H. Dejour
A posteriorly directed force produced, mainly
by the quadriceps, pushes the patella against the
trochlea. Both the articulating surfaces orientation and the tibial internal rotation during knee
flexion, create a medially directed vector,
directing the patellar tracking [13].
A trochlea without properly oriented facets
(TD) prevents the patella from sliding properly
up and down within the margins [14].
Trochlear shape guide the patellar tracking and
therefore an incongruency between trochlear and
patellar surfaces, has a high influence on patellar
tilt, subluxation and lateral displacement [11].
The PF joint reaction force, which is linked to
the onset and progression of orteoarthritis,
depends also on the trochlear prominence. The
bigger the trochlear prominence, the greater the
compressive reaction force in flexion. Therefore,
decreasing the protrusion would lead to an
expected reduction of the PF reaction force.
4
Goals
Sulcus deepening trochleoplasty has three functions while treating patients with trochlear dysplasia: it modifies the trochlear shape with a
central groove and oblique medial and lateral
facets; it decreases the patellofemoral joint
reaction force by reducing the supratrochlear
prominence (spur); and might reduce the TT–TG
value by a proximal realignment.
5
Indications
Sulcus deepening trochleoplasty has specific and
selective indications: e.g.patients with types B
and D trochlear dysplasia, in which the prominence of the trochlea (supratrochlear spur) is
relevant (>5 mm); recurrent patellar dislocation
and maltracking. In patients with patellofemoral
osteoarthritis, open growth plates, and pain with
no history of dislocations this procedure is
contraindicated.
Trochlear dysplasia type A is not considered a
severe morphologic abnormality, as the groove is
slightly modified: the sulcus is clearly visible
although the groove has a shallower angle. No
shape modifying procedures are necessary;
recurrent dislocations or maltracking should be
attributed to other anatomic risk factors: patella
alta, tibial tubercle—trochlear groove (TT–TG)
distance or patellar tilt.
Although trochlear dysplasia type C has a
shape substantially altered there is no prominence to be corrected, making the choice of the
proper treatment controversial. Sulcus deepening
trochleoplasty is not indicated for those patients,
usually undergoing an alternative procedure like
a mild medialization and/or distalization.
The degree of instability and clinical symptoms should also be considered when proposing
this procedure to a patient. Sulcus deepening
trochleoplasty, as any other surgical procedure, is
liable to failure and therefore, the indication
should not be given lightly.
Associated anatomic risk factors have to be
evaluated preoperatively in order to plan an
eventual correction: tibial tubercle distalization/
medialization and/or lateral release. Tibial tubercle medialization might be not necessary in cases
of increased TT–TG, as sulcus deepening
trochleoplasty lateralizes the groove, thus
decreasing the this distance. The sulcus deepening trochleoplasty is part of the “menu à la carte”,
meaning specific procedures for each of the main
anatomic risk factors in patellar instability.
The MPFL (Medial patello-femoral ligament)
reconstruction is systematically added to the
sulcus deepening trochleoplasty, in order to treat
the consequence of the ligament rupture occurred
during the first dislocation episode.
6
Surgical Technique
The procedure is generally performed with the
patient supine under both regional anesthesia and
sedation. A thigh tourniquet is positioned.
A straight midline incision is performed, with the
knee flexed at 90°, from the superior pole of the
patella to the tibiofemoral joint line. A transquadricipital approach is done.
Sulcus Deepening Trochleoplasty
495
Fig. 4 Surgical exposure. The periosteum is incised along the osteochondral edge and reflected away from the
trochlear margin. The anterior femoral cortex should be visible to guide the bone resection
The patella is not everted but retracted laterally and it is carefully inspected for cartilage
damages. The trochlea is exposed (Fig. 4). An
incision along the femoro-trochlear junction is
performed and the peritrochlear synovium/
periosteum are reflected using a periosteal elevator. The anterior distal femoral cortex should
be visible to evaluate the supratrochlear spur
adapting the amount of deepening.
With the trochlea fully exposed, the native
trochlear groove is marked with a sterile pen.
Two additional divergent lines, representing the
lateral and medial facet limits, are drawn, from
the notch going laterally and medially, through
the condylotrochlear grooves (sulcus terminalis).
Those two lines have to be out of the tibiofemoral articulation (Fig. 5).
The planned trochlear groove is marked in a
more lateral position according to the preoperative TT-TG value to be aligned with the
anatomical femoral axis.
Thereafter the under surface of the trochlea is
assessed. A thin strip of femoral anterior cortical
bone is removed all around the trochlea, with a
thickness equal to the height of the prominence
from the anterior femoral cortex, i.e., the bump
formed. A sharp osteotome is used to remove the
bone.
Subsequently, cancellous bone must be
removed from the under surface of the trochlea.
Using an offset guide-equipped drill, different
tunnels are made through the subtrochlear cancellous bone, from proximal to distal (top of the
notch) and parallel to the anterior cortex.
Fig. 5 After the surgical exposure, the new trochlea is drawn. From the intercondylar notch, the bottom of the sulcus
and the facets are planned
496
E. Giovannetti de Sanctis and D. H. Dejour
Fig. 6 In order to allow further modeling to the underlying bone bed, the osteochondral flaps may be cut in the sulcus
and facets lines
The offset guide tip is placed on the anterodistal part of the notch. The distance between the
drill and guide tip never goes below 5 mm to
ensure uniform thickness of the osteochondral
flap and prevent cartilage damage. Thereafter, a
high-speed burr is used to remove the cancellous
bone bridges between the tunnels. The guide
equipped with a cartilage palpator set at 5 mm is
used to determine the thickness of the bone
resection and avoid crossing the trochlea or
producing cartilage injuries inflicted by heat.
More cancellous bone could be then removed
from the central metaphyseal part towards the
notch, below the planned trochlear groove, to
make the deepest part of the groove flush with
the anterior cortex.
Light pressure should be able to model the
flap to the underlying cancellous bone bed in the
distal femur. The groove, and the lateral facet
external margin, might be cut to allow further
modeling (Fig. 6).
Pieces of bone graft, using the thin strip of
femoral cortical bone removed previously, might
be placed medially and laterally, between the flap
and the bone bed, to elevate the medial and lateral facet and increase the angle of the new trochlea if necessary. A 145° Polyethylene Pusher is
used to apply light pressure and mold the flap to
the underlying cancellous bone bed (Fig. 7).
The new trochlea is fixed by placing with one
absorbable anchor with 2 absorbable sutures
(Vicryl number 2) placed at the top of the notch.
Fig. 7 Lateral and anterior views of the dysplastic trochlea after trochleoplasty
Sulcus Deepening Trochleoplasty
Both ends of each suture are then fixed at the
proximal lateral and proximal medial (trochlear
facets) bone margins of the corresponding facet
with a knotless anchor. Patellar tracking is tested
and measures may be obtained. Periosteum and
synovial tissue are sutured to the osteochondral
edge.
The associated procedures are then carried
out.
The lateral retinaculum is systematically
released or lengthened due to its usual tightness.
The other instability factors like patella alta or
axial malalignment are corrected if needed
according to the “menu à la carte” with medialization and/or distalization. The chronology of
the procedure is trochleoplasty first, lateral
release, tibial tubercle osteotomy and then MPFL
reconstruction.
497
Phase 2 (46th to 90th day): closed kinetic
chain (e.g. cycling) and weight- bearing proprioception exercises are started initially respectively with weak resistance and in bipodal stance.
The anterior and posterior muscular chains are
stretched.
Phase 3 (4th to the 6th month): a gradually
return to sport might be started. Running is
allowed initially on a straight line. The patient is
encouraged to proceed with the rehabilitation on
his own. After 6 to 8 months sports might be
resumed.
An imaging follow-up is recommended a
6 weeks and 6 months respectively with radiographs (AP, sagittal and axial view at 30° of
flexion) and CT scan (Figs. 8 and 9).
8
7
Post-Operative Care
Sulcus deepening trochleoplasty by itself does
not need weight-bearing restriction, range of
motion (ROM) limitation or the use of a brace.
Continuous passive motion (CPM) might
improve cartilage healing. Furthermore, immobilization would decrease the trophism of
Quadriceps femoris muscle and lead to a higher
risk of postoperative knee stiffness.
The rehabilitation protocol presented hereafter
has to be used with patients undergoing only the
sulcus deepening trochleoplasty. Associated
procedures would need slight modifications like
an extension brace for walking during 30 days if
a tibial tubercle osteotomy is done.
The rehabilitation protocol is divided in 3
phases.
Phase 1 (1st to 45th day): passive and active
ROM are started to facilitate osteochondral
healing and further modelling of the newly
formed trochlea by patellar tracking. Range of
motion is gradually regained, avoiding forced
and painful postures. Immediate weight-bearing
is allowed. Quadriceps strengthening is allowed
through static isometric contraction and
stimulation.
Results
The sulcus deepening trochleoplasty results
described by different authors are difficult to
compare due to a non-uniformity in terms of
associated procedures performed, inclusion criteria used and the presence/absence of previous
surgery.
The best post-operative results have been
highlighted in patients with objective patellar
instability, high-grade trochlear dysplasia (type B
or D), and when all other anatomic risk factors
are corrected simultaneously.
This procedure has shown good postoperative
clinical outcomes, a high rate of both subjective
satisfaction and PF joint stability. Joint stiffness
and pain are common complaints at follow up.
Controversial is whether the sulcus deepening
trochleoplasty influences the development of
patello-femoral osteoarthritis.
Trochlear cartilage damage, incongruence
with the patella, and excessive or insufficient
correction are potential complications.
Schottle et al. [15] evaluated with a biopsy the
trochlear cartilage lining of three patients after
sulcus deepening trochleoplasty, outlining a low
risk of damage.
Instability recurrence is a rare complication
and is frequently due to missed associated risk
498
E. Giovannetti de Sanctis and D. H. Dejour
Fig. 8 Pre and postoperative
lateral x-rays showing the
resection of the supratrochlear
bump and trochlear
prominence correction
Fig. 9 X-ray axial views
before and after
trochleoplasty. The trochlear
sulcus is restored
factors (patella alta, TT-TG, excessive patellar
tilt).
Zaffagnini et al. [16] reviewed the clinical
outcomes of MPFL reconstruction with and
without sulcus deepening trochleoplasty in
patients affected by trochlear dysplasia. Altrough,
no difference was found in the overall redislocation rate between those two groups, they stated
that while treating severe trochlear dysplasia, the
redislocation rate is lower when sulcus deepening
trochleoplasty is added to MPFL reconstruction.
Balcarek et al. [17] confirmed that in OPI
patients with severe trochlear dysplasia, the sulcus deepening trochleoplasty has to be added to
the MPFL reconstruction to lower the risk of
post-operative redislocation/subluxation.
Dejour et al. [18] evaluated 24 knees with a
mean follow up of 66 months, undergoing a
sulcus deepening trochleoplasty for failure of
previous surgery with persistent patellar dislocation. Respectively 29.1% and 70.9% of patients
had type B and D trochlear dysplasia. After the
procedure, no recurrence of dislocation was
recorded up to the last follow-up. Pain decreased
significantly and the Apprehension sign was
negative in respectively 72% and 75% of cases.
Ntagiopoulos et al. [19] reviewed retrospectively the clinical outcomes of thirty-one sulcus
deepening trochleoplasties. No cases of stiffness
or instability recurrence or maltracking were
recorded. The apprehension sign remained positive in 19.3% of cases. The mean preoperative
and postoperative International Knee Documentation Committee (IKDC) score was respectively
51 (range, 25–80), and 82 (range, 40–100)
(p < 0.001). The mean Kujala score improved
Sulcus Deepening Trochleoplasty
from 59 (range, 28–81) to 87 (range, 49–100)
(p < 0.001).
PF stiffness has been shown as one of the
main factors decreasing the postoperative clinical
outcomes, leading sometimes to manipulation
under anaesthesia or arthroscopic arthrolysis
[20].
Zaffagnini et al. [16] have observed in their
systematic review that the addition of the
trochleoplasty to an MPFL reconstruction for the
treatment of severe trochlear dysplasia might
increase the risk of post-operative range of motion
(ROM) limitation.
Twenty-nine
arthroscopic
deepening
trochleoplasties were followed up for more than
twelve months by Blønd and Haugegaard [21].
No redislocations or arthrofibrosis were recorded.
The median Kujala score (range) improved from
64 (12–90) preoperatively to 95 (47–100)
postoperatively. The authors therefore stated
that the use of this technique is safe and
reproducible.
Song et al. compared trochleoplasty with nontrochleoplasty surgical procedures as a treatment
for patients with severe trochlear dysplasia, outlining inferior outcomes in terms of range of
motion (ROM) in the first group [22].
In Verdonk et al. [23] although the results of
the majority of patients scored fair/poor on an
objective scoring system, seventy-seven % were
satisfied with the procedure.
Seventeen consecutive sulcus deepening
trochleoplasties, with a one-year minimum follow up, were evaluated by Donell et al. [24]
Patellar tracking normalized in eleven knees and
had a slight J appearance in six. Seven patients
showed a mild residual apprehension. In terms of
subjective satisfaction, seven, six and two were
respectively very satisfied, satisfied, and disappointed. Three patients returned to full sports and
eight patients required further operations.
Carstensen et al. [25] evaluated the clinical
outcomes of 44 patients with Type B and D
trochlear dysplasia, treated with sulcus deepening trochleoplasties plus MPFL reconstruction,
with a minimum follow-up of 2-years. Although
a 18% rate of postoperative arthrofibrosis and
27% rate of overall reoperation, patients reported
499
a high rate in: satisfaction (mean of 9.1/10),
return to work (100%) and sport (84.8%).
Lutz et al. [26] stated that the addition of bony
procedures to MPFL reconstruction leaded to a
low redislocation rate, improved physical and
sexual activity and a quality of life comparable to
values
reported
after
isolated
MPFT
reconstruction.
Longo et al. [27] in their systematic review
outlined that the Dejour V-shaped sulcus deepening trochleoplasty leaded to the highest mean
Kujala post-operative score (79.3) compared to
the other trochlea modifying shape techniques.
Debated is the efficacy of this surgical procedure in decreasing PF pain.
Faruqui et al. [28] observed a greater risk of
postoperative anterior knee pain after sulcus
deepening trochleoplasty. Although four over six
patients reported postoperative anterior knee
pain, each one was satisfied with the postoperative clinical outcomes.
Also Beaufils et al. [20] confirmed the residual mild anterior knee pain as a frequent complication after this procedure.
Von Knoch et al. [29] evaluated forty-five
consecutive sulcus deepening trochleoplasty,
with a mean follow-up of 8.3 years; None of
those had recurrence of dislocation, However, PF
pain, referred pre-operatively in only 35 knees,
worsened in 15 (33.4%), remained unchanged in
four (8.8%) and improved in 22 (49%). Four
knees not referring pain pre-operatively (8.8%)
kept on being asymptomatic.
Rouanet et al. [30] evaluated thirty-four sulcus deepening trochleoplasties with a follow up
of 15 years. Sybjective patient satisfaction and
postoperative occasional pain rate were respectively 65% and 53%.
Controversial is the correlation between PF
arthritis, patellar dislocations and sulcus deepening trochleoplasty. Theoretically, the severe
altered morphology of the trochlea, influences
the patellar kinematics leading to a greater risk of
patellofemoral osteoarthritis [14]. Whether
patients with OPI and undergoing sulcus deepening trochleoplasty are respectively more prone
to and protected from developing osteoarthritis
has not been determined clearly yet [31].
500
E. Giovannetti de Sanctis and D. H. Dejour
Longo et al. [27] stated that sulcus deepening
trochleoplasty is associated with improved clinical outcomes and stability and a relatively low
rate of osteoarthritis and pain. In Von Knoch
et al. [29] 30% of knees undergoing sulcus
deepening trochleoplasty, evaluated at a mean
follow up of 8.3 years, developed PF degenerative changes. None of the twenty-seven patients
(thirty-one knees) evaluated by Ntagiopoulos
et al. [19] showed radiographic evidence of PF
cartilage severe degeneration at the latest followup. Song et al. [22] compared trochleoplasty with
non-trochleoplasty procedures as a treatment for
OPI patients with trochlear dysplasia type B to D.
The trochleoplasty group had a decreased risk of
redislocation and patellofemoral osteoarthritis
(Iwano grade 2 or greater) progression.
Rouanet et al. [30] evaluated thirty-four sulcus deepening trochleoplasties in terms of functional outcomes and rate of PF osteoarthritis. No
recurrent dislocation was found at the latest
follow-up. They highlighted that the outcomes
were significantly greater for patients undergoing
sulcus deepening trochleoplasty with a dysplasia
characterized by a supratrochlear spur. Preoperatively the PF OA was diagnosed only in 10
patients (all with < Iwano 2). At latest follow-up
the rate increased significantly. Osteoarthritis
was though identified in 33 over 34 patients, 65%
having more than Iwano grade 2.
9
Conclusion
Only knees with high grade trochlear dysplasia
(types B/D) in which the protuberance is over
5 mm, recurrent patellar dislocation and patellar
maltracking might be treated with sulcus deepening trochleoplasty.
It modifies the shape of the trochlea forming a
new central sulcus and two oblique facets; it
decreases the PF joint reaction force by reducing
the trochlear prominence and decreases the distance between trochlear groove and tibial
tuberosity.
It is effective in restoring PF stability and in
satisfying patients. Patients have to be aware of
the risk of developing postoperative Joint stiffness and pain.
Still Controversial is whether the sulcus
deepening trochleoplasty influences the development of patello-femoral osteoarthritis.
Acknowledgements The authors thank Paulo R.F. Saggin for his work on the previous edition of this chapter.
References
1. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc.
1994;2(1):19–26.
2. Masse Y. [Trochleoplasty. Restoration of the intercondylar groove in subluxations and dislocations of
the patella]. Rev Chir Orthop Reparatrice Appar Mot.
1978;64(1):3–17.
3. Dejour H, Walch G, Neyret P, Adeleine P. Dysplasia
of the femoral trochlea. Rev Chir Orthop Reparatrice
Appar Mot. 1990;76(1):45–54.
4. Dejour D, Saggin P. The sulcus deepening
trochleoplasty-the
Lyon’s
procedure.
Int
Orthop. 2010;34(2):311–6.
5. Maldague B, Malghem J. [Significance of the
radiograph of the knee profile in the detection of
patellar instability. Preliminary report]. Rev Chir
Orthop Reparatrice Appar Mot. 1985;71 Suppl 2:5–
13.
6. Malghem J, Maldague B. Depth insufficiency of the
proximal trochlear groove on lateral radiographs of
the knee: relation to patellar dislocation. Radiology.
1989;170(2):507–10.
7. Malghem J, Maldague B. Patellofemoral joint: 30
degrees axial radiograph with lateral rotation of the
leg. Radiology. 1989;170(2):566–7.
8. Merchant AC, Mercer RL, Jacobsen RH, Cool CR.
Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974;56(7):1391–6.
9. Davies AP, Bayer J, Owen-Johnson S, Shepstone L,
Darrah C, Glasgow MM, et al. The optimum knee
flexion angle for skyline radiography is thirty
degrees. Clin Orthop Relat Res. 2004;423:166–71.
10. Carrillon Y, Abidi H, Dejour D, Fantino O,
Moyen B, Tran-Minh VA. Patellar instability:
assessment on MR images by measuring the lateral
trochlear inclination-initial experience. Radiology.
2000;216(2):582–5.
11. Tavernier T, Dejour D. [Knee imaging: what is the
best modality]. J Radiol. 2001;82(3 Pt 2):387–405;
7–8.
12. Dejour D, Le Coultre B. Osteotomies in patellofemoral instabilities. Sports Med Arthrosc. 2007;15
(1):39–46.
Sulcus Deepening Trochleoplasty
13. Amis AA. Current concepts on anatomy and biomechanics of patellar stability. Sports Med Arthrosc.
2007;15(2):48–56.
14. Amis AA, Oguz C, Bull AM, Senavongse W,
Dejour D. The effect of trochleoplasty on patellar
stability and kinematics: a biomechanical study
in vitro. J Bone Joint Surg Br. 2008;90(7):864–9.
15. Schottle PB, Schell H, Duda G, Weiler A. Cartilage
viability after trochleoplasty. Knee Surg Sports
Traumatol Arthrosc. 2007;15(2):161–7.
16. Zaffagnini S, Previtali D, Tamborini S, Pagliazzi G,
Filardo G, Candrian C. Recurrent patellar dislocations: trochleoplasty improves the results of medial
patellofemoral ligament surgery only in severe
trochlear dysplasia. Knee Surg Sports Traumatol
Arthrosc. 2019;27(11):3599–613.
17. Balcarek P, Rehn S, Howells NR, Eldridge JD,
Kita K, Dejour D, et al. Results of medial
patellofemoral ligament reconstruction compared
with trochleoplasty plus individual extensor apparatus balancing in patellar instability caused by severe
trochlear dysplasia: a systematic review and metaanalysis. Knee Surg Sports Traumatol Arthrosc.
2017;25(12):3869–77.
18. Dejour D, Byn P, Ntagiopoulos PG. The Lyon’s
sulcus-deepening trochleoplasty in previous unsuccessful patellofemoral surgery. Int Orthop. 2013;37
(3):433–9.
19. Ntagiopoulos PG, Byn P, Dejour D. Midterm results
of comprehensive surgical reconstruction including
sulcus-deepening trochleoplasty in recurrent patellar
dislocations with high-grade trochlear dysplasia.
Am J Sports Med. 2013;41(5):998–1004.
20. Beaufils P, Thaunat M, Pujol N, Scheffler S, Rossi R,
Carmont M. Trochleoplasty in major trochlear dysplasia: current concepts. Sports Med Arthrosc Rehabil Ther Technol. 2012;4:7.
21. Blond L, Haugegaard M. Combined arthroscopic
deepening trochleoplasty and reconstruction of the
medial patellofemoral ligament for patients with
recurrent patella dislocation and trochlear dysplasia.
Knee Surg Sports Traumatol Arthrosc. 2014;22
(10):2484–90.
501
22. Song GY, Hong L, Zhang H, Zhang J, Li X, Li Y,
et al. Trochleoplasty versus nontrochleoplasty procedures in treating patellar instability caused by
severe trochlear dysplasia. Arthroscopy. 2014;30
(4):523–32.
23. Verdonk R, Jansegers E, Stuyts B. Trochleoplasty in
dysplastic knee trochlea. Knee Surg Sports Traumatol Arthrosc. 2005;13(7):529–33.
24. Donell ST, Joseph G, Hing CB, Marshall TJ. Modified
Dejour trochleoplasty for severe dysplasia: operative
technique and early clinical results. Knee. 2006;13
(4):266–73.
25. Carstensen SE, Feeley SM, Burrus MT, Deasey M,
Rush J, Diduch DR. Sulcus Deepening trochleoplasty
and medial patellofemoral ligament reconstruction
for patellofemoral instability: a 2-year study. Arthroscopy. 2020;36(8):2237–45.
26. Lutz PM, Winkler PW, Rupp MC, Geyer S,
Imhoff AB, Feucht MJ. Complex patellofemoral
reconstruction leads to improved physical and sexual
activity in female patients suffering from chronic
patellofemoral instability. Knee Surg Sports Traumatol Arthrosc. 2021;29(9):3017–24.
27. Longo UG, Vincenzo C, Mannering N, Ciuffreda M,
Salvatore G, Berton A, et al. Trochleoplasty techniques provide good clinical results in patients with
trochlear dysplasia. Knee Surg Sports Traumatol
Arthrosc. 2018;26(9):2640–58.
28. Faruqui S, Bollier M, Wolf B, Amendola N. Outcomes
after
trochleoplasty.
Iowa
Orthop J. 2012;32:196–206.
29. von Knoch F, Bohm T, Burgi ML, von Knoch M,
Bereiter H. Trochleaplasty for recurrent patellar
dislocation in association with trochlear dysplasia.
A 4- to 14-year follow-up study. J Bone Joint Surg
Br. 2006;88(10):1331–5.
30. Rouanet T, Gougeon F, Fayard JM, Remy F,
Migaud H, Pasquier G. Sulcus deepening trochleoplasty for patellofemoral instability: a series of 34
cases after 15 years postoperative follow-up. Orthop
Traumatol Surg Res. 2015;101(4):443–7.
31. Maenpaa H, Lehto MU. Patellofemoral osteoarthritis
after patellar dislocation. Clin Orthop Relat Res.
1997;339:156–62.
Arthroscopic Deepening
Trochleoplasty
Lars Blønd
1
Introduction
For a couple of decades, the trochleoplasty procedure has become a more established operation
for symptomatic trochlear dysplasia (TD). In a
cadaveric study TD was found in 17% of the
knees and here among 5% with high degree of
TD [1]. The fraction of those knees with TD that
becomes symptomatic is still unknown. Symptoms related to TD are first of all patellofemoral
instability (PFI), however some will experience
patellofemoral pain (PFP) and some will develop
isolated Patellofemoral osteoarthritis [2–8]. The
exact definition and classification of TD is still
evolving and yet there is no consensus on how to
define. The Dejour classification was the first and
is the most used, but due to problems with reliability, a new more reliable Oswestry-Bristol
classification has been introduced. Both classifications are subjective, which limits the use for
both clinical and scientific purposes. A classification based upon objective measures and
biomechanical studies is needed. For objective
measure the lateral trochlea inclination (LTI) has
L. Blønd (&)
Department of Orthopaedic Surgery, The Zealand
University Hospital, Koege, Denmark
e-mail: Lars.Blond@aleris-hamlet.dk
Department of Orthopaedic Surgery, Aleris-Hamlet,
Copenhagen, Denmark
been found useful and has been suggested as a
parameter to define TD [9–12]. Also measures
like trochlea depth [13, 14], trochlea asymmetry
[14], anterior posterior measurements [15] and
trochlea bump [16] can advantageously describe
the changes that separate TD from normal anatomy. The sulcus angle has commonly been used
to quantify the degree of trochlea dysplasia. The
sulcus angle varies from proximal to distal. The
sulcus angle is measured on axial MRI or CT at
the most proximal slice, depicting cartilage on
both medial and lateral trochlea facet. A common
limitation of the sulcus angle are those knees
where the medial facet is undeveloped and first
appears relative distal, since leads to lack of
recognition of TD. A recent study found the
sulcus angle less reliable [17]. Those problems
with defining TD and the shortage of good
quality comparable studies with longer follow-up
between trochleoplasty and alternative surgeries,
makes the indications of trochleoplasty surgery
debatable. The primary causes of restraint for
trochleoplasty have been risk of complications
and lack of healing of the cartilage flap, but these
concerns have proved unfounded [18]. So when a
symptomatic TD is present, and surgery is needed, the aim must be to normalize anatomy.
Surgery may not only be reserved for patients
with recurrent patellar instability but can also
include patients with patella subluxation after
first time patella dislocation, while others reserve
trochleoplasty for revisions of patellar instability.
In respect to indication for surgery for chronic
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_35
503
504
patellofemoral pain, only three studies have
reported on this and still restraint must be recommended [19–21]. Biomechanical studies have
spotted that TD affects the kinematics of the
patellofemoral joint and negatively influence the
stabilizing forces for the patella [16, 22, 23].
Reviews and metaanalysis have reported low rate
of re-dislocations, high satisfaction, a mean
reduction of pain and a low rate of complications
following trochleoplasty [24–27]. Several technical variations of deepening trochleoplasty
procedures have been published and the Arthroscopic deepening trochleoplasty (ADT) that is
going to be explained here, is a variant based
upon the thin thin flap Bereiter technique [21, 28,
31]. The ADT is less invasive and considered to
have the same known advantages from other
techniques based on minimal invasive surgery.
The ADT is in comparison to the open technique,
more demanding but also more precise due to the
enlargement of the arthroscope. The open
trochleoplasty is associated with the risk of
arthrofibrosis, infection, prolonged pain and scar
formation [32] and those complication have yet
not been observed by the ADT method. When
ether this is due to the minimal invasive surgery
itself or a less restrictive postoperative regime is
unclear. Though never reported in the scientific
literature it well known that there is a risk of
cartilage flap fracture during the open trochleoplasty procedure, and this is significantly reduced
with the ADT. A case series after ADT in combination with MFPL reconstruction demonstrated
results comparable with the results obtained for
open trochleoplasty procedures combined with
MPFL reconstruction [33]. Open trochleoplasty
surgery is considered complex and only for
experiences patellofemoral surgeons, and similar
applies for the ADT and additional arthroscopic
skills is needed. Training on cadaver knees is
recommend, despite cadaver knees typically
contains a V shaped trochlea with fragile cartilage, which means that the release of the cartilage
flake can be unachievable, but nonetheless it’s
important to practice portals and cartilage fixation technique. The cartilage release is more ease
when the trochlea is shallow or convex and the
cartilage is more elastic as in clinical cases. The
L. Blønd
purposes of the ADT procedure is reshape the
trochlea groove into a more normal configuration
and indirectly to unload the compressive forces
in the PF joint by deepening the trochlea. Indirectly this provides osseous stability by creating
a lateral trochlea wall. Another issue, can in cases
with a medialized groove, be to lateralize the
trochlea as this can help the tracking forces.
Ideally the trochlea is made approximately
4.5 mm deep and the trochlear should be lateralized to approximate a more normal figure of
50% trochlear symmetry [34]. By lateralizing the
groove the TT-TG is reduced [35]. In cases with
instability is the ADT technique combined with
MPFL reconstruction and eventually lateral
release or lateral lengthening. The MPFL reconstruction is needed since the trochlea do not
provide stability to the patella until there is sufficient overlap between trochlea and patella, and
that means for the first degrees of knee flexion a
patella stabilizing is needed to help the patella to
entrance the groove correctly. In cases with
chronic anterior knee pain without instability is
there no need to reconstruct MPFL. This chapter
will focus only on the ADT technique.
2
Indication
The main indication for ADT is symptomatic
patellar instability or severe chronic anterior knee
pain in patients with severe trochlear dysplasia
evaluated by MRI axial scans. The author’s
preferred parameters for evaluation of the degree
of trochlear dysplasia is the lateral trochlea
inclination angle and the threshold is 9 degrees,
when using the 2 image technique by Joseph
et al. [10, 12]. Other radiologic measurements
which are included in the evaluation is trochlear
asymmetry, trochlear depth and anterior posterior
measurements in relation to the width of the knee
[9, 14, 15]. Clinically the patellar instability
patients must have a positive reverse dynamic
patella apprehension test at a minimum of 30
degrees of flexion [36].
Contraindications are relative and can be
severe PF osteoarthritis and open growth plates.
Smaller grade 4 cartilage lesions are not
Arthroscopic Deepening Trochleoplasty
necessary a contraindication and healing of the
damaged cartilage flake occurs. Open growth
plates are relative contraindication. If the growing potential is nearing its end, meaning that the
patients are close to the height of the parents and
if the girls have had menstruation for more than a
year, the procedure can be done safely.
3
Technique
A tourniquet is avoided due to production of free
radicals that theoretically can impair healing and
cause increased inflammation. To reduce intraoperatively bleeding, reduction of leaks from the
portals in combination with gradually elevation
of the arthroscopic pump pressure can secure
visualization. One dose of intravenous antibiotics
is given preoperatively. Antithrombotic prophylactic treatment is considered in patients above
the age of 40 years or in cases with a history of
thrombotic complications.
3.1 Preparation and Portal
Placement
Initially a standard knee arthroscopy is done
through two small standard anterior portals and
the knee is inspected for other intraarticular
pathologies. The quality of the trochlear cartilage
is evaluated to assure that the procedure is
technically possible. A superior portal placed as
proximal as possible to reach an optimal view of
the trochlea and this is placed just medial to the
quadriceps tendon. In case of a suprapatellar
plica, this have to be resected such as the visualization is not inhibited. By insertion of a
hypodermic needle the correct placement is
identified, and a switching stick is introduced in
the same direction into the most proximal part of
the suprapatellar pouch followed by introduction
of the arthroscope. Preferable scope is 45degrees, but a 30- or 70-degree scope can be
used as well. With the scope introduced in the
suprapatellar portal, the position for the lateral
suprapatellar portal is localized by the needle
technique. Correct placement of this portal is
505
vital. The correct location is parallel to the
proximal extent of the flat part of the trochlear
groove in both the frontal and transversal planes,
to give the right working angle for the instruments. A too distal or too posterior placement
can be detrimental since it will not be possible to
get create the correct lateral wall angulation.
A too proximal portal can make it difficult to
reach the most distal part of the trochlea. A 8 mm
PassPort Button Canula (ArthrexInc. Naples, FL)
is useful as a working portal (Fig. 1).
3.2 Creation of the Cartilage Flap
A 90-degree radiofrequency device is introduced
through the lateral suprapatellar portal, the
synovium/periosteum is released from the area
proximal to the trochlear cartilage. The release is
continued as long proximal so a clear area is
ready for both using the shaver burrs and for later
placement of the proximal anchors when the flap
shall be reinserted. The cartilage flap is then
released by the use of respectively a 3- or 4-mm
round shaver burr without a shield, and a lambotte osteotome. Initially the shaver burr is
moved from medial to lateral and vice versa. The
cartilage is undermined, and the progression of
the shaver continues more and more distally
beneath the cartilage (Fig. 2). As a supplement to
the shaver, a straight and curved lambotte
osteotome (6 mm 27 cm) is needed. By adding the osteotome, the bone resection at the most
lateral part of the trochlea is minimized, helping
to achieve a normal lateral trochlear wall to
provide the patella with osseous stability
(Fig. 3). The cartilage flap separation from bone
is continued distally until the shaver meets the
curvature approximately 10 mm from the
femoral notch. Before this point is reached distally, it is recommended to change the 4 mm
shaver burr to a smaller 3 mm burr, thereby
minimizing the bone resection in the area close to
the hinge of the cartilage flap. The release should
be continued in the medial and lateral directions,
otherwise the hinge of the flap will not become
sufficiently elastic such to be able to fit into the
new trochlea.
506
L. Blønd
Fig. 1 This demostrates outside and inside view of the superior suprapatellar portal with the arthroscope introduced
and the lateral superopatellar portal with a PassPort canula mounted
3.3 Formation and Shaping
of a Deeper Trochlear
Groove
The aim is to achieve a 4.5 mm trochlear depth
and a more lateral sulcus orientation of the new
groove. Therefore, the groove needs to be
deepened and centralized using shaver burrs.
A PowerRasp (Arthrex Inc., Naples FL) can be
useful for smoothening the bony surface of the
lateral wall of the trochlea. Part of the trochlear
dysplasia is the medialized groove, so the
amount of lateralization of the new groove
should reflect the increased TT-TG measured
preoperatively. Part of TD is the so-called
crossing sign, meaning that the groove entrance
is localized anteriorly to the femoral shaft.
Therefor is amount of bone resection for the
deepening of the trochlea estimated during surgery by looking at the most anterior part of the
femur, since the resection proximally should
allow for a smooth transition between groove and
anterior cortex of the femur. The new groove is
trimmed with the shaver burr and/or PowerRasp
according to the preoperative plan and a good
lateral wall is aimed (Fig. 4). The cartilage flap
needs to have sufficient elasticity to integrate into
the new groove, to get in contact with the
underlying bone and to achieve the correct trochlea shape. The flap elasticity is tested, by
pressing the flap into the new deepened trochlea
using a blunt instrument (Fig. 5). In cases where
Arthroscopic Deepening Trochleoplasty
507
Fig. 2 This demonstrate the initial release of the cartilage flap using a shaver burr
the cartilage flap is too stiff, excessive bone on
the rear side of the flap should be gently and
gradually removed until the needed elasticity is
reached.
3.4 Fixation of the Cartilage Flap
With the arthroscope remaining in the superior
medial portal, the fixation of the cartilage flap is
started by placing a biocomposite 3.5 mm
PushLock anchor (Arthrex Inc., Naples FL) with
the eyelet loaded with a resorbable tape and a
suture, so the end of the tape and sutures are
equal in length (one tape—Vicryl 3 mm BP-1,
V152G, Ethicon and one 1–0 suture Vicryl CT-2
plus, V335 H) or since the tape is about to being
pulled out of production, alternatively multiple
1–0 suture Vicryl CT-2 plus, V335 H can be
used. The anchor is placed distal to the cartilage
hinge, just proximal to the notch, through the
medial joint line portal. In order to achieve a 90
degree insertion angle of the anchor, the knee has
to be flexed close to 45 degrees. A bone socket
508
L. Blønd
Fig. 3 This demonstrate outside and inside use of the osteotome to guide the direction of the osteotomy and to reduce
the bone loss most laterally
for the anchor is initially drilled central in the
most distal part of the trochlea, just proximal to
the notch and still distally from the cartilage
flap. After having introduced the anchor into the
socket, one of the tape endings are grasped and
brought out through the canula and loaded into
another similar anchor. On the lateral side, based
upon the hardness of the bone, the socket can be
prepared using either a taping device or a burr,
placed in a spot superior to the cartilage flap and
lateral to the center of the groove. The tape is
gradually tensioned thereby pressing the cartilage
flap into the new groove, and the anchor is
inserted into its position. With the anchor positioned, the tape is locked, and the excess is cut.
Next the arthroscope is introduced through the
superior lateral canula. The superior medial
portal is in a similar way used for insertion of the
next anchor. This should also be placed superior
to cartilage flap and medial to the center of the
groove. The cartilage flap is now sufficiently
stabilized into the new trochlea groove (Fig. 6).
In about 50% of the cases a gap between the
cartilage flap and the new trochlea and this
requires an additional anchor now loaded with
the vicryl (Fig. 7). Obviously, co-morbities are
treated as indicated, such as medial patellofemoral ligament insufficiency with MPFL reconstruction, distalizations of the tibial tubercle in
cases of patella alta, de-rotational osteotomies in
cases of torsional abnormalites, varising osteotomies etc.
From a biomechanical point it should be
stressed that when a MPFL reconstruction is
done in conjunction to an ADT, following issues
have to be taken into consideration. The axis of
rotation around the femoral epicondylar axis, as
described by Coughlin et al. [37], is affected due
to the bone resection caused by the ADT. The
distance (radius) from the center of rotation (the
foot print in the epicondyle) to the resection area
in the new groove is shortened. Consequently,
both the native MPFL and the MPFL graft are
relatively slack in extension. If this is not
Arthroscopic Deepening Trochleoplasty
509
Fig. 4 This demonstrate how the PowerRasp can help creating a smooth lateral wall of the new trochlea
accommodated this can have a detrimental
impact on the outcome. The MPFL insertion
point are more optimally placed in a little further
distal anisometrical position and should be fixed
with the knee in the specific degree of flexion
(approx 70 degrees), where the patella is placed
in the unaffected trochlea area, otherwise the
graft will become too tight in flexion and consequently leads to flexion problems resulting in
over tensioning of the graft and compression of
the PF articular cartilage.
4
Video
Latest video demonstrating ADT can be found
here: https://youtu.be/94BEtkhGS3o.
4.1 Postoperative Regime
Immediately after the surgery the patients are
allowed to do full range of movements and full
510
L. Blønd
Fig. 5 This demonstrate how the elasticity of cartilage flap can be tested using stump instrument
weight bearing. This regime has been practiced
for the past 8 years without related complications.
Postoperative rehabilitation is detailed in
Table 1.
5
Results
The author has conducted the ADT procedure in
more than 150 knees with a median age of 20
(range 12–51). The formalized registration has
ended due to GPDR issues. In seven cases were
the indication severe chronic patellofemoral pain
and no MPFL reconstruction was done. The
surgery has in all cases been one-day surgeries.
The results from the first 29 cases of ADT in
combination with MPFL reconstruction have
been published [28], in which significant
improvements in Kujala and KOOS scores were
observed with 93% satisfied with the outcome
and 55% returning to sports. In all cases the
preoperative range of movements or more have
been achieved. A later smaller case series with
similar results have been published as an abstract
[38].
6
Complications
Two complications (DVT) have occurred. Eight
patients have had further surgery. Three patients
who had high TT-TG distances above 20 mm
developed symptomatic subluxations postoperatively and were subsequently successfully
Arthroscopic Deepening Trochleoplasty
511
Fig. 6 This demonstrates how the cartilage flap in pressed into the new trochlear groove by the tape fixation
corrected by medialization of the tibial tubercle.
Those cases were all operated in the start of the
series and at that phase and due to lack of
knowledge, the new trochlear groove was not
lateralized during the trochleoplasty procedure.
Three patients also from the start of the series
experienced pronounced postoperative anterior
knee pain in flexion. On examination, tightness
of the lateral retinaculum was found, indicating
lateral hyper-pressure syndrome, and they all
responded positively to a subsequent lateral
release. This have resulted in a more liberal use
of a subsequent lateral release. Since there have
been no further cases developing symptoms of
hyperpressure. One patient who already have had
five operations, developed severe anterior knee
pain due to degeneration of cartilage in the lateral
part of the trochlear. At further examination
increased femoral anteversion was recognized.
The patients had undergone external rotational
distal femoral osteotomy and tibial internal
osteotomy elsewhere. This procedure worsened
the situation. Case number seven has redislocated (by report) due to overlooked excessive femoral anteversion.
7
Discussion
For the past fourteen years period the author has
performed the ADT in more than 150 knees, with
no cases of arthrofibrosis or infections, however
512
L. Blønd
Fig. 7 This demonstrates a cases with the use of the extra vicryl sutures in order to provide extra fixation compared to
Fig. 6
complication as mentioned above have occurred.
Since the original paper was published in 2010,
the procedure has undergone minor changes in
addition to above mentioned. The superior lateral
canula have been omitted, since it wasn’t necessary and the PowerRasp 4.0 mm 13 cm AR8400PR (Arthrex Inc., Naples FL) was successfully introduced in 2016 and this has helped
smoothening the lateral wall of the new trochlear
groove. The fixation method for the cartilage flap,
with the use of absorbable tapes in combination
with suture anchors, was adopted for the open
trochleoplasty several years ago. The ADT has
until now only been combined with osteotomy in
a single case, where the a distalisation of the tibial
tubercle was done due to significantly reduced
patellotrochlea overlap [39]. In the primary study,
a median VAS pain score of 3 was observed 24 h
postoperatively, and this equalized the level of
pain scores from MPFL reconstructions alone.
Based on these findings and later observations,
we have experienced that the combined ADT and
MPFL procedure unproblematic and can be carried out as one-day surgery. In a follow-up study
of a consecutive series of 29 knees in patients
troubled by patella instability and treated by
combined ADT and MPFL reconstruction, significantly improved median knee scores for all
measured parameters with no re-dislocations
were found [28]. These results have later been
confirmed in a second follow-up study including
18 more knees [38]. Based on the theory that the
trochleoplasty doesn’t provide sufficient stability
to the patella in the initial 20 degrees of flexion,
concomitant MPFL reconstructions are more
frequently a concomitant procedure with
trochleoplasty as is evident in four recent series of
trochleoplasty procedures [21, 40–43].
A significant relationship between trochlea
cartilage lesions and trochlea dysplasia has been
documented [5, 44, 45]. Neumann et al.
observed, in a 50-month follow-up of 46 patients
after trochleoplasty, that in a subgroup of 26
patients with radiographic degenerative changes
or intraoperative findings of chondromalacia, that
there were comparable subjective post-operative
improvements in this group, compared to the
patients without chondral changes [46]. Those
findings have encouraged the author to include
patients for ADT with more degenerative cartilage changes in the trochlea and the results have
been positive.
Arthroscopic Deepening Trochleoplasty
513
Table 1 The physiotherapy guided rehabilitation program after arthroscopic deepening trochleoplasty
Day
Goal
Exercise
0–1
Range of motion
(ROM): CPM
machine
Ankel pumps
Physical Therapy
RICE: Rest,
Compression, Ice
2–3 day:
30 min. Elevation
2–3
ROM, Focus
Extension
Heel slides, ankle pumps, seated heel
slides
PROM, retrograde massage, Pain
control
Strength
Isometric quadriceps, VMO
Maybe NMES (neuromuscular
stimulation 30–40 Hz)
Gait
FWB (full weight bearing) with 2
crutches
Gait training; heel-toe.
AlterG Anti‐Gravity: 40–50% WB,
0.5–1 km/hr, 4–5 incline. 5–10 min
RICE: Rest,
Compression, Ice
2–3 day:
30 min. Elevation
4–7
Electrotherapy
Vascularization 8 Hz and pain relief
(Endorfin 5 Hz, or TENS)
Laser
Level IV laser for pain and swelling
ROM: Focus
Extension
Heel slides, ankle pumps, seated heel
slides
PROM
Strength
Isometric quad sets, Assisted straight
leg raises: FLX, ABD, EXT, Terminal
knee extension (TKE), Bridge
NMES (neuromuscular stimulation
30–40 Hz)
Stretching
Hamstring supine with strap
Quad: prone with strap
Calf: standing on step, push heel
down
Gait
Weight bearing exercises
Stationary bike
High seat, slowly back and forth for
ROM, do not force the knee around
Manual therapy
Prioprioception
Gait traingn using two crutches
AlterG Anti‐Gravity: 50% WB,
1–2 km/hr, 2–3 incline. 10–15 min
Retrograde massage, Scar massage
with vitamin-e, Patella mobes
Superior-inferior. No Medial‐lateral
with MPFL reconstruction for 4 wks
Standing on 1 leg on even surface, if
able to stand without knee extension
dysfunction then close eyes
Electrotherapy
Vascularization 8 Hz and pain relief
(Endorfin 5 Hz, or TENS)
Laser
Level IV laser for pain and swelling
(continued)
514
L. Blønd
Table 1 (continued)
Day
Goal
Exercise
Physical Therapy
1–4 wks
ROM: Focus
Extension
Heel slides, ankle pumps, seated heel
slides, prone FLX-EXT with strap
If problems with getting full knee
extension, try low load long duration
stretch prone with rubber band
5–10 min daily
PROM
Strength
Isometric quad sets, Assisted straight
leg raises: FLX, ABD, EXT, Terminal
knee extension (TKE), Bridge, mini
squat, Heel glides on cloth supine
NMES (neuromuscular stimulation
35–40 Hz)
AlterG Anti-Gravity: 50% WB, 0
km/hr, 0 incline: bilateral heel lifts
(progres to eccentric and unilateral),
mini squat, single leg stance
Stretching
Hamstring supine with strap
Quad: prone with strap
Calf: standing on step, push heel
down
Manualstretching
Gait
Heel-Toe with 1–2 crutches
Gait training using 1–2 crutches
AlterG Anti-Gravity: 50% WB,
2–3 km/hr, 2 incline. 15–20 min
Stationary bike
High seat, slowly back and forth for
ROM, try to cycle around back and
forth with resistance: 10–15 min
Manualtherapy
Prioprioception
Retrograde massage, Scar massage
with vitamin-e, Patella mobes
Superior-inferior
No Medial-lateral with MPFL
reconstuction for 4 wks
Knee mobilisering: tibia A–P mobes,
general mobes for FLX/EXT gr I–II
Standing on 1 leg on even surface, if
able to stand without knee extension
dysfunction then close eyes
Electrotherapy
Vascularization 8 Hz and pain relief
(Endorfin 5 Hz, or TENS)
Laser
Level IV laser for pain and swelling
(continued)
Arthroscopic Deepening Trochleoplasty
515
Table 1 (continued)
Day
Goal
Exercise
Physical Therapy
4–6 wks
ROM: Full
Extension.
Fleksion 90–120
Heel slides, seated heel slides, prone
heel to buttocks with strap
PROM
Strength
Isometric quad sets, straight leg raises
(SLR): FLX, ABD, EXT, Terminal
knee extension (TKE), Bridge, mini
squat, Heel glides on cloth supine
NMES (neuromuscular stimulation
50–70 Hz)
AlterG Anti-Gravity: 50–80% WB,
0 km/hr, 0 incline: bilateral heel lifts
(progres to eccentric and unilateral),
mini squat, single leg stance
Stretching
Hamstring supine with strap
Quad: prone with strap
Calf: standing on step, push heel
down
Manual stretching
Gait
Gait training without crutches
Gait training without crutches: heeltoe
AlterG Anti-Gravity: 50%–80% WB,
2–4 km/hr, 2–3 incline. 15–20 min
Stationary bike
High seat, slowly back and forth for
ROM, do not force the knee around
Manual therapy
Retrograde massage, Scar massage
with vitamin-e, Patella mobes
Superior-inferior
No Medial-lateral with MPFL
reconstuction for 4 wks
Prioprioception
Standing on 1 leg on even surface, if
able to stand without knee extension
dysfunction then close eyes
Electrotherapy
Vascularization 8Hz and pain relief
(Endorfin 5Hz or TENS)
Laser
Single leg stance in trampoline, ball
catch
Level IV laser for pain and swelling
(continued)
516
L. Blønd
Table 1 (continued)
Day
Goal
Exercise
Physical Therapy
6–? Wks
Progression
as tolerated
ROM: Full
Extension.
Fleksion 135–140
Heel slides, seated heel slides, prone
heel to buttocks with strap
PROM
Strength
Isometric quad sets, SLR: FLX, ABD,
EXT (should be able to hold knee in
full extension, otherwise cont. Ass),
SLR with rubberband, Terminal knee
extension (TKE), Bridge with leg
lifts, wall squat, Heel glides on cloth
supine
Progression: standing slides on cloth,
side step without and with
rubberband, lunges, squats.
Machines: Leg press, squat in smith
rack, leg curls
Free weights when full AROM and
able to hold knee in full extension
with SLR
NMES (neuromuscular stimulation
50–70 Hz)
AlterG Anti-Gravity: 50–80% WB,
0 km/hr, 0 incline: bilateral heel lifts
(progress to eccentric and unilateral),
mini squat, single legstance
Stretching
Hamstring supine with strap
Quad: prone with strap
Calf: standing on step, push heel
down
Manual stretching
Gait
Gait training without crutches
Gait training without crutches: heeltoe
AlterG Anti-Gravity: 50%–80% WB,
2–4 km/hr, 2–3 incline. 15–20 min
Stationary bike
Normal cycling on stationary bike,
able to bike outside about 3 months
after surgery if full AROM and
Isometric strength normal compare to
opposite leg
Manual therapy
Prioprioception
8
Retrograde massage, Scar massage
with vitamin-e, Patella mobes
Superior–inferior. Medial-lateral gr
I–II Knee mobilisering: tibia A–P
mobes, general mobes for FLX/EXT
gr I–II
Standing on 1 leg on even surface, if
able to stand without knee extension
dysfunction then close eyes
Single leg stance in trampoline, ball
catch. Mini jog on trampoline
Electrotherapy
Vascularization 8 Hz and pain relief
(Endorfin 5 Hz, or TENS)
Laser
Level IV laser for pain and swelling
Conclusion
This is a description of the ADT, a technique that
has been slightly optimized since the original
paper. The technique has been found to be a
reproducible and a safe technique with limited
serious complications. Based upon personal
communications other centers have implemented
the technique achieving similar results. Clinically
the AT has been found to give significant
improvements in postoperative Kujala and
Arthroscopic Deepening Trochleoplasty
KOOS scores, and to provide stable patellae,
reduction of chronic anterior knee pain and with
no reported cases of arthrofibrosis.
9
Take Home Message
1. The ADT is today a routine surgery in several
countries.
2. With by good preparation and some effort the
technique can be learned by experienced
arthroscopists.
3. Practice on cadavers.
4. Focus on keeping the portals waterproof to be
able to maintain water pressure to avoid
bleeding that reduce vision.
5. Expect it to be more time consuming initially
compared to open technique.
10
Key Message
Minimal invasive surgery helps patients, and this
procedure is just the start of things to come
regarding robotic surgery.
517
5.
6.
7.
8.
9.
10.
11.
References
1. Jr GIO, Yalcin S, Kaar SG, Pace JL, Ferrua P,
Farrow LD. The evaluation of trochlear osseous
morphology an epidemiologic study. Orthop J Sports
Med. 2021;9(4):1–7. https://doi.org/10.1177/23259
67121994548.
2. Tuna BK, Semiz-Oysu A, Pekar B, Bukte Y, Hayirlioglu A. The association of patellofemoral joint
morphology with chondromalacia patella: a quantitative MRI analysis. Clin Imaging. 2014;38(4):495–
8. https://doi.org/10.1016/j.clinimag.2014.01.012.
3. Duran S, Cavusoglu M, Kocadal O, Sakman B.
Association between trochlear morphology and
chondromalacia patella: an MRI study. Clin Imaging.
2017;41:7–10.
https://doi.org/10.1016/j.clinimag.
2016.09.008.
4. Keser S, Savranlar A, Bayar A, Ege A, Turhan E. Is
there a relationship between anterior knee pain and
femoral trochlear dysplasia? Assessment of lateral
trochlear inclination by magnetic resonance imaging.
Knee Surg Sports Traumatol Arthrosc. 2008;16
12.
13.
14.
15.
16.
(10):911–5.
https://doi.org/10.1007/s00167-0080571-5.
Stefanik JJ, Roemer FW, Zumwalt AC, et al. Association between measures of trochlear morphology and
structural features of patellofemoral joint osteoarthritis
on MRI: the MOST study. J Orthop Res. 2012;30(1):1–
8. https://doi.org/10.1002/jor.21486.
Kalichman L, Zhang Y, Niu J, et al. The association
between patellar alignment and patellofemoral joint
osteoarthritis features–an MRI study. Rheumatol
(Oxford). 2007;46(8):1303–8. https://doi.org/10.
1093/rheumatology/kem095.
Askenberger M, Janarv P-M, Finnbogason T,
Arendt EA. Morphology and anatomic patellar instability risk factors in first-time traumatic lateral patellar
dislocations. Am J Sports Med. 2017;45(1):50–8.
https://doi.org/10.1177/0363546516663498.
Lewallen LW, McIntosh AL, Dahm DL. Predictors
of recurrent instability after acute patellofemoral
dislocation in pediatric and adolescent patients. Am J
Sport Med. 2013;41(3):575–81. https://doi.org/10.
1177/0363546512472873.
Paiva M, Blønd L, Hölmich P, et al. Quality
assessment of radiological measurements of trochlear
dysplasia; a literature review. Knee Surgery Sport
Traumatol Arthrosc. 2018;26(3):746–55. https://doi.
org/10.1007/s00167-017-4520-z.
Cheng C, Hedgecock J, Solomito M, Joseph S,
Pace JL. Defining trochlear dysplasia via the lateral
trochlear inclination angle. Orthop J Sport Med.
2020;8(4_suppl3):2325967120S0017.
https://doi.
org/10.1177/2325967120s00179.
Pace JL, Cheng C, Joseph SM, Solomito MJ. Effect
of trochlear dysplasia on commonly used radiographic parameters to assess patellar instability.
Orthop J Sport Med. 2020;8(7):1–8. https://doi.org/
10.1177/2325967120938760.
Joseph SM, Cheng C, Solomito MJ, Pace JL. Lateral
trochlear inclination angle: measurement via a 2-Image
technique to reliably characterize and quantify trochlear
dysplasia. Orthop J Sport Med. 2020;8(10):1–9. https://
doi.org/10.1177/2325967120958415.
Escala JS. Objective patellar instability: MR-based
quantitative assessment of potentially associated
anatomical features. Published online 2006:264–72.
https://doi.org/10.1007/s00167-005-0668-z.
Pfirrmann CW, Zanetti M, Romero J, Hodler J.
Femoral trochlear dysplasia: MR findings. Radiology. 2000;216(3):858–64. http://www.ncbi.nlm.nih.
gov/pubmed/10966723.
Biedert RM, Bachmann M. Anterior-posterior trochlear
measurements of normal and dysplastic trochlea by
axial magnetic resonance imaging. Knee Surgery Sport
Traumatol Arthrosc. 2009;17(10):1225–30. https://doi.
org/10.1007/s00167-009-0824-y.
Van Haver A, De Roo K, De Beule M, et al. The effect
of trochlear dysplasia on patellofemoral biomechanics: a cadaveric study with simulated trochlear
518
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
L. Blønd
deformities. Am J Sport Med. 2015;43(6):1354–61.
https://doi.org/10.1177/0363546515572143.
Ferlic PW, Runer A, Seeber C, Thöni M, Spicher A,
Liebensteiner MC. Linear anterior-posterior computed
tomography parameters used to quantify trochlear
dysplasia are more reliable than angular measurements.
Arthrosc J Arthrosc Relat Surg. 2021;37(4):1204–11.
https://doi.org/10.1016/j.arthro.2020.11.032.
van Sambeeck JDP, van de Groes SAW, Verdonschot N, Hannink G. Trochleoplasty procedures
show complication rates similar to other patellarstabilizing procedures. Knee Surgery Sport Traumatol Arthrosc. 2018;26(9):2841–57. https://doi.org/10.
1007/s00167-017-4766-5.
Goutallier D, Raou D, Van Driessche S. [Retrotrochlear wedge reduction trochleoplasty for the
treatment of painful patella syndrome with protruding trochleae. Technical note and early results]. Rev
Chir Orthop Reparatrice Appar Mot. 2002;88
(7):678–85. Accessed 1 Dec 2013. http://www.ncbi.
nlm.nih.gov/pubmed/12457113.
Zimmermann F, Milinkovic DD, Balcarek P. Outcomes after deepening trochleoplasty and concomitant realignment in patients with severe trochlear
dysplasia with chronic patellofemoral pain results at
2-year follow-up. Orthop J Sports Med. Published
online 2021:1–8. https://doi.org/10.1177/232596712
11010404.
Blønd L. Arthroscopic deepening trochleoplasty for
chronic anterior knee pain after previous failed
conservative and arthroscopic treatment. Report of
two cases. Int J Surg Case Rep. 2017;40:63–8.
https://doi.org/10.1016/j.ijscr.2017.09.006.
Amis AA, Oguz C, Bull AMJ, Senavongse W,
Dejour D. The effect of trochleoplasty on patellar
stability and kinematics: a biomechanical study
in vitro. J Bone Joint Surg Br. 2008;90(7):864–9.
https://doi.org/10.1302/0301-620X.90B7.20447.
Elias JJ, Cyrus Rezvanifar S, Koh JL. Groove‐
deepening trochleoplasty reduces lateral patellar
maltracking and increases patellofemoral contact
pressures: dynamic simulation. J Orthop Res. Published online 2021:330–44. https://doi.org/10.1002/
jor.25181.
Hiemstra LA, Peterson D, Youssef M, Soliman J,
Banfield L, Ayeni OR. Trochleoplasty provides good
clinical outcomes and an acceptable complication
profile in both short and long-term follow-up. Knee
Surgery Sport Traumatol Arthrosc. 2019;27(9):2967–
83. https://doi.org/10.1007/s00167-018-5311-x.
Longo UG, Vincenzo C, Mannering N, et al.
Trochleoplasty techniques provide good clinical
results in patients with trochlear dysplasia. Knee
Surgery Sport Traumatol Arthrosc. 2018;26(9):2640–
58. https://doi.org/10.1007/s00167-017-4584-9.
Wind RJP, Heesterbeek PJC, Wymenga AB. A combined procedure with Bereiter-type trochleoplasty
leads to a stable patellofemoral joint at 5-year follow-
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
up. Knee Surgery Sport Traumatol Arthrosc. 2018;27
(3):1–8. https://doi.org/10.1007/s00167-018-5014-3.
Leclerc J-T, Dartus J, Labreuche J, et al. Complications and outcomes of trochleoplasty for patellofemoral instability: a systematic review and metaanalysis of 1000 trochleoplasties. Orthop Traumatol
Surg Res. 2021;107(7):103035. https://doi.org/10.
1016/j.otsr.2021.103035.
Blønd L, Haugegaard M. Combined arthroscopic
deepening trochleoplasty and reconstruction of the
medial patellofemoral ligament for patients with
recurrent patella dislocation and trochlear dysplasia.
Knee Surg Sports Traumatol Arthrosc. 2014;22
(10):2484–90. https://doi.org/10.1007/s00167-0132422-2.
Blønd L. Arthroscopic deepening trochleoplasty: the
technique. Oper Tech Sports Med. 2015;23(2):136–
42. https://doi.org/10.1053/j.otsm.2015.02.011.
Blønd L, Schöttle PB. The arthroscopic deepening
trochleoplasty. Knee Surg Sports Traumatol
Arthrosc. 2010;18(4):480–5. https://doi.org/10.1007/
s00167-009-0935-5.
Bereiter H, Gautier E. Die Trochleaplastik als
Chirurgische Therapie der Reziderenden Patellaluxation
bei
Trochleadysplasie.
Arthroskopie.
1994;7:281–6.
Song G-Y, Hong L, Zhang H, et al. Trochleoplasty
versus nontrochleoplasty procedures in treating
patellar instability caused by severe trochlear dysplasia. Arthroscopy. 2014;30(4):523–32. https://doi.
org/10.1016/j.arthro.2014.01.011.
Balcarek P, Rehn S, Howells NR, et al. Results of
medial patellofemoral ligament reconstruction compared with trochleoplasty plus individual extensor
apparatus balancing in patellar instability caused by
severe trochlear dysplasia: a systematic review and
meta-analysis. Knee Surg Sports Traumatol Arthrosc.
2017;25:3869–77. https://doi.org/10.1007/s00167016-4365-x.
Ridley TJ,1 Hinckel BB,2 Kruckeberg BM,3 Agel
J1, Arendt E A1. Anatomical patella instability risk
factors on MRI show sensitivity without specificity in
patients with patellofemoral instability: a systematic
review. J ISAKOS. 2016;1(3):141–52. https://doi.
org/10.1136/jisakos-2015-000015.
Fucentese SF, Schottle PB, Pfirrmann CW,
Romero J. CT changes after trochleoplasty for
symptomatic trochlear dysplasia. Knee Surg Sports
Traumatol Arthrosc. 2007;15(2):168–74.
Zimmermann F, Liebensteiner MC, Balcarek P. The
reversed dynamic patellar apprehension test mimics
anatomical complexity in lateral patellar instability.
Knee Surgery Sport Traumatol Arthrosc. 2019;27
(2):604–10.
https://doi.org/10.1007/s00167-0185198-6.
Coughlin KM, Incavo SJ, Churchill DL, Beynnon BD. Tibial axis and patellar position relative to
the femoral epicondylar axis during squatting.
Arthroscopic Deepening Trochleoplasty
38.
39.
40.
41.
42.
2003;18(8):1048–55. https://doi.org/10.1016/S08835403(03)00449-2.
Blønd L. Arthroscopic trochleoplasty belongs to the
future. In: The 1st Annual World Congress of
Orthopaedics, Xian, China; 2014:s 131.
Munch JL, Sullivan JP, Nguyen JT, et al. Patellar
articular overlap on MRI is a simple alternative to
conventional measurements of patellar height.
Orthop J Sport Med. 2016;4(7):1–6. https://doi.org/
10.1177/2325967116656328.
Von Engelhardt L, Weskamp P, Lahner M, Spahn G,
Jerosch J. Deepening trochleoplasty combined with
balanced medial patellofemoral ligament reconstruction for an adequate graft tensioning. World J
Orthop. 2017;8(2):935–45.
Nelitz M, Dreyhaupt J, Lippacher S. Combined
trochleoplasty and medial patellofemoral ligament
reconstruction for recurrent patellar dislocations in
severe trochlear dysplasia: a minimum 2-year followup study. Am J Sport Med. 2013;41(5):1005–12.
https://doi.org/10.1177/0363546513478579.
Ntagiopoulos PG, Byn P, Dejour D. Midterm results
of comprehensive surgical reconstruction including
sulcus-deepening trochleoplasty in recurrent patellar
dislocations with high-grade trochlear dysplasia.
519
43.
44.
45.
46.
Am J Sport Med. 2013;41(5):998–1004. https://doi.
org/10.1177/0363546513482302.
Banke IJ, Kohn LM, Meidinger G, et al. Combined
trochleoplasty and MPFL reconstruction for treatment of chronic patellofemoral instability: a prospective minimum 2-year follow-up study. Knee Surg
Sports Traumatol Arthrosc. 2014;22(11):2591–8.
https://doi.org/10.1007/s00167-013-2603-z.
Mehl J, Feucht MJ, Bode G, Dovi-Akue D, Südkamp
NP, Niemeyer P. Association between patellar cartilage defects and patellofemoral geometry: a
matched-pair MRI comparison of patients with and
without isolated patellar cartilage defects. Knee Surg
Sports Traumatol Arthrosc. 2016;24(3):838–46.
https://doi.org/10.1007/s00167-014-3385-7.
Teichtahl AJ, Hanna F, Wluka AE, et al. A flatter
proximal trochlear groove is associated with patella
cartilage loss. Med Sci Sports Exerc. 2012;44
(3):496–500.
https://doi.org/10.1249/MSS.
0b013e31822fb9a6.
Neumann MV, Stalder M, Schuster AJ. Reconstructive surgery for patellofemoral joint incongruency.
Knee Surg Sports Traumatol Arthrosc. Published
online October 31, 2014. https://doi.org/10.1007/
s00167-014-3397-3.
Lengthening Trochleoplasty
Roland M. Biedert
1
Introduction
To understand the indications for a lengthening
trochleoplasty it requires knowledge of the
pathoanatomy of a too short proximal lateral
trochlea as a specific form of trochlear dysplasia
[1–4].
Our insight for the shape and kinematics of a
too short lateral trochlea as well as the main
indication to perform a lengthening trochleoplasty have evolved continuously during the last
20 years. The Albee procedure initiated our
attention to the importance of the proximal lateral
part of the trochlea [5]. Our key finding was that
not only the height of the lateral condyle but, in
particular, also the length of the lateral trochlea is
most important for lateral patellar stability.
Albee was the first to attribute an important
role to the lateral condyle and trochlea in patellar
stability [5]. He described the external condyle to
be on the horizontal plane much below that of the
internal condyle. He believed that the external
condyle is not only flat, but also relatively further
back than normal, mentioning also the importance of the rotation of the lower end of the
femur. Since the soft tissue procedures have been
R. M. Biedert (&)
Orthopaedic Surgery and Sports Traumatology,
Sportsclinic#1, Wankdorf Center,
Papiermühlestrasse 73, CH-3014 Bern, Switzerland
e-mail: r.biedert@bluewin.ch
far less successful in securing the patella, Albee
lifted the external femoral condyle with a wedge
bone graft to block the recurrence of patellar
dislocation. With this, the first reconstruction on
the lateral trochlear facet to improve patellar
stability was performed [5]. The procedure had
the desired effect on stability, but the additional
bony prominence caused problems by overtightening the lateral retinacular structures or by
increased pressure across the lateral facet of the
patellofemoral articulation with the potential to
generate pain or osteoarthritis. Over time, this
procedure fell out of favour. In addition, rising of
the lateral edge of the trochlea did not correct an
abnormal length of the lateral trochlea.
Later, Brattström also emphasized the importance of the lateral facet of the trochlea as
resisting lateral force against patellar instability
[6]. He described a low lateral condyle and
increased sulcus angle in patients with habitual
patellar dislocation [6, 7]. Various biomechanical
studies confirmed these descriptions [8–10].
The shape of the femoral trochlea and its
relationship to the patella dictate the patellofemoral kinematics [2, 11]. The normal articular
surface of the trochlea consists of the lateral and
medial facets of the femoral sulcus and is defined
by different criteria in the proximal–distal,
medio-lateral, and antero-posterior direction [12].
The normal trochlea is concave and deepens
from proximal to distal. It is longest laterally and
shortest on the medial side in the proximal–distal
direction (Fig. 1) [2, 12–14]. The deepened
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_36
521
522
Fig. 1 Normal articular morphology and supero-lateral
length of the trochlea (anterior view, left knee)
trochlear groove separates the lateral facet from
the medial part. In the antero-posterior measurements, the most anterior aspect of the lateral
condyle is normally higher than the medial
condyle and the deepest point is represented by
the center of the trochlear groove [15]. The large
lateral facet in extension is the feature that must
“capture” the patella when the knee starts to flex,
to ensure that it is guided into the trochlear
groove, and to achieve patellofemoral stability
[8, 9]. Normally, the contact between the articular surface of the trochlea and the articular
cartilage behind the patella is about one third of
the length of the patellar cartilage in extension [1,
2, 13]. In this normal situation, quadriceps
muscle contraction pulls the patella proximally,
but without lateral subluxation. The patella is still
guided by the most proximal articular lateral
trochlea.
Trochlear dysplasia is defined as variable
abnormality of shape and depth of the trochlear
groove and alters the patellofemoral congruency
[14, 16]. It represents an important pathologic
articular morphology and a strong risk factor for
permanent patellar instability [3, 14, 17, 18].
R. M. Biedert
Different forms of trochlear dysplasia are
described, such as decreased depth of the groove,
decreased inclination of the lateral facet, flat
trochlea, trochlear bump (anterior translation of
the trochlear floor), and hypoplasia of the medial
trochlea [5, 14, 16, 18–20]. Most forms of trochlear variations are located at its proximal
extent and cause decreased bony stability in the
trochlear groove. As a result, the patella is poorly
guided osseously at the entrance into the trochlea
in early knee flexion and lateral instability may
occur.
Various classifications for evaluating trochlear
dysplasia are described using radiographs or
computed tomography images, the best known
with the four-grade classification by Dejour [14].
However, these classifications describe the forms
of dysplasia only in the axial and sagittal planes,
the coronal view is not considered [1–3, 14]. As
the shape of the articular trochlea can also be
dysplastic in the coronal plane, we paid increased
attention to the too short proximal-lateral extension of the trochlea causing dynamic proximallateral patellar instability during the last two
decades [1–4] (Fig. 2).
Decades later, the concept of deepening the
dysplastic trochlea was published and first carried out by Masse in 1978 [21]. This technique
has been continuously modified and standardized
by H. Dejour and Bereiter to eliminate possible
complications [14, 19]. Today, deepening
trochleoplasty is a widely used complex surgical
treatment to improve patellar stability with precise indications, but also with late effects and
complications [20, 22]. Deepening of the trochlea mainly improves the guidance of the
patella from the point of entry into the new sulcus distally, but towards proximally it has no
influence. Neither shape nor length of the proximal lateral articular trochlea are changed with
this procedure.
Our findings and observations of a dynamic
proximal-lateral patellar instability could not be
explained by the concept with the four types of
trochlear dysplasia. The inclusion of the coronal
plane was missing. Therefore, the first goal was
to define a reliable method to assess the proximal
lateral cartilagineous extension of the lateral
Lengthening Trochleoplasty
523
facet. This discrepancy between a well-centered
patella under relaxed conditions and the dynamic
supero-lateral instability caused by quadriceps
muscle contraction confirms the proximal lateral
patellar instability.
This type of patellar instability may also be
depicted by manual examination in complete
extension of the knee. Manual pressure from
medial to lateral would cause subluxation, discomfort and often pain to the patient. With
increasing knee flexion, the patella shifts medially entering into the more distal and normal part
of the trochlear groove and becomes therefore
stable. Stability and gliding tests to medial are
normal.
It must be considered, that other pathologic
factors, such as patella alta, hyperlaxity, rotational abnormalities, excessively tight lateral
retinaculum, and increased TT-TG distance may
be present at the same time and influence the
physical examination.
Fig. 2 Too short lateral articular trochlea (proximal end
marked by arrow) in relation to the medial facet and the
normal trochlear sulcus (lateral view, left knee)
trochlea. With the application of the new lateral
condyle index (LCI) using sagittal MR images it
became possible to measure the proximal length
of the lateral trochlea and to document this type
of trochlea dysplasia [2]. With this, the importance of the shape and length of the proximal
lateral trochlea was confirmed [1, 2].
2
Physical Examination
The most important and specific finding during
physical examination is the dynamic superolateral patellar instability [1, 4, 13]. Under
relaxed conditions, the patella is well centered in
the trochlear groove (Fig. 3A). Muscular contraction of the extensor mechanism leads to
proximalization and lateralisation of the patella
resulting in dynamic supero-lateral subluxation
(Fig. 3B). The lateral subluxation of the patella is
caused by the absence of the osteochondral
opposing restraint of the short lateral trochlear
3
Imaging
3.1 Radiographs
Patients with a too short lateral facet of the trochlea have mostly normal radiographs. Specific
radiographic features of trochlear dysplasia in the
true lateral view, such as the crossing sign,
supratrochlear spur, double contour, or lateral
trochlear sign are missing or only present in
combination with other trochlear abnormalities.
In addition, the different radiographic indices to
assess patellar height are normal.
3.2 MR Measurements
MR images represent the best modality to assess
the proximal part of the trochlea [1, 2, 13, 23,
24]. According to this, the LCI is the preferred
diagnostic MR measurement tool with good
reliability in patients with suspected too short
lateral facet [2]. MR measurements are performed with the knees placed in a standard knee
524
(A)
R. M. Biedert
(B)
Fig. 3 A Well-centred patella under relaxed conditions. B Dynamic supero-lateral patellar subluxation (arrow) caused
by muscle contraction
coil in extension, the foot in 15° external rotation, and the quadriceps muscle consciously
relaxed [1, 2, 4].
All measurements are performed on sagittal
images. Firstly, on sagittal images showing the
anterior cruciate ligament, the longitudinal axis
(Ca) of the femoral shaft is defined by drawing a
proximal and a distal circle (C1 and C2, respectively) (Fig. 4A). Secondly, the most lateral
sagittal image on which the articular cartilage of
the lateral condyle still can be seen is selected.
The measurements include different parameters
(Fig. 4B) [1, 2, 4]. The length of the anterior
articular cartilage of the lateral trochlea (a) is
calculated using as a reference to the length of the
posterior articular cartilage of the lateral condyle
(p). For each individual subject p is always considered to be 100%. The variable length of a is
calculated in percentages with regard to p. The
LCI compares the length a with the length p and
is expressed in percentages [1, 2, 4].
The mean value of the LCI in a normal population without any patellofemoral complaints is
93% [1, 2, 4]. Therefore, an anterior length of the
lateral articular facet of the trochlea with index
values of 93% or more, compared with the length
of the posterior articular cartilage, is considered
normal. LCI values of less than 93% are considered pathologic, and values of 86% or less
confirm the presence of a too short lateral facet
(Fig. 5). LCI values between 86 and 93% need
additional assessment, such as patellotrochlear
index or radiographic patellar height measurements, to document or exclude patella alta [13].
Combinations of a short proximal-lateral trochlea
and patella alta are possible (Fig. 6A and B).
4
Differential Diagnosis
The dynamic supero-lateral patellar instability
must be differentiated from other diagnoses.
4.1 Patella Alta
Specifically, differentiation from patella alta may
be difficult [25, 26]. The most important differences in patients with a too short lateral trochlea
are: normal patellar height, no patellar
Lengthening Trochleoplasty
525
(A)
C1 Proximal circle in the femoral shaft.
C2 Distal circle in the femoral shaft.
Ca Central axis
Fig. 4 A. MR measurements [2, 3, 16] (Reused with
permission from Springer. From: The lateral condyle
index: a new index for assessing the length of the lateral
articular trochlea as predisposing factor for patellar
instability. Int Orthop. 2011; 35(9):1327–31). B MR
measurements [2, 3, 16]. (Reused with permission from
Springer. From: Lengthening osteotomy with or without
elevation of the lateral facet. In: Dejour D, Zaffagnini S,
Arendt EA (Eds) Patellofemoral pain, instability, and
arthritis. Springer, 2020)
subluxation under relaxed conditions, and
immediately improved patellar stability at the
beginning of knee flexion. However, it must be
considered that both pathologies can occur in
combination.
4.3 Lateral Pull Sign
The lateral pull sign occurs due to soft tissue
abnormalities (atrophy medially, hypertrophy laterally) by missed osteochondral opposing force on
the lateral trochlear facet [29]. The LCI is normal.
4.2 J-Sign
4.4 Hyperlaxity
The J-sign describes an excessive lateral translation of the patella in terminal knee extension.
The patella disengages from the intertrochlear
groove caused by excessively tight lateral retinaculum [27, 28]. As most important difference,
this lateral translation occurs when the knee is
extended from 90° of flexion to full extension.
General hyperlaxity may also be a cause of lateral patellar instability. Applied load at full
extension may show increased lateral patellar
mobility. With hyperlaxity, the Beighton score
is =<4 out of 9. Passive hyperextension of the
knee of 10° or more is present [27, 30].
526
R. M. Biedert
(B)
d Baseline distal condyle (perpendicular to Ca)
1 Superior most aspect of the anterior cartilage of the lateral condyle
2 Superior most aspect of the posterior cartilage of the lateral condyle
a Length of the anterior articular cartilage of the lateral condyle (red line)
p Length of the posterior articular cartilage of the lateral condyle (blue line)
Fig. 4 (continued)
4.5 Apprehension Test
5
The patellar apprehension test is performed in
20° to 30° of knee flexion under relaxed conditions [3, 4, 27]. A positive test is when decreased
medial stability allows increased lateral glide. In
contrast, the test for patients with a too short
lateral trochlea are performed in extension and
the supero-lateral patellar instability is caused by
muscle contraction.
Surgery
5.1 Preoperative Planning
Surgery aims to correct the underlying pathologic morphology. Considering this, lengthening
trochleoplasty is indicated when a too short lateral trochlea is documented (clinically and with
MRI) and when the patients remain symptomatic
Lengthening Trochleoplasty
527
Dotted red line: length of the anterior articular cartilage of the lateral condyle
Dotted blue line: length of the posterior articular cartilage of the lateral condyle
Fig. 5 MR measurement with too short anterior articular cartilage of the lateral facet of the trochlea. The LCI is 77%
after conservative treatment. A clear indication
for lengthening trochleoplasty is given when the
LCI is 86% or less. Lenghtening trochleoplasty is
designed to create a longer proximal extension of
the lateral trochlear facet to improve the contact
within the patellofemoral joint, both relaxed and
under muscle contraction. A longer lateral trochlear facet is the feature that must “catch” the
patella in extension before the knee starts to flex,
to ensure that it is guided and shifted medially
into the more distal trochlear groove. Normally,
the overlapping between the articular surface of
the trochlea and the articular cartilage of the
patella is about one third of the length of the
patellar cartilage (measured using the patellotrochlear index) [13]. This value is helpful both
in planning (using MRI) and during surgery to
determine how much lengthening to proximal
should be performed.
5.2 Lengthening
Using a short parapatellar lateral incision of
about 5 cm length, the superficial retinaculum is
localized [1, 3, 4]. It is longitudinally incised
1 cm from the border of the patella and carefully
separated from the oblique part of the retinaculum in the posterior direction to allow lengthening of the lateral retinaculum at the end of
surgery if needed. After incision of the synovial
membrane, the patellofemoral joint is open. The
proximal shape and extension of the lateral facet
of the trochlea and the length of the articular
cartilage are assessed with regards to the length
of the sulcus and the medial facet of the trochlea.
The presence of a too short lateral articular facet
is reconfirmed (Fig. 7A). In this situation, the
patellotrochlear overlap is decreased (less than
one third). The existing overlap allows the
528
Fig. 6 MR measurements
with too short anterior
articular cartilage of the
lateral facet of the trochlea
A and patella alta B in the
same patient
R. M. Biedert
(A) LCI of 76%
(B) Patellotrochlear index: 15%, too long patellar tendon (>56mm),
Caton-Deschamps index: 1.3
calculation of lengthening of the lateral facet.
The overlap should be about one third at the end,
measured in extension (0° of flexion) [1, 2, 4,
13]. The incomplete lateral osteotomy is performed at least 5 mm from the cartilage of the
trochlea to avoid necrosis or breaking of the
lateral facet. The osteotomy starts at the end of
the cartilage and is continued approximately 1 to
1.5 cm to distal into the femoral condyle and to
proximal into the femoral shaft, always according to the calculated lengthening and planned
patellofemoral overlapping (Fig. 7B). The
osteotomy is opened carefully with the use of a
chisel. Small fractures of the distal cartilage may
occur and have no consequences; however sharp
edges must be smoothed. Elevation above the
maximum height of the lateral trochlea should be
avoided to prevent hypercompression. Cancellous bone (obtained through a small cortical
opening from the posterior aspect of lateral
femoral condyle) is inserted into the osteotomy
site and impacted (Fig. 7C). Additional fixation
is possible using resorbable sutures. To finish,
the synovial membrane is adapted and the lateral
retinaculum reconstructed in about 60° of knee
flexion to avoid overtensioning.
Lengthening Trochleoplasty
529
(A) Too short lateral articular facet of the trochlea (arrow) .
(B) Completed lengthening osteotomy with inserted cancellous bone
(C) Amount of lengthening (arrow: end of the original trochlea; dotted arrow: new end).
Increased patellofemoral overlap
Fig. 7 Lengthening trochleoplasty. (Reused with permission from Springer. From: Osteotomien. Orthopäde. 2008;
37:872–883)
530
R. M. Biedert
(A) Preoperative MR measurement with too short anterior articular cartilage of the lateral
facet of the trochlea (red arrow). The LCI is 76%. Decreased patellofemoral overlap
(B) Postoperative MR measurement with lengthened anterior lateral facet of the trochlea
(green arrow). The LCI is 98%. Increased patellofemoral overlap
Fig. 8 Assessment of lengthening trochleoplasty
5.3 Postoperative Care
Physical therapy starts immediately after surgery
and is continued until normal knee function is
regained. Partial weight bearing (20 kg) is recommended for 3 to 4 weeks to avoid hypercompression of the osteotomy. Range of motion
is limited (0°–90°) during the 1st week to
decrease swelling and pain. Continuous passive
motion starts immediately to improve the patellofemoral gliding mechanism. Bicycling and
swimming are allowed after 2 to 3 weeks and
after complete wound healing. Sports activities
without any restriction are permitted after
3 months. The overall recovery time can be
expected to be about 4 months (Fig. 8A and B).
Lengthening Trochleoplasty
531
5.4 Complications
The risk for complications is low and include
deep vene thrombosis, infection, scar formations, and knee stiffness. The most important
complications specific to the described surgery
are small fractures and iatrogenic chondral
injuries. Necrosis of the partially detached lateral femoral condyle or breaking was never
noted.
•
•
•
6
Results
Clinical results are generally good and patella
stability is improved. Due to the relatively
small number of cases, a prospective outcome
study with a control group was not possible
so far.
7
Conclusions
The too short lateral articular trochlea in its
proximal extend is another relevant factor for
lateral patellar instability and represents a rare
form of trochlear dysplasia. Lengthening
trochleoplasty is indicated in patients with
dynamic supero-lateral patellar instability due to
a too short lateral articular facet not responding
to conservative treatment. The LCI is the most
reliable and reproducible method for assessing
the length of the lateral trochlea and to depict
exactly the patients suffering from this pathology. Index values of less than 86% confirm the
presence of a too short lateral facet. Lengthening
trochleoplasty improves the supero-lateral contact between the trochlear facet and the distal
patella. This maintains patellar stability against
lateral subluxation under muscle contraction.
8
Take Home Messages
• The too short lateral articular trochlea is
another relevant factor for lateral patellar
•
instability and represents a rare form of trochlear dysplasia in the coronal plane.
The discrepancy between a well-centered
patella under relaxed conditions and the
dynamic supero-lateral instability caused by
quadriceps muscle contraction confirms the
proximal lateral patellar instability.
The lateral condyle index is a reliable measurement method on sagittal MRI to assess the
length of the lateral trochlea
Index values <86% confirm a too short lateral
trochlear facet.
Lengthening trochleoplasty represents the
tailored surgical treatment to correct this
specific type of dysplastic trochlea.
References
1. Biedert RM. Trochlear lengthening osteotomy with
or without elevation of the lateral trochlear facet. In:
Zaffagnini S, Dejour D, Arendt EA, editors. Patellofemoral pain, instability, and arthritis. Berlin Heidelberg: Springer-Verlag; 2010. p. 209–15.
2. Biedert RM, Netzer P, Gal I, Sigg A, Tscholl Ph. The
lateral condyle index–a new index for assessing the
length of the lateral articular trochlea as predisposing
factor for patellar instability. Int Orthop. 2006;
35:1327–31.
3. Biedert RM. Osteotomies. Orthopade. 2008;37
(9):872–83.
4. Biedert RM. Lengthening osteotomy with or without
elevation of the lateral trochlear facet. In: Dejour D,
Zaffagnini S, Arendt EA, editors. Patellofemoral
pain, instability, and arthritis. Berlin Heidelberg:
Springer-Verlag; 2020. p. 335–41.
5. Albee FH. The bone graft wedge in the treatment of
habitual dislocation of the patella. Med Rec.
1915;88:257–63.
6. Brattstroem H. Shape of the intercondylar groove
normally and in recurrent dislocation of the patella.
A clinical and x-ray-anatomical investigation. Acta
Orthop Scand. 1964; Suppl 68:1–148.
7. Zaffagnini S, Pizza N, Del Fabbro G, et al. Anatomic
instability factors: principals and secondary for
patellar instability. In: Dejour D, Zaffagnini S,
Arendt EA, editors, et al., Patellofemoral pain,
instability, and arthritis. Berlin Heidelberg:
Springer-Verlag; 2020. p. 167–81.
8. Amis AA. Patellofemoral joint biomechanics. In:
Biedert RM, editor. Patellofemoral disorders. Chichester: John Wiley & Sons, Ltd.; 2004. p. 37–53.
532
9. Amis AA. Current concepts on anatomy and biomechanics of patellar stability. Sports med Arthrosc
Rev. 2007;15:48–56.
10. Senavongse W, Amis AA. The effects of articular,
retinacular, or muscular deficiencies on patellofemoral joint stability: a biomechanical study in vitro.
J Bone Joint Surg Br. 2005;87(4):577–82.
11. Biedert RM, Sigg A, Gal I, Gerber H. 3D representation of the surface topography of normal and
dysplastic trochlea using MRI. Knee. 2011;18:340–6.
12. Tecklenburg K, Dejour D, Hoser C, Fink C. Bony
and cartilaginous anatomy of the patellofemoral joint.
Knee Surg Sports Traumatol Arthrosc. 2006;14:
235–42.
13. Biedert RM, Albrecht S. The patellotrochlear index:
a new index for assessing patellar height. Knee Surg
Sports Traumatol Arthrosc. 2006;14:707–12.
14. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc.
1994;2(1):19–26.
15. Biedert RM, Bachmann M. Anterior-posterior trochlear measurements of normal and dysplastic
trochlea by axial magnetic resonance imaging. Knee
Surg Sports Traumatol Arthrosc. 2009;17(10):
1225–30.
16. Biedert RM. Patellar instability with increased knee
flexion due to lateral femoral condyle distal dysplasia: a report of two cases. Knee. 2012;19:140–3.
17. Dejour D, Le Coultre B. Osteotomies in patellofemoral instabilities. Sports Med Arthrosc. 2007;15
(1):39–46.
18. Von Knoch E, Böhm T, Bürgi ML, Von Knoch M,
Bereiter H. Trochleaplasty for recurrent patellar
dislocation in association with trochlear dysplasia.
Bone Joint Surg. 2006;88B:1331–5.
19. Bereiter H. Kniechirurgie in der Praxis. 2002.
p. 251–6.
20. McNamara I, Bua N, Smith TO, Ali K, Donell ST.
Deepening trochleoplasty with a thick osteochondral
flap for patellar instability: clinical and functional
R. M. Biedert
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
outcomes at a mean 6-year follow-up. Am J Sports
Med. 2015;43:2706–13.
Masse Y. Trochleoplasty: restorationof the intercondylar groove in subluxations and dislocations of
the patella. Rev Chir Orthop Reparatrice Appar Mot.
1978;64:3–17.
Van Sambeeck J, Van de Groes SAW, Verdonschot N, Hannink G. Trochleoplasty procedures
show complication rates similar to other patellarstabilizing procedures. Knee Surg Sports Traumatol
Arthrosc. 2017;26:2841–57.
Carrillon Y, Abidi H, Dejour D, Fantino O,
Moyen B, Tran-Minh VA. Patellar instability:
assessment on MR images by measuring the lateral
trochlear inclination-initial experience. Radiology.
2000;216(2):582–5.
Tavernier T, Dejour D. Knee imaging: what is the
best modality? J Radiol. 2001;82:387–405.
Biedert RM, Tscholl PM. Patella alta: a comprehensive review of current knowledge. Am J
Orthop. 2017;46:290–300.
Biedert RM. Patella alta: when to correct and impact
on other anatomic risk factors for patellofemoral
instability. Clin Sports Med. 2022;41:65–76.
Donell S, McNamara I. History and clinical examination of patellofemoral instability. In: Dejour D,
Zaffagnini S, Arendt EA, editors. Patellofemoral
pain, instability, and arthritis. Berlin Heidelberg:
Springer-Verlag; 2020. p. 187–97.
Wolfe S , Varacallo M, Thomas JD, Carroll JJ, Kahwaji CI. Patellar instability. In: StatPearls [Internet].
Treasure Island (FL): StatPearls Publishing; 2022
Jan.2021 Jul 20.
Kolowich PA, Paulos LE, Rosenberg TD,
Farnsworth S. Lateral release of the patella: indications and contraindications. Am J Sports Med.
1990;18(4):359–65.
Beighton P, Horan F. Orthopaedic aspects of the
Ehlers-Danlos syndrome. J Bone Joint Surg Br.
1969;51(3):444–53.
Tibial Tubercle Osteotomy
in Patients with Patella Supera
or Infera
Joan Carles Monllau and Enrique Sanchez-Muñoz
1
Historical Introduction
The patella is a sesamoid bone located in the
anterior part of the knee and being part of its
extensor mechanism. It grows the leverage that
the quadriceps tendon exerts on the tibia by
increasing the angle at which it acts. In conformity with its sagittal location, the patella can be
classified as either alta (supera) or baja (infera).
The alta is defined as an abnormally high-riding
patella in relation to the femur and the baja as an
abnormally low-lying patella. Blumensaat [1]
first described a practical radiographic technique
for measuring patellar height. Since then, several
other radiographic measurements have been
proposed. The Caton-Deschamps index (CDI), a
ratio between the length of the patellar articular
surface and its distance from the tibia, has been
J. C. Monllau (&)
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
e-mail: jmonllau@psmar.cat
Catalan Intitute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
E. Sanchez-Muñoz
Knee Unit, Department of Trauma and Orthopaedic
Surgery, Toledo University Hospital, Toledo, Spain
found one of the most reproducible. It has a cutoff value of 1.2 [2].
Patella alta is significantly associated with
patellar dislocation. To address the problem,
tibial tubercle osteotomy (TTO) with distalization is an effective technique that decreases
patellar height, thereby favoring the earlier
engagement of the bone in the trochlea during
knee flexion movement. In that way, it reduces
the risk of dislocations [3]. However, the indication for this procedure remains controversial
among orthopaedic surgeons as it can increase
patellofemoral contact pressure, which leads to
anterior knee pain and chondral degeneration
[3, 4] along with loss of fixation, impairment of
bone healing, and fractures.
Patella baja is the opposite of patella alta. It is
often associated with restricted range-of-motion,
crepitations, and retropatellar pain. Those conditions are probably due to its constant engagement in the trochlea. Patella baja sits too low
down. In that position, it causes significantly
increased patellofemoral contact pressures [5].
That increased wear and tear to the articular
cartilage,
and
eventually
patellofemoral
osteoarthritis. Patella baja can be a congenital
condition with a too short patellar tendon (PT).
However, it is often caused by tendon scarring
after trauma (Fig. 1) or surgical procedures like
patellar tendon harvesting for an ACL reconstruction or a total knee replacement. Much less
frequently, it can be the result of a tibial tubercle
transfer before the closure of the physis.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_37
533
534
J. C. Monllau and E. Sanchez-Muñoz
Fig. 1 AP and lateral-view
radiograph of left knee
showing a significant
posttraumatic patella baja
Treatment strategies for sagittal patella variants are still poorly explored. Therefore, further
study in that area is warranted. The aim of this
chapter is to present some techniques to address
these problems based on the author’s experience.
2
Indications and Contraindications
2.1 Patella Alta
The indications for TTO with distalization have
not been fully defined. Moreover, they depend on
multiple factors. In general, the indication of
surgery is based on measurements of patellar
height in skeletally mature patients. Several
measurements have been introduced over time.
In the author’s experience, the Caton-Deschamps
index is the most useful among them. Patella alta
is defined as a CDI of more than 1.2. However,
surgical treatment is not regularly recommended
until the ratio is more than 1.4 [6].
In case of patellar instability, MPFL reconstruction should also be considered as a crucial
part of the procedure since this ligament is a
primary restraint to lateral patellar dislocation.
Yet, patellar instability is the result of several
anatomical factors that include trochlear dysplasia and lateralized tibial tuberosity (TT) that
should also be corrected in some circumstances.
While an increased (more than 20 mm) tibial
tuberosity-trochlear groove (TT-TG) distance [9]
correction can be easily added to the index procedure by medializing its bony attachment, the
decision to perform a trochleoplasty can be
harder as the procedure is much more delicate
and there is no clear cut-off value.
2.2 Patella Baja
Patella baja is defined by a CDI of 0.6 or less or
and Insall-Salvati index of less than 0.8 or a
difference in the length greater than 15% in
comparison to the contralateral side [7].
Lengthening of the patellar tendon is indicated in
patients with symptomatic patella baja not
responsive to conservative treatment for more
than 3 months [7, 11]. The surgical options for
patella baja include the excision of the lower
Tibial Tubercle Osteotomy in Patients …
third of the patella, lengthening of the patellar
tendon with a PT plasty, reconstruction of the
patellar tendon using tendon allografts and
proximalization TTO, or a combination of the all
those procedures [7, 10, 11].
When associated with other conditions like
arthrofibrosis and soft-tissue adhesions between
the PT and proximal tibia, those pathologies
should also be addressed to arrive at good outcomes [10, 11]. If patella baja is associated with
a total knee replacement (TKR), a differential
diagnosis with pseudo patella baja is advised as
the latter condition needs a different approach
from patella baja [12].
3
Surgical Technique, Tips
and Tricks
3.1 Patella Alta
TTO with distalization is performed under spinal
anaesthesia. A tourniquet is placed high on the
thigh (although its use is optional) and the patient
is positioned supine with the surgical knee at 90º
flexion, with the help of a foot stopper. An
incision of approximately 6 to 8 cm is made just
distal to the knee, directly over the tibial
tuberosity. After identifying the patellar tendon
attachment and marking the osteotomy cut with 2
Kirschner wires, two 4.5 mm holes are drilled on
the anterior cortex of the tibial tuberosity for later
lag-screw compression fixation of the osteotomized bone. Afterwards, the osteotomy (some
6 cm in length and 8 mm deep) is performed
with the help of an oscillating saw and osteotomes. The cut is done from medial to lateral and
then the bone block is shifted downwards as
much as necessary, according to a prior calculation, either reducing the bone block of the tibial
tuberosity or removing some more cortical bone
in the distal part of the osteotomy. The detached
tibial tuberosity is then fixed back in its new
position using two 4.5 mm compression lagscrews (Fig. 2). Additionally, to reduce the PT
length, two anchors are positioned in the upper
part of the tibial osteotomy site and the distal
patellar tendon is sewn and fixed to the bone.
535
This tenodesis shortens the whole length of the
PT, otherwise the CD index is normalized but the
Insall-Salvati index remains the same (as the
tendon maintains its length unchanged).
Post-operatively, partial weightbearing is
allowed with two crutches, wearing a brace for
the first couple of weeks. Then, weightbearing
status is gradually increased. The knee is checked
with X-rays, and when the healing of the bone is
seen to be well under way (normally by about
6 weeks) in them, then the brace and subsequently the crutches are discarded.
3.2 Patella Baja
The aim of the surgical procedure is to proximalize the patella. Several techniques have been
proposed to that end. They include a transposition of the tibial tubercle and some variants of
patellar tendon lengthening. However, there is
currently no gold standard for treating patella
baja [7–12].
The transfer of the tibial tubercle is a popular
method to restore patellar height and has the
advantage of permitting early mobilization,
which may help in preventing the recurrence of
the condition [8]. However, it does not consider
the underlying cause. Additionally, changing the
extensor mechanism attachment point nearer to
the joint line might cause potential dysfunction
of the quadriceps muscle as a result of detachment of the PT [7]. Lastly, although the patellar
position can be normal at the end of the surgical
procedure, the PT length will remain the same
(Fig. 3).
Our preferred technique consists of a partial
TTO proximalization with a modified Z plasty of
the patellar tendon [7]. The anaesthesia, patient
positioning and surgical approach are the same as
previously described for patella alta. A midline
incision from the distal third of the patella to the
TT that goes along the midline of the patellar
tendon is made. In a Z-shape, two flaps are
developed, the medial one including an osteotomized bone block made from the medial portion
of the TT, that is distally detached, and the lateral
one including a periosteal flap proximally
536
Fig. 2 A Surgical view,
performing the TT osteotomy
with an oscillating saw.
B After removing some
cortical bone in the distal part
of the osteotomy the TT is
reduced and fixed back in its
new position using two lagscrews. C Image intensifier
sagittal view showing the final
result
J. C. Monllau and E. Sanchez-Muñoz
A
B
detached from the patella. The medial flap is
moved proximally while the lateral one is moved
distally, both at the same distance (Fig. 4). After
checking the X-rays to make sure that the adequate patellar position is reached. With the knee
at 90º of flexion, the lateral flap is proximally
fixed at the patella with suture anchors while the
bone block of the medial flap is fixed at the tibia
with a 3.5 mm cortical screw. Finally, the 2 reins
of the patellar tendon are sutured with #2–0
interrupted suture. In cases of high-risk of
recurrence or bad tissue quality, augmentation
with an Aquiles allograft with a bone block is
recommended (Fig. 5).
Tibial Tubercle Osteotomy in Patients …
C
537
4
Results
Patellar instability is the most usual indication for
TTO, usually in association with other procedures
[9, 13]. Good outcomes have been reported after a
distalization TTO with associated medialization, if
needed, to correct CDI, decrease pain and improve
functionality [9, 13]. Addressing concomitant
pathologies is mandatory to obtain good outcomes,
with and increased risk of persistent pain associated
to grade 3 and 4 ICRS cartilage lesions [13].
Regarding the proximalization TTO, current
evidence is scarce [9]. It is most usually presented
as a surgical complication with associated
arthrofibrosis and limited range-of-motion, results
of this procedure are not as predictable as with
distalization TTO. With proper preoperative planning, adequate correction of the CDI along with an
improvement in terms of pain and function is to be
expected [7, 9, 11, 14]. Although there is an
improvement relative to pain and function, outcome measures tend to remain diminished when
compared to the general population baseline [11].
Fig. 2 (continued)
Postoperatively, immediate passive motion is
of paramount importance to avoid recurrence of
arthrofibrosis and improve range of motion
(ROM). Together with ROM exercises, muscular
strengthening exercises are begun on the first
day post-op. For the first 2 weeks ROM is limited to 0–90°, with a brace looked in full extension that should only be removed for
physiotherapy exercises. Full weight bearing is
allowed with a brace looked in full extension for
the first 4 weeks, posteriorly discontinued if
there is good muscular control. Pivoting and
strenuous activities are allowed not before
3 months, with sports limited to light activities
for the first 6 months.
5
Scientific Evidence
The current bibliography on tibial tubercle
osteotomies is of low-quality, being mainly level
III and IV evidence studies that do not allow
solid meta-analysis [9]. In fact, most of the
studies are cases series with small sample sizes
[6, 11–14]. Thus, there is a need of better-quality
studies with larger sample sizes and better reports
on data and outcomes to make it possible to draw
any sound conclusion.
6
Complications
Painful hardware is the more common complication [9, 11, 13], and may need reoperation for
hardware removal [9, 11], but do not associates
538
A
J. C. Monllau and E. Sanchez-Muñoz
B
Fig. 3 A Operative image of a left knee. The patient placed in supine position with 90° flexed knee. B Image intensifier
sagittal view. A long sleeve of the tibial tuberosity has been detached and proximalized to the level of the joint line
worse functional outcomes [9]. Recurrent patellar
dislocation, TT fractures, proximal tibial fractures, infection and TTO non-union [14] are
potential complications with overall lowincidence rate [9, 13], and some series reporting no cases of them [11].
Concerns with this technique also focus
around patellofemoral contact pressure [7, 13] in
relation to patella cartilage damage. Many papers
have described persistent pain [9, 11], in general
correlated with patellar cartilage defect severity
[13]. This compares to our experience. Another
common objection to TTO is the concern with
failed osteotomy healing [14]. In our series (unpublished data), we had only seen one case of
non-union. A long (>6 cm) and thick (>8 mm)
bone fragment [13] had a good bony surface area
for healing and is stable. When performing a
distalization tubercle osteotomy, I do like to
place a bone autograft between the proximal tibia
bumper and the fragment to more closely calculate the exact amount of distalization.
7
Take Home Message
The tibial tubercle osteotomy with distalization is
an effective technique for patellar height correction and eventually to prevent recurrent patellar
dislocations.
The tibial tubercle osteotomy with proximalization with or without a patellar tendon plasty effectively corrects patella baja and brings improvement
in terms of pain, range-of-motion and knee function.
Patellar height disorders are usually associated
with other underlying conditions and, especially
in patella baja, previous surgeries. If these
problems are not adequately addressed, the tibial
tuberosity osteotomy alone will not bring about
good outcomes.
Tibial Tubercle Osteotomy in Patients …
A
539
B
C
Fig. 4 A Lateral imaging of posttraumatic patella baja,
showing Caton-Deschamps measurement. B Frontal view
of the same knee, after detached from the TT, the medial
half of the PT is moved proximally and the lateral one,
subperiostically dissected from the patella, is moved
distally the same distance. C Final result. A PF prothesis
was added in this case due to the degree of OA in the
articulating PF surfaces
540
J. C. Monllau and E. Sanchez-Muñoz
Fig. 5 Surgical view
showing augmentation of the
repair using an Aquiles
allograft with a bone block
References
1. Blumensaat C. Die Lageabweichungen und Verrenkungen
der Kniescheibe.
Ergebn
Chir
Orthop. 1938;31:149–223.
2. Enea D, Cane PP, Fravisini M, Gigante A, Dei GL.
Distalization and medialization of tibial tuberosity for
the treatment of potential patellar instability with
patella alta. Joints. 2018;6(2):80–4.
3. Magnussen RA, De Simone V, Lustig S, Neyret P,
Flanigan DC. Treatment of patella alta in patients
with episodic patellar dislocation: a systematic
review. Knee Surg Sports Traumatol Arthrosc.
2014;22(10):2545–50.
4. Payne J, Rimmke N, Schmitt LC, Flanigan DC,
Magnussen RA. The incidence of complications of
tibial tubercle osteotomy: a systematic review.
Arthroscopy. 2015;31(9):1819–25.
5. Yang JS, Fulkerson JP, Obopilwe E, et al. Patellofemoral contact pressures after patellar distalization:
a biomechanical study. Arthroscopy. 2017;33
(11):2038–44.
6. Caton J, Deschamps G, Chambat P, Lerat JL,
Dejour H. [Patella infera. Apropos of 128 cases].
Rev Chir Orthop Reparatrice Appar Mot. 1982;68
(5):317–25.
7. Perelli S, Ibañez M, Morales-Marin C, et al. Patellar
tendon lengthening: rescue procedure for patella baja.
Arthrosc Tech. 2020;9(1):e1–8.
8. Drexler M, Dwyer T, Marmor M, Sternheim A,
Cameron HU, Cameron JC. The treatment of
acquired patella baja with proximalize the tibial
tuberosity. Knee Surg Sports Traumatol Arthrosc.
2013;21(11):2578–83.
9. Saltzman BM, Rao A, Erickson BJ, et al. A systematic review of 21 tibial tubercle osteotomy studies
and more than 1000 Knees: indications, clinical
outcomes, complications, and reoperations. Am J
Orthop (Belle Mead NJ). 2017;46(6):E396-407.
10. Wierer G, Hoser C, Elmar H, Elisabeth A, Christian F. Treatment of patella baja by a modified Zplasty. Knee Surgery Sport Traumatol Arthrosc.
2016;24:2943–7.
11. Schmidt S, Mengis N, Rippke JN, et al. Treatment of
acquired patella baja by proximalization tibial tubercle osteotomy significantly improved knee joint
function but overall patient reported outcome measures remain diminished after two to four years of
follow up. Arch Orthop Trauma Surg. 2021.
12. Vandeputte FJ, Vandenneucker H. Proximalisation of
the tibial tubercle gives a good outcome in patients
undergoing revision total knee arthroplasty who have
pseudo patella baja. Bone Jt J. 2017;99-B:912–6.
Tibial Tubercle Osteotomy in Patients …
13. Leite CBG, Santos TP, Giglio PN, Pecora JR,
Camanho GL, Gobbi RG. Tibial tubercle osteotomy
with distalization is a safe and effective procedure for
patients with patella alta and patellar instability.
Orthop J Sport Med. 2021;9(1):2325967120975101.
541
14. Vives-Barquiel MA, Torrents A, Lozano L, et al.
Proximalize osteotomy of tibial tuberosity (POTT) as
a treatment for stiffness secondary to patella baja in
total knee arthroplasty (TKA). Arch Orthop Trauma
Surg. 2015;135:1445–51.
Tibial Tubercle Anteromedialization
Osteotomy (Fulkerson Osteotomy)
Andrew Gudeman and Jack Farr
1
Introduction
The tibial tubercle (interchangeable with
tuberosity) is the most distal attachment of the
extensor mechanism. As a result, it and can serve
as a tool in altering patellofemoral (PF) mechanics. Known collectively as tibial tubercle osteotomies (TTO) or distal realignment procedures,
osteotomies of the tibial tubercle are a useful
method to treat a variety of PF conditions by
allowing coronal, axial, and sagittal plane
adjustments of the patellofemoral articulation,
which redistribute patellar contact pressures
(force and contact area) and potentially improve
tracking. Numerous tibial tubercle osteotomies
have been described in the literature to treat PF
pain, chondrosis, and/or instability.
The procedure was initially described by
Goldthwaite in 1896 [1]. Roux, and later Elmslie
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_38.
A. Gudeman
Indiana University School of Medicine, Indianapolis,
IN, USA
J. Farr (&)
Knee Preservation and Cartilage Restoration Center,
OrthoIndy, Indianapolis, IN, USA
e-mail: jfarr@orthoindy.com
and Trillat, popularized their technique for the
treatment of PF instability [2]. Anteriorization of
the tibial tubercle was described by Maquet [3] to
treat PF pain associated with arthritis. Each of
these historical procedures takes advantage of
important alterations in patellar kinematics. To
avoid complications associated with the Maquet
procedure, Fulkerson [4] designed a tubercle
osteotomy known as the anteromedalization
(AMZ) technique to address PF pain in conjunction with patellar maltracking. The oblique
nature of the Fulkerson osteotomy allows for
simultaneous anteriorization and medialization of
the tibial tubercle. By varying the angle of the
osteotomy, the tubercle can be biased to a more
anterior or more medial position. Anteriorization
of the tubercle elevates the distal extensor
mechanism attachment and serves to shift patellar contact forces proximally as well as decrease
the applied force, while medialization results in a
decrease of the lateral force vector in patellar
instability.
It is necessary to be mindful that the Fulkerson osteotomy, while decreasing distal lateral
loads, concomitantly shifts contact forces to the
medial side of the patellofemoral compartment.
These load modifications were initially demonstrated in the lab with Fuji pressure sensitive
contact film [5] and with finite element analysis
by Cohen and Ateshian [6]. To address this, Rue
et al. introduced force/contact assessment with
TekScan sensors and showed that straight anteriorization of the tubercle significantly decreased
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_38
543
544
A. Gudeman and J. Farr
contact pressures in the trochlea (without an
increase in medial contact pressures) [7, 8].
Incidentally, the described technique was similar
to the Maquet technique but without bone
grafting [9].
2
Indications
When discussing the indications for AMZ it is
important to note that as with most patellofemoral surgeries, it should only be performed after
the patient has failed exhaustive nonoperative
measures that include a comprehensive “core to
the floor” program of rehabilitation as well as
bracing and orthotics. The indications for this
procedure have evolved and continue to be
refined. This has been primarily driven by the
evolution and outcomes of patellofemoral resurfacing procedures, as well as improved objective
measures of patellar alignment, contact area and
forces. These alterations redistribute the contact
forces within the patellofemoral compartment
and a keen understanding of these changes is
paramount in optimizing forces on areas of
chondral damage and restoration [10].
Indications for AMZ are primarily based upon
the mechanical and chondral pathologies specific
to each individual knee. Malalignment is a term
that has different meanings to different experts,
but for the purposes of this chapter it simply
means alignment that is different from the average asymptomatic individual. A comprehensive
review by Post et al. [11] demonstrated that the
“Q” angle was inadequate (within the studies
reviewed) to use as a measure of malalignment of
the tibial tuberosity. Although, a recent
improvement in Q angle measurement with a
long goniometer has the potential to improve the
intra- and inter-observer reliability [12].
The tibial tuberosity to trochlear groove (TTTG) distance, popularized by Dejour et al. [13] as
an objective measure of tuberosity position, has
helped quantify abnormal tuberosity position and
enhanced appropriate candidate identification for
all tuberosity osteotomies, including the AMZ.
This is important as patellar contact pressures are
very sensitive to distal realignment [14]. The role
of the TT-TG in surgical planning continues to
evolve. It is important to keep in mind the limitations of this measurement: Knee flexion/tibial
on femur rotation and trochlear dysplasia may
alter the measurement and thus make the measurement less “precise” [15]. Thus, some surgeons have suggested adding the tibial tubercleposterior cruciate ligament (TT-PCL) distance as
a reliable alternative [16, 17], as well as measuring the tubercle position as an angle within the
coronal plane.
The TT-TG in asymptomatic patients has been
reported from 11–13 mm and those with instability symptoms have average measurements of
over 15 mm [17, 18]. A panel of patellofemoral
experts agreed that TT-TG distances of over
20 mm were definitely abnormal and would be
potential (key word as other factors must also be
considered) candidates for moving the tibial
tubercle [19]. Results of medial patellofemoral
ligament reconstruction have also been shown to
improve with TTO for patients with TT-TG
distances of 17–20 [20]. The upper limit of
asymptomatic patient’s TT-PCL distance has
been reported at 24 mm [10]. Several studies
have compared the efficacy of a TT-TG of
20 mm versus a TT-PCL of 24 mm with mixed
results [21–23]. An understanding of both measurements and the limitations with abnormal PF
anatomy is important for the surgeon before
consideration of a distal realignment surgery.
Patients with isolated chondrosis of the distal
or lateral patella, who have excessive lateral
patellar tilt and/or subluxation associated with an
increased TT-TG distance and minimal trochlear
chondrosis are optimal AMZ candidates based on
a retrospective review of AMZ outcomes by
Pidoriano [24]. It has been argued that rotational
tuberosity abnormalities associated with subjective instability and pain may be sufficiently
treated with straight medialization or derotation
of the tibial tubercle, although Pritsch et al. [25]
found 80% of 66 patients undergoing tubercle
transfer for patellar instability and pain associated with maltracking required anteriorization
based on intraoperative examination. Secondly,
patients who are undergoing PF cartilage
restorative procedures have been shown to
Tibial Tubercle Anteromedialization Osteotomy …
545
Table 1 Summary of indications for anteromedialization
Summary of AMZ indications
• Lateral or distal patella chondrosis with an increased TT-TG distance, excessive lateral tilt/subluxation and the
absence of trochlea chondrosis
• As an adjunct procedure to patellofemoral cartilage restoration in an effort to improve the contact area and decrease
PF forces to optimize the biomechanical environment of the new cartilage implant
• Possibly, in conjunction with MPFL repair or reconstruction in patients with markedly increased TT-TG distance
benefit from a combined AMZ procedure [26,
27] where optimization of the biomechanical
environment and decreased stress across the
restored cartilage is required. Additionally, in
patients undergoing MPFL repair or reconstruction for recurrent lateral patella instability, AMZ
may be indicated only in the setting of a significantly increased TT-TG distance. However, it
should be noted that while this theoretically
decreases the lateral vector forces on the healing
MPFL tissues, there is no randomized study of
AMZ plus MPFL surgery versus MPFL surgery
alone published as of this writing. In addition,
combining AMZ with PF cartilage restorative
procedures such as autologous chondrocyte
implantation and osteoarticular grafting procedures within the PF compartment have demonstrated superior results to either procedure
performed independently [26, 27]. A summary of
AMZ indications is presented in Table 1.
3
Contraindications
Several contraindications to AMZ exist and
potential candidates must be assessed carefully
prior to surgery. Anteromedialization is
contraindicated in patients with a normal TT-TG
distance and in patients who have symptoms not
explained by an increased TT-TG distance. The
condition of the medial PF articulation should be
carefully assessed as medialization will significantly increase contact pressures between the
medial patellar facet and trochlea [7]. In addition,
AMZ is contraindicated for proximal patella,
panpatella and bipolar chondrosis based upon the
outcomes from Pidoriano et al. [24].
Advanced chondrosis of the central trochlea
has been associated with sub-optimal results and
is considered a contraindication to AMZ as an
isolated procedure [7, 28]. Standard contraindications to any osteotomy must also be considered, which includes smoking, infection,
inflammatory arthropathy, marked osteoporosis
inhibiting adequate fixation, complex regional
pain syndrome, arthrofibrosis, inability to minimally weight-bear and non-compliant patients.
A summary of AMZ contraindications is presented in Table 2.
A final caution has been championed by
Teitge: if the malalignmet is from excessive
femoral or tibial rotation, a correction of the
source of malalignment should be entertained
[29].
Table 2 Summary of contraindications to anteromedialization
Summary of contraindications to isolated AMZ
• Normal TT-TG distance
• Medial patellofemoral chondrosis (only if not combined with cartilage restoration procedure)
• As an isolated procedure, when not combined with cartilage restoration, to treat proximal pole, pan patella, trochlear
or bipolar chondrosis
• General contraindications to osteotomy (i.e. smoking, osteoporosis, inflammatory arthropathy)
546
4
A. Gudeman and J. Farr
Surgical Technique
Techniques for AMZ have classically been
described as an isolated procedure; however,
AMZ typically includes lateral retinacular release
or lengthening to untether the patella allowing
the patellar medialization component and is not
uncommonly performed in conjunction with
procedures such as MPFL repair/reconstruction
or cartilage restorative procedures. These procedures must be taken into consideration when
planning the surgical approach.
4.1 Pre-operative Assessment
and Planning
The desired amount of anteriorization and
medialization (based on the objective measurement of the TT-TG distance) may be calculated
pre-operatively and used as a reference during
surgery. Trigonometric ratios can be used to
determine the desired angle for the osteotomy.
Anteriorization of between 10 and 15 mm is
most commonly recommended as it decreases PF
stress loads by approximately 20% [6] and
results in minimal sagittal rotation of the patella.
In regard to the medialization component, the
goal of the osteotomy is to normalize the TT-TG
distance, which based on the literature, is within
a range of 10–15 mm. By varying the slope and
the extent of anteriorization, a variety of medialization distances can be achieved. The required
angle can be calculated by the inverse tangent of
the desired anterior movement divided by the
desired medial movement (Table 3). For example, a 60° osteotomy with 15 mm of elevation
will produce 8.7 mm of medialization, which
will normalize most tuberosity positions as it is
rare for TT-TG distances of over 25 mm. When
more medialization is required, the slope may be
decreased; a slope of 45° would move the
tubercle 15 mm medially with 15 mm of elevation. Surgeons may tend to underestimate the
anteriorization and osteotomy angle during
Fulkerson osteotomy, which must be taken in to
account [30].
4.2 Set up and Positioning
of the Patient
The patient is positioned in the supine position
with a side post and a gel-pad under the ipsilateral hemipelvis. This facilitates an initial arthroscopic evaluation of the knee and limits external
rotation of the limb during the osteotomy. All
extremities are well padded, a tourniquet is
applied, and prophylactic antibiotics are administered. General, spinal, epidural or regional
block anaesthesia can be used depending upon
patient and surgeon preference. A thorough
examination under anaesthesia includes assessment of range of motion, patella tracking and
patella displacement. The patient is then prepped
and draped in standard fashion.
4.3 Arthroscopic Evaluation
Initially, arthroscopic evaluation and documentation of patellofemoral chondrosis is performed.
The areas of chondrosis are regionally mapped
using the ICRS region knee mapping system
noting that significant patellar chondrosis may
lead to termination of the procedure unless concomitant cartilage restoration has been planned.
Certainly, other contraindications may be discovered at arthroscopy and would also halt proceeding with AMZ. At this stage, based on
Table 3 Reference guide for osteotomy slope
Osteotomy slope
Elevation (mm)
Medialization (mm)
60°
15
8.7
50°
15
12.5
45°
15
15
Tibial Tubercle Anteromedialization Osteotomy …
547
clinical tilt or CT/MRI documented patellar tilt, an
arthroscopic lateral release may be performed if
indicated. When combined with PF cartilage
restoration the lateral release or lateral lengthening
is performed in an open manner to allow direct
access for performing the cartilage restoration
procedure. Lateral release should allow neutralization of patella tilt and unrestricted central positioning of the patella relative to the trochlea,
however, care must be taken to ensure medial
patella subluxation does not occur. It should be
noted that lateral lengthening can maintain control
not offered by lateral release [31].
4.4 Incision and Exposure
The longitudinal incision runs approximately 8 to
10 cm distally beginning at the patellar tendon
insertion to the tibial tubercle. The incision may
be extended proximally to allow adequate
exposure if concomitant cartilage restoration is
being performed. The patella tendon is identified
and released from capsule medially and laterally
to allow protection with a retractor and later
tubercle elevation. The lateral incision is extended distally along the lateral margin of the tibial
tuberosity and tibial crest allowing subperiosteal
elevation of the anterior compartment musculature and thereby exposing the lateral wall of the
tibia. A retractor is positioned at the posterior
aspect of the lateral tibia in order to protect the
posterior neurovascular structures (deep peroneal
nerve and anterior tibial artery) (Fig. 1).
4.5 Performing the Osteotomy
For the highly experienced surgeon the osteotomy may be performed free hand. Fulkerson
originally used an external fixator pin clamp to
direct multiple pins in the osteotomy plane and
then complete it with osteotomes [4]. Today,
there are two commercially available AMZ
osteotomy systems available (Tracker, DePuy
Synthes Mitek Sports Medicine, Raynham, MA
and the T3 System, Arthrex, Inc., Naples, FL).
The Tracker system was available first and
Fig. 1 Anterior compartment musculature is elevated
from the lateral wall of the tibial with retractor protecting
neurovascular structures posteriorly
detailed illustrated surgical techniques using the
jig system have been published by both Fulkerson and Farr. The T3 system will be used in this
section to illustrate the operative technique;
however, the approach for each system and steps
following fixation of the cutting guide are similar. For the T3 system, an initial reference pin is
orientated perpendicular to the posterior cortex of
the proximal tibia (Fig. 2). The reference pin is
inserted through the pin guide into the tibial
tuberosity, just distal to the patellar tendon
attachment to the tibial tuberosity (Fig. 3). Using
preoperative calculations for anteriorization and
medialization, the desired slope angle guide is
assembled with the cutting block and cutting
block post. The cutting guide is then placed over
the reference pin and the cutting block is positioned immediately medial to the tibial crest
beginning directly in line with the medial border
of the patella tendon, as it attaches to the tibial
tuberosity (Fig. 4) and angled laterally to allow a
lateral exit of the osteotomy distally. For
emphasis, the desired osteotomy forms a triangle
shape that tapers distally allowing an exit
through the anterior cortex to the lateral wall of
the tibia. The desired pedicle length for the
osteotomy is approximately 7–10 cm. When
correct positioning has been achieved and the
entry and exit sites have been confirmed, two
548
A. Gudeman and J. Farr
Fig. 2 The reference pin guide is orientated so it is perpendicular to the posterior cortex of the tibia
Fig. 3 Reference pin is inserted through the guide just
distal to Gerdy’s tubercle
break-away pins secure the cutting block in
position (Fig. 5). With the retractor still protecting neurovascular structures posteriorly, the cut
is made with an oscillating saw, which is
simultaneously cooled with saline (Fig. 6). The
cutting block is removed, and the oscillating saw
is directed towards the distal exit of the osteotomy to finish the distal cut. A small osteotome is
used to complete the proximal osteotomy,
approaching the tibial tuberosity medially and
laterally at the level of the patella tendon insertion (Fig. 7). The tuberosity is now free. A recent
study showed that complete detachment of the
tubercle compared to leaving a hinge results in
higher rates of arthrofibrosis and must be used
judiciously when needed for exposure [32].
(Note that the senior author detached the tubercle
pedicle in all cases and complications were
within the ranges reported in the literature).
Tibial Tubercle Anteromedialization Osteotomy …
549
Fig. 4 The cutting guide is placed over the reference pin and the cutting block is positioned medial to the patella
tendon
4.6 Positioning and Fixation
Fig. 5 Break-away pins secure the cutting block after
positioning is confirmed
A ruler is used to measure the required amount of
anteriorization and medialization based on preoperative calculations and the pedicle position is
adjusted along the osteotomy slope. If required,
the pedicles can be moved proximally or distally to
address any underlying patella alta or infra.
A Kirschner wire is used to temporarily secure the
pedicle when correct positioning has been
achieved. The tuberosity fragment is then drilled
using interfragmentary lag technique and secured
using two countersunk 4.5 mm cortical screws
(Fig. 8). The screws are positioned perpendicular
to the osteotomy (angled from the anterolateral
aspect of the pedicle to posteromedial tibia) so they
are directed away from posterior neurovascular
550
A. Gudeman and J. Farr
Fig. 6 Oscillating saw
cooled with saline creates the
initial sloped osteotomy,
exiting on the protective
retractor
Fig. 7 Proximal cuts are
completed with small
osteotome
structures. Cosgarea prefers 3.5 mm headless
screws as he reports less hardware (screw) pain in
the delayed post-operative setting [33]. The surgical site is closed in a standard fashion.
5
Pearls and Pitfalls
5.1 Pearls
• Preoperative rehabilitation and expectation
counselling is extremely important to prepare
the patient for surgery and recovery.
• The TT-TG measurement is an objective
alternative to the Q-angle, quantifying the
concept of tibial tuberosity malalignment. It is
a single data point and should not be the sole
indication for TTO.
• The mean TT-TG distance is 11–13 mm in
asymptomatic patients and is considered
excessive when above 20 mm.
• The TT-PCL measurement can be a useful
adjunct in patients with trochlear dysplasia.
• The goal is to ‘normalize’ the tibial tubercle
position, that is, keeping within a range of
10–15 mm.
Tibial Tubercle Anteromedialization Osteotomy …
Fig. 8 The distance of
medialization and
anteriorization is measured
directly and the pedicle is
secured with 2–4.5 mm
screws
551
A
B
• The required amount of anteriorization and
medialization needed for normalization should
be considered independently. The required
angle for osteotomy angle is determined based
upon these values.
• The osteotomy angle is equal to tan−1 of the
desired anterior movement (y) divided by the
desired medial movement (x), e.g., Angle =
tan−1 (y/x). For simplicity, see Table 3.
• Assessment for patella alta using the CatonDeschamps ratio (normal range 0.8 to 1.2) is
required to determine if distalization is recommended (typically over 1.4) [10].
• Strengthening of proximal core muscles must
be a focus of rehabilitation in conjunction
with local musculature.
• Anteromedialization can be performed in
conjunction with other procedures including
lateral release/lateral lengthening, MPFL
repair or reconstruction or cartilage restoration
procedures.
5.2 Pitfalls
• Over medialization of the tibial tubercle can
be detrimental secondary to increased medial
patellofemoral and tibiofemoral stress
• Patients should be aware that pain over the
screw site is common, and they may need
removal at a future date.
• Weight bearing too early can lead to a fracture
of the proximal tibia if the patient is returned
to full weight bearing prior to radiographic
healing [34].
• The MPFL is recognized as the key restraint
to lateral patella dislocation. Isolated tibial
tuberosity AMZ is not a substitute for MPFL
repair or reconstruction.
552
A. Gudeman and J. Farr
• Excessive anteriorization of the tuberosity can
lead to skin healing problems and can cause
clinically significant sagittal plane rotation of
the patella altering contact areas.
• Isolated AMZ performed in the presence of
chondrosis will yield poor results when the
wear patterns are in the: proximal patella, panpatella or trochlea. However, AMZ in conjunction with cartilage restoration procedures
in these regions can achieve good results.
6
Complications
Potential complications include those generally
associated with osteotomies of the lower limb.
General complications include malunion, nonunion, fracture at the osteotomy site [34], venousthromboembolism, compartment syndrome,
infection and loss of fixation. The major complication rate of TTO has been reported to be
approximately 3% [35]. Complications specific to
AMZ include persistent pain, arthrofibrosis and
stiffness, progressive chondral deterioration,
symptomatic hardware, complex regional pain
syndrome and intraoperative injury to the neurovascular structures including the popliteal
artery and its trifurcation [36] and the deep peroneal nerve. Registry data have shown no
increased risk for adverse events between isolated
MPFLR and concomitant MPFLR and TTO [37].
7
Post-Operative Management
To improve postoperative recovery and prepare
for surgery, the patient should undergo a preoperative proximal core and kinetic chain
strengthening program (lower back, pelvis, hip
thigh, and leg). Postoperatively the patient is
treated with standard compression dressings,
protective bracing, cryotherapy and is monitored
for immediate complications. For the first
6 weeks the patient is limited to touch weight
bearing with crutches and begins transitioning to
full weight bearing after radiographs are noted to
be acceptable at 6 weeks. The knee is protected
with a hinged knee brace in extension which is
unlocked at 2 weeks and discontinued when
there is adequate lower extremity control (usually
by 8 weeks). Early core proximal strengthening,
quadriceps strengthening, and knee range of
motion exercises are essential and a close relationship with an experienced physical therapist is
key to optimal results. The safe range of motion
may need to be modified throughout the rehabilitation process to accommodate for concomitant
cartilage restorative procedures. Return to play
outcomes after TTO have been poorly reported,
with variable return criteria including quadriceps
strength, range of motion, radiographic healing,
and physical therapy protocols [38].
8
Key Message and Take-Home
Points
Key Message: AMZ has been shown to improve
outcomes for patients with patellar instability and
patellofemoral cartilage restoration when appropriately indicated with other concomitant procedures (Table 4).
Take Home Points:
• The expert consensus is that AMZ should be
considered in patients with TT-TG greater
than 20 mm and TT-PCL of 24 but has also
been shown to be beneficial in patients with
smaller distances.
• Careful scrutiny of other concomitant pathology including femoral anteversion and trochlear dysplasia must also be analyzed preoperatively and addressed.
• Pre-operative planning to determine desired
amount of anteriorization and medialization,
with the corresponding osteotomy angle, are
crucial for success.
• AMZ is contra-indicated in medial and panpatellar chondral defects due to increased
contact pressures.
• A straight anteriorization may be beneficial to
offload those chondral injuries that are not
amenable to AMZ.
Tibial Tubercle Anteromedialization Osteotomy …
553
Table 4 Anteromedialization outcomes
Author
Patient number
Mean follow-up (range)
Reported outcomes
Fulkerson [4]
8
n/a
Substantial relief of pain and disability for all patients
Cameron [39]
53
>12 mo
66% Excellent, 16% Good, 11% Fair, 7% Poor
Fulkerson [40]
30
35 mo (26–50)
35% Excellent, 54% Good or Very Good, 4% Fair, 7% Poor
Sakai [41]
21
5 yrs (2–13)
Pain relief in ascending and descending stairs for 20/21
Pidoriano [24]
37
47 mo (12–96)
87% Good to Excellent results with lateral or distal lesions,
55% Good to Excellent results with medial lesions, 20%
Good to Excellent results with proximal or diffuse lesions
Bellemans
[42]
29
32 mo (25–44)
Significant improvements in mean Lysholm (62 pre, 92 post,
p < 0.001) and Kujala scores (43 pre, 89 post, p < 0.001)
Buuck [28]
42
8.2 yrs (4–12)
86% Good to Excellent subjectively, 86% Good to Excellent
on clinical examination
Franciozi [20]
42 (18 in AMZ
group)
40.86 months
(24–60 months)
With TT-TG between 17–20 mm, TTO + MPFLR had
better PROs compared with MPFLR in isolation
Zarkadis [27]
72 with PF ACI
(91% with
AMZ)
4.3 years (2.0–9.9)
78% returned to moderate to very heavy occupational
demand
• Use of the pearls and pitfalls outlined in this
chapter can help minimize complications and
maximize success.
References
1. Goldthwait JE. Dislocation of the patella. JBJS.
1896;1(1):237–8.
2. Trillat A. Diagnostic et traitement des subluxations
recidevantes
de
la
rotule.
Rev
Chir
Orthop. 1964;50:813–24.
3. Maquet P. Biomechanics of the patello-femoral joint.
Acta Orthop Belg. 1978;44(1):41–54.
4. Fulkerson JP. Anteromedialization of the tibial
tuberosity for patellofemoral malalignment. Clin
Orthop Relat Res. 1983;177(177):176–81.
5. Ramappa AJ, Apreleva M, Harrold FR, Fitzgibbons PG, Wilson DR, Gill TJ. The effects of
medialization and anteromedialization of the tibial
tubercle on patellofemoral mechanics and kinematics. Am J Sports Med. 2006;34(5):749–56.
6. Cohen ZA, Henry JH, McCarthy DM, Mow VC,
Ateshian GA. Computer simulations of patellofemoral joint surgery. Patient-specific models for
tuberosity transfer. Am J Sports Med. 2003;31
(1):87–98.
7. Rue JP, Colton A, Zare SM, Shewman E, Farr J,
Bach BR, et al. Trochlear contact pressures after
straight anteriorization of the tibial tuberosity. Am J
Sports Med. 2008;36(10):1953–9.
8. Lansdown DA, Christian D, Madden B, Redondo M,
Farr J, Cole BJ, et al. The sagittal tibial tubercletrochlear groove distance as a measurement of
sagittal imbalance in patients with symptomatic
patellofemoral chondral lesions. Cartilage. 2021;13
(1_suppl):449S–455S.
9. Patel RM, Wright-Chisem J, Williams RJ. Anteriorizing tibial tubercle osteotomy for patellofemoral cartilage lesions. Arthrosc Tech. 2021;10(9): e2181–7.
10. Sherman SL, Humpherys J, Farr J. Optimizing
patellofemoral cartilage restoration and instability
with tibial tubercle osteotomy. Arthroscopy. 2019;35
(8):2255–6.
11. Post WR, Teitge R, Amis A. Patellofemoral
malalignment: looking beyond the viewbox. Clin
Sports Med. 2002;21(3):521–46.
12. Merchant AC, Fraiser R, Dragoo J, Fredericson M.
A reliable Q angle measurement using a standardized
protocol. Knee. 2020;27(3):934–9.
13. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc.
1994;2(1):19–26.
14. Kuroda R, Kambic H, Valdevit A, Andrish J. Distribution of patellofemoral joint pressures after femoral
trochlear osteotomy. Knee Surg Sports Traumatol
Arthrosc. 2002;10(1):33–7.
15. Elias JJ, Soehnlen NT, Guseila LM, Cosgarea AJ. Dynamic tracking influenced by anatomy
in patellar instability. Knee. 2016;23(3):450–5.
16. Seitlinger G, Scheurecker G, Högler R, Labey L,
Innocenti B, Hofmann S. Tibial tubercle-posterior
cruciate ligament distance: a new measurement to
define the position of the tibial tubercle in patients
554
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
A. Gudeman and J. Farr
with patellar dislocation. Am J Sports Med. 2012;40
(5):1119–25.
Daynes J, Hinckel BB, Farr J. Tibial tuberosityposterior cruciate ligament distance. J Knee Surg.
2016;29(6):471–7.
Schoettle PB, Zanetti M, Seifert B, Pfirrmann CW,
Fucentese SF, Romero J. The tibial tuberosity-trochlear
groove distance; a comparative study between CT and
MRI scanning. Knee. 2006;13(1):26–31.
International Patellofemoral Study Group 2006 Massachusetts Boston.
Franciozi CE, Ambra LF, Albertoni LJB, et al.
Anteromedial tibial tubercle osteotomy improves
results of medial patellofemoral ligament reconstruction for recurrent patellar instability in patients with
tibial tuberosity-trochlear groove distance of 17 to 20
mm. Arthroscopy. 2019;35(2):566–74.
Heidenreich MJ, Camp CL, Dahm DL, Stuart MJ,
Levy BA, Krych AJ. The contribution of the tibial
tubercle to patellar instability: analysis of tibial
tubercle-trochlear groove (TT-TG) and tibial
tubercle-posterior cruciate ligament (TT-PCL) distances. Knee Surg Sports Traumatol Arthrosc.
2017;25(8):2347–51.
Xu Z, Zhang H, Yan W, Qiu M, Zhang J, Zhou A.
Validating the role of tibial tubercle-posterior cruciate ligament distance and tibial tubercle-trochlear
groove distance measured by magnetic resonance
imaging in patients with patellar dislocation: a
diagnostic study. Arthroscopy. 2021;37(1):234–42.
Brady JM, Rosencrans AS, Shubin Stein BE. Use of
TT-PCL versus TT-TG. Curr Rev Musculoskelet
Med. 2018;11(2):261–5.
Pidoriano AJ, Weinstein RN, Buuck DA, Fulkerson JP. Correlation of patellar articular lesions with
results from anteromedial tibial tubercle transfer.
Am J Sports Med. 1997;25(4):533–7.
Pritsch T, Haim A, Arbel R, Snir N, Shasha N, Dekel S.
Tailored tibial tubercle transfer for patellofemoral
malalignment: analysis of clinical outcomes. Knee Surg
Sports Traumatol Arthrosc. 2007;15(8):994–1002.
Burger D, Feucht M, Muench LN, Forkel P,
Imhoff AB, Mehl J. Good clinical outcomes after
patellar cartilage repair with no evidence for inferior
results in complex cases with the need for additional
patellofemoral realignment procedures: a systematic
review. Knee Surg Sports Traumatol Arthrosc.
https://doi.org/10.1007/s00167-021-06728-z.
Zarkadis NJ, Belmont PJ, Zachilli MA, Holland CA,
Kinsler AR, Todd MS, et al. Autologous chondrocyte
implantation and tibial tubercle osteotomy for
patellofemoral chondral defects: improved pain relief
and occupational outcomes among US army servicemembers. Am J Sports Med. 2018;46(13):3198–208.
Buuck DA, Fulkerson JP. Anteromedialization of the
tibialtubercle: A 4-to 12-year follow-up. Op Tech
Sports Med. 2000;8(2):131–7.
29. Teitge RA. Patellofemoral syndrome a paradigm for
current surgical strategies. Orthop Clin North Am.
2008;39(3):287–311.
30. Liu JN, Mintz DN, Nguyen JT, Brady JM, Strickland SM, Shubin Stein BE. Magnetic resonance
imaging validation of tibial tubercle transfer distance
in the fulkerson osteotomy: a clinical and cadaveric
study. Arthroscopy. 2018;34(1):189–97.
31. Biedert RM, Friederich NF. Failed lateral retinacular
release: clinical outcome. J Sports Traumatol Rel
Res. 1994;16(4):162–73.
32. Merkely G, Ackermann J, Sheehy E, Gomoll AH.
Does flipping the tubercle for improved cartilage
repair exposure increase the risk for Arthrofibrosis.
Cartilage. 2021;13(1_suppl):311S-317S.
33. Johnson AA, Wolfe EL, Mintz DN, Demehri S,
Shubin Stein BE, Cosgarea AJ. Complications after
tibial tuberosity osteotomy: association with screw
size and concomitant distalization. Orthop J Sports
Med. 2018;6(10):2325967118803614.
34. Fulkerson JP. Fracture of the proximal tibia after
Fulkerson anteromedial tibial tubercle transfer. A report of four cases. Am J Sports Med. 1999;27(2):265.
35. Payne J, Rimmke N, Schmitt LC, Flanigan DC,
Magnussen RA. The incidence of complications of
tibial tubercle osteotomy: a systematic review.
Arthroscopy. 2015;31(9):1819–25.
36. Kline AJ, Gonzales J, Beach WR, Miller MD.
Vascular risk associated with bicortical tibial drilling
during anteromedial tibial tubercle transfer. Am J
Orthop (Belle Mead NJ). 2006;35(1):30–2.
37. Agarwalla A, Gowd AK, Liu JN, et al. Concomitant
medial patellofemoral ligament reconstruction and
tibial tubercle osteotomy do not increase the incidence of 30-day complications: an analysis of the
NSQIP database. Orthop J Sports Med. 2019;7
(4):2325967119837639.
38. Chatterji R, White AE, Hadley CJ, Cohen SB,
Freedman KB, Dodson CC. Return-to-play guidelines after patellar instability surgery requiring bony
realignment: a systematic review. Orthop J Sports
Med. 2020;8(12):2325967120966134.
39. Cameron HU, Huffer B, Cameron GM. Anteromedial
displacement of the tibial tubercle for patellofemoral
arthralgia. Can J of Surg. 1986;29(6):456–8.
40. Fulkerson JP, Becker GJ, Meaney JA, Miranda M,
Folcik MA. Anteromedial tibial tubercle transfer without bone graft. Am J Sports Med. 1990;18(5):490–6.
41. Sakai N, Koshino T, Okamoto R. Pain reduction after
anteromedial displacement of the tibial tuberosity: 5year follow-up in 21 knees with patellofomoral
arthrosis. Acta Orthop Scand. 1996;67(1):13–5.
42. Bellemans J, Cauwenberghs F, Witvrouw E, Brys P,
Victor J. Anteromedial tibial tubercle transfer in
patients with chronic anterior knee pain and a
subluxation-type patellar malalignment. Am J Sports
Med. 1997;25(3):375–81.
Rotational Osteotomy. Principles,
Surgical Technique, Outcomes
and Complications
Vicente Sanchis-Alfonso, Alejandro Roselló-Añón,
Cristina Ramírez-Fuentes,
and Robert A. Teitge
1
Introduction
There is growing evidence that increased external
tibial torsion and femoral anteversion (FAV) play
a major role in the genesis of anterior knee pain
(AKP) and patellar instability (PI) [1–26]. Torsional abnormalities can provoke an increment in
patellofemoral contact pressure that may result in
patellar cartilage damage, patellofemoral
osteoarthritis and patellar subluxation or dislocation [7, 11, 21, 27, 28]. Therefore, torsional
abnormality is a relevant clinical issue given that
it might contribute to the development of knee
osteoarthritis. Diederichs and colleagues have
recently analyzed rotational limb alignment in
patients with non-traumatic PI and in controls
using magnetic resonance imaging (MRI) [29].
They found that PI patients have greater internal
femoral rotation, greater knee rotation and more
of a tendency to genu valgum when compared
with healthy controls. However, those authors
did not find significant differences in tibial tor-
V. Sanchis-Alfonso (&) A. Roselló-Añón
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
C. Ramírez-Fuentes
Medical Imaging Department, Hospital Universitario
y Politecnico La Fe, Valencia, Spain
R. A. Teitge
Wayne State University, Detroit, MI, USA
sion in PI patients in comparison with the control
group. They concluded that rotational malalignment may be a primary risk factor in PI that has
so far been underestimated. The authors also
concluded that a concomitant rotational femoral
osteotomy should be considered along with
medial patellofemoral ligament reconstruction
(MPFLr) if increased FAV is present. Moreover,
it has been demonstrated that rotational osteotomy is a beneficial treatment for those patients as
good clinical results have been reported [1–6, 8–
10, 12–20, 22–26]. The objective of this chapter
is to present, in detail, how we perform a rotational osteotomy on both the tibia and femur
along with an analysis of the outcomes and
complications.
2
Principles of Rotational
Osteotomy Surgery
– Torsion of a long bone is the physiological
rotation of the bone on its longitudinal axis. It
is defined as the degree of twist between two
axes, one proximal and one distal (Fig. 1).
The range of normal values is broad for both
femoral and tibial torsion [30, 31]. Moreover,
there are differences between different ethnic
groups [32]. Our normal reference values are
a FAV of 13º for both sexes and 21º of
external tibial torsion in males and 27º in
females [33, 34]. Our preferred method to
measure femoral torsion is the one described
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_39
555
556
V. Sanchis-Alfonso et al.
only correct the transverse deformity in these
cases, not the coronal one (Fig. 2).
– An asymptomatic torsional abnormality
should never be corrected. Correction for
cosmetic reasons is contraindicated. We must
only correct symptomatic cases. However, the
problem is that we do not have scientific
evidence to tell us from which torsional
angles we should make a surgical correction
of the torsional abnormality in cases where
there are symptoms. Furthermore, the etiology
of pain is multifactorial. Moreover, we do not
know to what degree the torsional alteration
contributes to the magnitude of pain. This
might be why rotational osteotomy is not a
common operation.
– The selection of the level of the osteotomy is
the surgeon’s choice. There is no scientific
evidence to support decisions regarding the
level of osteotomy. Rotational osteotomy may
be performed, in theory, anywhere between
the reference lines used to measure torsional
abnormality. Osteotomies at different levels
would have the same effect on overall version.
However, we must note that healing in the
metaphyseal area is excellent and fast,
whereas healing in the diaphyseal region
Fig. 1 Planes defining femoral anteversion
by Murphy and colleagues in 1987 [35].
Regarding tibial torsion, our preferred method
is the one described by Yoshioka and colleagues in 1989 [34].
– An erroneous start makes for an erroneous
finish. Therefore, we must avoid an erroneous
diagnosis, because it will lead us to an error in
treatment, and we will cause iatrogenesis. In
many cases, pathological external tibial torsion is associated with knee varus (Fig. 2).
However, this varus is not real in most cases.
It reflects the tibial torsion. That is why we
speak about “pseudo-varus.” Obviously, we
can see varus correction after isolated internal
tibial rotational osteotomy. In the same way,
we can observe a “pseudo-valgus” in patients
with pathological FAV. Evidently, we must
Fig. 2 Left pseudo-varus in a A
patient with external tibial
torsion (A). Observe varus
correction after isolated
internal tibial rotational
osteotomy (B). In the same
way, we can observe a
“pseudo-valgus” in patients
with pathological FAV.
A true AP standing
radiograph shows a normal
mechanical axis (C).
(Figure C—Courtesy of
Robert A. Teitge, MD)
B
C
Rotational Osteotomy. Principles, Surgical Technique …
requires more time. The difference between
the two would be a point in favor of performing the osteotomy in the metaphyseal
region. Then again, the osteotomy should
theoretically be located in the osseous segment that mainly contributes to the deformity.
If done in that way, it would prevent the
creation of a new deformity on the coronal or
sagittal plane in spite of the fact that good
correction of the total torsional angle can be
obtained [36].
– Regarding FAV, both the femoral neck and
the diaphysis have an overall influence on
femoral torsion [36–38]. Archibald and colleagues [36] evaluated 1210 paired adult
femora from a well-preserved osteological
collection. They have shown that both the
femoral neck and femoral shaft substantially
contribute to femoral version. Seitlinger and
colleagues [37] have demonstrated that the
neck, mid and distal femur contribute to the
total femoral torsion. Sanchis-Alfonso and
colleagues [38] have shown that pathological
FAV in the AKP patient depends on both the
neck and the shaft. In those patients, the
increased anteversion of the femur is a result
of increased proximal anteversion of the
neck and reduced torsion of the diaphysis in
the opposite direction [38]. The version angle
of the neck and the diaphysis cannot separately explain the total FAV because it is a
global torsional deformity that involves the
entire femur. A strong negative correlation
between neck torsion and shaft counter
direction torsion has been found [38]. It suggests that the shaft version acts as a compensatory mechanism for the increased
version of the neck, and this compensatory
mechanism fails in pathological cases. They
have shown that the difference in total FAV
between healthy and pathological subjects is
due in 40% to the higher version of the neck
in the pathological group, and in 60% to the
decreased diaphyseal rotation in the opposite
direction [38]. Moreover, they observed that
shaft version values better explain the phenomenon of pathological FAV since the values of shaft version are less dispersed and
557
better fit the linear model than those of the
neck. However, the fact that the diaphysis
only explains 12% of the variability of the
total FAV angle in the linear regression
analysis performed in the pathological
group indicates that its influence on the total
FAV is not important enough to unequivocally recommend that the osteotomy be performed distal to the lesser trochanter [38].
Therefore, we must look for other arguments
to opt for an intertrochanteric or a diaphyseal
osteotomy to treat pathological FAV in AKP
patients. Our preferred options for the rotational osteotomy of the femur are at the
(1) intertrochanteric level and the (2) supracondylar level. In cases of an isolated transverse plane correction, the proximal
intertrochanteric osteotomy is our choice
because it prevents damage to and scarring in
the distal quadriceps avoiding the risk of knee
stiffness. Rotational osteotomy is the most
effective treatment for the AKP patient with
pathological FAV. It is well-known that the
quadriceps, is responsible for the force exerted on the patella. The osteotomy changes the
direction of the quadriceps and therefore the
force acting on the patella. This could be
another argument for an intertrochanteric
femoral osteotomy. However, if there is a
malalignment on the coronal plane that must
be addressed, our choice is a supracondylar
femoral osteotomy. On the other hand, Kim
and colleagues [39] showed that femoral torsion could occur either in the supratrochanteric region, the infratrochanteric
region, or in both sites. However, Waisbrod
and colleagues [40] have proposed that
femoral torsion is a subtrochanteric deformity.
– As with the femoral osteotomy, the tibial
rotational osteotomy has also been performed
at every level. In terms of the rotational
osteotomy of the tibia, our preference is the
infratuberosity osteotomy. On the other hand,
other orthopedic surgeons suggest a supratuberosity osteotomy. Yet again, there are
others who are inclined toward a mid-shaft or
distal (supramalleolar) osteotomy. We must
note that an osteotomy below the tuberosity
558
has poorer consolidation than one done above
the tuberosity even though it allows for good
fixation. We will do our best to explain our
option. Osteotomies above the tuberosity lead
to medial or lateral tuberosity displacement.
That is why it may be necessary to add a tibial
tubercle osteotomy if a supratuberosity
osteotomy is performed. However, the
infratuberosity osteotomy does not provoke
tuberosity translation. For example, in the
patient in Fig. 3 with a TT-TG distance of
14 mm, a 35º supra-tuberosity osteotomy will
produce a tuberosity medialization of 11.4 mm
that will provoke a postop TT-TG distance of
2.54 mm. That TT-TG distance is obviously
pathological given that normal TT-TG distance is from 10 to 15 mm. If we place the
osteotomy above the tubercle, we will move it
medially. Doing so will create joint imbalance.
Kuroda and colleagues [41] have demonstrated
that a medial tuberosity transfer from the normal position provokes an increase in medial
tibiofemoral compartment pressure and medial
patellofemoral pressure that theoretically leads
to medial compartment osteoarthritis, degenerative tears of the medial meniscus, and
medial patellofemoral osteoarthritis. Another
argument for the infratuberosity osteotomy is
that the goal of osteotomy is to realign the knee
joint axis with the ankle joint axis on the
transverse plane, leaving the TT untouched.
We must note that we should only medialize an
V. Sanchis-Alfonso et al.
–
–
–
–
Fig. 3 Calculation of tuberosity medialization after a
rotational tibial osteotomy
actual lateral placement of the TT on the
proximal tibia. Recently, Winkler and colleagues [42] have shown that increased external tibial torsion is an infratuberositary
deformity and is not correlated with a lateralized position of the tibial tuberosity.
There is no scientific evidence as to the
amount of torsion we should correct in a
patient with a symptomatic torsional abnormality. In our experience, undercorrecting is
better than overcorrecting. The objective is a
correction that is slightly less than what a
torsion measurement might indicate. For
example, the aim should be an external
femoral rotation of 30° but not more
(49 − 30 = 19) if a patient has a femoral
anteversion of 49°. For an external tibial torsion of 60°, we would propose an internal
rotational osteotomy of 30° (60 − 30 = 30).
But again, we do not know what minimum
correction is necessary for the surgery to be
successful. This might be another reason why
rotational osteotomy is not a common
operation.
The surgeon may select any internal (or
external) fixation device which allows for
maintaining the correction. Therefore, the
selection of the fixation device is also a surgeon´s choice.
The objectives of rotational osteotomy are:
(1) the correction of the deformity, (2) rapid
bone consolidation, (3) minimal soft-tissue
injury, (3) no restrictions in terms of range-ofmotion, and (4) immediate muscular
activation.
Changing the limb alignment by means of
osteotomy is the single most powerful and
underutilized treatment available for treating
AKP and PI patients with a pathological torsional abnormality. The quadriceps is
responsible for the force acting on the patella.
The osteotomy changes the quadriceps direction and therefore the force acting on the
patella. If one operates on the traumatized
tissue (bone, ligament or cartilage) without
changing the force which produced the
trauma, one should expect an unsuccessful
outcome.
Rotational Osteotomy. Principles, Surgical Technique …
3
Rotational Osteotomy. Surgical
Techniques Step-by-Step. Pearls
and Tips
3.1 Rotational Osteotomy
of the Tibia
3.1.1 Positioning
The patient is placed in the supine position on a
radiolucent table. The entire limb is draped from
the foot to the iliac crest. In that way, we can
look at the entire limb after correction. A tourniquet is not used. The image intensifier is placed
on the opposite side to the operated limb. The
knee is slightly flexed on a towel roll.
3.1.2 Surgical Approach
It proceeds with an anterolateral curved
approach. The fascia of the tibialis anterior is
sectioned longitudinally 1 cm lateral to the tibial
attachment for it to be reattached later. The
proximal tibialis anterior muscle is detached to
expose the proximal lateral tibia. If a fibular
osteotomy and release of the peroneal nerve is
necessary, the surgical incision is extended
proximally in a similar way to the incision used
in the reconstruction of the posterolateral corner
ligaments. Soft tissues are removed from the tibia
with a curved raspatory. The plate is positioned
A
B
Fig. 4 K-wire that help us to position the plate once the
osteotomy has been performed (1); K-wires marking the
osteotomy level (2) (A). K-wires at the desired correction
559
under the image intensifier on top of the lateral
tibia to evaluate the correct position. We insert a
K-wire if the position of the plate is correct. This
K-wire will aid in positioning the plate once the
osteotomy has been performed (Fig. 4A).
3.1.3 Fibular Osteotomy and Peroneal
Nerve Release
Like other authors, we perform a fibular osteotomy and peroneal nerve release when the rotational osteotomy of the tibia is going to be
greater than 20º [43]. We never perform a release
of the proximal tibiofibular joint. The fibular
osteotomy is recommended before making the
tibial rotation for two reasons. The first reason is
that the fibula limits internal rotation of the tibia.
The second is that the fibula pulls on the proximal and distal tibio-fibular capsule, which could
be painful. A long proximal oblique cut of the
fibula is recommended because it provides a
larger surface contact area between both segments of the bone, making healing easier. Note
that the peroneal nerve is at risk during a fibular
neck osteotomy. Therefore, the nerve must be
protected by using two hallux retractors around
the neck of the fibula while doing the osteotomy
with a small saw. Moreover, peroneal nerve
palsy, might be secondary to overextension of
the nerve due to internal tibial rotation (Fig. 5).
C
angle (3), using a triangle of 25° (B). The distal segment
of the tibia is de-rotated internally until both K-wires are
parallel (C)
560
V. Sanchis-Alfonso et al.
A
B
Fig. 5 Peroneal nerve (arrows) before internal rotation of the distal segment of the tibia (A). Overextension of the
nerve due to internal rotation of the distal segment of the tibia (B)
3.1.4 Tibial Osteotomy
The osteotomy plane must be perpendicular to
the mechanical axis of the lower limb. A long rod
(DePuy Synthes) is used to define the mechanical
axis intraoperatively. To make the cut perpendicular to the mechanical axis on both the
anteroposterior and sagittal planes, two K-wires
that will serve as a guide are used (Fig. 4A).
These K-wires are positioned under the image
intensifier viewer. Prior to the tibial osteotomy,
two threaded K-wires inserted bicortically are put
in place. One is placed perpendicular to the
proximal tibia and proximal to the plane of
osteotomy and the other one distal to the plane of
osteotomy at the desired correction angle
(Fig. 4A, B) using triangular measuring templates (Fig. 4B). Moreover, an iPhone app called
“angle meter” might be used to estimate the
angle of correction instead of triangular templates (Fig. 6). Saw 3D printed surgical guides
are not routinely used.They might improve surgical accuracy.
After that, we perform the osteotomy below
the tibial tuberosity. The cut of the osteotomy,
from lateral to medial, is performed using
0.6 mm thick saw blades under image intensification. If the saw blades employed in prosthetic
surgery are used, which are thicker (1.2 mm), the
control we have over the saw is decreased.
Therefore, the cut is less precise. Moreover, there
is more trauma to the bone and more heat is
generated with a thicker saw blade. This might
affect bone healing. A Hohmann retractor placed
Fig. 6 An iPhone app called “angle meter” might be used
to estimate the angle of correction
behind the tibia is used to protect the neurovascular bundle. It is necessary a complete circumferential soft tissue release to obtain an
unrestricted correction. After that, the distal
segment of the tibia is de-rotated internally until
both K-wires are parallel (Fig. 4C), and the
correction is checked. The osteotomy can be
stabilized temporarily, prior to the fixation of the
plate, using reduction forceps or K-wires.
The varus in patients with external tibial
rotation may be real or it may reflect tibial torsion
(pseudo-varus). In most cases, we can see a varus
correction after an isolated internal tibial rotation
osteotomy. Therefore, it is very important to
check whether there is neutral coronal plane
alignment after rotation before fixation by using
the image intensifier. We use the alignment rod
Rotational Osteotomy. Principles, Surgical Technique …
from the center of the femoral head to the center
of the talus to make sure the mechanical axis falls
near the medial tibial spine. A normal mechanical axis is near the medial tibial spine, not in the
middle of the knee joint. The patella must always
be pointing straight forward. In addition, it
should also be in the middle of the distal femur
on the anteroposterior image.
3.1.5 Fixation of the Osteotomy
We use a lateral tomofix plate (DePuy Synthes)
with 3 proximal and 3 distal screws. The plate is
positioned using the K-wire inserted at the
beginning of the procedure (Fig. 4A). This plate
does not fit well, because it is designed for the
valgus tibial osteotomy. Therefore, we usually
bend it so as not to pull the distal fragment into
valgus or leave the plate too far off the lateral
tibial cortex tenting the anterior compartment. In
cases of real varus, tension in the plate to compress the osteotomy pulls the tibia into valgus.
Therefore, no bone cut is necessary to do a corrective valgus osteotomy.
Correction Loss After Fixation—“Incongruity”
is the Problem
If the tibia had a circular section, the plate would
rest completely on the lateral aspect of both bone
segments when making a transverse osteotomy
and rotating the distal segment. However, the
cross section of the tibia is triangular. Therefore,
the anterolateral aspect of the proximal segment
of the tibia will be on a different plane than the
anterolateral aspect of the distal segment when
rotating the distal segment about the proximal
one after a transverse osteotomy. When positioning the plate, it only rests fully on the proximal segment. When we fix the distal part of the
plate using bicortical screws, there will be a loss
of correction.
“Incongruity” is to blame for correction loss
after fixation. A cortical screw permits compression of the focus of the osteotomy as it is
screwed into an oval plate hole eccentrically
(absolute stability). But the cortical screw, in
addition to compressing the focus of osteotomy,
also compresses the bone on the plate. That is, it
561
A
B
Fig. 7 Plate resting on the lateral aspect of the tibia after
rotational tibial osteotomy (A). Rotational tibial osteotomy smoothing the cortex of the proximal segment (B)
attracts the bone to the plate. Therefore, we will
bring the bone that was separated towards the
plate as we tighten the screw, losing correction.
How to Avoid the Correction Loss
There are three ways to avoid the loss of correction. This is done by using plate-threaded
screws in the part of the plate distal to the
osteotomy site. In this way, there is no compression of the focus of the osteotomy and all the
tension is supported by the plate (relative stability). Similarly, we do not attract the bone to
the plate as we squeeze it. Another way to avoid
the loss of correction would be by smoothing the
cortex of the proximal segment (Fig. 7). A third
way, using bicortical screws, would be to fill the
space between the bone and the plate with a
supplement and not remove it. If it is also
biodegradable, it can serve its purpose of facilitating the construction of an assembly with
absolute stability and compression of the
osteotomy focus until the osteotomy consolidates
and can then be resorbed. Custom supplements
could be designed with PLA (polylactic acid) and
3-D printed.
3.1.6 Closure
We always use a drain over 24 hours to reduce
the risk of hematoma and compartment syndrome. The fascia of the tibialis anterior muscle
562
is reattached, covering the plate if it is possible. If
the anterior compartment is very tight, we leave
the fascia open. It is not a problem.
3.1.7 Postoperative Management
We encourage active ankle and knee motion
immediately after surgery. We use CPM in the
hospital and at home if it is possible. The patient
uses crutches to prevent bearing weight with the
operated leg. Loading is permitted after 6 weeks.
3.2 Rotational Osteotomy
of the Proximal Fermur
3.2.1 Positioning
The patient is placed in the supine position on a
fracture table holding both legs under controlled
traction (Fig. 8). Abduct the unaffected lower
limb as much as possible to permit fluoroscopic
examination using an image intensifier (Fig. 8).
V. Sanchis-Alfonso et al.
3.2.2 Lateral Approach to the Proximal
Femur
A lateral longitudinal incision is made over the
hip. We locate the lesser trochanter with image
intensifier. The incision is made at the level of
the lesser trochanter, centered on the shaft and is
then prolonged proximally and distally. The
fascia lata is incised with a scalpel and split with
scissors. The vastus lateralis is separated by blunt
dissection from the fascia lata and then elevated
anteriorly. The perforating vessels must be ligated. Finally, the proximal femoral shaft is
exposed.
To expose the femur without sectioning the
muscle fibers of the vastus lateralis, the hiatus
must be located distal to the insertion of the
vastus lateralis on the lateral aspect of the greater
trochanter. This is done by means of blunt dissection with the finger. The inferior border of the
vastus lateralis is palpated until a space is found.
That makes for the passage of the finger towards
the anterior aspect of the femur. In this hiatus, a
Hoffman retractor will be placed to fold the
vastus lateralis anteriorly and expose the diaphysis (Fig. 9). To improve access, part of the
insertion of the vastus lateralis on the lateral
greater trochanteric aspect can be sectioned with
electrocautery when tensioned with a Hoffman
retractor.
3.2.3 Femoral Osteotomy
The plate is positioned under the image intensifier on the lateral proximal femur to evaluate the
correct position. If the position of the plate is
correct, we insert 2 K-wires. These K-wires aid
Fig. 8 Patient positioning for performing a rotational
osteotomy of the proximal femur
Fig. 9 Hiatus located distal to the insertion of the vastus
lateralis on the lateral aspect of the greater trochanter
Rotational Osteotomy. Principles, Surgical Technique …
563
Fig. 10 If the position of the plate is correct, we insert
2 K-wires (1) (2). These K-wires will help us to position
the plate once the osteotomy has been performed. K-wire
marking the osteotomy site (5). K-wires for performing
the rotational correction (3) (4)
in positioning the plate once the osteotomy has
been performed (Figs. 10 and 11).
After marking the osteotomy level with a Kwire (Figs. 10 and 11), two threaded K-wires are
inserted at an angle equal to the desired rotational
correction. One is put in place proximal and the
other distal to the osteotomy site (Figs. 11 and
12) using triangular measuring templates
(Fig. 12).
The cut of the osteotomy is performed using
0.6 mm thick saw blades under image intensification from lateral to medial while protecting soft
tissues with two Hohmann retractors. The C-arm
is used to confirm that the cut is perpendicular to
the shaft of the femur. After the osteotomy is
complete, external rotation of the distal fragment
is performed until both K-wires are parallel,
which indicates that the planned correction has
been achieved (Fig. 12). We can use reduction
forceps for temporary stabilization of the
osteotomy prior to the insertion of the plate
(Fig. 12). Another way to stabilize the osteotomy
is with K-wires.
Danger
The magnitude of the rotational osteotomy does
not show a 1:1 relationship with an effect on the
correction of the deformity in all the cases. Not
only does 3D technology permit measuring the
femoral torsion (see chapter “Femoral and Tibial
Rotational Abnormalities are the Most Ignored
Factors in the Diagnosis and Treatment of
Anterior Knee Pain Patients. A Critical Analysis
Review”), but also to quantify the effect of the
osteotomy on the femoral torsion after the planned osteotomy. In other words, it allows us to
564
V. Sanchis-Alfonso et al.
Fig. 11 Two K-wires (1) (2) will help us to position the plate once the osteotomy has been performed. K-wire marking
the osteotomy site (5). K-wires for performing the rotational correction (3) (4)
A
B
D
Fig. 12 Two threaded K-wires (3, 4) are inserted at an
angle equal to the desired rotational correction (A). One is
put in place proximal and the other distal to the osteotomy
site using triangular measuring templates (B, C). K-wire
marking the osteotomy site (5) (A). K-wires for
C
E
performing rotational correction (3) (4) (A, B, C, D).
Triangular measuring template (B, C). Stabilization using
reduction forceps (D). K-wires (3) (4) are parallel after the
planned correction has been achieved (D, E)
Rotational Osteotomy. Principles, Surgical Technique …
estimate the final effect of the derotational
femoral osteotomy (see Video Case # 1).
3.2.4 Fixation of the Osteotomy,
Closure and Postoperative
Management
We use a proximal femoral locking compression
plate (LCP) 4.5/5.0 (DePuy Synthes). The plate is
positioned using the K-wires inserted at the
beginning of the procedure (Figs. 10 and 11). We
always use a drain to reduce risk of hematoma.
Active hip, knee, and ankle motion immediately
after surgery is encouraged. The patient uses
crutches to prevent bearing weight with the
operated leg. Loading is permitted after 6 weeks.
3.3 Rotational Supracondylar
Femoral Osteotomy
3.3.1 Positioning
The patient is placed in supine position on a
radiolucent table. The entire limb is draped from
the foot to the iliac crest. Therefore, we can look
at the entire limb after correction. A tourniquet is
not used. The C-arm is placed on the contralateral side of the operated limb to assess the whole
lower limb in order to evaluate the alignment on
the frontal plane. It must be acknowledged that in
many cases there is a valgus associated with
transverse plane malalignment and therefore is
mandatory preop and postop evaluation in the
coronal plane.
3.3.2 Surgical Approach
The distal approach to the femur can be medial or
lateral. We do the lateral because this type of
surgery is done on patients with instability and
associated femoral anteversion. If an MPFLr is
associated with the osteotomy, the lateral
approach is better than the medial, because there
may be problems in achieving ideal femoral
anchoring of the MPFL if a plate is placed on the
medial aspect of the femur.
565
A standard lateral longitudinal incision is
performed, the iliotibial band is incised following
the fiber orientation and the vastus lateralis is
separated by blunt dissection from the fascia lata
and then elevated anteriorly. The septum intermusculare is detached from the femur at the level
of the osteotomy with a curved raspatory.
3.3.3 Femoral Osteotomy
After defining the osteotomy level on the femur
with a K-wire perpendicular to the mechanical
axis of the lower extremity, we insert two
threaded K-wires at an angle equal to the desired
rotational correction. One is put in place proximal and one distal to the osteotomy site using
triangular measuring templates. If the osteotomy
is not perpendicular to the mechanical axis of the
femur, it is possible to modify the mechanical
axis on the coronal plane. The osteotomy is
performed using an oscillating saw (0.6 mm
thick) while protecting posterior neurovascular
structures with two Hohmann retractors. After
the osteotomy is complete, external rotation of
the distal fragment is performed until both Kwires are parallel, which indicates that the planned correction has been achieved.
It is very important to check whether there is
neutral coronal plane alignment after rotation
before fixation by using the image intensifier
(Fig. 13). We use the alignment rod from the center
of the femoral head to the center of the talus to make
sure the mechanical axis falls near the medial tibial
spine. A normal mechanical axis is near the medial
tibial spine, not in the middle of the knee joint. The
patella must always be pointing straight forward. In
addition, it should also be in the middle of the distal
femur on the anteroposterior image.
Technical Considerations when an MPFLr is
Associated
The osteotomy must be carefully planned so that
the distal end of the plate is located proximally to
the MPFL femoral attachment point if a plate is
placed on the medial aspect of the femur. In
566
V. Sanchis-Alfonso et al.
Fig. 13 Evaluation of coronal plane alignment after rotation
addition, the direction of the femoral tunnel must
be evaluated by means of fluoroscopy to avoid
collision with the screws of the plate.
3.3.4 Fixation of the Osteotomy,
Closure and Postoperative
Management
We use a distal femoral lateral TomoFix plate
(DePuySynthes). However, other plates can as
well be used. We always use a drain to reduce
risk of hematoma. We also encourage active
ankle and knee motion immediately. We use
CPM in the hospital and at home if it is possible. The patient uses crutches to prevent
weightbearing on the operated leg. Loading is
permitted after 6 weeks.
4
Case Examples
CASE # 1 - SYMPTOMATIC EXCESSIVE FEMORAL
ANTEVERSION AND IN-TOEING GAIT. ROTATIONAL
OSTEOTOMY OF THE PROXIMALFERMUR
(INTERTROCHANTERIC OSTEOTOMY)
18 y/o female gymnast with severe right hip pain
and severe right AKP for 3 years, both recalcitrant to conservative treatment (NSAIDS and
Physical Therapy). AKP appeared several
months after hip pain. The contralateral side was
completely asymptomatic. There was a significant worsening in the last year.
Rotational Osteotomy. Principles, Surgical Technique …
BMI: 18.78 (1.68–53 kg). Knee VAS 7.
Hip VAS 8. Kujala score 86/100. IKDC
78.2/100. NAHS 77.5/100. Marx Activity Rating
Scale 15/16–Rhythmic gymnastics. HAD: Anxiety 2/21–Depression 1/21–(Cutting point 11;
no anxiety, no depression). Tampa Scale for
Kinesiophobia 34/68 (Cutting point 40; no
kinesiophobia). Pain Catastrophizing Scale
(PCS) 36/52 (Cutting point 24; catastrophizing). EuroQol-5D 0.429/1.
Conventional imaging studies normal or at
least without evident pathology. CT: TT-TG
distance: right 17 mm, left 18 mm; Patellar tilt:
right 20º, left 12º.
The presence of severe pain (VAS 7), absence
of objective structural anomalies in the knee,
absence of disability most of the time (Kujala 86,
IKDC 78.2) and the presence of psychological
problems (catastrophizing) is an explosive mixture that leads other people to believe the person
is mad. This patient had made 17 visits to the
emergency unit of the hospital in the year prior to
surgery due to severe pain. There were many
normal imaging studies. The doctors said that she
was a “somatizer”. However, nobody had ever
told her to undress to see her lower limbs while
she was standing straight up. In Fig. 14A, B, C,
you can see her legs. In the right one, one can
clearly see a squinting patella, a tibia varus, a
genu recurvatum and pronated foot. In this case,
there is an evident asymmetry. It seems clear that
there is abnormal torsion. From a clinical standpoint, there clearly is right femoral anteversion
given that internal rotation of the right hip
exceeds external rotation by more than 30º in
prone position (Fig. 15). Moreover, there was a
gait pattern with an internal foot progression
angle (i.e., an in-toeing gait). A Torsional CT
scan revealed femoral anteversion based on
Murphy´s method, right 39º and left 15º.
It is our belief that 39º of femoral anteversion
might be enough to cause some posterior
impingement between the neck and acetabulum
when the patient attempts to externally rotate the
limb (Fig. 16). Therefore, the hip muscles will
not work in a balanced fashion. This could justify
the hip pain in this patient. In fact, she had hip
567
pain with external hip rotation. On the other
hand, she had no pain with internal hip rotation.
A 20º external femoral rotation intertrochanteric osteotomy was performed (Fig. 17).
In Figs. 14D, E, F and 18 you can observe
clinical correction of torsional malalignment after
rotational femoral osteotomy. In Fig. 19 you can
see what she is able to do painlessly at the 3month follow-up. At the 6-month follow-up, the
knee VAS was 0 and the hip VAS was 0. Furthermore, there was no catastrophizing, no disability and the patient was leading a normal life.
At the 4-year follow-up, she was completely
asymptomatic, and the physical examination was
completely normal.
CASE # 2 -SYMPTOMATIC EXCESSIVE EXTERNAL
TIBIAL TORSION AND OUT-TOEING GAIT –
INFRATUBEROSITY ROTATIONAL OSTEOTOMY
OF THE TIBIA
18 y/o female gymnast with severe left AKP
for 2 years recalcitrant to conservative treatment
(NSAIDS and Physical Therapy). “My body is
out of whack!”, were her first words upon visiting my office.
BMI: 18.29. VAS 8. Kujala score 63/100.
IKDC 44.8/100. Marx Activity Rating Scale 1/16
–Before the onset of pain rhythmic gymnastics.
HAD: Anxiety 1/21 – Depression 2/21 – (Cutting
point 11; no anxiety, no depression). Tampa
Scale for Kinesiophobia 40/68 (Cutting point
40; low level of kinesiophobia). Pain Catastrophizing Scale (PCS) 13/52 (Cutting point 24;
no catastrophizing).
During physical examination, we saw a
bilateral squinting patella and tibia varus when
the patient was standing with their feet forward
(Fig. 20). We were also able to discern a correction of both squinting patella and tibia varus
with the legs in external rotation (Fig. 20). In
most cases, the varus is not real but reflects the
tibial torsion (pseudo-varus) (Fig. 20). During
gait, we observed that the left foot was externally
rotated during the swing phase. Therefore, an
internal rotational tibial osteotomy should result
in a neutral foot progression angle during the
stance phase, and that is good. If the foot is
568
V. Sanchis-Alfonso et al.
A
B
C
D
E
F
Fig. 14 Preop physical examination (A, B, C). On the
right side, squinting patella, a tibia varus, a genu
recurvatum and pronated foot can be seen. Postop
physical examination (D, E, F). Clinical correction of
torsional malalignment after intertrochanteric rotational
femoral osteotomy
Rotational Osteotomy. Principles, Surgical Technique …
569
Our option was an internal tibial rotational
osteotomy of 35º just distal to the tibial
tuberosity. Therefore, we have gone from 64º to
29º. Before the tibial osteotomy, a proximal
fibular osteotomy to obtain an easier tibial correction was performed. Moreover, a release of
the peroneal nerve was done to avoid a peroneal
nerve palsy.
However, the 35º of internal rotation planned in
the preop could not be reached. The reason for not
arriving at that degree was that the peroneal nerve
was too tense and flat at 30º and the perineural
vessels disappeared. To avoid nerve damage, we
did not go for the ideal correction. Five years after
surgery the patient was pain-free (VAS 0, Kujala
91, IKDC 95.4, anxiety 1, depression 1, kinesiophobia 24, and catastrophization 4).
5
Fig. 15 Right femoral anteversion. Internal rotation of
the right hip exceeds external rotation by more than 30º
neutral during the swing phase, then internal
rotational osteotomy can result in an in-toeing
gait during the stance phase, and that is not good.
An AP weight-bearing x-ray with the patient
standing with their feet forward demonstrated a
not well-centered patella and tibia varus. However, in the same radiological projection with feet
in external rotation, a well-centered patella and
correction of the tibia varus was seen (Fig. 21).
CT: TT-TG distance: right 13 mm - left 14 mm,
External tibial torsion: right 63º–left 64º,
Femoral anteversion: right 31º–left 30º.
A
B
Clinical Outcomes. Scientific
Evidence
From 1990 to June of 2021, only 22 published
papers in English could be found in which the
association between patellofemoral disorders
(anterior knee pain and patellar instability) in
adolescents and adult young patients and torsional abnormalities of the femur and/or tibia are
analyzed from a clinical point of view [44]. It has
been demonstrated that rotational osteotomy is a
beneficial treatment for those patients as good
clinical results have been reported [1–6, 8–10,
12–20, 22–26] Of the 22 papers, 19 (86%) were
case series (level of evidence IV), 2 (9%) were
cohort studies (level of evidence III) and only 1
C
Fig. 16 Posterior impingement between the neck and acetabulum when the patient attempts to externally rotate the
limb. Normal anteversion (A). Excessive anteversion (B). Excessive anteversion with “in-toeing” (C)
570
A
V. Sanchis-Alfonso et al.
B
Fig. 17 Preoperative position of the patella with respect
to the femur with the knee in extension (A). Position of
the patella with respect to the femur with the knee in
C
extension after the rotational femoral osteotomy. Correct
patellofemoral congruence can be observed (B). X-rays
after an intertrochanteric rotational femoral osteotomy (C)
Fig. 18 Clinical correction
of torsional malalignment
after an intertrochanteric
rotational femoral osteotomy
(5%) was a prospective cohort study (level of
evidence II). An important limitation and source
of bias in these papers is that, in many cases,
rotational osteotomy has been combined with
other surgical procedures like varization of the
femur, tibial tuberosity transfer, MPFLr, lateral
retinaculum release, etc. Therefore, we cannot
know which surgical procedure has been decisively responsible for the improvement in terms
of pain or instability with certainty. Furthermore,
77% of those papers have been published since
2004, the majority being carried out by European
authors. No surprise that what we are looking at
is a surgery that started to take off a relatively
few years ago, especially in Europe.
James, in 1979, presented a comprehensive
review of AKP in which he described the
condition of “miserable malalignment” for the
first time in the medical literature [45]. In other
words, that is increased femoral anteversion and
increased external tibial torsion [45]. In 1995,
James reported on 7 patients with “miserable
malalignment” who had been treated with an
internal rotational tibial osteotomy over an 18year period [2]. Torsional femoral deformity was
considered mild in all those cases, and they had
not been corrected. Subjectively, 85% of the
patients had satisfactory results. Functionally, the
results were good in 4 patients and excellent in 3
[2]. However, the most relevant finding of that
study was that the results do not degrade with
time (average follow-up, 10 years/range, 4–16).
Several years earlier, in 1990, Cooke and colleagues [1] described the internal rotational
Rotational Osteotomy. Principles, Surgical Technique …
571
Fig. 19 3-month follow-up after intertrochanteric rotational femoral osteotomy
proximal tibial osteotomy in 7 patients presenting with AKP. They drew attention to the
inwardly pointing knee as an unrecognized cause
of AKP. The outcomes evaluation after 3 years
of follow-up were excellent. In 1996, Cameron
and Saha [3] drew attention to an underrecognized cause of recurrent patellar dislocation,
which is the pathological external tibial torsion.
They analyzed 17 cases of this type of patients
who had undergone a rotational tibial osteotomy
proximal to the tibial tubercle with a mean
follow-up of 25 months. Some 76% of their
patients had a satisfactory clinical result. Delgado
and colleagues [4] presented 3 cases of double
level osteotomy (femoral and tibial) with a
marked decreased in knee pain. Server and
colleagues [5] evaluated 35 medial rotational
proximal tibial osteotomies performed in 25
patients with chronic disability due to AKP and
PI recalcitrant to conservative treatment in 1996.
The average follow up was of 4.3 years (range
1–8 years). The results were good or excellent in
88.5%, fair in 5.7% and poor in 5.7%. Twentythree patients were satisfied and 2 were not.
It took 8 years for another publication that
analyzed the relationship between patellofemoral
disorders and torsional abnormalities to appear in
the medical literature. In 2004, Bruce and Stevens [6] retrospectively reviewed 14 consecutive
AKP patients (27 limbs with both excessive
femoral anteversion and excessive external tibial
torsion), with a mean follow-up of 5.2 (2–12)
572
A
V. Sanchis-Alfonso et al.
B
Fig. 20 Bilateral squinting patella and tibia varus (A).
Correction of squinting patella and tibia varus with the
legs in external rotation (B). A varus correction after an
isolated internal tibial rotational osteotomy can be
observed on the left limb (C). (Republished with
A
C
permission of AME Publishing Company. From
Sanchis-Alfonso V, et al. Evaluation of anterior knee
pain patient: clinical and radiological assessment including psychological factors. Ann Joint, 3:26, 2018)
B
Fig. 21 X-rays with feet forward (A) and with feet in external rotation (B)
Rotational Osteotomy. Principles, Surgical Technique …
years. They had been treated by means of rotational femoral and tibial osteotomy with satisfactory clinical outcomes. The authors
highlighted that when evaluating AKP patients,
assessing the rotational profiles of the femur and
tibia is essential.
When evaluang paents with patellofemoral
disorders, assessment of the rotaonal profiles
of the femur and bia is prerequisite
In 2009, Paulos and colleagues [8] compared
two surgical techniques in a cohort of patients
with patellar instability and limb malalignment.
In one group, they performed a proximal
realignment associated with a rotational tibial
osteotomy and in the other one was an ElmslieTrillat-Fulkerson proximal–distal realignment.
They concluded that rotational abnormality correction produced significantly better results than
conventional proximal–distal realignment.
In 2014, Drexler and colleagues [12] evaluated 15 knees (12 patients) in which a rotational
tibial osteotomy proximal to the tibial tuberosity
associated with a tibial tubercle transfer was
performed in the face of a diagnosis of recurrent
patella subluxation secondary to excessive
external tibial torsion. The authors showed a
satisfactory clinical outcome at a median followup of 84 months (range 15–156). The high
number of patients with previous failed surgeries
in this series provides some evidence that tibial
tubercle medialization associated with soft tissue
plication is not sufficient to correct PI in patients
with excessive external tibial torsion.
Stevens and colleagues [14], in 2014, analyzed 16 consecutives patients (23 knees) with a
failed knee surgery (tibial tubercle osteotomy in
12 knees and arthroscopic debridement in 9)
before which a femoral or tibial torsional
abnormality was recognized and subsequently
treated by means of rotational osteotomy. They
demonstrated clinical improvement after osteotomies of the femur and/or tibia in those patients.
The authors stated that many orthopedic surgeons only focus on the knee when they see an
AKP patient. Torsional abnormalities often go
573
unrecognized. Those authors observed that
addressing rotational abnormalities in the index
surgery provides better clinical results than
osteotomies performed after previous knee
surgeries for treating AKP and/or PI.
Tibial tubercle medializaon is not sufficient to
correct AKP and/or patellar instability in
paents with torsional abnormalies
Just as the papers published on osteotomies
carried out up to 2014 focused on the tibial
osteotomy in most of the cases, most publications since 2014 are above all on the femoral
osteotomy indicated to treat patellar instability.
In 2015, Nelitz and colleagues [15] evaluated
12 consecutive PI patients (12 knees) with
pathological femoral anteversion that had undergone an anatomical MPFLr associated with
rotational femoral osteotomy. The average
follow-up after surgery was 16.4 months (range,
12–28 months). There were no redislocations of
the patella, and there were significant improvements in the Kujala score, IKDC score and VAS.
However, there were no statistically significant
changes in the activity level according to the
Tegner activity score. That finding was explained
by the fact that patients are aware that the risk of a
new dislocation is greater if they practice contact
sports. For that reason, they voluntarily reduced
their sports practice. Dickschas and colleagues
evaluated 35 rotational femoral osteotomies in 25
patients with AKP and/or PI in 2015 [16]. The
average follow-up was of 41 months (range 6–
113). No re-dislocation occurred during the
follow-up. Using the VAS, pain was significantly
reduced (from 5.6 to 2.4). Moreover, the functional scores (Lysholm and Japanese Knee Society score) improved significantly (Lysholm from
66 to 84 and Japanese from 73 to 87). However,
the Tegner activity score did not show significant
changes in the postop.
In 2017, Dickschas and colleagues [17] published a series of 49 supratuberositary tibial
internal rotational osteotomies performed on
patients with a tibial maltorsion with AKP or PI.
The VAS went down 3.4 points (SD 2.89), from
574
5.7 (SD 2.78; range 0–10) to 2.3 (SD 1.83; range
0–7). The Lysholm score increased 26 points (SD
16.32), from 66 (SD 14.94; range 32–94) to 92
(SD 9.29; range 70–100). Regarding patellar
instability, no redislocation occurred in the
follow-up period. The improved clinical scores
and VAS and no redislocations demonstrated the
value of this surgical procedure. Naqvi and colleagues [18] evaluated outcomes after proximal
femoral rotational osteotomy in patients with
symptomatic excessive femoral anteversion and
intoeing gait in 2017. They evaluated 21 patients
(35 operated limbs). In 13 out of 21 patients, the
reason for the visit was knee pain. The mean
follow-up after surgery was 16 months (6–
36 months). Ten out of 13 patients complained of
knee pain that was resolved. There was no
improvement for 3 after the surgery. The authors
highlight that excessive femoral anteversion is
associated with increased external tibial torsion in
some cases. In these cases, an isolated correction
of femoral anteversion can have a detrimental
effect on external tibial torsion and patellofemoral
tracking may worsen. In these selected cases a
double level osteotomy would be indicated.
Stambough and colleagues [20], in 2018,
showed that a rotational femoral osteotomy over
an intramedullary nail performed in adolescents
with AKP and excessive femoral anteversion is a
reliable surgical option. They found that it results
not only in deformity correction but also in a
significant improvement relative to both pain and
function. A relevant finding in their study is that
those adolescents with lower preop function
scores do significantly better in the postoperative
IKDC than those who had preoperative scores of
more than 70 points.
Frings and colleagues [22], in 2019, analyzed
31 distal rotational femoral osteotomies performed on 25 patients with PI and maltracking
secondary to a femoral torsional abnormality.
The average follow-up was 27 months (range
12–64). They also did 19 MPFL reconstructions,
14 tibial tuberosity transfers, varization in 4 cases
and a valgus correction in 1 case. The VAS
improved from 6.2 to 1.5, the Kujala score from
45.0 to 81.5, the Lysholm score from 40.3 to
V. Sanchis-Alfonso et al.
83.9, and the Tegner score went from 2.1 to 3.9.
No re-dislocations were observed. Preoperative
cartilage damage significantly influenced the
clinical outcome. They concluded that patellofemoral maltracking and PI in patients with
pathological femoral maltorsion can successfully
be treated by means of combined distal rotational
femoral osteotomies and it shows excellent
clinical results. Imhoff and colleagues [23]
evaluated 42 patients (44 knees) with PI that
underwent distal femoral rotational osteotomy
with a mean follow-up period of 44 months
(range 12–88) in 2019. In 28 cases, a rotational
osteotomy was associated with an MPFLr, with
valgus correction in 22 cases, patellofemoral
arthroplasty in 8, a trochleoplasty in 6 and a tibial
tubercle transfer in 6. During the follow-up period, no patellar re-dislocations were observed.
The authors concluded that combined rotational
osteotomy is a suitable treatment for PI due to
femoral torsional abnormality as it leads to a
significant reduction in pain and a significant
improvement in knee function. To avoid
overtreatment, the authors recommend doing the
rotational osteotomy first and follow it with a
physical examination to evaluate patellar tracking. Based on the results of these evaluations, an
MPFLr or a tibial tubercle transfer can proceed.
In 2020, Tian and colleagues [25] evaluated
17 femoral rotational osteotomies performed on
16 patients with recurrent patellar dislocation. In
8 cases, the rotational osteotomy was an isolated
procedure. In 5 cases, it was associated with
medial retinaculum reefing. It was associated
with an MPFLr in 4 cases. The authors have
shown that the supracondylar femoral rotational
osteotomy may be an effective treatment for
recurrent patellar dislocation induced by
increased femoral internal torsion as good clinical results and improvement in patellofemoral
congruence were obtained.
In a 2021 cohort study (level 3 of evidence),
Zhang and colleagues [26] evaluated the results
of the isolated MPFLr and those of the MPFLr
associated with the distal derotational femoral
osteotomy in patients with recurrent patellar
dislocation with increased femoral anteversion.
Rotational Osteotomy. Principles, Surgical Technique …
575
They conclude that the results are more favorable
when MPFLr is associated with a femoral
osteotomy, especially when the patients had a
preop high-grade J-sign.
Abnormal femoral torsion may be a primary risk
factor in PI that has so far been underesmated.
If increased femoral anteversion is present,
a concomitant rotaonal femoral osteotomy
should be considered along with MPFLr, especially
when the paents have a high-grade preop J-sign
Finally, Leonardi and colleagues [13] presented 3 patients in 2013 that had undergone a
double level (femoral and tibial) bilateral osteotomy (12 osteotomies) with a mean follow-up of
16 years. At final follow-up, no patient reported
knee or hip pain. According to those authors,
internally rotating the tibia alone is not sufficient
in cases of significant deformity because these
patients rarely have sufficient passive external
rotation of the femur to accommodate the operatively internally rotated tibia. Ipsilateral outward
femoral and inward tibial osteotomies performed
in the same surgical setting is the current recommendation of Leonardi and colleagues [13].
One-level osteotomy is not sufficient in cases
of significant
“miserable malalignment”
6
Complications. Scientific
Evidence (See Tables 1, 2, 3
and 4)
Rotational osteotomy is not a common surgical
technique in our armamentarium to treat AKP
and/or PI patients. A more widespread surgical
technique for treating AKP and PI is the tibial
tubercle osteotomy, which has clearly overshadowed the rotational osteotomy. Detractors of the
rotational osteotomy argue that it is an aggressive
surgery that is prone to bring on serious surgical
complications. However, the frequency and types
of complications seen in rotational osteotomy
surgeries are similar to those of the tibial tubercle
osteotomy. Payne and colleagues [46], in a systematic review, found an overall risk of major
complications of 3% after tibial tubercle osteotomy. Sanchis-Alfonso and colleagues [44] did a
systematic review with meta-analysis to evaluate
Table 1 Demographics
Demographics—(22 papers)
Author
Type of study
Mean age
Sex
Number of
patients
Number of
osteotomies
Cooke T.D.V et al., 1990
Case series (IV)
18 (one patient
46 yrs)
9 Females/3
Males
12
9
Meister K. and James S.
L., 1995
Case series (IV)
20.8 (15–30)
7 Females
7
8
Cameron J.C. and
Saha S., 1996
Case series (IV)
27.6 (14–42)
16 Females
16
17
Delgado E.D. et al., 1996
Case series (IV)
14.18 (10–18)
6 Males/3
Females
9
20
Server F. et al., 1996
Case series (IV)
20 (15–45)
22 Females/3
Males
25
35
Bruce W.D. and
Stevens P.M., 2004
Case series (IV)
14.9 (11.75–18)
13 Females/1
Male
14
54
Paulos L. et al., 2009
Cohort Study
(III)
20 (15–30)
9 Females/3
Males
12
12
Fouilleron N. et al., 2010
Case series (IV)
26.5 (18–44)
24 Females/5
Males
29
3
(continued)
576
V. Sanchis-Alfonso et al.
Table 1 (continued)
Demographics—(22 papers)
Author
Type of study
Mean age
Sex
Number of
patients
Number of
osteotomies
Leonardi F. et al., 2014
Case series (IV)
20.6 (17–24)
3 Females
3
6
Stevens P.M. et al., 2014
Case series (IV)
17 (9–30)
13 Females/3
Males
16
12
Drexler M. et al., 2014
Case series (IV)
34.6 (19–57)
11 Females/1
Male
12
15
Dickschas J. et al., 2015
Case series (IV)
30.5 (15–47)
19 Females/6
Males
25
33
Nelitz M. 2015
Case series (IV)
18.2 (15–26)
12 Females
12
12
Dickschas J. et al., 2016
Case series (IV)
27 (13–48)
29 Females/13
Males
42
49
Naqvi G. et al., 2017
Case series (IV)
13.3 (8–18)
15 Females/6
Males
21
35
Frings J. et al., 2017
Case series (IV)
24 (15–46)
–
25
31
Stambough J.B. et al.,
2018
Cohort study
(II)
12.7
16 Females/6
Males
22
32
Iiobst C.A. and Ansari A.,
2018
Case series (IV)
12
4 Males/4
Females
8
16
Imhoff F.B. et al., 2019
Case series (IV)
28
–
42
44
Manilov R. et al., 2020
Case series (IV)
30.5 (18–61)
50 Females/10
Males
60
60
Tian G. et al., 2020
Case series (IV)
20.8 (15–41)
11 Females/5
Males
16
17
Zhang Z. et al., 2021
Cohort study
(III)
21.3
59 Females/7
Males
66
70
major complications in rotational osteotomy
surgery. They found an overall risk of major
complications after rotational osteotomy of 3.3%
[44]. The authors concluded that rotational
femoral and/or tibial osteotomy is a safe surgical
procedure in the treatment of patellofemoral
disorders in adolescents and active young people.
Among all the complications, the most devastating is non-union at the osteotomy site.
Sanchis-Alfonso and colleagues [44] found that
1.08% had non-union at the osteotomy site. In all
those cases, a new surgical intervention was
required. Surgery involved additional plate
osteosynthesis, an autologous bone graft and
drilling of the non-union. The risk of non-union
was greater in femoral osteotomies (1.73%) than
in tibial osteotomies (0.75%), which is not surprising because the tibial osteotomies were
performed proximally to the tibial tuberosity in
most of the cases. In the proximal region of the
tibia, there is a lot of trabecular bone. Therefore,
union of the osteotomy is easier at this location.
Moreover, patient factors including obesity and
smoking may also affect the risk of non-union
[44]. Such factors should be modified before
osteotomy. It is advisable for the patient to lose
weight and quit smoking before osteotomy.
Careful attention to surgical technique might
minimize the risk of non-union. In some cases,
the fibula provides a considerable degree of
resistance to the rotation of the tibia. In those
cases, a fibular osteotomy must be carried out. As
soon as the fibula is cut, tibial rotation becomes
very easy. Fouilleron and colleagues [9], systematically cut the fibula to obtain easy tibial
correction. Proximal fibular osteotomy also
Type of osteotomy
Derotation valgus tibial osteotomy
Proximal tibial osteotomy
Proximal tibial osteotomy
Distal femoral (DF) (4) /Proximal Tibial
(PT) (6) / Distal Tibia (DT) (4), DF + PT
(2), DF + DT (1)
Proximal tibial osteotomy
Double-level: DF(13), Dyaphiseal femoral
(8), Intertrochanteric (6), Tibia
supramaleolar (20) Dyaphiseal tibia (7)
Derotational high tibial osteotomy
Proximal tibial derotation osteotomy
Double-level (3): Proximal femoral (2), DF
(4), PT (6)
Isolated F midshaft (1)/Isolated T (midshaft
vs. supramaleolar) (14)/Double level (8)
Derotational high tibial osteotomy
Isolated distal femoral osteotomy (27),
Double-level (3)
Author
Cooke T.D.V
et al., 1990
Meister K.
and James S.
L., 1995
Cameron J.C.
and Saha S.,
1996
Delgado E.D.
et al., 1996
Server F.
et al., 1996
Bruce W.D.
and
Stevens P.
M., 2004
Paulos L.,
et al., 2009
Fouilleron N.
et al., 2010
Leonardi F.
et al., 2014
Stevens P.M.
et al., 2014
Drexler M.
et al., 2014
Dickschas
J. et al., 2015
AKP (17), Patellar
instability (15)
Patellar instability
AKP and Patellar
instability
AKP
AKP (31), Patellar
instability (5)
Patellar instability
AKP
AKP (23 patients).
Patellar instability
(2 patients)
AKP
17 patients patellar
instabilty and 5
patients AKP
Anterior knee pain
Anterior Knee Pain
(AKP)
Indications
Surgical details and individual study complications (22 papers)
Table 2 Surgical details and individual study complications
Valgisation (8), Varisation
(6), Extension (2)
TTO
LRR (8 cases)
NO
TTO
Proximal realignment
LRR (13 limbs)
NO
NO
NO
TTO of medialization (2)
Lateral Retinaculum Release
(LRR)
Concomitant procedures
3.4
7
4.9
16.3
4.6
4.2
5.2
?
2.7
2.1
10.1
?
Follow
up
Non-union (2)
(continued)
Non-union (heavy smoker) (1), collapse at the site of
osteotomy with varus malalignment (1)
Femoral non-union (1), Peroneal nerve irritation (1)
NO
Stiffness (1), DVT (1), Transitory peroneal nerve palsy
(1)
Plate removal (1), Knee stiffness (1)
Painful fibular non-union (1) (22 fibular osteotomies)
Phlebitis (1) Fracture (1)
NO
Staples remove due to pain (2)
Staples remove due to pain (3)
NO
Complications
Rotational Osteotomy. Principles, Surgical Technique …
577
Type of osteotomy
Distal femoral osteotomy
Tibial osteotomy
Proximal femoral derotation osteotomy
Distal femoral osteotomy
Midshaft derrotational femoral osteotomy
Femoral ostetomy
Femoral osteotomy
High tibial derotational osteotomy
Femoral osteotomy
Derotational distal femoral osteotomy
Author
Nelitz M.
et al., 2015
Dickschas
J. et al., 2016
Naqvi G.
et al., 2017
Frings
J. et al., 2017
Stambough J.
B. et al.,
2018
Iobst Ch.
A and
Ansari A.
2018
Imhoff F.B.
et al., 2019
Manilov R.
et al. 2020
Tian G. et al.,
2020
Zhang Z.
et al., 2021
Patellar instability
Patellar instability
AKP
Patellar instability
AKP
AKP
Patellar instability
Int toeing (19),
AKP (13), Hip pain
(8)
AKP (42), Patellar
Instability (19)
Patellar Instability
Indications
Surgical details and individual study complications (22 papers)
Table 2 (continued)
MPFLr (66), TTO (30)
MPFLr (4), Medial
Retinaculum Constriction(5)
NO
Valgus correction (22),
(MPFLr (28), PFA (8),
Trochleoplasty (6), TTO (6)
NO
NO
MPFLr (19), TTO (14),
Varus correction (4), Valgus
correction (1)
NO
LRR in all the cases,
Valgisation (21), Fibular
osteotomy (7)
MPFL r
Concomitant procedures
3.7
2.2
5.5
3.7
0.8
1
2.3
1.3
3.5
1.4
Follow
up
NO
Stiffness (2)
Hardware removal (11), Knee Stiffness (2), Tibial
Fracturte (1), Transitory Peroneal Nerve Palsy (1),
Permanent Peroneal Nerve Palsy (1)
NO
NO
Non-union (1), Hardware removal (6)
Superficial wound infection (1)
Non-union (1)
Non-union (1), Compartment syndrome (1),
Transitory peroneal nerve palsy (1), Symptomatic
fibular pseudoarthrosis (1)
NO
Complications
578
V. Sanchis-Alfonso et al.
Rotational Osteotomy. Principles, Surgical Technique …
579
Table 3 Risk of major complications
Overall risk of major complications (22 papers)
Complications
Tibial
osteotomy
(n = 265)
Femoral
osteotomy
(n = 289)
Double-level osteotomies (At
the same time) (n = 94)
Total
(n = 648)
Osteotomy nonunion
2 (0.75%)
5 (1.73%)
–
7 (1.08%)
Transitory peroneal
nerve palsy
4 (1.50%)
–
–
4 (0.61%)
Permanent peroneal
nerve palsy
1 (0.37%)
–
–
1 (0.15%)
Neurologic damage
–
–
–
–
Vascular damage
–
–
–
–
DVT
1 (0.37%)
–
–
1 (0.15%)
Compartment
Syndrome
1 (0.37%)
–
–
1 (0.15%)
Fractures
2 (0.75%)
–
–
2 (0.30%)
Stiffness
4 (1.50%)
–
–
4 (0.61%)
Symptomatic fibular
pseudoarthrosis
2 (0.75%)
–
–
2 (0.30%)
Total
17 (6.41%)
5 (1.73%)
0
22 (3.39%)
Table 4 Risk of minor complications
Overall risk of minor complications (22 papers)
Complications
Tibial
Osteotomy
(n = 265)
Femoral
Osteotomy
(n = 289)
Combined Tibial and Femoral
Osteotomies (At the same time)
(n = 94)
Total
(n = 648)
Hardware
removal
17 (6.41%)
6 (2.47%)
–
23 (3.54%)
Phlebitis
1 (0.37%)
–
–
1 (0.15%)
Superficial
wound
infection
–
1 (0.36%)
–
1 (0.15%)
Total
18 (%)
7 (2.42%)
0
25 (3.85%)
presents a risk of non-union and can therefore be
a source of pain and require surgery. Two
patients (0.75%) in our systematic review had
symptomatic fibular pseudoarthrosis [44].
Sanchis-Alfonso and colleagues [44] found
peroneal nerve palsy in 1.87% of rotational tibial
osteotomies. It can be secondary to overextension of the nerve or entrapment due to internal
tibial rotation, or it could be secondary to a
fibular neck osteotomy. A large tibial correction
will put tension on the peroneal nerve. In those
cases of internal tibial torsion of more than 20°,
release of the peroneal nerve is essential to preventing peroneal nerve palsy. The fibular neck
osteotomy must be performed meticulously
because of the anatomical situation of the peroneal nerve.
The risk of an intraoperative tibial fracture is
0.3%. One way to prevent it is to make a precise
cut with the saw and dispense with the
580
V. Sanchis-Alfonso et al.
osteotome. A drain should be used to reduce the
risk of hematoma and compartment syndrome
(0.15%). If the anterior compartment of the leg is
very tight, we should leave the fascia open. In
our systematic review, only 1 postoperative case
of DVT was found (0.15%). Not using a
tourniquet may be a factor that is related to the
low incidence of DVT in that group of patients.
Immediate active ankle and knee motion and the
use of CPM in the hospital are advocated to
prevent DVT and avoid knee stiffness.
The most important finding of our systematic
review is that the location of the osteotomy (tibial
vs. femoral vs. double level) has an influence on
the risk of complications [44]. The risk of complications is greater in the tibial osteotomy
(6.41%) than when the osteotomy is performed
on the femur (1.73%) [44]. Surprisingly, the risk
of complications is nil in double level osteotomies [44].
7
The Patient Experience Before
and After Rotational Femoral
and/or Tibial Osteotomy.
A Qualitative Analysis
When evaluating an AKP patient with torsional
abnormalities before and after rotational osteotomy surgery, we usually use analog scales in
order to quantify the pain, functional scores to
evaluate disability, as well as biomechanical
tools and imaging techniques. However, it is not
usual to analyze the patient from the point of
view of her individual experience. We have done
a similar analysis to that carried out by Smith and
colleagues [47] in their study “The experience of
living with patellofemoral pain”. We have evaluated the personal experience of living with AKP
secondary to tibial and/or femoral maltorsion
before and after an isolated or combined femoral
and/or tibial rotational osteotomy. The participants have offered us the personal impact that
their pathology has had on them in detail. It
included the impact of the pain, the loss of
physical and functional capacity, the loss of own
identity, the confusion related to pain and the
difficulty making sense of their pain and fear of
the future. What has proved most impressively
with following these patients is the frequent
number of observations made by patients which
do not appear in any usual outcome measures.
This suggests that specific and validated outcome
measures must be developed for different clinical
conditions and diagnoses. Interestingly, Lutz and
colleagues [48] analyzed the limitations in sexual
activity in female patients with chronic patellar
instability and sexual function after complex
patellofemoral reconstructions including rotational osteotomy. The authors reported preop
restrictions of sexual activities due to patellar
instability preoperatively. Sexual activity was
improved in 60% of females with preoperative
restrictions. However, there are no studies that
analyze the limitations in sexual activity in
female patients with AKP secondary to torsional
abnormalities.
7.1 Patient Observations Before
Surgery Include
the Following
7.1.1 Uncertainty, Confusion and Sense
Making
When the patient comes to the consultation he
tries to explain to us what she thinks is causing
her pain. They are distraught because they have
gone to several doctors previously and the doctors have not understood them. The following are
typical expressions that the patient usually uses:
My body is out of whack.
My body is twisted.
I noticed a lot of pressure in my knee. It was as if
someone were squeezing my knee very hard.
When I bend my knee, it is as if it was going to
break, feeling pins and needles, or like being hit on
your finger with a sledgehammer. It is a very sharp
pain.
During a family trip, I stayed in the hotel room
most of the time due to the pain. However, I felt
OK after coming back. I did not understand why I
was so bad-off and I had excruciating pain and
suddenly the pain stopped, and I was able to carry
on with my normal activity. Similarly, on another
occasion, I went to a concert with my friends and
Rotational Osteotomy. Principles, Surgical Technique …
spent the whole time sitting because of the knee
pain, too. People around me thought I was doing it
on purpose.
7.1.2 Impact on Self and Loss of Selfidentity
Pain is omnipresent in the daily life of these
patients and results in a loss of physical capacity
and even in a loss of self-identity.
Every single day is complicated for me, from the
moment I wake up until I go to bed. Some days
when I get out of bed and put my feet on the floor, I
can already feel the pain in my knee. Other days, I
have no pain when I get out of bed but as soon as I
start to walk or do anything the pain appears again.
My knee severely limited my everyday activities,
like cleaning the house, making the bed, going for
a walk, etc.
Climbing the stairs was like climbing a mountain.
My knee hurt a lot and my leg was stuck. The pain
was horrible.
581
why I´m wearing scruffy jeans with holes on the
knees.
I like wearing high heels a lot, but the pain was so
strong that I was only able to wear them once or
twice a year.
7.1.4 Expectation of the Future
I would love to be a mum, but I dread to imagine
what my legs would have to go through due to the
extra kilos.
What will my life look like in 20 years’ time?
I would prefer not to live than live like that.
I have no idea why my boyfriend puts up with me.
I have so many limitations.
7.2 Patient Observations After
Surgery Include
the Following
I had to go down the stairs step-by-step, holding on
to the banister and, even so, at times I would fall.
When I would go to a party, my friends would
leave me behind, leaving me alone.
When I woke up after surgery, my thoughts were
automatically about my operated leg and I felt like
the bones were in their right place, that the tibia
was in its right place, that the femur was in its
correct place, everything was in its proper place.
Deciding on the clothes to wear is a nightmare.
There are no shoes that make me feel dressed up
and comfortable at the same time.
The operation was magical for me. The pain disappeared all of a sudden.
Driving to work is just terrible. Pressing the clutch
is very painful.
Before I had my surgery, I was very irritable, I
would get angry with my parents and friends for no
reason at all. I wasn’t myself anymore.
Teachers, especially in physical education as well
as doctors and physiotherapists told me I was
crazy, that I was nuts, that I was an idiot and that I
complained just for fun.
7.1.3 Coping Strategies and Activity
Beliefs
I try to sit idly most of the time.
I was usually in the emergency room every few
weeks due to pain so that they would give me
something for my pain.
The pain was very intense and would wake me up
at night. I could hardly sleep. I even had to take
painkillers and sleeping pills. The pain was
excruciating.
Putting my tight jeans on is extremely painful. The
touch of the fabric hurts my skin. This is the reason
My knee no longer hurts me, not at all. it’s really
incredible.
I have never again had pain.
The pain has completely gone away, and I can
sleep again.
I couldn’t be happier. After two years of severe
pain, I no longer have pain with anything I might
do.
Before, I was in continual pain. I did not feel
happy at not being able to find a good position
where I truly felt comfortable. Now I can sit in a
chair and not feel pain. And when I go to bed, I
don’t have any problem.
I have recovered the autonomy I didn’t have
before. I can go to the movies, go down stairs, take
a normal walk without having to use crutches or a
wheel chair or have someone help me.
Now I can go up and down stairs, bend my knees,
and do everything a girl of my age should do.
I go to bed, and I am calm, without having to move
around constantly to find a comfortable position so
as not to have pain in my knee. And I don’t have
nightmares any more about my knee.
582
V. Sanchis-Alfonso et al.
It’s like having a new leg.
Now I feel that my leg is finally no longer a dead
weight, that I can be pain-free, something I thought
was impossible before, and I can sleep all through
the night at one stretch.
I had never thought about a future with children.
But now I am pregnant and thrilled. My knee
hasn’t given me any trouble during my pregnancy.
This surgery changed my life completely.
My life and my personality as well as my relationship with my family have changed completely.
Before I was mad at the world, was always in a bad
mood, quite depressed, more aggressive, any
excuse to be angry. I am myself again, both
physically and mentally.
My personality is back again.
My knee feels perfect. I’m able to do things I
couldn’t do like go hiking, go clubbing and not
feel like sitting down, work standing on my feet
many hours, kneel, crouch, cross my legs, do
sports–in short, lead a normal life.
I’d have this operation a hundred times more,
without any doubt whatsoever.
I have recovered my life.
8
Take Home Message
The techniques described in this chapter, when
well-indicated and well performed technically,
provide very good results in AKP or PI patients
with pathological torsional abnormalities.
References
1. Cooke TD, Price N, Fisher B, et al. The inwardly
pointing knee. An unrecognized problem of external
rotational malalignment. Clin Orthop Relat Res.
1990;(260):56–60.
2. Meister K, James SL. Proximal tibial derotation
osteotomy for anterior knee pain in the miserably
malaligned extremity. Am J Orthop (Belle Mead NJ).
1995;24(2):149–55.
3. Cameron JC, Saha S. External tibial torsion: an
underrecognized cause of recurrent patellar dislocation. Clin Orthop Relat Res. 1996;328:177–84.
4. Delgado ED, Schoenecker PL, Rich MM, et al.
Treatment of severe torsional malalignment syndrome. J Pediatr Orthop. 1996;16(4):484–8.
5. Server F, Miralles RC, Garcia E, et al. Medial
rotational tibial osteotomy for patellar instability
secondary to lateral tibial torsion. Int Orthop. 1996;20
(3):153–8.
6. Bruce WD, Stevens PM. Surgical correction of
miserable malalignment syndrome. J Pediatr
Orthop. 2004;24(4):392–6.
7. Teitge RA. Patellofemoral syndrome a paradigm for
current surgical strategies. Orthop Clin N Am. 2008;
287–311.
8. Paulos L, Swanson SC, Stoddard GJ, et al. Surgical
correction of limb malalignment for instability of the
patella: a comparison of 2 techniques. Am J Sports
Med. 2009;37(7):1288–300.
9. Fouilleron N, Marchetti E, Autissier G, et al. Proximal tibial derotation osteotomy for torsional tibial
deformities generating patello-femoral disorders.
Orthop Traumatol Surg Res. 2010;96(7):785–92.
10. Dickschas J, Harrer J, Pfefferkorn R, et al. Operative
treatment of patellofemoral maltracking with torsional osteotomy. Arch Orthop Trauma Surg.
2012;132(3):289–98.
11. Teitge RA. Does lower limb torsion matter? Tech
Knee Surg. 2012;11:137–46.
12. Drexler M, Dwyer T, Dolkart O, et al. Tibial
rotational osteotomy and distal tuberosity transfer
for patella subluxation secondary to excessive external tibial torsion: surgical technique and clinical
outcome. Knee Surg Sports Traumatol Arthrosc.
2014;22(11):2682–9.
13. Leonardi F, Rivera F, Zorzan A, et al. Bilateral
double osteotomy in severe torsional malalignment
syndrome: 16 years follow-up. J Orthop Traumatol.
2014;15(2):131–6.
14. Stevens PM, Gililland JM, Anderson LA, et al.
Success of torsional correction surgery after failed
surgeries for patellofemoral pain and instability.
Strateg Trauma Limb Reconstr. 2014;9(1):5–12.
15. Nelitz M, Dreyhaupt J, Robert S, et al. Combined
supracondylar femoral derotation osteotomy and
patellofemoral ligament reconstruction for recurrent
patellar dislocation and severe femoral anteversion
syndrome: surgical technique and clinical outcome.
Int Orthop. 2015;39(12):2355–62.
16. Dickschas J, Harrer J, Reuter B, et al. Torsional
osteotomies of the femur. J Orthop Res. 2015;33
(3):318–24.
17. Dickschas J, Tassika A, Lutter C, et al. Torsional
osteotomies of the tibia in patellofemoral dysbalance.
Orthop Trauma Surg. 2017;137(2):179–85.
18. Naqvi G, Stohr K, Rehm A. Proximal femoral
derotation osteotomy for idiopathic excessive femoral
anteversion and intoeing gait. SICOT J. 2017;3:49.
19. Iobst CA, Ansari A. Femoral derotational osteotomy
using a modified intramedullary nail technique. Tech
Orthop. 2018;33(4):267–70.
20. Stambough JB, Davis L, Szymanski DA, et al. Knee
pain and activity outcomes after femoral derotation
Rotational Osteotomy. Principles, Surgical Technique …
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
osteotomy for excessive femoral anteversion. J Pediatr Orthop. 2018;38(10):503–9.
Teitge RA. The power of transverse plane limb malalignment in the genesis of anterior knee pain—
clinical relevance. Ann Joint. 2018;3:70.
Frings J, Krause M, Akoto R, et al. Clinical results
after combined distal femoral osteotomy in patients
with patellar maltracking and recurrent dislocations.
J Knee Surg. 2019;32(9):924–33.
Imhoff FB, Cotic M, Liska F, et al. Derotational
osteotomy at the distal femur is effective to treat
patients with patellar instability. Knee Surg Sports
Traumatol Arthrosc. 2019;27(2):652–8.
Manilov R, Chahla J, Maldonado S, et al. High tibial
derotation osteotomy for distal extensor mechanism
alignment in patients with squinting patella due to
increased external tibial torsion. Knee. 2020;27
(6):1931–41.
Tian G, Yang G, Zuo L, et al. Femoral derotation
osteotomy for recurrent patellar dislocation. Orthop
Trauma Surg. 2020;140(12):2077–84.
Zhang Z, Song G, Li Y, et al. Medial patellofemoral
ligament reconstruction with or without derotational
distal femoral osteotomy in treating recurrent patellar
dislocation with increased femoral anteversion: a
retrospective comparative study. Am J Sports Med.
2021;49(1):200–6.
Lee TQ, Anzel SH, Bennett KA, et al. The influence
of fixed rotational deformities of the femur on the
patellofemoral contact pressures in human cadaver
knees. Clin Orthop and Relat Res. 1994;302:69–74.
Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. J Orthop Sports Phys Ther.
2003;33(11):686–93.
Diederichs G, Kohlitz T, Kornaropoulos E, et al.
Magnetic resonance imaging analysis of rotational
alignment in patients with patellar dislocations. Am J
Sports Med. 2013;41(1):51–7.
Stephen JM, Teitge RA, Williams A, et al. A validated, automated, 3-Dimensional method to reliably
measure tibial torsion. Am J Sports Med. 2021;49
(3):747–56.
Scorcelletti M, Reeves ND, Rittweger J, et al.
Femoral anteversion: significance and measurement.
J Anat. 2020;237(5):811–26.
Cheng JC, Chan PS, Chiang SC, et al. Angular and
rotational profile of the lower limb in 2630 Chinese
children. J Pediatr Orthop. 1991;11:154–61.
Yoshioka Y, Cooke TD. Femoral anteversion:
assessment based on function axes. J Orthop Res.
1987;5(1):86–91.
Yoshioka Y, Siu DW, Scudamore RA, et al. Tibial
anatomy and functional axes. J Orthop Res. 1989;7
(1):132–7.
583
35. Murphy SB, Simon SR, Kijewski PK, et al. Femoral
anteversion. J Bone Joint Surg Am. 1987;69
(8):1169–76.
36. Archibald HD, Petro KF, Liu RW. An anatomic
study on whether femoral version originates in the
neck or the shaft. J Pediatr Orthop. 2019;39:e50–3.
37. Seitlinger G, Moroder P, Scheurecker G, et al. The
contribution of different femur segments to overall
femoral torsion. Am J Sports Med. 2016;44(7):1796–
800.
38. Sanchis-Alfonso V, Domenech-Fernández J, BeserRobles M, et al. Pathological femoral anteversion in
the anterior knee pain patient depends on both the
neck and the shaft (Submitted).
39. Kim HY, Lee SK, Lee NK, et al. An anatomical
measurement of medial femoral torsion. J Pediatr
Orthop B. 2012;21(6):552–7.
40. Waisbrod G, Schiebel F, Beck M. Abnormal femoral
antetorsion–a subtrochanteric deformity. J Hip Preserv Surg. 2017;4(2):153–8.
41. Kuroda R, Kambic H, Valdevit A, et al. Articular
cartilage contact pressure after tibial tuberosity
transfer. A cadaveric study. Am J Sports Med.
2001;29(4):403–09.
42. Winkler PhW, Lutz PM, Rupp MC, et al. Increased
external tibial torsion is an infratuberositary deformity and is not correlated with a lateralized position
of the tibial tuberosity. Knee Surg Sports Traumatol
Arthrosc. 2021;29:1678–85.
43. Van Heerwaarden RJ, Teitge RA. Rotational osteotomy of the tibia. In: Parikh SN, editor. Patellar
instability. Wolters Kluwer;2020.
44. Sanchis-Alfonso V, Domenech J, Ferras-Tarrago J,
et al. The incidence of complications after derotational femoral and/or tibial osteotomies in patellofemoral disorders in adolescents and active adult
patients. A Systematic Review with Meta-Analysis.
Knee Surg Sports Traumatol Arthrosc. (In press).
45. James SL. Chondromalacia of the patella in the
adolescent. In: Kennedy JC. editor. The injured
adolescent knee. Baltimore: The Williams & Wilkins
Company;1979.
46. Payne J, Rimmke N, Schmitt LC, et al. The incidence
of complications of tibial tubercle osteotomy: a
systematic review. Arthroscopy. 2015;31(9):1819–25.
47. Smith BE, Moffatt F, Hendrick P, et al. The
experience of living with patellofemoral pain—loss,
confusion and fear-avoidance: a UK qualitative
study. BMJ Open. 2018;8: e018624. https://doi.org/
10.1136/bmjopen-2017-018624.
48. Lutz PM, Winkler PW, Rupp MC, et al. Complex
patellofemoral reconstruction leads to improved physical and sexual activity in female patients suffering
from chronic patellofemoral instability. Knee Surg
Sports Traumatol Arthrosc. 2021;29(9):3017–24.
Bipolar Fresh Osteochondral
Allograft Transplantation
of the Patellofemoral Joint
Vicente Sanchis-Alfonso
and Joan Carles Monllau
1
Introduction
The treatment of large osteochondral lesions in
young patients is a great challenge for the
orthopedic surgeon. In this type of patient, there
is a reluctance to use prostheses for fear of wear
and loosening. An enticing therapeutic alternative would be fresh osteochondral allograft
transplantation. The objective of that technique is
to provide viable articular hyaline cartilage
without the size limitations imposed with the use
of autografts. It is unlike what occurs with other
techniques like autologous chondrocyte transplantation, which requires two surgeries, osteochondral allograft transplantation is performed in
a single surgical procedure. The ultimate goal is
to relieve pain, improve function, and delay the
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
J. C. Monllau
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
time for prosthetic surgery. Here, we present our
surgical technique for the treatment of massive
osteochondral lesions of the patellofemoral joint
in the young patient. The final objective is to
treat the osteochondral lesion along with anatomic and biomechanical abnormalities.
2
Indications and Contraindications
The ideal patient to perform a fresh osteochondral allograft would be a young person
(<50 years) with a grade III or IV osteochondral
or chondral lesion of more than 2 cm2, contained
or uncontained (Fig. 1). Moreover, there must be
a correct alignment of the lower extremity on the
three planes of space, and a correct patellofemoral tracking (negative J-sign).
Only patients with severe chronic pain recalcitrant to conservative treatment and significant
disability for activities of daily living as a result
of the injury are candidates for this surgical
technique. Wang and colleagues [1] have introduced the concept of “significant clinical benefit”
as a guideline in the clinical decision when
indicating an osteochondral graft. Those authors
show that the “significant clinical benefit,” a
concept that has nothing to do with “statistical
significance,” is 30 ± 6.9 for the IKDC. This
means that if the IKDC goes from 70 to 80 after
an osteochondral allograft, the patient will not
perceive any objective benefit from surgery even
if the difference between 70 and 80 was
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_40
585
586
V. Sanchis-Alfonso and J. C. Monllau
Fig. 1 The ideal indication
for a total resurfacing
osteochondral transplantation
is the presence of a large
cartilage injury or multifocal
lesions and a dysplastic
trochlea
statistically significant. For the patient to notice
an improvement in this case, it would have to go
from 70 to 100. Therefore, we must analyze the
patient’s expectations regarding the results of the
surgery and see if it is really feasible to achieve
that “significant clinical benefit”. Therefore, it
would be reasonable to operate on those patients
with an IKDC of <50 points.
The main exclusion criteria are advanced
osteoarthritis of other knee compartments, locally
aggressive rheumatic disease, infections, tumors,
diabetes, and vasculitis. Relative contraindications are being older than 50 years and having a
body mass index greater than 30 [2]. Smoking
must be stopped 30 days prior to surgery and for
at least 6 months after the operation [2].
3
The Keys for a Successful
Osteochondral Allograft
Transplantation
of the Patellofemoral Joint
We must make sure that chondropathy is
responsible for the pain that the patient has. This
is especially true in the patellofemoral joint,
where it is relatively common to find severe
chondropathies as an incidental finding.
The graft must be “fresh,” not cryopreserved.
In addition, what we transplant is an osteochondral “shell”, whenever possible. Osteochondral
grafts should not be too thick. The more bone the
graft has, there is a greater risk not only of an
immune response but also of graft necrosis. We
must use of the least amount of subchondral bone
possible, the minimum necessary for cartilage
fixation. The bone component of the osteochondral allograft acts as a support for the hyaline
cartilage and as a connecting link with the host
bone. In the future, the bone component of the
allograft will be replaced by bone from the host
through
a
phenomenon
of
“creeping
substitution”.
Patellofemoral chondropathy can be secondary to trauma, patellar instability, or lower
limb malalignment. Therefore, for the resurfacing
surgery to be successful, we must first correct the
instability and/or malalignment to eliminate the
shearing forces on the cartilage and the overload
of the repair. If we do not do this, the graft cartilage will deteriorate in the same way that the
original cartilage did, and the surgery will fail in
the medium or long term.
4
Surgical Thecnique
First of all, the distal femoral and patellar grafts
are inspected to ensure the absence of macroscopic damage and adequate morphology (that is,
non-dysplastic trochlea) (Fig. 2). The first step
when considering doing a massive osteochondral
Bipolar Fresh Osteochondral Allograft Transplantation …
587
Fig. 2 Distal femur and patella of a donor with adequate cartilage for transplantation and adequate trochlear
morphology (non-dysplastic trochlea)
allograft of the patellofemoral joint is to choose a
patella and trochlea with a size similar to that of
the recipient. In addition, the side must match. If
the recipient’s knee is the right, the donor’s side
must also be the right.
The patient is placed in the supine position
with a support for the foot and a lateral support
for the thigh to maintain the knee at 45° of
flexion. The contralateral limb is placed in full
extension. The surgical intervention should be
performed by two surgical teams that will work
simultaneously, two surgeons to work in the
surgical field (arthrotomy, preparation of the
recipient area and subsequent implantation of the
graft) and another to prepare the graft.
A longitudinal midline incision is used. Once
the joint is exposed through a conventional
medial parapatellar approach, the patella is
everted. The thickness of the patella is measured.
The surgical technique to prepare the patella is
identical to the one used in prosthetic surgery
when we are going to put in the patellar component. The articular surface of the patella is
resected using a standard cutting patellar guide
like that used in total knee arthroplasty (Fig. 3).
An oscillating saw is used, leaving a patella
remnant of about 13 mm (Fig. 3). We routinely
perform a peripatellar denervation with the
electrocautery with the theoretical idea of
reducing the postoperative incidence of anterior
knee pain. Resection of the recipient trochlea is
performed similarly to the anterior resection of
the distal femur in a patellofemoral arthroplasty
(Fig. 4).
Meanwhile, the other surgical team prepares
the allograft, also using the knee prosthesis
Fig. 3 Resection of the articular surface of the patella using a standard cutting patellar guide
588
V. Sanchis-Alfonso and J. C. Monllau
Fig. 4 Resection of the recipient’s trochlea using the Zimmer patellofemoral prosthesis guide
Fig. 5 Resection of the donor patella using a standard cutting patellar guide
instruments (Figs. 5 and 6). The proximal and
lateral part of the patella is marked with a sterile
skin marker to help place the graft in the recipient area in the appropriate position (normoposition) (Fig. 7). Resection of the donor trochlea is
performed similarly to the anterior resection of
the distal femur in a patellofemoral prosthesis
(Fig. 6). We must reduce the thickness of the
bone component of the graft as much as possible
(6–8 mm) to minimize the risk of immune reaction [3]. Before placing the patellar and trochlear
grafts, the bone component of the graft is cleaned
with a brush and washed for at least 15 min with
a pulsatile irrigation system with high-pressure
sterile saline solution to remove blood from the
graft and thus reduce a possible immunogenicity
(Fig. 8). During this cleaning process, care must
be taken not to injure the cartilage.
Then, the trochlear allograft is implanted, and
it is fixed with two medial and two lateral screws
associated or not with resorbable pins (Figs. 9
and 10). After that, the patellar allograft is
implanted over the reception area and provisionally fixed with two Kirschner wires introduced through the anterior cortex of the patella
(Fig. 11). The definitive fixation of the graft is
performed with resorbable pins. Once the patellar
graft is fixed, the K-wires are removed. Initially,
Bipolar Fresh Osteochondral Allograft Transplantation …
589
Fig. 6 Resection of the donor trochlea using the Zimmer patellofemoral prosthesis guide
we used four compression screws from the dorsal
aspect of the patella. They provided perfect fixation but caused artifact problems on the control
CT or MRI. The total thickness of the patella
after implantation of the patellar allograft should
be similar to that of the original patella.
Once the grafts have been fixed, it is verified
that the patellofemoral tracking is correct, and it
is closed plane by plane. Continuous passive
mobilization begins immediately. Assisted loading with two crutches is authorized the following
day depending on pain, with a knee brace locked
in extension and maintained for 4 weeks for
ambulation. Otherwise, the rehabilitation of these
patients does not differ at all from that conducted
with patients with a primary knee prosthesis.
5
What Can We Expect from a Fresh
Osteochondral Allograft?
Literature Review. Scientific
Evidence
Articular cartilage injuries in the patellofemoral
joint are quite a challenge for the orthopedic
surgeon. Due to the anatomy of the patellofemoral joint and its biomechanical complexity,
transplantation in this location is more demanding than in the tibiofemoral joint. This may
explain the high rates of allograft revisions, up to
60%, and the high percentage of failures (28.6%)
[4]. Gracitelli and colleagues [4] observed a graft
survival rate of 78% at 10 years and 56% at
590
V. Sanchis-Alfonso and J. C. Monllau
Fig. 8 Before placing the graft, the bone component is
cleaned with a brush and washed with a pulsatile
irrigation system with high-pressure saline to remove
blood from the graft
Fig. 7 Marking of the graft to place it in the proper
position. We mark the lateral edge of the patella with two
points and the proximal pole with one point
15 years follow-up. The authors conclude that
the patellar allograft is an effective treatment for
symptomatic chondropathies of the patella.
However, the results are much better in isolated
trochlear injuries. Cameron and colleagues [5]
published the results of a series with a minimum
evaluation at 2 years and a maximum evaluation
at 20 years (mean 7 years) with excellent clinical
results in terms of pain and function and high
patient satisfaction (90%). Those authors described a graft survival rate of 100% at 5 years and
91.7% at 10 years. Studies on bipolar patellofemoral osteochondral transplantation of the patella
and trochlea are few. The risk of failure is great
but allografts that survived showed significant
Fig. 9 Provisional fixation of the graft with Kirschner wires and definitive fixation with Acutrak screws
Bipolar Fresh Osteochondral Allograft Transplantation …
591
Fig. 10 Definitive appearance of the already implanted trochlea graft
Fig. 11 Provisional fixation of the graft with Kirschner wires. Definitive graft fixation with resorbable pins
improvements in function, pain relief, and rangeof-motion [6–10]. Torga Spak and Teitge [10]
presented 12 bipolar patellofemoral joint allografts for patellofemoral osteoarthritis. At the last
follow-up (mean, 10 years; range, 2.5–
17.5 years), 8 grafts were still functioning.
6
Conclusion
Fresh osteochondral allograft is a salvage surgery
intended for young patients with disabling
osteochondral or chondral lesions. The final
592
objective is to delay the moment of the prosthesis. If the patient is clear on the fact that it is a
“salvage surgery”, we avoid the frequent failures
related to not fulfilling the expectations of the
patient.
References
1. Wang D, Chang B, Coxe FR, et al. Clinically
meaningful improvement after treatment of cartilage
defects of the knee with osteochondral grafts. Am J
Sports Med. 2019;47(1):71–81.
2. Gelber PE, Ramírez E, Grau A, et al. Fresh
osteochondral resurfacing of the patellofemoral joint.
Arthrosc Tech. 2019;13(8):e1395–401.
3. Sherman SL, Garrity J, Bauer K, et al. Fresh
osteochondral allograft transplantation for the knee:
current concepts. J Am Acad Orthop Surg. 2014;22
(2):121–33.
V. Sanchis-Alfonso and J. C. Monllau
4. Gracitelli GC, Meric G, Pulido PA, et al. Fresh
osteochondral allograft transplantation for isolated
patellar cartilage injury. Am J Sports Med. 2015;43
(4):879–84.
5. Cameron JI, Pulido PA, McCauley JC, et al. Osteochondral allograft transplantation of the femoral
trochlea. Am J Sports Med. 2016;44(3):633–8.
6. Jamali AA, Emmerson BC, Chung C, et al. Fresh
osteochondral allografts: results in the patellofemoral
joint. Clin Orthop Relat Res. 2005;437:176–85.
7. Giannini S, Buda R, Ruffilli A. Failures in bipolar
fresh osteochondral allograft for the treatment of endstage knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2015;23:2081–9.
8. Meric G, Gracitelli GC, Gortz S, et al. Fresh
osteochondral allograft transplantation for bipolar
reciprocal osteochondral lesions of the knee. Am J
Sports Med. 2015;43:709–14.
9. Mirzayan R, Charles MD, Batech M, et al. Bipolar
osteochondral allograft transplantation of the patella
and trochlea. Cartilage. 2018:1947603518796124.
10. Torga Spak R, Teitge RA. Fresh osteochondral
allografts for patellofemoral arthritis: long-term followup. Clin Orthop Relat Res. 2006;444:193–200.
Patellofemoral Arthroplasty. Pearls
and Pitfalls
Pedro Hinarejos
1
Introduction
Isolated patello-femoral osteoarthritis (PF-OA)
without involvement of the femoro-tibial joint
(Fig. 1) is a common condition, which affects 9%
of the population in their forties and its incidence
increases significantly as age increases [1],
affecting 11% of men and up to 24% of women
over 55 years. Isolated PF-OA is much more
common in women, with an estimated 75% of
cases [2]. This is believed to be secondary to the
higher prevalence of trochlear dysplasia and
patellar instability in women.
Knee osteoarthritis has biological factors,
such as the presence of inflammatory pathology
or infection, and mechanical factors. In the case
of PF-OA mechanical factors, mainly trochlear
dysplasia and extensor mechanism malalignment, are of the greatest importance [3] although
some mechanical factors like obesity or genu
valgum are also frequently associated with global
osteoarthritis of the knee.
P. Hinarejos (&)
Consorci Parc de Salut Mar. Barcelona Universitat
Pompeu Fabra, Barcelona, Spain
e-mail: PHinarejos@parcdesalutmar.cat
2
History of Patellofemoral
Arthroplasty (PFA)
The first precedent of patello-femoral arthroplasty (PFA) was described by McKeever in
1955, and it consisted in the isolated replacement
of the patella by means of a metallic component
of vitalium, without a trochlear component, on
the basis where the patella is usually more
degenerated than the femoral side. The results
with these isolated patellar prostheses were poor,
with progressive degeneration of the femoral
trochlea.
PFAs have evolved and for the last 50 years
they have been made up of 2 components: a
femoral trochlea, which is metallic, and a patellar
component made of polyethylene.
The first generation of PFAs were first used in
1974. The most widely used were Lubinus®
(Waldemar Link, Germany) and RichardsBlazina® (Smith-Nephew Richards, USA), and
they had a relatively small trochlear component,
which was narrow and deep, with significant
constriction of the patella in the trochlear groove
as knee flexion increased. This first generation of
PFAs have been associated with a high rate of
patellar clunks, and patellar instability [4].
The second generation of PFAs were introduced in the 1990s, and they evolved to a wider
and shallower design of the trochlear component,
with a longer proximal extension and a sagittal
radius of curvature that better reproduces the
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_41
593
594
P. Hinarejos
Fig. 1 Isolated patellofemoral osteoarthritis, with
complete chondral lesions in
the femoral trochlea and
patella, but healthy cartilage
in the femoro-tibial
compartments
original anatomy. This evolution in design
reproduces the biomechanics of the patellofemoral joint in a better way [5]. In fact, the
design of the trochlea is more decisive in PFAs
than in TKAs, since more than 70% of patients
diagnosed with isolated PF-OA present trochlear
dysplasia [6] and poor alignment of the extensor
mechanism [7]. Ackroyd has reported a very
significant reduction in the rate of patellar
instability using the Avon® PFA (Stryker) compared to the Lubinus. Mid-term implant survival
of these second generation PFAs was significantly improved [8].
In the last decades, a third generation of PFAs
have appeared, which are anatomical (right or left
implants). They have a lateral facet of the trochlea
that is higher than the medial one to resist the
lateral translational forces of the extensor mechanism. Third-generation PFAs, e.g. the Journey®
(Smith & Nephew) or the Gender® (Zimmer)
incorporate a valgus alignment of about 7–10°
(Fig. 2). The length of the trochlea is different
from one model to another, in such a way that
some extend more proximally, favoring the contact of the patella with the trochlea even in full
extension, and others also extend distally,
increasing the contact of the patella with the trochlear component also in deep flexion.
3
Types of PFA Implants
Based on their design, PFAs can be classified
into two types: “inlay” (or resurfacing) and
“onlay” (or anterior trochlear cut).
1. “Inlay” or resurfacing PFAs
The design of these prostheses seeks to replace
only the articular cartilage, being very conservative in the sacrifice of bone and therefore, they
depend on the anatomy of the patient’s trochlea,
not allowing changing the original anatomy [7].
Some inlay prostheses are symmetrical
(Richards III® or Lubinus®) and tend to have a
fairly closed trochlar angle, while others are
asymmetrical (DePuy’s LCS® or FH’s Spherocentrica®), and these inlay PFAs have a very thin
implant in the trochlea (Fig. 3).
2. “Onlay” or anterior cut PFAs
In this type of PFAs, the preparation of the trochlear component begins with an anterior cut in
the trochlea area, very similar to the anterior cut
of the femoral component of the TKAs (Fig. 4).
Onlay PFAs can also be symmetrical (like Stryker’s Avon®) or asymmetrical (like Biomet’s
Vanguard®, Smith & Nephew’s Journey®, or
Zimmer’s Gender®).
Patellofemoral Arthroplasty. Pearls and Pitfalls
595
Fig. 2 Third generation onlay patello-femoral arthroplasty (Gender, from Zimmer) with anatomical design, with valgus
in the trochlear groove
component is usually cemented, with an additional fixation around small lugs or small keels.
The thickness of the trochlear component ranges
between 4 and 9 mm, although in onlay PFAs it
is greater than in inlay PFAs.
The patellar component consists of a polyethylene button, which can be symmetrical (domeshaped, or with 2 facets) (Fig. 2) or asymmetrical.
The patellar component is cemented and the
dome-shaped components have the advantage of
being more permissive with a residual tilt of the
patella allowing its self-centering. In case of
revision to a TKA the same patellar component
can be maintained due to its compatibility with the
femoral component of the TKA [9].
Fig. 3 Inlay patello-femoral arthroplasty (lateral view):
The metallic trochlear component is thin, to replace only
the cartilage, preserving as much bone as possible
All onlay PFA models have a cobaltchromium trochlear component (although they
may also have a titanium oxide coating such as
Smith & Nephew’s Journey®) and the trochlear
4
Indications (Table 1)
The success of PFAs is highly dependent on the
correct indication of surgery. The indication for a
PFA is severe PF-OA with indemnity of the
596
P. Hinarejos
Fig. 4 Anterior cut of the onlay patello-femoral arthroplasty, similar to that of TKA. Correct rotation of the trochlear
component is important for the stability of the extensor mechanism
Table 1 Patello-femoral arthroplasty indications
– Primary isolated patello-femoral osteoarthritis
– Osteoarthritis due to trochlear dysplasia
– Postraumatic osteoarthritis: Patella fractures
Fig. 5 Patello-femoral
osteoarthritis secondary to
trochlear dysplasia
femoro-tibial compartments. This isolated PFOA can be idiopathic, secondary to trochlear
dysplasia (Fig. 5) or post-traumatic, especially
after patella fractures.
The ideal requirements for a PFA are the
presence of severe signs and symptoms, without
improvement after a conservative treatment, the
absence of involvement of the femoro-tibial
Patellofemoral Arthroplasty. Pearls and Pitfalls
597
Table 2 Patello-femoral arthroplasty contraindications
Absolute contraindications
– Femoro-tibial significant osteoarthritis
– Active infection
– Inflammatory arthritis
– Flexion contracture >10°
– Significant malalignment (varus or valgus >5°)
Relative contraindications
– Patela baja
– Chondrocalcinosis
– Obesity
– Previous meniscectomy
– Elderly patients (>70 years)
compartments and the absence of a significant
femoro-tibial malalignment that suggests a quick
deterioration of the femoral or tibial cartilage after
PFA. PFA may be indicated as salvage surgery
after other surgeries as realignment of the extensor mechanism. It is frequently indicated in
patients with patellar instability who were previously treated with realignment, if this surgery has
improved the recurrent dislocation of the patella,
but the pain is significant because of the arthritic
changes that such instability have caused.
To confirm the correct criteria for the indication of PFA, we need a complete radiological
examination protocol, as it is later explained.
5
Fig. 6 Lateral view in maximum flexion in a patellofemoral arthroplasty with a low patella, where the patella
contacts distally, outside the trochlear component
Contraindications (Table 2)
Contraindications to PFA are the presence of a
significant femoro-tibial osteoarthritis, higher
than Ahlback grade I, the presence of a moderate
or severe limb malalignment (varus or valgus
>5°), the presence of an inflammatory arthritis, or
knee instability [10].
Other authors argue that chondrocalcinosis is
also considered a contraindication [2].
The presence of a low riding patella preoperatively is also considered a contraindication, at
least relative, since it would cause the patella not
to articulate against the trochlear component, but
more distally, in deep flexion (Fig. 6).
Obesity, with a body mass index greater than
30 kg/m2, is considered a relative contraindication, since obese patients have a higher risk of
disease progression to the femoro-tibial
compartments. Furthermore, the flexion of 60°
and 130° increases the reaction forces in the
patello-femoral joint 3.3 and 7.8 times with
respect to the body weight and could be excessive and facilitate loosening in very obese
patients. Obesity has also been observed to be a
risk factor for readmission and early reoperation
after PFA [11]. Nevertheless, a recent study has
found similar outcomes of PFAs in obese or nonobese patients in the mid-term and, according to
these authors, obesity should not be considered
an absolute contraindication [12].
Age is not an absolute contraindication for
PFAs, but in very young patients, younger than
40 years, it seems reasonable to try other surgical
treatments, while in elderly patients, older than
70 years, it seems reasonable to opt for a TKA,
because of its more predictable results.
598
P. Hinarejos
Although there is no evidence that a previous
meniscectomy or ligament injuries can lead to
worse results, it is better not to indicate this
partial replacement in cases of meniscal or ligament lesions, which are conditions that can
accelerate osteoarthritis of the femoro-tibial joint.
6
on palpation of the lateral aspect of the patella is
very common [3]. Patients also complain of pain
when a direct pressure is applied on the patella
against the femur.
Significant pain in the medial or lateral joint
lines, signs of knee instability in the saggital
plane or pain with meniscal maneuvers should
make us suspect of other knee lesions.
Diagnosis of PF-OA: Patient
Selection
6.3 Preoperative Radiology
6.1 Anamnesis
Pain is the main symptom of patients with PFOA. Usually the pain is referred in the anterior
aspect of the knee. A differential diagnosis with
anterior knee pain from other causes (tendinitis,
synovitis, etc.), or referred pain of spinal or hip
joint origin, must be done.
Usually the pain produced by PF-OA increases in closed chain movements with knee flexion
and the foot on the ground, such as when getting
up from a chair, squatting, rising up and down
stairs. In all these situations the contraction of the
extensor mechanism combined with the flexion
of the knee greatly increases the pressure supported by the articular surfaces of the patella and
trochlea, causing pain. The pain when walking
on flat surfaces is much lesser.
Another frequent symptom in PF-OA is the
presence of crepitus on the anterior aspect of the
knee. Recurrent joint effusions are frequent and
feeling of locking in the anterior aspect of the
knee can also occur.
6.2 Physical Examination
On inspection, rotational abnormalities of the
lower extremities during standing and walking
should be examined, as they cause a medial situation of the patella when the patient places the
feet facing forward. The alignment of the
extremities in the coronal plane must also be
explored, since a significant genu varum or genu
valgum should contraindicate the use of a PFA.
Pain and crepitus are frequent when the
patella is mobilized in the longitudinal axis. Pain
For the diagnosis of isolated PF-OA and surgical
planning of PFA the following X-rays are recommended [13]:
– Anterior–posterior weight-bearing view: It
must show the medial and lateral joint lines
preserved. This view is not necessary if a
good quality weight-bearing long X-ray centered on the knee is available.
– Rosenberg (or schuss) view: Posterioranterior projection made with weight-bearing
at about 40° of flexion. If an impingement of
the joint line height is observed, degenerative
changes in the posterior aspect of the knee
should be suspected.
– True lateral view (both femoral condyles must
be seen aligned) (Fig. 7). A decrease in the
patello-femoral joint line height can be seen,
with preservation of the femoro-tibial joint
line. On this view, the presence of a trochlear
dysplasia, common in PF-OA, can be analysed. On this view, an assessment of the
height of the patella should be done, usually
using the Caton-Deschamps index (CDI). The
presence of a high-riding patella or patella alta
(CDI > 1.2) may advise us to add a distalization of the anterior tibial tuberosity (TT),
while the presence of a low-riding patella or
patella baja (CDI < 0.8) is a contraindication,
at least relative, for a PFA.
– Patellar axial view (Fig. 8): with a knee flexion of about 30°. It allows us to observe the
involvement of the lateral and medial patellar
facets, as well as indirect signs of instability of
the extensor mechanism, like a lateral subluxation of the patella or an excessive tilt.
Patellofemoral Arthroplasty. Pearls and Pitfalls
599
considered a contraindication for PFA
(Remy), since it increases the risk of progression of osteoarthritis to the other compartments, and therefore the need for surgical
revision of a PFA.
6.4 Other Examinations
Fig. 7 True lateral view: significant decrease in the
patello-femoral joint line, with the femoro-tibial joint line
preserved. A trochlear dysplasia can be seen and the
patella height measured
– Full-limb length weight bearing view: It is
advisable to measure the hip-knee-ankle
angle, which is the angle that connects the
mechanical axes of the femur and the tibia.
A varus or valgus deformity greater than 5° is
Fig. 8 Patellar view: Made at
30° of flexion it shows the
impingement of the joint line
and signs of lateral instability
of the extensor mechanism
– Magnetic resonance imaging (MRI) (Fig. 9):
If there are concerns about the femoro-tibial
compartments condition, or about the association with meniscal or ligament pathology, it
can be studied by MRI. MRI would not be
routinely indicated in the preoperative evaluation of all PFA. If patellar instability is suspected, MRI (or computerized tomography)
can show the alignment of the extensor
mechanism, and the patellar tilt or subluxation
and the tibial tuberosity-trochlear groove distance (TT-TG) can be measured.
– Bone scintigraphy: In a recent study, Baker
et al. recommend the use of preoperative bone
scintigraphy to ensure that tracer uptake is
limited to the patello-femoral joint, and this
reduces the risk of progression of
osteoarthritis to the other compartments during follow-up [14], but it is not used in our
routine protocol.
600
P. Hinarejos
7.2 Medialization and Anteriorization
Osteotomy of the Tibial
Tuberosity
Fig. 9 Magnetic nuclear imaging showing severe patellofemoral osteoarthritis with joint effusion and lateral
subluxation of the patella in a patient with trochlear
dysplasia
This technique, described by Fulkerson [15],
consists of an oblique osteotomy (from anteromedial to postero-lateral) of the TT, which is
mobilized in a medial direction, achieving its
anteriorization (Maquet effect) in addition to the
medialization. Subsequently, the TT is fixed with
two compression screws in its new position. This
surgery would be indicated only in cases in
which osteoarthritis is isolated in the lateral facet
of the patella and there is an increased distance
TT-GT, especially if the cartilage lesions are not
full-thickness. The most frequently reported
complications after TT osteotomy are nonunion,
shaft fractures of the tibia distal to the osteotomy,
or discomfort caused by screw heads [3].
7.3 Patellectomy
7
Treatment Alternatives
When an isolated PF O-A is diagnosed, several
treatment alternatives to PFA have been
proposed.
7.1 Conservative Treatment
The initial treatment for any patient with isolated
PF-OA should be conservative: activity modification (avoiding squatting positions and the use
of stairs as much as possible), and overweight
control must be recommended in case of obesity.
Physical therapy should aim to strengthen the
thigh and gluteal muscles, as well as stretching
the contracted structures, especially the
hamstrings.
For pain control, the use of analgesics is recommended, and the use of injections for viscosupplementation may be indicated [3]. If knee
braces are used, it is recommended to use those
with a hole in the anterior part to minimize direct
pressure on the patella.
Resection of the patella and secondary reconstruction of the extensor mechanism was a
widely used technique for the treatment of isolated PF O-A in the past. However, this technique was associated with loss of strength, as
well as a feeling of instability and pain in a
significant number of patients. In 50% of the
cases in which the patellectomy was performed
as a treatment for osteoarthritis they were considered failures [16]. These poor results, associated with the rise of the prosthetic surgery, have
caused that this technique has been almost given
up for the treatment of PF O-A.
7.4 Partial Lateral Patella
Facetectomy
This technique has been used in short series of
patients with PF O-A with satisfactory results
[17]. It consists in a resection by vertical
osteotomy of the most lateral part of the lateral
patellar facet, with its corresponding osteophyte,
Patellofemoral Arthroplasty. Pearls and Pitfalls
leaving the lateral retinaculum open to reduce the
pressure on the lateral facet. It should only be
indicated if the osteoarthritis is limited to the
lateral facet and it is associated with a lateral
subluxation of the patella with an increase in its
tilt. Its results are more predictable when the
cartilage lesions of the lateral facet are not full
thickness.
601
meta-analysis [21] TKAs have a significant lower
revision rate than PFAs. For this reason, in
elderly patients, for whom a TKA has a high
chance of being a single surgery that does not
require further revisions, it is the preferred
indication.
8
7.5 Total Knee Arthroplasty (TKA)
Although the majority of TKAs are used for the
treatment of bi- or tricompartmental osteoarthritis
of the knee, several authors have reported good
results in the use of TKAs for the treatment of
isolated PF O-A, similar to those obtained with
TKAs for tricompartmental osteoarthritis [18,
19]. However, these cases often require a section
of the lateral retinaculum to achieve a good
patellar tracking [19].
TKA is probably still the best treatment for
isolated PF O-A in very advanced stages in older
patients, from 65 or 70 years of age. In studies
based on National Registries [20], and also in
Fig. 10 Preservation of
bone, ligaments and menisci
during implantation of a left
patello-femoral arthroplasty
Advantages of PFAs
Compared to the alternative of a TKA (which
probably remains the gold standard for the
elderly patients), PFAs have several advantages:
– Greater bone preservation (Fig. 10). This
allows the revision of a PFA to be performed
with a primary TKA, without the need for
metallic augments or stems (unlike TKAs, that
frequently need these elements and a greater
degree of constriction in their revision).
– More normal kinematics: By preservation of all
knee ligaments and both menisci, in addition to
the preservation of the femoro-tibial joint.
– Lower risk of perioperative complications
(infection or deep vein thrombosis)
602
P. Hinarejos
–
–
–
–
Less perioperative bleeding [22]
Less hospital stay
Faster postoperative rehabilitation
Better functional results: In a randomized
study with 100 knees with isolated PF-OA, a
higher score in the KOOS-Symptoms, less
pain in the SF-36 and a better range of motion
was observed in the PFA group than in the
TKA group [23]
– Greater possibility to return to sports activity
[22]
All the aforementioned advantages make
PFAs an alternative to be seriously taken into
account in young patients.
9
Surgical Technique
After an anterior longitudinal incision, a medial
parapatellar arthrotomy is usually performed
(although some authors recommend a lateral
arthrotomy) [13], taking special care not to injure
the medial meniscus anterior horn (Fig. 11).
Injury to cartilage in preserved areas must also be
avoided.
Fig. 11 Medial knee
arthrotomy, preserving the
anterior horns of both menisci
and the intermeniscal
ligament
A partial excision of retropatellar fat pad and a
synovectomy of the subquadricipital area are
performed. Intraoperatively, the indemnity of the
femoro-tibial joints must be verified.
In onlay prostheses (the most frequently used
today) an anterior cut of the femur is performed,
looking for an external rotation with respect to
the posterior bicondylar line to improve the
patellar tracking, trying to make this cut parallel
to the transepicondylar axis and perpendicular to
the Whiteside’s line [24] (Fig. 12). This cut must
end at the level of the anterior cortex of the
femoral shaft, avoiding a trochlear component
overstuffing that cause an increase in the anterior
space of the knee. The size of the component
must be adjusted to the size of the bone (Fig. 13),
trying to avoid an abrupt transition between the
metal component and the bone that can cause an
impingement of the patella. If we use a symmetrical trochlear component, we must seek to
align it in a certain valgus (usually 7–10°) with
respect to the joint line to improve the patellar tracking centered on the trochlea. In the
case of third-generation, anatomical PFA, the
valgus is already incorporated into the implant
[24].
Patellofemoral Arthroplasty. Pearls and Pitfalls
Fig. 12 Anterior cutting
guide of the trochlea in a left
PFA, oriented in external
rotation respect to the
posterior condyles, taking as
reference the epicondylar line
(and the Whiteside line)
Fig. 13 Trochlear
component should not be
raised with respect to the
anterior cortex or in flexion to
avoid protrusion of the patella
with the edge of the trochlea
603
604
P. Hinarejos
Fig. 14 Medialization of the
cemented symmetric patellar
component in the patellofemoral arthroplasty
The patella will be replaced trying to reproduce
the thickness of the original patella and trying to
medialize the patellar component to improve
patellar tracking (Fig. 14), although this medialization should not be excessive. Very frequently
the wear of the patella is not only from the cartilage, but also from the bone, and this can create a
mistake about the previous thickness of the patella.
In any case, a minimum thickness of 12 mm in the
bone remnant of the patella must be tried to be
mantained, since a smaller thickness increases the
risk of patellar fracture [13]. Some authors have
used PFAs without patellar replacement, but in
some cases thet have had to perform a patellar
resurfacing in a second surgery in a subgroup of
patients [25]. The systematic replacement of the
patella is widely recommended.
With the trial components, the correct patellar
tracking must be assessed (Fig. 15), and the lateral tilt or subluxation of the patella should be
corrected. If these signs of patellar instability are
found, a lateral patellar release must be performed. The rate of patients who required a lateral patellar release is highly variable between
series, reaching up to 82% in some of them [22].
Other authors suggest performing a vertical
patellectomy of 10–15 mm including the lateral
osteophyte of the patella [6], avoiding the lateral
patellar soft tissue release.
The absence of impingement between the
patella and the superior edge of the trochlea during
the range of motion must also be checked [26].
Associated procedures
– In cases of severe patella alta, a distalization
osteotomy of the TT may be associated to
ensure that the patella articulates with the
trochlea when the knee is in full extension [9].
Not treating a patella alta when implanting a
PFA has been associated with lower postoperative outcomes in some series [27], but not
in some others [28].
– In cases of severe instability with lateralization of the TT (high distance TT-GT), it may
be necessary to associate a medialization of
the TT to ensure that the patella moves centered on the trochlea.
– In cases of significant low patella, a proximalization osteotomy of the TT or lengthening of the patellar tendon may be indicated.
Patellofemoral Arthroplasty. Pearls and Pitfalls
605
Fig. 15 Checking of the
patellar tracking along the
flexion–extension range of
motion, without patellar
subluxation or excessive tilt
10
Postoperative Treatment
and Rehabilitation
Although the incidence of infectious or thromboembolic complications is lower than that of
TKAs, the use of antibiotic and antithrombotic
prophylaxis similar to that used in TKAs is recommended. The analgesic guidelines in the
postoperative period are also similar to those of
the TKAs, but the need for opioids after surgery
is frequently lower than after TKAs.
In the postoperative period, knee mobilization
and weight bearing should begin immediately.
Physiotherapy protocols after PFAs are usually
almost identical to those for TKAs.
11
PFAs Results
With first-generation PFAs, the percentage of
good and excellent results at 5–10 years was
highly variable: from just 45% with the Lubinus
prosthesis [4] to around 85% with the Richards
prosthesis, highly depending on the specific
implant design. With these models, a frequent
cause of revision was patella instability, up to
43% in some series [29].
With second-generation PFAs, designed with
a wider trochlear angle and less constriction, the
percentage of good and excellent results in the
short and mid term has increased to 85–94% [2,
8]. With these models, the need for revision due
606
to mechanical problems (patella instability) has
greatly decreased and the main cause of revision
is disease progression to the femoro-tibial compartments. A systematic review comparing the
functional outcomes (measured with KSS, OKS,
and WOMAC) of second-generation PFAs to
TKAs for the treatment of isolated PF O-A
concluded that there is no difference between
both treatments in terms of function [30].
Ackroyd reported in a 5.2 years follow-up
study with Avon PFA a revision rate of 15% and
progression of osteoarthritis to the other compartments was the main cause of revision [8].
Some series of second-generation inlay PFAs,
with a 5-year follow-up reported a similar revision rate of 17%, but in the case of inlay PFAs
the main cause of revision was persistent pain
[31]. When inlay PFAs were compared to onlay
PFAs in the Australian Registry, the 5-year
revision rate was higher than 20% for the former
and lower than 10% for the latter [2].
Leadbetter et al., in a multicenter study with
the Avon PFA and a follow-up of 2–6 years,
reported a 90% rate of patients without pain in
daily life activities, with an improvement in the
KSS from 56 to 83 points [10]. The results of
PFAs seem to be better in the group of patients
whose diagnosis was trochlear dysplasia than in
the group with primary osteoarthritis [27]. In a
comparative study between PFAs and TKAs in
young patients, it was concluded that the
improvement in symptoms and functionality
assessed by different scores is similar between
both groups at 2-years [32].
In a longer-term series, van Jonbergen et al.
reported a series of 185 Richards II type PFAs
with a survival rate of 84% at 10 years and 69%
at 20 years [33]. Survival was not influenced by
age, gender, or primary diagnosis, but it
decreased in obese patients. Femoro-tibial
osteoarthritis was observed in 45% of patients
in the long term, but had only required conversion to TKAs in 13% of them.
There are few publications of the third generation of PFAs, with an anatomical trochlear
component, but some of them suggest a low
revision rate (around 5%) in the short to medium
P. Hinarejos
term (5 years) [34, 35]. Nevertheless, the revision cumulate rates of PFAs from several
National Registries remain higher than those of
TKAs [36].
In addition to an improved survival rate in
recent decades, the functional result is similar to
or better than that of TKAs [23, 37, 38] and the
satisfaction rate is high, with 78% having no
residual postoperative symptoms. 80% of
patients would recommend this type of surgery to
others [34], and the rate of satisfied and very
satisfied patients exceeds 90% [35]. Moreover,
from an echonomical point of view, PFAs are
more cost-effective than TKAs, at least in the
short term [39].
The reported results of PFAs in the last decade
have encouraged some authors to expand the
indications, combining its use with unicompartmental prosthesis if it is associated with femorotibial osteoarthritis in only one of its compartments [25, 35].
12
Complications of PFAs
12.1 Early Complications
The incidence of readmissions after PFAs at
30 days (4.3%) is similar or slightly lower than
that of TKAs [11], and most of the causes that
require readmission are related to medical complications such as bleeding requiring transfusion,
urinary tract infections or deep vein thrombosis.
The reoperation rate at 30 days is 1.5% [11].
Most early complications (excluding infections) are secondary to poor surgical technique.
– Patellar instability: This complication was
much more frequent in first-generation PFAs,
with inlay components, in which the trochlea
had to be accommodated to the patient’s
anatomical trochlea. If a previous trochlear
dysplasia is present, it is not corrected with an
inlay component and a postoperative subluxation or excessive tilt of the patella could
remain if it is not diagnosed and corrected in
the same surgical act. With onlay
Patellofemoral Arthroplasty. Pearls and Pitfalls
components, a mistake to achieve a proper
external rotation of the trochlea can also cause
lateral instability of the extensor mechanism.
If patellar instability is observed during surgery, it must be corrected by adjusting the
rotation of the trochlear component and
associating lateral patellar release. When
necessary, a medialization osteotomy of the
TT should be added.
– Protrusion of the patella: Placing the trochlear
implant in flexion can cause a patellar clunk
when the patella engages with the elevated
trochlear component (Fig. 16).
– Perirpatellar pain: It may be the consequence
of an increase in the anterior space of the
knee, due to an insufficient cut or a too thick
component, either in the trochlea or in the
patella [40]. This pain can also appear if a
trochlear component that is too large is used,
protruding medially or laterally and irritating
the synovium at this level.
– Postoperative stiffness: A percentage of 3–
14% of patients may require a manipulation
under anesthesia to improve postoperative
knee flexion if postoperative flexion is less
Fig. 16 Excessive elevation of the trochlear component
over the anterior cortex of the patella. It can cause anterior
pain due to thickening of the anterior knee space, or
protrusion of the patella when beginning knee flexion
607
than 90° [8, 33]. This complication is more
frequent if the trochlear component is too
thick or it is implanted in a too anterior
position, or if a too thick patella is mantained,
causing excessive tension in the anterior space
of the knee.
12.2 Late Complications
– Prosthetic loosening and wear of the patellar
button: These are rare complications, but they
can be treated with an isolated revision of the
patellar component. Loosening rate is < 1%
at mid term follow-up [2].
– Persistent pain: The presence of persistent
pain, without evidence of any other complication, is the cause of revision of PFAs in up
to 16% of cases [41], and even higher in inlay
PFAs [31].
– Chronic effusions: It is not uncommon to
observe long-term joint effusions, especially if
there are technical errors like placement of the
trochlear component in internal rotation [10].
– Progression of degenerative disease to the
femoro-tibial compartments: It is the most
frequent cause of PFA revision in almost all
case series and all national registries [42]. In
the Australian Registry, the progression of
osteoarthritis to the other compartments is the
cause of the revision of PFAs in 56% of cases
[36]. For this reason, the proper selection of
PFA candidates is very important, as they
must not have degenerative femoro-tibial
changes at the time of surgery, morbide obesity, or varus or valgus malalignment, conditions that can make the evolution of the
disease easier. The progression of the disease
to the femoro-tibial joint (Fig. 17) seems to be
more frequent in cases of primary
osteoarthritis than in those cases with trochlear
dysplasia
or
post-traumatic
osteoarthritis [22]. A case–control study suggested that the use of second-generation inlaytype PFA (the Hemicap Wave from Arthrosaurace, USA) seems to be associated with a
lower rate of disease progression to other
608
P. Hinarejos
13
Fig. 17 Rosenberg view at long-term follow-up of PFA
(14 years): Progression of the degenerative disease to the
lateral femoro-tibial compartment
compartments in the short term (2 years) than
the use of an onlay-type PFA, and the cause
could be that a significant percentage of
patients after an onlay PFA have synovitis
and persistent effusions, with cytokines which
cause the evolution of degenerative changes
to the other compartments [43].
Fig. 18 Appearance of the
trochlea after removal of the
component during a revision
to a total knee arthroplaty:
Almost complete preservation
of the bone remnant
PFA Revision
Despite the progressive improvement in PFAs
results in the last four decades, the revision rate
of PFAs is still significantly higher than that of
TKAs, around 10% at 6 years and above 15% at
10 years follow-up [36].
There is a series of 14 first-generation Lubinus
PFAs, which were revised to new Avon secondgeneration PFAs, with clinical improvement
[44], but in these cases the revision was due to
patellar instability and wear of polyethylene.
A revision of a PFA to another PFA should only
be considered in the presence of a well-known
cause and in the presence of femoro-tibial compartments without any arthritic involvement. In
all other cases, the failure of a PFA must be
treated with a revision to a TKA [9].
The revision of a PFA to a TKA is usually a
simple surgery, similar to the implantation of a
primary TKA, since there are no significant bone
defects (Fig. 18) or problems with the ligament
balance. The TKA used in the PFA revision can
be performed with retention or with sacrifice of
the posterior cruciate ligament, and both strategies appear to give similar results [36].
Patellofemoral Arthroplasty. Pearls and Pitfalls
609
Fig. 19 Checking during a
revision of the PFA (due to
disease progression):
Adequate fixation and
absence of wear of the patellar
component of the PFA
As said before, the most common cause of
revision of PFAs is disease progression to the
femoro-tibial compartments [42]. Except when
there is an excessive wear or loosening of the
patellar component, the patellar button can be
preserved (Fig. 19). In a large series based on the
Australian registry only 42% of the patellar
components were revised during revision from a
PFA to a TKA [36].
One case series found that the results of
revision of PFA to a TKA are similar to those of
a primary TKA [45]. However, data from the
Australian Registry suggest that the survival of
TKAs after a PFA could be lower than that of
primary TKAs [36].
14
Take-Home Messages
1. Adequate patient selection is essential in the use
of PFAs. The preoperative study of the patient
must confirm that femoro-tibial compartments
are undamaged and it should rule out the presence of severe limb malalignment.
2. Careful surgical technique is also fundamental
to obtain satisfactory results. Contemporary
PFAs have instruments that make the technique more reproducible, but attention must
be paid to some technical details, such as the
correct choice of the size, the placement of the
correct degree of flexion of the trochlear
component, and avoiding to increase the
anterior space of the knee.
3. The results of contemporary PFAs appear to
be clearly superior to those of the models
used 2–3 decades ago. Although the survival
rate of PFAs is not yet the same as that of
TKAs, the fact that they have some advantages such as a faster postoperative recovery
and slightly superior functional results, the
use of PFA is recommended in young patients
with isolated PF-OA.
4. The most common cause of PFAs failure is
the progression of osteoarthritis to the other
compartments, but revision of the PFA is in
most cases a simple surgery with reproducible
results.
5. The use of PFAs is a useful treatment in
isolated PF-OA, especially in relatively
young patients, but in patients older than
70 years, the use of TKAs is recommended
because of their more reproducible results.
610
15
P. Hinarejos
Key Message
PFA is a useful treatment of isolated PF-OA in
relatively young patients, but an adequate patient
selection and careful surgical technique are
essential factors to achieve satisfactory results.
References
1. Davies AP, Vince AS, Shepstone L, Donell ST,
Glasgow MM. The radiologic prevalence of patellofemoral osteoarthritis. Clin Orthop Relat Res.
2002;402:206–12.
2. Lonner JH, Bloomfield MR. The clinical outcome of
patellofemoral arthroplasty. Orthop Clin North Am.
2013;44:271–80.
3. Grelsamer RP, Stein DA. Patellofemoral arthritis.
J Bone Joint Surg Am. 2006;88:1849–60.
4. Tauro B, Ackroyd CE, Newman JH, Shah NA. The
Lubinus patellofemoral arthroplasty. A five to ten
year prospective study. J Bone Joint Surg Br
2001;83-B:696–701.
5. Amis AA, Senavongse W, Darcy P. Biomechanics of
patellofemoral joint prostheses. Clin Orthop Relat
Res. 2005;436:20–9.
6. Dejour D, Saffarini M, Malemo Y, Pungitore M,
Valluy J, Nover L, Demey G. Early outcomes of an
anatomic trochlear-cutting patellofemoral arthroplasty: patient selection is key. Knee Surg Sports
Traumatol Arthrosc. 2019;27:2297–302.
7. Borus T, Brilhault J, Confalonieri N, Johnson D,
Thienpont E. Patellofemoral joint replacement, an
evolving concept. Knee. 2014;21(Suppl 1):S47-50.
8. Ackroyd CE, Newman JH, Evans R, Eldridge JD,
Joslin CC. The Avon patellofemoral arthroplasty:
five-year survivorship and functional results. J Bone
Joint Surg Br. 2007;89:310–5.
9. Lustig S, Magnussen RA, Dahm DL, Parker D.
Patellofemoral arthroplasty, where are we today?
Knee
Surg
Sports
Traumatol
Arthrosc.
2012;20:1216–26.
10. Leadbetter WB, Seyler TM, Ragland P, Mont MA.
Indications, contraindications and pitfalls of
patellofemroal arthroplasty. J Bone Joint Surg
(Am) (Suppl 4) 2006;88: 122–137.
11. Rezzadeh K, Behery OA, Kester BS, Dogra T,
Vigdorchik J, Schwarzkopf R. Patellofemoral arthroplasty: short-term complications and risk factors.
J Knee Surg. 2020;33(9):912–8.
12. Tishelman JC, Pyne A, Kahlenberg CA, Gruskay JA,
Strickland SM. Obesity does not affect patientreported outcomes following patellofemoral arthroplasty. J Knee Surg. 2020. https://doi.org/10.1055/s0040-1713862. Online ahead of print.
13. Remy F. Surgical technique in patellofemoral arthroplasty. Orthop Traumatol Surg Res. 2019;105(1S):
S165–76.
14. Baker JF, Caborn DN, Schlierf TJ, Fain TB,
Smith LS, Malkani AL. Isolated patellofemoral joint
arthroplasty: can preoperative bone scans predict
survivorship? J Arthroplasty. 2020;35:57–60.
15. Fulkerson JP, Becker GJ, Meaney JA, Miranda M,
Folcik MA. Anteromedial tibial tubercle transfer
without bone graft. Am J Sports Med. 1990;18:490–6.
16. Lennox IA, Cobb AG, Knowles J, Bentley G. Knee
function after patellectomy. A 12- to 48-year followup. J Bone Joint Surg Br. 1994;76:485–487.
17. Yercan HS, Ait Si Selmi T, Neyret P. The treatment of
patellofemoral osteoarthritis with partial lateral facetectomy. Clin Orthop Relat Res. 2005;436:14–19.
18. Mont MA, Haas S, Mullick T, Hungerford DS. Total
knee arthroplasty for patellofemoral arthritis. J Bone
Joint Surg Am. 2002;84:1977–81.
19. Parvizi J, Stuart MJ, Pagnano MW, Hanssen AD.
Total knee arthroplasty in patients with isolated
patellofemoral arthritis. Clin Orthop Relat Res.
2001;392:147–52.
20. National Joint Registry for England and Wales. 15th
Annual Report 2018. https://www.hqip.org.uk/resource/
national-joint-registry-15th-annual-report-2018.
21. Dy CJ, Franco N, Ma Y, Mazumdar M,
McCarthy MM, Gonzalez Della Valle A. Complications after patello-femoral versus total knee replacement in the treatment of isolated patello-femoral
osteoarthritis. A meta-analysis. Knee Surg Sports
Traumatol Arthrosc. 2012;20:2174–2190.
22. Dahm DL, Al-Rayashi W, Dajani K, Shah JP,
Levy BA, Stuart MJ. Patellofemoral arthroplasty
versus total knee arthroplasty in patients with isolated
patellofemoral osteoarthritis. Am J Orthop (Belle
Mead NJ). 2010;39:487–91.
23. Odgaard A, Madsen F, Kristensen PW, Kappel A,
Fabrin J. The mark coventry award: patellofemoral
arthroplasty results in better range of movement and
early patient-reported outcomes than TKA. Clin
Orthop Relat Res. 2018;476:87–100.
24. Thienpont E, Lonner JH. Coronal alignment of
patellofemoral arthroplasty. Knee. 2014;21(Suppl
1):S51–7.
25. Benazzo F, Rossi SM, Ghiara M. Partial knee
arthroplasty: patellofemoral arthroplasty and combined unicompartmental and patellofemoral arthroplasty
implants–general
considerations
and
indications, technique and clinical experience. Knee.
2014;21(Suppl 1):S43–6.
26. Lonner J. Patellofemoral arthroplasty. Pros, cons,
design considerations. Clin Orthop. 2004;428:158–165.
27. Dai Y, Diao N, Lin W, Yang G, Kang H, Wang F.
Patient-reported outcomes and risk factors for
decreased improvement after patellofemoral arthroplasty. J Knee Surg. 2021. https://doi.org/10.1055/s0041-1735159.
Patellofemoral Arthroplasty. Pearls and Pitfalls
28. Bernard CD, Pareek A, Sabbag CM, Parkes CW,
Krych AJ, Cummings NM, Dahm DL. Pre-operative
patella alta does not affect midterm clinical outcomes
and survivorship of patellofemoral arthroplasty. Knee
Surg Sports Traumatol Arthrosc. 2021;29:1670–7.
29. Blazina ME, Fox JM, Del Pizzo W, Broukhim B,
Ivey FM. Patellofemoral replacement. Clin Orthop
Relat Res. 1979;144:98–102.
30. Bunyoz KI, Lustig S, Troelsen A. Similar postoperative patient-reported outcome in both second generation patellofemoral arthroplasty and total knee
arthroplasty for treatment of isolated patellofemoral
osteoarthritis: a systematic review. Knee Surg Sports
Traumatol Arthrosc. 2019;27:2226–37.
31. Imhoff AB, Feucht MJ, Bartsch E, Cotic M,
Pogorzelski J. High patient satisfaction with significant improvement in knee function and pain relief
after mid-term follow-up in patients with isolated
patellofemoral inlay arthroplasty. Knee Surg Sports
Traumatol Arthrosc. 2019;27:2251–8.
32. Kamikovski I, Dobransky J, Dervin GF. The clinical
outcome of patellofemoral arthroplasty vs total knee
arthroplasty in patients younger than 55 years.
J Arthroplasty. 2019;34:2914–7.
33. Van Jonbergen H-P, Poolman RW, van Kampen A.
Isolated patellofemoral osteoarthritis. A systematic
review of treatment options using the GRADE
approach. Acta Orthopedica. 2010;81:199–205.
34. Rammohan R, Gupta S, Lee PYF, Chandratreya A.
The midterm results of a cohort study of patellofemoral arthroplasty from a non-designer centre using
an asymmetric trochlear prosthesis. Knee.
2019;26:1348–53.
35. Romagnoli S, Marullo M. Mid-term clinical, functional, and radiographic outcomes of 105 Genderspecific patellofemoral arthroplasties, with or without
the association of medial unicompartmental knee
arthroplasty. J Arthroplasty. 2018;33:688–95.
36. Lewis PL, Tudor F, Lorimer M, McKie J, Bohm E,
Robertsson O, Makela KT, Haapakoski J, Furnes O,
Bartz-Johannessen C, Nelissen RGHH, Van Steenbergen LN, Fithian DC, Prentice HA. Short-term
revision risk of patellofemoral arthroplasty is high:
611
37.
38.
39.
40.
41.
42.
43.
44.
45.
an analysis from eight large arthroplasty registries.
Clin Orthop Relat Res. 2020;478:1222–31.
Joseph MN, Achten J, Parsons NR, Costa ML; PAT
Trial Collaborators. The PAT randomized clinical
trial. Bone Joint J. 2020;102-B:310–318.
Peng G, Liu M, Guan Z, Hou Y, Liu Q, Sun X,
Zhu X, Feng W, Zeng J, Zhong Z, Zeng Y.
Patellofemoral arthroplasty versus total knee arthroplasty for isolated patellofemoral osteoarthritis: a
systematic review and meta-analysis. J Orthop Surg
Res. 2021;16(1):264.
Fredborg C, Odgaard A, Sørensen J. Patellofemoral
arthroplasty is cheaper and more effective in the short
term than total knee arthroplasty for isolated
patellofemoral osteoarthritis: cost-effectiveness analysis based on a randomized trial. Bone
Joint J. 2020;102-B: 449–457.
Mofidi A, Bajada S, Holt MD, Davies AP. Functional
relevance of patellofemoral thickness before and after
unicompartmental patellofemoral replacement. Knee.
2012;19:180–4.
Bendixen NB, Eskelund PW, Odgaard A. Failure
modes of patellofemoral arthroplasty-registries vs.
clinical studies: a systematic review. Acta
Orthop. 2019;90:473–478.
van der List JP, Chawla H, Villa JC, Pearle AD. Why
do patellofemoral arthroplasties fail today? A systematic review Knee. 2017;24:2–8.
Feucht MJ, Cotic M, Beitzel K, Baldini JF, Meidinger G, Schöttle PB, Imhoff AB. A matched-pair
comparison of inlay and onlay trochlear designs for
patellofemoral arthroplasty: no differences in clinical
outcome but less progression of osteoarthritis with
inlay designs. Knee Surg Sports Traumatol Arthrosc.
2017;25:2784–91.
Hendrix MR, Ackroyd CE, Lonner JH. Revision
patellofemoral arthroplasty: three- to seven-year
follow-up. J Arthroplasty. 2008;23:977–83.
van Jonbergen HP, Werkman DM, van Kampen A.
Conversion of patellofemoral arthroplasty to total
knee arthroplasty: a matched case-control study of 13
patients. Acta Orthop. 2009;80:62–6.
Clinical Cases—Primary and Revision
Patellofemoral Surgery Patellofemoral
Joint Preservation Surgery A
Case-Based Approach
In this section of the book, 11 clinical cases that
represent real situations that we encounter in our
daily clinical practice are presented. The goal of
case-based teaching is to engage the reader in
real-world decision making. This pedagogical
approach aims to apply the knowledge acquired
by the reader in the two previous sections of this
book to solve the clinical cases presented.
Another objective of this section is to
emphasize that prosthetic surgery is not necessarily the first option for treating patients with
severe patellofemoral chondropathies. This clinical entity is typical of active young people.
Therefore, all our efforts must be focused on
performing joint preservation surgery and
avoiding prosthetic surgery. In the cases that are
presented in this section, the importance of torsional abnormalities in the treatment of patients
with patellofemoral pain is emphasized. In
addition, the cases presented show that the etiology of patellofemoral disorders is multifactorial. Therefore, a complete physical examination
and imaging studies to discover all the anatomical abnormalities that the patient presents, of
which there are often many, is crucial. We must
strive to restore normal anatomy, because that
will create a better biomechanical environment
for the repaired tissue. We must understand
biomechanics because orthopedic surgery is a
mechanical engineering discipline.
I believe that these cases are a good stimulus
for our intellectual activity and will make us
forget many of the dogmas that we have been
taught. These cases will provide us with the
opportunity to learn something new.
Case # 1: Disabling Anterior Knee
Pain After Failed MPFL
Reconstruction in a Patient
with Patellar Chondropathy, Femoral
Anteversion and External Tibial
Torsion
Vicente Sanchis-Alfonso and Alejandro Roselló-Añón
1
Clinical Case
This is the case of a 22 years-old female (163 cm
in height and 51 kg, BMI 19.2) who came to our
office for a second opinion for disabling longlasting right anterior knee pain (AKP) since the
age of 16. It had shown itself resistant to conservative treatment. She also had right patellar
instability, but it was not her main complaint.
She had previously undergone a bilateral medial
patellofemoral ligament reconstruction (MPFLr).
The proposal made by the previous orthopedic
surgeon to solve the problem of her right knee
was a Tibial tubercle osteotomy (TTO).
Upon her visit to my office, the patient had
severe right AKP (VAS 7) despite her taking
medication (paroxetine, trazodone and tapentadol), and central sensitization (CSI 63). She
experienced quite significant limitations in her
daily living activities (Kujala score 36; IKDC
16.1) as well as a consequential decrease in her
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_42.
V. Sanchis-Alfonso (&) A. Roselló-Añón
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
quality of life (EuroQol 5D 2–2-2–2-2 [0.493]).
She had depression (HAD 11), catastrophizing
(PCS 30) and kinesiophobia (TSK 49). She also
had pain in the anterior aspect of her left knee.
But the knee that caused serious problems was
the right one and she wanted a resolution. For
her, the left knee was the good one.
2
Physical Examination
In the examination, we asked her to locate the
pain. She placed her hand over the anterolateral
aspect of the knee (see video). There was tenderness over the lateral retinaculum, pain with
the patellar glide test and with the axial compression test. Moreover, there was pain with
palpation of the inferior pole of the patella. The
patella could not be laterally dislocated but there
was a positive apprehension test with the lateral
displacement of the patella (see video). Patellofemoral tracking was normal (negative J-sign).
From a clinical standpoint, there was a right
femoral anteversion given that internal rotation
of the right hip exceeded external rotation by
more than 30 degrees (Fig. 1). Moreover, there
was excessive external tibial torsion on the right
side (Fig. 2). However, there was no squinting
patella despite the presence of femoral anteversion and external tibial torsion. In this patient, the
foot was externally rotated during the swing
phase of gait (see video).
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_42
615
616
V. Sanchis-Alfonso and A. Roselló-Añón
Fig. 1 During physical examination, the patient was seen to exhibit right femoral anteversion
Fig. 2 During physical
examination, the patient was
seen to exhibit right external
tibial torsion
Case # 1: Disabling Anterior Knee Pain After Failed MPFL Reconstruction …
617
Fig. 3 CT—patellar tunnels
for MPFLr. Arthroscopy—
Severe patellar chondropathy
Nobody had ever evaluated torsional
anomalies in this patient previous to visiting with me.
Femoral and tibial rotational abnormalities
are the most ignored factors in the diagnosis and treatment of AKP patients.
right 15 mm/left 14 mm; patellar tilt, right 3º/left
3º; femoral anteversion (Murphy´s method), right
39º/left 22º; external tibial torsion, right 43º/left
23º). Bone overload was detected using a
SPECT-CT scan (Fig. 4).
4
3
Imaging Studies
Plain radiographs were normal. There was no
lower-limb malalignment on the coronal plane.
In Fig. 3, one can see the patellar tunnels performed during MPFLr. The patellar tunnels
penetrate the articular face of the patella.
A CT scan was done to evaluate the patella
and the torsional abnormalities (TT-TG distance,
What to Do in Such a Situation?
The only objective pathological finding in this
patient was the torsional abnormality of both
femur and tibia. Therefore, our proposal was a
double level osteotomy, an intertrochanteric
external rotational femoral osteotomy of 20º
(39–20 = 19) and internal rotational tibial
osteotomy of 15º (43–15 = 28) just distal to the
tibial tuberosity. Since the proposed tibial derotation was less than 20º, the association of a
fibular osteotomy and the release of the peroneal
nerve were not considered.
618
V. Sanchis-Alfonso and A. Roselló-Añón
Fig. 4 The SPECT-CT scan showing an uptake increment in the lateral aspect of the patellofemoral joint (PFJ).
The SPECT-CT scan can reveal the metabolic and
geographic characteristics of bone homeostasis, which is
the normal osseous metabolic status of a living joint
5
7
Why not the Tibial Tubercle
Osteotomy?
First, the TTO is not done when the TT-TG distance is < 20 mm. Moreover, TT medialization
increases tibial external rotation, [1] which might
trigger more AKP. Lastly, femoral anteversion is a
poor prognostic factor in patients undergoing a
TTO. That is, the TTO does not prevent the negative effect of femoral anteversion on the PFJ [2].
6
Why Rotational Osteotomy?
Rotational osteotomy is the most powerful
treatment for the AKP patient with torsional
abnormalities.
The quadriceps, is responsible for the force
acting on the patella. Osteotomy changes the
quadriceps direction and therefore the force acting on the patella.
Special Considerations. Why
Double Level Rotational
Osteotomy?
This clinical case raises several questions. What
is more important in the genesis of AKP, femoral
anteversion or external tibial torsion? What
would be the ideal indication? Femoral osteotomy? Tibial osteotomy? Maybe both?
From an anatomical standpoint, the best
option to treat this patient would be a combination of the femoral and tibial osteotomy. Another
option would be to operate on the bone with the
greatest variance from normal. In this case, both
the torsional alteration of the femur and of the
tibia were of similar pathological magnitude.
Moreover, the foot was externally rotated during
the swing phase of gait in this patient. For this
reason, we decided on a double level (femoral
and tibial) osteotomy.
Case # 1: Disabling Anterior Knee Pain After Failed MPFL Reconstruction …
8
Follow-Up
In this case, the result was immediate relative to
the elimination of pain. Furthermore, twelve
months after surgery, the patient has no knee
pain at all and was able go up and down the stairs
in a natural way with no problem (see video).
Additionally, there is no apprehension. In Figs. 5
and 6, one can see the before and after of the
double level osteotomy. The X-rays at the 4month follow-up can be seen in Fig. 7. The
pattern of descending and ascending stairs has
been completely normalized. In the attached
video we can see how she went up and down the
stairs before the surgery, and at 3, 6, 9 and
12 months post-surgery. Moreover, in the
attached video you can hear the mother's testimony, which is sometimes more demonstrative
than the scores.
9
619
What Has This Case Taught Us?
Key Points
In the AKP patient, think about limb alignment,
not patellar alignment. Limb alignment is crucial,
especially torsional alignment. Skeletal torsional
abnormalities are the most ignored factors in the
diagnosis of AKP.
Not all patients with femoral anteversion have
squinting patella.
In some patients with torsional abnormalities,
as in the case presented here, the SPECT-CT
study reveals an uptake increment in the lateral
aspect of the PFJ that allows us to justify the pain
in these patients. Therefore, the SPECT-CT scan
helps to make a correct surgical indication.
Osteotomy is the most powerful and
underutilized treatment for the AKP patient with
torsional abnormalities.
Fig. 5 Correction of femoral anteversion after femoral rotational osteotomy
620
V. Sanchis-Alfonso and A. Roselló-Añón
Fig. 6 Correction of external tibial torsion after tibial rotational osteotomy
Fig. 7 X-rays at the 4-month follow-up
In this case, the patient is pain-free even
though the iatrogenic patellar chondropathy presented was left alone. In the PFJ, patellofemoral
congruence and smooth kinematics are much
more important than normal articular cartilage.
The presence of a psychological affectation, as
in the case at hand, should not be the excuse to
stop analyzing possible mechanical causes that
justify the pain of our patient and only send her
to a psychiatric unit. Even if it takes more
patience and tender loving care from the provider, we need to look hard for pathology and help
patients with psychological impairment.
In the same way, the presence of central
sensitization (CS) should not be the excuse to
stop analyzing possible mechanical causes that
justify the pain in our patient and send her to a
“Pain Unit”. There are patients with high values
in the CS score who have objective structural
causes that provide an explanation for the pain
Case # 1: Disabling Anterior Knee Pain After Failed MPFL Reconstruction …
that had gone undetected. Once the structural
cause is treated to improve or eliminate it, it
causes the CS score to drop drastically.
10
Conclusion
In the clinical case presented here, the restoration
of stability did not relieve the AKP, but it did
disappear after correction of femoral and tibial
maltorsion.
621
References
1. Mani S, Kirkpatrick MS, Saranathan A, et al. Tibial
tuberosity osteotomy for patellofemoral realignment
alters tibiofemoral kinematics. Am J Sports Med.
2011;39(5):1024–31.
2. Franciozi CE, Ambra LF, Albertoni LJ, et al.
Increased femoral anteversion influence over surgically treated recurrent patellar instability patients.
Arthroscopy. 2017;33(3):633–40.
Case # 2: Disabling Anterior Knee
Pain Recalcitrant to Conservative
Treatment in a Patient
with Patellofemoral Osteoarthritis
and Structural Femoral Retrotorsion
and Genu Varum
Vicente Sanchis-Alfonso and Alejandro Roselló-Añón
1
Clinical Case
This is the case of a 55 years-old female with
seriously disabling left anterior knee pain (AKP),
which was her main complaint, recalcitrant to
conservative treatment. Her VAS score stood at
between 6 and 7 almost every day. The VAS
score rose to 10 on various occasions throughout
the month. Moreover, she had pain in the left
groin area as well as ankle pain. It all started
when she was 48 years-old after a traffic accident. As a result of the accident, she suffered a
femur and tibia fracture that were not treated
adequately because the treating physicians
thought she was going to die. The injuries significantly limited her daily living activities
(Kujala score 31, IKDC 27). X-rays showed
lower left limb malalignment on the coronal
plane (genu varum of 4º) (Fig. 1). Computed
tomography (CT) showed patellofemoral
osteoarthritis (PFOA), left femoral retroversion
of 13º, measured with Murphy´s method (the
right side presented with a normal femoral
anteversion of 16º), left external tibial torsion of
25º (right side 18º) and a left knee rotation angle
of 7º (right side 4º). The diagnosis was left
V. Sanchis-Alfonso (&) A. Roselló-Añón
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
PFOA, a left femur fracture and a left tibia
fracture with a vicious consolidation (Figs. 1
and 2).
2
What to Do in Such a Situation?
She had visited various orthopedic surgeons that
had recommended different treatment options
like physical therapy, Fulkerson s osteotomy or a
patellofemoral replacement. However, all of
them said that her best option would be to handle
the pain and wait for a knee replacement.
The main problem in this case was the disabling AKP. Of course, the varus can contribute
to patellofemoral pain. Varus-valgus malalignment has been shown to influence the progression of PFOA [1]. Varus alignment increases the
likelihood of medial PFOA progression. In a
cadaveric study, Fujikawa and colleagues [2]
found an important alteration of the patellofemoral contact areas with the introduction of an
increment of varus alignment brought on by a
varus osteotomy. Nevertheless, it is our opinion
that the retroversion has more influence on her
knee pain. Moreover, we think that knee surgery
on a crooked skeleton is not what one would call
a good plan.
Our surgical plan was to perform a femoral
intertrochanteric internal de-rotational osteotomy
(25º) and a valgus opening wedge proximal tibial
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_43
623
624
V. Sanchis-Alfonso and A. Roselló-Añón
Fig. 1 Femur fracture with a vicious consolidation. Genu varum in the left side
Fig. 2 Bilateral tibial fracture with a vicious consolidation
Case # 2: Disabling Anterior Knee Pain Recalcitrant …
625
Fig. 3 Tibial osteotomy
osteotomy (Figs. 3, 4 and 5). Both surgeries were
performed in the same surgical time with a satisfactory clinical result.
3
The Conventional Thinking is ...
The association between femoral anteversion and
AKP or patellar instability has been welldocumented in the medical literature, but very
few clinical studies have looked at femoral
retroversion and AKP. Lee and colleagues [3, 4]
performed the most cogent study that demonstrated the importance of femoral rotation in the
genesis of AKP. They found that an external
rotational deformity of the femur augments
patellofemoral contact pressure on the medial
facet of the patella. External rotation has been
related to medial PFJ pain due to a nonlinear
increase in the patellofemoral contact pressures
on the contralateral facets of the patella [3].
A few authors have confirmed the importance of
external femoral rotation in the genesis of
AKP. Cibulka and Threlkeld-Watkins [5] reported an unusual case of patellofemoral pain in a
patient with excessive asymmetric external hip
rotation. Yildirim and colleagues [6] observed
that an external rotation deformity of the femur
greater than 10° could cause a deterioration in the
patellofemoral scores and provoke AKP. Karaman and colleagues [7] showed that both external
and internal rotational malalignment, greater than
or equal to 10° after closed intramedullary nailing of femoral shaft fractures, caused AKP while
climbing stairs. Finally, Jaarsma and colleagues
[8] found that patients with a torsional deformity
after femoral nailing due to shaft fractures had
difficulty with more demanding activities like
practicing sports activities and climbing stairs.
External rotational malalignment caused more
626
Fig. 4 Double level osteotomy
Fig. 5 Double level
osteotomy in the left side.
Physical examination. Preop
(above). Postop (below)
V. Sanchis-Alfonso and A. Roselló-Añón
Case # 2: Disabling Anterior Knee Pain Recalcitrant …
627
functional problems than internal rotational
malalignment in that series.
The ideal osteotomy site after post-fracture
deformity would be at the fracture site.
Double-level osteotomy surgery is an aggressive approach prone to major complications.
results in a resolution of pain. The patient noticed
an immediate improvement after the surgery. The
knee pain as well as the ankle and hip pain
completely disappeared.
References
4
What Has This Case Taught Us?
This Case Shows ...
Retroversion can cause AKP. Moreover, retroversion can be more symptomatic than anteversion.
Of course, correction at the fracture site is
preferable. The ideal osteotomy site to correct
retroversion would be at the fracture site. But the
risk of pseudoarthrosis and the important deformity at the fracture site, makes the surgery more
aggressive and difficult. Moreover, if we correct
the varus deformity at the fracture site, the correction would be very good, and the joint line
would not become oblique. However, we were
afraid of pseudoarthrosis. In this case, the correction away from the fracture site has given
good results.
There is not greater risk of DVT with doublelevel osteotomy surgery [9]. The key is an
“atraumatic surgery” that is a surgery without
excessive tissue trauma, without a tourniquet and
immobilization. CPM must begin immediately
after surgery.
5
Conclusion
Femoral retroversion should be considered in the
evaluation of the mechanical causes of
AKP. Restoring the normal rotational alignment
1. Elahi S, Cahue S, Felson DT, et al. The association
between varus-valgus alignment and patellofemoral
osteoarthritis. Arthritis Rheum. 2000;43:1874–80.
2. Fujikawa, K, Seedhom BB, Wright V. Biomechanics
of the patellofemoral joint. Part II: a study of the effect
of simulated femoro-tibial varus deformity on the
congruity of the patellofemoral compartment and
movement of the patella. Eng Med. 1983;12: 13–21
3. Lee TQ, Anzel SH, Bennett KA, et al. The influence of
fixed rotational deformities of the femur on the
patellofemoral contact pressures in human cadaver
knees. Clin Orthop. 1994;302:69–74.
4. Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. J Orthop Sports Phys Ther.
2003;33:686–93.
5. Cibulka MT, Threlkeld-Watkins J. Patellofemoral pain
and asymmetrical hip rotation. Phys Ther. 2005;85
(11):1201–7.
6. Yildirim AO, Aksahin E, Sakman B. The effect of
rotational deformity on patellofemoral parameters
following the treatment of femoral shaft fracture. Arch
Orthop Trauma Surg. 2013;133(5):641–8.
7. Karaman O, Ayhan E, Kesmezacar H, et al. Rotational
malalignment after closed intramedullary nailing of
femoral shaft fractures and its influence on daily life.
Eur J Orthop Surg Traumatol. 2013;24(7):1243–7.
8. Jaarsma RL, Pakvis DFM, Verdonschot N, et al.
Rotational malalignment after intramedullary nailing
of femoral fractures. J Orthop Trauma. 2004;18
(7):403–9.
9. Sanchis-Alfonso V, Domenech J, Ferras-Tarrago J,
et al. The incidence of complications after derotational
femoral and/or tibial osteotomies in patellofemoral
disorders in adolescents and active young patients.
A systematic review with meta-analysis. Knee Surgery
Sports Traumatol Arthrosc (In press).
Case # 3: Severe Anterior Knee Pain
Recalcitrant to Conservative
Treatment in a Patient
with Functional Femoral
Retrotorsion
Vicente Sanchis-Alfonso, Marc Tey-Pons,
and Joan Carles Monllau
1
Clinical Case
A 28-year-old female who practiced athletics
came to our office with a history of severe left
anterior knee pain (AKP) (VAS 8) of 1 year of
evolution. Pain onset was secondary to a direct
traumatism of the knee from playing football.
She had great difficulty driving because of the
pain caused upon engaging the clutch, going
downstairs, wearing high heels, and sitting with
the knee bent for a long period of time (positive
“movie sign”). The psychological evaluation that
we routinely perform on our patients with AKP
did not indicate anxiety or depression. She had
kinesiophobia, catastrophizing and central sensitization. Imaging studies of the knee (X-rays,
CT and MRI) were normal. The mechanical axis
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
M. Tey-Pons J. C. Monllau
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
J. C. Monllau
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
of the lower limb was normal. There were no
torsional abnormalities. The physical therapy
program performed in our institution over 6
months was unsuccessful in improving her
symptoms. This pain forced her to give up sports
activities but she kept going to the gym.
Ten months later, she came back to our office
due to severe left hip pain (VAS 8) with no
history of traumatism to justify it. The hip pain
was so significant that it not only forced her to
leave the gym but also made for significant
limitations in her regular daily activities. Moreover, she continued to suffer from knee pain
(VAS 8). The Kujala Knee Score was 22 and the
Non-arthritic Hip Score was 28.75. During
physical examination of the hip, there was a
positive impingement test and a positive
decompression test. A Dunn radiograph view
showed an alpha angle of 58º in both hips. An
angle of > 55º is considered pathological. However, the right hip was completely asymptomatic.
A study by means of an arthro-MRI of the left
hip showed a Cam lesion and a detachment of the
anterior labrum. The final diagnosis was Cam
femoroacetabular impingement (Cam-FAI).
Prior to hip surgery, she was evaluated using
kinetic and kinematic analyses during gait and
stair ascent as the latter activity was the one that
brought about a major limitation in her daily life.
A pathway with two extensometric force plates
on its surface was used to carry out the gait
analysis. She was asked to walk at a high
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_44
629
630
cadence rate because the faster the subject walks,
the more evident the functional impairment
becomes. Before the data were collected, she
walked on the pathway several times until she
was able to walk with a natural and constant gait.
A portable two-step wooden staircase and two
independent dynamometric platforms, placed as
indicated in (Fig. 1), were used to perform the
kinetic analysis during the stair ascent test. An
eight-camera computer-aided video motion
analysis system and reflective passive markers
that determined the spatial position of the segments of the lower limb were used to carry out
the kinematic analysis (Fig. 2). All the markers
were placed on the lateral aspect of the leg to
allow for a correct visualization by the cameras
(Fig. 2). The kinetic and kinematic parameters
were analyzed using the NedRodilla/IBV software (Instituto de Biomecánica de Valencia,
Valencia, Spain). Preoperative gait analysis
showed an altered gait pattern (Fig. 3). Preoperative kinematic analysis showed a gait (Fig. 4A)
and stair ascent (Fig. 5A) pattern with external
rotation of the involved hip. Moreover, the hip
external rotation torque of the involved hip
increased significantly during stair ascent
(Fig. 5C).
Fig. 1 Portable two-step wooden staircase and two
independent dynamometric platforms were used to perform the kinetic analysis during the stair ascent test.
(Reused from Hindawi Publishing Corporation. SanchisAlfonso V, Tey M, Monllau JC. Cam femoroacetabular
V. Sanchis-Alfonso et al.
2
What to Do in Such a Situation?
Our Surgical Treatment
We performed a femoral neck osteoplasty and
reattachment of the labrum. During arthroscopy,
we confirmed the impingement mechanism with
the hip at 90º of flexion and maximum internal
rotation. With external femoral rotation, we
prevent the impingement and, in theory, the hip
pain. After hip surgery, no specific physiotherapy
treatment for the AKP was performed.
3
Follow-Up
At 6 months after surgery, the patient had no
discomfort in the hip, and knee pain had completely disappeared.
At 7 months, kinetic and kinematic analyses
were performed to evaluate the effects of hip
surgery on the preoperative biomechanical
parameters. They showed a normal gait pattern
(Fig. 3B) and a symmetric pattern between both
hips (Figs. 4B and 5B,D).
At final follow-up (7.5 years), the patient is
completely asymptomatic. With reference to both
the hip and knee, activities that previously could
impingement as a possible explanation of recalcitrant
anterior knee pain. Case Rep Orthop. Vol 2016, Article ID
2,064,894, https://doi.org/10.1155/2016/2064894. Copyright © 2016 Vicente Sanchis-Alfonso et al.)
Case # 3: Severe Anterior Knee Pain Recalcitrant to Conservative …
631
Fig. 2 Subject with reflective
markers used for kinematic
analysis. (Reused from
Hindawi Publishing
Corporation. Sanchis-Alfonso
V, Tey M, Monllau JC. Cam
femoroacetabular
impingement as a possible
explanation of recalcitrant
anterior knee pain. Case Rep
Orthop. Vol 2016, Article ID
2,064,894, https://doi.org/10.
1155/2016/2064894.
Copyright © 2016 Vicente
Sanchis-Alfonso et al.)
not be done or had been done with much difficulty like walking at a high cadence rate, going
up or down stairs, squatting, making turns with
the hip or using a car with a clutch were done
without any problem. Moreover, she runs without any limitation. A Dunn radiograph view
showed an alpha angle of 32º. At 7.5-years, the
postoperative Kujala Knee Score was 99 and the
postoperative Non-arthritic Hip Score was 91.25.
Postoperative pain intensity on the VAS was 0
for the knee and 0 for the hip.
4
What Does the Medical Literature
Tell Us About the Association
Between External Rotational
Femoral Deformity and AKP?
Lee and colleagues [1, 2] demonstrated the
importance of femoral rotation in the genesis of
AKP. They found that an external rotational
deformity of the femur increases patellofemoral
contact pressure on the medial facet of the
patella. Karaman and colleagues [3] showed that
both external and internal rotational malalignment greater than or equal to 10° after closed
intramedullary nailing of femoral shaft fractures
provoked AKP while climbing stairs. Jaarsma
and colleagues [4] found that patients with a
torsional deformity after femoral nailing due to
shaft fractures had difficulty with more
demanding activities like running, sports, and
climbing stairs. External rotational malalignment
caused more functional problems than internal
rotational malalignment in this series. Other
authors have confirmed the importance of external femoral rotation in the genesis of AKP.
Cibulka and Threlkeld-Watkins [5] reported an
unusual case of AKP in a patient with asymmetric excessive hip external rotation. Finally,
Yildirim and colleagues [6] observed that an
external rotation deformity of the femur greater
632
V. Sanchis-Alfonso et al.
Fig. 3 Gait analysis. A Preoperative. B Postoperative.
Red line, right lower limb. Blue line, pathologic lower left
limb. The preoperative study showed a decrease of the
vertical heel contact force that could be a defense
mechanism to avoid the load on the pathologic limb.
Notice the gait pattern normalization after surgery.
(Reused from Hindawi Publishing Corporation. SanchisAlfonso V, Tey M, Monllau JC. Cam femoroacetabular
impingement as a possible explanation of recalcitrant
anterior knee pain. Case Rep Orthop. Vol 2016, Article ID
2,064,894, https://doi.org/10.1155/2016/2064894. Copyright © 2016 Vicente Sanchis-Alfonso et al.)
Fig. 4 Kinematic gait analysis. Hip external rotation
angle. A Preoperative. B Postoperative (at the 7-month
follow-up). Red line, right hip. Blue line, pathological left
hip. Blue band, band of normality. Notice how the
preoperative non-pathological hip values differ from those
of the postoperative ones of the same hip. This is because
the pathological limb influences the healthy limb in the
kinematic and kinetic studies. What is relevant is that after
surgery, the values of both hips are in the normality band.
Furthermore, the external rotation of the hip that has been
operated on has decreased relative to the preoperative
status. (Reused from Hindawi Publishing Corporation.
Sanchis-Alfonso V, Tey M, Monllau JC. Cam femoroacetabular impingement as a possible explanation of
recalcitrant anterior knee pain. Case Rep Orthop. Vol
2016, Article ID 2,064,894, https://doi.org/10.1155/2016/
2064894. Copyright © 2016 Vicente Sanchis-Alfonso
et al.)
Case # 3: Severe Anterior Knee Pain Recalcitrant to Conservative …
633
Fig. 5 Kinematic analysis during stair ascending test.
(A and B−Hip external rotation angle) A Preoperative.
B Postoperative (at the 7-month follow-up). Red line,
right hip. Blue line, pathological left hip. Kinetic analysis
during stair ascending test. (C and D−Hip external
rotation moment) C Preoperative. D Postoperative (at
the 7-month follow-up). Red line, right hip. Blue line,
pathological left hip. On the x-axis, one can note the
stance phase percentage. The stance phase begins with the
heel strike and ends with the toe off. The normalization of
the kinematic and kinetic parameters can be seen after
cam-FAI resolution. (Reused from Hindawi Publishing
Corporation. Sanchis-Alfonso V, Tey M, Monllau JC.
Cam femoroacetabular impingement as a possible explanation of recalcitrant anterior knee pain. Case Rep
Orthop. Vol 2016, Article ID 2,064,894, https://doi.org/
10.1155/2016/2064894. Copyright © 2016 Vicente
Sanchis-Alfonso et al.)
than 10° could cause a deterioration in the
patellofemoral scores and provoke AKP.
mechanism to avoid hip impingement and the
associated hip pain [7]. Therefore, cam-FAI may
be responsible for functional femoral retroversion. Functional femoral retrotorsion may eventually provoke a patellofemoral joint imbalance
that in turn might be responsible for AKP [7, 8].
A Cam resection normalizes hip biomechanics
in the same way that the derotational osteotomy
does in structural retroverted femora.
This case highlights the importance of torsional abnormalities, a functional torsional
abnormality in this case, in the genesis of AKP.
5
What Has This Case Taught Us?
This Case Shows …
External hip rotation conditioned by the cam
morphology of the femoral head to avoid hip
impingement and pain behaves from a functional
point of view as a femoral retrotorsion [7]. In this
case, external hip rotation is a defense
634
6
V. Sanchis-Alfonso et al.
Conclusion
Femoral osteoplasty eliminated hip impingement
and therefore hip pain and normalized lower
extremity biomechanics. This could be responsible for the knee pain going away.
4.
5.
6.
References
1. Lee TQ, Anzel SH, Bennett KA, et al. The influence of
fixed rotational deformities of the femur on the
patellofemoral contact pressures in human cadaver
knees. Clin Orthop. 1994;302:69–74.
2. Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. J Orthop Sports Phys Ther.
2003;33:686–93.
3. Karaman O, Ayhan E, Kesmezacar H, et al. Rotational
malalignment after closed intramedullary nailing of
7.
8.
femoral shaft fractures and its influence on daily life.
Eur J Orthop Surg Traumatol. 2013;24(7):1243–7.
Jaarsma RL, Pakvis DFM, Verdonschot N, et al.
Rotational malalignment after intramedullary nailing
of femoral fractures. J Orthop Trauma [Internet].
2004;18(7):403–9.
Cibulka MT, Threlkeld-Watkins J. Patellofemoral pain
and asymmetrical hip rotation. Phys Ther. 2005;85
(11):1201–7.
Yildirim AO, Aksahin E, Sakman B. The effect of
rotational deformity on patellofemoral parameters
following the treatment of femoral shaft fracture. Arch
Orthop Trauma Surg. 2013;133(5):641–8.
Sanchis-Alfonso V, Tey M, Monllau JC. Cam
femoroacetabular impingement as a possible explanation of recalcitrant anterior knee pain. Case Rep
Orthop. 2016. https://doi.org/10.1155/2016/2064894.
Sanchis-Alfonso V, Tey M, Monllau JC. A novel
association between femoroacetabular impingement
and anterior knee pain. Pain Res Treat. 2015;2015.
https://doi.org/10.1155/2015/937431.
Case # 4: Disabling Anterior Knee
Pain in a Multi-operated Young
Patient with Severe Patellofemoral
Osteoarthritis and Medial Patellar
Instability
Vicente Sanchis-Alfonso
1
Clinical Case
A 41-year-old woman came to our institution
complaining mainly of disabling right patellar
instability and severe right anterior knee pain
(AKP) that had not improved with appropriate
physical therapy. It is worth mentioning that she
had serious psychological problems. The Kujala
score was of 24 points. The contralateral knee
was completely asymptomatic. She had visited 5
doctors before coming to us.
This patient had undergone surgery 3 years
earlier due to lateral patellar instability, being
instability the main symptom. Moreover, there
was a secondary symptom of mild occasional
pain during physical activity. An Insall’s proximal realignment and lateral retinaculum release
(LRR) were performed. After the surgery, the
patient indicated that the patellar instability had
increased. She also stated that it was different and
more incapacitating than the one she had before
surgery. Moreover, there was a severe pain with
day-to-day activities. Both instability and pain
were much worse than the ones prior to the
realignment surgery. One year and a half after
her realignment surgery, another surgeon suggested a knee arthroscopy to which the patient
agreed. With this second procedure (partial syn-
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
ovectomy and denervation), the patient did not
see any improvement.
A physical examination of the knee showed a
positive apprehension sign when pressing the
patella medially and a positive Fulkerson’s
relocation test. Additionally, there was an
apprehension sign when pressing the patella laterally. The rest of the physical examination was
completely normal. Conventional radiography
showed patellofemoral osteoarthritis (PFOA)
(Fig. 1). The radiographs prior to the first surgery
had shown no degenerative changes. An MRI
examination showed a lateral subluxation of the
patella and severe patellar chondropathy. A CT
examination at 0° of extension and with a relaxed
quadriceps showed mild lateralization of the
patella. The TT-TG index was 10 mm. There
were no torsional abnormalities. The stress CT of
the patellofemoral joint (PFJ) in extension
revealed medial patellar instability and a lateral
patellar displacement that was significantly
greater in the right knee in comparison to the left
knee (Fig. 2). A bone scan with Tc-99 m showed
increased pathologic uptake only in the patella
(Fig. 3).
Kinetic and kinematic analyses were performed during stair descent (Fig. 4). They
showed that the patient had a stair descent pattern
with knee extension, which is a strategy to avoid
instability and the subsequent pain. A decrease in
the stance phase duration on the platform was
also seen. It is a strategy to reduce the extensor
moment. There were also reduced values of the
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_45
635
636
V. Sanchis-Alfonso
Fig. 1 Patellofemoral osteoarthritis
Fig. 2 Multidirectional patellar instability as is seen in
the stress CT. Arrows indicate the direction of the stress
applied to the patella during stress CT. Lateral stress
causes an upward tilt. The lateral retinaculum prevents the
upward tilt with lateral stress
Fig. 3 Increased scintigraphic uptake in the patella that may explain the AKP in this patient
extensor moment with the subsequent reduction
in quadriceps contraction and, therefore, a
reduction of the PFJ reaction force, being the
final goal to reduce pain. Furthermore, the
analyses showed reduced values of the abduction
moment that provokes, a reduction of the lateral
tibiofemoral compression force on one hand and
a reduction of the force exerted proximally by the
Case # 4: Disabling Anterior Knee Pain in a …
637
A
B
C
D
Fig. 4 Knee kinetics and kinematics during stair descent.
A Knee joint angles during stair descent. B Ground force
reactions during stair descent. C Flexion–extension knee
moments during stair descent. D Abduction–adduction
knee moments during stair descent
medial collateral ligament on the other hand.
Here, the result is the reduction of the lateral and
medial tibiofemoral compression forces.
2
Diagnosis
Iatrogenic medial patellar instability and PFOA.
3
Our Surgical Treatment
Before reconstruction of the lateral retinaculum,
arthroscopy was performed. A severe PFOA was
noted but not treated. The rest of the findings
were normal. A reconstruction of the lateral
retinaculum, using the fascia lata, was performed
following the technique described by Jack
Andrish (Fig. 5) [1].
Fig. 5 Deep transverse lateral retinaculum reconstruction
following Andrish’s technique [1]
638
4
V. Sanchis-Alfonso
Follow-Up
Twelve months after surgery, the patient was
asymptomatic and was able to go down the stairs
in a natural manner without any problem. The
current follow-up of this patient comes to
12 years, and she is now completely asymptomatic. She carries on a normal life and is fully
satisfied with the surgery. The Postop Kujala
score was 94 (24 in the preop). Kinetic and
kinematic analyses during stair descent were
performed at 6 months and 12 months after
surgery and showed a progressive recovery of the
kinetic and kinematic parameters (Fig. 4).
She is pain free despite the severe PFOA and
the increment of the extensor moment and,
therefore, the increase in the PFJ reaction force
after surgery.
should be suspected in a patient who has
undergone previous patellar realignment surgery that has made the pain worse [2, 3].
– Take special care with the “extensive” LRR
because it could provoke a medial patellar
instability [3].
– This patient had to go to 5 doctors before
obtaining a diagnosis and an appropriate
treatment. This demonstrates that medial
patellar instability is a clinical condition that
most orthopedic surgeons do not know about.
Therefore, our belief is that there is a need to
make the diagnostic procedures for recognizing this clinical condition more widely
known.
6
5
What Has This Case Taught Us?
This Case Shows …
– Not all PFOA are associated with severe pain.
There is poor evidence that all cartilage
lesions are painful. The mere presence of a
cartilage lesion does not mean it is the source
of pain. In other words, structural damage of
the patellar articular cartilage does not always
result in AKP. In this case, the patellofemoral
imbalance (medial patellar instability) was
responsible for the pain.
– In the PFJ, patellofemoral congruence and
smooth kinematics are much more important
than normal articular cartilage.
– Iatrogenic medial patellar instability is a
specific condition that frequently causes
incapacitating AKP, severe disability, and
serious psychological problems. The diagnosis
Conclusion
This is an example of PFJ preservation surgery.
This begs the question as to whether articular
cartilage is essential in the PFJ. In other words,
does the PFJ in fact need articular cartilage? [4].
References
1. Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC,
Andrish J. Deep transverse lateral retinaculum reconstruction for medial patellar instability. Arthrosc Tech.
2015;4(3):e245–9.
2. Sanchis-Alfonso V, Montesinos-Berry E, Monllau JC,
Merchant AC. Results of isolated lateral retinacular
reconstruction for iatrogenic medial patellar instability. Arthroscopy. 2015;31(3):422–7.
3. Sanchis-Alfonso V, Merchant AC. Iatrogenic medial
patellar instability: an avoidable injury. Arthroscopy.
2015;31(8):1628–32.
4. Blønd L, Donell S. Does the patellofemoral joint need
articular cartilage? Knee Surg Sports Traumatol
Arthrosc. 2015;23(12):3461–3.
Case # 5: Multidirectional Patellar
Instability After Over-Medialization
of the Tibial Tubercle in a Patient
with Severe Trochlear Dysplasia
and Patella Alta
Vicente Sanchis-Alfonso
1
Clinical Case
This is the case of a 43-year-old woman who
came to my office for a second opinion for right
patellar instability and severe anterior right knee
pain. Instability was the main complain. She had
undergone an operation on both knees in which a
bilateral medialization of the tibial tubercle
associated to lateral retinaculum release was
performed. She experienced very significant
limitations in her daily life activities as well as a
quite notable decrease in her quality of life.
Physical examination demonstrated multidirectional (lateral and medial) patellar instability.
2
Imaging Studies
Imaging studies of the right knee showed pseudoarthrosis at the level of tibial tubercle osteotomy, knee osteoarthritis, a patella alta and
trochlear dysplasia (Figs. 1 and 2). Computed
Tomography showed: (1) Femoral anteversion
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_46.
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
according to Murphy’s method, right 26°/left
29°; (2) Knee rotation, right 10°/left 12°;
(3) External tibial torsion, right 33°/left 25°;
(4) TT-TG distance, right −8 mm/left 7 mm.
3
What to Do in Such a Situation?
As can be seen in the video of this case, the
patient had a clear alteration of patellofemoral
tracking (J-sign+). Prior to surgery and with the
patient under general anesthesia, axial stress
radiographs of the patellofemoral joint (PFJ)
were performed. They demonstrated a complete
medial patella dislocation when a force was
applied to the lateral side of the patella to displace it medially (Fig. 3). Moreover, a lateral
displacement of the patella of more than 50%
was observed when a force was applied to the
medial side of the patella to displace it laterally
(Fig. 3). Moreover, lateral stress caused an
upward tilt of the patella. At this point, it is
interesting to note that the lateral retinaculum
prevents the upward tilt of the patella with lateral
stress, which is also why it adds resistance to a
lateral displacement force.
My therapeutic proposal was:
3.1 Surgical Approach
– Elevate the tibial tuberosity to improve the
exposure of the trochlea.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_46
639
640
V. Sanchis-Alfonso
Fig. 1 Normal lower-limb alignment can be seen on the coronal plane, as well as bilateral knee osteoarthritis
Fig. 2 Pseudoarthrosis at the level of the tibial tubercle osteotomy, a patella alta and trochlear dysplasia
Case # 5: Multidirectional Patellar Instability After Over-Medialization of the Tibial Tubercle …
641
Fig. 3 Axial stress radiographs of the PFJ. The red arrow shows the force applied to the patella to displace it laterally
or medially. In the image on the left, how the patella is displace medially without applying stress to it can be seen
3.2 Correction of Patellofemoral
Maltracking
– A deepening trochleoplasty because the trochlear dysplasia is a major factor for patellar
instability.
– A lateralization and distalization of the tibial
tubercle because there is a patella alta and an
over-medialization of the tibial tubercle.
3.3 Stabilization of the PFJ: Ligament
Reconstruction
– MPFL and LPFL reconstruction if the patella
can be dislocated in both directions in spite of
maltracking correction.
Finally, we only carried out a trochleoplasty and
lateralization and distalization of the tibial
tubercle (Figs. 4 and 5), because instability
completely disappeared after the maltracking
correction (see video).
4
Follow-Up
12 months after the surgery, the patient had no
pain or instability and can go up and down the
stairs in a natural way with no problem. In
addition, she discharges her physically demanding work activity without problems.
5
Key Points
– The common belief that the presence of
osteophytes, that are a common radiographic
finding (Fig. 1), is pathognomonic for the
presence of osteoarthritis and that it is predictive of its progression is foolish [1].
In Fig. 6, severe chondropathy with exposed
642
A
V. Sanchis-Alfonso
B
C
Fig. 4 A Tubercle sulcus angle. B Over-medialization of the tibial tubercle. C Re-osteotomy of the tibial tubercle
(tubercle sulcus angle of 0°)
Fig. 5 Postop X-ray
bone in the patella can be observed. However,
there are no gross signs of osteoarthritis in the
femoral condyles.
– Not all PFOA are associated with severe pain.
In the PFJ, patellofemoral congruence and
smooth kinematics are much more important
than normal articular cartilage [2].
– Over-medialization of the tibial tubercle can
be avoided by means of an intraoperative
evaluation of the tubercle sulcus angle
(Fig. 4A). The intraoperative goal should be a
tubercle sulcus angle of 0° (Fig. 4C).
– In cases of multidirectional patellar instability
with patellofemoral maltracking, the first step
is always to correct the maltracking. Once the
maltracking has been corrected, we must
explore the stability of the PFJ again. If the
instability has disappeared, we should not do
a ligamentous reconstruction. If the instability
persists, despite correcting the maltracking,
the next step will be to reconstruct the MPFL.
If there is still medial instability afterwards,
the last step is to reconstruct the lateral
patellofemoral ligament.
– The medial transfer of the tibial tubercle has
been commonly used for the treatment of a
recurrent dislocation of the patella and patellofemoral malalignment. Kuroda and colleagues [3] have shown that tibial tubercle
medialization significantly increases both the
patellofemoral contact pressure and the contact pressure in the medial tibiofemoral compartment. Therefore, over-medialization of the
tibial tuberosity should be avoided in the
varus knee, the knee after medial meniscectomy, and the knee with preexisting degenerative arthritis of the medial compartment.
Case # 5: Multidirectional Patellar Instability After Over-Medialization of the Tibial Tubercle …
643
Fig. 6 Exposure of the surgical field after a tibial tubercle osteotomy
References
1. Teitge RA. CORR Insights®: Lateral-compartment
osteophytes are not associated with lateralcompartment cartilage degeneration in arthritic varus
knees. Clin Orthop Relat Res. 2017;475(5):1393–4.
2. Blønd L, Donell S. Does the patellofemoral joint need
articular cartilage? Knee Surg Sports Traumatol
Arthrosc. 2015;23(12):3461–3.
3. Kuroda R, Kambic H, Valdevit A, et al. Articular
cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med. 2001;29
(4):403–9.
Case # 6: Failed MPFL Reconstruction
in a Patient with Severe Trochlear
Dysplasia and Malpositioning
of the Femoral Attachment Point
Vicente Sanchis-Alfonso
1
Clinical Case
This is the case of a 35-year-old female (171 cm
in height and 53 kg, BMI 18.1) who came to my
office for a second opinion for right anterior knee
pain (AKP) after having undergone a previous
medial patellofemoral ligament reconstruction
(MPFLr). The AKP was the main complaint and
the secondary complaint was patellar instability.
Upon her visit to my office, the patient had
severe AKP in the right knee (VAS 8). She
experienced significant limitations in her daily
life activities (Kujala score 42; IKDC 40.2) as
well as a noteworthy decrease in her quality of
life (EuroQol 5D 2-1-2-2-2). She had a diagnosis
of anxiety (HAD 12), catastrophizing (PCS 40)
and kinesiophobia (TSK 58). She also had lateral
patellar instability and pain in the anterior aspect
of her left knee. However, it was the right knee
that caused serious problems and she wanted a
resolution.
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_47.
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
2
Physical Examination—Key
Points
At rest with the knee in extension, the patella is
located excessively lateral (Fig. 1) and she needs
to flex and to rotate the limb for the patella to line
up with the trochlea. Then, she is able to function
when the patella is in the trochlea (see video).
She must keep the knee flexed to function and to
prevent the excessive lateral position in extension. This is why she keeps her knee bent while
coming downstairs (see video). With knee flexion, the patella is centered. She can then walk
safely in flexion. Moreover, she has evident
bilateral patellofemoral maltracking (evident
J-sign).
3
Imaging Studies
X-rays demonstrated a minor degree of valgus of
the right limb, a misplaced MPFLr (a femoral
tunnel very proximal and anterior) and severe
trochlear dysplasia (Grade D) (Figs. 2 and 3).
Computed tomography showed: Patellar tilt,
right 44°/left 40°; TT-TG distance, right
22 mm/left 20 mm; Femoral anteversion
according to Murphy’s method, right 19°/left 8°;
Knee rotation, right 5°/left 8°; External tibial
torsion, right 31°/left 31°.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_47
645
646
V. Sanchis-Alfonso
Fig. 1 Significant lateral
dislocation in extension and
severe trochlear dysplasia
4
Questions Raised by This Case
In the medical literature, it is accepted that valgus
is a predisposing factor for lateral patellar instability [1]. This patient has a very discreet valgus.
Normally, the mechanical axis is near the medial
tibial spine. Could that degree of valgus be
considered pathological? In theory, coronal
alignment is more significant with height. This
patient is tall, and this makes the valgus vector
that displaces the patella laterally greater than
that of a shorter person who has the same valgus
(Fig. 4). Body weight has to be transferred
through the knee to the ground. We assume
weight transfer is “normalized” when the
mechanical axis is near the medial tibial spine,
about 1–2° varus. If there is a valgus (or varus)
deformity, the mechanical axis is shifted. The
longer the tibia and femur, the further the
mechanical axis is shifted. We often see no pain
or disability in children with limb deformity, but
pain often develops in adolescence. We assume
this is because of growth. The growth leads to
lengthening of the lever arms as well as increased
weight that is transferred to the ground. We
assume the long bones act as long lever arms. In
Fig. 4, the length of the limb on the left is ½ of
the length on the right. A tibiofemoral angle of
10° has been drawn. The mechanical axis deviation is almost double. Therefore, the mechanical
axis deviation is lateralized relatively more on
the longer limb. Of course, adding abnormal
torsion probably multiplies this effect.
Could the combination of a small degree of
valgus and a small degree of patella alta and
some external tibial rotation be enough to
Case # 6: Failed MPFL Reconstruction in a Patient with …
647
Fig. 2 Lower-limb alignment
on the coronal plane. Minor
degree of valgus
provide a lateral vector to the quad so the patella
will sit so far lateral?
Wilson and colleagues [1] observed a disappearance of the lateral patellar instability after an
isolated osteotomy of the distal femur, that is to
say, without any more associated surgical procedures. This shows how important genu valgum
is in the etiopathogenesis of lateral patellar
instability. Therefore, a logical approach would
be to treat genu valgum if a significant genu
valgum is present. If necessary, do an MPFLr in
a second procedure. However, our patient has a
very discreet valgus.
Could a Trochleoplasty Be Sufficient to Keep the
Patella Centered?
Trochlear dysplasia seems to be the most
important of all the main risk factors for the
development of chronic lateral patellar instability
[2–5]. Trochlear dysplasia is a recognized factor
that favors lateral patella instability. The trochlear dysplasia of this patient is very severe
(Fig. 5). In theory, we should act on the most
serious one when there are many predisposing
factors for instability. In this case, we should
possibly act only on trochlear dysplasia. In a
consensus statement from the AOSSM/PFF about
patellar instability, the Deepening trochleoplasty
is considered when several factors are present at
the same time. They are a J-sign, a boss or 5 mm
supratrochlear spur, and a convex proximal trochlea [6]. Our patient met all these requirements.
5
What to Do in Such a Situation?
My proposal was:
First Step—Arthroscopy to rule out other
pathological conditions, a chondral evaluation
(Fig. 6) and resection of the previous MPFLr.
Second Step—Correct patellofemoral maltracking (J-sign) by means of a Deepening trochleoplasty to keep the patella centered.
648
V. Sanchis-Alfonso
Fig. 3 Femoral tunnel very proximal and anterior. Severe trochlear dysplasia
Third Step—Stabilize—Balance. Revision
MPFLr using a medial quadriceps tendon
autograft.
6
What Has This Case Taught Us?
This Case Shows …
– Not all PFOA are associated with severe pain.
There is poor evidence that all cartilage
lesions are painful. The mere presence of a
cartilage lesion does not mean it is the source
of pain. In other words, structural damage of
the patellar articular cartilage does not always
result in AKP. In this case, the patellofemoral
imbalance (lateral patellar instability) was
responsible for the pain.
– In the PFJ, patellofemoral congruence and
smooth kinematics are much more important
than normal articular cartilage [7].
7
Conclusion
In the case presented here with trochleoplasty,
we have completely corrected the patellofemoral
maltracking. In addition, with the stabilization of
the patella, we have eliminated the AKP even
though we have not acted on the severe cartilage
injury. Now, at rest with the knee in extension,
she does not need to flex and rotate the limb for
the patella to line up with the trochlea (see
video).
Case # 6: Failed MPFL Reconstruction in a Patient with …
Fig. 4 Variation of the
valgus vector as a function of
the length of the femur and
tibia
Fig. 5 Severe trochlear
dysplasia
649
650
V. Sanchis-Alfonso
Fig. 6 Severe chondropathy
on the medial facet of the
patella
References
1. Wilson PL, Black SR, Ellis HB, et al. Distal femoral
valgus and recurrent traumatic patellar instability: is an
isolated varus producing distal femoral osteotomy a
treatment option? J Pediatr Orthop. 2018;38:e162-7.
2. Nelitz M, Theile M, Dornacher D, et al. Analysis of
failed surgery for patellar instability in children with
open growth plates. Knee Surg Sports Traumatol
Arthrosc. 2012;20:822–8.
3. Wagner D, Pfalzer F, Hingelbaum S, et al. The
influence of risk factors on clinical outcomes following anatomical medial patellofemoral ligament
(MPFL) reconstruction using the gracilis tendon. Knee
Surg Sports Traumatol Arthrosc. 2013;21(2):318–24.
4. Kita K, Tanaka Y, Toritsuka Y, et al. Factors affecting
the outcomes of double-bundle medial patellofemoral
ligament reconstruction for recurrent patellar dislocations evaluated by multivariate analysis. Am J Sports
Med. 2015;43(12):2988–96.
5. Dejour D, Byn P, Ntagiopoulos PG. The Lyon’s
sulcus-deepening trochleoplasty in previous unsuccessful patellofemoral surgery. Int Orthop. 2013;37
(3):433–9 [PMID: 23275080]. https://doi.org/10.1007/
s00264-012-1746-8.
6. Post WR, Fithian DC. Patellofemoral instability: a
consensus statement from the AOSSM/PFF patellofemoral instability workshop. Orthop J Sports Med.
2018;30;6(1):2325967117750352. https://doi.org/10.
1177/2325967117750352.eCollection, January 2018.
7. Blønd L, Donell S. Does the patellofemoral joint need
articular cartilage? Knee Surg Sports Traumatol
Arthrosc. 2015;23(12):3461–3.
Case # 7: Lateral Patellar Instability
in a Multi-operated Young Patient
with Severe Patellofemoral
Osteoarthritis and Severe Trochlear
Dysplasia
Vicente Sanchis-Alfonso
and Joan Carles Monllau
1
Clinical Case
This is the case of a 29-year-old female (178 cm in
height and 54 kg, BMI 17) who came to the office
due to severe long-lasting left lateral patellar
instability. She had had two left patellar dislocations and 4 recurrent right patellar dislocations.
She also suffered from anterior left knee pain, but
it was not her main complaint. She had been putting up with the pain but not with the instability.
She was a physiotherapist. She practised paddle,
swimming, Pilates and went to the gym despite her
instability. Using the terminology of the ACL
deficient knee, we would classify this patient as a
copper. On several occasions, surgery was performed on her left knee with less than satisfactory
results (medial retinacular plication—2001—,
Albee’s osteotomy + TT osteotomy (Emslie) +
open-wedge patellar osteotomy—2002—, medial
patellar tendon transfer—2006—). Physical
examination showed evident patellofemoral maltracking (positive J-sign). The patella dislocated
laterally with knee flexion.
X-rays showed no lower-limb malalignment
on the coronal plane but there was evidence of
tricompartmental knee osteoarthritis (Fig. 1). In
axial views, one can observe how the patella
dislocates with knee flexion (Fig. 2). You can
also note a half-moon patella. The CT image
reveals a patella magna and a severe trochlear
dysplasia (Fig. 3). No torsional abnormalities
were found in the lower extremities.
In short, the patient is looking for a solution to
her instability, which is what limited her in sports
activities. It would never have occurred to her to
go to the doctor because of knee pain as she was
able to live with it.
2
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
J. C. Monllau
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
What to Do in Such a Situation?
Obviously, the easiest thing to do is to indicate
total knee arthroplasty (TKA). However, there is
a question to be answered. Is this the best choice
for a young patient who is consulting mainly due
to instability but not severe pain? Another option
would be patellofemoral arthroplasty or a bipolar
patellofemoral fresh allograft, but they are not
options if tricompartmental knee osteoarthritis is
observed in the X-ray. Moreover, the pain the
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_48
651
652
V. Sanchis-Alfonso and J. C. Monllau
Fig. 1 Normal lower-limb
alignment can be seen on the
coronal plane, as well as the
tricompartmental knee
osteoarthritis
Fig. 2 Left patella dislocates with knee flexion. Severe
trochlear dysplasia can be observed in the left knee. Some
hardware from prior surgeries (namely, the lateral facet
elevating trochleoplasty as well as the anterior tibial
tuberosity transposition) (Reprinted with permission from
Am J Orthop. 2017; 46:139–145. ©2017, Frontline
Medical Communications Inc.)
patient has is bearable and the main indication
for arthroplasty or an osteochondral allograft
procedure is severe pain recalcitrant to
conservative treatment. Another option would be
to tell her to give up sport. That would be
inconceivable as the practice of sport is this
patient’s profession and passion. There is yet
another option even though it may seem rather
far-fetched. We can simply advise the patient to
stop living her life and wait until she is of an age
suitable for TKA.
Prior to moving forward with our treatment
plan, the objectives were thoroughly discussed
with the patient. Keep in mind that the patient
was quite familiar with the subject because she is
physiotherapist and is used to dealing with
patients who have undergone knee operations. It
should be remembered that the patient’s values
and preferences are one of the three legs of
Evidence Based Medicine. The first step in the
treatment plan was to correct the maltracking by
means of a sulcus deepening trochleoplasty and a
patellar osteotomy to obtain smooth PFJ kinematics. The second step called for stabilization of
the patella with an MPFL reconstruction. The
patient knew that the aim of preserving-joint
surgery is to delay arthroplasty for as long as
possible. Our treatment does not close the doors
to a possible future arthroplasty.
Case # 7: Lateral Patellar Instability in a Multi-operated Young …
653
Fig. 3 Preoperative CT imaging showing severe trochlear dysplasia and a concave patella magna
3
Our Surgical Treatment
The patient has both severe patellofemoral
osteoarthritis (PFOA) and trochlear dysplasia
(Fig. 4). Therefore, it is difficult to cause more
damage. In this case, maltracking can be reproduced passively. With knee flexion, we can
reduce the patella. This marks the difference
between true fixed lateral patellar instability in
flexion due to a retraction of the extensor
mechanism of the knee and patellofemoral maltracking due to severe trochlear dysplasia.
A Dejour’s sulcus deepening trochleoplasty,
associated with a closed-wedge patellar osteotomy, was indicated (Figs. 5 and 6). To that end,
A
a periosteal patella sleeve was elevated from the
midline, and a longitudinal dorsally closing
wedge osteotomy was performed down to the
subchondral bone using a small oscillating saw.
Care was taken not to disturb the remnant articular cartilage. The wedge was carefully closed
with a clamp and then the osteotomy was fixed
with two 3.5 mm cannulated screws entering
medially. After that, patellar tracking was reassessed. Then, a reconstruction of the MPFL using
a semitendinosus tendon autograft was performed. Due to the abnormally thin patella, the
reconstruction was performed using a method
that does not require anchoring bone tunnels at
this level (i.e. the medial quad tendon). In this
case, avoiding patellar bone tunnels was
B
Fig. 4 A Note the severe convex dysplastic trochlea. B The concave patella has lost all the cartilage (Reprinted with
permission from Am J Orthop. 2017; 46:139–145. ©2017, Frontline Medical Communications Inc.)
654
V. Sanchis-Alfonso and J. C. Monllau
A
B
Fig. 5 A burr, starting from the medial proximal part of
the joint, is used to remove the cancellous bone from the
under surface of the femoral trochlea. B Final result after
A
molding the flap to the underlying cancellous bone bed
and fixation with a resorbable anchor device and sutures
B
Fig. 6 A follow-up CT scan image after the combined sulcus deepening trochleoplasty and patellar osteotomy. A Note
the supratrochlear spur resection in the lateral view as well as B the new shape of the patella in the axial view
particularly safer since a patellar osteotomy was
also performed. For the graft femoral fixation, a
technique that uses the Adductor Magnus tendon
as a dynamic post was preferred.
4
Follow-Up
Six years have passed since the surgery and the
patient has fulfilled her goal of being able to
practice recreational sports. She is pain-free and
has no instability.
5
The Conventional Thinking Is …
Trochleoplasty is contraindicated in high-grade
trochlear dysplasia with instability associated
with PFOA [1].
Dejour and Le Coultre [2], considered the
patellar osteotomy an attractive surgical technique when associated with trochleoplasty in
cases with a flat patella, but did not recommend it
for several reasons. They determined that there is
a significant risk of non-union and necrosis and it
Case # 7: Lateral Patellar Instability in a Multi-operated Young …
is difficult to determine the amount of articulation
for each facet and exactly where the ridge is to be
placed.
6
Is There an Indication for Patella
Osteotomies?
The indication for patella osteotomy is exceptional. We should only perform it in cases of an
important patellofemoral mismatch after performing a trochleoplasty, as occurs in the clinical
case that we have presented. The goal is that the
congruence between the patella and the newly
formed sulcus angle is the best possible. The
final decision for patella osteotomy is taken
during surgery by means of direct observation of
the tracking of the PFJ after trochleoplasty.
The Patellar closing wedge osteotomy was
first reported by Griss [3]. Koch and colleagues
[4] presented 2 patients out of 85 trochleoplasties
performed. At 2 years follow-up, both patients
showed a stable patella with correct tracking.
Both patients considered their functional result
excellent. However, Badhe and Forster [5] presented 4 patients suffering from patellar instability due to an underlying trochlea dysplasia and
treated it with elevation of the lateral femoral
condyle according to Albee in combination with
a Dorsal closing wedge patellar osteotomy. The
result was fair. The patella was stable but patients
experienced residual patellofemoral pain in the
absence of necrosis or non-union. Elevation of
the lateral condyle as described by Albee provokes and increment in PFJ pressure. Dejour
does not recommend this technique.
7
What Has This Case Taught Us?
This Case Shows
– Not all PFOA are associated with severe pain.
– TT-TG distance cannot be calculated in all the
cases, especially in those in which there is a
severe trochlear dysplasia, as in this case.
655
– This case calls into question the necessity of
performing patellar osteotomies to fit the
patella into the new trochlea. The Closing
wedge patellar osteotomy can be helpful in
combination with trochleoplasty in patients
with patellofemoral instability due to trochlear
and patellar dysplasia.
– In the patellofemoral joint, patellofemoral congruence and smooth kinematics are much more
important than normal articular cartilage [6].
– Caution must be exercised when performing a
surgical indication in a patient with patellofemoral instability. This patient had been
operated on several times without any
improvement and the result was patellar
instability along with PFOA. The patient had
gone through several episodes of instability of
the contralateral knee, but it has not been
operated on and there is no osteoarthritis
(Fig. 2). This case should serve as a warning
of the damage that inappropriate surgery can
cause.
8
Conclusion
This is an example of the challenging PFJ
preservation surgery in a borderline case. This
case asks us to question whether articular cartilage is in fact essential in the PFJ. In other words,
does the PFJ truly need articular cartilage?
References
1. Vasta S, Castelhanito P, Dejour D. Trochleoplasty
techniques: deepening Lyon. In: Dejour D, et al.
editor. Patellofemoralpain, instability and arthritis.
Springer;2020.
2. Dejour D, Le Coultre B. Osteotomies in patellofemoral instabilities. Sports Med Arthrosc.
2007;15:39–46.
3. Griss P. Modification of sagittal osteotomy of the
patella as treatment of excentric chondromalacia or
retropatellar arthrosis. Preliminary communication.] (in
German). Z Orthop Ihre Grenzgeb. 1980;118: 822–4.
656
4. Koch PP, Fuchs B, Meyer DC, et al. Closing wedge
patellar osteotomy in combination with trochleoplasty.
Acta Orthop Belg. 2011;77(1):116–21.
5. Badhe NP, Forster W. Patellar osteotomy and Albee’s
procedure for dysplastic patellar instability. Eur J
Orthop Surg Traumatol. 2003;13:43–7.
V. Sanchis-Alfonso and J. C. Monllau
6. Blønd L, Donell S. Does the patellofemoral joint need
articular cartilage? Knee Surg Sports Traumatol
Arthrosc. 2015;23(12):3461–3.
Case # 8: Extensor Mechanism
Reconstruction After Resection
of a Soft Tissue Sarcoma
that Infiltrates the Patellar Tendon
Vicente Sanchis-Alfonso, Alejandro Roselló-Añón,
Eloisa Villaverde-Doménech, Onofre Sanmartin,
and Juan Pablo Aracil-Kessler
1
Clinical Case
A 65-year-old woman with a painless subcutaneous mass in the anterior aspect of the knee was
referred to our hospital for a second opinion. The
lesion had recurred twice. The pathological diagnosis was glomangiosarcoma. It is a rare malignant tumor with a tendency to local invasion and
recurrence after excision. The tumoral extension
evaluation revealed no other lesions. Physical
examination showed a transverse excision scar of
10 cm along with a palpable mass adhered to the
skin. Magnetic resonance imaging (MRI) showed
a mass adjacent to the patellar tendon with both
cutaneous and patellar tendon infiltration (Fig. 1).
2
What to Do in Such a Situation?
Obviously, limb-sparing surgery is indicated.
There are 3 steps in this type of surgery.
V. Sanchis-Alfonso (&) A. Roselló-Añón
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
E. Villaverde-Doménech J. P. Aracil-Kessler
Plastic and Reconstructive Surgery Department,
Hospital Provincial de Castellón, Castellón, Spain
O. Sanmartin
IVO’s Dermatology Department, Instituto
Valenciano de Oncología (IVO), Valencia, Spain
2.1 First Step—Tumor Resection
(Fig. 2)
The tumor was removed with wide surgical
margins. A wide resection of the tissues surrounding the tumor including the skin, patellar
tendon (resected transversely from the inferior
pole of the patella), Hoffa fat pad and pes
anserinus was performed. Biopsy detected negative margins. The definitive diagnosis was a
subcutaneous GLI1-amplified neoplasm.
2.2 Second Step—Reconstruction
of the Extensor Mechanism
(Fig. 3)
Extensor mechanism disruption is a devastating
lesion. Several techniques for reconstruction
have been published. However, few techniques
adequately restore the function of the extensor
mechanism. In many surgical techniques, appears
a persistent extension lag. Furthermore, there is a
deficit in flexion in many cases. In our patient, a
reconstruction using an allograft (tibial bone—
patellar tendon—patella—quadriceps tendon)
was performed in accordance with the technique
described by Fiquet and colleagues in 2019 [1].
The postoperative care and rehabilitation
protocols proposed by Burnett and colleagues [2]
after massive extensor mechanism allograft
reconstruction were followed. The knee is not
flexed intraoperatively to evaluate flexion after
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_49
657
658
Fig. 1 Preoperative MRI
Fig. 2 Tumor resection
V. Sanchis-Alfonso et al.
Case # 8: Extensor Mechanism Reconstruction After Resection …
Fig. 3 Reconstruction of the extensor mechanism (Drawing by Noelia Bonet-Miralles)
659
660
V. Sanchis-Alfonso et al.
Fig. 4 Skin coverage
the reconstruction. A knee orthosis in full
extension was put in place for 8 weeks, and then
rehabilitation began. We did not allow any flexion during that period.
2.3 Third Step—Skin Coverage
(Fig. 4)
Adequate soft tissue coverage is necessary for a
successful extensor mechanism allograft reconstruction. Although most wounds around
the knee can be managed by medial gastrocnemius muscle flap, we opted for a free flap in this
case.
A perforator anterolateral thigh (ALT) free
flap from the contralateral thigh was chosen [3].
We prefer the free graft for various reasons. One
of them is that the skin defect that we must close
is very large because we must resect 2 cm at least
of skin per side. We must also consider that the
female gastrocnemius is shorter and more
atrophic than that of the male. Therefore, it may
not be sufficient to close the skin defect in our
case. Another advantage is that a free flap heals
sooner. That being the case, radiotherapy could
be done in the third or fourth week after surgery
if it were necessary. Furthermore, the free flap is
less aggressive than the gastrocnemius flap and,
there is a minimal donor site morbidity.
The main difficulty with this case was performing the anastomosis with total knee extension as the knee is not flexed intraoperatively
after the extensor mechanism reconstruction
according to the surgical protocol published by
Burnett and colleagues [2]. For this reason, we
performed the arterial anastomosis end-to-end to
the posterior tibial artery (instead of end-to-side).
3
Outcome—The Key
for a Successful Reconstruction
of the Extensor Mechanism
of the Knee
At the 6-month follow-up, she had functionally
adequate knee flexion (Figs. 5 and 6). More
importantly, she can raise her leg without an
extension lag.
Burnett and colleagues evaluated two techniques of reconstruction of the extensor mechanism
of the knee using an extensor mechanism allograft
[4]. They described Group I with the allograft
minimally tensioned and Group II with the allograft
Case # 8: Extensor Mechanism Reconstruction After Resection …
661
Fig. 5 Clinical aspect at the
6-month follow-up
Fig. 6 X-rays at the 6-month
follow-up
tightly tensioned in full extension. They demonstrated that the results of surgery depend on the
initial tensioning of the allograft. The loosely tensioned allograft results in a persistent extension lag
and clinical failure. Allografts that are tightly
tensioned in full extension can restore active knee
extension and result in clinical success. They concluded that an extensor mechanism allograft
transplantation will be successful only if the graft is
initially tensioned tightly in full extension.
662
References
1. Fiquet C, White N, Gaillard R, et al. Combined patellar
tendon lengthening and partial extensor mechanism
allograft reconstruction for the treatment of patella
infera: a case report. Knee. 2019;26(2):515–20.
2. Burnett RS, Berger RA, Della Valle CJ, et al. Extensor
mechanism allograft reconstruction after total knee
arthroplasty. J Bone Joint Surg Am. 2005;87(Suppl
1):175–94.
V. Sanchis-Alfonso et al.
3. Philandrianos C, Mattei JC, Rochwerger A, et al. Free
antero-lateral thigh flap for total knee prosthesis
coverage after infection complicating malignant
tumour resection. Orthop Traumatol Surg Res.
2018;104(5):713–7.
4. Burnett SJ, Berger RA, Paprosky WG, et al. Extensor
mechanism allograft reconstruction after total knee
arthroplasty. A comparison of two techniques. J Bone
Joint Surg Am. 2004;86(12):2694–9.
Case # 9: Severe Patellofemoral
Chondropathy in an Active
47-Year-Old Patient
Erik Montesinos-Berry
1
Clinical Case
A 47-year-old male came to our institution
complaining mainly of disabling left anterior
knee pain. He works as a police officer, now
doing mostly desk work because of his disability,
he also walks with a cane because of it. The pain
was located on the anterolateral aspect of the
knee. The inferior pole of the patella was not
painful upon examination. The pain was recalcitrant to an appropriate conservative treatment
for more than two years. The patient was hesitant
to undergo a surgical procedure on his knee
because he was not completely satisfied with the
results of a tibial tubercle medialization osteotomy performed on his right knee in 2011.
The imaging study showed no malalignment
in the coronal plane or any torsional abnormalities. The CT-scan showed a TT-TG distance of
21 mm. MRI exam showed a stage IV lateral
facet chondropathy.
2
What to Do in Such a Situation?
When we need to unload lateral and/or distal
painful chondral lesions, even in advanced isolated patellar lateral facet arthrosis, in cases with
a lateral patellar subluxation and a TT-TG distance of more than 20 mm, a Fulkerson’s
osteotomy might be a good solution (Fig. 1).
Obviously, proximal and medial healthy cartilage
onto which to transfer load is mandatory. Diffuse, proximal or medial patellar lesions or central trochlear lesion are contraindications for
Fulkerson’s osteotomy.
In our case, during the arthroscopic examination, a severe lateral facet chondropathy and a
mild medial facet chondropathy was confirmed
(Fig. 2). Therefore, a tibial tubercle anteromedialization osteotomy (Fulkerson’s osteotomy) was
performed.
3
Outcome
The patient is now pain-free, his left knee no
longer hurts. In fact, he is happier with the result
of his left knee than with his right knee, and now
he wants the same type of surgery that was performed on the left knee to be performed on the
right one.
E. Montesinos-Berry (&)
ArthroCentre—Agoriaz, Riaz & Clinique CIC
Riviera, Montreux, Switzerland
e-mail: erik.montesinos@gmail.com
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_50
663
664
E. Montesinos-Berry
Fig. 1 Left knee postoperative radiographs and CT scan. The inferior pole of the patella was not painful
Fig. 2 During arthroscopic examination. Severe chondropathy of the lateral facet, and mild chondropathy of the medial
facet
4
What Has This Case Taught Us?
This Case Shows …
The clinical examination is still our most
important tool to identify the origin of pain. Most
surgeons would have considered a resection of
the inferior pole of the patella just by looking at
the X-rays, when in fact the inferior pole was not
painful. The pain was located on the lateral
aspect of the knee.
This case really emphasizes the importance of
unloading. The biomechanical effect we get from
a medialization is not same one we get from a
anteromedialization. The pressure reduction in
the lateral facet is greater with an anteriomedialization [1]. Our patient would agree with this
since his subjective feeling is of a great
improvement with an anteromedialization in the
left knee, and only a mild improvement with a
medialization in the right knee, to the point of
wanting to undergo surgery again on his right
knee to have the same procedure as on his left
knee.
Kuroda and colleagues [2] have shown that
tibial tubercle medialization significantly increases both the patellofemoral contact pressure and
the contact pressure in the medial tibiofemoral
Case # 9: Severe Patellofemoral Chondropathy in an Active …
Fig. 3 Radiographs of the right knee operated in 2011.
Medialization of the tibial tuberosity. Degenerative
changes in the medial compartment can be observed
compartment. Therefore, over-medialization of
the tibial tuberosity should be avoided in the
varus knee, the knee after medial meniscectomy,
and the knee with preexisting degenerative
arthritis of the medial compartment. Interestingly, degenerative changes in the medial compartment on the right knee have been observed in
our patient (Fig. 3).
5
The Key for a Successful
Fulkerson’s Osteotomy
Fulkerson’s osteotomy is indicated when we
need to realign the patella, that is when we need
to restore central tracking. Therefore, the presence of a lateral patellar subluxation and a TTTG distance of more than 20 mm, is mandatory.
The results of Fulkerson’s osteotomy depend
on the location of the chondral lesion. The
location of the chondral lesion is essential to
665
indicate an anteromedialization osteotomy of the
tibial tubercle (Fulkerson’s osteotomy). Pidoriano and colleagues [3] reported a higher number
of successful results when the lesion was only on
the lateral aspect of the patella. An MRI mapping
of the chondral lesion of the patella and/or an
arthroscopic examination of the cartilage of the
patella, confirming the lateral facet damage, and
the medial facet preserved cartilage, are mandatory before performing this type of osteotomy. In
the paper published by Pidoriano and colleagues
ten patients with type I (distal) patellar lesions
and thirteen with type II (lateral facet) patellar
lesions showed 87% good to excellent subjective
results [3]. Every single one of these patients
indicated he/she would undergo this procedure
again. Nine patients with type III (medial facet)
lesions showed 55% good to excellent results [3].
Five patients with type IV (proximal or diffuse)
lesions barely showed 20% good to excellent
results [3]. In short, patients with type I or II
lesions were considerably more inclined to show
good or excellent results compared to those with
type III or IV lesions. They observed that central
trochlear lesions were involved in medial patellar
lesions and that the results were poor for all the
patients with central trochlear lesions [3]. No
significant correlation was detected between the
Outerbridge grading of the patellar lesion and the
overall results [3].
We must avoid an over-medialization. Our
goal is a TT-TG distance of 10–15 mm. In our
patient the postoperative TT-TG distance was
14 mm.
6
Conclusions
– In patients with a lateral facet chondropathy,
and a TT-TG distance over 20 mm a Fulkerson’s osteotomy can be considered as long as
the medial facet cartilage is in good condition.
An arthroscopic examination will allow us to
determine this.
666
– Even in cases of severe chondropathy
including bone on bone, a Fulkerson’s
osteotomy could be better than patellofemoral
arthroplasty.
– In this case, since both knees have been
operated on, with different techniques, the
feedback we get from the patient is very
valuable. The patient had been reluctant to
have surgery on the left knee for over two
years, but now he did not hesitate and had the
operation on his right knee within the year.
E. Montesinos-Berry
References
1. Elias J, Jones KC, Copa AJ, et al. Computational
simulation of medial versus anteromedial tibial
tuberosity transfer for patellar instability. J Orthop
Res. 2018;36(12):3231–8.
2. Kuroda R, Kambic H, Valdevit A, et al. Articular
cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med. 2001;29
(4):403–9.
3. Pidoriano AJ, Weinstein RN, Buuck DA, et al.
Correlation of patellar articular lesions with results
from anteromedial tibial tubercle transfer. Am J Sports
Med. 1997;25(4):533–7.
Case # 10: Dislocated Patella After
Revision Total Knee Arthroplasty.
Case # 11: Patella Baja and Valgus
Limb 56 Years After Tibial Tubercle
Transfer
Robert A. Teitge
1
Clinical Case
76 year-old-male presented on referral from
treating orthopaedic surgeon 30/09/2008.
Chief complaint: recurrent dislocation
of patella post-revision of tibial component right total knee.
TKA right knee in 1992 no complaints until 2007
when the knee felt unstable. Progressive laxity of
the right knee with increased valgus. Laxity and
valgus felt to be due to lateral polyethylene insert
wear. Replacement of Poly insert with 25 mm
spacer reduced valgus and provided stability
under anesthesia. At 3-month post-op the knee
gave way while going up stairs followed by
recurrent dislocation in which the knee suddenly
gives way with no power. The knee is weak on
stairs. The kneecap “pops out of place” without
warning frequently and he has fallen a number of
times. He underwent arthroscopy with lateral
retinacular release with no change. Patient is
unable to walk on uneven ground like the beach
or climb stairs or ride a bicycle.
Examination: 180.3 cm, 109 kg. Alignment
clearly valgus compared with minimal valgus on
the left. Feet, heels and patella straight. Going on
toes and heels normal but cannot do minimal
squat as the patella dislocates. Motion 0–130°.
Straight leg raising to 90°. A small effusion is
present with no heat, swelling, bursitis or synovitis. No crepitation with extension from 40°
but the patella dislocates when flexion is more
than 40°. There is clinically increased mobility of
the patella in both the medial and lateral direction
with no apprehension or discomfort. Manual
pressure on the lateral side of the patella cannot
prevent dislocation with knee flexion. Q angle is
15°. There is visible and palpable atrophy in the
right quadriceps compared with the left. Thigh
circumference is 49.5 cm on the right and 53.3
on the left. Varus-Valgus stress and Anterior–
Posterior drawer test appear normal bilateral.
There is no pain at any location with palpation.
The Ober test is 0 but with 40° of knee flexion
the patella dislocates. In the prone position hip
Internal/External rotation is 30°/45° on the right
and 45°/15° on the left.
Radiological evaluation: Radiographs reveal
what appears as well fixed femoral, tibial and
patellar components (Fig. 1). The whole limb
standing film reveals a valgus limb alignment of
15° (Fig. 2). There is a valgus of the tibia. The
femoral component is in 9° of valgus compared
with normal alignment, The tibial component is
R. A. Teitge (&)
Wayne State University, Detroit, MI, USA
e-mail: rteitge@med.wayne.edu
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_51
667
668
Fig. 1 Well-fixed femoral,
tibial and patellar components
Fig. 2 Valgus limb
alignment of 15°. The angle
of medial femur joint line to
mechanical axis is 93°. The
angle of medial tibial joint
line to mechanical axis is 87°
R. A. Teitge
Case # 10: Dislocated Patella After Revision Total …
in 6° of valgus compared with normal. The
mechanical axis was tilted medially a normal 3°.
First question: Is there an alignment
deformity?
Answer: Yes. Knee valgus
Second question: How much?
Answer: 15° Valgus deformity
Third question: Where is the
deformity?
Answer: 15° valgus deformity could be
at 3 sites: femur, joint and tibia. In this case:
femur = 9° (102−93 = 9); joint = 0°; and
tibia 6° (93−87 = 6). The mechanical axis is
inclined 3°. The joint line is horizontal.
2
What to Do in Such a Situation?
Options
(1) Revision of femoral and tibial components
will require resection of more femur and
669
tibia or require addition of femoral and tibial
component augments.
(2) Medial
patellofemoral
ligament
reconstruction.
(3) Coronal plane osteotomy will require 15°
correction.
Decision Making (see Figs. 3 and 4).
(1) Revision of well-fixed components will
likely result in greater bone loss and still
present the challenge of making perfect
femoral and tibial cuts. The possibility of
creating varus-valgus instability will
increase.
(2) MPFLR is not guaranteed to prevent further
dislocation in the presence of genu valgum.
(3) Osteotomy of just the femur or tibia will
create an undesirable joint line obliquity.
(4) Osteotomy of the femur and tibia will
maintain a horizontal joint line.
(5) Closing wedge osteotomy of femur and tibia
should not create varus-valgus instability.
Fig. 3 Clinical pictures after double level osteotomy. Valgus correction
670
R. A. Teitge
Fig. 4 Radiological
evaluation after double level
osteotomy
(6) Closing wedge osteotomy of femur and tibia
with compression should yield rapid bone
healing.
(7) MPFLR was probably unnecessary as the
observed patellar tracking after osteotomy
remained midline with no tendency to dislocate, but it was added rather as an “insurance” policy.
3
Outcome
Patient was progressed to full weight bearing at
4 weeks. At 1 year follow-up he was comfortable walking on a beach, riding a bicycle and
walking up 4 flights of stairs. He had no sense of
instability, insecurity or weakness of the patella
and knee. He was delighted with the outcome.
4
What Has This Case Taught Us?
This Case Shows …
Limb Alignment is Very Important in the Resolution of Patellofemoral Disorders.
The case presented below further
emphasizes the great importance of limb
alignment in the resolution of patellofemoral pain.
68-year-old female. Right Incapacitating knee
pain. She has been in a wheelchair for the past
2 years. History: TTO at age 12; fractured distal
tibia at age 40 (Fig. 5).
Case # 10: Dislocated Patella After Revision Total …
Fig. 5 Patella infera, valgus limb alignment, lateral
compartment osteoarthritis. The knee points forward, with
the foot pointing outward indicates an external tibial
671
rotational deformity, there is evidence of prior tibial
tubercle osteotomy and tibial diaphyseal fracture
5
Diagnoses
Right tibial mal-union
" Femoral
anteversion
" External tibial
torsion
Recurrent dislocation
Patella Baja
Tibia valgus growth
Tibia valgus
congenital
Lateral compartment
OA
Valgus joint
convergence
Fig. 6 The post-operative radiographs after tibial varus
internal rotation osteotomy + proximal transfer of the
tibial tuberosity show a neutral mechanical axis, the knee
joint and ankle joint appear to be normally aligned in
rotation. The patellofemoral joint is congruent
Right (37°) and Left
(39°)
Right (54°) and Left
(36°)
Left patella
Right
Right
Left
Right
Right
672
6
R. A. Teitge
Options
• Total Knee?
• Tibial Osteotomy?
– Rotation
– Varus
Proximal
Mid
Distal
• Femoral Osteotomy?
• Lengthen patellar tendon?
7
Surgery
The arthroplasty surgeon did not want to do TKA
unless the patella baja was corrected and the
quadriceps was functionally normally. I thought
it was foolish to consider a proximal tuberosity
transfer and leave the tibia with the valgus and
external rotation deformity. I elected pre-op to
accept the joint line obliquity post-op rather than
add femoral osteotomy.
Tibia: Varus + Rotation at Diaphysis + Tibial
Tuberosity Osteotomy Moved Proximal (Fig. 6).
8
Outcome
2 years. postop. She is walking. “I don’t need a
total knee, right is better than left with recurrent
patellar dislocation”.
New Frontiers in Anterior Knee Pain,
Patellar Instability and Patellofemoral
Osteoarthritis Evaluation
and Treatment
Kinetic and Kinematic Analysis
in Evaluating Anterior Knee Pain
Patients
Vicente Sanchis-Alfonso
and Jose María Baydal-Bertomeu
1
The Need for an Objective
Measurement of Outcomes
Given that clinical practice modification is based
on outcome studies, the ability to evaluate and
quantify the effects of treatment in anterior knee
pain (AKP) patients is vital. Due to the limitations of the current methods like the Visual
Analog Scale (VAS) and functional scores such
as the Kujala score and IKDC, new technologies
are needed to measure the benefits of AKP
treatment and to compare different methods of
treatment. The final objective should be measurement during dynamic activities that cause or
aggravate the symptoms. This objective might be
achievable by means of kinetic and kinematic
analysis given that both are useful in the objective measurement of lower limb function.
The application of kinetic and kinematic
analysis in the objective assessment of AKP
patients is discussed in this chapter. Moreover,
kinetic and kinematic analyses can also be useful
to help us to understand the knee osteoarthritis
mechanisms in this population group.
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
2
What Provoking Activity is
the Best to Evaluate AKP? The
Rationale
Stair climbing is a demanding locomotor task
that is frequently performed during daily activities. From a functional point of view, it is wellknown that going up and down stairs requires
high levels of quadriceps activity and is one of
the most painful and challenging activities of
daily living for subjects with AKP. Moreover,
going downstairs is more challenging than going
up stairs due to the level of eccentric control
required during step descent. In fact, Costigan
and colleagues [1] have reported that during stair
descent there is an increment in the patellofemoral joint reaction force (PFJRF), being eight
times greater compared to level walking. Therefore, stair descent is demanding enough from a
biomechanical standpoint to not only aggravate
pain in those patients with AKP, but also to
trigger the use of defense strategies. Therefore,
we propose the stair descent test to evaluate and
to quantify the effects of both surgical and nonsurgical treatment in AKP patients.
Another interesting aspect that will be analyzed in this chapter are the compensating
strategies to reduce load and the resulting pain
that, in theory, an AKP patient may develop
during the stair descent test. Those strategies that
J. M. Baydal-Bertomeu
Instituto de Biomecánica de Valencia (IBV),
Valencia, Spain
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_52
675
676
V. Sanchis-Alfonso and J. M. Baydal-Bertomeu
may seem good at reducing pain might have an
adverse mid-term and long-term effect on the
knee joint (knee osteoarthritis).
3
Kinetic and Kinematic Analysis
in Evaluating AKP
To evaluate the way the stair descent is performed we use kinematic information, registered
through photogrammetric instruments and kinetic
information, picked up on dynamometric platforms. Both systems are combined to determine
the most relevant variables that characterize
going down stairs.
3.1 Instruments—Motion Analysis
System—Dynamometric
Platforms
A four-camera computer-aided video motion
analysis system1 and two independent dynamometric platforms that register the force exerted by
the foot on the floor in the three directions of
space are used for this test. Dynamometric platforms are placed as indicated in Fig. 1. To carry
out the test, a portable two-step wooden staircase, and passive markers2 are needed. Three
boxes with the following dimensions are used:
20 cm high step riser and 40 cm footprint,
forming a two-step staircase (Fig. 1). The box
that serves as the first step was built to adapt
perfectly to the dynamometric platform to avoid
vibrations when stepping on it. Sixteen reflecting
markers are used, eight for each leg. They
determine the spatial position of the segments of
the lower limb. The markers are placed tracing
two triangles in each segment (leg and thigh),
with the apex in opposing directions in each of
the segments (Fig. 2). All the markers are placed
on the lateral aspect of the leg to allow for a
1
Motion analysis. Interpretation of computerized data that
documents an individual’s lower and upper extremities,
pelvis, trunk, and head motion during ambulation.
2
Passive markers. Joint and segment markers used during
motion analysis that reflect visible or infrared light in
contrast with active markers that emit a signal.
correct visualization by the cameras. Two of the
markers are placed on the lateral condyle and on
the lateral malleolus respectively to determine
the position of the knee and ankle joints.
3.2 Laboratory Protocol
To do the test, the subject starts in a standing
position with both arms crossed over the chest for
the first step. The test involves descending the
two steps of the staircase. First, the subject puts
one foot on the first step, which has one of the
platforms underneath it. Then, the other foot is
placed on the floor where the other platform is.
The test is repeated four times (two with each leg)
for this analysis. Participants are given a visual
demonstration of the task prior to testing. Following a verbal cue, the participants perform the
task (Fig. 3). To ensure that the task is always
performed in the same fashion, we always position some examiners beside the subject to instruct
him/her on how to perform the task correctly and
to make sure he/she follows the instructions while
carrying out the task. We also have a video
camera recording our patients to confirm that it is
performed correctly. To avoid the possible effects
of footwear on gait when descending stairs, all
subjects undergo data collection in their barefeet.
Apart from standardized stair descent, the patient
performs a free one, meaning going down the
stairs the way he/she feels more comfortable.
3.3 Kinematic and Kinetic Variables
The video-photogrammetric system provides the
coordinates of the markers. From this raw data,
the finite displacements from the body-reference
position were computed using an in-house
developed software based on the algorithms
described by Woltring [2]. This software provides angular displacements expressed as the
attitude vector. The projection of the attitude
vector on the medio-lateral and antero-posterior
axis provides an estimation of the flexionextension and abduction-adduction angle based
on the procedure described by Page and
Kinetic and Kinematic Analysis in Evaluating Anterior Knee …
677
Fig. 1 How the step is
adapted to the platform: step
disposition
Fig. 2 Marker disposition.
A With calibration markers.
B, C Without calibration
markers
A
colleagues [3]. Using the spatial position and the
forces registered with the dynamometric platform, the knee joint moments were calculated.
We have used a smoothing technique based on a
local polynomial-fitting. The width of the window was optimized in each measurement for the
minimum self–correlation of the residuals [3].
The variables specific to the test are (Table 1):
(1) knee flexion angle—measured in degrees;
B
C
(2) stance phase duration—time during which the
subject is in contact with the first step and is
measured in seconds; (3) normalized3 heel contact force—ground reaction force (GRF) that
appears on the platform when the heel strikes on
3
The forces are measured in N and they have been
normalized for subject weight; therefore, it is a dimensionless magnitude.
678
V. Sanchis-Alfonso and J. M. Baydal-Bertomeu
Fig. 3 Photographic sequence of the stair descent test
Table 1 Variables specific
to the test in a control
group
Control group
Knee flexion angle
Average
SD
Max
Min
99.12
7.54
63.45
121.23
Stance phase duration
0.88
0.12
0.62
1.24
Heel contact GRF
1.45
0.15
1.16
1.76
Oscillation GRF
0.75
0.07
0.54
0.94
Toe-off GRF
0.95
0.08
0.75
1.14
Heel contact A/A moment
0.20
0.05
0.12
0.33
Toe-off A/A moment
0.16
0.04
0.08
0.26
−0.13
0.07
−0.54
−0.02
0.29
0.05
0.18
0.42
Heel contact F/E moment
Toe-off F/E moment
the first step; (4) normalized oscillation force—
GRF that appears on the platform when the
contralateral leg is oscillating; (5) normalized
toe-off peak force—GRF that appears on the
platform when the foot steps off of it; (6) heel
contact abduction-adduction moment4—maximum torque on the coronal plane5 that is produced during the foot-strike phase on the
platform; (7) toe-off abduction-adduction
moment—maximum torque on the coronal
plane that is produced during the foot take-off
phase on the platform; (8) heel contact flexion-
extension moment—maximum torque on the
sagittal plane6 that is produced during the foot
heel-strike phase on the platform; and (9) toe-off
flexion-extension moment—maximum torque on
the sagittal plane that is produced during the foot
take-off phase on the platform.
Kinetic and kinematic variables are expressed
on a curve. In each graphic, a band of normality
(color, light blue), the control group’s mean
value (a dotted line) and the mean value of our
patients (a black line) are presented (Figs. 4, 5, 6,
7, 8, 9, 10 and 11).
4
The moment is measured in Nm, it has been normalized
for subject weight and knee height; therefore, it is a
dimensionless value.
5
Coronal plane. The plane that divides the body or body
segment into anterior and posterior parts.
6
Sagittal plane. The plane that divides the body or body
segment into the right and left parts.
Kinetic and Kinematic Analysis in Evaluating Anterior Knee …
4
Clinical Relevance: Understand
the Knee Osteoarthritis
Mechanisms in the AKP Patient
It is well known that the moments that act upon a
joint must be balanced by an equal and opposite
muscle force to maintain joint equilibrium. In the
healthy subject, the knee joint starts from a relatively stable extended position and flexes
towards an increasingly unstable position while
going downstairs. The increased joint flexion
causes a progressive increment in the external
flexion moment7, which is matched by progressively increasing eccentric quadriceps contraction to prevent collapse. In doing so, the internal
(muscle) extensor moment8 increases during stair
descent as knee flexion occurs. As the PFJRF is
dependent on the magnitude of the quadriceps
force and knee flexion angle [4], the compressive
force acting between the patella and femoral
trochlea during stair descent would be expected
to be significant. It would also increase the
patellofemoral joint (PFJ) stress (force per unit
contact area), which is a factor responsible for
the PFJ cartilage degeneration. Although articular cartilage is aneural, it has been proposed that
articular cartilage degeneration renders the subchondral bone susceptible to pressure variations
that would normally be absorbed by healthy
cartilage.
Although the knee abduction-adduction
moment (valgus-varus moment) is not on the
primary plane of motion (the primary plane is the
sagittal plane), its magnitude should not be
ignored when trying to understand the stability
and function of the knee during stair climbing
and the future life of the knee. Kowalk and colleagues [5] have demonstrated that coronal plane
moment patterns are exclusively abductor
throughout stance. When an external knee valgus
moment occurs, an internal (muscle) joint
moment will be generated by the medial muscles
7
External moment. The load applied to the human body
due to ground reaction forces, gravity and external forces.
8
Internal joint moment. The net result of all the internal
forces acting about the joint which include moments due
to the muscles, ligaments, joint friction and structural
constraints.
679
(pes anserinus) to balance the joint. An abduction
moment will induce a valgus rotation of the tibia.
This rotation is limited by two forces, the MCL
force, a proximally oriented force at the medial
aspect of the knee joint, and a joint contact force
acting distally on the lateral tibial plateau [6].
In the young patient with AKP, we and other
authors [7, 8] have observed a significant
reduction in the knee extensor moment while
going downstairs when compared to healthy
control group subjects (Fig. 4), which is generally reversed after pain relief with physiotherapy
treatment. However, in some cases, Grenholm
and colleagues [9] have demonstrated that these
compensatory strategies may remain even after
the pain has disappeared. This finding goes
against the use of this test as a patient evolution
control system. The reduction of the knee
extensor moment, which is suggestive of a
quadriceps avoidance gait pattern [10], could be
a primary compensatory strategy used by patients
with AKP to reduce the muscle forces acting
across the PFJ. Doing so, pain aggravation during walking downstairs is minimized. The
reduction of the knee extensor moment with the
subsequent smaller quadriceps contraction, will
cause a decrease in the PFJR force and a decrease
in PFJ loading while going downstairs. In this
sense, Brechter and Powers [7] have demonstrated that subjects with AKP did not show
increased PFJ stress during stair descent in
comparison to a pain-free control group. We
have found that when a patient goes down the
stairs using his/her strategy for maximum comfort, the extensor moment is lower than when the
stair descent is performed following the standard
protocol. This confirms the fact that we have
discovered a defense strategy (Fig. 5).
One factor that may contribute to the knee
extensor moment reduction is the decrease of
knee flexion angle during the stance phase9 of
stair ambulation when compared to control
healthy subjects (Fig. 6). It is a strategy to reduce
the extensor moment and therefore pain during
stair descent. With less knee flexion, the lever
9
Stance phase. Period of time when the foot is in contact
with the first step.
680
V. Sanchis-Alfonso and J. M. Baydal-Bertomeu
Fig. 4 Knee extension
moment
arm of the ground reaction force is shortened.
Consequently, the knee extensor moment is
reduced, with equilibrium being achieved by
fewer quadriceps contractions. Although we have
observed a decrease of the flexion angle in most
of our cases, it has not been a uniform finding. In
this sense, there are authors who have found a
decrease in the flexion angle during stair descent
[11, 12], while others have found no significant
differences in the flexion angle during stair descent [7–9, 13, 14] in AKP patients. The decrease
of the knee flexion angle during stair descent is
therefore not a constant adaptive strategy or
defense mechanism. It could be possible that the
lack of a decrease of the flexion angle during
stair descent is because this activity may not
cause enough pain in some people to cause them
to use compensatory strategies like knee flexion
reduction. Another possible reason for this lack
of knee flexion reduction with stair descent could
be the activation instant of the VMO when
compared to the VL. Crossley and colleagues
[11] have demonstrated that those subjects with a
higher deficit in the activation moment of the
VMO when compared to that of the VL show a
higher reduction in knee flexion during stair
descent. This is because these patients show an
increment in PFJ stress due to the altered patellar
tracking. Finally, another fact to justify not
finding a decrease of the flexion angle might be
how long the pain has been felt. It makes sense to
think that some time is required for the patient to
develop adaptive measures like flexion reduction.
Other strategies besides a decrease in knee
flexion to reduce the extensor moment would be
the decrease in the vertical ground reaction force
in comparison to the healthy limb (Fig. 7). This
may reflect an apprehension to load the knee
joint at the beginning of the stance phase.
According to Salsich and colleagues [8], other
strategies employed to reduce the knee extension
moment could be the decrease in the stance time
duration and the pace. This way, the decrease in
the vertical ground reaction force or the speed at
which he/she performs the stair descent might
contribute to the decrease in the PFJRF. Therefore, the patient may not need to reduce knee
flexion during stair descent.
According to Hinman and colleagues [15],
quadriceps dysfunction may be important in the
development and progression of structural changes
in osteoarthritis. Quadriceps dysfunction may
compromise the protective mechanisms of the
knee. The decrease in the extensor moment, which
Kinetic and Kinematic Analysis in Evaluating Anterior Knee …
Fig. 5 Knee extension
moment. A Standard stair
descending test. B Stair
descending test following the
comfort strategy
681
A
B
is a strategy to reduce pain, can have destructive
long-term effects on the knee joint. In this sense, the
decrease in active shock absorption10 during
weight-bearing from the eccentric quadriceps
muscle contraction [4, 11, 13] means greater shock
absorption through the bone and cartilage that
could explain tibiofemoral pain. It might also be a
predisposing factor to tibiofemoral osteoarthritis of
10
Shock absorption. The progressive damping of an
applied force. Damping is a complex, generally nonlinear,
phenomenon that exists whenever energy is dissipated.
the knee. There is growing evidence that subchondral bone and its turnover may play a causal
role in the pathogenesis of osteoarthritis as well as
its related symptoms, especially in the knee. This
data supports the findings by Naslund and colleagues [16] using bone scintigrams in patients
suffering from AKP. They found that tracer accumulation occurred as often in the proximal tibia as
in the patella.
We have been able to demonstrate a decrease
in the knee abduction (valgus) moment while
682
Fig. 6 Knee flexion during
stair descending test (A).
B Stair descending with a
severe knee extension pattern
V. Sanchis-Alfonso and J. M. Baydal-Bertomeu
A
B
walking downstairs in almost all cases in AKP
patients when it is compared to a healthy painfree knee (Fig. 8). The decreased abduction
moments around the knee seen on the coronal
plane may help to reduce joint loading, which
may be a mechanism that prevents degeneration.
We have found that when the patient goes
downstairs with his best comfort strategy, the
abduction moment is lower than when it is done
following a standard protocol. This is confirmation that the decrease in the abductor moment is a
defense strategy. The increment in the knee
abduction moment would cause a lateral tibiofemoral overload. In this way, Elahi and colleagues [17] correlate PFOA with increased
valgus knee alignment.
Kinetic and Kinematic Analysis in Evaluating Anterior Knee …
Fig. 7 Vertical ground reaction force during stair descending test
Fig. 8 Knee abduction
moment during stair
descending test
683
684
5
V. Sanchis-Alfonso and J. M. Baydal-Bertomeu
Case Studies: A “Snapshot”
Case #1. Disabling AKP in a Multi-operated
Young Patient With a Chronic Patellar Tendon Rupture and Loosening of the Femoral
Component of the Patellofemoral Prosthesis
Here, we cite a 29-year-old woman whose left
knee was operated on 7 times beginning at the
age of 20 (arthroscopic shaving, patella osteotomy, tibial tubercle anteromedialization with
lateral patellar retinaculum release, and finally a
patellofemoral arthroplasty with primary repair
and augmentation of a chronic patellar tendon
rupture). She had severe and constant left AKP
even during rest (8 in the visual analog pain
scale). She also had evident instability during
activities of daily living. She went up and down
the stairs one step at a time and was very limited
in her activities of daily living. The patient even
had difficulties getting up from a chair without
using the armrest (Preoperative Lysholm 26,
preoperative IKDC 25, preoperative Tegner
activity scale of level 1). She used to work as a
hairdresser but can no longer do it because she is
unable to stand up for long periods of time. She
only tolerates activities where she can sit.
A kinetic and kinematic study during stair
descent test revealed the following defense
mechanisms: a reduction in the extensor moment
(Fig. 9), a reduction of the ground reaction force
(Fig. 10). We also found an increase in the abductor
Fig. 9 Physical examination shows a patella alta. Lateral radiograph of the left knee showing a patella alta and a
patellofemoral arthroplasty. Knee flexion-extension moment during stair descending test
Kinetic and Kinematic Analysis in Evaluating Anterior Knee …
685
Fig. 10 Vertical ground reaction force during stair descending test
Fig. 11 Standard Technetium 99 methylene diphosphonate (Technetium-99m MDP) bone scan showing increased
osseous metabolic activity in femoral condyles. Knee abduction moment during stair descending test
moment, hence a tibiofemoral overload (Fig. 11).
The extensor moment reduction entails the suppression of one of the impact absorption mechanisms of the knee. This is clearly going to favor the
development a tibiofemoral osteoarthritis.
Case # 2. Severe Patellofemoral Osteoarthritis
and Medial Patellar Instability in a Multioperated Young Patient
A 41-year-old female came to our institution
complaining mainly of disabling right patellofemoral instability and of severe right AKP that
had not improved with appropriate physical
therapy. She had severe PFOA. A reconstruction
of the lateral retinaculum using fascia lata was
performed following the technique described by
Jack Andrish.
Kinetic and kinematic analyses were performed during stair descent (Fig. 12). They
showed that the patient had: (1) a stair descent
pattern with knee extension (strategy to avoid
instability and therefore pain), (2) a decrease in
the stance phase duration on the platform,
(3) reduced values of the extensor moment (with
the subsequent reduction in quadriceps contraction and therefore, a reduction of the PFJ reaction
686
V. Sanchis-Alfonso and J. M. Baydal-Bertomeu
A
B
C
D
Fig. 12 Knee kinetics and kinematics during stair
descent. A Knee joint angle during stair descent.
B Ground force reactions during stair descent.
force, being the final goal to reduce pain), and
(4) reduced values of the abduction moment that
provokes a reduction of the lateral tibiofemoral
compression force on one hand and a reduction
in the force exerted proximally by the medial
collateral ligament on the other hand (the final
result is the reduction of the lateral and medial
tibiofemoral compression forces). Kinetic and
kinematic analyses during stair descent were
performed at 6 months and 12 months after
surgery (Fig. 12) and showed a progressive
recovery of the kinetic and kinematic parameters.
She is pain-free despite the severe PFOA and the
increment in the extensor moment. When this is
the case, there is an increment in the PFJ reaction
force after surgery.
C Flexion-extension knee moments during stair descent.
D Abduction-adduction knee moments during stair
descent
6
Take Home Messages
– Most assessments of AKP treatment progression are made using subjective measurements.
Kinetic and kinematic analyses would be
appropriate to rovide the physician with an
objective dynamic measurement of treatment
progression.
– However, we must insist that the kinetic and
kinematic analysis of stair descent is not a
diagnostic tool.
– AKP patients use strategies to decrease PFJ
loading while going downstairs when they are
compared to a pain-free control group. The
problem is that compensatory strategies
Kinetic and Kinematic Analysis in Evaluating Anterior Knee …
require some time to develop and may remain
even when pain disappears, which weakens
the usefulness of this measurement technique as a treatment progression evaluation
method.
– Kinetic and kinematic analysis helps us to
understand some of the mechanisms behind
the development of knee osteoarthritis in AKP
patients.
References
1. Costigan PA, Deluzio KJ, Wyss UP. Knee and hip
kinetics during normal stair climbing. Gait Post.
2002;16:31–7.
2. Woltring H. 3-d attitude representation: a standardization proposal. J Biomech. 1994;27:1399–414.
3. Page A, De Rosario H, Mata V, et al. Effect of
marker cluster design on the accuracy of human
movement analysis using stereophotogrammetry.
Med Biol Eng Comput. 2006;44:1113–9.
4. Fulkerson JP. Disorders of the patellofemoral joint.
Philadelphia: Lippincott Williams & Wilkins; 2004.
5. Kowalk DL, Duncan JA, Vaughan CL. Abductionadduction moments at the knee during stair ascent
and descent. J Biomech. 1996;29:383–8.
6. Grood ES, Noyes FR. Diagnosis of knee ligament
injuries: biomechanical precepts. In: Feagin JA,
editor. The crucial ligaments. New York: Churchill
Livingstone; 1988. pp 245–60.
7. Brechter JH, Powers ChM. Patellofemoral joint stress
during stair ascent and descent in persons with and
without patellofemoral joint. Gait Post. 2002;16:
115–23.
687
8. Salsich GB, Brechter JH, Powers ChM. Lower
extremity kinetics during stair ambulation in patients
with and without patellofemoral joint. Clin Biomech.
2001;16:906–12.
9. Grenholm A, Stensdotter AK, Hager-Ross CH.
Kinematic analyses during stair descent in young
women with patellofemoral pain. Clin Biomech.
2009;24:88–94.
10. Powers CM, Landel R, Perry J. Timing and intensity
of vastus muscle activity during functional activities
in subjects with and without patellofemoral pain.
Phys Ther. 1996;76:946–55.
11. Crossley KM, Cowan SM, Bennell KL, et al. Knee
flexion during stair ambulation is altered in individuals with patellofemoral pain. J Orthop Res.
2004;22:267–74.
12. Greenwald AE, Bagley AM, France EP, et al. A
biomechanical and clinical evaluation of a patellofemoral knee brace. Clin Orthop. 1996;324:187–95.
13. Crossley KM, Cowan SM, McConnell J, et al.
Physical therapy improves knee flexion during stair
ambulation in patellofemoral pain. Med Sci Sports
Exerc. 2005;37:176–83.
14. Powers CM, Perry J, Hsu A, et al. Are patellofemoral
pain and quadriceps femori muscle torque associated
with locomotor function? Phys Ther. 1997;77:1063–
75.
15. Hinman RS, Crossley KM, McConnell J, et al. Does
the application of tape influence quadriceps sensorimotor function in knee osteoarthritis? Rheumatology.
2004;43:331–6.
16. Näslund J, Odenbring S, Näslund UB, et al. Diffusely
increased bone scintigraphic uptake in patellofemoral
pain syndrome. Br J Sports Med. 2005;39:162–5.
17. Elahi S, Cahue S, Felson DT, et al. The association
between varus-valgus alignment and patellofemoral
osteoarthritis. Arthritis Rheum. 2000;43:1874–80.
Patellofemoral Instrumented Stress
Testing
Ana Leal, Renato Andrade, Cristina Valente,
André Gismonti, Rogério Pereira,
and João Espregueira-Mendes
1
Background
Patellofemoral disorders display a high incidence
in the population and mostly affect the younger
and more active population. There is a wide
spectrum of presentation of patellofemoral disorders, and may include anterior knee pain,
potential patellar instability (PPI) and objective
patellar instability (OPI). These conditions are
associated with a higher risk to develop joint
osteoarthritis, which will have an important and
negative long-term both life-quality and
A. Leal
CMEMS—Center for MicroElectroMechanical
Systems, University of Minho, Campus Azurém,
Guimarães, Portugal
R. Andrade C. Valente R. Pereira
J. Espregueira-Mendes (&)
Dom Henrique Research Centre, Porto, Portugal
e-mail: espregueira@dhresearchcentre.com
R. Andrade C. Valente A. Gismonti R. Pereira
J. Espregueira-Mendes
Clínica Espregueira - FIFA Medical Centre of
Excellence, Porto, Portugal
R. Andrade
Porto Biomechanics Laboratory (LABIOMEP),
Faculty of Sports, University of Porto, Porto,
Portugal
socioeconomic impact. An accurate and early
diagnosis of the patellofemoral abnormalities has
the potential to indicate the most adequate
treatment approach and implement secondary
prevention strategies which will positively
impact the long-term health-related quality of life
of these patients, as well as their socioeconomic
status.
The risk for patellofemoral instability is usually determined using four anatomical risk factors initially defined by Dejour et al. in 1994 [1]:
(1) trochlear dysplasia, (2) quadriceps dysplasia
R. Pereira
Faculty of Sports, University of Porto, Porto,
Portugal
Health Science Faculty, University Fernando Pessoa,
Porto, Portugal
J. Espregueira-Mendes
3B’s Research Group–Biomaterials, Biodegradables
and Biomimetics, Headquarters of the European
Institute of Excellence on Tissue Engineering and
Regenerative Medicine, AvePark, Parque de Ciência
e Tecnologia, Zona Industrial da Gandra, University
of Minho, 4805-017 Barco, Guimarães, Portugal
ICVS/3B’s–PT Government Associate Laboratory,
Braga/Guimarães, Portugal
School of Medicine, University of Minho, Braga,
Portugal
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_53
689
690
(patellar tilt), (3) patellar subluxation as expressed as excessive distance between the tibial
tubercle and the trochlear groove (TT-TG), and
(4) patella alta. Although these risk factors show
reasonable sensitivity, there are limited by poor
specificity in patients with patellofemoral instability [2], compromising their discriminative
capabilities. Moreover, trochlear dysplasia is
usually considered the most reliable discriminator of patellofemoral instability [2], but patellar
morphology and morphometry is highly variable
in knees with and without patellofemoral instability and there is minimal association between
morphometric measurement and trochlear dysplasia [3].
A myriad of other anatomical and biomechanical factors has been identified in the literature [2, 4–9], but most notably for patellofemoral
instability is the insufficiency or rupture of
structures of the medial patellofemoral complex:
medial patellofemoral ligament (MPFL), medial
quadriceps tendon femoral ligament (MQTFL),
medial patellotibial ligament (MPTL) and medial
patellomeniscal ligament (MPML) [10–13]. All
these factors—isolated or combined—can lead to
unbalanced biomechanical behaviour of the
patellofemoral joint that promotes abnormal
patellofemoral tracking and altered joint contact
forces which can result in patellofemoral instability and/or joint degeneration [14, 15].
The etiopathogenesis of patellofemoral instability is thus multifactorial and complex. There
are currently many limitations in the physical
examination of patellofemoral instability that will
underscore the capability of an accurate diagnosis. Most notably, the current techniques and
tools to only provide an approximate and subjective estimation of patellofemoral joint laxity.
The physical examination has poor reproducibility and reliability [16, 17] and the imaging
techniques lack validity to measure joint laxity.
Instrumented-assisted biomechanical testing
of patellofemoral joint laxity contribute to better
understand the dynamic role of the soft tissues
and their active interplay on the pathomechanics
of patellofemoral instability. Instrument-assisted
examination emerges as a clinical solution to
overcome the current limitations in measuring
A. Leal et al.
patellofemoral laxity. It has thus a crucial role in
objectifying, quantifying and standardizing the
assessment of individuals with patellofemoral
disorders.
2
Instability Versus Laxity
Joint instability is a symptom that the patient
describes as the joint feeling unstable when
moving, walking, running, jumping or twisting.
Frequently, patients will refer that the joint
“gives away”. Instability is subjective and only
reported by the patient. Conversely, joint laxity is
the passive response of joint movement as a
result of an externally applied force or torque.
Joint laxity is an objective and measurable
parameter. Human joints may present physiological laxity (normal laxity) or pathological
laxity (abnormal laxity). Physiological joint laxity is normal within any human joint as a result of
joint movement. Abnormal joint laxity occurs
when there is more joint movement than what
can be considered as physiological laxity.
Instability and laxity are thus different and not
interchangeable clinical terms, which may or
may not exist concomitantly—i.e., we may find a
patient with feeling of instability without joint
laxity, a patient with pathological laxity but
without joint instability, or even a patient with
both joint instability and pathological laxity. The
joint laxity profile varies among individuals.
Inter-individual differences in joint laxity can
arise from differences related to age and sex,
bone morphology and morphometrics, soft tissue
insufficiency, and among other factors.
3
Clinical and Imaging Assessment
of Patellofemoral Joint Instability
Diagnosis of patellofemoral instability is firstly
made through a clinical history survey and physical
examination [18–20]. The clinical diagnosis is then
reinforced by imaging exams, including radiography, magnetic resonance imaging (MRI) and/or
computed tomography (CT) [19, 21]. The final
diagnosis of patellofemoral instability is then
Patellofemoral Instrumented Stress Testing
achieved by a correlation of clinical history,
physical examination and imaging findings.
During physical examination, there are many
clinical static and dynamic physical tests available to assess the patellofemoral joint [16, 18,
20]. Most of these tests are assessed qualitatively
(rather than quantitatively) and not supported
accuracy and/or validity for the existent methods
[17]. Whilst manual clinical examination is still
paramount for an adequate diagnosis of patellofemoral instability, it is subjective both in the
examiner’s technique and interpretation [19].
Manual examination of patellofemoral joint laxity is limited because it lacks precision (objective
quantification) and reproducibility [16, 17, 19].
The examiner evaluates the patellofemoral joint
laxity manually by pushing the patella medially
and laterally and then subjectively quantifying
the patellar movement in quadrants (0 to 4
quadrants). This measure lacks precision because
it cannot ascertain how much millimeters the
patella displaced, but only an approximation (in
quadrants). Moreover, this measurement also
fails to be reproducible because the amount of
force applied and interpretation of movement can
vary according the examiner’s experience and
sensibility (either when comparing between different examiners, or the same examiner in different
evaluations).
With
accumulated
experience, the intra-rater reliability can achieve
good results, but inter-rater reliability is poor
when using manual tests to assess laxity in
patellofemoral instability [16, 17]. Traditional
and available physical examination methods to
measure patellofemoral joint laxity are thus not
suitable for universal application and can result
inaccurate measurement of laxity and misdiagnosis of patellofemoral instability.
The imaging findings play a crucial role in
detecting any structural damage (e.g., MPFL
damage) and identifying potential anatomical,
morphological and morphometric factors that are
associated with an increased risk for patellar
dislocation and/or patellofemoral instability [1, 2,
4, 6, 9]. Although imaging has great clinical
value to assess structural damage and anatomical
risk factors, it is a static assessment and is not
691
capable to measure the biomechanical competence of soft tissue structures in restraining joint
laxity. For the case of patellofemoral joint,
imaging technique can identify an uninjured
MPFL, but cannot ascertain if the MPFL is lax
and if it is able to maintain joint stability while
withstanding medio-lateral and tilt stress in the
patella. Therefore, the currently available imaging methods do not provide a dynamic assessment of joint instability and lack an association
with the injury pattern [22].
The poor reproducibility and reliability of
physical examination allied to the lack of validity
of imaging techniques to measure joint laxity
clearly highlight the need for other tools that can
provide an accurate, reliable and reproducible
method to measure patellofemoral joint laxity.
4
Measurement of Joint Laxity
Instrumented assessment has emerged as a
potential solution to obtain a precise quantification
of joint laxity, thus providing a more objective
assessment of joint stability. Instrument-assisted
tools to measure patellofemoral joint laxity aim to
describe and quantify the bony displacement of the
patella in relation to the femoral trochlea upon the
application of an external force. Results of joint
laxity measurement can then be used as cut-off
values to serve as dichotomic screening tools to
elicit one of two diagnostic results: biomechanically incompetent or competent ligaments. The
diagnostic result of biomechanically incompetent
(lax) ligaments will be linked to an increased risk
of patellar dislocation. Results of joint laxity can
be interpreted as unilateral or then compared by
side-to-side difference (SSD). Beyond the
dichotomous application, laximetry can become
an important diagnosis and profiling tool of different patterns of patellofemoral ligament laxity
(stiffness) and their interference in patellofemoral
arthrokinematics, treatment decision-making and
surgical planning, for prognostic purposes or to
quantify post-operative joint laxity.
There have been a few attempts to develop
instrument-assisted
methods
to
measure
692
patellofemoral laxity [23–31], but the currently
available methods show high heterogeneity in the
methods for assessing patellofemoral laxity and
report variable measurement outcomes [32].
These existing instrument-assisted methods are
additionally limited regarding its reproducibility
as some of these methods apply the stress manually (subjective variability in the force applied),
and all lack precision and accuracy as the measure the joint laxity is made externally to the joint
(i.e., measured visually or using electronic tools),
which only provides an approximation of the true
(intra-articular) patellar displacement. Only one
study [30] reported an arthrometer aided by
radiography to measure the patellar displacement. However, stress radiographs imply exposure to radiation and are not able to
concomitantly provide imaging evidence of
structural damage.
Safety, validity, reproducibility, precision and
accuracy are key factors when developing a
measuring device to enable a screening system
with clinical usefulness that is supported by its
sensitivity and specificity. We acknowledge that
majority of clinical tests and testing principles
yields value. Even that manual testing has its
limitations and pitfalls, it still provides a safe and
valid approximate estimation of joint laxity.
However, if reproducibility, precision and accuracy are lacking, the outcome can be deceptive
(misdiagnosis) and is not a reliable measure
when comparing with the contralateral side,
among different patients or assessors, and to use
as a reference value for benchmarking during
post-treatment assessments.
The variability found in the literature [32]
reinforces the need to develop a simple and
universally applicable instrument that is able to
reliably and objectively quantify the patellar
mobility, and thus standardize the patellofemoral
laxity assessment. The precision and accuracy of
instrumented joint laxity measurements can be
improved when it is combined with imaging
assessment. Due to the limitations identified
above for radiographs, the combination of laxity
measurement with MRI or CT seems the obvious
next step [19]. Moreover, by combining the
instrument-assisted assessment with MRI, it is
A. Leal et al.
possible to assess, within the same exam, the
joint laxity and any structural damage to the
ligaments or cartilage.
5
Porto Patella Testing Device
(PPTD)
The Porto Patella Testing Device (PPTD) is an
MRI-compatible laxity testing device, made of
an inert polymer, for the measurement of patellofemoral joint laxity (Fig. 1). The PPTD operates through two modular components with
movable activators that are triggered by air pump
systems with compressed air cylinders to stress
the patella in multiple directions. One activator
induces a medio-lateral translation of the patella
and the other an external tilt to the patella. The
force is applied progressively and is usually up to
a maximum of 0.5 Bar—converted to approximately 52.5 N load—which is a safe range to
prevent damage to the MPFL (which has a tensile
strength of 208 N [33]). The operator can manually control the magnitude of force transmission
and the force applied is also subjectively controlled by feedback from patients or by noticing
any signs of patient’s apprehension. After the
movements are applied to the patella, by using
anatomical landmarks at the MRI/CT images as
reference points, it is possible to measure the
patellar bony displacement (in relation to its
resting position) and infer the joint laxity.
5.1 PPTD Operation Protocol
The PPTD evaluation protocol starts with the
patient positioning. The patient is placed in the
device with the knee in full extension, without any
rotation or flexion of the hip and ankle joints. All
patients are instructed to avoid muscle guarding
which could interfere with joint laxity. The
patient’s anatomical axis (interline of the knee
joint) is aligned with the mechanical axis of the
PPTD and the modular components are adjusted
to the size of the patient. The lower limb is then
fixed to the PPTD using velcro straps at the thigh
and foot to restrict lower limb movement.
Patellofemoral Instrumented Stress Testing
693
Fig. 1 Photograph of the
Porto Patella Testing Device
(PPTD)
The first set of MRI/CT sequences are made
after patient positioning, but without the application of any stress at the joint. These first
sequence is made to set the resting position,
which will be used latter for benchmarking when
making the measurement of patellar displacement (Fig. 2A). Then, the second set of MRI/CT
sequences is taken after being applied a mediolateral force to the medial border of the patella
with the medial activator at 30 degrees (in relation to the patellar horizontal plane) to apply a
lateral movement to the patella (Fig. 2B). Lastly,
the medio-lateral stress is withdrawn and with the
A
B
Fig. 2 Porto Patella Testing Device (PPTD) setup for
stress-testing evaluation within imaging equipment: A initial setup without any stress to obtain the position of the
PPTD lateral actuator is placed at 70 degrees (in
relation to the patellar horizontal plane) and the
patella is pushed in an oblique anteroposterior
direction at the extreme of its anterolateral facet
to apply an external tilt movement (Fig. 2C).
5.2 Measurement Protocol
All MRI/CT sequences are taken in the axial
plane. If using MRI, the measurements are done
with sets of 1 mm spacing within the MRI slices.
Patella position is calculated as the distance
C
patella at rest; B patella stressed on its medial facet for
lateral translation; C patella stressed at the extreme of its
anterolateral facet for external tilt
694
A
A. Leal et al.
B
C
Fig. 3 PPTD sequential stress testing of a patient with
recurrent patella dislocations, with the left knee with an
MPFL tear: A patella rest position (2 mm and 22°);
B lateral transition, the patella displaced 16 mm and 8°
(moved to 18 mm and 30°); C lateral tilt, the patella
displaced 19 mm medially and increased 10° (moved to
−17 mm and 32°)
between two parallel lines—perpendicular to the
tangential line of the posterior femoral condyles—
one crossing the deepest point of the trochlear
groove and other the center of the patellar ridge
(Fig. 3). The lateral patellar angle is measured the
angle formed by the line crossing the major
transversal axis of the patella and the line tangential to the posterior femoral condyles.
The patella position is firstly measured with
the patella at rest (Fig. 3A) and then after stress is
applied. The lateral patella displacement is measured by calculating the difference between the
patella position after medio-lateral stress and the
patella position at rest (Fig. 3B). The external tilt
angle is measured by calculating the difference
between the patella position after external tilt
stress and the patella position at rest (Fig. 3C).
The patella displacement can then be interpreted
as a single unilateral displacement or as compared
to the contralateral side by calculating the SSD
of the bilateral assessment. Additionally, by
using MRI/CT sequences of incremental force
applied to the patella, it is also possible to calculate the force–displacement curves and relate it
to the ligament stiffness of the patellofemoral
joint.
5.3 PPTD Validity, Reliability
and Outcomes
The PPTD is a valid tool and reliable to assess
patellofemoral joint laxity. The PPTD is a more
valid tool to ascertain patellofemoral laxity than
manual examination because it is able to produce
a pre-determined and reproducible stress-force
application to the patella. Conversely, the manual
exam is imprecise stress-force application that is
variable to the examiner sensibility. In patients
that have withstand maximum translation force,
the PPTD yields greater lateral patellar translation (converted in quadrants) as compared to
manual exam. Measurement of patellar displacement using PPTD is thus more accurate and
precise than the visual estimation of translated
quadrants by manual exam. Moreover, the PPTD
provide a reliable measurement of patellofemoral
joint laxity with excellent intra-rater agreement
(intraclass correlation coefficient 0.83–0.98) [34].
The PPTD is also a useful tool to discern
between different patellofemoral disorders
according to the profile of patellofemoral joint
stiffness (Fig. 4). The force–displacement curves
of patients with PPI (those with risk factor for
Patellofemoral Instrumented Stress Testing
695
Fig. 4 Graphical illustration
of force–displacement curves
(stiffness) for a representative
case of a patient with AKP
(green line), PPI (blue line)
and OPI (orange line)
patellofemoral instability, but without any dislocation episode) and patients with OPI (those
with clinical history of patellar dislocation) display a similar stiffness pattern, which differs from
the stiffness pattern seen in patients with anterior
knee pain. When comparing both types of
patellofemoral instability (PPI and OPI), those
with PPI display greater stiffness (a higher force
was required to displace the patella) than those
with OPI [35]. The stiffness pattern can also be
useful to compare with the contralateral uninjured side (Fig. 5) or after MPFL reconstruction
(Fig. 6) or any patellofemoral joint corrective
surgery.
Fig. 5 Graphical illustration of force–displacement
curves (stiffness) for a representative case of a patient
with OPI (recurrent dislocations), showing the curve for
the knee with OPI (red line) and the asymptomatic
contralateral knee (green line)
696
A. Leal et al.
Fig. 6 Graphical illustration
of force–displacement curves
(stiffness) for a representative
case of a patient after MPFL
reconstruction at follow-up,
showing the curve for the
MPFL-reconstructed knee
(red line) and the
asymptomatic contralateral
knee (green line)
Besides patellofemoral instability, the PPTD
can be used to assess any ligament insufficiencies
in other patellofemoral disorders. We have previously found that patients with idiopathic unilateral anterior knee pain and with
morphologically equivalent knees display greater
lateral patellar translation in the painful knee
[36], suggesting a potential insufficiency or
imbalance of the medial static patellar stabilizers.
5.4 PPTD Possible Clinical
and Research Applications
The ability of the combined evaluation of the
PPTD with the MRI to visualize the soft tissues
concomitantly with the accurate and precise
measurement of joint laxity allows to correlate
the structural integrity of the ligaments with its
functional competence. Moreover, it allows
within the same evaluation to identify any damage to other structures, such as the articular cartilage, as also to correlate with bony
morphological and morphometric features (such
as, trochlear dysplasia and patella alta or baja).
Ultimately, this combined evaluation provides a
precise and complete assessment of the patellofemoral status that will be helpful for diagnostic
purposes of patellofemoral disorders. Therefore,
the PPTD adds diagnostic value and contributes
in the therapeutic decision-making and surgical
planning.
The PPTD can play an important role in
establishing cluster profiles of patellofemoral
joint laxity as it combines the assessment of both
“anatomy” and “function”. For example, the
MRI exam might identify absence of MPFL tear
after a patellar dislocation, but the addition of the
PPTD assessment can reveal incompetent MPFL
to provide stability to the patellofemoral joint
that warrants conservative or surgical intervention. Using the PPTD, we may identify subclinical groups of patellofemoral instability that may
require differentiated or additional surgical
interventions and thus refine our surgical indications and individualize the treatment. For
example, we may identify a patient with extensive patellofemoral joint laxity that may benefit
from combined reconstruction of the MPFL with
the MQTFL [10] or with the MPTL [37]. Eventually, we may establish joint laxity cluster profiles that are able to provide prognostic value for
each subclinical group with patellofemoral
instability.
The PPTD can also have clinical value to
evaluate the joint laxity outcomes of patients
with patellofemoral instability that underwent
ligament reconstructive surgery. With the PPTD,
we can prospectively monitor the patellofemoral
joint laxity and evaluate if there is any residual
Patellofemoral Instrumented Stress Testing
laxity in the operated knee by comparing to the
pre-surgery laxity profile of the operated knee
and to the non-operated contralateral side. It can
also be useful to compare the joint laxity outcomes between different surgical techniques
(with or without concomitant surgeries) and any
conservative approaches. Lastly, by providing
information about the potential presence of
residual laxity, the PPTD can be useful for the
decision to clear athletes to unrestricted sporting
activities or pinpoint those that may require further rehabilitation or surgical reintervention.
697
4.
5.
6.
7.
8.
6
Conclusions
The PPTD is an MRI/CT compatible testing
device to evaluate patellofemoral joint laxity. It
provides a valid, reliable, accurate and precise
measurement of patellar displacement under
applied stress to the patella and thus identify
patients with pathological patellofemoral joint
laxity. By analyzing the joint laxity and stiffness
profile, this instrument-assisted MRI evaluation
can identify subclinical cluster groups of patients
with patellofemoral instability and thus personalize the treatment to the patient’s individual
needs. The use of the PPTD can thus be very
useful in the clinical practice to support diagnostic decisions, customize the therapeutic
decision-making and surgical planning, and follow the joint laxity profile outcomes after conservative or surgical interventions.
References
1. Dejour H, Walch G, Nove-Josserand L, Guier C.
Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc.
1994;2:19–26.
2. Ridley TJ, Hinckel BB, Kruckeberg BM, Agel J,
Arendt EA. Anatomical patella instability risk factors
on MRI show sensitivity without specificity in
patients with patellofemoral instability: a systematic
review. J ISAKOS. 2016;1:141–52.
3. Jimenez AE, Levy BJ, Grimm NL, Andelman SM,
Cheng C, Hedgecock JP, Cohen A, Pace JL. Relationship between patellar morphology and known
9.
10.
11.
12.
13.
14.
15.
16.
anatomic risk factors for patellofemoral instability.
Orthop J Sports Med. 2021;9:2325967120988690.
Arendt EA, England K, Agel J, Tompkins MA. An
analysis of knee anatomic imaging factors associated
with primary lateral patellar dislocations. Knee Surg
Sports Traumatol Arthrosc. 2017;25:3099–107.
McCarthy MI, Hinckel BB, Arendt EA, Chambers CC. Putting it all together: evaluating patellar
instability risk factors and revisiting the “Menu.”
Clin Sports Med. 2022;41:109–21.
Diederichs G, Issever AS, Scheffler S. MR imaging
of patellar instability: injury patterns and assessment
of risk factors. Radiographics. 2010;30:961–81.
Neyret P, Robinson AH, Le Coultre B, Lapra C,
Chambat P. Patellar tendon length–the factor in
patellar instability? Knee. 2002;9:3–6.
Escala JS, Mellado JM, Olona M, Giné J, Saurí A,
Neyret P. Objective patellar instability: MR-based
quantitative assessment of potentially associated
anatomical features. Knee Surg Sports Traumatol
Arthrosc. 2006;14:264–72.
Kaiser P, Schmoelz W, Schoettle P, Zwierzina M,
Heinrichs C, Attal R. Increased internal femoral
torsion can be regarded as a risk factor for patellar
instability-a biomechanical study. Clin Biomech
(Bristol, Avon). 2017;47:103–9.
Espregueira-Mendes J, Andrade R, Bastos R,
Joseph S, Fulkerson JP, Silva LD. Combined soft
tissue reconstruction of the medial patellofemoral
ligament and medial quadriceps tendon-femoral
ligament. Arthrosc Tech. 2019;8:e481-8.
Hinckel BB, Gobbi RG, Demange MK,
Pereira CAM, Pécora JR, Natalino RJM,
Miyahira L, Kubota BS, Camanho GL. Medial
patellofemoral ligament, medial patellotibial ligament, and medial patellomeniscal ligament: anatomic, histologic, radiographic, and biomechanical
study. Arthroscopy. 2017;33:1862–73.
Hinckel BB, Gobbi RG, Kaleka CC, Camanho GL,
Arendt EA. Medial patellotibial ligament and medial
patellomeniscal ligament: anatomy, imaging, biomechanics, and clinical review. Knee Surg Sports
Traumatol Arthrosc. 2018;26:685–96.
Tanaka MJ, Chahla J, Farr J 2nd, LaPrade RF,
Arendt EA, Sanchis-Alfonso V, Post WR, Fulkerson JP. Recognition of evolving medial patellofemoral
anatomy provides insight for reconstruction. Knee
Surg Sports Traumatol Arthrosc. 2019;27:2537–50.
Mäenpää H, Lehto MU (1997) Patellofemoral
osteoarthritis after patellar dislocation. Clin Orthop
Relat Res. 156–62.
Elliott CC, Diduch DR. Biomechanics of patellofemoral instability. Op Tech Sports Med. 2001;9:112–21.
Smith TO, Clark A, Neda S, Arendt EA, Post WR,
Grelsamer RP, Dejour D, Almqvist KF, Donell ST.
The intra- and inter-observer reliability of the
physical examination methods used to assess patients
with patellofemoral joint instability. Knee.
2012;19:404–10.
698
17. Smith TO, Davies L, Donell ST. The reliability and
validity of assessing medio-lateral patellar position: a
systematic review. Man Ther. 2009;14:355–62.
18. Kantaras AT, Selby J, Johnson DL. History and
physical examination of the patellofemoral joint with
patellar instability. Op Tech Sports Med.
2001;9:129–33.
19. Leal A, Pereira R, Pereira H, Silva FS, Flores P,
Espregueira-Mendes J. Patellofemoral evaluation: do
we need an objective kinematic approach? In: The
patellofemoral joint. Springer;2014. p. 37–44.
20. Calderón CA, Andrade R, Bastos R, Valente C,
Maestro A, Peña RS, Espregueira-Mendes J. Examination of the patients with patellofemoral symptoms.
In: The patellofemoral joint. Springer;2022. p. 27–37.
21. Mayfield A, Koh JL. Imaging evaluation in the
patient with patellofemoral symptoms. In: The
patellofemoral joint;2022. p. 39–44.
22. Tompkins MA, Rohr SR, Agel J, Arendt EA.
Anatomic patellar instability risk factors in primary
lateral patellar dislocations do not predict injury
patterns: an MRI-based study. Knee Surg Sports
Traumatol Arthrosc. 2018;26:677–84.
23. Egusa N, Mori R, Uchio Y. Measurement characteristics of a force-displacement curve for chronic
patellar instability. Clin J Sport Med. 2010;20:458–63.
24. Fithian DC, Mishra DK, Balen PF, Stone ML,
Daniel DM. Instrumented measurement of patellar
mobility. Am J Sports Med. 1995;23:607–15.
25. Joshi RP, Heatley FW. Measurement of coronal
plane patellar mobility in normal subjects. Knee Surg
Sports Traumatol Arthrosc. 2000;8:40–5.
26. Kujala UM, Kvist M, Osterman K, Friberg O,
Aalto T. Factors predisposing Army conscripts to
knee exertion injuries incurred in a physical training
program. Clin Orthop Relat Res. 1986;203–12.
27. Ota S, Nakashima T, Morisaka A, Ida K, Kawamura M. Comparison of patellar mobility in female
adults with and without patellofemoral pain. J Orthop
Sports Phys Ther. 2008;38:396–402.
28. Reider B, Marshall JL, Warren RF. Clinical characteristics of patellar disorders in young athletes. Am J
Sports Med. 1981;9:270–4.
A. Leal et al.
29. Skalley TC, Terry GC, Teitge RA. The quantitative
measurement of normal passive medial and lateral
patellar motion limits. Am J Sports Med.
1993;21:728–32.
30. Teitge RA, Faerber WW, Des Madryl P, Matelic TM.
Stress radiographs of the patellofemoral joint. J Bone
Joint Surg Am. 1996;78:193–203.
31. Wong YM, Ng GY. The relationships between the
geometrical features of the patellofemoral joint and
patellar mobility in able-bodied subjects. Am J Phys
Med Rehabil. 2008;87:134–8.
32. Leal A, Andrade R, Flores P, Silva FS, EspregueiraMendes J, Arendt E. High heterogeneity in in vivo
instrumented-assisted patellofemoral joint stress testing: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2019;27:745–57.
33. Amis AA, Firer P, Mountney J, Senavongse W,
Thomas NP. Anatomy and biomechanics of the
medial patellofemoral ligament. Knee. 2003;10:215–
20.
34. Leal A, Andrade R, Hinckel BB, Tompkins M,
Flores P, Silva F, Espregueira-Mendes J, Arendt E.
A new device for patellofemoral instrumented stresstesting provides good reliability and validity. Knee
Surg Sports Traumatol Arthrosc. 2020;28:389–97.
35. Leal A, Andrade R, Hinckel B, Tompkins M,
Bastos R, Flores P, Samuel F, Espregueira-Mendes
J, Arendt E. Patients with different patellofemoral
disorders display a distinct ligament stiffness pattern
under instrumented stress testing. J ISAKOS.
2020;5:74–9.
36. Leal A, Andrade R, Flores P, Silva FS, Fulkerson J,
Neyret P, Arendt E, Espregueira-Mendes J. Unilateral
anterior knee pain is associated with increased
patellar lateral position after stressed lateral translation. Knee Surg Sports Traumatol Arthrosc.
2020;28:454–62.
37. Hinckel BB, Gobbi RG, Demange MK, Bonadio MB,
Pécora JR, Camanho GL. Combined reconstruction
of the medial patellofemoral ligament with quadricipital tendon and the medial patellotibial ligament with
patellar tendon. Arthrosc Tech. 2016;5:e79-84.
Anterior Knee Pain and Functional
Femoral Maltorsion in Patients
with Cam Femoroacetabular
Impingement
Marc Tey-Pons, Vicente Sanchis-Alfonso,
and Joan Carles Monllau
1
Introduction
Previous chapters have shown how anterior knee
pain, with an estimated prevalence between 12 and
25% of the population in the 2nd to 4th decade of
life, is a common reason for consultation in
orthopedic surgery and frequently has no clear
cause to justify it [1, 2]. Anatomical alterations and
biomechanical imbalances of the knee are usually
studied to rule out mechanical overload, secondary
patellar cartilage alteration and pain as the ultimate
consequence. However, anatomical and biomechanical studies of the knee frequently do not
identify an obvious patellofemoral disorder. It is in
this context that the differential diagnosis should
M. Tey-Pons (&)
Department of Orthopaedic Surgery, iMove
orthopaedics, Hospital Mi Tres Torres, Barcelona,
Spain
e-mail: mtey@imovetrauma.com
V. Sanchis-Alfonso
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
J. C. Monllau
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
focus on proximal or distal causes of patellar pain
[3]. Torsional disorders, discussed in chapters
“Femoral and Tibial Rotational Abnormalities Are
the Most Ignored Factors in the Diagnosis and
Treatment of Anterior Knee Pain Patients. A Critical Analysis Review”, “Why is Torsion Important in the Genesis of Anterior Knee Pain?” and
“Rotational Osteotomy. Principles, Surgical
Technique, Outcomes and Complications”, are an
important element in this biomechanical imbalance of the proximal knee musculature. Other
alterations in the morphology of the proximal
femur, such as cam-type morphology of the
femoral head, which causes femoroacetabular
impingement syndrome (SFAI), have been related
to the manifestation of anterior knee pain [4].
A distinct morphological alteration with an adaptive process with similar consequences could be
termed a functional torsional disorder.
2
Proximal Causes of Anterior Knee
Pain
The most current evidence suggests that patients
with patellofemoral pain (PFP) have altered neuromuscular activity in the proximal musculature
during various activities such as running, jumping
or stair climbing [5–7]. Weakness of the Gluteus
Medius [8] but also of the vastus medialis obliquus
[5], an important medial stabilizer of the patella,
has been widely studied. The result of this muscular imbalance is an increase in the abductor
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_54
699
700
moment of the knee, with an overload on the
external patellofemoral joint that initiates the
pathophysiological process that will lead to pain,
as has been amply explained in previous chapters.
There is a broad consensus on the association of
PFP with Gluteus Medius weakness and hip
external rotation deficit. Meira et al. in an
exhaustive review conclude that the relationship
between hip position and anterior pain is clear,
finding several references to increased hip
adduction and internal rotation in relation to
anterior pain [9], despite the bias since most of the
studies have been carried out in a female population and runners and the causal relationship is not
established. Other studies, such as that of Boling,
identify increased external rotation strength in
runners with anterior knee pain compared to
controls. Therefore, the question arises as to
whether patients with abductor weakness have
greater patellar pain or whether patellar pain
generates more abductor muscle exhaustion.
Tibial torsional disorders involve a rotational
disturbance in the frontal plane of the patella [10],
which is radically different from rotational disorders of the femur in which the patella undergoes a
translational disturbance [10]. Rotational disorders result in joint pressure increases at the patella,
while patients with femoral torsional disorders
experience an adaptive disorder, whereby they
alter limb rotations at the hip to compensate for the
rotational disturbance, thereby altering the relationship between hip position and patella, related
to anterior knee pain.
Alterations of the hip and proximal femur may
favor some of the force balance disorders
responsible for the increased abductor moment of
the knee, causing the onset of patellar pain. One
could think of the proximal femur as a distant
cause of the PFP, or of anterior knee pain as a
distant symptom of proximal femoral imbalances.
In the approach to hip pathology proposed by
Kelly, in which a layered analysis is established,
the last layer is the kinematic chain [11].
According to this, the semiology at a distance
from the original problem is analyzed, and anterior knee pain should be recognized as a symptom
of the pathology of the proximal femur. This
could be presented as a purely semantic discussion, but it has important clinical implications that
M. Tey-Pons et al.
should be carefully analyzed. This chapter will
analyze how these morphological variations of
the hip alter the biomechanics of the limb, in the
same way as torsional changes, so we call them
functional torsional alterations, having as clinical
manifestation some local signs at the hip level,
and some distal signs at the knee level.
3
Biomechanical Conflicts
of the Hip
Osteoarthritis of the hip is a highly prevalent
pathology, classically labeled as primary or of
idiopathic etiology. With very well-known
exceptions, such as avascular necrosis, posttraumatic deformity, rheumatic or depositional
diseases, and some systemic diseases with joint
involvement, hip osteoarthritis has been considered linked to aging, but without a clear cause to
justify it. The Stolzalpe school represents a
paradigm shift, since it defines osteoarthritis of
the hip in young adults, that which occurs before
the age of 50–55 years, as secondary to identifiable processes in 95% of the cases. Among the
identifiable causes, mechanical conflicts play a
prominent role, accounting for 70% [12].
The progressive development of hip preservation surgery techniques led by the Bern school has
increased the interest and study of biomechanical
conflicts, as they represent a potentially treatable
pathology that could change the natural history of
osteoarthritis. These biomechanical conflicts are
divided into two large groups, according to the
alteration of joint kinematics, although with
important kinetic implications, ultimately responsible for favoring and initiating joint degeneration.
On the one hand, we find the dynamic conflicts of
space, where the articular kinematic excursion is
diminished by alteration of the femoroacetabular
relationship, or by morphological alteration of one
or both parts. On the other hand, dynamic stability
conflicts are described, where the joint loses its
congruence during movement, due to a lack of hip
stabilizing mechanisms, favored by an alteration in
the joint contact area or in the acetabular coverage
of the femoral head. These conditions imply an
alteration in the articular kinematics, with the
alteration of the normal articular mobility and
Anterior Knee Pain and Functional Femoral Maltorsion …
conflict of the periarticular soft tissues, and of the
articular kinetics, with an abnormal distribution of
articular loads. This alteration of loads, together
with the lesion of periarticular soft tissues, will be
responsible for initiating the joint degenerative
process, the ultimate evolution of these conflicts as
we announced [13].
Dynamic space conflicts have been grouped
under the SFAI, in which the patient experiences
groin pain associated with a conflict between the
femur and acetabulum. Initially described by
Ganz as a biomechanical imbalance attributed to
a morphological alteration of the femoral head
(cam-type SFAI) and/or an alteration of the
acetabular coverage (pincer-type SFAI) [14], but
later extended to other causes of mechanical hip
space conflict, either intra- or extra-articular
causes such as Subspine Impingement, Ischiofemoral Impingement or torsional disorders [15].
4
Anterior Knee Pain
in Biomechanical Conflicts
of the Hip
Morphological alterations of the proximal femur
can favor a biomechanical conflict in the hip as
explained. The clinical picture is determined by
the joint impingement, such as the alteration of
the normal range of motion, the suffering of
articular tissues such as the acetabular labrum or
the articular cartilage, but also by the adaptive
mechanisms that are put in place to compensate
for the conflict. Thus, in patients with hip dysplasia, with insufficient anterolateral femoral
coverage, the gait pattern is altered [16] unbalancing the normal biomechanical functioning,
responsible for the appearance of pain due to
overload or misuse in the groin, but also in the
posterior and lateral aspect of the hip [17].
Similarly, patients with SFAI have groin pain
due to anterior joint impingement but may also
experience pain in the gluteal region or on the
lateral aspect of the hip [18]. The impact of torsional disturbances on hip muscle balance and
thus on the imbalance of the knee extensor
apparatus, with increased knee abductor moment
and the occurrence of PFP is well demonstrated
701
by biomechanical studies [10] and proven in
routine clinical practice.
Biomechanical conflicts of the hip may be
responsible for the occurrence of anterior knee
pain by several mechanisms. Femoral internal
rotation (or increased femoral antetorsion) leads
to mechanical disadvantage for the abductor
musculature, which loses leverage and increased
internal rotation of the hip as a compensatory
mechanism for muscle fatigue to increase the
moment of force. The alteration of the sphericity
of the femoral head, called cam morphology due
to the kinematic alteration it produces, responds
to a particular type of morphology of the proximal femur which in biology is called coxa recta.
It is the hip presented by mammals adapted to the
savannah, with a powerful hip for running, in
which there is a decreased cervical-cephalic offset or a loss of sphericity of the femoral head,
with an increased radius in the anterior and lateral region of the femoral head [19]. However,
this powerful proximal femur has a more limited
range of motion, and impinge with the anterior
acetabular rim at flexion with internal rotation.
Damage to the soft tissues may start pain and it is
known as SFAI. Image 1 shows a patient with
cam-type femoral head during hip arthroscopy
before and after osteochondral resection. Damage
to femoral cartilage explains how impingement
limits flexion and why external rotation is needed
to increase flexion without impinging. An
abnormal gait with increased external rotation,
similar to patients with femoral retrotorsion can
be observed.
The cam-type morphology of the proximal
femur may not only be responsible for an alteration in hip joint kinematics but produces an
adaptive disorder of the entire lower extremity,
as has been demonstrated by gait studies. The
alteration in gait produced by FAI cam leads to
an increase in external rotation, similar to
femoral retrotorsion [20–22]. Therefore, when
analyzing the muscle imbalance produced by
cam-type SFAI and the subsequent increased
abductor moment of the knee, it can be assumed
as a functional femoral retrotorsion. If we
understand anterior knee pain as a distant
symptom of cam-type SFAI, in the same way as
702
M. Tey-Pons et al.
A
B
Image 1 A Cam-type femoral head with damaged
cartilage (black arrow) due to impingement with the
acetabular rim. View of peripheral compartment of right
hip from anterolateral portal. B Osteochondroplasty is
performed and impingement has been eliminated
it is in femoral retrotorsion, SFAI should be
considered in patients with cam morphology,
without groin pain but with anterior knee pain.
Cam-type femoral head may produce SFAI
because of anterior impingement.
Cam-type femoral head may produce external
rotation to avoid impingement, with secondary
muscle imbalance similar to that produced by
retrotorsion.
5
Take-Home Messages
Proximal ethiology of anterior knee pain is well
known, and it is related to imbalance of proximal
muscles.
Abnormal torsions have been related to that
imbalance.
6
Key-Message
PFP can be a distant symptom of cam-type FAI.
Anterior Knee Pain and Functional Femoral Maltorsion …
703
References
12.
1. Mujahid Z, Afzal W, Ahmad A, Gilani SA, Akram F,
Ashiq A. Prevalence of patellofemoral pain disorder
or anterior knee pain in both genders ages between
18 and 35. Rawal Med J. 2019;44(1).
2. Roush JR, Curtis Bay R. Prevalence of anterior knee
pain in 18–35 year-old females. Int J Sports Phys
Ther. 2012;7(4).
3. Powers CM, Bolgla LA, Callaghan MJ, Collins N,
Sheehan FT. Patellofemoral pain: proximal, distal,
and local factors, 2nd international research retreat.
J Orthop Sports Phys Ther. 2012;42(6):A1-54.
4. Sanchis-Alfonso V, Tey M, Monllau JC. A novel
association between femoroacetabular impingement and
anterior knee pain. Pain Res Treat. 2015;2015:1–4.
https://www.hindawi.com/journals/prt/2015/937431/.
5. Aminaka N, Pietrosimone BG, Armstrong CW,
Meszaros A, Gribble PA. Patellofemoral pain syndrome alters neuromuscular control and kinetics
during stair ambulation. J Electromyogr Kinesiol.
2011;21(4):645–51.
6. Bolgla LA, Malone TR, Umberger BR, Uhl TL.
Comparison of hip and knee strength and neuromuscular activity in subjects with and without patellofemoral pain syndrome. Int J Sports Phys Ther. 2011;6
(4):285–96. http://www.ncbi.nlm.nih.gov/pubmed/
22163090.
7. Bolgla LA, Malone TR, Umberger BR, Uhl TL. Hip
strength and hip and knee kinematics during stair
descent in females with and without patellofemoral
pain syndrome. J Orthop Sports Phys Ther. 2008;38
(1):12–8. https://doi.org/10.2519/jospt.2008.2462.
8. Prins MR, van der Wurff P. Females with patellofemoral pain syndrome have weak hip muscles: a
systematic review. Aust J Phys. 2009;55(1):9–15.
https://linkinghub.elsevier.com/retrieve/pii/
S0004951409700558.
9. Meira EP, Brumitt J. Influence of the hip on patients
with patellofemoral pain syndrome: a systematic
review. Sports Health. 2011;3(5):455–65.
10. Lee TQ, Morris G, Csintalan RP. The influence of
tibial and femoral rotation on patellofemoral contact
area and pressure. 2003. www.jospt.org.
11. Draovitch P, Edelstein J, Kelly BT. The layer
concept: utilization in determining the pain generators, pathology and how structure determines treatment. Curr Rev Musculoskelet Med. 2012[cited 2022
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Jan 29];5(1):1–8. https://doi.org/10.1007/s12178011-9105-8.
Hofmann S, Tschauner C, Graf R. Mechanical causes
of osteoarthritis in young adults. In: HIP international. 2003.
Ganz R, Parvizi J, Beck M, Leunig M, Nötzli HSKA.
Femoroacetabular impingement: a cause for
osteoarthritis of the hip. Clin Orthop Relat Res.
2004;417:112–120.
Leunig M, Beck M, Dora C, Ganz R. Femoroacetabular impingement: etiology and surgical concept.
2005;247–55.
Bech NH, Haverkamp D. Impingement around the
hip: beyond cam and pincer. EFORT Open Rev.
2018;3(2):30–8. https://eor.bioscientifica.com/view/
journals/eor/3/2/2058-5241.3.160068.xml.
Loverro KL, Khuu A, Kao P-C, Lewis CL. Kinematic variability and local dynamic stability of gait in
individuals with hip pain and a history of developmental dysplasia. Gait Posture. 2019;68:545–54.
https://linkinghub.elsevier.com/retrieve/pii/
S0966636219300141.
Nunley RM, Prather H, Hunt D, Schoenecker PL,
Clohisy JC. Clinical presentation of symptomatic
acetabular dysplasia in skeletally mature patients.
J Bone Joint Surg Ser A. 2011;93(Suppl. 2):17–21.
Hammoud S, Bedi A, Voos JE, Mauro CS, Kelly BT.
The recognition and evaluation of patterns of compensatory injury in patients with mechanical hip pain.
Sports Health Multidiscip Approach. 2014;6(2):108–
18. https://doi.org/10.1177/1941738114522201.
Hogervorst T, Bouma HW, de Vos J. Evolution of
the hip and pelvis. Acta Orthop. 2009;80(Sup336):1–
39. https://doi.org/10.1080/17453690610046620.
Bedi A, Dolan M, Leunig M, Kelly BT. Static and
dynamic mechanical causes of hip pain. Arthrosc J
Arthrosc Relat Surg. 2011;27(2):235–51. https://
linkinghub.elsevier.com/retrieve/pii/
S0749806310007267.
Yoo WJ, Choi IH, Cho T-J, Chung CY, Park MS,
Lee DY. Out-toeing and in-toeing in patients with
perthes disease. J Pediatr Orthop. 2008;28(7):717–
22. https://journals.lww.com/01241398-20081000000004.
Sanchis-Alfonso V, Tey M, Monllau JC. Cam
femoroacetabular impingement as a possible explanation of recalcitrant anterior knee pain. Case Rep
Orthop. 2016;2016:1–5.
Finite Element Technology
in Evaluating Medial Patellofemoral
Ligament Reconstruction
Vicente Sanchis-Alfonso, Diego Alastruey-López,
Cristina Ramirez-Fuentes, Erik Montesinos-Berry,
Gerard Ginovart, Joan Carles Monllau,
and María Angeles Perez
1
Introduction
Finite element (FE) analysis originated as a
method for structural analysis in the British
aerospace industry. This methodology made it
possible to perform multiple simulations with the
computer to avoid numerous experimental tests
with the consequent savings in material, equipment and resource consumption. There are two
types of modelling that use FE technology, real
models and parametric models (PM) (Fig. 1).
A PM is a generic model, a simplified model of
reality, valid in our specific case for any knee, in
which we can introduce the patient-specific knee
variables that we want to evaluate. On the contrary, a real model is complex, expensive and
Supplementary Information The online version
contains supplementary material available at https://doi.
org/10.1007/978-3-031-09767-6_55.
V. Sanchis-Alfonso (&)
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
e-mail: vicente.sanchis.alfonso@gmail.com
time-consuming. It also requires the work of
several engineers and a system of computers
connected in series. A PM is quite the opposite.
The use of a PM can be seen in the making of
mechanical simulations in many aspects of
architecture.
Our work group has developed a PM of the
patellofemoral joint (PFJ) that makes it possible
to evaluate the reconstruction of the medial
patellofemoral ligament (MPFL) [1]. This model
has already been clinically validated in a previous study in which we evaluated different MPFL
reconstruction (MPFLr) techniques [1]. With this
technology, different MPFL surgical reconstruction techniques for a specific patient can be
simulated with the appropriate software on our
laptop [1, 2]. Moreover, different associated
E. Montesinos-Berry
ArthroCentre - Agoriaz, Riaz and Clinique CIC
Riviera, Montreux, Switzerland
G. Ginovart
Department of Orthopaedic Surgery, Hospital Terres
de l’Ebre, Tortosa, Spain
D. Alastruey-López M. A. Perez
Instituto de Investigación en Ingeniería de Aragón
(I3A), Instituto de Investigación Sanitaria Aragón
(IIS Aragón), Multiscale in Mechanical and
Biological Engineering, University of Zaragoza,
Zaragoza, Spain
J. C. Monllau
Department of Orthopaedic Surgery, Hospital del
Mar, Barcelona, Spain
C. Ramirez-Fuentes
Medical Imaging Department, Hospital Universitario
y Politecnico La Fe, Valencia, Spain
Universitat Autònoma de Barcelona (UAB),
Barcelona, Spain
Catalan Institute of Traumatology and Sports
Medicine (ICATME), Hospital Universitari Dexeus,
Barcelona, Spain
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_55
705
706
V. Sanchis-Alfonso et al.
Fig. 1 Real finite element
A
model (FEM) (A, B) and
Parametric FEM (C, D) of the
PFJ
B
C
D
surgical gestures, for example, a trochleoplasty
can be added. This means that distinctly different
surgical simulations can be performed for each
patient. In this way, one can determine what the
best surgical approach for a specific patient is, at
least from the biomechanical point of view. The
objective of this chapter is to analyze the role of a
PM of the PFJ in evaluating MPFLr.
2
Parametric Model of the PFJ—
Our Protocol (See Video)
First, a reconstruction of the knee under study
using MIMICS software (MIMICS, Materialise NV, Leuven, Belgium) is made. Next, the
patella is isolated and its maximum mid-lateral
and proximal–distal length as well as its thickness are measured. In addition, the geometry of
the patella is also evaluated. That means the
shape of the patella. The PM is developed using
ABAQUS FEA, the model simulation software
(Abaqus/CAE v.6.14 software, Dassault
Systèmes, Suresnes, France). Initially, we simulate the patella as an elliptical disc. Subsequently,
the specific parameters of the patella that are
going to be analyzed (thickness and major and
minor diameters) are introduced. Then, different
cuts are made to give the patella the appropriate
shape to obtain a geometry that is like the
geometry of the patella that is going to be evaluated. Then, the patellar cartilage is created using
the geometry of the patella. A fixed thickness of
3 mm is assumed. The femur geometry is based
on four main elements: a revolution shape that
defines the bottom geometry, a solid loft for the
irregular section, a revolution shape in the posterior geometry and two revolution shapes that
represent the femoral epicondyles. Then, the
femoral cartilage consists of a revolution shape
for the bottom geometry and a combination of
elements that makes it possible to define the
upper region. Again, a fixed thickness of 3 mm is
assumed. Finally, the finite element mesh is
created (Fig. 2). Next, the same process is repeated with the femoral trochlea. If, for example,
Finite Element Technology in Evaluating …
707
the patient has grade D dysplasia in conformity
with the Dejour classification, it can be incorporated into the PM. In short, a PFJ like that of
the patient for whom we want to simulate surgery
is obtained. Besides the MPFLr, the model also
permits the simulation of other procedures done
in association with MPFLr like trochleoplasty.
An important parameter to consider in the
design of the model is the thickness of the cartilage because it can theoretically influence the
contact pressure. In the present case, as previously indicated, a uniform cartilage thickness of
3 mm is considered as it is widely accepted in the
specialized literature [3]. A prior sensitivity
analysis, making simulations with thicknesses of
2, 2.5, 3, 3.5 and 4 mm, showed that the cartilage
thickness did not significantly affect patellar
contact pressure, the differences being less than
0.005 MPa [1]. The cartilage is a multiphasic,
inhomogeneous and anisotropic structure. Due to
the computational costs and the time required to
perform modelling with 3D FE, the cartilage has
been considered a homogeneous and isotropic
material with linear elastic behavior from the
computational point of view [4–8]. Interstitial
fluid flow is not considered despite it being a
poroelastic material.
Once the bone structures (distal femur and
patella) and the femur and patellar cartilage have
been modelled, the ligaments (MPFL and lateral
retinaculum-LR-) and the tendons that surround
the patella (quadriceps and patellar tendons) are
Fig. 2 Parametric geometry of the four main parts of the
PFJ model: A Patellar cartilage; B patellar bone;
C femoral bone; D femoral cartilage; E geometric
parameters of the patellar bone; F geometric parameters
of the femoral bone (Reproduced from Sanchis-Alfonso
V, Alastruey-López D, Ginovart G, et al. Parametric finite
element model of medial patellofemoral ligament reconstruction model development and clinical validation.
J Exp Orthop. 2019; 6 (1), 32. © The Authors)
708
V. Sanchis-Alfonso et al.
Fig. 3 Final model reconstruction including the joint
ligaments and tendons. (Reproduced from SanchisAlfonso V, Ginovart G, Alastruey-López D, et al. Evaluation of patellar contact pressure changes after static
versus dynamic medial patellofemoral ligament reconstructions using a finite element model. J Clin Med. 2019;
8 (12), pii: E2093. © The authors)
introduced into the PM as beam elements
(Fig. 3). The LR ligament has the same position
in all the simulations. It is defined as a group of
six beam elements that connect the patella and
the femur through six of their nodes. The MPFL
is defined as a group of two beam elements that
connect the patella and the femur through two of
their nodes. The femoral insertion of this ligament is different for each reconstruction technique. The quadriceps tendon (QT) and patellar
tendon (PT) are modelled as a group of four and
two truss elements, respectively. The material
properties of these ligaments and tendons are
sourced from the specialized literature [9–11].
The inclusion of the patellar tendon and the
quadriceps tendon in the current model is crucial
for two reasons. The first reason is because its
presence helps stabilize the patella. If these tendons are not included in the model, it will cause
excessive rotation of the patella when tension is
applied to the ligaments. However, the rotational
movement of the patella upon applying tension to
the surrounding ligaments will be practically
non-existent when the tendons are present. The
second is because the presence of these two
tendons aids in making patellar contact pressure
distribution more uniform. In the FE models
designed for the study of the PFJ, emphasis is
placed on achieving an adequate orientation of
the quadriceps and patellar tendons. This
maneuver aims to prevent a valgus alignment
that would result in a lateral displacement of the
patella. From a mechanical point of view, valgus
alignment increases lateral pressure in the patella
due to the increase in the so-called Q angle. In
the present model, uniform pressure distribution
was achieved in the patella because the patellar
and the quadriceps tendon were introduced. It
ensures that there is no pathological valgus that
can skew the results obtained. All the structures
are in a situation of balance in our model.
One of the most complex points in this kind of
model with different parts (the patellar bone,
patellar cartilage, femoral cartilage and femoral
bone) is defining how all the parts interact. In this
study, bone (patella and femur) is considered a
rigid part. Therefore, its geometry remains nondeformable when loads and displacement are
applied. On the other hand, the cartilages are
deformable solids. When the interactions are
defined, it is necessary to assign a master or slave
behavior to each contact surface. Therefore, the
Finite Element Technology in Evaluating …
709
Fig. 4 Initial patellar cartilage contact pressure (MPa) (right)—Contact pressure after applying tension to the ligaments
(middle)—Relative contact pressure (left) (L = lateral; M = medial)
two main different interactions are patellar bone
with patellar cartilage and femoral bone with
femoral cartilage. The interactions are modelled
as a tie constraint between bone and cartilage (a
tie constraint implies the union of two regions
without regard to whether the meshes created on
their surfaces are similar or not). Patellar cartilage with femoral cartilage is modelled as a
surface-to-surface contact with a friction coefficient of 0.02.
We generate different models for each degree
of knee flexion [1]. The first thing is to draw the
patella to the femur to generate contact (initial
contact pressure). Then, the ligaments and tendons are brought into play. Next, tension is
slowly and progressively applied to the ligaments. Tension is applied according to the variation in graft length during knee flexion [12].
With this, the initial contact pressure is increased.
To this final contact pressure value, we subtract
the initial contact pressure. With that, we are
really evaluating the relative contact pressure
value (Fig. 4). Specifically, the pressures resulting from the incorporation of the MPFL to the
model are evaluated. This is the reason negative
pressures are found. In this way, different surgical
techniques can be compared under the very same
conditions. In a previous work, the changes in
graft length used to reconstruct the MPFL with
knee flexion were analyzed and it was shown to
differ in each type of MPFLr [12]. Particularly,
the static and the dynamic types of MPFLr were
analyzed in prior studies done by our group [1, 2].
3
The Clinical Problem—What is
Going to Happen with the PFJ
in the Long-Term After a MPFLr?
Currently, MPFLr is the procedure of first choice
for the treatment of patients with chronic lateral
patellar instability (CLPI). An MPFLr technique
is good when the clinical result is good, which is
when pain and instability disappear and no new
problems like patellofemoral chondropathy or
even patellofemoral osteoarthritis (PFOA)
develop over the long term. PFOA is the result of
an excessive increase in PFJ pressure due to an
inappropriate MPFLr. It has been shown that the
femoral attachment point in MPFLr is of utmost
importance for MPFL-graft length change during
710
knee flexion and relative graft length [12]. Both
factors influence the long-term success and failure rate of the MPFLr surgery [12]. Graft
overtensioning and/or non-anatomic positioning
of the femoral attachment point during MPFLr
increases PFJ contact pressures [13–15]. This
increment in PFJ contact pressure might lead to
joint degeneration [13, 16].
In the medical literature, there are many surgical MPFLr techniques published with different
fixation points and different types of grafts that
have shown good short-term clinical outcomes. It
seems like they are all good, but they certainly
are not. These techniques have noticeably short
follow-ups and have been evaluated only by
means of clinical tests that are not sensitive
enough to evaluate a surgical technique. MPFLr
assessment using FEM is more sensitive than
evaluations using only clinical or radiological
tools. FEM can demonstrate the validity of a
surgical technique in the long term since it
enables one to determine whether a specific
technique will lead to an increase in PFJ contact
pressure, which is closely related to the future
development of PFOA.
An important question arises here. What is
going to happen with the PFJ in these MPFL
reconstructions techniques in the long run? We
do not know. To respond to this question, we
could use the PM of the PFJ developed with
FEM technology using the computed tomography images (CTs) of patients with patellar
instability. Therefore, we would have those with
the specific anatomical characteristics of a knee
with a CLPI. This technology would give us the
ability to evaluate PFJ pressures after an MPFLr
in the entire range-of-motion of the knee (0120º). Additionally, we would be able to compare the new pressures with the ones found in a
normal knee with a native MPFL (gold standard).
This technology also provides the means to
determine the maximum stress of the MPFL graft
in all the knee flexion–extension positions. Our
evaluation tool makes it possible for us to compare the maximum stress of the graft with the
maximum stress of a native MPFL (gold standard). Our FE model of the PFJ predicts the
V. Sanchis-Alfonso et al.
stress distribution on the patellar cartilage and the
MPFL stresses in their different configurations,
depending on the different surgical techniques
that can be simulated. Therefore, our simulations
allow us to compare the different surgical techniques to evaluate a likely patellofemoral chondropathy or even PFOA in the long term.
4
Native MPFL Evaluation Using
FEM Technology. The Ideal MPFLr
from a Biomechanical Standpoint
In a native knee with an intact MPFL, the maximum patellar cartilage contact pressures are
0.18 MPa at 0º and 0.016 MPa at 30°. The
contact pressures at 60°, 90° and 120° are
exceptionally low compared to those at 0° and
30°. The maximum MPFL stress at 0° is
8.85 MPa and at 30° it is 0.78 MPa. At 60°, 90°
and 120°, the MPFL is loose. There is no tension.
Therefore, we should reproduce both the patellar
pressure and the graft tension behavior of a
native knee when doing an MPFLr. Nevertheless,
it is logical to think that we are risking a new
rupture if we perform the reconstruction with a
graft that has the same maximum stress as the
one that just tore. Therefore, we should use a
graft that is stronger than the native MPFL to
compensate for the anatomical factors predisposing to patellar dislocation. Those factors
include an increased tibial tuberosity-trochlear
groove (TTTG) distance, patella alta, femoral
anteversion, external tibial torsion and trochlear
dysplasia. However, it is especially important not
to increase the maximum MPFL-graft stress by
increasing the patellar contact pressure, because
it will result in an injury to the cartilage that
would eventually cause PFOA in the long term.
Patellar chondropathy is quite common in
patients with CLPI. Therefore, it is particularly
important not to increase the patellar contact
pressure at high degrees of knee flexion after an
MPFLr because it will aggravate the previous
chondropathy. This chondropathy could be
responsible for AKP after MPFLr. In short, an
ideal MPFLr technique must combine a perfect
Finite Element Technology in Evaluating …
A
B
711
C
Fig. 5 Static and anatomic MPFLr (A). MPFLr using the
AMT as a pulley (B). MPFLr using the quadriceps tendon
as soft attachment point (MQTFL reconstruction) (C).
(Reproduced from Sanchis-Alfonso V, Ginovart G,
Alastruey-López D, et al. Evaluation of patellar contact
pressure changes after static versus dynamic medial
patellofemoral ligament reconstructions using a finite
element model. J Clin Med. 2019; 8 (12), pii: E2093. ©
The authors)
balance between optimal patellar pressure and
maximum graft stress, making a new tear less
likely.
120° are very low. We must note that increased
patellofemoral contact pressure helps to stabilize
the patella. The objective would be not to exceed
the safety levels for pressure so as not to induce
patellofemoral chondropathy and finally PFOA.
The problem is that we do not know the safety
level for contact pressure in the PFJ. The maximum MPFL-graft stress at 0° and 30° is higher
than in a native knee. Moreover, as occurs in a
native knee, the MPFL-graft is loose at 60°, 90°
and 120°. It has no tension. Many orthopedic
surgeons recommend robust grafts to compensate
for predisposing anatomical factors for a dislocation. If we use an anatomical technique with a
semitendinosus autograft, the maximum patellar
contact pressures at 0° and 30° are a bit greater
than with using a gracilis autograft (Fig. 6).
However, the contact pressures at 60°, 90° and
120° are quite low. The maximum MPFL stress
at 0° and 30° is greater than when the gracilis is
used. At 60°, 90° and 120° the MPFL is loose. In
other words, the type of graft does matter, at least
from a biomechanical point of view.
In a number of cases, the static MPFLr is not
anatomic because of a surgical mistake. In these
cases, we can see two biomechanical patterns.
Firstly, there is a non-anatomic but physiometric
MPFLr. This type of reconstruction behaves
kinematically, like a native ligament [12]. The
clinical results of this type of reconstruction are
5
Analysis of the Types of MPFLr
Using FEM Technology
We have evaluated three types of fixation techniques: (1) Static and anatomic MPFLr in which
both graft attachments are fixed rigidly to the
bone; (2) Dynamic MPFLr using the adductor
magnus tendon (AMT) as a pulley and
(3) Dynamic MPFLr using the quadriceps tendon
as one of the attachment points, medial quadriceps tendon-femoral ligament (MQTFL) reconstruction (Fig. 5) [1, 2].
5.1 Static and Anatomic MPFLr—The
Type of Graft Does Matter
Currently, the most widespread surgical technique for MPFLr is the anatomical technique
using a gracilis tendon autograft with bone
anchoring in both the femur and patella. With
this type of reconstruction, the patellar contact
pressures at 0° and 30° are greater than in a
native knee (Fig. 6). Likewise, as occurs in a
native knee, the contact pressures at 60°, 90° and
712
Fig. 6 Contact pressure (MPa) on the patellar cartilage.
A Intact knee. B Anatomic MPFLr with a semitendinosus
autograft. C Anatomic MPFLr with a gracilis autograft.
D MPFLr with a semitendinosus autograft using the AMT
as a pulley. E MPFLr with a gracilis autograft using the
AMT as a pulley. F MQTFLr with a semitendinosus
autograft. G MQTFLr with a posterior tibial tendon
V. Sanchis-Alfonso et al.
allograft (M = Medial; L = Lateral). (Reproduced from
Sanchis-Alfonso V, Ginovart G, Alastruey-López D, et al.
Evaluation of patellar contact pressure changes after static
versus dynamic medial patellofemoral ligament reconstructions using a finite element model. J Clin Med. 2019;
8 (12), pii: E2093. © The authors)
Finite Element Technology in Evaluating …
good [12]. Second, we have a non-anatomic,
non-physiometric reconstruction. This type of
reconstruction behaves kinematically in a manner
opposite to that of a native ligament [12]. This
provokes high patellar contact pressures at
high degrees of knee flexion that can lead to
patellar chondropathy and finally PFOA. The
clinical results of this type of reconstruction are
quite bad [12].
5.2 Dynamic MPFLr
FEM validates using the AMT as a pulley in
MPFLr in our clinical practice [2]. From a
biomechanical point-of-view, it is a good technique. It does not increase patellar contact pressure when it is compared to the pressure in a
native MPFL. Moreover, the maximum MPFL
stress is like the native ligament. It is an
exceedingly good technique in cases without
severe predisposing factors to CLPI. Moreover,
FEM also validates MQTFL reconstruction in
our clinical practice [2]. From a biomechanical
perspective, it is an excellent technique. It does
not significantly increase patellar contact pressure when it is compared to the pressure in a
native MPFL. Moreover, the maximum ligament
stress is greater than that of the native ligament,
which could compensate for the anatomical factors predisposing to patellar dislocation. In the
MQTFLr, the posterior tibial allograft has a
greater stress to failure relative to a semitendinosus graft without increasing the patellar contact pressure [2]. In theory, a new tear is less
likely with a posterior tibial allograft.
5.3 Static Versus Dynamic MPFLr.
Clinical Relevance
The patellar contact pressures from 0° to 30° of
knee flexion after a dynamic MPFLr were like
those of the native knee, whereas the static and
anatomic reconstruction resulted in greater pressures. This may eventually increase the risk of
PFOA after a static MPFLr, at least from a
713
biomechanical standpoint, in the long term. In
the static and anatomic technique, the maximum
MPFL-graft stress at 0° and 30° was higher than
in a native MPFL. However, at 60°, 90°, and
120° the MPFL-graft was loose, that is, it had no
tension, like a native ligament. Then again, the
maximum stress of the MPFL-graft at 0° was less
than that of a native ligament in the dynamic
MPFLr using the AMT as a pulley. However, at
30°, the maximum MPFL-graft stress was significantly more than in a native ligament. After
30° of flexion, the MPFL-graft loosened, like a
native knee. In the dynamic MQTFL reconstruction, the maximum stress of the MPFL-graft
was much greater at 0° and 30° than that of a
native MPFL. After 30° of flexion, the MQTFL
graft also loosened as does the native knee.
The MPFLr using the AMT as a pulley is the
most common dynamic MPFLr technique in
current use [17–21] There are authors that have
evaluated the validity of this surgical technique
and found satisfactory clinical results in the
short-term follow-up. From a biomechanical
point of view, this is a good technique in cases
without severe predisposing factors to patellar
dislocation like severe trochlear dysplasia. Alm
and colleagues [19] found an elevated redislocation rate after MPFLr in children and adolescents with this surgical technique. The authors
concluded that this technique could only be
recommended in the absence of additional
patellofemoral maltracking, caused by an elevated tibial tuberosity-trochlear groove (TT-TG)
distance (>15 mm), patella alta, or especially
severe trochlear dysplasia. Monllau and colleagues obtained satisfactory results with this
technique, but it was associated with realignment
surgery in 56% of their cases [18]. This approach
might explain their satisfactory clinical results.
To obtain satisfactory results after an MPFLr
using the AMT as a pulley, the associated risk
factors for dislocation must be addressed during
surgery. Otherwise, this technique as an isolated
procedure should only be used in patients without severe trochlear dysplasia. Recently Marot
and colleagues [21] have published a multicenter
longitudinal prospective comparative study to
714
V. Sanchis-Alfonso et al.
compare the functional outcomes after an isolated MPFLr using either a quasi-anatomical
technique (elastic femoral fixation) or an
anatomical MPFLr. Patients with trochlear dysplasia types C and D were excluded from this
study. They concluded that an isolated quasianatomical MPFLr using a gracilis tendon autograft provides outcomes as good as the isolated
anatomical MPFLr at the 2.5-year follow-up in a
selected subgroup of patients with CLPI and with
no severe trochlear dysplasia.
MQTFLr described by Fulkerson and Edgar
[22] fulfills all the criteria for an ideal MPFLr,
biomechanically. It combines a perfect balance
between optimal patellar contact pressure and
maximum graft stress. While the MPFLr using
the AMT as an elastic femoral fixation is a nonanatomic technique, the soft tissue technique
using the quadriceps tendon as the soft tissue
fixation point is an anatomic technique as it
reconstructs the MQTFL. This technique also
shows good clinical results in the short term [22].
The question is which surgical technique is
better. Is it the static or dynamic? To definitively
answer this question, we must consider not only
biomechanical factors but also the number of redislocations with each technique as well as the
functional results as well as the ability to return
to sports practice. However, there are currently
no high-quality clinical studies that allow us to
conclusively answer this question. Well-designed
prospective studies with a substantial number of
patients and a longer follow-up are necessary to
allow us to answer this question.
6
Examples Demonstrating
the Good Correlation Between
Computational Predictions
and Clinical Evaluation
In the case of Fig. 7 (case #1), the computational
simulation projects high contact pressures at 60°,
90° and 120° of knee flexion compared with the
native knee. In theory, this will lead to patellar
chondropathy and finally AKP. In fact, our
patient had disabling AKP and severe patellar
chondropathy, as can be seen in the arthroscopic
image. Moreover, the MPFL is tense at 60°, 90°
and 120° of knee flexion and it is completely
loose at 0° and 30° of knee flexion in this case.
This tension pattern projects the presence of
lateral patellar instability as was seen upon
physical examination. This tension pattern is
typical of a non-anatomic and non-physiometric
MPFL reconstruction. In fact, in this case, we can
observe a very incorrect femoral attachment
point in the 3D-CT.
In the case of Fig. 8 (case # 2), the computational simulation projects remarkably high
contact pressures at 60°, 90° and 120°. In theory,
this will lead to PFOA. During revision surgery,
we observed an evident PFOA with exposed
bone in the medial facet of the patella. Indeed,
the maximum patellar contact pressure was in the
medial facet of the patella. This patient complained of disabling AKP. Moreover, the tension
pattern is typical of a non-anatomic and nonphysiometric MPFL reconstruction. You can
observe a very anterior and superior femoral
fixation point in the 3D-CT. Moreover, the tension pattern justifies the lateral patellar instability
that we can see during physical examination
(Fig. 8).
7
Clinical Relevance of FE
Technology—Discussion
FE technology shows that the native MPFL is
more tense during the first 30° of knee flexion,
and then loses a considerable amount of tension
with higher degrees of knee flexion [1]. After
30°, the ligament loosens and the patellofemoral
contact pressure, which also contributes somewhat to patellofemoral stability and is already
low during the first 30 degrees (0.23 MPa),
decreases considerably (0.0046 MPa) [1]. This
indicates, as shown by previous studies [23–25],
that the MPFL contribution to resisting lateral
patellar dislocation is greatest during the first 30
degrees of knee flexion. Precisely after 30° of
knee flexion, lateral patella stability depends
more on the femoral trochlea than on the MPFL.
The current tendency is to perform static
anatomic MPFL reconstructions. Sanchis-
Finite Element Technology in Evaluating …
715
TENSION PATTERN
Flexion Angle
Maximum MPFL Stress (MPa)
Maximum LR Stress (MPa)
60
90
120
59.03
119.2
252
1.62
5.38
7.06
Fig. 7 Case # 1. Surgical failure secondary to an anterior
femoral attachment point. Contact pressure (MPa) on the
patellar cartilage. L = lateral, M = medial (A). Parametric
model of this patient (B). Femoral attachment point is too
far anterior (black arrow) (C). Severe patellar chondropathy during arthroscopy (D). At 0° and 30° the ligament is
loose. There is no tension. (Reproduced from SanchisAlfonso V, Alastruey-López D, Ginovart G, et al. Parametric finite element model of medial patellofemoral
ligament reconstruction model development and clinical
validation. J Exp Orthop. 2019; 6 (1), 32.© The Authors)
Alfonso and colleagues [1] have demonstrated
that there is an increase in patellar contact pressure at 0° and 30° of knee flexion after a static
anatomic MPFLr (2.17 MPa at 0° and 0.14 MPa
at 30° when using the semitendinosus as a graft)
when compared to the pressure found in a nonoperated knee (0.18 MPa at 0° and 0.016 MPa at
30°). This leads us to consider the possible
deleterious long-term effects from slightly greater
patellar contact pressures. However, in theory,
the patellar contact pressures found in the static
anatomic MPFL reconstructions are not great
enough to cause symptomatic PFOA since they
are lower than those causing knee osteoarthritis
[26]. The objective would be not to exceed safe
levels of patellofemoral pressure so as not to
induce patellofemoral chondropathy and, ultimately, PFOA. It should also be remembered that
the increase in patellofemoral contact pressures
helps to stabilize the PFJ. Therefore, this factor
would be beneficial in the classic anatomic
reconstruction. Thus, a discrete increase in contact pressure, as we have observed, is desirable.
There is an ongoing debate about the exact
clinical consequences of a non-anatomical
MPFLr. There are only two papers that correlate the femoral fixation point with clinical
results of MPFLr surgery [12, 27]. Servien and
colleagues [27] found no negative effects on the
clinical results from a non-anatomical femoral
fixation point after a 2-year follow-up. A reason
for this might be that the femoral fixation point
was not so malpositioned from its ideal position
to have a negative effect. In our series, we have
only found clinical consequences with fixation
points that were too anterior. Another reason for
which Servien and colleagues justify the fact that
no correlation was found between the nonanatomical femoral fixation point and the clinical result is because of the short follow-up of
716
V. Sanchis-Alfonso et al.
TENSION PATTERN
Flexion Angle
Maximum MPFL Stress (MPa)
Maximum LR Stress (MPa)
60
90
120
19.51
29.52
34.70
4.56
7.54
8.37
Fig. 8 Case # 2. Surgical failure secondary to anterior
femoral attachment point. Contact pressure (MPa) on the
patellar cartilage. L = lateral, M = medial (A). Parametric
model of this patient (B). Femoral attachment point is too
far anterior (black arrow). Severe grade D trochlear
dysplasia according to the classification of Dejour (red
arrow) (C). Severe PFOA during arthrotomy (D). At 0°
and 30° of knee flexion, the ligament is loose. There is no
tension. (Reproduced from Sanchis-Alfonso V, AlastrueyLópez D, Ginovart G, et al. Parametric finite element
model of medial patellofemoral ligament reconstruction
model development and clinical validation. J Exp
Orthop. 2019; 6 (1), 32. © The Authors)
their patients (2 years). This is particularly relevant relative to the risk of developing PFOA.
Currently, what is being discussed is the precise
clinical consequences of from the physiological
point of view of the non-anatomical techniques
for the MPFLr in which the MPFL-graft behaves
like a native MPFL (physiometric behavior).
Servien and colleagues [27] and Sanchis-Alfonso
and colleagues [12] found no negative clinical
effects after 2 years when using these reconstructions, which could be due to the short
follow-up in both cases. In this type of reconstruction, the FEM shows an increase in patellofemoral contact pressure at 0° and 30° of knee
flexion in comparison to these pressures in the
native knee (2.77 MPa at 0° and 1.91 MPa at 30°
vs 0.18 MPa at 0° and 0.016 MPa at 30°). This
pressure increase mainly occurs on the medial
patellar facet. What is not known is whether this
increase in pressure results in chondropathy in
the long run and ultimately in symptomatic
PFOA. As far as we know, there is no study of
the PFJ that has determined the contact stress
threshold that is predictive of symptomatic
PFOA. In 2009, Segal and colleagues [26]
observed that a threshold of 3.42 to 3.61 MPa
had a 73.3% sensitivity with specificity ranging
from 46.7% to 66.7% for the prediction of
symptomatic knee osteoarthritis. Obviously,
these values cannot be extrapolated to the PFJ,
which is the joint with the thickest cartilage in
the human body. It is logical to think that the
pressures causing symptomatic PFOA would be
greater.
In
non-anatomical
MPFL
Finite Element Technology in Evaluating …
reconstructions, the maximum patellofemoral
contact pressures are on the order of 2.77 MPa,
values that are considerably below the cut-off
point mentioned above. Therefore, it is likely that
a non-anatomical but physiometric reconstruction would not have long-term negative effects
on the PFJ. Consequently, it would seem more
important for the ligament to be “physiometric”
rather than perfectly anatomical. With the FEM,
it is possible to predict which MPFLr has an
increased risk of severe patellofemoral chondropathy resulting in symptomatic PFOA and
requiring active treatment. In the cases in which
PFOA occurred, it was because the MPFL-graft
was loose, with knee flexion from 0° to 30°, and
was tense from 60° onward. In these cases, the
patellofemoral contact pressures were over
5 MPa from 60° onward, the femoral attachment
point being extremely non-anatomical (too far
anterior) and the MPFLr was not physiometric.
The predictive value of the parametric model of
the PFJ has made its clinical validation possible.
Our findings could have meaningful potential
implications for clinicians in terms of MPFLr
surgery. In theory, a healthy knee with a native
isometric MPFL during the knee’s entire rangeof-motion should have no negative repercussion
on the PFJ, since the native MPFL is not a robust
structure. A healthy PFJ shows no underlying
chondropathy. However, a degree of chondropathy of the medial facet of the patella is
frequently found in a knee with a chronic lateral
patellar instability. If, on top of this, we consider
that the graft we use to replace the MPFL is more
robust and rigid than the native MPFL, we could
expect that maintaining isometry during the
entire range-of-motion of the knee would produce greater patellofemoral compression in a
joint with a pre-existing medial patellar chondropathy, which would evidently worsen.
Therefore, it would be desirable to have ligament
isometry just from 0° to 30° in a knee with a
chronic lateral patellar instability. It is what
Thaunat and Erasmus [28] called a “favorable
anisometry.” With it, we would achieve our goal
717
of stabilizing the patella in the 0° to 30° range,
thusly avoiding the previously mentioned
problems.
Another interesting finding using FE technology is that the type of graft does matter, at
least from a biomechanical perspective. Our FE
parametric model study showed significant differences in terms of patellar contact pressure and
the maximum MPFL graft stress. For example,
the gracilis autograft has been recommended in
the MPFLr using the AMT as a pulley because
the gracilis tendon appears to be long and strong
enough to duplicate the MPFL function [18].
However, based on the results found using the
FE method, the semitendinosus tendon has
greater stress to failure relative to the gracilis
without significantly increasing the patellar contact pressure. In theory, a new tear is therefore
less likely with a semitendinosus tendon
autograft.
8
Take Home Messages
– The use of a parametric finite element model
of the PFJ enables us to evaluate different
types of surgical techniques for MPFLr relative to the effect on patellofemoral contact
pressure, the kinematic behaviour of the
MPFL-graft with knee flexion and the maximum MPFL-graft stress with knee flexion.
– The patellar contact pressures after dynamic
MPFL reconstructions are like those in the
intact situation. Therefore, a dynamic MPFLr
may be a safer option than a static reconstruction, reducing the chance of PFOA in the
long term.
– From diagnostic images like a CT, for
example, we can simulate different surgical
treatments and choose the most optimal
technique for each patient. That is, we can
customize treatment for individual patients.
– A PM of the PFJ is useful in predicting surgical outcomes and reducing complications
after MPFLr surgery.
718
References
1. Sanchis-Alfonso V, Alastruey-López D, Ginovart G,
et al. Parametric finite element model of medial
patellofemoral ligament reconstruction model development and clinical validation. J Exp Orthop. 2019;6
(1):32.
2. Sanchis-Alfonso V, Ginovart G, Alastruey-López D,
et al. Evaluation of patellar contact pressure changes
after static versus dynamic medial patellofemoral
ligament reconstructions using a finite element
model. J Clin Med. 2019;8(12):E2093.
3. Cohen ZA, Mow VC, Henry JH, et al. Templates of
the cartilage layers of the patellofemoral joint and
their use in the assessment of osteoarthritic cartilage
damage. Osteoarthritis Cartilage. 2003;11:569–79.
4. Klets O, Mononen ME, Tanska P, et al. Comparison
of different material models of articular cartilage in
3D computational modelling of the knee: data from
the Osteoarthritis Initiative (OAI). J Biomech.
2016;49:3891–900.
5. Yang NH, Nayeb-Hashemi H, Canavan PK, et al.
Effect of frontal plane tibiofemoral angle on the stress
and strain at the knee cartilage during the stance
phase of gait. J Orthop Res. 2010;28:1539–47.
6. Peña E, del Palomar AP, Calvo B, et al. Computational modelling of diarthrodial joints. Physiological,
pathological and post-surgery simulations. Arch
Comput Methods Eng. 2007;14:47–91.
7. Mononen M, Julkunen P, Töyräs J, et al. Alterations
in structure and properties of collagen network of
osteoarthritic and repaired cartilage modify knee joint
stresses.
Biomech
Model
Mechanobiol.
2011;10:357–69.
8. Donahue TLH, Hull M, Rashid MM, et al. A finite
element model of the human knee joint for the study
of tibio-femoral contact. J Biomech Eng.
2002;124:273–80.
9. Ciccone WJ II, Bratton DR, Weinstein DM, et al.
Viscoelasticity and temperature variations decrease
tension and stiffness of hamstring tendon grafts
following anterior cruciate ligament reconstruction.
J Bone Joint Surg Am. 2006;88:1071–8.
10. Drez DJr, Edwards TB, Williams CS. Results of
medial patellofemoral ligament reconstruction in the
treatment of patellar dislocation. Arthroscopy.
2001;17:298–306.
11. Elias JJ, Cosgarea AJ. Technical errors during medial
patellofemoral ligament reconstruction could overload medial patellofemoral cartilage: a computational
analysis. Am J Sports Med. 2006;34:1478–85.
12. Sanchis-Alfonso V, Ramirez-Fuentes C, MontesinosBerry E, et al. Femoral insertion site of the graft used
to replace the medial patellofemoral ligament influences the ligament dynamic changes during knee
flexion and the clinical outcome. Knee Surg Sports
Traumatol Arthrosc. 2017;25:2433–41.
V. Sanchis-Alfonso et al.
13. Stephen JM, Kaider D, Lumpaopong P, et al. The
effect of femoral tunnel position and graft tension on
patellar contact mechanics and kinematics after
medial patellofemoral ligament reconstruction.
Am J Sports Med. 2014;42:364–72.
14. Stephen JM, Kittl C, Williams A, et al. Effect of
medial patellofemoral ligament reconstruction
method on patellofemoral contact pressures and
kinematics. Am J Sports Med. 2016;44:1186–94.
15. Elias JJ, Kelly MJ, Smith KE, et al. Dynamic
simulation of the effects of graft fixation errors
during medial patellofemoral ligament reconstruction. Orthop J Sports Med. 2016;4(9):232596711
6665080.
16. Rood A, Hannink G, Lenting A, et al. Patellofemoral
pressure changes after static and dynamic medial
patellofemoral ligament reconstructions. Am J Sports
Med. 2015;43:2538–44.
17. Arendt EA. MPFL reconstruction: the adductor sling
approach. In: Dejour D, Arendt EA, editors. Patellofemoral Pain, Instability, and Arthritis; In: Zafagnini S.
Berlin, Germany: Springer; 2010. p. 175–9.
18. Monllau JC, Masferrer-Pino A, Ginovart G, et al.
Clinical and radiological outcomes after a quasianatomical reconstruction of medial patellofemoral
ligament with gracilis tendon autograft. Knee Surg
Sports Traumatol Arthrosc. 2017;25:2453–9.
19. Alm L, Krause M, Mull C, et al. Modified adductor
sling technique: a surgical therapy for patellar
instability in skeletally immature patients. Knee.
2017;24:1282–8.
20. Lind M, Enderlein D, Nielsen T, et al. Clinical
outcome after reconstruction of the medial patellofemoral ligament in paediatric patients with recurrent
patella instability. Knee Surg Sports Traumatol
Arthrosc. 2016;24:666–761.
21. Marot V, Sanchis-Alfonso V, Perelli S, et al. Isolated
reconstruction of medial patellofemoral ligament
with an elastic femoral fixation leads to excellent
clinical results. Knee Surg Sports Traumatol
Arthrosc. 2021;29(3):800–5.
22. Fulkerson JP, Edgar C. Medial quadriceps tendonfemoral ligament: Surgical anatomy and reconstruction echnique to prevent patella instability. Arthrosc
Tech. 2013;12:e125–8.
23. Conlan T, Garth WP Jr, Lemons JE. Evaluation of
the medial soft-tissue restraint of the extensor
mechanism of the knee. J Bone Joint Surg Am.
1993;75:682–93.
24. Desio SM, Burks RT, Bachus KN. Soft tissue
restraints to lateral patellar translation in the human
knee. Am J Sports Med. 1998;26:59–65.
25. Hautamaa PV, Fithian DC, Kaufman KR, et al.
Medial soft tissue restraints in lateral patellar instability and repair. Clin Orthop Relat Res.
1998;349:174–82.
26. Segal NA, Anderson DD, Iyer KS. Baseline articular
contact stress levels predict incident symptomatic
Finite Element Technology in Evaluating …
knee osteoarthritis development in the MOST cohort.
J Orthop Res. 2009;27:1562–8.
27. Servien E, Fritsch B, Lustig S. In vivo positioning
analysis of medial patellofemoral ligament reconstruction. Am J Sports Med. 2011;39:134–9.
719
28. Thaunat M, Erasmus PJ. The favourable anisometry:
an original concept for medial patellofemoral ligament reconstruction. Knee. 2007;14:424–8.
Biomechanical Analysis
of the Influence of Trochlear
Dysplasia on Patellar Tracking
and Pressure Applied to Cartilage
John J. Elias
1
Trochlear Dysplasia
During normal knee function, the patella has
limited engagement with the trochlear groove
with the knee extended, and becomes captured
by the trochlear groove as the knee flexes to 30°.
The patellar ridge is typically aligned with the
deepest part of the trochlear groove during
function. The resultant force applied to the
patella by the quadriceps muscles and patellar
tendon has a lateral component, and the lateral
ridge of the trochlear groove provides an articular
restraint to resist lateral patellar translation and
maltracking.
Trochlear dysplasia is characterized by a
shallow trochlear groove providing limited
articular constraints to resist lateral forces applied
to the patella (Fig. 1). Supratrochlear spurs are
also associated with trochlear dysplasia. Supratrochlear spurs refer to a protrusion of the femur
at the proximal edge of the trochlear groove that
can interfere with smooth entry of the patella into
the groove. The groove can also extend more
proximally than normal, which can induce
interaction of the patella with the groove earlier
in knee flexion [1].
J. J. Elias (&)
Department of Health Sciences, Cleveland Clinic
Akron General, 1 Akron General Ave, Akron, OH
44302, USA
e-mail: eliasj@ccf.org
Several measurement systems have been
described to characterize anatomy of the trochlear groove. Lateral trochlear inclination and
sulcus angle are commonly used to quantify
depth of the trochlear groove. These measurements are based on axial slices from MRI or CT
scans. Lateral trochlear inclination is quantified
as the angle between a line along the lateral ridge
of the trochlear groove and a line representing
the posterior condylar axis of the femur, and
increases with trochlear depth (Fig. 2). Sulcus
angle is quantified as the angle between lines
representing the medial and lateral ridges of the
trochlear groove and decreases with trochlear
depth. Trochlear dysplasia is also evaluated
based on the Dejour classification system,
including trochlear shape and prominence of a
supratrochlear spur [2]. Dejour classification is
determined from a lateral knee radiograph, along
with axial CT or MRI imaging. A crossing sign is
characterized by a curve along the deepest points
of the trochlear groove crossing the anterior
border of the femoral condyles, indicating a
shallow proximal groove.
Trochlear dysplasia is a primary anatomical
feature of lateral patellar instability. Trochlear
dysplasia has been identified in more than 60%
of knees that have experienced a lateral patellar
dislocation [3, 4]. While other anatomical features of patellar instability have been identified,
such as patella alta and a lateral position of the
tibial tuberosity, trochlear dysplasia has been
consistently identified as a primary contributing
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_56
721
722
Fig. 1 A computational model representing a knee with
trochlear dysplasia in the pre-operative condition and
following groove-deepening trochleoplasty with removal
of the supratrochlear spur. (Adapted with permission from
Elias JJ et al. Groove-deepening trochleoplasty reduces
lateral patellar maltracking and increases patellofemoral
contact pressures: Dynamic simulation. J Orthop Res.
2021 Sep 24. https://doi.org/10.1002/jor.25181)
J. J. Elias
factor to initial patellar dislocations [3], dislocations following conservative treatment [5], and
dislocations following surgical patellar stabilization [6–8].
Trochlear dysplasia, along with lateral patellar
maltracking, also influences patellofemoral contact during function. Abnormal patellofemoral
contact patterns can be related to degradation of
patellofemoral cartilage. Trochlear dysplasia has
been related to cartilage lesions associated with
osteoarthritis (OA) [9] and shown to increase the
risk of patellofemoral OA following patellar
dislocation [10].
Trochlear shape can be surgically modified.
Of the numerous surgical options available for
patellar stabilization, trochleoplasty is the
approach that directly addresses the constraint
provided by the lateral ridge of the trochlear
groove [11, 12]. The most common form is a
groove-deepening trochleoplasty to address a flat
or laterally convex trochlear groove [13, 14]
(Fig. 1). The approach includes deepening and
realigning the subchondral bone with the articular surface pressed into the gap. Groove deepening trochleoplasty has been shown to increase
the average lateral trochlear inclination from 3°
to 23° at the proximal groove and from 15° to
27° at the distal groove [15]. The deepest part of
the groove is also typically lateralized by an
average of 6 mm. A supratrochlear spur is also a
characteristic of trochlear dysplasia, and is
commonly flattened as part of groove-deepening
trochleoplasty [16, 17].
2
Fig. 2 An axial view of the knee showing measurements
used to characterize trochlear depth (lateral trochlear
inclination, sulcus angle) and patellar tracking (bisect
offset index, lateral tilt)
Biomechanical Analysis
Numerous biomechanical studies have been
performed to characterize how trochlear dysplasia influences knee function. Characterization
of knee function has primarily focused on lateral
patellar tracking during daily function or patellar
stability in response to a laterally directed force.
Some studies have included characterization of
Biomechanical Analysis of the Influence of Trochlear Dysplasia …
contact pressure applied to patellofemoral cartilage. Most biomechanical studies have focused
on trochlear depth as an anatomical factor
influencing function. A few have represented
trochleoplasty as a surgical option to correct
trochlear dysplasia.
Three primary techniques are used for
biomechanical analysis of trochlear dysplasia.
Mechanical rigs are commonly used to simulate
function with cadaveric knees. Due to limited
access to dysplastic knees, knees with normal
anatomy are manipulated to represent trochlear
dysplasia. The relationship between trochlear
anatomy and patellar tracking is also commonly
evaluated in patients being treated for patellofemoral disorders. Patellar tracking is quantified
based on diagnostic imaging with the knee at
multiple positions of flexion. To induce quadriceps activation, resistance is applied at the foot
with a loading rig or an unsupported leg is elevated against gravity. Computational simulation
models are also used to evaluate the influence of
trochlear groove anatomy on patellofemoral
function. Computational simulation allows controlled variation in anatomy like the in vitro
studies, and also allows representation of pathological conditions that commonly accompany
trochlear dysplasia.
Fig. 3 Schematic
representation of a knee
attached to an in vitro testing
frame to simulate knee
function. (Adapted from
Elias JJ et al. Computational
assessment of the influence of
vastus medialis obliquus
function on patellofemoral
pressures: model evaluation.
J Biomech. 2010;43:612–7.
https://doi.org/10.1016/j.
jbiomech.2009.10.039)
723
2.1 In Vitro Simulation of Knee
Function
In vitro simulation represents knee function with
cadaveric knees engaged with a mechanical
simulator to induce motion (Fig. 3). The cadaveric knees are manipulated to vary the shape of
the trochlear groove from normal to shallow. The
advantages of in vitro simulation include controlled variation of patellofemoral anatomy,
application of sensors to characterize patellofemoral kinematics, and control of applied muscle
forces. Limitations include representation of a
limited number of soft tissues and muscle forces,
compromised strength of cadaveric tissues, and
utilization of old knees to represent young subjects who are treated for patellar instability.
Although the specimens can be manipulated to
represent a shallow groove, the corresponding
shape of the patella is not consistently represented. Other forms of pathologic anatomy, such
as a lateral position of the patellar tendon and
patella alta are also not consistently represented.
Several studies focused on the influence of
trochlear dysplasia on patellar tracking with
muscle forces applied at multiple positions of
knee flexion. One study manipulated the native
trochlear groove to elevate the central anterior
724
trochlea to simulate dysplasia [18]. The study did
not find a significant change in patellar kinematics related to representation of trochlear
dysplasia. One study modeled a shallow trochlear
groove and the corresponding change in the
shape of the patella to represent trochlear dysplasia [19]. Articular surfaces of the patella and
femur were replaced with 3D printed components to represent normal anatomy, Dejour type
A trochlear dysplasia, and Dejour type B trochlear dysplasia. This study also did not find a
variation in patellar kinematics related to trochlear dysplasia. Another study also used 3D
printed components to represent a normal trochlear groove with Dejour types A through D
included in representation of trochlear dysplasia
[20]. The study represented two types of knee
motion: knee squatting and open chain extension.
For knee squatting over a range from 35° to 75°,
patellar internal rotation and lateral tilt were
larger for representation of trochlear dysplasia
than for a normal trochlear groove. For knee
extension over a range from 5° to 65°, patellar
internal rotation, lateral tilt and lateral shift were
larger for the trochlear dysplasia group than for
representation of a normal trochlear groove.
Overall, these studies indicate the influence of
trochlear dysplasia on patellofemoral kinematics
is limited, primarily noted for patellar rotation
and tilt, with lateral shift also noted for representation of knee extension.
Some studies focused particularly on patellar
stability related to trochlear dysplasia. For a
study that manipulated the trochlear groove to
represent trochlear dysplasia, the lateral force
required to shift the patella laterally decreased by
approximately 50% with the knee at 30° of
flexion, with smaller significant differences at
lower and higher flexion angles [18]. Similar
results were obtained for another study that
quantified the translation in response to a 100 N
lateral force [20]. Another study that also
manipulated the trochlear groove to represent
trochlear dysplasia similarly showed that representation of trochlear dysplasia decreased the
force required to laterally displace the patella
despite representation of reconstruction of the
MPFL [21]. These studies show that trochlear
J. J. Elias
dysplasia limits patellar stability in response to a
direct lateral force acting on the patella.
Groove-deepening trochleoplasty has also
been represented with cadaveric knees to determine the influence on patellar tracking and stability. Trochleoplasty was shown to restore the
force needed to translate the patella 10 mm laterally to approximate the stability of a normal
knee [18]. For patellar tracking with simulated
muscle forces, however, position of the patella
was unexpectedly more lateral following
trochleoplasty than for the dysplastic condition.
Some studies included pressure sensors to
characterize patellofemoral contact pressures.
Two studies measured contact pressures while
using 3D printed surfaces to represent trochlear
dysplasia. One study showed that trochlear dysplasia tended to shift patellofemoral contact forces from the medial facet of the patella to the
lateral facet from 50°–70° of knee flexion, but
the contact forces did not increase [19]. This
study included variation in patellar shape while
representing trochlear dysplasia. The other
showed that trochlear dysplasia tended to
decrease contact area and increase contact pressures, with the highest contact pressures noted
for Dejour types B and D [20]. The changes were
largest with the knee flexed for knee squatting
and the knee extended for knee extension. This
study did not vary the shape of the patella as the
trochlear shape changed. Another study showed
that anterior osteotomy of the lateral femoral
condyle to deepen the trochlear groove increased
patellofemoral contact pressures [22]. The
cadaveric specimens used to deepen the trochlear
groove were not dysplastic. Overall these studies
seem to indicate that trochlear dysplasia influences the distribution of patellofemoral contact
forces, but the primary factor that increases
contact forces is altering the normal congruence
between the patella and trochlear groove.
2.2 Functional Imaging
Functional imaging characterizes patellar tracking and pathologic anatomy for patients being
treated for patellar instability. Functional
Biomechanical Analysis of the Influence of Trochlear Dysplasia …
imaging addresses several limitations of in vitro
simulation. Functional imaging focused on
patients being treated for patellofemoral disorders includes representation of pathologic anatomy, including trochlear dysplasia. Other forms
of pathologic anatomy, including patella alta and
a lateral position of the tibial tuberosity are also
included. In vivo motion of the knee is also
evaluated, without approximating muscle forces
or orientations. Functional imaging studies are
limited by the activities that can be performed by
patients within a diagnostic scanner. Also, anatomy cannot be controlled, so studies rely on
variations between subjects to relate anatomy to
patellar tracking. Functional imaging studies
have been based on dynamic CT, dynamic MRI,
and static MRI at multiple flexion angles. Knee
motion has been represented by knee extension
against gravity or an MRI-compatible load frame
has been used to apply resistance to knee
extension at the foot.
For functional imaging, trochlear dysplasia is
characterized by a measure of trochlear depth
determined from anatomical landmarks. The
studies also typically utilize measures of patellar
tracking characterized from anatomical landmarks. The most common measures used to
characterize trochlear depth are lateral trochlear
inclination and sulcus angle. The two primary
parameters of patellar tracking are bisect offset
index and patellar tilt (Fig. 2). Bisect offset index
characterizes patellar tracking with respect to the
trochlear groove. Bisect offset index is measured
as the portion medial/lateral width of the patella
lateral to the deepest part of the trochlear groove,
measured in an axial plane at each position of
knee flexion. The patella tends to be in the most
lateral position with the knee extended, particularly for patients being treated for patellofemoral
disorders. The average bisect offset index with
the knee extended is 0.55 to 0.6 for healthy knees
[23]. A bisect offset index of 0.75 is considered a
cut-off between normal patellar tracking and
maltracking [24]. Patellar tilt is measured as the
angle between the medial/lateral axis of the
patella and the posterior condylar axis. Patellar
tilt on the order of 15° or higher is considered
maltracking [25].
725
Some functional imaging studies create computational models for 3D representation of the
knee rather than identifying anatomical landmarks directly on slices from the acquired
imaging [26–28]. A 3D model of the knee,
including bones, cartilage surfaces and ligament
attachments, is created from a high resolution
MRI scan performed with the knee extended and
unloaded. Computational models of the bones
are also created from imaging performed with the
knee at multiple flexion angles. One computational representation of the knee is developed
including bones, cartilage, relevant soft tissue
attachments, fixed anatomical landmarks, and
reference axes. Shape matching techniques are
used to align the model with the landmarks and
reference axes to the bones at each position of
knee flexion to represent each position of knee
flexion with a consistent set of landmarks and
axes. This approach eliminates potential error
related to repeated identification of landmarks.
The reference axes are used to measure patellofemoral and tibiofemoral kinematics, while the
landmarks are used to characterize trochlear
depth and patellar tracking.
For patients being treated for patellar dislocations, multiple studies have shown that lateral
patellar maltracking is correlated with a shallow
trochlear groove. The relationships between
patellar tracking and trochlear depth were primarily observed with the knee at low flexion
angles [26–28]. The studies also showed that the
strongest relationships were established between
trochlear depth and patellar tilt. For the most
recent study, with the knee at full extension,
lateral trochlear inclination accounted for 46% of
the variation in bisect offset index and 60% of the
variation in patellar tilt [26]. For the vast majority
of patients, bisect offset index and patellar tilt
with the knee extended would be considered
lateral maltracking. The study further showed
that the influence of trochlear depth on patellar
tracking was particularly prominent for knees
without patella alta (Caton-Deschamps index <
1.2). In absence of patella alta, the patella is
engaged with the trochlear groove at low flexion
angles, so the depth of the trochlear groove plays
a large role in resisting lateral forces applied to
726
J. J. Elias
Fig. 4 Patellar tracking with the knee extended determined by functional imaging for two knees without
patella alta. A shallow trochlear groove results in lateral
maltracking while a deep trochlear groove provides
normal patellar tracking. (Adapted with permission from
Conry et al. Influence of tibial tuberosity position and
trochlear depth on patellar tracking in patellar instability:
Variations with Patella Alta. Clin Biomech.
2021;87:105,406. https://doi.org/10.1016/j.clinbiomech.
2021.105406)
the patella (Fig. 4). For these subjects, lateral
trochlear inclination accounted for 84% of the
variation in bisect offset index between subjects.
Studies focused on healthy control subject and
subjects with patellofemoral pain have also
identified relationships between lateral patellar
tracking and a shallow trochlear groove. A study
including subjects with and without patellofemoral pain found similar correlations between
sulcus angle and both bisect offset index and
patellar tilt at low flexion angles [29]. For this
study, bisect offset index and patellar tilt would
be considered lateral maltracking for a small
minority of the subjects. The influence of sulcus
angle on lateral patellar tracking was strongest
with the knee at full extension, and generally
stronger for patellar tilt than patellar shift. The
results were similar for another study focused on
healthy subjects and patients with patellofemoral
pain [30]. The study used measurements of
patellar lateral shift and tilt from six degree of
freedom kinematics. For healthy control subjects
and subjects characterized as lateral maltrackers,
lateral trochlear inclination was significantly
correlated with lateral patellar shift and tilt near
full extension, with the relationships strongest for
patellar tilt.
Overall, these studies indicate that lateral
patellar tracking increases as the depth of the
trochlear groove decreases for healthy knees and
knees being treated for patellofemoral pain and
patellar instability. These relationships are
observed with the knee at low flexion angles. The
relationship between a shallow trochlear groove
and patellar tracking is stronger for patellar tilt
than patellar shift due to the lateral facet of the
patella articulating along the lateral ridge of the
trochlear groove. The relationships can also be
influenced by other parameters, such as being
stronger for knees with normal patella height,
with the patella engaging the trochlear groove at
low flexion angles.
2.3 Dynamic Simulation of Knee
Function
For dynamic simulation of knee function, computational models are also used to characterize
the relationship between patellar tracking and
trochlear depth, but the motion is simulated
based on finite element analysis or multibody
dynamic simulation. Dynamic simulation models
can be made to represent patients being treated
Biomechanical Analysis of the Influence of Trochlear Dysplasia …
Fig. 5 Computational model for dynamic simulation of
knee function. The model is used to simulate a dual limb
knee squat and is shown with the knee extended and at
50° of flexion. (Reprinted with permission from Elias
et al. Allowing one quadrant of patellar lateral translation
during medial patellofemoral ligament reconstruction
successfully limits maltracking without overconstraining
the patella. Knee Surg Sports Traumatol Arthrosc.
2018;26:2883–2890. https://doi.org/10.1007/s00167-0174799-9)
for patellar instability to incorporate realistic
pathologic anatomy (Fig. 5). Models can also be
manipulated to vary the depth of the trochlear
groove for individual subjects. Patellofemoral
kinematics and patellar tracking can be quantified
during the simulated motions. Computational
models characterize reaction forces at the trochlear groove to drive patellofemoral motion.
Patellofemoral contact pressures can be quantified based on the reaction forces. Computational
models also allow representation of functional
activities that patients cannot perform within a
diagnostic scanner, incorporating higher muscle
forces and deeper flexion angles. The primary
limitation of dynamic simulation is that output
data depends on mathematical representation of
interactions between tissues and approximations
of muscle forces and tissue properties. Rigorous
validation of simulation models against data from
in vitro simulation of function or functional
727
imaging should be performed to characterize
accuracy of the simulated motion and loads
applied to cartilage.
Computational simulation studies have indicated that a shallow trochlear groove contributes
to lateral patellar maltracking and reduces patellar stability. One study simulated knee squatting
and knee extension as the depth of the trochlear
groove was manipulated [31]. Lateral trochlear
inclination was varied to represent a normal
value (24°), borderline trochlear dysplasia (12°),
and trochlear dysplasia (6°). During simulated
knee extension, with the knee fully extended the
average bisect offset values were 0.86 for a
normal groove, 0.95 for borderline trochlear
dysplasia, and 1.02 for trochlear dysplasia. For
knee squatting, with the patella entering the trochlear groove at 15°, the average bisect offset
index values were 0.57 for a normal groove, 0.64
for borderline dysplasia and 0.71 for trochlear
dysplasia. Further, with representation of trochlear dysplasia, the peak bisect offset index
during knee squatting was highly correlated with
lateral position of the tibial tuberosity (r2 = 0.81,
p = 0.006). Another computational study characterized patellar stability in response to a lateral
force applied directly to the patella with models
representing healthy knees and knees with trochlear dysplasia [32]. The force required to displace the patella laterally by 10 mm was
approximately 30% larger for healthy knees than
dysplastic knees with the knee at full extension,
with the percentage change increasing as the
knee was flexed.
Simulation studies have indicated that
trochleoplasty improves patellar constraint
applied by the trochlear groove, but with an
adverse influence on patellofemoral contact
pressures. One simulation study represented
knees with trochlear dysplasia and characterized
the influence of groove-deepening trochleoplasty
on the force needed to displace the patella laterally [32]. Trochleoplasty had minimal influence on patellar stability with the knee fully
extended but restored stability similar to healthy
knees with the knee flexed. A dynamic simulation study represented groove-deepening
trochleoplasty performed to stabilize the patella,
728
and characterized the influence on patellar
tracking and pressure applied to patellar cartilage
[33]. The study was based on computational
models representing patients treated for patellar
instability with trochlear dysplasia categorized as
Dejour type B or D. For all knees, the trochlear
groove was manipulated to increase the lateral
trochlear inclination to 23° at the proximal trochlear groove and 27° at the distal groove.
Trochleoplasty significantly decreased lateral
patellar tracking, particularly at low knee flexion
angles. For simulated knee squatting, trochleoplasty decreased average bisect offset index with
the knee extended from 0.87 to 0.75, representing a change from lateral maltracking to borderline
normal patellar tracking [24].
Trochleoplasty also significantly decreased contact area and increased the maximum contact
pressure at multiple flexion angles. Trochleoplasty decreased the average contact area by
approximately 10% in mid-flexion, with a corresponding increase in the average maximum
contact pressure of 13% to 23%. Decreased
contact area and increased contact pressures were
related to altered patellofemoral congruity due to
reshaping the femur without a corresponding
change to the patella.
The simulation studies show that trochlear
dysplasia compromises the ability of the trochlear groove to constrain the patella. For lateral
forces directly applied to the patella and simulated knee motion, the patella is in a more lateral
position for knees with trochlear dysplasia,
placing the knee at risk of lateral patellar dislocation. A lateral position of the tibial tuberosity
amplifies the influence of trochlear dysplasia on
patellar tracking. Trochleoplasty to increase the
depth of the trochlear groove helps to restore
patellar stability, although the benefit is limited
with the knee fully extended and the patella not
captured by the trochlear groove. Trochleoplasty
does alter patellofemoral congruity, however,
which tends to elevate patellofemoral contact
pressures during function.
J. J. Elias
3
Discussion
Trochlear dysplasia is associated with a shallow
trochlear groove that limits articular resistance to
the lateral force applied to the patella by the
quadriceps muscles and patellar tendon, particularly with the knee extended. Although not consistently identified with in vitro studies,
functional imaging and computational simulation
indicate that limited articular resistance results in
lateral patellar tracking during normal function,
with the level of patellar tracking with the knee
extended considered maltracking that can contribute to patellar dislocations. Patellar stability in
response to a direct lateral force applied to the
patella is also compromised for knees with trochlear dysplasia. Trochlear dysplasia acts in
combination with other types of pathologic
anatomy to influence patellar tracking. Lateral
position of the tibial tuberosity influences patellar
tracking in combination with trochlear dysplasia.
Combination of a large lateral force applied to the
patella by the patellar tendon and quadriceps and
limited articular constraint is particularly problematic for maintaining patellar stability. Trochlear dysplasia has a greater impact on patellar
tracking for knees with normal patellar height
than patella alta due engagement of the patella
with the trochlear groove at lower flexion angles.
Lateral patellar maltracking and pathologic
shape of the patella and femur associated with
trochlear dysplasia do not necessarily increase the
pressure applied to patellofemoral cartilage during stable functional activities. Dynamic activities
that potentially induce instability may be associated with low contact area and elevated contact
pressures for patients with trochlear dysplasia.
Studies that included measurement of contact
pressures generally showed that any change that
alters natural patellofemoral congruity increases
pressure applied to patellofemoral cartilage when
the patella is captured by the trochlear groove.
Potential for elevated post-operative contact
pressures should be considered when performing
a groove-deepening trochleoplasty.
Biomechanical Analysis of the Influence of Trochlear Dysplasia …
References
1. Van Haver A, Mahieu P, Claessens T, Li H, Pattyn C,
Verdonk P, et al. A statistical shape model of
trochlear dysplasia of the knee. Knee. 2014;21:518–
23. https://doi.org/10.1016/j.knee.2013.11.016.
2. Dejour D, Le Coultre B. Osteotomies in patellofemoral instabilities. Sports Med Arthrosc Rev.
2007;15:39–46. https://doi.org/10.1097/JSA.0b013e
31803035ae.
3. Arendt EA, England K, Agel J, Tompkins MA. An
analysis of knee anatomic imaging factors associated
with primary lateral patellar dislocations. Knee Surg
Sport Traumatol Arthrosc. 2017;25:3099–107.
https://doi.org/10.1007/s00167-016-4117-y.
4. Nelitz M, Lippacher S, Reichel H, Dornacher D.
Evaluation of trochlear dysplasia using MRI: correlation between the classification system of Dejour
and objective parameters of trochlear dysplasia. Knee
Surg Sport Traumatol Arthrosc. 2014;22:120–7.
https://doi.org/10.1007/s00167-012-2321-y.
5. Huntington LS, Webster KE, Devitt BM, Scanlon JP,
Feller JA. Factors associated with an increased risk of
recurrence after a first-time patellar dislocation: a
systematic review and meta-analysis. Am J Sports
Med. 2020;48:2552–2562. https://doi.org/10.1177/
0363546519888467.
6. Nelitz M, Theile M, Dornacher D, Wölfle J,
Reichel H, Lippacher S. Analysis of failed surgery
for patellar instability in children with open growth
plates. Knee Surg Sport Traumatol Arthrosc.
2012;20:822–8. https://doi.org/10.1007/s00167-0111599-5.
7. Hopper GP, Leach WJ, Rooney BP, Walker CR,
Blyth MJ. Does degree of trochlear dysplasia and
position of femoral tunnel influence outcome after
medial patellofemoral ligament reconstruction? Am J
Sports Med. 2014;42:716–22. https://doi.org/10.
1177/0363546513518413.
8. Feucht MJ, Mehl J, Forkel P, Achtnich A, Schmitt A,
Izadpanah K, et al. Failure analysis in patients with
patellar redislocation after primary isolated medial
patellofemoral ligament reconstruction. Orthop J
Sport Med. 2020;8:1–10. https://doi.org/10.1177/
2325967120926178.
9. Stefanik JJ, Roemer FW, Zumwalt AC, Zhu Y,
Gross KD, Lynch JA, et al. Association between
measures of trochlear morphology and structural
features of patellofemoral joint osteoarthritis on MRI:
the MOST study. J Orthop Res. 2012;30:1–8. https://
doi.org/10.1002/jor.21486.
10. Sanders TL, Pareek A, Johnson NR, Stuart MJ,
Dahm DL, Krych AJ. Patellofemoral arthritis after
lateral patellar dislocation: a matched populationbased analysis. Am J Sports Med. 2017;45:1012–7.
https://doi.org/10.1177/0363546516680604.
11. Liu JN, Steinhaus ME, Kalbian IL, Post WR,
Green DW, Strickland SM, et al. Patellar instability
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
729
management: a survey of the international patellofemoral study group. Am J Sports Med. 2018;46:3299–
306. https://doi.org/10.1177/0363546517732045.
van Sambeeck JDP, van de Groes SAW, Verdonschot N, Hannink G. Trochleoplasty procedures
show complication rates similar to other patellarstabilizing procedures. Knee Surg Sport Traumatol
Arthrosc. 2018;26:2841–57. https://doi.org/10.1007/
s00167-017-4766-5.
Longo UG, Vincenzo C, Mannering N, Ciuffreda M,
Salvatore G, Berton A, et al. Trochleoplasty techniques provide good clinical results in patients with
trochlear dysplasia. Knee Surg Sport Traumatol
Arthrosc. 2018;26:2640–58. https://doi.org/10.1007/
s00167-017-4584-9.
Weber AE, Nathani A, Dines JS, Allen AA, ShubinStein BE, Arendt EA, et al. An algorithmic approach
to the management of recurrent lateral patellar
dislocation. J Bone Jt Surg Am. 2016;98:417–27.
https://doi.org/10.2106/JBJS.O.00354.
Fucentese SF, Schöttle PB, Pfirrmann CWA,
Romero J. CT changes after trochleoplasty for
symptomatic trochlear dysplasia. Knee Surg Sport
Traumatol Arthrosc. 2007;15:168–74. https://doi.org/
10.1007/s00167-006-0140-8.
Nolan JE 3rd, Schottel PC, Endres NK. Trochleoplasty: indications and Technique. Curr Rev Musculoskelet Med. 2018;11:231-240. https://doi.org/10.
1007/s12178-018-9478-z.
Rouanet T, Gougeon F, Fayard JM, Rémy F,
Migaud H, Pasquier G. Sulcus deepening trochleoplasty for patellofemoral instability: a series of 34
cases after 15 years postoperative follow-up. Orthop
Traumatol Surg Res. 2015;101:443–7. https://doi.
org/10.1016/j.otsr.2015.01.017.
Amis AA, Oguz C, Bull AMJ, Senavongse W,
Dejour D. The effect of trochleoplasty on patellar
stability and kinematics: a biomechanical study
in vitro. J Bone Jt Surg Ser B. 2008;90:864–9.
https://doi.org/10.1302/0301-620X.90B7.20447.
Spang R, Egan J, Hanna P, Lechtig A, Haber D,
DeAngelis JP, et al. Comparison of patellofemoral
kinematics and stability after medial patellofemoral
ligament and medial quadriceps tendon-femoral
ligament reconstruction. Am J Sports Med.
2020;48:2252–9. https://doi.org/10.1177/036354652
0930703.
Van Haver A, De Roo K, De Beule M, Labey L, De
Baets P, Dejour D, et al. The effect of trochlear
dysplasia on patellofemoral biomechanics: a cadaveric study with simulated trochlear deformities. Am J
Sports Med. 2015;43:1354–61. https://doi.org/10.
1177/0363546515572143.
Vinod A V., Hollenberg AM, Kluczynski MA,
Marzo JM. Ability of medial patellofemoral ligament
reconstruction to overcome lateral patellar motion in
the presence of trochlear flattening: a cadaveric
biomechanical study. Am J Sports Med. 2021:1–6.
https://doi.org/10.1177/03635465211041087.
730
22. Kuroda R, Kambic H, Valdevit A, Andrish J. Distribution of patellofemoral joint pressures after femoral
trochlear osteotomy. Knee Surg Sport Traumatol
Arthrosc. 2002;10:33–7. https://doi.org/10.1007/
s00167-001-0256-9.
23. Draper CE, Besier TF, Fredericson M, Santos JM,
Beaupre GS, Delp SL, et al. Differences in
patellofemoral kinematics between weight-bearing
and non-weight-bearing conditions in patients with
patellofemoral pain. J Orthop Res. 2011;29:312–7.
https://doi.org/10.1002/jor.21253.
24. Tanaka MJ, Elias JJ, Williams AA, Demehri S,
Cosgarea AJ. Characterization of patellar maltracking
using dynamic kinematic CT imaging in patients
with patellar instability. Knee Surg Sport Traumatol
Arthrosc. 2016;24:3634–41. https://doi.org/10.1007/
s00167-016-4216-9.
25. Pal S, Besier TF, Beaupre GS, Fredericson M,
Delp SL, Gold GE. Patellar maltracking is prevalent
among patellofemoral pain subjects with patella alta:
an upright, weightbearing MRI study. J Orthop Res.
2013;31:448–57. https://doi.org/10.1002/jor.22256.
26. Conry KT, Cosgarea AJ, Tanaka MJ, Elias JJ. Influence
of tibial tuberosity position and trochlear depth on
patellar tracking in patellar instability: Variations with
Patella Alta. Clin Biomech. 2021;87: 105406. https://
doi.org/10.1016/j.clinbiomech.2021.105406.
27. Biyani R, Elias JJ, Saranathan A, Feng H,
Guseila LM, Morscher MA, et al. Anatomical factors
influencing patellar tracking in the unstable patellofemoral joint. Knee Surg Sport Traumatol Arthrosc.
J. J. Elias
28.
29.
30.
31.
32.
33.
2014;22:2334–41. https://doi.org/10.1007/s00167014-3195-y.
Elias JJ, Soehnlen NT, Guseila LM, Cosgarea AJ. Dynamic tracking influenced by anatomy
in patellar instability. Knee. 2016;23:450–5. https://
doi.org/10.1016/j.knee.2016.01.021.
Powers CM. Patellar kinematics, part II: the influence
of the depth of the trochlear groove in subjects with
and without patellofemoral pain. Phys Ther.
2000;80:965–73. https://doi.org/10.1093/ptj/80.10.
965.
Harbaugh CM, Wilson NA, Sheehan FT. Correlating
femoral shape with patellar kinematics in patients
with patellofemoral pain. J Orthop Res.
2010;28:865–72. https://doi.org/10.1002/jor.21101.
Rezvanifar SC, Flesher BL, Jones KC, Elias JJ. Lateral patellar maltracking due to trochlear dysplasia: a
computational study. Knee. 2019;26:1234–42.
https://doi.org/10.1016/j.knee.2019.11.006.
Kaiser D, Trummler L, Götschi T, Waibel FWA,
Snedeker JG, Fucentese SF. Patellofemoral instability in trochleodysplastic knee joints and the quantitative influence of simulated trochleoplasty—a finite
element simulation. Clin Biomech. 2021;81:105216.
https://doi.org/10.1016/j.clinbiomech.2020.105216.
Elias JJ, Rezvanifar SC, Koh JL. Groove-deepening
trochleoplasty reduces lateral patellar maltracking
and increases patellofemoral contact pressures:
Dynamic simulation. J Orthop Res. 2022;40:
1529–37. https://doi.org/10.1002/jor.25181.
Brain Network Functional
Connectivity Clinical Relevance
and Predictive Diagnostic Models
in Anterior Knee Pain Patients
María Beser-Robles, Vicente Sanchis-Alfonso,
and Luis Martí-Bonmatí
1
Background
Anterior knee pain (AKP) is the most common
reason young people consult with a knee orthopedic surgeon. However, despite its great
prevalence and the abundance of research, the
pathogenesis of AKP is still debated. AKP literature is dominated by local biomechanical
models that attempt to explain the mechanisms of
pain. However, the structural abnormalities analyzed in those biomechanical models, such as
patellar tilt, patellar subluxation, chondropathy,
and skeletal torsional abnormalities, may be
present in the absence of AKP. The reasons of
such clinic-morphological discrepancies remain
unsettled. Another peculiar characteristic of AKP
is the large variability regarding magnitude of
pain, disability, and pain experience, despite the
cause of pain being the same. Also, a great
M. Beser-Robles (&)
Biomedical Imaging Research Group at Health
Research Institute, Valencia, Spain
e-mail: marti_lui@gva.es
V. Sanchis-Alfonso
Department of Orthopaedic Surgery, Hospital Arnau
de Vilanova, Valencia, Spain
L. Martí-Bonmatí
Medical Imaging Department and Biomedical
Imaging Research Group at Hospital, Universitario y
Politecnico La Fe and Health Research Institute,
Valencia, Spain
variability in the response to an adequate treatment is observed among different AKP patients
with the same disease status. In addition, AKP
patients might present different psychological
impairments, from none to severe levels of
involvement. Interestingly, catastrophizing is the
most important aspect among the psychological
factors presented in AKP patients, being significantly related to pain and disability. This spectrum of variability might reflect the existence of
different other factors, in addition to biomechanical and structural alterations, to explain the
origin of the pain and its clinical heterogeneity.
As described, there are many questions that
cannot be properly answer at this time. Why is
there so much variability in the magnitude of
pain and in the pain experience among AKP
patients? Why do some individuals present AKP
while others with similar pathological findings
do not? Why does pain persist in some patients
after the painful structural stimulus has been
removed?
Functional Magnetic Resonance Imaging
(fMRI) analyses provides a better understanding
of the mechanisms underlying the development
of chronic pain by evaluating the brain resting
state functional connectivity (rsFC) [1]. As AKP
is a paradigm of chronic pain, we hypothesized
that AKP is associated with functional interconnected brain networks changes, which may
modulate the variable impairments that accompany this condition, explaining the different
treatment responses.
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_57
731
732
The first objective of this chapter is to show
that rsFC networks are different in AKP patients
compared with healthy subjects, mainly among
those brain areas involved in affective and cognitive stimulus processing and in regions
involved in pain modulation. Moreover, we will
define the rsFC changes related to the feeling of
catastrophizing. In addition, we will explore the
predictive ability of fMRI analyses with a clinical
decision support system (CDSS), providing a
complementary tool to help clinicians in the
clinical assessment of this condition.
1.1 Functional Magnetic Resonance
Imaging
Pain related changes can be captured by objective markers of functional brain activity. Blood
oxygen-level-dependent imaging, or BOLDcontrast imaging, is a method used in fMRI to
determine where and when brain activity occurs.
The BOLD signal change is the keystone of
fMRI, being used to construct spatial parametric
maps indicating which brain regions are activated
by certain tasks or react to specific stimulus.
Neurons do not contain any internal stores of
energy, either in the form of glucose or oxygen.
Therefore, when a brain region is activated,
adjacent capillaries provide it an increased
regional blood flow through a hemodynamic
response with a large increase in oxygen supply.
This inflow causes a change in the level of
oxyhemoglobin and deoxyhemoglobin balance
that can be detected using their differential
magnetic susceptibility, as deoxyhemoglobin is
strongly paramagnetic.
fMRI is a safe and noninvasive image technique able to map and measure regional brain
activity. fMRI is used to determine which brain
regions and networks are activated during different process by evaluating the increase in
oxygen consumption. This technique improves
our understanding of how the brain operates,
which regions are activated during specific
mental tasks or at rest, and how these regions are
organized into networks [2].
M. Beser-Robles et al.
fMRI has been widely used in patients with
neurological or psychiatric disorders, to analyze
the differences in synchronous and spontaneous
fluctuations of various networks compared with
healthy matched control subjects. Both taskbased and resting state studies have been performed for this purpose. In comparison to
specific task-based fMRI, resting state fMRI (rsfMRI) is acquired in the absence of a stimulus or
task, being therefore focus on the spontaneous
alterations of the brain BOLD signal. The
absence of a task makes rs-fMRI particularly
attractive for understanding the inherent connectivity patterns of interoperable brain regions
in patients suffering from neurological, neurosurgical, or psychiatric diseases and their differences with healthy controls, to improve the
understanding of these diseases [3, 4].
1.2 Pain Neuromatrix
It has been shown that several functional brain
regions are activated in a coordinated manner
when pain occurs, constituting what is known as
the “pain neuromatrix” [5]. This functional network is the basis of the multidimensional experience of pain. Specifically, under chronic pain
conditions, the main regions being affected are
the primary and secondary somatosensory cortex
(S1 and S2), spinal cord, thalamus, insula, anterior cingulate cortex (ACC), posterior cingulate
cortex (PCC), the medial and dorsolateral prefrontal cortex (mPFC/dlPFC), amygdala, nucleus
accumbens, and various mesencephalic areas
such as the periaqueductal grey matter (PAG)
and the cerebellum [6].
The human brain is intrinsically organized into
dynamic, anticorrelated functional networks [5].
It has been found that there are four main
brain networks whose dynamic interactions are
related to chronic pain [7]. One of them, the
Salience Network (SN), comprises the anterior
insula and the ACC, and is responsible for the
reception of sensory stimuli and the production
of affective responses. The Default Mode Network (DMN) consists of the PCC and the mPFC
Brain Network Functional Connectivity Clinical Relevance …
and it is mainly activated during resting state, as
the “automatic pilot” of the brain, it is related
with introspection. The third pain-related system
is the antinociceptive system (AS), which is
classically associated with pain modulation and
includes a hub of multi-connected regions in the
periaqueductal gray matter of the brainstem.
Finally, the sensorimotor network (SMN), which
consists of the basal ganglia, thalamus, posterior
insula, SI and SII, relates to the awareness of
bodily sensations and generation of appropriate
motor responses. Although these are the most
relevant, other functional networks such as limbic, attentional, and central executive, are also
active during the processing of pain stimuli [8]
(Fig. 1).
Pain pathways comprise a complex sensory
system, which is activated to provide protective
responses to noxious stimuli. Inputs regarding
noxious stimuli are transmitted from nociceptors
via primary afferent fibers to the brain. When a
Fig. 1 Overview of pain
pathways and functionally
altered areas in chronic pain,
divided according to the
neural networks to which they
belong. Green = SMN;
Blue = DMN;
Copper = Cerebellar network;
Dark blue = AS.
Amy = amygdala;
ACC = anterior cingulate
cortex; Ins = insula;
PAG = periaqueductal gray;
mPFC = medial prefrontal
cortex; BG = Basal ganglia;
Thal = thalamus;
PCC = posterior cingulate
cortex; S1, S2 = primary and
secondary somatosensory
cortex
733
painful stimulus occurs, peripheral nociceptors
are activated and ascending fibers transmit this
stimulus to the spinal cord. Ascending pathways
transmit the painful stimulus from the spinal cord
to the brain carrying sensory information from
the body to the brain. In addition, descending
pathways are established in mesencephalic areas
such as the PAG, descending down the spinal
cord and has a role in the modulation of pain [9].
The mechanism of pain transmission can be
oberved in Fig. 2.
Patients with chronic pain have increased
BOLD oscillations in DMN regions such as the
mPFC and, to a lesser extent, the PCC [4, 10]. In
addition, chronic pain has been shown to influence the functional connectivity of the ACC,
insula and SII. These regions are known to
receive nociceptive information from the
periphery and are involved in pain perception
and modulation [11]. Furthermore, it has been
suggested that weaker communications appear
734
M. Beser-Robles et al.
PFC
A
B
S1/S2
ACC
NAc
Thalamus
AMG
Brain
PAG
LC
Brain
Stem
RVM
Spinal dorsal
horn
Dorsal Spine
Nociceptor
Painful sƟmulus
Fig. 2 A Anatomical sites showing functional changes in
patients
suffering
chronic
pain.
Sensorimotor,
emotional/affective, cognitive/integrative, and modulatory
regions are involved in the complex processing of pain,
with some areas participating in more than one pain
domain. An example is the thalamus, which contains a
somatotopic representation of pain and processes the
emotional aspects of the pain experience. B Ascending
pathway (blue line): Pain signals ascend from the spinal
dorsal horn to the rostral ventral medulla (RVM) and
periaqueductal grey matter (PAG). They are then transmitted to the thalamus, where they are sent to higher brain
centers, such as the primary and secondary somatosensory
cortices (S1/S2), prefrontal cortex (PFC), anterior cortex
(ACC), amygdala (AMG), and nucleus accumbens (NAc).
Descending pathway (red line), involves important areas
of the brainstem such as the RVM, PAG, and locus
coeruleus (LC)
between the DMN and SN networks in patients
with chronic pain, making difficult for individuals to “switch off” their pain [5]. In healthy
subjects, there is a negative correlation between
DMN and SN. That is, when the DMN is active
the SN is inactive, and vice-versa. As the SN
coordinates the activation of the DMN and the
central executive network. However, in chronic
pain patients, there is a reduce in this anticorrelation. The cause of the increase of correlation
between the DMN and the SN can be due to an
alteration of the normal functioning of the SN
because a constant state of attention given by the
continuous input of nociceptive stimuli, so that
the introspection capacity of the DMN decreases
as it needs the coordination of the SN for its
correct functioning. So, we can see a loss of the
SN's ability to inhibit the DMN, due to a continuous input of nociceptive information.
1.3 Clinical Decision Support System
(CDSS)
A CDSS has the aim to improve healthcare
provision by refining medical decisions accuracy
with specific clinical knowledge and imaging
extracted information. To obtain a direct clinical
decision gain, the characteristics of an individual
patient must be compared against a computerized
clinical knowledge database, and then specific
assessments or recommendations are presented to
the clinician to help taking decisions on that
patient [12]. Validated CDSS have been shown
Brain Network Functional Connectivity Clinical Relevance …
735
to increase the capacity of healthcare professionals in a range of patient care decisions and
tasks, and nowadays actively support the provision of quality care. In our scenario, the CDSS
aims to predict whether a subject has chronic
AKP or not.
Machine learning is a field of artificial intelligence based on the paradigm that systems learn
from data, identify patterns, and provide decisions with minimal human intervention. In our
example, we will define a machine learning
classification algorithm, which is a supervised
learning technique. In this type of algorithm, the
program learns from previously classified
observations and with this information it classifies a new one [13].
Demographic recorded variables which can
influence the brain functional network were
recorded (age, dominant hand, scholarship, and
pain duration), and participants completed a selfreporting questionnaires regarding neuropathic
pain, anxiety, depression, kinesiophobia and
catastrophizing. Clinical pain intensity was
obtained by asking subjects to rate their pain on a
Visual Analogue Scale (VAS) [14]. Anxiety and
depression were evaluated using the Hospital
Anxiety and Depression Subscale (HAD) [15].
Pain-related fear associated with avoidance of
movement and physical activity was measured
using the Tampa Scale for Kinesiophobia
(TSK) [16], and catastrophizing was measured
using the Pain Catastrophizing Scale (PCS) [17].
2
2.2 Resting State MRI Data
Acquisition
Our Clinical Results
2.1 Participants and Clinical
Assessments
To prove the relationship between functional brain
modifications associated to chronic knee pain, we
will report here on a prospectively evaluated series
of 40 subjects, all young women to avoid biases,
equaly distributed (20 women with 6 months
duration chronic AKP, 27.4 ± 9.0 years,
mean ± SD, 18–44 range; and 20 healthy women
without any knee or other types of pain, aged
28.85 ± 7.6 years, 20–43 range). Patients and
controls were matched for age, both groups having
a normal distribution. All subjects gave written
consent for this study. The AKP group included
patients with self-reported pain around or behind
the patella aggravated by activities that load the
joint, without identifiable pathological causes.
Cases for the control group were excluded if they
presented acute or chronic pain in the last
6 months and a history of psychologic or psychiatric disorders. The study was approved by
the hospital Institutional Review Board (IRB)
(CEIm:3/2018) and conducted according to the
Declaration of Helsinki.
MR images were acquired on a 3 T magnet
(Achieva, Philips Healthcare Best, Netherlands)
using an 8-channel head coil with parallel
acquisition technology (SENSE). All participants
were instructed at the beginning of the acquisitions to avoid movements, keep their eyes closed,
stay awake and think of a blue sky.
The acquisition protocol consisted of a high
spatial resolution T1 weighted 3D gradient echo
sequence with the following parameters: TE = 3
s, TR = 6.2 s, FA = 100, voxel size = 1 1
1 m m3, and 6 min of duration. This sequence
provides a high contrast between white matter
(WM), grey matter (GM) and cerebrospinal fluid
(CSF) to segment and parcellate the different
brain regions.
The rs-fMRI T2* weighted 2D EPI BOLD
sequence was acquired with the following
parameters: TE = 35 ms, TR = 2000 ms, temporal dynamics = 265, voxel size = 1.8 1.8
5 mm3, and an overall duration of 9 min. This
sequence allows to explore FC networks by
sampling the brain hemodynamic response during neuronal activation at the resting state,
736
acquiring the whole brain volume with a temporal resolution of 2 s per partition.
2.3 Image Processing
To increase reproducibility, all MR images were
preprocessed using the CONN and SPM12
toolboxes. The rs-fMRI images were corrected
(intra-patient registration) from slice time and
patient movement, normalized to MNI space,
registered with the structural images and
smoothed. Artefact detection was used to depict
intensity peaks and excessive patient movements
by using ART-repair software and a componentbased noise correction method (CompCor).
Acquisitions showing a mean image shift greater
than 0.9 mm or global BOLD signal changes
greater than 5 standard deviations were flagged
as possible outliers.
The intensity level of BOLD timeseries was
normalized and images were spatially registered
towards a standardized MNI space, with 2-mm
isotropic voxels for the functional data and 1 mm
for the structural. Segmentation GM, WM and
CSF was applied before the Harvard–Oxford
probabilistic atlas brain parcellation on 91 cortical and 15 subcortical regions of interest (ROI),
plus 26 cerebellar regions defined by the Automated Anatomical Labelling (AAL) atlas. Commonly characterized networks were obtained by
seed-areas on known networks (SN, DMN,
Dorsal Attention Network-DAN, Sensorimotor
Network-SMN, Visual Network-VN and Cerebellar Network-CN). Spatial smoothing was used
to minimize sharp edges for multi-subject averaging, to increase the BOLD signal-to-noise
ratio.
The main confounder effects (24 parameters
for head movement obtained from the ARTrepair programme and intensity effects that do
not correspond to the grey matter) were included
in a linear regression model, with a bandpass
filtering (0.008–0.09 Hz) to obtain BOLD timeseries signal free of unwanted effects.
M. Beser-Robles et al.
2.4 Image Analysis
An atlas-based ROI-to-ROI analysis represented
the level of partial correlation between all pairs
of brain ROIs, using a general linear model
(GLM) to estimate the strength of connectivity
between brain areas by analyzing the correlation
of the BOLD signal of each pair of brain ROIs.
The effect sizes are represented by Pearson's
correlation coefficients (r) with a Fisher's ztransformation.
In the statistical analysis, significant clusters
were determined by two thresholds, one at voxel
level and one at cluster level (grouping of voxels). The significance level was defined by a
voxel-level threshold of p < 0.001 uncorrected to
control for cluster spread, and a cluster-level
threshold of p < 0.05 corrected for false discovery rate (FDR), for multiple comparisons across
the whole brain [18]. The first analysis consisted
of a between-group comparison to study significant unbiased differences in functional connectivity of each pair of regions between patients
and controls, adding laterality, scholarship, anxiety, and depression as covariates in a GLMbased regression statistical analysis. The second
analysis was a study of significant differences in
functional connectivity related to the level of
catastrophizing in patients. For both analyses, a
student’s t statistic was used, considering as
significant only pair of regions presenting a pvalue that fulfills the above conditions.
2.5 Classification Model
With the aim of identifying AKP patients using a
clinical decision system, we trained and evaluated 6 supervised learning classifiers: Logistic
Regression (LR), Linear Discriminant Analysis
(LDA), K-neighbors (KNN), decision Trees
(DT), Gaussian Naive Bayes (GNB) and Support
Vector Machine (SVM). All were implemented
with the Scikit-learn machine learning library.
These algorithms use as inputs the significant
Brain Network Functional Connectivity Clinical Relevance …
results of the correlation analysis between pairs
of regions and their correspondence with patients
or controls, learning to classify any new data as
patient or control. As each classifier uses a different learning method, we evaluated the most
optimal by analyzing the accuracy of the 6
models [19].
When dealing with supervised learning models, data must be separated into the training set
and the test set. To avoid bias due to the splitting
of the data set, a cross-validation approach was
used to ensure that results are independent of the
partition between training and test data. There are
many methods of cross-validation, although the
leave-one-out (LOO) maximizes the robustness
of the classifier. This method consists of training
the classifier with the n-1 observations and testing with the remaining one, doing this as many
times as the number of observations in the study
sample. To build our CDSS, we trained and
evaluated the 6 models determining their accuracy and area under the curve (AUC), which
measures the classifier's ability to distinguish
between classes.
2.6 Results
Regarding the clinical data collected from the
pain patients, the mean VAS score obtained was
6.84 ± 1.7. In addition, a large proportion of
patients presented results compatible with kinesiophobia (75%) and catastrophic thoughts
(55%). Anxiety (30%) and depression (10%)
Table 1 Demographic
characteristics of AKP
patients, expressed as
percentage for categorical
variables and mean for
quantitative variables
737
were also observed in smaller amounts. Patients’
demographics and clinical evaluation are summarized in Table 1.
Regarding the functional connectivity analysis, significant differences in regions and networks (p-FDR < 0.05) were found between AKP
patients and matched healthy controls (Table 2).
For most functional connectivity changes, a
higher correlation in absolute terms was observed
between patients’ ROIs compared to controls,
except for the sensorimotor network and the
temporal planum with their respective ROIs,
where a lower correlation was observed in
chronic pain conditions. We do highlight the
fMRI changes produced in the mPFC, as a region
of the DMN, and the superior regions of the
SMN, because of their role in the processing of
pain stimuli, which has been seen in different
studies [20]. We also observed differences in the
thalamus, which acts as a transmitter of the
nociceptive stimulus to the rest of the higher
structures. Also, the role of the cerebellum was
highlighted as many regions showed FC alterations. A visual representation of these significant differences in FC is shown in Fig. 3.
In the analysis performed to evaluate the
effect of catastrophizing, statistically significant
differences (p-FDR < 0.05) were observed in FC
in different regions (Table 3). A lower correlation
in absolute value was observed when patients
present catastrophic ideas, except in the posterior
cingulate gyrus (PC) with the Vermis area. We
can also highlight the changes produced in the
mPFC and some regions of the cerebellum, and
Demographic variables
Patient group
Duration of symptoms (mean ± std)
9.32 ± 7.96
Laterality (right-handed %)
85%
VAS (mean ± std)
6.84 ± 1.7
Anxiety (%)
30%
Depression (%)
10%
Kinesiophobia (%)
75%
Catastrophization (%)
55%
Education level (high level %)
80%
738
M. Beser-Robles et al.
Table 2 FC AKP patients vs. Controls. ROI1 and ROI2 constitute the pair of evaluated regions on which the rs-fMRI
connectivity showed significant differences between patients and controls. ß values for Patients and Controls represent
the correlation between ROI1 and ROI2. Columns 2 and 4 indicate the spatial location of the regions in the Montreal
Neurologic Institute (MNI) coordinates. The correlation strength represents the behavior of the correlation between the
two ROIs, whether it increases or decreases in the case of patients
ROI 1
MNI
coordinates
ROI 2
MNI
coordinates
ß
Patients
ß
Controls
Thalamus r
(10, 2, 8)
LG r
(20, −44,
−8)
−0.06
−0.13
Cereb45 r
(−8, −32,
−12)
pSTG l
(−57, −47,
15)
−0.16
mPFC
(1, 55, −3)
PO r
(51, −30,
28)
Cerebellar Network
(posterior)
(0, −79,
−32)
LG l
SMN-Sup
(9, −31,
67)
PT l
(−60, −30,
8)
Fig. 3 Ring view of the
significant differences in the
correlation of ROIs pairs
between patients and controls.
The color bar represents the
value of the T-statistic,
reddish colors denote a
positive association (greater
correlation/FC in patients than
in controls) and blue colors
denote a negative association
(lower correlation/FC in
patients than in controls).
ROIs shown in mid-axial
slices
T
Student
p-FDR
Correlation
strength
4.54
0.0118
" in patients
−0.25
4.32
0.0219
" in patients
−0.10
−0.17
4.31
0.0224
" in patients
(−18, −42,
−6)
0.03
−0.07
4.19
0.0322
" in patients
lPFC l
(−43, 33,
28)
0.03
0.08
−4.81
0.0053
# in patients
Ver9
(1, −55,
−35)
0.04
0.14
−4.35
0.0201
# in patients
Brain Network Functional Connectivity Clinical Relevance …
739
Table 3 FC AKP Catastrophizing subjects. ROI1 and ROI2 constitute the pair of evaluated regions on which the
rsfMRI functional connectivity has shown significant differences between patients and controls. ß represents
the catastrophizing patient’s correlation between ROI1 and ROI2. Columns 2 and 4 indicate the spatial location of the
regions in the Montreal Neurologic Institute (MNI) coordinates. The correlation strength represents the behavior of
the correlation between the two ROIs, whether it increases or decreases in the case of catastrophizing patients
ROI 1
MNI
coordinates
ROI 2
MNI
coordinates
PC
(1, −37, 30)
Ver8
(1, −64, −34)
PC
(1, −37, 30)
Cereb3
l
rPFC
(30, 48, 9)
mPFC
(1, 55, −3)
ß
T
Student
p-FDR
Correlation strength
0.13
4.03
0.0211
" with
catastrophization
(−9, −37,
−19)
−0.13
−4.36
0.0159
# with
catastrophization
Cuneal
l
(−12, −90,
22)
−0.08
−4.20
0.0256
# with
catastrophization
Cereb1
l
(−36, −66,
−30)
−0.07
−4.12
0.0328
# with
catastrophization
Fig. 4 Ring view of the
significant differences in the
correlation between pairs of
ROIs when studying the effect
of catastrophizing thoughts.
The color bar represents the
value of the T-statistic,
reddish colors denote a
positive association (higher
correlation/FC in
catastrophizing patients) and
blue colors denote a negative
association (lower
correlation/FC in
catastrophizing patients).
Position of ROIs shown in
mid-axial slices
in the PC as a region of the SMN. A visual
representation of these significant differences in
FC is shown in Fig. 4.
Finally, the significant correlations results
between regions and AKP patient networks were
used as inputs to feed the classification models.
After testing the 6 supervised learning classification models, the K-nearest neighbors
(KNN) model was chosen as it gave the best
results from the accuracy and the AUC curve
(Table 4).
740
M. Beser-Robles et al.
Table 4 Classification System Results. Shows the accuracy and AUC classifier results for each supervised
learning model. LR: Logistic Regression; LDA: Linear
Discriminant Analysis; KNN: K-neighbors; DT: Decision
Trees; GNB: Gaussian Naive Bayes; SVM: Support
Vector Machine. The best result obtained in accuracy
and AUC has been highlighted in green
Supervised learning model
tested
Accuracy
(%)
AUC
LR
57.5
0.55
LDA
65
0.67
KNN
67.5
0.70
DT
57.5
0.52
GNB
57.5
0.62
SVM
67.5
0.60
3
Discusion
Patients with AKP have significant rsFC differences compared to matched healthy subjects.
Comparing rsFC between patients and controls,
there is an absolute increment in the correlation
between regions appear for AKP patients, highlighting the connections of mPFC/POr, Thalamus
r/LG r, Cereb45/pSTG and the posterior part of
the cerebellar network with the LG l. Moreover,
absolute decreases in the correlation between
regions appear for AKP patients in the regions of
PT/Ver9 and the superior part of the SMN with
the lPFC. Catastrophizing has an effect on the
rsFC of AKP patients, with an increase in the
correlation between PC/Ver8 and a decrease in
the correlation between the regions of
PC/Cereb3, rPFC/cuneus and mPFC/Cereb1. In
addition, the connectivity between regions was
able to reach a 68% cross-validation accuracy to
discriminate AKP patients from controls.
Several other studies have found functional
nodes involved in the development of chronic
pain, mainly in the DMN, SMN and SN [21, 22].
The mPFC is one of the most important regions
in the DMN, being related to pain modulation
and emotional appraisal. mPFC presents a significant increase in correlation with the POr in
patients against controls, increasing the existing
anticorrelation between these regions. The POr is
a region of the SII which has been involved in
the discriminative sensory aspect of pain. These
results are in line with those of Pujol and colleagues [23], where we can see that in chronic
pain condition there is an increased connectivity
between the SII and DMN. In addition, previous
studies reported that cortical prefrontal areas are
involved in cognitive functions, such as planning, decision making and detection of unfavorable outcomes, avoidance of risky choices
based on emotions, and goal-oriented behaviors
[24, 25].
The role of the thalamus in chronic pain is
also relevant, showing a higher correlation with
the right part of the lingual gyrus (LG r). The
thalamus is one of the most important regions in
the development of chronic pain, as it receives
projections from multiple ascending pain pathways and modulates ascending nociceptive
information [26], while the LG is involved in
sensorimotor integration [27]. The increased
anticorrelation between these regions has also
been shown in previous studies [28, 29].
On the other hand, previous studies [30, 31]
have shown that the role of the cerebellum seems
very important in the development of chronic
pain, since there are alterations in the correlation
of the cerebellum with multiple regions. Here, we
found an increased correlation of two cerebellar
regions with different regions (pSTG and LG l)
and a decreased correlation between area Vermis
9 (structure located between the cerebellar
hemispheres) and PT l. Evidence suggests that
specific nociceptive activation is processed in the
deep cerebellar nuclei, the anterior vermis and
bilaterally in lobules IV, V and VI of the cerebellar hemispheres [30]. This suggests that cognitive processing areas in the cerebellum may be
related to pain encoding.
In patients with AKP we have also observed
an increased correlation between regions of the
superior part of the somatosensory network
(postcentral gyrus, precentral gyrus and supplementary cortex) with the dorsolateral prefrontal
cortex (lPFC), a region that is part of the central
executive network and is related to pain modulation and regulation [32]. These regions are
correlated in healthy subjects, and a decrease in
Brain Network Functional Connectivity Clinical Relevance …
the correlation between them could indicate
lower suppression of nociceptive impulses, due
to the chronic pain condition.
Catastrophizing is the most important aspect
among all the psychological factors affecting
AKP patients, being significantly related to pain
and disability (see Chap. 6). Pain catastrophizing
is a psychological construct that includes cognitive, emotional, and behavioral processes (fearavoidance behaviors, altered mood and motivation) that amplify perceived painful sensations
and predispose to the perpetuation of pain [33].
When studying this in AKP patients, significant
differences were found in the FC of AKP patients
showing catastrophizing. Patients with catastrophizing showed, in general, a decrease in correlation between regions, especially between
regions of the cerebellum and the DMN. We
highlight the effect of the posterior cingulate
gyrus (PC) region with different areas of the
cerebellum, showing a significant increase in the
correlation with the Vermis 8 area, and a significant decrease in the correlation with the third
lobe of the cerebellum. We can also observe a
decrease in different regions of the prefrontal
cortex. On the one hand between the mPFC and
the first lobe of the cerebellum, which as we have
seen is a key region in the development of
chronic pain. On the other hand, between the
rostral prefrontal cortex and the cuneus, which
has the function of integrating and processing
somatosensory information. These results are in
line with previous studies showing changes in the
connectivity patterns of different areas, including
the PC, mPFC and cerebellum [30]. The deactivation of the mPFC and PC during nociceptive
stimulation has been associated with the attentional capture of pain [32, 34, 35], which is
enhanced by negative pain cognitions, such as
catastrophizing. This suggests that patients with
high catastrophizing scores may have increased
attentional capture by pain and, thus, an inability
to divert their attention away, resulting in a
decreased ability to modulate their pain.
Development of a predictive diagnostic model
using a pattern of FC to differentiate subjects
with chronic pain is relevant in clinical practice.
Significant results obtained from the analysis of
741
fMRI images allowed the construction of a
classifier with an accuracy of 67% for the identification of AKP patients. Although these
promising results need external validation to
assess reproducibility, they show that the information provided by rs-fMRI analysis can be use
for pattern detection. This clinical decision support tool may be a step towards improving our
understanding of pain mechanisms. Insurance
companies and legislation have a great interest in
objective measurements of pain-related disability, but we still have a long way to go before
brain imaging can be used as a diagnostic tool
after validation and regulatory acceptance. These
issues are being addressed from different perspectives, including neuroethics. If valid objective processes can be established to detect/define
pain, this would have huge implications for the
insurance industry and the legal field, as a significant number of cases are related to pain,
suffering and disability. In addition, it will provide patients with objective evidence of their
condition and its evolution over time [36].
Regardless of the wide impact that patellofemoral pain has today, there are few studies that
focus on this specific area to depict the implications that chronic pain has on brain connectivity.
We have demonstrated that chronic patellofemoral pain altered the FC in regions of the DMN
and the SMN. These areas can also be observed
in other types of widely studied chronic pain,
such as low back pain [37]. As a difference,
regions such as the insula or the ACC are not so
affected in the patellofemoral pain model. This
study is in line with a previous one [27], showing
that in AKP sensorimotor regions and thalamus
acquire greater importance than SN regions. As a
result, pain‐disrupted sensorimotor connectivity
may influence patients with patellofemoral pain
perception of function, pain, and fear of movement, and that it can be resultant to altered central neural processes. This could be due to the
fact that in this type of pain the sensory and
cognitive components acquire greater relevance.
However, to determine the specific differences
between the different mechanisms of chronic
pain, future studies comparing these conditions
are needed.
742
M. Beser-Robles et al.
A major limitation is the transversal design as
the study does not track individuals before the
onset and through the development of pain.
Therefore, the observed rs-fMRI changes cannot
be specifically determined to be caused by the
presence of chronic pain. In addition, the number
of patients and control subjects in our study was
relatively small. But based on a previous study
about the minimum sample size [38], and estimating an effect size of 0.15 and a minimum
AUC around 0.70 as an acceptability cut-off, we
would need a sample size between 38 and 46
subjects, which is very close to our 40 subjects.
We do believe that the magnitude of the effects
balance the small sample size; moreover, larger
samples are necessary given that the variability in
symptomatology of these patients is large. Age,
handedness and received education were included as covariates to endorse that the observed
changes were mainly due to AKP. To control the
error rate, a threshold of p-FDR 0.05 (uncorrected p values of 0.001) was established
to improve the consistency and robustness of the
results. Finally, alterations in FC could depend
on the intensity and duration of pain, both of
which were highly variable in our series, so
future studies will be necessary to investigate the
influence of these variables on chronic patellofemoral pain.
4
Future Oportunities
The following aspects can he highlighted for
future studies on relevant challenges and developments. New studies might be design to
develop a predictive model that will allow to
determine the probability that a knee pain is or is
not of patellofemoral origin. Also, new studies
are needed to evaluate resting state connectivity
fMRI as a tool to monitor the follow-up of these
patients after treatment. Finally, further studies
should lay the groundwork for using repetitive
transcranial magnetic stimulation treatments in
this type of pathology.
In summary, the following aspects can be
highlighted from the use of re-fMRI in chronic
pain studies:
– Chronic pain has a disruptive effect on some
functional brain networks. FC is altered in
patients with AKP compared to matched
control subjects, having a generalized impact
on global brain function.
– The level of catastrophization presented by
the patients conditioned new alterations in
functional connectivity.
– Functional brain networks alterations allow
the use of a clinical decision support system to
help clinician to accurately identify patients
suffering from chronic pain. This could be a
first step towards the objectification and
identification of pain.
References
1. Valdes-Hernandez PA, Montesino-Goicolea S,
Hoyos L, et al. Resting-state functional connectivity
patterns are associated with worst pain duration in
community-dwelling older adults. Pain Reports.
2021;6: e978.
2. Magnetic Resonance Imaging (MRI). https://www.
nibib.nih.gov/science-education/science-topics/
magnetic-resonance-imaging-mri.
3. Lv H, Wang Z, Tong E, et al. Resting-state functional
MRI: everything that nonexperts have always wanted
to know. AJNR Am J Neuroradiol. 2018;39:1390.
4. Loggia ML, Jensen KB. Imaging pain in the human
brain. In: Imaging of the Human Brain in Health and
Disease (Elsevier, 2014), 427–451.
5. Kucyi A, Salomons T, Davis K. Mind wandering
away from pain dynamically engages antinociceptive
and default mode brain networks. Proc Natl Acad
Sci USA. 2013;110:18692–7.
6. Moseley G. A pain neuromatrix approach to patients
with chronic pain. Man Ther. 2003;8:130–40.
7. Fox MD, Snyder AZ, Vincent JL, et al. The human
brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc Natl Acad Sci.
2005;102:9673–8.
8. Tracey I, Mantyh P. The cerebral signature for pain
perception
and
its
modulation.
Neuron.
2007;55:377–91.
9. Yang S, Chang MC. Chronic pain: structural and
functional changes in brain structures and associated
negative affective states. Int J Mol Sci.
2019;20:3130.
10. Baliki MN, Geha PY, Apkarian AV, et al. beyond
feeling: chronic pain hurts the brain, disrupting the
default-mode network dynamics. J. Neurosci.
2008;28.
Brain Network Functional Connectivity Clinical Relevance …
11. Thorp S, Healthcare CR, Thorp SL, et al. Functional
connectivity alterations: novel therapy and future
implications in chronic pain management. Pain
Physician. 2018;21:207–14.
12. Sutton RT, Pincock D, Baumgart DC, et al. An
overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med.
2020;3:1–10.
13. Classification Algorithm in Machine Learning.
https://www.javatpoint.com/classification-algorithmin-machine-learning.
14. Crossley K, Bennell K, Cowan S, et al. Analysis of
outcome measures for persons with patellofemoral
pain: which are reliable and valid? Arch Phys Med
Rehabil. 2004;85:815–22.
15. Zigmond A, Snaith R. The hospital anxiety and
depression
scale.
Acta
Psychiatr
Scand.
1983;67:361–70.
16. Kori SH, Miller RP, Todd DD. Kinesiophobia: a new
view of chronic pain behavior. Pain Mang. 1990;
35–43.
17. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7:524–32.
18. Benjamini Y, Drai D, Elmer G, et al. Controlling the
false discovery rate in behavior genetics research.
Behav Brain Res. 2001;125:279–84.
19. De Andrés J, Ten Esteve A. Predictive clinical
decission system using machine learning and imaging biomarkers in patients with neurostimulation
therapy: a pilot study. Pain Physician.
20. Tu Y, Jung M, Gollub RL, et al. Abnormal medial
prefrontal cortex functional connectivity and its
association with clinical symptoms in chronic low
back pain. Pain. 2019;160:1308.
21. Alshelh Z, Marciszewski KK, Akhter R, et al.
Disruption of default mode network dynamics in
acute and chronic pain states. NeuroImage Clin.
2018;17:222–31.
22. Van Ettinger-Veenstra H, Lundberg P, Alföldi P,
et al. Chronic widespread pain patients show disrupted cortical connectivity in default mode and
salience networks, modulated by pain sensitivity.
2019.
23. Pujol J, Macià D, Garcia-Fontanals A, et al. The
contribution of sensory system functional connectivity reduction to clinical pain in fibromyalgia. Pain.
2014;155:1492–503.
24. Orestes Pérez A, Jiménez Gutiérrez M, Vega
Cisneros L. Regiones del encéfalo vinculadas a la
interpretación del dolor. Rev Habanera Ciencias
Médicas. 2018;17.
743
25. Kucyi A, Moayedi M, Weissman-Fogel I, et al.
Enhanced medial prefrontal-default mode network
functional connectivity in chronic pain and its
association with pain rumination. J Neurosci.
2014;34:3969–75.
26. Ab Aziz CB, Ahmad AH. The role of the thalamus in
modulating pain. Malays J Med Sci. 2006;13:11.
27. Diekfuss JA, Grooms DR, Nissen KS, et al. Does
central nervous system dysfunction underlie patellofemoral pain in young females? Examining brain
functional connectivity in association with patientreported outcomes. J Orthop Res. 2021.
28. Molina J, Amaro E, da Rocha LGS, et al. Functional
resonance magnetic imaging (fMRI) in adolescents
with idiopathic musculoskeletal pain: a paradigm of
experimental pain. Pediatr Rheumatol. 2017;15:
1–10.
29. Shen W, Tu Y, Gollub R, et al. Visual network
alterations in brain functional connectivity in chronic
low back pain: a resting state functional connectivity
and machine learning study. NeuroImage Clin.
2019;22.
30. Moulton E, Schmahmann J, Becerra L, et al. The
cerebellum and pain: passive integrator or active
participator? Brain Res Rev. 2010;65:14–27.
31. Kong J, Loggia ML, Zyloney C, et al. Exploring the
brain in pain: activations, deactivations and their
relation. Pain. 2010;148:257.
32. Seminowicz DA, Moayedi M. The dorsolateral
prefrontal cortex in acute and chronic pain. J Pain.
2017;18:1027.
33. Galambos A, Szabó E, Nagy Z, et al. A systematic
review of structural and functional MRI studies on
pain catastrophizing. J Pain Res. 2019;12:1155.
34. Davis KD, Moayedi M. Central mechanisms of pain
revealed through functional and structural MRI.
J Neuroimmune Pharmacol. 2013;8:518–34.
35. Mathur VA, Moayedi M, Keaser ML, et al. High
Frequency migraine is associated with lower acute
pain sensitivity and abnormal insula activity related
to migraine pain intensity, attack frequency, and pain
catastrophizing. Front Hum Neurosci. 2016;10:489.
36. Borsook D, Sava S, Becerra L. The pain imaging
revolution: advancing pain into the 21st century.
Neurosci. 2010;16:171–85.
37. Kregel J, Meeus M, Malfliet A, et al. Structural and
functional brain abnormalities in chronic low back
pain: a systematic review☆. Semin Arthritis Rheum.
2015;45:229–37.
38. Hajian-Tilaki K. Sample size estimation in diagnostic
test studies of biomedical informatics. J Biomed
Inform. 2014;48:193–204.
Robotic-Assisted Patellofemoral
Arthroplasty
Joseph C. Brinkman, Christian Rosenow,
Matthew Anastasi, Don Dulle,
and Anikar Chhabra
1
Introduction
Isolated patellofemoral osteoarthritis (PFOA)
involves defects in the articular cartilage lining
the patellar facets or femoral trochlea. It is a relatively common condition that affects approximately 10% over 40 years of age and 20% over
55 years of age [1, 2]. The prevalence and
debilitating nature of the condition has prompted
interest in optimizing treatments for it. Traditionally, conservative treatment of isolated PFOA
is similar to that of multicompartment
osteoarthritis (OA) and includes short-term bracing, taping, physical therapy, and corticosteroid
injections [3]. Joint preservation interventions
such as chondroplasty, microfracture, and extensor mechanism realignment operations also exist,
but do not completely address the joint surfaces.
While total knee arthroplasty (TKA) has long
been the standard for knee OA, its efficacy in
patients with PFOA is somewhat limited. TKA
restricts activity tolerance and disrupts normal
J. C. Brinkman C. Rosenow M. Anastasi
D. Dulle A. Chhabra (&)
Department of Orthopaedic Surgery, Mayo Clinic,
5777 E. Mayo Blvd, Phoenix, AZ 85054, USA
e-mail: Chhabra.Anikar@mayo.edu
Department of Sports Medicine, Mayo Clinic, 5777
E. Mayo Blvd, Tempe, Phoenix, AZ 85054, USA
Alix School of Medicine, Mayo Clinic, 5777 E.
Mayo Blvd, Phoenix, AZ 85054, USA
extensor mechanism function while removing
functional native connective tissues, such as the
menisci and cruciate ligaments [4]. Additionally,
in patients with isolated patellofemoral arthritis,
TKA involves unnecessarily replacing the intact
medial and lateral compartments. Patellofemoral
arthroplasty (PFA) was subsequently developed
to address only the affected compartment, leaving the remaining compartments and associated
soft tissues in their native state.
Patellofemoral arthroplasty (PFA) was first
described by McKeever in 1955 utilizing a
Vitallium alloy patellar shell [5]. This was later
advanced when Lubinus described a dedicated
resurfacing implant in 1979 [6]. Initial success
was limited by issues regarding patellar maltracking, alignment, and patellar catching [7–10].
Second-generation components developed in the
1990’s utilized anterior femoral resection and
valgus tracking angles with wide trochlear surfaces designed to promote improved tracking [4].
Overall, modern PFA techniques more reliably
restore patellofemoral anatomy and function.
These implants have demonstrated favorable
survivorship with 10 and 20 year survival rates
of 83.3% and 66.6%, respectively [11]. However, interest in optimizing technique and
implants has continued.
The advent of robotic surgical systems has
driven development of numerous robotic techniques in orthopaedics. Robotics has been particularly prominent in hip and knee arthroplasty,
where it has been reported to improve the
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_58
745
746
accuracy and precision relative to manual techniques [12]. Success in total, as well as unicompartmental, knee arthroplasty has prompted
recent interest in applying robotic technology to
patellofemoral arthroplasty. This technology
allows for preoperative and virtual PFA templating utilizing the patient’s computed tomography (CT) as a reference. Intraoperatively, a
robotic arm assists with bone cuts and correct
positioning of the components. The goal with
these measures is to optimize the sizing, alignment, and positioning of the components relative
to the patient’s patellofemoral anatomy. As poor
results of manual PFA are typically due to
excessive internal rotation of the trochlear component, these features of RA-PFA are believed to
contribute to improved reproducibility and success of the procedure [13, 14]. Investigations of
RA-PFA are few, but outcomes have demonstrated accurate alignment and functional benefit
in short-term follow-up studies [15]. Additionally, minimally invasive RA-PFA is associated
with smaller incision size, faster recovery, and
reduced soft-tissue disruption [16–18].
The procedure also has downsides that should
be considered. First, PFA, either robotic or
manual, is often considered a temporizing repair
reserved for young, active patients in whom
TKA would significantly limit functional capacity. It is believed that many of these patients will
eventually require TKA as a result of tibiofemoral arthritis advancement. In these cases,
performing PFA with a fair likelihood of eventual TKA increases the patient’s exposure to a
second procedure, operative risk, anesthetic, and
carries a significantly greater use of resources
[19, 20]. Widespread adoption of RA-PFA is also
limited by capital and infrastructure factors as it
carries increased costs associated with robotic
arm installment, maintenance, and operation.
Many centers may be unwilling to invest in these
systems given the above factors without studies
evaluating long-term outcomes, survivability,
and cost–benefit analyses. Further, the presence
and availability of CT scanners for preoperative
planning is a requisite for adoption of roboticassisted techniques. Lastly, apprehension
regarding the learning curve for robotic
J. C. Brinkman et al.
techniques may exist; however, multiple studies
have demonstrated that surgeon comfort with
robotic systems develops quickly without a
learning curve impact on component alignment
[21–23].
2
Indications and Contraindications
Success with PFA is known to depend on proper
patient selection [19]. Generally, PFA is reserved
for young, active patients with severely limiting
pain and evidence of isolated PFOA. These
patients typically report anterior knee pain with
activities that load the knee such as descending
stairs, squatting, or sitting for a prolonged period
[24]. Classically, pain is less severe with ambulation on even surfaces or when the knee is in the
fully extended position. Surgical management is
considered in patients who have failed extensive
attempts at nonoperative management including
activity modification, non-steroidal medication,
physical therapy, and bracing. Extensive chondrosis, malalignment of the PFJ, and dysplasiainduced OA are also relative indications for PFA
[25]. It is believed that the procedure is most
appropriate for patients between the ages of 40
and 60 [19, 26].
Several contraindications also exist. Primarily,
the surgery relies on native knee kinematics
created by a stable joint, functional ligaments,
and intact soft tissue structures including the
menisci. These are considered a fundamental
requirement for successful PFA. Tibiofemoral
arthritis is reported as a common cause of PFA
failure and the most common contraindication
[25]. As PFA does not address the soft tissues
affecting the joint, a significantly increased Qangle is a contraindication as this would indicate
patellofemoral malalignment that cannot be corrected with PFA. However, retinacular releases
and patellar osteoplasty can be performed to
address milder patellar subluxation or tilt forces
[24]. Contraindications also include inflammatory arthritis, active infection, or complex
regional pain syndrome. Mechanical limb axis
malalignment of >8 degrees valgus or >5 degrees
of valgus requires alternate intervention, as does
Robotic-Assisted Patellofemoral Arthroplasty
patella baja [27]. Obesity, although not an
absolute contraindication, does portend poorer
results and is, at times, utilized as a relative
contraindication [28]. Utilizing robotics is up to
the discretion of the surgeon. Generally, indications and contraindications do not vary significantly from manual techniques, though
consideration of longer operative time should be
included in decision-making.
3
Preoperative Planning
A standard series of X-rays should first be
obtained. These include standing AP, flexion PA
(Rosenberg), lateral, and sunrise views of the
knee in addition to full-length standing radiographs (Fig. 1). The sunrise view may be taken at
various degrees of flexion in order to evaluate for
patellar subluxation tilt, or femoral trochlear
dysplasia. Typically, 30 degrees of flexion is
sufficient [29]. The lateral view affords investigation for patellofemoral joint space, alignment,
and patellar size. The full-length standing radiographs allow for evaluation of complete lower
limb alignment. If desired, this can be further
investigated with CT scan or Magnetic Resonance Imaging for formal measurement of the
tibial tubercle-trochlear groove (TT-TG) distance
may assist in operative decision-making as it
relates to the need for tubercle osteotomy. In
order to create a preoperative template for use in
the robotic system, a CT scan must be obtained
in order to identify bony landmarks that can be
later referenced to ensure reproducible intraoperative findings.
4
Surgical Technique
4.1 Patient Positioning
The patient should be placed supine on the
operative table. A post of the surgeon’s preference is placed on the operative side to assist in
maintaining leg positioning while allowing for
747
full knee range of motion. The authors prefer to
utilize a nonsterile tourniquet and the limb is
prepped and draped in standard sterile fashion.
For robot positioning, the robotic arm is typically
positioned on the operative side to allow for
optimized and independent use by the surgeon.
The computer referencing monitor and stand is
placed on the opposing side. The monitor is
ideally placed at a comfortable and easily visible
location for the surgeon. It is imperative that the
nonoperative side of the patient is free of any
obstructions as a clear line of sight is required for
robotic tracking. The camera is angled toward the
operative knee, using laser alignment if available.
Lastly, the guidance module should be placed
where a robotic representative can easily maintain visibility of the surgeon.
4.2 Operative Technique
After induction of anesthesia, an examination
under anesthesia is performed to assess for range
of motion, patellar tracking, crepitation, and knee
stability. Prior to incision for arthroplasty, a
diagnostic arthroscopy (DA) should be performed. Standard anteromedial and anterolateral
portals are utilized to arthroscopically assess
each of the three knee compartments with a
special focus on evaluating the cartilage integrity. This scrutinization ensures that cartilage
integrity reflects that of preoperative imaging and
ensures that cartilage to the tibiofemoral articulation is preserved, thus not contraindicating
PFA. Additionally, diagnostic arthroscopy
allows for assessment of the soft tissues of the
knee, including the cruciate and collateral ligaments. Again, confirmation of isolated PFOA is
required prior to proceeding with PFA.
Upon completion of the diagnostic arthroscopy, a medial parapatellar approach to the joint
is initiated. This is started approximately 3 cm
above the superior pole of the patella and extends
distally to the tibial tubercle. In the MAKO
(Stryker, Kalamazoo, MI) system, two reference
pins are then inserted into the anterior femur
748
J. C. Brinkman et al.
A
B
C
Fig. 1 Isolated patellofemoral osteoarthritis plain radiographs as demonstrated on sunrise (A), lateral (B), and
anteroposterior (C) radiographs
Robotic-Assisted Patellofemoral Arthroplasty
749
Fig. 2 Mako guide pins attached through right femur with receiver in place
proximal to the incision percutaneously (Fig. 2).
Registering the femur may then be performed
utilizing the reference pins, allowing the robotic
system to overlay the intraoperative data with the
preoperative CT. Arthrotomy then allows further
visualization of the articular surface. Care is
taken to avoid disrupting the menisci, intermeniscal ligaments, and articular cartilage. The
infrapatellar and suprapatellar fat pads can be
partially removed to allow for lateral patellar
subluxation. Care should be taken to avoid
removing soft tissue medial to the patella in
anticipation of eventual soft tissue balancing.
Next, a rongeur can be utilized to remove any
visible osteophytes, soft tissue adhesions, or
chondral defects.
Mapping is started at the trochlea. Mapping is
achieved using both a blunt- and a sharp-tipped
probe and Knee End Effector Array (Fig. 3).
Calibration of these systems to ensure accurate
triangulation of the position of the probe is vital
for adequate intraoperative mapping of the joint.
Articular surfaces are mapped by marking points
with the sharp-tipped probe. Two points are
marked on the superior edge of the trochlea, one
medial and one lateral. Five points are marked
along the trochlear groove. Finally, three points
are marked on each side of the medial and lateral
transition zones. These points are matched with
preoperative CT. The sharp probe can be used to
push through the cartilage for accurate mapping,
as cartilage is not detected on the preoperative
CT scan.
Preoperative templating may then be adjusted
according to the intraoperative mapping that has
been performed. The robotic arm may then be
advanced into position over the operative field,
with centering of the robotic base at the patient’s
hip, located one to two meters away from the
operative table. The cutting handle is also
brought in and placed approximately 10 cm
directly above the knee joint. Once in position,
beginning with the burring arm, bone over the
trochlear surface is removed in accordance with
750
J. C. Brinkman et al.
A
B
Fig. 3 Intraoperative mapping of the patellofemoral joint. Mako Registration to sync to preoperative computed
tomography as seen from the navigation console
the future trochlear implant (Fig. 4). Of note, the
robotic burr does not allow removal of bone
outside of the templated plan. Implant lug holes
are created using the burr with special attention
to only plunge once to create lug holes in order to
avoid creating excessively large lug holes. The
trochlear implant may then be trialed to ensure
adequate sizing and smooth patellar tracking.
Robotic-Assisted Patellofemoral Arthroplasty
A
Fig. 4 The robotic arm guides preparation of the joint. A
Robotic arm in position for trochlear resection view from
professional representative’s monitor; B Trochlea status
Once the trochlear implant is appropriately in
place, attention is turned to the undersurface of
the patella. The everted patella should be measured for maximal thickness utilizing a caliper at
the lateral and medial aspects. For patellar sizing,
size is estimated by measuring the proximal–
distal height of the patellar articular surface. The
ideal patellar size is one that does not exceed the
inferior or superior margins. Patellar resurfacing
is then performed using a reamer or saw,
depending on surgeon preference. A patellar
reaming guide can be clamped in order to ensure
the spikes are fully seated and that the guide sits
flush. For optimized patellar tracking, the drill
guide should be placed medially on the patella.
In doing so, this will lateralize the remaining
patellar surface to avoid over-tightening of the
vastus lateralis and thereby decrease the risk of a
lateral subluxation force. Once in an acceptable
position, the peg holes are then drilled followed
by placement of the trial patellar component
(Fig. 5). Remeasurement of the patellar thickness
is performed to ensure appropriate remaining
thickness. Additionally, the knee can be taken
through range of motion with special attention to
751
B
postresection with retractors in soft tissue to allow for
visualization. Three peg hole burr cuts visible
Fig. 5 Final components in position
752
J. C. Brinkman et al.
patellar tracking and transitioning through flexion and extension.
Once the trials are deemed acceptable, they
are removed to allow for irrigation of the bony
surfaces. Cement can then be mixed and applied
to the trochlear implant and resected trochlear
notch. The trochlear implant is then placed and
impacted, followed by removal of excess cement.
The implant is manually held in place until the
cement is fully cured, as can be deemed by
manufacturing time or the hardening time of an
additional sample of cement. Cementation is then
performed of the resurfaced patella, peg holes,
and patellar implant. The patellar component is
then positioned and held in place by clamping to
allow for an adequate compression force of the
patellar implant. Again, excess cement is resected followed by clamp removal once fully cured.
The joint is then irrigated and taken through
another manual range of motion check. There
should be no patellar tilt or subluxation as the
knee is put through flexion and extension.
Arthrotomy closure is made using ethibond
figure-of-eight sutures followed by an additional
A
layer of #0 vicryl suture in a running locking
fashion. Again, soft tissue balancing and patellar
tracking is confirmed with range of motion.
Layered closure is then performed, with the
authors’ preference for #0 vicryl followed by #2–
0 vicryl sutures. Skin closure is typically performed with staples. A soft dressing is placed in
accordance with the surgeon’s preference.
5
Postoperative Course
Rehabilitation following robotic-assisted PFA
should follow the same protocol as manual PFA.
Weight-bearing as tolerated with an emphasis on
range of motion exercises may be initiated in the
immediate postoperative period, with gradual
increase in activity. Physical therapy may be
initiated based on surgeon preference within the
first 1–2 weeks. Patients are generally permitted
to stationary bike at 4 weeks, with gradual return
to full activity within 6–8 weeks. During follow
up, postoperative radiographs should include
standard anteroposterior, lateral, and merchant
B
Fig. 6 Postoperative A lateral and B anteroposterior plain radiographs
Robotic-Assisted Patellofemoral Arthroplasty
view imaging (Fig. 6). Alignment can be assessed with patellar symmetry, patellar tilt, and
subluxation distance [16].
6
Discussion
Robotic-assisted patellofemoral arthroplasty is a
viable approach to operative management of
isolated patellofemoral osteoarthritis. It offers
several unique advantages when compared to
manual PFS (Table 1). Pre-operative planning
using 3-dimensional reconstructed images allows
for more accurate appreciation of joint condition,
alignment, and eventual implant sizing. Intraoperative cartilage mapping then affords reproducible joint alignment and positioning. These
advantages may avoid sources of inconsistency
or error that could cause ongoing symptoms in
patients that undergo PFA.
Owing to the recency of the robotic application to PFA, outcome studies are few. Turktas
et al. examined 30 RA-PFA knees with a follow
up of 15.9 months. In this series, there were no
patients with patellar mal-tracking or misalignment. Additionally, there was a significant
increase in post-operative Oxford Knee Score
when compared preoperatively. Similar increases
in outcome scores were also demonstrated in a
study by Ackroyd et al. These studies suggest
that RA-PFA offers a reliable procedure that
affords patients predictable benefit in functional
outcomes. However, its associated limitations
should also be acknowledged. Longer term follow up studies are still needed in order to fully
753
assess the outcomes, survivability, and issues not
appreciable in shorter term follow up. Additionally, RA-PFA requires a significant financial
investment into the robot itself as well as preoperative CT scanning. This financial cost is
further increased at institutions that prefer to
always undergo arthroscopic evaluation of the
knee prior to PFA. Together, these capital costs
may limit its availability to all institutions.
7
Conclusion
Robotic-assisted patellofemoral arthroplasty is an
emerging treatment for isolated patellofemoral
arthritis. It has the potential to allow for more
accurate and anatomic implant sizing and positioning. Although further studies are required to
determine its long-term outcomes, it appears to
have favorable short-term survivability, outcomes, and joint alignment. Comparable studies
to non-robotic PFA will afford data that can be
utilized in cost–benefit analyses and to better
inform its future role.
8
Take Home Messages
• Patellofemoral arthritis is common and can be
a debilitating condition for which treatment
options typically include total or isolated
patellofemoral knee arthroplasty.
• Standard patellofemoral arthroplasty is associated with several issues including patellar
mal-tracking and inconsistent alignment.
Table 1 Advantages and Disadvantages of Robotic-Assisted Patellofemoral Arthroplasty
Advantages
Implant design and fixation more anatomical than previous systems
Reduced malalignment and mal-tracking
Short-term follow-up positive
Disadvantages
Long-term follow-up not yet available
Capital investment and operating costs for robot are significant
Preoperative CT scan required
Note CT: Computed tomography
754
J. C. Brinkman et al.
• Robotic-assisted patellofemoral arthroplasty
was recently developed in order to address
issues with standard arthroplasty and allows
for patient-specific templating for implant
size, alignment, and positioning.
• Outcomes of robotic patellofemoral arthroplasty are promising and demonstrate low
rates of malalignment and mal-tracking in
addition to encouraging outcome scores
• Several operative pearls including avoiding
oblique reference pins, achieving appropriate
soft tissue balancing, and checking for lateral
facet deficiency are key to reliable outcomes.
• Further longer-term studies will assist in full
analysis of the outcomes, results, and cost–
benefit nature of robotic patellofemoral
arthroplasty.
9
Key Message
• Robotic patellofemoral arthroplasty appears to
be a reproducible, beneficial, and feasible
treatment for isolated patellofemoral arthritis.
Acknowledgements Figures adapted from Elsevier Inc.
https://doi.org/10.1016/j.eats.2019.11.013.
References
1. Davies AP, Vince AS, Shepstone L, Donell ST,
Glasgow MM. The radiologic prevalence of patellofemoral osteoarthritis. Clin Orthop Relat Res.
2002;402:206–12.
2. Grelsamer RP, Stein DA. Patellofemoral arthritis.
J Bone Joint Surg Am. 2006;88(8):1849–60.
3. Sisk D, Fredericson M. Taping, bracing, and injection treatment for patellofemoral pain and patellar
tendinopathy. Curr Rev Musculoskelet Med. 2020;13
(4):537–44.
4. Strickland SM, Bird ML, Christ AB. Advances in
patellofemoral arthroplasty. Curr Rev Musculoskelet
Med. 2018;11(2):221–30.
5. Mckeever DC. Patellar prosthesis. J Bone Joint Surg
Am. 1955 (5):1074–84.
6. Lubinus HH. Patella glide bearing total replacement.
Orthopedics. 1979;2(2):119–27.
7. Blazina ME, Fox JM, Del Pizzo W, Broukhim B,
Ivey FM. Patellofemoral replacement. Clin Orthop
Relat Res. 1979;144:98–102.
8. Tauro B, Ackroyd CE, Newman JH, Shah NA. The
Lubinus patellofemoral arthroplasty. A five- to tenyear prospective study. J Bone Joint Surg Br.
2001;83(5):696–701.
9. Kooijman HJ, Driessen APPM, van Horn JR. Longterm results of patellofemoral arthroplasty. A report
of 56 arthroplasties with 17 years of follow-up.
J Bone Joint Surg Br. 2003;85(6):836–40.
10. Krajca-Radcliffe JB, Coker TP. Patellofemoral
arthroplasty. A 2- to 18-year followup study. Clin
Orthop Relat Res. 1996 Sep;(330):143–51.
11. van der List JP, Chawla H, Zuiderbaan HA,
Pearle AD. Survivorship and functional outcomes
of patellofemoral arthroplasty: a systematic review.
Knee Surg Sports Traumatol Arthrosc. 2017;25
(8):2622–31.
12. Deckey DG, Rosenow CS, Verhey JT, Brinkman JC,
Mayfield CK, Clarke HD, et al. Robotic-assisted total
knee arthroplasty improves accuracy and precision
compared to conventional techniques. Bone
Joint J. 2021;103-B(6 Supple A):74–80.
13. Cobb J, Henckel J, Gomes P, Harris S, Jakopec M,
Rodriguez F, et al. Hands-on robotic unicompartmental knee replacement: a prospective, randomised
controlled study of the acrobot system. J Bone Joint
Surg Br. 2006;88(2):188–97.
14. Law J, Hofmann A, Stevens B, Myers A. Patellofemoral arthroplasty technique: Mako. In: Lonner JH,
editor. Robotics in Knee and Hip Arthroplasty:
Current Concepts, Techniques and Emerging Uses
[Internet]. Cham: Springer International Publishing;
2019 [cited 2021 Nov 13]. p. 115–22. Available
from: https://doi.org/10.1007/978-3-030-16593-2_12
.
15. Turktas U, Piskin A, Poehling GG. Short-term
outcomes of robotically assisted patello-femoral
arthroplasty. Int Orthopaedics (SICOT). 2016;40
(5):919–24.
16. Dahm DL, Al-Rayashi W, Dajani K, Shah JP,
Levy BA, Stuart MJ. Patellofemoral arthroplasty
versus total knee arthroplasty in patients with isolated
patellofemoral osteoarthritis. Am J Orthop (Belle
Mead NJ). 2010;39(10):487–91.
17. Laskin RS, van Steijn M. Total knee replacement for
patients with patellofemoral arthritis. Clin Orthop
Relat Res. 1999;367:89–95.
18. Odumenya M, McGuinness K, Achten J, Parsons N,
Spalding T, Costa M. The Warwick patellofemoral
arthroplasty trial: a randomised clinical trial of total
knee arthroplasty versus patellofemoral arthroplasty
in patients with severe arthritis of the patellofemoral
joint. BMC Musculoskelet Disord. 2011;12(1):265.
19. Leadbetter WB, Ragland PS, Mont MA. The appropriate use of patellofemoral arthroplasty: an analysis
of reported indications, contraindications, and failures. Clin Orthop Relat Res. 2005;436:91–9.
Robotic-Assisted Patellofemoral Arthroplasty
20. Woon CYL, Christ AB, Goto R, Shanaghan K,
Shubin Stein BE, Gonzalez Della Valle A. Return to
the operating room after patellofemoral arthroplasty
versus total knee arthroplasty for isolated patellofemoral
arthritis-a
systematic
review.
Int
Orthop. 2019;43(7):1611–20.
21. Begum FA, Kayani B, Morgan SDJ, Ahmed SS,
Singh S, Haddad FS. Robotic technology: current
concepts, operative techniques and emerging uses in
unicompartmental knee arthroplasty. EFORT Open
Rev. 2020;5(5):312–8.
22. Kayani B, Konan S, Huq SS, Tahmassebi J, Haddad FS. Robotic-arm assisted total knee arthroplasty
has a learning curve of seven cases for integration
into the surgical workflow but no learning curve
effect for accuracy of implant positioning. Knee Surg
Sports Traumatol Arthrosc. 2019;27(4):1132–41.
23. Mahure SA, Teo GM, Kissin YD, Stulberg BN,
Kreuzer S, Long WJ. Learning curve for active
robotic total knee arthroplasty. Knee Surg Sports
Traumatol Arthrosc. 2021.
24. Walker T, Perkinson B, Mihalko WM. Patellofemoral arthroplasty: the other unicompartmental knee
replacement. J Bone Joint Surg Am. 2012;94
(18):1712–20.
755
25. Lonner JH. Patellofemoral arthroplasty. J Am Acad
Orthop Surg. 2007;15(8):495–506.
26. Delanois RE, McGrath MS, Ulrich SD, Marker DR,
Seyler TM, Bonutti PM, et al. Results of total knee
replacement for isolated patellofemoral arthritis:
when not to perform a patellofemoral arthroplasty.
Orthop Clin North Am. 2008;39(3):381–8, vii.
27. Leadbetter WB, Seyler TM, Ragland PS, Mont MA.
Indications, Contraindications, and Pitfalls of Patellofemoral Arthroplasty. JBJS. 2006;88(suppl_4):
122–37.
28. Sabatini L, Schirò M, Atzori F, Ferrero G, Massè A.
Patellofemoral joint arthroplasty: our experience in
isolated patellofemoral and bicompartmental arthritic
knees. Clin Med Insights Arthritis Musculoskelet
Disord. 2016;9:189–93.
29. Iwano T, Kurosawa H, Tokuyama H, Hoshikawa Y.
Roentgenographic and clinical findings of patellofemoral osteoarthrosis. With special reference to its
relationship to femorotibial osteoarthrosis and etiologic factors. Clin Orthop Relat Res. 1990;
(252):190–7.
Modern Patellofemoral Inlay
Arthroplasty—A Silver Lining
in the Treatment of Isolated
Patellofemoral Arthritis
Marco-Christopher Rupp, Jonas Pogorzelski,
and Andreas B. Imhoff
1
Key Notes
• Contemporary patellofemoral inlay arthroplasty demonstrates high patient satisfaction
with significant improvements in knee function and pain relief while avoiding progression
of tibiofemoral arthritis at mid-term follow-up.
• Patient selection is the key to success.
• In patients with significant trochlea dysplasia
or with (minor) rotational malalignment, an
onlay prosthesis might be beneficial as its
design addresses those factors better than an
inlay design.
2
Introduction
Isolated patellofemoral osteoarthritis (PFOA) is a
complex and multifactorial pathology. Primary OA of the patellofemoral joint is a relatively rare entity and is defined as isolated OA to
the patellofemoral joint without concomitant or
underlying pathologies in the sense of tibiofemoral malalignment or patellofemoral instability.
Secondary OA however is much more common
M.-C. Rupp J. Pogorzelski A. B. Imhoff (&)
Department of Orthopaedic Sports Medicine,
Hospital Rechts der Isar, Technical University of
Munich, Munich, Germany
e-mail: imhoff@tum.de
and is the result of non-physiologic patellofemoral biomechanics, e.g. due to trochlear dysplasia or axial/torsional malalignment of the
femur and tibia with subsequent maltracking of
the patella or patellofemoral instability.
With multiple etiological factors exhibiting a
combined effect on the biomechanical and clinical outcome following PFIA, the surgical management for PFOA is part of a nuanced
therapeutical concept and should be viewed in
the context of concomitant pathologies.
Patellofemoral inlay arthroplasty (PFIA) as a
design variant of patellofemoral arthoplasty was
first described in the literature in 1979 [1]. In
principle, the idea behind the PFIA design was to
retain the anatomy of the trochlea and replace
only the degenerated part of the cartilage without
having to perform a more invasive resection of
the subchondral bone. The trochlear component
was inserted flush with the surrounding cartilage
of the trochlea (“inlay”). However, the first
results of these arthroplasty models led to high
failure rates due to the suboptimal geometry of
these models [2, 3] A trochlear groove that was,
by design, non-physiologically deep and an
insufficient mediolateral coverage of the trochlea
in the first arthroplasty models often resulted in
patellofemoral maltracking with persistent pain
and additional patellofemoral instability [2, 3].
Based on these experiences, novel surgical
techniques and a new generation of inlay
arthroplasty models have been developed in
recent years (Fig. 1).
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_59
757
758
M.-C. Rupp et al.
Fig. 1 Modern patellofemoral inlay prosthesis (Kahuna Prosthesis, Arthrosurface, Franklin, MA, USA)
However, as PFOA is a multifactorial pathology, concomitant soft-tissue and bone-based
reconstructive procedures have to be considered
during conception of the surgical plan. In the case
of accompanying malalignment of the femur,
surgical procedures such as alignment corrective
osteotomies to optimize mechnical leg alignment
and patellofemoral tracking [4] may be indicated,
since performing an isolated PFIA may not be
fully able to restore physiological alignment.
Compared to total knee arthroplasty (TKA) in the
treatment of isolated PFOA, the procedure is
relatively minimal invasive and the tibiofemoral
joint compartments can be preserved during the
PFIA procedure [5–7]. Lower intraoperative
morbidity, shorter intraoperative tourniquet times
and a shorter rehabilitation time in young patients
postoperatively [8–10] typically result in
improved mobility and extension strength of the
knee joint with a comparable postoperative satisfaction compared with TKA [7, 8, 11, 12]. Since
the PFIA can also be converted to a TKA in cases
where the tibiofemoral OA progresses [9], the
implantation of a modern PFIA is a viable therapeutic alternative to TKA, especially in younger
patients.
This chapter aims to provide an overview of
the indications and contraindications for PFIA
and recommendations for clinical practice.
3
Indication
PFIA is indicated in patients suffering from isolated disabling PFOA with minimum grade III–
IV (Kellgren-Lawrence classification) or chondral defects grade III–IV (Outerbridge classification) that refractory to conservative treatment
and/or failed prior surgery. Performing an isolated PFIA is generally reserved for patients
without patellofemoral instability. High-grade
patellofemoral or tibiofemoral malalignment as
defined by a mechanical valgus or varus of more
than 5°; a femoral anteversion of more than 30°;
a tibial torsion of more than 40°; a tibial
tuberosity trochlear groove distance of more than
20 mm or less than 8 mm; a Caton-Deschamps
Index of more than 1.2 or less than 0.8; or a
lateral patellar tilt of more than 5° should be
managed according to a previously published
algorithm [4] additionally to the implantation of a
PFIA.
4
Contraindication
Contraindications for PFIA implantation are
symptomatic tibiofemoral OAwith pain at the
joint line during activities of daily living, chronic
Modern Patellofemoral Inlay Arthroplasty …
759
regional pain syndrome, active infection,
inflammatory arthropathy, chondrocalcinosis,
and a fixed loss of knee range of motion.
5
Surgical Technique
Contemporary inlay arthoplasty models typically
consist of a cobalt chrome trochlear component
that is connected to a titanium taper post via a
taper interlock and an (optional) additional allpolyethylene patella component. Most systems
are distributed with multiple implant sizes with
varying offsets to facilitate a patient-specific
geometry match. All inlay prostheses are
designed to be implanted flush with the surrounding cartilage into a bone bed within the
native trochlea sparing the femoral bone stock
(Fig. 2). Typically, inlay arthroplasty models
include a trochlear groove that narrows distally to
allow for sufficient patella tracking without
causing lateral hypercompression of the patella.
Compared to an onlay design, the more anatomic
principle of the inlay design closely reproduces
the complex patellofemoral kinematics. By desing, this avoids soft tissue irritation due to
patellofemoral overstuffing, which is an accepted
risk factor for the development and progression
of tibiofemoral OA due to secretion of proinflammatory cytokines [13].
The arthroplasty procedure is performed
according to the specific manufacturers instructions. Typically, the PFIA procedure is performed via a minimally invasive lateral
parapatellar approach to spare the medial patellastabilizing soft tissue structures. A further
advantage of the lateral approach is that overhanging patellar osteophytes, that are typically
located laterally, can be resected without compromising the approach to the trochlea for the
implantation of the PFIA. An offset drill guide is
used to correctly localize the center for the
reamer with the knee in full extension. In principle, the correct placement for the drill guide is
located at the center of the trochlear articular
surface to confirm trochlear defect coverage
(Fig. 3). A guide pin is advanced into the bone,
Fig. 2 Second-Generation patellofemoral inlay arthroplasty model (WAVE Prosthesis, Arthrosurface, Franklin,
MA, USA) implanted flush with the surrounding cartilage
after creation of a bone bed within the native trochlea
Fig. 3 An offset drill guide is used to establish a working
axis prependicular to the central trochlear articular surface
and to confirm trochlear defect coverage
once the superior and inferior drill guide feet are
optimally aligned with the trochlear orientation.
In order determine the adequate implant size, the
760
M.-C. Rupp et al.
fixation stud. Finally, the trochlear component is
positioned using an impactor.
Subsequently, debridement of patellar osteophytes, circumpatellar denervation and resurfacing of the patella are performed. To replace the
patellar surface, a drill guide is inserted emplyoing an alignment guide. The medial/lateral and
superior/inferior offsets are measured and an
implant bed is reamed. The patellar component is
then mounted onto the implant holder and
cemented into the bone bed. Postoperative
radiographs in three planes are obtained routinely
to confirm optimal implant positioning. (Fig. 6).
6
Fig. 4 The implant bed is reamed employing a guide
block
medial/lateral as well as superior/inferior offsets
are measured using specific measurement
instrumentation. Next, the implant bed is reamed
three-dimensionally using a guide block (Figs. 4
and 5). Subsequently, the screw fixation stud is
advanced into the bone. The trochlear component
is then aligned with the appropriate offsets of the
implant holder and placed onto the taper of the
Rehabilitation
All patients are discharged once they are able to
flex the knee joint to a minimum of 90° and can
climb stairs on crutches safely. All patients are
limited to partial weight bearing with 20 kg for
two weeks until the healing process of the soft
tissue is consolidated. Early rehabilitation
includes lymphatic drainage and continuous
passive motion for the first two weeks as tolerated. Patients are then allowed to increase weight
bearing in a step-wise fashion until full weight
Fig. 5 The correct positioning of the implant is confirmed by positioning of a trial implant that will be used for
positioning the tape post
Modern Patellofemoral Inlay Arthroplasty …
761
Fig. 6 Postoperative radiographs of the inlay implant in three planes routinely obtained to confirm implant positioning
bearing is achieved approximately six weeks
after surgery. Full active range of motion is
typically allowed two weeks after surgery.
7
Clinical Outcome
The results after PFIA are mainly influenced by
the patient selection, the surgical technique and
the arthroplasty design. Early complications are
common and mainly caused by implant misplacement and/or postoperative patella maltracking or patellofemoral instability, while longterm failures are mainly the result of progression
of tibiofemoral osteoarthritis.
An adequate patient selection may be the key
factor in achieving favorable outcomes following
PFIA. As such—according to the current state of
knowledge—risk factors for inferior clinical
outcome include an increased body mass index
(BMI) prior surgery, an etiology of primary
PFOA as compared to secondary PFOA, presence
of degenerative changes in the tibiofemoral joint
compartments, lack of retropatellar resurfacing
during the PFIA procedure as well persistent
patellofemoral instability and malalignment following the PFIA procedure [14–17].
As of biomechanical studies, peak pressure
following patellofemoral arthroplasty significantly increases compared to the native joint [5,
18]. As such, if patellar resurfacing is not performed at index surgery, non-physiological
pressure conditions may predispose for an abrasion of the native patellar cartilage in contact
with the inlay arthroplasty [5]. This may consequently lead to a progression of retropatellar
cartilage degeneration resulting in pain as wells
as poor postoperative results and may require
revision surgery. This finding was confirmed by
a multi-center case series, in which the lack of
patellofemoral resurfacing at the index surgery
was significantly correlated with failure [16].
Interestingly, the presence of primary OA of
the patellofemoral joint also seems to be a risk
factor for inferior outcome after implantation of a
PFIA as compared to patients with secondary
PFOA. In this regard, a prospective case series
reported that there is a significant progression of
tibiofemoral OA in patients with primary PFOA
while the tibiofemoral compartments remains
762
relatively unchanged in patients undergoing
PFIA for secondary PFOA [15]. Patients with
secondary PFOA due to patellofemoral instability, in which the anatomical risk factors predisposing for patellofemoral instability were
addressed during PFIA implantation, were shown
to benefit significantly more from undergoing
PFIA than patients with primary PFOA [15].
Potentially patients with primary OA are more
prone to degenerative changes in the tibiofemoral
joint compartments as part of the inflammatory
reactions that occurs within the joint during primary OA [13]. This is in accordance with subsequent outcome studies that reported
significantly better results following PFIA in the
presence of secondary OA due to trochlear dysplasia with concomitant patellofemoral instability
[19–21].
An increased BMI was identified as a further
independent factor in PFIA predictive of unfavorable clinical outcome postoperatively [16,
22]. As such, obesity may lead to rapid progression of tibifemoral OA and predispose for an
early conversion to TKA. According to the current literature, this is still the main reason for the
failure of PFIA [14, 17, 23].
When respecting these risk factors during
patient selection, the PFIA procedure is a viable,
minimally invasive alternative to the traditional
TKA procedure for isolated PFOA. In a study
regarding the midterm outcome following PFIA
[24], the patient reported outcome scores
improved significantly both at short- and midterm follow up with no significant difference
between the two time points. In this case series,
17.1% of the patients failed leaving a survival
rate of 83% after five years, reflecting the early
experiences with modern generation PFIA. In
patients who did not fail, no changes in the
vertical patellar alignment or significant progression of tibiofemoral OA were observed until
final follow up. The main mode of failure
reported in this case series was persistent knee
pain. An independent case series on the early
experiences of modern generation PFIA, who
evaluated the outcome after a mean follow-up of
35 months following PFIA, confirmed the
promising
clinical
outcome.
Significant
M.-C. Rupp et al.
improvements were observed across all patient
reported outcome measures and similarly, no
radiological progression of tibiofemoral OA was
noted. Around 10% of the patients were converted to TKA, again with persistent pain being
the main reason for failure.
In the largest series to date, including a total
of 263 patients (49 ± 12 years) at mid-term
follow-up, 93% of the patients included in the
final analysis were satisfied with the procedure
with a mean transformed WOMAC Score of
84.5 ± 14.5 points, a mean KOOS Score of
73.3 ± 17.1 points, a mean Tegner Score
of 3.4 ± 1.4 points and a mean VAS pain of
2.4 ± 2.0 points. With an overall failure rate was
11% (28 patients), the authors concluded that
PFIA shows high patient satisfaction with good
functional outcomes at short- to mid-term followup.
However, the outcomes reported following
isolated PFIA are heterogenous throughout the
literature. In a prospective case series of 18
patients [25], a significant progression of OA in
the medial tibiofemoral compartment caused a
total of 5 implants (28%) to fail within six years.
However, even when acknowledging for this
high failure rate, clinically significant improvements were observed for clinical and functional
outcomes; with an improvement in the the
American Knee Society Subjective Score
(AKSS) of more than 20 points in 91% of the
patients. The relatively high revision rate reported in this case series [25] highlights the necessity for careful preoperative patient selection.
A recent review article analyzing the clinical
outcome following patellofemoral arthroplasty
depending on the size of the respective center
proposed found that the outcome in specialized
centers with substantial cumulative experience
with the procedure may be superior, highlighting
the multifactorial complexity of the management
of PFOA [26].
This notion is highlighted retrospective cohort
of 20 patients who underwent PFIA. 55% of the
patients with an increased patellofemoral congruence angle and an elevated Insall–Salvati
index and showed an initial satisfactory result,
but failed due to pain during follow-up after a
Modern Patellofemoral Inlay Arthroplasty …
median time of 25 months. Beckmann et al.
concluded that patients with craniolateral types
of PFOA as well as a patella alta should be
treated with an patellofemoral onlay arthroplasty,
as this type of implant is superior in covering the
proximal part of the patellar track as compared to
the PFIA design [27].
Accordingly, Feucht et al. [28] found that
preoperative patellofemoral anatomy is significantly associated with clinical improvement and
failure rate after isolated inlay PFA. It was
demonstrated that less clinical improvement and
a higher failure rate must be expected in patients
with patella alta (ISI > 1.2 and PTI < 0.28),
absence of trochlear dysplasia, and a lateralized
position of the tibial tuberosity (TT-PCL distance > 21 mm), further highlighting the necessity for an adequate patient selection for the PFIA
procedure [28].
Overall, when respecting risk factors associated with inferior outcomes during a concise
diagnostic work-up and careful patient selection
process, PFIA implantation has been shown to be
a viable, minimally invasive alternative to TKA
in the treatment of PFOA. Yet, future studies
reporting on the the long-term outcome following PFIA are required and further research is
necessary to define risk factors for failure or
insufficient clinical improvement following
PFIA.
References
1. Blazina ME, et al. Patellofemoral replacement. Clin
Orthop Relat Res. 1979;144:98–102.
2. Borus T, et al. Patellofemoral joint replacement, an
evolving concept. Knee. 2014;21(Suppl 1):S47-50.
3. Cartier P, Sanouiller JL, Khefacha A. Long-term
results with the first patellofemoral prosthesis. Clin
Orthop Relat Res. 2005;436:47–54.
4. Imhoff AB, et al. Prospective evaluation of anatomic
patellofemoral inlay resurfacing: clinical, radiographic, and sports-related results after 24 months.
Knee Surg Sports Traumatol Arthrosc. 2015;23
(5):1299–307.
5. Vandenneucker H, et al. Isolated patellofemoral
arthroplasty reproduces natural patellofemoral joint
kinematics when the patella is resurfaced. Knee Surg
Sports Traumatol Arthrosc. 2016;24(11):3668–77.
763
6. Tanikawa H, et al. Influence of total knee arthroplasty on patellar kinematics and patellofemoral
pressure. J Arthroplasty. 2017;32(1):280–5.
7. Odgaard A, et al. The mark coventry award:
patellofemoral arthroplasty results in better range of
movement and early patient-reported outcomes than
TKA. Clin Orthop Relat Res. 2018;476(1):87–100.
8. Dahm DL, et al. Patellofemoral arthroplasty versus
total knee arthroplasty in patients with isolated
patellofemoral osteoarthritis. Am J Orthop (Belle
Mead NJ). 2010;39(10):487–91.
9. van Jonbergen HP, Werkman DM, van Kampen A.
Conversion of patellofemoral arthroplasty to total
knee arthroplasty: a matched case-control study of 13
patients. Acta Orthop. 2009;80(1):62–6.
10. Kamikovski I, Dobransky J, Dervin GF. The clinical
outcome of patellofemoral arthroplasty vs total knee
arthroplasty in patients younger than 55 years.
J Arthroplasty. 2019;34(12):2914–7.
11. Walker T, Perkinson B, Mihalko WM. Patellofemoral arthroplasty: the other unicompartmental knee
replacement. J Bone Joint Surg Am. 2012;94
(18):1712–20.
12. Dy CJ, et al. Complications after patello-femoral
versus total knee replacement in the treatment of
isolated patello-femoral osteoarthritis. A metaanalysis. Knee Surg Sports Traumatol Arthrosc,
2012;20(11):2174–90.
13. Kapoor M, et al. Role of proinflammatory cytokines
in the pathophysiology of osteoarthritis. Nat Rev
Rheumatol. 2011;7(1):33–42.
14. van der List JP, et al. Survivorship and functional
outcomes of patellofemoral arthroplasty: a systematic
review. Knee Surg Sports Traumatol Arthrosc.
2017;25(8):2622–31.
15. Beitzel K, et al. Prospective clinical and radiological
two-year results after patellofemoral arthroplasty
using an implant with an asymmetric trochlea design.
Knee Surg Sports Traumatol Arthrosc. 2013;21
(2):332–9.
16. Imhoff AB, et al. The lack of retropatellar resurfacing
at index surgery is significantly associated with
failure in patients following patellofemoral inlay
arthroplasty: a multi-center study of more than 260
patients. Knee Surg Sports Traumatol Arthrosc, 2021.
17. Bendixen NB, Eskelund PW, Odgaard A, Failure
modes of patellofemoral arthroplasty-registries vs.
clinical studies: a systematic review. Acta Orthop,
2019;90(5):473–478.
18. Calliess T, et al. Patella tracking and patella contact
pressure in modular patellofemoral arthroplasty: a
biomechanical in vitro analysis. Arch Orthop Trauma
Surg. 2016;136(6):849–55.
19. Dahm DL, et al. Patellofemoral arthroplasty: outcomes and factors associated with early progression
of tibiofemoral arthritis. Knee Surg Sports Traumatol
Arthrosc. 2014;22(10):2554–9.
20. Nicol SG, et al. Arthritis progression after patellofemoral joint replacement. Knee. 2006;13(4):290–5.
764
21. Feucht MJ, et al. Preoperative patellofemoral anatomy affects failure rate after isolated patellofemoral
inlay arthroplasty. Arch Orthop Trauma Surg, 2020.
22. Liow MH, et al. Obesity and the absence of trochlear
dysplasia increase the risk of revision in patellofemoral arthroplasty. Knee. 2016;23(2):331–7.
23. van Jonbergen HP, et al. Long-term outcomes of
patellofemoral arthroplasty. J Arthroplasty. 2010;25
(7):1066–71.
24. Imhoff AB, et al. High patient satisfaction with
significant improvement in knee function and pain
relief after mid-term follow-up in patients with
isolated patellofemoral inlay arthroplasty. Knee Surg
Sports Traumatol Arthrosc, 2018.
25. Laursen JO. High mid-term revision rate after
treatment of large, full-thickness cartilage lesions
M.-C. Rupp et al.
and OA in the patellofemoral joint using a large inlay
resurfacing prosthesis: HemiCAP-Wave(R). Knee
Surg Sports Traumatol Arthrosc. 2017;25
(12):3856–61.
26. Benignus C, et al. When nothing else works:
patellofemoral joint arthroplasty. Sportverletz Sportschaden. 2021;35(4):227–33.
27. Beckmann J, et al. Patella alta and patellar subluxation might lead to early failure with inlay patellofemoral joint arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2019;27(3):685–91.
28. Feucht MJ, et al. Preoperative patellofemoral anatomy affects failure rate after isolated patellofemoral
inlay arthroplasty. Arch Orthop Trauma Surg.
2020;140(12):2029–39.
Virtual Orthopaedic Examination
in Patellofemoral Disorders
Casey L. Wright and Miho J. Tanaka
1
Introduction
Telehealth (also referred to as telemedicine or
virtual care) is a rapidly emerging field encompassing a wide range of care paradigms utilizing
electronic platforms to provide healthcare services. Telehealth models include triage, radiographic assessment, remote monitoring devices,
“store-and-forward” telehealth, asynchronous
care, an “at-home” model, and a “regional-hub”
model [1]. Virtual musculoskeletal care has primarily been provided through the latter two
models. In the “at-home” model, physicians
connect directly with patients via a virtual platform to provide healthcare services. Studies
comparing at-home telehealth and in-person care
demonstrate the success of telehealth in diagnosing and treating a variety of musculoskeletal
problems. A study of face-to-face and telehealth
visits conducted on the same day for 42 patients
with chronic shoulder, knee, or lumbar spine
issues demonstrated 83.3% diagnostic and management agreement with an 89% patient satisfaction rating [2].
Despite such encouraging results, prior to the
COVID-19 pandemic, telehealth historically
C. L. Wright M. J. Tanaka (&)
Department of Orthopaedic Surgery, Massachusetts
General Hospital, Harvard Medical School, Boston,
MA 02114, USA
e-mail: mtanaka5@mgh.harvard.edu
played only a small role in orthopaedic practices.
The unanticipated global spread of severe acute
respiratory syndrome coronavirus 2 (SARSCoV2), however, accelerated reliance on telehealth within orthopaedic surgery to enable surgeons
to
continue
providing
routine
musculoskeletal care during a period in which inperson evaluation was limited to urgent or
emergent issues [3]. King and colleagues, who
detailed their department’s telehealth implementation process during the pandemic-enforced
restrictions, expanded the use of telehealth from
0.4 to 76% of their daily encounters [4]. Early
studies evaluating the ability of virtual visits to
develop appropriate surgical plans validate the
quality of telehealth care. Within sports medicine
surgeries, only 4% of surgical plans formulated
during telemedicine visits subsequently changed
during in-person re-evaluation [5].
In the evaluation of patellofemoral disorders,
the diagnoses rely heavily on history and physical examination. When converting the patellofemoral evaluation to a virtual encounter over
telemedicine, adaptations to known examination
techniques can be considered. Several orthopaedic departments who have published their experience with the rapid implementation of
telehealth have advocated for a consistent,
structured approach to promote the efficiency and
success of the virtual encounter, with instructions
for patients to review prior to the visit [1, 4, 6].
Virtual assessments can be augmented with
the use of digital measurements or goniometers
© The Author(s), under exclusive license to Springer Nature Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6_60
765
766
C. L. Wright and M. J. Tanaka
and can be performed either within a telemedicine platform or through a screen capture
process. Virtual goniometers are an effective tool
to standardize measurements across patients and
are available in a variety of formats. They are
available as browser extensions (Protractor, ben.
builingham),
smartphone
applications
(DrGoniometer, CDM s.r.l., Milano, Italy [7]),
and through the use of a standard goniometer
during a virtual visit, including to assess a
screen-captured image [8]. Virtual goniometers
demonstrate compatibility with multiple telehealth platforms utilized as a browser extension
[6]. Several studies have demonstrated high
reliability in range of motion measurements
obtained virtually [7–10]. Dent and colleagues
reported success with the use of a standard
clinical goniometer to assess individuals during
virtual encounters, which is applicable regardless
of telemedicine platform [8]. They noted high
agreement between elbow flexion and extension
measurements taken during an in-person
encounter and when using the same goniometer
during a teleconference (Pearson coefficient in
flexion: 0.93, in extension: 0.86). Some studies
suggest digital knee range of motion assessments
using still images have equivalent accuracy and
increased precision compared to both visual
assessment and standard goniometry [11, 12].
The goals of this chapter are to highlight the
considerations when performing evaluation of
the patellofemoral joint through a telemedicine
visit. We discuss the examination workflow,
modifications of standard examination maneuvers, benefits and limitations of the virtual visit,
as well as guidelines for optimizing the efficiency
and efficacy of the virtual examination.
2
Preparation for the Telemedicine
Visit
Preparation for the telemedicine visit by both the
patient and physician are integral to ensuring a
successful and efficient visit. Protocols for the
virtual visit, including payment policies, consent,
technology requirements, and instructions for the
visit, should be discussed at the time of scheduling.
X-rays performed in advance of the visit should be
made available for review prior to or at the time of
the visit. If images are performed at a facility
outside of one’s institution, those images should
be submitted in advance so they may be uploaded
for review prior to the start of the encounter.
Adequate audiovisual capabilities on the part
of the patient can significantly improve the
quality and flow of the examination. Patients can
be instructed to visit a remote verification site to
confirm they have the appropriate software and
audiovisual capabilities to participate in the
appointment. Educational materials sent to the
patient in anticipation of the virtual visit should
set appropriate expectations and include written,
photographic, or video instructions of the physical examination maneuvers to be performed
(Tables 1 and 2) Instructions provided in advance
of the visit allows patients to familiarize themselves with the upcoming examination, advises
of the expectations of the patient during the visit,
and allows the patient to prepare for the visit. A
standardized protocol for both the preparation for
and performance of the virtual visit can improve
the diagnostic accuracy and efficiency of the
evaluation.
3
Inspection
Similar to in an in-person evaluation, the virtual
examination begins with inspection, which can
be easily performed with the patient standing and
facing the camera. Thorough inspection should
note skin changes, erythema, incisions, scars, and
the presence of an effusion. Asymmetries in
patellar position, or muscle bulk and tone may be
noted. As with other musculoskeletal assessments, it is helpful to utilize the contralateral leg
as a control throughout the examination. However, physicians should be mindful that many
patients with patellofemoral disorders may have
bilateral involvement, which may influence
examination findings [13, 14]. In a recent randomized control trial of 112 patients with patellofemoral pain syndrome, Hott and colleagues
Virtual Orthopaedic Examination in Patellofemoral Disorders
767
Table 1 Example of patient instructions to prepare for a virtual visit (Adapted from Tanaka et al. JBJS 2020 [6])
How to prepare for a virtual visit
After speaking with a physician or provider regarding your symptoms, he or she will guide you through a physical
examination. To improve the success of the visit, please ensure you conduct the virtual appointment in a space that
allows for the following:
Privacy: Please conduct the visit in a quiet space with minimal background noise in which you are able to speak
privately with your physician regarding your health concerns
Space: The visit should be conducted in a space that allows for the camera to be positioned 6 feet (1.8 m) in front of
you on a low surface (2–3 feet off the ground), such as a chair or low table. This allows for appropriate visualization of
your knees during the examination. Sufficient floor space for 6–8 strides should be available for assessment of your
gait
Camera: The camera should be positioned on a table top or chair such that it does not need to be held during the
encounter, yet can be repositioned as needed throughout the examination
Lighting: Adequate lighting is crucial to ensure your provider is able to visualize the necessary details of the physical
examination. Please minimize backlighting by facing the camera away from windows and light sources
Seating: It is best to utilize a swivel chair or easily moveable chair during the examination that will allow you to
transition from facing the camera to having your side facing the camera. The physician will also need to evaluate you
while you are lying down, so it is necessary to either have a couch or adequate floor space available for you to lie
down
Clothing: For appropriate visualization, please wear shorts that end 3″ above your knees and remove your shoes and
socks
Table 2 Summary and workflow for the virtual patellofemoral examination
The virtual examination
Seated in chair
Inspection (frontal view)
• Skin changes, erythema, incisions, scars, effusion
• Asymmetries in patellar position, muscle bulk, tone
Palpation (frontal view)
• Tibial tubercle, patellar tendon, quadriceps tendon insertion, medial and lateral patellar
facets, medial and lateral joint lines, medial and lateral femoral condyles, medial and
lateral collateral ligaments
• Adductor tubercle (“Bassett’s sign”)
Patellar Instability (frontal view)
• J sign
• Patellar apprehension
• Patellar glide
Range of Motion
• Hip internal and external rotation (frontal view)
• Hip flexion with upper extremity assistance (lateral view)
• Knee flexion and extension (lateral view)
Muscle Strength (lateral view)
• Knee extension
• Extensor lag
• Hip extension – rise from seated without upper extremity support
Foot Pronation (lateral view)
Standing
Gait
Hypermobility (Beighton scale) (frontal view)
Lower Extremity Alignment (frontal view)
• Leg lengths, muscular atrophy
• Q angle
• Genu valgum, tibial tubercle lateralization, tibial torsion, femoral anteversion
(continued)
768
C. L. Wright and M. J. Tanaka
Table 2 (continued)
The virtual examination
Range of Motion
• Hip abduction and adduction (frontal view)
• Hip flexion and extension (lateral view)
• Knee flexion and extension (lateral view)
Muscle Strength (frontal and lateral view)
• Single-leg knee bend
Seated or laying on
ground
Range of Motion (lateral view)
• Hip flexion and extension (side-lying or supine)
• Hip abduction and adduction (side-lying)
Muscle Strength (lateral view)
• Hip abduction (side-lying)
• Hip flexion (straight leg raise) (supine)
• Knee flexion (prone)
found 72% of included patients had bilateral
symptoms [13].
Muscular atrophy is an important finding to
identify in patellofemoral disorders. This can be
assessed virtually by assessing for side-to-side
differences between the symptomatic and contralateral leg. Atrophy can be assessed in the
seated, standing, or supine position. The use of
digital pixel measurements, aided by a browser
extension such as Page Ruler Redux (rocha.codes)
can be incorporated to detect subtle differences as
a percentage relative to the contralateral side
(Fig. 1). Vastus medialis oblique (VMO) atrophy
has been associated with a variety of patellofemoral disorders [15, 16], and discordant atrophy
between the VMO and vastus lateralis has been
shown contribute to lateral patellar instability [17].
In patients with patellar maltracking, patellar tilt
has been correlated with the differential activation
of the vastus lateralis and medialis [18]. VMO
inhibition has been noted to occur at smaller volumes than for other quadriceps muscles, resulting
in a dynamic quadriceps imbalance [19]. Identification of muscular atrophy can serve as the basis
for a targeted rehabilitation protocol.
Assessment for hypermobility should be performed using the Beighton scale [20]. During
scoring, one point per side is assigned for the
ability to extend each fifth metacarpophalangeal
joint beyond 90°, to touch each thumb to the
forearm with the wrist flexed, to hyperextend
each elbow beyond −10°, and to hyperextend
each knee beyond −10°, as well as one point for
the ability to place both palms flat on the floor
while standing with the knees extended. A score
of four or greater indicates hypermobility, which
may contribute to instability. A recent study
comparing 82 individuals with recurrent patellar
dislocation to age- and sex-matched controls
found those with a history of patellar dislocations
were more likely to have generalized joint laxity
(24% vs 10% of controls, P = 0.013) [21].
Among 174 patients who underwent isolated
MPFL reconstruction, 55.1% had a positive
Beighton score, although this was not found to
influence post-operative outcomes [22].
4
Lower Extremity Alignment
Assessment of lower extremity alignment is an
integral aspect of the patellofemoral exam, as the
presence of malalignment can contribute to
instability and pain [23]. For assessment of limb
alignment and symmetry, the patient should
assume a bipedal stance facing the camera with
equal distribution of weight between each foot
and toes pointing forward (Fig. 2). The presence
of “squinting patellae”, where the patellae appear
to be internally rotated, can indicate the presence
of excessive femoral anteversion or tibial torsion
[24].
The Q angle is the angle formed by the
intersection of two lines drawn from the anterior
Virtual Orthopaedic Examination in Patellofemoral Disorders
A
Fig. 1 Pixel measurements can aid in side-to-side
comparison of muscle bulk and can be described as a
percentage. In this image, the patient’s right thigh
A
769
B
measures 73 pixels (A) and the left thigh measures 69
pixels, indicating 95% symmetry (B)
B
Fig. 2 Standing alignment is assessed from both the frontal (A) and lateral (B) views
770
superior iliac spine (ASIS) to the center of the
patella and from the center of the patella to the
tibial tubercle. Genu valgum, lateralization of the
tibial tubercle, increased external tibial torsion,
and increased femoral anteversion can increase
the Q angle. The relationship between the Q
angle and patellofemoral disorders remains controversial [25–31] as it may be influenced by the
lack of standardization in how the Q angle is
measured. Consequently, Merchant and colleagues proposed a validated protocol for the
assessment of a “Standard Q Angle” to improve
inter- and intra-observer reliability [32]. During
the virtual examination, adaptation of this technique consists of measuring the Q angle using a
web-based goniometer with the patient in the
standing position facing the camera and the
patellae pointing forward. (Fig. 3). The patient
Fig. 3 The Q angle can be measured on the frontal
standing view as the angle between a line connecting the
anterior superior iliac spine (ASIS) to the midpoint of the
patella and another connecting the midpoint of the patella
to the tibial tubercle. Asking the patient to place their
thumb or index finger on the ASIS enables its
identification
C. L. Wright and M. J. Tanaka
can be asked to place their thumb or index finger
on their anterior superior iliac spine to aid in
obtaining this measurement. The patient should
be instructed to relax their quadriceps muscles
prior to measurements being taken. It should be
noted that lateral subluxation of the patella may
falsely decrease the Q angle measurement.
Assessment of hip range of motion can be
helpful in detecting rotational abnormalities. Hip
internal and external rotation can be measured
with the patient seated in a chair facing the
camera and the knees flexed to 90° (Fig. 4). The
addition of digital lines overlying the image may
assist in comparison of leg lengths, while muscular atrophy may again be assessed using
comparison of pixel measurements. Careful
attention should be paid to noting modifiable
asymmetries, which may be addressed through
treatment options such as orthotics or tailored
rehabilitation programs [6].
An assessment of patellar height, while commonly performed on radiographs, has also been
described clinically by noting whether the patella
faces superiorly (alta) or inferiorly (baja) while
viewing the knees of a seated patient from the
front with the knees in 90° of flexion [33]
(Fig. 5). Patella alta is an important risk factor
for instability as it hinders engagement of the
patella in the trochlear groove during early flexion (0–30°), predisposing to lateral subluxation
and tilt in extension [34]. While the severity of
patella alta is confirmed using radiographic
measurements, the presence of patella alta on
examination can help identify patients in whom
lower extremity malalignment may be contributing to their symptoms [35, 36].
Foot pronation, resulting in internal tibial
rotation, can affect dynamic patellofemoral
alignment [37] and has been shown to correlate
with patellofemoral pain [16, 38, 39]. Barton and
colleagues found individuals with PFPS demonstrated significantly greater foot pronation as
detected by longitudinal arch angle (effect size,
0.90) and foot posture index (effect size, 0.71)
[38]. Foot pronation may be assessed using
standing heel position or navicular drop, which
are adaptable to the virtual visit. Foot pronation
may be quickly assessed using hindfoot valgus
Virtual Orthopaedic Examination in Patellofemoral Disorders
A
771
B
Fig. 4 During seated range of motion testing, hip internal and external rotation can be measured with the knee at 90° of
flexion
with the patient facing away from the camera in
the bipedal standing position. To assess navicular
drop, the patient can mark the proximal aspect of
the navicular tuberosity on the symptomatic leg
(Fig. 6). The distance from the mark to the floor
should then be measured while the patient is
seated in a relaxed position with the foot resting
on the floor [39]. For adequate visualization, the
chair should be oriented 90° from the camera
with the medial aspect of the examined foot
facing the camera. The measurement is then
repeated in a weightbearing single leg stance,
using a chair or wall for balance only. While a
ruler or calibrated sheet of paper may serve as a
reference to enable more accurate measurements,
the proportion of navicular drop may provide an
estimate of foot pronation. Assessment of foot
pronation utilizing the navicular drop test has
been shown to have good inter- and intraobserver reliabilities (ICCs 0.73–0.91 [40];
ICCs > 0.86 [39]) and can identify a modifiable
risk factor that can be addressed through the use
of an orthotic support.
5
Gait
Assessment of gait from the front and back
allows for evaluation of antalgia, asymmetry,
stride length, patellar orientation, alignment, and
pelvic tilt. Assessing 6–8 stride lengths is generally sufficient and can be performed during the
virtual encounter, provided the encounter is
conducted in an area with adequate floor space
[6]. A shortened stance is suggestive of ipsilateral leg pain. Circumduction, which can be
assessed on either the frontal or posterior view,
may indicate difficulty with knee flexion. Pelvic
tilt, on the other hand, suggests contralateral hip
abductor weakness, which often results in
772
C. L. Wright and M. J. Tanaka
condyles, quadriceps tendon insertion, medial
and lateral patellar facets, and the medial and
lateral collateral ligaments. Tenderness over the
adductor tubercle (“Bassett’s sign”) is suggestive
of MPFL disruption at its femoral attachment
[43], which can be associated with patellar
instability. In their prospective observational
study of 23 patients with acute patellar dislocations, Sallay and colleagues noted a sensitivity of
70% for Bassett’s sign [44]. Tenderness may
guide providers in prognostication, as well. In
their randomized control trial of 112 patients
with PFPS, Hott and colleagues found an
increased number of pain locations correlated
with inferior 1-year outcomes [13].
7
Fig. 5 Digital markers placed at the proximal and distal
aspects of the patella, as well as at the proximal aspect of
the tibial tubercle, can aid in approximation of patellar
height
increased IT band tension [16]. In-toeing is
suggestive of femoral anteversion, which can
contribute to a lateralizing force on the patella
due to an external rotation moment at the knee
[41].
6
Palpation
Physician-guided palpation can be a useful
aspect of the virtual examination. Palpation is
ideally performed with the patient seated facing
the camera with their feet hanging freely [42]. As
in the in-person examination, physicians should
begin by asking patients to point to the area of
their pain with one finger before guiding them
through a series of palpation points. Instructions
mailed to the patient prior to the visit can provide
a helpful visual reference of where to identify
such points. Areas to be palpated include the
tibial tubercle and patellar tendon, medial and
lateral joint lines, medial and lateral femoral
Range of Motion
Virtual range of motion assessments can be
performed in either the standing, seated, or
supine position. With the patient in the standing
position facing the camera, the physician can
note hip range of motion in abduction and
adduction. From the lateral view, with the patient
facing 90° from the camera, the physician can
assess the flexion/extension arc of the hip and
knee. Knee hyperextension may be assessed by
asking the patient to push their knees posteriorly
while maintaining a bipedal stance. Patients who
have difficulty maintaining their balance may
hold on to a chair for stability. Alternatively, the
assessment may be performed in both the seated
and supine positions.
The seated position allows assessment of hip
internal and external rotation, hip flexion with
upper extremity assistance, knee flexion and
extension and evaluation of the presence of an
extensor lag. While oriented 90° from the camera, the lateral view may be utilized to visualize
knee extension, antigravity strength, and the
presence or absence of an extensor lag. Asking
the patient to bring the heel in toward the buttock
allows for flexion assessment. The lateral supine
position allows near full assessment of hip range
of motion as the patient ranges the superior hip
from maximal flexion sequentially to abduction,
extension, and adduction [16].
Virtual Orthopaedic Examination in Patellofemoral Disorders
B
A
Fig. 6 Navicular drop, a measure of foot pronation, can
be assessed by measuring the height of the navicular
tuberosity in the unloaded and loaded positions. In these
8
773
Muscle Strength and Functional
Testing
Assessment of strength remains a vital aspect of
the patellofemoral exam, as quadriceps weakness
[15, 45] and hip abduction, external rotation, and
extension weakness [46–49] have been demonstrated to be prevalent in patellofemoral disorders. While the virtual exam may be limited in
the ability to detect subtle weakness or side-toside differences in strength, particularly in
patients whose habitus or range of motion limitations limit participation, antigravity strength
remains an important aspect of the physical
exam. While knee extension is readily assessed
in the seated position, knee flexion (prone), hip
flexion (supine straight leg raise), and hip
abduction (lateral supine) are best assessed with
the patient lying on a couch or bed. Hip
images, navicular height measures 30 pixels in the
unloaded position and 23 pixels in the loaded position,
indicating a 23% change
extension strength may be assessed by asking the
patient to stand from the seated position without
utilizing upper extremity support [6] (Fig. 7).
Functional assessments of strength, which
may lend themselves to the virtual examination,
may be more predictive of patellofemoral disorders than manual strength testing [50]. When
assessing functional strength, Nunes and colleagues found patients with PFPS climbed stairs
more slowly and performed fewer consecutive
chair stands (by 12%), which can be assessed
during the virtual encounter. Stair climbing may
be simulated with step-up-step-down testing. The
utility of functional strength assessments is further supported by their high intra-rater reliability
and association with variations in pain scales
[51].
Numerous specialized tests for the evaluation
of functional strength, dynamic alignment/
tracking, and severity of symptoms are easily
774
C. L. Wright and M. J. Tanaka
latency in gluteus medius activation, decreased
hip abduction torque, and decreased lateral flexion force [52], which may contribute to symptomatology among patients with patellofemoral
symptoms [53].
9
Fig. 7 Hip extension strength can be tested by having the
patient transition from seated to standing without using
his or her upper extremities
adaptable to the virtual examination. A simple
squat and single-leg knee bend viewed from
anteriorly and laterally provide an assessment of
functional strength, lower extremity support
(core, hip, and quad strength and foot pronation),
dynamic patellar tracking, pain, and subjective
crepitus. Dynamic valgus alignment of the knee
and pelvic tilt can be identified during during this
maneuver (Fig. 8). The step-down test, which
simulates a single-leg squat similarly allows
assessment of balance, eccentric quadriceps
strength, dynamic alignment, and support. To
perform, the patient can be observed stepping
down off a small step first with one leg and then
the other. Crossley and colleagues demonstrated
good inter- and intra-rater reliability (k = 0.800–
0.600 and k = 0.800–0.613, respectively) when
utilizing the step-down test to evaluate hip
muscle dysfunction [52]. Providers assessed
overall functional movement with respect to
Patellar Tracking
Assessment of patellar tracking is an integral
component of any patellofemoral assessment.
The J sign represents lateralization of the patella
in knee extension, which reduces into the trochlear groove during early knee flexion (Fig. 9).
Tanaka and colleagues evaluated the correlation
between patellar maltracking identified on
dynamic kinematic computed tomography
(DKCT) with symptoms of patellar instability
among 76 knees [14]. They identified a J sign
pattern, with increased lateral translation of the
patella in knee extension, among 82% of individuals with patellar instability symptoms, with a
sensitivity of 93% among individuals who
demonstrated greater than three quadrants of
lateral patellar motion in extension.
Several studies have evaluated the ability to use
video assessment of knee flexion and extension to
assess patellar tracking with variable results.
Fujita and colleagues utilized video analysis to
quantify patellar tracking among 23 knees with
prior patellar dislocation, 23 asymptomatic contralateral knees, and 23 healthy controls [54].
Video-based measurements were able to successfully quantify patellar tracking, which was noted
to be similar between affected and unaffected
knees, as well as significantly different than
healthy controls at low flexion angles. Best and
colleagues, on the other hand, found orthopaedic
surgeons correctly identified patellar maltracking
in web-based video assessment of the J sign in
only 68% of cases (k = 0.45) when compared with
4DCT [55]. Future advances to improve the precision of J sign assessment may help better identify risk factors and prognoses in the evaluation
and treatment of patellar instability [35, 56–58].
Virtual Orthopaedic Examination in Patellofemoral Disorders
775
B
A
Fig. 8 Frontal and lateral views of the patient performing a single-leg squat can provide information regarding lower
extremity strength by evaluating for changes in coronal and sagittal alignment
A
B
Fig. 9 Patellar tracking can be assessed in the frontal
plane by having the patient extend (A) and flex (B and
C) the knee. The J sign is observed when the patellar
C
displaces laterally in extension and can be quantified by
quadrants of patellar motion
776
10
C. L. Wright and M. J. Tanaka
Patellar Apprehension
The patellar apprehension test was first described
by Fairbank in 1937, in which patients exhibited
apprehension when a laterally-directed force was
applied to the patella [59]. A positive result
occurs when there is verbal or non-verbal (e.g.
quadriceps contraction) expression of apprehension. Notably, expression of pain does not constitute a positive test. Although the test has been
shown to have limited sensitivity (<37%) [60]
and fair to moderate inter-rater reliability
(j = 0.30–0.65) [61], it has moderate specificity
(70–92%) [60]. Recently, Lamplot and colleagues described a modification of the apprehension test for the virtual examination [62]
(Fig. 10). While seated facing the camera,
patients should place the ankle of the extremity
being examined over the contralateral ankle,
maintaining the knee in 20–30° of flexion. They
should then use their thumbs to apply a laterally-
Fig. 10 Patellar apprehension can be evaluated in the
seated position with the ankle of the examined leg resting
on the contralateral ankle and the knee in 20–30° of
directed force to the patella while the provider
observes for any anxiety and evaluates nonverbal apprehension. Assessment of increased
translation, referred to as patellar glide and
measured in patellar quadrants, may be suggestive of injury to medial or lateral restraints.
Decreased translation, conversely, may be suggestive of lateral retinacular tightness or
arthrofibrosis. Despite limited sensitivity and
inter-observer reliability, the apprehension test
remains a mainstay for the evaluation of patellar
instability, as well as an outcome measure following patellar stabilization surgery.
11
Limitations to the Virtual
Examination
Despite efforts to describe adaptations to perform
a comprehensive patellofemoral examination
during the virtual visit, several limitations exist
flexion. The patient should then be assessed for verbal and
non-verbal apprehension while applying a laterallydirected force to the patella
Virtual Orthopaedic Examination in Patellofemoral Disorders
777
and should be communicated to the patient. 13 Take Home Points
Certain tests that require manipulation of the:
extremity or provocative testing, remain limited.
Additionally, the sensitivity, specificity, and Tips for a successful virtual examination
reliability of many of the virtually performed
Preparation
The virtual visit format, including
tests has not been established. Recent efforts to
payment policies, consent, technology
standardize the virtual examination can increase
requirements, and structure, should be
discussed at the time of scheduling to
the utility and reproducibility of this modality.
manage patient expectations
Additionally, the presence of incidental or
appropriately
unexpected findings in other areas of the body
A pre-visit instruction packet mailed
may not be easily identified through a focused
to the patient in anticipation of the
virtual examination. Confirmation of the virtual
visit, providing a detailed preparation
checklist and written or video
examination findings with an in-person clinical
instructions for examination
evaluation is recommended prior to proceeding
maneuvers, allows patients to prepare
with intervention.
for the visit and facilitates efficiency
Furthermore, while telehealth has the potential
A remote verification website enables
to improve access to care, it may also exacerbate
patients to confirm their setup meets
healthcare disparities for specific populations.
the audiovisual requirements in
advance of the visit, mitigating both
Individuals who lack access to necessary audioanxiety and inefficiencies
visual capabilities and reliable internet connecLoose fitting clothing exposing at
tions may not be able to participate in the virtual Set-up
least 3″ above the knee allows for
evaluation [4]. Those at increased risk include
appropriate visualization during the
older adults, individuals in rural communities,
exam
individuals with low household incomes, those
Adequate lighting with minimal
with limited education, or individuals with disbacklighting improves the provider’s
ability to detect subtle physical
ability. As physicians expand the use of teleexamination findings
medicine and further refine the virtual visit,
A moveable camera, in conjunction
specific attention to how to facilitate access to
with a swivel office chair or easily
care for all populations is necessary to avoid
moveable chair, allows for evaluation
compounding healthcare disparities.
in the frontal and lateral views
Examination
12
Conclusion
Telemedicine is a rapidly evolving field that
has expanded the reach of orthopaedic care.
Many components of the patellofemoral
examination can be adequately adapted to the
virtual examination, and incorporation of technological advances continue to improve the
capabilities of this modality. When performing a
virtual examination, adequate preparation by
both the patient and physician is critical for
optimizing efficiency and efficacy of the telemedicine visit.
A standardized sequence of
examination maneuvers designed to
limit transitions between the standing,
seated and supine positions improves
the efficiency of the virtual visit
(Table 2)
Physical examination findings should
be performed in a consistent manner
across patients to improve reliability
Critical interpretation of the
examination maneuvers should seek
to identify instability, which may be a
surgical indication. Examination
maneuvers that aid in identifying
instability include limb alignment, the
Q angle, the J sign, patellar
apprehension, and patellar glide test
(continued)
778
C. L. Wright and M. J. Tanaka
Tips for a successful virtual examination
After visit
Additional imaging studies are useful
adjuncts to the history and clinical
examination completed during the
virtual encounter. Limitations of the
virtual examination should be
discussed with the patient and inperson visits planned accordingly
9.
10.
11.
14
Key Message
When performing a virtual examination, adequate preparation by both the patient and physician is critical for optimizing efficiency and
efficacy of the telemedicine visit.
12.
13.
14.
References
1. Emara AK, Zhai KL, Rothfusz CA, Minkara AA,
Genin J, Horton S, et al. Virtual orthopaedic
examination of the lower extremity: the know-how
of an emerging skill. JBJS Rev. 2021;9(9).
2. Cottrell MA, O’Leary SP, Swete-Kelly P, Elwell B,
Hess S, Litchfield MA, et al. Agreement between
telehealth and in-person assessment of patients with
chronic musculoskeletal conditions presenting to an
advanced-practice physiotherapy screening clinic.
Musculoskelet Sci Pract. 2018;38:99–105.
3. Services USCfMM. CMS adult electivesurgery and
procedures recommendations: limit all non-essential
plannedsurgeries and procedures, including dental,
until further notice.
4. King D, Emara AK, Ng MK, Evans PJ, Estes K,
Spindler KP, et al. Transformation from a traditional
model to a virtual model of care in orthopaedic
surgery: COVID-19 experience and beyond. Bone Jt
Open. 2020;1(6):272–80.
5. Crawford AM, Lightsey HM, Xiong GX, Striano BM,
Schoenfeld AJ, Simpson AK. Telemedicine visits
generate accurate surgical plans across orthopaedic
subspecialties. Arch Orthop Trauma Surg. 2021.
6. Tanaka MJ, Oh LS, Martin SD, Berkson EM.
Telemedicine in the era of COVID-19: the virtual
orthopaedic examination. J Bone Joint Surg Am.
2020;102(12): e57.
7. Ferriero G, Vercelli S, Sartorio F, Muñoz Lasa S,
Ilieva E, Brigatti E, et al. Reliability of a smartphonebased goniometer for knee joint goniometry. Int J
Rehabil Res. 2013;36(2):146–51.
8. Dent PA, Wilke B, Terkonda S, Luther I, Shi GG.
Validation of teleconference-based goniometry for
15.
16.
17.
18.
19.
20.
21.
22.
23.
measuring elbow joint range of motion. Cureus.
2020;12(2): e6925.
Mehta SP, Kendall KM, Reasor CM. Virtual assessments of knee and wrist joint range motion have
comparable reliability with face-to-face assessments.
Musculoskeletal Care. 2021;19(2):208–16.
Russell TG, Jull GA, Wootton R. Can the internet be
used as a medium to evaluate knee angle? Man Ther.
2003;8(4):242–6.
Russo RR, Burn MB, Ismaily SK, Gerrie BJ, Han S,
Alexander J, et al. Is digital photography an accurate
and precise method for measuring range of motion of
the hip and knee? J Exp Orthop. 2017;4(1):29.
Russo RR, Burn MB, Ismaily SK, Gerrie BJ, Han S,
Alexander J, et al. Is digital photography an accurate
and precise method for measuring range of motion of
the shoulder and elbow? J Orthop Sci. 2018;23
(2):310–5.
Hott A, Brox JI, Pripp AH, Juel NG, Liavaag S.
Predictors of pain, function, and change in patellofemoral pain. Am J Sports Med. 2020;48(2):351–8.
Tanaka MJ, Elias JJ, Williams AA, Demehri S,
Cosgarea AJ. Characterization of patellar maltracking
using dynamic kinematic CT imaging in patients
with patellar instability. Knee Surg Sports Traumatol
Arthrosc. 2016;24(11):3634–41.
Pattyn E, Verdonk P, Steyaert A, Vanden Bossche L,
Van den Broecke W, Thijs Y, et al. Vastus medialis
obliquus atrophy: does it exist in patellofemoral pain
syndrome? Am J Sports Med. 2011;39(7):1450–5.
Post WR. Clinical evaluation of patients with
patellofemoral disorders. Arthroscopy. 1999;15
(8):841–51.
Petrera M, Dwyer T, Gobbi A. Patellofemoral
Instability. Berlin, Heidelberg: Springer Berlin Heidelberg;2014. p. 59–66.
Pal S, Besier TF, Draper CE, Fredericson M,
Gold GE, Beaupre GS, et al. Patellar tilt correlates
with vastus lateralis: vastus medialis activation ratio
in maltracking patellofemoral pain patients. J Orthop
Res. 2012;30(6):927–33.
Spencer JD, Hayes KC, Alexander IJ. Knee joint
effusion and quadriceps reflex inhibition in man.
Arch Phys Med Rehabil. 1984;65(4):171–7.
Beighton P, Horan F. Orthopaedic aspects of the
Ehlers-Danlos syndrome. J Bone Joint Surg Br.
1969;51(3):444–53.
Nomura E, Inoue M, Kobayashi S. Generalized joint
laxity and contralateral patellar hypermobility in
unilateral recurrent patellar dislocators. Arthroscopy.
2006;22(8):861–5.
Hiemstra LA, Kerslake S, Kupfer N, Lafave MR.
Generalized joint hypermobility does not influence
clinical outcomes following isolated MPFL reconstruction for patellofemoral instability. Knee Surg
Sports Traumatol Arthrosc Off J ESSKA. 2019;27
(11):3660–7.
Brattstroem H. Shape of the intercondylar groove
normally and in recurrent dislocation of patella.
Virtual Orthopaedic Examination in Patellofemoral Disorders
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
A clinical and x-ray-anatomical investigation. Acta
Orthop Scand Suppl. 1964;68(Suppl 68):1–148.
Miller MD. Patellofemoral joint disorders. In:
Orthopaedic knowledge update: sports medicine,
5th ed. Wolters Kluwer Health; 2018. p. 205–20.
Aglietti P, Insall JN, Cerulli G. Patellar pain and
incongruence. I: Measurements of incongruence.
Clin Orthop Relat Res. 1983(176):217–24.
Rauh MJ, Koepsell TD, Rivara FP, Rice SG,
Margherita AJ. Quadriceps angle and risk of injury
among high school cross-country runners. J Orthop
Sports Phys Ther. 2007;37(12):725–33.
Thomeé R, Renström P, Karlsson J, Grimby G.
Patellofemoral pain syndrome in young women. I. A
clinical analysis of alignment, pain parameters,
common symptoms and functional activity level.
Scand J Med Sci Sports. 1995;5(4):237–44.
Caylor D, Fites R, Worrell TW. The relationship
between quadriceps angle and anterior knee pain
syndrome. J Orthop Sports Phys Ther. 1993;17
(1):11–6.
Freedman BR, Brindle TJ, Sheehan FT. Reevaluating the functional implications of the Qangle and its relationship to in-vivo patellofemoral
kinematics. Clin Biomech (Bristol, Avon). 2014;29
(10):1139–45.
Sheehan FT, Derasari A, Fine KM, Brindle TJ,
Alter KE. Q-angle and J-sign: indicative of maltracking subgroups in patellofemoral pain. Clin
Orthop Relat Res. 2010;468(1):266–75.
Messier SP, Davis SE, Curl WW, Lowery RB,
Pack RJ. Etiologic factors associated with patellofemoral pain in runners. Med Sci Sports Exerc.
1991;23(9):1008–15.
Merchant AC, Fraiser R, Dragoo J, Fredericson M.
A reliable Q angle measurement using a standardized
protocol. Knee. 2020;27(3):934–9.
Sankineani SR, Karnatzikos G, Chaurasia S,
Gobbi A. Clinical examination of the patellofemoral
joint. Berlin, Heidelberg: Springer Berlin Heidelberg;2014. p. 23–7.
Ward SR, Terk MR, Powers CM. Patella alta:
association with patellofemoral alignment and
changes in contact area during weight-bearing.
J Bone Joint Surg Am. 2007;89(8):1749–55.
Sappey-Marinier E, Sonnery-Cottet B, O’Loughlin P,
Ouanezar H, Reina Fernandes L, Kouevidjin B, et al.
Clinical outcomes and predictive factors for failure
with isolated MPFL reconstruction for recurrent
patellar instability: a series of 211 reconstructions
with a minimum follow-up of 3 years. Am J Sports
Med. 2019;47(6):1323–30.
Caton JH, Dejour D. Tibial tubercle osteotomy in
patello-femoral instability and in patellar height
abnormality. Int Orthop. 2010;34(2):305–9.
Tiberio D. The effect of excessive subtalar joint
pronation on patellofemoral mechanics: a theoretical
model. J Orthop Sports Phys Ther. 1987;9
(4):00160–5.
779
38. Barton CJ, Bonanno D, Levinger P, Menz HB. Foot
and ankle characteristics in patellofemoral pain
syndrome: a case control and reliability study.
J Orthop Sports Phys Ther. 2010;40(5):286–96.
39. Mølgaard C, Rathleff MS, Simonsen O. Patellofemoral pain syndrome and its association with hip,
ankle, and foot function in 16- to 18-year-old high
school students: a single-blind case-control study.
J Am Podiatr Med Assoc. 2011;101(3):215–22.
40. Sell KE, Verity TM, Worrell TW, Pease BJ, Wigglesworth J. Two measurement techniques for
assessing subtalar joint position: a reliability study.
J Orthop Sports Phys Ther. 1994;19(3):162–7.
41. Lee TQ, Yang BY, Sandusky MD, McMahon PJ.
The effects of tibial rotation on the patellofemoral
joint: assessment of the changes in in situ strain in the
peripatellar retinaculum and the patellofemoral contact pressures and areas. J Rehabil Res Dev. 2001;38
(5):463–9.
42. Bickley LS, Szilagyi P. Bates’ guide to physical
examination and history taking. Philadelphia: Wolters Kluwer Health. 13th ed.; 2020. p. 745–840.
43. Bassett F. Acute dislocation of the patella, osteochondral fractures, and injuries to the extensor
mechanism of the knee. Instr Course Lect.
1976;25:40–9.
44. Sallay PI, Poggi J, Speer KP, Garrett WE. Acute
dislocation of the patella. A correlative pathoanatomic study. Am J Sports Med. 1996;24(1):52–60.
45. Thomeé R, Renström P, Karlsson J, Grimby G.
Patellofemoral pain syndrome in young women. II.
Muscle function in patients and healthy controls.
Scand J Med Sci Sports. 1995;5(4):245–51.
46. Ireland ML, Willson JD, Ballantyne BT, Davis IM.
Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33
(11):671–6.
47. Piva SR, Fitzgerald K, Irrgang JJ, Jones S, Hando BR,
Browder DA, et al. Reliability of measures of
impairments associated with patellofemoral pain
syndrome. BMC Musculoskelet Disord. 2006;7:33.
48. Cichanowski HR, Schmitt JS, Johnson RJ,
Niemuth PE. Hip strength in collegiate female
athletes with patellofemoral pain. Med Sci Sports
Exerc. 2007;39(8):1227–32.
49. Nunes GS, Barton CJ, Serrão FV. Hip rate of force
development and strength are impaired in females
with patellofemoral pain without signs of altered
gluteus medius and maximus morphology. J Sci Med
Sport. 2018;21(2):123–8.
50. Nunes GS, de Oliveira SD, Crossley KM, Serrão FV,
Pizzari T, Barton CJ. People with patellofemoral pain
have impaired functional performance, that is correlated to hip muscle capacity. Phys Ther Sport.
2019;40:85–90.
51. Loudon JK, Wiesner D, Goist-Foley HL, Asjes C,
Loudon KL. Intrarater reliability of functional performance tests for subjects with patellofemoral pain
syndrome. J Athl Train. 2002;37(3):256–61.
780
52. Crossley KM, Zhang WJ, Schache AG, Bryant A,
Cowan SM. Performance on the single-leg squat task
indicates hip abductor muscle function. Am J Sports
Med. 2011;39(4):866–73.
53. Nunes GS, Stapait EL, Kirsten MH, de Noronha M,
Santos GM. Clinical test for diagnosis of patellofemoral pain syndrome: systematic review with metaanalysis. Phys Ther Sport. 2013;14(1):54–9.
54. Fujita Y, Tsuda E, Yamamoto Y, Naraoka T,
Kimura Y, Sasaki S, et al. Quantitative analysis of
dynamic patellar tracking in patients with lateral
patellar instability using a simple video system.
Knee. 2016;23(4):604–9.
55. Best MJ, Tanaka MJ, Demehri S, Cosgarea AJ. Accuracy and reliability of the visual assessment of patellar
tracking. Am J Sports Med. 2020;48(2):370–5.
56. Zhang Z, Zhang H, Song G, Wang X, Zhang J,
Zheng T, et al. A High-grade J sign is more likely to
yield higher postoperative patellar laxity and residual
maltracking in patients with recurrent patellar dislocation treated with derotational distal femoral
osteotomy. Am J Sports Med. 2020;48(1):117–27.
57. Zhang Z, Zhang H, Song G, Zheng T, Feng H. A preoperative grade 3 J-sign adversely affects short-term
C. L. Wright and M. J. Tanaka
58.
59.
60.
61.
62.
clinical outcome and is more likely to yield MPFL
residual graft laxity in recurrent patellar dislocation.
Knee Surg Sports Traumatol Arthrosc. 2020;28
(7):2147–56.
Milinkovic DD, Jovandic I, Zimmermann F, Balcarek P. The J-sign and the body mass index
determine the disease-specific quality of life in
patients with lateral patellar instability. Knee Surg
Sports Traumatol Arthrosc. 2021.
Fairbank HA. Internal derangement of the knee in
children and adolescents: (section of orthopaedics).
Proc R Soc Med. 1937;30(4):427–32.
Cook C, Mabry L, Reiman MP, Hegedus EJ. Best
tests/clinical findings for screening and diagnosis of
patellofemoral pain syndrome: a systematic review.
Physiotherapy. 2012;98(2):93–100.
Hiemstra LA, O’Brien CL, Lafave MR, Kerslake S.
Common physical examination tests for patellofemoral
instability demonstrate weak inter-rater reliability.
Arthrosc Sports Med Rehabil. 2021;3(3):e673-7.
Lamplot JD, Pinnamaneni S, Swensen-Buza S,
Lawton CD, Dines JS, Nawabi DH, et al. The virtual
shoulder and knee physical examination. Orthop J
Sports Med. 2020;8(10):2325967120962869.
Epilogue
The pathology of the patellofemoral joint has been
a major concern amongst the orthopaedic community, with a high prevalence in the athletic and
general population. Anterior knee pain and patellar
instability often creates diagnostic and treatment
challenges to the orthopaedic surgeon, with recalcitrant and enigmatic cases that are difficult to
resolve. The pathophysiology of these challenging
cases is nowadays more comprehensively—but not
fully—understood under multifactorial models
(anatomical,
biomechanical,
neuromuscular,
genetic, psycho-emotional, environmental and
socioeconomic factors) of complex interplay of the
diverse
contributing
modifiable
and
non-modifiable risk factors. Recent predictive
diagnostic models into the brain network functional connectivity of patients with anterior knee
pain is also shedding some light on the pathways
and drivers of pain which can help explain why in
a subgroup of patients with structural abnormalities, some have pain and others do not, as well as
to potential links to other predisposing factors.
A manyfold of new research developments have
also contributed to significant and important
advances in the diagnosis, management and treatment of patellofemoral pathological conditions.
The available diagnostic options are today more
advanced, reliable and precise. Not only we have a
more complete understanding of the several contributing factors, but we are also better equipped to
assess their prevalence and potential impact on the
patellofemoral joint. Emerging techniques are now
available that can help the orthopaedic surgeon in
the diagnosis process, as well as in the
decision-making of the best course of treatment
and better plan surgical procedures.
With recent events, the relevance and usefulness
of virtual consultation and tele-rehabilitation has
gain ground and have become increasingly popular. The recent developments on virtual orthopaedic examination will play an important role in the
future, allowing clinicians to reach a wider range
of patients that, for many different reasons, are not
available to attend physical consultations. This will
be one of the stepping-stones for higher equity in
the access for high-quality medical orthopaedic
services for the population.
Dynamic CT enhances our diagnostic arsenal
and helps us to better measure the individual
contribution of anatomic and pathomechanic factors on the course of patellar tracking during the
full knee range of motion. The dynamic 3D CT
will improve our ability to identify which biomechanical deficiencies that need to be corrected and
which are the most adequate surgical approaches to
restore normal patellar tracking. This technique
can also be used postoperatively to evaluate the
results of the different patellofemoral corrective
techniques.
Instrumented evaluation of patellofemoral laxity
is also an important step to dynamically assess
patellofemoral instability. These devices have the
potential to overcome the limitations of measuring
laxity during physical examination (qualitative
assessment under manual exam) and available
imaging procedures (which are mostly static
evaluations). The Porto Patellofemoral Testing
Device (PPTD) has emerged as clinically relevant
tool to standardly quantify patellar position and
displacement under external stress to the patella.
The compatibility of the PPTD with CT and MRI
offers the clinician a device able to measure
patellofemoral laxity with high reliability, accuracy and precision, and with low intra- and
inter-individual variability. The PPTD has shown
clinical application in identifying anatomic and
pathomechanic factors in both anterior knee pain
and patellar instability. It can also be a helpful tool
in evaluating any residual laxity after corrective
surgery and better understand the surgical outcomes of the available surgical techniques.
The use of finite element modelling (FEM) allows to evaluate the kinematic behavior of patellofemoral joint and simulate morphological
changes of different pathological conditions using
patient-specific models. The FEM helps the clinician to better understand the contributing factors
that causing the patellofemoral disorder, it has its
most relevant potential to improve the surgical
approaches. Using FEM, orthopaedic surgeons can
© The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature
Switzerland AG 2023
V. Sanchis-Alfonso (ed.), Anterior Knee Pain and Patellar Instability,
https://doi.org/10.1007/978-3-031-09767-6
781
782
better prepare their surgical planning by simulating
different techniques and fixation points under the
patient-specific morphology, which will individualize the surgical procedure to the specific needs of
each individual.
Several clinically relevant advances have also
been accomplished in surgical techniques for
patellofemoral disorders. Although patellar cartilage injuries still pose a challenge to orthopaedic
surgeons, we have today a larger range of available
and advanced techniques to deal with chondral and
osteochondral patellar lesions and thus to treat the
patient’s symptoms and associated disability, while
aiming to prevent further damage to the cartilage
and delay the early onset of osteoarthritis. With
enhanced understanding of the medial patellofemoral ligament complex of the previously neglected role of the medial quadriceps-tendon femoral
ligament (MQTFL) and the individual contributions of other relevant ligamentous structures
(medial patellotibial and medial patellomeniscal
ligaments) has also nudged orthopaedic surgeons to
innovate and improve their surgical techniques of
Epilogue
MPFL reconstruction. Robotic-assisted surgery is
already a reality and something to eagerly look for
in the future to improve the outcomes of patellofemoral replacement.
The path to better manage patellofemoral disorders may still be tortuous and often enigmatic,
but with recent developments in this field, the
future that lies ahead it is also bright. The key for
improved care will rely on better understanding of
the several predisposing factors that interplay in
the physiopathology of patellofemoral disorders
and in the individualization of treatment to the
patient-specific needs. We keenly look forward for
what the future may hold…
João Espregueira-Mendes, MD Ph.D., Porto,
Portugal.
Director of Clínicas Espregueira – FIFA Medical
Centre of Excellence.
Vice-President of ISAKOS.
President of ESSKA 2012–2014.